
3
Defining Quality
Terry Fulmer, The John A. Hartford Foundation (JAHF) and session moderator, noted in her introduction that identifying optimal approaches to facilitate systemic change to improve the quality of care for people with Alzheimer’s disease and related dementia (ADRD) will require collaboration among all organizations engaged in research efforts. Fulmer cited several JAHF initiatives to illustrate opportunities for foundations to collaborate with the National Institute on Aging (NIA), the Centers for Disease Control and Prevention (CDC), and health care systems to accelerate innovation for improving the quality of care for people with ADRD. These initiatives include
- dissemination and implementation of the evidence-based 4 Ms framework (what matters, medication, mentation, and mobility)1 in 2,900 geriatric care settings;
- improvement in emergency care with geriatric emergency department (GED) accreditation and a GED collaborative;
- a geriatric surgical verification program (Hwang et al., 2022);
___________________
1 What matters: understanding an individual patient’s health goals and care preferences across settings and aligning care (including but not limited to end-of-life care) with those goals and preferences. Medication: if medication is necessary, using age-friendly medications that do not hamper the other 3 Ms. Mentation: preventing, identifying, treating, and managing dementia, depression, and delirium across care settings. Mobility: ensuring older people move safely daily to sustain function and do the things identified in what matters (JAF, 2018).
- the recently released National Academies of Sciences, Engineering, and Medicine consensus study report, The National Imperative to Improve Nursing Home Quality;
- the UCLA Alzheimer’s and Dementia Care Program;
- Best Practice Caregiving,2 which provides free online resources to assist organizations and consumers to select evidence-based programs that support family caregivers; and
- the Milken Institute Alliance to Improve Dementia Care (NASEM, 2022).3
THE NATIONAL IMPERATIVE TO IMPROVE NURSING HOME QUALITY
Betty Ferrell, City of Hope, began the session with a discussion of the National Academies of Sciences, Engineering, and Medicine 2022 consensus study report, The National Imperative to Improve Nursing Home Quality: Honoring Our Commitment to Residents, Families, and Staff. Ferrell, who was the committee chair for the consensus study, explained that the project sought to “examine how our nation delivers, regulates, finances, and measures the quality of nursing home care [and] delineate a framework and general principles for improving the quality of care in nursing homes” (NASEM, 2022). The committee envisioned nursing home quality as follows: “Residents of nursing homes should receive care in a safe environment that honors their values and preferences, addresses goals of care, promotes equity, and assesses the benefits and risks of care and treatment” (NASEM, 2022). The consensus report included a robust discussion of inequities in nursing home care and noted that quality improvement measures must not exacerbate existing disparities. The development of the report included an 18-month process of weighing evidence and consulting with experts, family members of people residing in nursing homes, and residents of nursing homes. She said that the committee’s first conclusion was that the United States’ current approach to financing and delivering care in nursing homes “is ineffective, inefficient, fragmented, and unsustainable” (NASEM, 2022). Another conclusion noted the need for high-quality research to address quality-of-care issues. The committee also found that underinvestment in mechanisms to ensure quality of care and a lack of accountability related to resource allocation have had a negative effect on the nursing home sector.
Ferrell (with assistance from Terry Fulmer, due to technical issues) briefly described each of the report’s seven key goals that provide a framework for
___________________
2 See https://bpc.caregiver.org/#home (accessed July 26, 2022).
3 See https://milkeninstitute.org/centers/center-for-the-future-of-aging/alliance-to-improve-dementia-care (accessed September 28, 2022).
improving quality of care in nursing homes and highlighted pertinent recommendations for achieving those goals (a more detailed discussion of the consensus report goals and recommendations can be found in that report). The first goal is for nursing homes to provide care that is comprehensive, person centered, and equitable; ensures residents’ health, quality of life, and safety; promotes autonomy; and manages risks (NASEM, 2022). Recommendations to achieve this goal address care planning, models of care, emergency preparedness, and the physical environment. The second goal connects to the previous workshop discussion about the caregiving workforce. That goal is to ensure that the nursing home workforce is well prepared, empowered, and appropriately compensated (NASEM, 2022). She noted that this is essential for the delivery of high-quality care. Recommendations to achieve this goal emphasize competitive wages and benefits, staffing standards, empowering skilled nursing assistants, education and training, data collection, and research.
The third goal is to increase the transparency and accountability of nursing home finances, operations, and ownership (NASEM, 2022). A key recommendation for this goal is to collect, audit, and report detailed facility-level data. That data should be publicly available and easily searchable. The fourth goal is to develop a more “rational, robust financing system,” with a recommendation for research into establishing a federal long-term care benefit as well as exploring broader application of other alternative payment models, such as bundled payment (NASEM, 2022). The fifth goal is to design an effective and responsive system of quality assurance. Recommendations to achieve this goal address CMS oversight and support of state nursing home surveys as well as improved transparency and accountability (NASEM, 2022).
The sixth goal is to expand and enhance quality measurement and continuous quality improvement. Recommendations related to this goal call for improved measures of resident and family experience; enhancement and expansion of Care Compare; development and adoption of new quality measures; development of health equity strategies; as well as technical assistance for quality improvement (NASEM, 2022). The seventh goal is to adopt health information technology (HIT) in all nursing homes. Recommendations consider pathways to provide financial incentives for electronic health record (EHR) adoption; measures of HIT adoption and interoperability; perceptions of HIT usability; and training in core HIT competencies (NASEM, 2022).
Ferrell explained that the findings and recommendations included in the study also apply to improving quality of care for people with ADRD that reside in nursing homes. She added that the implications of the findings in the study should be regarded with an additional sense of urgency when considering how to best meet the needs of patients with ADRD. Since the report’s release in April 2022, members of the consensus study committee have presented the report’s conclusions and recommendations to several congressional commit-
tees and policy makers at all levels of government. They have also discussed the report with members of the media and members of the general public. She noted that these interactions have elicited a uniformly positive response, which highlights the importance of prompt action on the report’s findings.
DEFINING QUALITY
Dr. Eric Schneider is a health disparities researcher who now leads digital quality transformation at the National Committee for Quality Assurance (NCQA). NCQA accredits health plans and home- and community-based organizations, offers recognition programs for patient-centered medical homes and diabetes care, and provides awards of distinction that are awarded to health insurers that meet those standards. He contributed to the development of NCQA’s Healthcare Effectiveness Data and Information Set (HEDIS) performance measurement system,4 which was primarily developed for health insurers, and has since been repurposed for application to diabetes, cardiovascular disease, medication management, and other topics.
Schneider began with a personal story that illustrated several of the challenges that people with ADRD and their families can encounter in the health care system. His stepmother was living in an independent living community when the COVID-19 pandemic began. Over time she lost the ability to participate in video calls, which were her primary source of social interaction. Her condition continued to worsen, which resulted in her being transferred to the independent living community’s personal care unit. She then received numerous treatments for delirium, including medication, hospitalizations, and rehabilitation over the course of several months. However, she did not receive a full neurological evaluation until her delirium resolved and her worsened memory became more apparent. Schneider explained that he had observed patients and their families encounter similar experiences several times in his practice as a primary care physician. He noted that navigating the experience in the role of caregiver provided him with a new perspective.
Schneider explained that this experience illustrated several quality-of-care issues encountered by people with ADRD and their families. The first issue was that early stages of memory loss may not be noticeable to facility staff, which can lead to staff framing ADRD behavioral symptoms as intentional rather than a manifestation of the disease. Schneider noted that another issue was that his observations were frequently disregarded by facility staff. Additionally, he said the difficulties encountered while attempting to obtain a neuropsychiatric evaluation for his stepmother illustrated the urgent need to increase access to specialty care in rural areas. He also emphasized that when a person has a diagnosis of ADRD, proper and adaptive medication management is critical.
___________________
4 See https://www.ncqa.org/hedis/ (accessed on June 7, 2022).
Schneider said his stepmother’s experiences also highlighted the need for improved coordination of care for people with ADRD. The conceptual model from the National Academies National Imperative to Improve Nursing Home Quality (Figure 3-1) presents a well-structured quality model but is organization specific. He said that organization-specific quality models usually are not designed to address issues outside of the target organization. This includes areas that affect the quality of care for people with ADRD, such as gaps in coordination of care that extend outside of the institution, such as obtaining a primary care physician, accessing specialty care, and understanding health insurance coverage. This coordination occurs between organizations such as insurers, care delivery organizations, public health agencies, social service agencies, and community-based organizations, all of which interact with patients and caregivers. He noted that from the patient’s perspective, the root of gaps in quality of care originates with inadequate coordination among organizations and clinicians. This could be addressed through an approach similar to the patient-centered medical home that has been used to improve quality in primary care.
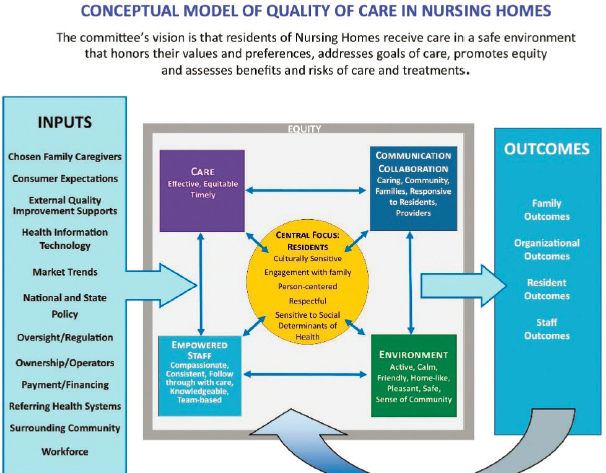
SOURCE: Presented by Eric Schneider, May 23, 2022, at Mechanisms for Organizational Behavior Change to Address the Needs of People Living with Alzheimer’s Disease and Related Dementias: A Workshop. Reproduced from National Academies of Sciences, Engineering, and Medicine. 2022. The National Imperative to Improve Nursing home quality: Honoring our commitment to residents, families, and staff. Washington, DC: The National Academies Press. https://doi.org/10.17226/26526.
Schneider provided an example of one such model that is centered on a stepwise approach to implementation (Figure 3-2). This approach begins with a foundation of a quality improvement strategy and engaged leadership. Then, each step requires specific fundamental components, such as empanelment and continuous and team-based healing relationships, to be in place before progressing to the next step. All of the fundamental components of the model must be in place to result in reduced barriers to care through improved access and coordination of care (Wagner et al., 2014).
Schneider proposed several accountability imperatives for the quality of care for people with ADRD. He described the first imperative, situational awareness, as the capability of all participants in the care of a person with ADRD to exchange data quickly so problems can be identified more quickly. Most quality measurement systems have relied on insurance claims data, which are usually reported several months after the episode of care and may not
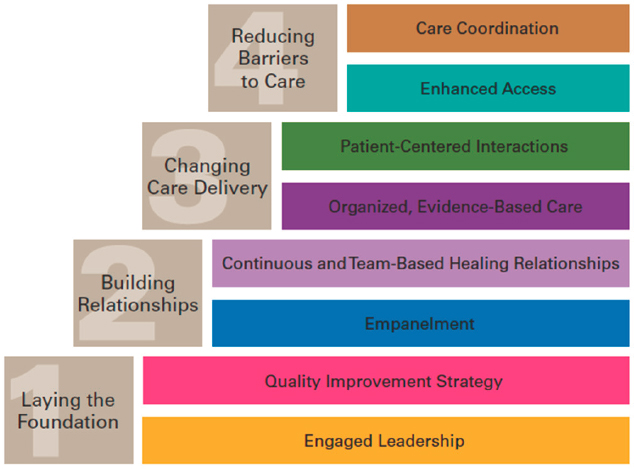
SOURCE: Presented by Eric Schneider, May 23, 2022, at Mechanisms for Organizational Behavior Change to Address the Needs of People Living with Alzheimer’s Disease and Related Dementias: A Workshop. Reprinted from Primary Care: Clinics in Office Practice, Vol. 39 Issue 2, Wagner, E. H., K. Coleman, R. J. Reid, K. Phillips, M. K. Abrams, J. R. Sugarman, The Changes Involved in Patient-Centered Medical Home Transformation, pp. 241-259, Copyright 2012, with permission from Elsevier.
include specific date and time information. That creates challenges for using these data to understand a sequence of events. Schneider emphasized that care coordination and effective communication among all involved are necessary. He noted this becomes particularly crucial as patients with ADRD experience disease progression, which can result in multiple transitions in where a patient lives and receives care. Quality metrics must be thoughtfully designed to avoid creating incentives for staff caring for patients with ADRD to act in ways that are counterproductive for the patient’s well-being. He offered an example of a quality metric for fall prevention that leads to staff reprimanding patients for standing up from their chairs. Data should be obtained on intermediate health outcomes, such as functional status, cognitive ability, and behavioral symptoms instead of prioritizing end-state outcomes. Quality measurement systems should also integrate care goal attainment in addition to the commonly used clinical measures, he said.
Schneider noted that the more timely and robust data exchange that he described requires improvements in the existing health care data infrastructure. NCQA is focused on expanding the use of electronic data in order to improve the information available for quality measurement. This work has gained momentum following passage of the 21st Century Cures Act,5 updated data exchange and interoperability regulations, and federal broadband investments. Schneider cautioned that while changing payment incentives is fundamentally necessary, additional strategies and investments may be necessary to attain needed digital infrastructure updates, systems reengineering, and other organizational changes.
QUALITY IN ADVANCED ADRD CARE TRANSITIONS
Lisa Gwyther, Duke School of Medicine and founder of the Duke Aging Center’s Dementia Family Support Program, discussed her experience navigating acute care transitions as a family caregiver with expertise in quality care for people with ADRD. Gwyther’s husband, Bob, a retired clinician and professor of family medicine, has advanced Lewy body dementia.
Gwyther described the quality indicators and systemic issues she observed when Bob experienced two transitions from a skilled nursing facility to different hospitals, one week apart, due to acute respiratory distress. During the first care transition, Gwyther and her husband experienced several benefits of
___________________
5 See https://www.congress.gov/bill/114th-congress/house-bill/34 and https://www.federalregister.gov/documents/2020/08/04/C2-2020-07419/21st-century-cures-act-interoperability-information-blocking-and-the-onc-health-it-certification (both accessed September 29, 2022).
systems that were designed to be dementia friendly. When the care transition occurred, a geriatrician on call at the skilled nursing facility recommended transfer to a hospital that had completed specific steps to be classified as dementia friendly. When Gwyther arrived at the hospital and explained to staff that her husband had dementia and could not be left unattended, she was quickly able to join her husband in the emergency department (ED). The staff at the dementia-friendly hospital had received specific training to support the unique needs of patients with ADRD and their family caregivers. The attending physician in the ED suggested that Gwyther consider completing a medical order for scope of treatment (MOST) form for end-of-life planning.6 When Bob returned to the skilled nursing facility, the speech therapist there observed Gwyther feeding Bob and posted notes for staff about how to help him eat and drink safely.
Gwyther also encountered several barriers to effective treatment for her husband during the first episode of care transitions. The ambulance emergency medical technicians (EMTs) initially resisted Gwyther’s hospital choice and argued for taking her husband to the closer academic medical center. Bob had to spend 3 days under NPO (nothing by mouth) orders while waiting for a swallowing evaluation because of procedural regulations and staff shortages at the hospital.
The second care transition from the skilled nursing facility to an ED illustrated several systemic problems that negatively affected quality of care. The ambulance EMTs took Bob to the nearby academic medical center ED, despite the MOST form on file at the skilled nursing facility and Gwyther’s wishes. Gwyther and her husband were kept separated at the ED for several hours due to that hospital’s COVID-19 protocols, which were not specifically designed in a dementia-friendly manner. When Lisa was able to join Bob in the ED, he was visibly upset. Gwyther then spent the next 12 hours negotiating a transfer to a dementia-friendly hospital, where he was later discharged 8 hours after admission.
Gwyther described several lessons learned through her experiences that could inform quality care for people with ADRD:
- The goals and preferences of the patient and family change depending on the circumstances.
- Clinicians should incorporate the family as a resource for understanding the patient’s goals, especially during care transitions.
___________________
6 See https://www.kymost.org/most-form-v2 (accessed on July 7, 2022).
- Quality dementia care should be led by clinicians and direct-care staff with geriatric and dementia-specific skills.
- Cordial, practiced working relationships between hospital discharge planners and skilled nursing facility clinicians are needed to ensure quality, safe transfers.
- Existing systems, structures, and protocols (such as an insistence on taking a patient with ADRD to the nearest hospital) may unintentionally negatively affect the quality of care for people with ADRD.
- Constant communication, checking mutual understandings, and timely action are keys to quality in dementia care transitions.
DISCUSSION
Lessons from Lived Experiences
Terry Fulmer began the discussion by asking Ferrell to reflect on Gwyther’s and Schneider’s experiences in relation to the National Academies nursing home consensus study. Ferrell began by noting that patients with ADRD frequently encounter disconnects in medical care. Those issues are often exacerbated without a family caregiver to advocate on the patient’s behalf. Ferrell explained that the nursing home consensus study report emphasized that quality care initiatives should begin by identifying the people who would be affected by those initiatives and considering how those initiatives would affect those people’s quality of life. She added that efforts to develop a model to improve quality of care for people with ADRD should ensure that quality care is not limited to those patients with the greatest resources. Schneider noted that despite relatively good circumstances, the dedicated and compassionate staff were unable to coordinate care across systems for Gwyther’s husband. He added that these challenges highlight the need for reengineering the health care ecosystem to reduce current fragmentation.
Schneider suggested that electronic data could be used for early detection of problems. Credit card companies rapidly identify irregular patterns that could indicate a problem such as fraud. Patient portal applications, such as MyChart, have the capability to send alerts to users. He suggested that if health care systems had a similar data monitoring and interpretation system in place to detect abnormalities, it could speed the delivery of appropriate care to address that issue. He noted that a patient being placed on NPO status for 3 days is an example of an abnormality that should raise an alert in an EHR just as unusual charges would raise an alert with a credit card company.
Gwyther said that while navigating a relative through dementia care is challenging, caregiver expectations should incorporate an understanding
of the challenging circumstances health care workers often encounter while providing care for people with ADRD. She added that having a caregiver who knows the patient well and a comprehensive care team can have a positive effect on quality of care. Fulmer highlighted the importance of personal stories, such as Gwyther’s and Schneider’s, in communicating the necessity of systemic change to improve the quality of care for people with ADRD to multiple audiences.
Reframing Reliance on EDs
Several participants noted that, in the current system, ED visits have become central to the care of individuals with ADRD. Vladeck explained that EDs are generally not ideal care settings for people with ADRD. He added that frequently the hospital ED where a patient with ADRD is transported to does not have a relationship with the physicians that manage the person’s care. He suggested that reducing reliance on EDs could be translated into a measurable quality-of-care indicator.
Culturally Responsive Quality
Faith Mitchell, Urban Institute, noted the disproportionately high rates of ADRD in the Black population, who have historically experienced health inequity. She added that most quality-of-care recommendations do not specifically address the contributors to that inequity, such as inadequate access, distrust, and language barriers. She asked how the discussion of strategies to improve quality of care could be better translated to more specifically address quality of care for people with ADRD that have experienced chronic health inequities.
Ferrell noted that health equity is integrated throughout the goals and recommendations in the National Academies of Sciences, Engineering, and Medicine consensus study report. Quality care should integrate culturally responsive care. Ferrell added that culturally responsive care requires practitioner training, and a strong recommendation of the report was to hold nursing homes accountable for this training. Schneider noted that NCQA is launching a redesigned health equity accreditation program. He explained that efforts to develop quality measures to address issues of distrust and unequal treatment should include engagement with communities. Schneider described the example of West Side United,7 a community-based organization in Chicago that collaborated with seven hospitals serving the people that live and work
___________________
7 See https://westsideunited.org/ (accessed September 29, 2022).
on the West Side of Chicago to identify key quality indicators and create joint accountability.
The Relationship Among Staffing, Training, Pay, and Care
Schneider remarked that at the time of the workshop, 30 to 40 of the staff at his stepmother’s skilled nursing facility were not at work because of COVID-19 infection, and he added that these settings were already understaffed and experienced high rates of staff turnover before the pandemic. He asked fellow participants to discuss possible approaches to address staffing issues in facilities that care for people with ADRD. Ferrell noted that the high nationwide rate of COVID-19 infections among nursing home staff are illustrative of broader safety issues in the industry. She explained that the high staff turnover rates in nursing homes affects quality of care and health equity because staff are less familiar with each resident and that person’s values and preferences. Staff compensation affects the ability to attract and retain qualified nursing home staff.
Ferrell also discussed the need to harness innovations in technology to develop quality, nationally disseminated training programs for nursing home staff. She emphasized that addressing core issues of staff pay, training, and retention is necessary to achieve improved quality of care. Several participants also noted the effects of labor shortages, most notably in nursing, on quality of care for people living with ADRD. Peter Hollmann, Brown University, noted the need to recognize the importance of long-term care, and the need to treat the people that work in that field as professionals. He opined that the nursing shortage is one of the most significant crises facing the United States.
Hollmann explained that fragmentation of the health care system has created substantial barriers for a patient care team to effectively cross care settings. He added that it is likely that a patient with ADRD who has been transferred several times among different care settings has also had to begin care with a new care team with each transfer. Gwyther added that this highlights the importance of a comprehensive, coordinated, and consistent care team that “becomes an expert in that individual” to improve quality of care for people with ADRD. She suggested that examples of quality team-based care can be used in training and scaled up from small settings. Schneider said quality care for people with ADRD should foster a team-based model of care that includes community caregivers along with professionals; provide training in these interactions; and disincentivize the adversarial relationship that can develop between different sectors when they are caring for people with ADRD.
Strategies to Reduce Stigma
Fulmer asked speakers to comment on the role of ageism in existing barriers to quality of care for people with ADRD. Gwyther noted, “I think that people think of older people as less interesting, less complicated than they really are, and less diverse than they really are.” She added that the Gerontological Society of America is working to reframe aging in a manner that is less stigmatizing, less discriminatory, and recognizes the diversity of the aging experience. Sarah Lenz Lock, AARP and Global Brain Health Initiative and a speaker in a later session of the workshop, suggested that education and training for younger health care providers may offer an opportunity to address some issues related to ageism. Those providers and their patients will benefit if the provider understands how to have conversations with patients about their priorities. Those providers should also understand that while ADRD does not currently have a cure, some challenges associated with the disease can be effectively addressed.
Fulmer noted the collaboration between JAHF and the Institute for Healthcare Improvement (IHI) on age-friendly health systems. A key component of that work is to center care on the 4 Ms—what matters, mentation, medication, and mobility, specific to each patient. Ferrell added that including social workers as part of the care team for patients with ADRD is helpful because they have skills and training to directly interact with patients and ensure that their identity and needs are preserved across the care continuum. She emphasized that high-quality care provided by qualified people in a safe environment is possible for people with ADRD, and family members should have that expectation. Sharon Inouye added that conversations about improving quality of care for people with ADRD are often accompanied by fear, hopelessness, and a sense of inevitability that create a sense of inertia around creating change. She noted that while this is a complex problem, there are many possible solutions, but that inertia must be overcome.
Creative Solutions for Quality Care
Elisabeth Belmont, MaineHealth and planning committee member, asked for speakers’ perspectives on the most effective payment model to promote quality care for people with ADRD. Schneider noted that the health care system is transitioning from fee-for-service reimbursement models to value-based contracting. That transition is another reason to ensure quality measurement systems are well designed. He cautioned against overestimating the improvements that could be achieved through an approach that relies only on financial incentives. He encouraged participants to consider approaches that incorporate infrastructure improvements and direct payments.
Julie Robison, University of Connecticut School of Medicine and planning committee member, noted that emergency medical service (EMS) companies, whose providers respond to 911 calls, are usually not reimbursed for care provided unless they transport the patient to a hospital. She asked speakers to share their thoughts about training EMS staff to provide care to people with ADRD in the patient’s home and changing reimbursement rules to support that approach. Schneider noted that he believed there were organizations that were investigating this approach. Fulmer described the variety of care providers and community organizations that could collaborate to provide care and support for people with ADRD and their caregivers. She offered an example from her home town in upstate New York. In that small town, if there is a significant staff shortage at the local hospital, the National Guard provides patient care. She added that while it can be unnerving to see the National Guard at the health care facility, they provide excellent care. Fulmer explained that in small towns, the first responder to a 911 call is usually a firefighter, who also lives in that town. Those local first responders are usually familiar with the people in their town who have a memory problem. Fulmer suggested that conversations about coordination of care for people with ADRD should include first responders. She added that another opportunity for collaboration is with community organizations, such as YMCAs and libraries, that are resources for adult day programs for people in preclinical or mild stages of ADRD. She emphasized that the United States has large infrastructures in place that could collaborate to improve care and support for people with ADRD, their families, and caregivers.
Schneider noted that caregivers should not be overlooked as sources of innovation because they often must find creative solutions to problems encountered when caring for a person with ADRD. He cited an example of an engineer who had a family member with health issues who used inexpensive components to create a motion detection system to alert the family to problems. Schneider suggested increasing support for caregiver innovations. Fulmer added that Japan, which has a dearth of young people relative to its older adult population, innovates with robotics. She also recommended participants review a recent World Health Organization (WHO) framework developed to help countries strengthen their long-term care systems and services (WHO, 2021).
This page intentionally left blank.













