
Proceedings of a Workshop
OVERVIEW OF THE WORKSHOP1
“Psychosis” refers to conditions that affect the mind and how the brain processes information to cause a disconnect with external reality. According to the National Institute of Mental Health (NIMH) approximately 100,000 people develop psychosis in the United States every year, with early episodes often appearing when a person is in their late teens to mid-twenties. Psychotic illnesses, such as schizophrenia and bipolar disorder, come with a risk of significant individual long-term impairment.2
Research has demonstrated that appropriate treatments and supports can help prevent the full onset of psychotic illness for persons in a high-risk state and can improve long-term outcomes for those who have already experienced a first episode (Correll et al., 2018; Fusar-Poli et al., 2017; McGorry, 2015). This research has enabled specialized early intervention and treatment programs that can benefit millions of young people who are experiencing a first episode of psychosis or are at risk for psychosis.
___________________
1 The planning committee’s role was limited to planning the workshop, and the Proceedings of a Workshop has been prepared by the workshop rapporteurs as a factual summary of what occurred at the workshop. Statements, recommendations, and opinions expressed are those of individual presenters and participants, and are not necessarily endorsed or verified by the National Academies of Sciences, Engineering, and Medicine, and they should not be construed as reflecting any group consensus.
2 See https://www.nimh.nih.gov/health/publications/understanding-psychosis (accessed October 4, 2022).
To explore how to improve care for people experiencing psychosis, including prevention and early identification, treatment, and recovery, the Forum on Mental Health and Substance Use Disorders at the National Academies of Sciences, Engineering, and Medicine (National Academies) hosted a workshop, Early Interventions for Psychosis: First Episodes and High-Risk Populations, on July 11, 2022. In the introductory remarks, planning committee co-chair Ruth Shim,3 associate dean and the Luke and Grace Kim Professor in Cultural Psychiatry at the University of California—Davis (UCD), observed that despite psychosis being relatively rare with a lifetime prevalence of approximately 3 percent (Sullivan et al., 2020), untreated individuals suffer, family relationships are disrupted, and communities absorb new burdens because of the serious impacts of the condition. “The good news, though, is that in the last 20 years or so, we have begun to see a lot of promise in this area,” she said, referring specifically to coordinated specialty care (CSC) programs that demonstrate the ability to assess and improve outcomes (Read and Kohrt, 2022). The goal of CSC, a recovery-oriented treatment program for people with first-episode psychosis, is to promote shared decision making by using a team of specialists to work with individuals to create a personal treatment plan (Bello et al., 2017; Hamilton et al., 2019).
Shim noted that while early-psychosis programs originated in Australia and Europe, the number of U.S. programs has grown from 12 in 2008 to more than 160 in 2018 and more than 350 in 2021 (Heinssen and Azrin, 2022; Read and Kohrt, 2021). Improved outcomes from these programs include greater work and school involvement, lower symptom severity, fewer interactions with the legal system, and fewer psychiatric hospitalizations. However, Shim noted that these outcomes have not been delivered equitably across different populations.
The workshop unfolded across four sessions that explored the epidemiology of first-episode psychosis and those populations that are at high risk; examined several effective care models and the associated challenges and barriers such as workforce, access to care, funding, and sustainability; considered short- and long-term outcomes of early interventions; and explored policy opportunities to support, advance, and improve early interventions. Appendixes A and B contain the workshop Statement of Task and agenda, respectively. The objectives were to discuss the following:
- The epidemiology of first-episode psychosis and the population at high risk for psychosis, including international data and gaps in knowledge;
___________________
3Appendix C provides complete titles and affiliations for all speakers.
- The current models of effective or promising interventions and service delivery for patients with early psychosis and populations at high risk for psychosis; and
- Evidence on short- and long-term outcomes of early prevention efforts for those at high risk and interventions for those who are experiencing a first episode.
This Proceedings of a Workshop summarizes the presentations and discussions. The speakers, panelists, and workshop participants presented a broad range of views and ideas, and Box 1 provides a summary of key observations from individual participants about care for people with early psychosis. Appendix C provides biographical sketches for the workshop
speakers and moderators. The workshop speakers’ presentations (as PDF and video files) have been archived online.4
IDENTIFYING POPULATIONS AT RISK FOR PSYCHOSIS AND INTERVENTIONS TO REDUCE RISK
Patrick McGorry, executive director of Orygen and professor of youth mental health at the University of Melbourne, Australia, described how, when he first began his training in the 1970s, psychiatrists were telling young people with a schizophrenia diagnosis that they had no hope of recovery and their lives were over. McGorry explained that this notion, which has proved to be wrong, came from Emil Kraepelin’s concept of
___________________
4 See https://www.nationalacademies.org/event/07-11-2022/early-interventions-for-psychosis-first-episodes-and-high-risk-populations (accessed September 16, 2022).
schizophrenia as a deteriorating dementing illness, which even Kraepelin discounted eventually (Ebert and Bär, 2010). Early intervention has been one of the key antidotes to that pessimism, said McGorry.
The current goal of treatment for schizophrenia and other psychotic illnesses is to bend the outcome curve and reduce the burden of disease (Light and Swerdlow, 2015). These treatments are not curative, but they do offer a better prospect of leading a fulfilling life. The key is to treat these individuals as early as possible, and research focusing on the early stages of psychosis has identified an early-stage or subthreshold and prodromal phase with a gradual onset in most patients (Addington, 2003; Modinos and McGuire, 2015). This finding allowed McGorry and colleague Alison Yung to define the criteria that predicted the transition to more sustained psychosis and thereby identify people who are at high risk of early transition (McGorry, 2015).
McGorry referenced a 2012 meta-analysis of transition outcomes in individuals that met the criteria for subthreshold psychosis, which showed that about a third of them developed psychotic illness or continued in a subthreshold state in the subsequent 3 years. (Fusar-Poli et al., 2012). Determining options for treating these high-risk individuals in the subthreshold state becomes a challenge. Interventions including cognitive behavioral therapy (CBT), antipsychotic medication, and integrated psychological interventions aim to reduce the risk of progressing further by delaying the transition and alleviating patient distress (Mei et al., 2021; van der Gaag et al., 2013), but some meta-analyses indicate that treatment does not reduce the risk of progression (Davies et al., 2018). McGorry referred to a Cochrane Review that he said was poorly conducted, with a conclusion that although treatment has not been shown to be particularly effective, some interventions were worthy of further study (Kuharic et al., 2019). McGorry and his collaborators have written several critiques of these studies (McGorry and Nelson, 2020; Nelson et al., 2020). McGorry acknowledged that the currently available early interventions for psychosis are not sufficient and that researchers need to develop interventions that are more effective at the earliest stages of illness and false positives are common with early-stage conditions.
McGorry explained that the prodromal phase is a clinical phenotype with a “need for care” because it has a substantial risk of transitioning to psychosis. “We can sharpen prediction, but biological markers so far have not been particularly useful,” according to McGorry. He emphasized that research is needed to develop new treatments and to clarify the sequence of treatments for the ultra-high-risk population. McGorry pointed to the complexity of this task, given that research on new interventions will have to account for the heterogeneity of psychotic illnesses. Moreover, other comorbid syndromes tend to emerge that require treatment in their own
right. McGorry referred to the NIMH Accelerating Medicines Partnership Program—Schizophrenia (AMP-SCZ), which is developing tools that aim to improve success in developing early-stage interventions for individuals at risk of developing schizophrenia.5
McGorry explained that he and his colleagues conducted a randomized trial of interventions for individuals at ultra-high risk6 in which they tested a sequential intervention strategy that increased treatment intensity over time (Nelson et al., 2018). “We found that adding intensity did not particularly improve the response, which was unexpected,” he said. Antidepressants did not seem to help in reducing symptoms or improving functioning, and CBT did not produce better results than normal supportive case management, “We do need to redouble our efforts to look for more innovations and treatments,” he concluded.
As part of the AMP-SCZ, McGorry and his collaborators are participating in the largest global schizophrenia study ever funded,7 examining a range of biomarkers through sophisticated statistical analyses to find subgroups of patients with particular disease mechanisms, with the goal of improving biomarker-assisted prediction (Polari et al., 2018). McGorry shared that after 2 years of preparation and organizing sites, the study began recruiting in the fourth quarter of 2021.
McGorry explained that because 93 percent of the ultra-high-risk individuals develop other psychopathologies (Lin et al., 2015), the field has moved to a transdiagnostic approach for identifying individuals at risk for psychosis, which he believes is the way forward for research and clinical care (McGorry and Nelson, 2016; McGorry et al., 2018; McGorry and Hickie, 2019). “The ultra-high risk or at-risk mental state has been a very heuristic concept, allowing us to see what we need to do in terms of diagnostic flexibility going forward for biological research,” he explained. The original goal of his work was to try to sharpen the prediction for psychosis, but he and his collaborators realized that the micro phenotypes that they were seeing in the early stages are actually relevant to a range of different late macro phenotypes, such as schizophrenia, depression, bipolar disorder, personality disorder, and substance use disorder. His research is now focusing on the opportunity to identify biomarkers for these conditions and to intervene earlier in these other mental health disorders as well. Biomarkers,
___________________
5 See https://www.nimh.nih.gov/research/research-funded-by-nimh/research-initiatives/accelerating-medicines-partnershipr-program-schizophrenia-ampr-scz (accessed September 16, 2022).
6 Individuals are considered ultra-high-risk for psychosis if they meet a set of standardized criteria including presumed genetic vulnerability (trait), recent history of attenuated psychotic symptoms, or brief limited intermittent psychotic symptoms (McHugh et al., 2018).
7 See https://www.ampscz.org/scientists/design/ (accessed February 7, 2023).
noted McGorry, could also lead to novel therapies and might map more closely onto the stage of illness than they do to the overall syndrome.
EARLY INTERVENTION FOR FIRST EPISODES OF PSYCHOSIS
McGorry emphasized that treatment delays for individuals who develop psychosis can have a significant impact, as research has shown that the duration without treatment once sustained psychosis is apparent is a key factor in patient outcomes (Drake et al., 2020; Hegelstad et al., 2012). In the United Kingdom, this finding has translated into a requirement that patients with sustained psychosis need to be treated within 2 weeks, with financial penalties on care providers for a longer delay (NHS England et al., 2016; Reichert and Jacobs, 2018). NIMH’s research project, Recovery After an Initial Schizophrenia Episode (RAISE),8 found that the window of opportunity was perhaps a little longer for benefit from early-intervention programs, but beyond 74 weeks, the programs had no benefit (Kane et al., 2016).
McGorry noted that many jurisdictions in Europe, North America, Australia, and Asia have scaled early-intervention programs based on evidence developed over the past 30 years, with the International Early Psychosis Association9 playing a key role. A 2018 meta-analysis provided a stronger evidence base that supports the value of early intervention and has helped drive care reform across the United States (Correll et al., 2018). Between fiscal years (FYs) 2014 and 2021, the U.S. Congress allocated more than $400 million to support evidence-based treatment programs that address the needs of individuals experiencing a first episode of psychosis (Thomas, 2022), and NIMH and the Substance Abuse and Mental Health Services Administration (SAMHSA) collaborated in translating scientific insights from RAISE into practical guidance to states for establishing recovery-oriented programs that coordinate medical, psychosocial, and support services. With roughly 3 million people in the United States living with schizophrenia, there are more than 350 publicly funded early-intervention programs for first-episode psychosis operating in all 50 states, serving tens of thousands of adolescents and young adults each year (Heinssen and Azrin, 2022). McGorry noted that the U.S. government provided $100 million in FYs 2016 and 2017 to establish 187 community clinics that provide early intervention for psychosis.
McGorry emphasized that early intervention is cost effective and not intervening for first episodes of psychosis is actually wasting money (Cam-
___________________
8 See https://www.nimh.nih.gov/health/topics/schizophrenia/raise (accessed September 16, 2022).
9 Now rebranded as the IEPA Early Intervention in Mental Health: https://iepa.org.au (accessed September 16, 2022).
pion and Knapp, 2018). “It is the best buy, actually, in psychiatry, that we have so far, so it is important that every service offers this now,” he observed. More importantly, early intervention saves lives, with early mortality rates four times lower compared to those with first-episode psychosis who did not use early intervention services (Anderson et al., 2018). Noting that the full potential of early intervention has not yet been realized, McGorry added, “We have to think how we can actually maximize the benefit of these reforms and the evidence that we have so far.”
Approaches for maximizing these benefits include a greater focus on youth mental health (Malla et al., 2016) and reducing the untreated duration through communication programs and detection teams, approaches that nations such as Norway are implementing (Joa et al., 2015, 2021). Safely identifying individuals resistant to early treatment and providing low-dose clozapine10 might also be an option, McGorry added.
McGorry noted that an important feature of early-intervention programs, like the RAISE study, is their holistic approach to care that includes preventive physical health care, sexual health care, substance use treatment, family care, and vocational recovery. Digital augmentation of these programs through the MOST (Moderated Online Social Therapy) program at Orygen11 is another approach for strengthening early-psychosis care. McGorry called attention to one unanswered question: whether a subgroup of patients can safely cease medication or reduce dosage in the early phase as opposed to continuing standard maintenance therapy.
McGorry stressed that the key is to strengthen early intervention, make it the global standard of care, and put it in the context of broader youth mental health care and early intervention, given that most adult psychotic disorders emerge in the adolescence/young adult period.
The Epidemiology and Social Patterning of Psychosis
Deidre Anglin, associate professor of clinical psychology in the Department of Psychology Doctoral Clinical Program at City College of New York, said that although much of the research on social location12 and iden-
___________________
10 Clozapine is U.S. Food and Drug Administration– (FDA-) indicated for treatment-resistant schizophrenia and suicide prevention in patients with schizophrenia or schizoaffective disorder with chronic suicidal behaviors. Clozapine is not authorized for use in first line treatment for schizophrenia due to the high burden of adverse effects, requires regular blood work, and has not outperformed other medications in first-episode patients.
11 See https://www.orygen.org.au/Clinical-Care/Clinical-services/most (accessed December 6, 2022).
12 An individual’s social location is defined as the combination of factors including gender, race, social class, age, ability, religion, sexual orientation, and geographic location.
tity and their relation to the incidence of psychosis comes from northern Europe, some of the earliest studies were in the United States, particularly in terms of how psychosis incidence is related to migration or being part of a minoritized group. She noted that one study from the early 1930s, for example, found that Norwegian immigrants to the United States were twice as likely to receive a schizophrenia diagnosis compared to people born in the United States or living in Norway (Odegaard, 1932, 1935). The view at the time was that this was a selective migration phenomenon, but other research from the early 1930s connected psychosis incidence to ecological characteristics in urban neighborhoods, such as population density and poverty, for both Black and White individuals (Faris and Dunham, 1939). “The idea that psychosis is not randomly distributed in the population is a very old thought,” observed Anglin.
Anglin explained that this early research work inspired some robust studies that also found a higher incidence of psychosis among immigrant populations, particularly in Black Caribbeans and Black Africans (Fearon et al., 2006; Kirkbride et al., 2006). Studies also found an elevation among non-Western immigrant populations, such as people from Morocco, Suriname, and the Dutch Antilles (Veling et al., 2006, 2008), and White immigrants to Sweden (Hjern et al., 2004). Other studies in the United Kingdom looking at racial disparities revealed a pattern consistent with social and environmental mechanisms—the risk of schizophrenia was greater in second-generation compared to first-generation immigrants (Cantor-Graae and Selten, 2005) and also found that those living in their countries of origin were not at increased risk for psychosis and schizophrenia compared to those who had emigrated (Bhugra, 2006; Sharpley et al., 2001). A World Health Organization study also found no evidence of elevated neurodevelopmental or familial risk factors and exposures in people who experience psychosis (WHO World Mental Health Survey Consortium, 2004). These studies, said Anglin, highlighted a range of potential social mechanisms involved in psychosis.
Anglin noted the persistent relationship between ethnic and racial group and schizophrenia in the United States. A recent meta-analysis found that Black individuals are 2.4 times more likely than White individuals to receive a diagnosis of schizophrenia (Olbert et al., 2018), a comprehensive literature review found that Black and Latino/a individuals are disproportionately overrepresented in the patient population with psychosis (Schwartz and Blankenship, 2014). The results of a study exploring the relationship between ethnicity and diagnosis using a national database of serious mental illness in veterans confirms continued ethnic disparities in diagnostic patterns (Blow et al., 2004) and a birth cohort study found a two- to threefold increase in psychosis among Black individuals compared
to White individuals, although accounting for all sociodemographic factors attenuated this disparity (Bresnahan et al., 2007). More recently, a study of more than 300,000 people in the All of Us Research Program13 found increased odds for experiencing psychosis for Black individuals compared to White individuals, while multiracial individuals had even higher odds (Barr et al., 2022).
Anglin noted that one explanation for these findings is bias among clinicians and misdiagnosis that underemphasizes depression and overemphasizes psychosis (Adebimpe, 1981; Gara et al., 2012, 2019; Mukherjee et al., 1983; Strakowski et al., 2003). One U.S. study, for example, found that Black individuals at outpatient clinics reported having depression to the same degree as White individuals but were more likely to receive a schizophrenia diagnosis.
Anglin noted that current U.S. studies are focused on subclinical experiences of the type that McGorry discussed. One study, for example, found that the median prevalence of subclinical psychosis was 7.2 percent (Linscott and van Os, 2013), and a study of high-risk individuals found some differences among Asian and Pacific Islander and Black individuals compared to White individuals in conversion to psychosis among those identified as high risk (Brucato et al., 2017). Numerous studies have also found racial disparities in experiences and symptoms (Anglin et al., 2021; Calkins et al., 2014; Cohen and Marino, 2013; Karcher and Barch, 2021).
To tease apart the factors that contribute to these ethnic and racial disparities, Anglin has been examining the role that different types of discriminatory experiences might play. One finding has been that racial microaggressions14 and major discriminatory events, independent of one another, can explain ethnic and racial differences in psychotic experiences (Anglin and Lui, 2021). Another group of investigators examined these disparities through an intersectional15 lens and identified clusters that had the most difficult pathways to access care from the time they first experienced psychosis (van der Ven et al., 2022). Anglin noted that one cluster included Asian and Latinx individuals who had depression, suicidality, and psychotic symptoms. Another cluster comprised predominantly of Black individuals with many structural disadvantages, such as homelessness or interaction
___________________
13 See https://allofus.nih.gov/ (accessed October 18, 2022).
14 A microaggression is defined as “a comment or action that subtly and often unconsciously or unintentionally expresses a prejudiced attitude toward a member of a marginalized group (such as a racial minority).” https://www.merriam-webster.com/dictionary/microaggression (accessed October 4, 2022).
15 Intersectionality is defined as “the complex, cumulative way in which the effects of multiple forms of discrimination (such as racism, sexism, and classism) combine, overlap, or intersect, especially in the experiences of marginalized individuals or groups.” https://www.merriam-webster.com/dictionary/intersectionality (accessed October 4, 2022).
with the police in terms of how they got into the system. These clusters, said Anglin, were predictive of a tougher or longer path to access care than any ethnic or racial group alone.
Neighborhood ethnic density is another potential factor that researchers are examining. Anglin found, for example, that people of color living in neighborhoods where they were the ethnic minority had a higher incidence of psychotic experiences (Anglin et al., 2020). Other studies have generated comparable findings (Das-Munshi et al., 2012; Kirkbride et al., 2007; Veling et al., 2008; Zammit et al., 2010). To better understand the role of neighborhood, social determinants, and racism has on ethnicity and diagnoses, Anglin and her collaborators examined well-being among young Black people with first episode psychosis through a different lens. Anglin and her collaborators are trying to understand the role of neighborhood, social determinants, and racism in well-being among young Black people with a first episode of psychosis. They developed a photo voice project called “Black Photos Speak,” which involves people taking pictures of things in their neighborhoods based on different prompts, such as “How does racism show up for you, and how does it affect your well-being and your neighborhood?”
As an example, Anglin displayed a picture of a city street sign with parking information—2-hour parking on these days and no parking on another day—and another homemade sign that read “Stop Killing Black People.” The young person who took this photo explained that the sign was a trigger because it served as a stark reminder that their life could be put in danger for no reason. They also noted there was more to Black people than violence and wondered why the sign did not say that Black people are funny or smart. Anglin noted that this approach is one way to hear the voices of the people in the community—the specific population that programs are trying to reach.
Anglin said that the contribution of structural racism to the social patterning of psychosis risk remains a neglected area of study in the United States and needs to be more of a focus for funding priorities, training, and thinking about how to incorporate more social and environmental factors into research to improve public health overall. Investigators should also study the intersection of other social locations with ethnic and racial groups. Anglin reiterated that in addition to structural factors, neighborhood cultural and social context are important factors for risk and resilience.
Online Screening for Mental Health
Theresa Nguyen, chief program officer and vice president of research and innovation at Mental Health America (MHA), said that her organization has been advocating for mental health screening of children since 1913. In 2014,
MHA launched a mental health screening website (mhascreening.org). At the beginning of the program, several thousand young people would complete the screen per week. Visitors to the website have completed an average of 5 million screens a year and more than 14 million screens since 2014.16
Nguyen pointed out that MHAScreening.org reflects the experiences of a help-seeking population. People who take an online screening provide demographic data voluntarily, so not everyone answers every question and 20 percent do not answer any questions. The demographic data that MHA has been able to collect reveals that 70 percent of the users are female, 45 percent are under age 18, and 49 percent identify as a member of a racial or ethnic minority. More users screen for depression than any other condition. Nguyen also noted that although users skew female and young, these data are consistent with demographic data trends from the U.S. Census Bureau’s Pulse Survey and surveys of the Centers for Disease Control and Prevention (CDC), also consistent with trends seen related to the COVID-19 pandemic (Cai et al., 2021).17
Nguyen explained that when people hear about online screening, they typically think that young people are not actually struggling with mental health issues and are just exploring what it means to do so early in life. For example, the online venue is unlike taking the Patient Health Questionnaire 9 (PHQ-9)18 screen for depression in a doctor’s office, which is a one-and-done experience. “Young people come ….and they play with the screen in a different way than you would in a clinical context,” said Nguyen, “but that does not mean that our young people are not struggling.”
Nguyen said that MHA launched the brief prodromal questionnaire (PQ-B) to screen for ultra-high-risk of psychosis in 2015, and the number of people taking it increased from 11,198 in 2015 to 454,142 in 2021. The 2021 total includes a significant number of international screens for the first time. She added that 191,300 people took the PQ-B screen between January through May of 2022. The PQ-B has 21 items, with a score of six positive symptoms signaling a risk for psychosis (Loewy et al., 2011). The median number of items endorsed by users was 12. When an individual endorses a symptom, they then rate the degree to which they experience distress. The median score for all people who have taken this screen is 43, but the median score for young people is 52, indicating that the young people taking the screen are having numerous and diverse symptom experiences. Nguyen
___________________
16 See https://screening.mhanational.org/screening-tools/ (accessed October 4, 2022).
17 See https://mhanational.org/mental-health-and-covid-19-what-mha-screening-data-tells-us-about-impact-pandemic (accessed November 1, 2022).
18 The PHQ-9 is a self-administered screening tool comprising nine questions that assess the severity of depressive symptoms.
and her colleagues are learning about the challenges the younger population faces in terms of trying to find resources for the first time after getting these results online. Nguyen pointed out that resources in the community are inadequate to support all the individuals who are suffering.
A significant change in the data includes the number of youths struggling increased during the COVID-19 pandemic, consistent across all online mental health screens, Nguyen observed. Those who scored at risk for psychosis jumped from 66 percent in 2020 to 76 percent in 2021. She explained that it is difficult to uncouple the effects of the pandemic from her organization’s outreach efforts to publicize the website, but in her view, this is a sign of the elevated level of stress that put individuals at higher risk of scoring positive. “What does this mean about the duration of untreated psychosis, or the likelihood that a young person might experience their first episode as a result of stress related to COVID?” she asked. This number has not decreased since then, similar to the trends seen with suicide or global transdiagnostic mental health conditions resulting from stress, she added.
Nguyen said it is not surprising that youth experiencing psychosis retake the screen repeatedly, given that people who are hearing voices and experiencing paranoia have feelings of fear and ambivalence that will drive them to try to make sense of their illness and learn more. MHA’s research has found that encouraging young people with psychosis to seek care quickly has not resulted in increased use of treatment, because they either are not ready to receive care or have negative experiences in treatment. “For us, this is a critical period where we want to make sure that what we are providing to young people matches what their concerns are and what their needs are,” said Nguyen, “but we also know that our young people are not just taking the psychosis screen. They are taking anxiety screens, they are experiencing depression, and they are experiencing incredible trauma.”
When Nguyen and her colleagues asked young people to think about the key factors contributing to their mental health problems, they report that depression, anxiety, intrusive thoughts, post-traumatic stress disorder (PTSD), and obsessive-compulsive disorder are major drivers. They are young, but they have the insight to know that something is going on; they are trying to wrestle with the possibilities given that it is unclear who will have a diagnosis of schizophrenia versus bipolar disorder versus complex PTSD. Nguyen said that there is little understanding of how acute PTSD affects psychotic disorders or how to help educate young people to make sense of what is happening and reduce the fear they have of talking to somebody about their experiences. “The biggest challenge is that fear of what it means to disclose your illness to someone who may or may not be a trusted adult,” she said.
Nguyen shared that MHA has accumulated enough data to map its findings at the county level (see Figure 1).19 MHA updates the map quarterly, with the plan to add more demographic data to assist with planning where resources are needed and addressing clinic closures (which increase online services use). Nguyen hopes to use the map, in collaboration with MHA’s local affiliates, to gain insights into how stress from local current events affects risk for psychosis.
Nguyen observed, “If we are going to move the needle on early identification and intervention, you have to go where young people are, which means for us as a system, we have to be savvier in the way that we think about using digital tools and how we create them in a way that is engaging and allows young people to learn.” One challenge to explore with digital tools, she added, is how to measure clinical outcome, as the window of interaction in use of digital supports is not months long and may be as short as a single 5-minute session.
Nguyen noted that 30 percent of young people say they do not want to do anything after taking the screen, but they do want to learn what the results mean for their life. For Nguyen, that is a clear indication that research needs to determine how learning can help an individual feel
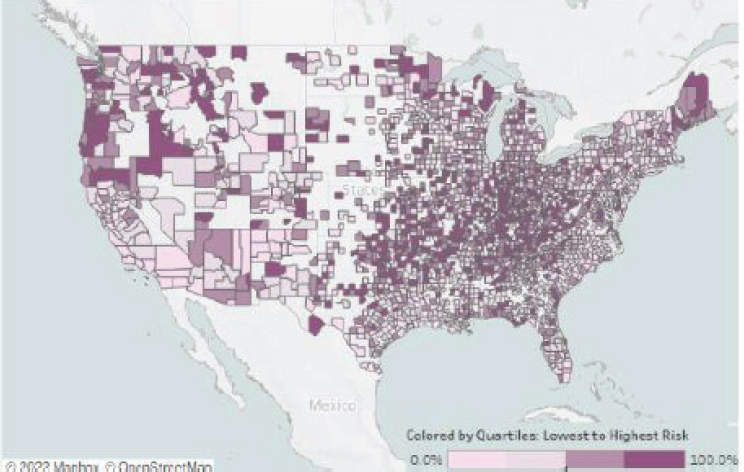
SOURCE: Presented by Theresa Nguyen on July 11, 2022.
___________________
19 See https://mhanational.org/mhamapping/mha-state-county-data (accessed November 13, 2022).
empowered, brave, and able to seek care and overcome individual, family, and community barriers to care. Nguyen noted that she agreed with Anglin that psychosis is historically underserved, particularly among young people who are multiracial, Native American, or LGBTQIA+. “We are particularly concerned about looking at subpopulations and how we can do targeted support for those communities,” she concluded.
Discussion
Alana Kirby, assistant professor at Rush University Medical Center, asked Nguyen about the increasing scores MHA captured since the start of the pandemic or other data that might help identify a direct effect of COVID-19 on the high-risk population. Nguyen replied that these data have untapped potential, and MHA has a portal for researchers who want to mine the data for that kind of connection, but no researcher has yet approached her to take a deeper dive relating to COVID-19. However, she and her colleagues have heard from staff at CDC, NIMH, and SAMHSA who are concerned about COVID-related psychosis. Nguyen noted that all the mental health screens revealed an increase in risk during 2020 and that those numbers are still elevated.
Anglin added that she and her collaborators are conducting a study in the Bronx, NY, a community that suffered a great deal of trauma during the pandemic and has seen more young people scoring higher on the PQ-B screen. She did not anticipate that finding because this study is looking at all adolescents, not only those who have had psychotic experiences. This makes her wonder whether the environmental impact of COVID-19, combined with the pandemic-imposed isolation and the stressors they report, is playing a role in the increase in symptoms. Nguyen added that she sees a great deal of trauma and distress among young people, and it is not known what this will mean for them and their brains at such a critical stage of development.
Dost Öngür, chief of McLean Hospital’s Psychotic Disorders Division, asked whether a more troubled society will mean more psychotic disorders and, given the lead time for the emergence of these conditions, whether the burden of mental illness, and particularly severe mental illness, will be higher in the coming decades. If so, he noted, it has implications for building treatment facilities, training clinicians, and preparing society for what is to come. Anglin replied that people in the community have been asking her whether the incidence of psychosis will be higher and whether this can be prevented, given what is known about the stressors involved. She wondered whether making screening less stigmatizing should be a priority, since the screening process itself can cause stress and trauma. She asked whether CSC programs might be a place to accomplish that and whether there should be a lower the age limit for providing support.
Nguyen said that she is absolutely concerned about the increased trauma to young people, including from online exposure to information that earlier generations did not have access to. “We do not understand what that means for a developing brain,” she said. She added that early psychosis is connected in some manner to puberty, and she hopes that MHA’s data can help elucidate what the developmental impact will be across the lifespan. She plans to examine the data to see how MHA’s numbers compare to the age at which young people are seeking help, either online or in clinics, and whether that reveals any information about the duration of untreated psychosis.
Nguyen said that it is also important to reduce the fear and shame associated with psychosis, and to provide hope to patients; “giving a person a sense of hope for the future is so profound.” As a mental health advocate and someone living with a mental illness, Nguyen said she believes that this type of connection and reassuring messages can be as powerful as medication in many ways for reducing symptoms. “This is where engaging with patients and community participatory research helps reorient ourselves to what matters for young people as they are recovering,” she said. She said it is important to recognize the value of education and teaching young people how to manage psychosis as a chronic condition. However, she added that more research is needed because “We do not know enough about best practices in education and management of chronic illness over time, especially when you think about combining that with messages of hope and recovery.”
On a final note, Anglin said that researchers are trying to understand what happens when a person becomes uncomfortable, drops out of a program at a community center, and does not follow up with their care. To address those situations, she said strategies are needed to create a more psychosis-friendly environment in community centers that see people with trauma and other issues.
CURRENT MODELS OF CARE
Team-Based Model for Collaborative Care
Carol Ott, clinical professor of pharmacy practice at Purdue University’s College of Pharmacy and clinical pharmacy specialist at Sandra Eskenazi Mental Health Center and Prevention and Recovery Center (PARC) clinic, began by explaining that in 2009, two psychiatrists, a nurse, and a case manager/therapist asked her to join the clinic, which they were launching to provide team-based care for early psychosis. Its parent organization, Eskenazi Health, is affiliated with the Indiana University School of Medicine (IUSM) and Purdue College of Pharmacy, and the clinic serves as a training ground for psychiatry, pharmacy, social work, nursing, and
therapy students. The staff includes a psychologist, several therapists, case managers who support education, employment specialists, a nurse, and Ott as the clinical pharmacist.
Ott pointed out that this model differs from other early-psychosis clinics in that a board-certified psychiatric pharmacist is part of the team. Including Ott required the clinic to develop a collaborative practice agreement, which was required by Indiana’s state pharmacy board (other states may have different requirements). This agreement allows Ott to provide per-protocol medication management, which means that she can receive a referral for a mental health assessment, medication initiation or discontinuation, dose adjustments, laboratory monitoring, medication refills, and assessments for medication effectiveness and side effects. Ott consults with the clinic’s nurse and psychiatrists before authorizing medication. She added that her ability to provide patient consultations around medication can create more time for psychiatrists to provide other services.
The PARC clinic has launched several health initiatives. Fit Happens, its metabolic monitoring program, includes weight management along with blood glucose, cholesterol, and blood pressure monitoring. Ott said that these assessments are identifying health issues in younger patients, which allows the clinic to intervene with treatment. For example, the clinic’s protocol includes recommendations for blood pressure medications and statins that the team can initiate, which triggers a referral to primary care. The clinic also refers patients to dietitians and health coaches, in addition to offering wellness education. Another initiative—the Healthy Me Eskenazi specialty clinic—helps patients with metabolic conditions, which are common among patients treated for psychosis.
PARC has also started an initiative to evaluate all the Sandra Eskenazi Mental Health Centers’ processes for addressing women’s health. Ott explained that her team examines the medications the clinics use; provides any needed harm reduction, including initiation of pre-exposure prophylaxis therapy to prevent HIV infection and follow-up; offers pregnancy testing and planning, referrals for annual exams, and contraception; and evaluates vitamin D and folic acid levels. Ott said that the care team tries to have a conversation with pregnant clients about the medications they take to ensure that they continue with these during pregnancy.
Ott said that she can make referrals for services outside of her scope of practice. For example, she can refer a patient to a dietitian if she identifies someone who needs the Healthy Me program, and she can refer to a weight management specialist, who could be an outpatient ambulatory care clinical pharmacist to evaluate weight management in an outpatient clinic. Other referral options include primary care, obstetrics/gynecology, and occupational therapy.
Ott and her colleagues have the opportunity to conduct research with pharmacy residents at Eskenazi and the Purdue College of Pharmacy. One study, for example, compared treatment adherence and persistence among the clinic’s clients with early psychosis for long-acting injections versus oral medications (Titus-Lay et al., 2018). Another study monitored and treated metabolic conditions in clients with early psychosis on antipsychotic medications (Bozymski et al., 2018). The clinic team also participates in many research projects with IUSM.
Turning to policy-related work, Ott noted that in 2005, the Indiana legislature passed the House Enrolled Act 132520 that allowed for open access to mental health medications, including all FDA-approved drugs with a mental health indication and all dosage forms. That bill also created a mental health quality advisory committee, which Ott was appointed to in 2005 and on which she still serves. This committee evaluates antipsychotics, antidepressants, anxiolytics, and cross-indication medications, such as valproate or carbamazepine, which have mental health indications as well as their use to control seizures. The committee sets prior authorization criteria based on clinically appropriate use of these medications; when it began, it focused on practices that should not happen, such as prescribing two selective serotonin reuptake inhibitors or two benzodiazepines for the same patient. Seventeen years later, Ott trains Indiana University psychiatry residents in this open-access model for Indiana Medicaid, something other states may not allow.
Ott shared that the committee has considered how the antipsychotic clozapine fits in with other antipsychotic medications and has set a prior authorization criterion that results in a clinician receiving a questionnaire when they prescribe a second oral antipsychotic instead of clozapine for a beneficiary of Indiana Medicaid. The questionnaire asks the clinician to explain why they have not tried clozapine and why it would not be appropriate. The answer, said Ott, cannot be that the clinician feels uncomfortable prescribing it. If so, then Ott has a discussion with the clinician to address their concerns. Acceptable answers include the patient has a needle phobia due to the regular blood draws when people are on clozapine, is unable to come in for the monitoring required, or is affected by social determinants of health.
Ott discussed the benefits of medical management by a pharmacist. Pharmacists, she said, think differently than other clinicians. “We think in terms of receptor pharmacology, dosing side effects, and how medications fit together,” she explained. When she has a patient who is experiencing
___________________
20House Enrolled Act No. 1325, Public Law 101, 114th Indiana General Assembly, 1st sess. (April 26, 2005), http://archive.iga.in.gov/2005/bills/HE/HE1325.1.html (accessed October 18, 2022).
side effects, for example, she will examine whether those effects result from a combination of medications or one specific medication. She will also consider how to optimize the medication regimen to minimize or eliminate the side effects. Pharmacists can also order laboratory monitoring, assess medication adherence, and even discuss challenges with the patient to understand why they are having a hard time adhering to their medication regimen.
New Journeys Program of Washington State and Pathways to Care
Oladunni Oluwoye, assistant professor in the Department of Community and Behavioral Health at Washington State University’s Elson S. Floyd College of Medicine, noted that discussions about the CSC model typically address the different core components, such as individual psychotherapy, family psychoeducation, case management, and medication management, but rarely consider the structures and supports that CSC programs need to be successful. New Journeys, the CSC program of Washington State, is supported by an evaluation and measurement team at Washington State University, which trains clinicians on how to use measures to inform care and monitors data quality in the program. It is also supported by an implementation team that offers training on how to deliver the individual components of the program, and a health care authority that provides oversight and money to the different components.
New Journeys has a comprehensive assessment, comprising a battery of measures that it uses with clients and families (Oluwoye et al., 2020). The measures allow the program to provide data-informed, person-centered care planning and treatment. Beginning with one site in 2015, New Journeys has expanded to 12 sites, but the majority of the sites are in the western part of the state, leaving clear gaps in other areas. The state has made a concerted effort to work with counties to identify other options to provide services in those areas without a nearby CSC program. Oluwoye and her colleagues have examined areas with disparities in access to care to inform efforts to provide resources to rural communities. She noted that the spatial distribution of services contributes to referral decisions and treatment delays, which, as previous speakers pointed out, can have consequences for the duration of untreated psychosis (Oluwoye et al., 2022a).
Approximately 50 percent of referrals to the program, said Oluwoye, come from mental health care providers. Family members account for 20 percent, medical care providers 11 percent, inpatient units 7 percent, and schools, the justice system, faith-based organizations, community centers, friends, and other sources account for the remaining 12 percent. The
program has limited funds for community-based outreach, which limits the pathways to care for some populations.
Oluwoye explained that Black and Latinx individuals are significantly less likely to use outpatient mental health services compared to non-Hispanic White individuals experiencing their first episode of psychosis (Heun-Johnson et al., 2021). They are also more likely to have used emergency services, such as the emergency department, in the year prior to the onset of psychosis. Black individuals are up to five times more likely to receive a diagnosis of schizophrenia spectrum disorder, which Anglin referred to as overdiagnosis. In addition, Black individuals’ experiences of racism and discrimination contribute to mistrust of the medical system, disengagement, and delays in and lack of treatment (Oluwoye et al., 2021).
Oluwoye encouraged attendees to think about ways to approach inequities in care. Much of her and her colleagues’ research focuses on downstream factors, such as treatment preferences, insurance coverage, family dynamics, and family engagement in services (see Figure 2). She would like to see more work on upstream factors and how they contribute to disparities in treatment and equitable access to services, and she wondered about the best way to use resources already established in certain communities to deliver treatment or get individuals to coordinated care programs (Anglin et al., 2020). Other areas that need more study with regard to disparities in access and care include the role of structural discrimination, which has been hard to capture in clinical studies, and health care policies.
Oluwoye identified a number of areas of improvement, including implementing multilevel interventions that truly include the community, are centered on community, and focus on using community resources, not only
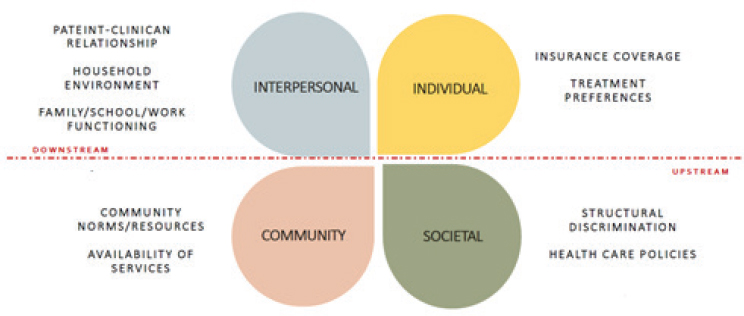
SOURCE: Presented by Oladunni Oluwoye on July 11, 2022.
for CSC but also to improve the pathways to care more broadly. The goal is for individuals to have fewer negative experiences in seeking care so that they are more engaged in CSC when they get a referral. She also suggested focusing on the ways that implementation science can improve services and equitably increase these programs’ reach, improve the initial contact with the health care system, and improve navigation services and linkages between different parts of the system. She said research shows that engaging people in the first appointment in CSC increases the likelihood of sustained engagement through the treatment program (Oluwoye et al., 2022b).
Oluwoye also pointed out that disparities in access need to be considered when selecting locations for CSC clinics. Oluwoye underscored that screening should occur in other settings, such as schools and within the criminal justice system, but she also emphasized that getting needed care for people with early psychosis involves more than just screening. “We can screen people as much as we want, but if there are not enough places and coordinated specialty care programs, then we are creating another problem in and of itself,” concluded Oluwoye.
Strengths of CSC in California and Challenges to Growth
Tara Niendam, professor in psychiatry, vice chair for research, and executive director of the early-psychosis programs at UCD, noted that different models of CSC have been implemented across the country, but the original model, proposed in 2014 (Heinssen et al., 2014), centers the client within the team and includes five components: care management, medication/primary care, psychotherapy, family education and support, and supported employment and education. This model stands in contrast to standard community treatment, which comprised medication management, case management, and individual, group, and family therapy.
The team-based approach, explained Niendam, is probably the most important aspect of CSC. “This is not individual care providers, each in their own separate spaces; this is a team that comes together and that responds rapidly to the needs of the client and the family,” she said. In California, the teams work intensively with clients, peers, and family partners and on providing gold-standard assessment leading to individual, group, and family treatment, including for substance use disorders. That model provides supported education and medication management and community outreach and education. Teams include the voice of caregivers of someone with psychotic illness to provide the lived experience perspective.
Niendam said that one challenge in California is that health services are delivered by county, which means that funding is divided and different programs are implemented by counties. Thus, the state has no uniformity in early-psychosis services. Niendam and her colleagues are trying to use
a program called the California Collaborative Network to Promote Data-Driven Care and Improve Outcomes in Early Psychosis (EPI-CAL)21 to build statewide leadership and support for such programs and address that lack of uniformity. Counties use different models, serve different populations and age groups for different durations, and have different funding mechanisms. In addition, some state universities, including her institution, have commercial insurance–funded clinics.
Niendam observed that even with all the different programs and funding mechanisms, access to early-psychosis programs is still limited. Programs tend to be small, so they cannot reach the entire community, and funding is so limited in rural areas and other regions with low population density that those counties cannot start a program. In addition, the lack of a statewide approach to data collection has made it difficult to demonstrate the impact of these programs and bolster support for them. Niendam noted that funding from the National Institutes of Health (NIH) Early Psychosis Intervention Network (EPINET) has enabled her team to develop a statewide approach to data collection.22
Niendam explained that California’s programs consider the psychosis continuum, from people at-risk to those with full psychosis, and have moved away from a diagnostic-specific approach, which means that many programs serve both affective and nonaffective psychosis.23 At least three-quarters of the state’s programs serve both high-risk individuals and people with active psychosis. Niendam said she is encouraged that more programs are accepting people who previously have been excluded, including the increasing number of young people who develop psychosis after cannabis use and individuals with postpartum psychosis. “One of the strengths that we focused on here in California is this idea of looking at psychotic symptoms and serving and treating those symptoms, not focusing on particular diagnoses,” she said. This latter point is important, she said, because there is nothing worse than telling someone they are not eligible for the program because their diagnosis does not meet some criteria or because substance use triggered their psychosis. “That is devastating to the family or the young person,” she added. Being more inclusive and acknowledging that psychosis is a broad syndrome is an important piece of this work to consider.
___________________
21 See https://epical.ucdavis.edu/en/about-epi-cal.php (accessed September 19, 2022).
22 See https://nationalepinet.org/ (accessed October 4, 2022).
23 The National Association of State Mental Health Program Directors defines “affective psychosis” as a term used to describe symptoms of psychosis that are present with mood episodes and most typically involve bipolar disorders or major depressive disorder. The umbrella term “non-affective psychosis” refers to schizophrenia spectrum disorders such as schizophrenia, schizoaffective disorder, schizophreniform disorder, brief psychotic disorder, psychosis not otherwise specified, or delusional disorder.
California’s programs also take a strong developmental view, with some accepting children as young as 8. A population health approach requires centering programs on this developmental perspective, which affects both assessment and treatment, said Niendam. For assessment, one of the most important differentials the programs are making at intake is whether the individual has an autism spectrum disorder or some other neurodevelopmental disorder. “If you assume that it is just schizophrenia having an onset in adulthood, you are apt to miss those neurodevelopmental issues that are common in childhood,” she explained.
Niendam explained that 90 percent of program clients in California still live with their families, so they have to include families in care planning. “Their families are the safety network, the frontal lobe that helps these folks survive in our community, and so by excluding them, we are actually doing a disservice to our clients,” said Niendam. She also noted the importance of addressing social determinants of health and thinking about how to access food, housing, work, and transportation. Feeling safe in one’s community is an important factor in getting people to come to the clinic. Trauma is another important consideration because it is so common among the individuals these programs serve. “We definitely need to develop treatments that allow us to work with the trauma that people have experienced, because [that experience] often maintains or exacerbates the psychotic symptoms or other symptoms,” Niendam remarked.
Turning to the challenges of implementing CSC in California, Niendam began with the lack of stable and sufficient funding, something she acknowledged is a problem many programs face. As both Nguyen and Oluwoye pointed out, the needs of the population are increasing, but the funds are not, which leaves programs trying to do more with limited resources. A related issue, explained Niendam, is that commercial insurance will pay for medication and psychotherapy but not the recovery-oriented services included in the model. In addition to making it difficult to build a program to serve the population in need, limited funding makes it difficult to recruit psychiatrists, psychologists, licensed social workers, and other highly skilled individuals to staff a team and to pay a competitive salary, particularly in rural areas.
In addition, there is a shortage of appropriately trained and diverse care providers and significant staff turnover. Training is still focused on adults or children rather than taking a developmental perspective. Adult practitioners often are not oriented to recovery, systems, or family and often have negative views of psychosis based on seeing people with chronic illness in a hospital or incarceration setting, while youth practitioners often receive little training on serious mental illnesses. Having a diverse workforce is critical, in terms of being able to communicate in languages other than
English, and also to understand how to integrate culture and religion in the context of psychosis.
Another challenge involves partnering with the community to ensure steady and appropriate referrals. Insurance does not pay for outreach, yet these programs are expected and required to educate the community about psychosis so that when they see it, they will refer people to available programs. A strong historical focus on biology and medication does not always align with an individual’s experience or culture, which can create separation between the patient and staff. “I think an important task for us in this field as researchers and clinicians is to broaden our understanding of psychosis, its causes, its consequences, and what sort of treatments work best for whom, because I think the way we continue to approach things is often a turnoff to a lot of our families and clients,” observed Niendam. In addition, programs are often limited to a 2–3-year treatment plan—some only allow 1 year—that does not match a client’s needs or recovery trajectory, particularly for someone who has experienced a great deal of trauma or has a history of substance use, family and housing instability, or a parent with a mental health history. Niendam said the current model does not allow for that level of adjustment.
Niendam identified an additional challenge: the lack of step-down or transition care. Too often, young people return to community mental health care with medication and case management, usually in an adult system that sees their illness as chronic and debilitating with no hope for recovery. This is not a great space to move into after a supportive and hopeful environment.
Niendam’s suggestions for next steps included establishing stable and sufficient funding. Combining California census data and published incidence estimates (Radigan et al., 2019; Simon et al., 2017) suggests that the state needs 357 clinics serving 75 people a year to meet the demand for early-psychosis services—it can currently meet one-tenth of the demand. For too long, said Niendam, youth with early psychosis have been under-treated or untreated in typical community care, which leads to poor outcomes, including disability, death, homelessness, and incarceration (Popovic et al., 2014; Wander, 2020; Volavka and Citrome, 2008).
Addressing workforce issues is essential, she said, and that will require ongoing training, supervision, professional development, and a supporting infrastructure. Each state is tackling this challenge in its own way, which can be good given the state-by-state differences, but some of this work can be scaled at a national level, in Niendam’s view. Accreditation organizations can play an important role in ensuring that medical school and graduate school students have the training they need for psychosis care. Niendam said she often hears the argument that patient peers can address the workforce issues: “I love peers, and they are essential to our programs—they do
amazing work—but they are not sufficient, and they certainly should not be treated as frontline clinicians.”
Niendam suggested that this work be reframed along a biopsychosocial model. She said when she was trained and during the early part of her career treating individuals with psychosis, she focused on “brains, biology, and emotion.” Her work in these programs and in the community helped remind her that “heads are attached to bodies, and bodies exist in a community.” This means treating the whole person, acknowledging the role of social determinants and trauma, focusing on an individual’s goals for recovery, and allowing adequate time for each person to move through treatment at their pace. It also means enhancing natural supports and connections to family and community and addressing systemic issues that contribute to marginalization. “Our charge as scientists, as leading practitioners in the field, is to shift our model and our approach to this broader view and to challenge each other to do this so that we can hopefully make better strides, both in the science of psychosis and also in the development of treatment for psychosis,” concluded Niendam.
OnTrackNY
Lisa Dixon, professor of psychiatry and director of the Division of Behavioral Health Services and Policy Research at Columbia University Medical Center and director of the Center for Practice Innovation at the New York State Psychiatric Institute, explained that OnTrackNY24 is a mental health treatment program that empowers young people across the state to make meaning of their experiences and pursue their goals for school, work, and relationships. It does this by supporting the well-being of those who are impacted by unexpected changes in their thinking and perceptions. She noted that based on stakeholder feedback, the program does not use “psychosis” in its name and positioning statement but recently added equity, rapid access, and self-determination.
OnTrackNY has 14 locations in New York City, 2 in Buffalo, and 9 in areas with sufficient population density, which does leave some areas, such as the northeastern region, without a site. Using federal funds, the program plans to expand to 31 sites by 2023. Dixon noted that a key factor for sustainability has been the commitment of the New York Office of Mental Health to support the program’s teams and connect them to stakeholders, including regional leadership and field offices. The program acts as an intermediary between agencies and that office and bridges the gap between the state and agencies that deliver services. OnTrackNY supports evidence-based implementation of the Office of Mental Health’s model and provides
___________________
24https://ontrackny.org/ (accessed October 18, 2022).
technical assistance, oversight, and monitoring for the agencies as well as support for data collection activities. Dixon noted that the program is in the Office of the Medical Director with connections to adult and children’s services, which helps bridge the adult–child divide.
Turning to the details of the program, Dixon explained that eligibility is limited to individuals within 2 years of onset of non-affective psychosis, which is more specific than California’s program. OnTrackNY also deploys its resources in the post-help-seeking phase of care, develops strategies for care providers aimed at reducing the duration of untreated psychosis and funds, and monitors the outreach activities that it expects its teams to conduct. It works with Medicaid, managed care organizations, social media, and youth leaders for outreach activities.
Ongoing work to address gaps in the program’s “before treatment” phase includes expanding eligibility requirements in more rural and less populated areas to 5 years from onset and to include affective psychosis. To address equity and inclusion, OnTrackNY emphasizes presenting a diverse array of individual and family stories on its website in its messaging to support engagement and address stigma. Based on stakeholder input, it has developed more online materials that use individual stories to connect with potential clients and explain what the program is and what it can help them accomplish. It is also funding projects on pathways to care for Asian and Latinx participants, the prison population on Riker’s Island, and online strategies.
The treatment model follows the CSC approach (see Figure 3). Peer support, said Dixon, touches all individual treatment components, as do outreach and engagement to counter patient ambivalence, and shared decision making ties the elements together. Each team has at least 4.5 full-time equivalent staff and serves 40–50 participants; teams with more participants have additional staff.
In the “during-treatment” phase, efforts to address gaps include revising training to include a focus on racial equality, structural competence, and cultural humility. During the pandemic, Dixon explained, the program shifted to some online and asynchronous training components to deal with massive staff turnover, and it is continuing to use telehealth even as the pandemic moves into a less dangerous phase. She noted that OnTrackNY is creating a CSC designation process for payment purposes, and the state is working on a per-person bundled rate payment strategy. Data collection involves both participant self-reports and clinician-generated data, and the program is developing data dashboards as part of an EPINET project to support the use of these data in quality improvement activities. Areas of focus in the during-treatment phase include reducing suicide risk, enhancing shared decision making for people of color and around prescribing, enhancing physical health, addressing aggression and violence, optimizing
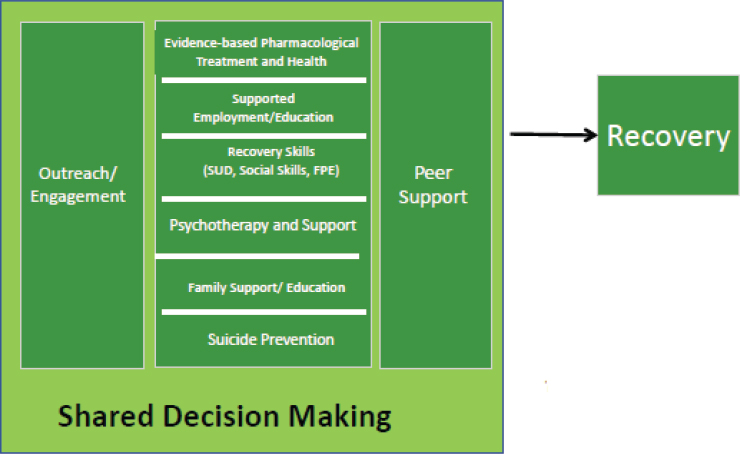
SOURCE: Presented by Lisa Dixon on July 11, 2022.
prescribing, and dealing with disability. Other efforts aim to enhance the program’s ability to engage people from marginalized communities.
In the “after-treatment phase,” Dixon said more work is needed on the duration of treatment and keeping individuals in the program. Each client’s primary clinician helps the participant and family prepare to transition out of the program by equipping them with knowledge about mental health care, developing a comprehensive plan, encouraging strong relationships with new treatment providers, and including families in all of these activities. That clinician also encourages participants to advocate for recovery-oriented services after transition. Dixon noted the limited availability of recovery-oriented, flexible youth- and family-oriented services that use shared decision making, and of supported education, employment, peer support, and family-based services.
Dixon stressed that workforce shortages lead to increased wait times, even in a state committed to providing these types of services. Potential solutions include creating step-down units that would provide an intermediate level of care between the program and community-level care through certified community behavioral health clinics. OnTrackNY also has projects focused on the role of family navigators and the potential use of Horyzons, an online social support intervention for discharged patients (Alvarez-Jimenez et al., 2019). Dixon characterized OnTrackNY as a well-specified but flexible model consistent with CSC.
Discussion
Session moderator Kathy Pham, director of policy and professional affairs at the American College of Clinical Pharmacy, asked the panelists to share ideas on potential billing or funding opportunities that might enhance the care models they discussed. Ott addressed a potential billing opportunity by describing how having clinical pharmacists embedded throughout the PARC clinic recognizes pharmacists as care providers, which would allow them to bill insurance companies for their services. Some state Medicaid plans allow this, but Indiana does not. She said that sustainable funding and being able to access more federal funds would help broaden what her program could do in Indiana.
Niendam noted that California has been considering case-based rates for commercial insurance that might help people with insurance to access this type of care. California’s Medicaid programs, she said, have been more open to paying for services from trainees or people with other credentials. The challenge is for commercial insurance to pay for more than a psychiatrist or licensed clinician (e.g., psychologist) and include coverage to support education, peer and family services, and recovery-oriented services. Another challenge, said Niendam, is adjusting payment for different levels of care when people are ready to transition out of a program.
Oluwoye said she would like to see funding for outreach activities that help educate individuals about psychosis. She said that clinicians are not paid for the work they are expected to perform in the community, which may contribute to high staff turnover. Dixon noted that a team-based care model will not be fundable through individual billing, adding that an ideal payment strategy would be based on case-rate payments.
Howard Goldman, professor of psychiatry at the University of Maryland, School of Medicine, noted that several online participants had asked whether Medicaid’s coverage exclusion for institutions for mental disease25 would affect CSC financing. Goldman explained that CSC is an ambulatory care (versus 24-hour) service, so that exclusion would not apply.
Niendam observed that in California, young adults will drop from their parents’ commercial insurance and enroll in California’s Medicaid plan just so they can access CSC programs. That, however, is not how the system should work, she stressed. “We should be having these insurance companies provide appropriate care,” she said, just as they do for cancer care.
Anita Everett, director of the Center for Mental Health Services at SAMHSA (the federal agency that administers the mental health block grant set-aside for first-episode psychosis programs), asked the panelists
___________________
25 States are prohibited from using Medicaid funds for care provided in institutions for mental disease (psychiatric hospitals or other residential treatment facilities with more than 16 beds) (Maclean et al., 2021).
to talk about exclusion criteria for these programs. Dixon, who had noted that her program excluded individuals with affective psychosis, said that narrow inclusion criteria have not diminished enrollment because demand for services still exceeds supply. She explained that the state has limited resources and decided to devote those resources to programs with the greatest evidence of a differential benefit (non-affective psychosis).
Nev Jones, assistant professor at the University of Pittsburgh, asked the panelists to comment on the challenge of balancing prevention and intervention for serious mental illness and providing funding for programs that reach individuals at high risk versus only treating individuals with first-episode psychosis. Niendam replied that adding high-risk people to the population her program treats would triple the demand for already-limited services, which makes this a funding policy question. Niendam suggested a solution would be to take a population health approach and think about how to build a system that serves people appropriately at each level of symptomology. Otherwise, programs are forced to make choices that limit their ability to meet the demand.
EVIDENCE ON SHORT- AND LONG-TERM OUTCOMES
Five-Year Outcome Data from the RAISE Early Treatment Program
John Kane, professor of psychiatry at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, discussed the 5-year results from the NIMH RAISE study, a multicenter, randomized, controlled trial (Robinson et al., 2022)26 that aims to develop a comprehensive and integrated intervention to promote recovery, minimize disability, and maximize functioning, which can be delivered in real-world settings using current funding mechanisms. The study recruited 404 patients experiencing first-episode psychosis at 34 clinics in 21 states and used cluster randomization27 to provide either the NAVIGATE28 CSC intervention or usual community care. Inclusion criteria included being 15–40 years old, having a DSM-IV diagnosis of a schizophrenia spectrum disorder or first-episode psychosis, and an antipsychotic medication lifetime history of less than 6 months. Most enrollees had fewer than 2 months of medication and one prior hospitalization. On average, they were 23 years old, male, and White, with the majority not working or going to school at baseline (Kane et al., 2016).
___________________
26 See https://www.nimh.nih.gov/health/topics/schizophrenia/raise (accessed September 19, 2022).
27 Cluster randomization are used to compare interventions that are allocated to entire groups of subjects.
28 See https://navigateconsultants.org/ (accessed September 19, 2022).
Kane reported that the first results from U.S. nonacademic community treatment settings found the average duration of untreated psychosis was a “shocking” 74 weeks, with 68 percent of participants waiting more than 6 months (Addington et al., 2015). Factors that correlated with a longer duration were earlier age at first symptoms, substance use disorder, symptom severity, poorer functioning, and referral from outpatient settings. Kane explained that 56 percent of these individuals already had dyslipidemia—unhealthy blood levels of one or more kinds of lipids that is a common side effect of antipsychotics—even though they had been treated with antipsychotic drugs for only 1.5 months. Half were smokers and had received little treatment for smoking cessation, and the incidence of prediabetes and diabetes—also common side-effects—was also high for the age of this population.
One NAVIGATE component included psychopharmacology, and Kane and his collaborators developed computerized decision support system for the prescribers. Other components were measurement-based treatment; family treatment, including psychoeducation; individual resiliency training, supported employment, and supported education (see Figure 4). The primary outcome measure was the Heinrichs-Carpenter Quality of Life Scale (QLS) (Heinrichs et al., 1984), which covers sense of purpose, motivation, emotional and social interaction, role functioning, and engagement in regular activities. Secondary measures included the Positive and Negative Syndrome Scale (PANSS) scores for symptoms severity and the Calgary Depressions Scale for Schizophrenia, service use, and participant self-report measures.
Kane pointed out that NAVIGATE had a significant advantage for QLS scores, though the duration without treatment played a role; patients who waited longer than 74 weeks for treatment were significantly less likely to benefit from CSC. Individuals receiving CSC also had less severe psychotic and depressive symptoms compared to the control group and more gains in working or going to school (Kane et al., 2016). Individuals in NAVIGATE were also more likely to receive a prescription medication that conformed to treatment guidelines and to experience fewer side effects. Kane emphasized that these results demonstrated that it was possible to implement a CSC model in a diverse range of community clinics and such programs could improve quality of life for patients with a first episode of psychosis.
Kane shared that he was most disappointed that hospitalization rates did not differ significantly between the experimental and control groups, with one-third of patients having a hospital admission over the subsequent 2 years (Kane et al., 2016). He said that there is debate about the significance of relapse, with some arguing that relapses can vary enormously in severity and impact, but hospitalization is an outcome to avoid for many reasons. Factors that contributed to the incidence of hospitalization
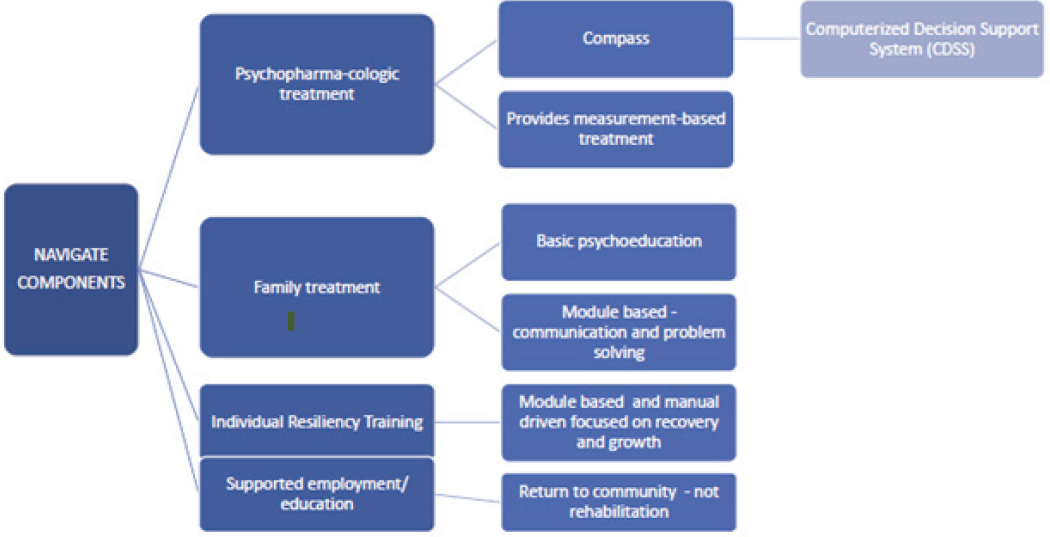
SOURCE: Presented by John Michael Kane on July 11, 2022.
included duration of untreated psychosis, days of substance use, positive symptoms on the PANSS measure, and answers to three questions about patient attitudes toward medications for schizophrenia. “We believe from this and from many other studies that adherence in medication taking is a critical factor when we talk about outcomes,” observed Kane.
Kane and his collaborators conducted a meta-analysis that compared outcomes from 10 studies conducted worldwide and involving more than 2,000 patients (Correll et al., 2018). Kane noted that all the measures, including hospitalizations, were better for early-intervention services compared to usual care. However, 32 percent of the individuals receiving early intervention services had at least one hospitalization over the next 16 months, similar to the results from the RAISE trial. Kane emphasized that “even with state-of-the-art interventions, we are seeing one out of every three patients hospitalized within about a year and a half … we have to do a better job of controlling that.” He noted that the advantage regarding hospitalizations seen in the meta-analysis resulted from the comparison group doing even worse than the intervention group, whereas in the RAISE trial, the rate of hospitalization was similar in the control group.
Kane said he is a proponent of long-acting injectable medication formulations. He referred to a cluster-randomized study involving 39 U.S. community mental health centers that found 85 percent of patients in first-episode psychosis or early-phase treatment were willing to consider such a medication if it was presented in the right fashion and involved shared decision making to ensure understanding of the benefits and risks (Kane et al., 2020). Individuals receiving once-monthly injections were 44 percent less likely to be hospitalized, which translated into a need to treat seven patients to prevent one additional hospitalization. However, there is a lot of controversy surrounding long-acting medications, Kane stressed that “the notion that this is unacceptable to most patients in the early phase of schizophrenia is just not true in my opinion” and found that young people are willing to consider the use of long-acting formulation through patient education. “It has a lot to do with the training of the staff,” he added.
Kane said that over the 5 years of follow-up, QLS scores strongly favored NAVIGATE, as did PANSS scores and hospitalization rates. However, Kane pointed out that only 31 percent of patients were available for the 5-year follow-up, a problem that has bedeviled most long-term followup studies involving first-episode psychosis or schizophrenia (Robinson et al., 2022). Nonetheless, the data suggest a lasting benefit for quality of life and symptom outcomes with NAVIGATE during both the early-intervention services and post-treatment periods.
Kane observed that the finding of long-term benefit both during and after early intervention was in contrast with the findings of some earlier
European studies. Possible explanations include the different settings, that the RAISE trial used a longitudinal assessment model as opposed to the cross-sectional model in some of the other studies, and a different statistical methodology for “missing not at random” statistics.29 The RAISE trial did not use “missing not at random” because the patients in the community care sites who dropped out of treatment were more likely to be sicker and have a poorer quality of life, and the opposite was true for those patients who dropped out of the early intervention or CSC programs. Kane added that when the RAISE trial ended, clinics struggled to pay for team leadership, team-level activities, case management, and supported employment and education.
Kane emphasized that studies have now shown that CSC and early intervention services provide important benefits for those with early-phase schizophrenia, though the duration without treatment remains a target (Kane et al., 2016). However, that duration was a moderating factor in the 2-year but not 5-year outcomes. He reiterated that relapse and hospitalization rates should be reduced to the extent possible and that sustained program implementation can be a challenge.
Racial Analysis of Social Determinants of Psychosis: A Better Frame for Unmet Needs?
Sabrina Ereshefsky, a postdoctoral research scholar in the early-psychosis program at UCD, explained that the biopsychosocial model of psychosis expands on the bio-ecological model that Anglin discussed in the workshop’s first session by including the interactions of context and environmental factors with biological, psychological, and social factors that lead to various health and mental health outcomes. For example, a young Black person growing up in the United States would have various aspects of their environment, such as their teachers, school system, and systemic racism, that affect them differently from how they would affect a White individual.
Predominant models for the onset of psychosis include two-hit (Maynard et al., 2001), stress-vulnerability (Walker et al., 2013), and diathesis-stress (Walker and Diforio, 1997), said Ereshefsky. Each has a similar premise: psychosis develops from a combination of genetic or biological vulnerability, placing an individual at increased risk or creating a predisposition, but activation requires an interaction with stress. These models largely ignore the sociocultural environment and systemic factors that
___________________
29 When data are “missing not at random,” the fact that the data are missing is statistically related to the unobserved data, that is, the missingness is related to events or factors that are not measured by the researcher.
impact individuals over time. “We need to do a better job of understanding what drives psychosis and incorporate that into our work,” emphasized Ereshefsky.
Based on a review of the U.S. literature, a group of researchers, including Anglin and Ereshefsky, proposed a model that links systemic racism and psychosis (see Figure 5) (Anglin et al., 2021). Ereshefsky explained that systemic racism is not linked exclusively or uniquely to psychosis but does help shape the observed extended psychosis phenotype.30 As with other psychopathologies, varied adverse experiences contribute to the expression of distress, but what stress means and where it originates has not been a topic of much discussion.
Ereshefsky noted that the racial trauma is deeply rooted in the United States, due to pervasive systems of structural racism that have also shaped the historical and current practices of diagnosing and treating individuals with psychosis. Systemic racism and social environments are fundamental causes of U.S. health inequity (Anglin et al., 2021; Churchwell et al., 2020; Gee and Ford, 2011). She pointed out that policy and social norms create pervasive nationwide inequities that directly and in concert with biological risk factors affect the onset, severity, and remission of psychopathology (Compton and Shim, 2015). Thus, race and ethnicity themselves are not the determinants—systemic racism and the social environments one falls in are the determinants (Anglin et al., 2021).
Ereshefsky observed that no representative studies adjust for race-based misdiagnosis and social disadvantage. She identified the factors that affect diagnostic accuracy, such as wealth inequities that lead to differential access to resources and health care, distrust of health systems and medical care providers arising from historical mistreatment of minorities, and a lack of appropriate clinician training on cultural competency and humility. The latter may lead clinicians to misinterpret spiritual or cultural experiences or healthy mistrust or hypervigilance in one’s community. This may lead to inappropriately pathologizing individuals’ experiences as delusions, clinical paranoia, or psychosis. Ereshefsky pointed out that it is not known how often clinicians misinterpret a minority individual’s symptoms to overdiagnose psychosis spectrum disorders and underdiagnose mood disorders (Anglin et al., 2021).
Adverse neighborhood conditions, Ereshefsky explained, confer disadvantage with cumulative stress and are conceivably linked to increased prevalence and severity of psychosis. Factors include social, economic, and political issues; formal and informal segregation; and institutional racism
___________________
30 An extended psychosis phenotype is a phenotype that shares demographic, environmental, familial, and psychopathological features and is both phenomenological and temporally continuous with clinical psychotic disorder (van Os and Reininghaus, 2018).
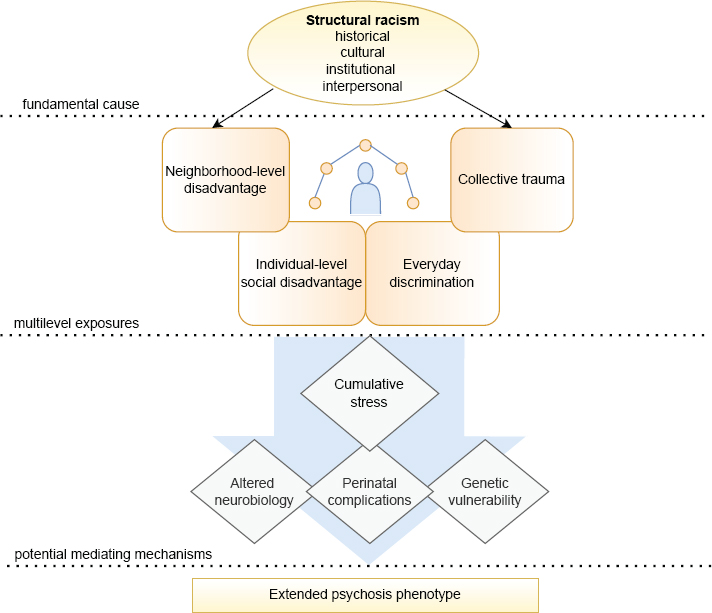
SOURCE: Presented by Sabrina Ereshefsky on July 11, 2022; Reprinted with permission from the American Journal of Psychiatry, Volume 178, Issue 7, “From Womb to Neighborhood: A Racial Analysis of Social Determinants of Psychosis in the United States,” Anglin et al. (Copyright © 2021). American Psychiatric Association. All Rights Reserved.
that together have evolved to perpetuate disadvantage—systemically and generationally—for minorities. Such factors also include lack of access to resources, opportunities, and services; urbanicity plus low socioeconomic status; discordant neighborhood ethnic density; neighborhood disorder and disruption; and housing instability. These factors combine to produce higher rates of psychosis through stressful racial dynamics, delays in diagnosis or receiving services, and earlier onset linked to a more severe course of symptoms (Anglin et al., 2021). “A better understanding of these factors will provide helpful context to early-psychosis programs,” said Ereshefsky. “It is essential we incorporate things like needs assessments and help clients and families meet their most basic needs so they may be ready for treatment.”
Ereshefsky explained that trauma and stressors are a common fact of U.S. life, with approximately 60 percent of the population and approximately 85 percent of those on the psychosis continuum reporting at least one adverse childhood experience (Anglin et al., 2021). Psychosis rates are also higher in individuals from minoritized backgrounds with trauma. Ereshefsky noted that once someone has experienced trauma, they are more likely to be revictimized—and with more exposure to trauma, psychosis frequency and severity also increases (Anglin et al., 2021).
Other important factors at the individual level include discrimination—when someone is “othered” or marginalized within the social hierarchy—police victimization, and exposure to gun violence and gun fatalities that disproportionately affect minoritized racial communities. Ereshefsky emphasized that police victimization and gun violence are unique collective traumas in this country. Communities have been intimately and vicariously affected, which has been found to be associated with psychotic experiences, she added. Ereshefsky stressed that these issues deserve greater attention regarding their roles in stress- and trauma-related social determinants of psychosis in the United States. For Ereshefsky, this requires incorporating a trauma-informed lens during assessment, conceptualization, and treatment; understanding how individual and collective trauma have affected families in different communities; and including other predictors of outcomes, such as child welfare, criminal justice involvement, and homelessness or housing instability (Hong et al., 2019).
Underlying or mediating the development of the expanded psychosis phenotype, Ereshefsky explained, is the exposure to cumulative stress and the biological consequences and mechanisms, including pre- and perinatal factors. Rates of such factors, such as obstetric or birth complications, are higher in racial minoritized populations, acculturated immigrants, and other groups experiencing discrimination in the United States. Within the frame of systemic racism, she noted, these complications likely develop as a result of an interaction with cumulative stress and repeated discrimina-
tory experiences, which increase when neighborhood factors are present. In pregnant individuals experiencing systemic racism, for example, stress biomarkers can look similar to those in people with PTSD, and cumulative stress can cause biological and genetic changes in the infant and can increase birth complications that can be linked to psychosis, explained Ereshefsky (Anglin et al., 2021).
Reduced access to prenatal care and income do not fully explain disparities in birth complications, according to Ereshefsky, nor does immigration status or ethnicity the longer one lives in the United States. “This is likely due to cumulative or intergenerational exposures to discrimination during the acculturation process,” said Ereshefsky. She noted there are consistent findings from studies that obstetric or prenatal complications are risk factors for psychosis (Davies et al., 2020; Ellman et al., 2018), but additional studies are needed to capture the relationship between racial and ethnic disparities in birth complications and to incorporate those findings into explanatory models for psychosis.
Ereshefsky additionally explained that discrimination, disproportionately impacting racial and ethnic minority individuals, is the common link to the aforementioned experiences and may lead to changes in biological mechanisms associated with the development of psychosis. Physiological and neurobiological changes that occur from trauma or other chronic activation of stress systems can alter brain development and increase neural activity or functional connectivity in certain brain regions.
Ereshefsky emphasized that discrimination affects other marginalized groups as well, including the LGBTQIA+ community, religious minorities, non-English-speaking individuals, poor and rural communities, and individuals with disabilities. These groups also suffer disproportional social determinants of health, and historically, they have also not been included in explanatory models of psychosis (Anglin et al., 2021). “We need to amplify different experiences and bring them into our work,” said Ereshefsky; “efforts are needed to increase cultural understanding on the societal level to help create environments where everyone can live with dignity, respect, and equity.”
She said it is essential to devote more effort to address and dismantle structural racism and social policies and norms via training and education, better integrating work on racial trauma in mental health training and practice, and understanding the social and economic conditions that shape these various factors and people’s lives. Training, said Ereshefsky, should include use of the free DSM-5 Cultural Formulation Interview,31 which can
___________________
31 See https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM5_Cultural-Formulation-Interview.pdf and https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM5_Cultural-Formulation-Interview-Supplementary-Modules.pdf (accessed October 18, 2022).
help with reasoning and decision making about symptoms, and supporting efforts to individualize treatments for minoritized individuals with different types of experiences and individual or collective traumas.
Ereshefsky also recommended optimizing and personalizing interventions by incorporating social determinants in early intervention and treatment models (Weisman de Mamani et al., 2014), testing multilevel and intergenerational approaches to early interventions using mixed methods and participatory methods, and adjusting health care policy to change the approach to early intervention of psychosis for minoritized populations. “We need research designed to provide reliable psychosis estimates for minorities, taking into account misdiagnosis, and we need multilevel targets and to fund community-partnered participatory research,” she said.
Ereshefsky said that a systemic racism frame may better describe the development of psychosis. Building a critical consciousness about the way behaviors and symptoms link to the context in which people live can enhance practice effectiveness, as well. “The disproportionate number of marginalized and disadvantaged people represented among individuals with psychosis in the United States may reflect how these traumas, discrimination, and neighborhood violence are influencing ability to receive adequate treatment and avoid traumatic pathways to and through care,” said Ereshefsky. “More research is necessary to fully understand the interplay between adversity, minority status, and other dynamic factors in U.S. communities and how the unique experiences of these groups influence psychotic experiences, illness development, access to care, and ability to recover,” she concluded.
State Mental Health Agency Support for CSC Programs and Use of the Federal Mental Health Block Grant 10 Percent Set-Aside
Ted Lutterman, senior director of government and commercial research at the National Association of State Mental Health Program Directors (NASMHPD) Research Institute (NRI), explained that the NRI and NASMHPD have been working with states for the past 9 years to document implementation of their funded early-psychosis programs, provide technical assistance and advice on policy issues, and assist in measuring and benchmarking data.
Lutterman also reminded workshop attendees that the national 9-8-8 emergency number for people with a behavioral health crisis would be going live in July 2022.32 Its launch, together with mobile crisis teams and state crisis stabilization programs, will help remove law enforcement from the response for people in crisis and reduce the trauma associated with
___________________
32 The 9-8-8 Suicide and Crisis Lifeline launched on July 16, 2022.
those events. He added that the 9-8-8 system provides an excellent opportunity for early identification and referral of individuals with psychosis. “We are trying to think how we can combine the work on 9-8-8 crisis services to get people better engaged and identified and into services sooner for early psychosis,” explained Lutterman.
Based on the NIMH RAISE study’s demonstration of the positive impact of CSC on early-psychosis outcomes, Congress passed a 5 percent set-aside from the mental health block grants to states in order to fund treatment for early psychosis in 2014, which added $22.9 million in new funds so that states would not have to allocate money from existing programs to establish new ones (SAMHSA, 2014). SAMHSA encouraged states to use CSC programs and follow the RAISE model rather than issue the money to any program claiming to address early psychosis. The following year, Lutterman explained, Congress saw what states were doing with SAMHSA’s support and increased the set-aside to 10 percent.
He noted that this year, states have had an unprecedented, one-time infusion of federal funds, and his organization is helping states decide how to best use those funds to improve their mental health systems. As part of a COVID-19 supplement in 2021, Lutterman explained, Congress doubled the block grant, maintained the 10 percent set-aside, and gave states 1 year to spend the additional grant funds. The American Rescue Plan doubled the block grant yet again and maintained the 10 percent set-aside (SAMHSA, 2021). This time, Lutterman explained, Congress gave the states 3 years to spend these supplemental funds. All told, Congress provided more than $200 million in additional funds, or $307 million in appropriations from the set-aside, COVID-19 supplement, and American Rescue Plan. This is a tremendous opportunity to advance mental health care, but states are struggling to determine how best to spend those one-time funds. Some are considering opening new clinics, though they are concerned about sustainability.
Lutterman noted that NIMH, SAMHSA, and the HHS Assistant Secretary for Planning and Evaluation (ASPE) jointly funded an evaluation of how the states were using these funds. The first step was to survey states to identify all existing CSC programs, the models they used, and how they were measuring model fidelity and client outcomes. The study team recruited 36 sites to participate in a multiyear evaluation, contribute data, engage in site visits, and take part in fidelity reviews (Ghose et al., 2022).
Lutterman said that of the 36 sites, block grants supplied total funding for 5 and 80 percent or more of funding for 8. Block grant funds accounted for 10–79 percent of funding for 18 sites and less than 10 percent for the remaining 5 (Ghose et al., 2022). Some programs also relied on state funds, and very few, said Lutterman, received reimbursements from private insurance or Medicaid. “We are working with the states to try to improve that,” he noted.
An examination of outcomes, explained Lutterman, revealed that the programs funded by the 10 percent set-aside saw improvements in a range of adverse events, including homelessness, psychiatric inpatient hospitalization, emergency department visits, legal issues, and attempted suicides (see Figure 6). The evaluation also asked program participants about how they thought their well-being had changed since starting the program (see Figure 7). Over one-third of the 116 respondents reported a reduction in their core symptoms, and nearly one-third reported their relationships improved, as did their ability to be social. However, said Lutterman, self-reported improvement was much less for substance use, suicidal ideation, self-harm, and being homebound.
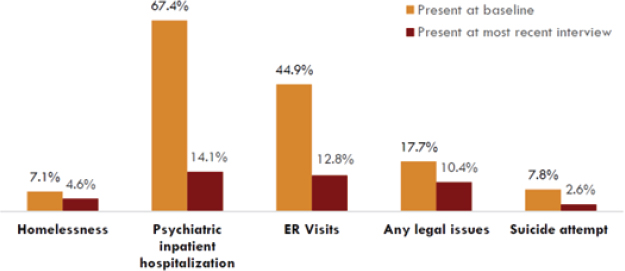
SOURCE: Presented by Ted Lutterman on July 11, 2022 (Nossel et al., 2018).
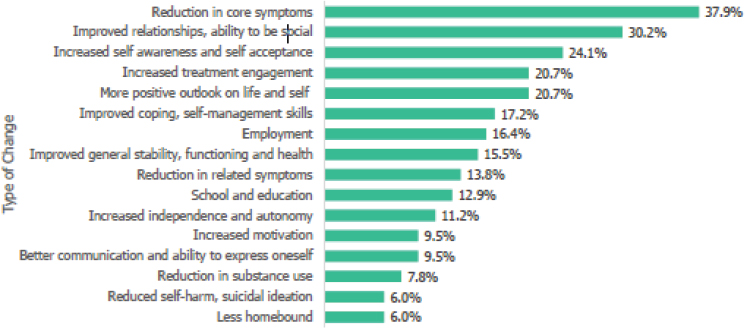
SOURCE: Presented by Ted Lutterman on July 11, 2022 (Nossel et al., 2018).
Following this evaluation, NIMH established and funded EPINET to enable CSC programs to build a research base and pool data across sites. Some of the measures EPINET uses, explained Lutterman, came from the evaluation. As part of EPINET, the NASMHPD updated the national census of known programs for early-psychosis intervention in 2022. It surveyed every state to identify all such programs, regardless of whether they receive grant block funding, and any other CSC programs (see Figure 8). Lutterman and his colleagues followed that census by asking individual programs for more details about their components, clients, financing arrangements, data measures, and other items, with 46 states and 116 programs responding.
For CSC components, 90 percent or more of the programs were providing family education and support, pharmacotherapy, supported education, supported employment, individual CBT, and case management (see Figure 10), and 171 of 211 programs were using standardized measures to assess outcomes (see Figure 11). Two-thirds used the Colorado Symptoms Index (Boothroyd and Chen, 2008)—a measure used in the block grant evaluation—and over half used a QLS.
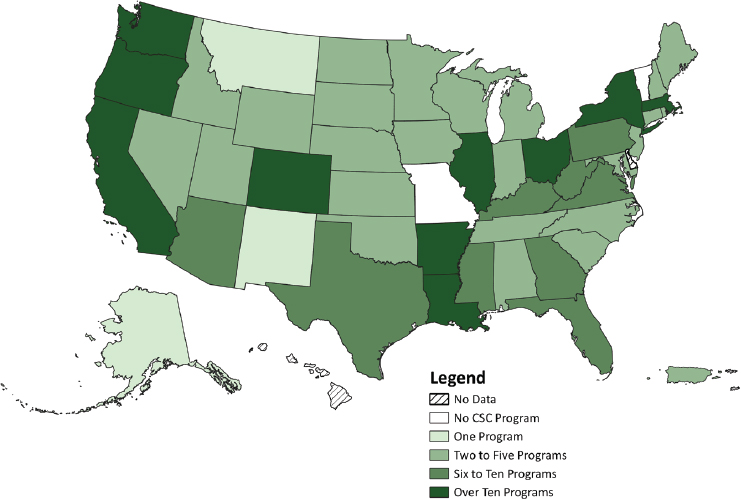
SOURCE: Presented by Ted Lutterman on July 11, 2011 (Kane et al., 2015). Lutterman noted that CSC programs have increased from 59 in 2014 to 353 in 2021. The majority of the programs are using the NAVIGATE, Early Assessment and Support Alliance, or OnTrack protocols (see Figure 9).
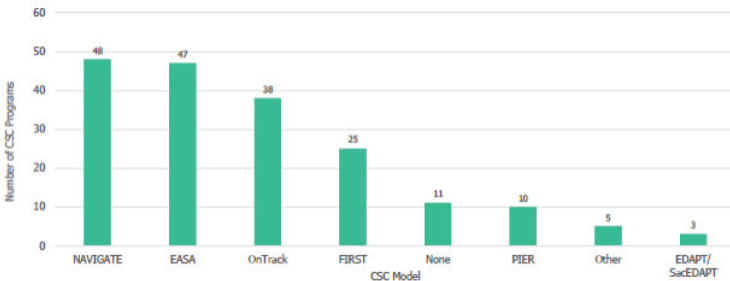
SOURCE: Presented by Ted Lutterman on July 11, 2022.
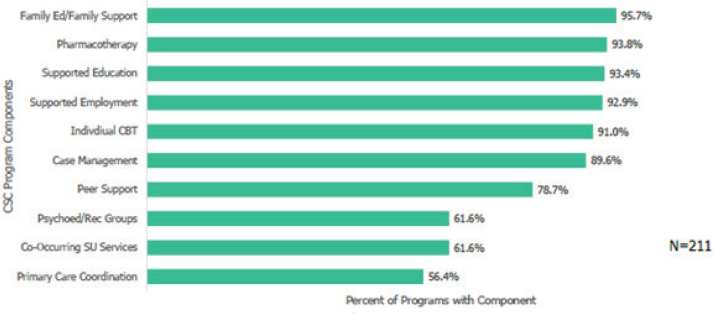
SOURCE: Presented by Ted Lutterman on July 11, 2022.
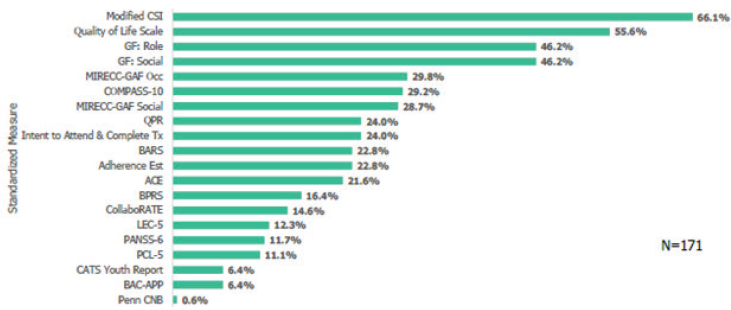
NOTE: CSI = Client and Service Information; GF = Global Functioning; MIRECCGAF = Mental Illness Research, Education, and Clinical Center-Global Assessment of Functioning; QPR = Question, Persuade, Refer; Tx = treatment; ACE = Adverse Childhood Experiences; BPRS = Brief Psychiatric Rating Scale; LEC-5 = Life Events Checklist for Diagnostic and Statistical Manual of Mental Disorders (DSM)-5; PANSS-6 = Positive and Negative Syndrome Scale; PCL-5 = Posttraumatic Stress Disorder Checklist for DSM-5; CATS = Child and Adolescent Trauma Screen; CNB = University of Pennsylvania Computerized Neurocognitive Test Battery.
SOURCE: Presented by Ted Lutterman on July 11, 2022.
Lutterman noted that nearly 60 percent of the programs require that patients have no more than 24 months of untreated psychosis, with just under 14 percent allowing a longer duration, including those with no maximum. Sixty-nine percent do not accept clients with clinical high risk, focusing solely on people with a diagnosed psychosis disorder, and just over one-third are in states working to create a team-based Medicaid case payment rate for CSC. Lutterman pointed out that several states have already approved a team-based case rate, and his team is trying to share how they accomplished that with other interested states. Only 12 percent of programs are in states working with private insurers to create a case-based rate, though Illinois passed a law requiring private insurance to cover all CSC components except for supported employment and education. Other states, said Lutterman, are examining the Illinois model. Optum has asked Lutterman’s team to determine whether any CSC programs with clients covered by Optum would be willing to share information to help it design coverage and determine a cost for specialty coordinated care for early psychosis.
Twenty-three states are also putting their own funds into early-psychosis services; in 2021, that was $18.2 million in addition to federal block grant funds. “The basic take-home we hear is that the block grant and state dollars are subsidizing people with Medicaid and private insurance,” said
Lutterman. “We are picking up the tab for people who should be covered if we could force parity and get better coverage.”
States intend to use their supplemental block grant funds in several ways. For example, 33 states are considering new first-episode programs, 32 are planning to provide additional training for first-episode care providers, and 31 intend to enhance existing programs. Lutterman shared that one state spent a great deal of time and money establishing CSC programs with model fidelity and found that these programs are not fully subscribed, which makes the cost per client high. Because the epidemiology suggests that people should be filling these slots, the state is considering a public education campaign to identify those who would benefit from a first-episode program and get them referred into one. Nineteen states intended to implement a public education campaign for first-episode programs. Nineteen states also noted their intention to enhance their data infrastructure.
Lutterman said his team has been working with state leaders to identify areas where they would find technical assistance related to first-episode psychosis programs useful. The supports that states identified as their top priorities included the following:
- Public education campaigns, to shorten the duration of untreated psychosis by increasing awareness of existing programs among the general public and targeted audiences;
- A multistate consortium to implement and test novel strategies for serving people with first-episode psychosis in rural and remote areas;
- Training for state staff on how to implement and evaluate interventions to help assure cultural relevance of programming for first-episode psychosis;
- Analysis and consultation to support payment design and payment rates; and
- Assistance in analyzing and benchmarking outcome data.
Discussion
Öngür asked Kane whether he had an explanation for the finding that the duration of untreated psychosis was a moderating factor for the 2-year but not the 5-year outcome from the RAISE study. Kane replied that other studies have also suggested that this duration is not as important in longer-term follow-ups and may have more influence acutely. H. Wesley Clark, from the University of Michigan, School of Medicine, asked the panelists how they would propose addressing racism and systemic factors. Ereshefsky replied that it is important to have ongoing conversations and weave them
into all work. Anglin added that the more people talk about this, especially in an interdisciplinary context, the more it will be normalized.
Box 2 lists additional suggestions from workshop participants for future research.
EXPLORING POLICY OPPORTUNITIES
SAMHSA’s Role in Addressing First-Episode Psychosis
Anita Everett, director of the Center for Mental Health Services at SAMHSA, said that SAMHSA comprises four main centers and a variety of offices under the leadership of Miriam Delphin-Rittmon, the Assistant Secretary of Mental Health and Substance Use Disorders. The Center for Mental Health Services, Everett explained, has 45 different types of discretionary grants and three main types of formula grants, including mental health block grants (MHBGs). As described in the previous section, each year, 10 percent of the MHBG is to be set aside by states to support developing and maintaining first-episode psychosis programs. In federal FY 2022, the MHBG was just under $758, so about $75 million was distributed for these programs. She noted that the block grant set-aside enabled
SAMHSA to take the newly generated evidence about CSC and scale it over the past 7 years, with most programs implementing the majority of CSC components. “We are not where we need to be, but we are considerably better off than we were several years ago; this is a very short time to scale up the program in policy terms,” said Everett.
The programs are far short of the number needed to reach everyone with first-episode psychosis, and these CSC clients fell in 2020 and 2021. She said this likely reflects the effects of the COVID-19 pandemic on the outreach and infrastructure supports these programs provide for the youth and young adults they serve.
Everett explained that in 2022, 15 state mental health agencies identified technical assistance needs related to CSC and early serious mental illness programs in their MHBG applications. The most common request had to do with financing and sustainability, with other frequent requests for help with training care providers beyond what they receive in graduate-level programs, curricula on cultural and linguistic competence, expanding programs into rural and remote areas, and collecting and monitoring data for outcomes.
SAMHSA is focused on several policy areas, such as enhancing implementation to accelerate uptake of evidence-based practices. Everett noted that SAMHSA has partnered with NIMH on incorporating dissemination and implementation science into grant programs, including the first-episode psychosis program that SAMHSA supports. Other policy areas relate to sustaining interventions, rural adaptations, linking the early serious mental illness programs with first-episode psychosis programs, and assessing longer-term value. SAMHSA wants to collect data on outcomes for people who leave a first-episode program and enter the regular public health system to gain information about how people are managing when they are years out from participation.
Community Programs for Outreach and Intervention with Youth and Young Adults Through the Clinical High Risk for Psychosis Grant Program
Melinda Baldwin, director of SAMHSA’s Division of Prevention, Traumatic Stress, and Special Programs, oversees programs across the intervention and developmental spectrum, including the Clinical High Risk for Psychosis program. This program funds services that accept youth aged 10–25 who are at high risk and provides them with more intensive, evidence-based services to reduce the risk of psychosis onset. The grants this program funds aim to improve symptomatic and behavioral functioning; enable youth and young adults to resume age-appropriate social, academic, and vocational activities; delay or prevent the onset of psychosis; and mini-
mize the duration of untreated psychosis for those who do develop symptoms. Baldwin clarified that this program differs from the Comprehensive Community Mental Health Services for Children with Serious Emotional Disturbances program for children and young adults, which works with youth under age 21 who are also at risk for psychosis.
Baldwin said that for FYs 2019–2021, the Clinical High Risk for Psychosis program served 1,213 individuals, almost 60 percent of whom were ages 16–25. Slightly more clients identified as female versus male, with a small number identifying as transgender. Fifty-seven percent identified as White, 21 percent as Black or African American, and 25 percent as Hispanic. National Outcomes Measurement System data showed that 64.6 percent of the 281 individuals who completed this assessment reported improved functioning in everyday life, 42.0 percent reported feeling more socially connected, 26.3 percent reported experiencing no serious psychological distress, 22.0 percent said they were healthy overall, and 20.3 said they were either fully employed or retired.
Baldwin observed that it has become clear through experience that outreach is critical to ensure adequate enrollment, adding that it is essential that screening and assessment be highlighted and coordinated with first-episode programs The program’s most recent funding opportunity announcement asked applicants to identify a specific person who would engage in outreach. Baldwin also noted workforce challenges at every level across programs.
Expanding, Improving, and Sustaining Early-Psychosis Services in the United States
Robert Heinssen, director of the Division of Services and Intervention Research at NIMH, noted the “phenomenal success” that the early-psychosis research and practice community has achieved over the past decade, including a sustained effort to implement evidence-based services nationwide. In 2020, for example, the American Psychiatric Association issued practice guidelines that recommended CSC as an intervention for first-episode psychosis. Several federal agencies, including SAMHSA, the Centers for Medicare & Medicaid Services (CMS), the Veterans Health Administration, and the Department of Labor, have endorsed CSC as an evidence-based treatment and have undertaken efforts to implement it broadly. From Heinssen’s vantage point as a long-time NIMH health scientist administrator, this may be the fastest and most extensive U.S. implementation of an evidence-based mental health treatment. He also pointed out that a sizable early-psychosis learning community has emerged, with about 1,500 members in the Psychosis-Risk and Early Psychosis Program
Network.33 It sponsors an annual meeting that draws several hundred frontline clinicians, program administrators, and researchers to talk about their experience providing CSC, share their learning, and identify new scientific opportunities. “Congratulations to all of you for making this happen,” said Heinssen.
Despite this progress, challenges remain to address, such as speeding access to care; engaging participants in care; sustaining high-quality services over time; organizing services to support long-term recovery; addressing inequities in service availability and delivery; and strengthening the CSC business model by streamlining reimbursement mechanisms, reducing staff turnover, and growing the workforce. Heinssen stated that President Biden, in his first State of the Union address, laid out a national strategy for addressing the mental health crisis, as part of his unity agenda,34 which focused on strengthening system capacity, connecting Americans to care, and creating a continuum of support for people with mental health conditions.
In terms of policy opportunities to address some of those challenges, Heinssen said that the national 9-8-8 system, along with the 9-8-8 Implementation Act that Congress introduced this year,35 provides an opportunity for the early-psychosis care community to engage in conversations about how mobile crisis units, crisis respite centers, and other emergency treatment services can connect to CSC programs. The goal is a seamless referral process that will allow a person who is experiencing an episode of psychosis to move rapidly from an acute crisis into a warm and welcoming space that provides necessary stabilization services. Such arrangements, he explained, could reduce the frequency of law enforcement being involved in psychiatric crisis situations. This point is important because research has shown that individuals with early psychosis who come in contact with the criminal justice system can incur up to two additional years of waiting before they receive proper care (Ramsay Wan et al., 2014).
Heinssen noted that the NIMH-funded EPINET is developing tools that may help early-psychosis programs to sustain high-quality services over time. Standard assessment measures have been adopted by 101 clinical programs in the United States EPINET will analyze large datasets based on these measures to develop CSC performance metrics that can help identify best practices. Performance dashboards and quality benchmarks based on national norms will help local programs to evaluate their effectiveness and
___________________
33 See https://med.stanford.edu/peppnet/whoweare.html (accessed November 1, 2022).
34 See https://www.whitehouse.gov/briefing-room/statements-releases/2022/03/01/fact-sheet-president-biden-to-announce-strategy-to-address-our-national-mental-health-crisis-as-part-of-unity-agenda-in-his-first-state-of-the-union/ (accessed October 18, 2022).
359-8-8 Implementation Act of 2020, HR 7116, 117th Cong., 2nd sess., Congressional Record 168, no. 48, daily ed. (March 17, 2022):H3827.
inform quality improvement efforts. Heinssen noted that NIMH has proposed a complementary research initiative to develop, validate, and implement quality measures in mental health broadly but with a specific focus on measures that apply to CSC.36
Heinssen pointed out encouraging policy developments that should help organize services to support long-term recovery. The Department of Labor has identified the youth and adult programs authorized by the Labor Workforce Innovation and Opportunity Act of 201437 as a mechanism to broaden supported education and employment services and provide a career ladder for people with first-episode psychosis. The certified community behavioral health clinics expansion initiative38 announced in March 2022 establishes step-down care from CSC programs to tailored outpatient treatment that may consolidate CSC gains and foster long-term recovery.
In terms of improving the early-psychosis care business model, Heinssen said that the president’s intention to expand and strengthen the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 200839 could result in private insurance coverage of CSC treatment, rehabilitation, and program support services. Heinssen noted that one potential approach is to broaden the spectrum of services to include in SAMHSA-supported clinical high-risk programs. One clinical team would be able to serve first-episode and high-risk populations in complementary programs. This approach might be attractive to early-psychosis programs that serve rural areas with low population density.
President Biden’s plan to address the national mental health crisis also includes goals for research on new practice models. The scientific hubs of EPINET’s eight regional networks address this goal via practice-oriented research projects that aim to close knowledge gaps in early-psychosis treatment. The hubs contribute de-identified clinical data and research findings to the National Data Coordinating Center (NDCC)40 for rapid dissemination to early-psychosis stakeholders. For example, the NDCC, through a consensus process involving the scientific hubs, has developed a core assessment battery that covers 21 dimensions of first-episode psychosis symptoms, functioning, treatment, and recovery outcomes. Heinssen explained
___________________
36 See https://www.nimh.nih.gov/funding/grant-writing-and-application-process/concept-clearances/2022/developing-quality-measures-to-advance-mental-health-care-access-and-outcomes (accessed November 1, 2022).
37Workforce Innovation and Opportunity Act, Public Law 128, 113th Cong., 1st sess. (July 22, 2014).
38 See https://www.samhsa.gov/grants/grant-announcements/sm-21-013 and https://www.samhsa.gov/grants/grant-announcements/sm-22-012 (accessed October 18, 2022).
39Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008, Public Law 343, 110th Cong., 2nd sess. (October 3, 2008), § 511.
40 See https://nationalepinet.org/endcc/ (accessed October 4, 2022).
that all 101 EPINET clinics have agreed to implement it as a common basis for evaluating patients and CSC interventions, planning quality improvement activities, and pursuing practice-oriented research. The NDCC has developed a Web-based system that makes the assessment battery, which is both free and available in multiple languages, accessible to CSC clinics outside of EPINET, along with performance dashboards and benchmarks to facilitate their quality improvement activities. He added that EPINET only includes about one-third of all U.S. CSC programs, so “We owe it to those other programs to give them the best services and scientific information available.”
Heinssen said that NDCC recently launched the Web-based system and that a growing number of community programs are already contributing data. The NDCC is analyzing and evaluating clinical data and sending results back to the programs so that they have comparative feedback about their own CSC performance. This feedback can help clinicians to understand their individual clients’ needs and support clinical decision making. Program administrators can use clinic-level data to understand how their program is performing compared to others in the national network. The data can also enable state mental health authorities to set quality improvement targets, launch practice-oriented research, and participate in empirical policy analysis. Heinssen also observed that Virginia has enrolled 12 of its programs in the core assessment battery program, which effectively creates a ninth regional EPINET network.
Advocacy for Improved Policies
Mary Giliberti, chief public policy officer for MHA, said that the mental health community has worked with Congress to establish new sources of funding devoted to mental health. Among the successes are the Bipartisan Safer Communities Act41 and Community Mental Health Services Block Grant programs. She noted that the House of Representatives has passed a bipartisan bill that would reauthorize the block grant program42 and retain the 10 percent set-aside for early-psychosis programs. To Giliberti, this shows how important it is for the mental health community to keep educating policy makers about the value of this program and what it does. She mentioned a discussion in Congress about adding a 5–10 percent set-aside for crisis care, which could create an opportunity for more education and outreach and creating a set-aside for prevention and early intervention
___________________
41Bipartisan Safer Communities Act, Public Law 159, 117th Cong., 2nd sess. (June 25, 2022).
42Community Mental Health Services Block Grant Reauthorization Act, HR 7241, 117th Cong., 2nd sess., Congressional Record 165, no. 106, daily ed. (June 22, 2022):H5810.
more broadly. NASMHPD has been a supporter of this latter idea in part because it would increase flexibility around outreach efforts.
Giliberti explained that the Substance Use Block Grant program allocates 20 percent of the grant to early intervention and prevention, in contrast to the lack of a set-aside requirement in the MHBG.43 The House reauthorization bill allows 5 percent of the MHBG block grant to be used in evidence-based early-intervention and prevention programs but does not require it. “We will see what happens as those bills continue to make their way through Congress, but I want to reiterate that there is always a need for continuing education with our policy makers,” said Giliberti. She added that the difficulty in securing long-term financing is part of the larger problem of financing mental health care in the United States.
CMS has issued guidance around Medicaid financing for CSC, but Medicaid does not cover the employment and supportive education components except under very complicated funding mechanisms, explained Giliberti. This creates challenges for organizations seeking reimbursement. “Any time you start making something complicated, it is going to be difficult to scale,” said Giliberti. “We want to make financing as easy as possible.” She pointed out that paying for hospitalization through Medicaid is simple yet financing for these mental health programs and care components that could prevent hospitalizations is difficult, which leads states to request technical assistance on how to do so. “Wouldn’t it be a wonderful world if we did not need technical assistance because it was so darn easy that you did not have to hire a whole bunch of people to help you do it?” she asked. She hopes that CMS will revisit that restriction and treat CSC as a comprehensive, evidence-based, team-based service rather than many individual pieces.
Medicare, given the age group it serves, does not pay for first-episode programs, but the lack of Medicare guidance affects the private insurance sector, since it tends to follow whatever Medicare does. Perhaps Medicare could create a Current Procedural Terminology code that encompasses all of CSC, which would simplify billing. Giliberti noted that some states have taken the lead in requiring private insurance to cover CSC and that the federal Mental Health Parity and Addiction Equity Act that Heinssen mentioned does require private insurance to cover mental health and substance use services. Still, she said much work remains, particularly with the states. The diagnoses that meet “medical necessity” criteria also need to be better defined.
Another critical aspect Giliberti noted is patient experience and the importance of measuring it in the mental health care setting. Hospitals
___________________
43 See 42 U.S.C. Section 300-22(a)(1) (Substance Abuse Treatment and Prevention Block Grant); 42 U.S.C. Section 300x-1 (Community Mental Health Block Grant) https://uscode.house.gov/view.xhtml?req=granuleid%3AUSC-prelim-title42-chapter6A-subchapter17-partB&edition=prelim (accessed November 1, 2022).
measure it and are reimbursed partly based on patient experience scores. However, people whose primary diagnosis includes a mental health condition are excluded from those scores, which points to the long history of a lack of caring about their and their family members’ experiences. She said, “It is important in all services, including coordinating specialty care, that we start requiring patient experience data and ultimately paying on it because it matters how you are treated as a person in these services.” Moreover, those data should be broken down by demographics to inform and address equity issues.
Giliberti also noted that resources are being devoted to place mental health professionals in schools and elsewhere, which is a positive move. However, she expressed some concern about the level of training they will receive and whether they will learn about CSC. She noted that MHA and other organizations have been working to get mental health literacy requirements included in K–12 education, but so far, she sees little of this in curricula other than in New York and Michigan.
Giliberti said that parity should be included in the analyses undertaken by the Department of Labor, particularly regarding treatment limits that result in less coverage for programs such as CSC compared to physical health services. It might also be useful to see how financing team-based care services for other conditions, such as diabetes, is handled.
Policy Futures
Nev Jones, assistant professor in the School of Social Work at the University of Pittsburgh, explained that in addition to being a researcher, she started out as a patient in an early CSC program between 2007 and 2011. She added that when she looks at research on outcomes in CSC, what she wants to see is whether people are really on a path to a “career” and making a living wage. Jones said that two areas in need of improvement within CSCs are long-term outcomes and patient and family engagement, particularly among those at the highest risk of long-term poverty, homelessness, and/or incarceration. She presented three concrete focus areas for improving CSC impact: (1) strengthening the workforce; (2) recalibrating the outcomes measured to better shape services, focusing on outcomes that matter most to those receiving services; and (3) “being the change,” particularly around including and hiring people with lived experience and intersecting experiences of marginalization and minoritization.
Based on her work with state- and program-level data, Jones described disengagement as a substantial, largely unaddressed problem in CSC. The majority of clients who disengage do so for a variety of reasons, including social and structural disadvantage, discrimination, and structural racism; conflicts or disagreements over medication and treatment; and disagree-
ment with clinical interpretations of the problem. Some clients are doing well and do not want the intensity of CSC, but her research suggests that many leave the programs under suboptimal circumstances, with no clear prospects of a viable, living-wage career. “Our impact on long-term outcomes will be diminished,” she said, “if we do not address those leaving prematurely, especially those who are unemployed and not in training or education when they leave.”
Jones said that there are few reasons to believe that standard (non-CSC) care will provide the support these individuals need to put them on a path to long-term success, so it is imperative to develop solutions to the disengagement problem and strengthen supports to ensure that young people have every possible opportunity and support to pursue educational and work goals.
Patients who do not have good outcomes, are not earning a living, and receive supplemental security income44 based on a disability determination frequently end up in what has been called a “poverty trap”—often including suboptimal subsidized housing with limited budgets for nutritious food and community participation. Jones hypothesized that their poorer long-term physical outcomes result in part from the long-term poverty that disproportionately affects people with ongoing disability. However, no clear evidence yet suggests that access to CSC alone substantively changes long-term poverty and unemployment rates, largely because the literature fails to measure quality of work or education and prospects for actually supporting socioeconomic mobility (versus short-term placements that may never lead to financial independence). Research in early psychosis focused on poverty remains underdeveloped, with major gaps in our understanding of how socioeconomic disadvantage influences long-term outcomes.
For solutions, Jones reiterated the importance of strengthening the workforce and echoed Niendam’s idea of working with professional associations to ensure that curricula, particularly for social work and counseling programs, include some basic training on early psychosis and other serious mental illnesses. Peer workers are essential but not sufficient, and one challenge is the scant research on the effect of peers in psychosis-specific contexts, such as CSC. In addition, there are almost no standardized hiring criteria, training, tools, or structure for peer workers, nor has much attention been paid to hiring peers with ethnic and cultural backgrounds that match the local patient population or who have had the lived experience of psychosis. “I think we are very far from understanding what we would need to be focusing on to strengthen peer support services,” said Jones.
Peer specialists are typically at the bottom of the pay hierarchy, as is supported education and workforce training. This is ironic, Jones said;
___________________
44 See https://www.ssa.gov/benefits/ssi/ (accessed September 16, 2022).
for all the talk about the social determinants of health, the intervention most aligned with addressing them is compensated at the lowest rates. Many of the peer specialists Jones has interviewed report not being able to support themselves because of low pay or only part-time hours. “Work that addresses social determinants is high-level skilled work and should be compensated accordingly,” said Jones.
To support employee retention, Jones suggested expanding loan repayment programs for health workers who are in disadvantaged areas or in certain types of programs, such as CSC. Medicaid should also recalibrate Medicaid reimbursement so that workers are paid a living wage, which is not the case in parts of the country with a high cost of living.
To measure the outcomes that matter, Jones said that a high-level metric could be material living conditions, which would include earning a living wage and living independently. In her opinion, this problem stems from structural racism and classism embedded in the larger problem of psychosis. “We have to fix the big picture of psychosis outcomes or we risk undermining racial equity,” said Jones. Metrics of success would look at people’s career preparation, the steps they are taking and have support for, and whether they can get a job with a pathway to a living-wage career. Measures should include quality of work, educational activities, career development, and income sources relative to the local cost of living. These measures could enable critical learning and lead to programs adapting to optimize outcomes.
Data from these types of measures would help researchers develop more robust interventions. Jones noted the tremendous amount of research on career development among young adults (without disabilities) that could provide important lessons for the early-psychosis care community. But she said that can only happen after identifying the problem, measuring it to determine how substantial it is, and then aligning interventions to address it.
Jones said she wants to see this community address inequality with respect to who is working in these clinics and who is involved in planning and evaluating services. This is particularly true for people with the lived experience of psychosis or long-term disability. She noted that in the nearly 15 years that she has been involved in this field, she is usually the only person in the room at early-psychosis events and summits with that lived experience. She emphasized that efforts to increase diversity need to go beyond integrating peer specialists and include lived experience social workers, clinical psychologists and psychiatrists, nurse practitioners, and researchers. What saddens her is that she has met many young people and emerging researchers who want to get involved, but the barriers to entry are too high.
Anglin commented that she has been mentoring students with lived experiences as a doctoral adviser and asked about mechanisms or programs
that can support these students. Jones responded that she runs a group at her institution for such students and researchers across all mental health conditions, though she has received so many emails from early-career researchers and students who have lived experience specifically with psychosis that she is thinking of creating a subgroup. She would like to see an expansive network of mentors who truly understand the challenges these individuals are facing.
Shim said that she has been surprised by the number of patients or clients that she has had in early-psychosis programs who are in medical or graduate school when they first develop symptoms. Many have been able to succeed, but she noted that professional schools are not structured to allow people to take time off to deal with a major health issue and continue with their care; “we built in a very discriminatory system where we are excluding people and preventing people who would be exceptional Ph.D.s, exceptional M.D.s, and exceptional D.O.s that we are not allowing to be successful in the field because of the policies that we have created and the ways that we have thought about higher education.” Based on the number of students she is managing clinically, she suspects that many people in the field have psychotic illness and do not feel they can safely disclose their condition because of a fear of not getting licensed to practice. Giliberti noted that the Department of Education is planning to rewrite Section 504 of the Rehabilitation Act of 1973,45 and MHA has pointed out that students with mental health conditions often do not know they are covered by Section 504, which enables them to ask for modifications, such as taking time off, and their institution should grant those requests.
Discussion
Howard Goldman, the session moderator, pointed out that Individual Placement and Support (IPS) for employment has a strong evidence base of benefit. The challenge is finding a case rate that will cover it because it is the one item most insurance policies explicitly exclude. Everett replied that SAMHSA is trying to provide stronger support for IPS and recently created new opportunities to apply it in transitional-aged youth, including those with first-episode psychosis.
Jones mentioned education funding streams from the Departments of Education and Labor that are focused on antipoverty career development projects; they do not explicitly exclude youth or adults with psychosis or serious mental illness, but they do not target them, either. Giliberti won-
___________________
45Rehabilitation Act of 1973, Public Law 112, 93rd Cong., 1st sess. (September 26, 1973) 87 Stat. 255.
dered whether Medicaid Section 1115 waivers46 might enable states to create templates that would allow coverage for supported education and employment services with CSC, given that it has proved to be cost effective or at least cost neutral. Jones replied that New York does have programs that fund the IPS component through Section 1115 waivers, though it limits eligibility to former CSC clients with a fairly significant level of functional disability; many more who do need supports do not qualify. Reaching young people before a clear history and pattern of functional disability will require more expansive eligibility criteria, said Jones.
Kane also raised a fundamental concern about criteria for admission to these programs: the diagnostic process is not what it should be, and the evidence for psychopharmacologic interventions is based on research on schizophrenia, not psychosis, drug-induced psychotic disorder, or delusional disorder. His concern is that many of the people diagnosing in community mental health centers are not psychiatrists. Rather, they are social workers, case workers, and other staff who have not had adequate training in the diagnostic processes necessary for psychosis, which is quite challenging. One result is premature closure of the diagnostic process, and another is that once a diagnosis is made and medication prescribed, that diagnosis may never be revisited. “Revisiting the diagnosis and avoiding premature closure is incredibly important because we are talking about committing someone to long periods of treatment with medications that can have a lot of side effects,” said Kane. “We have to figure out a way to make the diagnostic process more reliable, more valid, and more scalable because we still do not have laboratory tests or technological processes for facilitating the differential diagnosis of psychosis.” He noted that speech and voice analysis may help at some point, as could many other biomarkers, but those are still in development.
Several audience members asked the panelists to comment on whether telehealth or other online methods are working in less populated areas. Everett replied that they have been. “Yes, I think that is part of the answer to how we get to geographically less dense population areas,” she said. Goldman added that the work he does with the Social Security Administration (SSA) on IPS-supported employment has found that remote job development is challenging but possible.
Jones commented that telehealth has its limits in some rural areas, such as the heart of Appalachia, where no Internet access is possible and calling people does not work. In these locations, relying solely on telehealth would make inequality worse. The early-psychosis teams that he works with have tried creating telehealth hubs, but they still end up driving 3 hours to pro-
___________________
46 See https://www.medicaid.gov/medicaid/section-1115-demonstrations/about-section-1115-demonstrations/index.html (accessed November 14, 2022).
vide services in their clients’ homes because that is the only way to engage them. In addition, some communities with a history of cultural distrust require in-person contact to gain their trust.
Giliberti remarked that Medicaid has given states the option to decide whether they will continue using telehealth, which expanded greatly during the COVID-19 pandemic, and early signs are that most will. She noted a draft bill that would allow Medicare to remove the 6-month in-person exam requirement for Medicare coverage of telehealth-based mental health services,47 which could prompt commercial insurance to do the same, assuming that change makes it into law. Goldman added that it may be fruitful to get Medicare to fund assertive community treatment for the substantial population that is younger than 65 but is covered by Medicare due to a disability determination by SSA, and to have that serve as a model for commercial insurance to follow for community-based treatment of first-episode psychosis.
Leah White, senior project manager at the Foundation for NIH,48 noted that the Foundation is able to broker collaborations among multiple government agencies; she asked the panel for ideas on how to bring together different government departments and agencies to work on a common solution. Goldman replied that the National Academy of Social Insurance recently released a comprehensive report addressing that issue (Edwards and Murphy, 2022). Heinssen replied that the new federal Behavioral Health Coordinating Committee49 brings together various agencies with responsibility for different aspects of the lives of people with mental illness. No specific group is focused on CSC, but this group has covered many of the topics the workshop speakers have discussed and would be a place to raise the issues the workshop has identified. Everett added that the Interdepartmental Serious Mental Illness Coordinating Committee,50 which the 21st Century Cures Act51 established, brings together the various federal agencies responsible for different aspects of the lives of adults with serious mental illness and children with serious emotional disturbance, and links them with relevant private-sector partners.52 The committee makes specific recommendations for actions that agencies can take to better coordinate service delivery. One of its first recommendations was to scale CSC. The
___________________
47 42 C.F.R. § 410.78(b)—Telehealth Services.
48 See https://www.fnih.org/ (accessed November 14, 2022).
49 See https://www.naatp.org/advocacy/public-policy/hhs-creates-behavioral-health-coordinating-council/may-18-2021 (accessed November 14, 2022).
50 See https://www.samhsa.gov/about-us/advisory-councils/ismicc (accessed November 14, 2022).
5121st Century Cures Act, Public Law 255, 114th Cong., 2nd sess. (December 13, 2016).
52 See https://www.samhsa.gov/about-us/advisory-councils/ismicc (accessed October 18, 2022).
good news, said Goldman, is that federal agencies recognize these problems. SSA, for example, sponsored two large demonstration programs on employment for people with mental illness (Drake et al., 2013, 2016; Riley et al., 2021).
Öngür commented that funding or resources for mental health is often seen as a zero-sum game that requires taking scarce resources from existing programs to fund new ones, which is what happened with first-episode versus chronic psychosis services. “We need to be ambitious about bringing in the resources and arguing forcefully for this,” said Öngür. To do that, he said, the early-intervention movement needs to leverage the science to capture the attention of the policy makers and the federal government and to bring together various forces and align them in a way that actually brings additional resources into the field.
Everett remarked that policy advances when a window of opportunity opens, and she believes that such a window exists for mental health, given what has happened during the COVID-19 pandemic. She noted that SAMHSA has seen a significant increase in bipartisan requests for advice on bills related to mental health. Giliberti agreed that interest has increased, though the vast majority of attention and funding goes to later-stage illness. Giliberti emphasized the critical need for more people to talk to policy makers about early-intervention and prevention and explain how it works, because many worry about money being misspent on these two areas.
Goldman underscored the strong evidence to support these interventions, and Heinssen emphasized that this evidence was generated in real-world care settings without disrupting real-world care processes. In addition, he said the research community has created a learning health care framework for early-intervention and prevention science that looks to incrementally improve services through measurement and assessment. He believes that the early-intervention community’s learning health care framework is influencing mental health care writ large. “We are getting a new framework for how you implement, how you improve, and how you move the whole system forward in an enduring way,” said Heinssen.
Jones noted that a recent survey of thousands of faculty and graduate students found an overrepresentation of individuals with lived experience among those in clinical psychology training programs for almost every mental health disorder except psychosis (Victor et al., 2022); only one person reported having a psychotic disorder. Jones said that Stephania Hayes, a postdoctoral research scholar at UCD, has organized a group of early-psychosis clinicians with lived experience. Jones shared how difficult it is for clinicians to disclose this information. “We both have to change the culture in our own programs and recognize the real disparities [i.e., in terms of equity and inclusion of students, trainees and early-career researchers with
psychosis and other serious psychiatric conditions], because if we do not understand that there is incredible underrepresentation, we are not fixing it,” concluded Jones.
CLOSING REMARKS
Öngür summarized the key themes based on the discussions at the workshop. The field already has a beachhead, he said; a developing system that has been rapidly transforming how the nation cares for individuals with early psychosis and making a difference in their lives. Quoting Winston Churchill, Öngür said this “is not the beginning of the end, but it is the end of the beginning.” Now we need to be ambitious and think about the next steps given the hundreds of clinics around the country, thousands of people receiving CSC, and a good scientific database.
The first step, he said, should be to scale these programs at a population level because there is a huge unmet need, as several speakers noted. Without scaling, early-psychosis programs will remain an academic exercise. However, some clinics in rural areas are not at capacity, pointing to the need to increase outreach efforts, rethink how we deliver care, and address the fragmentation of the health care system that impedes the development of a rational design for this system. It will also be important to address the adverse experiences, structural racism, and other factors that are creating a greater need for mental health care.
Öngür recounted a trip he took to Denmark in 2021; he found that Denmark is reaching 60–70 percent of the people who would benefit from a first-episode psychosis clinic and there is a proposal to the government to open new services in order to get closer to reaching 100 percent of those in need. “At that level, if early intervention is making an impact, we should see it at the population level in terms of reduced number of hospitalizations for psychosis in the country and fewer people who need disability income. Once you are at that population level, you actually should start to see those numbers move, and that is just such an exciting prospect,” he said. “I think this is something we should aspire to.”
Other suggestions that Öngür highlighted included the following:
- Breaking down the silos among community care providers and specialty programs for first-episode psychosis, clinical high-risk individuals, and other psychopathologies;
- Developing a long-term plan for how to train the right people for early interventions and how to retain them, including how to pay them better and support them in their work;
- Determining the optimal duration for CSC interventions, and creating step-down referral options, perhaps to other specialty services in the community, at the appropriate time;
- Increasing effective outreach and education about early psychosis to youth and their communities, to both increase the number of people receiving care they could benefit from and raise awareness and transform the way society thinks about early psychosis; and
- Attending to underserved communities and marginalized populations that historically have not had a voice in discussions about psychosis and yet represent a significant number of individuals who would benefit from early interventions.
In closing, Öngür offered one final suggestion for increasing outreach and education: create a public service announcement or social media challenge, like the ice bucket challenge in 2014 that successfully increased awareness about amyotrophic lateral sclerosis (ALS) and the need for research on ALS, which occurs far less frequently than psychotic disorders.
Box 3 summarizes additional suggestions to improve care made by workshop participants.





























































