
2
Keynote Presentations
DEMENTIA CARE: GETTING IT RIGHT FOR EVERYONE
David Reuben, director of the University of California-Los Angeles (UCLA) Alzheimer’s disease and dementia care program and director of UCLA’s Multi-campus Program in Geriatric Medicine and Gerontology, offered an overview of dementia and dementia care in the United States. He began by explaining that dementia is an umbrella term for loss of memory and other thinking abilities that reaches a level of severity sufficient to interfere with daily life. Alzheimer’s disease (AD) is responsible for 60 to 80 percent of all dementias, with the remaining cases attributable to Lewy body dementia, vascular dementia, frontotemporal dementia, or other neurological disorders, such as Parkinson’s and Huntington’s diseases. Multiple disorders may coexist in the same individual, producing mixed dementia. AD affects 5 percent of individuals age 65 to 74, 13 percent of those age 75 to 84, and 33 percent of those age 85 and older (Alzheimer’s Association, 2022). The number of people diagnosed with AD is expected to reach 7.2 million by 2025 (Alzheimer’s Association, 2022). Reuben noted that rates of AD diagnosis are higher in people who identify as Black or Latinx than in those that identify as White or not Latinx (Alzheimer’s Association, 2022).
Reuben explained that in 2011, the National Institute on Aging (NIA) and the Alzheimer’s Association redefined AD to recognize three distinct stages of disease, which may be distinguished by biomarkers (Alzheimer’s Association, 2022). The first stage is referred to as the preclinical stage, progression from which is defined by changes in certain biomarkers (as compared to individuals with normal cognition). The second stage is referred to as mild
cognitive impairment (MCI) and is characterized by impairment in cognition mild enough to preserve overall function, and biomarkers of AD may be present. The third stage, dementia, is characterized by impairments in both cognition and function, and biomarkers may help to exclude AD as the cause of cognitive and functional impairment. In 2017, 46.7 million Americans were estimated to have positive biomarkers for one of these stages (McDade et al., 2020). The vast majority of these were in the preclinical or MCI stage (Brookmeyer et al., 2018). However, 10 to 15 percent of people with MCI convert to dementia each year, and roughly 50 percent convert in 5 years (Alzheimer’s Association, 2022). He emphasized that this represents a rapid progression of disease severity and prevalence.
Reuben explained that the natural history of AD is characterized by progressive cognitive decline, as measured by the Mini Mental State Examination, at a rate of approximately10 percent per year (Pangman et al., 2000). Approximately 30 to 50 percent of people with Alzheimer’s disease and related dementias (ADRD) experience non-cognitive symptoms (Masters et al., 2015). Those symptoms, including apathy, depression, agitation or aggression, sleep disorders, and delusions, can be very disruptive and last for years. Survival after the onset of symptoms is 3 to12 years (Larson et al., 2004; Ryman et al., 2014). The currently available tests for predicting AD are of reasonable quality and continue to improve, said Reuben. As methods of detecting dementia improve, so are strategies for managing the disease. Reuben expects the current modalities of detection, treatment, and support will be supplemented with risk factor identification, monitoring, and prevention by 2030. He compared the use of biomarkers to detect those at risk for AD to that of serum cholesterol and other blood biomarkers in the management of coronary artery disease as a model for disease prediction.
Reuben next highlighted the cost of ADRD care in relation to quality of care. Total annual payments for ADRD care are $321 billion as of 2022, of which $206 billion has been paid by Medicare and Medicaid (Alzheimer’s Association, 2022). Patients and families contribute about a quarter of that payment total ($81 billion) in the form of out-of-pocket payments (Alzheimer’s Association, 2022). People living with ADRD also receive a great deal of care that is not paid for by any entity. In 2021, unpaid caregivers provided approximately 16 billion hours of care, valued at $271.6 billion (Alzheimer’s Association, 2022). The average lifetime cost of care for a person living with ADRD is $371,621 (Alzheimer’s Association, 2022). He noted that despite its high cost, there is substantial opportunity for improvement in the quality of paid ADRD care, citing a published analysis that employed the Assessing Care of Vulnerable Elders (ACOVE-3) and Physician Consortium for Performance Improvement (PCPI) quality indicators (American Medical Association, 2011; Jennings et al., 2016; Wenger et al., 2007). This analysis graded the quality
of dementia care provided by community-based physicians at 38 percent; addition of a nurse practitioner increased quality to 60 percent (Reuben et al., 2019). However, adding a nurse practitioner or physician’s assistant who focused solely on dementia increased the quality of care grade to 92 percent (Jennings et al., 2016).
Reuben emphasized that dementia is a lifetime disease with no cure, which requires caregivers to adapt to the changing nature of their role, particularly related to decision making, as the disease progresses. During early disease, while the person living with dementia still has cognitive capacity to do so, they should be included in advance-care planning and other decision making, such as participation in clinical trials. He added that care goals during early disease should focus on maintaining the highest level of independence that is feasible for all involved (including the family and caregivers); treating the disease; managing potentially contentious issues, such as driving; managing symptoms; and managing comorbidities. In the later stages of disease, as cognition declines, families and caregivers must become responsible for making progressively more, and eventually all decisions.
Reuben explained that a caregiver is the most important person in the life of an individual with dementia. However, he said over 50 percent of caregivers develop depression. Several caregiver training and support programs have been found to reduce caregiver depression and increase the quality of care, such as Resources for Enhancing Alzheimer’s Caregiver Health II (REACH II);1 the New York University (NYU) Caregiver Intervention;2 and programs run by the Alzheimer’s Association (Belle et al., 2006; Gaugler et al., 2018).3 These programs have been found to enhance caregiver knowledge, well-being, and confidence; increase the duration of time from diagnosis to institutionalization; and reduce behavioral symptoms of people living with ADRD. However, Reuben also noted that there is a financial cost for these programs. They are not well integrated into health care systems, and further pragmatic testing is needed. He suggested that the additional pragmatic testing could be a good opportunity for collaboration with the NIA Impact Collaboratory.4
Reuben highlighted several new models of comprehensive ADRD care. Many of these models focus on the patient–caregiver dyad and are either community based, such as the Benjamin Rose Institute Care Consultation
___________________
1 See https://www.apa.org/pi/about/publications/caregivers/practice-settings/intervention/reach-protocol (accessed August 30, 2022).
2 See https://www.caregiver.org/resource/new-york-university-caregivers-program/ (accessed August 30, 2022).
3 See https://www.alz.org/help-support/caregiving (accessed July 5, 2022).
4 See https://impactcollaboratory.org (accessed July 5, 2022).
(BRICC),5 Johns Hopkins Maximizing Independence (MIND) at Home,6 and the University of California-San Francisco (UCSF) Care Ecosystem.7 Others are based in the health system, such as the Indiana University Healthy Aging Brain Center (HABC),8 the UCLA Alzheimer’s and Dementia Care Program (ADC),9 and Emory University’s Integrated Memory Care Clinic (IMCC)10 (Clevenger et al., 2018; French et al., 2014; Reuben et al., 2019). While each of these models differs in certain respects (see Table 2-1), they all employ what Reuben described as the essential pillars of comprehensive ADRD care:
- Continuous monitoring and assessment
- Ongoing care plans
- Psychosocial interventions for both people living with ADRD and caregivers
- Self-management
- Treatment of related conditions
- Coordination of care
Most of the models have been shown to benefit both patients and caregivers, and while they cost money to administer, they also produce savings. Despite their effectiveness, these programs are not widely available. Reuben cited several possible barriers that may be responsible for limited adoption. One challenge is the misaligned incentives that can occur when initial costs associated with implementation are not well reimbursed, and cost savings associated with the models are instead realized by stakeholders that did not invest in the implementation process. Other reasons that he cited for limited adoption of these models include the need to train practitioners; the need to identify, vet, and establish a payment stream for community-based partners; and inertia.
Reuben offered an example of the interaction between severity of ADRD and cost of care based on 2017 data from 5,000 patients living with ADRD in UCLA’s Population-Based Dementia Care Model. The model illustrates levels of dementia as a pyramid stratified by severity of disease (see Figure 2-1). The
___________________
5 See https://benrose.org/-/bricareconsultation (accessed July 5, 2022).
6 See http://www.mindathome.org (accessed July 5, 2022).
7 See https://memory.ucsf.edu/research-trials/professional/care-ecosystem (accessed July 5, 2022).
8 See https://www.eskenazihealth.edu/health-services/brain-center/aging-brain-care-program (accessed September 28, 2022).
9 See https://www.uclahealth.org/dementia/ (accessed July 26 2022).
10 See https://www.emoryhealthcare.org/centers-programs/integrated-memory-care-clinic/index.html (accessed September 28, 2022).
TABLE 2-1 Comparison of Select Dementia Care Models
| BRI CC | Care Ecosystem | MIND | HABC | UCLA ADC | IMCC | |
|---|---|---|---|---|---|---|
| Structure/process | ||||||
| Key personnel | SW, RN, MFT | Non-licensed APN, SW, pharmacist | Non-licensed RN, MD | Non-licensed MD, SW, RN, psychologist | NP, PA, MD | APN |
| Key personnel base | CBO | Community | Community | Health system | Health system | Health system |
| Face-to-face visits | No | No | Yes | Yes | Yes | Yes |
| Access 24/7/365 | No | No | No | Yes | Yes | Yes |
| Communication with PCP | Mail, fax | Fax, phone | Phone, mail, fax | EHR, phone, mail | EHR, phone | N/A |
| Order writing | No | No | No | Yes | Yes | Yes |
| Benefits | ||||||
| High quality of care | N/A | N/A | N/A | Yes | Yes | Yes |
| Patient benefit | Yes | Yes | Yes | Yes | Yes | NS |
| Caregiver benefit | Yes | Yes | Yes | Yes | Yes | NS |
| Costs of program | ++ | ++ | +++ | +++ | ++++ | ++++ |
| Cost savings,gross | ++ | ++ | None | ++ | ++++ | ++++ |
NOTE: + = represent qualitative estimates, with a single + representing the least and four + representing the most; Non-licensed = personnel that are not licensed professionals, but usually have a bachelor’s or master’s degree in a nonclinical area; APN = advanced practice nurse; CBO = community-based organization; EHR = electronic health record; MD = medical doctor; MFT = marriage and family therapist; NP = nurse practitioner; PA = physician assistant; PCP = primary care provider; RN = registered nurse; SW = social worker.
SOURCE: Presented by David Reuben on May 23, 2022, at Mechanisms for Organizational Behavior Change to Address the Needs of People Living with Alzheimer’s Disease and Related Dementias: A Workshop. Adapted from Lees Haggerty, K., G. Epstein-Lubow, L. H. Spragens, R. J. Stoeckle, L. C. Evertson, L. A. Jennings, and D. B. Reuben. 2020. Recommendations to improve payment policies for comprehensive dementia care. Journal of the American Geriatrics Society 68(11):2478-2485.
top of the pyramid represents the 1 percent of patients whose severe functional impairments, behavioral problems, and comorbidities require intensive individualized care that costs on average $186,000 annually. The cost of care for patients in the second tier averages $65,000 annually, while the cost of care for those in the third tier averages $20,000 annually. The patients in the second and third tier differ in their intensity of behavioral symptoms and hospital visits, but individuals in both tiers are likely to require a high- or low-intensity dementia care program, as well as neurological and psychiatric care. Patients in the fourth and fifth tiers typically have less intense behavioral symptoms and fewer hospital visits than those in the other three tiers and can rely on a less intensive and far less expensive dementia care program as well as caregiver education and monitoring. He noted that the fourth and fifth tiers of the pyramid may also represent an opportunity for incorporating referrals to community-based resources into patient care.
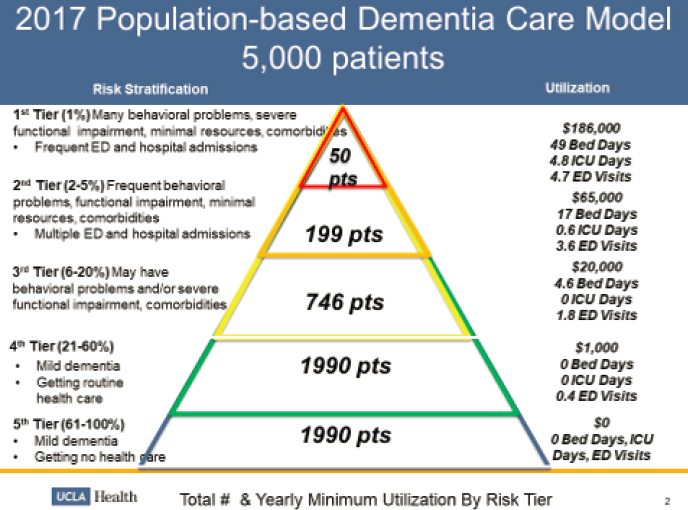
NOTE: ED = emergency department; pts = patients; ICU =intensive care unit.
SOURCE: Presented by David Reuben on May 23, 2022, at Mechanisms for Organizational Behavior Change to Address the Needs of People Living with Alzheimer’s Disease and Related Dementias: A Workshop. Adapted from “How A Population-Based Approach Can Improve Dementia Care,” Health Affairs Blog, May 8, 2019.
CONNECTING PAYMENT TO PRACTICE THROUGH MEDICARE
Meena Seshamani, director of the Center for Medicare at the Centers for Medicare and Medicaid Services, discussed its ongoing work and future opportunities to drive improvement in the quality of care for people with ADRD and support for their families and caregivers. She noted that Medicare has the power to propel systemic change due to the immense size of the program. Medicare covers 63 million people, including all Americans age 65 and older, as well as younger individuals with disabilities or end-stage renal disease. Medicare partners with more than one million clinicians and 6,000 hospitals and reimburses almost one trillion dollars in annual claims—about one in five health care dollars (CMS, 2022b). Approximately 11 percent of Medicare claims are for the care of people with ADRD (Hurd et al., 2013). She noted that these patients would benefit from a more holistic and less siloed approach to care.
Seshamani described Medicare’s vision for better serving people with ADRD, their families, and caregivers as being organized into several categories. The first category is a recommitment to advancing health equity (Seshamani and Jacobs, 2022; Seshamani et al., 2022). People from groups that have been historically made vulnerable and are lacking in resources are frequently systemically overlooked. She opined that to address inequity at the level of the Center for Medicare’s everyday operations it is essential that supporting those individuals remains central to operational decisions that affect system oversight, quality metrics, and navigability. The Center for Medicare is developing specific policies to address disparities in health care and to support health care organizations as they address those disparities. This includes designating 200 new physician residency slots in rural and underserved areas each year for the next five years (CMS, 2021).
The Center for Medicare is also seeking comment on a health equity index for Medicare Advantage insurance plans to ensure that those plans serve people from groups that have been historically made the most vulnerable (CMS, 2022a). Another category for Medicare’s vision is focused on access to coverage and care, which has particular relevance to people with AD. Medicare has been able to use reimbursement to facilitate the integration of cognitive screening into covered beneficiaries’ annual wellness visit. It is also seeking additional opportunities to use payments to encourage additional improvements in care, such as the integration of behavioral health care into primary care. She said the Center for Medicare is also considering strategies for using payments to achieve equity in behavioral health care and primary care, including address-
ing issues of language access and needs related to social determinants of health (social needs).
Seshamani explained that another category for Medicare’s vision involves innovations to create more holistic models that facilitate higher quality care for more people. Accountable care organizations (ACOs) will play a central role in those efforts. She noted that ACOs emphasize a team-based holistic approach to care while attaining high quality metrics and generating shared cost savings. The Center for Medicare aims to bring all beneficiaries of traditional Medicare into an ACO by 2030. There will be a particular focus on increasing participation in ACOs in rural and underserved areas. However, she noted that improved quality of care for people with ADRD requires more than enrolling providers in these models. Therefore, the Center for Medicare is seeking to develop partnerships that will support those who care for people with ADRD. Opportunities to accomplish this include possible partnerships with the Health Resources and Services Administration (HRSA) and the Centers for Disease Control and Prevention (CDC) that could fund innovations on the community level that advance whole-person care for people with ADRD. She also noted that in order to increase momentum for system change, social services, health care, other support services, foundations and government grant makers, resources from ACO learning communities, and funding streams within CMS itself all need to be in alignment.
Seshamani emphasized the importance of research partnerships, noting the power of research tools to evaluate changes and reveal inequities that have emerged during the COVID-19 pandemic, such as the expansion of telehealth, the use of community health workers, and integration of public health into the traditional health care system. Research can identify areas where these changes were effective and what may need to be modified to make some changes more effective. Seshamani noted that researchers should evaluate every program change against the goals of advancing equity, furthering whole-person care, stewarding Medicare (reducing waste, fraud, and abuse), and preventing future complications. Finally, Seshamani encouraged an approach to care that extends beyond the medical office or hospital to include family, community, and social needs, in a manner that leads to better care, smarter spending, and improved health.
DISCUSSION
Addressing the Most Urgent Needs in ADRD Care
Richard Frank began the discussion by asking what evidence is needed to understand which policy levers are most crucial to facilitate systemic change to support improved quality of care for people with ADRD. Reuben responded
that payment policy directed at improving quality of care should be comprehensive, instead of focusing on discrete services, and include nontraditional types of care to address the many services frequently needed by people with ADRD that are not covered by insurers. He noted that legislation has been introduced in the U.S. Congress related to the Center for Medicare and Medicaid Innovation (CMMI) studying alternative approaches for financing ADRD care. He added that care for people with ADRD requires a different approach than that applied to many other diseases, due to the inability of many patients to participate in their own decision making and the tremendous psychosocial and behavioral complications associated with ADRD. Seshamani added that several considerations should be evaluated prior to the large-scale implementation of new approaches, such as the movement of more care into the home setting that occurred during the COVID-19 pandemic. These considerations include identifying the target patient population, clarifying how the change will affect patient well-being, the patient’s family members and other caregivers, patient-reported outcomes, health care outcomes, health care utilization, and health care spending.
Addressing Systemic Health Inequities
Jennie Chin Hansen asked how CMS could address the significant effect of ADRD on Black people that are dually eligible for Medicare and Medicaid, noting that people in this group have historically faced barriers to economic stability and health care inequities. Seshamani noted that Black people enrolled in Medicare have a higher rate of ADRD than other populations. She explained that addressing Medicare’s daily operations with a focus on culture, language, and the environment in which a person is living while they are receiving care will help to address general issues of health inequity as well as the greater effects of ADRD on Black people. She noted that the CMS expansion of graduate medical education (GME) residencies in underserved areas reflects an effort to bring providers to settings where they are most needed. She added that CMS will gauge the effect of innovations on quality of care for Black enrollees in part through race and ethnicity data collected as part of Medicare Advantage and Medicare Part D enrollment.
Reuben noted health equity is a significant issue for caregivers and communities. People living with AD and their families frequently receive substantial support from their communities, which highlights the important role of ethnicity and culture, including local culture in ADRD care. He added that the important role of community support highlights the need for adequate reimbursement for the work done by community-based organizations. Bruce Vladeck, Greater New York Hospital Association and LiveOnNY, added that the workforce providing in-home care is disproportionately composed of
people of color that identify as female. He said their compensation, training, and working conditions represent a significant equity issue. Reuben agreed, adding that many paid caregivers are immigrants, and many lack health care benefits or insurance in addition to other challenges related to their immigration status, creating an “extraordinarily complicated issue, but one that we need to tackle.” Seshamani agreed on the importance of including caregivers in initiatives related to improving equity. She added that CMS, in cooperation with HRSA, has a role in efforts to support the health care workforce, including training and expanding the pipeline of future professional caregivers, and burnout prevention. She added that efforts should not overlook people she referred to as double caregivers, people that are employed as caregivers and also serve as caregivers at home.
Barriers to Innovation in Dementia Care
Sharon Inouye, Harvard Medical School and planning committee member, noted that effective models for ADRD care that reduce costs and improve quality of care exist and asked the speakers to address the major barriers to their implementation. Reuben began by explaining that he has spoken to 60 to 70 health care systems in his efforts to disseminate the UCLA Alzheimer’s and Dementia Care Program.11 He said that while many health care systems were generally supportive of the model and interested in its benefits, they were also concerned about the cost of the needed additional staff members, such as nurse practitioners. He described three common barriers to implementing these models. The first barrier, which he also mentioned in his presentation, is the initial cost of implementation, as the financial benefits of implementing these models are frequently accrued elsewhere in the health care system. The second barrier is the need to train practitioners, who are not often trained in this specific type of care. The third barrier is the need to provide adequate funding for community-based organizations to provide supports tailored to patients with ADRD and their families.
Seshamani, in response to the same question, explained the three types of authority that Medicare can engage to different degrees to facilitate adoption of these models (CMS, 2022c; Jaeger-Fine, 2020). The first is statutory authority. The Medicare program derives its authority via statute; some improvements require changes in the statute, which usually involve congressional action. The second is regulatory authority, as current statute gives Medicare regulatory authority. The third authority is direct effect on the provision of care by including support for training providers and caregivers, support for
___________________
11 See https://www.uclahealth.org/dementia/ (accessed July 26, 2022).
local community partnerships, and increased engagement with family caregivers, said Seshamani.
Funding Care at Home
Peter Hollmann, Brown University and Lifespan Health Alliance, asked if funding programs designed for people with developmental disabilities might offer useful lessons for funding at-home care for people living with ADRD, particularly whether an approach similar to the Katie Beckett Medicaid Waiver or merging Medicare and Medicaid could be possible solutions. Hollmann opined that one of the greatest challenges related to providing people with ADRD care at home is paying for care provided by community-based organizations and paying for the long-term support services that are generally considered the obligation of the patient and their family but are often prohibitively expensive. Seshamani said that the Medicare and Medicaid coordination office is considering opportunities to improve care for dually eligible individuals. She noted that CMS recently released a regulation that requires social needs screening for people that are dually eligible. She added that Medicare continues to partner with Medicaid to find opportunities to develop better aligned infrastructure to support care for people that are dually enrolled. Reuben noted that not everybody with ADRD is eligible to enroll in both Medicare and Medicaid because many people have an income that is just above the level that would allow them to be eligible for Medicaid. He added that funding gaps can be particularly problematic for those individuals. Reuben noted that additional research will be needed to determine the most effective approach for funding ADRD care and support provided by community-based organizations.
Sarah Lenz Lock, AARP and the Global Council on Brain Health, noted that most people with ADRD present to their health care providers with other comorbidities that their health care provider may prioritize over managing ADRD. She asked if addressing the cognitive and behavioral issues related to the patient’s ADRD before addressing other comorbidities could improve quality of care. Dr. Reuben explained that specialty care for those comorbidities, such as diabetes, hypertension, or chronic obstructive pulmonary disease (COPD) is important because it decreases the likelihood of hospitalization for people with ADRD. He added that those providers often lack the resources and expertise to adequately address ADRD. He noted this highlights the importance of coordinated dementia care models.
This page intentionally left blank.












