
8
Suicide
Suicide was among the 10 leading causes of death in the United States among working-age adults (ages 25–64) in 2015, 2016, and 2017, when recent declines in life expectancy emerged, and despite the small overall increase in U.S. life expectancy in 2018, suicide mortality continued to increase in that year (Xu et al., 2020). During the study period, 1990–2017, suicide accounted for 569,099 deaths among the working-age population (Centers for Disease Control and Prevention [CDC], 2020b). Historically, suicide mortality has been substantially higher among men than women and among non-Hispanic (NH) Whites (Whites) than NH Blacks (Blacks) and Hispanics, and this was the case among working-age adults during the study period. During this period, moreover, suicide mortality increased substantially mainly for Whites, with the largest absolute increases occurring among White males across the 25–64 age range.1 Suicide is clearly a prominent preventable cause of death, particularly among working-age Whites, and an important public health concern.
This chapter focuses on the trends and disparities in and explanations for the recent rise in suicide mortality among U.S. working-age adults. For purposes of this report, suicide deaths do not include suicides by drug poisoning (which are counted as drug-related deaths in the data shown in Chapter 7) because of the difficulty of differentiating between intentional
___________________
1 Among all racial/ethnic groups, suicide mortality is highest among American Indians/Alaska Natives (Leavitt et al., 2018). As noted in Box 4-2 in Chapter 4, because of data quality concerns, mortality trends among this population subgroup are not examined in this report.
and accidental drug poisoning.2 First, the trends in suicide mortality are presented by age, sex, race and ethnicity, and geography for the study period (1990–2017). This is followed by a review of the research literature on factors related to suicide mortality and the degree to which such factors have changed to bring about the recent rise in suicides. Given that the rise in suicide mortality rates was driven by the rising rates among Whites, explanations for the increase in suicide mortality should focus mainly on working-age Whites. A paucity of existing research, however, examines suicide by race and ethnicity or seeks to explain the recent rise in suicide. Nevertheless, this chapter presents the committee’s assessment of the literature in explaining the trends in suicide, along with its recommendation for addressing related data needs.
Research on suicide mortality tends to focus in four general areas: economic factors; social engagement, religious participation, and social support; access to lethal means; and mental, emotional, and physical health. Some of the stronger evidence has been found for the role of economic conditions. Periods of economic downturn, wage stagnation, weak safety nets, and increasing foreclosure rates are associated with rising suicide mortality in national- and state-level data. While the research literature provides some compelling evidence for links between changes in economic conditions, social integration, and psychological and physical well-being and the rise in suicide mortality among Whites, most of this evidence is suggestive and obscures the fact that these factors are interrelated and operate across the societal, community, and individual levels.
TRENDS IN SUICIDE
As noted, the increase in suicide mortality over the past three decades occurred primarily among Whites, with both the levels and absolute increase being higher among men than women (Figure 8-1). From 1990 to 2017, the contribution of suicide to the overall mortality increase among White men ranged from 12.8 percent at ages 25–44 to 8.0 percent at ages 55–64 (see Table 4-1 in Chapter 4). In 2017, suicide was the second leading cause of death among White men ages 25–44, the fourth leading cause among those ages 45–54, and the seventh leading cause among those ages 55–64 (Heron, 2019).
Although at lower levels, suicide rates began to rise among White women after 2000 (Figure 8-1), contributing to the rise in White female mortality from 1990 to 2017. The contribution of suicide to the overall
___________________
2 As detailed later in the chapter, between 1990 and 2017, drugs contributed to 11.5–16.7 percent of all suicides, depending on the year, with their contribution being higher for women than for men.
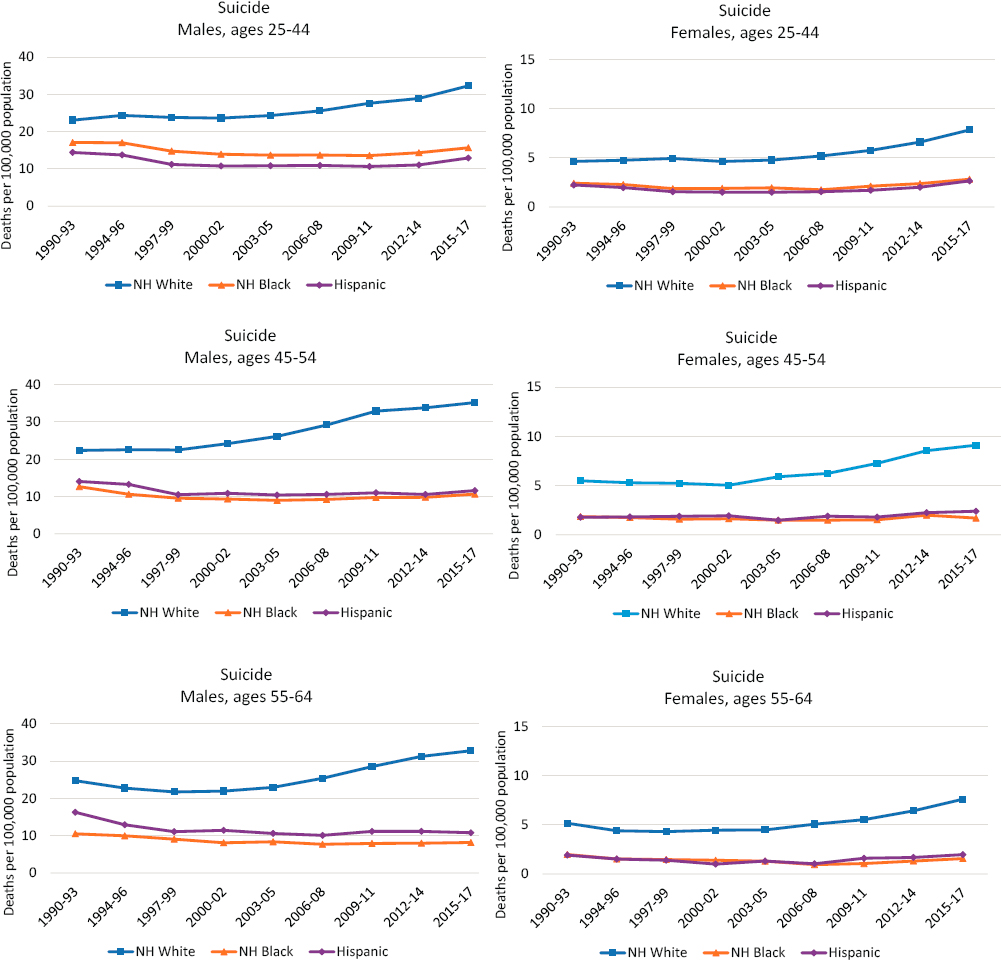
NOTE: Suicide deaths by drug poisoning are not included. Each panel shows suicide rates for non-Hispanic (NH) Whites (blue lines), NH Blacks (orange lines), and Hispanics (purple lines). Suicide rates for males are shown in the lefthand panels, while those for females are shown in the righthand panels. Suicide rates are shown for three age groups: 25–44 (top panels), 45–54 (middle panels), and 55–64 (bottom panels). Rates are age-adjusted to reflect a standard population age distribution.
SOURCE: Data from National Vital Statistics System Detailed Mortality Files, https://www.cdc.gov/nchs/nvss/deaths.htm.
mortality increase among White women ranged from 7.0 percent at ages 25–44 to 2.6 percent at ages 55–64 (see Table 4-1 in Chapter 4). In 2017, suicide was the second leading course of death among White women ages 25–34, the fourth leading cause among those ages 35–44, the fifth leading cause among those ages 45–54, and the ninth leading cause among those ages 55–64 (Heron, 2019).
Compared with the suicide rates among Whites, the rates among Blacks and Hispanics were relatively flat or declined between 1990 and 2017 (Figure 8-1). Still, suicide was among the 10 leading causes of death among Black men ages 25–64, Black women ages 25–44, Hispanic men ages 25–64, and Hispanic women ages 25–54 (Heron, 2019). During the 1990s, suicide rates among working-age Blacks and Hispanics generally decreased. Beginning in the 2000s, suicide rates increased among working-age Whites, particularly White males, while remaining steady among working-age Blacks and Hispanics. However, starting in about 2010, suicide rates also began to increase among Black and Hispanic males and females in most age groups, although these increases were smaller than those among working-age Whites.3
At the same time, working-age Whites experienced consistently higher suicide rates relative to working-age Blacks or Hispanics throughout the period. As the rates declined among Black and Hispanic adults in the 1990s, the gap between White adults and Black and Hispanic adults grew. This disparity widened through the remainder of the period as the rates increased steadily among White adults.
At the beginning of the study period, there was little difference in suicide rates by metropolitan status among White adults. Over time, however, suicide rates increased more slowly in large central metropolitan areas (hereafter referred to as “large central metros”) than in less-populated areas, initiating a widening nonmetro suicide “penalty” in nonmetropolitan areas (hereafter referred to as “nonmetros”) (Figure 8-2). The nonmetro disadvantage was largest among White males ages 25–44 and is a trend that the research literature has noted for all males (Singh and Siahpush, 2002).
In contrast, differences by metropolitan status among working-age Blacks were much smaller, although they also grew for Black women ages 45–64. Among younger working-age Hispanics, suicide rates were highest
___________________
3 Between 2009–2011 and 2015–2017, the absolute increase in the suicide rate among younger working-age Black men (ages 25–44) was as large as the absolute increase in the rate among younger working-age White women (ages 25–44). While the absolute increase in suicide rates was the same for these groups in this most recent period, the levels of suicide are always lower for women than for men. In 2015–2017, for example, the suicide rate for younger working-age Black men ages 25–44 was twice as high (15.7) as the rate for younger working-age White women (7.9), compared with the higher suicide rate for younger working-age White men (32.3) (see Tables A-1, A-2, and A-4 in Appendix A).

NOTE: Suicide rates are shown for two age groups—25–44 (panels a-c and g-i) and 45–64 (panels d-f and j-l)—across four levels of metropolitan status: large central metropolitan counties (blue lines), large fringe metropolitan counties (orange lines), small or medium metropolitan counties (gray lines), and nonmetropolitan counties (yellow lines). Trends in these four groups are presented separately by sex (males in panels a-f, females in panels g-l) and for non-Hispanic (NH) Whites (panels a, d, g, and j), NH Blacks (panels b, e, h, and k), and Hispanics (panels c, f, i, and l). Rates are age-adjusted by 10-year age group.
SOURCE: Data from National Vital Statistics System Detailed Mortality Files, https://www.cdc.gov/nchs/nvss/deaths.htm.
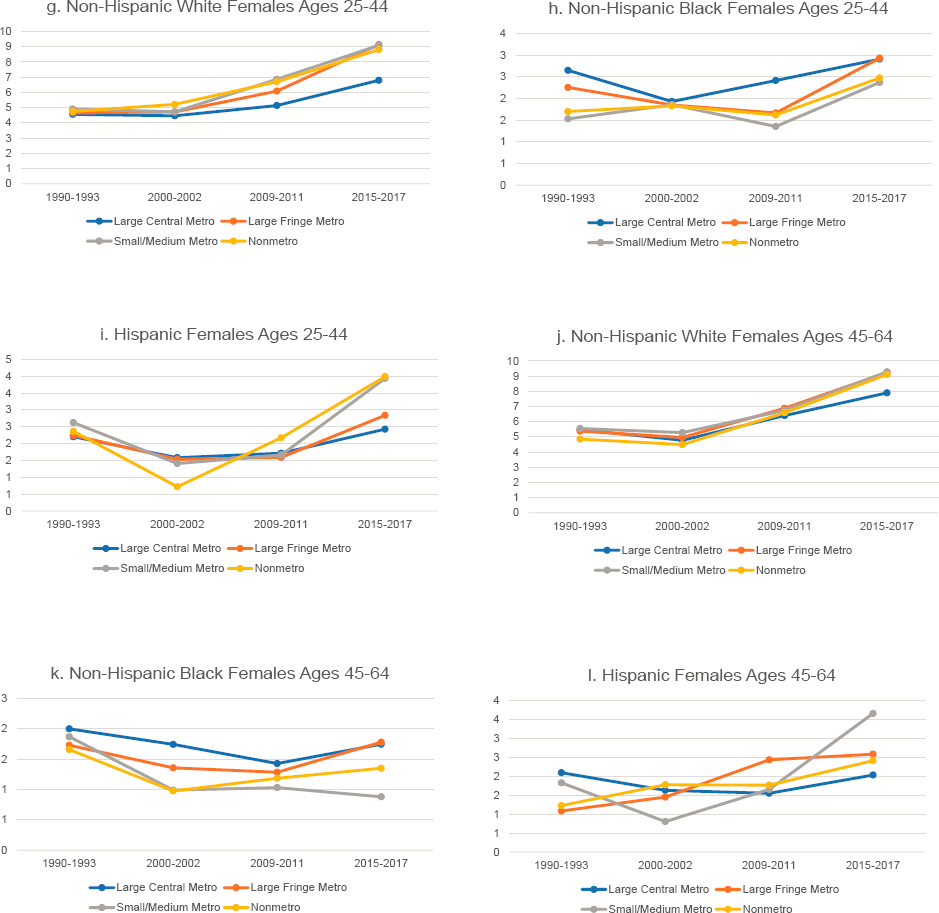
in nonmetro counties and lowest in large central metro counties throughout the period. Among older Hispanic males, the rates in nonmetro areas were the highest throughout the period, declined less in the 1990s, and increased more in the 2010s relative to other areas. They were lowest in large fringe metropolitan areas (hereafter referred to as “large fringe metros”) in 1990–1993 but increased in these areas during the 2000s, surpassing suicide rates in large central metros and small/medium metropolitan areas (hereafter referred to as “small/medium metros”) after 2010.
In the working-age (ages 25–64) population overall, male suicide rates increased by varying amounts in all but seven states between 1990 and 2017 (Figure 8-3), leading to increasing state-by-state variability in suicide mortality. This state-by-state variation in suicide mortality is not new (Miller, Azrael, and Barber 2012; Phillips, 2013), but it has widened during recent decades. The absolute increases were especially large in several Midwestern,
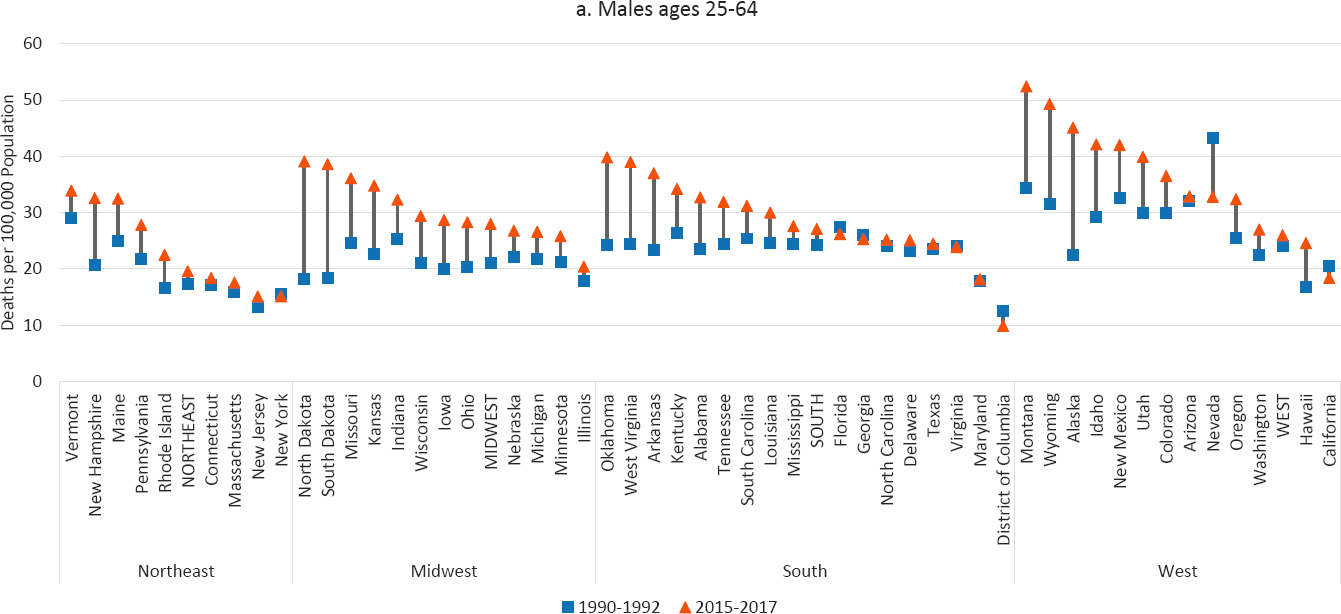
NOTE: Suicide rates are shown for 1990–1992 (blue squares) and 2015–2017 (orange triangles), along with the changes over time (black connecting lines). Suicide rates for males are shown in panel a above, while those for females are shown in panel b on the next page. Rates are age-adjusted by 10-year age group. For males, the 1990–1992 rate for Alaska represents 1991 and 1992 only; the rate is suppressed for 1990. For both males and females, North Dakota is excluded to comply with Centers for Disease Control and Prevention (CDC) suppression criteria (fewer than 10 deaths in 1990–1992). For females, the District of Columbia is excluded for the same reason. States are ordered from highest to lowest mortality rate in 2015–2017 within region.
SOURCE: Data from CDC WONDER Online Database, https://wonder.cdc.gov.
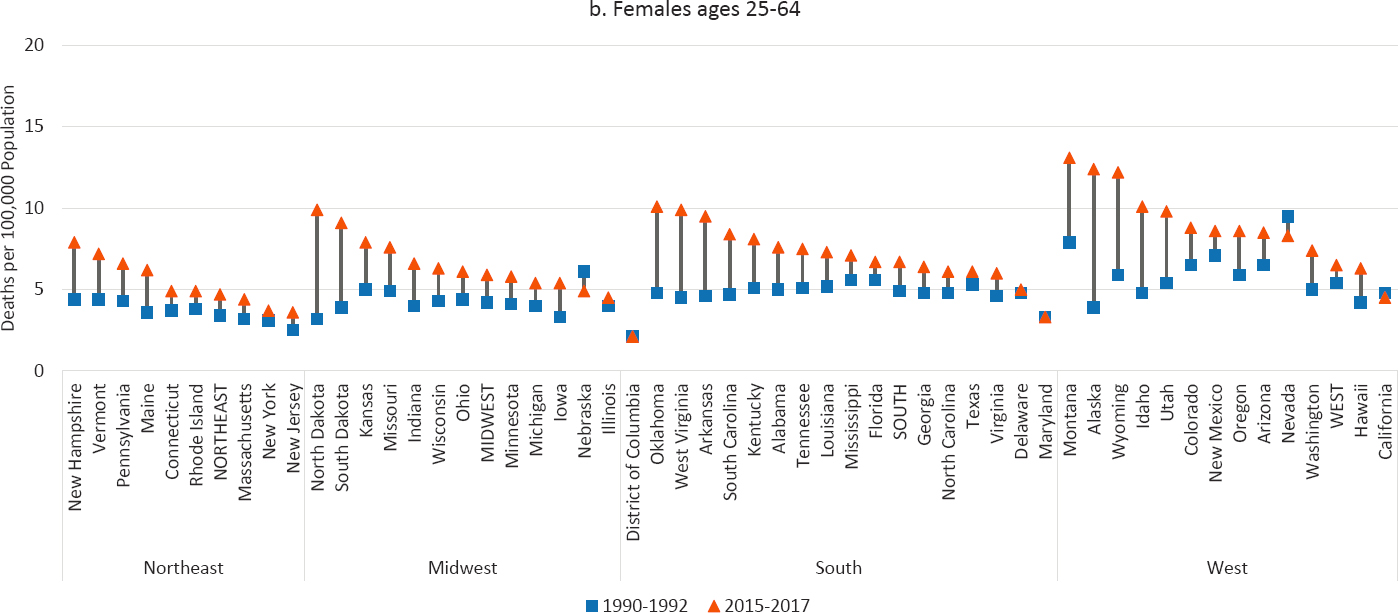
Southern, and Western states, whereas the percentage increases were largest in North and South Dakota, Oklahoma, West Virginia, and Arkansas. The largest percentage declines were in Nevada, the District of Columbia, and California. The highest rates in 2015–2017 were all in the West: Montana, Wyoming, Alaska, Idaho, and New Mexico. Among females ages 25–64, the rates increased in all but four states, and there were small declines in California, Nevada, and Nebraska. As with men, the absolute increases among females were most pronounced in several Midwestern, Southern, and Western states, and the largest percentage increases were in North and South Dakota, West Virginia, Oklahoma, and Idaho. The highest female suicide rates in 2015–2017 were in Montana, Alaska, Wyoming, Oklahoma, and Idaho.
Research suggests that suicide mortality began to rise for the baby boom cohorts in the late 1990s and continued to climb in succeeding birth cohorts. This pattern appears to be most evident for those without a 4-year college degree (Case and Deaton, 2017, 2020; Phillips et al., 2010). Using three different approaches to estimate an age–period–cohort model of suicide mortality, Phillips (2014) found that, although baby boom cohorts did not have higher suicide rates than previous birth cohorts, male and to a lesser extent female suicide rates began to rise and continued to do so for subsequent birth cohorts. Thus, the baby boom cohorts appear to have ushered in new cohort patterns of suicide rates over the life course. Chauvel, Leist, and Smith (2016) studied suicide mortality in 1990–2010 for birth cohorts, net of age and cohort linear time trends, and further documented sharp increases in suicide mortality for White men with low levels of education among cohorts born between 1955 and 1970.
Explanations for the Rise in Suicide Mortality
A range of societal, community, relationship, and individual factors undoubtedly contribute to suicide ideation, attempts, and mortality, as conceptualized in Figure 6-1 in Chapter 6. At the same time, the risk can be mitigated by protective factors, such as community and family supports, access to mental health and substance use services, and cultural and religious beliefs (Conejero et al., 2016; Denney et al., 2009; Pescosolido, 1990; Pescosolido and Georgianna, 1989; Wray, Colen, and Pescosolido, 2011). Durkheim’s (1951) focus on the role of social integration and societal regulation in times of rapid social change in shaping suicidal behavior is informative in this regard. According to research in the Durkheim tradition, individuals’ social ties within the family, with religious and other organizations, and in political domains (including participation in the labor force) reduce social isolation and buffer against suicidal behavior (Abrutyn and Mueller, 2018; Bearman, 1991; Durkheim, 1951; Pescosolido, 1994). These
social ties may be particularly critical for individuals facing stressful life events and other personal crises. The interpersonal theory of suicide mortality in turn proposes that feelings of perceived burdensomeness and thwarted belonginess can precipitate a suicidal desire and the act itself (Chu et al., 2017). The reasons for the increase in suicide mortality among Whites and its geographic variation, as well as factors that account for trends among other racial/ethnic groups, are likely to be multifactorial and thus to escape simple explanations. While it is important to consider the role of both predisposing and protective factors (Shanahan et al., 2019), their role in the increase in suicides among Whites has not been extensively studied. The review that follows includes research that has considered various factors that may have played a role: economic factors; social engagement, religious participation, and social support; access to lethal means; and mental, emotional, and physical health.
Economic Factors
The available evidence suggests that suicide mortality can be responsive to economic conditions. Employment may mitigate against suicide risk in a number of ways, including steady income, employment-based social networks, access to informational resources and health and other employment-based benefits, and a sense of self-worth. Historical data for the United States between 1928 and 2007 link trends in suicide mortality to business cycles, with rates rising during recessions and declining during economic expansions among working-age adults (Luo et al., 2011). An increase in the unemployment rate has been associated with higher death rates from suicide, although this association may depend on the time period in which unemployment occurs (Catalano et al., 2011; Modrek et al., 2013; Tapia Granados, 2005; Tapia Granados et al., 2009). Using longitudinal state-level data for the period 1972–1991 with state fixed effects and controls for state-level educational attainment, race and ethnicity, per capital income, and age, Ruhm (2000) found that suicide mortality increases by 1.3 percent for every 1 percent increase in state unemployment rates. Using similar methodology, with controls for a set of economic, demographic and social/cultural variables,4 Phillips and Nugent (2014) found a significant positive association between unemployment and suicide mortality in midlife based on state-level data from 1997 to 2010; this association appeared stronger in states with higher female labor force participation rates. In a separate study between 1976 and 2000 (Phillips, 2013), however, unemployment was not
___________________
4 Female labor force participation rate, percent employed in manufacturing, per capita income, sex composition, age structure, percent foreign-born, percent divorced, alcohol consumption (gallons per capita), and antidepressant drug use.
associated with elevated suicide mortality. Similarly, DeFina and Hannon (2015), using state-level data on rates of unemployment and suicide mortality with state fixed effects, found a significant positive association between the two rates from 1995 to 2010 but not between 1979 and 1995. They attribute this pattern to growing economic insecurity resulting from wage stagnation, changes in employment and hiring practices, and more stringent requirements for safety net programs in the latter period that made individuals more vulnerable to the effects of unemployment (DeFina and Hannon, 2015; Hacker et al., 2010).
That economic insecurity may play some role in the recent increase in suicide mortality is apparent from analyses of the National Violent Death Reporting System (NVDRS), which provides information on circumstances surrounding completed suicides. Hempstead and Phillips (2015) used these data to examine circumstances surrounding suicide mortality between 2005 and 2010 and found that economic troubles (e.g., job, financial, or legal problems) increased significantly among individuals ages 40–64, and that these increases were related to suicide by suffocation, a lethal method that has increased in recent years. Similarly, Kerr and colleagues (2017), who also used the NVDRS data, found poverty to be strongly associated with suicide mortality between 2005 and 2011, as were foreclosure rates at ages 45–64, while Houle and Light (2014) document a significant association between state-level foreclosure rates and suicide mortality at ages 46–64. Employment has also been tied to a lower risk of suicide in analyses of data from the National Health Interview Survey (NHIS) and the National Longitudinal Mortality Study (NLMS) (Denney et al., 2009; Kposowa, 2001), as have higher levels of education, such that those with lower levels of schooling are at higher risk of suicide (Case and Deaton, 2015, 2017; Denney et al., 2009). A study by Geronimus and colleagues (2019) documents changes in educational disparities in mortality among working-age (and older) adults between 1990 and 2015 for both Black and White women and men, demonstrating that both White women and White men exhibited small increases in educational disparities in working-age mortality due to suicide. These authors measured educational attainment in quartiles to help account for increasing educational attainment across time and showed that working-age Whites with lower levels of education experienced slightly higher increases in suicide rates relative to those with more education.
Indeed, some of the strongest evidence for a link between economic conditions and suicide mortality has been found among those with lower levels of schooling. Kaufman and colleagues (2020) used state-level monthly data to examine the effects of differences between the state and federal minimum wage on suicide mortality among adults ages 18–64 from 1990 to 2015. Their difference-in-differences model found that a $1 increase in the state minimum wage reduced the suicide rate by 3.4–5.9 percent among
those with a high school education or less, and the effects were greatest during periods of high unemployment. Similar findings are reported by Dow and colleagues (2019), who examined the effects of state variation in minimum wages and the Earned Income Tax Credit (EITC) on suicide mortality among those ages 18–64 from 1999 to 2015. They report that a 10 percent increase in the minimum wage reduced nondrug suicides among adults with a high school education or less by 3.6 percent; a 10 percent increase in the EITC reduced suicides in this group by 5.5 percent. Unfortunately, many of these studies, and much of the research on economic conditions, do not examine racial/ethnic differences in the role of economic factors in suicide mortality.
As noted, the recent increase in suicide mortality among Whites is a phenomenon seen primarily among those with a high school education or less (Case and Deaton, 2015, 2017, 2020). Since the 1970s, the wages for this population have stagnated, and their rates of labor force participation have declined (Case and Deaton, 2020). Since the late 1960s, for example, when labor force participation rates among working-age males were fairly similar across all education groups, the rates have steadily declined among those with a high school education or less (Krause and Sawhill, 2017), and they continued to decline following the Great Recession despite historically low unemployment rates in recent years. Between 2009 and 2016, the labor force participation rate among Whites ages 25–64 with less than a high school education declined from 58 percent to 53 percent; the decline for those with a high school education was from 76 percent to 72 percent. In contrast, labor force participation rates among those with a bachelor’s degree or higher remained steady at 86 percent (National Center for Education Statistics [NCES], 2020a, 2020b). At the same time, the loss of manufacturing employment and the growth of service-sector jobs have changed the nature of work and compensation for those with low levels of education. Case and Deaton (2020) argue that the long-term economic trends have had a cumulative negative impact on the lives of cohorts born since the 1940s.
Although these changes are not unique for Whites, evidence suggests that the association between the changing economy and “deaths of despair,” of which suicide mortality is a key component, is stronger for Whites than for other racial/ethnic groups (see Chapter 7). Pierce and Schott (2020) found this to be the case in counties more exposed to economic shocks due to trade liberalization. Likewise, a recent study by Graetz and colleagues (2020) found higher levels of manufacturing employment to be a significant predictor of lower suicide mortality among White men and women in 1999 and 2017 in 704 U.S. commuting zones (see also Phillips and Nugent, 2014). The working class is facing some of the bleakest prospects for upward mobility recorded in recent generations, and White cohorts do not appear to be any less immune to these adverse trends relative to other
racial/ethnic groups (Cherlin, 2018; Chetty et al., 2017). This erosion of the American Dream for less-educated White Americans means that they have experienced a relative loss of status in recent decades and can no longer place themselves above other racial/ethnic groups in a class-based social hierarchy (Hochschild, 2016; Silva, 2019). Changing economic conditions and the nature of work, however, are unlikely to explain all of the rise in suicide mortality among White Americans.
Social Engagement, Religious Participation, and Social Support
In the face of stagnating wages and deteriorating economic conditions for those with low levels of education, social institutions could potentially play an important supportive role (Wilcox et al., 2012). Social engagement other than through employment, whether through local civic organizations, school boards, volunteer activities, religious involvement, friendship and family networks, or other forms of community engagement, is hypothesized to reduce social isolation and feelings of loneliness and buffer against self-harm. Yet it appears that such engagement has declined during the past few decades. Although not without his critics, Putnam (2000) draws attention to the decline in several forms of civic participation in the United States in his book, Bowling Alone. At the same time, social capital, measured at the individual or the community or state level, has been associated with measures of health and mortality, including suicide, although these associations are likely to be sensitive to what measure of social capital is used and subject to the ecological fallacy5 (e.g., Kawachi et al., 1997; Lee and Kim, 2013; Smith, Lucia, and Kawachi, 2014). Smith, Lucia, and Kawachi (2014) examined associations between various dimensions of social capital and suicide rates at the state level during 1999–2002, controlling for other state-level characteristics that had been associated with suicide mortality in prior studies, including state-level Gini coefficient, gun ownership, alcohol and drug use, serious mental illness, poverty and unemployment rates, suicide belt state,6 urbanization, and population instability. They found that suicide rates for White men and women were lower in states with higher levels of social capital, controlling for other state-level characteristics, but not for Black men, the only other group that had sufficient numbers of suicides to be included in the analysis. The results are suggestive for a possible
___________________
5 The ecological fallacy refers to an incorrect interpretation of statistical data that occurs when inferences about the nature of individuals are deduced from inferences about the group to which those individuals belong. An example of this fallacy would be to infer that if states with more Catholics have lower suicide rates, Catholics must be less likely to commit suicide.
6 The suicide belt is a region of the Western United States where the suicide rate is particularly high compared with the national average. It comprises Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, and Wyoming (Wray, Colen, and Pescosolido, 2011).
role of social engagement in White suicide mortality, although the authors’ cross-sectional analysis does not speak to whether changes in social capital and civic engagement are potential contributors to rising suicide mortality among White men and women.
Another important form of social engagement is participation in religious organizations. Although some of the association between more frequent attendance at religious services and lower mortality is due to health selection (i.e., unhealthy individuals are less likely to attend religious services), the association is robust to controls for health status, including status related to external causes of death such as suicide (Hummer et al., 1999). Other studies have documented a lower suicide risk in areas with a greater proportion of Catholics, with the results for other denominations being more mixed (Klugman, Condran, and Wray, 2013; Wray, Colen, and Pescosolido, 2011). Similar to the findings of Hummer and colleagues (1999), participation in religious activities predicted lower suicide rates in multivariate analysis of the 1993 National Mortality Followback Survey (Nisbet et al., 2000). The proportion of Americans who do not affiliate with any particular religion has grown over the past decade with each successive younger generation, as has the percentage who do not attend religious services regularly. In 2018–2019, more than 50 percent of White adults said they attended religious services only a few times a year or less, reflecting a growth of close to 10 percent since 2009 and proportions higher than those among Blacks and Hispanics (Pew Research Center, 2019). Based on the General Social Survey, weekly church attendance at ages 40–59 also declined more rapidly for Whites without a college degree than for those with a bachelor’s degree between 1970 and 2018 (Case and Deaton, 2020, Figure 12.3). Wilcox and colleagues (2012) similarly document a decline in participation in religious services among Whites ages 25–44 without a college degree, but not among their Black and Hispanic counterparts.
Another significant type of social support is a stable marital relationship. Prior research has documented a lower risk of suicide for married than for unmarried individuals among participants in the NHIS and NLMS, with the association being stronger for men than for women (Denney et al., 2009; Kposowa, 2001). A significant positive association has also been documented between suicide risk and the proportion divorced in one’s county and state of residence (Phillips, 2013; Reckera and Moore, 2016; Singh and Siahpush, 2002; Trgovac, Kedron, and Bagchi-Sen, 2015), suggesting that stronger family ties may buffer against self-harm. One of the notable changes in American family life is the decline in marriage, especially among those with lower levels of education (Cherlin, 2018; Ruggles, 2015). Since 1970, being currently married declined for most White women, with the largest declines seen among those with a high school education or less and those with some college. By 2000, White women without a college degree
were less likely to be married than in 1940 or 1970 and less likely to be married than those with a college degree (Torr, 2011). For Black women, this pattern of marital status by educational attainment had emerged by 1970 such that those with lower levels of schooling were less likely to be married than those with a college education (Torr, 2011). Thus, the decline in marriage among White women, and particularly among less-educated White women, is more recent (Cherlin, 2009; Murray, 2012), overlapping with the time period when suicide rates were increasing among Whites.
Not only are women with less than a college degree less likely to be married, but they are also more likely to be divorced or in cohabiting unions with children. Declining wages for men with less than a college degree have made these men less attractive marital partners for women, and a sharp differentiation in marriage patterns and family circumstances has emerged between men and women with and without a college education (Cherlin, 2014). Autor, Dorn, and Hanson (2019) document a link between marriage and a lack of well-paying jobs, especially in regions where automation and trade have led to reductions in such jobs. They found further that these employment shocks are associated with “male idleness and premature mortality, and raise the share of mothers who are unwed and the share of children living in below-poverty, single-headed households” (Autor, Dorn, and Hanson, 2019, p. 161).
Taken together, the above evidence suggests that social support, whether from formal institutions such as churches or other community-based social support networks or from stable interpersonal relationships within marriage, has deteriorated in the past several decades for individuals with lower levels of education, and that these trends have had a more profound impact on Whites than on other racial/ethnic groups. Research examining links between these patterns and suicide rates, however, has been mainly descriptive. To what extent these changes can explain the increase in suicide mortality among White men and women and whether such changes interact with the growing economic stratification and individual-level risk factors requires further investigation.
Access to Lethal Means
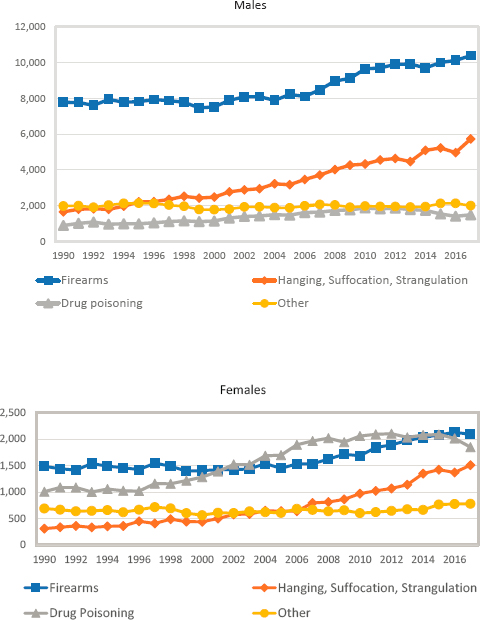
Another societal factor that can influence suicide risk is access to lethal means. Recent research has drawn attention to the role of firearms in patterns of suicide mortality by geography and gender. For example, the higher mortality from suicide among males is related to their use of more lethal means (e.g., firearms) relative to females (Miller, Azrael, and Barber, 2012) (Figure 8-4).
Rates of firearm-related suicide are higher in states with looser gun regulations and more gun ownership, and in nonmetropolitan than in
SOURCE: CDC WONDER Online Database, https://wonder.cdc.gov.
larger metropolitan counties (Anestis and Anestis, 2015; Anestis, Selby, and Butterworth, 2017; Fleegler et al., 2013; Ivey-Stephenson, Blair, and Crosby, 2018; Kaufman et al., 2018). Anestis, Selby, and Butterworth (2017) studied trends in suicide by firearms between 1999 and 2015 and found that at the state level, the absence of laws requiring universal background checks and imposing a mandatory waiting period for the purchase of firearms were associated with a more steeply rising trajectory of statewide suicide rates. Furthermore, where firearm suicide rates were declining, this decline was not offset by increases in suicide by other means. Others have documented higher suicide rates in states with higher gun ownership (Opoliner et al., 2014), and handgun ownership has been associated with higher rates of firearm-related suicide mortality (Studdert et al., 2020). These findings
suggest that strengthening state gun control laws has the potential to reduce suicide rates and possibly rural–urban differentials in these rates.
In 2017, suicide by firearms accounted for nearly half of all suicides among White men ages 25–64 but only about one-third of suicides among their female counterparts, whereas drug poisoning was a more common means of suicide among women than men. (Recall that in this report, suicides due to drug poisoning are included in the discussion of drug-related mortality [Chapter 7] and are not included in the trends shown in Figures 8-1 through 8-3 above). This gender difference in suicide by drug poisoning may explain some of the lower suicide mortality among women documented in this chapter, which considers only suicide deaths classified as “intentional.” However, given that rates of male suicide are 3 to 4 times higher than female rates, the exclusion of deaths from drug poisoning, many of which are accidental, probably plays a small role in the gender differences shown in Figures 8-1 through 8-3. It is also possible that suicides due to drug poisoning are underreported for both males and females (see Rockett et al., 2018).
As seen in Figure 8-4, although the number of suicides by firearms increased among White men between 1999 and 2017, their share of all suicides declined from 63 percent in 1990 to 53 percent in 2017, during the period when suicide mortality was increasing most notably. At the same time, suicides by hanging, suffocation, and strangulation increased from 13 percent to 29 percent among White men. Similarly, among White women, suicides by firearms increased over the period, but their share of all suicides also declined, from 43 percent to 34 percent, while the percentage of suicides due to hanging, suffocation, and strangulation almost tripled, from 9 percent to 24 percent. While the levels are much lower, the distributions of suicides by type are similar for Blacks and Hispanics (not shown). Although looser state gun laws are associated with higher suicide rates by firearms and suicide by firearms contributed to the increase in suicide mortality over this period, suicide by other means made a larger contribution to the overall increase in suicide mortality. The increased contribution of hanging, suffocation, and strangulation to rising suicide rates suggests that changes in gun availability cannot be the primary reason for rising suicide mortality among White men and women.
Mental, Emotional, and Physical Health
An individual’s risk of suicide is related to a family history of suicide; prior suicide attempts; psychiatric disorders, including depression and substance use; pain and other health problems; social adversity and deprivation during childhood and adolescence; and impulsivity (Conejero et al., 2016; Denney et al., 2009; Fazel and Runeson, 2020; Ilgen, 2018; Petrosky et
al., 2018). Furthermore, suicide can be precipitated by the experience of stressful life events with or without the presence of mental health problems. An analysis of the NVDRS, for example, found that in 27 states in 2015, relationship problems/loss, life stressors, and recent impending crises were more common among those without versus those with known mental health conditions, although they were common among both groups (Stone et al., 2018).
One of the most important individual risk factors for suicidal behavior and mortality is the presence of mental illness. As discussed in Chapter 7, however, the role of mental illness has been challenging to study because ongoing representative population surveys and other nationwide surveillance instruments do not include comprehensive diagnostic indicators of adult mental illness. Many such studies tend to be conducted in variously selected populations, such as military or veteran populations, prisoners, and the homeless. Several national surveys include nondiagnostic indicators of mental health, such as self-reports of depressive symptoms, anxiety, depression, panic attacks, and psychological distress, but none include the array of commonly diagnosed mental illnesses thought to be most associated with suicide risk, such as anxiety disorders, bipolar disorder, phobias, personality disorders, eating and gambling disorders, schizophrenia and other psychoses, and panic disorders. These mental conditions predict different levels of suicidal behavior (Fazel and Runeson, 2020), but while not all cases of completed suicide are among people with a history of mental illness, the presence of such illnesses is extremely common. A study of risk factors for suicide attempts among U.S. Army soldiers, for example, found that 63.7 percent had a prior history of mental illness (Ursano et al., 2018). Too and colleagues (2019) conducted an extensive meta-analysis of record linkage studies of suicide deaths and calculated the pooled rate ratio for mental illness antecedents (i.e., the rate of suicide deaths in persons with specific mental illnesses over the rate in those without those illnesses). They report a pooled rate ratio of 13.2 for psychotic disorders and 12.3 for mood disorders (e.g., depression).
An issue of concern with regard to the control and mitigation of suicide is access to professional mental health and related care. This issue has also been difficult to study, as “access to care” has varying meanings in research studies and operates at multiple levels for individuals. Variation in access may reflect the density of licensed therapists of various kinds in a geographic area; the presence of various community-based programs for treatment of general mental illness or more specific problems, such as substance use disorders; or inpatient hospital “beds” for management of more serious or immediate mental illnesses. Access may also refer to having personal or family insurance for mental health conditions. Even if such insurance
is present, however, it may have important limitations with respect to the services covered and/or a requirement for substantial copayments. Many mentally ill and suicidal patients seek care at general hospital emergency departments, where infrastructure for suicide management and prevention may not be adequate (Asarnow, Babeva, and Horstmann, 2017). Finally, access may refer to nonfiscal barriers, such as stigma or social impediments. As noted in Chapter 7, it is generally believed that personnel and facilities for adequate psychiatric care are lacking in many American regions and jurisdictions, and many counties have no mental health professionals whatsoever. The lack of access to mental health services is especially acute in the nonmetropolitan areas where male suicide mortality has been historically high (Andrilla et al., 2018).
An older review of 40 studies examined the relation between access to mental health care and suicide rates (Luoma, Martin, and Pearson, 2002). This multinational study found that only 19 percent and 32 percent of decedents, respectively, had made contact with the mental health care system in the month before death and in the year before death, highlighting the need for more attention to the role access to mental health care can play in reducing suicide mortality. Holliday (2018) conducted a more recent review and concluded that the evidence for this association was “mixed,” noting that even if mental health services were proximately available, not all persons with mental illnesses might need them. However, she found that two policy-oriented studies offered more evidence that access to mental health care could yield some reduction in suicide rates. Using cross-sectional state-level data, Tondo, Albert, and Baldessarini (2006) found that states receiving more federal mental health aid had lower suicide rates, and aid was a stronger correlate of suicide rates than was the proportion of uninsured individuals in the state, density of psychiatrists or physicians, or sociodemographic variables. Lang (2013) examined the causal impact of mental health parity laws on suicide rates between 1990 and 2004; parity laws require health insurance plans to provide comparable coverage for physical and mental health. Using variation in implementation dates, Lang found that in the first year after states enacted parity laws, the suicide rate for adults ages 18–64 declined by 5 percent, and these effects were maintained 2 years or longer after the laws had been enacted, although the magnitude of the change decreased somewhat over time.
A paucity of research examines the relationship between mental illness and suicide mortality separately by race and ethnicity because of the limited data sources and measurement issues mentioned earlier. For example, race-specific suicide rates and rankings as determined by death certification may be affected differentially by different suicide methods (e.g., gunshot wound versus drug poisoning) (Warshauer and Monk, 1978) or the types of
opioids used by decedents with substance use disorders (Alexander, Kiang, and Barbieri, 2018). Nonetheless, the racial/ethnic patterns of mental health reflect the racial/ethnic patterns of suicide mortality. For example, there is evidence of higher lifetime risks of mental illness among Whites compared with Blacks and Asians (Alvarez et al., 2019). In what is known as the “minority mental health paradox,” non-Whites report mental health that is equal to or somewhat better than that of Whites (Williams and Earl, 2007). The 12-month prevalence of most psychiatric disorders, including depression (Hasin et al., 2018), tends to be lower among non-Whites (Breslau et al., 2005; Miranda et al., 2008; Vilsaint et al., 2019). Once adjustments for socioeconomic status are included, Blacks almost always report better mental health on dimensional measures of depression (Barnes and Bates, 2017), while Hispanics report a lower prevalence (Breslau et al., 2005) and Asians an especially low prevalence (Takeuchi et al., 2007) of psychiatric disorders generally relative to Whites. It should be noted, however, that racial/ethnic minorities are significantly more likely than Whites to conceal their mental health symptoms and avoid treatment because of the stigma associated with mental illness (Clement et al., 2015); while findings are mixed on whether racial/ethnic minorities experience higher levels of stigma than Whites (Wong et al., 2017).
The racial gap in mental illness has sometimes been explained by differential levels of access to health care and treatment. African Americans receive fewer prescription medications, and even among insured patients with the same condition, Black and Hispanic patients use significantly fewer medications relative to White patients (Briesacher, Limcangco, and Gaskin, 2003). A recent study attempted to address the minority mental health paradox by examining a common argument that Whites compared with non-Whites have more access to and receive better health care, including for mental illness. Using data from the 2008–2013 Medical Expenditure Panel Survey, Schnittker and Do (2020) show that Whites consume more pharmaceuticals than non-Whites for a wide variety of medical conditions, and although these drugs are effective in treating their particular condition, depression or suicide can be a side effect. The authors report a strong relationship between the use of medications for which suicide is a potential side effect and significant distress, such that the disproportionate use of these medications by Whites partially explains the non-White advantage in mental distress. This study did not address whether the use of these medications is also associated with a higher suicide rate among Whites compared with non-Whites.
Some evidence points to a decline in mental health among individuals of low socioeconomic status since the mid-1990s. For example, Goldman, Glei, and Weinstein (2018) document a decline in life satisfaction, psychological
well-being, and positive affect7 between the mid-1990s and 2011–2014 among middle-age and older Whites of low-socioeconomic status, the population subgroup that has experienced rising death rates from suicide (Case and Deaton, 2015, 2017, 2020; Goldman, Glei, and Weinstein, 2018). A caveat regarding the research in this area is that it tends to focus on declines in the positive manifestations of mental health, and it is not clear whether poor mental health increases in step with declining positive mental health (Cherlin, 2018). As noted in Chapter 7, Graham and Pinto (2019) found racial/ethnic differences in optimism for the period 2010–2015 using data from the Gallup Healthways Survey, which showed that lower-income Blacks and Hispanics had higher levels of optimism about their future life satisfaction8 compared with lower-income Whites, especially Whites living in rural areas. The role of lower and declining psychological well-being among Whites of low socioeconomic status may be important given that greater psychological well-being has been associated with significantly lower overall mortality (Alimujiang et al., 2019; Keyes and Simoes, 2012; O’Connor and Graham, 2019) and with lower suicide mortality (Too et al., 2019).
Another factor that may play a role in suicide mortality is an increase in the reported prevalence of pain among U.S. adults. As noted in Chapter 7, a study using two cross-sectional waves of the Midlife in the United States (MIDUS) Study found an increase in the prevalence of pain between 1995–1996 and 2011–2014, reporting that pain accounted for an important share of the increase in drug misuse, often correlated with suicide, over this period (Glei, Stokes, and Weinstein, 2020). Additional evidence that chronic pain may have played some role in the surge in suicide mortality since the early 2000s comes from the NVDRS. Petrosky and colleagues (2018) used NVDRS data from 18 states on 123,181 decedents who had died from suicide from January 2003 through December 2014. They found that the percentage of suicides with evidence of chronic pain was up from 7.4 percent in 2003 to 10.2 percent in 2014.
With respect to physical illness, Stickley and colleagues (2020) found that persons with four or more such illnesses had 3–4 times greater odds of suicidal behavior compared with those with no such illnesses. In a multinational systematic review of antecedent physical illness and functional disability, suicidal behaviors were more common in patients with such disabling conditions as malignant diseases, liver disease, neurological disorders, male genital disorders, and arthritis. Because chronic illness and its
___________________
7 How much of the time in past 30 days the respondent felt cheerful, in good spirits, extremely happy, calm and peaceful, satisfied, and full of life.
8 Respondents were asked where on a ladder with a scale of 1–10 they thought their life satisfaction would be in 5 years.
comorbidities are associated with higher levels of physical and emotional pain (Fässberg et al., 2016; Racine, 2018), these findings resonate with the above trends in pain, especially for Whites, who tend to seek and receive more health care relative to Blacks and Hispanics (Institute of Medicine [IOM], 2003; Schnittker and Do, 2020). In general, however, less attention has been paid to the physical illness and multimorbidity antecedents of suicide than to pain, and it may be that further investigation would support screening of these patients for suicide risk, with subsequent management.
Increased mortality from drug- and alcohol-related causes among White Americans ages 25–64 is documented in Chapter 7. The fact that substance use is a risk factor for suicide accords with those findings, and several studies show that suicide is often associated with acute alcohol consumption (see Cherpitel, Borges, and Wilcox, 2004, for a review). Kaplan and colleagues (2015) document an increase in the percentage of suicides showing the presence of alcohol intoxication from 2005–2007 to 2010–2011 among most racial/ethnic groups, including White men and women. Acute alcohol intoxication may be a mechanism connecting worsening economic conditions to suicide (Kawohl and Nordt, 2020; Nordt et al., 2015). For example, Kaplan and colleagues (2015) and Kerr and colleagues (2017) show that alcohol ingestion itself (particularly acute alcohol intoxication) was a key risk factor for suicide during and following the Great Recession. Using data from the NVDRS, Kerr and colleagues (2017) also found a positive association between poverty and alcohol involvement in suicides in 2005–2011 for both males and females in all age groups.
SUMMARY
Trends and disparities in suicide mortality among U.S. working-age adults over the study period (1990–2017) indicate that suicide rates increased substantially mainly among Whites, especially White males. Although at lower levels, suicide rates also increased among working-age White women, especially since 2000. Although Black and Hispanic working-age adults generally experienced declining (1990s) and then steady (2000s and 2010s) trends in suicide deaths, the trends among those in the younger working-age group (25–44) showed a slight increase from 2012–2014 to the end of the period. Nevertheless, the rising trend among working-age Whites compared with the relatively flat trend among Blacks and Hispanics resulted in a widening racial/ethnic gap in suicide mortality during the study period. The nonmetro–metro gap also widened, especially among younger working-age (ages 25–44) White males, for whom suicide rates rose more slowly in the latter areas. Suicide rates also were higher in Western states, especially those with large rural populations, relative to other regions of the country.
The potential causes of rising suicide mortality among Whites are complex, involving multiple factors that operate independently and interactively across the societal, community, and individual levels to affect suicide risk. Research tends to focus in four general areas: economic factors; social engagement, religious participation, and social support; access to lethal means; and mental, emotional, and physical health. Unfortunately, little of this research examines differences by race and ethnicity, estimates causal impacts, or attempts to explain change in suicide mortality (mainly differential rates). Therefore, understanding of why working-age suicide rates increased among Whites during the study period is mainly inferential.
Some of the stronger evidence has been found for the role of economic conditions in suicide mortality. Periods of economic downturn, wage stagnation, weak safety nets, and increasing foreclosure rates are associated with rising suicide mortality in national- and state-level studies. While employment is protective against suicide, the negative effects of unemployment appear to be conditional on the context of economic insecurity. Because economic insecurity is more common among those with less education or household income, groups of lower socioeconomic status are especially sensitive to changes in economic conditions. On the other hand, the economic recovery from the Great Recession and low unemployment rates since 2016 have not benefited the less educated as much as those with a college degree, especially among Whites, who have not been able to rebound from periods of economic insecurity as they have in the past. Thus, deteriorating economic conditions among those without a college degree may be an important factor explaining rising suicide mortality among Whites, especially White men.
Extensive research documents the Durkheimian premise that social integration within institutions, communities, and friendship and family networks is protective against suicidal behavior and death, and descriptive evidence suggests that such social capital resources are associated with lower suicide rates among Whites. Whether levels of social engagement have changed in recent decades to bring about the rise in suicide mortality, however, is more difficult to determine. Evidence indicates that social integration has declined in recent decades so that social isolation and lack of social support have increased. Engagement in religious organizations, for example, an important factor related to lower suicide rates, declined in the past decade, especially among Whites without a college degree. Marriage, another social context that is protective against suicide risk, also declined over the past several decades for White women without a college degree in particular, following a similar trend in marriage among Blacks seen several decades earlier.
Although suicide mortality by firearms rose over the study period, its contribution to the rise in overall suicide mortality declined as suicides by
other means increased more rapidly. Thus access to lethal means of suicide can only partially explain rising suicide mortality among Whites. While there is evidence that more firearm-related suicides occur in states with looser gun regulations and greater gun ownership and are higher in nonmetropolitan versus large metropolitan areas, the proportion of all suicide deaths related to firearms declined from 1990 to 2017. Further research is needed on lethal means of suicide to better understand the increase in different suicide modalities, how they differ by sex, and what factors might precipitate the choices made. In particular, research on the role of gun control laws and gun availability in suicide mortality is warranted, with attention to the causal effect of changes in gun control laws and gun availability on trends in suicide mortality.
Within the category of mental, emotional, and physical health, factors identified as especially relevant to suicide mortality are life-course traumas and stressors, especially those that occur early in life as adverse childhood experiences, and mental illness. Not surprisingly, those with a history of mental illness have a much higher risk of suicide. Poor access to mental health care may explain this relationship, although the evidence is inconclusive given the many different forms of access that are typically not measured in the databases available for study (e.g., density of licensed therapists, community-based programs, insurance, hospital emergency rooms). The important role of mental illness in explaining the rising trend in suicide mortality among Whites is supported by the concordance between the racial/ethnic patterns of mental health and the racial/ethnic patterns of suicide mortality. Whites have higher levels of lifetime mental illness relative to Blacks, Hispanics, or Asians, and this racial gap may be explained by differential levels of access to health care and treatment. Not only does better access to health care provide more opportunity to be diagnosed with a mental illness, but it also makes Whites more likely to receive prescription medications relative to Black or Hispanic adults, medications that sometimes induce depression or even suicide as a side effect, which might partially explain Whites’ higher rates of mental distress relative to nonWhites. Comorbidities related to physical illnesses, disabilities, and drug and alcohol use also contribute to levels of mental illness and pain, all of which represent important predisposing factors to suicide.
While the research literature provides some compelling evidence for links between changes in economic conditions, social integration, and psychological and physical well-being and the rise in suicide mortality among Whites, most of this evidence is suggestive and obscures the fact that these factors are interrelated and operate across the societal, community, and individual levels. For example, employment provides economic security, which reduces suicide risk, but employment also provides work-based social
networks, access to health information, health benefits, a sense of self-worth, instrumental social capital, health care, and psychological well-being, all of which are protective against suicide. Better understanding of the key factors involved and improved data explaining the recent rise in suicide mortality will require research in several areas, highlighted below.
IMPLICATIONS FOR RESEARCH AND POLICY
Because suicide rates increased from 1990 to 2017 mainly among Whites, research needs to focus on what changed for Whites, and why changes in economic conditions, social integration, or mental health and access to mental health care appear to have affected their suicidal behavior differently relative to other racial/ethnic groups. This information may be fruitful in understanding the smaller, but still concerning, recent increases in suicide among Black and Hispanic young adults. Although evidence indicates that recent trends in religious involvement, marriage rates, experience with pain, and psychological well-being coincided with rising rates of suicide among working-age Whites, especially those of low socioeconomic status, research has yet to forge explicit links between macro-, community-, family-, and individual-level trends and changes in suicide rates by sex, race and ethnicity, socioeconomic status, or geography. For example, the continued rise in suicide rates over the past several years among White Americans despite low unemployment and the prolonged economic expansion following the Great Recession points to the need to consider differential impacts of economic restructuring on population subgroups and geographic regions of the United States.
Prior studies have relied on either individual-level data (e.g., NHIS, NVDRS, NLMS) or aggregate-level data, typically at either the county or state level. Studies combining both of these types of data could help elucidate the relative importance of individual- and contextual-level factors and their possible interactions in suicide trends, with attention to the role of both protective and predisposing characteristics. For example, a multilevel study design would enable researchers to disentangle the effects of individual-level economic status, such as unemployment status and poverty, from those of upstream community-level economic conditions, such as declining manufacturing industries. Such a design could also help determine whether changes in the latter economic conditions interact with individual-level family characteristics, such as marital status and household income. These studies would benefit from considering geographic measures of social and economic factors from large social science surveys, such as the American Community Survey, and from continued linkage of the NHIS and the NLMS to the National Death Index (NDI).
A paucity of research on factors related to suicide mortality addresses differences by sex, race and ethnicity, socioeconomic status, and geography. Growing evidence suggests that the economic insecurity that characterizes the lives of population subgroups of lower socioeconomic status and with less education is linked to suicide mortality, but Whites of low socioeconomic status appear to be more vulnerable in this regard relative to their non-White counterparts. Given that the recent rise in suicide mortality has been driven mainly by Whites in nonmetro areas, understanding why the same economic, social, and geographic factors associated with rising suicide rates among Whites are not related to rising rates among other groups could provide insights into how to reduce suicide among Whites. Moreover, recent trends showing a slight rise in suicide deaths among Black and Hispanic young adults (ages 25–45) call for research on how the economic and social factors associated with suicide operate differently by sex, race and ethnicity, and geography in order to identify modifiable factors that can shed light on factors contributing to the rise among younger Blacks and Hispanics and help reduce disparities in suicide mortality. As noted in Chapter 7 (see Recommendation 7-3) and elaborated in Chapter 11 (see Recommendation 11-6), using a multilevel study design that combines aggregate- with individual-level data to uncover the individual-, meso-, and macro-level explanations for changes in mortality will advance research on suicide and the other major causes of death that this report documents as contributing to the recent rise in working-age mortality. Similarly, understanding how changes in suicide and other causes of death vary by sex, race and ethnicity, socioeconomic status, and geography is imperative for uncovering protective and predisposing factors unique to specific population subgroups to inform policies aimed at reducing disparities in mortality.
Accordingly, the committee developed a cross-cutting recommendation calling for quantitative and qualitative studies that would aid in assessing the role of upstream versus downstream factors in suicide risk and uncover the multilevel mechanisms that explain the demographic and geographic differences and temporal changes in suicide rates (see Chapter 11, Recommendation 11-6; see also Recommendation 7-3 in Chapter 7). There is a critical need for research on the role of access to mental health care in rising trends and disparities in suicide mortality (see also Chapter 7 and Recommendations 7-2 and 7-5). The lack of detail and specificity that characterizes existing research hampers the development of prevention strategies designed to improve access to mental health care and treatment for vulnerable populations, including non-Whites but also Whites of lower socioeconomic status. For example, measures and data regarding types of access and treatment are inconsistent and incomplete. In addition, research is needed on the geographic distribution and availability of mental health
services, substance use treatment programs, and emergency medical services that can play an important role in mental health treatments and suicide prevention (see Recommendations 7-2 and 7-5 in Chapter 7).
The findings presented in this chapter also point to the need for additional research on lethal means of suicide. Although rates of firearm-related suicide are higher in states with looser gun control regulations and greater gun ownership, the share of all suicides due to firearms declined during 1990–2017, while the share due to hanging, suffocation, and strangulation increased. More needs to be known about trends in different suicide modalities, variations by sex, and the causal role of access to and availability of firearms in trends in suicide mortality.
RECOMMENDATION 8-1: Federal agencies, in partnership with private foundations and other funding entities, should support research on lethal means of suicide aimed at better understanding the increase in use of different suicide modalities, how modalities differ by sex, and what factors might precipitate the choices made. Research on the role of gun control laws and gun availability is particularly warranted, with attention paid to the causal effect of changes in gun control laws and gun availability on trends in suicide mortality.
Studies taking a life-course approach to the study of mental health and suicide mortality using longitudinal data are also needed. Longitudinal data enable researchers to track predisposing and protective factors as they unfold across the life course to identify the most vulnerable life stages in the development of suicide behavior and deaths. Research taking this approach could answer such questions as the role of early-life and adolescent environments in predicting adult mental health outcomes, the extent to which those environments are moderated by adult characteristics and exposures, and whether these factors interact in their influence. Such datasets could also be used to assess childhood, adolescent, and adult precursors associated with suicide, including pain and disability. Several longitudinal studies that follow individuals over time, such as the National Longitudinal Study of Adolescent to Adult Health (Add Health), the Panel Study of Income Dynamics, the Wisconsin Longitudinal Study, MIDUS, and the Health and Retirement Study link their data to the NDI. Add Health, which has followed its respondents from adolescence into midlife, conducts ongoing death surveillance of its sample that includes the collection of death certificates to obtain primary and secondary underlying causes of death, hospital records, and interviews with next of kin for all decedents. To advance research in this area, all longitudinal studies, especially studies of early life and young adulthood, when mental health patterns are often established,
should routinely link their data to the NDI. Funders of longitudinal studies, especially the National Institutes of Health, could be instrumental in this regard by facilitating the regular linking of longitudinal study data through its administrative relationship with the NDI.
RECOMMENDATION 8-2: Directors and funders of longitudinal studies should routinely link these survey data to the National Death Index to support a life-course approach to the study of mental health and suicide mortality.




























