
4
Vaccines and Therapeutics
The second session of the second part of the workshop, which focused on advancements in tuberculosis (TB) vaccines and therapeutics, was moderated by Kent Kester, vice president and head of Translational Science and Biomarkers at Sanofi Pasteur, and Charles Wells, head of Therapeutics Development at the Bill & Melinda Gates Medical Research Institute. The session began with presentations on strategies to make better use of existing tools and new technologies. Alex Schmidt, head of vaccine development at the Bill & Melinda Gates Medical Research Institute, discussed the history and current state of policies regarding the use of the Bacillus Calmette–Guérin (BCG) vaccine and the potential role of BCG revaccination in TB elimination. Steve Reed, cofounder, president, and chief executive officer at HDT Bio, discussed the breadth and diversity of ongoing research in the TB vaccine pipeline. Daniel Kalman, professor of pathology at Emory University School of Medicine, examined the use of host-directed therapeutics for treating antibiotic-resistant TB. Rhea Coler, senior investigator at Seattle Children’s Research Institute Center for Global Infectious Disease Research and professor at the University of Washington School of Medicine, focused on immune mechanisms of protection against TB.
The next set of presentations explored strategies to transform treatment options for TB. Payam Nahid, professor of pulmonary and critical care medicine and director of the Center for Tuberculosis at the University of California, San Francisco, described lessons learned from designing and conducting a successful regimen-shortening trial for TB treatment. Adrian Thomas, vice president of Global Strategy, Programs and Policy for Global
Public Health at Johnson and Johnson (J&J), and Norbert Ndjeka, director of drug-resistant TB (DR TB), TB, and HIV at the National Department of Health, South Africa, both discussed the rollout of bedaquiline, a treatment for multidrug-resistant (MDR) TB. David Hermann, deputy director at the Bill & Melinda Gates Foundation Global Health Division overseeing the TB drug initiative, highlighted progress toward a shorter, simpler, safer pan-TB regimen for treating multiple forms of TB. Anna Vassall, director of the London School of Hygiene and Tropical Medicine Global Health Economics Centre and Joep Lang Chair at the Amsterdam Institute for Global Health and Development, discussed the value of conducting context-specific economic analyses of novel TB treatment regimens. The session concluded with reflections on critical elements in the implementation of new treatments for TB. Ezra Tessera, senior advisor of TB surveillance at the TB Data, Impact Assessment, and Communications Hub at U.S. Agency for International Development (USAID), John Snow Institute, focused on patient-centered implications of advancements in TB treatment and care. Richard Chaisson, professor of medicine, epidemiology, and international health and director of the Center for Tuberculosis Research at Johns Hopkins University School of Medicine, emphasized the urgency of framing TB as a global health emergency.
EXISTING TOOLS AND NEW TECHNOLOGIES
Bacillus Calmette–Guérin Revaccination
Presented by Alex Schmidt, Bill & Melinda Gates Medical Research Institute
Schmidt discussed the history and current state of policies regarding the use of the BCG vaccine and whether BCG revaccination can play a role in TB elimination.1 Over the past century, most countries have implemented national BCG vaccination policies for all individuals (see Figure 4-1).
Evidence for BCG Vaccination
Schmidt noted that because BCG vaccines were first implemented 100 years ago, not all of the evidence supporting the use of BCG meets today’s
___________________
1 BCG is a vaccine for tuberculosis that consists of live-attenuated Mycobacterium bovis, generally found to provide protection from extrapulmonary TB in children. See https://www.cdc.gov/tb/publications/factsheets/prevention/bcg.htm (accessed December 30, 2021).
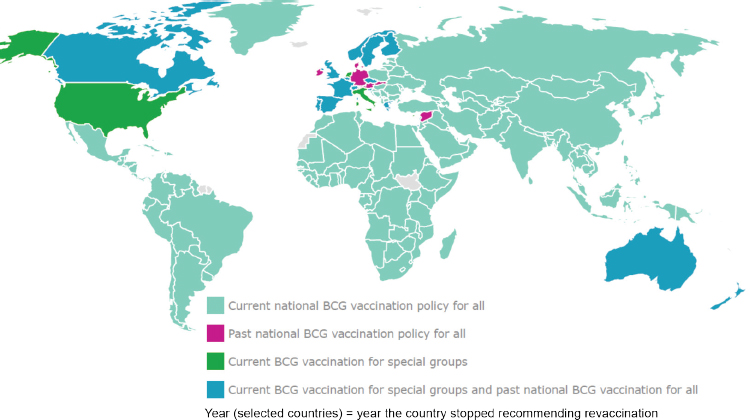
SOURCES: Presented by Alex Schmidt on September 15, 2021; http://www.bcgatlas.org.
evidentiary standards. Furthermore, there have been variations in not only the bacterial strains used in the vaccine, but also variations in geography, incidence, and observed vaccine efficacy. The Ulleval nurses study in Norway, published in 1948, found that BCG was highly efficacious against TB disease, and such studies motivated the introduction of national BCG vaccination policies (Heimbeck, 1948). A large study of adolescents in the UK from 1950 through 1967 who tested negative with a tuberculin skin test found that BCG vaccination was 78.4 percent effective in the prevention of tuberculosis in adolescence and early adulthood (Fourth Report, 1972). Data on the efficacy of BCG vaccines from the United States have been more heterogeneous. A long-term study of BCG in American Indian and Alaska Native communities initiated in 1936 found efficacy rates of around 80 percent in the first 15 years following vaccination and between 50 and 60 percent in subsequent decades, suggesting that primary BCG vaccination protects children and adolescents with negative skin test results from TB (Aronson and Aronson, 1952; Aronson et al., 2004). However, a long-term study of BCG vaccination in children and adults in the southern United States reported only a 14.2 percent BCG vaccination efficacy rate (Comstock and Palmer, 1966). Overall, Schmidt considered, data from children and young adults with negative skin test results who received BCG vaccinations shows that the BCG vaccine provides protection from TB disease.
Evidence for BCG Revaccination
Today, most neonates around the world receive BCG vaccines.2 Schmidt considered whether a second dose of this vaccine would affect the global TB burden. BCG’s vaccine efficacy is known to wane with age and, and since the modern TB epidemic in high-burden countries is mainly driven by cases among adolescents and young adults, neonatal BCG vaccination likely does not continue to offer protection in these older populations. Schmidt discussed two randomized trials that examined the efficacy of BCG revaccination, but also noted that the lack of data regarding baseline TB infection status in the study participants makes these study outcomes difficult to interpret, as BCG is not expected to work in people with current TB infection. One trial in Malawi evaluated a second dose of BCG or BCG plus a killed Mycobacterium leprae vaccine in over 23,000 BCG scar-positive children and adults, and found no protective effect for BCG revaccination (Karonga Prevention Trial Group, 1996). The second trial was a cluster randomized trial that studied the effects of BCG revaccination on the incidence of TB in school-age children in Brazil (Barreto et al., 2002, 2011). This study was conducted in two cities and found that revaccination offered no protection in the overall population, but a modest (statistically nonsignificant) effect was observed in Salvador, which is 1,000 km further away from the equator than the second study site in Manaus. One hypothesis to explain this observation is that exposure to environmental mycobacteria, which are more abundant in warmer climates near the equator, may offer protection against TB, therefore diminishing the protective effects of BCG vaccination. Thus, BCG might offer some protection in climates with less abundance of environmental mycobacteria.
A 2018 trial looked at the efficacy of a candidate subunit vaccine H4:IC31 compared with BCG revaccination in preventing Mycobacterium tuberculosis (MTB) infection (Nemes et al., 2018). The primary endpoint was prevention of initial interferon gamma release assay (IGRA) conversion, as an indicator of MTB infection, and no statistically significant efficacy was observed. However, evaluation of the secondary endpoint—sustained IGRA conversion defined as an initial conversion that remains positive at 3 and 6 months after the conversion—revealed a 45 percent efficacy for BCG revaccination. While there were fewer initial conversions in the BCG revaccination group compared with the placebo group, the bigger driver of the efficacy read-out was the number of IGRA reversions. He suggested that an optimistic interpretation of this observation is that IGRA reversion—that is,
___________________
2 BCG is given as a single dose to neonates in most countries. See https://apps.who.int/immunization_monitoring/globalsummary/schedules?sc%5Br%5D%5B%5D=AFRO&sc%5Br%5D%5B%5D=AMRO&sc%5Br%5D%5B%5D=EMRO&sc%5Br%5D%5B%5D=EURO&sc%5Br%5D%5B%5D=SEARO&sc%5Br%5D%5B%5D=WPRO&sc%5Bd%5D=&sc%5Bv%5D%5B%5D=BCG&sc%5BOK%5D=OK (accessed February 8, 2022).
from having an immune response to MTB proteins to not having an immune response—is indicative that MTB has been cleared, but that cannot yet be conclusively established.
Since no more than 10 percent of latently MTB-infected (IGRA-positive) individuals progress to active TB disease, it is unclear whether a 45 percent reduction in sustained IGRA conversion (prevention of sustained MTB infection) would result in prevention of TB disease. It is possible that a subset of the individuals who reverted to IGRA-negative following BCG revaccination would have never progressed to active disease in the absence of revaccination. Therefore, it is not yet possible to conclude whether the study outcome translates to less development of active TB disease over the longer term, said Schmidt.
An ongoing randomized controlled trial (BCG ReVax) is generating data to potentially support new policies for BCG revaccination.3 The primary objective of this trial is to demonstrate the efficacy of revaccination in preventing sustained MTB infection, and an important secondary objective is to explore or develop correlates of risk and protection. If the correlates of risk and correlates of protection from the earlier trial can be described and tested in this current large-scale study, it could lead to the identification of candidate indicators for the prevention of sustained MTB infections. This trial will also contribute to an improved understanding of the mechanisms of protection, which is necessary to develop the next generation of vaccines, Schmidt believes. However, it is not clear whether results from this study will be sufficient to spur policy changes such as implementation of BCG revaccination. To convince policy makers to implement BCG revaccination, it may be necessary to draw on additional data sources, including phase 3 trials and real-world evidence from the discontinued BCG revaccination programs.
Current State of Evidence and Ways Forward for BCG Revaccination
Schmidt provided an overview of evidence to date for BCG revaccination and suggested several paths forward to further elucidate the effectiveness of this strategy. BCG revaccination is associated with a higher rate of IGRA reversion. The mechanism of this effect is not yet fully understood, but it could be an indication of a protective immune response that potentially leads to MTB clearance. However, as discussed above, it is unknown what percentage of BCG revaccinated individuals who reverted to IGRA-negative would have progressed to develop TB disease in the absence of IGRA reversion. To demonstrate such a preventive effect, the correlates or indicators
___________________
3 This clinical trial was mentioned in Chapter 2. See more information about the NCT04152161 trial at https://clinicaltrials.gov/ct2/show/NCT04152161 (accessed November 18, 2021).
for prevention of sustained infection must be linked to the correlates for prevention of disease.
Given its availability and affordability, BCG revaccination could contribute to accelerating the end of the TB epidemic, but a potential policy change will likely depend on a definitive link between prevention of sustained infection to prevention of disease. The evidence generated by the BCG ReVax study may provide useful data for policy makers considering the implementation of BCG revaccination. Further evidence may be generated by forthcoming randomized controlled trials (e.g., rBCG phase 3)4 or from real-world data. However, factors such as the potential effects of geography, the abundance of environmental mycobacteria, and differences in commercially available vaccines will likely shape those policy deliberations. Schmidt emphasized that if robust correlates of risk and correlates of protection can be established for TB vaccines, the effect on vaccine development could be transformational, leading to faster, less expensive, and easier-to-iterate vaccines.5
Pathway to Effective Tuberculosis Vaccines: Promising New Adjuvants and Late-Stage Clinical Development of Vaccine Candidates
Presented by Steven Reed, University of Washington and HDT Bio
Reed discussed the breadth and diversity of ongoing research in the TB vaccine pipeline within which numerous vaccine candidates are being studied, including those based on live or whole-cell organisms, vector platforms, and recombinant proteins. He explained that there is a range of strategies and potential uses of TB vaccines (see Figure 4-2). For instance, pre-infection vaccines are intended to prevent infection and/or disease by reducing the risk of either the initial infection or establishment of granuloma. Post-infection vaccines aim to prevent disease progression after initial infection and/or prevent reactivation from latent infections. Immunotherapeutic vaccines can be used to treat TB disease, shorten the course of chemotherapy for active TB, and decrease relapse or reinfection rates.
Promising Vaccines and Advancements in Vaccine Technology
Reed suggested that focusing on effective adjuvants for protein vaccines as well as alternative delivery of vaccine antigens, such as delivering antigens via nucleic acids instead of proteins, are two promising research
___________________
4 See https://www.clinicaltrials.gov/ct2/show/NCT03152903 (accessed December 30, 2021).
5 BCG revaccination is a debated topic. For other references related to this topic, see Ahmed et al., 2021.
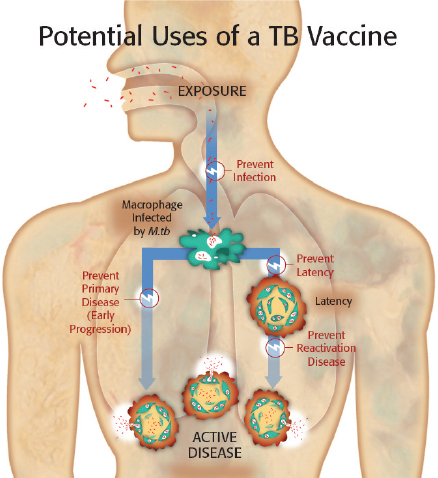
NOTE: M.tb = Mycobacterium tuberculosis.
SOURCES: Presented by Steve Reed on September 15, 2021; adapted from Bill & Melinda Gates Foundation.
areas to further advance and accelerate TB vaccine development. He shared the example of the M72/AS01E vaccine, which was developed by Reed and his colleagues over 25 years ago and has been evaluated for its effect in prevention of disease with promising results, but has faced slow progress in advancement since. Reed also discussed potential areas of research that could accelerate the development of promising vaccines, such as M72/AS01E (Van Der Meeren et al., 2018).6,7
Reed highlighted the effect of intellectual property constraints on current toll-like receptor agonists that are used as vaccine adjuvants. In the past, access to several of these components used in adjuvants such as AS01E has been restricted by intellectual property regulations (e.g., licensing requirements).8 With the expiration of key patents and the evolution
___________________
6 QuantiFERON-TB is an interferon-gamma release assay (IGRA) for the diagnosis of Mycobacterium tuberculosis infections. A positive assay result indicates MTB infection. See https://www.cdc.gov/tb/publications/factsheets/testing/igra.htm.
7 Van Der Meeren et al., 2018, conveys the results of an interim analysis. A final analysis was published by Tait et al., 2019, which demonstrated results of 49.7 percent efficacy.
8 AS01 stands for Adjuvant System 01 and is a vaccine adjuvant that consists of monophosphoryl lipid A (a TLR4 agonist often derived from bacterial cell membranes) and saponin (a plant-derived natural product) in a liposomal formulation. See Garçon and Di Pasquale, 2017.
of synthetic biology, TLR4 agonists are now freely available and can be derived using synthetic ingredients.9 Reed explained how synthetic biology may occupy an important role in developing next-generation AS01. AS01 has traditionally been made using natural products, including a semi-synthetic cholesterol that is in high demand for various lipid formulations in pharmaceutical products. Reliance on natural products for production can be expensive. However, synthetic or partially synthetic versions of each of these products are now available, which will broaden access to AS01. Reed encouraged researchers to consider this approach to replicate M72/AS01E data with a focus on improving global access to vaccination.
New adjuvants also hold great promise in immunotherapy, said Reed. Based on evidence to support the use of vaccines for immune therapy for TB, efforts are underway to further explore this application (Coler et al., 2013). The M72/AS01E vaccine has been considered for immunotherapy, though its use was discontinued owing to reports of adverse events. Still, Reed posited that one takeaway from this observation could be that the selection of an adjuvant may best be linked to the application, as in whether it is used as part of an immunotherapeutic or as a prophylactic vaccine.
Nucleic Acids as Vaccine Platforms
Reed next discussed nucleic acid vaccine platforms, where instead of using traditional protein antigens, antigen-encoding DNA or RNA is delivered by the vaccine for subsequent transcription or translation to produce the target antigen. He began with RNA vaccines, emphasizing lessons learned from the COVID-19 pandemic. RNA vaccine development has struggled in the past but demonstrated success during the COVID-19 pandemic, building in part on prior research that identified the target protein antigen. However, COVID-19 has also shown that local manufacturing and global access to vaccines are critical for halting pandemics. Accordingly to Reed, RNA vaccines offer numerous important advantages:
- They can be developed using cost-effective synthetic processes.
- They are safe, and they create potent antibody and cellular responses.
- They can also encode multiple antigens, adding to their cost-effectiveness.
Despite the promise of RNA vaccines, the extent and durability of RNA vaccine T-cell responses are not yet known.
___________________
9 TLR4 stands for toll-like receptor 4. Toll-like receptors detect pathogens and initiate immune responses. See Celine and Yuanqing, 2014.
In contrast to the recent progress with RNA vaccines, research to develop DNA vaccines has been challenging, Reed said. He believes that DNA vaccines can provide sufficient T-cell response, but methods to effectively deliver DNA immunization (e.g., electroporation) are difficult to achieve. Furthermore, efficient protein expression from DNA vaccination requires the vaccine material to be delivered into the cells’ nuclei, while efficient expression of RNA vaccination requires only cytoplasmic delivery. In addition, RNA vaccines may use either nonreplicating mRNA or self-replicating RNA.10 Reed believes that replicating RNA produces more proteins and generates more virus-like particles, resulting in more potent T-cell responses than mRNA vaccines and requiring smaller doses. Reed noted that his team is focusing on replicating RNA vaccines for these reasons.
Formulation of RNA Vaccines
Lastly, Reed discussed formulation for RNA vaccines. The most common type of formulation has been lipid nanoparticles that encapsulate the RNA. Lipid nanoparticles allow for a single-vial vaccine product, but these products are complex to manufacture and scale up, and each target RNA must be encapsulated within the nanoparticles (Malone et al., 1989). Cationic nanoemulsion RNA vaccine formulations create a kinetic surface chemistry on the oil particles that allows the RNA to adhere to the outside of the particle (Brito et al., 2014). This formulation allows for stockpiling of formulation and rapid use with different target RNAs. However, it also requires a two-vial presentation that can be mixed at bedside. Nanostructured lipid carriers are similar to cationic nanoemulsions, but they include a solid oil component and have historically been used for the delivery of lipophilic small-molecule drugs.
Reed discussed the lipid inorganic nanoparticle (LION) RNA formulation that his team has developed, where adjuvant oils and inorganic metal particles in the core are surrounded by cationic lipids with replicating RNA stabilized on the outside surface. The use of LION or other formulations that have RNA adhered to the outside allows for easier scaling up of production, and the use of replicating RNA could lower the required dose of the potential vaccine. Reed pointed out that these two factors may be critical for TB and COVID-19 control, as controlling these diseases requires a large number of individual doses.
RNA delivery technology has been optimized to provide single shot protection for TB, said Reed. This technology has shown promising results
___________________
10 While two nonreplicating, mRNA-based vaccines had received emergency use authorization for COVID-19 at the time of the workshop, self-replicating or self-amplifying RNA vaccines have not yet been approved. See Bloom et al., 2021, for a review on self-replicating or self-amplifying RNA vaccines.
among mice and ideally those results will be predictive of efficacy in nonhuman primates (NHPs) and humans. Importantly, the delivery of TB protection in a single shot will help meet the need for hundreds of millions of doses of vaccines. HDT Bio has ongoing work to set up centers for technology transfer and capacity development in several countries, including Brazil, South Africa, India, South Korea, and China. Reed added that they have found technology transfer efforts to be very successful in India because of existing efforts conducted by lead investigators in that country.
Advances in Host-Directed Therapeutics for Antibiotic-Resistant Tuberculosis
Presented by Daniel Kalman, Emory University
Kalman discussed how the use of host-directed therapeutics (as opposed to conventional antibiotics) for treating DR TB has the potential to change the development landscape. New solutions are needed to counter both DR TB and TB-induced impairment of lung function, which is associated with a substantial global economic burden (Menzies et al., 2021). Host-directed therapeutics for TB may help address both of those issues by circumventing antibiotic resistance and improving lung function.
Kalman suggested that COVID-19 may increase deaths from bacterial infections by causing impaired antibacterial immune responses—a condition that Kalman classified as “immune amnesia.”11 Kalman worried that COVID-19-induced lymphopenia may have similar consequences, further surmising that COVID-19 patients with lung damage may be more susceptible to TB and vice versa. Moreover, COVID-19 pandemic response measures have led to reductions in TB control in Africa. Given these challenges, he considered whether host-directed therapeutics may offer a solution.
Development of the Host-Directed Therapeutic Imatinib
Host-directed therapeutics were originally developed for malaria, Kalman noted. They offer activity against antibiotic-resistant strains because they target the host, reducing the likelihood of developing antibiotic resistance, and it is possible for host-directed therapeutics to synergize with
___________________
11 Immune amnesia is a term applied to the loss of immune memory described after infection by the measles virus. See Gorvett, 2021. Influenza is also associated with subsequent susceptibility to bacterial lung infections owing to immunological mechanisms; see Paget and Trottein, 2019.
antibiotics. Furthermore, host-directed therapeutics may act against nonreplicating MTB.12
Kalman discussed an example of host-directed therapeutics with imatinib, a tyrosine kinase inhibitor that is approved for cancer and certain types of blood disorders (brand name: Gleevec).13 He shared that the development process began with three research questions: (1) how do pathogens move into, throughout, and out of host cells; (2) how can the host immune response be altered to disrupt pathogen–host equilibrium in chronic infections; and (3) is it possible to target immune or cellular functions that MTB has evolved to circumvent? Kalman focused on the ABL1 gene, which appears to mediate the trafficking of MTB within cells by preventing lysosomal fusion, allowing TB to stay outside of the lysosome (Korbee et al., 2018).
Use of Imatinib to Treat Tuberculosis
Kalman explained that in addition to being safe and effective as a chemotherapeutic agent, imatinib is also effective in “resetting” the immune response to TB through stimulating emergency hematopoiesis and has shown promise of potentiating the efficacy of existing antibiotics against MTB (Napier et al., 2011, 2015).14 Evidence supporting the use of imatinib have been generated in primate infection models. Treatment with imatinib in NHPs with active TB infection was found to increase myelopoiesis. Kalman described a model wherein active or latent TB infection was established in rhesus macaques. In this model, latent TB can be reactivated by additional infection with simian immunodeficiency virus. The animals with active TB were treated at the peak of disease with either imatinib and antibiotics or with antibiotics alone. NHPs with reactivated latent TB were treated with imatinib alone (no antibiotics). Survival rates among these NHPs are lowest among those with active TB, but the combination of imatinib with antibiotics was found to reduce bacterial load more than antibiotics alone. With reactivated TB, imatinib was also found to reduce bacterial load. This finding suggested that using imatinib may be useful for reducing the length of treatment. Furthermore, chest X-ray imaging showed that imatinib reduced signs of pulmonary disease in TB-infected animals. Kalman added that imatinib was also shown to reduce disease pathology by reducing granulomas,
___________________
12 Nonreplicating or dormant M. tuberculosis in the patient are recalcitrant to treatment with typical antibiotics treatment. See Connolly et al., 2007.
13 Kalman noted that imatinib was initially developed for chronic myelogenous leukemia. One of its targets is ABL1 (also known as c-ABL).
14 Emergency hematopoiesis is a process where hematopoietic stem cells are activated to differentiate and generate immune cells in response to stress signals, including bacterial infections. See Zaretsky et al., 2014.
which may contribute to the observation of synergy between imatinib and antibiotics.
Ongoing Imatinib Dosing Trials
IMPAc-TB has begun a phase 2 trial in collaboration with the National Institutes of Health (NIH) to find the right dose of imatinib, said Kalman.15 The trial will investigate the safety, pharmacokinetics, and hematologic effects of low doses of imatinib in healthy volunteers when it is given with and without isoniazid and rifabutin. This trial will test the hypothesis that imatinib increases myelopoiesis at low doses and promotes MTB killing ex vivo. Another phase 2 trial will compare the combination of imatinib and antibiotics against the use of antibiotics alone in adult patients with drug-susceptible (DS) TB. This trial will test the hypothesis that imatinib shortens treatment period (measured as a decrease in the time needed to achieve negative sputum culture) and improves lung function.
Prospects for Imatinib Regulatory Approval and Clearance for Use
Kalman discussed regulatory progress toward approval and clearance for imatinib use in TB patients by 2025.16 Dosing and safety trials in normal patients are underway and expected to be complete by the end of 2022. Efficacy trials are being developed, and an efficacy trial for TB patients with the Aurum Institute in South Africa is in progress. In the future, it will be necessary to test the use of imatinib in patients with MDR TB, he noted. Because imatinib is off-patent (i.e., cheaper generics may be available if there is sufficient market demand) and its safety is well established (thus reducing the need for further expensive clinical trials), the use of imatinib to treat TB is commercially viable. To deliver imatinib as a TB treatment globally, a commercialization and distribution plan will be needed for high-burden countries such as Africa, China, India, and Russia. Currently, imatinib is relatively expensive, but Kalman predicted that as it becomes widely used for TB treatment, the price will drop rapidly. He suggested that the distribution and sale of imatinib for TB treatment could eventually use a commercial
___________________
15 The Immune Mechanisms of Protection against Mycobacterium tuberculosis Centers (IMPAc-TB) program is an initiative established by the National Institute of Allergy and Infectious Diseases. See https://www.niaid.nih.gov/research/immune-mechanisms-protection-mycobacterium-tuberculosis (accessed December 31, 2021).
16 At the time of this publication, imatinab was one potential host-directed therapeutic candidate for TB among many others. For a landscape review of host-directed therapeutics, see Young et al., 2020.
model wherein a slimmer profit margin from low pricing is offset by the high volume of doses.
Immune Mechanisms of Protection Against Tuberculosis
Presented by Rhea Coler, Seattle Children’s Research Institute
Coler focused on immune mechanisms of protection against TB by providing an overview of the immunology of MTB infection, possible targets of vaccine development, innate and adaptive (mucosal and humoral) immune systems, and correlates of protection. She also introduced work that she and her colleagues are conducting related to the IMPAc-TB study.
Coler pointed out that it has been more than two decades since the World Health Organization (WHO) first declared TB to be a global health emergency and emphasized both the burden of TB and the need to develop new products to prevent, diagnose, and cure the disease. However, progress toward these aims has been slow. In 2020, approximately 10 million people developed TB and 1.4 million people died of the disease. The spread of TB is influenced by a variety of factors, including age, geography, socioeconomic status, and comorbidities. Furthermore, it is known that DR TB is a major contributor to the burden of antimicrobial resistance, which itself is a significant threat to global health security. Each of these factors has implications for strategies for disease control.
Immune Response to Mycobacterium Tuberculosis
Many immune mechanisms have been proposed to control TB, including innate immune responses, antibodies, innate cell interactions by Fc receptors, and lung-resident T cells. Coler described the respiratory mucosal responses following MTB infection of airway epithelial cells (Brazier and McShane, 2020; Stylianou et al., 2019). MTB enters the body via aerosolized droplets that are inhaled into the airways. Although alveolar macrophages are the principal target of these bacilli, they are also capable of infecting human lung epithelial cells. These airway epithelial cells express a variety of pattern recognition receptors. Further, there are surfactant proteins that combine with components of the mycobacterial cell wall. The epithelial recognition of MTB activates numerous signaling pathways that induce the production of cytokines, such as tumor necrosis factor alpha, interferon gamma, and chemokines, such as interleukin (IL)-6 and IL-8. These airway epithelial cells are also potent responders to cytokines, such as IL-1 beta and type 1 interferons released by infected macrophages. Epithelial cells are capable of directly presenting intracellular antigens to resident CD8 T cells through
major histocompatibility complex class I molecules, which stimulate interferon gamma production.
Technical Feasibility of Vaccine Development
Several factors support the technical feasibility of a vaccine, said Coler. For instance, it is estimated that 90 percent of persons infected with MTB do not progress to active disease.17 Additionally, the history of the BCG vaccine supports the feasibility of a vaccine for TB. However, the BCG vaccine is only partially protective in children and prevents only 5 percent of vaccine-preventable deaths attributable to TB, underscoring the need for an alternative vaccine. Moreover, because the term tuberculosis is used to refer to multiple diseases,18 a variety of vaccines may be needed to prevent infection, prevent disease progression, or be used as treatment or adjunctive immunotherapy.
Coler explained that a principal barrier to MTB vaccine development is the complexity of the immune response to infection, along with uncertainty regarding what constitutes immunological correlates of protection. NIH has awarded three contracts to IMPAc-TB with the aim of comprehensively identifying the complex immune responses required to prevent MTB infection or active disease by comparing and investigating the mycobacteria- and vaccine-induced protective immunity in animal and human subjects. IMPAc-TB is working with its partner investigators to advance understanding of the basic immunological mechanisms that regulate host resistance to MTB and vaccine-mediated protection. The hope is that this work will lead to new insights into TB vaccination, she added.
Roadblocks to Vaccine Development
Coler discussed known roadblocks to vaccine development, approaches to overcoming these obstacles, and how the results of those efforts would facilitate effective vaccine development. The current lack of immune correlates has limited the development of vaccine candidates with clinical efficacy. This barrier may be overcome through specific and exploratory immune system interrogation of local (i.e., mucosal) and systemic responses across multiple interventions in preclinical and clinical models, combined with statistical analysis of immune responses. The resulting correlates of protection would help to accelerate the vaccine development pipeline and facilitate a
___________________
17 Progression to active TB is host dependent and is affected by factors such as host age. See Narasimhan et al., 2013.
18 Different forms of TB include active disease, latent infection, and extrapulmonary TB. See https://tbfacts.org/types-of-tb (accessed December 31, 2021).
more rational vaccine design process.19 However, the tool sets available for high-throughput standardized vaccine candidate evaluation are currently limited. This barrier can be approached by aligning mycobacterial and vaccine intervention regimens and kinetics of host immune interrogation across mouse, guinea pig, NHP, and human studies. Such efforts would facilitate vaccine development through model alignment; furthermore, standardization could be used to test novel candidates with greater throughput.
The effect of prior nontuberculous mycobacteria (NTM) infection on vaccine efficacy also presents challenges to vaccine development, said Coler. These challenges can be approached through evaluation of vaccine efficacy and concurrent immune response while accounting for NTM exposure (preclinical) or positive NTM recall responses (clinical). This approach will support the rational design of TB-specific vaccines that preclude NTM interference and improve efficacy, further informing clinical trial participant criteria. Uncertainty regarding the effect of prior BCG interventions on vaccine efficacy is another challenge for vaccine development. This can be addressed through the evaluation of vaccine efficacy and concurrent immune responses while accounting for planned BCG exposure (preclinical) or positive BCG recall response (clinical). This approach will facilitate the development of rationally designed TB-specific vaccines to preclude BCG vaccine interference or strengthen and enhance BCG vaccination. Finally, the narrow focus on single-vaccine platforms in head-to-head comparison is a barrier to vaccine development. She suggested that this barrier can be approached through specific and exploratory immune system interrogation across multiple interventions. BCG priming, protein antigen and adjuvant combinations, and RNA vaccine candidates can each be explored. This will allow for the design of TB-specific vaccines that positively influence lung pathology and offer protective efficacy with long-lasting immune responses. This approach will also inform platform development decisions so platforms can meet correlates of protection requirements.
Immune Mechanisms of Protection Against Mycobacterium tuberculosis Center Program
Coler presented an overview of the IMPAc-TB program, which is a cross-species mechanistic interrogation of mycobacterial and vaccine-induced immunity. The overarching paradigm of IMPAc-TB is to identify and validate common protective correlates of immunity against MTB in
___________________
19 Rational vaccine design is an approach where antigens, adjuvants, and delivery systems are combined to elicit an expected immune response against the target pathogen. This is distinct from the historically used empirical vaccine design approach. See Rueckert and Guzmán, 2012.
order to escalate preclinical animal models of TB, NTM exposure, and human challenge experimental medicine studies. She posited that these efforts will be critical for the rational designing and development of candidate vaccines that generate robust levels of durable, protective immunity against TB. The program is using three animal models and human hosts, and it will harmonize assays across various partner sites. The program will use state-of-the-art technologies to increase vaccine efficacy, optimize vaccine delivery, and dissect the immune responses dictated by candidate vaccines. The aim is that novel vaccine candidates can be tested and used with greater throughput through harmonization strategies, such as clinical grading of different BCG vaccines, ultra-low-dose models, various clinical MTB isolates, and various immunological stimulation reagents, such as the MTB 300 peptide pools and NTM peptide pools.
Coler highlighted three contracts that IMPAc-TB was awarded in 2019. Two of these contracts are located at Seattle Children’s Research Institute and the University of Washington. Given the close proximity of these facilities, collaboration and synergies are expected to be amplified. The third grant was awarded at the Harvard T.H. Chan School of Public Health. The IMPAc-TB program will use cutting-edge technologies to better understand the immune responses that provide protection against TB infection. She highlighted collaborative efforts within the IMPAc-TB program. Program participants use shared controls, serum samples, and barcoded MTB strains for competition assays, allowing for plug-and-play compatibility between sites. The program also shares standard operating procedures and protocols. She noted that the program organizers hope to back-translate human results into experimental models so they can be more rapidly advanced.20
TRANSFORMING TREATMENT OPTIONS
Developing a New Treatment-Shortening Regimen for Drug-Susceptible Tuberculosis
Presented by Payam Nahid, University of California, San Francisco
Nahid described lessons learned from designing and conducting a trial that was successful in developing a new shorter regimen to advance TB treatment to serve as a potential blueprint for future treatment-shortening work. The Tuberculosis Trials Consortium Study 31/AIDS Clinical Trials Group
___________________
20 Back-translating refers to incorporation of new knowledge from the disease in humans to inform the improvement of existing or development of new animal models. See Denayer et al., 2014.
A5349 (TBTC Study 31/A5349) was a randomized, open-label, phase 3, noninferiority trial that was co-funded by the Centers for Disease Control and Prevention (CDC) Tuberculosis Trials Consortium and the NIH AIDS Clinical Trials Group (Dorman et al., 2021).21 This international multicenter study spanned 34 sites in 13 countries across 4 continents.
Study Design and Conduct
TBTC Study 31/A5349 was a three-arm trial that compared two investigational 4-month rifapentine-based regimens with a standard 6-month control regimen. More than 2,500 participants (age 12 years or older) newly diagnosed with DS pulmonary TB were enrolled in the study.22 The primary efficacy outcome was survival free of tuberculosis at 12 months post-randomization.
The 6-month control arm regimen, endorsed by the CDC and WHO, included 8 weeks of once-daily isoniazid, rifampicin, pyrazinamide, and ethambutol (2HRZE) and followed by 18 weeks of once-daily isoniazid plus rifampicin (4HR). Both investigational arms substituted dose-optimized rifapentine for rifampicin. Participants in the rifapentine-only investigational arm were treated with a regimen of 8 weeks of once-daily isoniazid, rifapentine, pyrazinamide, and ethambutol (2HPZE) followed by 9 weeks of once-daily isoniazid and rifapentine (2HP). Participants in the other investigational arm, which substituted moxifloxacin for ethambutol, received a regimen of once-daily rifapentine, isoniazid, pyrazinamide, and moxifloxacin for 8 weeks followed by once-daily rifapentine, isoniazid, and moxifloxacin for 9 weeks (2HPM). Rifapentine was administered at a dose of 1,200 mg daily—based on extensive pharmacometric modeling work—and moxifloxacin administered at 400 mg daily in accordance with the package insert; the other drugs were given at standard body-weight-adjusted doses. Five of the seven daily doses per week were administered via directly observed treatment. Rifapentine was given with food and rifampicin without, because of the differential food effect on the two drugs.
Efficacy Results and Safety Outcomes
The results of the study demonstrate that the 2HPZM/2HPM regimen is safe and effective for treating DS TB, said Nahid. He presented the pri-
___________________
21 This clinical trial was mentioned in Chapter 2. More information about the Tuberculosis Trials Consortium Study 31/AIDS Clinical Trials Group A5349 is available from https://clinicaltrials.gov/ct2/show/NCT02410772 (accessed December 15, 2021).
22 Participants with HIV co-infection were included with a CD4 threshold of ≥100 cells/mm3.
mary efficacy results of the study, which had a noninferiority design with a margin of 6.6 percent (see Figure 4-3). To demonstrate noninferiority, the upper bound of the 95 percent confidence interval for the difference in proportions of unfavorable outcomes between investigational and control regimen had to be below 6.6 percent. Noninferiority also had to be demonstrated in both the assessable population and microbiologically eligible study populations.23
Compared to the control regimen, the rifapentine-moxifloxacin regimen met the noninferiority criteria for efficacy for both of the co-primary analysis populations, with the upper bound of the 95 percent confidence interval well within the margin across all analyses. The rifapentine-only arm did not meet noninferiority criteria for efficacy versus the control arm in either co-primary analysis population. Nahid added that the results of 14 pre-specified sensitivity analyses, as well as pre-specified analyses conducted in the intention to treat per protocol, were all consistent in meeting noninferiority for this new experimental 17-week rifapentine-moxifloxacin regimen; the rifapentine-only regimen did not meet the noninferiority criteria throughout those analyses.
The primary safety outcome—experiencing any grade 3–5 adverse event during study treatment—was comparable across the three study arms, experienced by 19.3 percent of participants in the control arm,
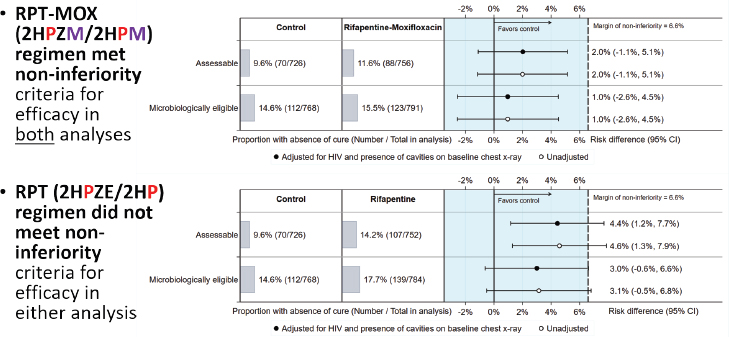
NOTES: CI = confidence interval. Abbreviations for the individual drugs in the treatment regimen are color-coded.
SOURCE: Presented by Payam Nahid on September 15, 2021.
___________________
23 More information on the study analysis and criteria are described in Dorman et al., 2021.
14.3 percent of participants in the rifapentine-only arm, and 18.8 percent of participants in the rifapentine-moxifloxacin arm. In secondary safety analyses, there were some numerical but not statistically significant differences across the study arms. Participants in the rifapentine-moxifloxacin arm had a slightly higher proportion of treatment-related grade 3–5 events compared to the control arm. This could be attributed to the open-label trial design because treatment relatedness of the reported adverse events was determined by site investigators unblinded to the regimen. The proportions of participants with treatment discontinuations, at least one serious adverse event during study treatment, and all-cause death during study treatment were slightly lower in participants on both rifapentine regimens compared to the control.
Comparative Context for the New Regimen
Nahid situated the results of this safe and effective 4-month 2HPZM/2HPM regimen within the context of other recent randomized controlled trials for DS TB treatments among microbiologically eligible analysis populations. The rifapentine-moxifloxacin regimen in TBTC Study 31/A5349 is the most potent regimen study to date and is the only regimen that has met noninferiority criteria for efficacy. Although the rifapentine-only regimen in TBTC Study 31/A5349 did not meet noninferiority criteria, it is still the second-most potent regimen compared to other recent trials of treatment-shortening regimens, including: (1) isoniazid-rifampicin-pyrazinamide-moxifloxacin/isoniazid-rifampicin-moxifloxacin (REMoxTB, 2014),24 (2) moxifloxacin-rifampicin-pyrazinamide-ethambutol/moxifloxacin-rifapentine (RIFAQUIN, 2013), (3) moxifloxacin-rifampicin-pyrazinamide-ethambutol/moxifloxacin-rifampicin (REMoxTB, 2014), and (4) pretomanide-moxifloxacin-pyrazinamide (TB Alliance, 2022).
Advancing Treatment Regimen Development Through Lessons from Previous Studies
Nahid explained that the study design for this safe and effective 4-month 2HPZM/2HPM regimen was informed by lessons from more than two decades of murine, preclinical, and pharmacokinetic studies around rifapentine, which was initially used intermittently. Pharmacometric studies then established animal and human linkages and integrated that knowledge in terms of the effectiveness and efficacy of the rifapentine regimens.
___________________
24 More information about REMoxTB, is available from https://www.tballiance.org/portfolio/trial/5093 (accessed December 15, 2021).
This foundational information effectively reduced the risk of many of the study design decisions for TBTC Study 31/A5349. For instance, the study consortium prioritized experimental murine models throughout and conducted iterative phase 2 trials with moxifloxacin-rifapentine. Further, it embedded intensive, sparse, and specific pharmacokinetic substudies to support exposure-response analysis. This allowed for extensive modeling of pharmacokinetic efficacy data, tolerability data, and biomarker data to define the effect of key variables (e.g., sex, race, cohabitation status, HIV status, food effect) in determining the optimal dose. Nahid noted that contrary to prior development approaches, the investigators did not seek to establish the lowest effective dose or the maximally intermittent dose. Rather, they targeted the dose that would facilitate the maximum tolerated exposure, representing a change in the perspective on regimen development for DS TB.
Quantitative Translation Toolbox for Tuberculosis Regimen Development
A quantitative translational toolbox is now available for TB regimen development that is spurring advancement in the field (Ernest et al., 2021). This toolbox integrates multifaceted sources of data on the preclinical side, including plasma pharmacokinetics, lesion pharmacokinetics, immunology, pharmacokinetics/pharmacodynamics of monotherapies, multitherapies, and drug resistance. Also on the preclinical side, new biomarkers—such as the ribosomal RNA (rRNA) synthesis ratio25—are providing orthogonal information far beyond that provided by the traditional marker, colony-forming units (Walter et al., 2021). Nahid added that on the clinical side, there is emerging value in looking across lesion pharmacokinetics and then integrating data and information from phase 2A studies and beyond, beginning a new chapter in TB regimen development.
Mitigating Risk Through Study Design and Conduct
The investigators were also able to mitigate risk and optimize lessons from Study31/A5349 through the design and conduct of the trial itself, said Nahid. The large sample size (more than 2,500 participants) allowed for assessment across subgroups, which was useful given the uncertainty at the outset as to whether the regimen would be effective against TB disease of various degrees of cavitary severity. By embedding sparse pharmacokinetics in the study protocol across all arms for all TB drugs and participants, the
___________________
25 The rRNA synthesis ratio measures the effect of drugs on ongoing bacterial rRNA synthesis.
trial provides the richest data set available to date with broad geographic representation, including information about the standard 6-month control regimen in addition to the new regimen. Thus, the data set can serve as a benchmark for future TB regimen development work. Owing to uncertainties related to the potential for drug–drug interactions between efavirenz and high-dose rifapentine, enrollment of HIV-positive participants was staged with pharmacokinetics and viral load assessments to assess safety; the two drugs were found to be safely co-administered. The trial also focused upon measuring adherence and maximizing retention; both must be robust to provide practical understanding of how regimens perform in the field—a concept referred to as “high assay sensitivity for noninferiority” by regulatory authorities.
Additionally, the study investigators invested in a multiyear, multinetwork effort to harmonize laboratory practices across sites, based on decades of mycobacteriology experiences, to help reduce noise and differences in data readout across sites (Dorman et al., 2020). Despite these standardized practices often differing from local practices, they were adopted uniformly at the study sites around the world, said Nahid. Real-time data management and reports facilitated quality assurance at sites as well as supporting monitoring and reviews by the Data Safety Monitoring Board. Moreover, the investigators prioritized efforts to minimize bias when measuring endpoints in this open-label study by providing extensive trainings on the trial’s standard operating procedure and by developing a new “Possible Poor Treatment Response” procedure.26 The latter is a guide to collecting a standardized suite of data to understand patient-specific endpoints when investigators are concerned about trial participants. They also embedded substudies of innovative biomarkers, pharmacokinetics, and other investigations co-funded by NIH and others (e.g., intensive pharmacokinetics analyses from this data pool, TBTC Study 31A and 31B to analyze sputum transcriptomics, quantitative GeneXpert indications of treatment outcome, and bacterial drug susceptibility) to learn more from the trial even if the regimen had not proven to be safe and effective. Nahid concluded by highlighting major lessons learned during the design and conduct of Study31/A5349 (see Box 4-1). Additional relevant lessons from the design and conduct of recent TB therapeutics trials are also summarized in a special collection “Advances in Clinical Trial Design for Development of New Treatments for Tuberculosis” (Lienhardt and Nahid, 2019).
___________________
26 Nahid noted at the time of the workshop that the manuscript for the “Possible Poor Treatment Response” procedure is under development.
Rolling Out a New Treatment Regimen for Drug-Resistant Tuberculosis: Industry Perspective
Presented by Adrian Thomas, Johnson & Johnson
Thomas presented a case study of the rollout of bedaquiline, a treatment for MDR TB. This drug led to the founding of the Global Public Health team at J&J, which addresses HIV, TB, mental health, soil-transmitted helminths, global surgery, a vaccines portfolio, and an early development portfolio that includes dengue fever, malaria, and postpartum hemorrhage. The group uses a model of collaboration at scale, working with over 100 partners at the global, regional, and local levels. The Global Public Health team has its own research and development (R&D) organization, a fully dedicated and accessible team, and an implementation team that works in 26 countries. Using expertise in insight generation, consumer marketing, and human-centered design, the team brings broad business skills and capabilities to the areas it serves.
J&J’s Tuberculosis Initiatives
Thomas noted that J&J has long been committed to addressing TB, particularly DR TB. In December 2012, bedaquiline—the first novel mechanism of action TB drug released in nearly 50 years—was approved. Phase 2 data indicated potential for QT interval prolongation27 and cardiotoxicity. Given the settings within which J&J implements new technologies, creating the infrastructure to monitor for these conditions using electrocardiogram (ECG) and other technology was a challenge. Additionally, reticence to adopt new technologies created an adoption curve for TB that looks very different than for commercial therapeutic areas such as oncology or immunology. Thomas described that, to date, J&J has shipped over 420,000 6-month treatments to MDR TB patients in 147 countries, 47 of which have formal regulatory approvals in place.
A 10-year J&J initiative, spanning from 2018 to 2028, aims to broaden access to TB treatment, improve detection of undiagnosed cases, and accelerate R&D to discover next-generation treatments. An innovation toward expanded access came in the form of a regulatory waiver issued by WHO, which enabled the rapid increase and adoption of treatment in some of the most difficult countries to expand access. For instance, the Democratic Republic of the Congo can have a time lag of 8–12 years for innovation to reach full regulatory approval or adoption. Thomas emphasized the role of USAID, the Stop TB Partnership’s Global Drug Facility, WHO, and the Global Fund in supporting the donation program with flexibility, amplifying medical education for appropriate use, and building the infrastructure for ECG monitoring and resistance testing. Private-sector constituency partnerships have also played a large role in expanding access for TB treatment and diagnostic capability. One such partnership is with Cepheid, the company that manufactures the GeneXpert platform used in diagnosing MDR TB and determining the drug resistance profiles. Cepheid and J&J worked with the Chinese government to conduct a pilot TB case-finding study that covered 10 million persons in western provinces of China. The study found the prevalence of DR TB in that region to be about twice the country’s previous estimate and created a novel and accelerated pathway to care in China that has continued during the COVID-19 pandemic, said Thomas.
Partnerships and collaboration are also important to research efforts, Thomas noted. Since beginning the 10-year TB initiative in 2018, J&J has continued to progress in the development of bedaquiline, producing a pediatric
___________________
27 QT interval prolongation is a heartbeat irregularity in which the Q and T waves, during which heart cells repolarize after a contraction, are longer than normal. See Al-Khatib et al., 2003.
formulation and completing pediatric trials.28 J&J has advanced an early portfolio in discovery and early science, as well as pursuing licensing partnerships with other private-sector entities. He described how private-sector companies across the pharmaceutical and diagnostic industries have formed partnerships with one another in addition to collaborating with academic, government, and nonprofit organizations. For example, in 2021, J&J launched the Satellite Center for Global Health Discovery at the London School of Hygiene and Tropical Medicine. The Project to Accelerate New Treatments for Tuberculosis (PAN-TB) was established with a consortium of philanthropic, nonprofit, private-sector, and academic partners. Additionally, J&J has joined the Innovative Medicines Initiative to develop new TB antibiotics in collaboration with eight European and academic biotechnology partners.
Collaboration to Address the Challenge of Tuberculosis in South Africa
Thomas described the work J&J has carried out in conjunction with the government of South Africa, USAID, local implementing partners, nongovernmental organizations (NGOs), academic institutions, and health delivery services to comprehensively address the challenge of TB in South Africa. This effort required the creation of a novel paradigm for innovation delivery in the pharmaceutical industry. Typically, new technologies are rapidly absorbed into health systems and followed by cycles of innovation. However, in this case, the delivery model first needed to be broken down to address six different areas: access, medical education, appropriate use, data generation, patient finding, and awareness campaigns. Increasing access involved expanding regulatory access, establishing a donation program to fuel familiarity and use, and aggressive equity-based tiered pricing to ensure affordability and sustainability. Medical education was important in communicating the need for monitoring for QT prolongation with bedaquiline and audiometry testing for signs of early ototoxicity of injectable aminoglycosides, said Thomas. This was seen when South Africa led the world in the move to all-oral, noninjectable regimens for DR TB. Appropriate use refers to ensuring that the appropriate diagnostic technologies are used for DR TB patients and that patients remain on therapy to avoid early development of resistance. It also involves investment in background surveillance programs to monitor for the emergence of drug resistance in the prevalent population.
Thomas stated that data generation has been key, and that South Africa led the effort of establishing the world’s largest cohort analysis of DR TB patients. This analysis occurred twice over 5 years and showed that the survival rate for patients with XDR TB increased from 20 percent to 80 percent, resulting in a series of guideline changes, both at WHO and at the local ministry level. This illustrated the dynamic effect the introduction of
___________________
28 See https://clinicaltrials.gov/ct2/show/NCT02354014 (accessed December 31, 2021).
a new technology can have. Lastly, awareness campaigns about TB disease and the availability of less-toxic treatments that provided faster sterilization, faster cures, and better overall survival have been critically important, Thomas noted. Mass media and social media were used for above-the-brand communication starting in 2012 and are continuing today.
Lessons Learned in Collaborating Toward a TB-Free South Africa
Thomas emphasized that these efforts required collaboration at every level. Global, catalytic, capacity-building partnerships worked to understand how to best use resources and contribute capabilities, technologies, and products with organizations such as USAID. Global networks allowed implementing partners to bring innovation to the people who need it. Stop TB Partnership’s Global Drug Facility created a unique 188-pill bottle that contains a complete course of therapy with simplified regulatory language in four languages. This design enabled therapy availability in 140 countries through a regulatory waiver and a regulatory approval mechanism that accelerated access to patients. Additionally, the Global Drug Facility established an agreement to rapidly decrease the lowest pricing tier to ensure access and market penetration. An innovation in both access and pricing, this mechanism secured growth to over 100,000 treatments in 1 year.
Thomas pointed out that South Africa demonstrated what can be accomplished by using political will, a strong medical system willing to advance the standards of care, and broad engagement with private-sector implementing partners. Pharmaceutical companies cannot accomplish such work on their own; they need the help of other sectors. Thomas called for a needs-based approach to address issues in medical education; patient and consumer education; consumer-centered design; and simplification in the testing, diagnosis, and care pathway, as well as other health needs such as adequate nutrition that affects whether a medical intervention will have a successful outcome. Noting the years required to conduct TB trials, Thomas highlighted the need for the generation of reliable real-world evidence. Data on an intervention’s effect on disease relapse after 100 weeks of treatment inherently calls for a long follow-up period. He suggested that the use of credible real-world cohorts could generate useful interim data. Successful regional efforts, such as those from South Africa, should be used globally. The Global Fund and J&J are currently conducting case-finding pilots in Indonesia and the Philippines. The company is forming similar partnerships in Russia and the Commonwealth of Independent States (CIS), and they are partnering with NGOs in China, India, and other parts of Southeast Asia. Building on what they learned from the MTV Staying Alive Foundation, J&J is carrying out a mass media campaign on social media and mainstream broadcast media in India to destigmatize TB and demonstrate the improvements in outcomes that are possible.
Implementing a New Treatment Regimen for Drug-Resistant Tuberculosis: Lessons Learned
Presented by Norbert Ndjeka, National Department of Health, South Africa
Ndjeka discussed the planning and implementation of a new shorter treatment regimen for DR TB—bedaquiline—in South Africa, with a focus on the factors that contributed to its success as well as the challenges that were encountered.
Drug-Resistant Tuberculosis in South Africa and the Effect of COVID-19
South Africa has one of the highest burdens of DR TB in the world, said Ndjeka. More than 13,000 cases of rifampicin-resistant (RR TB) and MDR TB were diagnosed in the country in 2019. During the same year, the estimated global incidence of RR TB and MDR TB was about 465,000 (WHO, 2020). Moreover, South Africa also has a high burden of HIV. Ndjeka noted that three-quarters of people with MDR TB in the country are also living with HIV, putting substantial pressure on systems of care for TB. However, despite South Africa’s burden of DR TB, it outperforms the global rate for DR TB treatment initiation by almost twofold (WHO, 2020). In 2019, more than 9,000 people in the country were initiated on treatment for RR TB and MDR TB—including 406 cases of XDR TB29—representing 70 percent of all DR TB cases nationwide that year. Globally, about 177,000 patients began treatment for RR TB and MDR TB in 2019, representing around 38 percent of MDR TB cases.
Success rates for the treatment of DR TB in South Africa are also relatively high and have recently exceeded the global averages for both MDR TB and XDR TB (WHO, 2020). In 2017, the success rate for treatment of RR TB and MDR TB was approximately 60 percent in South Africa, surpassing the global rate of about 57 percent. The success rate for patients started on second-line treatment for XDR TB in 2016 in South Africa and worldwide were 60 percent and 47 percent, respectively.
Unfortunately, DR TB case-finding rates in South Africa have substantially declined since the onset of the COVID-19 pandemic, said Ndjeka. Between 2019 and 2020, the number of DR TB cases diagnosed dropped by 27 percent (2019: 11,274 cases; 2020: 8,229 cases), and this trend is predicted to continue through 2021. He posited that the nationwide lock-
___________________
29 XDR TB is a type of MDR TB that is resistant to isoniazid and rifampicin, plus any fluoroquinolone and at least one of three injectable second-line drugs—amikacin, kanamycin, and/or capreomycin. See https://www.cdc.gov/tb/publications/factsheets/drtb/xdrtb.htm (accessed December 31, 2021).
downs implemented to control the pandemic have been a major contributing factor, but more research will be needed to fully understand the effect of the pandemic on the country’s TB control program.
Planning and Implementing the Bedaquiline Clinical Access Programme in South Africa
Ndjeka provided an overview of the planning and implementation of the Bedaquiline Clinical Access Program in South Africa between 2011 and 2015, highlighting components that could potentially inform the rollout of novel shorter treatment regimens in other settings (Ndjeka et al., 2020). The first step was to establish a collaborative public–private working group that included representation from the national government, J&J, NGOs, and academia. This consortium led efforts to develop study protocols, obtain university ethics approval, engage with the medical product regulatory authority of South Africa (the Medicines Control Council), deliver training in both leadership and good clinical practice, engage with stakeholders across multiple sectors, and communicate with the managers of provincial TB programs. In addition to in-country work, the consortium also engaged with similar working groups around the world to better understand how to effectively roll out a new therapeutic and garner the necessary support. After developing the Bedaquiline Clinical Access Program, it was first implemented at five clinical sites prior to wider scale-up to additional sites.
Ndjeka remarked that numerous stakeholders and sectors are involved in implementing a new DR TB treatment regimen, such as the national and provincial TB programs, regulatory and ethics bodies, medicine procurement bodies, laboratory services, data management, and various national and international partners. Thus, a strong champion is needed to harmonize and lead the collaborative effort in addition to guidance from an expert committee. For example, because provinces in South Africa have a level of autonomy similar to U.S. states, gaining provincial-level buy-in for the bedaquiline rollout was also important.
Training of health care workers was central to the successful implementation of bedaquiline in South Africa, said Ndjeka. Treatment guidelines had to be revised to accommodate the new therapeutic regimens. Tools also needed to be aligned with those revisions and with the assessment of training needs. He noted that South Africa did not have sufficient resources to deliver trainings and obtain tools—for example, those used to detect adverse events, such as ECG and audiometers. However, various partnerships contributed funding and resources to provide training, acquire tools, and monitor training and results on the ground.
Robust cross-sector coordination across the government, academia, pharmaceutical sector, and finance sectors was another pillar of the rollout
of bedaquiline, said Ndjeka. Strong political commitment from the national government—driven by strong engagement by the minister of health—was fundamental in gaining public buy-in and garnering resources to support the effort. The pharmaceutical sector provided support in procurement of medicines and other facets of supply chain management, while NGOs and academia provided technical support for the decentralized rollout of bedaquiline to provinces and districts.
Ndjeka emphasized that partnerships were critical in the implementation process. These partnerships facilitated the establishment of a broad network for diagnosing and treating MDR TB patients, as well as managing adverse events. For instance, the extent to which ototoxicity is an issue in managing MDR TB patients was initially underestimated, but this was better understood after most of the implementation sites were provided with portable audiometers. Partners also provided resources and support to improve electronic recording and reporting systems and to train health care workers on data and treatment management.
Factors Contributing to Success in Implementation
Ndjeka outlined several factors that contributed to the success in implementing the Bedaquiline Clinical Access Program. He extolled the benefits of a functional national committee bolstered by province-level clinical and programmatic subteams, as well as effective coordination between the National TB Program and the expert committee. Cooperation with the regulatory authority and other government sectors helped to streamline amendments to study protocols, for example. Initially the program was able to acquire the first round of doses through donation from J&J but later began purchasing doses directly. Developing a functional data system and effective laboratory services contributed to more accurate diagnostics, recording, reporting, and monitoring. The program also benefited from the availability of funds to convene various events to deliver trainings and share best practices. He highlighted a set of major lessons learned during the bedaquiline rollout that could be applicable to similar efforts in other settings (see Box 4-2).
Challenges Encountered in Implementation
Various challenges were encountered during the bedaquiline rollout in South Africa, said Ndjeka. At the early stages, it was challenging to secure buy-in from key stakeholders and manage their resistance to change. Obtaining regulatory authority for a new therapeutic is a lengthy process—even if only an amendment or new protocol is needed—that can delay implementation. Quantification and stock management pose additional challenges. For instance, scaling up bedaquiline in South Africa required running down and/-
or writing off the large existing stock of existing drugs such as kanamycin. Moreover, it is challenging to ensure that the new regimen is being used universally in the field and to trace patients who may have been unnecessarily initiated on older injectable regimens. He also noted that the COVID-19 lockdown reduced the numbers of patients attending and presenting for care, and it may be difficult to re-engage them in treatment.
Effect of Bedaquiline Implementation
Ndjeka presented data on the DR TB treatment initiation, outcomes, and success rates in South Africa before and after the implementation of bedaquiline.30 Between March 2013 and March 2015, 1 percent of all DR TB patients on treatment received the bedaquiline regimen (200/24,688 patients). Between March 2015 and December 2015, that proportion had risen to 12 percent (1,239/10,001) and by 2016, it had grown to 25 percent (2,973/11,994 patients). In 2017, the proportion of DR TB patients on treatment who were receiving the bedaquiline regimen reached 77 percent (8,240/10,754 patients).
DR TB treatment outcomes in South Africa improved markedly between 2010 and 2018 after the introduction of bedaquiline, particu-
___________________
30 Bedaquiline received approval from the U.S. Food and Drug Administration in December 2012: https://www.jnj.com/media-center/press-releases/fda-grants-accelerated-approval-for-sirturo-bedaquiline-as-part-of-combination-therapy-to-treat-adults-with-pulmonary-multi-drug-resistant-tuberculosis (accessed December 31, 2021).
larly for patients with XDR TB. During that period, the treatment success rate for patients with XDR TB increased from 10 percent to 61 percent, while the death rate decreased from 49 percent to 21 percent. For MDR TB patients, the treatment success rate rose from 51 percent to 65 percent and the death rate declined slightly, from 19 percent to 17 percent. Among all patients initiated on treatment for DR TB in South Africa in 2017, a bedaquiline-containing regimen had a treatment success rate of 70 percent and death rate of 13 percent. In contrast, a non–bedaquiline-containing regimen (i.e., an older regimen consisting of injectable drugs) in the same cohort had a treatment success rate of 53 percent and a death rate of 23 percent. Ndjeka described these results as encouraging and catalytic for continued improvement.31
Bringing Innovation to the Development of New Transformative Tuberculosis Regimens
Presented by David Hermann, Bill & Melinda Gates Foundation
Hermann highlighted progress toward a shorter, simpler, safer pan-TB regimen—that is, a regimen for treating multiple forms of TB. He highlighted the R&D activities for TB over the past decade that are spurring progress toward a shorter, simpler, safer pan-TB regimen, which included the first approvals for several new TB drugs—bedaquiline, delamanid, and pretomanid—in a number of years. In 2020, the TBTC Study 31/A5349 and TB Alliance’s Nix-TB bedaquiline-pretomanid-linezolid trial indicated that shortened TB course treatments are feasible. He emphasized the importance of this milestone, noting that years ago, regimen shortening was considered impossible because of the slow-growing nature of the TB bacteria. Moreover, adequate substrate for the R&D pipeline has been established and the new candidates bedaquiline, delamanid, pretomanid, sutezolid, and a decaprenylphosphoryl-ß-d-ribose-2'-oxidase (DprE1) inhibitor being developed by Otsuka Pharmaceutical may lead to the first generation of pan-TB regimens. At the same time, the COVID-19 pandemic has caused R&D disruptions such as closure of laboratories and clinics, which paused discovery research programs and clinical trial enrollment. While much TB research had resumed by the time of this workshop, the previous momentum has not yet been fully regained, said Hermann.
___________________
31 Bedaquiline, though successful, has experienced slow rollout in sub-Saharan Africa owing to limited funding.
Optimal Pan-Tuberculosis Target Regimen Profile
Achieving a considerable decrease in TB incidence will involve transformative regimens that offer substantive improvements and help minimize the efficacy–effectiveness gap.32 Although the results in clinical trials using the standard of care are promising, numerous factors create an efficacy–effectiveness gap, including tolerability, long duration of regimens, and the need for drug-susceptibility testing. Hermann explained that the target regimen profile (TRP) features a pan-TB product that does not require drug-susceptibility testing, has a shortened duration of 2 months or less, and is well-tolerated and affordable (see Table 4-1). Coupling this TRP with an improved point-of-care diagnostic would enable a pivot toward a “test and treat” paradigm in which a patient could be rapidly diagnosed and provided with pills in the same visit, leading to a high cure rate. He acknowledged the difficulty in fully achieving this scenario, and suggested that regimens that fall short of this aspirational goal could still be highly effective in the field. For example, the Nix-TB bedaquiline-pretomanid-linezolid regimen showed an efficacy rate of over 90 percent in the hardest-to-treat patients.
The goal of meeting the pan-TB TRP faces a number of challenges, Hermann noted. Although the portfolio of TB drugs is more vibrant and diverse in size and scope than ever before, antimicrobial candidates remain too few in number to achieve the TRP. More work is needed in discovery to identify novel drug targets to create more effective treatment combinations. Additionally, translational science is limited, and innovation is needed in biomarkers, dose selection, and efficient experimental design. Furthermore, quantitative translational modeling could be used. Continuing to establish connections between nonclinical tools, pharmacometrics modeling, and success in the clinic, as described by Nahid earlier from the experience with TBTC Study 31/A5349, would be beneficial. The TB toolbox is fairly extensive, and as more evaluations of regimens in the clinic are conducted, the tools that are essential in driving decision making can be identified. Hermann stated that no single organization will own the best candidates to build the most effective regimen, and therefore collaboration in TB R&D is critical. In working toward an aspirational TRP, the perfect should not be made the enemy of the good, he said. The focus should not be on finding a perfect nonclinical package that might translate into a regimen that meets TRP. Instead, good regimens with the potential to meet TRP should be moved into clinics in order to collect clinical outcomes data and translate this back to nonclinical results, said Hermann.
___________________
32 The efficacy–effectiveness gap refers to the difference in observed outcomes in a controlled trial and those observed in clinical practice.
TABLE 4-1 Optimal Pan-Tuberculosis Target Regimen Profile
| Target Regimen Profile Criteria | Hypotheses |
|---|---|
| Pan-tuberculosis | No drug-susceptibility testing required |
| Fewer patients lost to the system after diagnosis | |
| Shorter (<2–3 months) | Shorter → Improves adherence → Improves outcome → Less transmission |
| Safe and well-tolerated | No baseline or ongoing safety monitoring |
| Well-tolerated → Improves adherence | |
| Simpler | All oral; once-daily dosing, no drug–drug interactions to manage |
| Efficacious | Short, forgiving regimen noninferior to standard of care to minimize the efficacy–effectiveness gap |
| Affordable | Low barrier to uptake |
SOURCE: David Hermann workshop presentation, September 15, 2021.
Innovation in Mycobacterium Tuberculosis Antimicrobial Discovery
Innovation is currently taking place in the area of Mycobacterium tuberculosis antimicrobial discovery, Hermann noted. For instance, clustered, regularly interspaced short palindromic repeats—known as CRISPR—interference was used as a platform to aid in lead target generation (Bosch et al., 2021). This platform was designed to allow titration of gene expression from full strength to virtually eliminated in a high-throughput in vitro system. This graded gene expression allows for measurement of bacterial fitness in vitro. Graphing the relationship between the magnitude of gene inhibition and cell fitness demonstrates that for some genes, a slight lowering in expression can have a profound effect on bacterial fitness, while others can be virtually knocked out with very little effect on fitness of the bacteria. The data derived from this system are used to create a vulnerability index for the potential target genes. Currently, the vulnerability index is being used by the TB Drug Accelerator (TBDA), a collaboration that focuses on drug discovery, to prioritize targets for TB discovery efforts. For example, transfer RNA synthetases and the DNA polymerase dnaE1 have distinguished themselves from other targets and are therefore receiving additional research focus, Hermann shared.
Innovation in Dose Selection
Hermann remarked that effective dosing is essential for any antibiotic, and particularly for a combination of drugs to treat TB. This disease results in complex, heterogeneous pathology; therefore, estimating the human dose across different sites of infection is challenging. Current research is generat-
ing pharmacokinetic and pharmacodynamic data across different sites of infection—plasma, lung, cell lesion, caseous lesion, cavity wall, and lymph node—in a rabbit model (Lakshminarayana et al., 2015). These data are used to estimate the human dose needed to provide lesion coverage, which is more difficult for drug penetration than other sites of infection. Hermann explained that if researchers focused on the plasma concentration to calculate the total dosing, appropriate lesion coverage would only be provided for a fraction of the overall dosing interval. Therefore, data on various infection sites are being used in the development of new TB drugs.
Collaboration is a key component in the R&D landscape. The European Regimen Accelerator for Tuberculosis program from the Innovative Medicines Initiative (IMI) is focused on early, preclinical, and phase 1 drug development, said Hermann. A company can set forth a new molecule, and the IMI will help drive it through the characterization of the early asset. Further downstream, IMI’s UNITE4TB will then carry the work through phase 2. He noted that the Bill & Melinda Gates Foundation also sponsors similar collaborations through the TBDA, which has been active for 10 years and is a lead identification and optimization platform (Aldridge et al., 2021). Also downstream, the PAN-TB collaboration is composed of the TB Alliance, GlaxoSmithKline, J&J, Evotech, Otsuka, and the Gates Medical Research Institute. Hermann remarked that these collaborations drive the portfolio forward, and that data sharing is fundamental to this effort. Therefore, the Bill & Melinda Gates Foundation has embedded a basic tenet of data sharing in their investments that applies across organizations within a collaboration and across collaborations. Thus, the IMI collaborations work closely with PAN-TB and TBDA. Furthermore, the Critical Path Institute is a mechanism for sharing data with external partners.
Collaborating to Drive Innovation
Hermann highlighted innovation born of these collaborations, including work from PAN-TB on designing phase 2 trials to de-risk phase 3 trials. Hermann explained that drug developers may be wary of entering a 500-patient study with little additional clinical data. In one of the efforts to address this, PAN-TB is examining a stage design for a phase 2 trial through a pilot evaluation that studies the safety, tolerability, and trajectory of response for various TB regimens. This is a duration-finding study where a new regimen is dosed at different durations and the relationship between the regimen duration and outcomes is examined.33 The study compares the trajectory
___________________
33 Hermann noted that this innovative design builds off the work of many others, including Michael Hoelscher, German Center for Infection Research; the European and Developing Countries Clinical Trials Partnership; and Patrick Phillips and Rada Savic, Center for Tuberculosis at the University of California, San Francisco, among others.
of response for the standard of care with the trajectory for new regimens. Should a new regimen shorten the time in which the response trajectory moves from unfavorable to favorable status, these data can be used to de-risk the next stage of investment.
While much growth and progress have occurred in TB R&D, it has been slowed by the COVID-19 pandemic, said Hermann. However, the TB community is encouraged by current innovation and the potential PAN-TB studies that are staged to launch. The substrate for potentially effective regimens has been established and will continue to grow. Hermann remarked that this research warrants global engagement and funding comparable to that given to COVID-19.
Economic Analysis of Novel Tuberculosis Treatment Regimens
Presented by Anna Vassall, London School of Hygiene & Tropical Medicine
Vassall explored the value of conducting context-specific economic analyses of novel TB treatment regimens to inform future program design and investment. She explained that in the TB field, the conventional approach adopted by researchers is to perform economic analyses after positive trial results—such as those from TBTC Study 31/A5349, described by Nahid—with the aims of disseminating the results and convincing policy makers that the regimen is not only clinically effective, but also cost-effective, to promote funding and uptake. She offered an alternative perspective from a stakeholder who will fund the scale-up of a novel TB treatment regimen—particularly in low- and middle-income countries. Typically, the payer’s goals are to use funding to (1) improve health-sector equity and efficiency, (2) strengthen the systems that are being implemented to inform priority setting within health sectors, and (3) conduct sectoral- and population-level economic analyses, which may be slightly different than economic analysis of an individual trial. Given the consistent lack of funding for TB over the past 20 to 30 years, understanding how that sectoral process works is pivotal to designing economic analyses that are more aligned with goals of payers, examining why uptake of a new regimen may be limited and potentially informing intervention design. Vassal explored how these systems for setting national priorities are evolving, with a focus on national-level payers and development partners—and reflected upon why previously effective TB interventions have not been funded to scale. She also discussed the specific case of shortened and universal TB regimens and aspects of the analyses that may be particularly promising.
Evolution of National Priority-Setting Systems Toward National Benefits Packages
Vassall provided an overview of the evolution of the systems for setting national priorities over the past decade, during which time many countries have created national strategic health plans that typically span from 3 to 5 years. Traditionally, people working in TB have focused on two strategies: garnering funding for new TB regimens within those national strategic plans sufficient for scaling up to high levels of coverage, and obtaining development assistance through various types of funding applications. However, the focus has shifted over the past 5 years toward universal health care (UHC) benefit packages, which involves examining the services that health sectors provide and defining the packages of care that should be publicly funded. This movement toward UHC benefit packages frames efforts to strengthen the health sector less in terms of how to plan finances for scale-up within 3 to 5 years and more in terms of whether a given intervention should be publicly funded at all. A component of this approach is to use a formal process of health technology assessment to evaluate new interventions or technologies in a way that extends beyond traditional guideline-type evaluation processes to consider cost-effectiveness within a local context. Vassall noted that several countries with high TB burdens have been embarking on this process of developing UHC benefits packages (e.g., Pakistan, India, Ethiopia) and others have already initiated health technology assessments around the rollout of national health insurance (e.g., China, India, South Africa, Ethiopia, Ghana, Kenya).
Inclusion of Tuberculosis Treatment in National Benefits Packages
As an example of how new TB treatment regimens can fit within national benefits packages, Vassall described cost-effectiveness analyses conducted in Ethiopia and Pakistan to inform which interventions would be included in their essential health packages. In Ethiopia, 159 health interventions were analyzed to determine which would be included as public-sector provisions (Eregata et al., 2021). Although various TB interventions analyzed were found to be less cost-effective than reproductive maternal and child health interventions and interventions for other infectious diseases, such as antiretroviral therapy for HIV, Ethiopia nonetheless decided to include most of the TB interventions in their intentionally ambitious package. However, the resulting package is unaffordable in many respects, necessitating priority setting that may delay the immediate inclusion of those TB interventions in practice.
Pakistan has adopted a more conservative approach to the inclusion of TB interventions in its benefits package by attempting to plan within its relatively limited fiscal space—the amount of financing that is actually avail-
able for the government to spend in the coming years—of just $8 dollars per capita at the district level to deliver an entire range of health services.34,35 According to Vassall, a cost-effectiveness analysis of the district-level Essential Package Health Services in Pakistan found that the current treatment for DS TB is ranked 11th at $17 per disability-adjusted life year (DALY) averted. Even if that regimen becomes slightly more expensive, it is still affordable within the current fiscal space. In contrast, the current treatment for DR TB—which costs $757 per DALY averted—could only be afforded if there were increased expenditure. Vassall noted that from a human rights perspective, TB treatment should be considered in the context of other interventions. For example, the COVID-19 vaccine, at $6 per DALY averted, ranks 72nd in terms of cost-effectiveness and is considered affordable within Pakistan’s current fiscal space. In a limited fiscal space, there is a trade-off between including a greater number of TB interventions in benefits packages regardless of their cost-effectiveness—and consequently achieving low coverage of all of them—versus including a smaller number of only the most cost-effective interventions and achieving full coverage.
Economic Assessment of Shortened Tuberculosis Treatment Regimens
Most analyses examining noninferior DS TB and DR TB regimens have found shortened regimens to be either cost saving or highly cost-effective at prices of around $1 to $5 per day compared to standard of care, said Vassall.36 A caveat is that these analyses typically presume that DR TB treatment is fully financed, yet it is unclear whether even shorter regimens for DR TB would fit within the available fiscal space in many countries. Moreover, most of these modeling studies are based on limited direct effect on outcomes and trends transmission (i.e., 1–4 percent incidence). However, these savings could create considerably more potential for indirect health improvement for TB patients than if that funding were spent elsewhere. A moderately priced 4-week DS TB regimen would yield a 60 percent reduction in costs, both to health services and to patients. In absolute terms, the gains mainly accrue for households of patients with DS TB, because the cost per patient is much greater than the cost incurred by health services for each case of DS TB.
Such cost-efficiency gains to health systems are highly dependent upon context-specific factors, such as guideline adherence, the cost of current
___________________
34 Vassall noted that prior to the COVID-19 pandemic, it was estimated that this amount would grow maximally to $12 dollars per capita, but given the fiscal situation in Pakistan and the effects of the pandemic, there is unlikely to be much growth from $8 dollars per capita.
35 Costs in this analysis are given in U.S. dollars.
36 Costs in this analysis are given in U.S. dollars.
delivery, and the baseline level of default. She noted that new regimens tend to yield fewer benefits when they are implemented within TB care systems that are already efficient compared with when implemented within less efficient systems. Additionally, the baseline level of treatment default can also underlie large differences in both outcome and costs. For example, the current delivery in Bangladesh was already cost-efficient and community based, so the cost savings for the community appear dampened compared with other settings. The experience in South Africa also demonstrates that guideline adherence—or the extent to which treatment is observed by health care workers—will determine the amount of treatment cost savings.
Pricing for a Future Universal Drug Regimen
Vassall and colleagues have looked ahead to 2030 to examine the pricing and value of a shortened universal drug regimen for TB when it eventually comes to market.37 They considered the effect of changes in the size of the future fiscal space, the uptake of health technology assessments, and implementation of national strategic plans in the current planning and TB programs to estimate the potential revenues that would occur when those drugs were introduced. The price of the drug was estimated as the maximum price that would still ensure that the new TB regimen would fall into the package at that time, given the fiscal space available; that price was used to estimate revenues.
The modeling for India found that—depending upon the introduction of vaccines—higher revenues would be generated around treatment if the program performs well and creates more access to TB services, as intended over the next 10 years. Researchers also looked at the gain or loss in terms of price if the program does not achieve that level of performance—meaning, how the maximum price that could be charged would be affected by different regimen characteristics—and estimated the following maximum regimen prices (in U.S. dollars):
- Universal drug regimen, no drug-susceptibility testing requirement, 2-month duration, but laboratory monitoring required: $485.86.
- Two-month duration, no laboratory monitoring, but not universal (XDR not eligible), and drug-susceptibility testing required: $376.79.
- Universal drug regimen, no drug-susceptibility testing requirement, no laboratory monitoring, but 6-month duration: $112.47.
___________________
37 This is ongoing, unpublished work from Vassall and colleagues.
Effect of Tuberculosis on Household Economic Status
The greatest economic gains from improvements in TB treatment and care are likely to be experienced by patients and their households in terms of protection from catastrophic expenditure and poverty, said Vassall. The effect of TB on the economic status of households is now well established. For instance, a modeling study estimated how many cases of poverty would be averted in India and South Africa by improvements in different types of TB treatments, finding a substantial increase in the number of households that would be pulled out of poverty (Verguet et al., 2017). However, she acknowledged that such arguments from the economic perspective do not necessarily appeal to the health-sector payer. In fact, there is an ongoing debate within health economics over whether health sectors should consider this type of information when allocating funding. To address this issue, Vassall and colleagues are exploring how to use economic evidence to make the case for investing in TB to ministries of finance and other non-health ministries who may be more interested in achieving poverty-reduction goals than specific TB-related health goals. The approach will vary by setting, but researchers are looking at how to integrate different types of modeling (e.g., return on investment, computable general equilibrium economic modeling) to effectively engage with stakeholders within ministries of finance.
Strategies for Using Economic Analyses of New Tuberculosis Regimens
Vassall highlighted several strategies for using economic analyses of new TB regimens to inform program design and garner investment in TB treatments and care. Cost-effectiveness analyses have long been used informally in this area, but formal cost-effective evidence is increasingly required. This work would benefit from a more comprehensive understanding of where TB currently sits, in terms of comparative efficiency, within the health sectors and how that varies by context and setting. Specifically, it is important to understand the cost gains that could be achieved with shortened TB regimens and in which countries those regimens would have the greatest effect. She noted that for DR TB treatments, those cost gains may enable scale-up, although that is likely to be different for DS TB treatments. A clear economic case can be made in terms of poverty reduction, but more work remains to elucidate how to make strong arguments to transform that evidence into investment by policy makers. She also underscored the value of using evidence brokers to inform investments and of empowering stakeholders working on the clinical and programmatic sides to optimize the use of economic evidence.
REFLECTIONS AND DISCUSSION ON CRITICAL ELEMENTS FOR IMPLEMENTATION
Centering the Patient’s Experience and Using Available Data
Presented by Ezra Shimeles Tessera, USAID and John Snow, Inc.
Tessera offered reflections that focused on patient-centered implications of advancements in TB treatment and care. He also presented an overview of a standardized monitoring and evaluation framework developed by USAID to help track a country’s progress in ending the TB epidemic.
Improving Individual Lives Through Better Tuberculosis Care: Clinical Vignettes
Tessera presented two clinical vignettes drawn from his early days of clinical practice to explore the profound personal consequences of improving TB care. As a young clinician in the 1990s, Tessera encountered the first patient with symptoms suggestive of TB at a rural health center. Tessera diagnosed the patient in accordance with the national protocol; the next step was to discuss the test results with the patient, reassure him, and prepare him for the inconvenience of long-term TB treatment. However, Tessera was surprised by the patient’s unexpected reaction, which was to express happiness upon learning of the diagnosis. When Tessera explained that the best treatment option for the patient would be a long-term regimen—but one that did not require an injection every 2 months—the patient was even happier and Tessera even more mystified. Eventually, he learned that the patient was happy because TB was the only disease for which treatment was provided free of charge and, by the time he was diagnosed, he had already spent so much of his limited resources that he could not afford to incur any further treatment costs. Furthermore, he was happy that he would not have to come into a facility to receive a painful streptomycin injection every 2 months, which he would have to pay for at a pharmacy out of pocket and was often out of stock. In contrast, he would receive the 8-month all-oral regimen at no cost.
Tessera remarked that it was beneficial for this patient to feel happy about embarking upon a long-term oral TB regimen, but questioned whether the patient’s happiness was genuine or actually rooted in frustration—that is, could this patient have received better care? For instance, the patient could have been provided with good-quality vaccines, preventive therapy, infection control, and other key interventions against TB. Early detection could have averted years of financial burden that the disease placed upon him, and a
shorter treatment regimen—had it been available—could have allowed the patient to return to work more quickly. A better data system could have also contributed to a higher standard of care. Those interventions were not available at that time in that setting, but advances in TB care are moving in the direction of providing high-quality care that can provide patients with genuine cause for happiness.
Tessera’s second vignette focused on a patient with MDR TB he encountered in 2011, at an event that invited the first cohort of MDR TB patients who successfully completed treatment to come together and share their personal stories. Prior to developing MDR TB, this patient was wealthy by his community standards and ran his own public transport facility, driving people from different locations. He developed symptoms but was unable to find care at facilities he visited. As his clinical condition deteriorated, he was forced to sell his car—the sole source of income for his family—and ultimately had to leave his home, after which he was unable to work and pay his rent. When he was ultimately diagnosed with MDR TB, relatively little was known about the disease, and neither clinicians in the health system nor local traditional treatments could help him. In yet another profound loss, his wife and family had to leave him owing to the burden upon his wife. Finally, he was diagnosed with MDR TB and was among the first to receive treatment when it was initiated in his country; he eventually recovered and began to rebuild his life. He told the group that he now felt happy because he was still alive, but it was too late to recover from the financial and personal ruin that the disease had wrought upon him. This patient’s story illustrates the potentially disastrous consequences of TB not just at the individual level, but at the family and community levels as well. For people with TB, the effect of the disease could be mitigated and their lives could be profoundly changed by good-quality prevention, early detection, shorter regimens, and stronger systems of care. The advancements and innovations in TB care to date are promising, said Tessera, adding “We still have a long way to go.”
Performance-Based Monitoring and Evaluation Framework
Data issues represent major barriers to improving systems for TB treatment and care, said Tessera. He introduced USAID’s Performance-Based Monitoring and Evaluation Framework (PBMEF),38 which is the cornerstone of the organization’s efforts to ensure the effective accountability of investments in TB at the global, regional, and country levels and accelerate progress to end the TB epidemic (TB DIAH, 2021). The PBMEF is designed to
___________________
38 For more information on PBMEF, visit https://www.tbdiah.org/resource-library/pbmef (accessed February 8, 2022).
provide a systematic way to use the available data to track a country’s progress toward major global TB targets, such as USAID strategy targets and UN high-level targets (see Figure 4-4). To help contextualize a country’s status on key TB indicators, the PBMEF provides (1) a set of standardized indicators to measure essential TB program outputs and outcomes; (2) details on the performance of TB programs in specific technical areas (e.g., diagnosis, treatment, TB/HIV, private sector), and (3) treatment cascades and patient pathways for identifying gaps and needed improvements. A benefit is that using the framework does not require any substantial investment in collecting additional data; the available data are simply repackaged and used to monitor programs and inform decision making.
Core Indicators
The framework includes 10 core indicators (see Box 4-3) that capture fundamental elements of USAID’s TB strategy—Reach, Cure, Prevent, and Sustain—and more than 180 extended indicators that fall under 14 technical

NOTE: WHO = World Health Organization.
SOURCE: Presented by Ezra Shimeles Tessera on September 15, 2021.
categories. For instance, under the Reach domain are indicators that pertain to TB case-finding activities; under Cure are indicators related to treatment success; under Prevent are indicators tracking progress in infection control and delivering TB preventive therapy; and under Sustain are indicators covering financing, policies, guidelines, and governance. The PBMEF is a living document that can be continuously updated, harmonized, and adapted to individual country contexts and needs, he added. The core indicators are collected and used for monitoring, informing programmatic decision making, and facilitating collaboration with academics, researchers, and other technical partners.
Disease Cascade Analyses
The data collected using PBMEF indicators are also used to construct cascade analyses, said Tessera. For instance, USAID researchers have developed an HIV/TB infection cascade designed to help identify missing cases and—more importantly—to understand why they were missed in order to improve the system. If the core indicators are not sufficient to provide that insight, then extended indicators can contribute to a more in-depth and holistic analysis of the situation. Similarly, USAID has developed a cascade for DS TB disease that begins with an assessment of TB incidence in a population and then flows down through the numbers of individuals who (1) are eligible for screening, (2) have been screened, (3) have been evaluated, (4) have accessed a WHO-recommended rapid diagnostic test, (5) have bacteriologically confirmed pulmonary TB, (6) have accessed a drug-susceptibility
test, (7) have notified DS TB, (8) have started TB treatment, and (9) have been successfully treated.
Framing Tuberculosis as a Global Health Emergency
Presented by Richard Chaisson, Johns Hopkins University School of Medicine
Chaisson’s presentation focused on the need to frame TB as a global health emergency. He noted that WHO declared TB a global public health emergency in 1993 (Nakajima, 1993) and declared COVID-19 a public health emergency of international concern on January 30, 2020.39 Those declarations are the sole similarity between the global responses to these global health emergencies. The COVID-19 response from the scientific, public health, medical, and pharmaceutical communities has been spectacular in developing diagnostics, therapeutics, and vaccines at a dizzying pace, he remarked. The resulting armamentarium of tools provides the means to control and end the COVID-19 pandemic. Although the effective and equitable deployment of these tools remains a monumental challenge, science clearly answered the call of this global crisis. In contrast, TB has never been treated as a true global health emergency. This may be attributable to TB’s long-standing history, the absence of a rapid escalation in case numbers, and the golden age of discovery in the twentieth century that has come and gone. However, the worldwide distribution of TB is just as great as that of COVID-19. Chaisson stated that TB’s effects on health and survival are similarly dire, and the need for a rapid, coordinated, and adequately resourced scientific response is equally evident.
Treating an epidemic as an emergency generates substantive differences in response, as demonstrated by the response to COVID-19, stated Chaisson. The development of diagnostic tests for COVID-19 proceeded at near miraculous speed. Most academic medical centers in the United States and Europe established their own in-house diagnostic polymerase chain reaction tests within weeks. Referencing his work on a COVID-19 treatment trial with Novartis and the AIDS Clinical Trials Group funded by NIH, he described how the U.S. Food and Drug Administration (FDA) review, institutional review board (IRB) approval, and clinical launch of a phase 3 randomized, double-blind, placebo-controlled clinical trial for hydroxychloroquine
___________________
39 See Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV), https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed January 1, 2022).
and azithromycin all took place within 6 weeks. COVID-19 vaccines went from sequence to phase 1 in less than 8 weeks, moved to phase 3 about 4 months later, and were approved by the FDA within 11 months. Institutions treated COVID-19 as a crisis and operated in crisis mode, said Chaisson. For example, the IRB at Johns Hopkins University met 5 days per week to review COVID-19 protocols. NIH issued supplemental awards within 2 weeks, and $500 million was invested in diagnostics in less than 2 months.
Chaisson described TB vaccines as far more challenging to develop than those for COVID-19. In the absence of adequate investment and an emergency response, the pace of implementation of TB trials is slow. For instance, Johns Hopkins University is currently conducting a suite of studies funded by Unitaid to promote broader implementation of TB preventive therapy with short-course regimens. Chaisson recalled priorities outlined earlier in the workshop by Matteo Zignol, head of the Prevention, Care, and Innovation Unit of the Global TB Programme at WHO, noting that regulatory processes are delaying (1) trials on interactions of rifapentine and antiretroviral drugs in pregnant women and children infected with HIV, (2) implementation in high-burden settings, and (3) the use of short-course regimens in populations that have not yet been studied, such as household contacts. Review by the WHO Ethics Committee takes an average of 10 to 12 months. National IRBs in Brazil and India take up to a year. Although the United States conducts review processes in less time, the overall timeline for conducting TB research remains long. Treatment for TB is lengthy and endpoints are slow to accrue, leading to time-intensive TB clinical trials. However, TB studies are prolonged unnecessarily by a lengthy administrative and regulatory review process, he stated.
The problem is greater than the mechanics of any individual agency or body, Chaisson noted. Part of the issue is a lack of urgency around TB; the response to COVID-19 illustrates that when a disease is treated as an emergency, processes move rapidly. An example of the slow processes delaying TB trials is the 6-month time frame for an IRB review of a protocol amendment to take place. In addition, the research infrastructure—from investigators to IRBs to regulatory agencies—is underfunded and undersupported, said Chaisson. Just as individual research is underfunded, so too is the machinery of clinical research. The WHO Ethics Committee requires a year to review protocols owing to inadequate staffing and a reliance on volunteer reviewers who have other full-time jobs to perform. The trials for COVID-19 therapeutics and vaccines demonstrated that it is possible to conduct game-changing trials in record time without cutting corners when the situation is treated as an emergency and enormous human and financial resources are allocated to the emergency.
A twofold approach can be used to address regulatory issues hampering TB innovation, Chaisson stated. First, more investment is needed in regulatory and research ethics and administrative aspects of clinical research and clinical trials to ensure that requirements do not stifle innovative research.
Second, regulatory review could be streamlined to eliminate unnecessary processes that add delay while doing little to protect study participants or communities. For example, local institutions have a legal responsibility to protect research participants as they carry out IRB reviews, yet a WHO review is also conducted, adding little value to the process while causing substantial delays, said Chaisson. Advances in TB diagnosis, treatment, and prevention that will translate into progress in TB elimination could be pursued as an emergency. He stated that unless TB is treated as a global health emergency, advances in the development of tools to end TB will continue to be very slow, and unacceptably high rates of disease, suffering, and death will continue.
DISCUSSION
Strengthening the Tuberculosis Response
Gail Cassell, senior lecturer on global health and social medicine at Harvard Medical School, remarked that in her experience with TB, she has observed a lack of harmonization in regulatory processes, drug facilities and timing, and drug expiration, all of which create challenges. She suggested that the National Academy of Medicine consider a future workshop focused on the issue of regulatory harmonization with specific emphasis on TB. Kester commented that the science and technology needed to address many public health issues are relatively straightforward, and generating political will and investment is the major hurdle. However, TB also entails substantial development costs. Clinical trials for regulatory approval are expensive, and the cost of deployment is a challenge in its own right. Kester contrasted the attention given to TB—which has existed for a long time and is a huge global problem—with COVID-19, which is constantly featured in the news, and case counts by county are reported daily. He asked how the public can be sensitized to the huge public health issue that TB is in order to increase the rate of progress, which is currently very slow.
Chaisson replied that TB remains a long-standing, difficult problem to solve because of a general lack of concern about the disease. In 2020, COVID-19 surpassed TB as a global cause of death. Despite TB having killed more people than any other infection in history, it does not garner the attention that COVID-19 does. He stated that the governmental response to COVID-19 has been appropriate, but a similar response to TB is necessary. People do not view TB as an emergency right now, but this was the case even when it was declared an emergency 28 years ago. The current response to COVID-19 is unsustainable, said Chaisson. For instance, institutional review boards have become fully dedicated to COVID-19 trials while processes for other diseases are halted. He remarked that the approach taken with HIV
is an example of a sustainable path forward. Grants related to HIV are prioritized, with the NIH review process for HIV taking 2 to 2.5 months, in comparison with 10 to 12 months for grants for TB and other conditions.
Chaisson explained that an HIV grant submitted in early September is typically reviewed by October or November and funded by January. Thus, implementation of interventions for HIV takes place more quickly than for other conditions. When an innovation such as dolutegravir—an antiretroviral medication used to treat HIV—becomes available, countries demand it, WHO recommends it, Unitaid funds expansion of its production, and it is implemented, he remarked. In contrast, implementation of innovations for TB such as bedaquiline—a drug used to treat MDR TB—can take many years. Chaisson said that people must care about TB in order to adequately address it, and the magnitude of the problem should be emphasized to make it more compelling. Wells remarked that creating a focus on TB and generating resources to address it is an ongoing challenge. Prior efforts include marketing XDR TB as “Ebola with wings” and connecting TB with HIV in the President’s Emergency Plan for AIDS Relief.
Monique Mansoura, executive director for Global Health and Biotechnology at the MITRE Corporation, commented that coronavirus vaccine development was de-prioritized for 17 years. The 2003 emergence of severe acute respiratory syndrome (SARS) and its reemergence in 2012 were not met with aggressive action to address coronaviruses as a public health or national security threat. When taking a longer view of investment in coronaviruses, one can see passivity. She emphasized that the opportunities for collaboration and cost savings in addressing both TB and COVID-19 need to be recognized. Tackling TB builds the capabilities that have value in addressing future outbreaks, epidemics, and pandemics. Instead of positioning TB against other threats, the shared benefits of addressing all threats can be highlighted.
Data Sharing and Standardization
Kester asked how data sharing and standardization can be organized to generate data that can be compared across trials and across regions, and thus making it relevant for various future actions. Hermann replied that much progress is needed in TB’s development as an R&D discipline. Inefficiencies occur when extracting information from across trials and also from translating nonclinical experimental models to clinical models. Data sharing is the only way to advance R&D progress, said Hermann. Both nonclinical and clinical trial data should be shared, and this presents challenges and legal aspects to consider. He noted that the Bill & Melinda Gates Foundation has a fundamental tenet of data sharing being the expectation, and all investments made by the foundation include data-sharing commitments. This has
resulted in two TB investments in which patient-level data were aggregated through a data repository, and analysis of these pooled data led to insights. Hermann noted that data sharing is not easy, but it is possible, and important lessons can be derived from pooled analysis efforts.
Nahid remarked that some people question the value of data sharing in relation to the amount of effort it requires. He shared a recent experience in pooling the data from four fluoroquinolone-substitution trials. Even though these trials found the experimental 4-month regimens to be inferior, he and his colleagues were able to learn about disease phenotypes, the critical importance of standardizing TB outcomes, and the effect of nonadherence (Imperial et al., 2018). For example, they found that one of the biggest drivers of an unfavorable outcome was missing as few as 1 in 10 doses. This illustrates the value of pooling data for clinical applications, and this value extends to the preclinical space. Pooled data analysis de-risks decision making for the entire TB therapeutics community, said Nahid (Lienhardt and Nahid, 2019).
Considerations for Tuberculosis Research and Authorization
Cassell commented on how little was initially known about COVID-19, particularly in respect to its broad clinical manifestations and the long-term damage it can cause. Despite the virus not being fully understood, rapid developments took place to address COVID-19. Emergency authorizations were used to allow earlier approval of vaccines and treatments to combat COVID-19 while continuing to collect and analyze real-world data. If resources and time were unlimited, knowing everything possible about the pathogen before proceeding would be preferable. However, Cassell wondered if perhaps a lesson from this is that moving forward faster—without having all scientific questions answered first—may be beneficial in addressing infectious diseases, including TB, and whether the approach should be considered.
Chaisson remarked that clinical product development needs a foundation of robust basic research and discovery. He pointed to a 1992 commentary that identified TB as an emerging problem and described how TB research funding dwindled in the 1960s because of decades of disease decline in the United States (Bloom and Murray, 1992). He further noted that during his years at medical school, TB was only mentioned once during a pathology course and was omitted from all other courses, including microbiology. TB was no longer considered modern science at that time, he said. In the 1980s, Chaisson’s chief of medicine tried to dissuade him from conducting research on TB in San Francisco residents with HIV. The research ethos around TB was deconstructed in the 1960s and has not been reconstructed since. Nonetheless, TB researchers today are taking up and using modern techniques. He
noted that the Johns Hopkins University Center for Tuberculosis Research shares a building with cancer research labs, and he and his colleagues have found that TB research has much in common with cancer research and microbiome research, as they use similar methodologies. Product studies can identify new targets that inform the development of new medicines that eventually become the focus of clinical trials, he emphasized. Comprehensive basic science and pathogenesis research is being rebuilt, and this is necessary in advancing TB research, said Chaisson.
Translational Medicine and Human-Centered Design
Wells noted that workshop sessions have highlighted the role of translational medicine in TB innovation and discovery, in translation from the clinical trial to implementation, and in economics. A shorter regimen would be transformative for TB treatment, and efficient TB treatment could reduce poverty. He asked how much communication is needed between the upstream clinical space and the downstream implementation space as trials are designed and executed. Nahid replied that human-centered design, patient preference aspects, and program preference aspects are essential to incorporate in the early development of a new regimen or tool. He added that this is a growth area for the TB community. The WHO Guideline Development Committee approach to endorsing a regimen includes a multidimensional examination of benefits and harms that includes the patient experience of the implementation of the new regimen (WHO, 2014). Collecting data early in the design process can help WHO endorse and facilitate the scale-up of new designs.
Capacity for mRNA Technology and Vaccine Production
Schmidt remarked that more research on pathogenicity and antigen discovery is needed. He noted that with mRNA platforms, it is possible to express a dozen antigens easily, yet researchers do not know which antigens to express. Understanding the biology to guide development requires the investment of money and effort. Reed agreed that discovery of new target antigens is time-intensive, and delivery mechanisms can be developed in parallel. At the same time, the good should not be killed in search of the perfect, he emphasized, noting that a vaccine antigen that provides up to and beyond 50 percent protection can advance the goal of disease elimination. Cassell noted that Moderna announced that they will manufacture mRNA vaccines for HIV. She asked whether HDT Bio has a TB vaccine center in Rwanda. Reed replied that HDT Bio’s most active center is in India, and the Indian and Korean centers have committed to providing vaccines to Africa. The organization seeded a pilot production facility in Cape Town several years
ago, and this will be expanded to other countries—including Rwanda—to increase local capacity. The Korean facility is a modern factory built to manufacture recombinant TB vaccines. Although TB is not a major problem in Korea, the country is committed to addressing it and has invested heavily in the company. In fact, Korea has two state-of-the-art facilities: the recombinant vaccine technology center and a center for BCG vaccine funded in part by the Green Cross. Korea will assist HDT Bio in transferring technology once African sites have the ability to receive it, said Reed. He added that the focus in these sites should be on the infrastructure and training needed to receive and sustain local production capability. Brazil has all the components in place, including machines, good manufacturing practices, trained personnel, and funding. Reed stated the hope that Africa will likewise be able to establish capacity. He noted that discovery should continue, and it should focus on antigens as well as delivery mechanisms, as the delivery of an RNA or new antigen can increase the vaccine’s efficacy.
Reflections on the Session
Kester remarked that the multipronged approaches presented at this workshop are promising, from the potential for new lessons in the use of well-characterized products such as BCG to the emerging RNA vaccine technology, given that they can be paired with political will and investment funding. COVID-19 has not only been the impetus for COVID-19 vaccines, it has accelerated new vaccine technology, including mRNA approaches. The COVID-19 pandemic has also sensitized policy makers and funders to the value of vaccines. He noted that not all vaccines will be able to be developed, tested, deployed, and approved in the shorter time frame in which COVID-19 vaccines were created. Researchers should guard against the perception that such a timeline is feasible for all vaccines. The continued demonstration of value of new adjuvants holds the potential to increase the efficacy of antigens via the appropriate adjuvant formulation. Kester commented that host-directed approaches and the interaction of pathogens with the host are areas meriting further study. The possibility of shortening the regimen holds promise, as data indicate that the long-held view that TB treatment must be slow and lengthy is not necessarily accurate. He noted that all approaches hold both risk and opportunity, and that the challenge is using the existing science rather than searching for the perfect solution.
Wells remarked that he has worked on TB for many years—seeing much transformation—and the current moment is unprecedented in terms of opportunity for innovation. At the same time, TB efforts have experienced setbacks because of COVID-19, particularly in terms of case finding. He stated that the rapid progress of development and innovation in finding new drugs and vaccines give him hope for TB. Although the disease is challeng-
ing to combat owing to its lower incidence in high-income countries, the TB research space is more active than ever before. Kenneth Castro, professor of global health, epidemiology, and infectious diseases at Emory University, added that the latest developments renew his optimism that advances can be achieved. The ball was dropped with TB, and now is the time to pick it up and use the current opportunities discussed at this workshop, he added.
Cassell noted that host-directed therapies, particularly Gleevec (imatinib), could offer a major advantage if they are able to act synergistically with antibiotics. This area warrants attention and could yield considerable advances, she believes. In addition, the IMPAc-TB study funded by the National Institute of Allergy and Infectious Diseases is examining immunological aspects of TB in a collaborative way that has not before been attempted. She emphasized that a vaccine that provides 50 percent protection can substantially curb the TB epidemic, and therefore technologies for these products should be advanced. Data indicates that via mRNA, a combination of antigens could help control TB and reduce the costs of doing so. Regulatory harmonization is an issue that should be addressed quickly to decrease the time it takes to receive WHO approval for manufacturing, said Cassell. She noted that in her experience, the approval process for companies to manufacture TB drugs can take up to 2 years; during that time, lives could be saved by the tried-and-true drugs awaiting approval.


















































