
6
Scaling and Spreading Whole Health
While a national transition to a whole health system of care must be grounded in well-articulated theory supported by a solid research base, it will also demand a seismic cultural shift in attitudes, structures, processes, and policies to support the committee’s five foundational elements of whole health: people-centered, comprehensive and holistic, upstream-focused, accountable and equitable, and grounded in team well-being (see Chapter 2 for a detailed description of the foundational elements). This would constitute a radical departure from the current state of U.S. health care, which is largely problem based, siloed, reactive, transactional in nature, and built on a fee-for-service payment system that is not well suited to support a national whole health system. The study’s statement of task (see Chapter 1) instructed the committee to consider ways to transform health care by scaling and disseminating whole person care to the entire population. This chapter and the one following will consider how the Department of Veterans Affairs (VA) might best scale its Whole Health System (WHS) at full enterprise level and how WHS and other whole health approaches may be scaled and spread across other health systems. The committee defines scaling whole health as expanding, adapting, and sustaining successful models within an organization, locality, or health system over time to reach a greater number of people (Greenhalgh and Papoutsi, 2019; Hartmann and Linn, 2008). The committee defines spreading as replicating whole health models elsewhere to serve as much of the U.S. population as possible (Barker et al., 2015; Charif et al., 2017; Greenhalgh and Papoutsi, 2019; Milat et al., 2016; Stewart, 2022).
To guide the discussion in Chapters 6 and 7, the committee—extending the framework for foundational elements of whole health introduced in Chapter 2—developed a framework (Figure 6-1) depicting the contextual conditions (shown at the top) and foundational infrastructure (shown at the bottom) necessary for scaling and spreading whole health. These factors mutually reinforce one another and, in doing so, enable the scale and spread of whole health. Building on this framework, this chapter and the one following will consider how VA might best scale its WHS to the full enterprise level and how whole health may be spread across other health systems. This chapter addresses three key contextual conditions that will
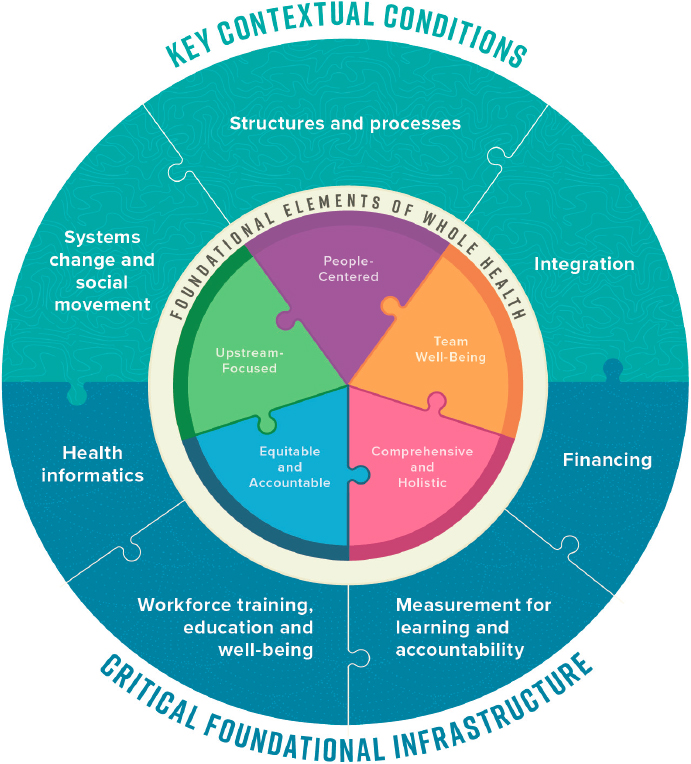
directly enable whole health. First, it reviews theoretical models for systems change and social movement, considers cultural and systems change needed to facilitate whole health transformation across U.S. health care, and shares pertinent historical examples. It then describes the structures and processes required for scale and spread and the need to integrate siloed health and social services to achieve whole health at any scale. Chapter 7 will address the foundational infrastructure needed to establish the information flows, workforce training, education, well-being programs, measurement systems for learning and accountability, and innovative financing required to support the contextual conditions and thus indirectly facilitate the scaling and spreading of whole health throughout the United States.
SYSTEMS CHANGE AND SOCIAL MOVEMENT
As described in earlier chapters of this report, most people in the United States receive medical care that is episodic, reactive to medical symptoms or identified health risks, and passive from the patient’s perspective. A shift from the current state to whole health care will require a transformation that incorporates individuals’ core values, goals, and priorities and focuses on upstream factors while maintaining high-quality disease management. It will also require breaking down conceptual, administrative, financial, and policy barriers that isolate clinical care from the coordinated assessment and management of upstream factors, such as adequate housing, financial security, food security, and social support, which account for most of the variance in health outcomes (Magnan, 2017).
The committee acknowledges how difficult it will be to scale and spread whole health nationally, yet it believes that the nation can make progress through innovation and creativity, by learning from past experience and by identifying existing bright spots and ready opportunities for change. Previous National Academies of Sciences, Engineering, and Medicine (National Academies) reports, the policy window model, and historical examples of major transformational change in the U.S. health system can inform current and future efforts to scale and spread whole health.
Lessons from the National Academies
The committee’s strategy for scale and spread builds upon previous National Academies reports, including Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care (NASEM, 2021), Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being (NASEM, 2019b), Integrative Medicine and the Health of the Public: A Summary of the February 2009 Summit (IOM, 2009) and Crossing the Quality Chasm: A New Health System for the 21st Century
(IOM, 2001). An essential lesson from these reports, which also sought to galvanize major systemic change in U.S. health care, was their recognition that effective systems change depends, in part, on bidirectional dialogue, connections, and interactions between and across all system levels (Carayon et al., 2015; Côté-Boileau et al., 2019) (Table 6-1). It also requires committed actors fostering change from the top down (macro and meso levels) and from the bottom up (the micro levels). Similarly, scaling and spreading whole health systems throughout the United States will require changes at all three levels, and there are actions that actors at each level can take independently to facilitate progress toward the goal of accessible whole health for all.
The whole health models this report describes in Chapter 4 provide good examples of how local and regional health systems can shift their philosophical approach and service delivery design within their local policy environments. Extending whole health across the entire United States will, however, require strong bottom-up demand from patients, families, health care professionals, and the public at large at the national level as well as top-down macro and meso public policy and infrastructure change to support and operationalize it.
A transformation to whole health will require such dramatic shifts in
TABLE 6-1 Implementation Framework for Effective Systems Change
| System Level | Public | Private | ||
|---|---|---|---|---|
| Example Actor | Example Actions | Example Actor | Example Actions | |
| Macro | Federal/state legislative branch | Policies, laws, funding | Coalitions, associations | Policy advocacy, public accountability, professional standards |
| Meso | Federal, state, local executive branch; federal payers; public delivery systems; educators | Regulations, contracting, payment, administrative practices, training | Private delivery organizations, private payers, corporations, institutions, educators | Management policies and practices, training |
| Micro | Individuals and interprofessional teams delivering care in private, public and government health systems | Self-education, quality assessment and improvement, behavior practice | Individuals and families seeking care | Self-education, behavior practice |
SOURCE: Adapted from NASEM, 2021.
the structure and mindset of most health care systems that those seeking to spread and scale whole health may struggle to determine where to begin. Fortunately, as Table 6-1 indicates, change may begin in one of many sectors or across sectors. In parallel with the way that patients progressively engage whole health through thoughtful assessment of personal opportunities and challenges, each health system can identify small, manageable steps that align with its current mission, capabilities, and priorities to help it move along the path of systems transformation.
The Policy Window
The “policy window” model, introduced in 1984 and cited by some 30,000 scholars since, is perhaps the most referenced model from the literature on major transformational systems change. It describes three separate elements of public policy that must align to create a window of opportunity for change: political imperative, effective policy, and a perceived problem (Kingdon and Stano, 1984). The model suggests that all three elements must be present for major, systems-level change to take hold (Figure 6-2). Their intersection provides the opportunity and impetus for innovation, scaling, and spread.
The policy window model suggests that policy entrepreneurs can facilitate systems change by creating windows of opportunity. VA is well positioned to unite and focus the voices of a large population of patients, clinicians, administrators, organizations, and politicians at state, regional, and national levels to achieve whole health. Through the development of uniform metrics, the generation of new evidence, and the development of new policy, VA can promote the political imperative among veterans and across the wider electorate. It also has the advantage of managing nearly all aspects of care for enrolled veterans, including the ability to mobilize resources in support of housing, education, vocational rehabilitation and training, and financial security through in-house mechanisms or in partnership with other federal, state, and philanthropic programs.
Examples from History
Three historical examples, the mental hygiene movement (Novick, 1949), the Flexner report (Flexner, 2002), and the desegregation of American hospitals through the passage of the 1965 Medicare and Medicaid Act (Smith, 2003) demonstrate that positive change is most likely to occur when top-down and bottom-up approaches proceed concurrently. The mental hygiene movement altered the course of American mental health, yet it began with an event in the life of an individual with no previous association with health care practice or policy. In 1900, 24-year-old Clifford Beers
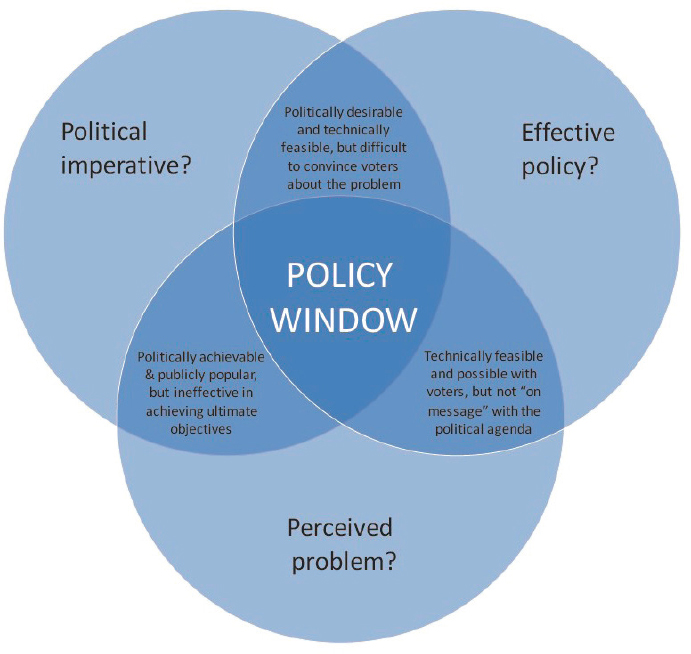
SOURCE: NZIER, 2018; adapted from Kingdon, 1995.
attempted suicide. He spent the next 3 years in psychiatric hospitals. Out of his personal observations came a best-selling autobiography, A Mind That Found Itself (Beers, 1907), which detailed the appalling conditions of asylum life and protested the lack of effective treatment. Beers’ stated intent was to alert the public to society’s misunderstanding and mishandling of mental illness. This boiled down to a chilling message: If this could happen to me, it could happen to you or someone you love.
Beers extended his advocacy beyond the grassroots/micro level of his readership. His strategy was to engage leaders in American mental health and establish partnerships of lay people, mental health professionals, and policy makers within chapters organized at local, state, and national levels. Beers shared his unpublished manuscript with William James, father of American psychology, who in turn introduced him to Adolph Meyer, chief psychiatrist at Johns Hopkins Medical School (Parry, 2010). Beers, James, and Meyer formed the National Committee for Mental Hygiene
in 1909 (Mental Health America, 2022a), which became the National Mental Health Association and, later, Mental Health America. The mental hygiene movement advanced reforms to prevent and treat mental illness and achieved successful scaling and spread through concurrent, coordinated top-down and bottom-up efforts to drive change.
A second historical example of transformative change in American health care was also instigated by someone who was not a health care professional. Abraham Flexner, a professional educator, exposed excessive variation among medical schools in admissions criteria, curriculum, length of training, the qualifications of faculty, and the application of basic science and new research to clinical training (Flexner, 2002) in his 1910 report, Medical Education in the United States and Canada. By revealing an entrenched system of for-profit education that churned out accredited but unqualified physicians, he created the momentum to transform medical training from an apprenticeship to an academic enterprise (Frenk et al., 2010) and accelerated the rate at which basic science and clinical research were translated into clinical practice. Flexner’s indictment of the status quo mobilized medical societies and legislators at state and federal levels and led to strong regulatory support through professional sanctions and new licensing laws.
Although his efforts boosted the development of modern academic medical centers across North America and beyond, Flexner’s primarily top-down, macro-level strategy also produced significant negative consequences, including a devastating effect on historically Black medical schools across the United States (Savitt, 2006). By 1920, 10 years after the Flexner Report was published, 8 of the nation’s 10 Black medical schools had closed their doors because of negative statements about the schools and Black physicians, with only Howard University Medical Department and Meharry Medical College surviving (Savitt, 2006). The damage done to aspiring Black medical students, access to care for Black Americans, and the medical capacity of the entire nation is incalculable. This disaster might have been avoided had Flexner cultivated reciprocal, bottom-up input from the micro and meso levels of American medicine. In addition, Flexner’s personal admiration for the German medical educational system, which prioritized the science of medicine over the art and practice of patient care, helped foster the reductionistic biomedical model with which whole health must compete today (Duffy, 2011).
The desegregation of most American hospitals accomplished by the Medicare and Medicaid Act (also known as the Social Security Amendments of 1965)1 provides a third example of health care transformation through concurrent top-down and bottom-up approaches. Medicare
___________________
1 Public Law 89-97.
required hospitals to adhere to Title VI of the 1964 Civil Rights Act2 which prohibits discrimination based on race, color, or national origin in any institution receiving financial aid from the U.S. government. Just three weeks before the new law came into effect, then–Surgeon General William H. Stewart issued a one-page report making it clear that hospitals could no longer discriminate based on race and that hospital admission policies, patient room assignments, availability of services and facilities, staff privileges, and training programs must also comply with Title VI (Stewart, 1966). The report emphasized elements of the new legislation designed to ameliorate damage done, in part, by the Flexner report.
At the time, the Public Health Service had 300 professional field inspectors to work with hospital administrators to help ensure the new policies were implemented. Knowing this limited workforce was inadequate to enforce compliance across the entire nation, Stewart also called on local physicians to assist in facilitating hospital policy change, support local administrators, and help create a culture of change.
According to David Barton Smith, author of The Power to Heal: Civil Rights, Medicare, and the Struggle to Transform America’s Health Care System, the three people writing the regulations to implement the law were committed to civil rights themselves and also followed the “…direction and pleading of the civil rights organizations” (Andrews, 2016). Additionally, volunteer workers from the Social Security Administration and the Public Health Service who were also dedicated to civil rights augmented the ranks of the original 300 field inspectors. Inspectors’ site visit reports also show that they relied on local people, civil rights activists, and black hospital employees to tell them if hospitals were complying with the new regulations (Andrews, 2016).
The federal courts also played a role in assuring compliance: A Black physician and two of his patients sued a hospital for failing to adhere to the new policies. A lower court ruled that they did not have a case because the hospital had, on previous review, been cleared to receive federal funds by meeting requirements of Title VI (Stewart, 1967). The Fourth Circuit Court of Appeals reversed that decision, pointing out that past certification afforded no assurance of current compliance. The higher court also upheld the legality and constitutionality of the new federal desegregation guidelines. By February of 1967, Assistant Secretary of Health Philip Lee reported that 95 percent of hospitals were receiving Black patients (DeWalt et al., 2005).
The success of the mental hygiene movement, the consequences, for good and ill, of the Flexner report, and the transformative change wrought by the Medicare and Medicaid Act in the 20th century offer lessons for the
___________________
2 42 U.S.C. § 2000d et seq.
scale and spread of whole health in the 21st. In particular, they demonstrate that optimal scale and spread requires collaboration between health care systems and those they serve, an articulation of shared core values and priorities, and new alignment across multiple sectors of society within a social movement. Optimal scale and spread require scientific evidence, but as per the policy window model, systemic change is unlikely to occur unless there is a political imperative, effective policy, and widespread perception of a problem that needs fixing (Kingdon and Stano, 1984). Finally, transformation requires the dynamic interplay of concurrent top-down and bottom-up processes. Resonance across micro, meso, and macro sectors synergizes such efforts and may help insure against serious and enduring negative consequences, intended or unintended, resulting from unilateral, top-down change. Transformation requires recognition that all members of society are the stakeholders and future beneficiaries of whole health.
STRUCTURES AND PROCESSES FOR SCALE AND SPREAD
Beyond, and in support of, the systems change described in the previous section, scaling and spreading whole health systems will require new structures and processes along with practical ways to integrate them. The statement of task asked the committee to describe strategies, including implementation science strategies, that can overcome barriers to scaling and implementing components of whole health, such as integration of mental health, complementary and integrative health, health coaching, peer-to-peer approaches, and well-being. Barriers include overcoming current characteristics of U.S. health care that are inhospitable to whole health and identifying new drivers of change capable of scaling of whole health throughout VA and spreading it across the rest of U.S. health care. This section reviews research findings that can be applied in that effort.
Key Contextual Factors
Scale and spread will require an awareness of and accommodation to a variety of contextual factors that underlie the U.S. health care system. Among these are significant barriers to whole health, including the high-stakes/high-risk and time-pressured nature of biomedical care (Martinez et al., 2011) which is not focused on maintaining well-being for individuals, families, or communities but rather is designed to respond to patients with acute or chronic health problems. Even considering biomedical care alone, clinicians must deal with poor adherence to guidelines or a lack of evidence for care modalities (Pronovost et al., 2009) along with the high information demands (Chaudhry et al., 2006) that thinly stretched personnel experience (George et al., 2018). New structures and processes should
address or overcome these barriers. In addition, a health system characterized by multiple siloed stakeholders, steep hierarchies, rigid disciplinary boundaries (Braithwaite et al., 2016), and patients increasingly presenting with multiple complex chronic conditions (Boersma et al., 2020) creates a pressing need for enhanced integration. The following sections describe structures and processes that could support scale and spread in the face of these contextual challenges.
Structures Supporting Scale and Spread of Whole Health
Structures capable of supporting whole health scaling within VA and of facilitating its spread across U.S. health care in the face of the barriers described above include health ecosystems at the macro level, integrated delivery systems at the meso level, and interprofessional care teams at the micro level (Mitchell et al., 2010). A variety of other structural elements can also support whole health, including, for example, patient and family advisory councils, health coaches, and peer-support specialists as well as the other workforce innovations, health information technology, measurement, and financing reforms described as supportive infrastructure and discussed in Chapter 7.
A “health care ecosystem” is a term used to describe fully interconnected systems of capabilities and services for caring for people and keeping them well, centered around consumers (Sudbury-Riley and Hunter-Jones, 2021). Accountable health communities and medical neighborhoods are similar concepts. Accountable health communities link community members with community services that may address their health-related social needs (i.e., housing instability, food insecurity, utility needs, interpersonal violence, and transportation needs) (Alley et al., 2016). A medical neighborhood is a narrower concept, given its focus on biomedical capabilities and services (Fisher, 2008). Ecosystems include traditional modalities, but also home and self-care, social care, activities of daily life, and financial support. Providing whole health will require intentionally developing and sustaining health care ecosystems capable of overcoming contextual barriers and delivering whole health services to individuals, families, and communities in accordance with the committee’s five foundational elements of whole health.
Integrated delivery systems are vertically integrated networks capable of providing a broad spectrum of coordinated inpatient and outpatient care. They may include physicians, hospitals, post-acute services, and, in some cases, such as Kaiser Permanente, offer health insurance as well. VA is a vertically integrated delivery system that both finances and delivers health care services. Although integrated systems exist in the private sector, few are capable of delivering the full array of services that constitute whole health.
While integrated delivery models are better positioned than freestanding clinics or hospitals to provide whole health, most lack the scope and depth of services needed to fully address the committee’s five foundation elements. For example, a few U.S. health systems provide support for higher education, vocational training, or sustained housing within their delivery models and are thus able to fully address many of the upstream factors of whole health without partnering with outside organizations.
An interprofessional care team is an essential structure that supports whole health. Such teams comprise clinicians and nonclinicians who collaborate across disciplines, health care system components, and community and social services to deliver patient-centered care (Gittell et al., 2015). Examples of interprofessional care team structures include VA’s patient-aligned care teams and, outside VA, patient-centered medical homes. These teams integrate colocated, collaborative primary care and mental health services (including access to substance use services), share information, and coordinate the care they provide. Federally qualified health centers (FQHCs) also provide care through interprofessional care teams which are effective in coordinating a broad variety of health services to meet the diverse needs of their patients (Wright, 2012; Wright et al., 2017). To fully realize the concept of whole health, health systems should recognize people seeking care and their self-defined families as full team members rather than treating them as passive recipients of health care services.
Most VA primary care teams incorporate at least some degree of colocated, collaborative mental health services, but few non-VA health systems have reached that level of interprofessional integration (Ion et al., 2017; VA, 2020b). Creating interprofessional care teams will require meeting all the other contextual conditions and supportive infrastructure that facilitate a whole health mindset, including communication, coordination, and integration of the services that policy and procedural guidance and monitoring by leadership support; developing and fielding an interoperable medical record system that clinicians across disciplines, services, and locations can access easily; aligned measures and financial incentives; and a workforce trained and educated to work within interdisciplinary teams (see Chapter 7). A few other examples include service agreements, huddles, checklists (Haynes et al., 2009), and physical redesign of spaces to enable co-location within which team members can interact (Alidina et al., 2016).
Patient and family advisory councils are a structural innovation that can improve patient experience and lead to better care and improved clinical outcomes (Cunningham and Walton, 2016). In scaling and spreading whole health, patient and family advisory councils offer an important mechanism for increasing the likelihood that systems provide care and pursue organizational and clinical changes consistent with the values and preferences of patients. Also helpful for scaling and spreading whole health
are structures that create the capacity for continuous improvement, innovation, and learning within and across organizations, including learning management systems, training programs, learning collaboratives, and reward systems (IOM, 2007).
Designing Whole Health Teams
Whole health delivery systems are built upon—and scaled and spread through—integrated, interprofessional teams of clinicians, other professionals, and, increasingly, peer-support specialists. This team-based approach to care can improve quality and reduce use and cost (Pany et al., 2021; Reiss-Brennan et al., 2016) and is associated with higher job satisfaction (Song et al., 2017) and lower burnout (Willard-Grace et al., 2014). Appropriately formed teams are better able to engage meaningfully with people, families, and communities; to better address their unique whole health goals in concert with shared values and desired outcomes of care; and to build stronger relationships over time (Mitchell et al., 2010; NASEM, 2021; Sullivan and Ellner, 2015).
To function effectively, teams must have clear, congruent, and well-organized workflows that are monitored by organizational leadership who respond to population demands. As the 2021 report Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care (NASEM, 2021) describes, teams should both reflect the diversity of their local communities and contain a mix of professions, services, and expertise to sufficiently meet the specific needs of the population to which they are accountable. This community-oriented approach (described in greater detail in Chapter 2) calls for health systems or facilities to conduct population assessments to identify local medical and social needs (IOM, 1983), an approach that the Health Resources and Services Administration (HRSA) requires for health center program certification (see Chapter 2). For example, given disproportionately high rates of psychiatric disorders, including substance use and post-traumatic stress disorders, as well as high rates of military service among American Indian and Alaska Native (AI/AN) peoples (Herron and Venner, 2022), it is important to consider and respect these factors when working with these groups. While a large proportion of the AI/AN population is concentrated in just a few states, they are present in significant numbers in every state.3 As such, virtually every U.S. health system should assess the size and health needs of its AI/AN population and coordinate their care with tribal organizations, the federal Indian Health Service, and VA in designing appropriate whole health teams. Such assessments also help determine the ratio of primary care teams to the population served and
___________________
3https://www2.census.gov/geo/maps/DC2020/AIANWall2020/2020_AIAN_US.pdf (accessed December 15, 2022).
other demographic factors that can affect the demand for services, such as the percentage of the population age 65 and older (HRSA, 2018).
Within VA, the Patient-Aligned Care Team (PACT) model is an example of how teams address the primary needs of patients, including mental health, through VA’s primary care–mental health integration program at many, if not most, VA sites and coordinate the remaining needs, including specialty care. PACTs, part of VA’s patient-centered medical home transformation, are organized into “teamlets” comprising clinical and support staff and are assigned a panel of 1,200 individuals. While PACTs are focused primarily on core clinical services and do not generally have embedded social services such as homeless coordinators, nutritionists, or the many other disciplines required to comprehensively address whole health, they are associated with several positive clinical outcomes. These include fewer hospitalizations, specialty care visits, emergency department visits, and specialty mental health visits; an increase in mental health visits in primary care settings and in use of preventive services; lower levels of staff burnout; higher patient satisfaction with access to care; and clinical improvements for patients with diabetes, heart disease, and hypertension (Bidassie, 2017; Hebert et al., 2014; Leung et al., 2019; Nelson et al., 2014; Randall et al., 2017; Rodriguez et al., 2014).
Implementing PACTs has, however, been challenging. One review highlighted the implementation barriers resulting from inadequately staffed teams, a lack of training, poor team cohesion, a lack of clearly defined roles, communication difficulties, and the involvement of trainees whose required transitions cause disruptions in continuity (Yano et al., 2014). Early implementation efforts were also associated with high levels of emotional exhaustion, a key symptom of burnout (Meredith et al., 2015), and team members have reported inadequate training, incomplete implementation, limited guidance from leadership, and poorly defined team structure and roles. Overall, while PACTs have produced positive outcomes, their implementation also highlights the potential difficulties when systems shift to team-based approaches.
The committee is aware of one study that looked at workforce issues related to WHS implementation in VA (Haun et al., 2021). This qualitative study of VA WHS staff identified implementation barriers and facilitators across five VA WHS design sites and one flagship site.4 While there was variation across sites, common barriers to implementation included the lack of progressive culture to embrace whole health, a misalignment of leadership priorities with whole health implementation, administrative barriers such as slow hiring, the lack of sufficient space and investment, excessive caseloads
___________________
4 VA Whole Health design sites are locations that have implemented elements of VA Whole Health. Flagships sites have implemented the full Whole Health System.
and a lack of time, and the lack of clear policies and procedures. That said, most participants indicated that they were invested in WHS implementation and valued it greatly. They embraced the new focus on wellness rather than on illness and reported improved relationships with veterans as well as reduced stress and burnout among staff.
As illustrated in the description of PACT implementation, clearly defining roles within a team is essential to the team’s ability to function efficiently and effectively and to foster an environment that enhances team well-being. Poorly defined roles can lead to a misdistribution of effort, emotional exhaustion, and suboptimal care, and can erode a sense of purpose among the team (Hysong et al., 2019). In contrast, a study of 23 high-performing primary care team–based practices, including at one VA clinic (Sinsky et al., 2013), found that shifting from a physician-centric model to a shared team-based model emphasizing thoughtful distribution of tasks among different team members contributed to improved satisfaction and greater joy in practice. Team culture reflects organizational culture, mission, and values and, in turn, reflects how a team functions together, distributes tasks, and supports other team members (NASEM, 2019b, 2021).
Team Composition and Size Considerations
A well-designed whole health team has much in common with a high-quality primary care team, with similar structures, culture, and a focus on stability (Bodenheimer et al., 2019; Schottenfeld et al., 2016). However, whole health teams must have additional flexibility and adaptability to ensure that an individual can achieve his or her whole health needs and personal goals. While a well-functioning, interprofessional primary care team includes a core team, an extended health care team, and an extended community care team (Kerrissey et al., 2022), a whole health team integrates community care team members within the overall team. Community care team members could include social support professionals to help with housing, food insecurity, childcare, elder care, educational, training, and employment needs; peer-support specialists; home health aides; disability support professionals; and religious or spiritual supports, among others. In addition, community care teams have the capacity to address many upstream factors—one of the committee’s five foundational elements of whole health (see Chapter 2). Because of the integral role of community care team members in a whole health approach, it does not make sense to treat community care separately from the rest of the whole health team. In some systems, especially smaller practices and health care organizations, professionals and peers with expertise specific to upstream factors may operate primarily within partnered community organizations, but even in such cases they can be aligned functionally with the whole health team for
optimal effectiveness. Effective whole health systems will need to ensure that the integration of services is relatively seamless both within and outside a single organization.
In general, a core team includes a person seeking whole health, that person’s family and informal caregivers, and the team members most directly involved in helping the individual achieve his or her whole health goals and addressing the person’s most pressing health needs (NASEM, 2021). An individual’s core team will look different depending on that person’s specific needs. For example, a core team for an older veteran with post-traumatic stress disorder (PTSD) and diabetes who seeks to be more active with his or her grandchildren may include a primary care clinician, a health coach, a mental health professional, and a nutritionist as well as office staff and a medical assistant. A core team for a younger person experiencing homelessness and chronic pain may include a primary care clinician, a social worker, a community health worker, a behavioral health specialist, and a yoga instructor as well as office staff and a medical assistant. The most important feature of a person’s core team is that it is composed to optimally assist in achieving that individual’s whole health goals by addressing personal clinical and nonclinical needs.
Extended whole health care teams include members and services more peripheral to an individual’s care plan but still involved on an as-needed basis to augment the core team. For example, someone with recurrent major depression that is usually managed by their primary care clinician may have a mental health specialist as part of the extended care team for consultation and occasional check-ins. Such coordination is a significant responsibility of the core team (NASEM, 2021). Extended care team members may support several core teams (Bodenheimer and Laing, 2007; Mitchell et al., 2019). One important feature of team composition is that it is flexible and able to change over time to meet the evolving needs and whole health goals of people at different points in their lives. In this way, whole health systems can incorporate a health trajectory approach that conceptualizes and responds to health issues across the lifespan from a people-centered perspective (Wyman and Henly, 2011). This people-centered point of view emphasizes changes in health over time within individuals, families, groups, and communities.
In general, whole health teams include a greater variety of members than those described above and should reflect the populations they serve. For example, the Southcentral Foundation Nuka System of Care (described in Chapter 4), a whole health model that serves an Alaska Native population, integrates traditional Alaska Native healers into its teams. For VA’s WHS (and other whole health models), health coaches are an integral part of the care team and work closely with patients and staff over time. Complementary and integrative health (CIH) professionals are also core team
members. While there is no one-size-fits-all formula for team composition and size, research suggests that transitioning from physician to team-based practice can occur through reconfiguration without substantial change to practice size or personnel (Chien et al., 2018; Meyers et al., 2018). Teams for panels with higher social needs, for example, may include community health workers, behavioral health specialists, and other social supports but fewer physicians. Those with a greater proportion of geriatric patients require more team members dedicated to complex care management, and teams for smaller rural panels generally include a community health worker but are smaller overall. Team structure and membership should also be fluid, adapting to the changing needs and resources of communities and systems.
Despite the shift to more team-based approaches in recent years, much of the guidance regarding panel size is typically based on a per-physician framework. At VA, for example, even within its team-based PACT model, the standard primary panel size is 1,200 veterans for every full-time physician (Shekelle et al., 2019). The physician has at least three supporting team members, but these may also work across multiple panels. This often-cited description of the PACT model is, however, based on an assessment from 2009 and is difficult to extrapolate across the entire VA system. The committee is not aware of specific guidance regarding team composition, size, or panel size for VA’s WHS.
Interprofessional team-based models often have panels below 2,000, but the size depends on the level of task sharing, workflow, and the distribution of skill sets across the team (Altschuler et al., 2012). Southcentral Foundation’s Nuka System of Care, for example, employs a 1,500-person panel plan with an entire department dedicated to managing panel assignment and support (Gottlieb, 2013). Risk adjustment is also important in designing a team to match the needs of a given population. With risk adjustment, systems account for population characteristics such as age, gender, comorbidities, disability, acuity, unique exposures, and other health risks and characteristics based on data they extract from electronic health records (EHRs), claims, needs assessments, and public health findings. Health systems can then configure teams and panels to best match the needs and level of risk of an empaneled population (Kivlahan et al., 2017).
Processes Supporting Scale and Spread of Whole Health
Scaling and spreading whole health also requires teams, systems, and ecosystems to deploy supportive processes of at least five types: adjudication, teaming, implementation, learning, and social. Adjudication refers to decision-making processes and the establishment of evidence criteria for making decisions. For example, health systems will require adjudication
processes to determine which specific treatment modalities they will promote and reimburse as part of a whole health approach (Held, 2019). Systems and payers should consider how to incorporate, coordinate, and pay for services that address upstream factors, complementary and integrative modalities, health coaching, and peer-to-peer supports, along with other services and programs that standard care delivery does not typically include. Chapter 7 discusses financing issues in greater detail.
Teaming processes support interprofessional (team-level), interorganizational (systems-level), and intersectoral (ecosystem-level) integration. These processes include establishing safe cultures and psychologically safe work environments, social integration facilitated by trust and respect building, shared understanding of whole health, and facilitated communication, collaboration, coordination, and information exchange models among system leaders and frontline staff (Edmondson, 2018).
Implementation processes are methods and strategies for the prompt translation of evidence-based practices into clinical settings. By focusing on developing and operationalizing implementation strategy rather than simply raising awareness of an intervention’s effectiveness, implementation science accelerates uptake. This is accomplished through attention to the acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, penetration, and sustainability of new practices (Proctor et al., 2011).
Closely related are processes that enable learning within and across health systems. When professionals and teams need to work together, they require processes such as joint problem solving (Edmondson, 2018); humble inquiry that recognizes and defers to the expertise of patients, families, and communities (Schein, 2013); and adaptive leadership focused on empowering self-direction among those unused to asserting themselves (Heifetz and Linsky, 2002). These enable professionals, teams, and organizations to benefit from key learning practices such as education and training, experimentation, information collection, analysis, and information transfer, and are supported by leadership that reinforces learning, and supportive learning environments characterized by psychological safety, appreciation of differences, openness to new ideas, and ample time for reflection (Garvin et al., 2008; Singer et al., 2012).
Finally, whole health transformation requires social processes that motivate and shape new behaviors among consumers, clinicians, and administrators. Most notably, whole health requires social processes that shift power back to individuals, families, and communities (Toffler, 1999).
Action Steps in Scaling and Spreading Whole Health
As with any innovation, scaling WHS within VA and scaling and spreading whole health approaches across other health systems will likely
follow a path consistent with the diffusion of innovations, which normally proceeds via the following steps: social activation of potential innovation adopters; diffusion from innovators to early adopters followed by buy-in from the early majority, then by late majority; and, finally, uptake by laggards in a roughly normal distribution (Rogers, 2014). Early adoption tends to occur where the fit of the innovation with the adopting community is greatest (Milat et al., 2015; Pallas et al., 2013; Stewart, 2022), where there is stronger leadership and political support for the innovation, and when there is a more supportive policy environment (Hirschhorn et al., 2013; Stewart, 2022). Contextual factors at local and institutional levels that may affect the rate of diffusion (Øvretveit et al., 2017) include the presence of competing or complementary innovations, social influence processes, intentional action to trigger interest and demand, implementation efforts, policy change, and re-invention and adaptation of the innovation (Dearing and Cox, 2018). A variety of factors can affect the rate and reach of innovation. For example, dissemination is facilitated when the innovation is promoted to communities and population segments where need is greatest, capacity is sufficient to adopt and implement, targeted learning opportunities are made available, and barriers that arise are addressed effectively (Dearing and Cox, 2018).
This process of spreading and scaling whole health can build on lessons from other health delivery innovation models both inside and beyond VA, several of which Chapters 4 and 5 describe (Kilbourne et al., 2012). Different systems at different stages may rightly choose different approaches at different points in time. There are, however, common principles that systems can adopt or adapt. Among the many available approaches, the committee describes five instructive examples: the ExpandNet/WHO framework for scaling up; the Institute for Healthcare Improvement’s Framework for Spread; Ariadne Labs’ Arc framework for spread; the Nonadoption, Abandonment, Scale-up, Spread, and Sustainability (NASSS) framework; and VA’s Diffusion of Excellence model.
The World Health Organization’s ExpandNet program’s framework is intended to guide those seeking to scale successfully tested interventions, assuming feasibility and effectiveness has been established locally (Figure 6-3). It suggests that a scaling-up strategy involves five interrelated elements (top oval) and highlights five strategic choices required for formulating a scaling-up strategy (boxes outside the oval), which consists of nine steps: (1) planning actions to increase scalability, (2) increasing the capacity of the end-user organization, (3) assessing the environment and planning actions to increase the potential for success, (4) increasing the capacity of the resource team to support scale and spread, (5) making strategic choices to support scaling, (6) making strategic choices to support spreading (expansion/replication), (7) determining the role of diversification, (8) planning
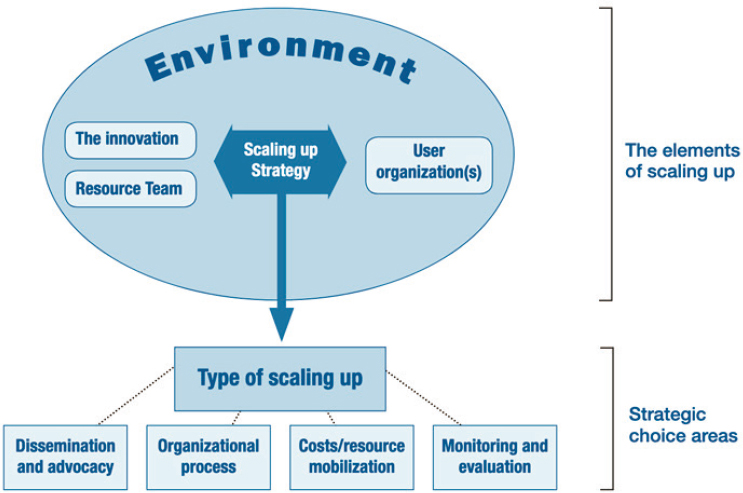
SOURCE: WHO, 2009.
actions to address spontaneous scaling, and (9) finalizing the scaling and spread strategy and identifying next steps (WHO, 2009).
The Framework for Spread, introduced by the Institute for Healthcare Improvement (Figure 6-4) (Massoud et al., 2006), has guided successful collaborative efforts, including a VA-sponsored collaborative initiative to enhance access to care (Nolan et al., 2005). This framework, which applies to efforts to spread new ideas or operation systems both within and across organizations, emphasizes the responsibilities of leadership, the iterative identification of better ideas, targeted communication, strengthened social systems, standardized measurement and feedback systems, and knowledge management as key components.
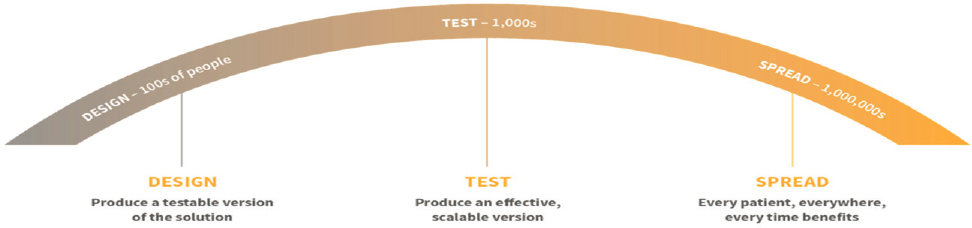
A third framework, targeting large-scale spread of innovations with demonstrated effectiveness, the Ariadne Labs Arc, envisions spread as a process of continual learning and collaboration (Figure 6-5). Solutions, such as safe surgical checklists, advance through three stages: design, test, and spread (Ariadne Labs, 2022). Accomplishing this arc requires collaborating with implementation partners, iterating as new knowledge is discovered, and continuously refining the approach. Spread proceeds by distributing implementation tools and support materials broadly; providing
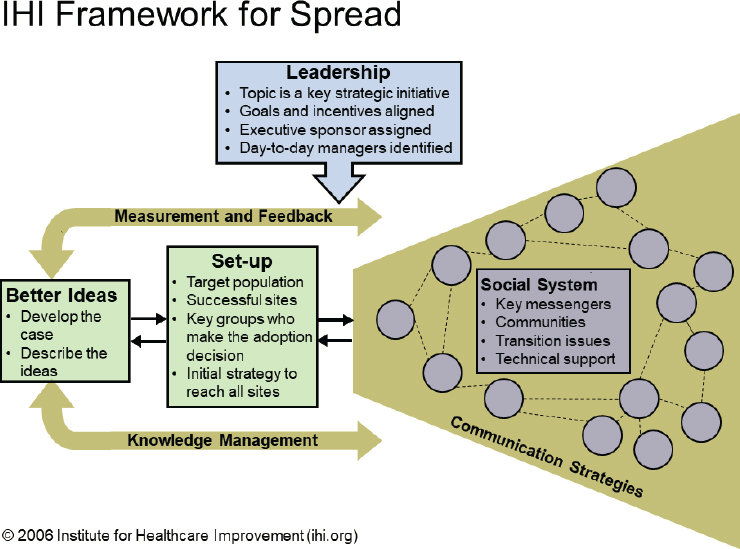
SOURCE: Massoud et al., 2006.
direct implementation support to a select group of implementers; developing an education strategy complete with associated curriculum and training materials; creating and supporting communities of practice in which practitioners share implementation strategies and can guide each other; disseminating and promoting key ideas through peer-reviewed publications, other media coverage, and coalition-building; incorporating feedback and promoting adaptability; and measuring impact.
The fourth framework, NASSS, was derived from 28 previous technology implementation frameworks and empirical testing. It was designed specifically to help predict and evaluate the success of a technology-supported health or social care program (Greenhalgh et al., 2017). NASSS contains seven domains (Figure 6-6): condition or illness, technology, value proposition, adopter system (comprising professional staff, patient, and lay caregivers), the organization(s), wider institutional and societal context, and the interaction and mutual adaptation between all these domains over time (Greenhalgh et al., 2017). This model holds that innovation
SOURCE: Ariadne Labs, 2022.
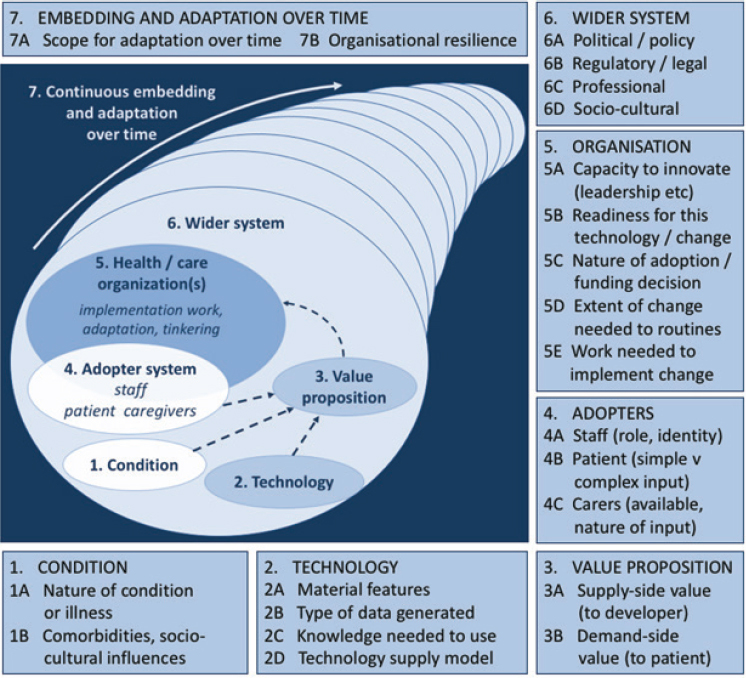
SOURCE: Greenhalgh et al., 2017.
becomes increasingly difficult to implement across these domains when it is characterized as complicated and complex rather than simple. VA has used the NASSS framework to examine factors influencing its national rollout of an automated texting system to support patient self-management (Yakovchenko et al., 2021).
The fifth framework, VA’s Diffusion of Excellence model (Vega et al., 2019), categorizes initiatives for different implementation strategies (e.g., an initiative that will be packaged for potential organic implementation by other VA facilities versus an initiative destined for nationwide implementation and standardization with support of a national diffusion team versus an initiative whose implementation will be discontinued) based on factors such as the degree of enterprise-wide need, availability of outcome metrics, complexity of implementation, and projected impact. This model sets forth
a five-step systematic process to identify, replicate, and eventually scale and spread practices with the greatest potential for positive impact (Figure 6-7). These steps are (1) identify promising practices and clinical interventions; (2) find champions; (3) adapt and replicate; (4) measure real-world impact; and (5) scale and spread best practices.
Within the first 4 years of its application, the five-step Diffusion of Excellence model succeeded in replicating 47 high-impact innovative practices more than 412 times at VA hospitals across the country (Vega et al., 2019). More than 100,000 veterans gained access to new clinical approaches, and VA avoided approximately $22.6 million in costs. Practices scaled and spread through this process have produced substantial reductions in patient mortality, such as with Project HAPPEN (Hospital-Acquired Pneumonia Prevention by Engaging Nurses to Complete Oral Care) (Munro et al., 2018). Providing special-purpose funding to hire and train new staff, purchase needed equipment/materials, and, when necessary, refurbish, lease,

SOURCE: Reproduced from (Figure 1) Vega et al., 2019, with permission from the Permanente Federation.
or construct new space often incentivized scale and spread. Beyond the value associated with any one initiative, each successful iteration of the Diffusion of Excellence cycle advances the development of a culture of continuous quality improvement across VA.
Each of these five frameworks has value, and different systems should use whichever one best aligns with their current operations and culture to address the implementation they plan to achieve, overcome the challenges they anticipate, and advance the capabilities of their organization. Key principles for scale and spread that emerge across the five frameworks include
- A focus on a high-priority need shared by a broad range of stakeholders.
- Selection of effective practices which address that need.
- Pre-implementation attention to the acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, penetration, and sustainability of the planned intervention.
- Strong buy-in from clinical, administrative, and policy leaders within the health care system and, when appropriate, at community, state, and federal levels.
- Engagement of stakeholders to build implementation capacity and specify needed practice adaptations and evaluation goals.
- Development of learning systems that train and motivate clinicians and other line staff to adopt effective practices.
- Identification and coordination of well-trained local champions capable of leading change at the front lines of health care.
- Adaptation of the medical record and other reporting systems to enable reliable measurement of implementation and outcomes using valid, standardized metrics.
- Ongoing analysis of system data and stakeholder feedback, which either makes a strong business case for sustaining new practice or guides next steps in adaptation.
- If successful, a handoff to local operational leaders to continuously refine local adaptation and own practice sustainment over time.
SCALING AND SPREADING WHOLE HEALTH TO ALL ENROLLED VETERANS
The statement of task charged the committee to comment on how VA can accelerate clinical integration with community services to expand whole person care to veterans who receive their care outside VA through the VA MISSION Act’s provisions. It also charged the committee with identifying strategies that VA can use to overcome barriers to scaling and implementing components of the whole health approach, such as integration of mental health, CIH, health coaching, peer-to-peer approaches, and well-being
programs. In response, this section focuses on two key questions: (1) How can VA scale whole health to reach all enrolled veterans, including those who receive care outside of VA through the VA MISSION Act? and (2) What strategies can help overcome barriers to spreading components of whole health across other sectors of U.S. health care?
Through a series of internal VA policy changes and implementation efforts as well as federal mandates, VA has expanded its WHS steadily since its launch in 2012. WHS is currently available at 37 sites, with at least one “flagship” site in every veterans integrated service network. In 2022, just over 1 million veterans (approximately 16 percent of veterans actively receiving care) had received at least one component of whole health care.5,6 COVID-19 also illustrated the impact of WHS scaling (see Box 6-1). Recent outcome-evaluation studies of WHS users compared with non-users found greater reductions in opioid usage as well as improvements in perceptions of care, engagement in care, self-care, life meaning, and purpose, pain, and perceived stress (see Chapter 5 for more details). These findings provided the basis for a new executive decision memo that mandated VA integration of whole health principles and practices into mental health and primary care across the entire VA system. VA plans to complete WHS implementation at full enterprise scale between 2024 and 2027 (Kligler et al., 2022).
The growth of and commitment to WHS across VA bodes well for future scaling efforts, yet, as Chapter 4 notes, some barriers remain in place. VA evaluations suggest that the fidelity of WHS implementation varies across the locations where it is already available and that whole health services are not yet available throughout the system. In addition, as described in Chapter 4, the committee’s foundational elements of whole health are not fully available at every site where VA has implemented WHS.
Addressing Barriers to Scaling Whole Health within VA
Despite the progress implementing the WHS within VA to date, significant barriers hinder its scale and spread throughout the system. Some of these barriers reflect lingering negative concerns about the WHS rollout among at least some VA staff members at multiple levels. Others have to do with how veterans first gain access to VA services at the point of separation from military service and how veterans who receive care in non-VA health systems lack access to whole health services. Still others reflect historical schisms built into VA itself which VA will have to resolve to optimize its effectiveness as a whole health system. None of these barriers are beyond solving, but each will require initiative, creativity, flexibility, funding, and
___________________
5 After a prepublication version of the report was provided to VA, this section was edited to correct the number of veterans receiving whole health care.
6 Personal communication, Ben Kligler, Department of Veterans Affairs, February 13, 2022.
inspired leadership if VA is to achieve the desired health outcomes for veterans and optimal efficiencies for its system.
While VA’s WHS rollout has generally been welcomed, a recent study of staff perceptions of VA WHS implementation identified some barriers to scaling, including
- Cultural barriers, including the absence of a flexible, progressive culture;
- Leadership barriers, including a lack of perceived authority to implement change;
- Administrative barriers, including excessive lags in hiring which, in part, reflect a failure to develop appropriate position titles, and credentialing standards;
- Resource barriers, including inadequate allocation of space and funding;
- Clinical barriers, including a failure to factor in the challenge of managing large, complex caseloads which, in turn, limit the length and frequency of whole health appointments; and
- Policy and procedural barriers, including unclear policies regarding when certain interventions or services are permitted (e.g., increasing medical staff membership of integrative medicine providers in VA medical centers and when and how integrative practices may be provided either through in-house consultation or by outsourcing to qualified community providers) (Haun et al., 2021).
These concerns led employees to recommend that VA hire more staff to support WHS activities and, in particular, institute a faster hiring process so that facilities could keep pace with the demand for the new and broader range of services associated with whole health (Haun et al., 2021). VA employees also recommended establishing WHS as its own service line reporting directly to the facility director; improving systems for whole health workload capture and credit; and developing templates for better documentation and for tracking the delivery and outcomes of whole health services. VA employees working at WHS test sites also recommended developing communication networks that build facility capacity to identify and coordinate the full range of WHS services within a community. This aligns with the committee’s discussion in Chapter 4 that VA’s current WHS implementation does not fully address all of the committee’s five foundational elements. Local networks could enhance collaboration between VA facilities and their surrounding region, while national communication networks identify and align WHS services nationwide.
Given the wide range of VA settings, there is no single cookie-cutter solution that can address these issues at enterprise scale. Such concerns can, however, be effectively addressed by encouraging and supporting the creativity and flexibility of local teams and leaders through application of one of the four health delivery innovation models described earlier in this chapter and also demonstrated by the many whole health systems described throughout this report. In any effort, it is essential to balance efforts at the macro and meso levels (e.g., leadership support from top VA officials and policy guidance from VA program offices) with a “boots on the ground” understanding and opportunities at the micro level.
Need for Increased Emphasis on Upstream Factors within VA WHS
As Chapters 4 and 5 discussed, the VA WHS does address upstream factors through its Circle of Health model, but it is unclear how it operationalizes the model with practical services that veterans can use, nor is it clear how effective the model is at addressing social needs. While other VA WHS assessment tools such as the Personal Health Inventory (VA, 2022e) and My Personal Health Plan Wallet Card (VA, 2022c) inquire specifically about certain upstream factors, including social support, housing safety,
and nutrition, they are less explicit in assessing the effect of other key social determinants of health, including known obstacles to accessing health care such as reliable access to transportation (Health Research & Educational Trust, 2017) or a need for child or elder care services to ensure a veteran’s ability to take part in gainful employment, clinical appointments, or other important activities of daily life. These assessment tools also fail to identify important life transitions such as becoming a parent or preparing for healthy aging. The lack of a more comprehensive assessment consistent with its own foundational Circle of Health concept undercuts VA’s WHS approach and constitutes a barrier to scaling WHS across VA (VA, 2021a).
While a full discussion of this issue is beyond the scope of this report, VA’s National Center for PTSD has helped develop a tool—the Well-Being Inventory (WBI)—that could be useful for broadening WHS assessments of upstream factors (Vogt et al., 2019). This multidimensional assessment tool was specifically designed to measure veterans’ status, functioning, and satisfaction within the four life domains of vocation, finances, health, and social relationships. In total, there are 21 sections of the WBI and 126 questions/statements with anchored responses scored using a five-point Likert scale. Measures within each domain may be extracted for use as separate entities depending on the purpose of the assessment. While the concept of well-being is not entirely congruent with that of whole health, the WBI is a psychometrically sound set of measures that could be useful for deepening and contextualizing VA’s whole health assessment. Given that it is already part of VA’s toolbox, VA could integrate it easily into its WHS. In addition, researchers at VA are currently developing and validating a Well-Being Brief measure (VA, 2021b). Periodic application of the WBI or similar measures within the WHS would be of unique value because such measures of wellbeing provide a common language in which patients, clinicians, researchers, administrators, and policy makers can converse and come together to define shared values, goals, and actions (VHA, 2021).
De-Siloing VHA and VBA Services to Address Upstream Factors
As Chapter 1 described, VA is officially a single entity, yet in many ways it operates as three separate entities: the Veterans Health Administration (VHA), which oversees VA health care, including WHS; the Veterans Benefits Administration (VBA), which provides a broad array of benefits and services, including financial, educational, vocational, and mortgage assistance to veterans and their dependents; and the National Cemetery Administration. Each has a distinct mission and receives a separate budget allocation. As a result, these three administrations have a natural tendency to be unaware of one another’s initiatives, even as they often compete with one another in addressing specific issues. For example, both VHA and VBA have programs to support veterans on college campuses: VHA’s Veterans Integration to Academic
Leadership Program addresses veterans’ clinical needs (VA, 2020e), while the VBA’s VetSuccess on Campus administers their VA benefits (VA, 2022i). Both programs have significant value, yet important opportunities for synergy are lost because they employ different staff with different training and, for the most part, operate on different campuses and in isolation from one another.
Enhanced integration or coordination of VHA and VBA efforts could achieve veteran-centered synergies in support of VA’s WHS scale and spread because a large portion of VBA’s portfolio addresses issues relevant to the upstream factors that are foundational to whole health. For example, as Chapter 1 describes, VBA has a variety of programs that provide direct financial compensation for service-connected disabilities, employment benefits, educational benefits, low-interest home loans and mortgage delinquency assistance, financial management assistance, independent living assistance, and other means of support that directly address the social determinants of health (VA, 2022h). Because many of these benefits align well conceptually with whole health approaches, the integration of VHA and VBA’s efforts has the potential to maximize the efficacy of VA’s WHS while also reducing health inequities among veterans (NASEM, 2019a).
While VA has implemented a number of systems-level changes since its inception, it is a large government agency, and the challenge of de-siloing programs across VHA and VBA is formidable. There are precedents for success, however. For example, in the course of a high-priority VA campaign, VBA, VHA, and other federal, state, and local agencies, including the Department of Housing and Urban Development, collaborated to achieve a significant decrease in homelessness among veterans (VA, 2022k). Given equal priority, many VHA and VBA services could potentially meld within a single, integrated system to privilege the whole health needs of individual veterans above VA’s venerable organizational structures and processes. It is beyond the scope of this committee to assess the operational complexity and feasibility of better VHA–VBA integration, but as VA’s WHS expansion continues, VA could consider strengthening the integration between the two administrations to potentially bolster, streamline, and better integrate its whole health efforts.
In fact, VA has already begun efforts to better integrate its internal systems to some degree. The mission of the recently established Veterans Experience Office (VA, 2022g) is to “coordinate across the department to meet the health and benefits needs of our veteran customers by establishing community-level, public and private partnerships to bridge gaps in services, foster knowledge exchange, and conduct outreach with underserved communities to support Veterans experiences.” VA could apply these same principles and strategies to better integrate the efforts of VHA and VBA. Though this de-siloing effort would be ambitious, it is a fundamental step that VA could take to overcome internal barriers to WHS implementation.
Whole Health and the Transition between the Department of Defense and VA
Like all life transitions, adjustment from military to civilian status is associated with potential health risks (Montgomery et al., 2022), but this particular transition (Derefinko et al., 2019) also provides a unique opportunity for new veterans and their families to acquire a whole health perspective and engage VA’s WHS. Unfortunately, current transition practices fail to incorporate a whole health approach. This limits the opportunities for veterans and their families to participate in proactive, preventive whole health efforts that could have significant value for individuals, families, communities, and government agencies at multiple levels. It also represents a critical barrier to scaling WHS across VA and facilitating its spread it across the rest of U.S. health care.
More than 200,000 service members exit the military every year (DoD, 2022). As part of that process, they receive substantial training on VA programs and benefits through the VBA’s Transition Assistance Program (TAP) (VA, 2022j). Recognizing that women veterans may be less likely to enroll for services (Newins et al., 2019), VA has developed a Women’s Health Transition Training to engage them. Despite these efforts, many veterans still fail to enroll for VA services at the time of separation. VA’s Office of Public Health reports that only 62 percent of service members who deployed to combat areas after September 11, 2001, had accessed even one VA health service by June 2015 (VA, 2020c). The RAND Corporation reported that although about 60 percent of U.S. veterans are eligible for VA care based on length of service, service-connected injuries, service in designated combat theaters, and income, fewer than half use VA health benefits (Farmer et al., 2016).
Enrollment in VA health and benefits programs is not automatic: new veterans must opt in at the time of separation. Unfortunately, many veterans report being put off by rumors that VA is difficult to engage and believe that the effort is not worth the payoff (Crawford et al., 2015). Having spent years receiving their training, occupational assignments, location, housing, medical care, and even their clothing and meals from the military, new veterans are often unprepared for the challenges of civilian life. By the time that many come to realize they need better access to health care or assistance with housing, education, or employment, they have often lost track of their VA options or a designated period of eligibility has expired (5 years for those who have deployed to combat operations in Afghanistan or Iraq). This is particularly important regarding mental health needs. According to VA’s Office of Public Health, more that 58 percent of recent combat veterans who presented to VA as of June 2015 received at least one mental health diagnosis. In addition, RAND’s longitudinal Deployment
Life Study concluded that addressing psychological problems at the time of military separation could help avoid serious long-term impairments such as increased morbidity, homelessness, unemployment, or substance use (Meadows et al., 2016). Failure to engage VA health care in the course of separation could carry severe consequences for such veterans.
Recent efforts to enhance transition assistance at the time of separation from the military may help. VBA’s new Solid Start Program7 inaugurated a series of three telephone contacts with every newly separated service member during their first year of civilian life (VA, 2020d). Through this new system, specially trained VA benefits representatives update contact information, review the new veteran’s progress toward goals developed at the time of separation, and offer help ranging from obtaining a home loan, accessing physical or mental health care, or pursuing academic studies, technical training, or occupational opportunities. Through these and other efforts, Solid Start incorporates VA whole health principles by engaging a population of veterans who might otherwise be lost to follow-up during a vulnerable state of transition. Incorporating the Well-Being Inventory (described above) or a brief, validated measurement such as VA’s Well-Being Signs (Vogt et al., 2019) into the Solid Start program could augment this approach. The Well-Being Signs tool asks veterans to consider the most important things that they do or wish to do in their daily lives. This might include having a job, spending time with family and friends, participating in leisure-time activities, or managing one’s health or finances. Ideally, veterans would take a baseline measure of well-being during the TAP weeks or, preferably, months before termination and be followed over the course of Solid Start.
VA’s proactive investment in engaging these new veterans could produce downstream advantages for veterans, their families, and for VA itself. These advantages could be multiplied if Solid Start were to include “fast track” enrollment in VA’s WHS that engaged new veterans in comprehensive whole health care early enough in their civilian careers to have maximum impact on their well-being and social determinants of health. The simple act of orienting new veterans and their families to whole health principles and practices—whether or not they chose to enroll in VA care—could have the added benefit of increasing awareness of and demand for whole health practices in non-VA health systems.
___________________
7 Additional information is available at https://benefits.va.gov/transition/solid-start.asp (accessed February 14, 2023).
Engaging Veterans Who Seek Care Through Non-VA Health Systems in WHS
More than half of the 19 million living U.S. veterans do not receive health care through VA. Of the 9 million who enroll in VA health care, many receive at least some portion of their care in non-VA systems. This is important because most health care systems fail routinely to ask or record the response to a basic question: “Have you or someone you care about served in the military?” (Kilpatrick et al., 2011).
While it is true that, for most of the nation’s history, fewer than 1 percent of its citizens served in the military (Segal and Segal, 2004), the combined number of service members, veterans, and their dependents who are potentially eligible for military or VA benefits today approaches 60 million people, or one in five U.S. citizens. Any of these individuals is a potential point of engagement with VA WHS, and a failure to ask about and document veteran status is a major yet avoidable barrier to that engagement. Furthermore, when veterans who are enrolled in VA care choose to seek care in non-VA settings, they may not be recognized as potentially eligible to participate in VA’s Community Care program. This could significantly disadvantage both the patient and the health system and contribute to discontinuity of care.
One reason that clinicians in non-VA settings routinely fail to ask about veteran status may be indicated by a RAND Corporation study which found that non-VA health care providers generally lack the necessary clinical and cultural competence required to understand and respond to the health needs of veterans. In addition, non-VA providers may lack the necessary understanding of the significant health and social resources that may be available to military-related populations (Tanielian et al., 2014).
Veterans are at higher risk than the average patient for a number of important health risks, including PTSD, traumatic brain injury, exposure to toxins and tropical diseases, and physical trauma. As such, they may be eligible through VA for a unique set of important health resources, including access to specialty and subspecialty care, sophisticated diagnostics, pharmaceuticals, surgical procedures, inpatient services, and long-term residential and rehabilitation services—but only if their non-VA health care providers identify them as veterans. In fact, both veterans and their non-VA providers stand to benefit if they realize that they may be eligible for reimbursement and coordination of care through VA’s Community Care program. Relevant to the spread of whole health across non-VA systems and given VA’s ongoing scaling of its WHS, improved coordination of care between VA and non-VA providers could serve as a valuable driver of whole health culture, principles, and practices in non-VA settings. In short, it makes good medical sense for non-VA health care systems to identify veterans under their care.
The MISSION Act and Coordinating Care between VA and Community Care
Implementation of the bipartisan John S. McCain III, Daniel K. Akaka, and Samuel R. Johnson VA Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act of 2018,8 which built on the preceding Veterans Access, Choice, and Accountability (Veterans Choice) Act of 2014,9 illustrates the complex process of integrating services between VA and non-VA systems. Upon its implementation in June 2019, the MISSION Act established a new community care program designed to improve access to non-VA care for eligible veterans. The statement of task (see Chapter 1) asked the committee to consider ways in which VA can accelerate clinical integration with community services to expand whole person care to veterans who receive their care outside VA through the VA MISSION Act provisions.
The MISSION Act permits VA-enrolled veterans to receive care in the community if they meet any of the following six eligibility requirements:
- A veteran needs a service not available at any VA medical facility.
- A veteran lives in a U.S. state or territory without a full-service VA medical facility. Specifically, this would apply to veterans living in Alaska, Hawaii, New Hampshire, and the U.S. territories of Guam, American Samoa, the Northern Mariana Islands, and the U.S. Virgin Islands.
- A veteran qualifies under the “grandfather” provision related to distance eligibility under the Veterans Choice program.
- VA cannot furnish care within certain designated access standards pertaining to
- drive time, as calculated using geo-mapping software, of greater than a 30-minute average drive time for primary care, mental health and noninstitutional extended care services or a greater than 60-minute average drive time for specialty care or
- appointment wait time of 20 days from the date of request for primary care, mental health care, and noninstitutional extended care services, unless the veteran agrees to a later date in consultation with his or her VA health care provider, and 28 days for specialty care from the date of request, unless the veteran agrees to a later date in consultation with his or her VA health care provider.
___________________
8 John S. McCain III, Daniel K. Akaka, and Samuel R. Johnson VA Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act of 2018, Public Law 182, 115th Congress, 2d sess. (June 6, 2018).
9 Veterans Access, Choice, and Accountability Act of 2014, Public Law 146, 113th Congress, 2d sess. (August 7, 2014).
- The veteran and the referring clinician agree it is in the best medical interest of the veteran to receive community care based on defined factors.
- VA has determined that a VA medical service line is not providing care in a manner that complies with VA’s standards for quality based on specific conditions.
The MISSION Act also established a new urgent care benefit that eligible veterans can access through VA’s network of urgent care providers in the community (VA, 2019).10
During the Veterans Choice program era, over one-third of VA-enrolled veterans used community care (Mattocks and Yehia, 2017), and in 2020 the MISSION Act authorized more than 2.3 million veterans to seek care from community providers (CRS, 2021). The most common referrals to community providers have been for physical therapy, chiropractic care, orthopedics, and acupuncture, with the latter being an integrative service often included as an element of whole health systems, providing an important precedent for including other whole health services under the MISSION Act. Such referrals likely reflected the VA’s increasing focus on non-pharmacologic treatment for pain care (Mattocks et al., 2021). In addition, from June 2019 to February 2020 nearly 140,000 veterans, or 2.4 percent of eligible veterans, made over 175,000 urgent care visits under the new MISSION Act urgent care benefit, costing VA over $23.3 million (Vashi et al., 2021). During the same period, 7.3 percent of eligible veterans visited a VA emergency department or urgent care clinic.
As part of its effort to operationalize the MISSION Act, VA established the Community Care Network (CCN) (VA, 2022a). CCN is meant to link VA with community providers to ensure that veterans receive timely, high-quality care by applying industry-standard approaches and guidelines to administer services, pay for services promptly, and manage the network to its full potential. Included are medical, surgical, complementary, and integrative health services, durable medical equipment, pharmacy, and dental services for eligible veterans. At present, CCN comprises five regional networks covering all U.S. states and territories and is being deployed in a phased approach (VA, 2022a). Once fully implemented, CCN will be the preferred national network VA uses to purchase care for veterans in their communities. VA has awarded contracts to Optum Public Sector Solutions, Inc., part of UnitedHealth Group, Inc., and TriWest Health Care Alliance to serve as third-party administrators, with each responsible for different geographic regions across the country. In most cases other than urgent or
___________________
10 Additional information is available at https://www.va.gov/opa/pressrel/pressrelease.cfm?id=5264 (accessed December 2, 2022).
emergency care, veterans need a VA referral through a local VA medical facility community care office before they may visit an enrolled community provider.
Currently, there are limited data regarding whether the availability of the MISSION Act’s community care options is improving veterans’ access to care, quality of care, or health outcomes. One review of wait times for over 1.1 million veterans who received care from community providers under the Veterans Choice program between fiscal year (FY) 2015 and FY 2018 found that while average wait times for both rural and urban veterans and for all services had decreased over that time, average wait times for most services were longer for community care than for care at VA facilities (Gurewich et al., 2021).
In terms of quality of care, a systematic review (IOM, 2001) found that VA facilities compared favorably with non-VA facilities across many dimensions of quality (O’Hanlon et al., 2017). For example, in 22 of 34 studies of safety and 20 of 24 studies of effectiveness, VA facilities demonstrated the same or better quality compared with non-VA facilities. VA facilities performed similarly or better in most, but not all, studies comparing morbidity and mortality. VA facilities also had similar or superior quality to non-VA facilities with respect to preventive, recommended, and end-of-life care as well as managing medications (O’Hanlon et al., 2017). Given these findings, it is important to ensure that when veterans receive community care, the quality of that care is at least equal to that provided by VA.
Even if well intentioned, the Veterans Choice program and the MISSION Act have not yet succeeded in their stated purpose of improving access to care for veterans or guaranteed a uniform quality of care. In fact, the significant challenges that VA has encountered in implementing the MISSION Act’s requirements portend substantial difficulties in any future effort to integrate whole health services delivered in non-VA settings under the Act’s provisions. For example, on July 14, 2022, nine senators wrote to Department of Veterans Affairs Secretary Denis McDonough to raise concerns regarding access to community care as authorized by the MISSION Act (Daines et al., 2022). According to the letter, constituents have voiced frequent concerns and have provided evidence that VA is not always following its own guidelines regarding access to community care and in some cases has denied care to eligible veterans. There are also reports that VA is rescheduling care without the veteran’s consent, that internal VA training materials are pushing to reduce community care, and that VA administrators are, in some cases, overruling decisions by VA doctors who wish to send their patients to community providers (Castellano, 2021).
VA leaders may have good reason to be concerned about the cost of implementing the MISSION Act. A December 2021 report from the VA Office of the Inspector General (OIG) found that community-based care
has made veterans’ care significantly more costly. High costs were, at least in part, attributed to a lack of financial controls under the MISSION Act. A VA OIG review team found that in FY 2020 more than 37,900 community providers billed and were paid nearly $40 million for significantly more high-level evaluation and management codes compared to their peers in the same specialties (OIG, 2021). In addition, VA paid out another $37.8 million to 45,600 providers who billed for evaluation and management services that were already covered by bundled payments. According to the OIG report, some 38 percent of the 218,000 participants in the VA Community Care Network created under the MISSION Act have engaged in the fraudulent billing practice known as upcoding.
The VHA operates with a fixed allocation from Congress, so excessive expenditures in community care reduce support for in-house VHA staffing, services, and facilities. Critics of the Choice and the MISSION Acts have raised an alarm that, despite the avowed purpose of improving access to care for veterans, these acts would cripple VA and open the door for complete privatization of veterans’ health care (Lemle and Gordon, 2021).
According to the Congressional Budget Office, VA spending on community care has grown sharply, both in terms of dollars spent and as a portion of VA’s total spending. In 2014, VA’s Community Care program accounted for $7.9 billion, or about 12 percent, of VHA’s budget. By 2021 the cost of community care programs had more than doubled to $17.6 billion, representing approximately 20 percent of VHA’s budget (Bass et al., 2021). When the committee was writing this report, VA’s Community Care program accounted for one-third of VA’s total health care expenditures, a 26 percent year-to-year increase.
One major barrier in implementing the MISSION Act has been difficulty enrolling community providers in community care networks. A survey of VA facility directors identified the following major impediments to enrolling community providers: delays in reimbursement, low Medicare reimbursement rates, and confusing VA rules for prior authorization and bundled care (Mattocks et al., 2021). Furthermore, 35 percent of VA facility leaders surveyed could not identify sufficient capacity to deliver non-VA mental health, orthopedic, dermatology, or neurology services within their geographic area. Nearly 30 percent of these VA leaders reported that community providers practicing within their area were not accepting new patients and that almost 45 percent of community providers in their area were unwilling to take VA patients. In addition, as Chapter 1 described, wait times for services at VA facilities tend to be similar to, and in many cases shorter than, those in the surrounding community, suggesting that veterans seeking community care because of wait times at their local VA facility may not fare better elsewhere (CRS, 2021).
Several studies have found that care across VA and non-VA facilities is often not well coordinated (Charns et al., 2022; Mohr et al., 2019; Vanneman et al., 2022; Zulman et al., 2022). One study reported system failures with the potential to significantly undermine patient safety and veteran satisfaction (Schlosser et al., 2020). For example, only 5 percent of community clinicians reported that they always or very often received notification that their patients were receiving VA care, whereas 44 percent of VA clinicians reported that they always or very often received such notification (Schlosser et al., 2020). Providers in both VA and the community reported difficulty in communicating medication changes, sharing laboratory and imaging results, communicating with specialists, sharing discharge summaries, and managing medication renewals between systems of care. One study (Benzer et al., 2020) found that the lack of interoperable EHRs between VA and community care systems, combined with “bureaucratic and opaque procedures,” created significant obstacles to care coordination. The authors of that study recommended that VA implement enhanced monitoring of patients’ experience of care coordination, surveys of referring and consulting clinicians, and pilot testing and evaluation of interventions to improve care coordination (Benzer et al., 2020).
In a recent cross-sectional study of community health informational exchanges and access standards set forth in the MISSION Act, investigators identified important barriers to shared information (Martin et al., 2021). Some barriers stemmed from technical limitations among the many different platforms deployed across the nation (Chapter 7 will discuss the pressing need for interoperability among health information technologies). The investigators found that only 37.8 percent of the health care systems that responded to their survey reported current active exchange of information with any of VA hospitals within their coverage area. Another concern that this study identified was the lack of a uniform national standard to establish consent to share information. Some states require a veteran to actively opt in for exchange of records, while others only offer an opportunity to opt out, resulting in an uneven patchwork quilt of policies and procedures from state to state and within individual VA networks. In addition, non-VA health care systems are generally unable to identify veterans within their own caseloads, which limits their ability to create and use databases to further understand potential veteran populations in order to enhance their access to MISSION Act services. Such databases could also serve to identify eligible veterans in non-VA care systems who could benefit by enrollment in VA’s WHS.
Many of these same problems make transitions between community-based hospitals and follow-up VA care inefficient and potentially unsafe. Investigators have found that transitions from medical hospitalizations to VA primary care outpatient follow-up were often delayed because providers
at community hospitals were unable to identify patients as veterans or notify the VA primary care clinician that they had discharged the veteran (Ayele et al., 2019). In addition, community providers at non-VA hospitals were unable to write orders for VA formulary medications that veterans could fill at VA pharmacies, to transfer non-VA medical records to the veteran’s primary care clinician, or to arrange for follow-up appointments for veterans with the VA primary care clinician. Because the study’s authors could not identify standardized processes for these transitions, they suggested that VA create a liaison position to provide care coordination and educate veterans about the transition process.
A systematic review of care coordination across VA and community facilities for rural veterans highlighted many of these same coordination challenges. In addition, this review also identified other barriers as well as potential facilitators for coordination across systems (Garvin et al., 2021). For example, care coordination was more successful between VA and community settings when organizational policy and administration practices, such as credentialing, contracting, authorization, scheduling, performance measurement, reimbursement, and eligibility, were clear, closely aligned, or agreed upon between VA and community care systems. An organizational culture that was characterized as bureaucratic, insular, and risk averse was a perceived barrier to coordination, especially when present at VA. Timely, bidirectional information sharing was often a problem between VA and community settings, forcing veterans to bear responsibility for carrying their own records back and forth between systems. Cultural facilitators for coordination included VA’s commitment to people-centeredness, interprofessional teams, CIH, and cultural sensitivity. The authors concluded that VA leadership responsible for care coordination can learn from best and worst practices to continuously improve both processes and culture.
In summary, the MISSION Act was developed to boost veterans’ access to timely, high-quality health care through integration of the VA and community health systems. However, for a variety of reasons outlined above, many of which are outside VA’s control, VA has struggled to meet its intended purpose. While many of the new collaborations between VA and community systems and services developed through the MISSION Act could potentially accelerate scaling of whole health care to enrolled veterans receiving health services outside of VHA facilities, these same challenges apply.
Another key question for VA’s WHS is whether the MISSION Act, which specifies its focus on hospital care, medical services, and extended care services to covered veterans through health care providers, would even cover services that address upstream factors of health and well-being that are critical to scaling and spreading a whole health approach but that are typically delivered outside traditional clinical settings. If VA wants to scale
and spread whole health for veterans receiving care through MISSION Act eligibility, it will likely have to clarify if community providers under current MISSION Act rules can provide all whole health services, particularly those that address the upstream factors that contribute to health and well-being.
While resolving these difficult issues is beyond the scope of this committee, these are barriers that VA must confront in scaling whole health services for veterans eligible for VA care. Integrating across systems is particularly challenging because each VA site of care must deal with a wide range of procedural, communication, data sharing, and interoperability issues specific to its community and region while simultaneously managing local differences in population demographics and needs. (See Box 6-2 for information on communication networks to facilitate linkage to whole health services.) Addressing these issues calls for new flexibilities in forming partnerships, sharing space, expediting hiring processes (possibly including the option to jointly hire staff who can operate between systems), setting reimbursement schedules, and ensuring prompt and appropriate payment. Third-party administrators should be held to national standards that ensure that veterans have robust access to integrated primary/mental health and specialty care within their communities via physical or virtual means.
Success in overcoming these barriers will require effective coordination across dozens of disparate programs and services, each of which is staffed with people accustomed to doing things their own way. VA itself will need to overcome challenges with the interoperability of its EHR (see Chapter 7), as will other health systems, small practices, and independent providers. As required by the MISSION Act, community partners must achieve the cultural competence and knowledge of VA programs and benefits necessary to effectively serve veterans and coordinate care with VA. It is imperative that VA makes the process of integration attractive and efficient for community providers while also ensuring that financial abuse of the system is minimized.
Until such progress is made, VA’s clinical integration with community services to expand whole person care to veterans receiving care outside VA through the VA MISSION Act will remain elusive. This is unfortunate because successful implementation of the MISSION Act could serve as a powerful driver of whole health spread across the nation.
INTEGRATING SERVICES TO SCALE AND SPREAD WHOLE HEALTH
Along with systems change and structures and processes required for scale and spread, achieving whole health at scale will require services to be integrated. Integrated health care is care coordinated across professionals, facilities, and support systems; that is continuous over time and between visits; and that is tailored to personal and family needs, values, and preferences
(Singer et al., 2011). It is not the same as integrative health or integrative care, also known as complementary and integrative health, which is best described as medical practice that retains many of the characteristics and strengths of conventional medical care while also embracing more holistic, complementary concepts and methods whose theory and practice may not be part of traditional western biomedicine (Rakel and Weil, 2003). While delivering whole health requires the integration of biomedicine and CIH, integration applies to the health system broadly. Effectively spreading whole health services requires enabling integrated services within and among interprofessional care teams, delivery systems, and health ecosystems. It also requires integrating services across clinical and nonclinical services that support the foundational elements of whole health and that may or may not exist within a given health system as well as integrating services over people’s lifespans (Singhal et al., 2020).
Integrating within organizational boundaries is challenging, albeit often less challenging than integrating beyond them. Research suggests that integration was better within practice sites than within physician organizations and within health systems and that it was lowest for care provided outside health systems (Singer et al., 2020b). In determining how it will deliver whole health, each health system will need to assess its own capacity and strengths and determine the array of services it will provide itself; the rest it will need to outsource by acquiring those capacities from other organizations that offer them through some form of contracted relationship. These “make-versus-buy” decisions will have significant implications for health systems’ ability to integrate whole health care. Considerations will include physical, functional, and financial challenges in creating necessary clinical space; availability of partners with the necessary capabilities, capacity, and quality; proximity and accessibility of potential partners for patients and referral sources; tax implications of different arrangements; implications for potential return on investment; availability of reliable, secure, and interoperable EHRs and data systems; and the challenges of effectively integrating new partners/contract workers into existing systems (Calnan, 2008).
Enabling integrated services in practice, within or across organizational boundaries, requires consideration beyond ownership arrangements between health care entities (Blumenthal, 2020). This committee adopts the comprehensive theory of integration (Singer et al., 2020a), which suggests that integration encompasses organizational components, including both structural features and clinical and administrative functions, as well as social components, including norms and interpersonal relationships, that together facilitate the integration of clinical processes, which result in integrated care (Singer et al., 2020a; Valentijn et al., 2015). Research indicates that integration becomes harder to achieve outside of existing health systems (Singer et al., 2020a) and that both organizational and social
aspects of integration are important for providing truly integrated services (Kerrissey et al., 2022; Singer et al., 2020a). Integration thus calls for more than mere co-location or coordination; it requires creating a unified whole among disparate parts through shared programs, processes, and ways of thinking, as the examples presented in Chapter 4 convey.
To achieve whole health, different individuals will require different combinations of integrated services. Patients with multiple chronic conditions may receive care from multiple specialists as well as from home- and community-based services, while young families in socioeconomic distress may primarily require coordination between primary care, mental health, assistance with housing, and access to good nutrition. The processes that support integration must also be able to adapt to the values and needs of a diverse population with different preferences as to where and how to receive care, whether individuals access care in person or virtually, or whether they access care individually or with family or caregivers.
The array of services needed to support scaling and spreading whole health includes clinical services offered within health systems as well as support services that address upstream factors that contribute to health, such as housing, vocational assistance, childcare, and well-being programs that are not customarily considered part of patient care. As the Implementing High-Quality Primary Care report details (NASEM, 2021), these services are best anchored in the framework of primary care. That report suggests—and whole health requires—that high-quality primary care includes
- Collaborative engagement through longitudinal relationships;
- Co-located, coordinated mental health care;
- Access to substance use interventions;
- Efficient handoff procedures to more specialized care in both ambulatory and inpatient environments;
- Reliable, affordable access to rehabilitative services when needed;
- Practice agreements that return patients to lower levels of care as acuity and severity improve; and
- CIH services such as acupuncture, yoga, mindfulness, and meditation.
Successful, high-quality or high-value organizational integration of clinical services in any setting, VA or otherwise, requires that systems have supportive structures in place and that they act to scale and spread in accordance with the 10 key principles described earlier in this chapter. Overcoming barriers to scaling and spreading whole health requires integration across all services and settings as well as consideration of changing needs and preferences at different life stages as valued by individuals, families, and communities. In the following sections the committee highlights some key
areas where enhanced integration could substantially improve movement toward whole health at scale. These include the integration and spread of
- Primary care with behavioral health care;
- Conventional medical care with complementary and integrative health;
- Social needs assessment and care with clinical care; and
- Health coaches, community health workers, peer specialists, and care coordinators.
After that, the committee considers mechanisms for integration. At the micro (patient with providers and care teams) and meso (within and across teams) levels, the committee suggests that developing, scaling, and spreading new health roles, including health coaches, peer-support specialists, care coordinators, and community health workers, could significantly enhance integration. At the macro level (integration within and across health systems), the committee suggests that by building on past achievements and its ongoing mission and responsibilities, the Health Resources and Services Administration could play a key role in integrating services to scale and spread whole health.
Integration and Spread of Primary Care and Behavioral Health Care
Of all the clinical integration efforts throughout U.S. health care, the evidence in support of integrating behavioral health with primary care is the strongest, with documented benefits of better health outcomes, better quality of care, lower costs, lower rates of emergency department visits, and lower rates of hospital admissions (NASEM, 2021). Within VA, integrated behavioral health and primary care is already the norm, with veterans assigned to a primary care team that includes an integrated mental health component of varying size and complexity appropriate to local needs and capabilities. VA’s Primary Care–Mental Health Integration program is a good example of integration that has increased veterans’ access to and use of mental health services (Johnson-Lawrence et al., 2012; Leung et al., 2017, 2019; Possis et al., 2020). At the national level, VA’s Center for Integrated Health provides a broad menu of clinical, research, and administrative resources upon which other health care systems can build.
Integrated primary care and mental/behavioral health programs assist patients across a wide range of health and wellness domains, such as prevention, assessment, and treatment. When needed, integrated primary care and mental/behavioral health programs can refer patients to more complex levels of service provided by a diverse array of specialty and subspecialty
mental health and substance use services, including inpatient and residential treatment. Treatment plans are developed in partnership with the patient and family and may include ways to help with stress, maladaptive behaviors, and other problems that interfere with daily life and pose short- and long-term threats to overall health. Examples include smoking cessation (Ebert et al., 2014), weight management (Ma et al., 2019), exercise/behavioral activation (Coenen et al., 2020; Gros and Haren, 2011), and enhanced coping skills such as mindfulness and problem-solving therapy for depression and anxiety (Leung et al., 2017; Zhang et al., 2018). Integrated primary care and mental/behavioral health programs play a particularly important role in addressing complaints frequently encountered in primary care settings, including sleep problems (Goodie et al., 2009), high blood pressure (Leung et al., 2022), diabetes (Chwastiak et al., 2017), asthma (Gait et al., 2019), and substance use (Karapareddy, 2019; Sterling et al., 2011), and are particularly valuable in addressing chronic pain either without opiates or by managing the risk for opioid dependence (Gleadhill et al., 2021; Leasure and Leasure, 2017). Studies have also found that consumers view integrated primary care and mental/behavioral health care favorably (Rollins et al., 2017; Tabvuma et al., 2022). Despite research that demonstrates significant value for patients and their health systems through integrated primary care and mental and behavioral health services (Huffman et al., 2014; Reed et al., 2016; Reiss-Brennan, 2014), these modalities remain separate within many if not most systems of care.
The Department of Health and Human Services (HHS) recently released its Roadmap for Behavioral Health Integration (Bagalman et al., 2022), which details policy solutions to help integrate mental health and substance use care into large health care systems. This approach is founded on three pillars: (1) strengthening system capacity by developing a diverse workforce that is prepared to practice in integrated settings, many of which operate outside of traditional health care settings such as hospitals or clinics, and investing in new infrastructure; (2) taking advantage of health financing arrangements, including efforts to fully realize the potential of mental health parity; and (3) making new investments in behavioral health promotion, upstream prevention, and recovery.
Collaborative chronic care models improve the outcome of multiple mental health conditions, such as major depression, when they are treated in a primary care setting (Archer et al., 2012; Bauer et al., 2019). In collaborative care, primary care physicians work with a care manager—often a psychiatric nurse, social worker (Chang et al., 2013), or psychologist—and a consulting psychiatrist to proactively identify, treat, and monitor people with mental health conditions. Key elements of collaborative care include population-based patient identification, continual symptom monitoring using an electronic registry, measurement-based care to track treatment
response and identify patients who are not improving, and a stepped-care approach to systematically adjust treatment for patients who are not meeting targets (Katon, 2012). The benefits of this approach to care are seen not only in adults but also in children and adolescents (Asarnow et al., 2015; Ougrin et al., 2015).
Research has found that implementing collaborative care can be challenging because it is a complex intervention. A meta-analysis of studies on collaborative care for depression and anxiety identified a number of barriers to and enablers of successful implementation (Overbeck et al., 2016). The engagement of the primary care team lead and psychiatrist was a critical enabler for successful implementation (Curran et al., 2012; Eghaneyan et al., 2014), while a lack of such engagement, resulting from time pressures, competing priorities, worries about clinical autonomy, and discomfort diagnosing and treating mental health conditions, was a significant barrier (Coupe et al., 2014; Eghaneyan et al., 2014; Knowles et al., 2013; Wozniak et al., 2015).
Several studies indicate that co-location of the primary care team and a care manager is an important enabler (Knowles et al., 2013; Oishi et al., 2003). Face-to-face communication between care managers and primary care clinicians in evaluating new patients as well as the level of professional and social skills of the care manager were associated with enhanced outcomes (Whitebird et al., 2014). One study concluded that the most important factor in implementing collaborative mental health care in primary care settings was having time to spend with patients (Curran et al., 2012). Other important enablers included the quality of training for clinical staff, having a physician champion for the collaborative model, supportive leadership (Sanchez and Adorno, 2013), and appropriate funding for team operating costs related to collaborative care (Whitebird et al., 2014).
Policy changes needed to spread primary care–mental health integration include changing the physical architecture of primary care clinics to accommodate co-located mental health team members, providing financial incentives for multidisciplinary team formation and functions, and increasing accountability for patient outcomes, which includes assessing and addressing the social determinants of health (McGinty and Daumit, 2020).
Integration and Spread of Complementary and Integrative Health
Many health care systems routinely integrate CIH into standard clinical models to better address their patients’ whole person needs (Singer and Adams, 2014), yet while research suggests that primary care clinicians are generally familiar with many CIH therapies and often discuss them with their patients (Schwartz et al., 2021), these services tend to be delivered in settings other than primary care and are often provided by consultants
external to the primary care team or the health care system itself. Such treatments and their outcomes may not be tracked reliably because of a lack of interoperable EHRs and the paucity of procedural terminology codes, which are used for billing purposes, for many CIH therapies (Zeliadt et al., 2020). These factors combine to frustrate efforts to understand the type and intensity of services rendered, assess their clinical benefit, inform future treatment or policy decisions, and better integrate whole health approaches.
According to the National Institutes of Health’s National Center for Complementary and Integrative Health (NCCIH, 2021),11 examples of CIH interventions include
- Nutritional, including special diets, dietary supplements, herbs, and probiotics;
- Psychological, including mindfulness techniques;
- Physical, including massage and spinal manipulation; and
- Combinations of the three, such as yoga, tai chi, acupuncture, dance or art therapies, and nutritional, such as mindful eating.
VA WHS has focused its efforts on six evidence-based CIH therapies: acupuncture, chiropractic, massage, tai chi, mindfulness, and yoga, all of the which HHS’s National Pain Strategy and the American College of Physicians’ low back pain clinical practice guidelines recommend as non-pharmacological pain therapies (Schwartz et al., 2021).
Research and clinical experience demonstrate that many patients find CIH approaches empowering because they provide them with a sense of personal control and achievement in managing their own health (Taylor et al., 2018). Veterans often advocate for access to forms of care that they both value and for which they can take personal responsibility. By providing access to such services, health systems lay the groundwork for their own cultural change and demonstrate a willingness to collaborate with patients, in keeping with the whole health model. As clinical staff become more familiar with CIH and its positive impact on patient health, they become increasingly competent and confident in integrating these practices into care plans. Patients, clinicians, and the health care system all gain from such integration.
VA’s concerted efforts to scale CIH interventions across its system provide a roadmap for spreading CIH across other health care systems. One study identified nine key factors that facilitate CIH integration and implementation: (1) organizing individual CIH approaches into one program instead of spreading them across several departments, (2) developing CIH
___________________
11 Additional information is available at https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name (accessed August 3, 2022).
strategic plans and steering committees, (3) identifying and empowering enthusiastic CIH program leads and practitioners, (4) building leadership support, (5) encouraging positive attitudes about CIH among clinicians, (6) paying attention to patients’ attitudes toward CIH interventions, (7) sharing research evidence of CIH effectiveness, (8) identifying CIH champions, and (9) effectively marketing CIH practices at multiple levels (Taylor et al., 2019). This study also identified common challenges to spreading CIH, including difficulties in hiring trained staff, insufficient and inconsistent CIH funding, lack of patient access to CIH approaches, difficulties in coding and documenting CIH use, insufficient or inappropriate space in which to deliver CIH services, insufficient allotment of staff and provider time, and adverse cultural and geographic environments.
The authors of this study shared several successful strategies in supporting CIH integration, such as facilitating the process for recruiting CIH practitioners. Until recently, a lack of national qualification standards for many CIH specialists hampered recruitment. In response, VA’s Integrative Health Coordinating Center recently developed nationally classified position descriptions for acupuncturists, yoga and tai chi/qi gong instructors, and massage therapists (VA, 2022b).12 Non-VA health care systems could employ these descriptions to accelerate their CIH integration efforts. VA’s efforts to develop CIH coding and tracking infrastructure and guidance provide ready models that non-VA health systems can apply to document CIH implementation and track health outcomes. Because health care workers may lack confidence in their ability to make appropriate CIH referrals, some VA facilities have appointed a clinical lead to review and advise on all CIH consultations. In this way, CIH services are better used, and clinicians are afforded new opportunities to gain competence and confidence in CIH implementation. Non-VA health care systems could replicate this same arrangement.
Unlike many systems, VA’s WHS has successfully integrated CIH therapies into its EHR system, allowing for real-time information monitoring of CIH activities in the same way that VA tracks other clinical activities (Schwartz et al., 2021). This has enabled administrators to better document and monitor WHS activities and inform top leadership responsible for clinical policy and resource decisions.
Research has found that initial steps to implement and integrate CIH practices within a health care system can enhance their spread through a virtuous cycle. One report found that multiple levels of consideration drove leaders’ decisions to provide or withhold support for CIH integration. These
___________________
12 Additional information about the Integrative Health Coordinating Center is available at https://www.va.gov/WHOLEHEALTH/professional-resources/IHCC.asp (accessed August 3, 2022).
considerations included their individual attitudes/knowledge, perceptions of evidence, and personal experiences; their interpersonal interactions with trusted brokers, patients, and loved ones/colleagues/staff; organizational concerns surrounding relative priorities, local resources, and metrics/quality/safety; and system-level policy, bureaucracy, and interorganizational networks (Bolton et al., 2021). Sound strategic planning that results in building critical infrastructure; appropriate, sustainable funding; and recruitment of qualified, respected CIH staff provides the basis for robust integration and spread of CIH within health care systems.
Integration and Spread of Social Needs Care into Health Care
As the 2019 report Integrating Social Needs Care into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health states, improving overall health depends on addressing social needs and vulnerability (NASEM, 2019a). Social needs are integral upstream factors of health—one of the committee’s five foundational elements of whole health—and include access to safe housing, food, and transportation; education, job opportunities, and employment; clean and safe built and natural environments; and financial security, among other factors. While some of these relate to overall community conditions for which local and national policy makers are accountable, such as the natural and built environments of a community, others fall within the purview of clinical and social services. For a whole health system of care to adequately address the upstream factors of health, it must integrate assessing and attending to social needs into its overall care delivery system. The degree to which social needs are integrated into health care delivery, can, however, vary across systems and settings, ranging from
- Screening for social needs in clinical settings and then referring to and relying on other organizations to provide needed services, to
- Developing formal partnerships between health care and social needs organizations to facilitate coordination and more seamlessly deliver and track social needs care, to
- Fully integrating social needs care and health care by addressing the majority of health and social needs within a single, integrated system (Kreuter et al., 2021).
Integrating Social Needs Care into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health details five fundamental activities through which health systems can integrate social needs care into their delivery systems. Specifics will vary depending on the level of integration and availability of resources, but in general will include
- Awareness activities to identify the social needs of patients, such as through either structured or informal assessment;
- Adjustment activities to alter care based on specific social needs, such as by shifting to telehealth services for people who face challenges in arranging leave from work or childcare required to appear for an in-person visit;
- Assistance activities to connect people with services and resources to address social needs and reduce social risk, such as by providing transportation vouchers or other assistance to connect people to services that may not be physically integrated;
- Alignment activities to understand and match social needs with available resources and partner and develop alliances that address population needs, such as by assessing local food bank resources and establishing a partnership or referral system with them; and
- Advocacy activities to promote policies that increase the access, availability, and quality of services that address social needs, such as by working with local social needs organizations, policy makers, and other stakeholders to change local, regional, or national policy to strengthen social needs services and integration.
Several systems that this report highlights demonstrate how integration can be operationalized in different settings to meet distinctive sets of social needs. The Program for All-Inclusive Care for the Elderly (PACE), for example, integrates social needs care into its care model for older, nursing home–eligible adults who want to age independently at home. Social workers are integral members of the PACE interprofessional care team and help ensure that participants’ social needs are met. Mary’s Center is another model that partners with and facilitates connection with social services resources in the surrounding community as needed. Mary’s Center also provides adult and early childhood educational services through partnership with a local public charter school. As an added benefit of integration, the school also serves as a point of entry into other health care services.
At VA, social workers are core PACT members who operationalize social needs–clinical care integration. In 2016 VA began implementing its Social Worker PACT Staffing Program, which increased the number of social workers in rural VA PACTs to help improve access to VA care and services (VA, 2020a). Social workers coordinate a range of services for veterans, including transportation, housing needs, financial needs, and in-home support. They also help identify and address family stress social isolation, mental health issues, substance use issues, and other upstream needs that could negatively affect well-being. While not formally part of VA’s WHS, this program is collaborating with the VA Office of Patient-Centered Care and Cultural Transformation to incorporate more whole health concepts
into its practice. An evaluation of the program found that it slightly reduced emergency room visits and hospitalization among high-risk veterans (Cornell et al., 2020).
As described earlier in this chapter, VA could further integrate social needs care into its WHS by strengthening integration between WHS and VBA services. VA has already achieved success through partnerships with other federal agencies. As an example, a partnership among the Departments of Defense, Labor, and Veterans Affairs established the National Resource Directory (NRD) (NRD, 2022), a resource website that connects wounded warriors, service members, veterans, their families, and caregivers to programs and services that support them. Information in the NRD comes from federal, state, and local government agencies; veteran and military service organizations; nonprofit and community-based organizations; academic institutions; and professional associations.
Another example is the U.S. Department of Housing and Urban Development–VA Supportive Housing (HUD-VASH) Program (VA, 2022d,f), which pairs HUD’s Housing Choice Voucher rental assistance with VA case management and supportive services for homeless veterans. These services assist homeless veterans and their families in finding and sustaining permanent housing and accessing the health care, mental health treatment, substance use counseling, and other supports necessary to help them in their recovery process and with their ability to maintain housing in the community.
Recently, VA initiated a new approach to developing veteran community partnerships (VCPs). VCPs are organized partnerships through which local VA facilities connect with state and local community services and agencies to address the social needs of veterans. Each of these innovations makes it easier for veterans—and those who serve them—to connect with needed support within their own communities and on their own terms.
VA established programs such as the NRD, HUD-VASH, and the VCPs to assist local communities in identifying and, when necessary, developing their capacity to address the committee’s five foundational elements. Unfortunately, many communities continue to face significant challenges (Kreuter et al., 2021) including
- Sustainability—programs are most often grant funded with uncertain futures, making long-term planning, budgeting, and staffing difficult;
- Measurement and outcomes—programs often lack the capacity to measure direct success in terms of defined goals, indirect success in terms of downstream effects, or cost-effectiveness, which can make future funding more difficult to secure and limits their ability to maximize effectiveness through continuous learning;
- Shared savings—programs often lack the ability to leverage shared savings;
- Data and technology—many programs struggle to integrate data from disparate sources, creating coordination challenges among partners; and
- Evidence-based guidance—similar to the case with measurement and outcomes, program leaders may have limited knowledge and skills base or may not be aware of accepted best practices guidance available to programs entering cross-sector partnerships (Amarashingham et al., 2018).
Chapter 7 will describe how many of these challenges reflect the importance of sound structural elements. Examples include supportive payment systems, robust metrics and data analysis, interoperable technology, and systematic diffusion of innovation and best practices.
Integration of Health Coaches, Peer-Support Specialists, Community Health Workers, and Care Coordinators
Health coaches, peer-support specialists, community health workers, and care coordinators all play an integral role in a whole health approach. Although these professionals and peers may have overlapping roles in at least some settings, including VA’s WHS, each tends to take on specific tasks as part of a whole health care team. Health coaches, for example, are expert in empowering patients to articulate and act on their personal health values and preferences in collaboration with their loved ones, clinicians, and community resources (Collins et al., 2015). Peer specialists often work with behavioral health issues and substance use disorders, sharing their own recovery stories, providing encouragement, instilling a sense of hope, and teaching skills (Gaiser et al., 2021). Community health workers are well positioned to build trust and develop collaborations with community partners that help address social determinants of health (Braveman and Gottlieb, 2014; Deng and Shih, 2020; Magnan, 2017). While most health systems tend to at least give lip service to such functions, they are often overlooked in actual practice.
Health Coaches
Health coaches help patients acquire the internal motivation, confidence, and tools they need to adopt and sustain behaviors that can prevent or manage chronic disease and improve overall health and well-being. VA, a leader in using health coaches in mental health and primary care settings, has developed a new workforce of health coaches to promote whole health
attitudes and practices for patients and care team members based on the realization that primary care and mental health professionals rarely have the time needed to sit with patients for discussing possible life changes that could help prevent or mitigate chronic health problems (Wolever et al., 2017). VA’s development of health coaching and the innovative tools and record systems that support their day-to-day function are key support structures in its progressive scaling of whole health. Having been developed by the federal government, these job descriptions, practices, and coding systems are also available to facilitate the spread of whole health principles and practices across the rest of health care.
In non-VA settings, there is evidence that health coaches can improve health outcomes by motivating behavior changes that improve the management of chronic conditions (Kivelä et al., 2014; Willard-Grace et al., 2015). Other examples in the literature demonstrate that interprofessional teams in primary care settings are generally open to integrating health coaches into their practice and value their contributions (Adelman, 2005; Reich et al., 2022). There is evidence that health coaching via telephone can be scaled to a broad population of patients with multiple health conditions (Scuffham et al., 2019; Thom, 2019).
A variety of studies have identified barriers and facilitators to integrating health coaching into health care teams. Research suggests, for example, that to be successful members of the care team, health coaches require extensive training in motivational interviewing, careful caseload management, and structured guidelines to address setting boundaries (Adelman, 2005). One study found that training health coaches to take the initiative and identify patients likely to benefit from coaching without requiring a referral from a provider increases clinician acceptance of health coaches as members of the care team (Reich et al., 2022). Important facilitators for integrating health coaches include instituting effective communication channels between health coaches and clinicians and providing clinicians with information on how health coaches can benefit health care team functioning (Liddy et al., 2014).
Peer-Support Specialists
VA defines a peer-support specialist as a veteran with mental health experience who is actively engaged in their own recovery and that has been trained and certified to help other veterans (VA, 2018). VA peer-support specialists were initially integrated into mental health services but are increasingly being embedded in primary care PACTs, where they encourage veterans to play a more active role in managing their own health and health care. Peer specialists often share their own experiences in dealing with mental health conditions, including PTSD and depression, and in using VA
health resources. They may also assist veterans in identifying and achieving specific life and recovery goals in accordance with whole health principles.
VA has developed a national certification program for its peer-support specialists. Peer-support specialists function in other health settings as well, but certification requirements and identified roles vary across the states, as do pay rates and options for employment. Mental Health America maintains a peer-support center (Mental Health America, 2022b) that describes the core functions of peer support, reviews its research base, and provides information about training programs across the country.
A study examining barriers and facilitators to integrating peer support into health care teams as a means of improving patient health and well-being cited a failure to clearly define and communicate the role of the peer-support specialist within the organization overall and the care team specifically as barriers to implementation (Cabral et al., 2014). Supervisors also reported that when there was a lack of clarity on peer-support roles, it caused confusion in terms of how to train them.
A qualitative study of peer-support specialists in VA primary care–mental health settings, but not VA’s WHS, also found that integration was challenging when peer-support roles were poorly defined. Supervisors reported that while VA resources supporting peer-support implementation were extensive, they were often confusing (Shepardson et al., 2019). Study participants, including the peer-support specialists themselves, stressed that the program lacked the flexibility needed to tailor services to the specific needs of the local veteran population. Team cohesion, stakeholder buy-in, support from leadership, adequate administrative support, and staff education were facilitators to successful integration. In addition, matching peer-support specialists with veterans who share similar lived experiences or who were managing similar conditions facilitated the building of rapport and engagement between the veteran and the peer-support specialist. Study participants reported they believed that evidence of success facilitated maintaining the peer-support program.
Community Health Workers
The American Public Health Association defines a community health worker as “a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served. This trusting relationship enables the worker to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery” (APHA, 2021). Community health workers are expert listeners with lived experience who can bridge culture, language, and literacy to reach people where they are comfortable and promote linkages to resources,
health education, and care coordination. The major areas of community health worker practice include preventive services, outreach to patients with chronic conditions, and connecting individuals to community resources that can address the social determinants of health (Barnett et al., 2018; Larkey et al., 2012; O’Brien et al., 2010; WestRasmus et al., 2012).
VA has implemented the Individualized Management for Patient-Centered Targets (IMPaCT) model, a standardized, scalable, evidence-based program that uses community health workers’ knowledge of the community and lived experience to help patients deal with complex social and behavioral needs, improve chronic disease control, increase access to care, and reduce costs (Kangovi et al., 2018, 2020). After its initial implementation at the Corporal Michael J. Crescenz VA Medical Center in Philadelphia, researchers found that it took only 6 months to develop an IMPaCT program capable of serving 2,000 patients a year. In VA’s experience, IMPaCT produces a 2:1 return within the fiscal year of investment by improving health and care among vulnerable veterans (Kangovi et al., 2018).
In its Community Health Worker Toolkit, the Centers for Disease Control and Prevention (CDC) has compiled a substantial evidence base to support the effectiveness of community health workers. According to the CDC, “this toolkit also includes information that state health departments can use to train and further build capacity for community health workers in their communities, as well as helpful resources that community health workers can use in their communities” (CDC, 2016). The developers of VA’s IMPaCT model have outlined a step-by-step approach for implementing and sustaining a community health worker program at an academic medical center (Morgan et al., 2016). The process begins with identifying high-resource organizations in the community that lose money when community members have poor health outcomes. The next step is to identify champions within those organizations who can define problems that community health workers can address along with metrics for assessing success. After identifying the at-risk population and learning from the perspectives of those at risk, qualitative data are used to evaluate the intervention and quantitative data to calculate the return on investment. Success depends on hiring the right people for the job, ensuring fidelity to the standardized model, and integrating community health workers into the care team through patient referrals, data infrastructure, team huddles, and effective communication via the EHR.
One study that reviewed successful efforts to integrate community health workers into patient-centered medical homes identified four themes as facilitators: the presence of leaders with knowledge of community health workers who championed the model, a clinic culture that favored piloting innovation rather than maintaining established care models, clinic prioritization of patients’ non-medical needs, and leadership perceptions of
sustainability (Rogers et al., 2018). Other studies recommend promoting an understanding of the community health worker’s role on the care team, adapting workflow to increase collaboration, and adopting compatible and user-friendly information technology tools for community health worker use (Lloyd and Thomas-Henkel, 2017; Payne et al., 2017).
Integrating community health workers into the workflow can be challenging. Research indicates that tension may arise about who is responsible for supervising this new workforce and about how to document their work (Garfield and Kangovi, 2019). Community health workers are most often hired, trained, and supervised by nurses, but it may be more effective to assign a social worker with established experience in community engagement to serve as program coordinator and supervisor. Another issue is the lack of policies to ensure that community health workers are reimbursed for their contribution to team-based care (Gutierrez and Campbell, 2014).
Care Coordinators
The CDC defines care coordinators as members of the health care team who manage client caseloads, conduct intake assessment and reassessment, facilitate conversations among interdisciplinary care team members, and expedite client services referrals (CDC, 2022). Many care coordinators are registered nurses, community health workers, or social workers. Some care coordinators have bachelor degrees and have undergone specialized training and supervised clinical experience, while others have a bachelor-level degree-plus and specialized training, including supervised clinical experience. Their main function is to help individuals manage their health throughout the care spectrum, simplify access to care, facilitate improved compliance with treatment plans and prevention measures, and, ultimately, improve care outcomes (Adamson, 2011; Fortuna et al., 2021). Care coordinators can help address barriers related to language and culture, communication, transportation, bias, and fear.
A recent systematic review of 45 articles reporting on 36 studies on the effectiveness of nurse care coordinators concluded that their impact on patient-reported and health service outcomes was inconsistent. However, this review did find an indication from higher-quality studies that nurse care coordination roles were more likely to result in improved patient and health service outcomes where they involved frequent, in-person interactions, had ongoing follow-up with monitoring of disease status, and involved transition care and the application of behavior change principles (Conway et al., 2019).
A survey of care coordinators identified barriers and facilitators to care coordination in patient-centered medical homes which fell into three categories: organizational/system, interpersonal, and individual (Friedman
et al., 2016). Organizational/system barriers included challenging caseloads, a lack of needed functionality in EHR systems, the need to establish alternate communication methods among care team members, and difficulty identifying community resources. Other studies have also documented challenges that care coordinators face managing health informatics, often with incomplete or insufficient health information, poor health IT usability, and lack of interoperability across systems and platforms (Alyousef et al., 2017; Carayon et al., 2012, 2019). Organizational/system facilitators included having strategies for identifying key resources and having onsite patient resources. At the interpersonal level, barriers included clinician and patient resistance and resistance from other health care facilities, while facilitators included developing strong relationships with clinicians and staff at outside organizations and having time to listen to patients and build trust. On the individual level, a barrier to coordination was a lack of attention to self-care and difficulty maintaining appropriate boundaries with patients. One facilitator was to create a forum for social networking and support to reduce care coordinator stress.
THE ROLE OF THE HEALTH RESOURCES AND SERVICES ADMINISTRATION IN SCALING AND SPREADING WHOLE HEALTH
A significant challenge in spreading whole health principles and practices beyond VA and across the United States is the lack of an identified national champion for whole health. As noted above, VA is uniquely qualified to implement a whole health system at enterprise scale because it already incorporates broad health care (VHA) and benefits (VBA) components. Few non-VA health systems are designed to address the full range of whole health needs and, despite the success of programs that Chapter 4 describes and others, most systems in most settings do not have the incentives or resources to adopt a whole health approach of their own. Transformation beyond VA will require leadership at a national level, coherent messaging, standardized metrics, and the capacity to monitor access to and quality of care across the United States. Ideally, a federal agency with close ties to policy makers, intimate experience in health care innovation, and experience in starting up successful national programs capable of changing the health care landscape would take on these tasks.
In considering potential candidates for this role, the committee focused on HRSA as an ideal lead agency for whole health implementation and spread. HRSA pursues a mission to “improve health outcomes and achieve health equity through access to quality services, a skilled health workforce, and innovative, high-value programs” (HRSA, 2022a), and it coordinates more than 90 programs and more than 3,000 grantees. While many of
its programs focus on ensuring equitable health care for people who are geographically isolated and economically or medically vulnerable, HRSA was created to support the entire nation’s health infrastructure and foster a health workforce capable of meeting the nation’s current and emerging needs (HRSA, 2021). Its vision statement of “Healthy Communities, Healthy People” succinctly expresses a core principle of whole health.
As described in HRSA’s 2019–2022 strategic plan, the agency works to achieve health equity, enhance population health, and improve health outcomes by enhancing community partnerships with entities across diverse geographic areas (HRSA, 2022a). HRSA accomplishes this by using local advisory councils to better understand community requirements, integrating public health practices and primary care services, using evidence-based decision making to address health disparities, and promoting illness prevention and healthy behaviors (HRSA, 2022a). By developing and supporting community-based partnerships, HRSA identifies and enhances vital linkages between individuals and communities in need and the services and resources that improve population health. In doing so, it supports community actions that address the social determinants of health and improve health-related infrastructure.
HRSA has demonstrated the ability to accomplish its goals by establishing innovative health systems at national scale. For example, every state in the nation has HRSA-funded maternal and child health programs providing infant screenings and prenatal care; residents receiving care and treatment services through HRSA’s Ryan White HIV/AIDS Program; a HRSA-funded state office of rural health; and services provided by HRSA’s regional telehealth resource centers (HRSA, 2022b).
Of particular relevance, HRSA is the government agency responsible for developing the Health Center Program, which now includes almost 1,400 health centers operating more than 13,500 service delivery sites across every state (HRSA, 2022b). As Chapter 3 discussed, health centers, including FQHCs, provide primary medical, dental, mental health, and substance use services, as well as access to hospital and specialty services, to nearly 29 million people. This constitutes health services for 1 of every 11 people in the United States, including one in three people in poverty, one in seven members of racial and ethnic minorities, one in five people on Medicaid, and one in five of the uninsured (NACHC, 2022). Health centers provide comprehensive services, including preventive health services, on site or by arrangement with community partners. They also arrange transportation as necessary to ensure access to care. Each FQHC has an ongoing quality control system (HRSA, 2020) that requires HRSA Health
Center Program awardees and look-alikes13 to report a core set of information annually, including data on patient characteristics, services provided, clinical processes and health outcomes, patients’ use of services, staffing, costs, and revenues as part of a standardized reporting system known as the Health Center Program Uniform Data System. Each HRSA health center operates under a community-based governing board of directors, a governance model that would be especially helpful in developing whole health approaches appropriate to the resources and needs of local communities. In summary, the nationwide system of HRSA-established health centers creates a node in virtually every community capable of spreading whole health principles and practices.
Two of the systems that Chapters 4 and 5 feature—Southcentral Foundation’s Nuka System of Care in Alaska and Mary’s Center in Washington, D.C.—are both FQHCs, and both illustrate how a whole health approach is compatible and aligned with the overall FQHC mission and certification requirements. While not all FQHCs currently have the resources and infrastructure necessary to meet the whole health needs of their communities, the examples cited in this report demonstrate that the national FQHC model is highly compatible in both mission and policy with a whole health approach. Given progressive development in policy and resource allocation, HRSA’s Health Center Program could fully incorporate the five foundational elements of whole health into its certification requirements.
HRSA was also responsible for starting up area health education centers (AHECs) across all 50 states. The purpose of the AHEC program is to develop and enhance education and training networks within communities, academic institutions, and community-based organizations (HRSA, n.d.). In turn, these networks seek to increase diversity among health professionals, broaden the distribution of the health workforce, enhance health care quality, and improve health care delivery to rural and underserved areas and populations. As such, the national AHEC system is well positioned to drive dissemination of whole health principles and practices across America.
FINDINGS AND CONCLUSIONS
This chapter has addressed key contextual conditions required for whole health scale and spread within VA and across the nation. In doing so, the committee emphasized the need for transforming mindset, culture, structure, and processes, and it reviewed models for systems change and social movement. The committee also identified numerous barriers, including barriers to integrating care, and strategies for overcoming them.
___________________
13 Health center look-alikes meet all of the requirements of a certified health center but do not receive Health Center Program funding.
The shift to whole health will demand top-down (macro and meso) and bottom-up (micro) engagement, support, and buy-in as well as a realignment of venerable infrastructure, policy, and payment systems (see Chapter 7). Change will require recognition that current systems of care are not equipped to deliver desired health outcomes or the bold initiatives that are necessary to achieve them. These are heavy lifts for established programs, but once systems adopt whole health as a core value, they will not need to do everything at once to establish momentum. Health systems are more likely to avoid unintended negative consequences when the gears of top-down and bottom-up change are well meshed. Success will depend on a shared recognition that all members of society are the stakeholders and future beneficiaries of whole health.
Committed leaders need to realign and, in some cases, retool existing structures and processes, and health systems will have to recognize interprofessional teams and integrated delivery systems that balance biomedical and social interventions as core elements of the whole health care ecosystem. Learning from early adopters will illuminate promising paths for whole health dissemination. Health systems can avoid pitfalls by adopting established health delivery innovation frameworks and applying them flexibly to address local conditions.
Although VA has long provided clinical care through the VHA while simultaneously addressing upstream factors through the VBA, it cannot succeed in scaling its WHS in a way that fully addresses all foundational elements of whole health or provide a compelling model for national whole health without greater integration of programs and services that promote education, employment, financial security, and other social determinants of health within VA’s WHS.
Because so many of the services needed to support whole health currently exist in isolation from clinical programs, VA and non-VA health care systems alike should create and strengthen collaboration with community care, social service, and public health systems at local, regional, and, when appropriate, national levels. Communication networks such the new 988 Suicide & Crisis Lifeline will be needed to provide veterans and their health care providers with the information backbone needed for whole health transformation.
Equally important will be integrating mental health and substance use services within primary care clinics through either physical or virtual co-location and maximizing access to CIH services such as acupuncture and yoga. Research has shown that engaging health care personnel in whole health principles and practices improves their resilience while driving diffusion across systems.
Veterans and the non-VA health care programs and systems that serve them are both disadvantaged by a failure to identify patients with a history
of military service. Identifying veterans in non-VA health settings and analyzing databases that describe their numbers and needs can significantly improve the use of whole health resources, reduce the likelihood of redundant and possibly dangerous interventions, and generate new revenue for non-VA health care systems through the provisions of the MISSION Act. Furthermore, enhancing care coordination between VA and non-VA systems could accelerate the spread of whole health.
The lack of a uniform national standard for establishing consent for health information exchange between VA and non-VA health systems, with some states requiring veterans to actively opt in while others only offer an opt out, creates a significant barrier to the safe and effective coordination of care. This could be solved if non-VA systems made it a standard practice to ask each identified veteran for consent to share health information with VA.
VA should extend its whole health approach to older veterans, women’s health, maternal health, family health, LGBTQ+ health, chronic disease management, and healthy aging. VA and non-VA systems should incorporate a longitudinal approach to whole health across each person’s life and health trajectories. Whole health care should be tailored to the community it serves, and each community needs to assess and address gaps which limit access to clinical and social services.
Because physical, mental health, social, and financial problems at the time of separation from the military are associated with long-term adjustment problems among veterans, the VA should incorporate assessment and early intervention strategies within its transition assistance program. Early identification of readjustment challenges, whether physical, mental, social, occupational, or spiritual, would facilitate veterans’ engagement with VA whole health and create significant downstream advantages for veterans, their families, and VA while also accelerating the scaling of WHS across VA.
Congress framed MISSION Act language specific to hospital care, medical services, and extended care services. These provisions are intended to enhance access to standard medical care, but it is unclear whether they also allow VA to extend WHS to veterans by taking advantage of community care through the MISSION Act. To ensure optimal access to WHS for all veterans served by VA, it will be necessary to clarify VA’s authority to purchase such services.
The most significant challenge in spreading whole health principles and practices beyond VA is the lack of a designated national champion for whole health. Transformation beyond VA will require leadership at a national level, coherent messaging, standardized metrics, and the capacity to monitor access to and quality of care across the country. Ideally a federal agency with close ties to policy makers, intimate experience with health care innovation, and experience in starting up successful national programs capable of changing the health care landscape would take the lead is this
effort. The committee has concluded that HRSA is the ideal lead agency for whole health implementation and spread because of its mission to improve health outcomes, equity, and quality with a focus on the undeserved. HRSA has demonstrated its ability to support and enhance the nation’s health infrastructure and foster a health workforce capable of meeting current and emerging needs. Its success through its Health Center Program and area health education centers speaks to its readiness to take on the task of national whole health spread.
REFERENCES14
Adamson, M. 2011. The patient-centered medical home: An essential destination on the road to reform. American Health and Drug Benefits 4(2):122–124.
Adelman, A. M. 2005. Integrating a health coach into primary care: Reflections from the Penn State Ambulatory Research Network. Annals of Family Medicine 3(Suppl 2):S33–S35.
Alidina, S., M. Rosenthal, E. Schneider, and S. Singer. 2016. Coordination within medical neighborhoods insights from the early experiences of Colorado patient-centered medical homes. Health Care Management Review 41(2):101–112.
Alley, D. E., C. N. Asomugha, P. H. Conway, and D. M. Sanghavi. 2016. Accountable health communities—Addressing social needs through Medicare and Medicaid. New England Journal of Medicine 374(1):8–11.
Altschuler, J., D. Margolius, T. Bodenheimer, and K. Grumbach. 2012. Estimating a reasonable patient panel size for primary care physicians with team-based task delegation. Annals of Family Medicine 10(5):396–400.
Alyousef, B., P. Carayon, P. Hoonakker, A. S. Hundt, D. Salek, and J. Tomcavage. 2017. Obstacles experienced by care managers in managing information for the care of chronically ill patients. International Journal of Human–Computer Interaction 33(4):313–321.
Amarashingham, R., B. Xie, A. Karam, N. Nguyen, and B. Kapoor. 2018. Using community partnerships to integrate health and social services for high-need, high-cost patients. Issue Brief (Commonwealth Fund) 2018:1–11.
Andrews, M. 2016. 1965: The year that brought civil rights to the nation’s hospitals. https://khn.org/news/1965-the-year-that-brought-civil-rights-to-the-nations-hospitals/ (accessed December 5, 2022).
APHA (American Public Health Association). 2021. Community health workers. https://www.apha.org/apha-communities/member-sections/community-health-workers (accessed September 1, 2022).
Archer, J., P. Bower, S. Gilbody, K. Lovell, D. Richards, L. Gask, C. Dickens, and P. Coventry. 2012. Collaborative care for depression and anxiety problems. Cochrane Database of Systematic Reviews 2012(10):CD006525.
Ariadne Labs. 2022. The Ariadne Labs. https://www.ariadnelabs.org/about-us/ariadne-labsarc/ (accessed November 8, 2022).
Asarnow, J. R., M. Rozenman, J. Wiblin, and L. Zeltzer. 2015. Integrated medical-behavioral care compared with usual primary care for child and adolescent behavioral health: A meta-analysis. JAMA Pediatrics 169(10):929–937.
___________________
14 The reference list was updated after a prepublication version of the report was provided to VA.
Ayele, R. A., E. Lawrence, M. McCreight, K. Fehling, R. E. Glasgow, B. A. Rabin, R. E. Burke, and C. Battaglia. 2019. Perspectives of clinicians, staff, and veterans in transitioning veterans from non-VA hospitals to primary care in a single VA healthcare system. Journal of Hospital Medicine 14(3):E1–E7.
Bagalman, E., J. Dey, L. Jacobus-Kantor, B. Stoller, K. D. West, L. Radel, A. Schreier, M. Rousseau, M. Blanco, T. B. Creedon, E. Nye, M. M. Ali, J. M. Dubenitz, D. Schwartz, J. O. White, A. J. Swenson-O’Brien, S. Oberlander, J. Burnszynski, M. Lynch-Smith, L. Bush, G. Kennedy, T. B. Sherry, and R. L. Haffajee. 2022. HHS roadmap for behavioral health integration. Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. https://aspe.hhs.gov/reports/hhs-roadmap-behavioral-health-integration (accessed November 8, 2022).
Barker, P. M., A. Reid, and M. W. Schall. 2015. A framework for scaling up health interventions: Lessons from large-scale improvement initiatives in Africa. Implementation Science 11(1):12.
Barnett, M. L., A. Gonzalez, J. Miranda, D. A. Chavira, and A. S. Lau. 2018. Mobilizing community health workers to address mental health disparities for underserved populations: A systematic review. Administration and Policy in Mental Health and Mental Health Services Research 45(2):195–211.
Bass, E., H. Goldberg, and J. Kerman. 2021. The Veterans Community Care Program: Background and early effects. Washington, DC: Congressional Budget Office.
Bauer, M. S., K. Weaver, B. Kim, C. Miller, R. Lew, K. Stolzmann, J. L. Sullivan, R. Riendeau, S. Connolly, J. Pitcock, S. M. Ludvigsen, and A. R. Elwy. 2019. The Collaborative Chronic Care Model for mental health conditions. Medical Care 57(Suppl 3):S221–S227.
Beers, C. W. 1907. A mind that found itself. London: Longmans, Green and Co.
Benzer, J. K., D. Gurewich, S. J. Singer, N. M. McIntosh, D. C. Mohr, V. G. Vimalananda, and M. P. Charns. 2020. A mixed methods study of the association of non-Veterans Affairs care with veterans’ and clinicians’ experiences of care coordination. Medical Care 58(8):696–702.
Bidassie, B. 2017. The Veterans Affairs Patient Aligned Care Team (VA PACT), a new benchmark for patient-centered medical home models: A review and discussion. London: IntechOpen.
Blumenthal, D. 2020. Making integration work. Health Services Research 55(Suppl 3): 1031–1032.
Bodenheimer, T., and B. Y. Laing. 2007. The teamlet model of primary care. Annals of Family Medicine 5(5):457–461.
Bodenheimer, L., J. DeGennaro, A. Chopra, and J. LeComte. 2019. Quality improvement: An interdepartmental pilot program to improve geriatric integrated behavioral health into a primary care practice. Journal of the American Geriatrics Society 67(Suppl 1):S46.
Boersma, P., L. I. Black, and B. W. Ward. 2020. Prevalence of multiple chronic conditions among U.S. adults, 2018. Preventing Chronic Disease 17:200130.
Bolton, R. E., B. G. Bokhour, K. Dvorin, J. Wu, A. R. Elwy, M. Charns, and S. L. Taylor. 2021. Garnering support for complementary and integrative health implementation: A qualitative study of VA healthcare organization leaders. Journal of Alternative and Complementary Medicine 27(S1):S81–S88.
Braithwaite, J., R. Clay-Williams, E. Vecellio, D. Marks, T. Hooper, M. Westbrook, J. Westbrook, B. Blakely, and K. Ludlow. 2016. The basis of clinical tribalism, hierarchy and stereotyping: A laboratory-controlled teamwork experiment. BMJ Open 6(7):e012467.
Braveman, P., and L. Gottlieb. 2014. The social determinants of health: It’s time to consider the causes of the causes. Public Health Reports 129(1 Suppl 2):19–31.
Cabral, L., H. Strother, K. Muhr, L. Sefton, and J. Savageau. 2014. Clarifying the role of the mental health peer specialist in Massachusetts, USA: Insights from peer specialists, supervisors and clients. Health & Social Care in the Community 22(1):104–112.
Calnan, J. B. 2008. Decisions, decisions. Medical office space: Buy, lease, or walk away? https://healthcarenews.com/decisions-decisions-medical-office-space-buy-lease-or-walk-away-2/ (accessed November 8, 2022).
Carayon, P., B. Alyousef, P. Hoonakker, A. S. Hundt, R. Cartmill, J. Tomcavage, A. Hassol, K. Chaundy, S. Larson, J. Younkin, and J. Walker. 2012. Challenges to care coordination posed by the use of multiple health it applications. Work 41(Suppl 1):4468--4473.
Carayon, P., P. Hancock, N. Leveson, I. Noy, L. Sznelwar, and G. van Hootegem. 2015. Advancing a sociotechnical systems approach to workplace safety—Developing the conceptual framework. Ergonomics 58(4):548–564.
Carayon, P., A. S. Hundt, and P. Hoonakker. 2019. Technology barriers and strategies in coordinating care for chronically ill patients. Applied Ergonomics 78:240–247.
Castellano, J. 2021. The Mission Act is supposed to help U.S. veterans get health care outside the VA. For some, it’s not working. USA Today, November 1. https://www.usatoday.com/in-depth/news/investigations/2021/11/01/mission-act-aid-veterans-healthcare-va-isnt-letting-it/8561618002/ (accessed November 10, 2022).
CDC (Centers for Disease Control and Prevention). 2016. Community health worker (CHW) toolkit. https://www.cdc.gov/dhdsp/pubs/toolkits/chw-toolkit.htm (accessed November 8, 2022).
CDC. 2022. STEPS to care: Care team coordination. https://www.cdc.gov/hiv/effective-interventions/treat/steps-to-care/dashboard/care-team-coordination.html (accessed November 8, 2022).
Chang, E. T., D. E. Rose, E. M. Yano, K. B. Wells, M. E. Metzger, E. P. Post, M. L. Lee, and L. V. Rubenstein. 2013. Determinants of readiness for primary care–mental health integration (PC-MHI) in the VA health care system. Journal of General Internal Medicine 28(3):353–362.
Charif, B. A., H. T. V. Zomahoun, A. LeBlanc, L. Langlois, L. Wolfenden, S. L. Yoong, C. M. Williams, R. Lépine, and F. Légaré. 2017. Effective strategies for scaling up evidence-based practices in primary care: A systematic review. Implementation Science 12(1):139.
Charns, M. P., J. K. Benzer, N. M. McIntosh, D. C. Mohr, S. J. Singer, and D. Gurewich. 2022. A multi-site case study of care coordination between primary care and specialty care. Medical Care 60(5):361–367.
Chaudhry, B., J. Wang, S. Wu, M. Maglione, W. Mojica, E. Roth, S. C. Morton, and P. G. Shekelle. 2006. Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Annals of Internal Medicine 144(10):742–752.
Chien, A. T., M. A. Kyle, A. S. Peters, K. H. Nguyen, S. A. Tendulkar, M. Ryan, K. Hacker, and S. J. Singer. 2018. Establishing teams: How does it change practice configuration, size, and composition? Journal of Ambulatory Care Management 41(2):146–155.
Chwastiak, L. A., S. L. Jackson, J. Russo, P. DeKeyser, M. Kiefer, B. Belyeu, K. Mertens, L. Chew, and E. Lin. 2017. A collaborative care team to integrate behavioral health care and treatment of poorly-controlled type 2 diabetes in an urban safety net primary care clinic. General Hospital Psychiatry 44:10–15.
Coenen, P., G. Hulsegge, J. G. Daams, R. C. van Geenen, G. M. Kerkhoffs, M. W. van Tulder, J. A. Huirne, J. R. Anema, and P. P. Kuijer. 2020. Integrated care programmes for sport and work participation, performance of physical activities and quality of life among orthopaedic surgery patients: A systematic review with meta-analysis. BMJ Open Sport & Exercise Medicine 6(1):e000664.
Collins, D. A., S. R. Shamblen, K. A. Atwood, D. L. Rychener, W. H. Scarbrough, M. H. Abadi, and L. A. Simmons. 2015. Evaluation of a health coaching course for providers and staff in Veterans Health Affairs medical facilities. Journal of Primary Care & Community Health 6(4):250–255.
Conway, A., C. O’Donnell, and P. Yates. 2019. The effectiveness of the nurse care coordinator role on patient-reported and health service outcomes: A systematic review. Evaluation & the Health Professions 42(3):263–296.
Cornell, P. Y., C. W. Halladay, J. Ader, J. Halaszynski, M. Hogue, C. E. McClain, J. W. Silva, L. D. Taylor, and J. L. Rudolph. 2020. Embedding social workers in Veterans Health Administration primary care teams reduces emergency department visits. Health Affairs 39(4):603–612.
Côté-Boileau, É., J. L. Denis, B. Callery, and M. Sabean. 2019. The unpredictable journeys of spreading, sustaining and scaling healthcare innovations: A scoping review. Health Research Policy and Systems 17(1):84.
Coupe, N., E. Anderson, L. Gask, P. Sykes, D. A. Richards, and C. Chew-Graham. 2014. Facilitating professional liaison in collaborative care for depression in UK primary care: A qualitative study utilising normalisation process theory. BMC Family Practice 15:78.
Crawford, E. F., E. B. Elbogen, H. R. Wagner, H. Kudler, P. S. Calhoun, M. Brancu, and K. A. Straits-Troster. 2015. Surveying treatment preferences in U.S. Iraq–Aafghanistan veterans with PTSD symptoms: A step toward veteran-centered care. Journal of Traumatic Stress 28(2):118–126.
CRS (Congressional Research Service). 2021. Department of Veterans Affairs FY 2022 appropriations. Washington, DC: Congressional Research Service.
Cunningham, R., and M. K. Walton. 2016. Partnering with patients to improve care: The value of patient and family advisory councils. Journal of Nursing Administration 46(11):549–551.
Curran, G. M., G. Sullivan, P. Mendel, M. G. Craske, C. D. Sherbourne, M. B. Stein, A. McDaniel, and P. Roy-Byrne. 2012. Implementation of the CALM intervention for anxiety disorders: A qualitative study. Implementation Science 7:1–11.
Daines, S., R. Scott, R. Johnson, R. Marshal, C. Lummis, M. Braun, J. Thune, M. Rubio, and T. Cruz. 2022. Letter to the honorable Denis R. Mcdonough. https://s3.documentcloud.org/documents/22088965/va-community-care-final-7142022.pdf (accessed August 24, 2022).
Dearing, J. W., and J. G. Cox. 2018. Diffusion of innovations theory, principles, and practice. Health Affairs (Millwood) 37(2):183–190.
Deng, I. X., and P. Shih. 2020. Social determinants of health: The unaddressed variable accounting for 80% of health outcomes. Arlington, VA: Care Journey.
Derefinko, K. J., T. A. Hallsell, M. B. Isaacs, L. W. Colvin, F. I. Salgado Garcia, and Z. Bursac. 2019. Perceived needs of veterans transitioning from the military to civilian life. Journal of Behavioral Health Services & Research 46(3):384–398.
DeWalt, D. A., J. Oberlander, T. S. Carey, and W. L. Roper. 2005. Significance of Medicare and Medicaid programs for the practice of medicine. Health Care Financing Review 27(2):79–90.
DoD (Department of Defense). 2022. Military discharge data. https://skillbridge.osd.mil/separation-map.htm (accessed August 28, 2022).
Dryden, E. M., R. E. Bolton, B. G. Bokhour, J. Wu, K. Dvorin, L. Phillips, and J. K. Hyde. 2021. Leaning into whole health: Sustaining system transformation while supporting patients and employees during COVID-19. Global Advances in Health and Medicine 10:21649561211021047.
Duffy, T. P. 2011. The Flexner report—100 years later. Yale Journal of Biology and Medicine 84(3):269–276.
Ebert, L., C. Malte, K. Hamlett-Berry, J. Beckham, M. McFall, and A. Saxon. 2014. Use of a learning collaborative to support implementation of integrated care for smoking cessation for veterans with posttraumatic stress disorder. American Journal of Public Health 104(10):1935–1942.
Edmondson, A. 2018. The fearless organization: Creating psychological safety in the workplace for learning, innovation, and growth. New York: Wiley.
Eghaneyan, B. H., K. Sanchez, and D. B. Mitschke. 2014. Implementation of a collaborative care model for the treatment of depression and anxiety in a community health center: Results from a qualitative case study. Journal of Multidisciplinary Healthcare 7:503–513.
Farmer, C. M., S. Hosek, and D. Adamson. 2016. Balancing demand and supply for veterans’ health care. Santa Monica, CA: RAND Corporation.
Fisher, E. S. 2008. Building a medical neighborhood for the medical home. New England Journal of Medicine 359(12):1202–1205.
Flexner, A. 2002. Medical education in the United States and Canada. From the Carnegie Foundation for the Advancement of Teaching, bulletin number four, 1910. Bulletin of the World Health Organization 80(7):594–602.
Fortuna, R. J., W. Johnson, J. S. Clark, S. Messing, S. Flynn, and S. R. Judge. 2021. Impact of patient-centered medical home transformation on providers, staff, and quality. Population Health Management 24(2):207–213.
Frenk, J., L. Chen, Z. A. Bhutta, J. Cohen, N. Crisp, T. Evans, H. Fineberg, P. Garcia, Y. Ke, P. Kelley, B. Kistnasamy, A. Meleis, D. Naylor, A. Pablos-Mendez, S. Reddy, S. Scrimshaw, J. Sepulveda, D. Serwadda, and H. Zurayk. 2010. Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. The Lancet 376(9756):1923–1958.
Friedman, A., J. Howard, E. K. Shaw, D. J. Cohen, L. Shahidi, and J. M. Ferrante. 2016. Facilitators and barriers to care coordination in patient-centered medical homes (PCMHs) from coordinators’ perspectives. Journal of the American Board of Family Medicine 29(1):90–101.
Gaiser, M. G., J. L. Buche, C. C. Wayment, V. Schoebel, J. E. Smith, S. A. Chapman, and A. J. Beck. 2021. A systematic review of the roles and contributions of peer providers in the behavioral health workforce. American Journal of Preventive Medicine 61(4):e203–e210.
Gait, L., C. Hepworth, A. Lilley, N. Minguard, and I. Sinha. 2019. Experiences of participating in a new integrated programme of asthma care: Patients and parents’ perspectives. European Respiratory Journal 54(Suppl 63):PA933.
Garfield, C., and S. Kangovi. 2019. Integrating community health workers into health care teams without coopting them. In Health Affairs Blog, May 10. https://www.healthaffairs.org/do/10.1377/forefront.20190507.746358/full/ (accessed November 8, 2022).
Garvin, D. A., A. C. Edmondson, and F. Gino. 2008. Is yours a learning organization? Harvard Business Review 86(3):109–116, 134.
Garvin, L. A., M. Pugatch, D. Gurewich, J. N. Pendergast, and C. J. Miller. 2021. Interorganizational care coordination of rural veterans by Veterans Affairs and community care programs: A systematic review. Medical Care 59(Suppl 3):S259–S269.
George, A. S., J. Campbell, and A. Ghaffar. 2018. Advancing the science behind human resources for health: Highlights from the Health Policy and Systems Research Reader on Human Resources for Health. Human Resources for Health 16(1):80.
Gittell, J. H., J. Beswick, D. Goldmann, and S. S. Wallack. 2015. Teamwork methods for accountable care relational coordination and teamstepps. Health Care Management Review 40(2):116–125.
Gleadhill, C., S. J. Kamper, H. Lee, and C. M. Williams. 2021. Exploring integrated care for musculoskeletal and chronic health conditions. Journal of Orthopaedic & Sports Physical Therapy 51(6):264–268.
Goodie, J., W. Isler, C. Hunter, and A. Peterson. 2009. Using behavioral health consultants to treat insomnia in primary care: A clinical case series. Journal of Clinical Psychology 65:294–304.
Gottlieb, K. 2013. The Nuka system of care: Improving health through ownership and relationships. International Journal of Circumpolar Health 72(1):21118.
Greenhalgh, T., and C. Papoutsi. 2019. Spreading and scaling up innovation and improvement. BMJ 365:l2068.
Greenhalgh, T., J. Wherton, C. Papoutsi, J. Lynch, G. Hughes, C. A’Court, S. Hinder, N. Fahy, R. Procter, and S. Shaw. 2017. Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research 19(11):e367.
Gros, D. F., and W. B. Haren. 2011. Open trial of brief behavioral activation psychotherapy for depression in an integrated Veterans Affairs primary care setting. Primary Care Companion for CNS Disorders 13(4):PCC.11m01136.
Gurewich, D., M. Shwartz, E. Beilstein-Wedel, H. Davila, and A. K. Rosen. 2021. Did access to care improve since passage of the Veterans Choice Act?: Differences between rural and urban veterans. Medical Care 59(Suppl 3):S270–S278.
Gutierrez, K. M., and J. Campbell. 2014. Best practice guidelines for implementing and evaluating community health worker programs in health care settings. Chicago: Sinai Urban Health Institute.
Hartmann, A., and J. F. Linn. 2008. Scaling up: A framework and lessons for development effectiveness from literature and practice. Brookings Institution working paper. https://www.brookings.edu/research/scaling-up-a-framework-and-lessons-for-development-effectiveness-from-literature-and-practice/ (accessed November 8, 2022).
Haun, J. N., C. Melillo, B. A. Cotner, J. McMahon-Grenz, and J. M. Paykel. 2021. Evaluating a whole health approach to enhance veteran care: Exploring the staff experience. Journal of Veterans Studies 7(1):163–173.
Haynes, A. B., T. G. Weiser, W. R. Berry, S. R. Lipsitz, A.-H. S. Breizat, E. P. Dellinger, T. Herbosa, S. Joseph, P. L. Kibatala, M. C. M. Lapitan, A. F. Merry, K. Moorthy, R. K. Reznick, B. Taylor, and A. A. Gawande. 2009. A surgical safety checklist to reduce morbidity and mortality in a global population. New England Journal of Medicine 360(5):491–499.
Health Research & Educational Trust. 2017. Transportation and the role of hospitals. Chicago: Health Research & Educational Trust. http://www.hpoe.org/Reports-HPOE/2017/sdoh-transportation-role-of-hospitals.pdf (accessed November 8, 2022).
Hebert, P. L., C.-F. Liu, E. S. Wong, S. E. Hernandez, A. Batten, S. Lo, J. M. Lemon, D. A. Conrad, D. Grembowski, K. Nelson, and S. D. Fihn. 2014. Patient-Centered Medical Home Initiative produced modest economic results for Veterans Health Administration, 2010–2012. Health Affairs 33(6):980–987.
Heifetz, R. A., and M. Linsky. 2002. Leadership on the line: Staying alive through the dangers of leading. Cambridge, MA: Harvard Business Review Press.
Held, C. 2019. When do we need clinical endpoint adjudication in clinical trials? Upsala Journal of Medical Sciences 124(1):42–45.
Herron, J. L., and K. L. Venner. 2022. A systematic review of trauma and substance use in American Indian and Alaska Native individuals: Incorporating cultural considerations. Journal of Racial and Ethnic Health Disparities. January 28:10.1007.
Hirschhorn, L. R., J. R. Talbot, A. C. Irwin, M. A. May, N. Dhavan, R. Shady, A. L. Ellner, and R. L. Weintraub. 2013. From scaling up to sustainability in HIV: Potential lessons for moving forward. Globalization and Health 9(1):57.
HRSA (Health Resources and Services Administration). n.d. Area Health Education Centers program. https://www.hrsa.gov/grants/find-funding/HRSA-22-053 (accessed August 7, 2022).
HRSA. 2018. Health center program compliance manual. Washington, DC: Health Resources and Services Administration.
HRSA. 2020. Health Center Program Uniform Data System (UDS) data overview. https://data.hrsa.gov/tools/data-reporting/program-data (accessed November 8, 2022).
HRSA. 2021. About HRSA. https://www.hrsa.gov/about (accessed August 2, 2022).
HRSA. 2022a. Strategic plan FY 2019–2022. https://www.hrsa.gov/about/strategic-plan/fy2019-2022 (accessed November 9, 2022).
HRSA. 2022b. 2021 agency overview. https://www.hrsa.gov/about/agency-overview (accessed November 8, 2022).
Huffman, J. C., S. K. Niazi, J. R. Rundell, M. Sharpe, and W. J. Katon. 2014. Essential articles on collaborative care models for the treatment of psychiatric disorders in medical settings: A publication by the Academy of Psychosomatic Medicine Research and Evidence-Based Practice Committee. Psychosomatics 55(2):109–122.
Hysong, S. J., A. B. Amspoker, A. M. Hughes, L. Woodard, F. L. Oswald, L. A. Petersen, and H. F. Lester. 2019. Impact of team configuration and team stability on primary care quality. Implementation Science 14(1):22.
IOM (Institute of Medicine). 1983. Community oriented primary care: New directions for health services delivery. Washington, DC: National Academy Press.
IOM. 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: The National Academies Press.
IOM. 2007. The learning healthcare system: Workshop summary. Washington, DC: The National Academies Press.
IOM. 2009. Integrative medicine and the health of the public: A summary of the February 2009 summit. Washington, DC: The National Academies Press.
Ion, A., N. Sunderji, G. Jansz, and A. Ghavam-Rassoul. 2017. Understanding integrated mental health care in “real-world” primary care settings: What matters to health care providers and clients for evaluation and improvement? Families, Systems, & Health 35:271–282.
Johnson-Lawrence, V., K. Zivin, B. R. Szymanski, P. N. Pfeiffer, and J. F. McCarthy. 2012. VA primary care–mental health integration: Patient characteristics and receipt of mental health services, 2008–2010. Psychiatric Services 63(11):1137–1141.
Kangovi, S., N. Mitra, L. Norton, R. Harte, X. Zhao, T. Carter, D. Grande, and J. A. Long. 2018. Effect of community health worker support on clinical outcomes of low-income patients across primary care facilities: A randomized clinical trial. JAMA Internal Medicine 178(12):1635–1643.
Kangovi, S., N. Mitra, D. Grande, J. Long, and D. Asch. 2020. Evidence-based community health worker program addresses unmet social needs and generates positive return on investment. Health Affairs 39(2):207–213.
Karapareddy, V. 2019. A review of integrated care for concurrent disorders: Cost effectiveness and clinical outcomes. Journal of Dual Diagnosis 15(1):56–66.
Katon, W. 2012. Collaborative depression care models: From development to dissemination. American Journal of Preventive Medicine 42(5):550–552.
Kerrissey, M., Z. Novikov, M. V. Tietschert, and S. Singer. 2022. When perceived team boundaries blur: Inconsistent perceptions and implications for performance. Academy of Management Proceedings 2022(1):17982.
Kilbourne, A. M., D. E. Goodrich, A. N. O’Donnell, and C. J. Miller. 2012. Integrating bipolar disorder management in primary care. Current Psychiatry Reports 14(6):687–695.
Kilpatrick, D. G., C. L. Best, D. W. Smith, H. Kudler, and V. Cornelison-Grant. 2011. Serving those who have served: Educational needs of health care providers working with military members, veterans, and their families. Charleston, DC: Medical University of South Carolina Department of Psychiatry, National Crime Victims Research & Treatment Center.
Kingdon, J. W., and E. Stano. 1984. Agendas, alternatives, and public policies. Vol. 45. Boston: Little, Brown.
Kingdon, J. W. 1995. Agendas, alternatives, and public policies. Second ed. New York City, NY: HarperCollins College Publishers.
Kivelä, K., S. Elo, H. Kyngäs, and M. Kääriäinen. 2014. The effects of health coaching on adult patients with chronic diseases: A systematic review. Patient Education and Counseling 97(2):147–157.
Kivlahan, C., K. Pellegrino, K. Grumbach, S. A. Skootsky, N. Raja, R. Gupta, R. Clarke, T. Balsbaugh, T. Ikeda, L. Friedman, L. Gibbs, and E. Todoki. 2017. Calculating primary care panel size. Oakland, CA: University of California Center for Health Quality and Innovation.
Kligler, B., J. Hyde, C. Gantt, and B. Bokhour. 2022. The whole health transformation at the Veterans Health Administration: Moving from “What’s the matter with you?” to “What matters to you?” Medical Care 60(5):387–391.
Knowles, S. E., C. Chew-Graham, N. Coupe, I. Adeyemi, C. Keyworth, H. Thampy, and P. A. Coventry. 2013. Better together? A naturalistic qualitative study of inter-professional working in collaborative care for co-morbid depression and physical health problems. Implementation Science 8:110.
Kreuter, M. W., T. Thompson, A. McQueen, and R. Garg. 2021. Addressing social needs in health care settings: Evidence, challenges, and opportunities for public health. Annual Review of Public Health 42(1):329–344.
Larkey, L. K., P. M. Herman, D. J. Roe, F. Garcia, A. M. Lopez, J. Gonzalez, P. N. Perera, and K. Saboda. 2012. A cancer screening intervention for underserved Latina women by lay educators. Journal of Womens Health 21(5):557–566.
Leasure, W. B., and E. L. Leasure. 2017. The role of integrated care in managing chronic pain. FOCUS 15(3):284–291.
Lemle, R. B., and S. Gordon. 2021. Broken promises: Veteran health care is being replaced by the private sector. The Hill, November 5. https://thehill.com/opinion/healthcare/580301broken-promises-veteran-health-care-is-being-replaced-by-the-private/ (accessed November 9, 2022).
Leung, L. B., J. Yoon, J. J. Escarce, E. P. Post, K. B. Wells, C. A. Sugar, E. M. Yano, and L. V. Rubenstein. 2017. Primary care–mental health integration in the VA: Shifting mental health services for common mental illnesses to primary care. Psychiatric Services 69(4):403–409.
Leung, L. B., L. V. Rubenstein, J. Yoon, E. P. Post, E. Jaske, K. B. Wells, and R. B. Trivedi. 2019. Veterans Health Administration investments in primary care and mental health integration improved care access. Health Affairs 38(8):1281–1288.
Leung, L. B., L. V. Rubenstein, E. Jaske, L. Taylor, E. P. Post, K. M. Nelson, and A.-M. Rosland. 2022. Association of integrated mental health services with physical health quality among VA primary care patients. Journal of General Internal Medicine 37(13):3331–3337.
Liddy, C., S. Johnston, K. Nash, N. Ward, and H. Irving. 2014. Health coaching in primary care: A feasibility model for diabetes care. BMC Family Practice 15(1):60.
Lloyd, J., and C. Thomas-Henkel. 2017. Integrating community health workers into complex care teams: Key considerations. Hamilton, NJ: Center for Health Care Strategies.
Ma, J., L. G. Rosas, N. Lv, L. Xiao, M. B. Snowden, E. M. Venditti, M. A. Lewis, J. D. Goldhaber-Fiebert, and P. W. Lavori. 2019. Effect of integrated behavioral weight loss treatment and problem-solving therapy on body mass index and depressive symptoms among patients with obesity and depression: The RAINBOW randomized clinical trial. JAMA 321(9):869–879.
Magnan, S. 2017. Social determinants of health 101 for health care: Five plus five. NAM Perspectives. National Academy of Medicine discussion paper. https://nam.edu/socialdeterminants-of-health-101-for-health-care-five-plus-five/ (accessed November 8, 2022).
Martin, T. R., H. Gasoyan, G. Pirrotta, and R. Mathew. 2021. A national survey assessing health information exchange: Readiness for changes to veterans affairs access standards. Perspectives in Health Information Management 18(3):1i.
Martinez, E. A., D. A. Thompson, N. A. Errett, G. R. Kim, L. Bauer, L. H. Lubomski, A. P. Gurses, J. A. Marsteller, B. Mohit, C. A. Goeschel, and P. J. Pronovost. 2011. High stakes and high risk: A focused qualitative review of hazards during cardiac surgery. Anesthesia & Analgesia 112(5):1061–1074.
Massoud, M., G. A. Nielsen, K. Nolan, M. W. Schall, and C. Sevin. 2006. A framework for spread: From local improvements to system-wide change. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement. Available at http://www.ihi.org/resources/Pages/IHIWhitePapers/AFrameworkforSpreadWhitePaper.aspx (accessed November 8, 2022).
Mattocks, K. M., and B. Yehia. 2017. Evaluating the Veterans Choice Program: Lessons for developing a high-performing integrated network. Medical Care 55(Suppl 7 Suppl 1):1–3.
Mattocks, K. M., A. Kroll-Desrosiers, R. Kinney, A. R. Elwy, K. J. Cunningham, and M. A. Mengeling. 2021. Understanding VA’s use of and relationships with community care providers under the Mission Act. Medical Care 59(Suppl 3):S252–S258.
McGinty, E. E., and G. L. Daumit. 2020. Integrating mental health and addiction treatment into general medical care: The role of policy. Psychiatric Services 71(11):1163–1169.
Meadows, S., T. Tanielian, and B. Karney. 2016. The Deployment Life Study: Longitudinal analysis of military families across the deployment cycle. Santa Monica, CA: RAND Corporation.
Mental Health America. 2022a. Home page. https://www.mhanational.org/ (accessed July 6, 2022).
Mental Health America. 2022b. MHA peer support. https://www.mhanational.org/center-peer-support (accessed November 8, 2022).
Meredith, L. S., N. Schmidt Hackbarth, J. Darling, H. P. Rodriguez, S. E. Stockdale, K. M. Cordasco, E. M. Yano, and L. V. Rubenstein. 2015. Emotional exhaustion in primary care during early implementation of the VA’s medical home transformation: Patient-Aligned Care Team (PACT). Medical Care 53(3):253–260.
Meyers, D., L. LeRoy, M. Bailit, J. Schaefer, E. Wagner, and C. Zhan. 2018. Workforce configurations to provide high-quality, comprehensive primary care: A mixed-method exploration of staffing for four types of primary care practices. Journal of General Internal Medicine 33(10):1774–1779.
Milat, A. J., A. Bauman, and S. Redman. 2015. Narrative review of models and success factors for scaling up public health interventions. Implementation Science 10:113.
Milat, A. J., R. Newson, L. King, C. Rissel, L. Wolfenden, A. Bauman, S. Redman, and M. Giffin. 2016. A guide to scaling up population health interventions. Public Health Research & Practice 26(1):e2611604.
Military OneSource. 2022. Home page. https://www.militaryonesource.mil/ (accessed July 13, 2022).
Mitchell, J. D., J. D. Haag, E. Klavetter, R. Beldo, N. D. Shah, L. J. Baumbach, G. J. Sobolik, L. J. Rutten, and R. J. Stroebel. 2019. Development and implementation of a team-based, primary care delivery model: Challenges and opportunities. Mayo Clinic Proceedings 94(7):1298–1303.
Mitchell, R., V. Parker, M. Giles, and N. White. 2010. Review: Toward realizing the potential of diversity in composition of interprofessional health care teams. Medical Care Research and Review 67(1):3–26.
Mohr, D. C., J. K. Benzer, V. G. Vimalananda, S. J. Singer, M. Meterko, N. McIntosh, K. L. L. Harvey, M. N. Seibert, and M. P. Charns. 2019. Organizational coordination and patient experiences of specialty care integration. Journal of General Internal Medicine 34(Suppl 1):30–36.
Montgomery, S. C., J. R. Short, T. Ledermann, J. G. Kimmes, K. E. Longley, E. Manhiri, and J. G. Grzywacz. 2022. Work and family transitions throughout adulthood and the impact on health: A systematic review. Journal of Population Ageing 52:100466.
Morgan, A. U., D. T. Grande, T. Carter, J. A. Long, and S. Kangovi. 2016. Penn Center for Community Health Workers: Step-by-step approach to sustain an evidence-based community health worker intervention at an academic medical center. American Journal of Public Health 106(11):1958–1960.
Munro, S., A. Haile-Mariam, C. Greenwell, S. Demirci, O. Farooqi, and S. Vasudeva. 2018. Implementation and dissemination of a Department of Veterans Affairs oral care initiative to prevent hospital-acquired pneumonia among nonventilated patients. Nursing Administration Quarterly 42(4):363–372.
NACHC (National Association of Community Health Centers). 2022. Community health center chartbook. Bethesda, MD: National Association of Community Health Centers.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019a. Integrating social care into the delivery of health care: Moving upstream to improve the nation’s health. Washington, DC: The National Academies Press.
NASEM. 2019b. Taking action against clinician burnout: A systems approach to professional well-being. Washington, DC: The National Academies Press.
NASEM. 2021. Implementing high-quality primary care: Rebuilding the foundation of health care. Washington, DC: The National Academies Press.
NCCIH (National Center for Complementary and Integrative Health). 2021. Complementary, alternative, or integrative health: What’s in a name? https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name (accessed November 8, 2022).
Nelson, K. M., C. Helfrich, H. Sun, P. L. Hebert, C.-F. Liu, E. Dolan, L. Taylor, E. Wong, C. Maynard, S. E. Hernandez, W. Sanders, I. Randall, I. Curtis, G. Schectman, R. Stark, and S. D. Fihn. 2014. Implementation of the patient-centered medical home in the Veterans Health Administration. JAMA Internal Medicine 174(8):1350.
Newins, A. R., S. M. Wilson, T. A. Hopkins, K. Straits-Troster, H. Kudler, and P. S. Calhoun. 2019. Barriers to the use of Veterans Affairs health care services among female veterans who served in Iraq and Afghanistan. Psychological Services 16(3):484–490.
Nolan, K., M. W. Schall, F. Erb, and T. Nolan. 2005. Using a framework for spread: The case of patient access in the Veterans Health Administration. Joint Commission Journal on Quality and Patient Safety 31(6):339–347.
North Carolina Governor’s Working Group. 2022. NC GWG 101: How the working group got its start. https://ncgwg.org/ (accessed August 2, 2022).
Novick, R. G. 1949. The mental hygiene movement. Chicago: Delphian Society.
NRD (National Resource Directory). 2022. Homepage. https://nrd.gov/ (accessed September 5, 2022).
NZIER (New Zealand Institute of Economic Research). 2018. Population ageing: Do we understand and accept the challenge? Wellington, NZ: Chartered Accountants Australia and New Zealand.
O’Brien, M. J., C. H. Halbert, R. Bixby, S. Pimentel, and J. A. Shea. 2010. Community health worker intervention to decrease cervical cancer disparities in Hispanic women. Journal of General Internal Medicine 25(11):1186–1192.
O’Hanlon, C., C. Huang, E. Sloss, R. Anhang Price, P. Hussey, C. Farmer, and C. Gidengil. 2017. Comparing VA and non-VA quality of care: A systematic review. Journal of General Internal Medicine 32(1):105–121.
OIG (Office of the Inspector General). 2021. VHA risks overpaying community care providers for evaluation and management services. Washington, DC: Department of Veterans Affairs.
Oishi, S. M., R. Shoai, W. Katon, C. Callahan, J. Unützer, P. Arean, C. Callahan, R. Della Penna, L. Harpole, M. Hegel, P. H. Noel, M. Hoffing, E. M. Hunkeler, W. Katon, S. Levine, E. H. Lin, E. Oddone, S. Oishi, J. Unützer, and J. Williams. 2003. Impacting late life depression: Integrating a depression intervention into primary care. Psychiatric Quarterly 74(1):75–89.
Ougrin, D., T. Tranah, D. Stahl, P. Moran, and J. R. Asarnow. 2015. Therapeutic interventions for suicide attempts and self-harm in adolescents: Systematic review and meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry 54(2):97–107. e102.
Overbeck, G., A. S. Davidsen, and M. B. Kousgaard. 2016. Enablers and barriers to implementing collaborative care for anxiety and depression: A systematic qualitative review. Implementation Science 11(1):165.
Øvretveit, J., L. Garofalo, and B. Mittman. 2017. Scaling up improvements more quickly and effectively. International Journal for Quality in Health Care 29(8):1014–1019.
Pallas, S. W., D. Minhas, R. Pérez-Escamilla, L. Taylor, L. Curry, and E. H. Bradley. 2013. Community health workers in low- and middle-income countries: What do we know about scaling up and sustainability? American Journal of Public Health 103(7):e74–e82.
Pany, M. J., L. Chen, B. Sheridan, and R. S. Huckman. 2021. Provider teams outperform solo providers in managing chronic diseases and could improve the value of care. Health Affairs (Millwood) 40(3):435–444.
Parry, M. 2010. From a patient’s perspective: Clifford Whittingham Beers’ work to reform mental health services. American Journal of Public Health 100(12):2356–2357.
Payne, J., S. Razi, K. Emery, W. Quattrone, and M. Tardif-Douglin. 2017. Integrating community health workers (CHWs) into health care organizations. Journal of Community Health 42(5):983–990.
Possis, E., B. Skroch, S. Hintz, C. Bronars, M. Mallen, H. Crowl, K. Moore, H. Bemmels, and D. Olson. 2020. Examining and improving provider adherence to the primary care mental health integration model. Military Medicine 185(9–10):e1411–e1416.
Proctor, E., H. Silmere, R. Raghavan, P. Hovmand, G. Aarons, A. Bunger, R. Griffey, and M. Hensley. 2011. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Administration and Policy in Mental Health and Mental Health Services Research 38(2):65–76.
Pronovost, P. J., C. A. Goeschel, J. A. Marsteller, J. B. Sexton, J. C. Pham, and S. M. Berenholtz. 2009. Framework for patient safety research and improvement. Circulation 119(2):330–337.
Rakel, D. P., and A. Weil. 2003. Philosophy of integrative medicine. In D. P. Rakel (ed.), Integrative medicine. Philadelphia: W.B. Saunders. Pp. 2–11.
Randall, I., D. C. Mohr, and C. Maynard. 2017. VHA patient-centered medical home associated with lower rate of hospitalizations and specialty care among veterans with posttraumatic stress disorder. Journal for Healthcare Quality 39(3):168–176.
Reddy, K. P., T. M. Schult, A. M. Whitehead, and B. G. Bokhour. 2021. Veterans Health Administration’s Whole Health System of Care: Supporting the health, well-being, and resiliency of employees. Global Advances in Health and Medicine 10:216495612110226.
Reed, S. J., K. K. Shore, and J. A. Tice. 2016. Effectiveness and value of integrating behavioral health into primary care. JAMA Internal Medicine 176(5):691–692.
Reich, K., S. W. Butterworth, M. Coday, and J. E. Bailey. 2022. Integrating lay health coaches into primary care: Acceptability, credibility, and effectiveness from the provider perspective. Cureus 14(5):e25457.
Reiss-Brennan, B. 2014. Mental health integration: Normalizing team care. Journal of Primary Care & Community Health 5(1):55–60.
Reiss-Brennan, B., K. D. Brunisholz, C. Dredge, P. Briot, K. Grazier, A. Wilcox, L. Savitz, and B. James. 2016. Association of integrated team-based care with health care quality, utilization, and cost. JAMA 316(8):826–834.
Rodriguez, H. P., K. F. Giannitrapani, S. Stockdale, A. B. Hamilton, E. M. Yano, and L. V. Rubenstein. 2014. Teamlet structure and early experiences of medical home implementation for veterans. Journal of General Internal Medicine 29(Suppl 2):S623–S631.
Rogers, E. A., S. T. Manser, J. Cleary, A. M. Joseph, E. M. Harwood, and K. T. Call. 2018. Integrating community health workers into medical homes. Annals of Family Medicine 16(1):14–20.
Rogers, E. M. 2014. Diffusion of innovations, 5th edition. New York: Free Press.
Rollins, A. L., J. Wright-Berryman, N. H. Henry, A. M. Quash, K. Benbow, K. A. Bonfils, H. Hedrick, A. P. Miller, R. Firmin, and M. P. Salyers. 2017. Managing physical and mental health conditions: Consumer perspectives on integrated care. Social Work in Mental Health 15(1):66–79.
SAMHSA (Substance Abuse and Mental Health Services Administration). 2022. 988 key messages. https://www.samhsa.gov/find-help/988/key-messages (accessed August 25, 2022).
Sanchez, K., and G. Adorno. 2013. “It’s like being a well-loved child”: Reflections from a collaborative care team. Primary Care Companion for CNS Disorders 15(6):PCC.13m01541.
Savitt, T. 2006. Abraham Flexner and the Black medical schools. 1992. Journal of the National Medical Association 98(9):1415–1424.
Schein, E. 2013. Humble inquiry: The gentle art of asking instead of telling. Oakland, CA: Berrett-Koehler.
Schlosser, J., D. Kollisch, D. Johnson, T. Perkins, and A. Olson. 2020. VA–community dual care: Veteran and clinician perspectives. Journal of Community Health 45(4):795–802.
Schottenfeld, L., D. Petersen, D. Peikes, R. Ricciardi, H. Burak, R. McNellis, and J. Genevro. 2016. Creating patient-centered team-based primary care. Rockville, MD: Agency for Healthcare Research and Quality.
Schwartz, M. R., A. M. Cole, G. A. Keppel, R. Gilles, J. Holmes, and C. Price. 2021. Complementary and integrative health knowledge and practice in primary care settings: A survey of primary care providers in the northwestern United States. Global Advances in Health and Medicine 10:216495612110233.
Scuffham, P. A., J. M. Byrnes, C. Pollicino, D. Cross, S. Goldstein, and S.-K. Ng. 2019. The impact of population-based disease management services on health care utilisation and costs: Results of the Capiche trial. Journal of General Internal Medicine 34(1):41–48.
Segal, D. R., and M. W. Segal. 2004. America’s military population. Population Bulletin 59:3–40.
Shekelle, P. G., N. M. Paige, E. A. Apaydin, J. D. Goldhaber-Fiebert, S. S. Mak, I. M. Miake-Lye, M. M. Begashaw, and J. M. Beroes-Severin. 2019. What is the optimal panel size in primary care? A systematic review. Washington, DC: Department of Veterans Affairs.
Shepardson, R. L., E. M. Johnson, K. Possemato, D. Arigo, and J. S. Funderburk. 2019. Perceived barriers and facilitators to implementation of peer support in Veterans Health Administration primary care-mental health integration settings. Psychological Services 16(3):433–444.
Singer, J., and J. Adams. 2014. Integrating complementary and alternative medicine into mainstream healthcare services: The perspectives of health service managers. BMC Complementary and Alternative Medicine 14(1):167.
Singer, S. J., J. Burgers, M. Friedberg, M. B. Rosenthal, L. Leape, and E. Schneider. 2011. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review 68(1):112–127.
Singer, S. J., S. C. Moore, M. Meterko, and S. Williams. 2012. Development of a short-form learning organization survey: The LOS-27. Medical Care Research and Review 69(4):432–459.
Singer, S. J., M. Kerrissey, M. Friedberg, and R. Phillips. 2020a. A comprehensive theory of integration. Medical Care Research and Review 77(2):196–207.
Singer, S. J., A. D. Sinaiko, M. V. Tietschert, M. Kerrissey, R. S. Phillips, V. Martin, G. Joseph, H. Bahadurzada, and D. Agniel. 2020b. Care integration within and outside health system boundaries. Health Services Research 55(S3):1033–1048.
Singhal, S., B. Kayyali, R. Levin, and Z. Greenberg. 2020. The next wave of healthcare innovation: The evolution of ecosystems. McKinsey Insights, June 23. https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/the-next-wave-of-healthcare-innovation-the-evolution-of-ecosystems (accessed May 30, 2022).
Sinsky, C. A., R. Willard-Grace, A. M. Schutzbank, T. A. Sinsky, D. Margolius, and T. Bodenheimer. 2013. In search of joy in practice: A report of 23 high-functioning primary care practices. Annals of Family Medicine 11(3):272–278.
Smith, D. B. 2003. Healthcare’s hidden civil rights legacy. Saint Louis University Law Journal 48(1):37–60.
Song, H., M. Ryan, S. Tendulkar, J. Fisher, J. Martin, A. S. Peters, J. P. Frolkis, M. B. Rosenthal, A. T. Chien, and S. J. Singer. 2017. Team dynamics, clinical work satisfaction, and patient care coordination between primary care providers: A mixed methods study. Health Care Management Review 42(1):28–41.
Sterling, S., F. Chi, and A. Hinman. 2011. Integrating care for people with co-occurring alcohol and other drug, medical, and mental health conditions. Alcohol Research & Health 33(4):338–349.
Stewart, M. 2022. Evidence on patient-centeredness, patient-centered systems, and implementation and scaling of whole person health. Paper commissioned by the Committee on Transforming Health Care to Create Whole Health—Strategies to Assess, Scale, and Spread the whole-person approach to health.
Stewart, W. H. 1966. Civil rights and Medicare. JAMA 196(11):993.
Stewart, W. H. 1967. The positive impact of Medicare on the nation’s health care systems. Social Security Bulletin 30:9–50.
Straits-Tröster, K. A., M. Brancu, B. Goodale, S. Pacelli, C. Wilmer, E. M. Simmons, and H. Kudler. 2011. Developing community capacity to treat post-deployment mental health problems: A public health initiative. Psychological Trauma: Theory, Research, Practice, and Policy 3(3):283.
Sudbury-Riley, L., and P. Hunter-Jones. 2021. Facilitating inter-professional integration in palliative care: A service ecosystem perspective. Social Science & Medicine 277:113912.
Sullivan, E. E., and A. Ellner. 2015. Strong patient–provider relationships drive healthier outcomes. Cambridge, MA: Harvard Business Review.
Tabvuma, T. S., R. Stanton, G. Browne, and B. Happell. 2022. Mental health consumers’ perspectives of physical health interventions: An integrative review. International Journal of Mental Health Nursing 31(5):1046–1089.
Tanielian, T., C. Farris, C. Batka, C. M. Farmer, E. Robinson, C. C. Engel, M. W. Robbins, and L. H. Jaycox. 2014. Ready to serve: Community-based provider capacity to deliver culturally competent, quality mental health care to veterans and their families. Santa Monica, CA: RAND Corporation.
Taylor, S. L., P. M. Herman, N. J. Marshall, Q. Zeng, A. Yuan, K. Chu, Y. Shao, C. Morioka, and K. A. Lorenz. 2018. Use of complementary and integrated health: A retrospective analysis of U.S. veterans with chronic musculoskeletal pain nationally. Journal of Alternative and Complementary Medicine 25(1):32–39.
Taylor, S. L., R. Bolton, A. Huynh, K. Dvorin, A. R. Elwy, B. G. Bokhour, A. Whitehead, and B. Kligler. 2019. What should health care systems consider when implementing complementary and integrative health: Lessons from Veterans Health Administration. Journal of Alternative and Complementary Medicine 25(S1):S52–S60.
Thom, D. H. 2019. Keeping pace with the expanding role of health coaching. Journal of General Internal Medicine 34(1):5–6.
Toffler, A. 1999. Powershift: Knowledge, wealth, and violence at the edge of the 21st century. New York: Bantam.
VA (U.S. Department of Veterans Affairs). 2018. Health Services Research & Development https://www.hsrd.research.va.gov/publications/vets_perspectives/1803_peer_support_specialists_contribution_to_veterans_health.cfm (accessed November 8, 2022).
VA. 2019. VA launches new health care options under MISSION Act. Office of Public and Intergovernmental Affairs. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=5264 (accessed November 8, 2022).
VA. 2020a. PACT social work staffing program evaluated by SERVE QUERI. https://www.hsrd.research.va.gov/publications/vets_perspectives/0420-PACT-Social-Work-Staffing-Program-evaluated-by-SERVE-QUERI.cfm#2 (accessed August 30, 2022).
VA. 2020b. Patient care services. https://www.patientcare.va.gov/primarycare/PACT.asp (accessed March 29, 2022).
VA. 2020c. VA health care utilization by recent veterans. https://www.publichealth.va.gov/epidemiology/reports/oefoifond/health-care-utilization/ (accessed August 28, 2022).
VA. 2020d. VA Solid Start. https://benefits.va.gov/transition/solid-start.asp (accessed November 8, 2022).
VA. 2020e. VITAL program. https://www.mentalhealth.va.gov/student-veteran/vital-program.asp (accessed July 12, 2022).
VA. 2021a. The Circle of Health. https://www.va.gov/WHOLE-HEALTH/circle-of-health/index.asp (accessed August 27, 2022).
VA. 2021b. Development and validation of the well-being signs (WBS): A clinical measurement tool. https://www.va.gov/WHOLEHEALTH/docs/DevelopmentValidation_WBS_FINAL_508_Aug22.pdf (accessed December 5, 2022).
VA. 2022a. Community Care Network—Information for providers. https://www.va.gov/COMMUNITYCARE/providers/Community_Care_Network.asp#FAQ (accessed November 8, 2022).
VA. 2022b. Integrative Health Coordinating Center (IHCC). https://www.va.gov/WHOLEHEALTH/professional-resources/IHCC.asp (accessed August 2, 2022).
VA. 2022c. My Personal Health Plan wallet card. https://www.va.gov/WHOLEHEALTH/docs/PHP-WalletCard-May22-fillable-508.pdf (accessed November 8, 2022).
VA. 2022d. National Center for Healthcare Advancement and Partnerships. https://www.va.gov/healthpartnerships/vcp.asp (accessed September 5, 2022).
VA. 2022e. Personal Health Inventory. https://www.va.gov/WHOLEHEALTH/docs/PHI-long-May22-fillable-508.pdf (accessed November 8, 2022).
VA. 2022f. U.S. Department of Housing and Urban Development–VA Supportive Housing (HUD-VASH) program. https://www.va.gov/homeless/hud-vash.asp (accessed September 5, 2022).
VA. 2022g. Veterans Experience Office (VEO). https://www.va.gov/ve/ (accessed August 2, 2022).
VA. 2022h. Veterans Health Administration: About VHA. https://www.va.gov/health/aboutvha.asp (accessed March 18, 2022).
VA. 2022i. VetSuccess on campus. https://www.benefits.va.gov/vocrehab/vsoc.asp (accessed July 12, 2022).
VA. 2022j. Your VA Transition Assistance Program (TAP). https://www.benefits.va.gov/transition/tap.asp (accessed November 8, 2022).
VA. 2022k. VA homeless programs. https://www.va.gov/homeless/ (accessed June 16, 2022).
Valentijn, P. P., I. C. Boesveld, D. M. Van Der Klauw, D. Ruwaard, J. N. Struijs, J. J. W. Molema, M. A. Bruijnzeels, and H. J. Vrijhoef. 2015. Towards a taxonomy for integrated care: A mixed-methods study. International Journal of Integrated Care 15(1):e003.
Vanneman, M. E., J. Yoon, S. J. Singer, T. H. Wagner, M. K. Goldstein, J. Hu, D. Boothroyd, L. Greene, and D. M. Zulman. 2022. Anticipating VA/non-VA care coordination demand for veterans at high risk for hospitalization. Medicine (Baltimore) 101(7):e28864.
Vashi, A. A., T. Urech, S. Wu, D. Boothroyd, P. Mehta, A. L. Dalton, E. Brill, C. Kessler, and S. M. Asch. 2021. Community urgent care use following implementation of the Veterans Affairs Maintaining Internal Systems and Strengthening Integrated Outside Networks Act. Medical Care 59:S314–S321.
Vega, R., G. Jackson, B. Henderson, C. Clancy, J. McPhail, S. L. Cutrona, L. J. Damschroder, and S. Bhatnagar. 2019. Diffusion of excellence: Accelerating the spread of clinical innovation and best practices across the nation’s largest health system. Permanente Journal 18:309.
VHA (Veterans Health Administration). 2021. Enhancing well-being measurement in health research, clinical care, and population health promotion. https://www.nccih.nih.gov/news/events/enhancing-well-being-measurement-in-health-research-clinical-care-and-population-health-promotion (accessed November 8, 2022).
Vogt, D., E. C. Taverna, Y. I. Nillni, B. Booth, D. F. Perkins, L. A. Copeland, E. P. Finley, F. A. Tyrell, and C. L. Gilman. 2019. Development and validation of a tool to assess military veterans’ status, functioning, and satisfaction with key aspects of their lives. Applied Psychology: Health and Well-Being 11(2):328–349.
WestRasmus, E. K., F. Pineda-Reyes, M. Tamez, and J. M. Westfall. 2012. Promotores de salud and community health workers: An annotated bibliography. Family & Community Health 35(2):172–182.
Whitebird, R. R., L. I. Solberg, N. A. Jaeckels, P. B. Pietruszewski, S. Hadzic, J. Unützer, K. A. Ohnsorg, R. C. Rossom, A. Beck, K. E. Joslyn, and L. V. Rubenstein. 2014. Effective implementation of collaborative care for depression: What is needed? American Journal of Managed Care 20(9):699–707.
WHO (World Health Organization). 2009. Practical guidance for scaling up health service innovations. Geneva: World Health Organization.
Willard-Grace, R., D. Hessler, E. Rogers, K. Dubé, T. Bodenheimer, and K. Grumbach. 2014. Team structure and culture are associated with lower burnout in primary care. Journal of the American Board of Family Medicine 27(2):229–238.
Willard-Grace, R., E. H. Chen, D. Hessler, D. DeVore, C. Prado, T. Bodenheimer, and D. H. Thom. 2015. Health coaching by medical assistants to improve control of diabetes, hypertension, and hyperlipidemia in low-income patients: A randomized controlled trial. Annals of Family Medicine 13(2):130–138.
Wolever, R. Q., K. L. Caldwell, L. C. McKernan, and M. G. Hillinger. 2017. Integrative medicine strategies for changing health behaviors: Support for primary care. Primary Care 44(2):229–245.
Wozniak, L., A. Soprovich, S. Rees, F. Al Sayah, S. R. Majumdar, and J. A. Johnson. 2015. Contextualizing the effectiveness of a collaborative care model for primary care patients with diabetes and depression (teamcare): A qualitative assessment using RE-AIM. Canadian Journal of Diabetes 39(Suppl 3):S83–S91.
Wright, B., A. J. Potter, and A. N. Trivedi. 2017. Use of federally qualified health centers and potentially preventable hospital utilization among older Medicare–Medicaid enrollees. Journal of Ambulatory Care Management 40(2):139–149.
Wright, D. B. 2012. Consumer governance and the provision of enabling services that facilitate access to care at community health centers. Medical Care 50(8):668–675.
Wyman, J. F., and S. J. Henly. 2011. Advancing nursing science through health trajectory research: An introduction. Nursing Research 60(3 Suppl):S1–S4.
Yakovchenko, V., D. K. McInnes, B. A. Petrakis, C. Gillespie, J. M. Lipschitz, M. B. McCullough, L. Richardson, B. Vetter, and T. P. Hogan. 2021. Implementing automated text messaging for patient self-management in the Veterans Health Administration: Qualitative study applying the nonadoption, abandonment, scale-up, spread, and sustainability framework. JMIR mHealth and uHealth 9(11):e31037.
Yano, E. M., M. J. Bair, O. Carrasquillo, S. L. Krein, and L. V. Rubenstein. 2014. Patient aligned care teams (PACTs): VA’s journey to implement patient-centered medical homes. Journal of General Internal Medicine 29(S2):547–549.
Zeliadt, S. B., S. Coggeshall, H. Gelman, M. H. Shin, A. R. Elwy, B. G. Bokhour, and S. L. Taylor. 2020. Assessing the relative effectiveness of combining self-care with practitioner-delivered complementary and integrative health therapies to improve pain in a pragmatic trial. Pain Medicine 21(Suppl 2):S100–S109.
Zhang, A., S. Park, J. E. Sullivan, and S. Jing. 2018. The effectiveness of problem-solving therapy for primary care patients’ depressive and/or anxiety disorders: A systematic review and meta-analysis. Journal of the American Board of Family Medicine 31(1):139–150.
Zulman, D. M., L. Greene, C. Slightam, S. J. Singer, M. L. Maciejewski, M. K. Goldstein, M. E. Vanneman, J. Yoon, R. B. Trivedi, T. Wagner, S. M. Asch, and D. Boothroyd. 2022. Outpatient care fragmentation in Veterans Affairs patients at high risk for hospitalization. Health Services Research 57(4):764–774.
This page intentionally left blank.














































































