
The first session of the workshop, which was moderated by Parris Glendening, president of Smart Growth America’s Leadership Institute and the Governors’ Institute on Community Design and governor of Maryland from 1995 to 2003, provided an overview of the relationship among the built environment, obesity, and health. In his opening remarks, he framed the session by describing the current built environment as a contributor to poor health outcomes, stating,
It simply does not make any sense that a 2,000-pound machine that we call an automobile drives 2 miles in order to get 1 quart of milk. Yet that is not only the way many people live, that is what we continue to build in significant parts of the country. . . . People are still getting sick, limiting their quality of life, and dying because of decisions that continue to be made about the built environment.
This topic was explored further by the session’s presenters. The first presenter outlined a broad framework that links urban planning and policy decisions to human health and well-being, and the next two presenters looked more closely at the roles of transportation, land use, and the food environment in the health of individuals and communities.
A FRAMEWORK FOR INTERVENTIONS
The 21st century poses many challenges to human health, including chronic disease, depression, road traffic injuries, air pollution, chronic noise, social isolation, fear of crime, and health inequities, observed Rodrigo Reis, professor of public health, Washington University, St. Louis, Missouri. All of these health challenges can be connected to urban planning, city design, and social policies, he asserted. He added that this connection between health and the built environment is garnering increased attention worldwide, noting further that six of the goals and 14 of the targets in the United Nations Sustainable Development Goals are connected to urban planning or design (United Nations, 2015).
Built environments are interconnected with human lives, Reis continued. To illustrate this point, he used the example of how urban planning can mediate the impact of natural disasters. During such a tragedy, he explained, a lack of proper urban planning can make life worse for people on the ground, and the consequences can be especially severe for people with limited resources. He noted that this workshop was being held shortly after Hurricanes Harvey and Irma had devastated parts of the Caribbean islands and the U.S. mainland, observing that “the human tragedies we are seeing now are reminding us how important it is to know where and how to make society a better place for everybody.”
Reis was co-author of a paper in the September 23, 2016, special issue of The Lancet on urban design, transport, and health (Giles-Corti et al., 2016). That paper lays out a comprehensive framework of direct and indirect pathways through which urban planning and design decisions influence health and well-being (see Figure 2-1). The authors also describe eight strategies that urban policy makers can use to improve the health of city dwellers. The urban and transport planning and design interventions in the framework are organized around eight constructs within regional planning (destination accessibility, distribution of employment, and demand management) and local urban design (design, density, distance to transit, diversity, and desirability).
Reis pointed out that this framework goes well beyond the health sector, calling for integration of policies around transport, employment and economic development, social and health services, education, land use and urban design, housing, public open space and recreation, and public safety. “We are advocating for those different sectors to coordinate their actions around planning and designing cities,” he said. He argued that although different sectors have different priorities, they can still work together on priorities they share, including health outcomes. Coordinated action, he explained, is key. “If we coordinate actions across those different sectors, we are more likely to make improvements in regional planning and local design,” he explained. “We are talking about a more comprehensive approach to improve cities for everybody.”
The interventions suggested by the framework cannot be implemented without proper governance, Reis insisted. He elaborated by explaining that good governance has several components: it is accountable, transparent, responsive, equitable, inclusive, effective, efficient, participatory, consensus oriented, and law-abiding. He observed that in places such as the United States, where the governance structure is well established, interventions can be easier to implement. “It is essential to talk about proper governance, because somebody needs to pay for changes,” he said. “Somebody needs to invest time, money, and political will.” He added that public demand is the major driver for changes in public transportation, and transportation demand is influenced by attitudes and preferences, social and cultural norms, and mobility needs. Therefore, he argued, if transportation is to change, people may need to advocate for access to high-quality public transportation, cycling, walking, and reduced use of private cars.
Reis continued by explaining that the framework (see Figure 2-1) identifies eight risk exposures—traffic, air pollution, noise, social isolation, personal safety, physical inactivity, prolonged sitting, and unhealthy diet—related to urban and transport planning and design decisions, which it divides into environmental, social, and behavioral categories. The interventions included in the framework are meant to reduce each of these risks.
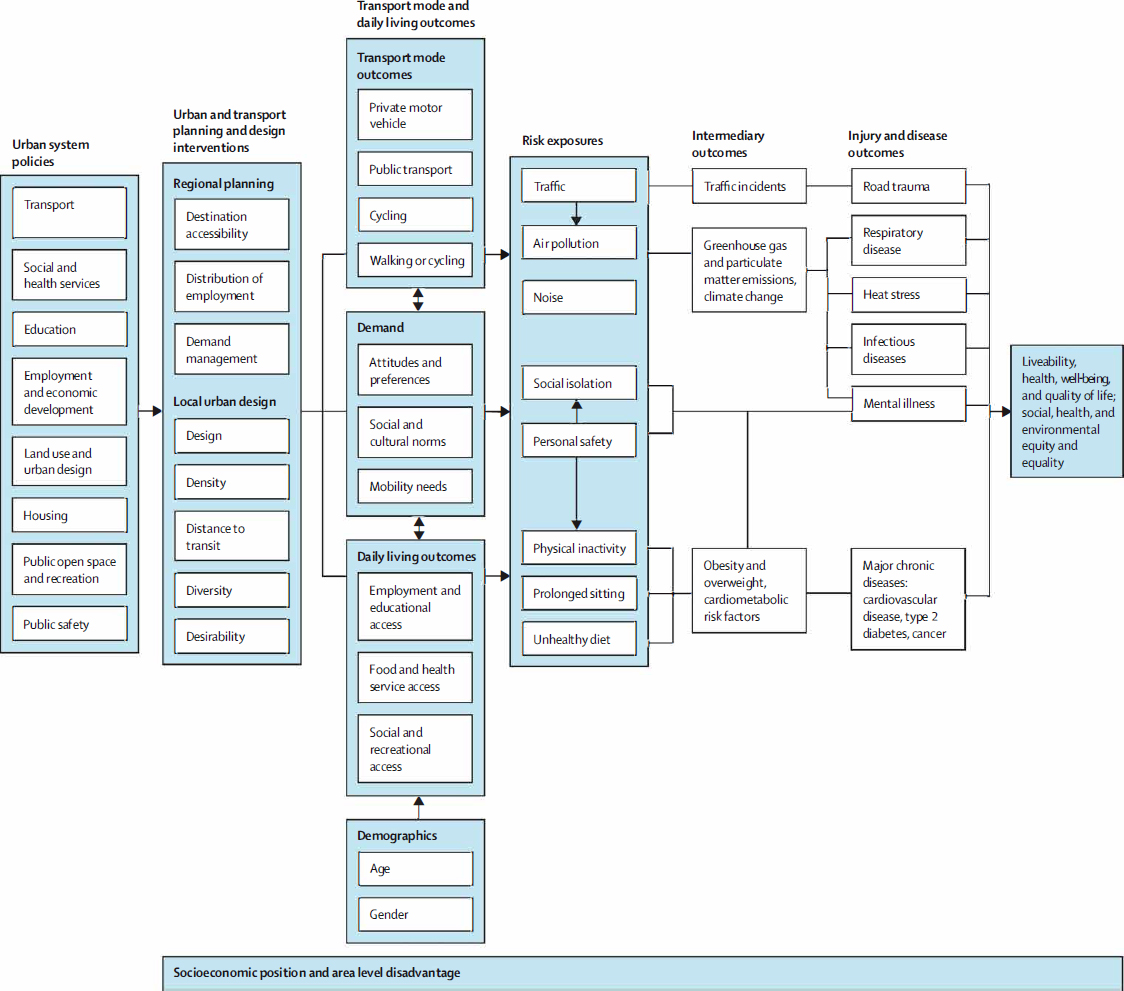
SOURCES: Presented by Rodrigo Reis, September 12, 2017. Reprinted from The Lancet, Vol. 388, Billie Giles-Corti, Anne Vernez-Moudon, Rodrigo Reis, Gavin Turrell, Andrew L. Dannenberg, Hannah Badland, Sarah Foster, Melanie Lowe, James F. Sallis, Mark Stevenson, Neville Owen, City planning and population health: A global challenge, 2912–2924, Copyright (2016), with permission from Elsevier.
Changing these risk exposures can have multiple effects, Reis observed. He gave the example of increasing active transportation (walking, cycling, and public transportation), which can have a direct health benefit for the people who partake, but can also reduce air pollution, noise, and social isolation and is likely to have other beneficial economic and social effects. Over time, he asserted, the switch to active transport could lead to lower prevalence of obesity and other metabolic risk factors. In this way, he added, interventions can address multiple risk factors and encourage multiple positive outcomes.
Reis went on to explain that the framework provides a set of indicators that can be used to monitor cities’ progress in implementing policies, interventions, and outcomes that enhance health and reduce noncommunicable diseases. These indicators include legislation and policies, government investments in transportation, urban and transportation planning and design practices, transportation outcomes, and risk exposure outcomes (Giles-Corti et al., 2016). According to Reis, cities can use these indicators to guide their investments and to monitor the progress and cost-effectiveness of those investments. Many cities, he observed, have done well in tracking risk exposure indicators (such as obesity and physical activity), but have struggled to track urban planning–related indicators. “We need a more integrated approach to monitor progress,” he asserted. “It is not only about monitoring health-related outcomes progress but also about a city’s progress across the whole spectrum of outcomes.”
Reis then cited another paper in the same issue of The Lancet, looking at how density, diversity of land use, distance from public transportation, and transportation patterns affect health-related outcomes in six different cities (Stevenson et al., 2016). The authors of that paper estimated the health burden due to land use and transport mode choices and found major differences among Boston, Copenhagen, Delhi, London, Melbourne, and São Paulo, in part, said Reis, because of “poor management or poor planning strategies.” The researchers then modeled the effects of increasing the diversity and density of land use by 30 percent each, reducing the distance to public transportation by 30 percent, and shifting the modes of transport by 10 percent so that people would bike and walk more. “This is a scenario that isn’t so difficult to imagine,” Reis observed. The result of the model, he explained, was substantial improvements in health in terms of cardiovascular disease, type 2 diabetes, and respiratory diseases. However, he added, this model did not account for infrastructure changes, so road trauma increased with more people walking or biking. Thus, he argued, “We have to invest in infrastructure. Let’s repair cities for people to be able to choose to walk or bike or use public transportation.”
Reis asserted that the framework shown in Figure 2-1 provides a solid way forward, but a major remaining question is how to engage people
in all sectors to make healthful changes in the built environment. He is in the process of surveying planners, designers, traffic engineers, public health professionals, and parks and recreation professionals across the United States about their priority actions for creating livable cities and communities. The early results, he reported, suggest the need to shift the message toward a comprehensive approach to engage practitioners from many sectors in developing healthy communities. He added that although practitioners from different sectors assigned different levels of importance to health, respondents from all sectors talked about community, economic development, and support for social systems. A message focused entirely on health “is not working,” he said. “Maybe to engage different sectors we have to message a little differently. . . . If people can’t live a decent life, if they can’t have access to a thriving community and city, how can they overcome the barriers they need to make healthy choices?” He suggested that emphasizing the co-benefits of changes to the built environment, which are identified by Sallis and colleagues (2015) in an extensive literature review, can be a useful way to engage nonhealth sectors. For example, he added, rather than talking about the health benefits of parks, community leaders can emphasize social benefits such as an enhanced environment and safety, and when talking about transportation systems or denser cities, they can describe the benefits in terms of environmental stability, social benefits, safety, and economic benefits. He closed by saying, “Let’s think about how we can message the work around urban planning, city design, and health, [taking] a more comprehensive and effective approach.”
TRANSPORTATION AND LAND USE
Daniel A. Rodríguez, chancellor’s professor in the Department of City and Regional Planning, University of California, Berkeley, used as the starting point for his presentation Reis’s observation that transportation and land use are two of the mediators of the built environment’s effect on health. Therefore, he asserted, research on these mediators is important to understanding the evidence regarding interventions.
To illustrate the importance of these environmental exposures, Rodríguez reviewed some of the research on the health impacts of transportation elements such as street connectivity, traffic, bicycling infrastructure, and access to mass transit. He began by observing that higher connectivity in street grids leads to shorter distances from one place to another and greater safety from traffic, which can encourage people to walk or bike rather than drive. He cited the example of the RESIDE project in Perth, Australia, which studied more than 1,800 participants in 73 neighborhoods from 2003 to 2012 and found that street connectivity was associated with more walking (Knuiman et al., 2014). In a follow-up to that study, however,
Veerman and colleagues (2016) found that in low-density cities, installing sidewalks in existing neighborhoods as a single intervention is unlikely to improve health in a cost-effective way. According to Rodríguez, this result “makes a lot of sense.” He explained that sidewalks, in conjunction with destinations to visit and higher population density, are likely to be more cost-effective than isolated sidewalk interventions. “The peek-a-boo sidewalks that we see in suburban U.S.—now you see them, now you don’t, they have dead ends—that doesn’t help us very much,” he asserted. “We want sidewalks that give us connectivity and lead to places and connect us with places.”
Rodríguez continued by reporting that with regard to traffic, Jerrett and colleagues (2010) found, after correcting for a wide variety of con-founders, that high traffic around the home was associated with higher obesity in children. The effect varied by the child’s proximity to traffic: children whose homes were closest (within 150 meters) to high-traffic areas had higher body mass indexes (BMIs) at age 18 relative to those whose homes were farthest (500 meters). The difference in BMI was fairly small—about a 5 percent difference at age 18—but, Rodriguez emphasized, this difference has substantial implications for a large population. He added that “the traffic was really acting as a surrogate for pollution, or maybe as a big barrier . . . for getting places.”
Rodríguez continued by noting that increasing rates of biking is one way to increase physical activity, but enthusiasm for biking varies from person to person. He cited a popular heuristic that divides commuters into four categories based on their attitudes toward cycling: strong and fearless (fewer than 1 percent), enthused and confident (about 7 percent), interested but concerned (60 percent), and uninterested (33 percent) (Geller, 2009). He also referred to a study of commuting and health in Cambridge, Massachusetts, that followed 809 adults over 3 years. He reported that after adjusting for a variety of individual-level characteristics and other physical activity, the researchers found that those who commuted by bicycle for 1 year had reduced their BMI by an average of 1.14 points at the end of the year (Mytton et al., 2016). He added that when new bicycle lanes were built in Salt Lake City as part of the city’s Complete Streets investments, longer cycling trips, as tracked by accelerometers and GPS loggers, were associated with lower BMI and more calories burned (Brown et al., 2016).
Finally, turning to mass transit, Rodríguez cited an analysis of National Household Travel Survey data in which it was found that people who walked to and from transit did so for a median of 21 minutes each day (Freeland et al., 2013). He reported that “50 percent of all transit commuters got 100 minutes a week of physical activity walking solely for getting to and from transit,” adding that “if this is not a public health intervention, I don’t know what is.” He further cited a pair of studies examining the
effect of new light rail transit systems in two cities, which found that new transit users reduced their BMI over time. In Salt Lake City, residents who started using the city’s new light rail became more active and decreased their BMI by 0.29. In contrast, people who previously were using the bus and then no longer did so increased their BMI over time, became more sedentary, and engaged in less physical activity (Brown et al., 2015). In Charlotte, North Carolina, new light rail commuters reduced their odds of becoming overweight or obese over time by 81 percent (MacDonald et al., 2010). Similarly, Rodríguez reported, at the county level, vehicle miles traveled were associated with higher obesity in California (Lopez-Zetina et al., 2006). “All the evidence in this case is fairly convincing and pointing in the same direction,” he asserted.
The second element of the built environment Rodríguez discussed was land use, with a focus on the mixing of land uses—such as intermingling residential, retail, and office space in the same neighborhood—and greater density of people, places, and things. He cited a recent review of 92 studies, which found that the lack of mixed land uses and urban sprawl are associated with overweight or obesity more consistently relative to other physical environmental factors (Mackenbach et al., 2014). He also noted that mixing land uses and mixing increasing residential density were two strategies recommended by the Community Preventive Services Task Force for increasing physical activity (Community Preventive Services Task Force, 2016b) and argued that it is the combination of these two elements that works. He added that increasing density can increase the efficacy and cost-effectiveness of certain built environment interventions.
Transportation and land use are part of a “package,” Rodríguez continued, and “it is all of these things mixed together that seem to matter more.” He cited walkability as an example of how land use and transportation can be packaged together, explaining that measures of walkability use density, land use mix, connectivity, safety, and overall location to estimate the feasibility of walking to reach many destinations. He reported that emerging cross-sectional evidence shows that environmental factors, when combined, are related to less overweight and obesity around the world. To illustrate this point, he cited a study of more than 14,000 adults in 17 cities across 12 countries demonstrating that a combination of two factors—safety from traffic and crime and close proximity to local destinations—was strongly correlated with lower BMI (De Bourdeaudhuij et al., 2015).
Rodríguez then described another study of 730 families in Seattle and San Diego, which found that characteristics of children’s neighborhoods were associated with their weight status, even after controlling for sociodemographic variables and their parents’ weight status (Saelens et al., 2012). Children living in neighborhoods with favorable measures of both physical
activity and neighborhood environments were less likely to have overweight and obesity than their peers in neighborhoods with unfavorable measures.
Rodríguez went on to report that the Multi-Ethnic Study of Atherosclerosis also found a relationship between characteristics of the built environment and the health of residents (Hirsch et al., 2014a). More than 5,000 participants with no diagnosed cardiovascular disease across six cities in the United States were enrolled in the year 2000. BMI and waist circumference were measured at baseline and at four subsequent follow-ups. Rodríguez reported that a higher development intensity, defined as a combination of density, land use, destinations, street patterns, and mass transit, was associated with a less pronounced increase in BMI and a decrease in waist circumference after adjusting for age, gender, race and ethnicity, education, income, employment, marital status, car ownership, health status, cancer, alcohol use, smoking, and time in transport (Hirsch et al., 2014a). He then cited a follow-up study in which the researchers found that individuals who moved to more walkable neighborhoods ended up walking for transportation, on average, 16 more minutes per week relative to those in less walkable neighborhoods (Hirsch et al., 2014b). These participants also had 11 percent greater odds of meeting the recommendations of the Every Body Walk! Campaign (which calls for 150 minutes per week of walking) and lowering their average BMI (Hirsch et al., 2014b).
Finally, Rodríguez turned to a study of people living in cities in southern Ontario, Canada, which found that the most walkable neighborhoods had lower rates of obesity than less walkable neighborhoods (Creatore et al., 2016). Moreover, over time, the adjusted prevalence of obesity among adults remained about the same in the most walkable neighborhoods, while the prevalence increased in neighborhoods categorized as less walkable. According to Rodríguez, “this summarizes really well the impacts of walkability on overweight and BMI.”
Moving on to challenges and opportunities, Rodríguez observed that more than half of the U.S. population—or more than 170 million people—currently lives in suburban environments. “This is the magnitude of the task ahead of us,” he added. At the same time, he argued, almost every city in the United States has the potential to improve its built environment. Planners, he suggested, are at the heart of the issue, both as a contributing cause and also as a remedy. He closed by saying, “The point here is to stitch a fabric of change that involves all these sectors and all this emerging evidence so that we can do something about this challenge.”
FOOD AND NUTRITION ENVIRONMENTS
“It is not big news that environments affect behavior,” observed Karen Glanz, George A. Weiss University professor and director of the Prevention
Research Center at the University of Pennsylvania. But, she continued, environments are complicated, especially with respect to food. The factors that influence what people eat, she observed, range from individual attitudes and genetics to macro-level conditions, such as societal and cultural norms, food and agricultural policies, and food and beverage marketing, and many mediating influences as well (Story et al., 2008) (see Figure 2-2). She explained that the societal-level factors interact with individual factors such as genes,
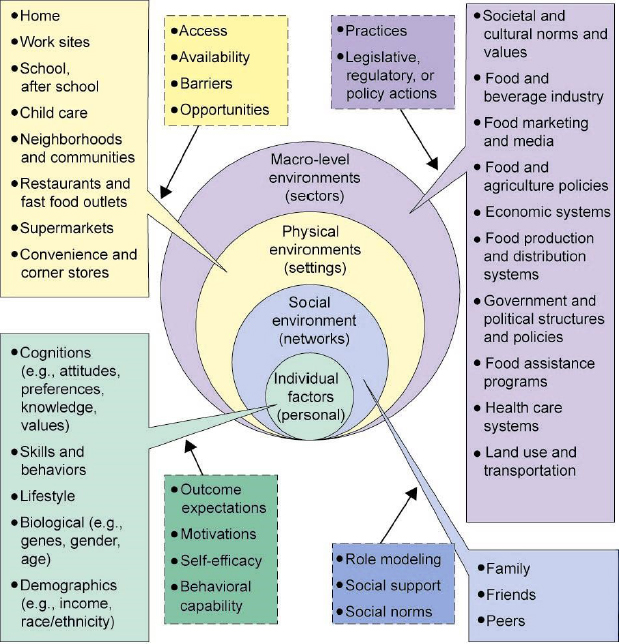
SOURCES: Presented by Karen Glanz, September 12, 2017; Story et al. (2008). Reproduced with permission of Annual Review of Public Health, Vol. 29 © by Annual Review.
biology, and psychology to produce behaviors, and these behaviors in turn influence health outcomes. One of the factors she has investigated is the food environment, which she defined as all of the places where people can find food (such as grocery and corner stores, restaurants, worksites, and schools), together with the policies (such as those concerning school food and catering) and economic factors (such as taxes, food assistances policies, and price supports) that influence what foods are available. The challenge, she stated, is to determine how much the environment contributes to what people eat and how that affects their health in this context.
Glanz continued by outlining several major differences between food environments and environments that affect physical activity. Food is a commodity, she elaborated, and food products are big business. She added that food is highly regulated for purposes of safety, taxation, and hygiene, and that organizational environments play a large role, particularly with respect to children. Food is also a complex substance, she observed, encompassing a variety of types and nutrients. She noted that while policies can play a role in shaping the food environment, environments often evolve without policies. To illustrate this point, she gave the example of the food retail sector: policies do not necessarily dictate where foods are located in stores or how much they cost, but they can have an effect on placement and prices. Therefore, she said, policies can act to improve or worsen health.
Glanz looked specifically at research into how stores, restaurants, and schools affect food intake, BMI, and obesity. Much of this research is descriptive and correlational, she explained. For example, she said, early findings on the retail food environment suggested that supermarkets produce healthier outcomes relative to fast food restaurants, which contribute to obesity, but more recent research has explored some of the ambiguities of these findings. She cited a systematic review by Cobb and colleagues (2015) of 71 studies representing 65 cohorts, which found that associations between fast food outlets and obesity are mostly null, that supermarket availability is often associated with adult obesity or null findings, that small stores are associated with child obesity in 50 percent of studies, that fast food availability is associated with child obesity (although many studies have found the association to be null), and that the overall quality of the studies was low. “The data are mixed,” said Glanz. “They are not all leaning toward supermarkets are good, fast food restaurants bad.”
Still, Glanz continued, research has shown an association between neighborhood of residence and a person’s weight status. She pointed to research showing that on the island of Manhattan, adult obesity rates are four times higher in east Harlem than in the Upper East Side (Black and Macinko, 2010). “That doesn’t segregate out food environments,” she observed, “but it shows us high environmental impact.” She noted that another study, conducted by Saelens and colleagues (2012), found a strong
association specifically between higher BMIs and neighborhoods with low levels of access to physical activity locations and nutritious foods.
According to Glanz, research on food environments also points to disparities in the types of foods available in different neighborhoods. She referred to a review of 49 studies by Beaulac and colleagues (2009), which found evidence that neighborhoods with a high proportion of low-income or minority residents had fewer supermarkets but more convenience stores relative to more advantaged areas. “These findings have occurred over and over again,” she observed.
Glanz identified as a major research question of interest whether putting a new supermarket in a food desert improves diet and reduces obesity. She pointed to two recent studies that found that new supermarkets produced increased perceptions of access to healthy food but no changes in consumption of healthy food or BMI (Cummins et al., 2014; Dubowitz et al., 2015). “You can also get much cheaper Krispy Kremes at the supermarket,” she observed. In fact, she noted, one recent study found that residents in food deserts buy most of their junk food at supermarkets (Vaughan et al., 2017). “We need to look beyond just the presence of supermarkets . . . [and] begin to look at the consumer environment, what is inside the store,” she argued. She added that a growing body of evidence suggests that interventions within supermarkets and food retail stores can be effective at increasing purchases of healthy foods (Adam and Jensen, 2016). For example, she and her colleagues have looked at how changing the placement of food in stores can increase sales of healthier items. When water is placed at the top of a display case rather than being hidden on the bottom shelf, for instance, it is purchased more often (Foster et al., 2014); the same is true for skim and low-fat milk and some frozen entrees. However, Glanz reported, placement and promotion strategies did not affect sales of other items, including cereal, sugar-sweetened beverages, diet beverages, and whole milk.
Glanz went on to note that interventions to increase healthy food access in small food stores—convenience stores, bodegas, and the like—have increased in recent years. She observed that evaluations of these interventions have shown mixed results. She cited a review by Gittelsohn and colleagues (2012) of 16 such trials, which found that availability and sales of healthy foods increased, and consumer knowledge improved. However, she noted, the trials had design and measurement limitations and showed limited impact on shopping behavior, and none of the trials showed an impact on obesity. In an evaluation of a large-scale urban corner store intervention, a component of the Communities Putting Prevention to Work initiative, Cavanaugh and colleagues (2014) found that to a modest degree, the environments in intervention stores were healthier, with greater availability of low-fat milk and fresh fruit. On the other hand, she reported, a companion study of the same stores by Lawman and colleagues (2015) that involved
bag checks and analysis of receipts found no differences in calories or nutrient content 1 year after the intervention was implemented. Likewise, a randomized controlled trial of a healthy corner store initiative found no changes in energy content per purchase and no differences in BMI z-score or obesity prevalence among urban, low-income youth (Lent et al., 2014). In summary, Glanz said, “the evidence is challenging assumptions about what we can achieve through corner store interventions.”
With respect to restaurant interventions, Glanz focused on policies that require calorie counts to be added to restaurant menus, which have been implemented in several cities, counties, and states. She pointed to a recent review of 16 studies that found reduced energy intake of orders in 4 of the studies and no significant effects in the other 12 (VanEpps et al., 2016). Glanz added that while the restaurant industry has been responsive to calorie labeling in menus, current regulations are local, and implementation of federal regulations included in the Patient Protection and Affordable Care Act has been postponed. If restaurants “start reformulating their foods or making portion sizes smaller,” she suggested, “that may be the big win, potentially.”
Turning to school food environments, Glanz observed that the 2010 Healthy, Hunger-Free Kids Act has produced major changes. She cited a study of 12 urban low-income schools, in which Schwartz and colleagues (2015) found that students took more fruit and threw away less of their fruits and vegetables after changes to the National School Lunch Program were implemented in their cafeterias. Likewise, a review conducted by the Community Preventive Services Task Force (2016a) on interventions to support healthier foods and beverages in schools found positive evidence for meal interventions, fruit and vegetable snack interventions, and multicomponent interventions. However, Glanz added, policies for healthier snacks and interventions for water access do not yet have positive evidence. “That doesn’t mean they don’t work,” she said. “It simply means that we don’t have enough studies that have found a positive effect.”
Finally, Glanz focused on multicomponent interventions, which she described as “programs that are community-wide, engaging the community, changing multiple environments and doing things to build skills and educate.” She cited a recent systemic review and meta-analysis of these community-wide programs, which looked at eight trials targeting children and adolescents, most of which were not randomized (Wolfenden et al., 2014). Seven of the eight trials showed a significant effect in reducing BMI, although the mean reduction in BMI z-scores was only 0.09. Glanz pointed out that this research was limited by difficulties in assessing changes in food environments and by selection bias. She added that the changes in health outcomes after these multicomponent interventions were implemented were modest, and it is not clear how to scale them up or make them sustainable.
Summarizing her observations, Glanz said that “inside the retail food environments, there is potential. If the food industry responds to awareness and the need to disclose information, that is a good thing. In schools, we are seeing a lot of positive changes if we can keep them going.” However, she warned, environmental strategies are not always effective, and there could be several reasons for this. The research may be limited by design, measures, or execution, she elaborated, and strategies may be limited by implementation or by an intervention’s dose, intensity, or duration. Or, she said, “it could be that we are using the wrong assumptions. You get back to those associations—supermarkets are good; fast food restaurants are bad. Maybe that is not the only place we should be looking.”
Glanz concluded by observing that changes in the food environment are inevitably linked to other issues, including food justice and social justice. “I think we can all agree that everyone should have a right to healthy, affordable food, that consumers have a right to know what is in their food when they eat out, [that] nobody wants kids to be hungry in schools,” she asserted. However, she cautioned that new policies can have both positive and negative consequences. For example, she explained, the Philadelphia soda tax is meant to support universal preschool education, but there is emerging evidence of the tax resulting in job losses and net tax losses to the city over time. “There are a lot of unanswered questions,” she said. “How much environmental change is needed? How long will it take to improve behavior and health? Who [what population] changes after the interventions are implemented, and do these changes reduce health inequity?” She closed by asserting that answering such questions requires applying and examining short-term results from a long-term perspective.














