
Key Messages Identified by Individual Speakers
- Effective risk communication can help people make informed decisions by providing structured ways to understand the uncertainties inherent in the choices with which they are presented.
- FDA press releases are often the source of primary information for the media and can be a tool for conveying benefit, harm, and uncertainty information to the public.
- Implementing standard procedures for developing and communicating regulatory decisions could improve the accuracy and impact of risk communication strategies.
- Public information at the time of a drug’s approval can be improved by clearly conveying benefits, harms, and uncertainties and concisely highlighting what is known, what is still being studied, and what is unknown.
- FDA uses a number of tools to communicate benefits, risks, and uncertainties to a variety of audiences.
Treating uncertainty in a structured manner can produce better and more useful science. Baruch Fischhoff, Carnegie Mellon University, explained that better science results from disciplined reflection on the uncertainties inherent in evidence, and useful science is the result of
taking the needs of the decision maker into account. Crafting messages to communicate the outcomes of science, and the inherent uncertainties, presents a powerful opportunity to inform and improve the decisions made by individuals. A number of workshop participants indicated that communicating uncertainty is at the heart of many of the issues and challenges associated with benefit–risk assessments.
OVERVIEW OF RISK COMMUNICATION1
The intent of effective risk communication is to help people make informed decisions; it does so by providing orderly, structured ways to understand the uncertainties inherent in their choices, explained Fischhoff. To make those informed choices, individuals need to understand both the facts and their own values: What positive and negative outcomes might follow each possible choice? Which set of possible outcomes offers the most acceptable trade-offs?
Individuals do not always realize that both facts and values can involve uncertainty, said Fischhoff. As an example of uncertainty about facts, for reasons that are unknown, a drug might produce the expected outcome for one person and not for another. Uncertainties about facts arise from three inevitable aspects of scientific research: (1) imperfections in evidence (internal validity), (2) differences between evidence and actual experience (external validity), and (3) the possibility of surprises in the underlying science. As examples of uncertainties about values, people might be so unfamiliar with some of the effects of a drug that they cannot predict their reactions to it or they might have erroneous expectations about their responses.
The job of a communicator is to find out which uncertainties are important to the individual, and deliver scientifically grounded messages that provide that information. Fischhoff indicated that poor communication about uncertainty can cause:
- Needless hesitation. People might postpone a decision while trying to get more information, when the uncertainty actually lies in their preferences.
- Unwarranted confidence. People might think they know themselves and their circumstance better than is actually the case.
- Inappropriate choices. People would have made better choices if they had a better understanding of the uncertainties.
__________________
1 This section is based on the presentation by Baruch Fischhoff, Howard Heinz University Professor, Department of Social and Decision Sciences, Department of Engineering and Public Policy, Carnegie Mellon University.
- Personal regret. People wish that they had made a different choice, which would have been possible with better understanding of the uncertainties.
- Interpersonal resentment. People might blame others who, they believe, should have helped them work through these uncertainties.
As the literature of risk communication demonstrates, Fischhoff noted, scientific rigor is needed to create accurate messages. Underlying any risk communication is an implicit decision tree representing the choice that the communicator seeks to inform (see Figure 5-1). Making that tree explicit allows a disciplined approach to selecting relevant information.
Fischhoff explained that there are three concerns of experts that can hamper taking a scientific approach to communicating uncertainty. First, experts might be reluctant to express uncertainty, which they perceive as misplaced imprecision. The second is that experts might have such a poor opinion of lay audiences that they expect to be misunderstood. The third is that experts might be afraid of being punished, by their employers or colleagues, for being candid about uncertainties.
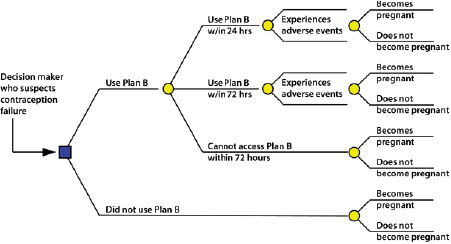
FIGURE 5-1 Decision tree for Plan B use after suspected contraceptive failure. Decision trees represent decision options, outcomes, and their associated uncertainties.
SOURCE: Reprinted from Social Science & Medicine, 67(4), T. Krishnamurti, S. L. Eggers, and B. Fischhoff, The impact of over-the-counter availability of “Plan B” on teens’ contraceptive decision making, 67:618-627, 2008, with permission from Elsevier.
Fischhoff offered two proposals to regulatory decision makers that could improve their risk communication efforts:
- Create standard procedures for making and communicating decisions. FDA’s benefit–risk framework (see Figure 1-1) provides a sound structure for summarizing uncertainty. Fischhoff noted the Prescription Drug Facts Box as a means for communicating that summary (see Figure 5-3).
- Create a resource center for eliciting and communicating uncertainty. Fischhoff noted that current support for risk communication efforts is largely haphazard and episodic. Establishing dedicated resource centers, akin to the statistics units (or “cores”) that are part of large medical research projects, would allow medical experts to receive high-quality support for applying the science of communication to conveying their science and its uncertainties. Such a center would provide:
- Quality assurance for eliciting and communicating uncertainty;
- Economies of scope, by addressing recurrent issues with a common base of knowledge;
- Enhanced professional relationships between scientists and communications, built on trust and mutual respect; and
- Stimulus for basic applied research, addressing communication challenges emerging from the work.
INCREASING PUBLIC AWARENESS AND UNDERSTANDING OF UNCERTAINTY
Decision Making from the Patient’s Perspective2
Regulators routinely evaluate a drug’s benefits and risks for a population, and health care providers routinely evaluate those benefits and risks for their individual patients. But the patients must ultimately weigh all of the information available to them in the context of their unique values, needs, and expectations, said Kimberly McCleary, Director, Strategic Initiatives, FasterCures.3
Patients are looking to answer three questions, she said: What benefits am I trying to enhance with the treatment I am considering, what
__________________
2 This subsection is based on the presentation by Kimberly McCleary, Director, Strategic Initiatives, FasterCures.
3 For more information on FasterCures’ Benefit–Risk Assessment program, see http://www.fastercures.org/r-and-d-policy/benefit-risk-assessment (accessed September 12, 2014).
risks or harms am I trying to avoid or mitigate, and how confident am I about the information I have at hand to make these decisions? Patients must contend with myriad inputs and influences that complicate their choices, and the choices themselves may change with time and changing circumstances.
To illustrate the complexity of the patient decision-making process, McCleary provided an overview of the sources of information and influence that affect uncertainty about treatment options. They include
• Purpose of the treatment option
- Is it for disease prevention, or is it curative? For a chronic condition, or to delay a chronic condition from developing? Acute care for life saving, or palliative care for end of life?
• Treatment options
- Medication, surgery, in-hospital treatments, cognitive therapy, “nutraceuticals,” possible inclusion in clinical trial
• Family decisions and family attitudes
• Information sources
- Peers, co-workers, friends
- The Internet (ranging from well informed, seemingly well informed, and not even pretending to be well informed)
- Support groups for various conditions, and these can be very well-organized, professionally facilitated support groups that have a particular intention in terms of informing about the choices
- Loosely organized online discussion groups
- Media coverage
• Other factors
- Insurance coverage, reimbursement, out-of-pocket costs, disability vs. employment, geographic proximity to treatment location, and support system
McCleary noted that to date, there has been no structured process for patients to evaluate all these factors in the context of their own personal and medical situations.4 Instead, as is true for anyone making decisions, people will make their choices based on whatever information is accessible, most memorable, or best fits with their values.
__________________
4 For an example of a patient-focused, structured decision-making approach, see the presentation in Chapter 3 by Robyn Lim, Senior Science Advisor, Office of Legislative and Regulatory Modernization, Health Products and Food Branch, Health Canada, on Health Canada’s Benefit–Harm–Uncertainty Initiative.
Communicating Uncertainty About Benefits and Harms of Pharmaceuticals5
Four common uncertainties are present at the time of approval that affect most, if not all, drugs, according to Lisa M. Schwartz, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice, and Steven Woloshin, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice.
1. Standard uncertainty. According to Woloshin, the standard uncertainty that applies to all new drugs has to do with their limited track record. To get drugs to market in a reasonable amount of time, approvals generally are based on relatively short-term clinical studies involving limited numbers of patients. Furthermore, clinical trials for regulatory approval are designed to detect benefit, not harm. Consequently, it cannot be known at the time of approval how well a drug’s benefits or safety will hold up over time when a drug is taken over periods of time that are longer than the trial duration. Unfortunately, Woloshin said, it is not unusual for serious adverse effects to emerge after large numbers of people use a drug for long periods of time.
While clinicians and researchers are usually aware that the true effects of new drugs are inherently uncertain, patients might not understand. This leads to what Woloshin called the standard misconception that “new is better.” This misconception is reinforced in advertisements targeting physicians and consumers that promote a drug’s newness as representing extra benefit, rather than extra uncertainty, noted Woloshin.
In an attempt to offset this misconception, regulators in Europe and the United Kingdom require companies to include a “black triangle” warning next to the name of a new drug on all prescriber and consumer information, alongside the statement “This medicinal product is subject to additional monitoring.”6 The intent is to alert the public that despite a rigorous approval process, the drug is “under probation,” as Woloshin
__________________
5 This subsection is based on the presentation by Lisa M. Schwartz, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice, and Steven Woloshin, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice.
6 For more information on the European Union’s use of the “black triangle” scheme, see http://www.mhra.gov.uk/Safetyinformation/Howwemonitorthesafetyofproducts/Medicines/BlackTriangleproducts/index.htm (accessed September 12, 2014).
termed it, reminding consumers that a drug’s track record is established over time as greater numbers of people use it over a longer period of time.
To test how communicating the concepts inherent in the black triangle would affect consumer enthusiasm for new drugs in the United States, Schwartz and Woloshin conducted a national randomized trial of approximately 3,000 adults (Schwartz and Woloshin, 2011). Participants were asked to choose between two heartburn drugs with the same benefits and harms—with the only difference being that one drug was approved in the current year and the other had been approved 8 years earlier. The control group received no other information, but the intervention group was told, “As with all new drugs, rare but serious drug side effects may emerge after the drug is on the market—when larger numbers of people have used the drug.” Woloshin reported that the study found that the simple one-sentence warning dampened enthusiasm for the new drug. The warning reduced the proportion of patients choosing the new drug by 19 percent (66 percent vs. 47 percent, 95 percent confidence interval: 13 to 24 percent) (Schwartz and Woloshin, 2011).
Woloshin suggested that graphics like the black triangle or text-only warnings should be applied to new drugs for the first few years they are on the market to highlight this inherent uncertainty to the public. He noted that the IOM study (2007) also called for the implementation of this new drug warning on all product labels.
2. Extra uncertainty due to accelerated approval. The second common uncertainty results when there is limited evidence of benefit at the time of approval. For example, drugs that are subject to FDA’s accelerated approval process when they are intended to treat serious diseases with limited treatment options. This approval pathway permits drawing on preliminary evidence (e.g., trials might use a surrogate endpoint as the primary outcome, might employ a single-arm design, or might be shorter in duration than FDA’s standard) to speed new drugs to patients who need them. A total of 11.7 percent (22 out of 188) of novel therapeutic agents approved by FDA between 2005 and 2012 were reviewed through the accelerated approval mechanism (Downing et al., 2014).
Woloshin explained that while the concept of accelerated approval is very useful and important, information conveying that there is extra uncertainty due to the accelerated nature of the approval is often buried in the various communication tools deployed by FDA. He argued that this uncertainty should be highlighted and featured prominently for physicians and patients. To illustrate, Woloshin compared the information on the package insert for Tysabri, a product that received accelerated approval, to what he considered a more appropriate disclosure (see Figures 5-2 and 5-3). Recent FDA guidance to industry on drug labeling
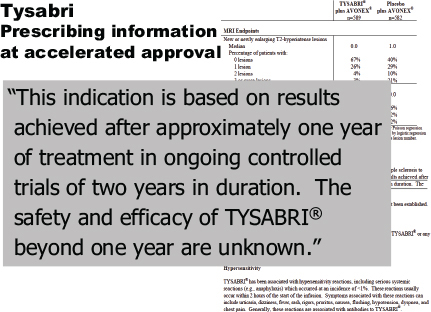
FIGURE 5-2 Tysabri prescribing information appearing on page 4 of the package insert.
SOURCE: Schwartz and Woloshin, 2014. Presentation at the IOM workshop series on Characterizing and Communicating Uncertainty in the Assessment of Benefits and Risks of Pharmaceutical Products.
now calls for this type of disclosure in the “Highlights” section of a drug label (FDA, 2014).
3. Extra uncertainty based on surrogate primary outcomes. Approximately half (48.9 percent) of the pivotal clinical trials for novel therapeutic agents approved by FDA between 2005 and 2012 included a surrogate outcome as the primary endpoint (Downing et al., 2014).7 Surrogates should translate into patient outcomes, said Schwartz, but they do not always. For example, the drug Iressa was approved to treat advanced lung cancer on the basis of the surrogate outcome of tumor shrinkage seen on X-rays. The hope was that tumor shrinkage would translate into reduction of lung cancer deaths. Unfortunately in this case, when the required randomized trial was completed, Iressa did not reduce lung cancer death and the drug’s label was changed to limit use in certain cancer patients.
__________________
7 A surrogate outcome is intended to substitute for a clinical endpoint; for example, lower blood pressure might serve as a surrogate for lower rates of heart disease.
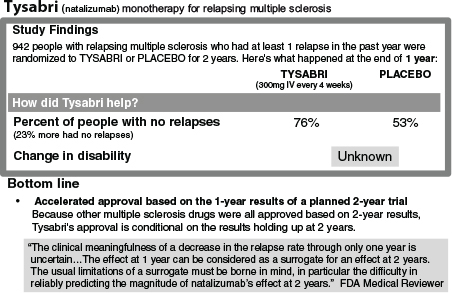
FIGURE 5-3 A Tysabri Drug Facts Box suggested by Woloshin and Schwartz to concisely highlight what was known, still being studied, and unknown at the time of Tysabri’s accelerated approval.
SOURCE: Schwartz and Woloshin, 2014. Presentation at the IOM workshop series on Characterizing and Communicating Uncertainty in the Assessment of Benefits and Risks of Pharmaceutical Products.
Because of the fundamental uncertainty of surrogate outcomes, Schwartz said, it is important that patients understand the inherent uncertainty when drug approvals are based on surrogate outcomes. The same randomized trial mentioned above (Schwartz and Woloshin, 2011) tested people’s perspectives on the concepts behind surrogate outcomes. The results revealed that a simple, 23-word, non-directive explanation about surrogate outcomes resulted in 12 percent more people (71 percent vs. 59 percent, 95 percent confidence interval: 7 to 18 percent) correctly choosing a drug that reduced myocardial infarctions over one only known to improve cholesterol levels.
Educating patients about the uncertainties of drugs approved on the basis of a surrogate outcome matters, Schwartz explained, because such drugs might be heavily promoted through direct-to-consumer advertising. For example, Zetia was heavily advertised to the public for several years before FDA began requiring that the prescribing information and marketing materials include the statement, “The effect of Zetia on cardio-
vascular morbidity and mortality has not been determined.” Schwartz indicated that this statement is an important step in the right direction, but FDA should also ensure that these crucial messages about uncertainty are routinely communicated to patients and are not buried at the bottom of lengthy, dense documents.
4. Extra uncertainty based on signals of harm. Schwartz suggested that when data supporting a newly approved drug indicate a potential signal of harm strong enough for FDA to require postmarketing studies, this is an important signal of uncertainty that should be clearly shared with patients. Many drugs are aggressively promoted, potentially increasing patient misunderstanding regarding the fundamental uncertainties about benefits and harms still being evaluated. Schwartz indicated that FDA could improve the consistency and impact of its communications by prominently featuring information about postmarketing requirements in press releases, information for prescribers, and labeling. Schwartz also noted the importance of including information about the direction of the uncertainty—for example, if the uncertainty is not that the effect of a drug on an outcome is unknown, but that there is an open question about a potential harm and that FDA is requiring specific postmarketing studies to better understand the magnitude of the problem. Box 5-1 includes a summary of routine disclosures for regulators suggested by Schwartz and Woloshin to proactively communicate uncertainties about newly approved drugs to the public.
The Drug Facts Box
Schwartz suggested that information about uncertainty is most helpful in the context of what is known about a drug’s benefits and harms. In general, people are more likely to tolerate uncertainties when the benefit-to-harm ratio is large than when it is small. Schwartz and Woloshin suggest that FDA consider summarizing the facts about benefits, harms, and uncertainties in a reader-friendly format such as the Drug Facts Box, a one-page summary of benefit and harm data for each indication of a drug that includes explicit acknowledgment of uncertainties (Schwartz and Woloshin, 2013). Schwartz noted that members of FDA’s Risk Communication Advisory Committee unanimously voted that FDA should adopt the Drug Facts Box as its standard format (FDA, 2009b), and the Affordable Care Act8 also suggests that FDA conduct a pilot study of the Drug Facts Box to improve communication.
__________________
8 Patient Protection and Affordable Care Act of 2012. Pub. L. No. 111-148, § 3507, 124 Stat. 119, 530 (codified at note following 21 U.S.C. § 352).
BOX 5-1a
Suggested Routine Disclosures for Regulators
Based on the common uncertainties that are present at the time any new drug is approved, Schwartz and Woloshin recommended a proactive approach to communicating these uncertainties to the public.
Flag New Drugs for the First Few Years on the Market
Use a graphic or text to communicate that the limited experience with new drugs means greater uncertainty.
Warn When Evidence of Benefit Is Especially Weak
Be clear about the extra uncertainty inherent with study duration shorter than FDA standard or use of surrogate outcome measures.
Point Out Postmarketing Trials Required for Signals of Harm
Specify what postmarketing trials were required, why, and when results will be available—in the Highlights of the label (in either “Limitations of Use” or “Warnings & Precautions” sections).
Prominently Acknowledge Uncertainty at Approval
Explain uncertainties about benefit or harm in FDA press releases, the professional label, and consumer information.
__________________
a This box is based on the presentation by Lisa M. Schwartz, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice, and Steven Woloshin, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice.
COMMUNICATING UNCERTAINTY: FDA AND MEDIA MESSAGES ABOUT TYSABRI9
Tysabri (natalizumab) was approved by FDA in 2004, on an accelerated schedule, as a promising new drug to treat patients with relapsing MS. Four months later, it was withdrawn from the market after two people developed a rare, deadly brain infection called PML. The drug
__________________
9 This section is based on the presentation by Lisa M. Schwartz, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice, and Steven Woloshin, Professor, Departments of Medicine and Community & Family Medicine, Dartmouth Medical School; and Co-Director, Center for Medicine and the Media, at The Dartmouth Institute for Health Policy and Clinical Practice.
was reintroduced after risk factors for PML were identified (see Box 3-3 for details about Tysabri).
Schwartz and Woloshin presented an analysis of media reports about Tysabri, focusing on the presentation of benefits, harms, and uncertainties stemming from the accelerated approval process, and the risk of PML. The analysis included 76 stories from major newspapers, and national radio and television transcripts for the 2 months following each of six major milestones in the story of Tysabri. The six milestones selected were: (1) Tysabri approval in 2004, (2) Tysabri withdrawal in 2005 after identification of two PML cases, (3) the convening of a 2006 FDA advisory committee meeting on Tysabri, (4) the remarketing approval of Tysabri in 2006, (5) the 2008 emergence of the first two new cases of PML after remarketing, and (6) FDA’s 2012 announcement of the first test to help determine the risk of PML in people taking Tysabri. Schwartz and Woloshin cautioned that the results they presented were preliminary.
FDA Messaging About Tysabri
Woloshin provided an excerpt from the FDA press release (2004) at the time of Tysabri’s original approval:
This innovative treatment for multiple sclerosis represents a new approach to treating MS—exciting news for patients with this serious disease. . . . While we eagerly await long-term results from ongoing clinical trials, we have reason to believe that Tysabri will significantly reduce relapses in MS.
Woloshin characterized this statement on the first page of the press release as overly enthusiastic, noting that the statement exhibited the standard misconception that new is better. The press release also failed to highlight the uncertainty that is inherent to all new drugs, and the extra uncertainty that existed because Tysabri received accelerated approval.
Also in the initial FDA press release was a statement that the approval of Tysabri was based on positive results seen in patients after 1 year of treatment:
The approval of Tysabri is based on positive results seen in patients after one year of treatment. This product received accelerated approval because it appears to provide substantial benefit for patients with a serious disease. As part of that approval, the manufacturer has committed to continuing its trials of this product for another year.
The reason presented for accelerated approval is factually correct, said Woloshin. The press release clearly acknowledges that long-term results are pending and that approval was based on 1 year of clinical trial
data instead of 2 years. However, he said, the press release did not state that all previous MS drugs were approved on 2 years of evidence, that the Tysabri approval was a departure from the norm, and that the shorter track record increased uncertainty about outcomes.
Also, Woloshin noted, the release included no acknowledgment that Tysabri’s effect on disability progression—another important clinical outcome—was unknown at the time of approval, but which the company was required to report when 2-year study data were available. The FDA press release also quantified the effect of the drug with a relative risk reduction (i.e., Tysabri reduced the frequency of relapses by 66 percent relative to placebo). But stating relative changes without also stating the base rate can exaggerate the perceived benefit of an intervention. For instance, imagine hearing that items in a store are 30 percent off without knowing what they cost originally. Woloshin explained that using the term “30 percent off” means much more savings with expensive items compared to less expensive ones. Woloshin further suggested that a clearer message about the effect of Tysabri would have been to indicate that, compared to a placebo, the drug reduced the relapse rate from 7.4 to 2.5 relapses out of 100 people per year.
How the Media Responded
Woloshin and Schwartz analyzed each of the five stories on Tysabri that appeared in the top 20 U.S. newspapers when the approval was announced10 (see Figure 5-4). Four out of five stories characterized the accelerated approval process as meaning “extra promise” rather than “extra uncertainty” about benefit, said Woloshin. Articles that quantified the treatment effect generally used relative risk numbers, rather than absolute risk, just as in the FDA press release. None mentioned the disability outcome, and none talked about how the drug compares to other drugs on the market in terms of harms. These factors also were not mentioned in the FDA press release.
Effect of Press Releases on Media Coverage
Schwartz presented an argument for using the press release to communicate about uncertainty as well as benefit. Evidence shows that press releases can influence media reporting. Schwartz and Woloshin compared medical journal press releases with news coverage and showed a strong association between what was in the press release and what appeared in the subsequent news stories (Schwartz et al., 2012). Relating these results
__________________
10 Due to time constraints, the study used a limited sample. Results are preliminary.
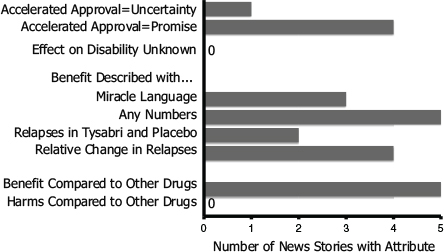
FIGURE 5-4 Media response to 2004 Tysabri approval announcement. Media coverage of the original Tysabri approval largely mirrored the statements and characterizations of the drug’s benefit from the FDA press release.
SOURCE: Schwartz and Woloshin, 2014. Presentation at the IOM workshop series on Characterizing and Communicating Uncertainty in the Assessment of Benefits and Risks of Pharmaceutical Products.
to the Tysabri case study, Schwartz noted that FDA issued another press release at the time Tysabri was withdrawn from the market in 2005:
During the review of Tysabri for remarketing approval, FDA conducted an intensive analysis of possible adverse events that might be related to the effect of the drug on the immune system. No cases of PML were seen in the clinical trials. However, for any approved therapy, new and unexpected adverse events may occur that were not seen in clinical trials.
The final sentence of this excerpt is a great warning, according to Schwartz. However, she added, this statement would be more effective in a press release at the time of approval, rather than after the unexpected adverse effect happens.
FDA could improve communication about uncertainty by being more proactive about communicating the benefits, risks, and uncertainties of a newly approved drug, Schwartz argued. Developing fair presentations of the data and including them consistently in press releases would help all decision makers—patients, providers, lawmakers, and payers.
CHALLENGES AND OPPORTUNITIES TO IMPROVE COMMUNICATION ABOUT UNCERTAINTY11
Carmen Bozic, Senior Vice President, Clinical and Safety Sciences, Biogen Idec; Robert Fox, Staff Neurologist, Mellen Center for Multiple Sclerosis and Vice-Chair for Research of the Neurological Institute, Cleveland Clinic; Alice Hughes, Deputy Director for Safety, Division of Neurology, CDER, FDA; Joyce Korvick, Deputy Director for Safety, Division of Gastroenterology and Inborn Error Products, Office of Drug Evaluation III, CDER, FDA; and Cynthia Sitcov, Patient Representative & Voting Member, FDA Central and Peripheral Systems Advisory Committee, participated in a panel discussion moderated by Gavin Huntley-Fenner, Human Factors and Safety Consultant, Huntley-Fenner Advisors, about the challenges and opportunities to improve communication about uncertainty. Patients, providers, the pharmaceutical development industry, and regulators often have different needs and expectations for communications regarding uncertainty about pharmaceutical products.
Balancing Benefits, Risks, and Uncertainties
Balancing what is known about the benefits, risks, and uncertainties of a new drug compared to older drugs with a longer track record is a complex task, highly dependent on the preferences and context for individual patients. The panel discussed the therapeutic environment for MS at the time Tysabri was approved in 2004 and the fact that there was a considerable level of optimism about the high level of effectiveness Tysabri offered in comparison to older MS treatments with a modest level of benefit. In 2004, the significant PML safety concern that would eventually arise was still an “unknown unknown.”
Fox suggested that his experience treating MS patients after Tysabri’s initial approval has changed his approach to conveying information to patients. In 2004, given the limited availability of other treatment options, he was comfortable recommending Tysabri as a highly effective therapy that seemed safe. Today, with a total of 10 FDA-approved MS therapies on the market, Fox generally suggests 2 or 3 therapeutic options for each
__________________
11 This section is based on the remarks by Carmen Bozic, Senior Vice President, Clinical and Safety Sciences, Biogen Idec; Robert Fox, Staff Neurologist, Mellen Center for Multiple Sclerosis and Vice-Chair for Research of the Neurological Institute, Cleveland Clinic; Alice Hughes, Deputy Director for Safety, Division of Neurology, CDER, FDA; Gavin Huntley-Fenner, Human Factors and Safety Consultant, Huntley-Fenner Advisors; Joyce Korvick, Deputy Director for Safety, Division of Gastroenterology and Inborn Error Products, Office of Drug Evaluation III, CDER, FDA; and Cynthia Sitcov, Patient Representative & Voting Member, FDA Central and Peripheral Systems Advisory Committee.
patient, tailored to their disease severity and treatment preferences. Fox noted that he is sure to explain to patients the extra uncertainty inherent in products that are new to the market, but, he added, this discussion also poses a challenge to the physician–patient relationship. Patients often interpret that the doctor is unknowledgeable instead of “there is uncertainty around this drug,” which are two very different things. Patients come to physicians for answers and often do not want to hear explanations about uncertainty around a drug.
Sitcov noted that as a Patient Representative & Voting Member of the FDA Central and Peripheral Systems Advisory Committee who reviewed evidence prior to the remarket authorization of Tysabri, and as an individual with MS, she had to consider the benefits of Tysabri in spite of the risks. Sitcov reflected on the overwhelming testimony from Tysabri users pleading for reapproval of the drug despite its risks. While Sitcov decided against using Tysabri herself, she considered the powerful testimony of a number of patients as she voted to reapprove the drug for the market. Hughes reflected on FDA’s decision to remarket Tysabri in 2006 and the careful communication strategy deployed by the agency to characterize the significant level of uncertainty that still remained about the risk of PML and Tysabri.
Fox discussed a risk tolerance study that showed a broad range of maximum risk tolerated by patients for the exact same disease (Fox et al., 2011). The Internet-based study included 5,446 patient volunteers and was conducted through the NARCOMS MS patient registry (a voluntary MS patient registry). The risk tolerance covered the spectrum of “no matter what the risks are, I would still take the treatment” to “regardless, if there was any risk of that, I would not take the treatment.” In this study, patients indicated a higher risk tolerance as the severity of their disease increased.
Bozic emphasized the importance of open communication, saying, “Every time we learned something new, we should share it with the regulators, we would share it with prescribers and patients, and we did it through multiple avenues, with the label being the primary approach.”
Stephen Sun, Chief Medical Officer, ParagonRx, discussed the management of uncertainties in benefit and risk assessments and suggested that (1) systematic approaches should be used for risk management, (2) a benefit lexicon should be established and could include a benefits table to accompany the adverse events table in a medical product’s package insert, and (3) the context in which medical products are used matters and could be better understood with individual stakeholder mapping.
Communication Tools and Quantification of Risk
Regulatory tools for communicating benefits, risks, and uncertainty surrounding a drug include labeling updates, drug safety communications, medication guides, and press releases, said Korvick and Hughes. According to Hughes, FDA issued drug safety communications as the primary communication tool when the agency thought it had information that might change or meaningfully inform discussions and decisions regarding initiation and continuing treatment for individual patients. FDA has wanted to be “transparent, but convey useful, interpretable information that will allow meaningful risk–benefit decisions.” Hughes highlighted that the key is to communicate with deliberate statements about the knowns and unknowns of a therapy.
FDA relied on the label as its primary communication tool with prescribers prior to and during the reauthorization of Tysabri because it provided a format to convey a significant amount of detailed information in a meaningful way. However, Hughes noted, given the workshop discussions regarding the importance of information presented in press releases, there might be better options to communicate uncertainty to prescribers.
As part of the REMS requirements following the remarketing of Tysabri, the medication guide was required to be provided to patients during each infusion of the drug. Hughes indicated that although FDA included quantitative estimates of PML incidence in information designed for prescribers (e.g., the label), this quantification of risk was not included in Tysabri’s medication guide provided to patients as part of REMS. Hughes suggested that the thinking behind this approach was that the quantification of PML risk would change over time and a quantitative risk discussion was best suited for the patient–physician interaction. Korvick noted the difficulty in conveying risk and uncertainty in the postmarketing setting because calculations of risk often lack a robust denominator reflecting the widespread use of a drug among patients.
Beyond labeling, said Bozic, industry uses other resources to communicate with patients and providers, including medical information channels, websites, and medical science liaisons. Bozic stressed that industry needs to be attentive to communicating a balance of benefit and risk information because patients and physicians have both indicated the desire to receive this balanced information to inform the decision-making process. Building on the workshop discussions earlier in the day regarding patients’ ability to understand quantitative estimates, Bozic and Robert Temple, Deputy Director for Clinical Science, and Acting Deputy Director, Office of Drug Evaluation I, CDER, FDA, suggested that industry and regulators could explore opportunities to include meaningful quantification of benefit and risk into medication guides and other communication tools.
This page intentionally left blank.


















