
In this session, workshop participants heard from stakeholders who shared their experiences innovating and adapting during the COVID-19 pandemic. Stakeholders included leaders from schools of public health, clinical educators, and students.
PUBLIC HEALTH
James Buehler, Drexel University
When the planning committee held listening sessions in preparation for this workshop, it heard from health professional educators, representing a wide array of perspectives, who spoke of the need to more substantially address social determinants of health and principles of health equity in their training programs. These are foundational concepts in the curricula of schools of public health, said James Buehler, clinical professor and interim chair of the Department of Health Management and Policy at Drexel University. As with other health professions, schools of public health seek interprofessional training opportunities for students and applied experiences outside of the classroom. However, said Buehler, rather than concentrating on the care of individual patients, public health students often work in communities with a variety of agencies and organizations, focus on promoting and protecting the health of populations, and work with people from a broad mix of health and nonhealth professions. To the extent that public health students are placed in health care organizations, they are positioned within administrative settings dealing with issues such as population health management, quality improvement, or performance management.
Like all other health professions education (HPE) programs, schools of public health suffered disruptions resulting from the COVID-19 pandemic, although the pandemic also presented new opportunities for engaging students. In this session, representatives of two programs of public health shared with workshop participants how they responded to those challenges and opportunities.
Academic Public Health Volunteer Corps
Neil Maniar, Northeastern University
In March 2020, Massachusetts Governor Charlie Baker convened the leadership of eight public health programs to find a way of engaging the programs in support of local health departments during the pandemic, said Neil Maniar, professor of practice and director of the M.P.H. program in the Bouve College of Health Sciences at Northeastern University. The group proposed an idea that would deploy volunteers into local health
departments, which were stretched beyond their capacity because of the pandemic. Out of these conversations, the Academic Public Health Volunteer Corps (APHVC) was born.1 The initial group of eight programs was expanded to additional schools and programs, including community health worker programs based in community colleges, as well as the Massachusetts Department of Public Health, the Massachusetts Public Health Association, and the Massachusetts Health Officers Association (see Box 3-1).
The eight original programs of public health had begun collaborating with the Massachusetts Department of Public Health in 2019, forming the Academic Health Department Consortium. Maniar noted how this preexisting relationship was instrumental in being able to bring these entities together and quickly develop the program. Although the participating organizations in the APHVC varied by size, reputation, and resources, Maniar said they all were committed to being equal partners in terms of their work, the weight of their voice, and the level of engagement for students. The
___________________
1 For more information, see https://academicpublichealthvolunteercorps.org (accessed March 31, 2021) and https://www.mass.gov/info-details/academic-health-department-academic-public-health-volunteer-corps (accessed March 31, 2021).
Massachusetts Health Officers Association acted as the key point of contact with the 351 local boards of health across the state.
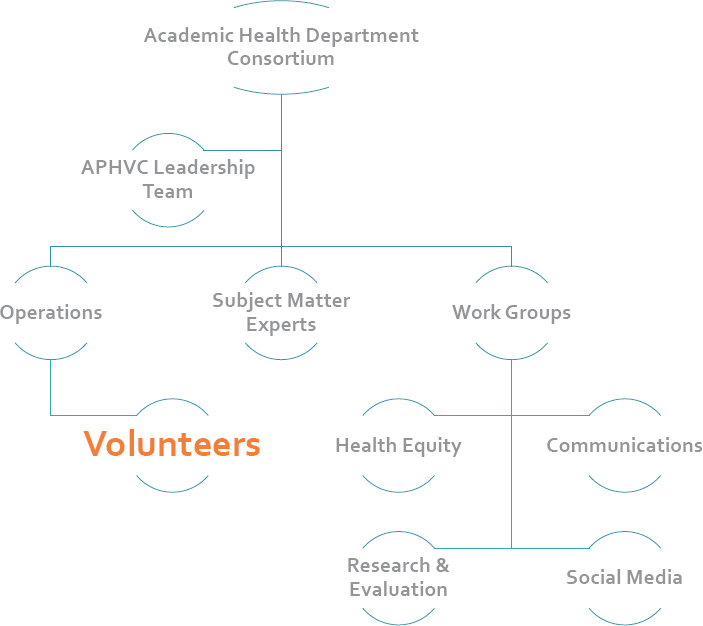
The mission of APHVC is “to support state and local public health agencies and to advance health equity in Massachusetts by engaging public health students, alumni, and expert volunteers through interdisciplinary collaboration.” The operational structure of the program took some time to develop, said Maniar, but eventually leaders of different parts of the program emerged, as well as working groups and subject-matter experts (see Figure 3-1).
APHVC began with a focus on contact tracing. Within 1 week of launching the program more than 2,000 volunteers had signed up, and 1,200 of these were deployed into about 80 communities across Massachusetts. The volunteers made more than 2,000 contact tracing calls in the first month and assisted communities with developing policy proposals. In addition, volunteers created dozens of infographics and geographic information system
SOURCES: Maniar presentation, December 3, 2020. King S, Maniar N, Gilbert Loinaz A, Levy C, Blinn A, Sibor D. June 2020. Copyright 2020.
(GIS) maps to support local public health education and surveillance needs, and they helped translate materials and messaging into different languages.
Health equity is a critical component of the APHVC mission, said Maniar, as he shared an example of the group’s work in this area. The towns of Randolph and Brockton have large Haitian and Cabo Verdean populations, and the local health departments identified challenges in these communities around the issues of testing, social distancing, mask wearing, and stigma. APHVC worked with the community to create a team that included community members and heritage speakers;2 key informant interviews were also conducted. The team translated materials, collaborated with local radio stations, and used social media to educate the community in a culturally sensitive and linguistically appropriate manner while responding to its needs. As the pandemic continues, said Maniar, APHVC will be focusing its efforts in a number of areas, including
- Increasing focus on health equity;
- Assisting with policy development related to reopening;
- Engaging additional local partners including community health centers, nonprofit partners, and local cultural organizations and coalitions; and
- Focusing on data analysis, epidemiology, and data translation needs at the local level.
The academic programs involved in APHVC, said Maniar, see it as a viable and sustainable collaborative that can help engage students and support public health efforts. To ensure the program remains relevant and effective beyond the current pandemic, APHVC is undertaking three actions: (1) establishing a development committee to secure long-term funding, (2) conducting interviews and surveys about local board of health perceptions of the APHVC experience, and (3) evaluating the work accomplished thus far. In this way, Maniar said, APHVC hopes to create a long-lasting, valuable collaboration among public health learners and experts across multiple sectors.
Dornsife School of Public Health
Jennifer Kolker, Drexel University
The M.P.H. program at the Drexel University Dornsife School of Public Health is accredited by the Council on Education for Public Health (CEPH),
___________________
2 Heritage speakers are “individuals raised in homes where a language other than English is spoken and who are to some degree bilingual in English and the heritage language” (Valdés, 2000).
said Jennifer Kolker, clinical professor of health management and policy. As part of the accreditation, all M.P.H. students are required to complete an applied practical experience (APE), which is a supervised, hands-on project or internship within a public health practice setting. Through the APE, students are expected to develop competencies commensurate with their area of focus (e.g., epidemiology), as well as three competencies that all students must meet:
- Communicate audience-appropriate public health content, both in writing and oral presentation;
- Perform effectively on interprofessional teams; and
- Apply systems thinking tools to a public health issue.
The accreditation guidelines, said Kolker, emphasize that the APE should generally take place outside the school of public health; in a governmental, nonprofit, or for-profit setting; and involve community engagement with external partners. M.P.H. students at Dornsife have completed the APE in a wide variety of settings, including public health departments and other governmental organizations, large nonprofit health and social service organizations, small community-based organizations, clinical settings, and regional planning associations. In these settings, students have worked on projects such as needs assessments, strategic planning, program evaluation, policy, and research, noted Kolker.
When the COVID-19 pandemic began in early 2020, she said, it was the “peak time” for coordination of sites and student placement decisions. Realizing the approach to APE would have to change dramatically, educators at Dornsife asked themselves two questions:
- How do we make the student APE experience as rich and rewarding as possible?
- How do we best serve our public health community?
To pivot the APE program in a way that served both students and the public health community, said Kolker, Dornsife focused its efforts on four areas: reassure students, strategize with partners, ask accreditors for flexibility, and develop nontraditional placements.
Reassure Students
Students had a number of worries, said Kolker. They were dealing with their own issues related to COVID-19, such as isolation and worrying about family members with health challenges. Students were anxious about missing out on a critical component of their MPH training. The APE
experience, she noted, is considered a key way that students get the training they need to get a job after school. Students were also concerned about the COVID-19 pandemic in general and wanted specific opportunities to feel part of the response to the pandemic. The school worked to ensure that students felt safe and supported, while assuring them there would be opportunities to get involved.
Strategize with Partners
Many of the projects that had been planned for students were cancelled owing to logistical challenges or changing priorities of the partner organizations. Partners were struggling to manage the shift to remote work for their own staff, and many were burdened with new responsibilities and circumstances. The idea of adding the task of supervising and mentoring students was overwhelming, said Kolker. Dornsife worked with its partner organizations to redefine opportunities and rethink how students could be a valuable addition during the pandemic.
Ask Accreditors for Flexibility
The accrediting guidelines for APEs are fairly specific in terms of setting, competencies, and deliverables, Kolker said. In the midst of the pandemic, Dornsife and other schools of public health determined that some of these guidelines would need to be relaxed. Kolker and others wrote a letter to CEPH asking for greater flexibility on a number of issues, including content, types of deliverables, preceptor requirements, and competency matching. The letter to CEPH expressed confidence that individual MPH schools and programs “can assure and manage the learning that will come from these APE experiences in ways that both meet our students’ learning needs and achieves the intent of the APE.” CEPH obliged and granted the necessary flexibility.
Develop Nontraditional Placements
Finally, said Kolker, Dornsife developed new options for students beyond the traditional 1:1 placements. Although some organizations were able to accommodate and host students, the demand for placements was greater than the supply. To fill this gap, the school created a consulting course where students worked in teams to develop products supporting the needs of six organizations, with some of the projects focused on the pandemic.
The experience of rethinking and restructuring the APE, said Kolker, was largely positive for both students and organizations. All students were
able to fulfill the APE requirement, either through a remote traditional placement or through one of the other options. The organizations reported that students made valuable contributions, particularly those who worked on COVID-related projects. Students who felt cut off from the world during the pandemic found the team-based projects, such as the consulting course, helped mitigate their sense of isolation. Of course, said Kolker, there were drawbacks as well. Students missed the experience of physically being in an organization, and they missed out on developing soft skills and the nuanced learning that stems from working with other people. In addition, mentoring and supervision were challenging in a remote setting. However, overall, the experience demonstrated the ability of the school and its partners to quickly adjust during a challenging and changing situation, she said.
Kolker offered two thoughts on using lessons from COVID-19 to inform the future of HPE. First, COVID-19 has driven home the idea that interprofessional education goes far beyond the clinical and health care setting. For example, if public health professionals are tasked with deciding whether schools or businesses should be open, public health students and trainees need to learn how these sectors are organized, staffed, and financed. Second, Kolker said, health professions educators need to consider how to “truly be responsive” to public health partners, particularly during a crisis. Specifically, do the competencies taught in school accurately reflect public health practice, are there ways that accreditors can be flexible in order to better meet the needs of the community, and how can educators be flexible and nimble both during an emergency as well as in normal times?
CLINICAL EDUCATION
Kimberly Lomis, American Medical Association
Experiences in the clinical learning environment are a critical element across all health professions education, said Kimberly Lomis, vice president for undergraduate medical education innovations at the American Medical Association (AMA). These experiences support the development of competencies as well as professional identity formation. During the pandemic, learners across the health professions were abruptly displaced from care settings because of concerns about both safety and education. Regarding safety, she said, there were concerns about student and patient safety, given the limited bandwidth of faculty to appropriately supervise clinical students. Regarding education, there were concerns that because of disruption of the case mix and disruption in how clinical settings were functioning, placements would not be meeting the traditional goals of clinical education. In this session of the workshop, speakers discussed innovations to ensure that learners had adequate clinical experiences during the pandemic.
Practice/Academic Partnership Model
Nancy Spector, National Council of State Boards of Nursing
COVID-19 put a significant demand on the nursing workforce, said Nancy Spector, director of regulatory innovations at the National Council of State Boards of Nursing (NCSBN). Because of the pandemic, it was more critical than ever for nursing students to be ready for practice upon graduation. However, at the same time, health care facilities were shutting doors to nursing students, and students were graduating without clinical experience. Spector recalled one board of nursing’s concern that “some students would graduate without even having touched a patient.” Although schools used simulations and virtual experiences, Spector said, “nothing can replace those clinical experiences with patients.”
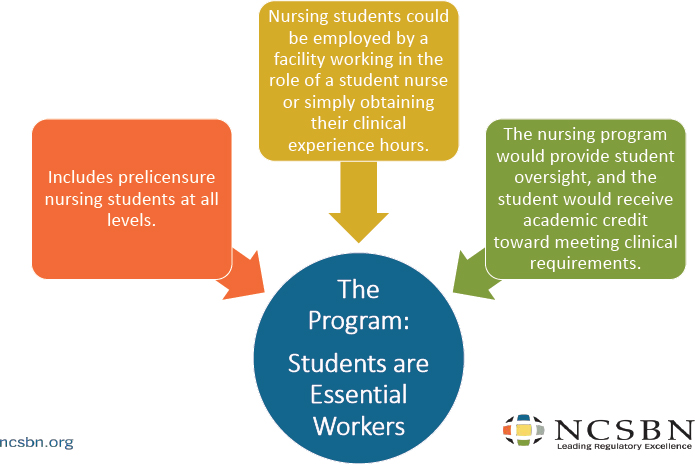
In March 2020, NCSBN convened a group of nursing leaders from practice, academia, and regulation to find a solution to this challenge, and together they developed the practice/academic partnership. The key to the program, said Spector, is for students to be considered “essential workers,” which is a designation from the college of nursing and the health care setting that, in her experience, is almost always agreed to by government officials. The partnership incorporates all levels of prelicensure nursing students as either facility employees or trainees obtaining clinical hours. Faculty provide oversight of the students, and in some cases, the practice setting also provides preceptors. Academic credit is awarded toward clinical experiences (see Figure 3-2).
This program, said Spector, is a win-win for practice and academic organizations, and it presents an unparalleled opportunity for students to work and learn in a time of crisis and to gain firsthand exposure to the principles of population health and emergency management. Clinical assignments for students in the program varied. Most cared for nonCOVID-19 patients to free up nurses, although some cared for COVID-19 patients directly. Students gained experience in areas including testing, vaccine administration,3 screening, and telehealth. The program was endorsed by numerous nursing organizations (see Box 3-2).
A number of lessons were learned during the process of developing and implementing this program, said Spector. First, communication between all stakeholders was key, particularly to clarify the expectations and responsibilities of all involved (e.g., oversight of students). Spector remarked that while it was critical to rely on already-established channels of communication, it was also important to establish new mechanisms for clear communication. Second, preexisting relationships between practice settings
___________________
3 At the time of the workshop, the vaccine was not being administered.
SOURCES: Spector presentation, December 3, 2020. Copyright 2020. National Council of State Boards of Nursing. Used with permission from the National Council of State Boards of Nursing.
and academic programs can be used in support of the new model, and new relationships can be formed, but it may require writing up new contracts, providing orientation specific to COVID-19 policies, and determining who will provide personal protective equipment (PPE) for the students. Spector expressed a note of surprise that rural critical access hospitals were eager to join the partnership because she and her colleagues had up to this point just assumed most of the practice partners would be medical centers. Third, faculty ought to collaborate closely with the practice setting in order to identify and meet the objectives of students and organizations, and to ensure the planned experience fulfills clinical requirements. Fourth, students need to be prepared for what will be expected of them in the practice setting. For example, trainees must be familiar with the COVID-19 policies, know the risks and responsibilities of working in a health care environment during the pandemic, and be proficient at safely donning and doffing PPE.
As of December 2020, said Spector, the program had been implemented in Georgia, Idaho, and Iowa, with more than 700 participating students and an overwhelmingly positive response from students, faculty, and practice partners. One student’s comment described a “pretty challenging but very rewarding experience,” while a faculty member said that students “embraced this opportunity to help meet the needs of the community during this unprecedented time.” A practice partner reported hiring 92 percent of the participating spring graduates, and 100 percent of the graduates passed the National Council Licensure Examination exam. Spector closed, saying while the main goal of the program was to provide clinical placements for students during COVID-19, this type of partnership between academia and practice could help close the education-practice gap that has been discussed by members of the forum and others in previous workshops held by the National Academies (NASEM, 2018).
Lessons Learned from the American Medical Association’s Accelerating Change in Medical Education Consortium
Kimberly Lomis, American Medical Association
In 2013, AMA launched the Accelerating Change in Medical Education Consortium, said Lomis. This baseline investment in innovation prepared AMA to better respond in a time of crisis, such as the COVID-19 pandemic. The consortium consists of 37 medical schools and programs that work together, with a major emphasis on the training of health professionals in health systems science. Medical education tends to have a rigid structure, she noted, so this emphasis on systems thinking is useful for contemplating alternative paths to the same outcomes when the traditional paths are disrupted.
In the early days of the pandemic, the consortium virtually convened on a regular basis to discuss struggles, share ideas, and strategize. Lomis described three major phases of response to the COVID-19-related disruptions to clinical experiences. First, as students were pulled out of the clinical environment, medical programs were offering alternatives through coursework in pandemic-specific areas, general clinical topics, and discipline-specific topics. These alternatives, said Lomis, were partially a way to “buy some time” to create alternative pathways for clinical learning.
The second phase involved engaging students in physically distanced patient care roles. This involved tasks such as working on COVID-19 hotlines, preparing educational materials, and conducting contact tracing. In addition, students could engage in general clinical training that could be conducted remotely. As others have mentioned, noted Lomis, the consortium also found medical students eager to add value and do their part in the fight against COVID-19. The third phase was getting students back to direct interaction with patients. This was accomplished in some areas in summer 2020, but it continues to be difficult.
One way of rethinking how to conduct clinical education in the midst of the pandemic, Lomis said, is to use competency-based approaches. A competency-based framework starts by identifying the desired learning outcomes, which is followed by a process of deconstruction to ensure the learning activities and assessments will lead to those predefined desired outcomes. Lomis noted how educators can be “a little bit entrenched” in traditional learning activities and can lose sight of the fact that outcomes—not the activities—are the ultimate goal. A competency-based framework views time as a variable, rather than as a fixed proxy for learning. For example, she said, medical school courses are traditionally defined by length (e.g., one semester), whereas a competency-based approach looks at when the learning outcomes are achieved.
Lomis gave an example of how a medical clerkship could be deconstructed in order to find alternate ways of giving students similar experiences and opportunities to develop the same competencies. There are layers of competency development, starting with the “big Cs” such as patient care, medical knowledge, professionalism, and interpersonal and communication skills. Next, there are overarching clinical skills that students develop through a clerkship, such as diagnostic skills, clinical reasoning, and ethics, followed by discipline-specific knowledge and skills. Developing most of the skills in these areas does not require direct physical contact with a patient. For instance, said Lomis, interpersonal skills can be gained through helping an elderly patient prepare for a telehealth visit, and clinical reasoning can be performed remotely. Identifying alternative approaches for developing some of these skills can allow educators to take full advantage of the “precious time” when students do have
direct contact with patients by concentrating only on skills that must be developed in person.
Using a competency-based framework can be enormously helpful during a challenging time such as the COVID-19 pandemic, Lomis said. A rapid response was required to ensure students’ medical education continued, but students and faculty felt strained as changes to education and practice occurred quickly and frequently. This framework can help show the reflection and thought that went into developing alternative educational pathways. The framework can also provide a stronger rationale for the choices made during the pandemic, she said. Showing learners the value in focusing on the most critical components can support the students’ understanding of why certain decisions that disrupted their education was in their best interest. However, said Lomis, “there’s no getting around” the fact that these students will have some gaps in their experiences, and the gaps will vary among learners. As these students move forward in their education and practice, a competency-based framework will be a tool for identifying and filling the gaps with additional experience and training.
STUDENTS
Emilia Iwu, Rutgers University
Emilia Iwu, clinical faculty at the Rutgers School of Nursing Newark, introduced three health professions students—from medicine, social work, and nursing—to speak about their experiences during the COVID-19 pandemic. Iwu asked the students to focus particularly on adaptations to education that should be continued post-COVID, and those that should be left behind.
MEDICINE
Londyn Robinson, University of Minnesota Medical School
Londyn Robinson, a fourth-year medical student at the University of Minnesota Medical School, began by noting that she and her fellow students had only 2–3 months of in-person clinical rotations during their final year of medical school. Because of this, she said, some students have doubts about whether they are prepared for residency. She added that the entire national cohort of 25,000 medical students missed out on this training, and said “You can’t replace the in-person clinical environment, full stop.” Robinson wondered how medical residency programs and other health professions programs will adapt to the lack of knowledge and experience
these students are bringing to the workplace, and how they will ensure competent patient care.
On the positive side, Robinson said the transition to online coursework was fairly seamless. She and her fellow students appreciated the online resources that were made available for free, and how the online format of learning increased student participation and engagement. However, many schools “continue to sweat the small stuff,” she noted, and students are being asked to do equal if not more work than before the pandemic. Robinson further remarked that while state public health officials urged people to stay home, students were still required to take the Medical College Admissions Test (MCAT) and medical licensing exams in person. Several students tested positive for COVID-19 after taking the MCAT, she said, and many students had to reschedule exams multiple times in multiple states. Robinson herself rescheduled her exam five times, and ended up taking it on the day of her grandmother’s funeral.
Robinson then shifted the presentation to share her personal response to the pandemic as a medical student in co-founding a nonprofit organization called Minnesota CovidSitters. She and other medical students recognized that childcare was one of the “major bottlenecks” preventing health care workers from working since the onset of the pandemic. With schools and day care centers closed, health care workers were “caught between choosing going to work to help care for people’s families, or staying at home to care for their own.” The students worked with a local technology company to develop an application that uses GPS coordinates to match health care workers’ needs with free babysitting services. The service quickly expanded beyond Minnesota to operate in 32 states and 5 different countries, serving more than 1,000 families. Robinson said the project was completely student led and interprofessional, and she emphasized that students did this work in their free time outside of courses and other responsibilities.
SOCIAL WORK
Angela Wilbon, Howard University School of Social Work
Angela Wilbon has a dual role at the Howard University School of Social Work. She is a doctoral student in the dissertation proposal writing phase and also works with M.S.W. students who are training to become behavioral health providers. During the pandemic, Wilbon admitted that she and other students experienced isolation, and they formed virtual writing or study groups in order to be able to connect. The M.S.W. students she trains have grappled with how to build rapport and connect with clients when meeting virtually or when meeting in person but physically distanced. To cope with the pandemic, she said, it has been critical to transparently
acknowledge the victories and challenges, and to practice self-care and continue connecting with others through virtual social activities. Above all, she said, both students and service providers need to grant grace and compassion to themselves and others.
There have been some positive educational experiences during the pandemic, said Wilbon. Students have felt well supported by faculty members, in terms of both academics as well as personal challenges. Faculty and leaders have supported and encouraged students through Zoom, email, and telephone calls at all hours of the day, she said. Another positive experience was the opportunity for students to participate in interactive, experiential, and problem-based learning, where “students can be engaged and pulled into the lectures and the conversations so they own the experience and that education.” Students also worked with standardized patient case telesimulation, which “they love” because they could hone their craft in a safe environment. In addition, some students were exposed to telehealth services, and were able to learn best practices and the ethical responsibilities of remote care.
Of course, said Wilbon, students also missed out on some opportunities and faced challenges during the pandemic. There were fewer field placement opportunities, and there is a continued need for students to learn how to build rapport with clients virtually. Some online educational methods—such as lectures and PowerPoint slides—were devoid of student engagement or interaction. Students missed out on in-person connection to fellow students, faculty, and clients. Finally, said Wilbon, there is a need for students and faculty to find strategies to reach and serve medically underserved communities who lack access to technology.
NURSING
Gusna Hoque, Rutgers University Nursing Program
The junior year of nursing school is generally the hardest year, said Gusna Hoque, a student in the nursing program at Rutgers University. This is the year when students take their foundational classes that shape them as nurses. The year started off normally, said Hoque, but in mid-March, all in-person classes and clinicals were suddenly cancelled because of the pandemic. Adjusting to this new reality was difficult, said Hoque, and students were concerned about their own health, their family’s health, and the stress of continuing their studies during a global pandemic. Many students lived with multiple family members and found it difficult to find a quiet space and time to study. Rutgers was able to restart clinicals for students in the fall semester, and students worried about bringing the virus home to their families. Some students, including Hoque, had family
members who suffered or died from COVID-19. During all of this, Hoque said, students were still expected to meet the high expectations of nursing school, rather than being given a pass/fail option like students in many other majors.
However, there were also positives: studying from home saved students time and money, the extraordinary circumstances created strong bonds between peers, and students experienced individual growth as they learned their own strengths and weaknesses. Students learned to cope with the stress through various strategies including peer-to-peer support and acknowledging their own struggles and emotions. Iwu added that as future frontline workers, it is critical that students learn these types of strategies during school. Hoque closed with the hope that as she and her fellow students move into the workplace with less experience under their belt, they will be helped and guided by experienced health care staff who acknowledge the challenges of education during a pandemic.
REFERENCE
NASEM (National Academies of Sciences, Engineering, and Medicine). 2018. Improving health professional education and practice through technology: Proceedings of a workshop. Washington, DC: The National Academies Press. (See Chapter 3.)
















