
| Proceedings of a Workshop—in Brief |
Advancing Diagnostic Excellence for Maternal Health Care
Proceedings of a Workshop—in Brief
To examine opportunities for improving diagnosis in maternal health care in the United States, the Board on Health Care Services of the National Academies of Sciences, Engineering, and Medicine hosted a hybrid workshop on July 27, 2023.1 The workshop highlighted unique challenges in achieving diagnostic excellence in maternal health care, diagnostic disparities, and interventions to mitigate these disparities, and strategies to advance diagnostic excellence. This workshop was the sixth in a series on diagnostic excellence funded by the Gordon and Betty Moore Foundation, with additional funding provided for this workshop by The Commonwealth Fund.2 This Proceedings of a Workshop—in Brief highlights the presentations and discussions that occurred at the workshop.3
BACKGROUND
Daniel Yang of the Gordon and Betty Moore Foundation described diagnostic errors as diagnoses that are delayed, inaccurate, or poorly communicated to patients, as defined by the Institute of Medicine report
___________
1 The workshop agenda and presentations are available at https://www.nationalacademies.org/event/07-27-2023/workshop-on-advancing-diagnostic-excellence-for-maternal-health-care (accessed September 8, 2023).
2 Past workshops in this series have explored improving diagnosis for sepsis, acute cardiovascular events, cancer, and older adults, as well as diagnostic lessons learned from the COVID-19 pandemic. More information about the workshop series is available at https://www.nationalacademies.org/our-work/advancing-diagnostic-excellence-a-workshop-series (accessed August 29, 2022).
3 This Proceedings of a Workshop—in Brief is not intended to provide a comprehensive summary of information shared during the workshop. The information summarized here reflects the knowledge and opinions of individual workshop participants and should not be seen as a consensus of the workshop participants, the planning committee, or the National Academies of Sciences, Engineering, and Medicine.
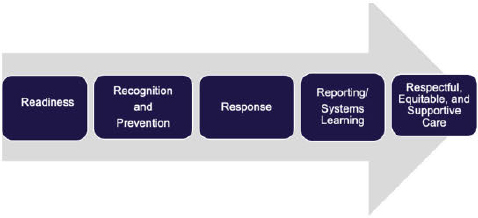
SOURCE: Andrew Bindman presentation, July 27, 2023.
THE ECOSYSTEM OF MATERNAL HEALTH CARE IN THE UNITED STATES
Charity Watkins, assistant professor at North Carolina Central University, shared her personal story of being diagnosed with pregnancy-related cardiovascular disease (CVD) when her daughter was just two months old. Following an uneventful pregnancy, she had an unplanned cesarean delivery and experienced significant postpartum hemorrhage. Two months later she went to the emergency department (ED) with shortness of breath, a nagging cough, and extreme fatigue that progressed to nausea, vomiting, and radiating pain in her left arm. After waiting several hours, she left the ED without being seen and days later saw a doctor who listened to her symptoms, ordered a chest x-ray which indicated an enlarged heart and edema, and discharged her to the ED, where she was eventually admitted to the cardiac intensive care unit. Her heart was functioning at less than 10 percent, and with medication she lost 20 pounds of fluid within two days of being admitted to the hospital. Watkins was told that the medications for her heart failure would not allow her to breastfeed her baby and that it was very likely she could not have any more children. Considering all the steps of the diagnostic process, she wondered what should have been done differently so that she could have received an accurate and timely diagnosis. Watkins emphasized that “Error should never be normalized. We have the resources to do better. If the financial costs are not enough, the human costs should be. We all deserve diagnostic excellence,” she concluded.
Zsakeba Henderson, senior health advisor at the National Institute for Children’s Health Quality, described the ecosystem of maternity care in the United States. She emphasized the importance of recognizing that numbers and statistics represent human beings—someone’s mother, sister, or child. The current maternal health landscape is complex and encompasses prenatal care, childbirth, and postnatal care but is also interwoven with primary, emergency, and specialty care, which demands coordination and collaboration among the many entities involved, both in the community and in the health care system, to deliver comprehensive and integrated maternity care and improve outcomes. Pregnant individuals are at the center of the maternal health care continuum and should play a crucial role in decisions made about their health, said Henderson. She also noted their active participation and engagement in decision making is essential for achieving optimal outcomes. Henderson pointed out that the U.S. maternal mortality rate is more than double that of other countries such as Canada, France, and Sweden, adding that the United States is one of the only industrialized nations where maternal mortality rates have increased in recent decades (Figure 2).
Henderson said data from maternal mortality review committees revealed that more than 84 percent of pregnancy-related deaths were preventable, with most occurring seven days to one year after pregnancy (Trost et al., 2022). The leading causes of pregnancy-related deaths are mental health conditions, excessive bleeding or hemorrhage, and cardiac or coronary conditions. Highlighting glaring disparities, Henderson noted that the mortality rate among Black pregnant women in 2021 was more than double that of the overall maternal mortality rate of 32.9 per 100,000 live births (Hoyert, 2023). Significant regional and racial disparities exist, especially for Black, American Indian, and Alaska
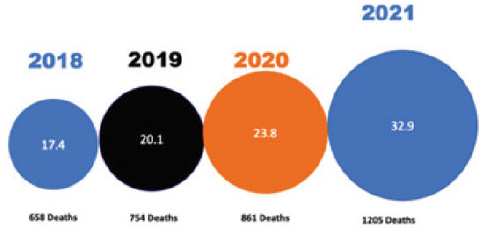
SOURCE: Zsakeba Henderson presentation, July 27, 2023 (Hoyert, 2020).
Native mothers (Fleszar et al., 2023). In addition to unacceptably high maternal mortality rates, each year approximately 60,000 women are affected by severe maternal morbidity, unexpected serious short- or long-term pregnancy-related health impacts. Henderson identified the key factors associated with poor maternal health outcomes: inadequate access to healthcare, structural racism and bias, social determinants of health (SDOH), various underlying health conditions, lack of timely and quality care, and systemic challenges in healthcare including adequate workforce and staffing. She offered approaches to address known vulnerabilities for diagnostic errors, including implementing hospital-wide safety bundles;4 addressing implicit bias, structural racism, and SDOH; using healthcare simulation; and improving communication and teamwork. By “understanding the multiple stages involved in a diagnostic journey, we can identify where diagnostic errors and failures commonly occur and then prioritize where we should focus our efforts for improvement,” concluded Henderson.
KEY CHALLENGES AND CONSIDERATIONS FOR DIAGNOSTIC EXCELLENCE
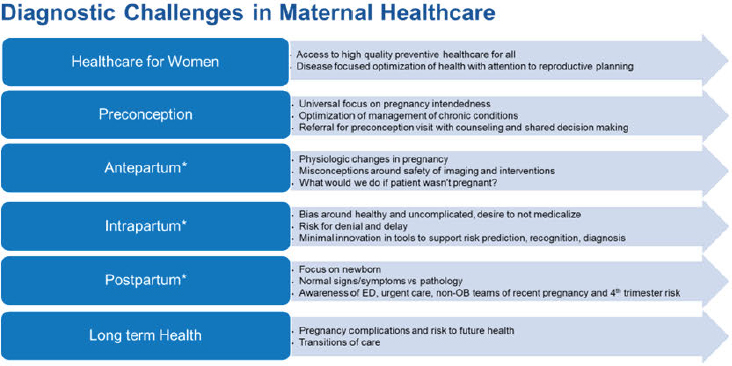
Dena Goffman, vice chair for quality and patient safety at Columbia University Irving Medical Center, discussed diagnostic challenges in maternal health care. Reiterating that the vast majority of pregnancy-related conditions are preventable, she discussed several Alliance for Innovation on Maternal Health (AIM) safety bundles to address conditions such as hypertension, hemorrhage, and mental health conditions.5 While highlighting improved resources to support implementation, checklists, and clinical algorithms, she said a focus on diagnostic excellence is still missing from such quality and patient safety innovations. Goffman said one of the key diagnostic challenges is bias; she highlighted the Centers for Disease Control and Prevention (CDC) campaign named HEAR HER6 and emphasized the need to share it more widely to improve communication between patients and clinicians and reduce bias. “We need to provide safe, high-quality preventive health care to all women,” she said, “well before a complication presents during birth or postpartum.” Goffman highlighted several diagnostic challenges across the care continuum (see Figure 3) and identified opportunities to improve maternal healthcare, such as reproductive planning with preconception evaluation for intended pregnancies; optimizing postpartum care; risk prediction models leveraging artificial intelligence; innovation in developing and evaluating therapies targeting causes of serious maternal morbidity and mortality; and further evaluating metrics that clearly delineate standards for treatment and intervention. She also suggested working with clinicians early in their training and career to focus on patient preferences and values, and prioritizing patient-centered huddles that include the patient and their support system to continually get feedback and input.
Shad Deering, associate dean of Baylor College of Medicine, described simulation in obstetrics as an opportunity to practice foundational skills, for refresher and sustainment training, or in situ training.7 Sixty percent of errors are communication and teamwork related, he said, and those skills cannot be learned or practiced in a lecture setting and require interactive practice using simulation. Deering emphasized the importance of simulation in obstetrics because it reduces harms associated with mistakes and can significantly improve outcomes. He explained that the most common causes of error in obstetrics are inadequate diagnosis, inappropriate treatment, and inadequate documentation—all of which can be addressed at no risk to actual patients through simulation. Without simulation, clinicians are essentially “practicing” on real patients during an emergency, discussing what went wrong and how best to address it, then waiting until it happens again to test the solution. Simulation can ensure that clinicians are prepared for emergencies and can test new solutions and different approaches before using them in patient care. He said simulation training can be done inexpensively and many resources are available online. To ensure participation, Deering
___________
4 Safety bundles are collections of evidence-informed best practices developed by multidisciplinary experts.
5 For more information on AIM, see https://saferbirth.org/aim-resources/aim-cornerstones/simulations/ (accessed September 24, 2023).
6 The CDC’s HEAR HER Campaign seeks to “raise awareness of urgent maternal warning signs during and after pregnancy and improve communication between patients and their healthcare providers.” See https://www.cdc.gov/hearher/about-the-campaign/index.html (accessed September 24, 2023).
7 In situ training refers to training in the labor and delivery unit.
SOURCE: Dena Goffman presentation, July 27, 2023.
suggested making it mandatory for clinicians to maintain their hospital privileges, while noting the importance of keeping simulation sessions short and manageable for busy clinicians. While simulation is not the only way to decrease diagnostic errors in obstetrics, it needs to be part of the solution, Deering concluded.
Emily Miller, associate professor at Brown University, discussed key diagnostic challenges related to maternal mental health. She noted that mental health conditions are the leading cause of maternal mortality in the United States, accounting for 23 percent of maternal mortality from 2017 to 2019. She emphasized that mortality is just the tip of the iceberg; untreated mental health conditions affect the quality and function of a birthing person’s life, as well as infant neurodevelopment. With depression, for example, many steps are necessary to achieve symptom remission, including screening, initiation of treatment, and provision of adequate treatment. However, data indicate that only 3 to 5 percent of people with perinatal depression will achieve remission of depressive symptoms. Screening presents the biggest challenge, noted Miller. Barriers to adequate screening include cultural and linguistic differences, as well as variability in expression of symptoms and manifestation of mental health conditions, Miller explained, adding that clinicians also have not earned the trust of some birthing people due to a history of structural racism and bias. She highlighted screening as an opportunity to incorporate the patient voice and stressed the importance of creating a space where people feel comfortable having a conversation and sharing information. Miller said research showed that 23 percent of people who screened positive on the Edinburgh Postnatal Depression Scale, indicating depression as the primary diagnosis, actually had bipolar disorder (Cox et al., 1987). Diagnostic overshadowing is another challenge, in which physical complications are misattributed to mental health conditions. For example, individuals with conditions like obstetric embolisms were more than twice as likely to be misdiagnosed if they also had a serious mental illness (Easter et al., 2021).
Jennifer Moore, founding executive director at the Institute for Medicaid Innovation, described evidence- based models of maternal health care in Medicaid. More than 86 million individuals are covered by the federal—state Medicaid program, a number which increased significantly during the COVID pandemic. Nearly half of all births in the United States are covered by Medicaid, ranging between 20 and 71 percent of births in different states, so it is important to ensure that those enrolled in Medicaid are receiving high-quality care. However, Moore said that Medicaid enrollees do not have the same level of access to services as those with commercial insurance, which is a barrier to receiving adequate mental health care. Moore added that the majority of women enrolled in Medicaid do not
have access to evidence-based doula care, midwife-led care, and perinatal mental health care, all of which are associated with improved outcomes. She said barriers to be addressed include variability in state policy for doula care, confusing credentialing practices for midwives, and limits on billing Medicaid for postpartum mental health services. The research supporting these services exists, she noted, but policy changes are needed to ensure access, coverage, and reimbursement for these services. People who are enrolled in Medicaid deserve the same level of care as those covered by commercial insurance, Moore concluded.
For postpartum care during the important “fourth trimester,” Moore said that payment and quality measures are key drivers of change, especially for Medicaid, but there are only a few alternative payment models that include services such as midwifery care, and scaling those across 50 states has been a challenge.
STRATEGIES TO IMPROVE DIAGNOSIS
Jennie Joseph, founder and executive director of Commonsense Childbirth, Inc., discussed strengthening community, patient, and health care provider collaboration. She said one difficulty in moving her practice from the United Kingdom to the United States was that access to care is not universal in this country. Her work in Florida has focused on demonstrating that a non-physiological approach to care can change health outcomes. For example, her organization has greatly reduced premature births and low birthweight in babies within the population they serve, which is mainly individuals with low income who are undocumented and uninsured. Her organization uses the midwifery model and employs the four tenets of access, connections, knowledge, and empowerment. Joseph said that midwifery has all the desired components of a care model, with the mother and baby inherently at the center of a collaborative health care system, but scaling the model has been difficult because of structural barriers. She suggested expanding the medical team to include anyone who interacts with the pregnant person, including those working the front desk of the health care setting. Joseph explained that her birthing center has great interdisciplinary relationships and partnerships with other health care providers and hospitals to optimize outcomes in cases where clients need to be transferred to the hospital. There are also poor experiences, however, due to what Joseph referred to as the “matemo-toxic zone”—defined by the National Perinatal Task Force (NPTF) created by her organization as “any area where it is unsafe to be pregnant, breastfeeding, or parenting.” 8 The NPTF is a national community of practice with nearly 200 perinatal “safe spots” around the country where individuals are working within these zones. Her organization also trains perinatal professionals who can serve as diagnosticians but are often ignored in the mainstream model. Joseph emphasized the importance of providing respectful maternity care to all people and acknowledging the injustices that contribute to health disparities.
Sheela Maru, assistant professor at the Icahn School of Medicine at Mount Sinai, described doula care in immigrant communities and noted that her neighborhood in Queens is one of the most diverse zip codes in the country, with a majority foreign-born population. Within the New York City public hospital system, most patients are covered by Medicaid or are uninsured, and many are immigrants. Maru described the poor maternal health outcomes among immigrant women, including higher rates of severe maternal morbidity and pregnancy complications such as gestational diabetes and preeclampsia. She said these are likely a product of inequities in access to care across the maternity care spectrum, including limited preconception care, late and inadequate prenatal care, and loss of postpartum insurance coverage. Maru suggested doula care as a way to address these problems because doula care is associated with better birth outcomes, such as shorter labor, fewer cesareans and preterm births, and improvements in breastfeeding, birth experience, and mental health. Maru explained that doulas are trained to provide nonclinical emotional, physical, and informational support for people before, during, and after labor and birth. Doulas help facilitate communication between the birthing person and clinician by helping
___________
8 An area might be unsafe because of a physical threat to health, freedom, or thriving, or because of the psychological and social pressures a person feels when in that environment.
people articulate their questions, preferences, and values. Doulas are often part of the communities they serve, providing emotional and social support and connecting birthing people with local resources. Maru described the Helping Promote Birth Equity through Community-Based Doula Care program, also known as the HoPE program. Together, she said, they have trained and supported 30 new doulas who speak 8 languages, providing each client with 4 two-hour prenatal home visits, continuous support during labor and birth, and 8 two- hour postpartum visits. Maru shared quotes from the program’s participants highlighting how doulas affect the immigrant health experience, concluding, “From these voices, we can understand how the community-based doula is impactful across multiple levels—individual, interpersonal, community, and societal—bringing hope in the face of the maternal health crisis.”
One challenge Maru noted is that the obstetric setting is not always supportive of doula care in the labor room, in part due to fear of litigation. She suggested focusing on the human aspect of building relationships and awareness about the role of doulas, emphasizing they are focused on helping to facilitate shared decision making. Maru also suggested learning from successful models that engage community health workers.
Miriam Kuppermann, professor at the University of California, San Francisco, spoke about group prenatal care, which is provided concurrently for a group of pregnant people with similar due dates and sometimes shared characteristics. Enthusiasm for this care model as a potential solution to adverse maternal outcomes and preterm birth stems from a 2007 study on viral transmission, she explained, with an incidental finding that women randomized to group prenatal care had a lower rate of preterm birth than those who received individual care (Ickovics et al., 2007). Subsequent systematic reviews of studies found no significant benefit (Carter et al., 2016; Catling et al., 2015), but there is still interest in group prenatal care models focused on high-risk populations. She said the Glow! group prenatal care and support program was eagerly received by participants, had deep community involvement, and addressed issues of social isolation.9 Kuppermann added that the ongoing Engaging Mothers and Babies; Reimagining Antenatal Care for Everyone (EMBRACE) study is assessing the comparative effectiveness of Glow! versus individual prenatal care, with emphasis on three key outcomes: preterm birth, depression and anxiety, and patient-centered maternity care (primarily focusing on Black and Latina populations).10
Kathleen Kerrigan, associate professor at University of Massachusetts Chan Medical School, discussed coordination to improve care transitions between obstetrics and emergency care. As noted earlier, Kerrigan reiterated that more than half (53 percent) of maternal deaths occur between seven days and one year after giving birth (22 percent occur during labor, and 25 percent occur in the first week postpartum). Postpartum patients seeking care in the ED typically have mental health conditions such as suicidal behavior, cardiac conditions such as chest pain or shortness of breath, or infections such as mastitis or urinary tract infections. Kerrigan highlighted the opportunity for educating emergency care providers to better address maternal health care needs through enhanced obstetric curriculum, simulations and drills, and toolkits. Kerrigan stressed the importance of gathering all the necessary information from a patient to ensure an accurate diagnosis. Specifically, she suggested the need for clinicians to ask, “Are you now or have you been pregnant in the past year?” Kerrigan suggested there is a “wellness bias” on the part of health care providers and current artificial intelligence tools, based on the assumption that pregnant people are intrinsically healthy and because they have been excluded from data that inform existing medical calculators and devices to guide diagnosis. Kerrigan concluded by suggesting improved methods of collecting data to support the development of more evidence-based, validated tools to reduce maternal mortality.
STRATEGIES TO MITIGATE DISPARITIES AND PROMOTE EQUITY
Ann Borders, executive director at Illinois Perinatal Quality Collaborative (PQC), discussed strategies to
___________
9 For more information on Glow!, see https://pretermbirthca.ucsf.edu/glow-and-embrace-study (accessed September 17, 2023).
10 For more information on EMBRACE, see https://pretermbirthca.ucsf.edu/glow-and-embrace-study (accessed September 17, 2023).
advance equity in maternal health care. She said the Illinois PQC launched a Birth Equity Initiative in 2021 with six key strategies: optimize race and ethnicity data collection, screen all patients for SDOH and link to community resources, standardize postpartum safety education, engage patients and community members for quality improvement input, provide training on implicit bias and respectful care for all staff, and survey patients on experience. The Birth Equity Initiative aims to have more than 70 percent of participating hospitals implement all key strategies by December 2023. Hospitals are working on implementing respectful care practices for birthing patients and patient-reported experience measures (PREM) to ask patients to report back on their care experience during their labor and delivery admission. Hospitals are now sharing PREM survey results with clinicians and translating patient responses into better care. The results show that improvements in shared decision-making are needed to achieve respectful care. For example, survey results indicated that 14 percent of Black patients felt pressured into accepting care they did not want or did not understand, and more than 20 percent of all patients reported that when the care team could not meet the patient’s wishes, they did not explain why. Borders underscored the importance of “hospitals recognizing that patients are the experts of their own experience and that we have to be empowering patients to make choices through accessible, nonjudgmental communication.” She also said they are trying to conduct SDOH screenings more thoughtfully and connect the patient with needed resources in the community, while also examining how those determinants may play a role in morbidity and mortality.
Christina Davidson, system chief equity officer at Texas Children’s Hospital, discussed incorporating health equity into quality improvement initiatives in maternal health care. She noted that one of the most important factors in preventing mortality and morbidity is through improved quality of care and standardizing care where possible to mitigate biases. She explained that in 2018 Texas launched an initiative inviting more than 200 birthing hospitals to participate in implementing the obstetrics hemorrhage patient safety bundle. The goal was to reduce severe maternal morbidity from hemorrhage by 25 percent by 2020. Considering the stark disparities that exist in maternal morbidity and mortality, Davidson and her quality team cross- walked the safety bundle with another AIM bundle focused on reduction of peripartum racial and ethnic disparities (Howell et al., 2018). Black women patients were twice as likely to experience morbidity from hemorrhage compared to White patients, so they used an equity impact assessment tool to systematically examine how groups of patients would be affected by a proposed action. They examined root causes of disparities, looked at outcomes in Black patients and tracked them after implementation of new policies and procedures. Davidson said this effort led to a significant decrease in the overall morbidity of Black patients and, interestingly, highlighted the power of presenting data and recognizing that a disparity exists; implementation of the safety bundle reduced severe maternal morbidity from hemorrhage for Black women from 44.12 percent in 2018 to 27 percent in 2020. Davidson summarized best practices for achieving health equity, such as standardizing clinical management; stratifying quality measures by race, ethnicity, and language and implementing a disparities dashboard; and approaching every quality improvement effort with a health equity lens. She added that organizations such as the Joint Commission are helping to support diversity and inclusion requirements.
Aimée Brill, co-director of JustBirth Space, discussed operationalizing birth justice metrics to achieve equity in maternal health. JustBirth Space provides individuals with free, responsive, and trustworthy virtual support to safely navigate pregnancy, birth, and the postpartum period. The organization’s three-pronged approach includes direct services, systems transformation, and workforce development. They work with health systems to educate clinicians on birth justice, promote accountability, and center community. Brill emphasized that the core elements of informed consent, respectful maternity care, and addressing intergenerational trauma are critical to achieving birth
justice. She further explained that the organization’s mission is to operationalize birth justice to foster connection, accountability, repair, and equity throughout the perinatal care system. Brill said the organization is working to reframe the concept of equity, moving toward definitions that apply a racial equity lens. For true systems transformation to be achieved, Brill explained, accountability cannot be punitive but should instead be a pathway to healing for birthing people, health care providers, institutions, and communities. Brill suggested reimagining the diagnostic journey model, by factoring in generational trauma, support systems, insurance access, and the individual’s history, as well as SDOH (see Figure 4).
EFFECTIVE DIAGNOSTIC TECHNOLOGIES AND QUALITY INNOVATIONS
Sindhu Srinivas, professor at the University of Pennsylvania, described remote monitoring and early diagnosis. Reiterating that CVD complications and pregnancy-related hypertension are leading causes of maternal morbidity and mortality, she said nearly 75 percent of maternal deaths associated with hypertensive disorders occur postpartum, and almost 40 percent occur more than 48 hours after delivery, often after obstetrical discharge. Srinivas explained that the American College of Obstetricians and Gynecologists issued new guidelines in 2014 advising two assessments of blood pressure (BP) in the first few days and one week after delivery for people with pregnancy-related hypertension. To accomplish this goal, Srinivas and her team developed the Heart Safe Motherhood program in 2015, a remote BP texting and monitoring program for 10 days after discharge. They conducted a randomized controlled trial and found participants using the program were less likely to experience postpartum hypertension readmission and more likely to attend the six-week postpartum appointment. She added that Black patients were more likely to miss office visits than non-Black patients, but the texting program eliminated this disparity. Remote monitoring allowed clinicians to see a trend in measurements and engaged patients so they were more aware of their numbers and problematic BP values. She noted that even up to six months post-discharge, participants had lower adverse outcomes including stroke, eclampsia, and pulmonary edema (Hirshberg et al., 2023). Srinivas summarized that “remote monitoring is a strategy for early, timely, and accurate diagnosis that allows for patient engagement and empowerment.” She concluded by noting that despite implementing this program in multiple hospitals, financial barriers exist related to how these models are paid for and how delivery of care aligns with the payment system.
Afshan Hameed, professor at the University of California, Irvine, discussed cardiovascular risk assessment in pregnancy, noting that CVD accounts
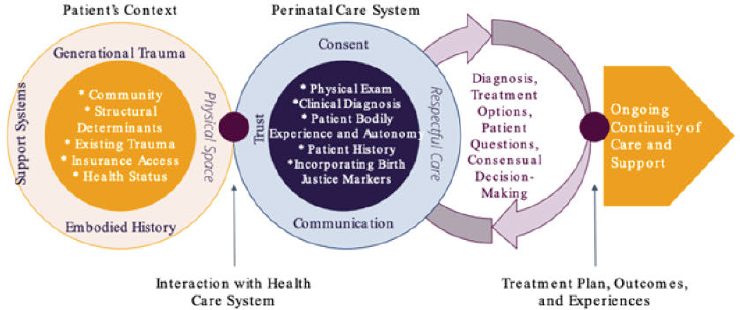
SOURCE: Aimée Brill presentation, July 27,2023.
for 29 percent of all pregnancy-related deaths in California. She said cardiomyopathy typically presents in the postpartum period, usually in the ED or primary care setting (Hameed et al., 2015). Data indicate that more than half of cardiovascular deaths occurred after discharge from the hospital: 22 percent occurred 7 to 42 days after pregnancy, and 32 percent occurred 43 to 365 days after pregnancy. To improve diagnosis of CVD, the California Maternal Quality Care Collaborative developed a CVD Toolkit using an algorithm that was validated in 64 cases of CVD death and had a 93 percent detection rate of high risk for CVD. It considers symptoms, vital signs, risk factors, and abnormal physical exam findings, and provides a positive or negative risk score. Findings from the initial implementation of the toolkit across five hospitals showed that 8 percent of patients screened positive, with a CVD diagnosis in 30 percent of these patients. The benefits of CVD screening in pregnancy, noted Hameed, include the identification of high-risk patients, patient and clinician awareness and education, and opportunity to modify risk factors.
George Saade, professor and chair at Eastern Virginia Medical School, described the challenges in developing biomarkers for adverse pregnancy outcomes. First, many diagnoses depend on clinical judgment, and it can be challenging to differentiate between conditions like preeclampsia, gestational hypertension, or another condition, especially when symptoms and signs overlap. Second, if a test predicts something, there is still a question of clinical utility, such as whether use of the test improves outcomes or decreases costs. Saade also cautioned that there are unintended consequences associated with many of these tests, such as increased resource utilization or preterm delivery. Test performance also needs to be compared to clinical evaluation, Saade said, but that is rarely standardized. Last, the mechanism is unknown for almost all adverse pregnancy outcomes, which makes it difficult to develop a screening test, he said. To address these challenges, Saade suggested developing objective outcomes, insisting on clinical utility in evaluating any test, using accurate dating and gestational age, requiring a clinical comparator, and finally, advocating for preclinical research to better understand the mechanisms.
ENVISIONING THE FUTURE OF DIAGNOSTIC EXCELLENCE
In the final session, panelists highlighted key themes. Watkins observed that, “As we gain more information and understanding of the problem, it is ridiculous that we are still seeing maternal deaths rising.” She said the person-centered models of midwifery and doula care need to be disseminated on a wider scale. Henderson suggested investing in things that are working locally and scaling them up, including perinatal quality collaboratives and maternal mortality review committees. Neel Shah, chief medical officer of Maven Clinic, said there are things “we know work and we have an opportunity to put into practice, but we can’t fix what we aren’t measuring.” He emphasized funding and accountability to enable scaling of successful interventions. Komal Bajaj, chief quality officer of NYC Health + Hospitals/Jacobi/NCB, said thinking more deeply about factors that lead to success is essential. She highlighted some of the fundamental challenges, such as expecting postpartum patients to go to the ED instead of going back to the obstetrical setting. “As we are talking about dismantling structural bias and injustice,” she added, “I think about how to structure the things that are working and hardwire them so we are promoting equitable care from the beginning.” To accelerate progress, Henderson called for “having an infrastructure in place that everyone could access … where we are not working in separate siloes and where we could take our different resources and ideas and pool them to reach the same goal.” In closing the workshop, Bindman called for zero preventable deaths as a measure of success and a commitment to that outcome.
BOX 1
SUGGESTIONS FROM INDIVIDUAL WORKSHOP PARTICIPANTS TO ACHIEVE DIAGNOSTIC EXCELLENCE IN MATERNAL HEALTH CARE
Improving Care Delivery, Training, and Operations
- Employ a dyadic approach in postpartum care, as the health of the mother and baby are inextricably linked (Henderson, Moore, Srinivas).
- Improve coordination and collaboration among primary, emergency, and specialty care in the community and health care systems to deliver comprehensive and integrated maternity care and improve outcomes (Henderson).
- Enhance obstetric curriculum, simulations and drills, and toolkits for emergency care providers to improve maternal health. Encourage clinicians to ask, “Are you now or have you been pregnant in the past year?” (Kerrigan).
- Adapt established successes in primary care into the obstetrics context (Miller).
- Optimize care in the postpartum period or “fourth trimester” to improve maternal morbidity and mortality (Borders, Brill, Goffman, Kerrigan, Maru, Moore, Srinivas).
Policy Opportunities
- Fully fund solutions that are working, including perinatal quality collaboratives and maternal mortality review committees across the country (Henderson).
- Emphasize funding and accountability to enable scaling of successful interventions (Shah).
- Cover effective care models, encourage co-location of services, remove barriers to support equitable reimbursement of services, and create a statewide requirement for direct billing (Moore).
- Advocate for policies to advance midwifery and doula care models focused on respectful and patient-centered care to improve maternal health outcomes (Henderson, Joseph, Maru, Watkins).
Emphasizing Patient-Centered Care
- Encourage active participation and engagement of pregnant people in the decisions made about their health to achieve optimal outcomes (Henderson).
- View patients as partners and experts in their own experience and allow them to speak and make choices through accessible, nonjudgmental communication (Bajaj, Borders, Henderson, Moore, Weingart).
- Leverage the power of storytelling, especially narrative comments in surveys and using the wide audience of social media (Bajaj, Watkins, Weingart).
- Speak to patients and one another in ways that support respectful care (Borders, Brill, Joseph).
Developing Innovations in Health Technology
- Require simulation training for clinicians to reduce diagnostic error in obstetrics (Deering, Henderson, Kerrigan).
- Invest in remote monitoring as a strategy for early, timely, and accurate diagnosis that allows for patient engagement, empowerment, and meaningful impact on long term health (Srinivas).
- Invest in preclinical research and clinical utility studies when developing screening tests (Saade).
Focusing on Access, Equity and Birth Justice
- Consider opportunities across the diagnostic journey to improve birth equity, including screening patients for social determinants of health, enhancing education and training, engaging patients and families, building community partnerships, and centering patient and community narratives (Borders, Brill, Henderson, Watkins).
- Standardize clinical management; stratify quality measures by race, ethnicity, and language; implement a disparities dashboard; and approach every quality improvement effort with a health equity lens (Davidson).
- To eliminate disparities, consider the complex causes such as health status, inadequate access to health care, and social determinants of health before pregnancy (Henderson).
- Improve access to doula care, midwifery-led care, and perinatal mental health care for Medicaid enrollees (Moore).
- Provide respectful maternity care and acknowledge injustices that contribute to disparities (Joseph).
Identifying Research Priorities
- Include pregnant people in research to develop technologies and tools, especially to inform artificial intelligence algorithms (Kerrigan).
- Focus on artificial intelligence tools to enhance risk prediction and early recognition of problems (Goffman).
NOTE: This list is the rapporteurs’ summary of points made by the individual speakers identified, and the statements have not been endorsed or verified by the National Academies of Sciences, Engineering, and Medicine. They are not intended to reflect a consensus among workshop participants.
Suggestions from workshop participants for improving diagnostic excellence in maternal health care are outlined in Box 1.
REFERENCES
Carter, E. B., L. A. Temming, J. Akin, S. Fowler, G. A. Macones, G. A. Colditz, and M. G. Tuuli. 2016. Group prenatal care compared with traditional prenatal care: A systematic review and meta-analysis. Obstetrics and Gynecology 128(3):551-561.
Catling, C. J., N. Medley, M. Foureur, C. Ryan, N. Leap, A. Teate, and C. S. Homer. 2015. Group versus conventional antenatal care for women. Cochrane Database of Systematic Reviews 2015(2):Cd007622.
Cox, J. L., Holden, J. M., and Sagovsky, R. 1987. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. The British Journal of Psychiatry 150(6):782-786.
David, E. N.-T., N. Najlla, C. S. Adam, Y.-M. Chihwen Winnie, D. C. Gwendolyn, W. Zheyu, Z. Yuxin, S. S. T. Ali, F. Mehdi, H. Ahmed, and S. Dana. 2023. Burden of serious harms from diagnostic error in the USA. BMJ Quality and Safety. https://doi.org/10.1136/bmjqs-2021-014130.
Easter, A., J. Sandall, and L. M. Howard. 2021. Obstetric near misses among women with serious mental illness: Data linkage cohort study. The British Journal of Psychiatry 219(3):494-500.
Fleszar, L. G., A. S. Bryant, C. O. Johnson, B. F. Blacker, A. Aravkin, M. Baumann, L. Dwyer-Lindgren, Y. O. Kelly, K. Maass, P. Zheng, and G. A. Roth. 2023. Trends in state-level maternal mortality
by racial and ethnic group in the United States. Journal of the American Medical Association 330(1):52-61.
Hameed, A. B., Lawton, E. S., McCain, C. L., Morton, C. H., Mitchell, C, Main, E. K., and E. Foster. 2015. Pregnancy-related cardiovascular deaths in California: Beyond peripartum cardiomyopathy. American Journal of Obstetrics and Gynecology 213(3):379-e1-10.
Hirshberg, A., Y. Zhu, A. Smith-McLallen, and S. K. Srinivas. 2023. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstetrics and Gynecology 141(6).
Howell, E. A., H. Brown, J. Brumley, A. S. Bryant, A. B. Caughey, A. M. Cornell, J. H. Grant, K. D. Gregory, S. M. Gullo, K. B. Kozhimannil, J. M. Mhyre, P. Toledo, R. D’Oria, M. Ngoh, and W. A. Grobman. 2018. Reduction of peripartum racial and ethnic disparities: A conceptual framework and maternal safety consensus bundle. Obstetrics and Gynecology 131(5):770-782.
Hoyert, D. L. 2020. Maternal mortality rates in the United States, 2020. National Center for Health Statistics E-Stats. Atlanta, GA: Centers for Disease Control and Prevention, https://dx.doi.org/10.15620/cdc:113967.
Hoyert, D. L. 2023. Maternal mortality rates in the United States, 2023. National Center for Health Statistics E-Stats. Atlanta, GA: Centers for Disease Control and Prevention, https://dx.doi.org/10.15620/cdc:124678.
Ickovics, J. R., T. S. Kershaw, C. Westdahl, U. Magriples, Z. Massey, H. Reynolds, and S. S. Rising. 2007. Group prenatal care and perinatal outcomes: A randomized controlled trial. Obstetrics and Gynecology 110(2 Pt 1)330-339.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015. Improving diagnosis in health care. Edited by E. P. Balogh, B. T. Miller, and J. R. Ball. Washington, DC: The National Academies Press.
Trost, S. L., J. Beauregard, G. Chandra, F. Nije, J. Berry, A. Harvey, and D. A. Goodman. 2022. Pregnancy- related deaths: Data from maternal mortality review committees in 36 U.S. States, 2017-2019. Atlanta, GA: Centers for Disease Control and Prevention.
DISCLAIMER This Proceedings of a Workshop—in Brief has been prepared by Laurene Graig, Jennifer Lalitha Flaubert, and Megan Snair as a factual summary of what occurred at the meeting. The statements made are those of the rapporteurs or individual workshop participants and do not necessarily represent the views of all workshop participants; the planning committee; or the National Academies of Sciences, Engineering, and Medicine.
*The National Academies of Sciences, Engineering, and Medicine’s planning committees are solely responsible for organizing the workshop, identifying topics, and choosing speakers. The responsibility for the published Proceedings of a Workshop—in Brief rests with the institution. Andrew Bindman (Chair), Kaiser Permanente; Komal Bajaj, NYC Health + Hospitals/Jacobi/NCB; Elizabeth Howell, University of Pennsylvania; Kathryn McDonald, Johns Hopkins University; Audra Meadows, University of California, San Diego; Mary Norton, University of California, San Francisco; Chanel Portia-Albert, Ancient Song Doula Services; and Saul Weingart, Brown University.
REVIEWERS To ensure that it meets institutional standards for quality and objectivity, this Proceedings of a Workshop— in Brief was reviewed by Shad Deering, Baylor College of Medicine, CHRISTUS Health, Sindhu K. Srinivas, University of Pennsylvania, and Charity S. Watkins, North Carolina Central University, Duke University. Leslie J. Sim, National Academies of Sciences, Engineering, and Medicine, served as the review coordinator.
STAFF Laurene Graig, Jennifer Lalitha Flaubert, Anesia Wilks, Adrienne Formentos, and Sharyl Nass, Board on Health Care Services, Health and Medicine Division, National Academies of Sciences, Engineering, and Medicine.
SPONSORS This workshop was supported by the Gordon and Betty Moore Foundation and The Commonwealth Fund.
For additional information regarding the workshop, visit https://www.nationalacademies.org/event/07-27-2023/workshop-on-advancing-diagnostic-excellence-for-maternal-health-care.
SUGGESTED CITATION National Academies of Sciences, Engineering, and Medicine. 2023. Advancing diagnostic excellence for maternal health care: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/27314.
| Health and Medicine Division Copyright 2023 by the National Academy of Sciences. All rights reserved. |













