
7
Respiratory Disease
Environmental exposures are the leading causes of respiratory disease worldwide. Exposures to tobacco smoke and household air pollution consistently rank among the top risk factors not only for respiratory disease burden but also for the global burden of disease (Lim et al., 2012). Less is known, however, about the attributable effects of cannabis use on respiratory disease despite shared similarities with that of cigarette use and the fact that cannabis is the most commonly used inhaled drug in the United States after tobacco, with an estimated 22.2 million people ages 12 years and older reporting current use (CBHSQ, 2015). Moreover, it is estimated that more than 40 percent of current users smoke cannabis on a daily or near daily basis (Douglas et al., 2015). Given the known relationships between tobacco smoking and multiple respiratory conditions, one could hypothesize that long-term cannabis smoking leads to similar deleterious
effects on respiratory health, and some investigators argue that cannabis smoking may be even more harmful than that of tobacco smoking. Indeed, data collected from 15 volunteers suggest that smoking one cannabis joint can lead to four times the exposure to carbon monoxide and three to five times more tar deposition than smoking a single cigarette (Wu et al., 1988). This may be, in part, because cannabis smokers generally inhale more deeply and hold their breath for longer than do cigarette smokers (Wu et al., 1988) and because cannabis cigarettes do not commonly have filters as tobacco cigarettes often do. On the other hand, cannabis cigarettes are not as densely packed as tobacco cigarettes (Aldington et al., 2008), and cannabis users usually smoke fewer cannabis cigarettes per day than tobacco users smoke tobacco cigarettes per day.
The committee responsible for the 1999 Institute of Medicine (IOM) report Marijuana and Medicine: Assessing the Science Base (IOM, 1999, p. 6) concluded that cannabis smoking was an important risk factor in the development of respiratory disease and recommended that “studies to define the individual health risks of smoking marijuana should be conducted, particularly among populations in which marijuana use is prevalent.” The literature search conducted by the current committee did not identify any fair- or good-quality systematic reviews for cannabis use and respiratory disease published since 2011 (the cutoff established by the current committee); however, the committee identified—and elected to include—a systematic review by Tetrault et al. (2007) that provides a detailed synthesis of the available literature through 2005. A review by Tashkin (2013) and a position statement by Douglas et al. (2015), which summarized current evidence of the link between cannabis smoking and respiratory disease, were also considered by the committee. Fourteen primary articles published since 1999 that were not included in the systematic review from Tetrault et al. (2007) provided additional evidence on the association between smoking cannabis and respiratory diseases (Aldington et al., 2007; Bechtold et al., 2015; Hancox et al., 2010, 2015; Kempker et al., 2015; Macleod et al., 2015; Papatheodorou et al., 2016; Pletcher et al., 2012; Tan et al., 2009; Tashkin et al., 2012; Van Dam and Earleywine, 2010; Walden and Earleywine, 2008; Weekes et al., 2011; Yadavilli et al., 2014).
PULMONARY FUNCTION
Pulmonary function refers to lung size and function. Common measures of pulmonary function include forced expiratory volumes, lung volumes, airways resistance and conductance, and the diffusion capacity of the lung for carbon monoxide (DLCO). Spirometry values include the measurements of forced expiratory volumes, including forced expiratory
volume at 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC. The latter is a measure of airflow obstruction and, when combined with bronchodilator therapy, is used in the diagnosis of chronic obstructive pulmonary disorder (COPD).
Is There an Association Between Cannabis Use and Pulmonary Function?
Systematic Reviews
Tetrault et al. (2007) systematically reviewed the evidence found in 34 publications, of which 12 reported on the effects of airway response and 14 reported on the effects of pulmonary function. The authors found that short-term exposure to cannabis smoking resulted in bronchodilation. Specifically, acute cannabis smoking was consistently associated with improvements in specific airway conductance, peak flow measurements, and FEV1, as well as reversed bronchospasm from challenges by either methacholine or exercise. Any short-term benefits, however, were offset by the effects of long-term cannabis smoking. Specifically, regular cannabis smoking was associated with a lower specific airway conductance on average by 16 percent and also with a lower FEV1. There was also a dose–response effect between average daily quantity of cannabis and a lower specific airway conductance. However, the clinical significance of the association between regular cannabis smoking and a lower specific airways conductance is not known. Other studies that examined the association between long-term cannabis smoke exposure and pulmonary function have inconsistently found lower or no change in FEV1, FVC, FEV1/FVC, DLCO, and airway hyperresponsiveness (Tetrault et al., 2007).
Primary Studies
Aldington et al. (2007) examined the cross-sectional relationship between long-term cannabis smoking and pulmonary function in a convenience sample of 339 participants in the Wellington Research Study. The inclusion criteria for cannabis and tobacco smokers were a lifetime exposure of at least 5 joint-years of cannabis (defined as smoking 1 joint per day for 1 year) or at least 1 pack-year of tobacco, respectively. Cannabis smoking was based on self-report. The researchers did not find an association between long-term cannabis smoking and pulmonary function variables. However, when cannabis smoking was analyzed in terms of joint-years, Aldington et al. (2007) found a significantly lower FEV1/FVC, lower specific airways conductance, and a higher total lung capacity per joint-year smoked in cannabis smokers compared to nonsmokers. Based
on their analyses, the authors estimated that the negative association between each cannabis joint and a lower FEV1/FVC was similar to that of 2.5 to 5 tobacco cigarettes. The committee identified a couple of problems with the analyses and the presentation of the results in the paper by Aldington et al. (2007). First, the authors reported main effects only from their analysis of covariance. A more conservative analysis would have considered the examination of interaction effects between cannabis smoke (or joint-years) and tobacco smoke (or pack-years) in a regression model to better dissect the contribution of cannabis smoke (or joint-years) versus tobacco smoke (or pack-years). Second, the authors incorrectly labeled the association with continuous measures of pulmonary function with cannabis smoke (or joint-years) as odds ratios (ORs) in tables 3 and 4; however, their methods correctly state that a multivariable analysis of covariance methods was used for continuous data.
Papatheodorou et al. (2016) analyzed cross-sectional data from 10,327 adults who participated in the National Health and Nutrition Examination Survey (NHANES) between 2007 and 2012. Cannabis smoking was based on self-report, but the researchers could not quantify joint-years. Cannabis smokers were categorized as never smokers (n = 4,794), past cannabis smokers (n = 4,084), cannabis smokers in the past 5–30 days (n = 555), and cannabis smokers in the past 0–4 days (n = 891). Current cannabis smokers were heavier tobacco smokers than were past and never smokers of cannabis, as measured by mean pack-years. In multivariable analyses, the investigators found that current smokers had a smaller FEV1/FVC than never smokers (−0.01 and −0.02, respectively), and they observed moderate to large increases in FEV1 (49 mL and 89 mL, respectively) and FVC (159 mL and 204 mL, respectively) when comparing current smokers to never smokers. There was also an important decrease in exhaled nitric oxide among current smokers when compared to never smokers (−7 percent versus −14 percent), but it is unclear if this effect was confounded by the high prevalence of tobacco smoking in current cannabis users or if it represented a true decrease in exhaled nitric oxide due to cannabis smoking. The study by Papatheodorou et al. (2016) has some shortcomings. First, the researchers’ analyses were based on cross-sectional data. Second, cannabis use was obtained by self-report and there may have been a bias of underreporting. Finally, there was a lack of data on the method of smoke inhalation and the frequency of cannabis smoking, thus not allowing for an analysis of the relationship between the frequency of cannabis use and pulmonary function.
Pletcher et al. (2012) analyzed longitudinal data from 5,115 adults in the Coronary Artery Risk Development in Young Adults (CARDIA) study and concluded that occasional and low cumulative cannabis smoking was not associated with adverse effects on pulmonary function. The
investigators noted that there was a trend toward decreases in FEV1 over 20 years only in the heaviest cannabis smokers (≥20 joint-years). Similar to the findings of Papatheodorou et al. (2016), CARDIA investigators found a higher-than-expected FVC among all categories of cannabis smoking intensity. Despite the large sample size, the study by Pletcher et al. (2012) had a small number of heavy cannabis smokers. Other limitations include the risk of bias due to the self-reporting of cannabis use, a lack of data on the method of cannabis smoke inhalation, and bias due to unmeasured confounders as cannabis smoking was not the main objective of this study.
The study by Hancox et al. (2010) analyzed data of a cohort of 1,037 adult participants in Dunedin, New Zealand, followed longitudinally since childhood and asked about cannabis and tobacco use at ages 18, 21, 26, and 32 years. Cumulative exposure to cannabis was quantified as joint-years since age 17 years. Spirometry was conducted at 32 years. Cumulative cannabis use was associated with higher FVC, total lung capacity, and functional residual capacity and residual volume, but not with lower FEV1 or FEV1/FVC.
A small feasibility study by Van Dam and Earleywine (2010) found that the use of a cannabis vaporizer instead of smoking cannabis in 12 adult participants who did not develop a respiratory illness was associated with improvements in forced expiratory volumes at approximately 1 month after the introduction of the vaporizer; however, this study did not have a control group.
Discussion of Findings
Overall, acute cannabis smoking was associated with bronchodilation, but many of the authors agreed that any benefits may be offset when cannabis is smoked regularly. The current findings are inconclusive on a variety of pulmonary function measurements, and the findings may be affected by the quality of the studies, a failure to adjust for important confounders, including tobacco and other inhaled drugs, and other occupational and environmental exposures. The committee’s findings are consistent with those reported in another recent review (Tashkin, 2013) and a position statement (Douglas et al., 2015).
The majority of studies, including those evaluated in the systematic review, relied on self-report for cannabis smoking. Many studies failed to control for tobacco smoking and occupational and other environmental exposures; did not control for the dose or duration of cannabis smoking; and did not use joint-years and instead based heavy cannabis smoking on having exceeded a specific threshold of joints. Even among studies that used joint-years, it is unclear how generalizable their findings are, given the potential high variability in lung-toxic content from joint to joint. Prior
studies have inconsistently documented decreases or no change in FEV1, FEV1/FVC, DLCO, and airway hyperresponsiveness. Moreover, neither the mechanism nor the clinical significance of the association between cannabis smoking and pulmonary function deficits is known beyond the possible impact of a high FVC in lowering the FEV1/FVC ratio. While elevated lung volumes could be indicators of lung pathology, an elevated FVC by itself has not been associated with any lung pathology.
CONCLUSION 7-1
7-1(a) There is moderate evidence of a statistical association between cannabis smoking and improved airway dynamics with acute use, but not with chronic use.
7-1(b) There is moderate evidence of a statistical association between cannabis smoking and higher forced vital capacity (FVC).
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
COPD is a clinical syndrome that consists of lower airway inflammation and damage that impairs airflow. Ranked as the fourth-leading cause of death worldwide by the World Health Organization, COPD has been estimated to cause more than 3 million deaths worldwide annually and has an estimated global prevalence of 10 percent in adults (Buist et al., 2007; Diaz-Guzman and Mannino, 2014). COPD is diagnosed with spirometry and is defined by a post-bronchodilator forced expiratory volume at 1 second divided by forced vital capacity (FEV1/FVC) <70 percent (fixed cutoff) or as a post-bronchodilator FEV1/FVC below the 5th percentile of a reference population (lower limit of normal). The committee responsible for Marijuana and Medicine: Assessing the Science Base (IOM, 1999) suspected, but did not conclude, that chronic cannabis smoking causes COPD.
Is There an Association Between Cannabis Use and COPD?
Systematic Reviews
There is no discussion about the association between cannabis and COPD in the systematic review by Tetrault et al. (2007). In the position statement of the American Thoracic Society (Douglas et al., 2015), workshop members concluded that there was minimal impairment in occasional cannabis smokers when controlling for tobacco use. In con-
trast, there was a trend toward higher prevalence in heavier users based on studies of lung function decline (Pletcher et al., 2012; Tashkin et al., 1987); however, workshop members determined that this association was incompletely quantified.
Primary Studies
The study by Aldington et al. (2007) examined high-resolution computed tomography scans among the subgroups of participants with cannabis smoking only, cannabis and tobacco smoking, tobacco smoking only, and never smokers. They found inconsistent results: a decreased mean lung density, which is suggestive of emphysematous changes (mean percent of area below −950 Hounsfield units in three slices at 2.4 percent [95% confidence interval (CI) = 1.0%–3.8%] for cannabis smokers, but −0.6 percent [−2.0%–0.8%] for tobacco smokers when compared to nonsmokers), but almost no evidence of macroscopic emphysema (1.3% versus 16.5% versus 18.5% versus 0% in cannabis-only smokers versus cannabis and tobacco smokers versus tobacco-only smokers versus non-smokers, respectively).
Tan et al. (2009) analyzed cross-sectional data collected in 878 adults ages 40 years and older from Vancouver, Canada, who participated in the Burden of Obstructive Lung Disease study on COPD prevalence. Current smoking of either tobacco or cannabis was defined as any smoking within the past year. Participants who had smoked at least 50 marijuana cigarettes but had no history of tobacco smoking were not at significantly greater risk of having COPD or more respiratory symptoms. There was inconsistent evidence for whether synergy from combined cannabis and tobacco smoking might affect the odds of having COPD or worse respiratory symptoms.
Specifically, the mean estimates for the tobacco and cannabis smoking versus tobacco-only smoking groups do not appear to be different, and the 95% CI for the tobacco and cannabis smoking group appears to overlap significantly with the tobacco-only smoking groups when evaluating either COPD or respiratory symptoms as the outcome.
Yadavilli et al. (2014) examined data from 709 participants over a 33-month period for hospital readmissions of COPD in illicit drug users and tobacco smokers. These investigators found that cannabis users had similar readmission rates to ex-tobacco or current tobacco users (mean readmissions at 0.22 versus 0.26) and much lower readmission rates than other illicit drug users (mean readmissions at 1.0). The unit for mean readmissions was not specified in either the tables or methods of this paper. The limitations of the study by Yadavilli et al. (2014) include a lack of spirometry data on all patients to confirm diagnosis of COPD, the self--
report of tobacco use, the risk for potential underreporting of illicit drug use, and the lack of outpatient visit frequency.
The study by Macleod et al. (2015) examined data from 500 adult participants, all of whom reported either tobacco smoking of ≥20 cigarettes per day for at least 5 years or cannabis of ≥1 joint per day for at least 1 year. There was no difference in the percent with COPD (FEV1/FVC <0.7) between tobacco-only users and tobacco and cannabis users (24.3 percent versus 25.2 percent; p = 0.90) for all ages or at any age group. Tobacco and cannabis users had more respiratory symptoms than did tobacco-only users (cough, phlegm, wheeze), but the investigators do not seem to report multivariable adjusted differences in the paper. The limitations of the study by Macleod et al. (2015) are that its cross-sectional design does not allow one to assess temporality between exposure and outcome, the lack of a nonsmoking group, the fact that its use of a convenience sample may have oversampled unwell participants, and the use of self-report for tobacco and cannabis.
Kempker et al. (2015) analyzed data from the 2007–2010 NHANES cohorts, similar to the work done by Papatheodorou et al. (2016). Kempker et al. (2015), however, also examined the information on cumulative lifetime use of cannabis available in the 2009–2010 NHANES cohort. Main findings were that 59 percent reported using cannabis at least once during their lifetime, and 12 percent reported use during the last month. When evaluating cumulative lifetime cannabis use, those with >20 joint-years had a two times higher odds (OR, 2.1; 95% CI = 1.1–3.9) of having a pre-bronchodilator FEV1/FVC <70 percent than those with no cannabis exposure. However, as noted by others, cannabis use was associated with a higher FVC and no association with FEV1, which would spuriously reduce the ratio FEV1/FVC. Beyond the limitations noted above for the paper by Papatheodorou et al. (2016), who also used NHANES data, the authors were limited to use pre-bronchodilator spirometry instead of using post-bronchodilator spirometry as commonly done in COPD studies.
Discussion of Findings
It is unclear whether regular cannabis use is associated with the risk of developing COPD or exacerbating COPD. Current studies may be confounded by tobacco smoking and the use of other inhaled drugs as well as by occupational and environmental exposures, and these studies have failed to quantify the effect of daily or near daily cannabis smoking on COPD risk and exacerbation. There is no evidence of physiological or imaging changes consistent with emphysema. The committee’s findings are consistent with those of a recent position statement from the American Thoracic Society Marijuana Workgroup which concluded that there
was minimal impairment in light and occasional cannabis smokers when controlled for tobacco use and that the effects in heavy cannabis smokers remain poorly quantified (Douglas et al., 2015). The review by Tashkin (2013) concluded that the lack of evidence between cannabis use and longitudinal lung function decline (Pletcher et al., 2012) argues against the idea that smoking cannabis by itself is a risk factor for the development of COPD. This is further supported by the findings of Kempker et al. (2015), who concluded that smoking cannabis was not associated with lower FEV1 after adjusting for tobacco smoking. However, smoking cannabis was associated with a higher FVC, which may have led to a spuriously lower FEV1/FVC. Therefore, their analyses also do not support an association between heavy cannabis use (>20 lifetime joint-years) and obstruction on spirometry. The position statement by Douglas et al. (2015) concluded that the lack of solid epidemiologic association suggests that regular cannabis smoking may be a less significant risk factor for the development of COPD than tobacco smoking.
Cross-sectional studies are inadequate to establish temporality, and cohort studies of regular or daily cannabis users are a better design to help establish COPD risk over time. Better studies are needed to clearly separate the effects of cannabis smoking from those of tobacco smoking on COPD risk and COPD exacerbations, and better evidence is needed for heavy cannabis users.
CONCLUSION 7-2
7-2(a) There is limited evidence of a statistical association between occasional cannabis smoking and an increased risk of developing chronic obstructive pulmonary disease (COPD) when controlled for tobacco use.
7-2(b) There is insufficient evidence to support or refute a statistical association between cannabis smoking and hospital admissions for COPD.
RESPIRATORY SYMPTOMS, INCLUDING CHRONIC BRONCHITIS
Respiratory symptoms include cough, phlegm, and wheeze. Chronic bronchitis is defined as chronic phlegm production or productive cough for 3 consecutive months per year for at least 2 consecutive years (Medical Research Council, 1965). Chronic bronchitis is a clinical diagnosis and does not require confirmation by spirometry or evidence of airflow obstruction. The committee responsible for Marijuana and Medicine: Assessing the Science Base (IOM, 1999) concluded that acute and chronic bronchitis may occur as a result of chronic cannabis use.
Is There an Association Between Cannabis Use and Respiratory Symptoms, Including Chronic Bronchitis?
Systematic Reviews
The systematic review by Tetrault et al. (2007) summarized information from 14 studies that assessed the association between long-term cannabis smoking and respiratory symptoms. Nine of these studies were cross-sectional, 3 were case series, 1 was a case-control study, and 1 was a longitudinal cohort study. Data were relatively consistent in both cross-sectional and cohort studies in indicating that long-term cannabis smoking worsens respiratory symptoms, including cough (ORs, 1.7–2.0), increased sputum production (ORs, 1.5–1.9), and wheeze (ORs, 2.0–3.0). Other studies have reported effects on more episodes of acute bronchitis and pharyngitis, dyspnea, hoarse voice, worse cystic fibrosis symptoms, and chest tightness.
Primary Studies
Aldington et al. (2007) reported higher prevalence of wheeze (27 percent versus 11 percent), cough (29 percent versus 5 percent), chest tightness (49 percent versus 35 percent), and chronic bronchitis symptoms (19 percent versus 3 percent) among cannabis smokers than among nonsmokers. There were no clear additive effects observed in the combined cannabis and tobacco smoking groups on respiratory symptoms.
Hancox et al. (2015) conducted a study in a cohort of 1,037 adults (52 percent male) in the Dunedin Multidisciplinary Health and Development Study. Cannabis and tobacco smoking histories were obtained at the ages of 18, 21, 26, 32, and 38 years. At each assessment, participants were asked how many times they had used cannabis in the previous year. Frequent cannabis users were defined as those who reported using marijuana ≥52 times over the previous year. Quitters were defined as a frequent cannabis user at the previous assessment but less than frequent at the current assessment. Because it was possible to quit frequent cannabis use more than once during the follow-up from 18 to 38 years of age, only the first recorded episode of quitting was used in analyses. In this study, the investigators found that frequent cannabis use was associated with morning cough (OR = 1.97, p <0.001), sputum production (OR = 2.31, p <0.001), and wheeze (OR = 1.55, p <0.001), but not dyspnea (p = 0.09) (see Figure 7-1). Quitters (open triangles) also had fewer respiratory symptoms than those who did not quit (solid squares).
Limitations of the study by Hancox et al. (2015) include its reliance on self-reported data of cannabis use without objective confirmation, the
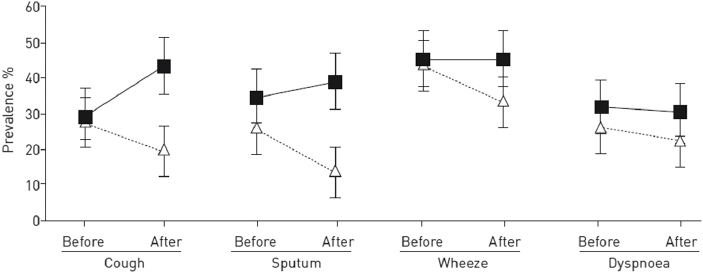
SOURCE: Hancox et al., 2015.
classification of nonusers as those with <52 times of cannabis use, and a lack of data as to whether cannabis use was specifically from smoking.
Walden and Earleywine (2008) conducted a cross-sectional Internet survey of 5,987 adults worldwide who used cannabis at least once per month. They quantified frequency, amount, and degree of usual and maximal intoxication, and they also asked about respiratory symptoms using a composite score produced from the answers to six standard questions about cough, morning phlegm, dyspnea, chest wheezing other than during colds, and nighttime awakenings because of chest tightness. They found that the frequency of use, the amount used (in quarter bags per month), and the degree of usual intoxication were all positively associated with more respiratory symptoms. Limitations for this study include its recruitment of participants from organizations that advocate drug policy reform, its reliance on self-reported data of cannabis or tobacco use without objective confirmation, and the lack of data about cannabis use for medical versus recreational purposes.
Tashkin et al. (2012) followed 299 participants from a longitudinal cohort study for at least two visits over 9.8 years and examined the relationship between symptoms for chronic bronchitis and cannabis use. They found that current cannabis users were more likely to have cough (OR = 1.7), sputum (OR = 2.1), increased bronchitis episodes (OR = 2.3), and wheeze (OR = 3.4) when compared to never users. They also found that current cannabis users were more likely to have cough (OR = 3.3), sputum (OR = 4.2), or wheeze (OR = 2.1) than former users. Similar to
the studies by Hancox et al. (2015) and Walden and Earleywine (2008), these findings demonstrated the benefit of cannabis smoking cessation in resolving preexisting symptoms of chronic bronchitis. The limitations of this study include its reliance on self-reported data of cannabis or tobacco use without objective confirmation and high rates of loss to follow-up or variable follow-up periods.
A small feasibility study by Van Dam and Earleywine (2010) of 12 adult participants who did not develop a respiratory illness during the trial found that the use of a cannabis vaporizer instead of smoking cannabis was correlated with the resolution of cannabis-related respiratory symptoms at approximately 1 month after the introduction of the vaporizer; however, this study did not have a control group.
Discussion of Findings
Regular cannabis use was associated with airway injury, worsening respiratory symptoms, and more frequent chronic bronchitis episodes. There were no clear additive effects on respiratory symptoms observed from smoking both cannabis and tobacco. Cannabis smoking cessation was temporally associated with the resolution of chronic bronchitis symptoms, and a small feasibility study suggests that use of a vaporizer instead of smoking cannabis may lead to the resolution of respiratory symptoms. The committee’s findings are consistent with those reported in a recent review (Tashkin, 2013) and position statement (Douglas et al., 2015).
The majority of studies relied on self-report for cannabis smoking. Many studies failed to control for tobacco, occupational, and other environmental exposures; did not control for the dose or duration of the cannabis smoke exposure; and did not use joint-years and instead based heavy cannabis exposure on exceeding a specific threshold of cigarettes. Even among studies that used joint-years, it is unclear how generalizable the findings are, given the potential high variability in tetrahydrocannabinol (THC) content from joint to joint and from year to year.
CONCLUSION 7-3
7-3(a) There is substantial evidence of a statistical association between long-term cannabis smoking and worse respiratory symptoms and more frequent chronic bronchitis episodes.
7-3(b) There is moderate evidence of a statistical association between cessation of cannabis smoking and improvements in respiratory symptoms.
ASTHMA
Asthma is a clinical syndrome that is associated with airways inflammation, airflow limitation, bronchial hyperresponsiveness, and symptoms of episodic wheeze and cough. It is predominantly an allergic disease. Worldwide, asthma is thought to affect 300 million people, and it is responsible for more disability-adjusted life-years lost than diabetes mellitus. Asthma was not specifically addressed in Marijuana and Medicine: Assessing the Science Base (IOM, 1999).
Is There an Association Between Cannabis Use and Asthma?
Systematic Reviews
The systematic review by Tetrault et al. (2007) referred to only one study that described the association between cannabis use and asthma exacerbations. Upon retrieving this study, the committee found that this was a letter to the editor which reported findings of a case-control study of 100 participants ages 18–55 years, with and without asthma, admitted to the emergency department. In this study, the authors found no association between THC and asthma (Gaeta et al., 1996).
Primary Studies
Bechtold et al. (2015) reported on a follow-up of a cohort of boys who participated in the Pittsburgh Youth Study. A total of 506 boys were followed longitudinally: 257 scored at or above the 70th percentile of a multi-informant conduct problem score, and 249 scored below the 70th percentile. This study found no link between cannabis use and self-reported asthma symptoms. The limitations of this study include a lack of generalizability to the general population, given the selection criteria for conduct problems, a lack of inclusion of women in their study, and the fact that health outcomes were based on self-report and biased to those who had sought care for health problems.
Weekes et al. (2011) studied a cohort of 110 black urban adolescents with asthma. In this study, the investigators found that 16 percent of the adolescents smoked cannabis, but there was no association between cannabis use and asthma concern or asthma severity or asthma symptoms. The limitations of this study include the reliance on the self-report of cannabis use, which the study authors speculated may be underreported in black adolescents when compared to whites, and a lack of data on asthma medication adherence.
Discussion of Findings
The committee did not find evidence for an association between cannabis use and either asthma risk or asthma exacerbations, and current studies failed to control for other important confounders, including adherence to asthma medications.
The evidence linking cannabis use with asthma risk or exacerbation is limited by the scope and sample size of available studies and by the use of more standardized approaches to measure asthma prevalence or exacerbations of asthma. Few studies have examined the link between cannabis and asthma, and no clear evidence exists of a link between asthma or asthma exacerbation and cannabis use. However, asthma symptoms such as wheeze appear to be common among cannabis users.
CONCLUSION 7-4 There is no or insufficient evidence to support or refute a statistical association between cannabis smoking and asthma development or asthma exacerbation.
RESEARCH GAPS
The effects of cannabis smoke on respiratory health remain poorly quantified. Further research is needed to better elucidate the influence of exposure levels to cannabis smoke on respiratory outcomes, the chronicity of cannabis smoking, the effects of an underlying predisposition to respiratory disease, and possible interaction effects with tobacco smoke to promote airway inflammation, worsen respiratory symptoms, accelerate lung function decline, or increase exacerbation of COPD and asthma. Previous studies have not been able to adequately separate cannabis smoke effects from tobacco smoke effects, and this has meant that some important questions remain unanswered. It is unknown whether or not:
- Long-term cannabis smoking, above and beyond that of tobacco smoking, leads to a more rapid decline in lung function and to the development of chronic bronchitis or COPD.
- Cannabis smoking increases the risk of allergic disease or asthma.
- Alternative inhaled delivery methods of cannabis result in fewer respiratory symptoms.
To address the research gaps relevant to respiratory disease, the committee suggests the following:
- Design better observational studies with both self-reported and quantitative measures of cannabis smoking and systematic approaches to measure the duration and dose to determine if
- long-term exposure to cannabis smoke, above and beyond exposure to tobacco smoke, leads to the development of chronic bronchitis or COPD or to a higher rate of COPD exacerbation.
- Design longitudinal studies to determine if long-term cannabis smoking is associated with the development of allergic disease and risk of asthma.
- Conduct clinical trials of alternative inhaled delivery methods versus cannabis smoking to determine if they reduce respiratory symptoms.
SUMMARY
This chapter summarizes all of the respiratory disease literature that has been published since 1999 and deemed to be good or fair by the committee. Overall, the risks of respiratory complications of cannabis smoking appear to be relatively small and to be far lower than those of tobacco smoking. While heavy cannabis users may be at a higher risk for developing chronic bronchitis and COPD or at an increased risk of exacerbating COPD and asthma, current studies do not provide sufficient evidence for a link. Limitations of reviewed studies are that it is difficult to separate the effects of cannabis smoking from those of tobacco smoking from current available data; that exposures have generally been measured by self-report of cannabis smoking; and that there is a lack of cohort studies of regular or daily cannabis users, of adequate controls for environmental factors, and of generalizability of findings. The committee has formed a number of research conclusions related to these health endpoints (see Box 7-1); however, it is important that each of these conclusions be interpreted within the context of the limitations discussed in the Discussion of Findings sections.
REFERENCES
Aldington, S., M. Williams, M. Nowitz, M. Weatherall, A. Pritchard, A. McNaughton, G. Robinson, and R. Beasley. 2007. Effects of cannabis on pulmonary structure, function and symptoms. Thorax 62:1058–1063.
Aldington, S., M. Harwood, B. Cox, M. Weatherall, L. Beckert, A. Hansell, A. Pritchard, G. Robinson, R. Beasley; and the Cannabis and Respiratory Disease Research Group. 2008. Cannabis use and cancer of the head and neck: Case-control study. Otolaryngology and Head and Neck Surgery 138(3):374–380.
Bechtold, J., T. Simpson, H. R. White, and D. Pardini. 2015. Chronic adolescent marijuana use as a risk factor for physical and mental health problems in young adult men. Psychology and Addictive Behaviors 29:552–563.
Buist, A. S., M. A. McBurnie, W. M. Vollmer, S. Gillespie, P. Burney, D. M. Mannino, A. M. B. Menezes, S. D. Sullivan, T. A. Lee, K. B. Weiss, R. L. Jensen, G. B. Marks, A. Gulsvik, and E. Nizankowska-Mogilnicka. 2007. International variation in the prevalence of COPD (The BOLD study): A population-based prevalence study. Lancet 370:741–750.
CBHSQ (Center for Behavioral Health Statistics and Quality). 2015. Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health (HHS Publication No. SMA 15-4927, NSDUH Series H-50).
Diaz-Guzman, E., and D. M. Mannino. 2014. Epidemiology and prevalence of chronic obstructive pulmonary disease. Clinics in Chest Medicine 35(1):7–16.
Douglas, I. S., T. E. Albertson, P. Folan, N. A. Hanania, D. P. Tashkin, D. J. Upson, and F. T. Leone. 2015. Implications of marijuana decriminalization on the practice of pulmonary, critical care, and sleep medicine. A report of the American Thoracic Society Marijuana Workgroup. Annals of the American Thoracic Society 12:1700–1710.
Gaeta, T. J., R. Hammock, T. A. Spevack, H. Brown, and K. Rhoden. 1996. Association between substance abuse and acute exacerbation of bronchial asthma. Academic Emergency Medicine 3(12):1170–1172.
Hancox, R. J., R. Poulton, M. Ely, D. Welch, D. R. Taylor, C. R. McLachlan, J. M. Greene, T. E. Moffitt, A. Caspi, and M. R. Sears. 2010. Effects of cannabis on lung function: a population-based cohort study. The European Respiratory Journal 35(1):42–47.
Hancox, R. J., H. H. Shin, A. R. Gray, R. Poulton, and M. R. Sears. 2015. Effects of quitting cannabis on respiratory symptoms. European Respiratory Journal 46:80–87.
IOM (Institute of Medicine). 1999. Marijuana and medicine: Assessing the science base. Washington, DC: National Academy Press.
Kempker, J. A., E. G. Honig, and G. Martin. 2015. The effects of marijuana exposure on respiratory health in U.S. adults. Annals of the American Thoracic Society 12:135–141.
Lim, S. S., T. Vos, A. D. Flaxman, G. Danaei, K. Shibuya, H. Adair-Rohani, et al. 2012. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2224–2260.
Macleod, J., R. Robertson, L. Copeland, J. McKenzie, R. Elton, and P. Reid. 2015. Cannabis, tobacco smoking, and lung function: A cross-sectional observational study in a general practice population. British Journal of General Practice 65:e89–e95.
Medical Research Council. 1965. Definition and classification of chronic bronchitis for clinical and epidemiological purposes. A report to the Medical Research Council by their Committee on the Aetiology of Chronic Bronchitis. Lancet 1:775–779.
Papatheodorou, S. I., H. Buettner, M. B. Rice, and M. A. Mittleman. 2016. Recent marijuana use and associations with exhaled nitric oxide and pulmonary function in adults in the United States. Chest 149:1428–1435.
Pletcher, M. J., E. Vittinghoff, R. Kalhan, J. Richman, M. Safford, S. Sidney, F. Lin, and S. Kertesz. 2012. Association between marijuana exposure and pulmonary function over 20 years. JAMA 307:173–181.
Tan, W. C., C. Lo, A. Jong, L. Xing, M. J. Fitzgerald, W. M. Vollmer, S. A. Buist, and D. D. Sin. 2009. Vancouver Burden of Obstructive Lung Disease (BOLD) Research Group. Marijuana and chronic obstructive lung disease: A population-based study. Canadian Medical Association Journal 180:814–820.
Tashkin, D. P. 2013. Effects of marijuana smoking on the lung. Annals of the American Thoracic Society 10:239–247.
Tashkin, D. P., A. H. Coulson, V. A. Clark, M. Simmons, L. B. Bourque, S. Duann, G. H. Spivey, and H. Gong. 1987. Respiratory symptoms and lung function in habitual heavy smokers of marijuana alone, smokers of marijuana and tobacco, smokers of tobacco alone, and nonsmokers. American Review of Respiratory Disease 135:209–216.
Tashkin, D. P., M. S. Simmons, and C. H. Tseng. 2012. Impact of changes in regular use of marijuana and/or tobacco on chronic bronchitis. COPD 9:367–374.
Tetrault, J. M., K. Crothers, B. A. Moore, R. Mehra, J. Concato, and D. A. Fiellin. 2007. Effects of marijuana smoking on pulmonary function and respiratory complications: A systematic review. Archives of Internal Medicine 167:221–228.
Van Dam, N. T., and M. Earleywine. 2010. Pulmonary function in cannabis users: Support for a clinical trial of the vaporizer. International Journal of Drug Policy 21:511–513.
Walden, N., and M. Earleywine. 2008. How high: Quantity as a predictor of cannabis-related problems. Harm Reduction Journal 5:20.
Weekes, J. C., S. Cotton, and M. E. McGrady. 2011. Predictors of substance use among black urban adolescents with asthma: A longitudinal assessment. Journal of the National Medical Association 103:392–398.
Wu, T. C., D. P. Tashkin, B. Djahed, and J. E. Rose. 1988. Pulmonary hazards of smoking marijuana as compared with tobacco. New England Journal of Medicine 318:347–351.
Yadavilli, R., A. Collins, W. Y. Ding, N. Garner, J. Williams, and H. Burhan. 2014. Hospital readmissions with exacerbation of obstructive pulmonary disease in illicit drug smokers. Lung 192:669–673.


















