
2
Human Health
INFLUENZA AS A GLOBAL CHALLENGE FOR HUMAN HEALTH RESEARCH
Todd Davis opened his remarks by emphasizing to participants that the influenza virus is very complex: There are multiple types of influenza, A and B being the most common genotypes. Among these types are many, many different subtypes of influenza. To date, as many as 18 different hemagglutinin (HA) genes have been detected. The influenza A viruses have potentially 11 neuraminidase (NA) genes. Two influenza A viruses have been detected in bats recently. These are, to date at least, viruses that have not been replicated in any in vitro or in vivo systems. Aquatic birds are believed to be the reservoir for these viruses, because all of these HA and NA subtypes, with the exception of the bat influenza viruses, have been found in aquatic birds. These viruses have crossed over to mammalian hosts and avian hosts, primarily terrestrial poultry, as well as to humans. This is just a very cursory overview of all the animals that have been infected by these viruses, there is a growing number of hosts susceptible to influenza viruses.
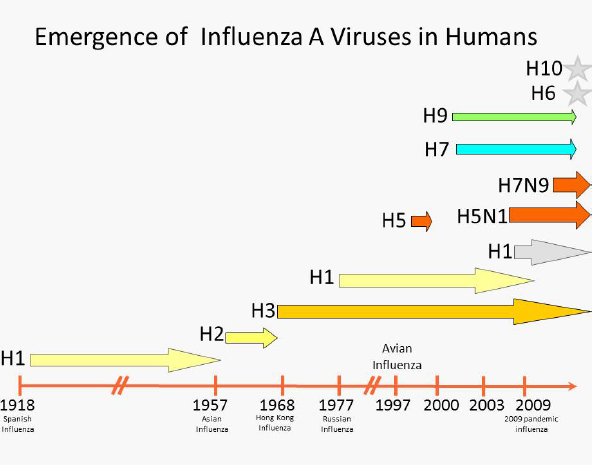
Davis displayed a diagram showing the timeline of influenza A viruses that have been detected over the years in humans (see Figure 2-1).
Other novel influenza A subtypes have recently been detected in humans, namely H10 and H6, found in parts of China and Taiwan. More and more examples of these influenza A viruses and subtypes can be found in humans with the potential to cause pandemic disease.
SOURCE: Todd Davis, presentation at the workshop.
As a segmented RNA virus, influenza is capable of evolving very rapidly, and does so via mechanisms such as mutation, recombination, and reassortment. Mutations occur through misincorporation of nucleotides in the absence of a proof-reading mechanism. Recombination is a rarer event, but does occasionally occur and can also lead to the development of highly pathogenic strains. The recent highly pathogenic virus that circulated in Mexico in 2014 is a good example of how recombination of a low-pathogenic virus can result in the circulation of a highly pathogenic virus. Reassortment involves two distinct viruses infecting a single cell, with the resulting progeny having swapped gene segments. Unfortunately, this is a common occurrence in influenza viruses and something that contributes to the pathway of transmissibility from animals to humans.
Influenza viruses are characterized by their surface receptors which are noted as alpha-2,3 sialic acid-linked (α-2,3) receptors and alpha-2,6 sialic acid-linked (α-2,6) receptors. Several key differences are important to recognize, mainly the α-2,3 linked receptors bind well to the avian host cells, and are thus avian-like viruses, versus the α-2,6 linked receptors which bind better to human host cells and are considered human-like viruses. Pigs function as a so-called mixing vessel. They are susceptible to being infected by both the avian and the human-like viruses, which experts believe has resulted in genetic reassortment, resulting in swine-like flu and leading to at least three previous pandemics, including the H1N1 pandemic of 2009. A great deal of the work Davis’s group conducts with U.S. Department of Agriculture focuses on understanding what is occuring in the animal host and understanding the evolutionary mechanisms that drive the adaptation of these animal viruses to circulate in human hosts and potentially lead to pandemic disease.1
This becomes important to human health because over the years there has been an increase in the number of human infections with the so-called variant swine viruses. For many years there were sporadic cases on the order of one or two cases per year. In 2012, there were more than 200 cases of an H3N2 swine variant virus, which resulted in many human infections, primarily in young children that were visiting agricultural fairs who came into close contact with pigs. Subsequently, due to public health messaging, the number of human cases of swine influenza has declined in the past 2 years. In 2013, there were only approximately a dozen cases, and as of November 2014, there were only three cases. Experts do not fully understand why this spike occurred and then declined in human cases, but it is of significant concern, considering the ability of these viruses to transmit easily to humans.
Prior to the 2009 pandemic, it was clear that there was a large number of reassortments in genotypes circulating in swine populations.
_____________________
1 There is a great deal that is still unknown about the avian influenza virus. The Centers for Disease Control and Prevention has received a few of the H7N9 viruses from China, Hong Kong, and Taiwan and has been able to characterize some of those viruses and use them for vaccine development.
SOURCE: Todd Davis, presentation at the workshop.
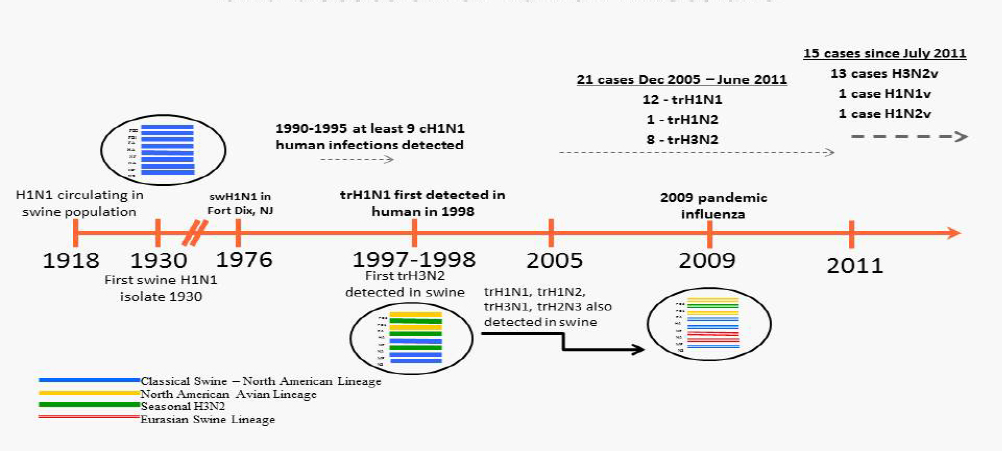
However, after 2009, and perhaps from reintroduction of the 2009 H1N1 back into the pig population, there has been a very comprehensive and confusing reassortment of the pandemic H1N1 genes into the already reasserted H3N2 virus backbone. Figure 2-2 shows the current understanding of influenza A viruses in pigs. Further understanding becomes increasingly difficult as more and more of these viruses continue to reassort.
With this background, Davis turned to the primary focus of his presentation, the H5N1 viruses in the context of biosafety and biosecurity. Currently, more than 60 countries have experienced H5N1 either in bird outbreaks or in human infections. Cambodia, China, Egypt, Indonesia, and Vietnam continue to struggle with the containment of the virus in poultry. Consequently, a large number of human infections have occurred in these countries. The genetic diversity within the H5N1 viruses creates a very complicated story. The term clade is used to describe the set of viruses that evolved from a common ancestor virus. In the early days of the H5N1 outbreaks that were primarily restricted to China and South East Asia, there was limited genetic diversity. As this virus has continued to spread and evolve over time, more clades have developed. A very large number of these clades have not yet been classified, which makes diagnostics, vaccine development, and the clinical picture difficult to address.
Human and animal virus surveillance, virus isolation, and genetic sequence generation feeds into sequence databases. Bioinformatics and
phylogenetics are used to understand the evolution of these viruses. As more is learned about the molecular features of these viruses, this information is fed into gain-of-function research where reverse genetic studies or other types of methods are used to actually pinpoint mutations, which are important to a specific phenotype of that virus. This information then feeds back into the molecular-based risk assessment, which then contributes to public health countermeasures. Such measures include diagnostics, candidate vaccine virus development, antiviral drug development, and ultimately biosafety considerations as well. Centers for Disease Control and Prevention (CDC) depends a great deal on molecular-based surveillance to inform decision-making, and in some cases even policy.
Davis then turned specifically to a recent example in Cambodia. In 2013, there was an unusual anomaly of 26 human cases of the H5N1 virus in comparison to only 21 human cases detected in Cambodia for the previous 7-year period.2 In the context of the increase of human cases, there were also genetic mutations identified in the hemagglutinin gene of these viruses, two of which were associated with increased transmissibility in a ferret model. These two particular mutations have been described by both Ron Fouchier’s lab and Yoshi Kawaoka’s lab as being important for the aerosol transmissibility of influenza viruses in a ferret model.3 Having seen these two mutations appear in the Global Initiative on Sharing All Influenza Data (GISAID) database, Davis and his group reached out to colleagues at the Pasteur Institute in Cambodia.
They started an epidemiological investigation to determine whether other viruses that had been isolated from humans in Cambodia might have also had these two mutations. The concern was that there may be some increased transmissibility that may have led to the increase of human cases. The possible reasons for this were not clear, although there is speculation that there was increased circulation of the virus in poultry or the environment. Potentially, there was increased testing in humans, and there was certainly improved clinical awareness about H5N1 in the country. They were dealing with a novel genotype: a virus that had
_____________________
2 For more information, see: https://www.cambodiadaily.com/archives/newmutation-in-bird-flu-virus-in-cambodia-54896/; accessed April 10, 2016.
3 For a brief overview of this research, see: http://www.nature.com/news/therisks-and-benefits-of-publishing-mutant-flu-studies-1.10138; accessed April 10, 2016.
acquired internal genes from a different H5N1 virus and had some unique properties.
Davis spent several weeks in Cambodia to try to understand the scope of this potential problem and then to conduct risk assessments, both in Cambodia and in Atlanta. They started by looking at the specific mutations in the hemagglutinin genes of H5N1 viruses that were detected in Cambodia.
The mutations shown in Figure 2-3 are noted in red, along the phylogenetic tree. Some of the mutations were conserved in all of the H5N1 viruses circulating in Cambodia in 2013, and some were found only in unique viruses.
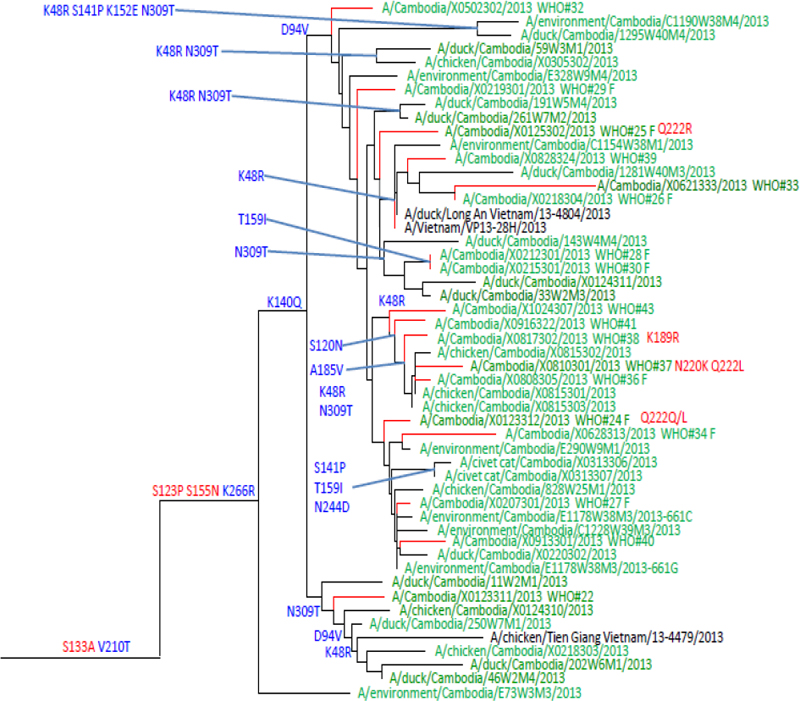
SOURCE: Todd Davis, presentation at the workshop.
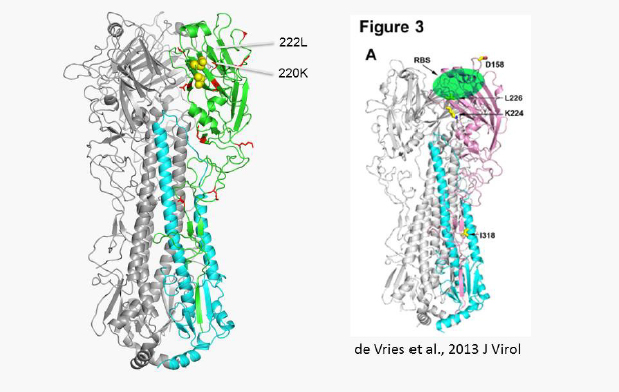
Figure 2-4, depicts WHO Case Number 37, which was a human infection obtained through aerosol transmission. Gain-of-function research detected two markers for mammalian adaptation that had been conducted, as well as other mutations that had previously been described in gain of function studies to enhance α-2,6 receptor binding specificity.
Eleven of the 26 specimens from Cambodia were sent to Atlanta, where Davis’s group attempted isolation from those 11 specimens. Nine viruses were isolated for additional characterization. They were particularly interested in knowing if any of the mutations had been detected in poultry or in environmental samples that had been collected in 2013. It became apparent from the beginning that these mutations were restricted only to human infections of H5N1. Follow-up investigations by the Cambodian Ministry of Agriculture, in response to the human cases, provided viruses that were also isolated. Even samples from the same flocks that may have been implicated in cases of human exposure did not have these mutations. That was very good news.
SOURCE: Todd Davis, presentation at the workshop.
Davis’s group wanted to try to understand, using more specific assays, whether these viruses might have a shift in receptor-binding specificity that could have been predicted based on the mutations. They used analogs of the sialic acid glycan receptors in a glycan array model to understand how these viruses behave, at least in an in vitro detection system. Davis found that many of the viruses in the isolates they made existed as quasispecies, or mixed-based populations, in the viruses. Using traditional plaque assays and plaque purification, they isolated viruses with a glutamine in position 222 versus an arginine at position 222 and viruses with the serine at 155 versus an asparagine at 155. Both positions, again, have been implicated in the adaptive feature of some viruses to replicate and transmit in mammalian models. Surprisingly, the glycan array data showed that all of these viruses, regardless of the single mutations, had specificity that was very similar to a typical avian H5N1 virus. They used the Vietnam/1203 virus as a control, and even with the mutations that were found, these viruses still displayed an avian-like receptor-binding specificity.
One of the disappointing findings from this study was that the virus happened to have the two mutations associated with the aerosol transmission as identified by Imai et al. in their ferret transmission studies. Unfortunately, the position 222 from a glutamine to a leucine was lost after egg isolation. Therefore, Davis’s group was never able to replicate that virus due to the loss of that marker after passage in the avian egg host. They used much of this molecular data to inform additional studies and additional characterization of influenza viruses as a means of understanding how they behave antigenically.
A large part of what Davis’s lab does at CDC is to understand how well a vaccine might cover a specific virus. Therefore, they conducted additional studies to determine how this virus with the ferret-transmissible mutations would be protected by ferret antisera generated against a small panel of reference antigens. Using a ferret model, they inoculated the animals with these viruses and produced antibody against the specific viruses. Then they looked at the antigenicity of the profiles of test antigens relative to some of these strains.
When they compared these strains to the Vietnam/1203 vaccine candidate, several of these viruses had at least a fourfold, and in some cases an eightfold, reduction in viral load. Whereas using the Cambodian virus detected in 2013, all of the new viruses from 2012 and 2013, the vaccine candidate tended to react equally, as did the vaccine produced against X081301, a reference strain. Using the molecular data and
incorporating the antigenic data, CDC can propose or recommend the selection of certain viruses for vaccine development, either for seasonal virus vaccine development or for prepandemic vaccine development.
This usually leads to production of a small pilot lot. Many of the H5N1 vaccine candidates, as well as H7N9 vaccine candidates (for example, some of the swine influenza vaccine candidates), have been developed as pilot lots. Some have been tested in Phase 1 clinical trials to understand the immunogenicity of these viruses should they be needed in response to pandemic disease caused by these viruses.
Davis then mentioned, in the context of this discussion, that all of this begins in a biosafety level 3 (BSL-3) enhanced laboratory for the highly pathogenic viruses, in particular, but also for any exotic low-pathogenic avian influenza viruses or other exotic animal influenza viruses. All of the initial work, even the extraction of virus RNA, is performed in a BSL-3 enhanced laboratory. After the initial work, further steps (e.g., cloning, sequencing, and screening of constructs), are conducted in a BSL-2 laboratory. Then, due to the features of these viruses, the transfected virus goes back into a BSL-3 enhanced laboratory, where the virus is harvested, passaged in eggs, and stored and titrated.
At that point, they assess biosafety risk and reclassification, which generally involves several different safety assessments. The first safety assessment is performed in chickens at the USDA’s Southeast Poultry Research Laboratory, where they determined that the multibasic cleavage site that has been removed in the vaccine no longer causes clinical illness in chickens. The vaccine passes an intravenous pathogenicity index test demonstrating a lack of a highly pathogenic phenotype in this animal model.
Meanwhile, Davis’s CDC group also conducts studies in Atlanta to examine the lack of a trypsin-independent replication. They want to be able to demonstrate that the virus cannot grow unless trypsin is supplemented in the cell culture media, another feature of a highly pathogenic avian influenza virus. They also look for a lack of chicken embryo lethality, again showing that the virus is no longer highly pathogenic. Finally, they conduct a risk assessment using a ferret model. In this assessment, they look for evidence of reduced pathogenicity of the candidate vaccine virus relative to the parental wild-type strain so that they can demonstrate reduction in clinical symptoms, that is, replication in the respiratory tract to a minimal level or no replication before they can then move into the declassification of these viruses and the
deselection of the virus as a select agent according to the USDA’S Animal and Plant Health Inspection Service and CDC regulations. The vaccine then enters a pipeline where the virus has become a BSL-2 level organism and can be handled by manufacturers for pilot lot production and vaccine development.
This is an ongoing activity that the CDC’s influenza division is involved in as part of its responsibility as a WHO collaborating center.
Davis stated that each of the steps that he discussed in his presentation involved at least three different biosafety lab levels. When considering the necessity for biocontainment laboratories in a surveillance setting, one begins with sample collection. It is essential to have good personal protective equipment (PPE) in the field, and good shipping guidelines to be able to transport viruses from the field into the BSL-3 enhanced laboratory. The molecular assays conducted in a BSL-2 environment are also very important. Davis’s group is trying to use BSL-2 molecular assays to understand more about these viruses before the isolation stage and the additional propagation of BSL-2 and BSL-3 organisms. The Influenza Division of CDC is working to try to improve their advanced molecular detection of viruses from clinical specimens so that they can avoid some of the additional isolation and propagation that occurs in the BSL-3 enhanced laboratory. Finally, vaccine development for zoonotic influenza viruses involves the use of recombinant DNA in research, which is overseen by CDC’s Institutional Biosafety Committee, and animal studies may also involve review and approval by the National Institutes of Health’s Institutional Animal Care and Use Committee.
There is a great deal of transparency regarding dual-use research now at CDC. Even for studies that are not considered to be dual-use research by definition, any research involving select agent work or exotic animal virus work is still submitted for review to be certain that the dual-use committees are aware of the research being conducted, this is a mechanism to provide as much transparency as possible within CDC.
Discussion
The discussion following Davis’s presentation focused on the role of mutations in his study, including those identified in previous studies.
A participant opened the discussion by asking if the reduced transmission, replication, and pathogenicity resulted from dominant mutations or recessive mutations. Davis replied that most of the known mutations are associated with reduced transmissibility and replication.
He thinks most of those are tied to the internal genes of these viruses. The virus that is used as the backbone for candidate vaccine production has known mutations that result in a phenotype that does not replicate well in a mammalian system. In this case, there are many mutations that function together, so it is not possible to say whether one is dominant or recessive; rather, it is a combination of mutations that give these viruses this phenotype.
Davis was asked if his group would have paid as much attention to these two mutations if they had not been previously identified in the ferret model. Davis replied that, no, they would not have paid that much attention to those mutations. Diane Griffin noted that in general it is useful to know about mutations because they may be of future benefit.
David Relman had the same question about the role of previous work studying induced enhanced transmissibility in the laboratory on Davis’s surveillance effort. The 222 mutation was known prior to 2012. Relman wanted to understand what in particular was learned from the Fouchier experiment on induced enhanced transmissibility. Davis replied that his group’s work was initiated because of the combination of the mutations that had not been seen previously in naturally circulating H5N1 viruses. It is absolutely correct that the leucine of position 222 is something that has been known for a long time. It leads to the swing to an α-2,6 receptor binding specificity. The mutation position 220 had not been previously seen in circulating H5 viruses, and it had never been seen in combination with the mutation at 222. This combination of mutations identified in this one virus was the impetus for starting the enhanced surveillance.
Another participant asked if there are patents protecting the sale of viruses based on the reverse genetic method used. Davis replied that these methods are all used within a research environment. If the viruses are distributed to manufacturers, those manufacturers then have to be certain that they understand their legal and financial obligations to the patent holder.
The participant also asked about the disappearance of the mutation. Davis responded that his group did do some next-generation deep sequencing of the virus used for the egg passage. They found that there was actually a low percentage of the avian mutation present in the first passage. Once it went back into eggs, it really shifted and outgrew the more human-like mutation that was identified. It was a quasispecies in the original infection.
CHALLENGES IN DIAGNOSIS OF PATHOGENS AND STATUS OF BIOSAFETY AND BIOSECURITY IN WHO’S SOUTH EAST ASIA REGION
Aparna Singh Shah began her presentation by quoting Dr. Margaret Chan, who said, “Today collaboration to achieve public health goals is no longer simply an asset. It is critical necessity.”4 There are 11 countries in WHO’s South East Asia region, which has six percent of the world’s land area, 25 percent of the population, and approximately 30 percent of the communicable disease burden. Despite this, there is relatively little laboratory capacity. Labs tend to receive low priority, even though they are the cornerstone for the surveillance and detection of communicable diseases.
What are the prerequisites for the detection, containment, and prevention of emerging infectious diseases? Adequate and trained public health staff are needed, as is coordination with other sectors and partners. Strong information gathering capabilities, reliable public health laboratory capacity, and efficient and swift management of public health measures, including logistics, are also needed. Adequate resources are essential to support each of these elements. WHO advocates for the support of various laboratory functions starting with surveillance and diagnostics, which then supports the treatment of patients. With the help of laboratories, WHO shares information and material with the global WHO network.
In 2003, when there was concern about the resurgence of severe acute respiratory syndrome (SARS), there were at least two cases of laboratory-acquired infections (LAIs) from Singapore and Taipei. These incidents drew international attention to the issue of lab biosafety and potential costs associated with the breakdown of lab safety.
In 2005, the WHO Assembly adopted a resolution on enhancement of laboratory biosafety. During the same assembly, International Health Regulations (IHR) were adopted, which came into effect in 2007. The IHR requires the 94 countries who have adopted them to develop minimum core capacities to prevent, protect against, control, and provide
_____________________
4 Margaret Chan, acceptance speech as Director-General of WHO, November 2006. See: http://www.who.int/mediacentre/news/releases/2006/pr66/en/; accessed April 10, 2016.
a public health response to the international spread of diseases and events of public health risk.
Following the adoption of IHR, this region developed the Asia Pacific Strategy for Emerging Diseases (APSED) to meet the challenges of emerging diseases and to provide a framework for compliance with the core capacity requirements of the IHR. The key aspects of APSED involve quality assured laboratories, safe laboratory environments, and safe practices. The APSED was further expanded to include the Asia Pacific Strategy for Strengthening Health Laboratory Services. The components of the Asia Pacific Strategy include biosafety, biosecurity, occupational health, and safety and waste management.
Shah then listed what she called the 11 M’s that are necessary for building laboratory core capacity to detect pathogens safely:
- Manpower
- Machinery (equipment)
- Materials (reagents)
- Methodology (SOPs and protocols)
- Management
- Motivation
- Monitoring and evaluations of techniques and infrastructure
- Maximum containment, safe environment in laboratories
- Matrix or network of laboratories
- Maintenance of expertise (infrastructure)
- Money
Shah continued by pointing out several major issues in health laboratories in the South East Asia region that prevent labs from meeting the 11 criteria. There is limited public health laboratory capacity, which varies from country to country, and not all member states have laboratory policy plans, focal points, or national frameworks for health labs. Not only do many people have limited access to laboratories, but there is also a lack of new technology and an inadequate number of trained staff. There is no continuous supply of reagents, and no systematic assessment of laboratory quality and biosafety. In other words, biosafety and biosecurity awareness and practices are inadequate. In addition, there are few regional and global linkages for technical support and collaborations, as well as inadequate resources. At this time, training is not specifically focused on biosafety and biosecurity: There are few training programs focused on biosafety, and when training is conducted, biosafety is often a
small part of laboratory quality training or it is occasionally combined with training on lab techniques. Designated biosafety officers are also rare, biosafety guidelines are often either not available or poorly implemented, and regular safety inspections and waste management programs are few. Mandatory immunizations for lab personnel are insufficient, and occupational health and medical surveillance programs are rarely mandatory. In addition, safety issues persist, including the following: The processes for biological safety cabinet certifications may need improvement, documentation of safety errors and LAIs are minimal, and often there is an inadequate supply of PPE. Expertise and facilities available to plan and construct BSL-3 and -4 labs exist, but coordination between and among various stakeholders is limited. Likewise, national funds dedicated for biosafety and biosecurity are often limited.
WHO conducts assessments of laboratories under the IHR capacity building program. Self-assessments are vulnerable to being subjective. For example, at times countries have very limited resources, but they report 100 percent biosafety in their facilities. Conversely, some countries have good biosafety measures in place, but they believe that their compliance is closer to 20 percent.
Table 2-1 lists the BSL-3 laboratories in member states. India has BSL-4 laboratories, five member states have BSL-3 laboratories, and almost all countries have BSL-2 laboratories.
Shah also mentioned that WHO has published a popular book providing overall information on biosafety, security, and biorisk management. WHO has conducted many biorisk management trainers’ workshops, as well as regional and national level trainings. Following the outbreak of Ebola, WHO conducted specific training, but none of the member states have facilities to perform laboratory testing of Ebola. WHO also developed a shipment project so that countries can ship their suspected specimens to WHO-designated laboratories; all member states were trained on shipping requirements and core team management.
Through WHO efforts, awareness and involvement of national policy-makers has gradually increased. National laboratory policies that include biosafety components are being developed, and in some countries, there are biosafety assessment committees, even in some of the countries that do not have BSL-3 facilities. Biosafety and biosecurity associations are being formed to foster biosafety and biosecurity practices. They hold regular biosafety trainings, which include sections
TABLE 2-1 Biological Safety Labs in South East Asia Region Member States.
| Country | BSL-2 | BSL-3 | BSL-4 |
| Bangladesh | + | + | - |
| Bhutan | + | - | - |
| DPR Korea | ? | - | - |
| India | + | + | + |
| Indonesia | + | + | - |
| Myanmar | + | - | - |
| Maldives | + | - | - |
| Nepal | + | + | - |
| Sri Lanka | + | - | - |
| Thailand | + | + | - |
| Timor Leste | - | - | - |
SOURCE: World Health Organization, 2014.
on PPE. Training also includes biological waste management, good laboratory practices, and infection prevention and control guidelines.
WHO plans to improve biosafety and biosecurity in South Asia by advocating for the development of national policies on biosafety and biosecurity. WHO also requests that national governments allocate resources to improve the status of biosafety and biosecurity. It assists the governments in reaching this goal by providing technical support for policy development and implementation. Additionally, it has developed and distributed guidelines, and member states are encouraged to form their own SOPs. WHO also assists member states in linking to global expertise by promoting networks and collaborations.
Discussion
The discussion following Shah’s presentation focused on diagnostic capabilities of regional and WHO-designated labs and WHO guidelines for regulatory policy.
A workshop participant asked about diagnostic facilities for Ebola and what capacities exist in the region. Shah replied that WHO
recommends that specimens be tested for Ebola in BSL-3 labs. These exist in Bangladesh, India, Indonesia, Nepal, and Thailand. However, after testing at least 50 specimens determined to be negative for Ebola, and 25 specimens determined to be positive for Ebola, results should be validated in WHO-designated labs. These countries can perform RT-PCR, but again, they need to validate their results by sending their representative specimens to designated laboratories.
Thomas Ksiazek asked how BSL-3 laboratories testing samples for Ebola are obtaining the necessary reagents and whether the tests are being validated. Shah replied that in India, Ebola testing occurred on a regular basis whenever there was a suspected specimen. Indonesia and Thailand have in-house kits for Ebola testing, but WHO and CDC also have provided them with iNtRON kits available for viruses. At times, when a country is not able to procure a reagent, they ask WHO to facilitate procurement. Indonesia is now in the process of sending their specimens for validation to designated labs.
A participant followed up on guidelines developed by the WHO South-East Asia Regional Office (SEARO). How many of WHO SEARO’s guidelines pertain to biosafety and biosecurity, and how many of the member states have actually used the WHO guidelines to develop regulatory policy or specific guidelines that require implementation at their own laboratories or medical institutions? Shah replied that WHO does have information about member states’ regulations. WHO requested that global experts conduct assessments and assist in implementing guidelines. Such assessments were conducted in Bhutan, Myanmar, and Nepal. As far as she knows, all BSL-3 laboratories have their own SOPs and guidelines, however, implementation of these guidelines in peripheral labs is inconsistent.
PERSPECTIVES ON THE WEST AFRICAN EBOLA OUTBREAK
Ksiazek recounted the 6-week trip he took to Sierra Leone at the invitation of CDC in August 2014. He provided some of his personal perspectives on the outbreak in Guinea, Liberia, and Sierra Leone, and described the history of the Ebola outbreak and the filoviruses within Africa (see Figure 2-5).
The first outbreaks of Ebola occurred in 1976, in what was then northern Zaire and southern Sudan. These were actually two different viruses, but that was not known for some time. There were two
simultaneous outbreaks in the same approximate region, bordering the Congo Basin. Since then there have been a number of outbreaks of Ebola in the Democratic Republic of Congo (DRC). The Ebola virus responsible for those outbreaks was the same as that found in the 2014 West Africa outbreak.
There was a fairly large hiatus after the 1976 outbreaks, with the exception of a smaller one that occurred in the area of the initial outbreak in 1979, and a single case in northwest DRC. No other cases were reported until 1995, when the Kikwit outbreak occurred.
The 1995 Kikwit outbreak itself was transformative; previously in the 1976 outbreaks the nature of Ebola and its transmission were not discerned. The people who investigated the original 1976 outbreak arrived very late in the process, so they were unable to observe the initial symptoms and transmission of the disease. In contrast, the 1995 Kikwit outbreak had been ongoing for only a month or so by the time infectious disease experts arrived, so there was an opportunity to observe transmission in the midst of the outbreak. The isolation facility parameters for operating safely with Ebola patients were established during the 1995 Kikwit outbreak; and control measures for health care workers were also established over the course of the outbreak. When outside healthcare workers initially arrived, facilities were largely abandoned. A small number of CDC workers cleaned up a hospital that had essentially been abandoned, including the removal of 23 bodies that had been left behind. They then led the effort to reestablish a treatment facility where infected individuals could be isolated and cared for by people who were appropriately protecting themselves with PPE.
What causes Ebola outbreaks? The virus is the etiologic agent, but that is not really the underlying cause of outbreaks, which are poor infection control practices in countries with poor health care systems. If it were not for a lack of resources to maintain some level of infection control, these outbreaks simply would not occur. In fact, hospitals are often the amplification foci largely responsible for the expansion of outbreaks and for much of the early transmission. This is not because of a lack of will or capability on the part of the individuals that operate these facilities. It is simply due to the lack of basic resources (such as running water) to practice infection control and standard precautions. These conditions create outbreaks in West Africa in general, and they were largely responsible for the early genesis and size of the 2014 outbreak in Sierra Leone in particular.
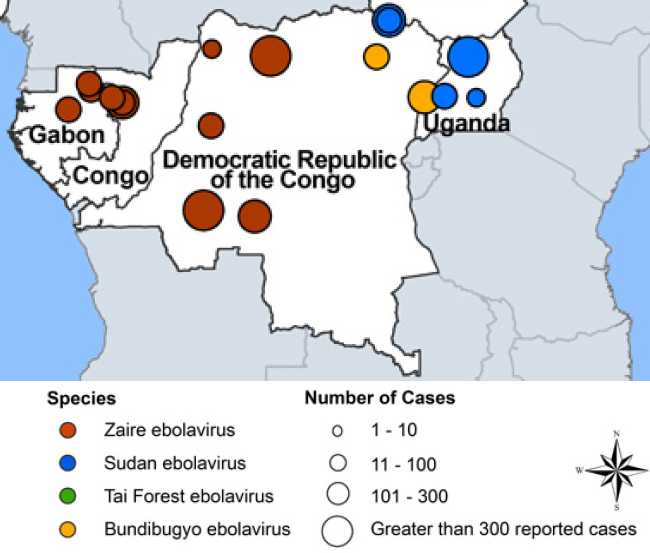
SOURCE: Centers for Disease Control and Prevention, E. Ervin CDC/VSPD 2014.
Part of the control efforts that were developed and implemented, which Ksiazek called the ‘Ebola play book,’ were simple methods: existing cases need to be found and isolated, and their contacts need to be quickly and accurately identified because those people may become sick. The contacts do not need to be isolated or quarantined, but they should be followed carefully. If they become sick, action must be taken to isolate them. If this can happen thoroughly and rigorously, an outbreak can be stopped.
Household quarantine, in contrast, is not an effective means of infection control. Following this method, if a case is found in a household, rather than removing that individual and placing him or her in an isolation facility, the house is merely closed up, leaving the infected person with family members. As a result, in a very short period of time a cluster of cases arises rather than a single case. Transmission does not occur before an individual becomes sick. Therefore, if the infected individual can be identified before he or she becomes seriously ill and develops diarrhea and heavy shedding of the virus, transmission can
probably be avoided. Other issues specific to the cultural practices prevalent in the outbreak area also increased transmission. Burials were a significant contributing factor in the West African outbreak, and are a critical source of infection. Specifically, after patients die they are often buried by their families in a manner that poses high risk for transmission. Therefore, it is important to ensure that burials are conducted safely, for example, through supervision or burial teams. Some cultural practices must be maintained without direct contact with the body, Ksiazek said, such as allowing family members to see the individual being buried.
There are also modes of transmission that have nothing to do with medicine or medical practices. Traditional healers are active in West Africa communities and may play a role in transmission by practicing traditional healing methods like scarification or cutting with razor blades or other sharp objects, or they may give injections of unknown substances rather than known medications.
Figure 2-6 provides a map showing the three countries mainly affected by Ebola in 2014: Guinea, Liberia, and Sierra Leone. Where these countries come together is where the outbreak began, in a town called Gueckedou. The outbreak was not successfully diagnosed until some cases had reached the Guinean capital of Conakry, on the Atlantic coast, and specimens were sent to Europe for diagnosis.
By the time the diagnosis had been made in Guinea, the outbreak had already spread through a number of cities in Guinea itself, and infected patients were suspected of having traveled across the borders of these three countries. Since these borders were open, people regularly moved in tribal groups or social organizations across them from country to country.
CDC was sent to West Africa based on a bilateral arrangement between CDC and the government of Sierra Leone to help with data management and tracking of the outbreak. The primary goal was, therefore, for CDC officers to assist in forming a national surveillance system that would inform outbreak control. Initially, the quality of data available was not very high. Early reports stated that mortality was running at about 30 percent, which did not accurately reflect the true mortality rate. As part of its response to the Ebola outbreak, CDC assisted in data collection by sending officers to the local areas of infection. Data collected in these areas also helped to create a database that allowed CDC to track the progress of the outbreak, or the lack of progress in controlling the outbreak, using a viral hemorrhagic fever
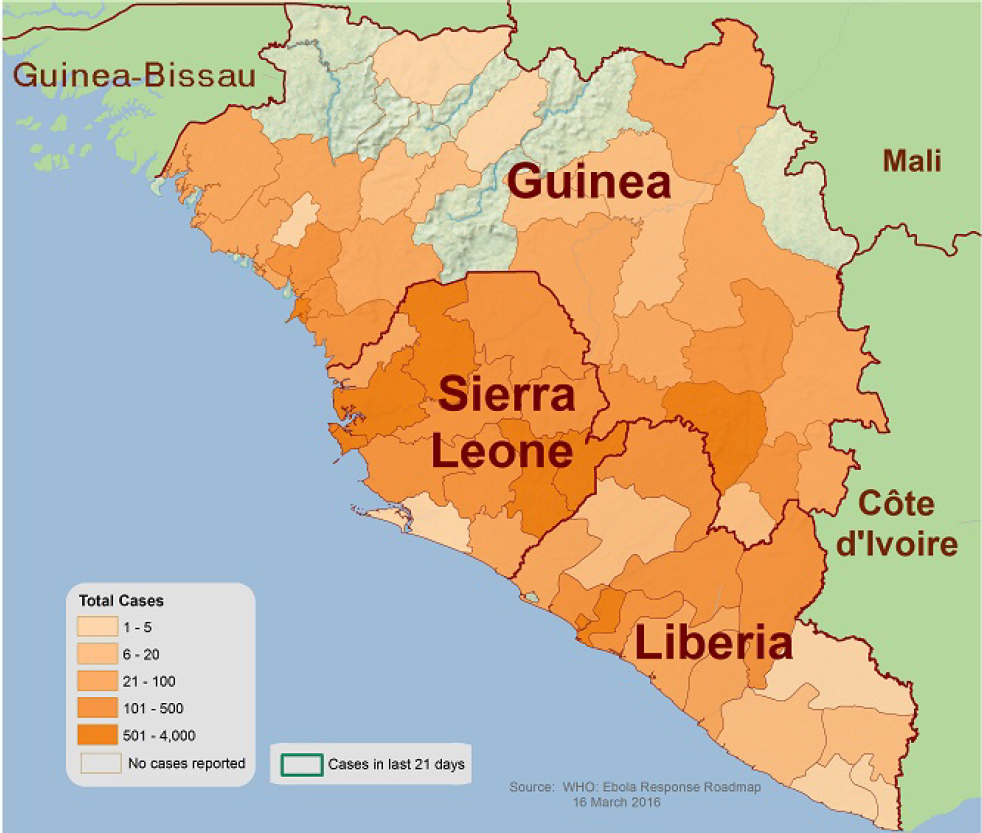
SOURCE: WHO Ebola Response Roadmap.
(VHF) database module in Epi Info, a common program used by epidemiologists that CDC developed in responding to previous outbreaks in Africa. Epi Info was designed primarily to deal with existing outbreaks, which were mostly local and small. This outbreak, however, was already in three countries and larger than the total sum of all the previous cases of Ebola.
The total death toll of the outbreak at the time of the workshop was about 5,000.5 In contrast, the total number of cases estimated for all previous outbreaks was approximately 1,200. Because existing tracking methods were designed to deal with smaller, more limited outbreaks,
_____________________
5 For information on the death toll of the 2014 Ebola outbreak in West Africa, see the U.S. Centers for Disease Control and Prevention: http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html; accessed April 10, 2016.
they had to be re-scoped to deal with much larger outbreaks. Several modifications were quickly made with assistance from programmers at CDC. One modification was to convert the program from a single-user application, one that could be used on a single laptop, into a sequel server version outfitted with Wi-Fi routers so that multiple people could enter data from multiple laptops onto a single server version. Another necessary modification was to devise a means by which data from individual regional or local databases could be uploaded into a national database to obtain national statistics. Some changes to the application were easily made, but the data still have to travel from one place to another, and communications networks in West Africa are not always adequate. Even though mobile phones have changed Africa, the bandwidth available with a mobile phone is often insufficient to transmit larger amounts of data.
Ksiazek was part of the first team that was sent by CDC to Sierra Leone in mid-August 2014. By the time he arrived, CDC was already operating at three locations: at the site of the original outbreak, in Kailahun District; in Kenema; and in Bo. Initially, approximately 12 people from CDC had been deployed in Sierra Leone. Subsequently, that number was increased to 37, and then to 70 individuals.
By the time Ksiazek arrived in mid-August 2014, there were already two epicenters in Sierra Leone. The virus was already spreading and was beginning to appear in and near Freetown, a city of over one million people, and in another district near Freetown. Yet the situation in Sierra Leone was better than the outbreak in Liberia, which was nearly out of control. The resources and logistics of bringing control efforts to bear were limited. For instance, finding and moving patients into an isolation facility requires ambulances or some other suitable form of transportation, which frequently were not available. Patients remained in remote villages or even in towns due to a lack of sufficient ambulances or crews. In addition, tracing and transporting contacts and safely removing dead bodies posed challenges. Ksiazek was there during the rainy season, which made it difficult to unload supplies and move them into warehouses immediately. In general, PPE and disinfection supplies were available nationally, but because they required distribution from a single entry point, supplies at the local level were insufficient.
Another challenge Ksiazek faced was case finding. Quarantine is not generally recommended or supported by either the WHO or the CDC in dealing with these outbreaks because they often lead to unhelpful isolation of officials and aid workers. However, because politicians and
other high-level people were frequently involved, quarantine became a regular part of the response. The goal was to stop transmission, but when it was determined that Ebola was occurring in one part of the country, and the decision-makers were in another part, communications were essentially cut off to the affected area. Hence, sufficient efforts to control the outbreak in that part of the country were not forthcoming, and the prevalence of disease kept growing, eventually spilling over and spreading into other areas. Ksiazek stated that more effort at the local level would have been more appropriate than trying to isolate the outbreak from a central point. Poor application of case finding and perhaps a lack of more beneficial distribution of resources more broadly contributed to the challenges.
When Ksiazek arrived, he found that the demand for facilities in which patients could be isolated exceeded the number of beds available, and the situation did not improve as time went on. This led to an escalation of the outbreak. Unfortunately, in the majority of facilities, infection of healthcare workers was quite common. Ksiazek did not believe that this was due to a lack of PPE per se, but rather that healthcare workers felt at risk and the number of infections supported that belief. Despite the risk health care workers faced and the incidence of disease in their ranks, they did not receive timely compensation for their work. This was not due to a lack of resources at the central level; rather, it was due to a lack of an efficient payroll distribution system. Another ongoing challenge is that there are simply not enough trained medical staff to maintain the existing facilities. Therefore, with the construction of new facilities, those resources had to come from the international community.
Ksiazek then turned to the epidemiology of the outbreak. Table 2-2 demonstrates the spread of the disease to September 2014, and indicates that not only were records lacking, but also the data in these records were often incomplete or non-existent.
TABLE 2-2 National Ebola Situation Report for Sierra Leone.
| District | Total Contacts listed during outbreak | Total Contacts who have finished their 21 days | Total Contacts Currently Being Followed | New contacts added in 24h | Contacts seen and healthy in last 24h | Contacts seen and ill in last 24h | Contacts not seem in last 24h | Contacts finished 21 days in the last 24h | % of Contacts seen by Tracers in last 24h |
| Bo | 592 | 456 | 136 | 0 | 86 | 8 | 0 | 42 | 69% |
| Bombali | 567 | 176 | 391 | 7 | 384 | 4 | 3 | 6 | 99% |
| Bonthe | 84 | 27 | 57 | 52 | 57 | 0 | 0 | 0 | 100% |
| Kailahun | 1416 | 1105 | 155 | 19 | 155 | 0 | 0 | 8 | 100% |
| Kambia | 68 | 12 | 56 | 38 | 55 | 1 | 0 | 0 | 100% |
| Kenema | 2483 | 1821 | 589 | 52 | 578 | 0 | 11 | 11 | 98% |
| Kono | 157 | 80 | 77 | 0 | 71 | 6 | 0 | 0 | 100% |
| Moyamba | 206 | 149 | 57 | 0 | 51 | 6 | 0 | 12 | 100% |
| Pujehun | 333 | 195 | 137 | 0 | 137 | 0 | 0 | 41 | 100% |
| Port Loko | 1514 | 234 | 1297 | 97 | 1155 | 3 | 139 | 51 | 89% |
| Tonkolili | 533 | 170 | 363 | 0 | 363 | 0 | 0 | 17 | 100% |
| Western Area Urban | 767 | 436 | 331 | 13 | 331 | 0 | 0 | 0 | 100% |
| Western Area Rural | 183 | 0 | 181 | 0 | 181 | 0 | 0 | 0 | 100% |
| National | 8903 | 4861 | 3827 | 278 | 3604 | 28 | 153 | 188 | 95% |
SOURCE: Tom Ksiazek, presentation at the workshop.
There appears to be no difference in infection rates among men and women, and the age distribution of infected men and women was approximately equal. Children experience lower infection rates simply because they do not perform some of the activities, such as burial rituals, that would put them at risk. Figure 2-7 shows infection rates by chiefdom compared with infection rates by district. Again, data are incomplete; it is nearly impossible to track infection rates at the tertiary level of geographic or political jurisdictions.
Downward trends in infection rates, Ksiazek suggested, were largely due to a change in people’s behavior. By the time Ksiazek departed in late September 2014, officers had been placed in a number of other districts where transmission had begun to pick up, in an effort to forestall infection. However, distribution maps suggest that efforts were not entirely successful. It would take several more months for the outbreak to be declared over in the affected countries of Guinea, Liberia, and Sierra Leone.
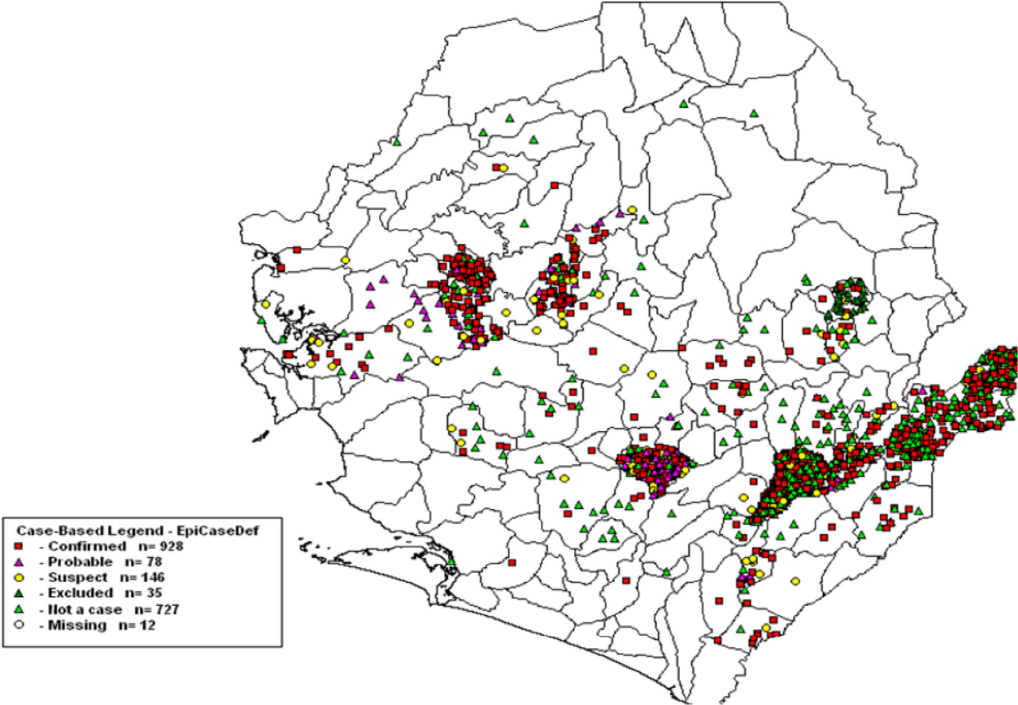
SOURCE: Tom Ksiazek, presentation at the workshop.
Discussion
The discussion following Ksiazek’s presentation focused on questions about the source and prevalence of the outbreak, including the role of sequencing, transport of samples, and WHO data.
Using Sequencing to Determine the Origin of Outbreaks
A participant asked Ksiazek about one theory regarding the original case in Guinea, that one child and his mother ate infected bat meat. Since that first case, the population reportedly continues to go to the forest and eat dead animals found there. Was there any evidence that new infections occurred as a result of this practice? Ksiazek responded by referring to sequencing issues. He did not think that there had been sufficient
examination of sequences that could determine the source of the outbreak with greater accuracy. However, it appears that in spite of the mutations, there is an accumulation of snips in the viruses that do occur. Ksiazek believes that all of the viruses clearly have the signature of the outbreak virus. He further believes that if there were another introduction, it would most likely have a slightly different signature that would fall outside of the bounds of, for instance, the sequences that occurred in hundreds of individuals. There is an accumulation of some mutations in the virus, but throughout outbreaks in the past these mutations were usually part of the outbreak itself. However, not enough sequencing had been done in all of these sites to fully determine what happened.
Issues with Transporting Viruses
Ksiazek also noted that it is hard to transport these viruses for sequencing and other sample testing, due to the constraints of biosecurity measures. There are efforts to make transport possible, but not in an acceptable real-time fashion, which would be much more helpful.
Discrepancies in WHO Data
A participant asked about the missing set of cases on the graph that Ksiazek presented (Figure 2-8). Did the missing cases include confirmed diagnosed cases? Ksiazek responded affirmatively and explained that when a patient came to a facility, a blood sample was taken upon admission, so these were patients that were definitely seen. The problem is that they were admitted to a hospital but the records did not indicate their outcomes. Even their relatives still do not know what happened to some of them.
This led to a follow up question about why WHO reports these case numbers if it is clear that they are incomplete? Ksiazek replied that the case numbers underrepresent the true number of cases, and that varies from country to country. There are many problems with the data, but in Sierra Leone, for instance, the way this system was put together was entirely lab-based from the beginning, so essentially the only cases reported were people whose specimens were drawn and sent to one of the three laboratories that were initially conducting diagnostic testing. They are real numbers, but the problem is that undoubtedly there were patients that no one counted, because they did not have a record established. In Sierra Leone, there were very few suspect or probable cases; they were almost all confirmed cases. The patient’s outcome was unknown in about
30 percent of the cases. In spite of their efforts, it was very difficult to locate either a hospital record that recorded the outcome for patients or a burial record. Ultimately, the mortality rate was approximately 65 percent.
THE EBOLA CONTROL STRATEGY IN INDIA
Ratnakar Sahoo focused his presentation on some of the measures the Indian government took to identify and isolate suspected cases of Ebola entering India. He began by recounting that as of the date of the workshop, there were six or seven suspected cases in India.
As is well known, transmission of Ebola occurs through close contact with bodily fluids of infected humans or animals. Figure 2-8 shows the epizootic life cycle that usually affects fruit bats as they come into contact with gorillas, chimpanzees, and monkeys, which in turn come into contact with humans. Human-to-human transmission then occurs and the virus is spread.
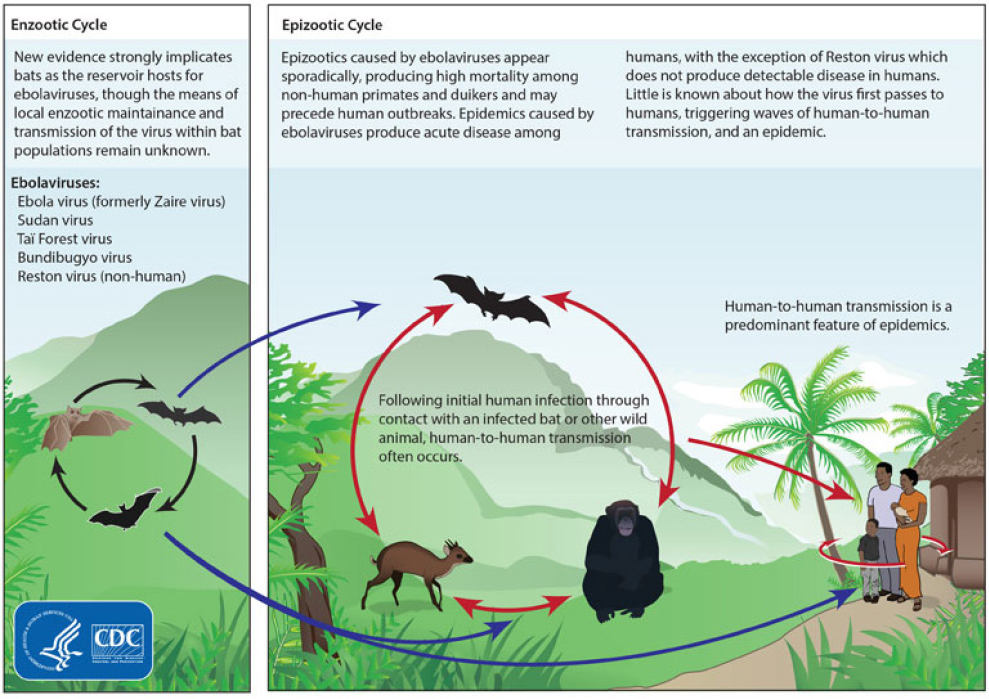
SOURCE: Centers for Disease Control and Prevention (http://www.cdc.gov/vhf/ebola/resources/virus-ecology.html accessed November 2014).
Symptoms of Ebola include headaches, weakness, fever, and fatigue. The incubation period is a maximum of 21 days. When the disease progresses, it produces severe vomiting, abdominal pain, diarrhea, pharyngitis, difficulty breathing and swallowing, conjunctivitis, intensive bleeding, high body temperature, and prostration and bleeding that could lead to shock. Clinical diagnoses and laboratory testing of blood samples can confirm the existence or absence of the virus. The Ebola virus is classified as a Risk Group 4 virus by the WHO.6 Enhanced clinical samples should be collected using all universal precautions, including PPE (long gloves, gowns, and eye shields), and then handled and kept in BSL-3 or BSL-4 labs. Before dispatching the sample, disinfectant (diluted bleach solution or sanitizer solution) should be used on all surfaces of the container. All vials containing Ebola-suspect samples should have bold labeling. Sample collectors should safely pack vials using the triple packing system and should transport the samples in accordance with the BSL-3 reference lab regulations. Usually, samples from Delhi are sent to the National Institute of Immunology and to the Indian CDC. Other BSL-3 labs across India have also been strengthened to handle potential Ebola cases.
Indian experts are concerned about a potential outbreak of Ebola in India because there are nearly 45,000 Indians now living in West Africa. Further, government health services, especially in rural areas, struggle to provide even basic health services on a daily basis. Another concern is that open defecation and urination is common especially in smaller towns and villages, increasing the potential for transmission.
As a precaution, Indian air transportation authorities have begun to use affordable, thermal scanners that beep if an incoming passenger has a temperature of over 37 degrees Celsius (98.6 degrees Fahrenheit). If a passenger has a higher temperature, health teams then place the person under surveillance. As of the date of the workshop, 22,150 passengers have been screened, of which 54 were identified as high risk and seven were identified as medium risk, and the others were categorized as low risk. The Minister of Health has instructed that thermal scanners be used at all of India’s 18 international airports. All planes are disinfected after passengers arrive, and the passengers on the next flight are allowed to board only 30 minutes after the disinfection process. Sanitizers can be
_____________________
6 Each country is responsible for classifying pathogens into risk groups, and all countries agree that Ebola is in Group 4.
seen at the entrances of Indian airports, and airport staff and other officials also can be seen wearing masks, goggles, and gloves on duty as a precaution. Figure 2-9 shows authorities in gowns and PPE at airports in India.
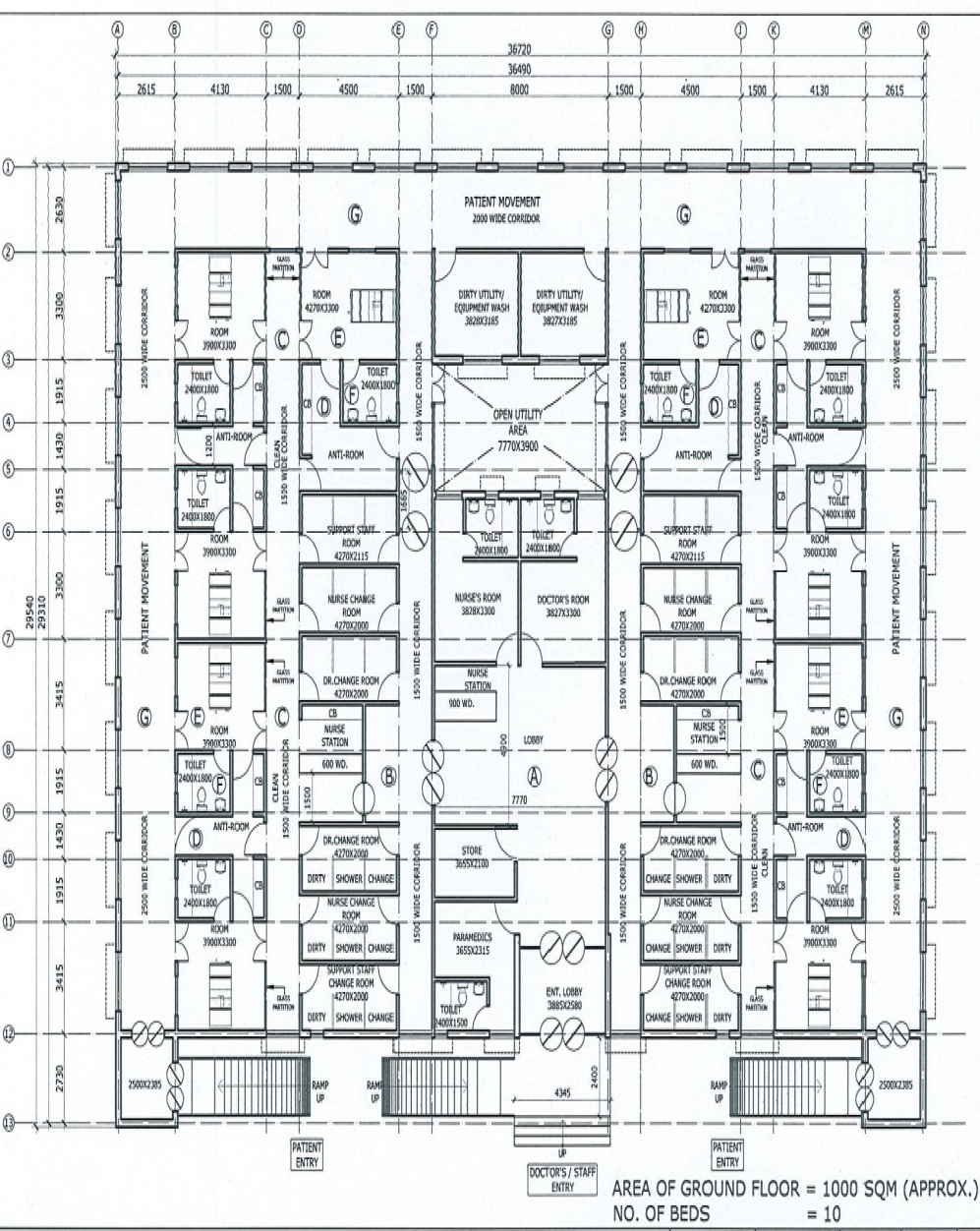
Preparations at designated hospitals have also been made and the facilities have been inspected by central teams in all states across the country. These central teams are comprised of a physician and a microbiologist. Doctors, nurses, and others at designated hospitals have been provided with infection control training and full body protection to deal with Ebola cases, should they arrive. Figure 2-10 shows the proposed layout of a designated isolation ward with ten beds. The area is around 1,000 square meters.

SOURCE: Ratnakar Sahoo, presentation at the workshop.
Discussion
The discussion following Sahoo’s presentation focused on the factors used to determine risk levels for Ebola.
A participant asked how high-risk, medium-risk, and low-risk categories are determined? By the temperature reading on the scanner? Sahoo replied that high-risk cases are those arriving from pandemic areas with symptoms. Medium-risk cases only have an elevated temperature. The lowest are those arriving from non-pandemic areas. The participant further inquired as to whether other symptoms are used to elevate risk-levels. Sahoo replied that if symptoms are seen and the person is arriving from an affected area, they are categorized as high-risk, as are those suspected of having a history of travel to an affected area or close contact with someone who had symptoms of the Ebola virus.






























