
3
EVIDENCE GENERATION RETURNS-ON-INVESTMENT
A question for health delivery systems is how to justify evidence generation from the standpoint of returns on investment (ROI). This question is also relevant to the funding of a national data infrastructure. In this session, Kate Goodrich, director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), discussed the value of research and data infrastructure to health and health care, describing the CMS Transforming Clinical Practice Initiative (TCPI) as an example of evidence-based quality improvement that rewards value. Peter Pronovost, senior vice president for Patient Safety and Quality at Johns Hopkins Medicine, described the reduction of central line–associated bloodstream infections (CLABSI) as a case example of the spread and scale of knowledge to advance policy and practice and improve outcomes. Thomas Carton, principal investigator at the Research Action for Health Network (REACHnet) and the Louisiana Public Health Institute, described the REACHnet process as an example of one Clinical Data Research Network’s (CDRN’s) approach to this problem. An open discussion followed the presentations. Highlights and main points of this session are summarized in Box 3-1.
THE VALUE OF THE RESEARCH AND DATA INFRASTRUCTURE
The ROI of evidence generation should be better outcomes at lower cost. CMS has long been involved in the improvement of care. Since the passage of the Patient Protection and Affordable Care Act, CMS has been working to help frontline clinicians improve care and transform the care delivery system to meet the three aims of better care, smarter spending, and healthier people. To meet these aims, CMS is focusing on three key areas: incentives, care delivery, and information. Changing the incentive structure includes promoting
value-based payment systems and transforming from fee-for-service to alternative payment models. CMS is doing this through a number of mechanisms, working with both the public and private sectors to test new models and bring proven models to scale. The focus on care delivery involves encouraging the integration and coordination of care and services; improving communication; improving population health; and meaningfully engaging patients, families, and caregivers in their care through shared decision making. Fundamental to transforming the care delivery system is improving how information is shared and distributed. Goodrich noted the need to create transparency on cost and quality information, and to bring electronic health information to the point of care for meaningful use.
In 2015, the US Department of Health and Human Services established specific goals for the Medicare program’s move toward value, and invited commercial payers and states to share in these goals (Burwell, 2015). The first goal, set for the end of 2016, was for 30 percent of Medicare payments to be tied to quality and value through alternative payment models where providers are held accountable for patient outcomes and cost of care. By the end of 2018, the goal is for 50 percent of Medicare payments to be through such alternative payment models. The second goal was for 85 percent of Medicare fee-for-service payments to be tied to quality and value by the end of 2016, reaching 90 percent of payments tied to quality and value by the end of 2018.
The CMS Transforming Clinical Practice Initiative (TCPI)
These goals compelled providers to improve outcomes for patients and to lower costs, and CMS recognized the need to provide support and tools for hospitals, doctors, and other frontline clinicians to help them achieve these goals. In 2015, CMS launched TCPI, a quality improvement initiative to help clinicians transform their practice and transition into alternative payment models. Nearly $700 million has been awarded by TCPI to support transformation.
The seven goals of TCPI, as outlined by Goodrich, are to
- support more than 140,000 clinicians in their practice transformation (Goodrich noted that 140,000 clinicians is the starting point and that there are about 1.3 million frontline clinicians that participate in the Medicare program);
- improve health outcomes for millions of Medicare, Medicaid, and Children’s Health Insurance Program beneficiaries and other patients;
- reduce unnecessary hospitalizations for five million patients;
- generate $1 billion to $4 billion in savings to the federal government and commercial payers;
- sustain efficient care delivery by reducing unnecessary testing and procedures by focusing on appropriate use of testing and diagnostics;
- transition 75 percent of practices completing the program into alternative payment models; and
- build the evidence base on practice transformation so that the solutions can be scaled.
Within the TCPI, there are five phases of transformation for practices. In the first phase, practices set very specific aims for how they want to improve. Next, practices are taught how to use data to drive improvement at the point of care. In the third and fourth phases, practices achieve progress on the aims they have set and achieve specific benchmarks that CMS sets for each of those aims. In the final phase, the goal is for the practice to thrive as a business through pay-for-value approaches.
TCPI has awarded contracts to two different types of networks: Practice Transformation Networks and Support and Alignment Networks. Practice Transformation Networks are organizations that provide “on-the-ground” technical assistance to clinician practices to help them understand where there is existing evidence on how to improve care in a particular area and how to collect data and generate evidence on how to improve care. Support and Alignment Networks help practices to align their multiple programs (e.g., continuing medical education, maintenance of certification, registries, and other requirements) with the aims of TCPI.
Overall, the TCPI model aims to transform practice, improve health outcomes, reduce unnecessary utilization, scale effective solutions, achieve savings, and reward value. Goodrich reemphasized that a major goal of the program is to build the evidence base for practice transformation so that these solutions can be scaled if they are found to be successful. She also emphasized the importance of collaboration and information sharing among all of the quality improvement networks that CMS supports. What works within a hospital may or may not work within an individual practice or a treatment facility.
SCALE AND SPREAD: A NETWORK OF CONTINUOUS LEARNING
Eliminating harm is an iterative process, and there have been many learning cycles over the years. When the landmark Institute of Medicine report To Err Is
Human was published (IOM, 2000), central line–associated bloodstream infections (CLABSIs) were so common that they were practically the norm, Pronovost noted. To emphasize the point, he mentioned the case of a young girl who died in his hospital of catheter infection around that time, and the root-cause analysis did not even mention her central line infection. But cases like hers challenged the medical professions and the country to eliminate these infections.
Fifteen years later, rates of CLABSI in intensive care units have been reduced by over 80 percent in all types of hospitals across the United States, in both children and adults (Pronovost et al., 2015). Pronovost and colleagues described this as a remarkable success story, and he reflected on what allowed this to happen, first at a policy level, and then at the local health system level.
Improvement Science
The science of improvement starts with the end goal (i.e., improved outcomes) and works backward (Dixon-Woods et al., 2013; Marshall et al., 2013). Improvement science involves both basic and applied science, but it is focused on solving specific problems. It requires partnerships among researchers and providers and is informed by transdisciplinary teams from medical and social sciences. Improvement science uses multifaceted interventions and employs mixed-methods evaluations to learn not just whether an approach worked, but why and how it worked so that it can be scaled and spread.
Pronovost and colleagues studied the improvement in the rates of CLABSI and identified five elements that contributed to this success at the national policy level (Pronovost et al., 2015). First, efforts at improvement used a reliable and valid measurement system that clinicians believed. He noted that CLABSI is one of the few harms for which there are valid measures. Efforts also relied on decades of National Institutes of Health (NIH) and Centers for Disease Control and Prevention basic and clinical research to identify strategies to reduce infections and develop guidelines and checklists for clinicians. There were investments by the Agency for Healthcare Research and Quality and others in implementation science to understand how to change behavior at the bedside. There were also “cascading structures” that supported peer learning communities and data collection. Finally, stakeholders were aligned and synergized their transdisciplinary efforts around a common goal and measure (the reduction of CLABSI).
To understand improvement at the provider level, Pronovost and colleagues employed an approach called peer-to-peer review, where social scientists and clinicians visited high- and low-performing institutions. While on the surface it might have appeared that the use of an implementation checklist created for clinicians was the solution, the reality was more complex, and they identified a
series of explicit requirements for improved performance. First, it was essential that the board and the CEO declare a goal of zero infections and communicate that broadly across the organization. It was also essential that leadership create an enabling infrastructure, with staff to coordinate project management, data, improvement science, and training to support clinicians. Frontline clinicians were engaged and connected in peer learning communities, and data were transparently reported to create a system of shared leadership accountability. This is accountability “from board to bedside,” Pronovost explained, where leaders, before holding clinicians accountable, must first ask themselves if they have provided the clinicians with the elements needed to succeed (e.g., clear goals, skills, time, and data). Finally, a key element of transformation was telling a new story. The old story was that harm was inevitable, and clinicians did not feel empowered to change the outcome. However, when clinicians felt they could succeed, this created intrinsic motivation. Importantly, the clinical community structure supported peer learning, and clinicians had a new story to tell, one that said that CLABSIs are preventable.
Applying Lessons to Broadly Eliminate Harms
How might these lessons from the approach to CLABSI reduction be applied to eliminate all harms across the health system? The first step, Pronovost suggested, is to create a governance and leadership system for quality that functions similarly to that for finance. There is one line of oversight of every dollar spent in a complex organization. Could a similar structure be created for quality of care?
Pronovost described applying the lesson of clinical communities to the health system. Health system clinical communities are clinician led, and their charge is to achieve the purpose of the health system: to help patients thrive; to prevent disease when possible; to cure when you cannot prevent; to care when you cannot cure; and, all along, to respectfully and empathetically partner with patients and their families to end preventable harm, continuously improve patient outcomes and experience, and eliminate waste. The institute serves as the enabling infrastructure to improve quality in the system, and to link operations, research, and training. One of the challenges, he noted, is financing this infrastructure and analytics and demonstrating the ROI.
Pronovost shared an example where building a capacity for improvement saved over $50 million in supply costs. Supply chain savings rely heavily on what clinicians use. The clinical communities added driving down supply costs to their purpose, under the conditions that physician choice was maintained and that some of the savings went to support comparative effectiveness research, analytics, and implementation. This combining of research and operations has been very successful.
The PCORnet Health Systems Demonstration Project
In preparation for this National Academy of Medicine (NAM) meeting, PCORI provided support to PCORnet CDRNs to engage health system leaders, and to work jointly to identify and prioritize a set of data-driven research activities of high interest to health systems and clinicians. The CDRNs were guided in their research topic selection by five principles: (1) topics should be rated as priorities by CEOs and health system leaders; (2) selection should involve iterative review and discussion between researchers and health system leaders; (3) the research should be of interest and add value to at least two PCORnet health systems; (4) projects should leverage existing data resources (e.g., PCORnet and the Common Data Model) with or without additional health system data; and, finally, (5) projects should be able to be completed in less than 1 year.
Carton described the Research Action for Health Network (REACHnet) CDRN approach to engaging health systems in defining the three research questions that REACHnet would bring to this NAM meeting for discussion. He emphasized that REACHnet is one of 13 CDRNs participating in this PCORI process and that the CDRNs employed a diverse array of methods to achieve the same goal of identifying research questions for discussion and prioritization at the NAM meeting. REACHnet is a network of health systems containing clinical records for more than 3 million patients in Louisiana and Texas. The network is focused on facilitating patient-centered, comparative effectiveness research. Partners include Ochsner Health System, Tulane University Medical Center, Louisiana State University and the Pennington Biomedical Research Center, Baylor Scott & White Health, and the Partnership for Achieving Total Health (a community-based health information exchange of 12 federally qualified health centers in the greater New Orleans area).
REACHnet, and all the CDRNs, seek to transform the culture of research by engaging patients, caregivers, and the broader health community in the research process, from idea generation to translation and dissemination. This is a three-phase approach. The first phase is topic solicitation, prioritization, and framing of the question, and Carton pointed out that this NAM meeting is part of the first phase. Next is selection of comparators and outcomes, conceptual frameworks, analysis plan, and data collection. The last phase is review of data, interpretation of results, translation, and dissemination.
Research question formation is a stakeholder-led approach. REACHnet brings together researchers, health system leaders, patients, clinicians, payer groups, and community health activists and workers, and creates a safe space for discussions,
learning together, and collaboration, with the ultimate goal of establishing PCORI research priorities and pursuing funding opportunities.
Identifying Research Needs on the Ground
The REACHnet Health Systems Demonstration Project engaged 38 unique stakeholders, including health system leaders (CEOs, chief medical officers, a chief quality officer, and systems vice presidents), patient representatives, clinicians, researchers, a medical student, payer representatives, and community health advisory board members, coordinated by staff from the REACHnet Coordinating Center.
The process spanned 6 months, from June 2015 until December 2015, and engaged different stakeholders at different events across three phases: generation, prioritization, and refinement (see Figure 3-1). In the generation phase, an administrative board of health systems leaders and payer representatives met to set goals and objectives and brainstormed ideas that would value system collaboration, use data outside of individual systems, and leverage the community that REACHnet brings. Twelve potential topics were selected. A community health advisory board (CHAB), including patients, participated in the prioritization phase and narrowed the dozen ideas down to three. These three ideas were then refined, and the research questions for discussion at this NAM meeting were finalized.
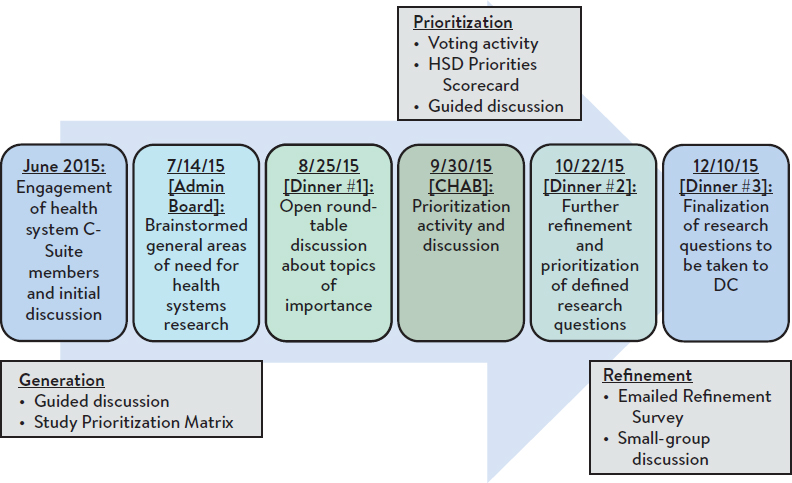
NOTE: HSD = Health System Demonstration
SOURCE: Carton presentation, January 21, 2016.
A number of tools were leveraged throughout the process. At the generation phase, a topic prioritization matrix was used by the two advisory-group boards to assess the feasibility of each of the 12 topics through various metrics such as congruence with the PCORnet Common Data Model and alignment with patient preferences, payer priorities, and national research priorities.
At the CHAB meeting, patients were oriented to the process, and three patients were selected by their peers to participate in the rest of the process. The patient orientation seminar highlighted the goals and objectives of the prior meetings, familiarized the patients with the process, and empowered them to participate and share their ideas. The prioritization process then employed a topic voting scorecard for those who were present and an online voting tool for those who were not. Finally, during the refinement process, REACHnet Coordinating Center staff presented a discussion guide and a literature review matrix, which allowed stakeholders to develop the topics into clear research questions. The final topics, research questions, and sample populations from the REACHnet process were then ready for discussion at this NAM meeting. (The REACHnet final topics are provided in Table 3-1; a summary of the discussion of all of the CDRN priority topics submitted for this meeting is provided in Chapter 4.)
TABLE 3-1 | REACHnet Final Topics
| TOPIC | QUESTION | SAMPLE |
|---|---|---|
|
Examine patterns of health care utilization 1 year prior to mortality to better understand comparative effects of advanced illness management/end-of-life care on patient health outcomes and resource utilization. | Patients with advanced illness who have died in the past year; condition-specific subsamples |
|
Evaluate the effects of multiple factors (change in mental health, medication regimen, etc.) on weight-loss maintenance after initial weight-loss success (e.g., postbariatric surgery). | Patients who experience a defined magnitude of weight loss during a specified time frame |
|
Compare the influence of postdischarge follow-up and encounter patterns postdischarge (e.g., time to followup and method of follow-up) on patient health outcomes. | All patients; condition-specific subsamples |
SOURCE: Carton presentation, January 21, 2016.
In closing, Carton highlighted several key points about the REACHnet process. The events took place over 6 months, which helped to increase stakeholder buy-in, dedication, and comfort. Multiple types of stakeholders contributed their unique perspectives, both independently (through CHAB and the Administrative Board) and collaboratively in larger groups (such as the dinner meetings). Numerous tools were used to collect and organize the ideas. The process was deemed worthwhile for the stakeholders. For example, the meet-and-greet sessions for networking before the dinners, proper compensation for patient partners, and the dinner meetings helped to create a community that was unified around the goals and objectives of the project. Finally, health system leaders were engaged both directly (through the meetings and discussions) and independently (via health system principal investigators), and they ultimately endorsed both the process and the findings (i.e., the three questions).
DISCUSSION
During the open discussion that followed, participants talked about the need for and benefits of synergy across networks and data systems, and increasing the focus on population health.
Synergy Among Networks and Data Systems
Participants pointed out the synergy between PCORnet CDRNs and CMS TCPI Practice Transformation Networks with regard to learning health systems. They also noted that one ROI for PCORnet is the ability to do research differently, moving away from traditional clinical trials and looking at common clinical data across multiple sites for comparative effectiveness. With PCORnet there is also an engaged community of stakeholders that can enable more rapid transformation of that evidence into practice.
Carton also commented on the design features of PCORnet for learning health systems. He mentioned the Health in Our Hands Patient Network, an initiative of REACHnet designed to engage patients in research. This registry incorporates a consent to contact that allows researchers to contact patients as clinical trials become available without having to go through the individual health systems. Another aspect is the ability for researchers developing a trial to query the database and connect to patients with particular characteristics who have agreed to be contacted. They are not being contacted to be research participants at that time, but to be part of the protocol development and grant writing.
John Gallin of NIH mentioned that the The All of Us Research Program (formerly the President’s Precision Medicine Initiative) is seeking to establish a
cohort of 1 million patients and noted that one of the challenges is integration with other data systems, perhaps through a common, national, clinical database. In response, Pronovost encouraged participants to think about broadening the lens beyond precision medicine to precision measurement. There will be other nonelectronic health record data of interest in addition to genomics (e.g., proteomics) and what is needed is a policy solution that will reduce the barriers to accessing data interfaces.
Increasing the Focus on Population Health
Gary Rosenthal of the University of Iowa asked about the infrastructure and partnerships that will be needed to drive population health improvements. He observed that prior CMS demonstration projects (e.g., Physician Group Practice Demonstration; Pioneer Accountable Care Organization [ACO] Model) have had relatively modest impact with regard to cost savings, which he said were about 1 percent per year. This is small relative to the potential, he commented. The findings of the Pioneer ACO project, for example, show that the only ACOs that were able to achieve cost savings were those located in high-cost areas of the country. Addressing population health requires a much broader framework and more consideration of the social determinants of health, as highlighted by Shah (see Chapter 2). Goodrich agreed with the need for an increasing focus on population health. She noted that there is a population health group within the CMS Innovation Center that is working on the Accountable Health Communities model and is also thinking more broadly about topics such as additional tests that could be done; how to integrate different partners within a community to improve population health; target metrics; and addressing the social determinants of health. Population health and community health are relatively new territories for CMS, but there is a tremendous amount of interest. There has also been more evidence generated from successes at the local and regional levels, where improvements have resulted, in part, from coordination across sectors. At a conceptual level, Pronovost observed, medical care, public health, personal health behavior, and community support still exist in silos, and clinical providers still see their role as medical care. He called for frameworks that can erase those silos and focus on helping people thrive in those different spaces. Moderator Larson referred participants to a recent NAM report on social and psychological determinants of health (NASEM, 2016) and noted that accountable care groups are beginning to recognize these domains in which they have to work.
This page intentionally left blank.












