
1
Introduction
As a nation, we invest in the health of some (85 percent) of the population by providing tax subsidies for the purchase of private health insurance or direct coverage through Medicare, Medicaid, and the State Children’s Health Insurance Program. What does it cost us as a society, in terms of health and social equity, as well as dollars, to leave 15 percent of our population uninsured? This fifth report of the Institute of Medicine (IOM) Committee on the Consequences of Uninsurance examines the implications of uninsurance primarily but not exclusively from the perspective of the national economic costs and financial transfers incurred as a result of our current policies regarding health insurance coverage.
Hidden Costs, Value Lost: Uninsurance in America consolidates information that the Committee has developed over the course of its examination of personal, familial, and community outcomes and considers these findings within the context of the national economy and political culture. In this report, the Committee presents aggregate estimates in monetary terms of
-
the costs of health care provided to those who lack health insurance that are borne both by uninsured individuals and their families and by the public and private programs and providers that subsidize uncompensated care and donate services;
-
the value of additional years of healthier life that would be gained by those without health insurance in the United States if health insurance coverage were extended to everyone; and
-
the cost of the additional health care that would be provided to the uninsured if they gained health insurance.
Hidden Costs, Value Lost attempts to answer another fundamental question: Who ultimately bears the costs consequent to uninsurance within the U.S. population? Understanding who eventually pays for the health care that uninsured people receive and the economic value lost as a consequence of not receiving adequate care are important to evaluating alternatives for expanding coverage.
CONTEXT
This report is the fifth in a series of studies that constitute a systematic assessment of the ramifications of failing to include millions of people each year in the predominant organizational form and financing mechanisms for health care services in the United States, private and public health insurance. The Committee has approached its task in a stepwise fashion. It has analyzed the highly complex and interactive health services and insurance sectors and government health and social welfare programs by focusing on different parts of the overall picture in each of its reports to date. Figure 1.1 displays this sequential and cumulative analytic approach as concentric rings spreading out from individual health outcomes, through families and communities, to the social and economic effects of uninsurance in the aggregate, at the national level. This report “slices” through each of these layers and consolidates information about the costs related to each one.
The rest of this section recaps in broad terms the subjects and general conclusions from the previous four reports and notes how their findings are used in this report.
Coverage Matters: Insurance and Health Care (IOM, 2001a), the Committee’s introductory report, presented an overview of the dynamics of health insurance coverage in the United States and estimates of the number and characteristics of the population that lacks coverage. It also highlighted discrepancies between the Committee’s findings based on empirical research and popular beliefs and understanding of the causes and implications of uninsurance in order to promote greater public awareness of and greater insight into the persistent national problem of uninsurance.
The second report, Care Without Coverage: Too Little, Too Late (IOM, 2002a), was a critical review of clinical and epidemiological health outcomes research that evaluated the effect of health insurance status on a variety of general and condition-specific indicators and outcomes for American adults younger than 65. The Committee concluded in this report that health insurance is associated with better health outcomes for adults and with the receipt of appropriate care across a range of preventive, chronic, and acute care services. Adults without health insurance have shorter lives and greater declines in health status over time than those with continuous coverage. Care Without Coverage developed illustrative estimates of excess deaths associated with being uninsured for the adult population under age 65, both overall and for several specific diseases. Overall, the Committee estimated that the uninsured adult population under age 65 experiences roughly 18,000
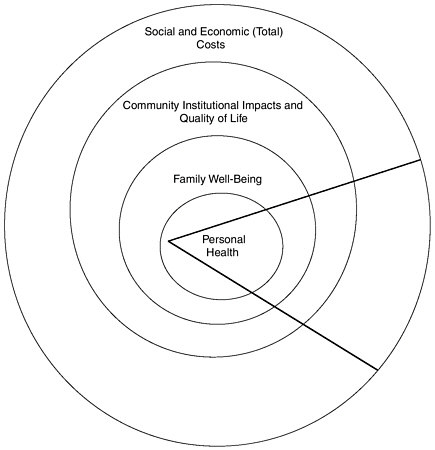
FIGURE 1.1 Levels of analysis for examining the effects of uninsurance.
premature deaths annually that can reasonably be attributed to the lack of coverage and the less adequate health care received as a result (IOM, 2002a). The Committee also developed illustrative estimates for deaths among nonelderly uninsured adults due to hypertension, breast cancer, and HIV/AIDS. The studies and findings of differential health outcomes for insured and uninsured adults contained in the second Committee report are used in this report to estimate the economic value of the healthier years of life forgone due to uninsurance within the U.S. population.
The Committee’s third report broadened the focus of analysis to the social and economic unit of the family. Health Insurance Is a Family Matter (IOM, 2002b) considers the impact of a lack of health insurance for individuals within a family on the family as a whole, including the financial consequences of burdensome medi-
cal expenses, psychosocial stress, and the dependence of children’s coverage and health care on their parents’ coverage status. The third report also reviewed the extensive body of health outcomes research for pediatric, prenatal, and maternity care as a function of health insurance status. It documented the gains in access to appropriate health care and better health outcomes for children and pregnant women with coverage. The Committee concluded in Health Insurance Is a Family Matter that all members of the family face financial risk and may imperil their physical and emotional well-being if anyone in the family lacks coverage. Fully one-fifth of the U.S. population, approximately 60 million people, is affected by the lack of health insurance within their immediate family. The findings and conclusions of the Committee’s third report are represented in Hidden Costs, Value Lost by the estimates of the value of health forgone due to uninsurance and in the costs of diminished financial security for families and the anxiety and stress that accompany the lack of health insurance within the family.
A Shared Destiny: Community Effects of Uninsurance (IOM, 2003a), the Committee’s fourth report, adopts yet a broader perspective on the phenomenon of uninsurance within the United States. It looks at how communities are affected by the lack of coverage that some of its members endure, through mechanisms such as the poorer health of uninsured people, their needs and use of health care services and the sources of payment for that care, and the social and economic disparities within communities that are deepened by a lack of health insurance. This report breaks new ground in the analysis of how uninsured populations affect the quality and accessibility of health services within communities generally, and the overall character of communities in terms of health, social cohesiveness, and economic vitality. The Committee concludes in A Shared Destiny that high levels of uninsurance within communities disrupt local systems of public health and personal health care and adversely affect the availability and quality of services within the community. Furthermore, the stability and financial viability of community institutions and health care resources are threatened by the amount of uncompensated care that health care practitioners and facilities render. Finally, the national goal of attaining community-wide a high quality of personal health care services across the spectrum of services and providers cannot be met while those without health insurance rely on ad hoc delivery of services.
A Shared Destiny identifies several of the costs of uninsured populations that are borne by others. Some of these spillover costs and economic transfers, such as uncompensated or charity care provided when someone without health insurance or the means to pay for care directly is hospitalized, are readily measured in dollars. Other spillover costs of uninsured populations, such as the loss for an urban neighborhood or rural community of a primary care clinic because too many among its clientele have no source of payment for their care, are theoretically quantifiable in monetary terms but the information that would be needed to measure these costs is not available. Still other societal consequences resulting from inequalities manifested in disparate access to health care because of uninsurance within a local community or the national population cannot be represented in
monetary terms. The Committee hypothesizes that uninsurance weakens social cohesiveness and exacerbates other social inequalities. Disparities among neighbors and fellow citizens in health insurance status and thus in access to highly valued medical care and attention may erode feelings of social belonging and trust within communities. Thus, with A Shared Destiny, the Committee began its investigation of some of the potential spillover costs of uninsurance.
PURPOSE
Hidden Costs, Value Lost continues this examination of the impacts of uninsurance from a national perspective and considers the benefits for American social and political life that could be achieved by guaranteeing health insurance coverage to all throughout their lives. It builds on the evidence presented in the Committee’s earlier reports and anticipates the concluding report, which will articulate core principles that derive from these studies and use them to analyze strategies for achieving complete health insurance coverage of the U.S. population. By estimating the resources now devoted to health care for 41 million uninsured Americans, the losses in terms of health and longevity that they experience, and some of the costs and benefits of extending coverage to them, this report provides a baseline against which health insurance reform strategies can be assessed.
The Committee hopes to reach a broad audience—including the voting public, legislators, and other policy makers—with this report, and attempts to present economic and policy research findings and analyses in nontechnical language whenever possible. (A glossary of technical terms is included as Appendix A.) The research and analytic tools of economists and other social scientists, epidemiologists, and public policy analysts are not widely disseminated or well understood by lay audiences. The Committee believes this lack of awareness of the powerful analytic tools of the social and health sciences, and of the information developed by using these tools, fosters a narrow understanding of the costs of having a large uninsured population. By discussing its assumptions, methods, and sources of information, along with its findings and conclusions, the Committee hopes to raise awareness of some of the real costs incurred as a result of widespread uninsurance and to inform policy debates. The analytic approach and estimates of costs presented in the report should be useful to those who are developing their own policy alternatives and strategies.
In preparing this report, the Committee and its Subcommittee on Societal Costs of Uninsured Populations reviewed economic research and policy analysis that offered models for evaluating the costs and benefits of various health interventions. Providing health insurance to those who now lack it can be viewed as one such health-enhancing intervention. Conversely, maintaining a population of 41 million uninsured people can be viewed as a health risk at the population level.
The Committee followed the general approach taken by government agencies that regulate health and safety (e.g., the Food and Drug Administration, the
Department of Transportation, the Environmental Protection Agency, and the Consumer Product Safety Commission) to assess investments in life-saving, health-enhancing, and risk-reducing endeavors. These agencies use an analytic methodology that involves estimating the value of a “statistical” or anonymous life in order to determine if the benefit of a particular risk-reducing or health-enhancing intervention or policy justifies the costs it imposes or entails. The Committee’s choice of approach was guided in large part by the highly aggregate nature of the information available on health outcomes dependent on insurance status and its conceptualization of uninsurance as a population-level risk factor. Chapter 2 discusses the Committee’s approach further, along with other analytic frameworks, such as those used in studies of the economic costs of discrete illnesses.
The Committee commissioned an analysis by economist Elizabeth Richardson Vigdor to estimate the economic value to those who now lack health insurance of their diminished health and longevity as a result of their lack of coverage. The results of this analysis are described and used in the body of the report, and Vigdor’s more technical and complete monograph is included as Appendix B. This analysis is the Committee’s major contribution in this report to the quantification of costs of uninsurance.
In addition to presenting quantitative and qualitative information about some of the costs that follow from uninsurance, the Committee reviews several sets of estimates of the costs of providing the additional health care that the uninsured would use once they became insured. This review of the additional costs of providing the benefits of coverage that would reduce morbidity and premature mortality among the uninsured is an essential part of the consideration of the economic and ethical choices to be made concerning universal health insurance coverage.
Finally, in this report the Committee considers important, less tangible aspects of the value of the collective provision of health insurance, whether through public or private mechanisms. The collective, social interests that are at stake when we consider and make choices about health insurance policy in the United States are best demonstrated through examples from our nation’s history. These are previewed in the remainder of this section.
Both altruism and justice have been offered as reasons for extending with public dollars health insurance benefits to those who cannot pay for their care or coverage themselves. Altruistic interests in providing access to health care accounted for the establishment of hospitals in the United States, initially by religious and charitable organizations, in the 18th and 19th centuries as places for caring for the poor who were ill and dying. This compassionate motivation was joined with a social ethic of mutual support that became more explicit over the course of the 20th century. By the time of the passage of Medicare and Medicaid in the 1960s, the provision of health benefits to the elderly and to poor families through the mechanism of social insurance was widely understood as a fair and compassionate way to distribute the burdens of ill health and to spread risk across generations and social classes (NASI, 1999). These programs, which now account
for 36 percent of national spending for personal health care services, are central features of the social contract in the United States.
Congress enacted Medicare’s End-Stage Renal Disease (ESRD) Program in 1972 in recognition that, without such a program, patients dependent on kidney dialysis would die in the near term (Starr, 1982; Bulger et al., 1995). The creation of Medicare benefits for this especially vulnerable group of Americans was perhaps foremost an expression of collective altruism. The ESRD program, however, was enacted without an accurate idea of how costly this expansion of life-preserving benefits would quickly become.1
Equity across members of a single society also motivates American social insurance programs. As medical interventions have become more effective in improving health and extending life (Cutler and Richardson, 1999; Murphy and Topel, 1999; Cutler and McClellan, 2001; Heidenreich and McClellan, 2003), the losses associated with not having health insurance also have increased. The Committee documented these losses in Care Without Coverage and Health Insurance Is a Family Matter. Questions about the equity of access to medical interventions for all members of society regardless of health insurance status have become more urgent as coverage affords access to increasingly effective services (IOM, 2003c).
Recently expanded access to public health insurance illustrates these principles well. The Breast and Cervical Cancer Prevention and Treatment Act of 2000 (P.L. 106-354) allows states to extend Medicaid coverage to women whose disease is identified through a publicly sponsored screening program (a federal program that began in 1990), regardless of meeting other eligibility criteria for Medicaid. This Medicaid option has been picked up by 45 states and the District of Columbia at a historically rapid rate (Miller, 2002a). Federal and state legislators’ actions can be understood as a collective response to the fundamental unfairness of life-saving care being beyond the means of most uninsured women, once public resources have been expended to identify the disease. This legislation recognizes the futility of screening for disease if treatment is not available. It also expresses compassion for those with these life-threatening diseases.
ORGANIZATION
Five chapters follow. Chapter 2 presents the analytic context and conceptual grounding for this report. It also articulates the Committee’s understanding of the incentives and motivations embedded in private health insurance and public coverage arrangements. Last, it provides a rationale for the particular measures of costs that the Committee adopted.
The third chapter assesses the costs of care now provided to those who lack health insurance and identifies who pays these costs. These include out-of-pocket payments for health care by the uninsured and uncompensated care costs supported by public appropriations and subsidies and by philanthropic support. The chapter also reviews evidence for uncompensated care as a factor contributing to inflation in health care costs and insurance premiums. Last, it considers the distribution of spending across the federal, local, and state governments to support services for uninsured people.
Chapter 4 considers the opportunity costs of extensive uninsurance. The first section presents estimates of the additional value of health and longevity that coverage could provide to those now uninsured. The second section considers the financial risks and other stresses that individuals and families bear when they lack coverage. The remaining four sections discuss in qualitative terms
-
impaired developmental outcomes for children,
-
the demands placed on Medicare, disability income support, and other public programs,
-
workplace productivity and labor force participation, in particular from the employer’s standpoint, and
-
effects on the availability and quality of health care and on public health.
Chapter 5 provides estimates of the likely increase in health care expenditures that would result from providing health insurance to those who now lack it. This investment, the Committee believes, will lead to the better (i.e., lower) morbidity and mortality experience of Americans and to an array of potential societal benefits summarized in Chapter 4.
In conclusion, Chapter 6 brings together the estimates and analyses from the earlier chapters and considers the cost-effectiveness of the increased services that would likely accompany coverage of those currently uninsured in the context of other investments in health that American society chooses to make. Here the Committee addresses the unquantifiable but critically important contribution that providing health insurance coverage to everyone would make to the fulfillment of values and norms deeply embedded in American history and culture: mutual caring, equal opportunity, and equal respect. Last, it summarizes the Committee’s conclusions regarding the national social and economic burdens of uninsurance and the costs and benefits of providing coverage throughout the U.S. population.








