
5
Measuring Influences on Children’s Health
A comprehensive system to monitor children’s health would contain an inclusive, continuing assessment and monitoring of the range of influences on children’s health, including children’s biology and behavior, social environments (family, community, culture, and discrimination), physical environments, and services and policy contexts. Development of such a system requires careful long-term consideration of which influences are important, how they are being measured, how to improve their measurement, and what additional measures might result in important benefits to children’s health.
We begin this chapter with an overview of current issues and challenges in measuring the multiple influences on children’s health. We then outline the current approach and particular challenges of measuring each of the influences identified in Chapter 3 and then discuss how the gaps in measurement of each influence might be improved, including potential future opportunities in light of advances in research methods. Many of the methodological problems and practical obstacles in measuring various health influences are the same as those in developing and implementing measures of health. These areas of overlap are not repeated here, although commonalities are briefly noted. Many of the current surveys that capture data on influences were mentioned in the previous chapter and are outlined in Appendixes A and B; descriptive information regarding specific surveys is not repeated here. Appendix B lists various data elements for the influences outlined in this report that are captured by 12 of the major national surveys.
For some types of influences discussed below, there is ample evidence of the effect they have on children’s health. The challenge is to ensure their adequacy in
date collection efforts so that differences across time and among subpopulations can be effectively monitored. For others, although there is evidence that they influence health, the challenge is to develop more adequate means of understanding the nature of their influences. In these instances, attention needs to be focused on using data collection to facilitate studies of the way in which they operation on populations and subpopulations.
OVERVIEW
The measurement of many influences poses methodological challenges that must be considered and systematically addressed in future research, surveys and evaluation studies. For such factors as biological influences on children’s health, invasive medical tests may be necessary and raise potential ethical questions about risk-benefit ratios of specific assessment procedures. In other cases, the need for highly personal information raises confidentiality concerns and concerns about unintended consequences of shared information. In still other instances, such measures as policy influences may require aggregation across governmental units and agencies.
Several overall issues must be considered to improve the measurement of influences on children’s health. First, how do various influences interact with one another over time to affect health? Specific influences may set in motion a chain reaction, unleashing other biological and behavioral processes than can cascade toward a specific outcome (final common pathway) or a range of potential outcomes (multiple pathways). Since each interaction in such a cascade is potentially a point to monitor and intervene, understanding and measuring such effects become important methodological challenges. As a specific developmental stage or sensitive period, exposure to a specific influence can unleash a cascade of effects with significant short- and long-term impacts, whereas the same exposure at a different stage may have a muted or minimal effect.
Another challenge is how to understand and model the effect of multiple influences for policy purposes. For example, when a child is exposed to multiple adverse influences at the biological, behavioral, family, and community levels, are these factors simply additive, or are they multiplicative (Rutter, 1994; Werner, 1993)? The most effective prevention and intervention strategies may target high-risk groups (i.e., those affected by multiple risk factors), rather than using strategies that address single risk factors. For policy purposes, which children may be most at risk for later adverse outcomes, and which may be most in need of special assistance?
Aggregation of data on influences at the individual, family, and community levels is complicated (Small and Supple, 2001) and prone to errors in the application of statistical techniques, drawing appropriate causal inferences, and estimating the relative size of influences’ effects.
Apart from biomarkers, the physical environment, family demography, and
results from formal medical evaluations, almost all influences require the subjective reports of people (often parents reporting for children) who must describe their perception of the presence or absence, severity, and duration of a particular health influence. Such perceptions tend to differ from person to person, raising important concerns about the validity of any single source of information, particularly when policy decisions (such as the distribution of resources) are to be based on such information.
Despite the fact that parents from different cultural backgrounds must complete these surveys, there are often insufficient data demonstrating that survey items are accurately understood by parents across different cultural contexts, and surveys are not consistently offered in multiple languages. While this challenge poses daunting obstacles to the interpretability of survey findings across cultures, new translation methods have been developed and described that may facilitate more valid responses across cultural groups (Erkut, Alacron et al., 1999b).
Another concept implicit in the committee’s conceptual approach is the important role of both positive and negative influences on health. If health trajectories are to be modified, then health measurement at a population level needs to clearly account for the presence and effect of influences, their direct and indirect relationship to each other, and to the health outcome of interest. For example, if substance abuse during adolescence is the outcome of interest, a conceptually driven and integrated health measurement strategy would measure and account for the effect of adverse influences on drug use (e.g., peer influences, school performance, lack of adequate parental supervision) as well as protective factors (e.g., mentoring relationships and educational and economic support).
Despite knowledge that adverse health influences often disproportionately fall on some population subgroups more than others, systematic collection of health care data on subpopulations at a local, state, or national level is episodic. Surveys rarely provide enough information to develop a comprehensive picture of the health of young children, or to understand the role of various influences during early childhood, or to assess their receipt of appropriate personal or public health services or the effect of health care on their health. While there has been recent increasing emphasis on the importance of early childhood, as well as considerable focus on adolescence, there has not been the same kind of focus on health influences in the intervening years.
MEASURING BIOLOGICAL INFLUENCES
The range of biological influences on children’s health are assessed using “biomarkers,” which are indicators signaling events in biological systems or samples (for review, see National Research Council, 1989). There are three categories of biomarkers: biomarkers of exposure, biomarkers of effect, and biomarkers of susceptibility (see Figure 5-1). The markers fall along the time course from exposure (e.g., prenatal exposure to alcohol) to health outcome (e.g.,
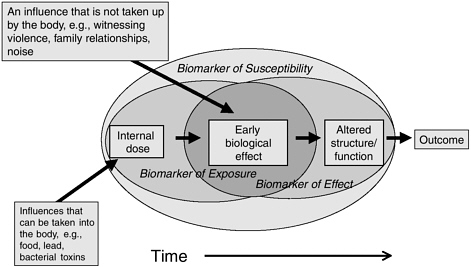
FIGURE 5-1 The three types of biomarkers.
NOTE: The three categories of biomarkers are biomarkers of exposure, biomarkers of effect, and biomarkers of susceptibility. The boxes represent the different steps in the progression from exposures to a health outcome. The solid arrows depict the rate of change from one stage to the next; the time of progression from one stage to the next is highly variable. The nested ovals represent the areas where biomarkers of exposure, effects, and susceptibility may be found and show their overlapping nature (adapted from Committee on Biological Markers of the National Research Council, 1987).
fetal alcohol syndrome). In general, biomarkers of exposure are nearer in time to the exposure (i.e., they are designed to detect exposure rather than the effect of exposure), while biomarkers of effect are generally nearer in time to the outcome (i.e., they are designed to detect the effect of exposure or the effect on health). The time course of moving from exposure to outcome is not continuous. For example, an internal dose can occur quickly after an acute exposure, while a biological effect may take decades (e.g., exposure to radioactive material and the development of thyroid cancer or exposure to asbestos and lung cancer). Biomarkers of susceptibility can mark increased vulnerability at any of the steps between exposure and outcome.
Biological factors that influence health, such as genotypes for functionally important genetic polymorphisms, variations in gene expression, and biochemical measures that reflect body stores or internal doses of environmental exposures, are useful biomarkers. Thus, the concept of biomarkers provides an organizational framework for considering existing indicators and the potential influence of the biological environment. We use this framework in considering current assessments of biological influences, as well as assessment gaps. Identification and
selection of particular biomarkers for a specific research or public health purpose would need to include careful consideration of such factors as the ease of collecting a particular biological specimen and the cost of biological analyses.
Biomarkers of Susceptibility
Biomarkers of susceptibility include such factors as biological measures of health and genes. A child’s current health as reflected in his or her level of immunity or level of cortisol production may also serve as a valuable indicator of biological susceptibility. Under certain circumstances, age can serve as a proxy for developmental susceptibility, such as the age of risk for sudden infant death syndrome (infants) or testicular cancer (adolescents). The composition of ages in a population, obtainable from the U.S. Census Bureau, can be used as an indirect indicator of susceptibility in the population for specific age-related health conditions. However, most measures of biological susceptibility require some form of biological assay.
As discussed in Chapter 3, polymorphisms (variations from person to person in a gene’s molecular structure) in certain genes may impart susceptibility to certain environmental exposures. A biomarker of susceptibility for the individual would be the specific genotype of that gene, while the biomarker of susceptibility for the population would be the frequency of that genotype. An example of an existing database for genes of susceptibility includes newborn screens. Newborn screen testing varies from state to state, but most states include screening for hyperphenylalaninemia (PKU), hypothyroidism, classical galactosemia, and hemoglobinopathies.1 While congenital hypothyroidism is not always caused by a genetic polymorphism, the screen identifies cases that are genetic in origin. The newborn screen is the only universal population-based database in the United States for children’s genetic susceptibilities.
Biomarkers of Exposure
There are several measurement activities for internal dose/body stores/body burdens. Two major programs are being conducted by the Centers for Disease Control and Prevention (CDC): the biomonitoring program and the National Health and Nutrition Examination Survey (NHANES) survey. The process of expanding biomonitoring capability to select state laboratories is currently under way (Federal Register, Vol. 68, No. 64/Thursday, April 3, 2003/Notices p. 16287).
|
1 |
A listing of the tests done in each state, as well as the summary results of the screening, can be found at the following web site: http://genes-r-us.uthscsa.edu. |
Biomonitoring is the direct measurement of environmental chemicals, their primary metabolites, or their reaction products in people—usually in blood or urine specimens. The CDC Division of Laboratory Services has developed methods to measure 200 substances in blood or urine, including but not limited to polychlorinated biphenyls, dioxins, furans, the persistent organic pollutants, DDT and its metabolite DDE, nonpersistent organic pesticides and their metabolites, polyaromatic hydrocarbon metabolites, phthalate metabolites, metals (e.g., lead), volatile organic compounds, and phytoestrogens.2
The NHANES survey also includes information about the health and diet of people in the United States. There are both questionnaire and laboratory measurements on a survey of 4,800 children younger than age 19 over a 2-year cycle. Laboratory measurements include iron status, vitamin stores and folate levels, and indicators of specific infections such as viral hepatitis.
Biomarkers of Effects
There are few measurement activities related to biomarkers of effects that are not measurements of health. For example, the NHANES survey measures a few, such as physical growth, biomarkers of inflammation and bone density, and liver, kidney, and respiratory function. NHANES also measures immunization status by measuring antibody levels as a result of immunization. While patterns of changes in gene expression may be a sensitive and specific biomarker of effect, no current population-based measurement activities of gene expression are currently taking place, except in clinical settings for research purposes.
Challenges in Measuring Biological Influences
Several methodological issues are of concern in measuring biological influences. First, obtaining biological samples from fetuses and children is difficult. Samples for biomarkers must be obtained ethically, non-invasively and with a minimum of pain, and be acceptable to both child and parent. Table 5-1 provides examples of types of samples with their advantages and disadvantages. Although it may soon be possible to determine multiple polymorphisms in individuals, the ethical issues in doing so are complex. Guidelines on the ethics of this testing have been proposed (Bakhtiar and Nelson, 2001).
Second, validating a biomarker as a true measure of a biological influence on health is difficult and time-consuming. A number of steps are necessary, includ
|
2 |
The current national status report of population exposure levels (from the CDC’s 2002 NHANES) for 116 of these chemicals can be found on the CDC web site: http://www.cdc.gov/exposurereport/. |
TABLE 5-1 Appropriate Biological Samples in Which to Measure Biomarkers Indicating Fetal/Pediatric/Adult Exposure/Effect
ing (1) developing and validating a biomarker to identify a chemical or biochemical exposure or exposure effect; (2) selecting the biological sample (e.g., blood, breath, or urine) to measure the biomarker; (3) addressing ethical, practical, and cost-related obstacles in actually obtaining the sample; (4) developing a method for analytical quantification of the biomarker in the specific sample (addressing how much biomarker can be recovered from the tissue sample, how much variation exists in recovery of the marker between samples, biomarker stability in the chosen sample, etc.); and (5) ascertaining biomarker sensitivity and specificity to exposure or effect.
Validation of a marker also depends on its expected use. Although biological markers observed well before the onset of disease may have little value for predicting the later occurrence of disease, they may be more useful for identifying exposed populations for long-term follow-up. Examples of biological samples appropriate for biomarker determination are hair, saliva, blood, urine, breath, umbilical cord, umbilical cord blood, placenta, stool (including the first stools passed by a newborn, called meconium), and toenails.
Addressing Gaps in Measuring Biological Influences
The importance of biomarkers has been insufficiently appreciated in assessing children’s health and its influences. Biomarkers may be useful even beyond measuring the effect of chemical or environmental agent exposure. For example, biomarkers might be developed that could indicate environmental interactions with the other spheres of influences. This is relevant for all aspects of health measurement, because for any influence to affect physical health or well-being, it must be translated through the child’s internal biological environment. Such biological events could potentially be measured. While biomarkers have been associated mainly with toxic events and poor outcomes, biomarkers of positive influences and positive effects could be developed.
When biomarkers of exposure and effect are collected, most often they are collected at the same time in the same person. Yet the effect of a particular exposure often does not occur until later and sometimes a long time after the exposure. Without longitudinal studies, the possibility of understanding the cause-effect linkage is lost, and the effect may be attributed incorrectly. Thus, the opportunity to develop high-impact health policies is lost.
Another methodological gap is the paucity of biomarkers when the exposure does not result in systemic absorption. Two examples are the respiratory system and the skin. While air pollution can be measured and quantified, indicators of dose to the airways or the biologically effective dose have not been developed. The absence of valid indicators may obscure the linkage of exposures to effects on health. Thus, the influence on occurrence of asthma or other important respiratory diseases of some elements in air pollution remains controversial. Development of new biomarkers using breath or nasal secretions may potentially be use-
ful in this area. Where biomarkers have been developed, such as the collection of urinary and salivary samples for cotinine levels, as biomarkers of environmental tobacco smoke, they have been very useful.
Finally, current biomarker methods are based mainly on analyzing one biomarker at a time. For biomarkers for which a battery of tests and an algorithm have been established, sensitivity and specificity improve, thus indicating that systems or arrays of biomarkers may have far more potential than isolated single measurement biomarkers. For gene expression alteration/biomarkers, further application of systems biology approaches with pattern identification/informatics technology are likely to be fruitful. A rapidly developing technology used for complex pattern recognition is the electronic nose. Inspired by the ability of dogs to determine complex patterns of odors, current testing on the device has been done on classifying bacteria or fungi by detecting their odors (such as identifying women with Type II diabetes by urine odor—(Mohamed et al., 2002). It is possible to imagine that this technology might be useful in measuring volatile biomarkers from skin (e.g., those emitted by melanomas and detected by dogs) (Church and Williams, 2001).
Currently, NHANES limits its biomarker assessment to children old enough to tolerate the drawing of blood. Smaller children are subjected to fewer laboratory assessments due to the smaller sizes of their blood samples. Development of more sensitive laboratory techniques using noninvasive biological samples is needed. Biomarkers in exhaled breath, urine, and saliva may prove very useful for this age group. Current examples of the usefulness of these techniques include using breath carbon monoxide levels to predict neonatal jaundice (Smith et al., 1984) and urine toxicology for parental substance use. Similarly, the development of programs, such as the newborn blood screen, could be extended to meconium, cord blood, cord, and placenta, which now are typically discarded. While some measures of infection are currently taken (e.g., rubella, herpes), development of biomarkers for emerging infectious diseases such as West Nile virus, Lyme disease, or hantavirus warrant additional research. Prior research has shown a correlation between the formation of chemical modifications of DNA (DNA-adduct) formation and health effects, yet current measurement activities do not include these genotoxic changes.
MEASURING BEHAVIORAL INFLUENCES
Given the central role of children’s behavior on their health, whether by active participation in health promotion or disease intervention efforts or by behaviors that increase the risk for poor health, a systematic strategy for assessing and monitoring such health influences is critical. However, apart from youth, parent, or teacher reports and limited use of urine or hair tests to detect the use of illicit drugs, there are no concrete or fully objective tests for the presence of such behaviors. Moreover, infants and young children pose especially difficult mea-
surement challenges, because they do not have the capacity to report on their moods or cognitions. To fully understand the relationship between children’s behaviors and health across regions and populations, optimal measurement strategies in most cases require (1) reliance on multiple informants (single-informant data on youth behavior are usually incomplete and should be used with caution), including reliable observational data about the behaviors of infants and young children; (2) combining measures of behavior across informants and settings; (3) demonstration that the behaviors are not simply normal variations; and (4) demonstration that the behavior is in fact related to adverse health consequences. Multi-informant reports are not always needed, but the validity and adequacy of single-informant data should be scrutinized during the planning and execution of studies of children’s behavioral influences. Moreover, because children’s behavior is constantly changing, measures must be sufficiently sensitive to detect such changes, as well as able to detect relevant differences in the timing, duration, and intensity of behavior influences on health.
To what extent do studies take into account these factors? Data regarding child and youth risk behaviors are gathered routinely from a number of national surveys (see examples below), some consisting of one-time investigator-initiated (even longitudinal) projects, and others consisting of programmatic efforts to collect such information regularly. However, across the broad range of studies listed in Appendixes A and B, most do not meet the requirements outlined above.
As an example, in the National Health Interview Survey (NHIS), four questions from a single informant (parent-caretaker) are asked about children’s risk behaviors. Similar limitations are found in most other national surveys, with the notable exceptions of the Youth Risk Behavior Survey (YRBS) and the current NHANES study, which devote significant time to interviewing children in major behavioral areas related to adverse outcomes (e.g., substance use). In the current NHANES survey, multi-informant interviews are conducted using a well-validated instrument (the Diagnostic Interview Schedule for Children—Shaffer et al., 1996; Jensen et al., 1995). However, for the NHANES study, valid determinations and differences within and across any single geographic policy region (such as a city, county, or state) are not possible, given the sampling frame and sample sizes for this particular survey, rendering the study inadequate for adapting regional policies to variations in regional behavioral influences on health.
The YRBS, which attempts to track 10 high-risk youth behaviors, based on representative samples of entire classrooms within schools within states, has modest promise for policy and planning purposes, although the data are self-reports. While innovative, this methodology is largely dependent on the states’ own resources to implement the surveys and, in any given year of the survey, as many as 50 percent of states may not have valid or presumably generalizable data. Moreover, rates of specific high-risk behaviors are solely dependent on youths’ self-reports (using a pencil and paper survey measure administered in classroom group settings); are often much higher than those found in more in-depth, meth-
odologically rigorous surveys; and systematically miss school dropouts and youth not at school that day or in alternative placement settings. Publicly available data are reported every 2 years. Under conditions of complete implementation and ideal circumstances, representative classroom data could be obtained from states concerning these high-risk behaviors among high school students. This survey also assesses exercise and positive health behaviors. However, due to the modest levels of funding and lack of centralized control of assessment and sampling procedures, the survey relies on each state to conduct and follow-up the data collection procedures. This produces great unevenness in actual survey execution.
Several other recurring national surveys offer highly relevant information in very specific, targeted areas. For example, the Substance Abuse and Mental Health Services Administration’s National Household Survey on Drug Use and Health (NHSDUH) assesses information relevant to the prevalence, patterns, and consequences of drug and alcohol use among individuals age 12 and older, as well as family environment and parenting practices or perceptions that might influence substance use practices among youth. The Monitoring The Future study (funded by the National Institute on Drug Abuse, conducted by the Institute for Social Research at the University of Michigan) assesses substance use, other behaviors, attitudes, and values of 50,000 U.S. secondary school students, college students, and young adults; periodic follow-up questionnaires are mailed to a sample of each graduating class for several years after study entrance.
Another source of behavioral data on younger children is the National Labor Survey on Youth, which continues to follow the children of women in the original cohort. This survey includes the child Behavior Problems Index, but the early rounds of the survey primarily include children born to young mothers.
Data regarding youth behavior and its implications for health are sometimes available from investigator-initiated surveys. For example, the National Longitudinal Survey of Adolescent Health (ADD-Health) began in 1994–1995 with a sample of 7th- through 12th-grade schools. Interviews were attempted with the more than 100,000 students attending these schools, with three follow-up personal interviews conducted with a random one-fifth of these students. Health-related behaviors have been relatively well measured in each survey wave through questionnaire responses.
Absent from current efforts to measure children’s behavioral influences is consideration of their attitudes, beliefs, expectations, and cultural factors that shape decisions to seek health care or engage in health promotion or illness prevention activities. For example, “local” instruments have been developed by researchers exploring in a cross-sectional and prospective fashion the relative roles of parents’ and peers’ perceptions and risk involvement on risk and protective behaviors among adolescents (Stanton, Li, Galbraith et al., 2000; Cottrell, Li, Harris et al., 2003). As noted in Chapter 3, substantial evidence indicates that these factors exert major influences on youths’ health behaviors and subsequent health, whether related to their health behavior choices, tobacco/alcohol/
substance use, diet, or exercise or to their compliance with health care interventions. According to findings from the Global Burden of Disease study, these behavioral aspects of health are likely to exert even greater influence in coming decades, as behavioral and life-style-related health conditions (e.g., auto accident injuries, consequences of smoking, depression) become predominant in their overall impact on children’s health and illness (Murray and Lopez, 1996).
Another area with significant measurement gaps concerns infant and young children’s behavior. Some data are gathered on a recurring basis through the National Household Education Surveys Program to address a wide range of education-related child behaviors, including emerging literacy and numeracy in very young children. These surveys assess, from the perspective of the parent and teacher, aspects of school readiness, children’s experiences in early childhood programs, and school adjustment, but they do not generate state or local estimates of differences in behavioral influences on health outcomes. However, other data pertaining to developmental milestones for cognition, behavior or social development are not assessed. An important exception to this rule is the Early Childhood Longitudinal Study—Birth Cohort (ECLS-B), a large-scale (N = 12,500), nationally representative, and longitudinal study that follows a single cohort of children from birth to entry into 1st grade. Because of its longitudinal design, this study will enable researchers to examine children’s cognitive, social, behavioral, and emotional growth and to relate their growth and change to their experiences in early child care programs. While this study is likely to yield important findings concerning children’s behavioral development, it is time-limited and cannot be used for ongoing monitoring of behavioral influences of U.S. infants and young children. A similar study of the 1998 kindergarten cohort (ECLS-K) also contains rich data on some aspects of behavior in a large cohort over time.
Challenges in Measuring Behavioral Influences
There are many special challenges in assessing children’s behavioral, emotional, and cognitive influences on health because information may be highly stigmatizing, raise fears that the child will be “labeled,” or may concern illegal activity, such as criminal acts or substance abuse. It has been well established in behavioral research that large variations in observers’ reports exist (e.g., see Achenbach, McConaughy, and Howell, 1987; Jensen et al., 1999), sometimes because there are differences in how different persons perceive the same behavior (perhaps as a function of different ethnic or cultural backgrounds), and sometimes because different persons do not always witness the same behavior, since behavior may vary from setting to setting.
For all of these reasons, measurement of behavioral influences calls for obtaining multiple sources of information, ensuring that the measures of behavior do not rely on single items, and including measures of functional impairment
with measures of behavior, in order to establish whether the behaviors have clinical significance. Finally, careful attention to gender-related, age-specific, and culture-specific behaviors is essential. Many behaviors must also be assessed in a developmental context. For example, bed-wetting or separation fears at age 4 are normal, but they convey different significance at later years. Similarly, aggression in young children is quite different from such behavior in adolescents, in part because older youth have much greater physical capacity, learned knowledge, and access to other ways to deal with anger. Thus, similar constructs might need to be measured differently across the age spectrum to track the effect of a particular behavioral or emotional construct on later health outcomes.
Addressing Gaps in Measuring Behavioral Influences
Among the influences on children’s health, the salience of behavior to long-term health, especially regarding obesity, HIV/AIDS, sexually transmitted diseases, substance or alcohol use and addiction, motor vehicle accidents, teenage pregnancy, school dropout, and homicide and suicide, is generally accepted (Murray and Lopez, 1996).
In addition to stigma, which makes these areas difficult to address a priori, failure to be conceptually clear about which behavioral constructs are being measured also contributes to difficulties in measurement. Thus, one may assess some form of behavioral problem, but whether it is a measure of a risky behavior (but not ostensibly a sign of health or illness per se) or a measure of the presence or absence of mental health or illness is not always clear. Many surveys include a few behavioral items, but rarely are there clear conceptual linkages to whether the items are related to a health condition per se (mental health or illness) or only to influences on future health (e.g., a risky behavior that may predispose to future adverse health outcomes).
Some of this conceptual confusion may be designed explicitly to avoid the possibility of stigma or stigmatizing a population, especially in surveys conducted by federal agencies of disenfranchised groups that are already prone to stigmatization (e.g., studies of economically depressed groups). As a result, most studies that attempt to assess children’s behavior rely on assessments of single behaviors or overall functioning, without reference to the central health conditions that reflect most of the population-attributable risk for adverse outcomes and persisting disability. One illustration of this lack of conceptual clarity is the extent to which surveys may attempt to measure adolescent suicidal ideation—essentially a normative behavior in youth—but fail to consider in the measurement strategy the assessment of major depressive disorder, the single greatest risk factor for completed suicide (Shaffer and Craft, 1999).
Most existing surveys have not devoted sufficient methodological attention to distinguishing sufficiently between behavioral information gathered for diagnostic purposes (e.g., major depressive disorder) and information obtained for
purposes of assessing risky behaviors. This difficulty is not the sole problem of survey designers, but it may have to do with how the mental health, education, and medical fields conceptualize mental health or illness and risky behaviors. Many mental health disorders seem to merge with the day-to-day problems experienced by everyone. This results in the absence of clear, critical indicators for mental health and illness that have strong face validity and that are clearly linked to functional impairment and the need for treatment. This reflects a more general failure in behavioral health research.
Another assessment gap is the fact that, among the few studies that attempt to address the problems noted above, few are nationally representative (NHANES, NHIS, National Household Education Survey, and NHSDUH being notable exceptions). Instead, most are samples representative only of a particularly community or region, usually with time-limited funding sources as a part of an investigator-initiated research study. While some regional studies are longitudinal, nationally representative surveys tend to be ad hoc or one-time-only. There is no clear ongoing commitment or funding, or health-monitoring strategy with explicit ties to national policy. Furthermore, no data are currently available meeting these three criteria that can also be used to assess these constructs in policy-relevant localities, such as cities, counties, or states.
In addition to the general methodological inadequacies in assessment of key behavioral characteristics among children, such as failing to obtain behavioral data from multiple informants and failing to distinguish between behavioral risk factors and actual behavioral disorders, most available datasets have not linked the behavioral measures to other influences that may affect behavior, such as family and parenting variables, peer influences, educational functioning, other aspects of physical health, and neighborhood and school resources. A notable exception is the ECLS of the National Center for Educational Statistics.
PHYSICAL ENVIRONMENTS
Our discussion of measurement of influences in the physical environment focuses on chemical exposures and aspects of the built environment to illustrate measurement challenges related to measuring the physical environment. Similarly complex measurement challenges and in most cases a paucity of data exist related to noise and other exposures of concern; home, school, and work settings; and safe environments free of injury.
Chemical Exposures
Environmental pollutants are measured in media, such as water, air, some foods, and soil, as reviewed in two recent Environmental Protection Agency (EPA) reports (U.S. Environmental Protection Agency, 2000a, 2003). However, these measures do not always take into account children’s unique exposure pat-
terns and pathways of exposure. In addition, there are few measures of microenvironments in private homes, such as indoor air pollution or noise or indicators of noise. Radon is measured in individual houses, and ultraviolet B radiation (UV-B) is measured in some regions. However, how these measures compare with children’s actual exposures is unknown. There are few surveillance systems for monitoring children’s exposures, job descriptions, work (including agricultural) at home, or their work-related injuries and illnesses.
Challenges in Measuring Chemical Exposures
Not much is known about specific aspects of the physical environments in which children spend their time, nor are there methods to determine the highly exposed subpopulations of children. The methods generally used are to determine exposure chemical by chemical, without consideration of mixtures of exposures or cumulative effects of exposure. Methods to predict individual exposures accurately from environmental indicators are under development (e.g., U.S. Environmental Protection Agency, 2000, 2003). Measurement of occupational risks to children, especially those in unregulated settings, may conflict with home-owners rights. The Bureau of Labor Statistics of the U.S. Department of Labor and state departments of labor need to develop mechanisms for more efficient data collection of children’s occupations and health effects, as well as for better access to datasets that are potentially useful, such as work permit information issued by school boards.
Addressing Gaps in Measuring Chemical Exposures
The health effect of a physical agent to which children are exposed may be unknown. A recent analysis by the EPA discovered that 43 percent of high production volume (HPV) chemicals (the 2,800 or more chemicals released at greater than 1 million pounds per year) have no basic toxicity testing, and only 7 percent have a complete set of basic toxicity tests (U.S. Environmental Protection Agency, 1998; Goldman and Koduru, 2000). Many fewer have any developmental toxicity testing. These chemicals are not monitored in the environment, nor is biomonitoring available for most of them.
Less clear than HVP chemicals are the other chemicals in the environment to which children are exposed. How should the decisions be made about which to monitor? The CDC has come up with a strategy for adding additional chemicals to the NHANES survey, but this strategy has yet to be evaluated.3 It focuses on chemicals with known toxicity or that are relatively easy to assay, such as heavy metals.
The Built Environment
In the United States cities have evolved rapidly toward the pattern known as sprawl, with geographically dispersed metropolitan areas, segregated land uses, heavy reliance on automobiles as the dominant transportation mode, low connectivity, and high neighborhood fragmentation. A majority of children in the United States now grow up in the suburbs. This built environment pattern has major health implications in four areas: air quality, physical activity patterns, injuries related to motor vehicle use, and “sense of community” (Frumkin, 2003). However, in all four cases, knowledge is incomplete, both in terms of understanding and assessing current problems and in terms of designing solutions. Researchers have identified key questions, and active investigations are under way. For instance, using multilevel exposure ascertainment, investigators are able to jointly assess neighborhood-level characteristics, such as collective efficacy and variations in violence, and individual-level characteristics (Sampson, Raudenbush, and Earls, 1997).
To measure physical features of a neighborhood (e.g., the exposure), many parameters of sprawl have been identified (e.g., percentage of the population living in urbanized areas, residential density, accessibility of the street network, proximity of different land uses to each other, pedestrian oriented design) (Frumkin, 2003) and combined into indices. Often these measures are limited by the availability of data; for example, in the relatively complex index proposed by Galster et al. (2000), data were available for only 13 cities. Moreover, when data are available, they can sometimes be mapped only to relatively large geographic units, such as metropolitan areas or counties. Data on smaller units, such as the census tract (geographic areas encompassing 4,000 to 6,000 individuals, with boundaries drawn to approximate neighborhood areas) or even the block, provide more information on individual and family exposures but are more elusive.
In studies of children’s health, the preferred measures of “exposure” to sprawl are perhaps best defined by what health outcomes are of interest and what biological mechanisms are hypothesized. For example, in studying the association between sprawl and physical activity, one could measure the proportion of roadway miles with sidewalks, the acreage of parkland per capita in a defined area, the mileage of bike paths, the mean distance of homes to the nearest parks, or the mean trip distance from homes to elementary schools. Such data are available from a variety of sources, including U.S. census data, Department of Transportation road data, marketing databases, and metropolitan planning agency databases.
In addition, direct observation using standardized instruments—analogous to the questionnaires used in epidemiological research—may be applied to the built environment. Such instruments need to be validated prior to use. An example of such a measurement approach is the Built Environment Site Survey Checklist (Weich et al., 2001). Using this instrument, research staff make and
record observations about housing type, density, age, space around the buildings, proximity of trees, accessibility of recreational facilities, playgrounds, and gardens, and even signs of vandalism and graffiti. While it is labor-intensive to collect data in this manner, a range of variables can be studied, including many that have great a priori appeal in characterizing the quality of places.
Some studies have assessed exposure by surveying respondents about their perceptions of these conditions. For example, people can be asked to rate the “walkability” of their neighborhoods (Leyden, 2003), the safety of allowing their children to walk to school (Dellinger and Staunton, 2002), or other perceived features of the built environment. In one investigation conducted as part of the Alameda County Study in California, participants were asked to rate the seriousness of six potential neighborhood problems: crime, nighttime lighting, traffic, excessive noise, trash and litter, and access to public transportation (Balfour and Kaplan, 2002). Other areas of concern may relate to the availability of stores that sell tobacco, firearms, and liquor to youth. Such measures carry the problems of many questionnaires, such as variable responses among participants and response bias. Moreover, there may be an element of self-fulfilling prophecy: respondents who rate their neighborhoods as more walkable are likely to walk more, but this may reflect factors other than the physical design of the neighborhood.
To the extent that environmental factors affect people’s behavior, that behavior might be considered an early biological effect (see Figure 5-1). An important example is travel behavior—the number of trips per household each day, the mode of travel used, and the distance per trip. A leading source of such information is the National Personal Transportation Survey, renamed in 2001 the National Household Travel Survey.4 Other features of traffic safety and injuries related to the physical constructions of vehicles and roads are also available. Additional data are gathered in academic and governmental travel studies such as SMARTRAQ.5 Such information was traditionally collected through surveys, using either retrospective recall or diaries; new techniques, such as personal digital assistants with global positioning system capability, have improved the completeness and accuracy of travel data.
Of note, studies may be conducted that assess the association between an exposure and a biological effect in the sense discussed here. For example, one might hypothesize that certain neighborhood features, such as low density or automobile dependence, are negatively associated with children walking or biking to school. While not extending all the way to a health outcome such as obesity, this association would be an important part of understanding the health implications of the built environment.
|
4 |
Available at http://www.fhwa.dot.gov/policy/ohpi/nhts/. |
|
5 |
See www.smartraq.net. |
Challenges in Measuring the Built Environment
Assessment of physical neighborhood and the built environment is burdened by several problems. First, in Sampson’s (2001) words, “the tendency of research on child development has been to focus quickly and narrowly on poverty,” especially in high-poverty urban neighborhoods. Moreover, most of the research in this area conceptualizes the neighborhood only as a social construct, using metrics of residential stability, income, education, employment, family structure, and crime, while neglecting physical aspects of the built environment. Finally, most of this research focuses on adolescents, perhaps because they spend more time out of the home and are therefore more exposed to neighborhood factors. This produces large gaps in data collection on other aspects of the built environment and its effects on children’s health across the age span.
Addressing Gaps in Measuring the Built Environment
Further research and systematic assessment are necessary to ascertain how the built environment affects sense of community or social capital in ways that shape the development of younger children. In addition, to improve measurement of the built environment, standardized instruments need to be developed, validated, and implemented at geographic levels useful for local planning.
SOCIAL ENVIRONMENTS
As with our discussion of social influences themselves, we organize our measurement discussion into categories of family, community, culture, and discrimination.
Family Environment
The Current Population Survey and the Survey of Income and Program Participation are prime examples of high-quality surveys conducted by the Census Bureau that gather information about many of the components of family demography and process—in particular, family income, family composition, parental schooling, and occupation. These surveys typically contain very few data on children’s health. Surveys focused on children’s health and its influences often collect some data on the components of family socioeconomic status (SES), but these data are often too crude to serve most analytical purposes. For example, data on family income are sometimes gathered or recoded into such categories as poor, near-poor, or nonpoor, so that it is impossible to estimate social gradients in health at all levels of income.
Vital statistics data contain relatively little information on SES. Birth records contain educational level achieved by the mother but, starting in 1995, do not
provide data on the education level of the father. Death records contain data on the decedent’s occupation and, beginning only in 2003, educational level. No information regarding parental SES is gathered on death certificates, a serious omission in the case of child deaths.
Other than gross indications of economic status by receipt of public health insurance, clinical data almost never contain any measure of SES, whether about income, education, or occupation of parents. Studies using clinical data or vital statistics sometimes rely on proxy measures of SES obtained by linking addresses to census tract data and attributing to individuals the SES characteristics of their neighborhoods, for example, mean levels of income or of educational achievement in a census tract. Given the heterogeneous nature of families living in a given neighborhood, neighborhood-based measures of family SES contain considerable error (Geronimus, Bound, and Neidert, 1996; Demissie et al., 2000).
When data on neither income nor education are available, race and ethnicity are often used as proxy measures of social class, based on knowledge of the higher frequency of low income among black and other minority groups. The fallacies of doing so are illustrated in data showing the health disadvantage for low-income white people in Appalachia, which is home to predominantly white populations (Centers for Disease Control and Prevention, 1998b). Thus, using race and ethnicity as proxies for social class makes invisible the health problems of low-income white children. Saliently, the risk of dying is higher in low-income groups, even after taking into account health risk behaviors (Lantz et al., 1998).
The National Survey of Early Childhood Health (NSECH) includes detailed assessment of hours and activities spent by parents with children; breast-feeding practices; daily routines including the frequency of playing, singing, and reading to the child; number of children’s books in the household; disciplinary practices; parental perceptions of infant temperament; the role of parenting, and their perception of themselves as parents; and pediatric care (including an assessment from the parent’s point of view of the usefulness of their provider’s health prevention education efforts). The NSECH also assesses family income, medical insurance coverage and adequacy, child care and child care affordability, and receipt of nutritional benefits such as WIC and other low-income benefits.
The Child Well-Being and Welfare module used in two states assesses income, health care coverage, day care utilization and costs, employment, income and job stability, relocation information, reading in the household, and information regarding school and out-of-school extracurricular involvement of the child. Parents are also asked questions about their relationship with and feelings about the child. The National Survey of Children with Special Health Care Needs (NSCSHCN) collected data on children with a wide range of health conditions and included a few questions on the effect on the family, but virtually no data on family structure.
The National Child Abuse and Neglect Data System, a partnership between the U.S. Department of Health and Human Services and the states, collects an-
nual statistics on child maltreatment from state child protective services agencies. The goal is to increase understanding of the magnitude of the problem, the characteristics of those affected, and what type of services are being provided by state and local agencies. Given that the majority of abusers are parents, these data do concern family and family functioning, albeit for a special subsample.
Available surveys also provide family environment information well beyond the traditional demographic variables. For example, the Current Population Survey and especially the Survey of Income and Program Participation augment their efforts with occasional questionnaire supplements to gather limited information regarding health and health insurance coverage, child care, and various other family topics. The NHIS assesses demographics and income, as well as health care seeking for each household member, including children. The U.S. Department of Agriculture’s Quality of Continuing Survey of Food Intakes by Individual Survey assesses the adequacy of diet of children ages 2 to 9 years nationwide. Data regarding limited aspects of parenting, nurturing, day care/child care, and school readiness are collected periodically in other surveys.
Challenges in Measuring Family Influences
Decades of methodological research have produced at least rough consensus on how to measure family environment components in surveys. As to SES components, Entwisle and Astone (1994) provide recommendations regarding the measurement of education and occupation, while Hauser and Warren (1997) do the same for occupation and Duncan and Peterson (2001) make recommendations regarding the measurement of income, wealth, and employment. As to family process measures of parenting and the home learning environment, national surveys such the National Longitudinal Surveys of Youth and the Early Childhood Longitudinal Study, Kindergarten Class of 1998–99 provide consensus measurement methods. Thus, one key challenge regarding family environmental measurement in surveys is less how to do it than how much of it should be carried over into surveys focused on health.
With regard to SES, although most health-focused survey data collection provides measures of at least one of the components, clinical data almost never contain any such measures, and there continues to be dispute about the appropriateness of doing so. Ross et al. (2000) summarized the various ways of measuring SES. They argue for the importance of a theoretically based choice, depending on the health measure and the context in which analyses are done. Duncan and Magnuson (2002) argue that estimating the importance of any single component of SES requires measurement of all of them to guard against omitted-variable bias.
Primary challenges to SES measurement are (1) including at least some measure of SES in all data collections and (2) choosing measures that best reflect the theory about the relationship between social disadvantage and the particular
measures of health being assessed. Health-focused data collection providing a myriad of health measures should consider collecting information on all of the important components of SES, since it is possible to do so without devoting excessive amounts of interviewing time to it.
A second level of SES challenges is to appreciate and account for their dynamic nature. Family incomes are often highly volatile from one year to the next (Duncan, 1988), and education levels can increase well into adulthood (Magnuson and McGroder, 2002), while occupation and wealth typically change more slowly. Designers of health-focused longitudinal surveys should realize that it may be necessary to include SES-related questions in a number of interviewing waves.
It is more difficult to draw general conclusions about the challenges of measuring the diverse set of other family environmental influences we have considered. With regard to family structure, an important challenge is to gather needed detail on the relationships among the individuals living in the same household. Whether an adult male is the biological father or stepfather to the children is an important distinction for assessing risks to child well-being. By the same token, whether two unmarried adults of the opposite or even same sex are functioning as partners or merely roommates also appears consequential for child well-being. And yet many surveys fail to gather household composition data in a way that captures these distinctions.
Data collection efforts that aspire to understand family environmental influences on children’s health should consider including measures of parenting and the home learning and physical environments but, here again, the measures used should match the conceptual orientation of linkages between family process and health outcomes.
Addressing Gaps in Measuring Family Influences
Clinical records pose a special challenge in regard to the assessment of SES influences. Clinical facilities are reluctant to collect information on aspects of SES from patients, believing that this may be interpreted as an attempt to discriminate on the basis of such aspects in providing health care. However, most clinical facilities collect residential address data, if for no other purpose than bill collecting. When geocoded and matched to characteristics of area of residence related to social class, address information can be very useful for population or subpopulation analysis of the relationship between receipt of health services and socioeconomic characteristics (Krieger, 2000).
Methodological advances now enable researchers to estimate multilevel models of the various ecological levels of influence on health. These techniques were developed for use in the social sciences (Blalock, 1984; Di Priete and Forristal, 1994) and have increasingly been used to study the interacting influences on
health at both individual and environmental levels in adults, but there are few such studies of children in the United States.
Analysis of the association of SES with health measures would be facilitated by the longitudinal and simultaneous ascertainment of most or all of the important SES components—income, education, occupation, and wealth. Analysis of the effect of income (or wealth) should be mindful of the likely confounding of influences as well as of interactions between SES levels and other influences. For example, Hispanics have better health than the majority population, despite having worse health behaviors and lower average income and education (Hayes-Bautista, 2003; Morales et al., 2002).
Community Environment
Most broad-based neighborhood studies rely on data gathered in the decennial census. Every 10 years, the U.S. Census Bureau provides information that can be used to construct neighborhood-based measures, such as the fraction of individuals who are poor, the fraction of adults with a college degree, and the fraction of adult men without jobs. Such data are available for census tracts as well as larger geographically defined areas. Matching neighborhood-level census information to survey or administrative data requires only a valid street address. The administrative, academic, and commercial value of such matched data has led to the development of a number of efficient address-matching computer programs, as well as a healthy market providing matching and other geography-related commercial services, including geographic information systems. Although such techniques have been useful in managing and analyzing neighborhood data, they are often cumbersome to apply to national datasets.
All in all, apart from privacy and confidentiality issues surrounding the need to gather and store information about the exact addresses of individuals and families, the decennial censuses provide the geographic dimension of demographic and many economic risk factors.
The Census Bureau is developing the American Community Survey (ACS)—a “rolling census” that involves a continuous sample survey of the nation’s population. Two noteworthy advantages to such a design are much lower cost and timelier information. The survey is designed to provide geographically specific demographic and economic information more frequently than once a decade (the interval depends on the size of geographic area). However, the fate of the ACS was not certain during the committee’s deliberation, as it was not yet funded by the U.S. Congress.
The social organization of neighborhoods’ (values and interactions of neighbors) appears influential for children’s health (Sampson, Morenoff, and Gannon-Rowley, 2002), but measures of social organization are unlikely to make their way into the decennial census or ACS. Approaches for measuring social organization
include surveys and systematic social observation. The Project on Human Development in Chicago Neighborhoods (PHDCN)6 illustrates both approaches. To gather information on its sample of children in a randomly chosen set of Chicago’s neighborhoods, the project conducted a separate survey of a representative sample of adults residing in those neighborhoods. The questionnaire for this second survey included questions on social interactions among neighbors. Mounting an independent survey to gather these kinds of neighborhood level data on social organization would be expensive, although a parsimonious set of observations might be added to existing surveys (such as the NHIS) that require home visits. For example, similar to an approach to measurements of the built environment, a measure described as systematic social observation (Reiss, 1971; Sampson and Raudenbush, 1999) relies on trained observers to systematically record such indicators of social organization as broken windows, vandalism, and evidence of drug use in a well-defined geographic area. Data can be gathered either with direct recording or by systematically coding videotapes taken of the neighborhood areas (Raudenbush and Sampson, 1999). Systematic social observation methods are less expensive than surveys, but they gather different kinds of data about social organization.
Standardized measures of neighborhood institutions and facilities (e.g., parks, the quality of local schools, churches, bus or train service, youth activity centers) are not readily available from any centralized source. Some of these characteristics can be obtained from surveys of the children or parents who are reporting on health outcomes. However, such reports can often identify what families use, but not what is actually present in their neighborhoods. A study by Morland, Wing, Diex Rouz, and Poole (2002) demonstrated that supermarkets are nearly nonexistent in the poorest fifth of the neighborhoods studied.
Investigators have generally considered both childhood victimization (direct exposure) and witnessed violence (indirect exposure) when studying the prevalence and effect of community violence in relation to children’s health (Martinez and Richters, 1993; Smith and Martin, 1995). Although most investigators define victimization in a consistent manner (e.g., intentional acts initiated by another person to cause harm), there is much more variability in the definition of witnessed violence. Some authors have referred specifically to eyewitnessed violence, while others have included hearing violent events (e.g., gun shots and screams), and others have included witnessing lesser crimes (e.g., property damage and the viewing of violence on television and in the media). With increasing interest and attention paid to a broader conceptualization of children’s exposure to violence (including victimization and witnessed violence) investigators are tending to view children’s exposure to violence in terms of levels, rather than direct or indirect exposures (Buka et al., 2001).
Typically investigators have developed their own questionnaires, used a modified version of the National Institute of Mental Health’s Survey of Exposure to Community Violence (Martinez and Richters, 1993), or used a modified version of the instrument used for the National Crime Victimization Survey (Katz, Kling, and Liebman, 2001). Most measures tend to weight violent events equally in spite of the obvious differences in item content (e.g., seeing someone hit versus seeing someone shot). Finally, with a few notable exceptions (Cooley, Turner, and Beidel, 1995; Selner-O’Hagan et al., 1998), the psychometric characteristics of these instruments are largely unknown (Buka et al., 2001). The instruments lack uniformity in their methods of administration, definitions of violent events, and descriptions of where the violence occurs. Importantly, most instruments fail to separate the nature or effect of exposure by setting, despite the acknowledged importance of such distinctions (Selner-O’Hagan et al., 1998).
Data regarding peer interactions and their implications for health are available from several national surveys. From a methodological perspective, the most remarkable is the National Longitudinal Survey of Adolescent Health, described above under behavioral influences. In addition to extensive measures of health and risk behaviors, the questionnaire asked each student to name his or her five best male and female friends. The study’s design provides data on direct reports from youth, coupled with limited information from all best friends and extensive information from a random subset of best friends. Peer relations also are assessed in a variety of surveys conducted by the U.S. Department of Education, the National Center for Health Statistics, the Substance Abuse and Mental Health Services Administration, the U.S. Department of Labor, and in surveys such as Monitoring The Future.
Challenges in Measuring Community Influences
As with other influences, the task of securing unbiased estimates of neighborhood effects is fraught with methodological challenges (Manski, 1993; Duncan and Raudenbush, 2001a). One important problem arises from the fact that families are not randomly allocated to their residential neighborhoods, which may lead researchers to mistakenly attribute to a neighborhood effects that are really caused by unmeasured differences in the children’s families.
A second challenge is to isolate effects of very high concentrations of certain risks (e.g., poverty, crime) from more general influences of urban neighborhoods (e.g., traffic, noise). Representative population surveys typically draw relatively few families from high-poverty urban neighborhoods. Analysts using these surveys base estimates of neighborhood effects on differences among relatively advantaged, mostly white families and children. If neighborhood conditions matter more for disadvantaged than advantaged children, then studies of neighborhood effects based on broad population samples may miss an important part of the story.
One solution to interpreting the effect of this bias is to analyze what neighborhood they moved into. The Department of Housing and Urban Development is conducting precisely such a study. The Moving To Opportunity experiment randomly assigned housing project residents in five of the nation’s largest cities to one of three groups: (1) a group receiving housing subsidies to move into low-poverty neighborhoods; (2) a comparison group receiving conventional Section 8 housing assistance but not constrained in their locations; and (3) a second comparison group receiving no special assistance. Orr et al. (2003) detail program effects 4–7 years after families were randomly assigned to these three groups. The evaluation showed significant improvements in neighborhood conditions and adult mental health but mixed results for children, with mental health improving for girls but behavior problems increasing for boys. A 10-year follow-up is planned as well.
Assessing the effect of violence on children is also challenging. First, investigators must measure simultaneously multiple facets of community violence. Measures of violence in the home (domestic violence) and violence in different community contexts (in the home, near home, in school and near schools) must be quantified so that the independent contributions of each exposure can be assessed. Second, few measures are available that distinguish among different forms and severity of violence. The adverse health consequences of exposure to extreme and acute violence (e.g., kidnapping, mass shooting) are likely to affect children differently than chronic exposure to community violence. Third, given the wide range of age and developmental diversity in children exposed to violence, multiple measures taken from children, parents, and other primary caregivers are needed. Moreover, the degree to which young children can reliably report exposure is an important concern. Also, sole reliance on parental reports of child exposure to violence are likely to underestimate children’s actual exposures (Martinez and Richters, 1993; Taylor et al., 1994). And compounding these above-noted difficulties, research evidence suggests that it is difficult to determine the relative effects of different types of violence exposure, because study subjects reporting to have witnessed violent events are also likely to have directly experienced lesser types of violence (Buka, Stichick, Birdthistle, and Earls, 2001).
Addressing Gaps in Measuring Community Influences
The decennial census and, if fully implemented, the ACS provide abundant and fairly timely demographic and economic information on the nation’s neighborhoods, cities and towns, counties, and states. Indeed, the United States gathers and releases much more of this kind of information than most other developed countries. However, the census questionnaire lacks comprehensive measures of health and health risk behaviors, and the linking of these data to other information sources is somewhat difficult.
Measures of most other important aspects of the community context (social
organization, amenities such as parks and public transportation, and safety) as well as media exposure currently can be gathered from administrative sources or special surveys, but at considerable expense and often not consistently from one geographic unit to the next and, hence, they do not permit generalizable interpretations.
Although there are routine sources of information on youth perpetration of violence, none exists to monitor youth exposure to community violence. Routine population surveys are needed to identify regional and secular trends. Such efforts would provide the foundation for attempts to collect data and design important intervention and support programs for the most affected communities. For example, there is a paucity of data on children’s exposure to community violence in nonurban settings (Buka et al., 2001; Smith and Martin, 1995).
At present only a few longitudinal multilevel studies of children’s exposure to community violence exists. Longitudinal studies, such as the PHDCN (Earls and Buka, 1997), hold the promise of allowing for a more comprehensive evaluation of the complexities of the types of exposure to violence, the context of exposure, and the contribution of potential risk and protective factors in determining child risk.
In addition to the major lack of systematic data collection, several important methodological issues confront future studies of the effects of violence on youth. These include the need to (1) develop consistent definitions of community violence; (2) develop violence exposure measures of proven validity and reliability; (3) determine how best to measure exposure to community violence in young children, including comparisons of child versus parent report and assessment of levels of violence witnessed; and (4) evaluate effects of acute and chronic violence separately.
In addition, research in this area would be facilitated by allowances that distinguish consistently between different forms and severity of violence. More attention should be paid to evaluating the extent to which the effects of children’s exposure to community violence are mediated by family and community response to community violence; for example, the family conditions that reduce the likelihood and consequences of exposure to community violence. Similarly, future research can improve understanding of the role that community violence plays in family violence. At least one team of investigators has noted a strong positive relation between exposure to community violence and the incidence of family violence (Osofsky et al., 1993). This challenge is further complicated by the issues and limitations in confidentiality and mandated reporting regulations under such circumstances, especially when a child’s health is in danger and the perpetrator is one of the child’s caregivers.
Many surveys include one or a few questions assessing aspects of peer relationships throughout childhood. Lacking in most are robust measures of peer relationships with strong psychometric properties that provide a cohesive story across the developmental stages. Thus, there is a need for at least some surveys to
gather in-depth information about peer relations, which was last done for middle and high school students in the National Longitudinal Survey of Adolescent Health in the middle 1990s. As youth approach adolescence, peer group acceptance becomes of even greater importance and conformity to perceived norms assumes an important role in the adolescent’s life; surveys assessing health and well-being should include a greater focus on these domains. Numerous surveys document involvement in risk behaviors, but few assess these aspects in any depth, and most rely on secondhand reports of peers by parents or the youth themselves.
Cultural Influences
Current national and regional efforts to assess population health collect data from population subgroups with different cultural backgrounds. Although the role of culture has been invoked as a contributor to observed health disparities (e.g., Hayes-Bautista, 2003), surveys typically gather few data that would help assess how culture contributes to health disparities.
One problem is that population samples include too few members of important population subgroups. Techniques for oversampling such subgroups can be used to draw large enough samples to support reliable statistical inference, particularly when subgroup members live in close geographic proximity to one another.
Another problem in most current measurement activities is the use of pan-ethnic labels that obscures cultural differences among groups. Pan-ethnic classifications, such as Hispanic, black, and Asian, reflect a classification system that neglects national origins and reflects membership in minority groups in the United States only in relation to the white Caucasian frame of reference (Portes and Rumbaut, 2001). The use of these convenient group definitions obscures important differences between the national groups in terms of migration, original culture, and social and cultural capital, all of which can have important consequences for children’s health.
For example, using the Hispanic Health and Nutrition Examination Survey, (conducted in 1982–1984) that oversampled Mexican Americans, Cubans, and Puerto Ricans, investigators have shown very different rates of asthma, lead levels, and health care utilization (Mendoza, Takata, and Martorell, 1994). Similarly, Becerra and colleagues (1991) have shown differences among these groups in infant mortality and low birthweight, including data to support the finding that recent immigrant women from Mexico have the best birth outcomes among Hispanic subgroups, despite their relatively low SES and poor acculturation to the dominant culture. Additional research to improve understanding of this “immigrant paradox” is warranted.
Another problem is that racial and ethnic information has been gathered in different ways in different surveys. For example, national health surveys and the official decennial census and survey data are not comparable in their use of eth-
nic/racial labels and the definition of such labels. In some instances, for example, the African American and black labels can be used interchangeably, while in other cases the label black might include West Indians or Africans who don’t consider themselves to be African Americans. These distinctions are important. The Office of Management and Budget (OMB) provides useful standards for gathering such information in both administrative records and surveys. The standards capture country of origin for those reporting Hispanic ethnicity and allow respondents to select more than one race. The 2000 census allowed Hispanics to designate multiple races independent of their ethnicity for the first time in U.S. history. The option of selecting more than one race reflects increasing recognition of interracial marriages and unions and the rejection of the “one drop rule” as historically defined (a person was automatically considered black if any close or distant relative was black). This option is likely to be used by increasing proportions of the population.
Surveys such as the Current Population Survey (CPS) have adopted the OMB standard related to racial and ethnic data and provide a timely and reliable method for capturing data on immigration. The CPS asks for the birth countries of the respondent, the respondent’s father, and the respondent’s mother. This allows children to be identified by generation and country of origin of self and parents. Health and access to insurance vary substantially across both immigrant generation and ethnicity.
Acculturation level has also been associated with health outcomes (Hayes-Bautista, 2003). Questions related to language(s) spoken at home, how long a child and his or her parents have been in the United States if not native born, and whether born a citizen, all included in the census, can serve as proxies for acculturation. Questions related to language may be the most useful. Children who speak a language other than English at home often have parents with limited labor market opportunities, which affects their employment, job benefits, and access to public services.
Challenges in Measuring Cultural Influences
There are many challenges to measuring the effect of culture on health. One is the definition and operationalization of culture. Assessing the effect of culture on health and its interactive relation with other influences requires standard definitions and measures of cultural processes. As discussed in Chapter 3, culture can refer to values, perceptions, and interpretations as well as behaviors that constitute daily routines and responses to environmental challenges that reflect such cultural views. There is little consensus on what is important and measurable.
Aside from the lack of standard definitions and measures, differences in cultural background in this country are highly confounded with socioeconomic and minority status, making it difficult to isolate the effect of one from the other or their interactions. When this is done, in some instances, cultural differences
disappear when education is controlled for (Laosa, 1980; Solis et al., 1990), and sometimes they remain (Gutierrez, Sameroff, and Karrer, 1988; Harwood, 1992; Ogbu, 2003).
These findings support the stance of some investigators that health outcomes are a function of the compounding effects of many characteristics that are, in reality, difficult to isolate (Boykin and Toms, 1985; García Coll et al., 1996). It might be more efficient to measure and delineate their interactive effects over time than to try to isolate them. In this view, cultural differences are most important when they are compounded by oppression, poverty, and discrimination. Although some health outcomes are still adverse as a function of cultural background in high socioeconomic groups (Steele, 1997; Ogbu, 2003), the expectation would be that cultural differences in the context of relative oppression, poverty, and discrimination would need most attention from the standpoint of health policy and health care delivery.
In addition, cultural differences may also be very important when demographic variables (i.e., poverty, lack of English proficiency) predict negative health outcomes but these adverse outcomes are not observed (Hayes-Bautista, 2003; Fuligni, 1997; Portes and Rumbaut, 2001). Measuring how cultural processes lead to resilience in health outcomes is an area in which knowledge is particularly lacking.
Given how little is known about the way in which culture directly influences health, or the extent to which it is confounded with other influences (such as social class), a research agenda to develop validated and standardized measures is warranted.
Addressing Gaps in Measuring Cultural Influences
In order to make data compatible for aggregation and analysis, collection of data on cultural group membership should be systematized and standardized across all levels of local, regional, and national data collection. Following the most recent OMB guidelines might be the way to work toward standardization, with the recognition that categories change over time and need to be clearly defined to ensure comparability of data over time. Specifically, the OMB standard related to capturing data on ethnicity, country of origin for self-identified Hispanic populations, and multiple races should be used in all health data-gathering efforts at the local, regional, and national levels.
Beyond this information, to help understand the established relationship between generation and health outcomes, it would be very beneficial to identify children by immigrant generation using questions about birth country for children and their parents and, if born elsewhere, how long they have been in the country. Ideally, this information should be obtained regardless of whether the parent lives in the household. Similarly, given the relationship been acculturation and health outcomes for some populations, if an acculturation measure cannot be
used, questions related to languages spoken in the home should be incorporated in studies.
Work toward standardizing the assessment of cultural group membership should also be done with the recognition that such membership alone does not capture cultural processes. Ethnic identification, place of birth, recency and pattern of migration, and language proficiency and choice are only proxies for cultural processes. Adding these items to extant or planned surveys or to any intake or identifier data will provide information on factors that have been found to correlate with health habits, practices, and outcomes (Portes and Rumbaut, 2001), but will not address the underlying mechanisms.
For example, there is a growing and consistent literature that points out the existence of health disparities along ethnic, racial, and cultural lines; however, the processes that underlie these differences, including the likely confounding effect of social class, are hardly understood. In order to address this knowledge gap, it is necessary to oversample subpopulations that are important because of their current or projected demographic growth or their overrepresentation in high-risk or resilient groups. In addition, future efforts should engage in the measurement of actual practices and daily routines that reflect in part cultural adaptation to present demands (e.g., Gallimore, Weisner, Bernheimer, Guthrie, and Nihira, 1993; National Research Council, 1984; Rogoff, 1990; Weisner, 1997, 2002).
Furthermore, not all members of an ethnic/racial group will be similar in their adherence to particular cultural values and practices. The role of acculturation—the adoption or rejection of new ways of being as a function of contact with a different culture—has been identified as a very significant source of variability among members of the same cultural group. Members of the same group can differ in how assimilated, resistant, or bicultural they can be; yet most surveys fail to use available methods for ascertaining these differences. Several scales have been developed for certain populations and could be further developed as a standard way to measure acculturation for inclusion in local, regional, and national surveys.
It is important to promote the development of measures that are psychometrically valid and reliable across all cultural groups being measured. Standardization on one group or on a national representative sample does not guarantee cross-cultural validity and reliability. Measures must also be linguistically accessible and valid. Translations and back translations, although a standard way of translating measures, do not guarantee cultural equivalence (e.g., How does one translate “nervous breakdown,” or “feeling down,” or “eating regularly?”). Other methods should be used to ensure linguistic accessibility and psychometric validity and reliability (see for example, the dual focus approach, Erkut et al., 1999a).
In general, measures and ways of administration need to be culturally sensitive (e.g., what is considered private information may vary according to age, gender, and cultural background of the interviewer and the interviewee). This requires extensive pilot testing of all assessments across all groups under study
and in-depth training of survey personnel on administration methods that will lead to reliable and valid data across cultural groups.
Discrimination
Studies have shown disparities in treatment and outcome between minority-and majority-culture children after controlling for other social indicators, such as SES. Discrimination is sometimes mentioned as possibly having a causative role in these disparities, but its contribution has rarely been studied directly. There are many possible reasons for this, including a lack of understanding of the multiple mechanisms by which discrimination may affect health; a lack of an a priori conceptualizing of discrimination as a potential influence separate from other social stratification mechanisms, such as race, ethnicity, and socioeconomic status; and difficulty in operationalizing and measuring discrimination.
As noted in Chapter 3, there is a sparse but growing literature on the effect of discrimination and racism on health. Most of the studies concern adults. Not surprisingly, these studies use instruments and questionnaires that measure discrimination (and perceptions of discrimination) in largely adult contexts and as such are not directly applicable to children. Instruments are lacking that are explicitly developed to measure experiences and perceptions of discrimination in child-specific contexts, sensitive to the particular conceptual and measurement issues regarding children of different developmental ages and from different ethnic groups. Thus, a concerted effort to develop measures is warranted.
Questions specifically pertaining to discrimination should be validated and then included in research related to minority child health and development. One example is provided by Erkut, Alarcon, García Coll, and colleagues, who developed questions pertaining to discrimination for their studies of the physical and psychological health of Puerto Rican children and adolescents in the greater Boston area (Erkut, Alarcón, and García Coll et al., 1999b; Alarcón, 2000). These questions are good examples of how researchers need to take into account developmental age (e.g., the wording and complexity of the questions for the 1st to 3rd graders compared with young adolescents) when constructing appropriate questions, and how to incorporate age-appropriate contexts into the questions. These questions have not been psychometrically validated; although they may service as a basis for further testing, they have some limitations, as noted below.
Challenges in Measuring Discrimination
One of the major challenges in studying the effects of discrimination, prejudice, and racism on children’s health and development is finding ways of disaggregating the effects of this particular social stratification mechanism from other interrelated variables, such as social class, ethnicity, and minority status. These
variables need to be clearly defined and operationalized and then placed into models for the study of the determinants of children’s health. Once such model has been proposed for the study of developmental outcomes in minority children (García Coll et al., 1996); similar models need to be constructed for the study of sociocultural disparities in children’s health.
Another challenge is that the effects of discrimination on children’s health are likely to be interrelated, that is, discrimination suffered by the child, the parent, the family, as well as neighborhood level-discrimination (e.g., segregation, with its effects on housing stock, neighborhood safety, social capital, and even differential exposure to environmental pollutants) may affect children’s health. An integrative, ecological approach is needed, one that is able to measure and tease out the complex interactions among institutional and personal discrimination at multiple levels and their unique and cumulative effects on children’s health.
The measurement of discrimination directed to and perceived by children poses unique methodological challenges. A child’s perception and understanding of the causes of a negative social interaction will depend in large part on his or her age and developmental level. An understanding of child developmental theory is necessary in order to create instruments and measures that are valid for children at different ages and stages. Children (as well as adults) will sometimes not attribute a negative social encounter to racial discrimination. The challenge for the researcher is to find methods to delve beneath the surface to see if racial or ethnic discrimination may be part of the child’s explanatory model, but to do it in a way that is not leading. Methods used in the cognitive social sciences (card sorts, ratings, triadic comparisons, and sentence frame formats; see Weller and Romney, 1988) may be helpful.
Since the dimensions of discrimination will be different for different minority groups, another challenge is to create instruments that tap into the unique aspects of discrimination in each group but can also be used comparatively in studies of multiple groups. Perceived discrimination may be based on such factors as language or accent, skin color, food preferences, family or household structure, or customs. Salient factors for one group may not be the same as for another group. Creating measures that have salience within a particular group (which anthropologists call emic) while also allowing for intergroup comparisons (i.e., etic) is a methodological and measurement challenge.
Researchers also differ on whether racial discrimination is best measured by experimental or experiential methods. Each method has its own advantages and disadvantages. The experiential survey approach takes into account the real-life social contexts in which discrimination is experienced, drawing on actual instances of discrimination encountered or perceived by the respondent. Because of this nonabstract approach, experiential surveys may be more developmentally appropriate for younger children. One benefit of the experimental approach is
that setting and stimulus are controlled for. However, experimental techniques could lead to an underestimation of negative situations as being attributed to discrimination (see Szalacha et al., 2003).
Concerns and worries over potential discrimination, and not actual experiences of discrimination, may also have effects on the health and well-being of minority children. In the study of Puerto Rican children discussed above, 47 percent of the sample indicated that they worried about possible discrimination, and this discrimination anxiety was significantly related to low self-esteem (global self-worth) (Erkut et al., 2000). Studies regarding stereotype threat in black college students (Steele and Aronson, 1995) also reflect the consequences of perceptions and worries that minorities face on a regular basis and may be applicable to encounters with the health care system.
Discrimination based on race and ethnicity is an indisputable fact of life for many members of racial and ethnic minority groups. Its effects on physical and mental health in adults have been documented, and it is beginning to be studied in children. Perhaps the most crucial question that can be asked is what accounts for the variation among individuals in both the perceptions of discrimination and more importantly in its effects on health and well-being? Why do two individuals who are exposed to the same stressful stimulus have different responses to that stimulus? What are the social and psychological milieus that allow one child to thrive under such circumstances while another child becomes emotionally, educationally, or physically distressed? Focusing on the variability of responses to discrimination will help guard against viewing minority children’s health disparities from a purely deficit model. It will allow for an analysis of health disparities that balances risk with resilience, perhaps explaining differences as being a function of protective and adaptive responses to a particular social context (LeVine, 1977).
Addressing Gaps in Measuring Discrimination
Discrimination is a social stratification mechanism that warrants further consideration as one of many mediators of health outcomes in minority children, including the multiple levels and mechanisms through which discrimination may have either direct or indirect effects on their health. These include both institutional and personal discrimination and discrimination not only directed to the child but also directed at other family members and caregivers, as well as neighborhood-level processes. It also includes actual experiences of discrimination as well as worries about being discriminated against. Since the relationships among discrimination, other social position variables, and children’s health are complex, analytic strategies that are robust and can account for the effects of indirectly measured (latent) constructs should be used. Health researchers need to become familiar with techniques, such as structural equation modeling, which can be
used to determine the direct and indirect effects of latent constructs, such as discrimination, racism, self-esteem, locus of control, cultural identity, and racial socialization.
Instruments need to be developed that can adequately measure perceptions of racism and discrimination in different age groups (from young children to adults) and different ethnicities. Such instruments should be tested for conceptual and measurement equivalency across ethnic and age groups within each group. Ultimately, large-scale national surveys such as the Health Interview Survey, NHANES, and National Longitudinal Survey of Youth should incorporate measures of racism and discrimination, whether limited to a single question or full instruments. One approach may be to create instruments that have a core set of generic items or subscales that are appropriate to measure racial discrimination among all minority groups, as well as additional items or questions salient to each particular ethnic minority group to ensure emic validity. Such instruments could potentially be used in comparative studies of the effects of discrimination among different groups as well in studies addressing the specific dimensions of discrimination salient within each group.
The development of such instruments is likely to require the use of both qualitative and quantitative methodologies, from ethnography and focus groups to confirmatory factor analysis and Rasch modeling. The utilization of multidisciplinary research teams, which include representation from such fields as public health, clinical health research, pediatrics, child development, education, anthropology, sociology, and psychometrics, would help to create instruments that are theoretically driven, conceptually valid, and psychometrically sound. Although not specific to children or to health, a recent National Research Council report (2004) outlines a series of recommendations related to measurement of discrimination.
SERVICES
Evaluating the effect of services on children’s health is an important consideration both in terms of understanding the relative role of various influences on health and in relation to public policy decisions regarding services expenditures. In 2000, federal spending on children under age 18 was estimated to be $25 billion on Medicaid and the State Child Health Insurance Program (SCHIP) and approximately $123 billion on a wide range of other services, including food stamps, nutrition programs, social services, and other health and human development programs (http://www.cbo.gov/showdoc.cfm?index=2300&sequence=0). These federal expenditures do not include additional spending by state and local governments directed at promoting the health of children or improving their neighborhoods, or expenditures by their parents, families, or their parent’s employers. From the standpoint of federal, state, and local policy, decision makers need to
know whether expenditures on services result in improved children’s health. Measurement systems can monitor trends in services and provide information to help target research on the effectiveness of specific services.
Given that the data systems and approaches to quality measurement are more advanced for health services than other services, the majority of the discussion that follows focuses on health services. The federal government has developed several different data collection mechanisms to monitor the delivery of health services and, more recently, the costs of these services. Existing surveys monitor the patterns of health service use and disease, but they lack the detail required to assess the appropriateness and effectiveness of the care provided. Nor do they provide a more nuanced assessment of health care access based on need. For example, evidence from health services research indicates that certain aspects of the regular source of care are associated with better outcomes at lower cost, but existing surveys, for the most part, do not adequately obtain information on such aspects of care as continuous person-focused care over time, comprehensiveness of care, and coordination of services.
Most approaches to assessing the quality of care focus on individual physician-patient encounters rather than on quality of the system that delivers care. With the exception of selected health services delivery systems, no existing data sources deals with the adequacy of the place where people receive their regular source of care as measured against well-accepted criteria of primary care. It is estimated that as much as 30 percent of U.S. health care costs are a result of inappropriate interventions (Schuster, McGlynn, and Brook, 1998); despite this, most quality measures focus exclusively on underprovision of services rather than overprovision of services.
Several recently designed surveys, including the NSCSHCN, the National Survey of Children’s Health, and the NSECH attempt to improve measurement of the performance of health services, including disparities and gradients in health service provision. For example, the NSCSHCN included several measures about the acceptability of care for this subset of children, including whether or not the care provided to a family is “family-centered,” meets their expectations, and provides a high standard of interpersonal quality. It also includes components of services that allow the measurement of some aspects of the system, in terms of operationalizing whether or not the children have a medical home. The NSECH provided information about perceived accessibility, continuity, the appropriateness of the content of care, as well as the acceptability of the care to parents. The NSECH also collected information about parental childrearing behaviors and assessed missed opportunities to provide specific components of well-child care that parents expressed an interest in receiving. It also collected information about parents’ reported discipline practices, inquired into whether their regular provider had discussed discipline issues with them, and, if not, whether or not parents would have found such a discussion useful, thus providing a measure of unmet need for health services and missed opportunities to provide a service
perceived by parents as useful (Regaldo, Sareen, Inkelas, Wissow, and Halfon, 2004).
While improving the quality of health care for both adults and children is recognized as a national imperative, there has been relatively slow progress in developing quality of care measures for children’s health. The Institute of Medicine’s (IOM) report Crossing the Quality Chasm (Institute of Medicine, 2001a), adapting and modifying a model proposed by the Foundation for Accountability, suggested that the focus of services should be on staying healthy, getting better, living with illness, and coping with the end of life. While these represent appropriate foci for adult health services, they omit the important role of development in the context of children’s health. Moreover, coping with the end of life—an important issue for the small proportion of children who have life-threatening or terminal illnesses—is a relatively rare occurrence in childhood. The “staying healthy” rubric misses the importance of promoting optimal health and development. In addition, it is important to consider how health services delivered by both the personal medical care system and population health services perform and affect health outcomes in children. Crossing the Quality Chasm outlines several domains to measure the quality of services provided. These include medical services that are safe, effective, patient- and family-centered, timely, efficient, equitable, and coordinated.
The Foundation for Accountability, through its Child and Adolescent Health Measurement Initiative, has developed consumer surveys that can be administered to parents by health plans, Medicaid programs, and medical practices in order to assess the content and quality of the services that are being provided. The Young Adult Health Care Survey assesses perceptions of the content and quality of care for adolescents (Bethell, Klein, and Peck, 2001a); the Children with Special Health Care Needs Module for the Consumer Assessment of Health Plans Survey assesses the quality of services provided to children with chronic conditions (http://www.faact.org/faact/site/CAHMI/CAHMI/home?action=ViewGuidedTourSection&id=80); and the Promoting Healthy Development Survey assesses the content and quality of developmental services to children from birth to age 3 (Bethell, Peck, and Schor, 2001b; Bethell, Reuland, Halfon, and Schor, 2004). Although these mailed surveys provide information on quality as perceived by individual responding consumers, they are used primarily in populations already receiving health services in certain types of facilities rather than in the population in general. Thus, they systematically exclude the populations that are most deprived of needed services.
At present the major system that is used to measure the quality of personal health care provided by large health care organizations in the United States is the Health Employer Data Information System (HEDIS), operated by the National Committee on Quality Assurance (NCQA). HEDIS also assesses enrollees in health plans and contains very few indicators of the quality of children’s health care or measures of the quality of care they receive. For example, the only mea-
sures of well-child care—which constitutes a major aspect of primary health care services for children—are the number of doctor visits children received and whether or not they have been immunized or screened for previously undetected health conditions (e.g., anemia) These are arguably important and necessary measures, but clearly not sufficient to determine if children have had their developmental risks assessed in a timely or appropriate fashion, whether their behavioral and emotional problems have been recognized and dealt with, or whether they have been followed to ensure resolution or improvement of their problems. They also assess only children in participating insurance plans (Kuhlthau, Walker et al., 1998; Perrin, Kuhlthau et al., 1997; Newacheck, Stein et al., 1996). Moreover, HEDIS has no comparable data collection on those without insurance, the under-insured, or those not enrolled in a health services organization that provides data to NCQA.
There has been progress over the last several years in measuring the quality of health services provided to children and the potential effect of different kinds of health services on their health. However, such measurements are not being collected as part of routine monitoring of quality and are not being collected at all on the most deprived segments of the population. Moreover, since the data collection mechanisms (even within HEDIS) are voluntary, some health maintenance organizations have decided not to monitor the health of children. Here, as in many other instances, the efforts are directed principally at the health of adults. Moreover, they are family-based and not a community of population-based assessments and give no clues either about averages or distributions in the population.
Challenges in Measuring Services
Although the United States has relatively good statistics on overall access to and use of health services, primarily through its national surveys, the data are notably inadequate for assessing access to and use of different levels of health services (including primary care and specialty care) and the effectiveness of those services. In current data, the concept of “access” is often confused with use of services, despite the fact that access facilitates care but does not reflect services sought or provided. Health surveys usually address the issue of access to and use of “a regular source of care,” which may or may not be a primary care source. Modifications of survey questions sometimes inquire whether the source is the same for both preventive and illness care (with increased likelihood that the source is primary care if both are the same), but there is still no direct data on the extent and distribution of primary care at any geographic level in the United States or on the actual services provided.
Although some effort has been directed at improving measurement of personal health care services, far less has focused on assessing the performance of the
community health infrastructure on which many parents rely (Fawcett, Pain, Francisco, and Vliet, 1993). The community service system includes a range of child development, behavioral, and mental health services and centers; programs to address the needs of children with learning disabilities and behavioral problems; health education programs provided through public health departments; educational services; nutritional services; and other programs provided by public health systems and communities (Halfon, Inkelas, Wood, and Schuster, 2001). At present, there is no systematic measurement of the effectiveness and efficiency of these community service systems or their capacity to meet the service needs of their communities and provide services acceptable to parents.
There are also major gaps in understanding the delivery of health services and the potential effect of these services on special populations. For example, although the number of children in foster care has increased dramatically over the past two decades and the high prevalence of mental health conditions in this population is solidly documented, there has been little focus on the accessibility and appropriateness of health services provided to children in foster care. It is not known whether health care providers and local health care systems are capable of providing mental health and developmental services to this high-risk group of children, the degree of continuity in the services provided, or whether the services are actually effective in addressing each child’s particular needs (Rubin et al., 2004; Simms, Dubowitz, and Szilagyi, 2000; Horwitz, Simms, and Farrington, 1994; Takayama, Bergman, and Connell, 1994; Halfon, Berkowitz, and Klee, 1992; Halfon and Klee, 1987). Such measures would not only be helpful in specifying the burden of illness in this high-risk group of children, but in better understanding whether local and state authorities responsible for ensuring the well-being of children in foster care are actually meeting their legal and morel responsibilities.
A similar case can be made for a number of other special populations. For example, while the Report of the Surgeon General’s Conference on Children’s Mental Health (U.S. Public Health Service, 2000) documented the increase in mental health needs and the widening gaps in unmet needs for services, there is very little information at the federal, state, or local level on the affect of preventive, treatment, or rehabilitation services on children with mental health problems or on monitoring of the extent to which gaps are being closed.
It is also important to consider how services may be arranged and delivered based on population health needs. In keeping with the concept of health that was adopted for this report, we consider the services not only to prevent and treat diseases, conditions, and impairments, but also to prevent the effect of adverse influences and promote optimal health. The latter factors are especially important for children with serious ongoing health conditions. While only a minority of children have such conditions, they use a disproportionate amount of personal health care services and their medical expenses account for a substantial portion of health care expenditures (Ireys and Perry, 1999).
Addressing Gaps in Measuring Services
Better questions about access to and use of services are required to obtain more adequate information about types of care needed and received. This requires an understanding of the relative importance of primary care and specialty care, to improve the quality of decisions on personnel training, resource distribution, and financing and organization of services.
A continuing imperative is to improve methods and measures for all services. Clinical measures of quality that are based on evidence from various types of research studies are developing at a relatively rapid pace, but efforts to develop measures of health services performance are not. Recent research has demonstrated that the quality of systems for delivering primary care for children can be assessed using criteria that are widely accepted as constituting good primary care. These are based on characteristics including accessibility for first-contact care, person-focused care over time, comprehensiveness of care, and coordination of care when people have to be seen elsewhere (Cassady et al., 2000; Starfield et al., 1998). However, there has been little movement to incorporate primary care measures into existing data collection efforts. Moreover, there has been no effort to develop ways of conceptualizing and assessing the adequacy of specialty care services. Recent research is showing the variable nature of need for specialty services, including the need for advice and guidance, confirmation of initial opinion, and need for definitive interventions that can be provided only at the specialty level (Forrest, Glade, Baker, Bocian, Kang, and Starfield, 1999; Forrest, Rebok, Riley, Starfield, Green, Robertson, and Tambor, 2001) Both national and international data indicate great variability in referral rates from primary care to specialists and from one cultural context to another (Forrest, Majeed, Weiner, Carroll, and Bindman, 2002a). Although much of this variability can be attributed to age and case-mix differences, considerable variability remains even after controlling for these characteristics. Moreover, there is consistent and robust evidence of gaps in coordination of care, even though better coordination has been demonstrated to improve at least some aspects of the results of care (Forrest, Glade, Baker, von Schrader, and Starfield, 2000). Thus, for policy-related measures to be available and adequate, policy makers need to encourage and support efforts to develop criteria for referral and then to develop evidence-based guidelines to monitor rates of referral in different areas and in different population subgroups to ensure the most effective and equitable use of health services personnel and resources.
To capture the performance of both the personal health care system and the public health system, allow systematic assessment across the range of different performance attributes, and consider disparities in the distribution of services across various populations, an integrated measurement system should adopt a broad set of performance categories. As illustrated in Table 5-2, these categories include the effectiveness, efficiency, availability, appropriateness, capability, safety,
continuity, acceptability, coordination, and equity of services. Such an approach would build on work in other countries, for example Australia, where broader measures are used to assess population effects as well as individual effects.
The table suggests how each attribute might be operationalized using a specific health service—developmental assessments—as an example. Although data would come from health service encounters and parents’ perception regarding services, the committee has not laid out the specific data collection necessary. These same attributes and a similar kind of matrix could be constructed to assess the performance of other services, including other health care services, such as prenatal care, primary services to children, and specialty services.
A growing body of scientific evidence highlights the importance of the early years and experiences, developmental supports, and services that children receive. National and local research studies have highlighted gaps in the availability and quality of existing early childhood health services (Bethell, Peck, and Schor, 2001b; Bethell, Reuland, Halfon, and Schor, 2004). The federal Maternal and Child Health Bureau (MCHB) has launched a State Early Childhood Comprehensive Systems Initiative. Through this initiative, specific states are starting to improve the availability of health, early intervention, education, and family support services. There is very little information on the performance of these emerging early childhood service delivery systems and their effect on children’s health.
Measurement of the effect of services on children also plays an important role in the context of other influences, especially when identifying the most effective and efficient intervention points along the pathway to health. Depending on the performance of a service, it may act to improve or modify health and reduce disparities that are due to social and economic differences or to environmental exposures. Understanding the potential effect of a service on populations requires understanding the variation in the performance of the service (e.g., effectiveness, efficiency, availability, and appropriateness) across populations, and the impact on variation in health. Performance is affected by factors intrinsic to the services delivery system and the context in which they operate. It is important to understand how its performance is affected by factors intrinsic to the service delivery system, geographic variations in the delivery of services, and a range of other potentially interacting factors. Accurate measurement of services and evaluation of their effect on children is important in order to partition the effects of the availability and delivery of services and their unique contribution to health outcomes in relation to the other influences on health.
POLICY
There are relatively few efforts to assess the effect of policy changes on health, particularly children’s health. In rare cases (e.g., welfare reform, residential mobility programs, health insurance), random assignment evaluation studies have been mounted. Occasionally, rigorous longitudinal designs have been imple-
TABLE 5-2 An Integrated Service System Performance Approach (Population-Level Developmental Assessment Examplea)
mented to assess the effect of specific policies. For the most part, laws are passed and regulations written without specification of the aspects of health that are likely to be affected, the mechanisms by which that is likely to occur, or funding for rigorous evaluations. As a general rule, evaluations of the effect of new policies on children’s health, including not only health policies, but also most environmental, education, welfare, and other social policy, come from academic research studies conducted after the policy is implemented.
The kinds of data systems that are the focus of the committee’s report can be used to provide a limited assessment of certain policies. In general, however, there is little activity in the United States to measure the effect of policies on children’s health. The United Kingdom, Canada, and Australia have gone several steps further by developing approaches that attempt to assess policy effects more systematically and comprehensively.
Data collection by agencies such as the National Center for Health Statistics and ongoing surveys by the MCHB and the Agency for Healthcare Research and
|
Measurement Strategies |
Example Measures |
|
Providers are using appropriate screening/ surveillance measures to detect problems |
Rates of children receiving indicated assessments with appropriate instruments |
|
Estimating costs of interventions |
Average expenditure per child identified |
|
Parents report services are available and they can have problem assessed |
Rates of children actually reaching indicated services |
|
Rates of services based on American Academy of Pediatrics guidelines |
Proportion of children appropriately identified |
|
1. Routine periodic survey of provider about knowledge, skill, and tracking needs |
1. Self-assessment of skill to conduct appropriate risk assessment |
|
2. Community health service—asset mapping of developmental services in community |
2. Adequate referral services |
|
Monitoring of avoidance of unsafe or unwarranted interventions |
Rates of initiation of inappropriate modes of therapy |
|
Same provider/practice conducting assessment |
Rates of children with regular person conducting assessment |
|
Assess parent satisfaction with assessment and its results |
Satisfaction with care by ethnicity, income, and practice type |
|
Spectrum of care provided without conflict in management strategies (e.g., drug |
Rates of conflicting advice or incompatible advice and/or management incompatibilities) |
|
Population-based monitoring of all aspects of health system performance |
No differences in access to or receipt of individual services |
Quality have unexplored potential for assessing the effects of policy changes on children’s health outcomes. For example, state trends in health insurance coverage using the Census Bureau’s CPS could be expanded to assess the effect of Medicaid or SCHIP policy changes on enrollment. Available national surveys such as the NHIS and the Medical Expenditure Panel Surveys could potentially provide insight into effects on access and utilization. They do not provide the state-level estimates necessary to monitor such programs as Medicaid and SCHIP, which are under state jurisdiction. National data systems provide very few data to assess whether policy changes designed to affect enrollment, access, or utilization of health care services actually result in changes in children’s health outcomes. The best attempts that have been made to examine the effect of changes in Medicaid on children’s health have been done using very long time frames and very gross and narrow measures of health outcomes, such as infant mortality (Currie and Gruber, 1996b).
Many health and other social policies are focused on reducing disparities in
access, utilization, and health outcomes based on such social factors as differences in income, race, ethnicity, and gender. Even when relatively good data can be collected on the outcome of interest—such as infant mortality—and overall trends in that outcome accurately measured, existing data systems do not include sufficient other variables to test what accounts for the observed trends. Moreover, existing data also may not be able to differentiate between overall and subgroup trends. For instance, even though infant mortality rates have decreased for all ethnic and racial groups, disparities between whites and blacks have actually increased. This indicates that the influence on the absolute trends is likely to be different from the influence on the disparities trend (Wise, 2003). Because one of the two goals of Healthy People 2010 is to eliminate disparities, it is important to develop data systems that can measure the effect of policies on health outcome disparities.
A success story in assessing the effect of a major health policy is the national Back to Sleep campaign (Wise, 2003). Because the outcome of interest is infant mortality and because there is a specific long-standing data collection system for this outcome, it has been possible to monitor the effect on sudden infant death syndrome (SIDS) specifically from the time that this national Back to Sleep campaign was introduced (American Academy of Pediatrics Task Force on Infant Position and SIDS, 1992; Pollack and Frohna, 2002; Lesko, Corwin, Vezina, Hunt, Mandel et al., 1998). Using infant mortality data, which contain some information on social class, it was shown that the Back to Sleep educational initiative dramatically reduced mortality rates due to SIDS, but also increased social disparities (Wise, 2003). Research studies were required to demonstrate that the effect of this new information and educational program has a bigger uptake and adoption by wealthier and more educated families. This was an important source of information for national, state, and local policy makers and programs interested in making midcourse corrections in their Back to Sleep campaign.
Measurement of the effect of policies related to the physical environment can be done at several different levels, including the monitoring of air, water and food quality, biomonitoring, and health effects. However, for environmental policy changes, the use of multiple indicators, as shown in Figure 5-1, allows rapid assessment of changes in influences by measuring environmental indices and biomarkers of exposure. These can then be correlated over time with changes in biomarkers of early and late effects, and finally with indicators of health. If a “significant risk” rather than an “actual harm” standard prevails in environmental policy (as it did for leaded gasoline), then biomarkers of exposure, while an indirect measure of children’s health, could be used to document significant risk. The presence of an environmental influence for which there is evidence of likely harm, as measured using biomarkers, can then be used to guide environmental policy decisions.
While Healthy People 2010 provides a possible framework for evaluating the effect of some influences on health, including policy changes, its structure does
not permit examination of changes (improvements or decrements) in children’s health from a dynamic perspective, as conceptualized in this report. Healthy People 2010 provides a large number of indicators that reflect particular aspects of health—for example, behaviors influencing health, mental health, injuries, and vaccination status—but it does not offer a model for assessing the interaction or accumulation of these indicators in children or groups of children. There has been little work on how indicators of health can be combined to form a composite of health at the individual or population level or to profile health and changes in health at the population level across the group of indicators. Similarly, developmental concepts (e.g., rates of change in health potential over time) are not incorporated in the 2010 goals or objectives. The effects of policy changes cannot be adequately assessed without tracking the way these changes and their consequences affect children’s developmental trajectories.
A number of other countries are ahead of the United States in monitoring both health overall and children’s health in particular. In England, Canada, and Australia, major efforts have been undertaken to monitor the health of children over time. Although health was conceptualized in conventional ways using such indicators as mortality and morbidity, rather than in a dynamic manner, a recent effort carried out in the Canadian province of Manitoba (Manitoba Centre for Health Policy, 2002) provides lessons for future U.S. efforts. Data were organized by regions of the province, with each region characterized by an overall measure of health—premature mortality—and the areas ranked from high to low. These rankings were similar to the areas’ ranking by socioeconomic status measures, reflecting worse health in more socially deprived areas. Areas were also ranked on the basis of mortality rates, adolescent reproductive health, acute and chronic conditions, and injury rates and these rankings were compared against the overall rankings. In this way, areas that performed better or worse than expected given their overall health status (i.e., premature mortality) were identified, making it possible to link particular policies (including those relating to health services) in different areas to level of performance on various health indicators. This is an important example of using ongoing data collection for monitoring children’s health. It represents public commitment to children and demonstrates the feasibility of implementing such an effort on a large scale.
In Vancouver, British Columbia, Canada, a major initiative has been launched to measure and link measurement of children’s health, development, and educational achievement for all school-age children to all existing programs and policies that affect these outcomes. Through the nationally sponsored Canadian Human Early Learning Partnership, this pilot project in Vancouver has mapped differences in children’s health and social outcomes at the neighborhood level and related those differences to the availability and delivery of different health education and social service programs (Hertzman, McLean, Kohen et al., 2002). While representing a step toward a more extensive, ongoing, and integrated data system to measure and monitor the longitudinal health and edu-
cational trajectories of children, this initial effort aggregates health, human services, and neighborhood data and links them at the level of the individual child and neighborhood. The framework used in Vancouver to collect and report data on children provides an opportunity to monitor continuously the effects of a range of policy changes.7
Challenges in Measuring Policy
Measuring the effect of policies on children poses extraordinary challenges, given the many other influences that concurrently affect children’s lives. Few attempts have been successfully mounted in this regard, particularly in areas in which the policy is not explicitly targeted toward children. As discussed previously, use of ongoing data collection for this purpose is exceptionally rare, but are noteworthy for the quality and effect of the information they provide.
One of the major challenges has to do with the frequently changing nature of the policy environment. Policies put in place during one administration may be accompanied by attempts to evaluate its effect, only to have that program changed or eliminated by the next administration.
The most convincing studies of policy effects involve random assignment to an experimental and control group. This is not only expensive and at times difficult to implement, but it can also be difficult to justify ethically, especially when a given policy is enacted with the purpose of benefiting children. Nonetheless, without such studies, the best intentions of policy makers can have untoward effects.
Promising alternative strategies rely on the natural experiments provided by changes in national or state policies over time (e.g., Currie and Gruber, 1996a) and ongoing data collection. In this case, sharp policy changes from one administration to the next or from one state to another aid evaluators, since they can then look for health care and health changes surrounding the policy changes. These evaluation studies require consistent and representative measurement of children’s health and other demographic as well as policy conditions before and after the changes of interest. Studies based on trends in state-specific policies benefit greatly from consistent information across states and time regarding exactly what state policies have been implemented.
Assessments of policy effects—indeed, the design of policies themselves—are limited by conceptualizations of what constitutes health for children. Current policy perspectives continue to focus largely on diseases and illnesses and health services relevant to those diagnoses rather than on facilitating healthy development. To embrace a more dynamic view of children’s health, policy approaches need to consider health in a developmental context, focusing on facilitating well-
|
7 |
For additional information, see http://www.earlylearning.ubc.ca/CHILD/. |
ness and health potential. This broader conceptualization will require consideration of not only biological factors, but also the range of behavioral, family, neighborhood, community, and system influences on children’s health. A good example is the Sampson, Raudenbush, and Earls (1997) analysis of the importance of a community’s “collective efficacy,” discussed in Chapter 3. Understanding the factors that enhance collective efficacy would allow a community to develop policies intended to improve it, thereby improving the healthy development of its children.
Evidence about the importance of particular influences on health usually comes from studies of the relative risk of particular influences on a specific health outcome. The information provides a numerical estimate of the extent to which exposure to an influence increases the likelihood that a particular health outcome will occur, compared with the situation when the influence is not present. Clinical decision makers usually rely heavily on such evidence to justify interventions to reduce exposure to such influences in individuals.
In contrast, policy makers concerned with population health are more appropriately interested in attributable risk, that is, the extent to which different influences contribute to health outcomes. This is important for making policy decisions about which influences are most likely to improve health outcomes in the population. Such evaluations have much more potential to contribute to rational decisions about the most effective strategies to improve health. The challenge for such evaluations, however, is to include multiple types of influences as well as their interactions, in order to avoid attributing more benefit to certain types than to others. For example, McGinnis and Foege (1993) reviewed studies of the effect of certain behaviors on subsequent death and concluded that the combined behaviors accounted for 50 percent of deaths. The study was relatively unusual in examining attributable risk and an important model for needed studies, although it did not include a full range of influences. Moreover, it did not assess the interactions among the various types of influences, thus raising the likely possibility that behavioral factors were a result of, confounded by, or interacted with other types of influences that were not studied. Their report, for example, explicitly recognized the importance of appropriate health services (in the form of primary care) and socioeconomic characteristics, but it did not consider the effect of these services on the prevalence of the behaviors.
Where there is evidence that certain exposures are likely to cause ill effects, the wise course of action is to avoid such exposures, especially for children. Ill effects experienced during childhood alter future health. Policies that limit the release of noxious chemicals or other agents and the building of safe schools, houses, roadways, and cities can be expected to maximize the potential for good health, both of children and the adults they become.
Addressing Challenges in Measuring Policy
Monitoring policy effects on child health has not been a national priority. While existing laws require that environmental impact statements be developed when new roads, bridges, or dams are built, there is no such requirement to monitor the effect of labor, health, housing, energy, or transportation policies on children’s health. Yet as noted earlier, such policies can exert important yet unintended and unanticipated effects on children’s health, sometimes positive and sometimes negative. Given strong evidence that children’s health sets the stage for life-long health, assessing the effects of policy on children’s health should be given much more attention.
Existing ongoing data systems have several limitations as a tool for assessing policy effects, including their limited focus on particular diseases, the relative lack of longitudinal data, and the inability to link data across systems. Given the latitude afforded to states to implement policy, there is also a need for better tracking of state-specific policy implementation from one year to the next. Approaches being undertaken in Canada, England, and Australia provide valuable models for the United States. These models should be considered as new approaches to measuring children’s health are developed.
CONCLUSION
Additional well-designed research and evaluation that address the challenges articulated throughout this chapter are needed to fully understand the range of influences and the interactions between them. The conceptual basis of many studies of children’s health would be improved by the simultaneous study of at least one factor from each important category of influences known to be associated with health—an exception is the assessment of social class. In this way, studies can avoid the most egregious biases from failing to include variables that influence health and that interact in powerful ways with variables that have been included. A prototype of such a study is that of Lantz et al. (1998), which included both behavioral as well as social factors in the analysis of a national dataset. This was a study of adults; similar studies are warranted for children.
No single survey collects data on all influences on children’s health in a comprehensive manner; it would be both financially and methodologically onerous to do so. Ensuring that the portfolio of surveys collects at least some data on multiple salient influences and improving the comprehensiveness of individual surveys drawing on the content of existing surveys should be priorities as research continues to elucidate the dynamism of health and its influences. Surveys focused on child outcomes other than health would profit from paying more attention to health outcomes and influences. For example, education-focused datasets often provide rich information on the child’s readiness for literacy, family access to resources, and school quality but lack data on the child’s biomedical markers and
family health care seeking and health care access. Similarly, surveys focused on health outcomes have comparatively little information on such influences as family and communities variables.
Over time, a comprehensive continuous measurement system should be informed and evolve based on knowledge gained from continued research and expanded data collection in existing surveys.
















































