
Appendix B
Building Data Capacity for Patient-Centered Outcomes Research: Interim Report 1–Looking Ahead at Data Needs
(Full text of the committee’s first interim report released on September 10, 2021.)1
___________________
1 https://www.nap.edu/catalog/26297/building-data-capacity-for-patient-centered-outcomes-research-interim-report.
This page intentionally left blank.
Building Data Capacity
for Patient-Centered
Outcomes Research
INTERIM REPORT 1–
Looking Ahead at Data Needs
Committee on Building Data Capacity for
Patient-Centered Outcomes Research:
An Agenda for 2021 to 2030
Committee on National Statistics
Division of Behavioral and Social Sciences and Education
Board on Health Care Services
Health and Medicine Division
Computer Science and Telecommunications Board
Division on Engineering and Physical Sciences
A Consensus Study Report of
![]()
THE NATIONAL ACADEMIES PRESS
Washington, DC
www.nap.edu
THE NATIONAL ACADEMIES PRESS 500 Fifth Street, NW Washington, DC 20001
This activity was supported by a contract between the National Academy of Sciences and the U.S. Department of Health and Human Services (award #HHSP23 3201400020B/75P00120F37102). Any opinions, findings, conclusions, or recommendations expressed in this publication do not necessarily reflect the views of any organization or agency that provided support for the project.
International Standard Book Number-13: 978-0-309-26824-0
International Standard Book Number-10: 0-309-26824-9
Digital Object Identifier: https://doi.org/10.17226/26297
Additional copies of this publication are available from the National Academies Press, 500 Fifth Street, NW, Keck 360, Washington, DC 20001; (800) 624-6242 or (202) 334-3313; http://www.nap.edu.
Copyright 2021 by the National Academy of Sciences. All rights reserved.
Printed in the United States of America
Suggested citation: National Academies of Sciences, Engineering, and Medicine. (2021). Building Data Capacity for Patient-Centered Outcomes Research: Interim Report 1—Looking Ahead at Data Needs. Washington, DC: The National Academies Press. https://doi.org/10.17226/26297.
![]()
The National Academy of Sciences was established in 1863 by an Act of Congress, signed by President Lincoln, as a private, nongovernmental institution to advise the nation on issues related to science and technology. Members are elected by their peers for outstanding contributions to research. Dr. Marcia McNutt is president.
The National Academy of Engineering was established in 1964 under the charter of the National Academy of Sciences to bring the practices of engineering to advising the nation. Members are elected by their peers for extraordinary contributions to engineering. Dr. John L. Anderson is president.
The National Academy of Medicine (formerly the Institute of Medicine) was established in 1970 under the charter of the National Academy of Sciences to advise the nation on medical and health issues. Members are elected by their peers for distinguished contributions to medicine and health. Dr. Victor J. Dzau is president.
The three Academies work together as the National Academies of Sciences, Engineering, and Medicine to provide independent, objective analysis and advice to the nation and conduct other activities to solve complex problems and inform public policy decisions. The National Academies also encourage education and research, recognize outstanding contributions to knowledge, and increase public understanding in matters of science, engineering, and medicine.
Learn more about the National Academies of Sciences, Engineering, and Medicine at www.nationalacademies.org.
![]()
Consensus Study Reports published by the National Academies of Sciences, Engineering, and Medicine document the evidence-based consensus on the study’s statement of task by an authoring committee of experts. Reports typically include findings, conclusions, and recommendations based on information gathered by the committee and the committee’s deliberations. Each report has been subjected to a rigorous and independent peer-review process and it represents the position of the National Academies on the statement of task.
Proceedings published by the National Academies of Sciences, Engineering, and Medicine chronicle the presentations and discussions at a workshop, symposium, or other event convened by the National Academies. The statements and opinions contained in proceedings are those of the participants and are not endorsed by other participants, the planning committee, or the National Academies.
For information about other products and activities of the National Academies, please visit www.nationalacademies.org/about/whatwedo.
COMMITTEE ON BUILDING DATA CAPACITY FOR PATIENT-CENTERED OUTCOMES RESEARCH: AN AGENDA FOR 2021 TO 2030
GEORGE ISHAM (Chair), HealthPartners Institute
JOHN F.P. BRIDGES, The Ohio State University
JULIE BYNUM, University of Michigan
ANGELA DOBES, IBD Plexus, Crohn’s & Colitis Foundation
OLUWADAMILOLA FAYANJU, The University of Pennsylvania
DEBORAH ESTRIN, Cornell Tech
CONSTANTINE GATSONIS, Brown University
ROBERT GOERGE, Chapin Hall, University of Chicago
GEORGE HRIPCSAK, Columbia University
LISA IEZZONI, Massachusetts General Hospital
S. CLAIBORNE JOHNSTON, The University of Texas at Austin
MIGUEL MARINO, Oregon Health & Science University
ELIZABETH MCGLYNN, Kaiser Permanente
DAVID MELTZER, University of Chicago
PAUL TANG, Stanford University and Palo Alto Medical Foundation
KRISZTINA MARTON, Study Director
MEGAN KEARNEY, Associate Program Officer (until June 2021)
RUTH COOPER, Associate Program Officer (from June 2021)
MARY GHITELMAN, Senior Program Assistant
BRIAN HARRIS-KOJETIN, Director, Committee on National Statistics
SHARYL NASS, Director, Board on Health Care Services
JON EISENBERG, Director, Computer Science and Telecommunications Board
SAUL RIVAS (National Academy of Medicine Fellow), University of Texas Rio Grande Valley
COMMITTEE ON NATIONAL STATISTICS
ROBERT M. GROVES (Chair), Georgetown University
ANNE C. CASE, Princeton University
MICK P. COUPER, University of Michigan
JANET M. CURRIE, Princeton University
DIANA FARRELL, JPMorgan Chase Institute
ROBERT GOERGE, Chapin Hall at the University of Chicago
ERICA L. GROSHEN, Cornell University
HILARY HOYNES, University of California, Berkeley
DANIEL KIFER, Pennsylvania State University
SHARON LOHR, Arizona State University (emerita)
JEROME P. REITER, Duke University
JUDITH A. SELTZER, University of California, Los Angeles
C. MATTHEW SNIPP, Stanford University
ELIZABETH A. STUART, Johns Hopkins University
JEANNETTE WING, Columbia University
BRIAN A. HARRIS-KOJETIN, Director
CONSTANCE F. CITRO, Senior Scholar
BOARD ON HEALTH CARE SERVICES
DAVID BLUMENTHAL (Chair), The Commonwealth Fund
ANDREW BINDMAN, Kaiser Foundation Health Plan, Inc.
NIRANJAN BOSE, Gates Ventures
MELINDA J. BEEUWKES BUNTIN, Vanderbilt University School of Medicine
NEIL S. CALMAN, The Institute for Family Health
PAUL CHUNG, Kaiser Permanente School of Medicine
PATRICIA M. DAVIDSON, Johns Hopkins University School of Nursing
MARTHA DAVIGLUS, University of Illinois at Chicago
JENNIFER E. DEVOE, Oregon Health & Science University
R. ADAMS DUDLEY, University of Minnesota
RICHARD G. FRANK, Harvard Medical School
TERRY FULMER, John A. Hartford Foundation
CINDY GILLESPIE, Arkansas Department of Human Services
ELMER HUERTA, The George Washington University Cancer Center
SHARON INOUYE, Harvard Medical School
JOHN LUMPKIN, Blue Cross Blue Shield of North Carolina Foundation
FAITH MITCHELL, The Urban Institute
DAVID B. PRYOR, Ascension Health
TRISH RILEY, National Academy for State Health Policy
WILLIAM SAGE, The University of Texas at Austin
HARDEEP SINGH, Baylor College of Medicine
SHARYL NASS, Director
COMPUTER SCIENCE AND TELECOMMUNICATIONS BOARD
LAURA HAAS (Chair), University of Massachusetts, Amherst
DAVID CULLER, University of California, Berkeley
ERIC HORVITZ, Microsoft Corporation
CHARLES ISBELL, Georgia Institute of Technology
BETH MYNATT, Georgia Institute of Technology
CRAIG PARTRIDGE, Colorado State University
DANIELA RUS, Massachusetts Institute of Technology
FRED B. SCHNEIDER, Cornell University
NAMBIRAJAN SESHADRI, University of California, San Diego
MARGO SELTZER, University of British Columbia
MOSHE VARDI, Rice University
JON EISENBERG, Director
Acknowledgments
This Consensus Study Report was reviewed in draft form by individuals chosen for their diverse perspectives and technical expertise. The purpose of this independent review is to provide candid and critical comments that will assist the National Academies of Sciences, Engineering, and Medicine in making each published report as sound as possible and to ensure that it meets the institutional standards for quality, objectivity, evidence, and responsiveness to the study charge. The review comments and draft manuscript remain confidential to protect the integrity of the deliberative process.
We thank the following individuals for their review of this report: Cheryl R. Clark, Health Equity Research & Intervention, Center for Community Health and Health Equity, Brigham and Women’s Hospital; Darrell J. Gaskin, Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health; Sherry Glied, Robert F. Wagner Graduate School of Public Service, New York University; Elizabeth Patzer, Department of Surgery and Health Services Research Center, Emory University; Robert L. Phillips, Jr., Center for Professionalism and Value in Health Care, American Board of Family Medicine Foundation; Russell Rothman, Institute for Medicine and Public Health, Vanderbilt University Medical Center; and Mariana F. Wolfner, Department of Molecular Biology and Genetics, Cornell University.
Although the reviewers listed above provided many constructive comments and suggestions, they were not asked to endorse the conclusions of this report, nor did they see the final draft before its release. The review of this report was overseen by Andrew B. Bindman, chief medical officer, Kaiser Foundation Health Plan and Hospitals and Alicia L. Carriquiry,
Department of Statistics, Iowa State University. They were responsible for making certain that an independent examination of this report was carried out in accordance with the standards of the National Academies and that all review comments were carefully considered. Responsibility for the final content rests entirely with the authoring committee and the National Academies.
This page intentionally left blank.
FIGURES
1-1 Patient-Centered Outcomes Research Trust Fund: Three streams of work and funding
1-2 ASPE’s strategic framework for the patient-centered outcomes research data infrastructure
2-1 Example of data available on social determinants of health
3-1 Evidation Health’s vision for person-generated health data framework
3-2 Episodic real-world evidence data points versus continuous data using digital technologies
TABLE
Summary
The Office of the Assistant Secretary for Planning and Evaluation (ASPE), in partnership with other agencies and divisions of the U.S. Department of Health and Human Services (HHS), coordinates a portfolio of projects that build data capacity for conducting patient-centered outcomes research (PCOR). PCOR focuses on producing scientific evidence on the effectiveness of prevention and treatment options to inform the health care decisions of patients, families, and health care providers, taking into consideration the preferences, values, and questions patients face when making health care choices. The data infrastructure includes data sources and functionalities that support the research. Major building blocks are the services, standards, policies, and governance that enable the use of the data.
ASPE asked the National Academies of Sciences, Engineering, and Medicine to appoint a consensus study committee to identify issues critical to the continued development of the data infrastructure for PCOR. The committee’s work will contribute to ASPE’s development of a strategic plan that will guide its work related to PCOR data capacity over the next decade.
As part of its information-gathering activities, the committee organized three workshops to collect input from stakeholders on the PCOR data infrastructure. This report, the first in a series of three interim reports, summarizes the discussion and committee conclusions from the first workshop, focused on looking ahead at data user needs over the next decade. The workshop included representatives of patient groups with a wide reach and researchers with broad research interests as well as an understanding of the
PCOR infrastructure. The high-level conclusions included in this interim report are based primarily on the input collected as part of the workshop, background documentation received from ASPE and other public sources, and the committee members’ synthesis and expert judgment regarding the input received. As an interim report based on one in a series of information-gathering activities, the scope of this report is narrowly focused on a subset of key topics relevant to the committee’s charge. The conclusions reached by the committee are, at this stage, fairly high level. After completing all of its information-gathering activities, which include but are not limited to the three workshops, the committee will also issue a final report, containing the study’s overall findings and conclusions.
FUNDAMENTAL DATA CHALLENGES
Most data that are available for PCOR are collected for clinical care, billing, or other nonresearch purposes. This presents a fundamental challenge to answering critical questions, but the workshop also made it clear that opportunities exist for making the data infrastructure more suitable for answering questions of interest, so long as the potential uses of the data are carefully considered.
CONCLUSION 2-2: The data available for patient-centered outcomes research are often collected for reasons other than research, which limits their usefulness. Opportunities exist for increasing the utility of the data infrastructure by carefully considering the multiple uses to which the data might be applied.
Researchers experience barriers that limit their ability to access data available in databases, which range from databases that can be considered a part of the PCOR data infrastructure to those owned by private companies. A focus on facilitating and simplifying access could further enhance the usefulness of PCOR data.
CONCLUSION 4-3: Researchers encounter substantial barriers to accessing existing data for patient-centered outcomes research. Facilitating and simplifying data access could further increase the usefulness of data for research.
DATA FRAGMENTATION
The data that exist for PCOR are collected and curated in a variety of databases across a fragmented health system. These databases are typically constructed as stand-alone entities for particular administrative or other
uses, and without factoring in potential linkages with other databases. The workshop identified these data silos as a major barrier, both to understanding the role of social determinants of health and to research more broadly. A focus on facilitating data linkages could greatly increase the usefulness of the information available.
CONCLUSION 2-3: Existing data on the social determinants of health are found in a variety of databases. Barriers to linking across these data silos represent a major challenge to understanding how social determinants of health affect health outcomes.
CONCLUSION 4-2: The data available for patient-centered outcomes research are fragmented across a variety of databases. Expanding data linkages could greatly increase the usefulness of these data for research.
HEALTH DISPARITIES
A theme that emerged from the workshop was the magnitude of the gaps in the data that are available to better understand and address health disparities. Health disparities represent an evolving and expanding area of research, with corresponding data needs. Limitations exist for a variety of social determinants of health data and for a range of populations. Improving the data available for understanding and addressing these disparities would require data strategies that prioritize this goal.
CONCLUSION 2-1: Health disparities can occur across a broad range of characteristics and populations. Data limitations affect the ability to identify and understand these disparities in many areas. Data for specific populations are sometimes unavailable or are not representative. In other cases, the data might not be timely or might have other gaps that make it difficult to understand the impact of changes over long periods of time.
CONCLUSION 2-5: Prioritizing and improving the collection of data can lead to a better understanding of health disparities and to potential solutions for reducing disparities.
The workshop also made it clear that the data available do not capture complexities that are necessary to understand how people’s characteristics and experiences influence health outcomes. Speakers at the workshop identified several potential ways of capturing data that reflect these complexities, emphasizing the need to build flexibility into the data collection systems to allow them to adapt to evolving terminologies and technologies
for capturing and processing data. These considerations are particularly important for social determinants of health, an area that may be rapidly changing.
CONCLUSION 2-4: Existing data do not capture the richness of people’s characteristics and experiences. While such limitations are to be expected, opportunities exist for capturing data that are better able to characterize these complexities. A robust data infrastructure builds on the strengths of what is available today and has the flexibility to adapt, both as measures and terminologies become obsolete and as new technologies emerge.
PATIENT DATA NEEDS AND ENGAGEMENT
Too often, the data available for PCOR are not focused on the issues that are truly important to patients and that would enable them to find answers to their questions about treatment options and potential outcomes. Information about the cost implications of medical care is an area in which data are particularly limited, because it has only recently been included in the statutory scope of PCOR.
CONCLUSION 3-1: The patient-centered outcomes research data infrastructure has not reached its full potential to provide data that can answer questions that matter to patients and enable them to make informed decisions. Information about the cost of care was highlighted among the types of data that would be particularly useful.
Even for the many areas where data on patient-centered outcomes are available, the information is rarely available in ways that would make it truly accessible to patients for decision-making purposes. More widespread dissemination of information that is easy to use could increase the engagement of patients and communities and could complement research efforts to improve health outcomes.
CONCLUSION 3-2: Dissemination and translation of the research findings could be greatly enhanced by using forms of communication that are relevant to those outside of the research community.
CONCLUSION 4-4: Making the data more visible and more widely accessible could enable patients and communities to use the information in ways that reduce health disparities, complementing research efforts in this area.
Both patient groups and researchers highlighted the clear need for more data on the total cost of care.
CONCLUSION 4-5: Data needs related to the total cost of care and a better understanding of cost considerations are areas that deserve more attention.
FOCUS ON THE PERSON AS A WHOLE
The input received from workshop participants made it clear that limiting the focus to the patient limits not only thinking about the data but also the outcomes and impacts that matter to people in general.
CONCLUSION 4-1: Broadening the focus from the patient to the person more generally would enable a more comprehensive approach to the data infrastructure and a better understanding of the outcomes and impacts that matter to people.
This page intentionally left blank.
1
Introduction
The Office of the Assistant Secretary for Planning and Evaluation (ASPE), in partnership with other agencies and divisions of the U.S. Department of Health and Human Services (HHS), coordinates a portfolio of projects that build data capacity for conducting patient-centered outcomes research (PCOR). The PCOR data infrastructure provides decision makers with objective, scientific evidence on the effectiveness of treatments, services, and other interventions used in health care. This research is frequently focused on analyzing existing data to study questions and provide objective information for the purpose of informing real-world health care decisions.
BACKGROUND
The legal framework that established funding for research on the outcomes and effectiveness of treatments and health care interventions dates back to the 2003 Medicare Prescription Drug, Improvement, and Modernization Act. This act provided authorization for the Agency for Healthcare Research and Quality (AHRQ) to support research comparing the outcomes and effectiveness of treatments and clinical approaches and to disseminate the findings from this research. In 2009, the American Recovery and Reinvestment Act provided additional funding to AHRQ, the National Institutes of Health, and HHS for research that compares the effectiveness of medical options. In 2010, the Patient Protection and Affordable Care Act provided further authorization for research that assists patients, clinicians, purchasers, and policy makers in making informed health decisions.
To facilitate PCOR, in 2010 Congress established the Patient-Centered Outcomes Research Trust Fund (PCOR Trust Fund) with the U.S. Department of the Treasury. The goals of the PCOR Trust Fund are to fund PCOR research, disseminate research findings, and develop a data infrastructure for PCOR. The PCOR Trust Fund has been reauthorized through 2029, through H.R. 1865 of the Further Consolidated Appropriations Act of 2020. The most recent statute specified intellectual and developmental disabilities, as well as maternal mortality, as research priorities. The statute also called for PCOR studies to include consideration of the full range of outcomes data. Specifically, the law states that:
Research shall be designed, as appropriate, to take into account and capture the full range of clinical and patient-centered outcomes relevant to, and that meet the needs of, patients, clinicians, purchasers, and policymakers in making informed health decisions. In addition to the relative health outcomes and clinical effectiveness, clinical and patient-centered outcomes shall include the potential burdens and economic impacts of the utilization of medical treatments, items, and services on different stakeholders and decision-makers respectively. These potential burdens and economic impacts include medical out-of-pocket costs, including health plan benefit and formulary design, non-medical costs to the patient and family, including caregiving, effects on future costs of care, workplace productivity and absenteeism, and healthcare utilization.1
The bulk of the PCOR Trust Fund funding (80%) is allocated for research and is made available through the Patient-Centered Outcomes Research Institute, a nongovernmental organization established by Congress for this purpose. Approximately 16 percent of the PCOR Trust Fund funding is set aside for disseminating research findings, incorporating findings into clinical practice, and training researchers in PCOR. The agency overseeing this work is AHRQ.
The remaining funding, which constitutes 4 percent of the PCOR Trust Fund, is allocated for building data capacity for PCOR and is overseen by ASPE. Specifically, Section 937(f) of the Public Health Service Act instructed the Secretary of HHS to:
… provide for the coordination of relevant Federal health programs to build data capacity for comparative clinical effectiveness research, including the development and use of clinical registries and health outcomes research networks, in order to develop and maintain a comprehensive, interoperable data network to collect, link, and analyze data on outcomes and effectiveness from multiple sources including electronic health records.2
___________________
1 https://www.ssa.gov/OP_Home/ssact/title11/1181.htm.
2 https://aspe.hhs.gov/collaborations-committees-advisory-groups/os-pcortf/about-os-pcortf.
Figure 1-1 shows how the PCOR funding and work is allocated across the three entities. This National Academies of Sciences, Engineering, and Medicine study is focused on issues relevant to ASPE’s continued work on the PCOR data infrastructure, in other words, on the priorities for the use of the 4 percent of the funding that is allocated for HHS.
As the coordinating agency for the data infrastructure investment portfolio across HHS agencies, ASPE guides the PCOR data infrastructure’s strategic framework and vision, sets funding priorities, and coordinates interagency workgroups. ASPE’s work is assisted by a Leadership Council for the PCOR Trust Fund, which includes representatives from other HHS agencies, including the Administration for Children and Families, the Administration for Community Living, AHRQ, the Assistant Secretary for Preparedness and Response, the Centers for Disease Control and Prevention (CDC), the Centers for Medicare & Medicaid Services, the Food and Drug Administration, the Health Resources and Services Administration, the Indian Health Service, the National Institutes of Health, the Office of the Chief Technology Officer, the Office of the National Coordinator for Health Information Technology, and the Substance Abuse and Mental Health Services Administration. The Leadership Council provides input on priorities for the portfolio, including projects to fund. During the period 2010 to 2019, the PCOR Trust Fund funded 53 projects, which translated to 76 agency awards, totaling approximately $131 million.
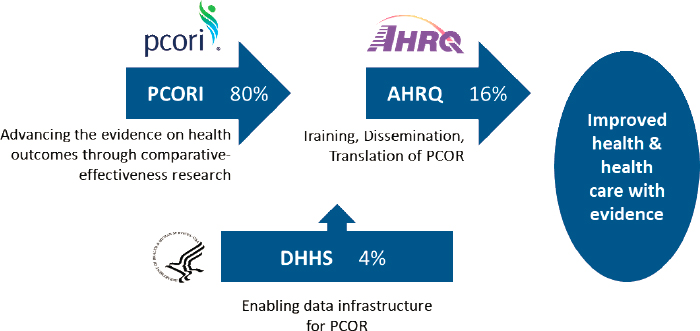
NOTE: AHRQ = Agency for Healthcare Research and Quality; HHS = U.S. Department of Health and Human Services; PCOR = Patient-Centered Outcomes Research; PCORI = Patient-Centered Outcomes Research Institute.
SOURCE: Workshop presentation by ASPE, May 3, 2021.
Figure 1-2 is a visual representation of ASPE’s current framework for the PCOR data infrastructure. The bottom row shows the main data sources feeding into the PCOR infrastructure. Data collected as part of clinical care include data collected for health care delivery and for billing purposes. Examples of primary data collected as part of research studies include data from clinical trials and national health surveys. Other examples of data sources include Medicare or Medicaid claims data; quality or outcomes data collected by health care providers for the purposes of improving health care value; Food and Drug Administration data on the safety of medications and medical devices; and CDC data on births and deaths provided by state public health authorities.
The framework describes the relationship between the data sources and the current key functionalities and focus areas (middle row) that support the research. The key functionalities are described in further detail in Box 1-1. Major building blocks are the services, standards, policies, and governance that enable the use of the data for research, described in further detail in Box 1-2. The top row shows the key data users and contributors of data. A more detailed overview of ASPE’s work and the projects funded to date will be included in the final report, at the conclusion of the committee’s review.
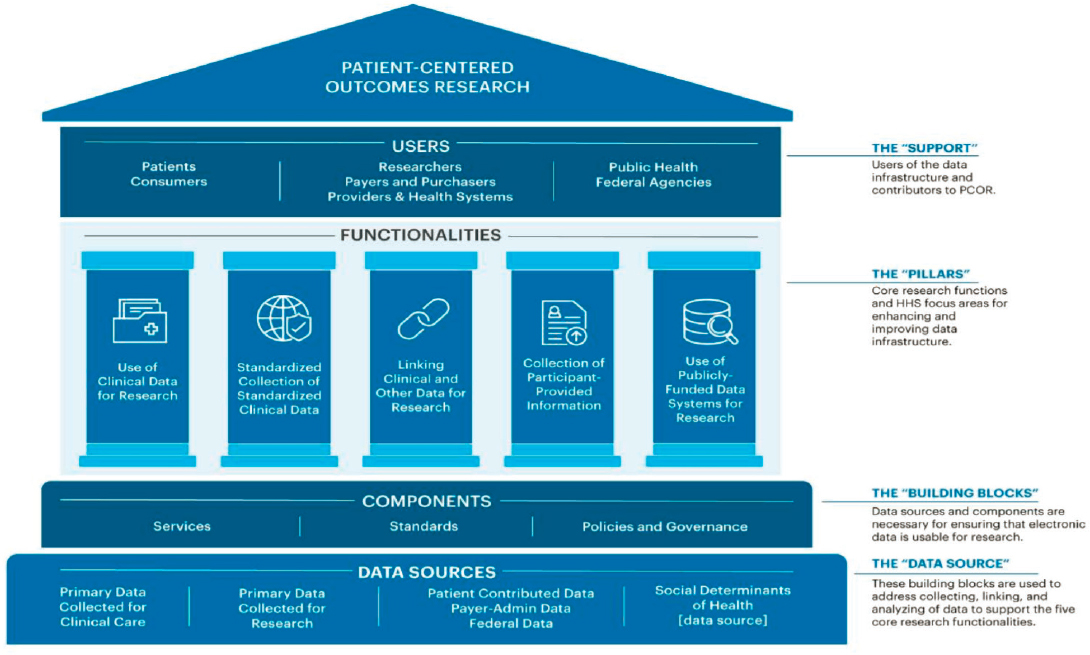
SOURCE: Workshop presentation by ASPE, May 3, 2021.
ISSUES FOR THE COMMITTEE
ASPE asked the National Academies to appoint a consensus study committee and identify issues critical to building data capacity for PCOR and for generating new evidence to inform health care decisions. The input provided by the committee will contribute to ASPE’s strategic planning for its work related to the data infrastructure over the next decade. The study is part of a broader initiative by ASPE intended to update the strategic plan in light of the reauthorization of the PCOR Trust Fund and advances in health information technology and interoperability tools in recent years.
The study is a collaboration of three units of the National Academies: the Committee on National Statistics, the Board on Health Care Services, and the Computer Science and Telecommunications Board. The consensus study committee of 15 members had a diverse membership, including experts with decades of experience, as well as emerging leaders, in the broad fields of (1) PCOR; (2) research methods, statistics, and demography; (3) computer science and data infrastructure; and (4) patient engagement and patient perspectives. Appendix A contains the biographical sketches of the committee members.
As part of its information-gathering activities, the committee was asked to organize three workshops to collect input from stakeholders on aspects of the charge developed in consultation with ASPE. The workshops focused on key topics that the committee believed would particularly benefit from broad input from a variety of data users and other stakeholders. The conclusions from each workshop are summarized in interim reports. This first interim report summarizes the discussion and conclusions from the first workshop, which focused on looking ahead at data user needs over the next decade. The second workshop in the series centered on data standards, methods, and policies that could make the PCOR data infrastructure more useful. The third workshop discussed research and data collaborations.
As an interim report focused on one in a series of information-gathering activities, the scope of this report is limited to a subset of the topics relevant to the committee’s charge and the conclusions reached by the committee are, at this stage, fairly high level. Some aspects of the topics discussed will be examined in further detail in subsequent workshops. For example, the first workshop focused on the additional data that stakeholders would like to have access to for PCOR. The second workshop will examine ways that the existing data could be better utilized to meet data needs, as well as the challenges associated with data sharing and addressing privacy concerns. After completing all of its information-gathering activities, the committee will issue a final report, which will integrate and examine these topics in further detail.
Box 1-3 shows the committee’s Statement of Task for the overall study; the committee will address this charge in its final report, integrating what
was learned from the workshops, and from all other forms of input, including public meetings with HHS staff and background documentation available on the history and operations of the PCOR Trust Fund. The final report will contain overall findings and conclusions from the study, on the basis of the committee’s further deliberations and integrated judgment on the input received and materials reviewed.
Appendix B shows the agenda for the workshop, which was held on May 3, 2021. The committee’s goal for this event was to bring together
researchers and representatives of patient organizations to understand the needs of these two important data user groups. Specifically, the goals of the workshop were to:
- Provide a high-level overview of the types of data included in the data infrastructure for PCOR.
- Identify key questions that stakeholders are most likely to want answered going forward, including general themes that cut across health conditions and circumstances.
- Discuss the implications of the broadened statutory scope for PCOR.
- Identify gaps in what stakeholders need and what the infrastructure allows. Consider both limitations in the existing data and improvements that could be made to new data collections.
- Discuss what questions cannot be answered and who is not served by the current PCOR data infrastructure.
- Discuss what HHS is best positioned to address and how the agency could maximize resources available for the PCOR data infrastructure (representing 4% of the PCOR Trust Fund), in the context of HHS’s public mission, authorities, programs, and data resources.
Invited speakers in each of the sessions were asked to reflect on the general topics above. The specific questions for each session are described in Chapters 2 through 4. An obvious limitation of any activity of this type is that only a small number of stakeholders can be invited to speak. To compensate for this limitation to the extent possible, the committee invited representatives of patient groups with a broad reach, representing a variety of different interests and medical conditions. The researchers included were also individuals with broad research interests and an understanding of the PCOR infrastructure. In addition to sessions focused on the data needs of patient groups and researchers, the workshop also included a session on health disparities research and the data needed to explore this topic in more depth. The workshop also featured a case study on data challenges encountered as part of a study related to COVID-19. Appendix C contains biographical sketches for the speakers. A recording of the workshop and the presentation slides used by the speakers are available on the National Academies’ website at www.nationalacademies.org/PCORData.
Information about the workshop was disseminated through National Academies’ mailing lists and on the project website. To collect additional stakeholder input, members of the public were invited to provide comments on topics related to the workshop (or any other topic related to the
committee’s charge), using a public input form available on the National Academies’ website.
OVERVIEW OF THE REPORT
This report is organized around the three main sessions of the workshop. Chapter 2 discusses presentations on the data needs related to health disparities, Chapter 3 focuses on patient organization needs, and Chapter 4 describes the input received from researchers. The points conveyed by the workshop participants do not necessarily reflect the views of the committee; instead, in each chapter, a summary of the input received is followed by the committee’s conclusions. These conclusions are based primarily on the input collected as part of the workshop, background documentation received from ASPE and other public sources, and the committee members’ synthesis and expert judgment. Because this is an interim report, the committee’s conclusions at this stage are big-picture conclusions, which will be integrated with additional input over the course of the study.
This page intentionally left blank.
2
Health Disparities Data Needs
This chapter summarizes presentations and discussion focused on data that could further the understanding of health disparities. Speakers participating in this session were asked to focus on the questions below. The brief overview of the input received from the presenters is followed by the committee’s conclusions.
- What are the limitations of the patient-centered outcomes research (PCOR) data infrastructure in terms of
- disparities in the data, including knowledge about patient outcomes, taking into consideration differences in patient preferences and values?
- challenges associated with using the data to understand disparities and health equity?
- lack of data on some populations?
- What are opportunities and priorities for enhancing data capacity in this area?
- What data capacity challenges is the U.S. Department of Health and Human Services (HHS) best positioned to address in the context of its public mission, authorities, programs, and data resources?
The first speaker, Karen Joynt Maddox, Washington University in St. Louis, argued that one of the main reasons why it is challenging to use health data for research in general, and for PCOR in particular, is that the health and personal data that are available are typically not collected for PCOR to begin with. Instead, the reasons for collecting the data tend to
be for recordkeeping for clinical care or for payment. As a result, the data available are not centered on the person and do not enable an understanding of the person’s context, including his or her medical journey, demographic information, health status, and comorbidities, as well as the social context in which the person lives.
Data that could be useful for studying disparities are collected in a variety of settings and are housed in separate databases. To take full advantage of the information, it is necessary to link these data, something that is often difficult to accomplish. Figure 2-1 is an illustration of these data silos. Joynt Maddox noted that one positive characteristic of the data collected on the social determinants of health is that some of the information available is particularly detailed. This includes, for example, data from hospitals’ electronic medical records modules, as well as data from social work and care coordination assessments.
Joynt Maddox highlighted Z-codes, which are a subset of the codes contained in the International Classification of Diseases (Tenth Revision, Clinical Modification, or ICD-10-CM). Z-codes are used to capture information such as the factors that influence a person’s health status and the reason for contact with health services. This includes information about employment, family characteristics, housing, psychosocial characteristics, socioeconomic characteristics, and nonadherence (e.g., intentional under-dosing of medication due to financial hardship). While these codes are widely available and detailed, they appear at a lower-than-expected rate in records, which suggests that they may be underused.
As an example of how data silos hinder the ability to answer policy questions, Joynt Maddox discussed efforts to answer the question of how
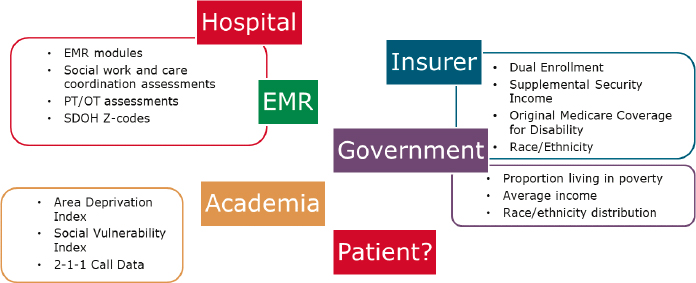
NOTES: EMR = electronic medical records; OT = occupational therapy; PT = physical therapy; SDOH = social determinants of health.
SOURCE: Workshop presentation by Karen Joynt Maddox, May 3, 2021.
potential Medicaid expansion in Missouri could impact equity in hospitalizations for complex cancer surgery. Box 2-1 summarizes the databases that could potentially be considered to examine this question, along with their limitations. None of these datasets has reliable information on social determinants of health.
Box 2-2 summarizes data sources that could be considered to examine another question with policy implications: the impact of the Hospital Value-Based Purchasing Program on equity in posthospitalization functional status.
The ideas shared by Joynt Maddox for improving the data available in this area were to (1) include hospital and state identifiers in national datasets, such as the National Inpatient Sample, and other related datasets from the Healthcare Cost and Utilization Project; (2) create mapping and linkages across data sources; (3) incentivize the collection of Z-codes relevant to social determinants of health and data on functional status through payment policy; and (4) make data available more quickly and more easily accessible for research and policy decisions.
Megan Morris, University of Colorado Anschutz Medical Campus, discussed data needs related to disability status. She noted that there is growing evidence that individuals with disabilities experience significant health
and health care disparities. She discussed recent work she conducted with support from the Patient Centered Outcome Research Institute (PCORI) to identify research priorities for advancing equitable health care for individuals with disabilities. As part of the study, she collected input from a range of stakeholders, including researchers, patient advocacy organizations, health systems, payers, policy makers, and agencies within the HHS. The key finding from this work was the need to improve data on people with disabilities.
Morris said that data on disabilities are rarely collected or documented in common data sources, such as electronic health records, patient experience surveys, or in big data sources, such as claims data. ICD-9-CM or ICD-10-CM codes are often insufficient for identifying who has a disability. For example, for a study of individuals who had total laryngectomies and were nonverbal, Morris reviewed medical charts and found that less than 30 percent of patients with this condition had an ICD-9-CM code for their communication disability in their medical record (likely because this code does not affect payment for the service).
Morris argued that the priority need in this area is for data that make it possible to (1) identify the quality of health and health care of individuals with disabilities; (2) develop, implement, and measure the effects of interventions; and (3) provide accommodations to individuals with disabilities.
In 2011, HHS released data collection standards that included standards for data on disability status. The HHS guidelines included six questions, and Morris suggested that these six could be integrated into electronic health
records, along with an additional question on communication disabilities. The question of communication disabilities has already been tested for potential inclusion in several national surveys. Box 2-3 reproduces these seven disability questions. Morris said her research indicates that these questions would be well received by patients.
To reduce disability disparities, Morris suggested (1) recognizing persons with disabilities as a population at high risk for experiencing health disparities; (2) supporting initiatives and infrastructure for documenting disability status at the point of care; (3) ensuring that disability demographics and accessibility quality measures are included in surveys; and (4) developing methods to identify persons with disabilities in claims data.
Mitchell Lunn, Stanford University, discussed health disparities among and the lack of data for sexual- and gender-minority populations. Lunn said that data collected by the Gallup organization indicate that sexual and gender minorities represent about 5.6 percent of the U.S. population. However, the lesbian, gay, bisexual, transgender, queer (LGBTQ+) population is a heterogeneous group, and the umbrella term encompasses people with differing health needs. Further, high-quality, detailed data on the breakdown of sexual and gender minorities by race and ethnicity are not available.
Lunn emphasized the differences among the concepts of sexual orientation, gender identity, and sex assigned at birth, and argued that data on sexual orientation and gender identity are inadequately collected in most clinical and research settings. As an example, the sexual orientation item
in the electronic health records used by Stanford Medicine collects information only on the identity construct, not on sexual attraction or sexual behavior. The options available to describe sexual orientation are more limited than the range of terms used by the community (for example, “pan-sexual” and “queer” are not available) and only one option can be selected, although a write-in option is available. In terms of gender identity, Stanford Medicine’s electronic health records also limit the answer to one option, with a narrower range of options than the terms used by the community.
To illustrate limitations in a research setting, Lunn discussed the All of Us program, a National Institutes of Health (NIH) research program that aims to enroll and collect data from more than one million participants. The sexual orientation and gender identity questions used by All of Us also measure the identity construct. The items were developed with input from subject matter experts and the community, and contain terms that are more commonly used by the community. It is also possible to select more than one answer for both sexual orientation and gender identity. Some of the options become available in the form of a submenu, and Lunn argued that it would be preferable to include more items on the initial list, since that would give respondents more options to consider that might be applicable to them. He added that some of the terms used in the NIH program are antiquated and are being revised.
Lunn also discussed the PRIDE study, a large-scale national health study of people who identify as LGBTQ+ or as another sexual or gender minority. He said that with multiple selections allowed in that study, around 35 percent of participants in the sample select more than one option for sexual orientation and around 18 percent select more than one option for gender identity. The terms used are revised every few years with community engagement.
Lunn argued that current clinical approaches, such as electronic health records systems and data models, do not allow patients to comprehensively report their sexual orientation and gender identity. Not using people’s stated identity (e.g., grouping or administratively classifying them instead) could result in the loss of valuable data that may have health implications. Research studies can serve as models for developing sexual orientation and gender identity data standards, because these studies tend to involve researchers who are focused on this field. Lunn also emphasized that sexual and gender minority terms tend to change at a rapid pace, and therefore frequent re-evaluation with community engagement is critical to selecting the optimal terms to use.
Kaleab Abebe, University of Pittsburgh, echoed comments made by other speakers related to some of the key challenges associated with the data infrastructure for PCOR. First, he said, regardless of what data are collected and in what context they are collected, it is important to ask
whether or not the data are representative of the population that could benefit from them. Second, data being housed in disparate locations and being owned by different entities leads to a substantial barrier to their use, and it is important to think of ways to curate and harmonize these data.
Abebe noted that the various data sources have varying degrees of completeness and representativeness. When these data sources are linked, the resulting datasets have their own patterns of data gaps and lack of representativeness, particularly in terms of the populations who could benefit from the availability of the data the most. He described this as “disparities on top of disparities.” If data are not available or are incomplete, it is difficult to act on the information in a way that could benefit people. Abebe also underscored the importance of efforts to standardize data but, again, without losing sight of the larger underlying question of whether the data have gaps in terms of the populations that are covered.
Thinking about opportunities, Abebe mentioned the example of the clinical trial infrastructure in the United Kingdom, which not only facilitates the carrying out of trials, but also aggregates the data that have been accumulated as part of trials. In the United States, it may be possible to build on what already exists to link more of the data. Abebe also highlighted opportunities to build on work already started that puts patient preferences in the center, including the development of an interoperable electronic care (eCare) plan. He also emphasized the need to develop metrics for the data infrastructure portfolio to enable researchers to better understand successes and failures and potentially utilize this information when considering future work.
Abebe noted that the social determinants of health can change over time, so measures need to be developed with the understanding that they need to be flexible. He also argued that there should be more of a spotlight on disparities, not only on measuring them but also on capturing metrics for ways of addressing disparities, whether in the form of interventions, therapeutics, or other potential solutions.
Thomas Sequist, Harvard University and Brigham and Women’s Hospital, discussed data needs with a particular focus on Native Americans. He said that during the COVID-19 pandemic it took a long time to recognize the impact of the pandemic on Native American communities, in part because of an inability to generate data at a level that would make it possible to understand the health issues specific to American Indians. One reason for this is that small sample sizes often result in data on American Indian populations being combined with data on other populations. Another challenge is that many studies on American Indians draw on data available from the Indian Health Service, but only about half of this population receives health care through that agency. The American Indian population that is left out of research that relies on that agency’s data is heavily skewed toward an urban population.
Sequist said that an important step toward addressing these challenges would be to develop more robust ways to identify American Indians in all existing datasets, which would make it possible to better characterize their experiences. Information about people’s tribal affiliations would further help in understanding their culture and the experiences they may have related to their health.
Sequist pointed out that social determinants of health come into play not only at an interpersonal level, but also at a geographic level, so better data are needed to understand these risk factors at that level. He discussed how geography can be relevant in addressing inequities, arguing that the use of geography needs to be carefully considered and standardized to better understand the interplay between it and race, ethnicity, and language.
Concerning language, Sequist highlighted the need for accurate and reliable data, noting that lack of standardization in the way language information is collected has been a challenge both for research and for improving health care. For example, he underscored the need to differentiate among someone’s preferred language, their primary language, the languages in which they are fluent, and the languages in which they have achieved health literacy. The COVID-19 pandemic, which affected non-English-speaking patients in a particularly severe way, has illustrated the need for language-appropriate care.
Sequist said that the array of information that exists on patient-reported outcomes does not always reflect the types of outcomes that patients themselves value or the experiences that they are having with the system, particularly concerning race-specific issues, ethnicity-specific issues, and language-specific issues. The relative value people place on various outcomes is likely to depend on their background, and substantial investments would be needed in patient-reported outcomes projects to begin to really understand those variations.
CONCLUSIONS
In this section we summarize the committee’s conclusions based on the presentations and discussion. The research of those experts who presented at the workshop focuses on health disparities in a variety of areas, affecting various populations. The underlying theme that emerged from the presentations was that there are data limitations for a variety of populations, and that these limitations hinder the ability to understand health disparities.
CONCLUSION 2-1: Health disparities can occur across a broad range of characteristics and populations. Data limitations affect the ability to identify and understand these disparities in many areas. Data for specific populations are sometimes unavailable or are not representa
tive. In other cases, the data might not be timely or might have other gaps that make it difficult to understand the impact of changes over long periods of time.
A fundamental reason for the data limitations that make it difficult to answer questions important for PCOR is that most of the data available for research are not primarily collected for research purposes. While research questions require a relational or integrative perspective, the data collected tend to be transactional, that is, collected for payment or treatment purposes, and therefore do not vary according to most personal characteristics. This has several implications for the data available. First, the data collected are typically limited to or organized within subpopulations (for example, those insured by Medicaid or Medicare). People who are uninsured, including those who have limited access or interactions with health care services, are likely to be underrepresented in many databases. Second, the information collected (and the absence of what is not collected) often makes the data poorly suited to answer a variety of research questions. Third, those who collect the data do not necessarily have an obvious incentive to collect information in a way that is useful for secondary purposes, such as research. The workshop identified a variety of data needs and potential opportunities for enhancing the data infrastructure, and these deserve further attention.
CONCLUSION 2-2: The data available for patient-centered outcomes research are often collected for reasons other than research, which limits their usefulness. Opportunities exist for increasing the utility of the data infrastructure by carefully considering the multiple uses to which the data might be applied.
The data that do exist are stored in a variety of databases across a fragmented health care system. The workshop identified data silos (e.g., within settings, at a point in time, or for a specific payer) as a major barrier to the efficient use of the information that is available.
CONCLUSION 2-3: Existing data on the social determinants of health are found in a variety of databases. Barriers to linking across these data silos represent a major challenge to understanding how social determinants of health affect health outcomes.
The workshop made it clear that the data available do not capture the complexities that are necessary to understand in order to determine how people’s characteristics and experiences influence outcomes. The speakers identified several potential ways of capturing more of these complexities, and they emphasized the need to build flexibility into the data collection
systems to allow them to adapt as both the terminologies and the available technologies for capturing and processing data evolve.
CONCLUSION 2-4: Existing data do not capture the richness of people’s characteristics and experiences. While such limitations are to be expected, opportunities exist for capturing data that are better able to characterize these complexities. A robust data infrastructure builds on the strengths of what is available today and has the flexibility to adapt, both as measures and terminologies become obsolete and as new technologies emerge.
The workshop underscored the magnitude of the data gaps in the area of health disparities. Improving the data available for understanding and addressing disparities would require an effort concentrated on this goal.
CONCLUSION 2-5: Prioritizing and improving the collection of data can lead to a better understanding of health disparities and to potential solutions for reducing disparities.
3
Patient Perspectives on Data Needs
This chapter summarizes data needs conveyed by patient organizations. Speakers in this session were asked to focus on the questions below. The brief overview of the input received from the presenters is followed by the committee’s conclusions.
- Looking ahead, what are the main data needs?
- What are the implications of the (recently broadened) statutory scope for patient-centered outcomes research (PCOR)?
- What questions cannot be answered and who is not served by the current PCOR data infrastructure?
- What new data sources could be incorporated into the PCOR data infrastructure?
- What data capacity challenges is the U.S. Department of Health and Human Services (HHS) best positioned to address in the context of its public mission, authorities, programs, and data resources?
Rebekah Angove shared her perspective based on her role as vice president for patient experience and program evaluation at the Patient Advocate Foundation (PAF), a nonprofit organization that provides case management services and financial aid to those with chronic, life-threatening, and debilitating illnesses. Angove also previously served as engagement director of REACHnet, a clinical research network that is part of the National Patient-Centered Clinical Research Network.
As part of its work focused on assisting patients, PAF also collects data from patients with the goal of translating evidence into research and
policy work focused on improving health care and the patient experience. Angove said that because PAF works with patients who experience access and affordability challenges, its patient and caregiver network represents populations that are often underrepresented in research initiatives because they are underinsured or uninsured and, consequently, are less likely to be represented in large health care systems that have robust data collections and clinical trials.
Angove discussed challenges associated with obtaining patient agreements for participating in data collection as well as broader engagement in research. PAF’s experience and the research it has done on this topic indicate that most patients have a very limited understanding of research, and especially of terminology such as “comparative effectiveness” research and “patient-centered outcomes” research. Patients are also often confused or uninformed about how research data are used and the implications of giving their consent for the use of their data. She argued that confusion in these areas leads to mistrust or distrust.
Angove highlighted several characteristics of meaningful patient engagement. First, she noted that engagement requires careful thinking about the range of experiences that are included in order to achieve representativeness. Beyond the dimensions of diversity discussed in Chapter 1, diversity along additional dimensions such as treatment experiences, life experiences, urban vs. rural, and ability to pay for and access health care also need to be represented. If the patients engaged in and contributing to research are not representative of a broad range of experiences, the findings could exacerbate disparities. Angove also underscored the role transparency plays in meaningful patient engagement. This means being clear about who owns the data and how the data are being used, as well as better communication about how patients are involved in the process.
Angove argued that meaningful patient involvement means involvement in all activities that are part of PCOR, and not just involvement in an activity that is specifically carved out for patient involvement (for example, recruitment and patient committees). For example, patients could be more involved in conversations about methodology, about how the results are interpreted, or about how information about the research is communicated. Angove emphasized that the fact that the data are patient reported does not necessarily mean they are patient centered. Validated measures for patient-reported outcomes (PROs) have historically been developed without patient involvement. For example, when patients are involved in projects, they often point out issues related to the PRO measurement scales that are used, but ultimately their input is not incorporated because researchers are reluctant to deviate from PRO measures that have been validated.
Another aspect of meaningful patient engagement discussed by Angove is training in how research is done, not only for patients but also for the
researchers themselves, as well as policy makers and health care workers. This is particularly important given the sensitive nature of the health information that patients are being asked to share. Angove also emphasized the importance of communicating to patients the value of their contributions.
Gary Epstein-Lubow, Brown University, discussed his experiences as team leader for the stakeholder engagement team for the National Institute on Aging’s Imbedded Pragmatic Alzheimer’s Disease and AD-related Dementias Clinical Trials Collaboratory (IMPACT Collaboratory). The IMPACT Collaboratory’s goal is to build the nation’s capacity to conduct pragmatic clinical trials of interventions imbedded within health care systems for people at risk of dementia, people living with dementia, and their family members and care partners.
While there are no disease-modifying treatments available for dementia, nonpharmacologic interventions show promise, although they have had limited adoption. Epstein-Lubow said that to address this, embedded pragmatic clinical trials (ePCTs) need improved patient-centered outcomes data that are systematically available. Patients and caregivers are important stakeholders who provide input to the trial implementation, and the interventions need to be integrated into the routine clinical flow and not add a reporting burden. To do this, it is essential for electronic health records to capture patient-centered outcomes in a systematic way, with special attention paid to confirming that data are collected from underrepresented groups and groups disproportionately harmed by dementia. Finally, outcomes of ePCTs must be relevant and usable by decision makers, including health care systems.
Epstein-Lubow said that there are special considerations for ePCTs when it comes to dementia research. From the perspective of patients, applicable ethical considerations and regulations deserve particular attention, because people living with dementia are a vulnerable population and there are questions about their capacity to provide informed consent and to self-report their preferences. Another area that deserves attention is the role of care partners and family members, including the potential for linking caregiver data with patient data.
Concerning data needs in the area of dementia, Epstein-Lubow highlighted five needs, namely the need for:
- information that can lead to improvements in person-centered care;
- improved reporting on functional status, including physical, social, occupational, and emotional functioning, in addition to cognitive functioning;
- data linkages between information provided by people living with dementia and their caregivers;
- strategies for capturing information about lived experiences; and
- methods for standardizing proxy reporting for people who have partial capacity or who lack capacity to report directly.
Epstein-Lubow argued that the broadened statutory scope for PCOR increases opportunities for learning about patient-centered outcomes but also involves some risks. For example, if inadequate attention is paid to underrepresented groups, including members of groups at higher risks of negative health effects of dementia, this could lead to underrepresented patient-centered outcomes data in these areas. There is also the risk of potential added burden for family members and caregivers in their roles as proxy respondents and missed opportunities for data linkage in the case of missing data from caregivers.
Additional data challenges exist for research on dementia, according to Epstein-Lubow, including the following:
- There is no standard measure set for people living with dementia.
- There is no standard measure set for family caregivers.
- Quality measures for dementia care are optional in most reporting systems.
- There are challenges regarding the collection of patient-centered outcomes from people living with moderate or severe dementia.
- Accommodations for data collection may be required for people with limited health literacy.
- There are methodological challenges associated with linking data from people living with dementia and their caregivers.
Epstein-Lubow highlighted several dementia measures that are part of the Merit-Based Incentive Payment System (MIPS), which is a Centers for Medicare & Medicaid Services (CMS) program that eligible health care clinicians can participate in to report data to better connect care quality with Medicare payments. These dementia measures are optional, but Epstein-Lubow argued that they could be required. The measures highlighted include
- dementia-associated behavioral and psychiatric symptom screening and management;
- dementia: cognitive assessment;
- dementia: education and support of caregivers for patients with dementia;
- dementia: functional status assessment; and
- dementia: safety concern screening and follow-up for patients with dementia.
In addition, Epstein-Lubow suggested that the Consumer Assessment of Healthcare Providers and Systems questions on patient and caregiver experience of care could be expanded to include proxy reports of dementia.
To strengthen the PCOR data infrastructure in ways that could benefit people living with dementia, Epstein-Lubow said that HHS would be particularly well positioned to address one of the recommendations made by the public members of the HHS Advisory Council on Alzheimer’s Research, Care and Services, which urged HHS to “Encourage further development, evaluation, and use of health care models for AD/ADRD that align performance measures, the experience of care by persons living with AD/ADRD and their caregivers, and payment.”1
Epstein-Lubow further suggested using the definitions of care “value” used by CMS and studying models that enhance value. One way to do this would be to rely on the CMS “Meaningful Measures” initiative, including use of new care planning codes, the annual wellness visit, and the MIPS dementia measures discussed earlier.
Elisabeth Oehrlein discussed insights from her work at the National Health Council (NHC), a nonprofit association of more than 140 health-related organizations, including leading patient advocacy groups. She identified a list of key data needs based on what the NHC’s patient groups are hearing from the patients these organizations serve, and based on NHC’s work in the areas of regulations, real-world evidence, and value assessment:
- patient-centered outcomes and impacts that really matter to patients, collected consistently;
- burden, including costs incurred by patients and their families;
- social determinants of health (for example, transportation, housing);
- evidence based on representative populations;
- quality and satisfaction with care, defined from the perspective of patients;
- accessibility of the research results to patients; and
- interoperability.
Oehrlein said that in addition to measuring the outcomes and impacts that patients truly care about, it is also important to use language that patients will use. For example, in the case of alopecia areata (an autoimmune disease that causes hair loss), the patient-reported outcome measure has traditionally been the percentage of the skin that is covered in hair, but talking to patients made it clear that what they care about is not
___________________
1 https://aspe.hhs.gov/public-members-advisory-council-alzheimers-research-care-and-services-2020-recommendations#clinical, see recommendation 5.
necessarily the difference between a 20 percent or 40 percent improvement in skin covered, but rather whether or not they need to wear a wig.
In terms of increasing patient accessibility of the research results and evidence, Oehrlein mentioned the expansion of dashboards that patients can use to enter certain criteria and find out what treatments might work better for them or what the outcomes experienced by others with similar conditions have been. These types of communication vehicles could be a model going forward.
To further illustrate the types of outcomes that matter to patients, Oehrlein discussed findings from a Food and Drug Administration report focused on chronic fatigue syndrome and myalgic encephalomyelitis (Table 3-1).2 The table shows that many aspects of a patient’s experience that are traditionally considered important to measure are indeed important to patients. These aspects include disease-related impacts, feelings, and functions. However, patients also care about and want more information on treatment-related impacts, financial impacts, and caregiver impacts. This type of patient input can help narrow the scope of the data that are collected in order to better focus resources and reduce the burden on patients.
Oehrlein said that the broadened statutory scope for PCOR presents opportunities to more effectively assess treatment alternatives and value from the patients’ perspective. In particular, she finds that patient advocates and patients are often surprised to discover that data on out-of-pocket costs and other costs important to patients have not been systematically collected. Having these types of data available would lead to more holistic evidence relevant to patient decision-making and more informed decisions as patients navigate their options and understand what the treatment impacts might be, beyond clinical outcomes. These types of decisions increasingly have an impact on patients’ access to care.
As an illustration of a model for moving forward, Oehrlein discussed the work of the EveryLife Foundation for Rare Diseases. Its report assessing the total economic burden of rare diseases was born out of the realization that the data that have been collected to date on direct medical costs really do not reflect the full patient experience, especially when it comes to rare diseases.3 EveryLife Foundation researchers have thought carefully about which costs are important to patients and how those data might be collected.
In terms of data needs that HHS would be best positioned to address, Oehrlein highlighted the need for better data for underserved populations and communities. Supporting dashboard-type solutions to make more of the data available to inform individual patient decisions would also be
___________________
2 https://www.fda.gov/media/86879/download.
3 https://everylifefoundation.org/wp-content/uploads/2021/02/The_National_Economic_Bur-den_of_Rare_Disease_Study_Summary_Report_February_2021.pdf.
| Disease-Related Impact on Feelings and Function | Treatment-Related Impacts | Financial-Related Impacts | Caregiver-Related Impacts |
|---|---|---|---|
|
|
|
|
SOURCE: U.S. Food and Drug Administration (2013). https://www.fda.gov/media/86879/download. Workshop presentation by Elisabeth Oehrlein, May 3, 2021.
useful. The COVID-19 dashboard operated by the National Center for Advancing Translational Sciences is an example of a government initiative along those lines.
Bray Patrick-Lake, Evidation Health, shared her insights in part based on her career working in patient advocacy, leading a patient foundation, and working on national research programs, such as All of Us and PCORnet. Her current work is focused on measuring what matters most to patients in everyday life. Evidation Health is a digital research and health engagement company whose members participate in research studies. Members provide person-generated health data, which enable continuous monitoring of health outcomes at the individual level. The platform collects 750 million data points daily. The data include individually generated, individually permissioned data, such as data from wearables and environment data, as well as system-generated individually permissioned data, such as data from electronic health records. Figure 3-1 illustrates the range of data sources considered by Evidation.
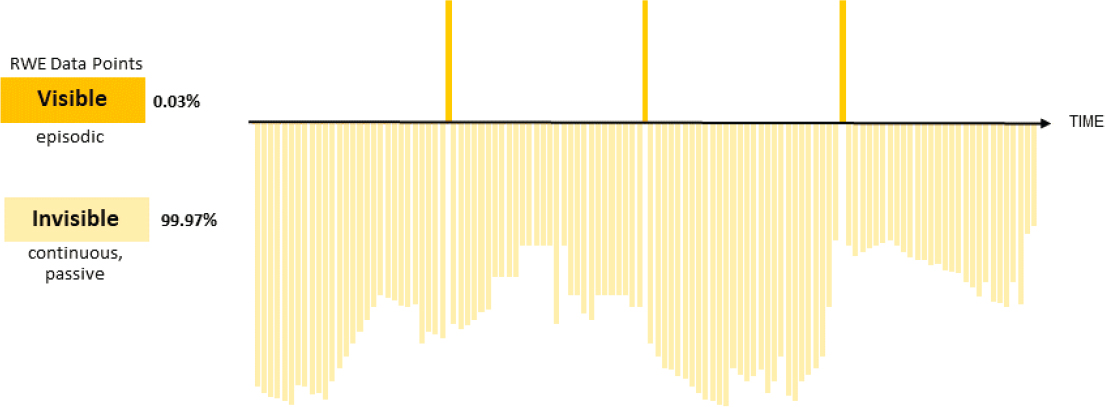
Patrick-Lake argued that the traditional sources of data (shown on the left side of Figure 3-1) provide episodic snapshots of the experiences of patients living with disease over time. Most of what constitutes people’s lives, and therefore the richest data about patients’ experiences with disease,
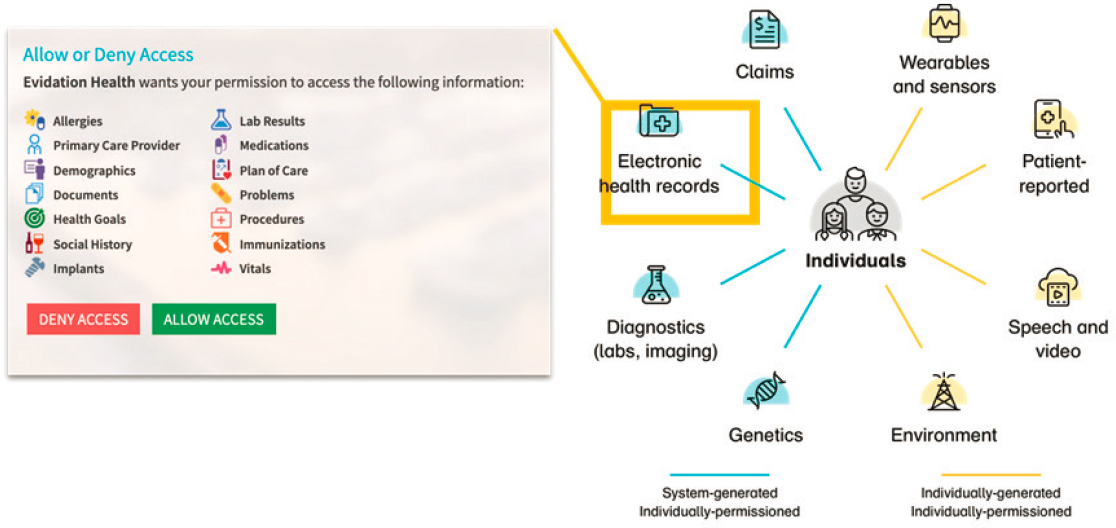
SOURCE: Workshop presentation by Bray Patrick-Lake, May 3, 2021. Evidation Health (2021).
is currently invisible to the health care system. Figure 3-2 illustrates how real-world evidence data points (i.e., evidence obtained from real-world data, such as data generated during routine clinical practice) contrast with data from digital technologies that have the potential to continuously and passively collect data, without substantial burden to patients.
Patrick-Lake argued that digital technologies that continuously collect data have the potential to result in:
- better characterization and understanding of living with the disease;
- better understanding of disease progression;
- earlier identification of at-risk individuals;
- real-world, objective Quality of Life and Activities of Daily Living measures; and
- pattern detection for public health.
Patrick-Lake echoed a point made by other speakers, namely that traditional sources of real-world data might not capture what is truly important to patients. For example, a measure used in the context of cardiac care is mortality, but a patient living with cardiac disease would more likely want information on how to improve his or her quality of life, what the progression of the disease might be like, and how the disease might impact activities of daily living over time.
As an illustration of how data from wearable devices can greatly enhance real-world data, Patrick-Lake suggested considering two asthma patients who seem to be nearly identical based on traditional sources of real-world data: they both have moderate or severe asthma; they are both nonsmokers; they are on the same inhaled medications; and they are both adhering to their physician-prescribed treatments. In terms of symptom control, one person might report waking up often (every night or almost every night) due to asthma symptoms, while the other reports waking up 2 or fewer days a month due to asthma symptoms. When data from (the same brand of) wearable device are added, it becomes clear that the first person is asleep 49 percent of the time, while the second person is asleep 90 percent of the time, while in bed.
Patrick-Lake argued that digital technologies can result in data that accelerate and enhance clinical care, accelerate clinical research, and improve public health. Examples discussed included predicting flare events in an autoimmune condition using wearable and survey data; enhancing recovery modeling for limb surgeries with personalized predictions of outcome tailored to individual characteristics; and early detection, monitoring, and management of COVID-19 in everyday life.
For a potential roadmap of how to achieve the full potential of person-generated health data and digital clinical measures, Patrick-Lake referenced
SOURCE: Workshop presentation by Bray Patrick-Lake, 2021. Evidation Health (2021).
The Playbook, a document released by the Digital Medicine Society.4 She highlighted the need for standards for organizing and analyzing digital data and to serve as a foundation for further developing methodologies for their use. There is also a need to develop an evidentiary framework, which would make this type of data more broadly accepted in health care, research, and public health settings.
Patrick-Lake argued that HHS could have a role in developing incentives and rewards that could reduce barriers to collaboration and promote the use and reuse of innovations. She said that there is also need for policy leadership to advance data rights and the work of the National Human Genome Research Institute’s Ethical, Legal and Social Implications Research Program, which supports the appropriate balance between individual protections and public benefit, ensuring that individuals are well informed and protected against discrimination based on their digital specimens.
CONCLUSIONS
Representatives of patient organizations argued that PCOR data are often not focused on the types of issues that are truly important to people and that would enable them to find answers to the questions they tend to have about their treatment options and potential outcomes. Information on costs was highlighted as particularly important, which is in line with the goals of the recently broadened scope of PCOR to take into consideration “the potential burdens and economic impacts of the utilization of medical treatments, items, and services.”
CONCLUSION 3-1: The patient-centered outcomes research data infrastructure has not reached its full potential to provide data that can answer questions that matter to patients and enable them to make informed decisions. Information about the cost of care was highlighted among the types of data that would be particularly useful.
While data on patient-centered outcomes are available in many areas that are important to patients, the information is rarely available in ways that would make it truly accessible to them for decision-making purposes. More widespread dissemination of information that is easy to use could also increase engagement.
CONCLUSION 3-2: Dissemination and translation of the research findings could be greatly enhanced by using forms of communication that are relevant to those outside of the research community.
___________________
This page intentionally left blank.
4
Researcher Perspectives on Data Needs
This chapter summarizes data needs conveyed by researchers. Speakers in this session were asked to focus on the questions below. The chapter also discusses a case study on the use of the patient-centered outcomes research (PCOR) infrastructure to study whether vitamin D can reduce the burden of COVID-19. The chapter concludes with the committee’s conclusions.
- Looking ahead, what are the main data needs?
- What are the implications of the (recently broadened) statutory scope for PCOR?
- What questions cannot be answered and who is not served by the current PCOR data infrastructure?
- What new data sources could be incorporated into the PCOR data infrastructure?
- What data capacity challenges is the U.S. Department of Health and Human Services (HHS) best positioned to address in the context of its public mission, authorities, programs, and data resources?
David Meltzer, University of Chicago, discussed the use of existing data, including PCOR datasets, to conduct research on whether vitamin D could reduce the burden of COVID-19. Box 4-1 summarizes some of the key studies to date, including the studies initiated by Meltzer at the beginning of the pandemic, using University of Chicago data. This case study was intended to illustrate a specific application of how the data infrastructure can be used to study an emerging health question, and how research projects can build on each other. Box 4-1 illustrates limitations and sum-
marizes Meltzer’s observations related to the usefulness of the PCOR data based on this work.
Andrew Bazemore, American Board of Family Medicine, noted that although we live in a time of unprecedented health-data availability, there are also some structural blind spots in the U.S. health care system. He cited Kerr White’s research on the ecology of medical care and the notion that out of 1,000 people in a community in a given month, 750 might experience illness or injury, 250 will seek primary care, and 10 will be hospitalized, of which just one will be hospitalized in an academic health center,
in other words in the type of place where most of the research is being conducted.1 While Kerr White’s original study was published in the early 1960s, this “ecology” has not changed. Bazemore said that it is important to understand where people land within the broader health care setting, and where the borders are between wellness and illness, between illness and care-seeking, and between primary care and the hospital, in order to
___________________
1 K.L. White, T.F. Williams, and B.G. Greenberg. (1996). The ecology of medical care. Bulletin of the New York Academy of Medicine 73(1), 187–212.
better understand how to provide access to high-quality care that is truly patient-centered.
Bazemore noted that primary care, which is the largest platform for health care delivery, is not well represented in the data available. For example, about 0.3 percent of National Institutes of Health (NIH) research funding ends up in family medicine research settings. A study that looked at the first six cycles and then the subsequent six cycles of funding from PCORI found that between 18 and 30 percent involved primary care sites, even though about half of U.S. health care delivery happens in those settings. Even in the case of studies that involved primary care sites, typically their role was focused on patient recruitment. Places where patients with the highest risk of poor patient-centered outcomes are receiving care, including safety net clinics, federally qualified health centers, small health clinics, and rural health clinics, would be even less likely to be included.
Bazemore said that it would be useful to better understand patients’ experiences in primary care settings, including how they differ from the experiences of those who receive care from a specialist, in an emergency room, or in other places. It would also be important to understand how the characteristics of primary care influence patient outcomes. Patients often report that what is important to them is that their primary care doctor involve them as much as they want to be involved in their health care. Information about community health risk factors facing patients would provide further context.
Among the data sources that are missing from the current PCOR data infrastructure, according to Bazemore, are not only primary care practices themselves but also two other data sources: primary care registries and health information exchanges focused on primary care and the safety net. On the analytical side, Bazemore noted that a major concern is that new technologies such as artificial intelligence and machine learning do not typically involve primary care patients in their algorithm development. This has implications for the data that are being generated for PCOR.
Bazemore also underscored the need to incorporate social determinants of health data into the data environments being built. This includes geo-coded secondary ecological data, ranging from individual variables to indices, such as the social deprivation index, the area deprivation index, and the social vulnerability index. Patient-reported data on social determinants of health are also needed, in combination with the ecological proxies. This information together can enable researchers to really understand the patient experience and the dynamic neighborhood features that inform and complement the patient perspective.
Kurt Stange, Case Western Reserve University, began by saying that as a family and public health physician, he has spent his career doing “stealth” research, trying to understand how to advance health and health care for
whole people in a system that is designed to fragment them into their parts. The problem for PCOR is not only fragmented and siloed data but also a system that is designed for fragmentation in data use.
Stange raised the question of whether it would be possible to shift the model from trying to use data to drive quality from the top down to using data to support the local agency of those on the front lines who are trying to integrate, personalize, and prioritize care for all people. In the effort to solve the puzzle of health and patient-centered health care, the current approach tends to divide things up into parts: diseases, risk factors, risk groups. The parts are valued, but efforts to integrate the whole are not sufficiently supported.
Regarding specific needs, Stange highlighted data that would support the functions of integrating, personalizing, and prioritizing care for whole people. There is also a need to support care for people whose health needs cannot be addressed by relying on a single disease label, or a risk label, or a group label. Linking different sectors affecting health is also necessary.
As a starting point for addressing the prioritizing function, Stange cited a 2015 National Academies of Sciences, Engineering, and Medicine Vital Signs report that provided a useful framework for identifying core metrics for assessing health and progress in health care.2 The report proposed the following criteria for core measures:
- importance for health,
- strength of linkage to progress,
- understandability of the measure,
- technical integrity,
- potential for broader system impact, and
- utility at multiple levels.
Stange argued that this is an efficient and effective way of thinking about data. He noted that the report also provides guidance on measuring performance for useful PCOR domains. Stange said that the broadened statutory scope of PCOR provides an opportunity to focus on the whole as well as the parts. It also provides opportunities to support those on the front lines trying to contextualize care, as well as to support relationship-centered care.
Concerning the question of who is poorly served by the current PCOR data infrastructure, Stange underscored previous points about the limitations of the data on people living with multiple chronic conditions and various disadvantaged groups. He added that the data also have limitations
___________________
2 Institute of Medicine. (2015). Vital Signs: Core Metrics for Health and Health Care Progress. Washington, DC: The National Academies Press.
for those who are not “helpfully defined by their disease” or are defined by other data collected for another purpose. The health care system tends to offer people a disease label, but that is not necessarily the label or the data most helpful to them in terms of what is important in their lives.
For additional data that could be incorporated into the PCOR data infrastructure, Stange suggested the Person-Centered Primary Care Measures, which he and his coauthors developed based on what patients, clinicians, and (to a lesser extent) payors said was important to them in health care.3 Box 4-2 shows these measures, which Stange said are widely used and are also pending endorsement by the National Quality Forum and the Centers for Medicare & Medicaid Services (CMS) for use in the CMS Quality Payment Program.
Stange also discussed specific data challenges that he believes HHS could be particularly well positioned to address. These include
- reframing data use to support primary care as a force for integration and equity for individuals and families;
- reframing data use to support public health as a force for integration and equity for communities and populations;
- supporting the integration of primary care and public health;
- supporting primary care research about the care of whole people;
___________________
3 R.S. Etz, S.J. Zyzanski, M.M. Gonzalez, S.R. Reves, J.P. O’Neal, and K.C. Stange. (2019). A new comprehensive measure of high-value aspects of primary care, The Annals of Family Medicine, 17(3), 221–230. http://www.annfammed.org/content/17/3/221.
- bringing together the Office of the Assistant Secretary for Planning and Evaluation, the Centers for Disease Control and Prevention, and the National Committee on Vital and Health Statistics in their congressionally mandated role to update the Health Insurance Portability and Accountability Act of 1996 to make data sharing safe and less onerous; and
- raising the budget cap for NIH research project grants.
Robert Califf, Verily Life Sciences and Google Health, started by saying that in his experience the key question people want answered in most health care scenarios is this: Out of the options at my disposal, which diagnostic strategy and treatment is best for me? While this is at the core of the terminology comparative effectiveness, the data available and associated context are not enabling researchers to design and conduct crisp, reliable comparative effectiveness studies.
Califf pointed out the important role the pragmatic randomized trial played in providing answers related to the COVID-19 pandemic. He said that a priority going forward should be to identify a core set of data that would provide reliable information that, when coupled with appropriate study design, could enable multiple pragmatic clinical trials to be conducted to answer the many questions that people have about the options they have, and about the option that would ultimately be best for them. These trials could include not only drugs and devices but also behavioral and health service interventions and systems of care as well. He noted that more data is not necessarily better, and that time invested in identifying the essential data that are needed would be time well spent.
Califf also pointed out that computing has changed since the early days of PCOR and that some questions that were not feasible to be examined before are within scope now. This includes questions related to the roles of deep molecular, behavioral, and social determinants of health, given that it has long been recognized that social, cultural, behavioral, and biological determinants not only interact to combine in complex ways to impact individual outcomes, but also have common dimensions across groups of people. Going forward, it will be important to look at opportunities afforded by different ways to integrate information using a different approach to computing. He cited the example of COVID-19 trackers, which constantly scrape information off the Internet, integrate the data, and present them at a variety of levels, ranging from countries to states, counties, and even individual hospitals. This information has been useful for optimizing clinical trial recruitment and for deploying interventions. In theory, this approach could now be used for all diseases, starting with a substrate of real-time information about the status of health from a geospatial and temporal reference point.
Califf also argued that “de-identified data” is somewhat of a myth, because re-identification is usually possible if someone is determined to accomplish that. Furthermore, in many cases identifiable data are going to be the most useful for research and the most valuable for translating research into practice. He argued that the current rules that exist are not fit for purpose, because they make research very difficult. What is needed, Califf said, is a system that enables researchers to use identifiable data more easily, while at the same time imposing extreme penalties on people who take advantage of this access and misuse the data. He added that health systems already use fully identified data for operations purposes, and if that is done, then the data should perhaps also be available to produce generalizable knowledge that could be spread across health systems and could benefit people beyond those involved in a specific health care operation.
Califf echoed the arguments made by others about the importance of integrating research and care. He noted that PCOR has already made a big difference in this area, but it would make a bigger difference yet to continue this work.
Califf also brought up the challenges associated with patient-reported outcome data collected through cell phones. The use of cell phones is widespread and access to broadband internet is also growing, but these types of data collections do not reach everyone equally. In the case of digital technologies, older people are one group that is likely to be underrepresented, not only because of challenges related to access to cell phones, but also due to more limited skills at using the technology effectively. Califf also echoed challenges associated with the lack of data for a variety of populations more broadly, as discussed in Chapter 2. He highlighted two additional groups that receive relatively little attention: people living in rural areas and those struggling with addictions. There are rising health concerns specific to both of these populations, and therefore there is a need to develop approaches that would address the data limitations associated with these groups.
David Cella, Northwestern University, summarized key data needs as a common data model for patient-reported outcomes; common data elements for patient-reported outcomes; comparative effectiveness metrics across conditions; and medical and nonmedical cost data. He said that despite advances in artificial intelligence and natural language processing, structured data are still useful, in part because they enable comparative effectiveness research not only within conditions, but also across conditions, and they enable a look at overall value for cost. Cella listed insurance deductibles, copayments, caregiver expenses, and work productivity (for example, absenteeism) as the key components of medical and nonmedical cost data needed.
Cella argued that the broadened statutory scope for PCOR opens a major opportunity to examine costs in the context of effectiveness, which
has not previously been possible. It also opens the potential for interagency collaboration around cost-effectiveness research and application. These collaborations could include Agency for Healthcare Research and Quality, NIH, CMS, and possibly the U.S. Food and Drug Administration. The broadened statutory scope of PCOR also provides ingredients for a learning health systems approach across provider organizations.
Concerning the questions that cannot be answered with the current PCOR infrastructure, Cella said it continues to be difficult to answer crosscutting comparative effectiveness research questions as they relate to patient-reported outcomes. He echoed earlier points about the difficulty of accessing patient-reported outcomes data, particularly through the Chicago Area Patient-Centered Outcomes Research Network, which is 1 of 13 Clinical Data Research Networks.
Cella mentioned that in 2014 he was part of the PCORnet Patient-Reported Outcomes Common Measures Working Group, which recommended a set of common measures for PCORnet. The recommendations included nine core items for adults, focused on general health, quality of life, physical function (two questions), depression, fatigue, sleep, social roles and activities, and pain. For children, the core items recommended were focused on: general health, quality of life, pain, fatigue, stress, depression, peer relationships, and family relationships. Most of these items are from the Patient-Reported Outcomes Measurement Information System, which provides deep and wide item banks to cover these domains. From each of the domains, the working group selected a single question that would work best, if one could only ask a single question. Cella said that with large networks such as PCORnet, sometimes one question is sufficient to obtain a good estimate for a cohort. The working group’s recommendations were not implemented, however, because of technology limitations, such as electronic health records that could not adequately speak to one another and share a common data model overall.
Cella cited a 2019 paper that found that among member organizations of the New England Journal of Medicine Catalyst Insights Council, around 38 percent used the Patient-Reported Outcome Measures System (PROMS) and an additional 17 percent had plans to start using it within 3 years. Cella added that even those who use PROMS capture information on less than 50 percent of patients, often excluding underrepresented minorities and patients with lower educational levels. Most who collect these data do so primarily for operational reasons, to improve their metrics, or to improve their own patients’ experience or engagement. And there is still not much outward-facing incentive for doing patient-reported outcome assessments in clinical settings.
Cella listed the following as data-capacity activities that he considers HHS to be best positioned to address:
- promoting technologies to capture patient-provided data, including patient-reported outcome measures;
- promoting patient activation and engagement;
- endorsing health care quality initiatives and patient-reported outcome performance measures; and
- “funding the mandate” or finding other ways of encouraging clinical providers and provider organizations to collect the data.
Giselle Corbie-Smith, University of North Carolina, argued that having incomplete data on race, ethnicity, and other social identities leads to erasures of the experiences of some populations. This lack of data and these erasures diminish the potential of PCOR to advance health equity. The data infrastructure needs to be robust enough to allow data to be disaggregated in ways that can detect differences among small populations. For example, an inability to disaggregate data to compare Filipino health care workers to other Asians and Pacific Islanders could mean missing a disproportionate impact of the COVID-19 pandemic on Filipino nurses and nurses of Filipino descent.
Corbie-Smith said there has been growing momentum to understand the social determinants of health and that some information of this kind is being captured in electronic medical records. However, she added, below that surface there is a need to better understand the role of structural racism, community context, and social drivers of health. There is a need for data on patients’ experiences within the health care systems, as well as outside the walls of hospitals and clinics. Specifically, there are limited data on community health resources outside the health care system: the data are either completely missing or, when available, are often dissociated from the health care system. In the case of the COVID-19 pandemic, it became clear that this information is necessary to be able to provide equitable testing resources and equitable vaccine resources.
Corbie-Smith also discussed the critical role of engagement, particularly engagement of patients, community-based organizations, and faith-based organizations, in the case of disasters such as the COVID-19 pandemic. Borrowing a term used by Ralph Ellison in the Invisible Man, Corbie-Smith said that the network of community service providers is “unvisible” to health care and public health systems. There is a tendency to think that health is created within the health care system when, in fact, community service providers are often the ones addressing social determinants of health. She also pointed out that there is a crisis around trust in science, and that misinformation is filling the gap. If researchers made their work more accessible to patients, providers, and communities, trust in the work of scientists would likely also increase.
With regard to opportunities, Corbie-Smith referred to “data democratization,” which echoed what other speakers said about the need to make the data more widely visible and accessible beyond the research community, and particularly to patients and communities. Beyond obviously benefiting from the use of the data, patients can also help researchers interpret the meaning of data.
Communities can also benefit from the use of data to think about how to effect change around health equity, because it is unreasonable to expect that achieving health equity could happen within the PCOR context alone. Corbie-Smith noted that data visualizations are a helpful tool for democratizing data.
As also discussed by others, collecting more complete data on race and ethnicity is another area that represents an opportunity. This includes avoiding misclassification and collecting data that allow for disaggregation to understand small populations. The data and research also need to reflect the intersection of social identities.
Corbie-Smith emphasized the need for robust stakeholder engagement in defining strategic areas of research. This includes not only stakeholder input on research questions within a particular study, but also input on the overall strategy for PCOR. Stakeholder engagement needs to include communities not commonly reflected or recognized.
Corbie-Smith also highlighted the opportunities presented by including networks of community service providers in the research. These stakeholders include not only federally qualified community health centers but also community service providers that are providing a matrix of care. Keeping these providers visible will lead to a better understanding of the lived experiences of patients, what is important to them, and how they actually can be healthy.
Corbie-Smith also discussed the use of mobile technologies to collect person- and community-level data. While not all of her patients are technologically savvy enough to use telehealth, many of them have smartphones. Smartphones, wearables, and methodologies such as ecological momentary assessment make it possible to understand what is happening with patients outside of the health care context. Combining person-centered data with community-level data makes it possible to understand the interaction between the community, the physical built environment, and the social environments and how that impacts health. Corbie-Smith said that ecological momentary assessment can help provide answers to questions such as the impact of structural racism and interpersonal racism on the health of individuals, particularly in communities that are over-policed.
In terms of analytical opportunities, Corbie-Smith said that there is a need for analyses that reflect the complexities. She said that traditional approaches assume that factors such as food insecurity, housing insecurity,
and intimate partner violence are independent of each other. There is also a tendency to assume linearity, instead of recognizing the complexity of the systems in which patients live, work, grow, play, and age. Corbie-Smith also underscored the need for transparency in research and around data democratization in order to demonstrate the trustworthiness of science, which fundamentally is what is needed to move forward.
Scott Ramsey, Fred Hutchinson Institute for Cancer Outcomes Research (HICOR), began by discussing that institute’s mission and its Value in Cancer Care initiative, which engages oncology providers, patient partners, payers, health system representatives, and researchers to improve the value and efficiency of cancer care delivery in Washington State. This initiative was formed based on the realization that the rising costs of cancer care and problems with care coordination threaten society’s ability to eliminate cancer as a cause of suffering and death.
HICOR’s community engagement program shares data about clinic performance and costs across a common population-based data platform. The network includes all of the 28 oncology practices in Washington State, five of the state’s major health insurance providers, representatives from local and state government, and a number of patient advocacy groups and patient advocates, including those who represent typically underrepresented minorities.
The database, which is updated on a regular basis throughout the year, includes insurance claims from major payors in the state and is linked to the two cancer registries. The data are used to produce an annual community cancer care report, which documents several oncology quality metrics and the average cost of care for each clinic for specific services. The database also serves as a platform for the oncology community to share best practices, and for a low-cost way to capture outcomes from prospective studies that have started in response to quality issues that were identified from the database and that were prioritized by the stakeholders.
Based on this work, Ramsey shared the lessons learned about key characteristics of databases that can best serve patients. His list included
- comprehensive capture of the patient experience;
- data elements informed by patients and other stakeholders;
- data relevant to treatment decisions;
- ongoing mechanism for direct feedback on patient-identified priorities;
- information that is relevant and accessible; and
- information that is timely.
He noted that in his experience, inadequate accessibility and timeliness have been problems for cancer data for many years.
Ramsey asked whether databases are built from the perspective of a patient or that of a researcher who is trying to adapt the patient perspective. Thinking about the patient as a data consumer is one way to begin to address this issue. When patients seek medical care, they arrive with a particular medical history and a range of social determinants might influence their perspectives. Their neighborhood and their network influence the care available to them, their interest and ability to understand the health system that serves them, their care plan, and the rationale for that plan. Because a subset of patients wants to interrogate the data themselves to understand what they should do, it is important to think about whether a proposed data infrastructure allows understanding of health systems and interrogation in a way that makes sense to patients. Ramsey said he believes that the technology industry is ahead of government agencies in thinking about these issues.
Thinking specifically about cancer care, Ramsey said that based on the literature and based on his own experience working with cancer patients, measures of patient satisfaction do not correlate well with the process measures of care and key outcomes. To address these disparities, there is a need for more granular and relevant measures of patient experience. According to Ramsey, the factors that influence patients’ sense of well-being during cancer care, and that are not always addressed by providers, include feeling that they are supported, dealing with uncertainty, perceived loss of autonomy, and trust in the health system.
Ramsey said that in seeking to understand the relationship between treatment and outcomes, the research community sometimes suffers from the well-known “streetlight effect,” using only the data that are available. Those data typically focus on what happens in the health care system, whereas, he believes, in many cases the individual’s experiences and environment play a bigger role in their care and outcomes.
The social determinants of health are generally not captured in traditional claims and electronic health records databases. However, it is becoming increasingly clear to the cancer care community that social determinants of health may play a bigger role than any other factor in the observed differences in outcomes among cancer patients. Social determinants of health influence patients over a lifetime, but to date little has been done to understand this at a level of specificity that can address policy. The limited data available certainly limit the ability to do this research.
Ramsey also discussed his research on financial toxicity in cancer care, and the emerging picture of vast and lasting impacts on patients’ financial well-being, which translates into impact on their well-being in other domains. He argued that there is a need for a data infrastructure that allows researchers to study this problem in other chronic conditions. This would necessitate linking to existing financial databases, such as credit reporting
databases, to understand the scale and scope of this problem. He noted that HICOR has been able to link its cancer registry with credit data from Transunion, although accomplishing this took 2 years.
Ramsey argued that HHS does not necessarily need to create new data. Instead, he said, the agency is best positioned to facilitate access to existing data that currently live in the private sector; create regulations that foster interoperability; establish privacy safeguards; and improve timeliness of databases, particularly in areas such as cancer care, which is quickly evolving.
CONCLUSIONS
The final session of the workshop included researchers working in a variety of areas related to patient-centered outcomes. Their input echoed many of the points made by others throughout the workshop. In particular, it is clear that limiting the focus to the person as the patient, as opposed to the person as a whole, limits not only thinking about the data but also the outcomes and impacts that matter to people, both inside their medical relationships when they are patients and, more generally, outside of medical relationships.
CONCLUSION 4-1: Broadening the focus from the patient to the person more generally would enable a more comprehensive approach to the data infrastructure and a better understanding of the outcomes and impacts that matter to people.
The fragmented nature of the data infrastructure and the data silos represents a particular hurdle for researchers. This hurdle could be overcome by a focus on facilitating data linkages, which in turn could increase the usefulness of the information available for research as well as for decision making more broadly.
CONCLUSION 4-2: The data available for patient-centered outcomes research are fragmented across a variety of databases. Expanding data linkages could greatly increase the usefulness of these data for research.
Researchers described a variety of barriers that limit their ability to access the data available in the many existing databases, ranging from databases that can be considered a part of the PCOR data infrastructure to databases owned by private companies. Focusing on facilitating and simplifying access represents an area that could further enhance the usefulness of PCOR data.
CONCLUSION 4-3: Researchers encounter substantial barriers to accessing existing data for patient-centered outcomes research. Facilitating and simplifying data access could further increase the usefulness of data for research.
Researchers echoed the need to make PCOR data more widely available to empower patients and communities to use this information. Efforts to reduce disparities, in particular, cannot be accomplished by research alone.
CONCLUSION 4-4: Making the data more visible and more widely accessible could enable patients and communities to use the information in ways that reduce health disparities, complementing research efforts in this area.
The need for information on the cost of health care and the ways cost factors into care decisions represented another area where researchers echoed the need expressed by other stakeholders for more data.
CONCLUSION 4-5: Data needs related to the total cost of care and a better understanding of cost considerations is an area that deserves more attention.
This page intentionally left blank.
Appendix
A Biographical Sketches of Committee Members
GEORGE ISHAM (NAM) (Chair) is a senior fellow at the HealthPartners Institute and a senior advisor for the Alliance of Community Health Plans. Previously, he served as a senior advisor to the board of directors and the senior management team of HealthPartners, and prior to that, he was HealthPartners’ medical director and chief health officer, responsible for quality of care and health and health care improvement. He has been active in health policy, serving as a member of the Centers for Disease Control and Prevention’s Task Force on Community Preventive Services, a member of the Agency for Healthcare Research and Quality’s United States Preventive Services Task Force, as a founding co-chair of the National Committee for Quality Assurance’s committee on performance measurement, and a founding co-chair of the National Quality Forum’s Measurement Application Partnership. He has an M.D. from the University of Illinois at Chicago and an M.S. in preventive medicine and administrative medicine from the University of Wisconsin–Madison.
JOHN F.P. BRIDGES is professor and vice chair of academic affairs in the Department of Biomedical Informatics at the Ohio State University (OSU) College of Medicine. He is also a professor in the Department of Surgery and an adjunct professor in both the Division of Epidemiology at the OSU College of Public Health and Department of Health Behavior and Society at the Johns Hopkins Bloomberg School of Public Health. Prior to joining OSU, he was on the faculty of the Johns Hopkins University Bloomberg School of Public Health, the Department of Tropical Hygiene and Public Health within the University of Heidelberg School of Medicine, and the
Department of Epidemiology and Biostatistics within the Case Western Reserve University School of Medicine. He has previously held positions in the Department of Economics at the Weatherhead School of Management at Case Western Reserve University, the National Bureau of Economic Research, Center for Medicine in the Public Interest, and the Center for Health Economics, Research and Evaluation in Australia. He has a Ph.D. in economics from the City University of New York.
JULIE BYNUM is the Margaret Terpenning Professor of Medicine in the Division of Geriatric Medicine and vice chair for faculty affairs in the Department of Internal Medicine at the University of Michigan. She is also a research professor in the Institute of Gerontology, Geriatric Center Associate Director for Health Policy and Research, and a member of the Institute for Healthcare Policy and Innovation. She currently leads a portfolio of National Institutes of Health–funded research that examines the quality of care, diagnosis, and treatment of people with Alzheimer’s disease and related dementia in the community, nursing homes, and assisted living and is the director of the Center to Accelerate Population Research in Alzhiemer’s. She is currently a member of the National Academies of Sciences, Engineering, and Medicine’s Forum on Aging, Disability, and Independence and was a member of a National Academies’ workshop planning committee on adverse consequences of cancer treatment. She has an M.P.H. from the Johns Hopkins University School of Hygiene & Public Health and an M.D. from the Johns Hopkins University School of Medicine.
ANGELA DOBES is vice president of the Crohn’s & Colitis Foundation’s IBD Plexus Program, a research-information exchange platform designed to centralize data and biosamples from diverse research initiatives to advance science, accelerate precision medicine, and transform the care of inflammatory bowel disease patients. Previously, she has worked for clinical technology and pharmaceutical organizations, where she has led implementation of various technology solutions focused on business optimization and accelerating the delivery of new therapies to patients safely. She is currently serving as principal investigator on a study to enhance engagement, research participation, and collaboration through the IBD Partners Patient Powered Research Network. She has an M.A. in public health from the Icahn School of Medicine at Mount Sinai.
OLUWADAMILOLA FAYANJU is the Helen O. Dickens Presidential Associate Professor of Surgery at the Perelman School of Medicine at the University of Pennsylvania. She is also chief of breast surgery at Penn Medicine. Previously, she was associate professor of surgery and population health sciences in the Duke University School of Medicine and director of the
Durham VA Breast Clinic. She was also associate director for Disparities & Value in Healthcare with Duke Forge, Duke University’s center for actionable data science. In 2019, she was recognized by the National Academy of Medicine as an Emerging Leader in Health and Medicine Scholar. She received an M.A. in comparative literature from Harvard University and her M.D. and M.P.H.S. from the Washington University in St. Louis.
DEBORAH ESTRIN (NAE/NAM) is a professor of computer science at Cornell Tech where she holds the Robert V. Tishman founder’s chair, serves as the associate dean for impact, and is an affiliate faculty at Weill Cornell Medicine. Her research activities include technologies for caregiving, immersive health, small data, participatory sensing, and public interest technology. Estrin was an Amazon Scholar, and before joining Cornell University she was founding director of the National Science Foundation’s Center for Embedded Networked Sensing at the University of California, Los Angeles, pioneering the development of mobile and wireless systems to collect and analyze real-time data about the physical world. Estrin cofounded the nonprofit startup, Open mHealth, and has served on several scientific advisory boards for early-stage mobile health startups. She has a Ph.D. in electrical engineering and computer science from the Massachusetts Institute of Technology.
CONSTANTINE GATSONIS is the Henry Ledyard Goddard University Professor of Statistical Sciences, director of statistical sciences, and professor of biostatistics at Brown University. He was founding director of the Center for Statistical Sciences and founding chair of the Department of Biostatistics at Brown University. He is a leading authority on the evaluation of diagnostic and screening tests and has made major contributions to the development of methods for medical technology assessment and health services and outcomes research. He is a world leader in methods for applying and synthesizing evidence on diagnostic tests in medicine and is currently developing methods for comparative effectiveness research in diagnosis and prediction and radiomics. Since 2016, he has served as a statistical consultant for the New England Journal of Medicine and was the Founding Editor-in-Chief of Health Services and Outcomes Research Methods. He has a Ph.D. in mathematical statistics from Cornell University.
ROBERT GOERGE is a senior research fellow at Chapin Hall at the University of Chicago. He is also a senior fellow and founder of the Master’s Degree in Computational Analysis in Public Policy at the University of Chicago Harris School of Public Policy. His research is focused on improving the available data and information on children and families, particularly those who require specialized services related to maltreatment, disability,
poverty, or violence. At Chapin Hall, he is principal investigator for the Family Self-Sufficiency Data Center, the Linking Federal Data to Local Data project, and the National Survey for Early Care and Education. He currently serves on the National Academies of Sciences, Engineering, and Medicine’s Committee on National Statistics. He has a Ph.D. in social policy from the University of Chicago.
GEORGE HRIPCSAK (NAM) is the Vivian Beaumont Allen professor and chair of the Department of Biomedical Informatics at Columbia University. He is also the director of medical informatics services for New York Presbyterian Hospital. He is also a board-certified internist. He led the effort to create the Arden Syntax, a language for representing health knowledge that has become a national standard. As chair of the American Medical Informatics Association Standards Committee, he coordinated the medical informatics community response to the Department of Health and Human Services for the health informatics standards rules under the Health Insurance Portability and Accountability Act of 1996. His current research is on the clinical information stored in electronic health records. Using data mining techniques, he is developing the methods necessary to support clinical research and patient safety initiatives. He has an M.D. and an M.S. in biostatistics from Columbia University.
LISA IEZZONI (NAM) is professor of medicine at Harvard Medical School and the Health Policy Research Center at Massachusetts General Hospital, where she served as director in the past. She was previously co-director of research in the Division of General Medicine and Primary Care at Beth Israel Deaconess Medical Center in Boston. Her research focuses on risk adjustment methods for predicting cost and clinical outcomes of care, and on health care experiences and outcomes of persons with disabilities. She has served on the editorial boards of the Annals of Internal Medicine, the Journal of General Internal Medicine, Health Affairs, Medical Care, Health Services Research, and the Disability and Health Journal, among others. She has an M.D. from Harvard Medical School and an M.Sc. from the Harvard T.H. Chan School of Public Health.
S. CLAIBORNE JOHNSTON (NAM) is the inaugural dean of Dell Medical School, vice president for medical affairs, and the Frank and Charmaine Denius Distinguished Dean’s Chair in medical leadership at The University of Texas at Austin. Previously, Johnston was associate vice chancellor for research at the University of California, San Francisco (UCSF). He also directed the Clinical and Translational Science Institute and founded the UCSF Center for Healthcare Value. His research is focused on clinical trials and health services research in stroke. He is also an expert in medi-
cal education, research administration, health care value, and population health. He has led several large-cohort studies of cerebrovascular disease and three international multicenter randomized trials. He has an M.D. from Harvard Medical School and a Ph.D. in epidemiology from the University of California, Berkeley.
MIGUEL MARINO is an associate professor with joint appointments in the School of Public Health Division of Biostatistics and the Department of Family Medicine at Oregon Health & Science University. His research focuses on the development and implementation of novel statistical methodology to address complexities associated with the use of electronic health records (EHRs) to study changes in policy; using EHRs to study health disparities; validation of EHRs as a reliable source for observational studies; pragmatic randomized trials; and preventive health maintenance. He was selected by the National Academy of Medicine as an Emerging Leader in Health and Medicine Scholar. He has a Ph.D. in biostatistics from Harvard University.
ELIZABETH McGLYNN (NAM) is vice president for Kaiser Permanente Research and executive director for the Center for Effectiveness & Safety Research at Kaiser Permanente. She is also interim senior associate dean for research and scholarships at the Kaiser Permanente Bernard J. Tyson School of Medicine. She is an internationally known expert on methods for evaluating the appropriateness and quality of health care delivery. She has led major initiatives to evaluate health reform options under consideration at the federal and state levels. She is the lead of Kaiser Permanente & Strategic Partners Patient Outcomes Research To Advance Learning (PORTAL) Network. She was a member of the Strategic Framework Board, which provided a blueprint for the National Quality Forum on the development of a national quality measurement and reporting system. She chaired the board of AcademyHealth, served on the board of the American Board of Internal Medicine Foundation, and served on the Board of Providence-Little Company of Mary Hospital Service Area in Southern California. She has a Ph.D. in public policy from RAND Graduate School.
DAVID MELTZER (NAM) is the Fanny L. Pritzker Professor in the Department of Medicine, chief of the section of Hospital Medicine and faculty in the Department of Economics and Harris School of Public Policy at the University of Chicago. He is also director of the Center for Health and the Social Sciences and of the Urban Health Lab at the University of Chicago. His research explores problems in health economics and public policy with a focus on the theoretical foundations of medical cost-effectiveness analysis and the cost and quality of hospital care. Since 1997,
he has developed the inpatient general medicine services at the University of Chicago as a Learning Health Care System to produce knowledge on how to improve the care of hospitalized patients, mobilizing the clinical care process to generate and learn from diverse data from electronic health records, claims data, patient interviews, and bio-specimens on more than 100,000 patients. He is the lead of the University of Chicago network site as part of the Chicago Area Patient Centered Outcomes Research Network. He has an M.D. and a Ph.D. in economics from the University of Chicago.
PAUL C. TANG (NAM) is an adjunct professor in the Clinical Excellence Research Center at Stanford University and an internist at the Palo Alto Medical Foundation. He was formerly chief innovation and technology officer at the Palo Alto Medical Foundation and vice president, chief health transformation officer at IBM Watson Health. He has more than 25 years of executive leadership experience in health information technology within medical groups, health systems, and corporate settings. He has directed innovation and technology teams in provider organizations, academic institutions, corporate research organizations, and product development organizations. Most recently, he led the creation, development, deployment, and evaluation of the application of artificial intelligence to physician point-of-care solutions integrated within an electronic health record system. He also led a corporate enterprise-wide design team. He has chaired numerous federal and private-sector advisory and professional association groups related to health information technology and policy. He received an M.S. in electrical engineering from Stanford University and his M.D. from the University of California, San Francisco.
Appendix B
Workshop Agenda
Building Data Capacity for Patient-Centered Outcomes Research:
An Agenda for 2021 to 2030
Virtual Workshop 1: Looking Ahead at Data Needs
MAY 3, 2021, 11 AM–5 PM EDT
OBJECTIVES FOR THE WORKSHOP
- Provide a high-level overview of what kind of data are included in the patient-centered outcomes research data infrastructure.
- Identify key questions that stakeholders are most likely to want answered going forward, including general themes that cut across health conditions and circumstances.
- Discuss implications of the broadened statutory scope for PCOR.
- Identify gaps in what stakeholders need and what the infrastructure allows. Consider both limitations in the existing data and improvements that could be made to new data collections (e.g., at point of care or in prospective studies).
- Discuss what questions cannot be answered and who is not served by the current PCOR data infrastructure.
- Discuss what HHS is best positioned to address and how the agency could maximize resources available for the PCOR data infrastructure (representing 4% of the PCOR trust fund), in the context of the HHS public mission, authorities, programs, and data resources.
| 11:00-11:05 AM EDT |
Goals for the Workshop
GEORGE ISHAM (Committee Chair) HealthPartners Institute |
| 11:05-11:30 AM EDT |
Overview of the Data Infrastructure for Patient-Centered Outcomes Research
Moderator: GEORGE ISHAM |
|
BENJAMIN SOMMERS, Deputy Assistant Secretary for Health Policy, ASPE NANCY DE LEW, Associate Deputy Assistant Secretary for Health Policy, ASPE SCOTT R. SMITH, Director, Division of Healthcare Quality and Outcomes, ASPE |
|
| 11:30 AM-1:00 PM EDT | PCOR Data Infrastructure Limitations and Opportunities: Disparities and Health Equity Research |
Discussion questions:
|
|
|
Moderator: OLUWADAMILOLA (LOLA) FAYANJU, Duke University |
|
| Speakers: | |
|
KAREN JOYNT MADDOX, Washington University in St. Louis |
|
MEGAN MORRIS, University of Colorado MITCHELL LUNN, Stanford University KALEAB ABEBE, University of Pittsburgh THOMAS SEQUIST, Harvard University and Brigham & Women’s Hospital |
|
| 1:00-1:10 PM EDT | Break |
| 1:10-1:30 PM EDT | PCOR Data Infrastructure Limitations and Opportunities: COVID-19 as Use Case |
|
Moderator: PAUL TANG, Palo Alto Medical Foundation and Stanford Clinical Excellence Research Center |
|
|
Speaker: DAVID MELTZER, University of Chicago |
|
| 1:30-2:45 PM EDT | Patient Perspectives on Data Needs |
Discussion questions:
|
|
|
Moderator: ANGELA DOBES, Crohn’s & Colitis Foundation |
|
| Speakers: | |
|
REBEKAH ANGOVE, Patient Advocate Foundation GARY EPSTEIN-LUBOW, Brown University ELISABETH OEHRLEIN, National Health Council BRAY PATRICK-LAKE, Evidation Health |
| 2:45-3:05 PM EDT | Break |
| 3:05-4:55 PM EDT | Researcher Perspectives on Data Needs |
Discussion questions:
|
|
|
Moderator: ELIZABETH MCGLYNN, Kaiser Permanente Research |
|
| Speakers: | |
|
ANDREW BAZEMORE, American Board of Family Medicine ROBERT CALIFF, Verily DAVID CELLA, Northwestern University GISELLE CORBIE-SMITH, University of North Carolina SCOTT RAMSEY, Fred Hutch KURT STANGE, Case Western Reserve University |
|
| 4:55-5:00 PM EDT |
Wrap-up
GEORGE ISHAM (Committee Chair) HealthPartners Institute |
Appendix C
Biographical Sketches of Speakers
KALEAB ABEBE is an associate professor of medicine, biostatistics, and clinical and translational science at the University of Pittsburgh. He also directs the Center for Research on Health Care Data Center as well as the Center for Clinical Trials & Data Coordination. His collaborative research focuses on design, conduct, coordination, and analysis of multicenter randomized controlled trials. Most recently, he led the Data Coordinating Center for the HALT-PKD Network, which comprised two seven-site clinical trials evaluating the impact of hypertensive medications and blood pressure control on the progression of polycystic kidney disease. Additionally, he collaborates with the Adolescent Medicine Division on the design and analysis of cluster randomized trials in sexual violence prevention. In addition to his research collaborations, Abebe is the director of the Clinical Trials Track for the M.S. in Clinical Research at the Institute for Clinical Research Education. He received his B.A. in mathematics from Goshen College and an M.A. and a Ph.D. in statistics from the University of Pittsburgh.
REBEKAH ANGOVE is vice president for patient experience and program evaluation at Patient Advocate Foundation (PAF), where her work is focused on strategically expanding PAF’s patient-centered research and program evaluation initiatives. Angove is a health services researcher and leader in patient engagement. She leads efforts to identify patient needs, translate those needs to direct service and policy recommendations, and evaluate the impact of these programs and services on patients and the patient community. In her previous role at the Louisiana Public Health Institute, she served as associate director of health services research and engagement director of
REACHnet, a PCORnet Clinical Data Research Network. Her expertise spans numerous clinical research programs and advisory groups including service on the PCORnet Engagement committee and the Tulane Preventive Medicine Residency Advisory Committee. Angove received her Ph.D. in public and community health from the Medical College of Wisconsin.
ANDREW BAZEMORE (NAM) is the senior vice president of research and policy at the American Board of Family Medicine and also serves as the director of the Robert Graham Center for Policy Studies in Family Medicine. Bazemore helped cultivate the growth and evolution of the Graham Center into an internationally known primary care research center with diverse funding sources. He guided and participated in the Graham Center’s research with special interest in access to care for underserved populations, health workforce and training, and spatial analysis. Bazemore also led the Graham Center’s emphasis on developing tools that empower primary care providers, leaders, and policy makers. He serves on the faculties of the Departments of Family Medicine at Georgetown University and Virginia Commonwealth University. Bazemore received his M.D. from the University of North Carolina and his M.P.H. from Harvard University School of Public Health.
ROBERT M. CALIFF (NAM) is the head of clinical policy and strategy for Verily and Google Health. Previously, Califf was the vice chancellor for health data science for the Duke University School of Medicine; director of Duke Forge, Duke University’s center for health data science; and the Donald F. Fortin, MD, professor of cardiology. He has led major initiatives aimed at improving methods and infrastructure for clinical research, including the Clinical Trials Transformation Initiative, a public-private partnership cofounded by the U.S. Food and Drug Administration (FDA) and Duke University. He also served in the FDA as deputy commissioner for medical products and tobacco from 2015 to 2016 and as commissioner of food and drugs from 2016 to 2017. He is a nationally and internationally recognized leader in cardiovascular medicine, health outcomes research, health care quality, and clinical research, and one of the most frequently cited authors in biomedical science. Califf received his M.D. from the Duke University School of Medicine.
DAVID CELLA (NAM) is Ralph Seal Paffenbarger professor and chair of the Department of Medical Social Sciences, and professor of neurology, pediatrics, preventive medicine (Health and Biomedical Informatics), and psychiatry and behavioral sciences, at Northwestern University. He is also director of the Institute for Public Health and Medicine Center for Patient-Centered Outcomes at Northwestern. Cella plays a leadership role in the
development and orchestration of transdisciplinary scientific collaborations and oversees basic and applied social science research to advance the understanding of the mechanisms and measurement of health and disease. Currently he is the multiple principal investigator of the Environmental Children’s Health Outcomes Consortium PRO Core grant, and he also leads a health systemwide symptom monitoring and management project under the National Cancer Institute Moonshot Program. A theme of his work has been ensuring that the voice of the patient is reflected in clinical care, research, and policy. A major focus of many of these initiatives has been ensuring that measurement is sensitive and appropriate to diverse populations. Cella received his Ph.D. from Loyola University of Chicago.
GISELLE CORBIE-SMITH (NAM) is a Kenan distinguished professor of the Departments of Social Medicine and Medicine, director of the University of North Carolina (UNC) Center for Health Equity Research in the UNC School of Medicine and associate provost for UNC Rural Initiatives at the UNC at Chapel Hill. She is nationally recognized for her scholarly work on the inclusion of disparity populations in research and is accomplished in drawing communities, faculty, and health care providers into working partnerships in clinical and translational research. Her empirical work, using both qualitative and quantitative methodologies, has focused on the methodological, ethical, and practical issues of research to address racial disparities in health. She is currently the co-principal investigator for the Advancing Change Leadership Clinical Scholars Program. Corbie-Smith currently serves as a multiple principal investigator on the National Institutes of Health/National Institute on Minority Health and Health Disparities–funded RADx-Underserved Populations Coordination and Data Collection Center. Corbie-Smith received her M.Sc. in clinical research from Emory University and her M.D. from the Albert Einstein College of Medicine.
NANCY DE LEW is the associate deputy assistant secretary for health policy in the Office of the Assistant Secretary for Planning and Evaluation at HHS. She leads a team who apply their skills in policy development, strategic planning, research, and evaluation to some of the department’s most challenging health policy problems. She provides executive leadership and coordination on a broad range of health care financing, coverage, access, public health, and quality issues. She has worked with Congress on a number of major pieces of legislation over the course of her career including the Affordable Care Act in 2010, the Medicare Modernization Act of 2003, the Balanced Budget Act of 1997, the Health Insurance Portability and Accountability Act of 1996, and the Medicare Catastrophic Coverage Act of 1988. De Lew received her M.A. and M.P.A. in political science and public administration from the University of Illinois at Urbana.
GARY EPSTEIN-LUBOW is an associate professor of psychiatry and human behavior and associate professor of medical science at Alpert Medical School of Brown University. He is also an associate professor of health services, policy and practice at the Brown University School of Public Health. Epstein-Lubow is a geriatric psychiatrist with research, teaching, policy, clinical, and administrative expertise related to geriatric psychiatry patients and family caregiver health, and serves as team leader of the stakeholder engagement team for the National Institute on Aging’s Imbedded Pragmatic Alzheimer’s Disease and AD-Related Dementias Clinical Trials Collaboratory. He is also an associate director of the Centers for Disease Control and Prevention BOLD Public Health Center of Excellence for Dementia Caregiving. He earned his M.D. from the Ohio State University’s College of Medicine and Public Health; he completed his general psychiatry residency, geriatric psychiatry fellowship, and postdoctoral research at Brown University and Butler Hospital.
KAREN E. JOYNT MADDOX is a practicing cardiologist at Barnes-Jewish Hospital and an assistant professor at the Washington University School of Medicine and School of Social Work, as well as a health policy advisor for BJC Healthcare. Her research interests include (1) improving the measurement of the quality and efficiency of physicians, hospitals, and health systems; (2) understanding the impact of policy interventions on health care, with a focus on value-based and alternative payment models; and (3) reducing disparities in care, with a focus on vulnerable populations including racial and ethnic minorities, individuals living in poverty, individuals with disabilities, frail elders, and those in rural areas. Joynt Maddox received her A.B. in public policy from the Woodrow Wilson School at Princeton University and her M.D. from the Duke University School of Medicine. She trained in internal medicine at Duke University Medical Center and in cardiovascular medicine at Brigham and Women’s Hospital. She also completed a research fellowship in health policy at the Harvard School of Public Health, from which she received her M.P.H.
MITCHELL (MITCH) R. LUNN is an assistant professor in the Division of Nephrology of the Department of Medicine at the Stanford University School of Medicine. As an internist and nephrologist with a strong interest in technology and sexual and gender minority (SGM) health, his research is designed to characterize the health and well-being of these populations. Through the use of existing and emerging technologies, Lunn focuses on improving understanding of the factors that positively and negatively influence SGM health including research on SGM health disparities, SGM societal experiences (in and out of health care), provider education about SGM health, and institutional climate toward SGM people. He is the
codirector of PRIDEnet, a participant-powered research network of SGM people that engages SGM communities at all stages of the biomedical research process: research question generation and prioritization, study design, recruitment, participation, data analysis, and results dissemination. He is also the codirector of The PRIDE Study, a national, online, prospective, longitudinal general health cohort study. He earned his M.D. from the Stanford University School of Medicine and his M.A.S. in clinical research from the University of California, San Francisco (UCSF). He completed internal medicine internship and residency training at Brigham and Women’s Hospital and nephrology fellowship at UCSF.
DAVID O. MELTZER (NAM) is the Fanny L. Pritzker Professor in the Department of Medicine, chief of the section of Hospital Medicine and faculty in the Department of Economics and Harris School of Public Policy at the University of Chicago. He is also director of the Center for Health and the Social Sciences and of the Urban Health Lab at the University of Chicago. His research explores problems in health economics and public policy with a focus on the theoretical foundations of medical cost-effectiveness analysis and the cost and quality of hospital care. Since 1997, he has developed the inpatient general medicine services at the University of Chicago as a Learning Health Care System to produce knowledge on how to improve the care of hospitalized patients, mobilizing the clinical care process to generate and learn from diverse data from electronic health records, claims data, patient interviews, and bio-specimens on more than 100,000 patients. He is the lead of the University of Chicago network site as part of the Chicago Area Patient Centered Outcomes Research Network. He has an M.D. and a Ph.D. in economics from the University of Chicago.
MEGAN MORRIS is an associate professor in the Division of General Internal Medicine at the University of Colorado, Anschutz Medical Campus, and she is the founder/director of the Learning Collaborative to Address Disability Equity in Healthcare, a national consortium of health care organizations working toward advancing equitable health care for patients with disabilities. Morris researches disparities in care experienced by persons with disabilities, with a focus on provider and health care organization-level factors that negatively impact the quality of care delivered to patients with disabilities. Using qualitative and mixed methods, she has led multiple studies in the area, including studies examining providers’ implicit disability bias and a Patient-Centered Outcomes Research Institute-funded trial comparing methods to improve the quality of communication between patients with disabilities and their health care team. Morris received her M.S. in speech-language pathology, her M.P.H. in health systems and policy, and her Ph.D. in rehabilitation science from the University of Washington.
ELISABETH M. OEHRLEIN is assistant vice president, Research and Programs at the National Health Council (NHC). In this role, she crafts the NHC’s annual research and programmatic agenda in service to the organization’s mission and leads the NHC’s research and programmatic work on value, real-world evidence, and patient engagement. She is a mixed-methods researcher with expertise in epidemiologic, qualitative, and patient-engagement methods, as well as patient-focused medical product development. Her research interests include developing new methods for applying patient-provided information when developing real-world evidence to ensure studies reflect the “real world” as closely as possible, as well as developing new methods for patient-journey mapping. Oehrlein holds an M.S. in epidemiology from the University of Maryland School of Medicine’s Department of Epidemiology and Human Genetics, and a Ph.D. in pharmaceutical health services research with a concentration in comparative effectiveness research/patient-centered outcomes research from the University of Maryland School of Pharmacy.
BRAY PATRICK-LAKE is senior director of Strategic Partnerships at Evidation Health, where she develops collaborations to support the design and implementation of participant-centered studies and the regulatory and clinical acceptance of digital measures. She serves on the Digital Medicine Society’s Scientific Leadership Board, Reagan Udall Foundation’s IMEDS Steering Committee, and American College of Cardiology’s National Cardiovascular Data Registry Oversight Board. Previously, she was a member of the All of Us National Advisory Panel, member of the National Academies of Sciences, Engineering, and Medicine Health Science Policy Board, and director of Stakeholder Engagement for the Clinical Trials Transformation Initiative (CTTI) at Duke University, where her work involved actively engaging patient advocacy organizations and other stakeholders in the CTTI’s efforts to improve clinical trials. She holds a B.S. from the University of Georgia and an M.F.S. from National University.
SCOTT RAMSEY is a physician, cancer researcher, and health economist. He codirects the Hutchinson Institute for Cancer Outcomes Research, or HICOR at Fred Hutch. The institute aims to reduce the economic and human burden of cancer by improving the efficiency and effectiveness of cancer care. Ramsey’s research focuses on cancer outcomes, health care delivery, and economic evaluations of new and existing cancer screening and treatment technologies. He also explores methods for engaging a diverse range of stakeholders to help inform how research studies are prioritized and designed. He designs and conducts studies that weigh the costs and benefits of various treatment and screening approaches. Ramsey
received his M.D. from the University of Iowa, College of Medicine, and his Ph.D. from the University of Pennsylvania, Wharton School.
THOMAS SEQUIST is the chief patient experience and equity officer at Mass General Brigham. In this role, he leads systemwide strategies for improving patient experience and health care equity, while also overseeing quality and safety. He is a practicing general internist at Brigham and Women’s Hospital and is a professor of medicine and professor of health care policy at Harvard Medical School. Sequist’s research interests include ambulatory quality measurement and improvement, with a focus on patient and provider education, and the innovative use of health information technology. He is particularly interested in health policy issues affecting care for Native Americans and has worked collaboratively with the Indian Health Service to evaluate the provision of care for this population. He is a member of the Taos Pueblo tribe in New Mexico and is committed to improving Native American health care, serving as director of the Four Directions Summer Research Program at Harvard Medical School and the medical director of the Brigham and Women’s Hospital Physician Outreach Program with the Indian Health Service. He graduated from Cornell University with a B.S. in chemical engineering. He received his M.D. from Harvard Medical School and an M.P.H. from the Harvard School of Public Health.
SCOTT R. SMITH is director of the Division of Health Care Quality and Outcomes in the Office of the Assistant Secretary for Planning and Evaluation. His division conducts research on how health policies influence health care quality and outcomes in state and federal programs. In addition, the division is responsible for managing the patient-centered outcomes research data infrastructure portfolio across HHS. His interests are studying quality metrics in Medicare and Medicaid, building national data capacity for conducting patient-centered outcomes research, strengthening research programs, and facilitating support for a learning health care system. He has directed research programs on comparative effectiveness and pharmaceutical outcomes at the Agency for Healthcare Research and Quality and was a member of the tenured faculty at the University of North Carolina at Chapel Hill. He received an M.S.P.H. from the University of Illinois at Urbana-Champaign and a Ph.D. from the University of Michigan.
BENJAMIN SOMMERS (NAM) was appointed the deputy assistant secretary for health policy in the Office of the Assistant Secretary for Planning and Evaluation (ASPE). Before joining ASPE, he was the Huntley Quelch Professor of Health Care Economics at the Harvard School of Public Health and professor of medicine at the Harvard Medical School and Brigham & Women’s Hospital. He is a health economist and primary care physician
whose main research interests are health policy for vulnerable populations and the health care safety net. He has received numerous awards including the Health Services Research Impact Award and the Article-of-the-Year Award from Academy Health, and the Outstanding Junior Investigator Award from the Society of General Internal Medicine. His research has been published in the New England Journal of Medicine, Journal of the American Medical Association, Journal of Health Economics, and Health Affairs, and covered by The New York Times, Wall Street Journal, and Washington Post. He received both his Ph.D. in health policy and his M.D. from Harvard University.
KURT C. STANGE (NAM) is distinguished university professor, Dorothy Jones Weatherhead professor of medicine, and professor in the Departments of Family Medicine and Community Health, Population and Quantitative Health Sciences, and Sociology at the Case Western Reserve University, where he serves as director of the Center for Community Health Integration. He is a family and public health physician, practicing at Neighborhood Family Practice, a federally qualified community health center in Cleveland, Ohio. Stange is active in practice-based, multimethod, participatory research and development that aims to understand and improve primary health care and community health. He uses complexity science to guide and interpret integrated qualitative and quantitative research, and has been working on participatory methods to advance community health and to develop computational models of primary health care and patient-centered, population health and equity outcomes. He has been locally active in the COVID-19 pandemic response and produced a report on the lessons of the pandemic for the National Academies’ report Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care. He is an American Cancer Society clinical research professor and a scholar of the Institute for Integrative Health. Stange received his M.D. from Albany Medical College and his Ph.D. from the University of North Carolina School of Public Health.


























































































