
Summary1
INTRODUCTION
Health equity is the state in which everyone has a fair opportunity to attain full health potential and well-being, and no one is disadvantaged from doing so because of social position or any other socially defined circumstance. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities and historical and contemporary injustices and eliminate health and health care disparities due to past and present causes. When individuals thrive, communities and the entire nation thrive.
Racial,2,3 ethnic, and tribal health inequities and their root causes have been substantially documented, and the evidence is clear—advancing health equity needs to be approached using a holistic view of health, one that considers all that impacts it: economic stability, access to quality education and health care, and vibrant and livable communities (such as access to housing,
___________________
1 This Summary does not include references. Citations for the discussion presented in the Summary appear in the subsequent report chapters, as does a detailed discussion of the policies and evidence reviewed to support the committee’s conclusions and recommendations.
2 The racial and ethnic categories discussed in this report should not be interpreted as being primarily biological or genetic. Race and ethnicity should be thought of in terms of social and cultural characteristics and ancestry and could be considered proxies for racism and social characteristics. Race and ethnicity are not biological categories or otherwise verifiable.
3 Over time, terminology related to racial, ethnic, and tribal health equity has significantly evolved. The committee strived to use language that is respectful, accurate, and maximally inclusive; however, there is not always consensus on preferred terms, and these preferences may evolve. See the “Key Terms” and Chapter 1 discussion on terminology.
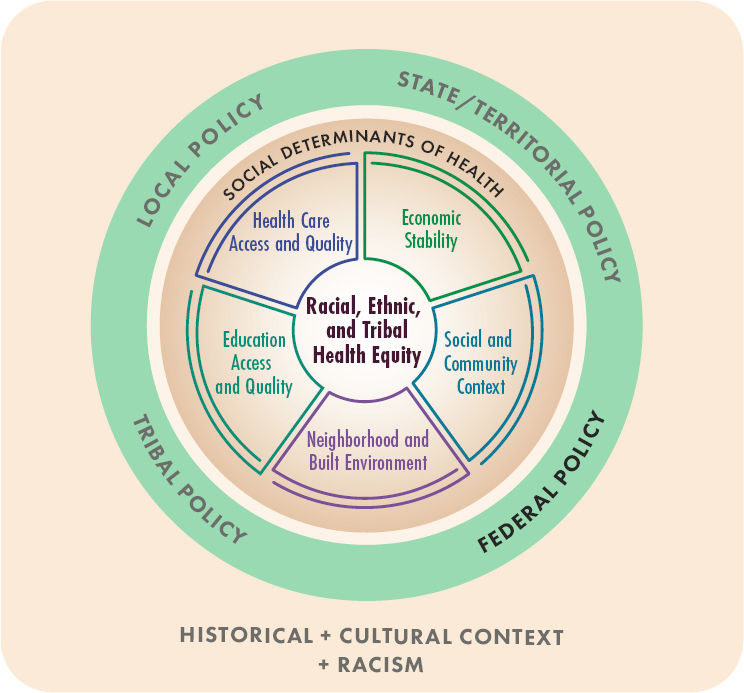
transportation, and healthy environments; see Figure S-1 and Box S-1). There are many levels at which to intervene; however, the committee was asked to (1) focus on federal policies that contribute to preventable and unfair differences in health status and outcomes experienced by all racially and ethnically minoritized4 populations in the United States and (2) provide
___________________
4 Rather than referring to “racial and ethnic minorities,” “members of minority groups,” or “underrepresented minorities,” this report uses the term “minoritized,” which refers to people from groups that have been historically and systematically socially and economically marginalized or underserved based on their race or ethnicity as a result of racism (such as American Indian and Alaska Native, Asian, Black, Latino/a, and Native Hawaiian and Pacific Islander communities). The committee uses this term to make the distinction that being minoritized is not about the number of people in the population but rather about power and equity. (See the Key Terms section for additional terminology used in this report.)
conclusions and recommendations that identify the most effective or promising approaches to policy change with the goal of furthering racial and ethnic health equity (the committee was asked to review both promising and evidence-based solutions). The committee also took into consideration federal activities already underway. Although there are many examples of policies that have advanced health equity, the committee was not asked to review such policies. In the context of the significant progress advancing health equity by federal policy makers, this report provides a framework for federal action that builds on that progress to address continued barriers.
Although membership in a particular racial, ethnic, or tribal group does not predict a given outcome, and each of the broad categories of race and ethnicity has considerable heterogeneity, the available data on health outcomes and other measures of well-being tell a consistent story of wide disparities in health. Research demonstrates that the inequitable patterns
of these social risk factors across race and ethnicity are in large part a consequence of structural disadvantages for minoritized communities that were, in no small measure, initiated by historical federal policy decisions. These decisions have guided the organization and governance of society and the distribution of resources. For example, the U.S. history of extermination, removal, and assimilation of American Indian people, enslavement of African and African American people, colonialism, and immigration policy have played a critical role in how the country is stratified, affecting contemporary outcomes across health, education, socioeconomic status, and other measures of well-being. There are higher rates of childhood asthma among low-income households, higher morbidity and mortality from chronic diseases among individuals with lower educational attainment, and higher exposure to air pollution among residents of disinvested communities—disproportionately individuals who are racially and ethnically minoritized. Moreover, the effects of the structural determinants of health on many health outcomes persist when accounting for income and education.
A policy could influence health inequities in many ways. For example, the report considered policies that are neutral in terms of racial, ethnic, or tribal inequity but have indirect equity implications (i.e., policies that aim to improve health or the factors that shape it without considering health equity may unintentionally improve equity or improve population health overall but fail to decrease, or even widen, gaps); policies that are intended to address inequities but fall short of this goal (i.e., they may be working but have aspects that can be improved or may have unintentionally worsened inequities); policies that intentionally worsened racial, ethnic, or tribal inequities (i.e., causing harm to some but not others); and the lack of policy in a given area. The report also describes federal policy levers, including implementation and enforcement.
Federal, state, local, tribal, and territorial policies have a complicated relationship. The federal government often sets priorities at all levels of government via funding and regulations. However, if federal policy makers want health equity to be prioritized at all levels of government, they need to set the standard of equity and lead with policies aligned with funding priorities that drive health for all. Practices consistent with this include providing supportive tools, coordination, and resources and incentivizing states, localities, tribal nations, and territories.
Report Key Principles
To guide its work, the committee adopted a set of principles informed by a large and growing body of research on the social determinants of
health (SDOH) and input from experts, policy leaders, and other key stakeholders.
- Health is more than physical and mental well-being—it also includes well-being in social, economic, and other factors, all of which are necessary for human flourishing;
- All federal policies have the potential to affect population health;
- Evidence is informed by quantitative, qualitative, and community sources;
- Federal policies should center health equity;5 and
- To advance health equity, structural and systems change are needed.
With these principles in mind, it is important to emphasize that equity is not interchangeable with equality—equality is the treatment of all individuals in the same manner and assumes a level playing field for everyone without accounting for historical and current inequities.
Data Limitations
Although the statistics on racial and ethnic inequities in health outcomes are striking, they are complicated by problems such as inaccurate and missing data within and between minimum Office of Management and Budget (OMB) race and ethnicity categories. For example, for Native Hawaiian and Pacific Islander populations, aggregation of data under broad categories, such as “Asian,” “Asian and Pacific Islander,” or “Asian, Native Hawaiian, and Pacific Islander,” masks the complexity of the challenges faced by these different populations. Given these limited and inaccurate data, the committee relied on a range of information to form a fuller understanding of the mechanisms that result in health inequities for these populations.
Role of Communities
Community voice and expertise have been critical for creating and implementing strategies to advance health equity, allowing many communities to flourish despite barriers. Including community leaders and organizations in the development and execution of federal policies that contribute to health equity is a key theme in this report. Although community participation is
___________________
5 Centering equity means prioritizing the needs of racially and ethnically minoritized populations and considering the consequences of current and future policies for advancing or impeding health equity.
frequently touted as a value in policy making and program design processes, specificity is often lacking as to what constitutes community engagement or inclusion. These processes also typically lack accountability mechanisms to ensure meaningful community input.
Committee Approach
The committee’s task was extremely broad, as many factors contribute to health inequities (see Figure S-1 and Box S-1). The committee could not review every relevant federal policy and program in the year it had to develop its report. To focus its review, the committee prioritized policies that (1) impact a large percentage of racially or ethnically minoritized populations; (2) have a body of literature or available data to assess them based on race and ethnicity; (3) continue to cause harm, based on the literature, even if those policies are historical; (4) illustrate how data gaps could fail to document health inequities (given that data gaps for these populations are well documented); and (5) were informed by available expertise from both the committee and invited speakers, verbal public comment at information-gathering meetings, and written public comment. Based on a combination of these considerations, the committee used its expert judgment to choose the policies to review and examined how they affected (both positively and negatively) racial, ethnic, or tribal health equity, with a focus on policies and programs controlled or influenced by the executive and legislative branches of the federal government.
The committee had to make difficult decisions regarding which policies to highlight in this report; omitting one does not mean it is any less important. Furthermore, the committee builds on the abundance of high-quality, evidence-based, and peer-reviewed reports from the National Academies and other organizations that have laid out the evidence for the root causes and mechanisms of health inequities or provided recommendations for specific federal actions to advance health equity. The topics, policies, and programs reviewed include the following:
- Economic Stability: The effect of incarceration and pretrial detention on income and wealth; the federal minimum wage; federal social benefit programs (e.g., Supplemental Nutrition Assistance Program [SNAP]); nonprofit sector partnerships; policies to support savings and wealth accumulation, such as baby bonds; and access to safe and affordable banking services, such as bank accounts and low-cost credit.
- Education Access and Quality: The Every Student Succeeds Act, the Individuals with Disabilities Education Act, the Higher Education Act, Section 504 of the Americans with Disabilities Act; early
- childhood education programs, such as Head Start; K–12 school spending/funding; school-based programs (e.g., health centers and meals programs); and higher education programs (e.g., Pell Grants and minority serving institutions).
- Health Care Access and Quality: Medicaid and the Children’s Health Insurance Program; policies and practices related to health literacy and language access; value-based payment; inclusion in clinical trials and the workforce; the Indian Health Service [IHS]; and maternal, territorial, and immigrant health.
- Neighborhood and Built Environment: Housing insecurity and segregation (e.g., redlining, housing on American Indian and Alaska Native [AIAN] reservations and for Native Hawaiian people, and federal rental assistance); disinvestment in infrastructure and the built environment (e.g., policies related to water, transportation, and aging and green infrastructure); environmental exposures that threaten health outcomes and well-being, particularly in the workplace (e.g., the Worker Protection Standard and exposure to pesticides); and food access and production (e.g., the Farm Bill and Food Distribution Program on Indian Reservations).
- Social and Community Context: Violence, public safety, and the criminal legal system, such as waiting periods for gun purchases, policies that increase accountability in policing and data collection, mass incarceration policies (e.g., long and mandatory minimum sentences); policies that acknowledge and provide redress for historical actions, practices, laws, and policies that caused enduring harm; and policies that build civic engagement and a sense of community and belonging.
Advancing health equity (or equity in areas that impact health, such as the environment, housing, and economic well-being) has garnered much attention recently from philanthropies, nonprofit organizations, and federal, state, and local governments. These efforts are described in this report, including Executive Order (EO) 13985, Advancing Racial Equity and Support for Underserved Communities Through the Federal Government, and the Equitable Long-Term Recovery and Resilience (ELTRR) plan released in November 2022. The committee built on these and other efforts and analyses in its report.
ACTION STEPS TO ADVANCE HEALTH EQUITY
Based on its review, the committee provides 36 conclusions in the five SDOH categories on their connection to health and conclusions for many of the reviewed policy areas (see Summary Annex for a listing of all
report conclusions). The committee identified four action6 areas through which the federal government can better support states, localities, tribes, territories, and communities to advance health equity.
- Implement sustained coordination among federal agencies;
- Prioritize, value, and incorporate community voice in the work of government;
- Ensure collection and reporting of data are representative and accurate; and
- Improve federal accountability, enforcement, tools, and support toward a government that advances optimal health for everyone.
On the path to eliminating health inequities, both short-term strategies (e.g., mitigation by getting people what they need now to thrive) and long-term structural and system change strategies that address the root causes (e.g., employment and economic development) will be needed. This report provides 13 recommendations for action with the goal of not only increasing access to important programs but also improving the effectiveness and coordination of government programs and policies. Several recommendations build upon actions underway in the federal government, as described in this report, and could be implemented in the short term. Additional details and considerations for each recommendation are available in Chapter 8.
Action 1: Implement Sustained Coordination Among Federal Agencies
The federal policy landscape is complex, with over 100 agencies in the executive branch, and the legislative and judiciary branches. Many federal policies affect health even if that is not their main focus. Coordination among federal agencies is critical to advance health equity. Some collaborative efforts are currently underway, such as the interagency ELTRR plan.
The importance of a whole-of-government approach to advance equity is central to EO 13985. Similar to a Health in All Policies approach, the committee recommends a parallel “whole person” and “whole community” approach. Just as health equity is not just about health care
___________________
6 Barriers and opportunities related to these action areas are discussed in this report. Chapter 1 provides important background and context, and Chapter 2 discusses the connection between health equity and history, federal policy, and data. Chapters 3–7 review federal policies in specific SDOH areas—each providing an overview of its connection to health outcomes and inequities and a review of specific past or current policies that have implications for health equity.
access and quality, it is the responsibility of not only the Department of Health and Human Services (HHS) but also multiple agencies that affect individual health and well-being. Therefore, achieving racial, ethnic, and tribal health equity requires centering equity in federal policy creation, decision making, implementation, and regulation, such as through accountability standards, across the board.
The ELTRR plan includes 10 crosscutting recommendations to address agency coordination and infrastructure in service of eliminating inequities. However, changing systems and organizations is challenging—the problems often persist because of complex interdependencies, where solving one aspect reveals or creates new challenges. In addition, federal programs can have different legal responsibilities, many of which cannot be easily coordinated around or may need to be rethought through new legislation. Furthermore, advancing equity typically involves complex, long-term change management that requires sustained attention.
Recommendation 1: To improve health equity, the president of the United States should create a permanent and sustainable entity within the federal government that is charged with improving racial, ethnic, and tribal equity across the federal government. This should be a standing entity, sustained across administrations, with advisory, coordinating, and regulatory powers. The entity would work closely with other federal agencies to ensure equity in agency processes and outcomes.
Multiple options to configure this entity exist, with pros and cons as described in this report.
Leadership for the Equitable Long-Term Recovery and Resilience Plan
A major component of the ELTRR plan is establishing an executive steering committee to guide and compel coordination across federal agencies at multiple levels. The group is expected to be composed of senior executive leaders from a significant number of representative departments and agencies; the Assistant Secretary for Health and one non-HHS agency lead (to be determined) will serve as cochairs. The committee affirms the crucial role of the executive steering committee:
Recommendation 2: The president of the United States should appoint a senior leader within the Office of Management and Budget (OMB) who can mobilize assets within OMB to serve as the cochair of the Equitable Long-Term Recovery and Resilience Steering Committee.
This configuration is ideal because unlike HHS, OMB has the capacity and authority to oversee the implementation of the ELTRR plan across the executive branch, including overseeing agency performance.
Equity Audit and Scorecard
When policies and budgets to address racial, ethnic, and tribal health equity are designed and policy alternatives reviewed, data are needed for Congress to better prioritize and debate their potential to address or exacerbate inequitable outcomes. Scoring legislation for its effect on racial, ethnic, or tribal equity is not currently required. Without sufficient data or analysis to understand the disparate effects of policies across racial and ethnic groups, policies are often adopted that inadvertently reinforce inequities.
If a health equity coordination entity is created per Recommendation 1, it could oversee and coordinate this process; however, such an entity is not required to implement this recommendation. The equity audit of existing federal policies in Recommendation 3b would build on the work by federal agencies under EOs 13985 and 14091, which direct each
one to develop a health equity team to implement its equity initiatives. An important consideration for those implementing this recommendation is how accountability will be ensured after audits are conducted. For example, if a policy does not meet the equity criteria, a plan should be developed and put in place to ensure needed changes are enacted; action would also need to be taken if lack of enforcement was identified as contributing to inequity (e.g., enforcing civil rights protections). Regarding Recommendation 3c, various mechanisms can be used for the scorecard and could vary based on available data, evidence, and process. However, legislation is the “bare bones” of a policy or program, and implementation through regulations and adjustments in the field to address unanticipated complications determine its impact. Therefore, even when an equity score is applied to proposed legislation, an equity audit would still be required after implementation. Although existing policies could be audited in the short term, the equity scorecard for proposed legislation will likely require more advance planning to implement. The report discusses additional details, including potential categories of metrics and other important considerations.
The implementation of Recommendations 1, 2, and 3 will help ensure the equitable and effective distribution of resources and signal that racial, ethnic, and tribal equity is a national priority and advance equity in domestic policy development, implementation, and evaluation across domains including health, economic security, the criminal legal system, and education.
Action 2: Prioritize, Value, and Incorporate Community Voice in the Work of Government
It is essential to base federal policy for all SDOH on the best available evidence—this includes communities’ experiences, knowledge/expertise, and needs. The reasons to value, prioritize, and incorporate community voice in the work of government are ethical and practical and include accountability and the achievement of intended outcomes. Affected communities need to be an integral part of the legislative process from beginning to end, as well as part of the process to decide how laws, regulations, programs, and policies are administered. Racial, ethnic, and tribal communities have been consistently left out of the federal policy-making process, and the effects have sometimes been egregiously inequitable. Community voices are needed to redress past harms; earn trust; secure partnership, buy-in, and collaboration; and ensure policies are fully responsive to their needs and advance health equity. A promising strategy to improve policies that do not currently
promote health equity is to elevate and empower community voice and expertise to influence outcomes through the following design principles:
- Prioritize meaningful community input by moving past simply keeping communities informed about policy and toward a more substantive level of input that involves consultation, involvement, collaboration, and empowerment whenever possible;
- Ensure effectiveness, efficiency, and equity in the way that community input is collected;
- Maximize coordination and sharing of information and insights on implementation across federal agencies while maintaining data privacy and client confidentiality; and
- Within each federal agency, maximize coordinating and sharing information and insights on implementation among federal, state, local, and tribal government counterparts.
Although there are many technical and scientific advisory bodies at federal departments and agencies, few recognize the unique perspectives of communities—including the recipients and beneficiaries of federal programs and services—as “expertise” and (lived) experience as essential for designing, implementing, and evaluating those programs and services.
As described in this report, several mechanisms for community input at the federal level are available to learn from, improve, and/or implement more broadly, such as community engagement associated with the decennial census, the White House Initiative on Asian Americans and Pacific Islanders Regional Interagency Working Group, and the Tribal Consultation and Urban Confer.
Action 3: Ensure Collection and Reporting of Data Are Representative and Accurate
To advance health equity, data need to better capture the experiences and needs of tribal and smaller racial and ethnic groups. A lack of representation in data collection, and sharing inaccurate or imprecise data about these communities, has meant that government agencies have been unprepared to understand, let alone reduce or eliminate, health inequities. High-quality data are required to understand the full extent of inequities and appropriately distribute resources. Federal government data collections have occurred without accountability or consideration of their effects and demands on communities (e.g., time and other resources), matters of tribal sovereignty, and community interest in the use of the data.
Data Equity for Small Minimum Reporting OMB Categories
Sample sizes in national surveys are often too small to obtain high-quality, reliable, nationally representative estimates required to monitor issues of health equity for all the minimum reporting OMB categories of race and ethnicity. The issues are more pronounced the smaller the category or survey. Omitting data for these minimum reporting OMB categories perpetuates inequities and promotes inaction—particularly when people are invisible in federal datasets. The data collected on these smaller minimum OMB categories are often biased due to incomplete representation, poorly designed sampling frames, inadequate collection approaches, language barriers (including failure to administer instruments in a person’s primary language), and culturally inappropriate question design.
Recommendation 5: The Office of Management and Budget (OMB) should require the Census Bureau to facilitate and support the design of sampling frames, methods, measurement, collection, and dissemination of equitable data resources on minimum OMB categories—including for American Indian or Alaska Native, Asian, Black or African American, Hispanic or Latino/a, and Native Hawaiian or Pacific Islander populations—across federal statistical agencies. The highest
priority should be given to the smallest OMB categories—American Indian or Alaska Native and Native Hawaiian or Pacific Islander.
Although there are barriers to expanding sample sizes and collecting data on small or geographically remote populations (e.g., cost, data reliability, privacy), expanding sampling frames to generate statistically reliable estimates of the population at varying levels of geography is important for policy and program development. Decisions to do so will need to consider several factors, such as population size, the magnitude of the disparity based on scientific research, and cost and feasibility.
Detailed-Origin Categories and Data Disaggregation
Each OMB minimum reporting category has important differences based on origin and/or tribe. The need to collect and disseminate data at this level of disaggregation for racial and ethnic groups has been discussed for decades. Recently, the Census Bureau has made positive strides, and many others have provided recommendations for accomplishing this goal. This need is recognized across multiple racial, ethnic, and tribal populations. In addition to disaggregation for minimum category OMB groups by origin and/or tribe, these communities have many important intersecting identities, including communities of lesbian, gay, bisexual, transgender, queer (or questioning), and other sexual identities people, people of varying immigration statuses, people with disabilities, women, and children.
Recommendation 6: The Office of Management and Budget (OMB) should update and ensure equitable collection and reporting of detailed-origin and tribal affiliation data for all minimum OMB categories through data disaggregation by race, ethnicity, and tribal affiliation (to be done in coordination with meaningful tribal consultation), including populations who self-identify as American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Pacific Islander, and Hispanic or Latino/a.
In January 2023, OMB released a Federal Register notice with proposed changes to the collection of data on race and ethnicity. Several of the proposed changes are generally in line with the committee’s recommendation (see report for more details). The report provides important considerations, including data privacy, checkboxes versus write-ins on surveys, expanding sampling frames to generate accurate statistical information on detailed-origin groups, and decisions regarding allocating resources to collect, analyze, and disseminate detailed origin with a view toward equity.
Measures of Social and Structural Inequities
Without proper social and environmental context, racial and ethnic health inequities may be incorrectly interpreted as the result of individual-level biological and behavioral factors, blaming individuals and groups for poor health outcomes. Including measures of racialized social and structural inequities at multiple levels of influence in national health surveys and other federal health data sources can facilitate contextualizing health inequities data and promote investigation of the effects of social and structural factors on these inequities.
Recommendation 7: The Centers for Disease Control and Prevention should coordinate the creation and facilitate the use of common measures on multilevel social determinants of racial and ethnic health inequities, including scientific measures of racism and other forms of discrimination, for use in analyses of national health surveys and by other federal agencies, academic researchers, and community groups in analyses examining health, social, and economic inequities among racial and ethnic groups.
Such measures should pertain to racism and other forms of discrimination and include social, economic, educational, political, and legal indicators in a range of societal domains as well as measures of interpersonal racism, individual-level experiences of structural racism, and sociocontextual measures of structural racism (see the full report for examples). These measures should be usable at the state, county, and neighborhood levels and developed in partnership with academic researchers, community groups and members, and other key stakeholders. Some of this work is already underway, and the health equity coordinating entity recommended by the committee (Recommendation 1) could facilitate these efforts.
Budget Needs
Oversampling and targeted data collection are admittedly costly. However, identifying health, socioeconomic, and environmental inequalities, which negatively affect outcomes for these groups across the life span is essential for determining solutions to achieve health equity goals. Furthermore, context on social factors when interpreting racial and ethnic health inequities is crucial to understand the multiple levels of influence that impact health outcomes.
Recommendation 8: Congress should increase funding for federal agencies responsible for data collection on social determinants of health
measures to provide information that leads to a better understanding of the correlation between the social environment and individual health outcomes.
These data will more accurately indicate the specific needs of underserved populations and improve overall equity in health and socioeconomic outcomes by identifying where policy change or interventions are needed to inform government investments to advance health equity.
Equitable Data Working Group
In April 2022, the Equitable Data Working Group (established under EO 13985) developed a report with recommendations for improvements in data equity and identified inadequacies in federal data collection programs, policies, and infrastructure across agencies. To ensure that this important work is enduring, the committee recommends:
Recommendation 9: The president of the United States should convert the Equitable Data Working Group, currently coordinated between the Office of Management and Budget (OMB) and the Office of Science and Technology Policy, into an Office of Data Equity under OMB with representation from the Domestic Policy Council, with an emphasis on small and underrepresented populations and with a scientific and community advisory commission, to achieve data equity in a manner that is coordinated across agencies and informed by scientific and community expertise.
To benefit from the guidance of scientific and community experts, the federal government should make interagency coordination on data equity a permanent feature of its work across statistical agencies. By situating the Office of Data Equity under OMB, the federal government will be able to ensure cross-agency coordination and collaboration on data improvements that advance health equity in all federal agencies and policies.
Action 4: Improve Federal Accountability, Enforcement, Tools, and Support Toward a Government That Advances Optimal Health for Everyone
Although states and other levels of government need to tailor their health equity efforts to the needs of their populations, they need the federal-level tools and support to do so. Often, politics can stand in the way of or stall good policy, so processes and guardrails are needed to support state, local, tribal, and territorial needs. For example, guidance that
has been vetted for health equity effects at the federal level needs to be in place for the implementation of policies and access requirements and to set expectations. Accountability mechanisms and processes can play a vital role in driving progress for health equity and require engaging with multiple diverse actors using dynamic accountability processes.
Program Implementation and Access
The committee’s review illustrates numerous examples of barriers in implementation and access to federal programs that exacerbate inequities, such as administrative burden. In addition, state variation in program implementation (such as in Medicaid expansion and participation in social benefits programs, such as SNAP) can lead to differential access based on geography. Equitable implementation supports government efficiency and effectiveness and can decrease inequities and improve outcomes for all.
This recommendation builds on work already in progress by federal agencies to identify mechanisms to reduce administrative burden for underserved communities. To enable agencies to leverage the full extent of their authorities, additional funding may be needed—for example, for enforcement of civil rights protections.
Eligibility for Federal Program and Services
Access to federally funded programs for all people in the United States who meet requirements is essential to move toward health equity. For example, formerly incarcerated people and immigrants have restricted
access to social service programs and incarcerated people cannot use Medicaid coverage; immigrants are not eligible for Medicaid until they have completed 5 years of legal U.S. residence. To increase access to federally funded programs for those who are categorically excluded, the committee recommends:
Recommendation 11: The president of the United States should direct the Office of Management and Budget to review federal programs that exclude specific populations, such as immigrants and those with a criminal record and, in some cases, currently incarcerated people (e.g., Medicaid coverage), to assess the rationale and implications for equity of excluding these populations, including potential impacts on their families and communities. A report on the findings and suggested changes (when applicable) should be made publicly available.
The pros and cons, including cost and health equity implications, should be weighed for each excluded category in federally funded programs.
Advance American Indian and Alaska Native Health Equity
Although the committee was expansive in its attempt to incorporate all minoritized racial, ethnic, and tribal communities impacted by federal policies, it paid special attention to AIAN communities, who are often overlooked in large national reports. For most measures of health, AIAN people are worse off than other racial and ethnic groups; this includes life expectancy, suicide, homicide, and chronic diseases resulting in earlier and increased functional disability and death. As detailed in this report, the United States has a complex relationship with this population. A critically important aspect is that the 574 federally recognized tribes are sovereign nations and have a formal nation-to-nation relationship with the U.S. government with a trust responsibility that has not been fully upheld. The traumas that have unfolded over generations have resulted in untold cumulative harm, the effects of which are still being felt. Federal responsibility for AIAN health care was codified in 1976 to form the legislative authority for the IHS, which receives less funding per person than Medicaid, Medicare, Veterans Affairs, or federal prisons. Furthermore, AIAN voices in federal leadership and influence in the executive and legislative branches have been few, although several notable appointments were made recently.
Although these actions will not address all barriers to health equity for the AIAN population, together, they will give more voice and prominence to AIAN people, which will help advance health equity for a population that is ignored and inadequately resourced.
Health Care Access
One major barrier to health equity is health care access, which includes health insurance coverage and the availability of and access to culturally appropriate, high-quality care, including preventive care, primary care, specialist care, chronic disease management, dental and vision care, mental health treatment, and emergency services. Lack of access to health insurance leads to adverse health outcomes and negative economic effects that exacerbate racial and ethnic inequities. However, health insurance is just one piece of the equation. Increasing access to high-quality, comprehensive, affordable, accessible, timely, respectful, and culturally responsive health care would advance racial and ethnic health equity.
Recommendation 13: The Departments of Health and Human Services, Defense, Veterans Affairs, Homeland Security, and Justice, as federal government purchasers and direct providers of health care, should undertake strategies to achieve equitable access to health care across the life span for the individuals and families they serve in every community. These strategies should prioritize access to effective, comprehensive, affordable, accessible, timely, respectful, and culturally appropriate care that addresses equity in the navigation of health care. While these strategies have a greater chance of success when everyone has adequate health insurance, there are ways the executive branch can improve and reinforce access to care for the adequately insured, the underinsured, and the uninsured.
There are a multitude of approaches that federal agencies can use to achieve this outcome, including ensuring access to health insurance coverage, primary care, enhancing inclusivity of language and communication/health literacy, engendering trust in the health care system, and other innovations. Although it is not a panacea for health care access, health insurance coverage remains critical for all individuals residing in the United States. Examples of mechanisms to increase access include persuading nonexpansion Medicaid states to adopt federal financial support for their uninsured residents and federal directed strategies. The committee notes that AIAN people have a legal right to quality physician-led health care under treaty and trust responsibility. Further integration across the federal health system will also help achieve this recommendation—implementing Recommendation 1 would facilitate the needed integration.
CALL TO ACTION
This report points to both the positive and negative impacts federal policy has had on racial, ethnic, and tribal health equity. Although federal policy has played an important role in correcting past harms and advancing equity, substantial opportunities remain. The four action areas outlined in this report are connected and impact each other. For example, without representative and accurate data, it is difficult to identify where resources and tools are needed and policy efforts should be focused. Lack of community voice and expertise in policy development can lead to blind spots and cause unintended consequences. Staying vigilant for such unintended consequences of implemented policies is essential and needs to be built into feedback monitoring loops and measured in equity audits. Furthermore, as the federal government works to advance health equity, it should keep front and center the guiding principles in this report. Federal policy can play a key role in eliminating health inequities by collecting and employing accurate data, doing a better job of including and empowering communities who are most impacted, and coordinating and holding those who implement policy accountable. Implementing this report’s recommendations will improve the circumstances in which people, families, and communities live, play, work, pray, and age so that all people living in the United States have the opportunity to meet their full health potential.




















