
6
Promoting Cardiovascular Health and Preventing Cancer
As a result of successes in infectious disease prevention and sanitation improvement, the burden of disease in low- and middle-income countries (LMICs) is rapidly shifting from communicable to noncommunicable diseases, demonstrating a paradox of success in global health. As a greater proportion of children survive into adulthood, and changes in diet and lifestyle occur, many countries now face a rise in chronic illnesses, such as cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), cancer, and diabetes, all of which are often associated with behavioral factors such as tobacco use, physical inactivity, and diets high in calories, sugar, and salt (WHO, 2017b). Globally, these chronic or noncommunicable diseases (NCDs) kill 40 million people per year, almost three-quarters of whom reside in LMICs (WHO, 2017b). Though media attention often portrays NCDs as a western, high-income country health challenge, the burden of NCDs disproportionately affects the poor in middle-income countries—a trend that will continue to grow alongside rising urbanization and globalization.
In a global trade environment, U.S. interests are affected by the rise of NCDs in LMICs and their resultant human and economic effects. Countries with a high NCD burden tend to have lower national productivity and higher health and welfare expenditures (Bloom et al., 2011). The costs resulting from productivity losses associated with disability, unplanned absences from work, and increased rates of accidents are as much as 4 times the cost of treatment. Research also has shown that investors, including U.S. businesses, are less likely to enter markets where the labor force suffers a heavy disease burden.
The committee has chosen to focus this chapter on cardiovascular disease and cancer (specifically vaccine-preventable cancers, such as cervical cancer and liver cancer), not only because of their global burden but also because of the amount of research and knowledge that exists and the opportunity for intervention worldwide. This chapter begins by characterizing the economic and epidemiological burden of NCDs, and demonstrates how they are both projected to rise in the next 20 years if no action is taken to curb rising incidence. It then explores motivations for U.S. involvement, and highlights existing cost-effective, successful interventions found globally for prevention and early treatment of CVD and select cancers. Finally, this chapter emphasizes a need to transform health systems to be more capable of managing these chronic conditions, particularly highlighting the potential of public–private partnerships.
THE RISING ECONOMIC BURDEN OF NONCOMMUNICABLE DISEASES
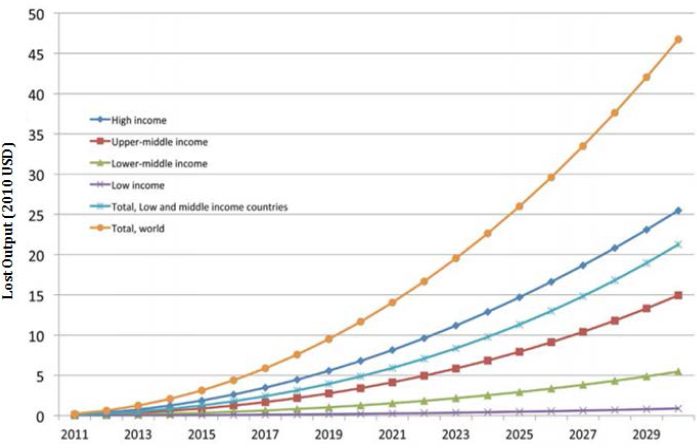
A study conducted by the World Economic Forum and the Harvard School of Public Health estimated that the projected increase in the global economic burden of five NCDs (CVD, chronic respiratory disease, cancer, diabetes, and mental health) would result in cumulative output losses of $47 trillion by 2030, which is roughly 75 percent of the 2010 global gross domestic product (GDP) (Bloom et al., 2011).1 CVDs were a primary contributor to lost output (33 percent), with 18 percent attributed to cancers (Bloom et al., 2011). As of 2015, the estimated annual global cost of CVD is expected to increase by 16 percent from $906 billion to more than $1 trillion by 2030 (see Figure 6-1). Furthermore, total output losses are projected to increase sharply over time (see Figure 6-2).
Researchers from the Netherlands conducted a series of systematic reviews to examine the global impact of NCDs at the macroeconomic level, including productivity, health care spending, and national income (Muka et al., 2015). CVD accounts for the highest health care expenditure in most countries, ranging from 12 to 16.5 percent of the overall health care budget (other NCDs ranged between 0.7 and 7.4 percent) (Muka et
___________________
1 These estimates were generated using EPIC, a tool developed by the World Health Organization to simulate the economic impact of diseases on aggregate economic output. EPIC links the value of economic output to quantities of labor and capital inputs, as well as to technology. The EPIC model adjusts labor and capital inputs according to population health. Namely, labor is diminished by disability and death caused by NCDs. Capital is also reduced because costs of screening, treatment, and care claim resources that would otherwise be available for public and private investment. The EPIC model predicts losses caused by different health conditions in terms of their effect on the value of economic output (WEF and WHO, 2011).
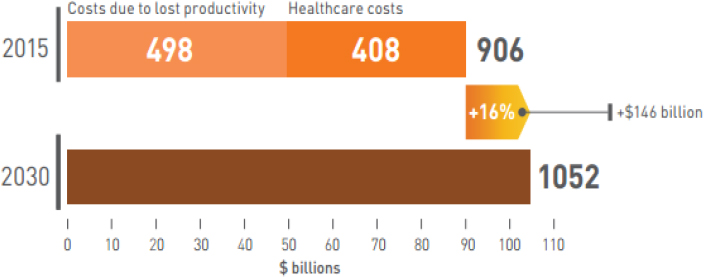
SOURCE: Reddy et al., 2016.
SOURCES: Bloom et al., 2011; World Economic Forum.
al., 2015). Additional analyses found a large economic impact of NCDs on productivity across WHO regions, albeit with large regional differences in disability-adjusted life years (DALYs)2 (Chaker et al., 2015).
Similarly, annual cancer costs worldwide were estimated at approximately $1.16 trillion3 in 2010, the equivalent of more than 2 percent of the global GDP (Stewart and Wild, 2014), with projections reaching $8.3 trillion in annual costs by 2030 (Bloom et al., 2011). Yet, investing in cancer care and control could result in millions of avoidable deaths, achieving between $100 and $200 billion in global economic savings (Stewart and Wild, 2014). These costs are astronomical for many countries, even those with high-income status, and demonstrate the imperative behind addressing these two major health burdens.
Finding: CVDs and cancers comprise more than 51 percent of the projected $47 trillion in cumulative lost output resulting from the increase in the global economic burden of five NCDs.
THE RISING EPIDEMIOLOGICAL BURDEN OF NONCOMMUNICABLE DISEASES
Of the 40 million deaths per year caused by NCDs, 17 million are considered to be “premature” (below the age of 70), and 87 percent of these occur in LMICs (WHO, 2017b). Tables 6-1 and 6-2 depict the heterogeneity of conditions that contribute to morbidity and mortality in 14 LMIC regions, and demonstrate the increasing burden of NCDs relative to communicable diseases in many parts of the world. Importantly, the health burden resulting from communicable and noncommunicable diseases is not always distinct. Recent studies have linked infections with the onset of chronic non-communicable diseases later in life. Following the 2009 H1N1 outbreak, multiple studies found an association between type 1 diabetes onset later in life and those who were diagnosed with H1N1 (Nenna et al., 2011; Piccini et al., 2012). This demonstrates a need for comprehensive preparedness and prevention efforts within a strong public health system to effectively combat NCDs as well as infectious disease threats—and their downstream consequences.
___________________
2 The burden of disability associated with a disease or disorder can be measured in units called disability-adjusted life years (DALYs). DALYs represent the total number of years lost to illness, disability, or premature death within a given population. See more at https://www.nimh.nih.gov/health/statistics/global/index.shtml (accessed April 1, 2017).
3 This figure is the sum of the costs of prevention and treatment, plus the annual economic value of DALYs lost as a result of cancer. It does not include the longer-term costs to families or the value that patients and families place on human suffering.
Cardiovascular Disease
Mortality due to CVDs has been growing around the world, with an increase of 12.5 percent between 2000 and 2015 (Wang et al., 2016). Though many incorrectly think that CVD and relevant risk factors are unique to high-income countries, the increase in global mortality is actually attributed to an increasing incidence of CVD in LMICs. In fact, 80 percent of all CVD related deaths occur in LMICs (Lozano et al., 2012; Pena and Bloomfield, 2015). CVD is now recognized as the leading cause of death globally, and in 2015 was responsible for nearly 18 million global deaths. The global burden of CVD is expected to continue to rise; premature deaths will increase from 5.9 million to 7.8 million between 2013 and 2025 if current risk factors for CVD do not change (O’Rourke, 2017).
Cancer
Cancer is the second largest cause of death worldwide, responsible for 8.8 million deaths (15.7 percent) globally in 2015 (Wang et al., 2016). The majority of the 14 million people diagnosed with cancer each year live in LMICs, where more deaths are caused by cancer than by human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), malaria, and tuberculosis (TB) combined (Ferlay et al., 2013; WHO, 2014). Around two-thirds of the 8.8 million global cancer deaths each year occur in LMICs because of late detection and poor access to treatment (WHO, 2017c), and this number is expected to triple by 2030 (Nyambura, 2017). Experts estimate that between 30 and 50 percent of cancers can currently be prevented, through evidence-based prevention strategies and reducing risk factors, meaning that up to 3.7 million lives can be saved each year, 80 percent of whom reside in LMICs (Stewart and Wild, 2014). Early detection and management can also contribute to the reduction of the cancer burden (WHO, 2017a). Nearly 70,000 women are diagnosed annually with cervical cancer in Africa alone, contributing to 22 percent of all cancers in women (Nyambura, 2017). As discussed later in this chapter, this and other types of cancer have been shown to be vaccine preventable; thus, there is a potential to substantially reduce cancer deaths by increasing vaccine coverage. In addition to mortality, cancer can also affect an individual’s ability to work, which extends negative effects to the broader productivity of a country. For cervical cancer in particular, the percentage of attributable absolute DALYs varied across countries, for example from 1.6 percent in New Zealand to 13.4 percent in Brazil (Chaker et al, 2015).
TABLE 6-1 Morbidity (DALY) Ranking of Top NCDs and Communicable Diseases
| Diseases | DALY Ranking | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| United States | Southern Latin America | Central Asia | Central Latin America | Andean Latin America | Caribbean | ||||||||||
|
Cardiovascular Diseases |
1 | 1 | 1 | 1 | 1 | 1 | |||||||||
|
Cerebrovascular Diseases |
11 | 4 | 3 | 11 | 10 | 3 | |||||||||
|
Chronic Respiratory Diseases |
3 | 3 | 9 | 7 | 7 | 8 | |||||||||
|
Diabetes |
4 | 7 | 13 | 3 | 9 | 4 | |||||||||
|
Chronic Kidney Disease |
18 | 15 | 22 | 5 | 11 | 16 | |||||||||
|
HIV/AIDS |
63 | 48 | 70 | 32 | 50 | 5 | |||||||||
|
Tuberculosis |
192 | 112 | 28 | 85 | 38 | 66 | |||||||||
|
Malaria |
256 | 244 | 247 | 226 | 220 | 196 | |||||||||
|
Lower Respiratory Infection |
25 | 5 | 4 | 9 | 2 | 6 | |||||||||
|
Upper Respiratory Infection |
113 | 128 | 158 | 111 | 119 | 142 | |||||||||
|
Hepatitis |
171 | 176 | 112 | 164 | 174 | 164 | |||||||||
|
Chronic Liver Disease |
21 | 17 | 6 | 10 | 13 | 26 | |||||||||
|
Road Traffic Injury |
12 | 8 | 12 | 6 | 4 | 10 | |||||||||
|
Cancer |
|||||||||||||||
|
Cervical |
100 | 46 | 73 | 60 | 45 | 51 | |||||||||
|
Liver |
52 | 69 | 47 | 70 | 59 | 65 | |||||||||
|
Breast |
24 | 26 | 41 | 49 | 55 | 37 | |||||||||
|
Tracheal, Bronchus, and Lung Cancer |
5 | 14 | 25 | 44 | 47 | 24 | |||||||||
NOTE: DALY = disability-adjusted life year; HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome; NCD = noncommunicable disease.
SOURCE: Global Burden of Disease Study 2015. Institute for Health Metrics and Evaluation 2016. http://ghdx.healthdata.org/gbd-results-tool (accessed March 10, 2017). See Annex 6-1 for details on reconstructing the tables.
| Tropical Latin America | East Asia | Southeast Asia | South Asia | N. Africa/Middle East | Southern Africa | West Africa | East Africa | Central Africa |
|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 1 | 4 | 8 | 5 | 3 |
| 3 | 2 | 2 | 9 | 6 | 12 | 13 | 13 | 14 |
| 6 | 5 | 5 | 4 | 9 | 11 | 16 | 17 | 13 |
| 7 | 13 | 6 | 12 | 8 | 8 | 29 | 24 | 26 |
| 17 | 22 | 14 | 18 | 20 | 27 | 39 | 57 | 56 |
| 22 | 52 | 25 | 26 | 91 | 1 | 4 | 1 | 5 |
| 76 | 54 | 9 | 10 | 55 | 6 | 17 | 11 | 12 |
| 219 | 245 | 63 | 40 | 70 | 54 | 1 | 6 | 1 |
| 11 | 20 | 7 | 6 | 7 | 5 | 3 | 3 | 2 |
| 126 | 118 | 143 | 156 | 131 | 144 | 160 | 152 | 141 |
| 149 | 129 | 112 | 58 | 129 | 169 | 86 | 101 | 118 |
| 18 | 23 | 11 | 20 | 19 | 40 | 19 | 31 | 32 |
| 4 | 7 | 8 | 13 | 5 | 9 | 24 | 18 | 16 |
| 59 | 80 | 67 | 101 | 141 | 43 | 81 | 67 | 66 |
| 69 | 10 | 33 | 107 | 65 | 62 | 44 | 70 | 63 |
| 39 | 45 | 36 | 63 | 47 | 48 | 98 | 79 | 79 |
| 30 | 8 | 27 | 54 | 38 | 36 | 105 | 129 | 104 |
TABLE 6-2 Mortality Ranking of Top NCDs and Communicable Diseases
| Diseases | Mortality Rankings | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| United States | Southern Latin America | Central Asia | Central Latin America | Andean Latin America | Caribbean | ||||||||||
|
Cardiovascular Diseases |
1 | 1 | 1 | 1 | 1 | 1 | |||||||||
|
Cerebrovascular Diseases |
11 | 4 | 3 | 11 | 10 | 3 | |||||||||
|
Chronic Respiratory Diseases |
3 | 3 | 9 | 7 | 7 | 9 | |||||||||
|
Diabetes |
4 | 7 | 13 | 3 | 9 | 7 | |||||||||
|
Chronic Kidney Disease |
18 | 15 | 22 | 5 | 11 | 12 | |||||||||
|
HIV/AIDS |
63 | 48 | 70 | 32 | 50 | 10 | |||||||||
|
Tuberculosis |
192 | 112 | 28 | 85 | 38 | 46 | |||||||||
|
Malaria |
256 | 244 | 247 | 226 | 220 | 157 | |||||||||
|
Lower Respiratory Infection |
25 | 5 | 4 | 9 | 2 | 4 | |||||||||
|
Upper Respiratory Infection |
113 | 128 | 158 | 111 | 119 | 172 | |||||||||
|
Hepatitis |
171 | 176 | 112 | 164 | 174 | 131 | |||||||||
|
Chronic Liver Disease |
21 | 17 | 6 | 10 | 13 | 18 | |||||||||
|
Road Traffic Injury |
12 | 8 | 12 | 6 | 4 | 17 | |||||||||
|
Cancer |
|||||||||||||||
|
Cervical |
100 | 46 | 73 | 60 | 45 | 32 | |||||||||
|
Liver |
52 | 69 | 47 | 70 | 59 | 33 | |||||||||
|
Breast |
24 | 26 | 41 | 49 | 55 | 21 | |||||||||
|
Tracheal, Bronchus, and Lung Cancer |
5 | 14 | 25 | 44 | 47 | 13 | |||||||||
NOTE: HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome; NCD = noncommunicable disease.
SOURCE: Global Burden of Disease Study 2015. Institute for Health Metrics and Evaluation 2016. http://ghdx.healthdata.org/gbd-results-tool (accessed March 10, 2017). See Annex 6-1 for details on reconstructing the tables.
| Tropical Latin America | East Asia | Southeast Asia | South Asia | N. Africa/Middle East | Southern Africa | West Africa | East Africa | Central Africa |
|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 1 | 3 | 2 | 1 | 1 |
| 3 | 2 | 2 | 5 | 3 | 7 | 8 | 6 | 5 |
| 5 | 5 | 5 | 3 | 10 | 10 | 18 | 14 | 12 |
| 8 | 21 | 8 | 11 | 9 | 8 | 19 | 22 | 22 |
| 13 | 19 | 12 | 14 | 13 | 18 | 29 | 50 | 46 |
| 22 | 40 | 20 | 24 | 68 | 1 | 5 | 2 | 4 |
| 53 | 36 | 9 | 9 | 38 | 9 | 15 | 8 | 9 |
| 172 | 184 | 69 | 38 | 70 | 56 | 1 | 9 | 3 |
| 6 | 14 | 6 | 6 | 8 | 6 | 3 | 3 | 2 |
| 179 | 173 | 177 | 179 | 182 | 180 | 171 | 172 | 166 |
| 109 | 90 | 81 | 50 | 82 | 135 | 76 | 82 | 101 |
| 14 | 18 | 11 | 16 | 12 | 28 | 14 | 20 | 19 |
| 10 | 11 | 13 | 15 | 7 | 11 | 20 | 18 | 16 |
| 39 | 48 | 43 | 61 | 78 | 29 | 49 | 38 | 41 |
| 38 | 9 | 18 | 59 | 33 | 42 | 22 | 45 | 35 |
| 27 | 30 | 27 | 40 | 29 | 34 | 61 | 58 | 53 |
| 15 | 8 | 14 | 25 | 19 | 21 | 51 | 68 | 55 |
Barriers to Adequate Care
Whereas the populations of high-income countries benefit from quality health care centers, well trained health care providers, and regulations on harmful substances, such as tobacco, those in LMICs often lack adequate health care infrastructure (Wirtz et al., 2011) and policy safeguards. Compounding the challenge, health systems in LMICs are typically designed to handle infectious disease, not to provide the continuity of care needed for NCDs. The Lancet report on Prevention and Management of Chronic Disease explains:
Chronic illness demands a complex health-systems response that needs to be sustained across a continuum of care. Evidence-based interventions should be delivered by health professionals with diverse skills. . . . Such interventions are possible only with a functioning health system, which can deliver disease prevention and education services alongside integrated care and intersectoral collaboration that extends beyond the health sector. (Samb et al., 2010, pp. 1785–1786)
In addition to ill-fitted health systems, traditional health care systems in LMICs often lack the fiscal infrastructure to meet patients’ long-term health needs. In many LMICs, out-of-pocket expenses account for approximately 50 percent of total health expenditures, which may only be lowered by increased central government investment in health (Zhang and Liu, 2014). However, increased decentralization of health care spending suggests that local governments in low-income countries will lack the capital to provide for their citizens’ health care needs, making this government investment more difficult. For many patients, high out-of-pocket expenditures lead them to opt out of seeking medical care and leave the hospital before it is recommended by their physicians (Babiarz et al., 2012). Increasing the number of patients who seek treatment and maintain their therapy regimen continues to be a challenge and hinders the efforts of global health actors and national governments in achieving CVD and cancer prevention targets.
Many countries experience difficulties effecting change in national policy and spending in part because NCDs like CVD are not prioritized in political agendas, despite their significant health and economic burden. In addition, the slow epidemic of NCDs does not create the type of panic or rapid response that infectious diseases like Ebola, multidrug-resistant tuberculosis (MDR-TB), or HIV/AIDS can generate (Reddy et al., 2016). The World Innovation Summit for Health 2016 Behavioral Insights report explains that it can be difficult for policy makers, politicians, and health care professionals to emphasize preventative care because of a tendency to “focus on the immediate problem in front of us, rather than the potential future problems that seem distant and abstract” (Hallsworth et al., 2016).
Finding: Although the mortality and morbidity burdens of CVD and cancers are high, there is evidence that investing in comprehensive health systems and prevention strategies can save millions of lives. Political challenges remain in mobilizing resources and support for NCDs that may not be seen as immediate priorities.
MOTIVATION FOR U.S. INVOLVEMENT
The growing global burden of mortality due to CVD and cancer poses a significant strategic problem that the United States cannot ignore. A 2014 Council on Foreign Relations Task Force report confirms this stance, stating that U.S. interests will be affected by the rise of NCDs in LMICs because of their human and economic impacts (Daniels et al., 2014). The majority of U.S. spending on global health is directed toward HIV/AIDS, TB, malaria, and other infectious diseases, in addition to maternal and child health, nutrition, and family planning. While some funding is directed toward strengthening health systems, there are no dedicated funding streams specifically for NCDs and no presidential initiatives established to reduce their burden. Even global dialogue about strengthening health systems neglects most chronic diseases (Samb et al., 2010). The 2014 Council on Foreign Relations Task Force report outlines steps the United States can take now to address the critical issues of NCDs, including promotion of cardiovascular health, and vaccination and screening programs to prevent cancer (Daniels et al., 2014). Many of these services can often be integrated into existing U.S. global health programs and platforms, motivated by three key benefits, which are discussed further in the sections below:
- universal purpose
- economic prosperity and trade benefits
- safeguarding U.S. global health investments
Universal Purpose
Because NCDs are a leading cause of morbidity and mortality in high-, middle-, and low-income countries, there is a tremendous opportunity for a shared innovation approach to developing solutions to common problems. By investing in CVD and cancer prevention programs abroad, the United States can identify cost-effective strategies to target these diseases domestically. The potential of this approach has already been demonstrated through a program in King County, Washington, that implemented a mobile health solution for NCD management based on interventions used in Bangladesh, China, and India (Global to Local, n.d.). Additionally, research conducted in other countries, such as that done on Cuba’s CIMAvax vac-
cine, may help to accelerate the discovery of cures and more effective treatments for cancers (Keck, 2016). For rare diseases in particular, expanding research efforts outside the United States could generate more opportunities for testing and information sharing.
Economic Prosperity and Trade Benefits
In today’s global travel and trade environment, when other countries have a healthy population and workforce, the United States benefits. According to the 2013 report by the Lancet Commission on Investing in Health, approximately 11 percent of economic growth in LMICs is attributable to reductions in mortality (Jamison et al., 2013). Healthy populations lead to more stable economies, and this increased stability can encourage business expansion and additional consumption of U.S. goods. When multinational businesses open in a new country, it is in their interest to ensure their workforce is healthy and productive.
Safeguarding U.S. Global Health Investments
Many patients suffering from chronic conditions have already been recipients of U.S. global health aid for communicable diseases such as tuberculosis, malaria, and HIV/AIDS. If those patients are unable to work or die prematurely because of CVD or cancer, then the return on investment is lost. This holds especially true in the case of The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) investments. In 2015, the PEPFAR program provided antiretroviral therapy for 9.5 million people (PEPFAR, 2017); it is critical to ensure these significant investments are not lost to morbidity and mortality attributable to NCDs. If these patients die prematurely from chronic illness, much of the progress gained from healthier societies and restabilized economies in PEPFAR partner countries could be at risk.
COST-EFFECTIVE AND HIGH-IMPACT GLOBAL INTERVENTIONS
A 2011 World Economic Forum report identified a set of highly cost-effective population- and individual-based “best buy” interventions for NCDs that can feasibly be implemented in resource-constrained LMIC health systems (WEF and WHO, 2011) (see Table 6-3). The cost of implementing the full suite of interventions across all LMICs between 2011 and 2025 would total $170 billion, representing less than 5 percent of overall health spending in those countries (WEF and WHO, 2011). Scaling up only the best buy interventions for CVD during that same time period, at a cumulative cost of $120 billion, would drive a 10 percent decrease in CVD-
TABLE 6-3 Cost-Effective Interventions for NCDs in Resource-Constrained Environments
| Risk Factor/Disease | Interventions |
|---|---|
| Tobacco use |
|
| Harmful alcohol use |
|
| Unhealthy diet and physical inactivity |
|
| Cardiovascular disease (CVD) and diabetes |
|
| Cancer |
|
NOTE: NCD = noncommunicable disease.
SOURCE: WEF and WHO, 2011.
attributable mortality and a $377 billion projected cumulative economic benefit (WEF and WHO, 2011).
Similarly, a 2015 working paper for the Disease Control Priorities project found that substantially increasing the coverage of four prevention and treatment interventions, gradually over 15 years, would reduce projected NCD mortality by 25 percent in LMICs (Nugent, 2015). The analysis demonstrated an average benefit-cost ratio of 8:1, with annual benefits of $63.3 billion at a global cost of only $8.5 billion per year (see Table 6-4).
In examining these “best buy” interventions at a more granular level, the suggested practices can either be classified as policies targeted at the population level, or at the point of service delivery. A growing body of research demonstrates that interventions, such as fiscal and regulatory policies, that target behavioral and environmental risk factors that contribute to NCDs have a positive impact on health outcomes and can be cost effec-
TABLE 6-4 Cost–Benefit Analysis of Increasing Coverage of Interventions
| Target | Annual Benefits (in $ millions) | Annual Costs (in $ millions) | Benefit for Every Dollar Spent |
|---|---|---|---|
| Aspirin therapy at the onset of AMI (75% coverage) | $836 | $27.40 | $31 |
| Reduce salt content in manufactured foods by at least 30% | $12,121 | $638 | $19 |
| Increase tobacco price by 125% through taxation | $37,194 | $3,548 | $10 |
| Secondary prevention of CVD with polydrug (70% coverage) | $13,116 | $3,850 | $3 |
| Total | $63,267 | $8,063.40 | $8 |
NOTE: AMI = acute myocardial infarction, CVD = cardiovascular disease.
SOURCE: Nugent, 2015.
tive (Cecchini et al., 2010; WEF and WHO, 2011). Of note, 7 of the top 10 risk factors contributing to global DALYs affect cardiovascular health (Forouzanfar et al., 2016).4 Given that risk behaviors associated with the onset of CVD later in life often form during childhood and adolescence, a life course approach is critical to the prevention of NCDs (Lobstein et al., 2015). It is therefore important to target interventions in a comprehensive manner and develop approaches and interventions that change the nature of the consumer environment across the life course (e.g., changing availability, price, marketing practices that influence food choices and preferences) (Hawkes et al., 2015).
In addition to targeting risk factors through policy and regulatory means, communities and institutions can reduce CVD and cancer risk and thereby improve the health and well-being of their population by targeting service delivery. A critical component of this approach includes vaccination campaigns and screening programs, which can prevent the disease or catch it in its early stages before it devolves into a life-threatening illness or adverse event. The reach of policies and programs can be expanded by targeting points where the population already interfaces with the health care delivery system. Examples include integrating additional services into health care visits and conducting screening programs in high-traffic locations.
___________________
4 These include blood pressure, smoking, fasting plasma glucose, body mass index, total cholesterol, alcohol use, and sodium intake. For more, see http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)31679-8/abstract, Figure 7 (accessed April 20, 2017).
Across these various types of policy or health services interventions, the committee chose to prioritize prevention and early diagnosis. The committee urges U.S. global health programs to hone in on prevention and screening efforts to reduce disease incidence, contain disease progression in early stages, and decrease the economic burden in countries with high rates of CVD and cancer. Solutions for prevention of these diseases may also have a parallel impact on many other health outcomes as well, as many NCDs share risk factors. Moreover, solutions developed in other countries have the potential for application in the United States, as Americans also suffer from high burdens of CVD and cancer.
Fiscal and Regulatory Policies to Reduce Risk Factors for NCDs
Changes in individual behavior are difficult to achieve and maintain and the effects of behavior changes manifest over a long period of time. Fiscal and regulatory population-based approaches, which have been successful in reducing NCD risk factors such as smoking and alcohol consumption, are among the most effective means to curb the burden of CVD and cancer. Examples of such policies are discussed in the sections below.
Fiscal Policies
Fiscal approaches, often considered as part of a philosophy of “nudging,” are an attempt to change behaviors through taxation or subsidization (Hector, 2012). In a study comparing interventions to address obesity (e.g., food labeling, fiscal measures, worksite interventions, mass media) in Brazil, China, India, Mexico, Russia, and South Africa, fiscal measures were consistently found to be cost saving and generated the largest or second largest health effects in 20- and 50-year projections, in comparison to the other interventions (Cecchini et al., 2010). Another recent review and meta-analysis showed that a 10 percent price reduction or subsidy increases consumption of healthful foods and beverages by 14 percent, whereas the same price increase or tax reduces consumption of unhealthy foods or beverages by 7 percent (Afshin et al., 2015). For example, a sugar tax employed in Mexico, where a one peso per liter tax was levied on sugar-sweetened beverages, resulted in an overall 7.6 percent reduction in sugar-sweetened beverage purchases 2 years after the tax was levied (Colchero et al., 2017). The decrease in purchase rate was even greater among low-socioeconomic status households (11.6 percent) (Colchero et al., 2017), demonstrating how these fiscal and regulatory policies often benefit a country’s poorest the most. The health effects of this tax from 2013 to 2022 are likely to include substantially lower incidence of type 2 diabetes cases, strokes, and
myocardial infarctions, and fewer deaths. As a result, the tax is projected to save Mexico $983 million (Sánchez-Romero et al., 2016).
Fiscal approaches have also been proven as an effective means to curb tobacco use. Over 100 studies, including those done in LMICs, have shown that taxation has a major effect on rates of smoking (Summers and Jamison, 2013). The Lancet Commission on Investing in Health found that adding a 50 percent price increase in cigarettes through tax in China would avert 20 million deaths and generate an extra $20 billion in revenue over the next 50 years (Summers and Jamison, 2013). Additionally, a study in China that analyzed the impact of a tax of 50 percent on tobacco products revealed that the tax would most benefit the poor: Of the 231 million years of life gained as a result of the tax over 50 years, one-third of those are expected to be gained by the lowest socioeconomic quintile, and of the $24 billion of decreased expenditures on tobacco-related disease, 28 percent would benefit the lowest quintile (Verguet et al., 2015).
Regulatory Policies
In addition to fiscal measures, policy makers have used regulatory means to influence behavioral and environmental factors contributing to NCD burden. For tobacco use, for example, a widely used approach is the requirement of warning labels, which has proven be to effective in raising awareness of the dangers of tobacco and reducing consumption (Mallikarjun et al., 2014). For example, a study set in India revealed that for those who noticed the labels on tobacco products, 71.5 percent reported that the labels made them think about quitting smoking, and those individuals had much greater knowledge about the relationship between tobacco use and lung cancer (Mallikarjun et al., 2014). Given that tobacco-related illnesses are projected to kill 8 million people per year by 2030 (ASH, 2015), a dual pronged prevention strategy using taxation and regulation can assist in decreasing the burden of cigarette smoking.
Another key risk factor for many NCDs, often related to cigarette smoking, is air quality. In fact, approximately 2 billion children live in areas where pollution levels exceed the minimum air quality standards set by the World Health Organization (WHO) (UNICEF, 2016). Every year, nearly 600,000 children under the age of 5 die from diseases either caused or exacerbated by indoor or outdoor air pollution. With the growing trends of globalization and urbanization, many experts expect this number to climb unless conditions are improved. Improving air quality through reductions in pollution will not only help the children exposed, but will also realize benefits for the whole society—through increased productivity and more sustainable development (UNICEF, 2016). Given that deaths from air pollution cost the global economy $225 billion in lost labor income and more
than $5 trillion in welfare losses in 2013 (World Bank and IHME, 2016), a concerted effort toward improving air quality is needed. Opportunities for regulation exist to address air pollution from several angles, including limiting the open burning of waste or developing regulations for the detection of environmental diseases. For example, Israel’s Clean Air Law of 2008 set limits for emissions on major industrial polluters, in addition to spot checks and penalties for violation, and the Pollution Control Department in Thailand adopted new vehicle emissions standards and low sulphur fuel, decreasing Bangkok’s air pollution (UNEP, 2014). When done in cooperation with the private sector, air quality can be improved in a sustainable and cost-effective manner—leading to reduced mortality rates and economic burden.
Screening Programs for Early Detection and Treatment of Cardiovascular Disease
Blood pressure screening is a relatively inexpensive and simple health service that could easily be integrated with the existing health services offered through established U.S. global health programs. By offering blood pressure screening at the same location and using the same staff (after a period of training, as discussed below), U.S. global health programs could cost-effectively initiate CVD care in partner countries. Early screening alerts individuals that they are at risk for developing CVD, which can prompt behavior change and regular health care visits for improved management of the condition. Given the burden of CVD in LMICs, where 80 percent of deaths from CVD occur (Lozano et al., 2012; Pena and Bloomfield, 2015), and the knowledge that hypertension is a major risk factor for CVD screening will be a vital tool for reducing the burden of NCDs.
However, due to the additional social, political, and economic concerns in LMICs, it is important to contextualize the screening programs being implemented, as they will be contingent on the care services available, the supply chain of treatment regimens, the abilities of the medical providers in different locations, and the physical infrastructure of the health facilities. Vedanthan et al. (2015) examined CVD programs in western Kenya, noting that screening programs are just the first step of many required to ensure successful CVD prevention, and argued that the entire care cascade must be used effectively in order for the programs to be successful (see Box 6-1).
Immunization Strategies for Vaccine-Preventable Cancers
In recent years, cancer prevention has moved beyond screenings and early detection into the realm of primary prevention—or the prevention of disease before it even occurs. The two most common cancers in Africa—
cervical cancer and liver cancer—have been linked to infections with human papillomavirus (HPV) and hepatitis B, respectively. Consequently, the risk of developing these cancers can be substantially reduced through vaccination. Of the 250 million people chronically infected with hepatitis B worldwide, 600,000 die each year as a result of liver cancer or liver failure due to viral infection (Gavi, 2012). Similarly, HPV is estimated to cause 275,000 deaths annually through progression to cervical cancer, the majority of which occur in LMICs. Without changes in prevention and control measures, this number is projected to rise to more than 400,000 deaths by 2035 (Gavi, 2015). Vaccines against HPV and hepatitis B have the potential to prevent many of these deaths caused by cervical and liver cancers.
Mother-to-child transmission is the most common route of hepatitis B infection (Franco et al., 2012), although sexual contact is also an important mode. WHO’s Sector Strategy to Prevent Viral Hepatitis calls attention to a timely hepatitis B virus birth-dose vaccination as a key method to prevent mother-to-child transmission, an approach that could be enhanced through antenatal testing and the use of antiviral drugs (WHO, 2016b). The WHO strategy sets targets for 50 percent coverage by 2020 and 90 percent coverage by 2030 (WHO, 2016b). By the end of 2014, all low-income countries
had introduced the hepatitis B vaccine into routine immunization programs, and global childhood hepatitis B virus vaccination coverage had increased to more than 82 percent (WHO, 2016b). However, coverage of hepatitis B virus birth-dose lagged behind at just 38 percent (WHO, 2016b). Improving this birth-dose coverage could reduce the number of deaths related to hepatitis B.
Since 2006, HPV vaccination has contributed to a decrease in HPV incidence in young women in the United States by two-thirds (Hoffman, 2016), and a decline in cervical cancer rates are expected as vaccinated women age. With the help of Gavi, the Vaccine Alliance (Gavi), 1 million girls have been immunized against HPV in 19 countries since 2013 (Gavi, n.d.). This has been achieved through lowering the vaccine price, using schools and community centers to reach school-aged girls, integrating the vaccine with other routine vaccinations and adolescent health programs, and improving communication at the community level to raise awareness about HPV (Gavi, n.d.). However, a strategy beyond reliance on Gavi will be necessary, as many countries with a high HPV burden may not be Gavi eligible or may have recently graduated from its assistance, as is the case in southeast Asia (amfAR, 2016). In order to reach the largest number of girls and women at risk for developing cervical cancer, more comprehensive operations are needed. This may prove challenging, as barriers to increased vaccination rates in LMICs include mistrust of government health care programs and association of the vaccine with sexual activity (Agosti and Goldie, 2007), which plagues vaccine implementation in many high-income countries as well. Regardless, a concerted effort to increase HPV vaccination rates, thereby reducing the risk for cervical cancer, is a worthy endeavor, as cervical cancer now ranks as the fourth leading type of cancer for women across the world (WHO, 2016a). In response to this need, global support for HPV vaccination programs has grown in recent years. By building on the valuable efforts of Gavi and working to fill the gaps in HPV vaccine coverage, the United States can capitalize on this momentum and significantly contribute to the progress being made to reduce the burden of cervical cancer.
Although routine vaccines for cervical and liver cancers are effective low-cost preventive tools, early-stage detection is also critical for effective, less costly treatment for those not covered by preventive interventions or who have disease etiology that is not vaccine preventable. For example, a 4-year pilot project on early diagnosis achieved a 34 percent decrease in presentation of late-stage cervical cancer by enabling women to receive early stage treatment (Devi et al., 2007). Additional success has been shown in detection and treatment of early cervical cancer in Zambia, where simple interventions can be conducted without the need for costly infrastructure or highly trained specialists (see Box 6-2).
Finding: Evidence-based strategies and interventions exist to address CVD and cancers both at the population level (such as fiscal and regulatory policies) and at the health care delivery level (such as early screening and immunization campaigns).
TRANSFORMING HEALTH SYSTEMS FOR NONCOMMUNICABLE DISEASES
Instead of creating a new “vertical” or singular disease program for CVD or cancers, U.S. global health programs can leverage existing stakeholders and programs to address risk factors and care delivery more holistically. A great example of this is the newly launched Global Hearts initiative, a collaboration among WHO, the U.S. Centers for Disease Control and Prevention (CDC), the World Heart Federation, the World Stroke Organization, the International Society of Hypertension, and the World Hypertension League (WHO, 2016c). The initiative will provide governments with technical support needed to implement and scale up interventions—such as those highlighted in this chapter—to reduce blood pressure and prevent heart attacks and strokes. Beyond leveraging existing programs, changing the approach of health system design to be more integrated and holistic in nature, and decentralizing services at the community level can be beneficial for ensuring cost-effectiveness of programs and contextual sustainability.
Additionally, there is clear interest from the private sector for many reasons (Hancock et al., 2011; Sturchio and Goel, 2012). For multinational companies, keeping their workforce healthy and productive will improve their bottom line. For those companies in the health sector, there is an opportunity to create a market for themselves in LMICs that have a high burden of NCDs. Creating health systems that enable robust and sustainable care delivery will also improve the sustainability and growth of their company’s business. For these reasons, the committee feels that optimizing available resources and stakeholders through changes in health system design will be highly effective for improving cardiovascular health and preventing cancer, as explored in sections below.
Integration of Services at the Community Level
The dual burden of NCDs and infectious diseases in LMICs is exacerbated by well-documented interactions between communicable and noncommunicable diseases. For example, TB has been linked to an increased risk for stroke (Sheu et al., 2010) and lung cancer (Simonsen et al., 2014; Yu et al., 2011). Similarly, HIV/AIDS has been linked to an increased risk of cardiovascular disease (Hsue et al., 2012), in part due to the transition of HIV/AIDS as a chronic condition and AIDS patients now often living
to old age (Rabkin et al., 2012), and side effects of antiretroviral therapy (Subbaraman et al., 2007). HIV/AIDS also has been linked to a specific set of cancers (Grulich et al., 2007). Cervical cancer, for example, is four to five times more common in women who are HIV positive (PEPFAR, n.d.).
With these examples in mind, the traditional siloed, disease-specific care system will be hard pressed to address both communicable diseases and NCDs if done in isolation. Given that patients often suffer from both kinds of diseases, the effectiveness of health programs can be increased by integrating services—an approach that would seek to share locations, staff, systems, tools, and strategies (Rabkin et al., 2012). Such integration has been found to be successful in varying locations and approaches, with examples described in Box 6-2.
PEPFAR—a well-known successful investment—offers a unique opportunity for such integration. Along with the George W. Bush Institute, the Susan G. Komen Foundation, UNAIDS, and other partners, PEPFAR initiated the Pink Ribbon Red Ribbon (PRRR) campaign in 2011 (PRRR, n.d.). Since then, PRRR has screened thousands of women for cervical and breast cancer and provided HPV vaccinations (see Box 6-3). Continuing this vision of cross-sector services, PEPFAR entered into a public–private partnership with AstraZeneca in 2016 called Healthy Heart Africa, which integrates HIV infection reduction programs with hypertension screening targeting older men, a cohort often missed by standard HIV efforts (AstraZeneca, 2016). These types of focused partnerships featuring complementary goals and overlapping patient populations offer great opportunity to expand the reach and effectiveness of existing U.S. global health programs.
Decentralizing Services at the Community Level
Complementing the shift toward integration, the infrastructure and systems of LMICs must be transformed to meet the changing national health profiles in the long-term. While this will take time and sustained effort, there are short-term methods that can increase the capacity of countries to better address the burden of NCDs, including a broader use of the existing workforce. A 2015 assessment of community health workers in Bangladesh, Guatemala, Mexico, and South Africa found that health workers without formal professional training can be adequately trained to effectively screen for and identify people with a high risk of cardiovascular disease (Gaziano et al., 2015). Training existing staff to perform new tasks could free up the higher-level trained professionals to focus on those tasks requiring greater expertise. The concept of task shifting more generally has been found to be feasible in the management of hypertension and reducing cardiovascular risk (Poulter et al., 2015). This concept has also been successfully applied in cancer screening; the cervical cancer screening program in Zambia dis-
cussed in Box 6-2 promoted task shifting from doctors to nurses and used mobile technology to fill in any gaps and improve decision making (Parham et al., 2015). Box 6-4 provides an example of a community-based approach, including task-shifting to address CVD management.
Leveraging Private-Sector Involvement
Multinational companies understand the value of a healthier workforce in terms of increased productivity. In addition to being able to work for a greater number of years before retirement (and thus, spending more time contributing to society and less time deriving benefits from social welfare systems), healthier people are able to achieve higher-quality results in a shorter time period (Bloom et al., 2011).
Decades of work through existing platforms, such as those established by the U.S. Agency for International Development (USAID), the National Institutes of Health (NIH), PEPFAR, and others, have enabled U.S. global health programs to build strong international, national, and community-level networks. Leveraging this U.S. knowledge base and infrastructure, and creating an environment conducive to catalytic, innovative support and partnerships, can lead to more sustainable programs and improved outcomes. However, according to an insights report from the World Economic Forum’s Future of Health project, the willingness of the private and public sectors to coinvest depends on the right investment mechanisms being in place, on there being proof that those returns will materialize, and on the existence of a business model that makes it possible to share the benefits (WEF, 2015). This willingness has been growing in recent years and at the
World Economic Forum Annual Meeting in 2017, a collaborative initiative among more than 20 companies—Access Accelerated—was launched. Fifty million dollars was initially committed to improve access to NCD prevention, care, and treatment, in partnership with the Union of International Cancer Control and the World Bank (Access Accelerated, n.d.; IP Watch, 2017). There is potential to capitalize on this willingness and interest from the private sector to augment the current knowledge base and infrastructure to advance NCD efforts globally.
The committee believes the United States should build on such shared commitments and is poised to assist other companies and multilateral groups in contributing to the advancement of progress against NCDs. Although the existing U.S. vertical platforms can be leveraged for integrating services and expanding the scope of the current workforce, there will likely be difficulty and opposition to using existing funds to purchase commodities for treating international patients with conditions such as hypertension,
which is often a manifestation of behavior choices. However, public–private partnerships present unique opportunities and have already demonstrated successful results in many areas. Consider the previous example of PEPFAR and AstraZeneca’s partnership, as well as PEPFAR’s Determined, Resilient, Empowered, AIDS-free, Mentored, and Safe women (DREAMS) initiative, where a pharmaceutical company is purchasing medication for treatment in young women who are not eligible for coverage under PEPFAR. Additionally, the practice of matching resources to incentivize private involvement has also proven useful for PEPFAR programs in the past, by leveraging established supply chains and developing reference laboratories (Sturchio and Cohen, 2012). This method has been recommended for maternal and child health issues, and could easily be applied to NCD-focused partnerships.
Health companies have a vested interest in reaching the populations throughout LMICs that suffer from CVDs and cancers. Because these
TABLE 6-5 Private Companies Investing Their Own Resources in NCDs in Developing Countries
| Company | Disease Target | Impact |
|---|---|---|
| AstraZeneca | Hypertension | Through Healthy Heart Africa, AstraZeneca aimed to reach 10 million people with treatment for hypertension by 2025. By 2015, it had screened over 1 million people (AstraZeneca, 2015). |
| Novartis Access Program | CVD, diabetes, breast cancer, and respiratory illnesses | Novartis Access portfolio includes 15 on and off-patent medicines addressing CVD, type 2 diabetes, breast cancer, and respiratory illnesses. It is offered as a basket to countries for $1/treatment/month. Its goal is to provide access to 20 million patients annually by 2020 (Novartis, n.d.). |
| Pfizer | Healthy aging | Pfizer joined with HelpAge International in 2012 to reduce the NCD impact among the elderly in Tanzania. The partnership has led to the development of a tool that measures healthy aging in the elderly (Pfizer, 2016). |
| Medtronic Foundation “Health Rise” Program | CVD and diabetes | Health Rise is a 5-year, $17 million global effort funded by the Medtronic Foundation to expand access to care for CVD and diabetes among underserved populations in targeted areas in Brazil, India, South Africa, and the United States. It also works to strengthen health care delivery in the community and home-based settings (HealthRise, 2015). |
NOTE: CVD = cardiovascular disease; NCD = noncommunicable disease.
populations may not have access to the right medications because of either systemic or financial barriers, there is a gap that can draw mutual interest. If companies can create opportunities for larger numbers of people to purchase and depend on their medications, vaccines, and devices, they can eventually translate that increase to larger profits and sustainable business growth. Many companies have already invested their own resources in curbing the human and cost burden of NCDs in many countries (explored in more detail in Chapter 8). As an overview of the breadth of this private-sector interest, Table 6-5 gives examples of companies already investing in reducing the burden of CVDs and cancers, among other NCDs, around the world, through their own motivation.5
___________________
5 For a comprehensive listing of health development programs involving the research-based pharmaceutical industry, see the International Federation of Pharmaceutical Manufacturers and Associations Health Partnerships Directory at http://ncds.ifpma.org/partnerships-and-prevention/index.html (accessed March 19, 2017).
Finding: Integration, decentralization of services at the community level, and public–private partnerships are promising methods for transforming health systems in LMICs to provide better care for patients suffering from NCDs.
SUMMARY AND RECOMMENDATION
NCDs, such as CVD, COPD, and lung cancer, kill 40 million people annually, almost three-quarters of whom are in LMICs (WHO, 2017b). CVD is the leading cause of death worldwide, killing 18 million people in 2015. In addition, 14 million people are diagnosed with cancer each year, leading to 8.8 million deaths in 2015 (Stewart and Wild, 2014). In LMICs, more people die from cancer than from AIDS, TB, and malaria combined (Ferlay et al., 2013; WHO, 2014).
NCDs are projected to cause cumulative global economic output losses of $47 trillion by 2030, approximately 75 percent of the 2010 global GDP. The global cost of CVD alone was estimated at $906 billion in 2015, and it is projected to rise to more than $1 trillion annually in 2030 (Reddy et al., 2016). Global cancer costs are expected to reach $8.3 trillion annually by 2030, yet investing in cancer care and control could result in millions of avoidable deaths and up to $200 billion in global savings (Stewart and Wild, 2014).
With similar rising human and economic burdens in the United States, U.S. global health programs have a clear opportunity to address these conditions that contribute to an enormous global disease burden. However, NCDs often are incorporated into other programs as an afterthought, and an overall coordination mechanism or strategy for these diverse diseases is lacking. U.S. global health programs have established strong networks and knowledge bases in countries as a result of decades of effort by various agencies through infectious disease and maternal and child health platforms. There is an opportunity to integrate NCD prevention and care into these established platforms. Private, multinational companies also are becoming more invested in addressing chronic diseases, and there is an opportunity to leverage these established networks and this private-sector interest to develop coordinated public–private partnerships focused on high-impact, evidence-based interventions.
Conclusion: Without intervention, the burden of NCDs will grow in both epidemiological and economic terms. This burden of disease will have massive adverse effects on societies of all income levels, including high rates of premature death and lost productivity that will reverse trends of improved economic growth and stability in many countries.
Conclusion: Global health programs are not devoting adequate attention to the promotion of cardiovascular health and prevention of cancer. National governments, donor governments, and NGOs need to address these priorities through policy changes, vaccination against vaccine-preventable cancers, and programs that are community based and integrated into existing health services.
Conclusion: The private sector has strong interest in addressing NCDs globally owing to their clear effects on workforce productivity, but such private-sector efforts are not synergized across countries or health systems. To be effective, private-sector efforts need to be better coordinated with those of other stakeholders and networks.
Recommendation 9: Promote Cardiovascular Health and Prevent Cancer
The U.S. Agency for International Development, the U.S. Department of State, and the U.S. Centers for Disease Control and Prevention, through their country offices, should provide seed funding to facilitate the mobilization and involvement of the private sector in addressing cardiovascular disease and cancer at the country level. These efforts should be closely aligned and coordinated with the efforts of national governments and should strive to integrate services at the community level. The priority strategies to ensure highest impact are
- target and manage risk factors (e.g., smoking, alcohol use, obesity) for the major noncommunicable diseases, particularly through the adoption of fiscal policies and regulations that facilitate tobacco control and healthy diets;
- detect and treat hypertension early;
- detect and treat early cervical cancer; and
- immunize for vaccine-preventable cancers (specifically human papilloma virus and hepatitis B vaccines).
ANNEX 6-1
Steps to Reconstruct Tables 6-1 and 6-2
The data used to construct the tables were extracted from http://ghdx.healthdata.org/gbd-results-tool, and the same steps were used for both mortality and morbidity rankings. Once at the site, the following parameters were chosen:
- Context: Cause
- Age: All
- Sex: Both
- Measure: “Deaths” for mortality and “DALY” for morbidity
- Metric: Number
- Year: 2015
- Cause: All nonbolded causes from the list of causes, with the exception of hepatitis, liver cancer, cardiovascular diseases, cerebrovascular diseases, cirrhosis and other chronic liver diseases, chronic kidney disease, and road injuries.
- Location: United States, Southern Latin America, Central Latin America, Caribbean, Tropical Latin America, East Asia, N. Africa/Middle East, Southern Africa, West Africa, East Africa, and Central Africa
The nonbolded categories for “Cause” were included as the committee was interested in learning about their ranking as a whole when compared to the infectious diseases being targeted in the report. Furthermore, as the diseases of interest (cardiovascular diseases and cancers) have common determinants and interventions, the committee felt it would be beneficial to consider their ranking as a whole.
To obtain the rankings, all the parameters except location were selected for each region at a time. Then, once downloaded into Excel, the data was sorted by “Measure” and then ranked.
REFERENCES
Access Accelerated. n.d. What is access accelerated. http://www.accessaccelerated.org/about (accessed February 14, 2017).
Afshin, A., J. Penalvo, L. Del Gobbo, M. Kashaf, R. Micha, K. Morrish, J. Pearson-Stuttard, C. Rehm, S. Shangguan, J. D. Smith, and D. Mozaffarian. 2015. CVD prevention through policy: A review of mass media, food/menu labeling, taxation/subsidies, built environment, school procurement, worksite wellness, and marketing standards to improve diet. Currrent Cardiology Reports 17(11):98.
Agosti, J. M., and S. J. Goldie. 2007. Introducing HPV vaccine in developing countries—key challenges and issues. New England Journal of Medicine 356(19):1908-1910.
amfAR (American Foundation for AIDS Research). 2016. Cervical cancer, human papillomavirus (HPV), and HPV vaccines in Southeast Asia: Key considerations for expanding vaccine coverage and improving population health. New York: The American Foundation for AIDS Research.
ASH (Action on Smoking and Health). 2015. Tobacco and the developing world fact sheet. Washington, DC: Action on Smoking and Health.
AstraZeneca. 2015. Access to healthcare sustainability update 2015. https://www.astrazeneca.com/content/dam/az/our-company/Sustainability/accesstohealthcare/Access%20to%20healthcare%20update%202015.pdf (accessed February 10, 2017).
AstraZeneca. 2016. PEPFAR and AstraZeneca launch partnership across HIV and hypertension services in Africa. Washington, DC: AstraZeneca.
Babiarz, K. S., G. Miller, H. Yi, L. Zhang, and S. Rozelle. 2012. China’s new cooperative medical scheme improved finances of township health centers but not the number of patients served. Health Affairs (Millwood) 31(5):1065-1074.
Bloom, D. E., E. T. Cafiero, E. Jané-Llopis, S. Abrahams-Gessel, L. R. Bloom, S. Fathima, A. B. Feigl, T. Gaziano, M. Mowafi, A. Pandya, K. Prettner, L. Rosenberg, B. Seligman, A. Z. Stein, and C. Weinstein. 2011. The global economic burden of noncommunicable diseases. Geneva, Switzerland: World Economic Forum.
Cecchini, M., F. Sassi, J. A. Lauer, Y. Y. Lee, V. Guajardo-Barron, and D. Chisholm. 2010. Tackling of unhealthy diets, physical inactivity, and obesity: Health effects and cost-effectiveness. The Lancet 376(9754):1775-1784.
Chaker, L., A. Falla, S. J. van der Lee, T. Muka, D. Imo, L. Jaspers, V. Colpani, S. Mendis, R. Chowdhury, W. M. Bramer, R. Pazoki, and O. H. Franco. 2015. The global impact of non-communicable diseases on macro-economic productivity: A systematic review. European Journal of Epidemiology 30(5):357-395.
Colchero, M. A., J. Rivera-Dommarco, B. M. Popkin, and S. W. Ng. 2017. In Mexico, evidence of sustained consumer response two years after implementing a sugar-sweetened beverage tax. Health Affairs (Millwood) 36(3):564-571.
Daniels, Jr., M. E., T. E. Donilon, and T. Bollyky. 2014. The emerging global health crisis: Noncommunicable diseases in low- and middle-income countries. Washington, DC: Council on Foreign Relations.
Devi, B. C., T. S. Tang, and M. Corbex. 2007. Reducing by half the percentage of late-stage presentation for breast and cervix cancer over 4 years: A pilot study of clinical downstaging in Sarawak, Malaysia. Annals of Oncology 18(7):1172-1176.
Ferlay, J., I. Soerjomataram, M. Ervik, R. Dikshit, S. Eser, C. Mathers, M. Rebelo, D. Parkin, D. Forman, and F. Bray. 2013. GLOBOCAN 2012 v1.0: Cancer incidence and mortality worldwide. Lyon, France: IARC CancerBase.
FHI 360 (Family Health International 360). 2014. Community-based hypertension improvement project (comHIP). https://www.fhi360.org/projects/community-based-hypertension-improvement-project-comhip (accessed March 24, 2017).
Forouzanfar, M. H., A. Afshin, L. T. Alexander, H. R. Anderson, Z. A. Bhutta, S. Biryukov, M. Brauer, et al. 2016. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. The Lancet 388(10053):1659-1724.
Franco, E., B. Bagnato, M. G. Marino, C. Meleleo, L. Serino, and L. Zaratti. 2012. Hepatitis B: Epidemiology and prevention in developing countries. World Journal of Hepatology 4(3):74-80.
Gavi (Gavi, the Vaccine Alliance). 2012. Vaccines and cancer control: From hepatitis B to HPV. http://www.gavi.org/partnersforum2012/session-summaries/22-%E2%80%93-vaccines-and-cancer-control--from-hepatitis-b-to-hpv (accessed February 14, 2017).
Gavi. 2015. Keeping children healthy: The Vaccine Alliance progress report 2015. Washington, DC: Gavi, the Vaccine Alliance.
Gavi. n.d. Human papillomavirus vaccine support. http://www.gavi.org/support/nvs/human-papillomavirus (accessed February 14, 2017).
Gaziano, T. A., S. Abrahams-Gessel, C. A. Denman, C. M. Montano, M. Khanam, T. Puoane, and N. S. Levitt. 2015. An assessment of community health workers’ ability to screen for cardiovascular disease risk with a simple, non-invasive risk assessment instrument in Bangladesh, Guatemala, Mexico, and South Africa: An observational study. Lancet Global Health 3(9):e556-e563.
Global to Local. n.d. Global to Local: Mobile health program. http://www.globaltolocal.org/programs/2016/4/5/mobile-health-program (accessed February 14, 2017).
Grulich, A. E., M. T. van Leeuwen, M. O. Falster, and C. M. Vajdic. 2007. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. The Lancet 370(9581):59-67.
Hallsworth, M. S., V. Snijders, H. Burd, J. Prestt, G. Judah, S. Huf, and D. Halpern. 2016. Applying behavioral insights: Simple ways to improve health outcomes. Doha, Qatar: World Innovation Summit for Health.
Hancock, C., L. Kingo, and O. Raynaud. 2011. The private sector, international development and NCDS. Globalization and Health 7(1):23.
Hawkes, C., T. G. Smith, J. Jewell, J. Wardle, R. A. Hammond, S. Friel, A. M. Thow, and J. Kain. 2015. Smart food policies for obesity prevention. The Lancet 385(9985):2410-2421.
HealthRise. 2015. What is HealthRise? https://www.health-rise.org/about-healthrise/what-is-healthrise (accessed February 14, 2017).
Hector, C. 2012. Nudging towards nutrition? Soft paternalism and obesity-related reform. Food and Drug Law Journal 67(1):iii-iv, 103-122,.
Hoffman, J. 2016. HPV sharply reduced in teenage girls following vaccine, study says. The New York Times, February 22.
Hsue, P. Y., S. G. Deeks, and P. W. Hunt. 2012. Immunologic basis of cardiovascular disease in HIV-infected adults. Journal of Infectious Diseases 205 (Suppl 3):S375-S382.
IP (Intellectual Property) Watch. 2017. Brief: Industry initiative against non-communicable diseases launched at WEF. Intellectual Property Watch, January 19.
Jamison, D., L. Summers, G. Alleyne, K. Arrow, S. Berkeley, A. Binagwaho, F. Bustreo, D. Evans, R. Feachern, J. Frenk, G. Ghosh, S. Goldie, Y. Guo, S. Gupta, R. Horton, M. Kruk, A. Mahmoud, L. Mohohlo, M. Ncube, A. Pablos-Mendez, S. Reddy, H. Saxenian, A. Soucat, K. Ulltveit-Moe, and G. Yamey. 2013. Global Health 2035: A world converging within a generation. The Lancet 382:1898-1955.
Janssens, B., W. Van Damme, B. Raleigh, J. Gupta, S. Khem, K. Soy Ty, M. Vun, N. Ford, and R. Zachariah. 2007. Offering integrated care for HIV/AIDS, diabetes and hypertension within chronic disease clinics in Cambodia. Bulletin of the World Health Organization 85(11):880-885.
Keck, C. W. 2016. The United States and Cuba—turning enemies into partners for health. New England Journal of Medicine 375(16):1507-1509.
Lobstein, T., R. Jackson-Leach, M. L. Moodie, K. D. Hall, S. L. Gortmaker, B. A. Swinburn, W. P. T. James, Y. Wang, and K. McPherson. 2015. Child and adolescent obesity: Part of a bigger picture. The Lancet 385(9986):2510-2520.
Lozano, R., M. Naghavi, K. Foreman, S. Lim, K. Shibuya, V. Aboyans, J. Abraham, et al. 2012. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet 380(9859):2095-2128.
Mallikarjun, S., A. Rao, G. Rajesh, R. Shenoy, and M. P. Bh. 2014. Role of tobacco warning labels in informing smokers about risks of smoking among bus drivers in Mangalore, India. Asian Pac Journal of Cancer Prevention 15(19):8265-8270.
Muka, T., D. Imo, L. Jaspers, V. Colpani, L. Chaker, S. J. van der Lee, S. Mendis, R. Chowdhury, W. M. Bramer, A. Falla, R. Pazoki, and O. H. Franco. 2015. The global impact of non-communicable diseases on healthcare spending and national income: A systematic review. European Journal of Epidemiology 30(4):251-277.
Nenna, R., P. Papoff, C. Moretti, A. Pierangeli, G. Sabatino, F. Costantino, F. Soscia, G. Cangiano, V. Ferro, M. Mennini, S. Salvadei, C. Scagnolari, G. Antonelli, and F. Midulla. 2011. Detection of respiratory viruses in the 2009 winter season in Rome: 2009 influenza A (H1N1) complications in children and concomitant type 1 diabetes onset. International Journal of Immunopathology and Pharmacology 24(3):651-659.
Novartis. n.d. Novartis Access. https://www.novartis.com/about-us/corporate-responsibility/expanding-access-healthcare/novartis-access (accessed February 14, 2017).
Novartis Foundation. 2016. ComHIP. http://www.novartisfoundation.org/_file/607/comhipfactsheet.pdf (accessed March 8, 2017).
Nugent, R. 2015. Benefits and costs of the noncommunicable disease targets for the post-2015 development agenda. Tewksbury, MA: Copenhagen Consensus Center.
Nyambura, Z. 2017. Cancer: Africa’s new health burden. Deutsche Welle, February 4.
O’Rourke, K. 2017. Projecting, reducing the burden of cardiovascular disease by 2025. http://www.healthdata.org/acting-data/projecting-reducing-burden-cardiovascular-disease-2025 (accessed March 29, 2017).
Parham, G. P., M. H. Mwanahamuntu, S. Kapambwe, R. Muwonge, A. C. Bateman, M. Blevins, C. J. Chibwesha, K. S. Pfaendler, V. Mudenda, A. L. Shibemba, S. Chisele, G. Mkumba, B. Vwalika, M. L. Hicks, S. H. Vermund, B. H. Chi, J. S. A. Stringer, R. Sankaranarayanan, and V. V. Sahasrabuddhe. 2015. Population-level scale-up of cervical cancer prevention services in a low-resource setting: Development, implementation, and evaluation of the cervical cancer prevention program in Zambia. PLOS ONE 10(4):e0122169.
Pena, M. S. B., and G. S. Bloomfield. 2015. Cardiovascular disease research and the development agenda in low- and middle-income countries. Global Heart 10(1):71-73.
PEPFAR (The U.S. President’s Emergency Plan for AIDS Relief). 2017. Congressional budget justification supplement: President’s Emergency Plan for AIDS Relief (PEPFAR). Washington, DC: U.S. Department of State.
PEPFAR. n.d. Pink Ribbon Red Ribbon: A global partnership fighting women’s cancers. https://www.pepfar.gov/partnerships/ppp/prrr/index.htm (accessed February 14, 2017).
Pfizer. 2016. Healthy aging. https://www.pfizer.com/files/investors/financial_reports/annual_reports/2015/healthy-aging.htm (accessed February 14, 2017).
Piccini, B., S. Toni, L. Lenzi, M. Guasti, F. Barni, and M. De Martino. 2012. Type 1 diabetes onset and pandemic influenza A (H1N1). International Journal of Immunopathology and Pharmacology 25(2):547-549.
Poulter, N. R., D. Prabhakaran, and M. Caulfield. 2015. Hypertension. Lancet 386(9995): 801-812.
PRRR (Pink Ribbon Red Ribbon). 2016. Our impact. http://pinkribbonredribbon.org/our-impact (accessed February 14, 2017).
PRRR. n.d. Pink ribbon red ribbon: Our story. http://pinkribbonredribbon.org/our-story (accessed February 14, 2017).
Rabkin, M., M. E. Kruk, and W. M. El-Sadr. 2012. HIV, aging and continuity care: Strengthening health systems to support services for noncommunicable diseases in low-income countries. AIDS 26(Suppl 1):S77-S83.
Reddy, S., F. Riahi, G. Dorling, R. Callahan, and H. Patel. 2016. Innovative approaches to prevention: Tackling the global burden of cardiovascular disease. Doha, Qatar: World Innovation Summit for Health.
Samb, B., N. Desai, S. Nishtar, S. Mendis, H. Bekedam, A. Wright, J. Hsu, A. Martiniuk, F. Celletti, K. Patel, F. Adshead, M. McKee, T. Evans, A. Alwan, and C. Etienne. 2010. Prevention and management of chronic disease: A litmus test for health-systems strengthening in low-income and middle-income countries. The Lancet 376(9754):1785-1797.
Sánchez-Romero, L. M., J. Penko, P. G. Coxson, A. Fernández, A. Mason, A. E. Moran, L. Ávila-Burgos, M. Odden, S. Barquera, and K. Bibbins-Domingo. 2016. Projected impact of Mexico’s sugar-sweetened beverage tax policy on diabetes and cardiovascular disease: A modeling study. PLOS Medicine 13(11):e1002158.
Sheu, J. J., H. Y. Chiou, J. H. Kang, Y. H. Chen, and H. C. Lin. 2010. Tuberculosis and the risk of ischemic stroke: A 3-year follow-up study. Stroke 41(2):244-249.
Simonsen, D. F., D. K. Farkas, M. Sogaard, C. R. Horsburgh, H. T. Sorensen, and R. W. Thomsen. 2014. Tuberculosis and risk of cancer: A Danish nationwide cohort study. International Journal of Tuberculosis and Lung Disease 18(10):1211-1219.
Stewart, B. W., and C. P. Wild. 2014. World cancer report 2014. Lyon, France: International Agency for Research on Cancer, World Health Organization.
Sturchio, J. L., and G. M. Cohen. 2012. How PEPFAR’s public-private partnerships achieved ambitious goals, from improving labs to strengthening supply chains. Health Affairs (Millwood) 31(7):1450-1458.
Sturchio, J. L., and A. Goel. 2012. The private-sector role in public health: Reflections on the new global architecture in health. Washington, DC: Center for Strategic and International Studies.
Subbaraman, R., S. K. Chaguturu, K. H. Mayer, T. P. Flanigan, and N. Kumarasamy. 2007. Adverse effects of highly active antiretroviral therapy in developing countries. Clinical Infectious Diseases 45(8):1093-1101.
Summers, L., and D. Jamison. 2013. Policy brief #3: Curbing non-communicable diseases and injuries. New York: The Lancet.
UNEP (United Nations Environment Programme). 2014. Actions on air quality: Policies & programmes for improving air quality around the world. Washington, DC: United Nations Environment Programme.
UNICEF (United Nations International Children’s Emergency Fund). 2016. Clear the air for children: The impact of pollution on children. New York: United Nations International Children’s Emergency Fund.
Vedanthan, R., J. H. Kamano, G. S. Bloomfield, I. Manji, S. Pastakia, and S. N. Kimaiyo. 2015. Engaging the entire care cascade in western Kenya: A model to achieve the cardiovascular disease secondary prevention roadmap goals. Global Heart 10(4):313-317.
Verguet, S., C. L. Gauvreau, S. Mishra, M. MacLennan, S. M. Murphy, E. D. Brouwer, R. A. Nugent, K. Zhao, P. Jha, and D. T. Jamison. 2015. The consequences of tobacco tax on household health and finances in rich and poor smokers in China: An extended cost-effectiveness analysis. The Lancet Global Health 3(4):e206-e216.
Wang, H., M. Naghavi, C. Allen, R. M. Barber, Z. A. Bhutta, A. Carter, D. C. Casey, et al. 2016. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. The Lancet 388(10053):1459-1544.
WEF (World Economic Forum). 2015. Maximizing healthy life years: Investments that pay off. Geneva, Switzerland: World Economic Forum.
WEF and WHO (World Health Organization). 2011. From burden to “best buys”: Reducing the economic impact of non-communicable diseases in low- and middle-income countries. Geneva, Switzerland: World Economic Forum and World Health Organization.
WHO (World Health Organization). 2014. Global health observatory: The data repository. http://www.who.int/gho/database/en (accessed April 5, 2017).
WHO. 2016a. Fact sheet: Human papillomavirus (HPV) and cervical cancer. http://www.who.int/mediacentre/factsheets/fs380/en (accessed March 30, 2017).
WHO. 2016b. Global health sector strategy on viral hepatitis 2016-2021: Towards ending viral hepatitis. Geneva, Switzerland: World Health Organization.
WHO. 2016c. New initiative launched to tackle cardiovascular disease, the world’s number one killer. Geneva, Switzerland: World Health Organization.
WHO. 2017a. Cancer fact sheet. http://www.who.int/mediacentre/factsheets/fs297/en (accessed April 4, 2017).
WHO. 2017b. Noncommunicable diseases fact sheet. http://www.who.int/mediacentre/factsheets/fs355/en (accessed March 20, 2017).
WHO. 2017c. Yearly, 8.8 million people die from cancer. Dhaka, Bangladesh: World Health Organization.
Wirtz, V. J., W. A. Kaplan, Y. S.-A. Téllez, and R. L. Ridaura. 2011. Affordable, quality, long-term care and pharmacotherapy of chronic diseases: A framework for low and middle income countries. Geneva, Switzerland: World Health Organization.
World Bank and IHME (Institute of Health Metrics and Evaluation). 2016. The cost of air pollution: Strengthening the economic case for action. Washington, DC: World Bank and Institute for Health Metrics Evaluation.
Yu, Y. H., C. C. Liao, W. H. Hsu, H. J. Chen, W. C. Liao, C. H. Muo, F. C. Sung, and C. Y. Chen. 2011. Increased lung cancer risk among patients with pulmonary tuberculosis: A population cohort study. Journal of Thoracic Oncology 6(1):32-37.
Zhang, L., and N. Liu. 2014. Health reform and out-of-pocket payments: Lessons from China. Health Policy Plan 29(2):217-226.


































