
6
Models of Care and Approaches to Payment
No single model of care will be able to meet the needs of all individuals who receive (or want to receive) home health care. As a variety of approaches are needed to deliver a range of services in the home, different approaches to payment also need to be considered. At the workshop, an overview of the current range of models and approaches to payment was provided, and then six speakers described their individual experiences (including both successes and challenges) in trying new models of care and using new approaches to payment. Together, these presentations consider how to facilitate the development of the models and payment approaches that will be needed to achieve a vision for the future role of home health care.
OVERVIEW OF THE RANGE OF MODELS AND APPROACHES TO PAYMENT
Peter Boling
Virginia Commonwealth University
Boling began his presentation by describing the scenes that he encounters when he takes his medical students to his patients’ homes, an aspect of clinical training that students rarely experience. Recent visits provided an opportunity for the students to see the deep connections that can develop between clinician and patient, he said. These stories, presented in Box 6-1, gave the students—and the workshop participants—a sense of the continuum of care and the diverse realities of patients’ worlds.
BOX 6-1
Two Virginia Men
Boling took his medical students to the home of a Virginia man, age 53 years, who has lost the use of his limbs and torso. He has been Boling’s patient for 20 years. He spends his days mostly in the prone position because that gives him the most maneuverability, given his limited use of his hands. As a result, he developed pressure ulcers on his elbows. He has had multiple hospitalizations because of urinary tract infections. On one occasion, he was placed in a nursing home, after which he said he is never going back. He is heavily dependent on medical technology, specifically, his bed and wheelchair.
This man runs a consumer-directed care model for himself. According to him, the three women assigned to comanage his care with him are not very competent, and he has had to teach them what to do. In fact, he has trained a number of different individuals to be his aides and how to properly care for a quadriplegic, “which is not easy,” Boling said.
The second patient Boling described is a man who was accidentally shot in the neck at age 16 years while walking with his sisters on Coney Island. He completed his college education, obtained a master’s degree, and became an effective teacher. One of his students is the sister of the woman who is now his personal care aide (again, a consumer-directed care arrangement), and she—along with her baby and husband—live in the front part of the house where he stays. She smokes a lot. Although it is not an ideal situation, he has been homeless in the past, so it is much better than what he has experienced at some other times in his life.
He has a laptop and is waiting for Internet service. Boling wants to help him reconnect with his teaching. In the past, this man also trained some of his aides, who at night worked in strip tease clubs. He says that was a very interesting period for him and that they actually did a pretty good job.
SOURCE: As presented by Peter Boling on September 30, 2014.
Measuring the value of Home Health Care
The diversity of home health care experiences makes the components of care as well as their effects hard to measure in a reliable, consistent manner, “so that you can say structure, process, [and] outcome and be able to categorize them in a way relevant to federal health policy,” Boling said. Nevertheless, it is necessary to define the population of care recipients and their needs in some manner. The really complicated patients—analogous to Thomas E. Edes’s 5 percent—simply do not fit into the usual care systems. “We need to carve these patients out,” Boling said, and provide them care by use of a different model in which care is paid for differently and outcomes are measured differently.
Boling said that a strong medical component is often left out of home health care and that it needs to be combined with social supports into a service that is truly patient-centered and affordable and that aligns funding with the care model. When quality is measured and value is estimated, it is important to adjust the cost estimates according to the risks for the population being served and to select quality measures specific to that population, as well as the care setting. These measures must be simultaneously accurate and not too burdensome to collect, he said.
Patient Needs
Home health care users fit into a variety of subtypes, Boling said (see Table 6-1). The most complicated, challenging, and expensive patients receiving home health care, Boling said, are those with a high comorbidity and illness burden who may need acute care at home, post-acute transitional care, or long-term health care. His estimates are that some 3 million to 4 million Americans are chronically limited to their homes and have three or more problems with activities of daily living (ADLs). Most but not all of them are elderly, he said, and although they may have a reduced life expectancy, they are not necessarily eligible for hospice. Some are dependent on medical technology, such as ventilators. A group of very ill patients—another 2 million to 3 million—also requires large amounts of medical care, but only for a relatively short time, because of an acute illness or injury or because of an advanced life-limiting condition.
TABLE 6-1 Home Health Care User Categories
| Category | Description of Home Health Care User |
| A | The user has no illness (acute or chronic) and uses self-help sources |
| B | The user is ambulatory, independent, and not “sick”; some chronic health conditions exist |
| C | The user is younger, and functions (ADLs) are limited by one condition; the user is not “sick” often but needs continuous ADL support |
| D | The user is older with chronic cognitive or functional impairment; the user is infrequently acutely ill (low cost) and needs support with ADLs |
| E | The user requires post-acute care at the end of a discrete illness episode but has a rapid return to stable condition and home health care ends |
| F | The user has a high comorbidity and illness burden and is sick, and the cost of care is high |
NOTE: ADLs = activities of daily living.
SOURCE: Reprinted with permission from Peter Boling, Virginia Commonwealth University.
Although the medical needs of these patients may be considerable, Boling said, they also need a matrix of social services, including, as other presenters have said, paid personal care, transportation, nutrition and home safety services, communication assistance, and legal and financial planning. The care system needs to make the services that cannot be provided by friends and family accessible, comprehensive, and coordinated and to make sure that these services are aligned with the patient’s goals and needs, he said.
Medicaid recipients needing home health care encounter a program that, Boling said, offers discontinuous skilled care, a weak medical model, a slow response to urgent problems (resulting in unnecessary hospitalizations), and inconsistent attention to needs for help with ADLs and a system that is not aligned with other programs and payers, notably, Medicare.
Models of Home-Based Care
As evidence that substantial improvements are possible, even for acutely ill individuals, Boling pointed to a number of programs, in addition to the programs previously described by Edes sponsored by the U.S. Department of Veterans Affairs (VA) (see Chapter 5). Boling reviewed evaluations of three models of care that have proved successful according to patient outcomes and cost reductions but that have not been adequately replicated or scaled up:
- An evaluation of Outcome-Based Quality Improvement, a 1990s performance improvement methodology that reduced hospitalizations by about one-quarter (Shaughnessy et al., 2002);
- A randomized trial of Hospital at Home, which provided hospital-level care at home and that resulted in fewer medical complications and lower costs (Leff et al., 2005); and
- A randomized trial of the effects of assignment of an experienced nurse practitioner (NP) to at-risk older adults while they were still in the hospital; the NP followed up with these adults once they were home, managed their care, and ensured that the care plan was followed; this approach resulted in reduced hospital readmissions and a 50 percent cost savings (Naylor et al., 1999).
Concerns that have limited the spread of these highly targeted programs are that they are not considered scalable, which is not necessarily true, Boling said. A key question is who benefits from the savings from such programs? Although they are good for the Medicare program, participat-
ing hospitals experience reduced reimbursements. Boling tells his hospital and the subspecialists who practice there, “You will not miss these patients if we carve them out. You lose money on them. They clog up the works and slow down the clinics.” Finally, not all patients in the NP-centered program described above could function without additional help after the NP visits end. “That’s a limitation of this new silo—the transitional care silo—that we are starting to create,” he said. Stimulated by this problem, a less expensive, less intensive intervention was tested on a slightly less sick group of patients and also proved effective, but it provided lower cost savings (Coleman et al., 2006). This model involved patient empowerment, improved communication and records transfer, and had “a lighter clinical touch,” Boling said. Although it may be more easily scalable, the problem of who will pay for it remains.
Boling then reviewed a number of other innovative programs.
Community-Based Care Transitions Program
The Community-Based Care Transitions Program,1 created under Section 3026 of the Patient Protection and Affordable Care Act of 2010 (ACA),2 has devoted up to $500 million to tests of new transitional care models at more than 100 participating sites so far. Again, this program provides short-term assistance for patients, Boling said, but the program “starts to reorient people’s thinking in the community and involves a lot more people in the process of improving health care.”
Geriatric Resources for Assessment and Care of Elders
The Geriatric Resources for Assessment and Care of Elders (GRACE) model was tested in a randomized trial and showed considerable improvement in clinical care processes (Counsell et al., 2007). Selected patients were discharged home, where they received quarterly visits from an NP for 2 years. The NPs reported back to clinic-based geriatricians and made recommendations. Analysis showed an approximately 30 percent reduction in overall costs, attributable to fewer hospitalizations and emergency room visits in the highest-risk subgroup, Boling said.
______________
1 See http://innovation.cms.gov/initiatives/CCTP (accessed December 24, 2014).
2 Patient Protection and Affordable Care Act of 2010, Public Law 111-148, 111th Cong., 2nd sess. (March 23, 2010).
Program of All-Inclusive Care for the Elderly
The Program of All-Inclusive Care for the Elderly (PACE)3 is an established benefit for individuals dually eligible for Medicare and Medicaid that has been used by only a small number of participants (Wieland et al., 2010). It requires people to give up their traditional Medicare and Medicaid and enter a structured, high-overhead, mostly center-based program providing comprehensive health and social services. Although the savings that it achieves are modest, Boling said, the quality of services for those who like the model is high, and it decreases the cost burden for government programs by accepting the full risk for enrollees.
Home-Centered Primary Care
Boling noted a non-VA home-centered primary care program tested in a case-control study that used an interdisciplinary team model to provide medical care and hospice services in the home (De Jonge et al., 2014). This model achieved better care and reduced costs 17 percent over 2 years and reduced costs 31 percent for the most complex, sickest patients through reductions in hospitalizations and nursing home use. It requires an experienced care team, and traditional fee-for-service payments do not cover its costs.
Independence at Home
Independence at Home,4 funded by Section 3024 of the ACA, is targeted to post-acute care patients with several serious chronic conditions and disabilities. The participating sites, which are using various organizational models, may be able to share in program savings. This is a key, Boling said, to creating incentives for medical care providers to become involved in longitudinal home-based care for a high-cost population and to fund the program longer term. If the model works, legislation will be needed to expand it.
Boling responded to a question from James Pyles of Powers Pyles Sutter & Verville PC about how Independence at Home works for seriously chronically or terminally ill individuals who may need help on a 24-hour-per-day basis. Realistically, Boling said, the only people in the home 24 hours per day are patients and their family members. Then, depending on what they can afford, an aide may be present for 8 hours or more. If someone truly
______________
3 See http://www.npaonline.org/website/article.asp?id=12&title=Who,_What_and_Where_Is_PACE (accessed December 5, 2014).
4 See http://innovation.cms.gov/initiatives/independence-at-home (accessed December 5, 2014).
needs care 24 hours per day, whether they are in hospice or getting to that point, the care process is often supported by a constellation of friends and family, neighbors, and paid aides under existing financial models, Boling said.
Further Considerations
Overall, Boling noted the following lessons from these models:
- Significant cost savings are achievable.
- Targeting of the highest-risk patients is the key to achieving savings.
- Transitional care models need to transition to longer-term care for many patients.
- To continue, successful models need stable sources of funding.
This litany of successful and promising programs also suggests the need to look at some models that have not worked. Lessons from these approaches, Boling said, include
- The coordination of care through a call center or the like does not work unless good integration with primary care is achieved.
- Patient-centered medical homes are not sufficiently patient centered for the sickest people who are homebound, although they may be effective for the majority of patients.
- Accountable care and managed care models need some kind of a carve out for the frailest population.
Standards of care that recognize that some of the treatments that make sense in younger, healthier populations may not be relevant to frail individuals who are in their 80s and 90s are needed, Boling said. In some cases, these treatments do not save lives or improve outcomes and instead create troubling side effects and increase risk. Low-value services are too expensive at almost any price point, he concluded.
Teresa L. Lee, Alliance for Home Health Quality and Innovation, asked how the system can navigate toward new delivery models that make more optimal use of comprehensive home health care without setting up more silos. Boling advocated for carving out this population from the hospitals and clinics and bringing in a well-trained home health care workforce to deliver team-based care using an integrated medical-social model.
Jeffrey Burnich
Sutter Health
Sutter Health is a large, not-for-profit integrated delivery system in Northern California. Like other providers, Sutter faces the urgent need to transform its care delivery practices across the health care continuum to better serve very frail, very sick, very-high-cost patients, particularly in the last few months of life, Burnich said. Many, but not all, of these patients are Medicare beneficiaries. In doing so, one of Sutter’s greatest challenges, Burnich said, has been system fragmentation.
In 2009, Sutter Health developed the Advanced Illness Management (AIM)5 program by bringing together a cross-disciplinary group (including doctors, nurses, home health care and hospice professionals, and data analysts) to try to develop a new approach to integrating services for its home health care population. Burnich said that it built on Sutter’s managed care experience and a strengthened telesupport system. The result was the creation of transition teams in the home-based care program and the capacity to respond to emergencies, such as acute exacerbations of illness, pain crises, and family anxiety for patients receiving either end-of-life care or other services. The integrated care system is organized around patients’ goals and is targeted to people who are both frail and the sickest. Referrals can come from a hospital, a doctor’s office, or a skilled nursing facility. Burnich noted that about 40 percent of the referrals come directly from physician practices, and “without the doctors’ support, this program wouldn’t be where it is today.” The combination of AIM and integrated care management expertise in the home is yielding person-centered, evidence-based, coordinated care, he said.
The Sutter system uses a single electronic health record to record most of the services that it provides, although the home health care nurses use a separate database. The record system that Sutter uses also does not have a hospice platform, but Burnich believes that it will be adopted when it is developed.
About 2,100 patients are in this system at present, with the number increasing by about 5 percent per month, but the number of patients included is limited by the need to find trained home health care providers. The program leaders attribute this growth to the strong demand from physicians: “We can’t keep up,” Burnich said. Program staff make sure that they
______________
5 See http://www.sutterhealth.org/quality/focus/advanced-illness-management.html (accessed December 5, 2014).
communicate with referring physicians to assure them that their patients are receiving good care but do not inundate them with data.
According to Burnich, the following are essential parts of the program for each patient:
- An advance care plan,
- A self-management plan for patients of symptoms that raise a red flag,
- Medication management,
- Ongoing follow-up visits, and
- Engagement and self-management support.
All of this, he said, rests on a curative plus palliative care foundation.
The Sutter project received a health care innovation grant from the Centers for Medicare & Medicaid Services (CMS), and at the time of the workshop, Burnich was preparing to present its preliminary results to that agency. These include a 59 percent reduction in hospitalizations for patients enrolled in the AIM program for 90 days, a 19 percent reduction in emergency department use, and a 67 percent reduction in high-cost days in intensive care units. Significant cost savings attach to each of these reductions.
Initially, Burnich said, hospital administrators thought that they did not want to lose these patients because they contribute to the hospital’s fixed costs (“contribution margin”), but in fact, after day 9 or 10, they cost the hospital more than the reimbursement covers, creating negative income. By keeping these high-cost patients at home, hospitals actually make more money by losing less. When the staff in the finance department understand that, they are more comfortable with a program that does not fill beds, Burnich said.
Sutter has analyzed the profit and loss implications of the program for hospitals, for doctors’ practices (because they might lose revenue), and for home hospice, Burnich said. The doctors actually benefit financially from it, because there is no other way to cover the high cost of caring for these patients and providing the lengthy consultations that they need. The savings amount to $11,000 per beneficiary per year, and over the 3 years of the CMS grant, Burnich said, Sutter plans to serve 10,800 patients. It committed to save $29 million on these patients but is on track to actually save $118 million. The impetus for pursuing a program of this type arises because of the extent of capitation within Sutter, which means “we are on the hook for managing these patients,” Burnich said.
Richard Lopez
Atrius Health
Atrius Health is a nonprofit alliance of six leading independent medical groups in eastern Massachusetts that has created an integrated delivery system that includes both home health care agency and hospice services. Atrius Health provides care for 1 million adult and pediatric patients. The Visiting Nurse Association Care Network and Hospice (VNACNH), which has been part of the system for the past few years, is a wholly owned subsidiary, and Lopez said that its integration with the rest of Atrius’s providers is an ongoing process. This acquisition was deemed necessary to take care of the alliance’s capitated patients through Medicare Advantage, its accountable care organization (ACO) patients through the CMS Pioneer program, and, ultimately, Lopez said, its commercially insured patients. About 35,000 Atrius patients are involved with its Pioneer ACO, and some 25,000 are enrolled in Medicare Advantage. Together, they account for a half billion dollars in risk. The demographic trends and illness projections mentioned by previous workshop speakers are very relevant to Atrius’s strategic planning, Lopez said.
One strong point in acquiring VNACNH, Lopez said, was that its geographical coverage area was relatively congruent with that of Atrius. The availability of both physician services and services from VNACNH allowed Atrius managers to plan effectively and be financially aligned to serve a large, high-risk population. To do that, Lopez said, Atrius has created interfaces that
- Improve communication between home health care providers and physician offices;
- Foster teamwork across providers and disciplines;
- Facilitate the development of a collaborative program designed to meet patient-centered care goals, regardless of payment source; and
- Provide metrics for accountability.
Communication and Teamwork
Although the visiting nurses complete the usual lengthy intake forms that assess patients for everything from the risk of falls to the medications that they take and the presence of depression, these records are often not well incorporated into the patients’ records, Lopez said. Atrius’s electronic health records system ensures that current assessments appear where they are convenient for physicians to access. Practice care managers receive a
weekly email report on clinical data for active patients. The report includes progress toward goals, response to teaching, discharge planning, and any hospice team meeting notes. The report is then distributed to physicians. (Lopez noted that the Atrius system uses encrypted email for communication among providers.)
Atrius has instituted an automated referral system through the electronic health records, so that when a referral is made it goes to VNACNH intake staff, who can then access the patient’s record to set up the case for VNACNH. At present, VNACNH uses an end-of-life information system, and Lopez said that Atrius is considering adopting a home health care module in the next year or two to make records more fully integrated.
A steering committee comprising senior staff oversees the development of the Atrius-VNACNH relationship and clarifies policies and procedures to ensure care coordination and collaboration, Lopez said. In addition, many specific activities have been undertaken to transform VNACNH’s relationship with Atrius Health from one in which VNACNH is a vendor to one in which VNACNH and Atrius have a true partnership.
In primary care practices, Lopez noted that an effort has been made to integrate members of the patient-centered team with VNACNH staff in relevant places along the continuum of care. In particular, work has concentrated on educating practice staff about palliative care and end-of-life challenges, he said. Another specific team-building strategy is “geriatric roster reviews,” which are regular team meetings in the doctor’s office in which case reviews are done for patients identified to be at high risk.
Program Design and Metrics
VNACNH has developed a palliative care consult team that works with the primary care practice and the home health care staff to better manage patients near the end of life, and it also has a robust advance care planning program. According to Lopez, one goal of the end-of-life efforts is to encourage earlier hospice enrollment, contrary to current practice patterns in Massachusetts, which overall has one of the nation’s shortest hospice lengths of stay. “A lot of low-hanging fruit is there,” Lopez said, as Atrius attempts to improve quality and reduce costs of care.
The system has developed a one-time-visit home assessment system paid for not through Medicare but by the physician groups. They assess patients’ homes for safety and adequacy as a care environment. Atrius’s total joint program, also paid for by the physician groups, enables patients to undergo rehabilitation at home rather than in a skilled nursing facility or inpatient rehabilitation facility. Those who can go home with help after knee or hip replacement incur about $3,500 less in care costs and have the same or better outcomes, Lopez said.
Lopez also noted that by using the programmatic flexibility allowed under the Pioneer ACO program, Atrius’s VNACNH staff help patients who end up in the emergency department go home with support rather than experience an unnecessary hospital admission or referral to a skilled nursing facility.
According to Lopez, other program initiatives in some stage of planning or initial implementation include the following:
- Expansion of telehealth care for congestive heart failure patients beyond the Medicare episode;
- Implementation of physician/VNACNH visits by video and through the use of remote diagnostic technology; and
- Expansion of home-based primary care, which entails streamlined communication and scheduling as a team.
The philosophy underlying all these programs is one of care management and not medical management, Lopez said, and home visits are based on need, not insurance coverage.
The results of this integration of home health care and Atrius Health’s physician practices are being assessed monthly through the use of measures examining cost and utilization, quality, and the patient experience. Lopez said that the data collected for the Pioneer ACO and Medicare Advantage patients receiving VNACNH home health care services indicate that in comparison with the outcomes in previous years,
- Hospital readmission rates are down;
- VNACNH is providing an increasing proportion of home health care;
- Eighty-five percent of patients admitted to VNACNH are screened for the risk of falls and for depression (with the outcome of the screening being documented in the electronic record); and
- Ninety percent of patients have had a discussion about medicines, pain management, and home safety.
According to Lopez, work still needs to be done to increase the proportion of patients with advance care planning discussions and documentation and to improve patient satisfaction (84 percent of patients give the VNACNH a rating of 9 or 10).
In the future, Atrius Health is considering developing an internal bundled payment system, providing clinical pharmacy management in the home, and more fully integrating home health care and hospice services with the system’s existing medical record system. The system will continue
to work on its major challenge, Lopez said, of “bridging that communication gap between the doctor’s office and the home.”
EXPERIENCE OF THE VISITING NURSE SERVICE OF NEW YORK
Rose Madden-Baer
Visiting Nurse Service of New York
The Visiting Nurse Service of New York (VNSNY) is the nation’s largest not-for-profit home health care organization, Madden-Baer said. It offers home health, hospice, and palliative care; Medicare Advantage; a managed long-term care plan; paraprofessional and private duty nursing; and aide services. On any given day, she said, approximately 66,000 people are under the agency’s direct or coordinated care, and in 2013, its staff made some 2.3 million clinical visits for patients of all ages.
VNSNY is involved in a number of acute, post-acute, and community-based care models for population health, and according to Madden-Baer, the agency has a dual imperative to transform itself from not only providing excellent home health services to also using its expertise to develop centers of excellence around care coordination and to provide new models of care as alternative payment structures develop. “We use our care coordination expertise as a laboratory for development and testing of new community-based health care models,” Madden-Baer said. The vision is to be the region’s best-in-class not-for-profit community-based integrated delivery system so that it may play a role well beyond that of a traditional home health care agency.
VNSNY Platform
The platform that VNSNY has developed is used for the coordination of population care, management of delegated care, and population health, depending on the needs of particular programs or clients. The platform covers the following:
- Evidence-based tools;
- Person-centered goals and care plans;
- Nurse-conducted assessment and care coordination;
- Health coaching and support;
- Collaboration with primary care and other providers;
- Financial and clinical outcomes measurement and reporting; and
- Predictive analytics and risk stratification.
At the center of all these activities is the individual patient and his or her family, Madden-Baer said, whom VNSNY staff interact with in multiple ways: face-to-face, by telephone, and electronically. These interactions are based on a person-centered goal and care plan that includes opportunities, goals, and interventions.
A set of predictive analytics has been developed with the agency’s research center. These tools allow the stratification of patients into low-risk, rising risk, and high-risk categories. The type of risk may vary, she said, from risk for hospitalization to risk for care management, for example. The agency uses a care management documentation system (not a home health care documentation system) that includes a comprehensive health risk assessment and also has the New York State–mandated uniform assessment tool embedded in the system. Data from the risk assessments contribute to the calculation of the risk score. Madden-Baer said that once a person is appropriately categorized, the agency uses a “dosed mix” of interventions and evidence-based tools to improve patient activation, depression symptoms (as applicable), and medication adherence.
Workforce
Madden-Baer noted that patient assessments are performed by registered nurses (RNs) who are trained in a 12-week intensive program at the Duke University School of Nursing to be population care coordinators. Their training modules cover topics such as care transitions, evidence-based practices, social determinants of health, health literacy, sociodemographics, and biopsychosocial issues. The RN population care coordinators lead teams that include NPs, psychiatric NPs, pharmacists, hospital-based RN liaisons (who, in some cases, serve as transitional care coordinators), social workers, and health coaches. In addition, they work with a wide range of other health care providers and organizations as needed.
The health coaches, who are trained in Eric Coleman’s Care Transitions Model, not only provide health coaching and patient navigation but may also accompany high-risk patients to their first primary care appointment and ensure that patients understand the medical terminology and patient-provider discussion. The health coaches can help address health literacy barriers, Madden-Baer said, because they often come from the same community as the patient or speak the same foreign language.
New Projects
VNSNY is engaged in two CMS demonstration projects on bundled payments, Madden-Baer said, and is embarking on a hospital-at-home project with a large academic medical center. Some health plans have delegated
their disease management services to VNSNY, for example, for diabetic and prediabetic enrollees. The agency is working with ACOs and health plans to provide posthospitalization transitional care. It has two projects under way to provide health and wellness services with behavioral health support for posttraumatic stress disorder and reconnections to primary care services for people affected by Hurricane Sandy. VNSNY also provides care coordination for the largest managed long-term care plan in the state.
New York State has sponsored a major initiative, the Delivery System Reform Incentive Payment Program, to encourage care coordination, attention to social determinants of health, behavioral health, and better management of services for Medicaid recipients and recipients dually eligible for Medicare and Medicaid. Madden-Baer said that at present VNSNY is partnering on at least 11 different projects, drawing on the agency’s expertise in population health and the coordination of care.
Successes and Challenges
According to Madden-Baer, factors that have been important to the success of the agency are the use of evidence-based tools, commitment to staff training at all levels, a partnership with a leading academic institution to conduct training, the use of standardized approaches across service lines, and the use of interventions tailored to the specific needs of patients.
The agency’s challenges, said Madden-Baer, are the current reimbursement model, the need to change the perception of VNSNY—internally and externally—to recognize that it is more than a home health care agency, and the need to capture data for program monitoring and evaluation.
Eric C. Rackow
Humana At Home
According to Rackow, Humana is pivoting from a health plan to a health care company, creating an integrated care model to support its members. Humana At Home manages a suite of programs intended to provide care for older adults with multiple chronic conditions and functional, behavioral, or cognitive limitations. It has 60 home health care clinical offices in 13 states and almost 15,000 employed and contracted field care managers in its nationwide network. It has developed a national database that care managers can use to link members to local organizations that provide a range of supports, from Meals on Wheels to audio books for the blind and an online portal to support family caregivers. Rackow said that the program currently manages 600,000 Humana members who
are in Medicare Advantage programs, Medicare Advantage special needs programs, or Medicare Advantage programs for individuals who are dually eligible for Medicare and Medicaid.
Pyramid of Services
The organization provides programs for managing individuals with an escalating intensity, depending on their functional and activity limitations as well as the number and severity of their illnesses (see Figure 6-1). Patient management starts with a telephonic program that offers in-home support when needed. About 25 percent of the population served by the telephonic program has an in-home visit to assess the home and the patient’s circumstances, and about 10 percent has ongoing, in-home care management.
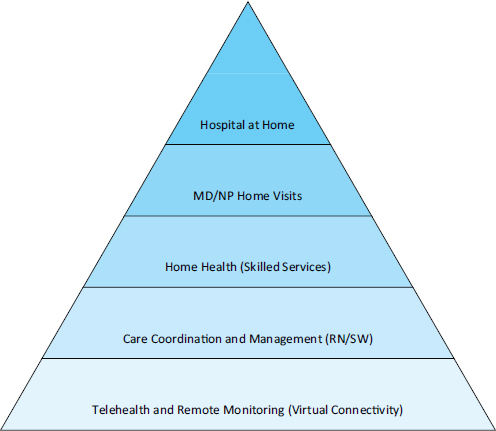
FIGURE 6-1 Humana At Home’s goal for a range of home-based services. NOTE: MD = medical doctor; NP = nurse practitioner; RN = registered nurse; SW = social worker.
SOURCE: Reprinted with permission from Eric Rackow, Humana At Home.
As other workshop presenters have emphasized, Rackow said that Humana At Home focuses its services on care coordination and management for the sickest 25 percent of members who drive almost 80 percent of the program’s costs. “We are not going to solve this in the hospital,” Rackow said. They target this population through the Humana At Home Chronic Care Program, which is an ongoing care management program for this population with critical needs, complex illnesses, and multiple chronic conditions. To identify the members most at risk for future severe illness, Rackow said, the organization looks at both the presence of chronic illnesses and functional limitations affecting ADLs. In Humana’s experience, impairment of functionality “drives health care utilization and cost in the chronically ill, especially in seniors,” Rackow said.
Humana’s home health care pyramid begins on a base of telephone counseling, Rackow said, and then the middle levels of care use licensed home health aides to provide personal health care support. Furthermore, Humana is developing a program that provides skilled services that will be certified by Medicare. Care managers and members involved in the in-home personal and skilled care program have the additional support of community health educators, social service providers, behavioral management professionals, and an interdisciplinary care team of consultant nutritionists, pharmacists, and physicians.
At present, the top of the pyramid is the home delivery of physician services. This represents a distinct evolution from care coordination to direct clinical care. Ultimately, the organization sees developing these increasingly intense services all the way up to a hospital-at-home model. Humana At Home also offers a 30-day transitions program with three visits—one in the hospital before discharge, one within 48 hours of arriving home and before the primary care appointment, and a follow-up visit after that appointment. According to Rackow, at the time of his presentation at the workshop, some 30,000 Humana members had been served by that program.
Results
According to Rackow, 2013 data for the 116,000 members newly involved in care management showed a 42 percent decrease in hospital admissions, and the data for 2014 available to the time of his presentation showed a similar reduction. Among the 16,000 members participating in the posthospitalization transition program, 2013 data showed a 39 percent reduction in hospital readmissions, a decline that, again, was replicated in 2014, he said.
“But is keeping people out of the hospital the right thing to do?” Rackow asked. Humana data show that management at home not only is decreasing hospitalizations and readmissions but also is having a beneficial
effect on patient mortality. Compared with the survival of matched control patients, those members involved in the chronic care program had a 2.8 percent absolute improvement in survival.
The country is in the middle of a paradigm shift, Rackow concluded, from a situation in which care is provided for acute conditions to one in which care is provided on a chronic basis, from a situation in which medical events trigger care to one in which medical events trigger holistic support, from a mind set in which health care is oriented toward a cure to one in which it is provided to enhance the patient’s function, from fragmented care to integrated care, from a situation in which payment is provided per care episode to one in which payment is provided for a continuum of care, and from a situation in which care is provided in person to one in which it is provided virtually. A key element in this shift, he said, is the movement of the site of care from a hospital to the home.
EXPERIENCE OF OPTUM COMPLEX POPULATION MANAGEMENT
Ronald J. Shumacher
Optum Complex Population Management
Optum Complex Population Management is part of the UnitedHealth Group family of companies and a direct care delivery and care management business. (Other lines of business of Optum include data analytics, pharmacy benefits management, health care financial services, and consulting.) Like the other organizations that were described at the workshop, Shumacher said that Optum also serves a high-risk, vulnerable population that has high health care costs because of its utilization of hospital and emergency care. This population is poorly served by fragmented care and the lack of coordination of care for multiple chronic conditions and receives inadequate care at the end of life, he said. Typical Optum clients are managed care plans and, increasingly, programs for dually eligible individuals that delegate the delivery of services for their high-risk populations to Optum.
Although Optum has a range of programs for people who are in transition, have long-term service and support needs, or need palliative or end-of-life care, Shumacher focused his comments on Optum’s Care Plus community program, a longitudinal home health care delivery model provided largely by NPs but with some services provided by physicians. Like the other programs described at the workshop, Optum uses data analytics to stratify patients on the basis of the risk of future service utilization and costs. “Essentially,” Shumacher said, “we are providing a house call program with home-visiting providers that is paired with a care management and technology company to serve high-risk individuals.”
The traditional approach within managed care for members with medically complex, multiple chronic conditions, Shumacher said, “really under-performs in a lot of ways.” It entails numerous providers, patients receive many different medications, care is disjointed and confusing, and sometimes, elements of care plans are contraindicated or conflicting. Usually, he said, in-office medical care is insufficient both in time and in quality for these patients. Doctors do not receive the right insights, and patients do not develop the relationships with their clinicians required for the care of medically complex conditions.
In contrast, Shumacher said, Care Plus is a system that delivers clinical care and that is adaptable to all types of payers. It provides proactive, preventive maintenance and disease education services to teach people how to manage their care better. It uses care providers—NPs who work with the patients’ primary care physicians—who can manage care in the home and write orders for laboratory tests and medications. They engage in advanced discussions with the patient about the patient’s illness and explain different care options. A centralized care management team provides back office support.
The NPs specialize in having patients avoid unnecessary hospitalizations and emergency department visits. Similar to other models in various markets, Shumacher said, the baseline hospitalization rates for its population of patients are high but the use of in-home care services has helped achieve a reduction in hospital admissions of more than 60 percent. Furthermore, Care Plus can reduce overall health care costs for members with medically complex conditions by 42 to 52 percent compared with the costs for members whose care is not managed. In addition, as these extremely ill individuals approach the end of life, their rates of health care service utilization and costs are much lower than those for all Medicare patients, especially high-risk Medicare patients. In the last 6 months of life, Shumacher said, Care Plus can reduce costs by 61 percent. In addition, when they are asked to rate their satisfaction with the services of Care Plus, patients and families give Care Plus high scores.
In the future, in addition to working with managed care organizations, Care Plus could work with delegated provider groups, ACOs, and state and federal government programs, instead of only through health plans, Shumacher said. Care Plus is typically paid on a case rate per engaged member per month. However, it can be paid on a capitated basis, through a gain-sharing program with quality goals, and through a system in which some customers assume the full risk and take a percentage of the premium.
EXPERIENCE OF THE CAPABLE MODEL
Sarah L. Szanton
Johns Hopkins University School of Nursing
Szanton discussed the challenges faced by people with functional limitations that affect ADLs and how a project at the Johns Hopkins University School of Nursing works to improve function for many clients. (See Box 6-2 for a story related by Szanton.)
Szanton said that the Community Aging in Place—Advancing Better Living for Elders (CAPABLE) model6 was developed with foundation and federal support and is now being tested under a Center for Medicare & Medicaid Innovation (CMMI) grant and through a randomized controlled trial funded by the National Institutes of Health. If these tests are successful, she said, the program may be implemented nationwide. “CAPABLE focuses directly on people’s own functional goals, with the idea that if we address those, then they can take care of their medical issues,” she said. It is client directed and not just client centered, and the clients’ goals are exemplified by the following: “I want to be able to get up my stairs, so I can sleep in my bed instead of on my couch.” Or, “I want to be able to stand long enough to be able to eat some foods, so I don’t have to go back to the hospital.”
Program Approach
By and large, program participants are low-income, dually eligible individuals recruited from community centers and mailings, but they are at high risk for functional limitations. CAPABLE provides clients with a team member who can make household repairs, a nurse, and an occupational therapist over 4 months. The initial visit is with the occupational therapist. In traditional home health care, occupational therapists cannot start a case, but in this model, function is the driver, and that is what occupational therapists address best, she said. They assess client needs for every ADL and instrumental activity of daily living (IADL), and then the clients prioritize those needs that they want to be addressed.
On the second visit, the occupational therapist goes through the whole house, examining all the areas that the client uses and assessing the causes of the client’s limitations. The assumption is that “a limitation is a combination of what a person’s qualities are and what the environment throws at them,” Szanton said. “If you can give them grab bars or if you can fill in
______________
6 See http://nursing.jhu.edu/faculty_research/research/projects/capable (accessed December 24, 2014).
BOX 6-2
Mrs. B’s Story
Baltimore, Maryland, resident Mrs. B has hypertension, congestive heart failure, diabetes, and arthritis. She was recently hospitalized for an exacerbation of her heart failure and just finished an episode of post-acute care in a skilled nursing facility. Like a cascade of dominoes, the precipitating heart failure problem occurred partly because she cannot stand up long enough to cook and cannot get groceries in the house. Therefore, she often eats some kind of prepackaged food, which tends to be a high-salt food, that she can just grab.
She keeps her clothes in her dining room, because that is where she lives. She can no longer climb the stairs to her bedroom. She cannot even really get dressed, because this “closet” is a sweater bag that is held together with safety pins, and her arthritic hands cannot undo the pins, Szanton said.
When first contacted by the CAPABLE program, Mrs. B was spending most of the day, every day, sitting in a chair. Holes in her floor made it dangerous to walk on. The Astroturf covering of the steps from the sidewalk to her front porch was ripped and hazardous. “None of us should walk up those front stairs,” Szanton said, and certainly not someone with a shuffle, gait problems, and bad balance. Older adults who have lived in the same place for a long time and who do not have money to fix problems often similarly have houses that are starting to fall apart.
Although the expense associated with functional limitations is well-known, the impact of the home environment on people’s function and how environmental improvements can reduce limitations in activities of daily living receive less attention. Mrs. B—and people like her—want to be more functional and often can be. CAPABLE program case management considered questions like the following: can she get her foot over the side of the bathtub, can she stand long enough to cook, and can she get dressed? These are often the issues that older adults care about more than their diseases, and these needs are mostly unaddressed.
What Mrs. B most wanted was to be able to stand long enough to make her meals. The CAPABLE program team tackled the problem: the nurse worked on her arthritis pain and her leg strength; the occupational therapist worked with her on the use of different cooking tools and ways to conserve energy; and the team member who made household repairs lowered the kitchen shelves, put in a microwave, and gave her a crock pot. These are simple steps, and all were related to achieving her goals.
SOURCE: As presented by Sarah Szanton on September 30, 2014.
the holes in their chair seats, sometimes they no longer have limitations.” Together, the therapist and client fill out a work order for the person who will make household repairs, who tackles jobs in the client’s priority order within a budget of $1,300. (Installation of a second banister is one of the most common requests, Szanton noted.)
At the end of the first month, the nurse starts. The nurse does not do anything about medication adherence, diet, or exercise unless it is the client’s goal. The visits—six in total for the occupational therapist and four in total for the nurse—continue, with the occupational therapist and nurse working on a different goal at each visit. If a client has fewer goals, the program stops.
Results
The program has been pilot tested and may be ready to be scaled up, Szanton said. According to Szanton, the pilot tests showed that the one-time cost of the 10 professional visits averages $3,300 per enrollee, including travel, clinical care coordination, and home repair and modification. In contrast, nursing home care costs about $75,000 per year. If CAPABLE prevents even 3 weeks of nursing home care, she said, it has saved money; if it can avert hospitalization for one client in every five, it has saved money.
“As you can imagine,” Szanton said, “the clients love it.” One of the best program outcomes is decreased depression. Depression lifts because people can do what they want to be able to do, she said. For example, they can bathe themselves, they are cooking, and they are getting out of the house to go to church. “It’s depressing to sit in a chair all day long.” For most participants, the level of depression decreased or at least did not increase.
Rates of occurrence of functional limitations also followed a downward trend, Szanton said, with the number of functional limitations decreasing from an average of about four to about two, with almost 80 percent of clients seeing improvements in functional limitations and only 7 percent seeing declines. Szanton expects that stronger results would emerge with a post-acute care population.
In closing, Szanton described the following example. One client was taking 26 medications when she started the program. On the occupational therapist’s first visit, it took 30 minutes for the client to walk the short distance from the bathroom to her bedroom, yet her goal was to go downstairs and wash her hair in the kitchen sink. “This shows the power of asking people what they want to be able to do,” Szanton said.
An open discussion followed the panelists’ presentations. Workshop participants were able to give comments and ask questions of the panelists. The following sections summarize the discussion session.
Policy and Payment
Lee asked the panelists what kinds of health policy changes are needed, particularly in Medicare, to facilitate the more appropriate use of home health care. For example, she asked, for those who received CMMI grants, were any Medicare rules waived? Rackow said that CMS needs to recognize functionality as an important component of keeping people healthy. At present, he said, Medicare does not reimburse for home health aide services that support beneficiaries’ functional needs; it reimburses only for medical care, yet much health care utilization and cost are driven by those problems with function. Madden-Baer noted that for a congestive heart failure project that VNSNY is running with 50 hospitals, beneficiaries are not required to be homebound after the initial episode of care from a certified home health agency, as is usually required for subsequent care under the 90-day bundled payment. Also, the home health agency has the flexibility to engage a pharmacist consultant to simplify dosing schedules and to deploy NPs to the home when an appointment with a primary care physician is unavailable.
Boling suggested that the framework that focuses on chronic conditions be abandoned, because almost all elderly people have at least two chronic conditions. Instead, he said, the focus should be on function-limiting chronic conditions. He also advised that the expansion of the scope of various projects be managed, because if it is not, a project soon becomes unaffordable. The monitoring present under the CMMI grant helped Burnich’s project avoid this tendency to expand. He said further that projects should not expand faster than the speed with which they can hire staff with the competence and skills to produce high-quality, reliable services. Rackow said that Humana has best practices and protocols that precisely define the amount of services, the time to be spent on those services, and the costs that the health plan pay per member per month, which, again, establishes boundaries.
Lee further asked what approaches to payment might be critical for future reforms. Capitated payments allow organizations to make the best decisions to support the health of their members, Rackow said. At present, access to a program like Humana’s is limited to people enrolled in particular health plans and using particular provider groups. Shumacher said that programs that have strong results could be made more available to broader groups of people under a payment-for-value rubric.
Medicare Advantage is growing rapidly but under the ACA has built in some payment cuts that will discourage plans and providers from participating, Burnich said. Despite the advantages of capitation, not every senior will join Medicare Advantage, he said, and his organization is experimenting with other types of chronic care management programs.
Consolidation and Integration
A workshop participant asked if additional consolidation and integration of home, community, and post-acute care services will drive value. The participant further asked about the importance of integration in and of itself.
The company acquired by Humana that is now Humana At Home would never have been able to scale up its home health care program without being under the Humana umbrella, Rackow said, according to either its national coverage or the number of clients. Because of Humana’s support, the Humana At Home program has expanded its horizons, seeing home health care as “the glue in the system” for keeping people as healthy as possible.
Lopez said that integration has been important to Atrius Health on multiple levels: alignment of mission and care delivery goals, provision of a financial bottom line, communication, and medical information sharing. Although Atrius could have worked with several visiting nurse associations in eastern and central Massachusetts instead of just one, he said, the alignment, goals, and financial and communications issues would have to have been worked out with each one of the associations and would have been burdensome.
The blurring of distinctions between providers and health plans, Burnich said, creates some risks. In the 1990s, plans that began serving as providers failed. The renewed trend “could be good,” he said, “but we will have to see.”
UnitedHealth Group’s acquisition of INSPIRIS gave Optum increased ability to implement a successful delivery model that could reach many more payers and their members, Shumacher said. The bringing together of disparate businesses and the creation of a common platform take time, so it may be a while before the full value of integration can be realized, he said.
Madden-Baer said that VNSNY, being both a provider and a health plan, is learning to be “a lot less transactional and more care management focused” over the longer term. An example is the shift in the call center’s approach: it supports the management of care when a patient calls, instead of instinctively advising patients to call 911 after hours.
Operating at a Smaller Scale
Terrence O’Malley, Massachusetts General Hospital, asked the panelists what lessons from their organizations can be applied to organizations that operate on a much smaller scale.
Telephone and telehealth care coordination, supported in various ways,
can be scaled down, said Rackow. Humana is testing interactive voice response systems with patients with congestive heart failure.
Madden-Baer said that VNSNY’s home health care program started small and thought of itself as a laboratory for testing models of care, which have been added over time and which have allowed the evolution of VNSNY into a much larger organization.
Technology is not the be-all and end-all, because “the warm touch is still a critical component,” said Burnich, but there are ways to scale down through the use of technology, including through the use of sensory devices and video visits, for example.
A good first step for smaller agencies is to start tracking their data, Shumacher said. If they can show that they are providing better care, that quality is improving, and that costs are going down, they can grow from there. “A lot of what I talked about,” Szanton said, “you can do for free.” Just rephrasing the questions about function and asking the person about his or her goals are free. Home repair is going to provide such a strong return on investment that even with low levels of capitation, it can easily be provided. She suggested the mobilization of healthy older people who have skills, who have some time, and who may be eager to help fix up other people’s homes.


























