
3
CARE SYSTEMS COVID-19 IMPACT ASSESSMENT: LESSONS LEARNED AND COMPELLING NEEDS
INTRODUCTION AND SECTOR OVERVIEW
Health systems in the U.S. are constituted by a number of different care delivery units and a diverse workforce of clinicians and allied health professionals. This discussion paper will focus on the perspectives of America’s more than 600 health systems—including both for-profit and not-for-profit systems and many of the nation’s academic medical centers (AMCs), safety net facilities, critical access hospitals (CAHs), community hospitals, and rural hospitals—which collectively contain the majority of the nation’s hospital beds, employ nearly half of the country’s physicians, and provide health services ranging from basic primary care to complex surgical procedures (AHRQ, 2017). While this sector assessment will seek to broadly capture the experiences of care delivery organizations during the pandemic, and while many of the challenges and lessons identified in this discussion paper may apply to a range of delivery systems across the country, the review will not address the nuances of specific systems or provider types, such as the Veterans Health Administration (the largest delivery system in the U.S.), correctional care health systems, independent physician practices, and various types of community clinics and health centers. Many of the health systems encompassed in this sector assessment play a critical role in caring for vulnerable patients, serving predominantly low-income populations and shouldering a high burden of uncompensated care (Furukawa et al., 2019; AHRQ, 2018). Beyond clinical care, health systems also occupy a foundational role in their communities, from supporting scientific research to serving as the largest employer in many states across the country (Gooch, 2020). The landscape of U.S. health systems is summarized in Figure 3-1.
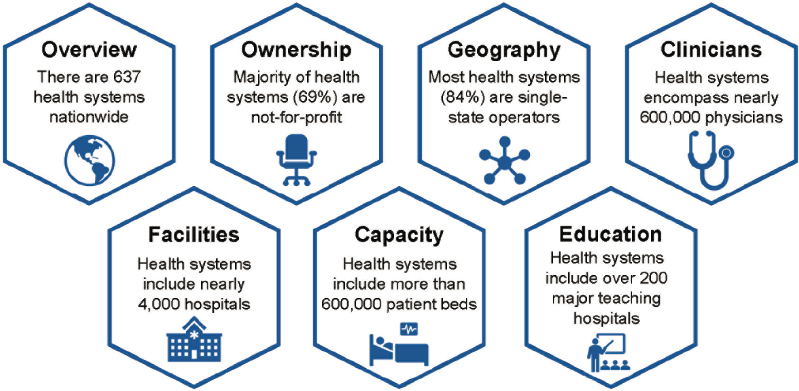
SOURCE: Figure includes data from Compendium of U.S. Health Systems, 2018. Content last reviewed March 2021. Agency for Healthcare Research and Quality, Rockville, MD. Available at: https://www.ahrq.gov/chsp/data-resources/compendium-2018.html.
In recent years, health systems in the U.S. have evolved in response to the growing complexity of patient needs, elevated market pressures, and a changing regulatory and payment environment. For example, as America’s population ages and becomes more diverse, and the burden of chronic disease grows, health systems have increasingly invested in strategies to address complex population health challenges and created new care models that emphasize coordination, service integration, and the social determinants of health (SDoH) (Horwitz et al., 2020; AHA, 2019; The SCAN Foundation, 2018a; The SCAN Foundation, 2018b). As care delivery models have transformed, the market landscape for health systems has also shifted, with notable developments in vertical integration (e.g., payer-provider partnerships, provider group and nursing home acquisitions), horizontal consolidation (e.g., hospital mergers), and site-of-service migration (e.g., from inpatient facilities to outpatient settings or into the home) (Boston Consulting Group, 2020; Furukawa et al., 2020). These industry trends have occurred amidst a rapidly evolving regulatory environment, with health systems navigating a number of key policy issues including the effects of fiscal pressure on Medicare rates, changes to fee schedules, and new proposed rules for price transparency (Ehnes et al., 2020; Kliff, 2019).
These clinical, economic, and policy trends frame the environment for health systems prior to the COVID-19 pandemic. Since the beginning of the outbreak, health systems have (quite literally) operated at the frontlines, providing care to infected patients, taking steps to ensure the safety of providers and staff, and reconfiguring delivery systems to accommodate surges in service demand. As the
COVID-19 pandemic has progressed, health systems have also developed crosscutting public health functions, from augmenting testing and contact tracing capacity for their communities to taking action to address the long-standing health inequities exposed by COVID-19. In most cases, health systems’ pandemic response activities have entailed reducing or canceling non-emergent surgeries and minimizing non-COVID-19 inpatients. Freeing up bed space and staffing resources enabled hospitals to accommodate surges in infected patients, but also greatly reduced profitable service volume. Thus, the response to COVID-19 has carried a high price; disruptions to care delivery have deeply impacted health system finances, while adaptations for surge capacity have strained supply chains and taken a toll (mental, emotional, and physical) on the provider workforce.
This discussion paper seeks to describe the response and experience of hospitals and health systems within the U.S. health care system during COVID-19. At the time of this paper’s publication, the pandemic remains ongoing and health systems’ responsibilities and functions continue to evolve in response to public health needs—including most recently for COVID-19 vaccination campaigns. However, the core challenges for care delivery organizations during the pandemic—financial and operational disruption, supply chain and staffing strain, equity considerations, and cross-sector coordination—remain salient amidst an ever-shifting landscape, and offer a useful lens for navigating present uncertainties and future considerations. Consequently, in this paper, leaders from the care delivery sector will explore how pandemic-era challenges and innovations provide these health systems with an opportunity to transform care delivery to become more accessible, efficient, and equitable for all while fostering preparedness for future public health emergencies. (Recognizing the sector’s heterogeneity and the diversity of delivery system experiences during the pandemic, the author group has supplemented the perspectives presented in this paper through interviews conducted by the Chartis Group with academic health system leaders from the following organizations: University of Pennsylvania, Brigham and Women’s Hospital, Michigan Medicine, Yale New Haven Health System, Beth Israel Lahey, New York Presbyterian, Mt Sinai, University of Chicago, UT Southwestern, Vanderbilt University Medical Center, Emory, Washington University, West Virginia University Health System, and Thomas Jefferson.)
THE HEALTH SYSTEM RESPONSE TO COVID-19
Patient Care Functions
From the outset of the outbreak of COVID-19 in the U.S., health systems began mobilizing to shore up care delivery capacity for COVID-19 patients
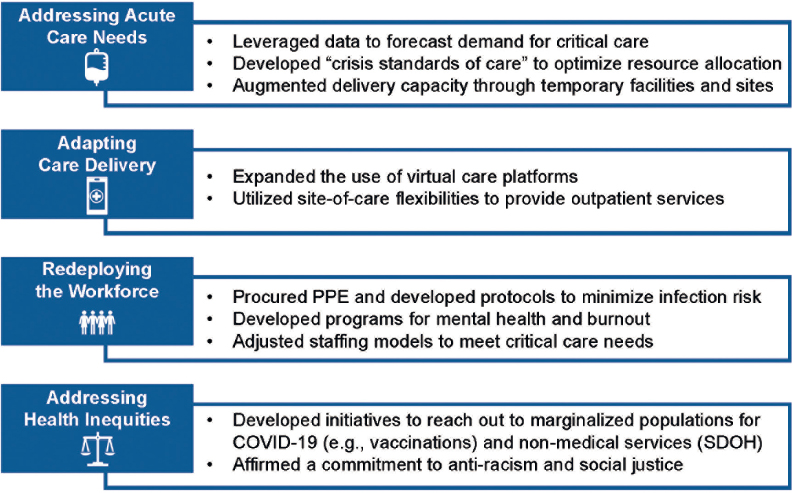
while developing contingencies to account for disruptions in non-COVID-19 care. Redesigning patient care during a pandemic required not only adapting delivery modalities (e.g., virtual platforms, site-of-care flexibilities), but also rethinking supply chains and staffing models to account for the stochasticity of infection rates. Key facets of health systems’ pandemic response for patient care are presented below and summarized in Figure 3-2.
Addressing Acute Care Needs
With health systems possessing the majority of the nation’s inpatient capacity, their first and foremost priority was ensuring that the health care facilities in their system had the capacity and resources needed to treat COVID-19 patients. Key strategies for managing inpatient surge capacity included the following.
First, a primary area of focus was anticipating demand for critical care. 63% of intensive care unit beds in U.S. hospitals were already occupied prior to the pandemic, leaving the health system with approximately 32,000 unoccupied intensive care unit beds at baseline (Tsai et al., 2020). With the virus spreading exponentially in hotspot areas but unevenly across the country, several health systems developed tools to predict needs based on published data, while others leveraged larger regional projections made possible by data initially compiled by the CDC’s National Healthcare Safety Network (Moghadas et al., 2020; NHSN, 2020; Weissman et al., 2020). Health systems then worked with state and
local entities to share the latest data on bed availability and to triage the most appropriate and efficient use of all bed resources, including in skilled nursing facilities (SNFs), rehab, and long-term care centers.
Second, health systems developed new protocols to optimize limited resources and bed capacity. For example, experts proposed a series of “crisis standards of care,” which offered a guide for allocating scarce resources (e.g., ventilators) and clarified trigger events for when health systems should consider activating such emergency protocols (Hick et al., 2020). Additionally, health systems developed new discharge protocols to facilitate care handoffs to home or to post-acute care facilities.
Third, health systems took steps to augment their overall delivery capacity. For example, systems leveraged regulatory flexibilities such as the “Hospital Without Walls” initiative to repurpose alternative sites for inpatient care (e.g., ambulatory surgery centers) (Podulka and Blum, 2020). Other systems leveraged telehealth, existing home health nursing programs, and relationships with third-party entities to implement the Centers for Medicare & Medicaid Services (CMS) Acute Hospital at Home (HaH) program—a care delivery paradigm that entails the provision of care in the patient’s home, obviating the need for an inpatient admission and expediting discharge from inpatient facilities (Sitammagari et al., 2021; CMS, 2020a). Some systems have also leveraged temporary facilities to some extent, such as New York City’s use of a tent hospital site in Central Park and the U.S. Navy Ship (USNS) Comfort. However, utilization of temporary facilities was challenging due to the complexity of transferring acutely ill patients.
Adapting Care Delivery Modalities and Locations
The pandemic significantly disrupted the delivery of non-COVID-19 care, with notable declines in emergency department visits, inpatient admissions, and outpatient visits. For example, studies have reported declines in emergency department volume to exceed 40% in some states between January 2020 and April 2020 (Jeffrey et al., 2020). Likewise, outpatient visits declined by nearly 60% between February 2020 and April 2020 (Mehrotra et al., 2020a). To meet patient needs, health systems leveraged new regulatory flexibilities to adapt care delivery to different modalities and sites of service.
First, health systems reported substantial growth in the use of virtual care platforms following announcements from public and private payers to temporarily expand coverage and reimburse telehealth at parity with in-person visits for the duration of the public health emergency. For example, leaders of the health systems interviewed for this discussion paper reported that telehealth utilization increased from negligible levels prior to COVID-19 to account for the majority of nonemergent patient interactions for the first quarter of 2020
(Koonin et al., 2020). While rates of virtual visits have declined as in-person care has resumed, rates of telehealth utilization still continue to substantially exceed pre-pandemic levels. As of October 2020, telehealth visits accounted for over 6% of all ambulatory care appointments in the U.S.—below the April 2020 peak of nearly 14%, but well above the pre-pandemic rate of 0.1% (Mehrotra et al., 2020b).
Second, health systems leveraged site-of-care flexibilities to ensure continuity of care and continue to meet patient needs within the constraints of shelter-in-place restrictions. For example, many systems shifted the delivery of outpatient services to home-based settings (e.g., wound care, chemotherapy) (Laughlin et al., 2020). While the long-term feasibility of these innovations will depend on the regulatory and payment environment, many patients noted the convenience and efficiency of home and virtual care, and surveys of health care leaders indicate that systems are exploring how these pandemic-era innovations could be better integrated into delivery models for continued use after the pandemic.
Redeploying the Workforce and Ensuring Staff Safety
A leading priority for health system leaders was ensuring the health and safety of staff throughout the pandemic. Health systems took several steps to protect their workforce while also reconfiguring clinical workflows to meet the needs of COVID-19 patients.
First, many health systems focused on ensuring staff safety by developing protocols for testing, tracing, and infection control, and procuring necessary personal protective equipment (PPE), with national shortages at the outset of the pandemic creating challenges for the protection of health care workers. For example, some health systems redesigned their workflows to minimize exposure and maximize safety. Key strategies included limiting clinician activities across sites, reducing the total number of physician and nursing staff at risk of exposure, and ensuring the availability of substitute team members and locations or facilities in the event of exposure.
Second, some health systems worked to develop support systems to alleviate the stress and strain of COVID-19 on their clinician workforce. Common strategies included centralizing mental health resources for providers, providing support for self-isolation requirements, and conducting proactive screenings for symptoms of anxiety, depression, and post-traumatic stress disorder in providers (NYC Health + Hospitals, 2020; UCSF, 2020). However, not all health systems—particularly those in rural communities and those serving safety net populations—possessed the same resources. Additionally, with the pandemic persisting for over a year, the accumulated stress of escalating waves of infection did take a toll on many health
professionals, with emerging evidence highlighting significant burnout in the clinician workforce (Matsuo et al., 2020).
Third, health systems that were able sought to adjust their staffing models to meet patient needs. For example, during COVID-19, some care areas faced staff shortages (e.g., Emergency Departments, Intensive Care Units), while others had underutilized staff due to the delay of scheduled, non-emergent procedures and outpatient services. With shortages ranging from respiratory therapists to physicians with critical care training, some health systems relied heavily on staffing firms and traveling providers to fill gaps during the early days of the pandemic. However, with the virus eventually affecting health systems across the country, hospitals later had little spare capacity, and the cost of locum tenens (substitute providers) increased substantially, adding to the financial strain of the pandemic (Capstone Headwaters, 2021). Other systems sought to rapidly cross-train health professionals to address surge staffing needs, developed specialized COVID-19 training for staff, and reassigned residents at AMCs from other inpatient service lines (e.g., obstetrics and gynecology, radiology, and surgery) to support COVID-19 care (Keeley et al., 2020). Yet while these measures highlight the adaptability of health systems during COVID-19, the prolonged nature of the pandemic and recurrence of staffing shortages well into the end of 2020 and beginning of 2021 created substantial pressures on hospitals across the country (Goldhill, 2020).
Addressing Health Disparities and Health Equity
COVID-19 magnified America’s long-standing disparities in health care quality, access, and outcomes across racial and ethnic groups, socioeconomic strata, and geographies. In response, health systems worked to meet patients where they were and address non-medical needs. For example, several health systems created community outreach programs that sought to tailor public health resources to their community’s context (e.g., development of Spanish language communication tools) and facilitate access to COVID-19 diagnosis and treatment (e.g., coordination for free testing sites) (AHA, 2020a). Partnerships with community organizations was key to outreach, with health systems frequently collaborating with the faith community to disseminate public health best practices, counter misinformation related to COVID-19 and vaccine mistrust, and organize drive-through testing sites (mHealth Fairview, 2020; Tupponce, 2020). To help address the environmental drivers of COVID-19’s disparate impact, many health systems worked to screen their patients for non-medical but critical needs (e.g., food or housing insecurity), and accordingly collaborated with local medical (e.g., pharmacies) and non-medical (e.g., food banks, housing agencies) organizations to coordinate the provision of wraparound services.
Furthermore, in the wake of nationwide protests following the deaths of George Floyd, Breonna Taylor, and many other Black Americans, numerous health systems reaffirmed their commitment to combating health inequities, with many organizations beginning their work by launching task forces focused on anti-racism and social justice (McLean Hospital, 2020; Megerian, 2020; Michigan Medicine Headlines, 2020; VUMC Reporter, 2020). For example, a group of 39 of the nation’s largest health systems pledged in September to take several steps to address health care disparities and structural racism in their organizations (Megerian, 2020; Paavola, 2020; VUMC Reporter, 2020). This group’s pledge and statement was modeled after a June statement signed by 36 Chicago-area health systems (Paavola, 2020).
Public Health Functions
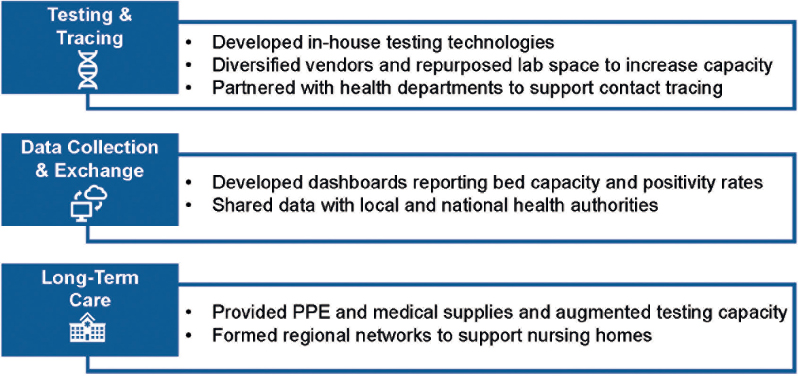
In addition to their primary functions for care delivery, health systems also played a critical role in the public health response, from supporting the development of medical countermeasures including diagnostics, therapeutics, and vaccines to scaling testing capacity and exchanging data to inform disease surveillance. Examples of cross-cutting public health functions are presented in Figure 3-3.
Testing and Tracing
Accurate and timely testing for COVID-19 was critical for health systems to effectively respond to the pandemic (OIG, 2020; HHS, 2020a). Many health systems were able to develop testing capacity through a combination of internal
resources and external vendors. However, a key challenge for system leaders was determining how to allocate or prioritize testing resources with different turnaround times for distinct operational (e.g., surveillance testing of staff) and care delivery (e.g., urgent scenarios) needs. Additionally, responses by systems may have varied according to their unique context, resources, and community needs, with some rural systems facing distinct challenges from integrated delivery systems in urban environments. Additionally, backlogs in test processing created bottlenecks for decision-making about patient care, which in turned slowed service allocation (e.g., whether a patient required a negative pressure room) and care transitions (e.g., discharge to post-acute care facilities) (Grabowski and Joynt Maddox, 2020).
Faced with an uncertain and rapidly evolving regulatory and scientific landscape, health systems took action to augment testing and tracing capacity. For one, hundreds of health systems developed their own diagnostic tests for SARS-CoV-2, with multiple health systems even receiving Emergency Use Authorizations from the Food and Drug Administration (FDA) for the molecular assays which they developed in-house (King, 2020; FDA, 2020a). In addition to developing their own tests, care delivery organizations leveraged their research laboratories to alert the FDA about issues with test performance (Pradhan, 2020).
As testing methods improved, care delivery organizations took steps to scale their testing capacity and support contact tracing efforts. Common strategies to mitigate the risk of supply shortages included diversifying laboratory supply vendors and opening new laboratory facilities to meet demand (Johnson, 2020). Many health systems also developed robust contact tracing programs for both their own staff and patients, with internal programs including the use of digital contact tracing tools and dedicated infection control teams (Brigham and Women’s Hospital, 2020; Cohen, 2020). Health systems then used this expertise to support contact tracing at the community level, working to augment local health department capacity by offering to collect and process specimens and in some cases even providing training programs for newly hired contact tracers (Kennedy, 2020; Kurtzman, 2020). Notably, health systems often launched these initiatives without additional resources or funding, and often still faced regulatory and technical challenges for implementation.
Data Collection and Exchange
Due to their role in caring for COVID-19 patients and the in-house testing programs that many care delivery organizations developed, health systems possessed valuable data for COVID-19 to help inform both internal care planning as well as local disease surveillance. Indeed, several health systems developed their
own COVID-19 dashboards to keep the public informed. By aggregating data on disease surveillance with information on test positivity rates and bed capacity, health systems were able to help streamline provider and patient decision-making with respect to referrals and accordingly to manage supplies and surge capacity (Texas Medical Center, 2020).
Support for Long-Term Care
Nursing homes have been described as “ground zero” for COVID-19 in the U.S.—a trend that has persisted throughout the pandemic, with cases and fatalities peaking in December 2020 and January 2021 (The COVID Tracking Project, n.d.). Despite the vulnerability of nursing home residents, efforts to support long-term care facilities have been stymied by both existing systemic challenges (e.g., funding, staffing) and cross-cutting governance and regulation across levels of government (Barnett and Grabowski, 2020). In response, health systems have stepped up to support nursing homes during the pandemic, ranging from the sharing of infection control best practices and COVID-19 training materials to donations of PPE to facilities experiencing shortages and the provision of diagnostic capacity to reduce turnaround times for COVID-19 testing (Herman, 2020). As the pandemic progressed, several health systems were also formally contracted to develop regional collaboratives for coordinating testing, medical supplies, and rapid response team deployments for nursing homes experiencing rising caseloads (Lord, 2020).
KEY PANDEMIC-ERA CHALLENGES FOR HEALTH SYSTEMS
The harrowing experiences of health systems and health professionals in early pandemic epicenters illustrated the unprecedented challenges imposed on health systems from a care delivery perspective (Khullar, 2020). Yet as it became clear the outbreak had evaded early control and achieved national spread, the challenges for care delivery organizations began to evolve beyond patient care. The key challenges included:
- Financial pressures from care delays, cancellations, and additional costs for pandemic response;
- Supply chain strain for products ranging from PPE to essential medicines;
- Workforce limitations and staffing shortages; and
- The need to develop cross-cutting functions to support community needs (see Table 3-1).
TABLE 3-1 | Health System Challenges During COVID-19
| Theme | Challenges | Example |
|---|---|---|
| Financial Impact |
|
|
| Supply Chain |
|
|
|
|
|
| Workforce |
|
|
|
|
|
| System and Community-Wide Coordination |
|
|
|
|
Financial Impacts
Health systems encountered a paradox during COVID-19. Despite operating beyond their inpatient capacity during spikes in COVID-19, many health systems experienced substantial financial instability resulting from delayed or cancelled care that has persisted throughout the public health emergency. The sector incurred hundreds of billions of dollars in financial losses during the spring of 2020 (AHA, 2020b; Kaufman Hall, 2020a). Financial relief from the Coronavirus Aid, Relief,
and Economic Security (CARES) Act partially alleviated the impact, with federal appropriations limiting the overall decrease in the median hospital operating margin between 2019 and 2020 to a decrease of 1.2% (there would have been a decrease of nearly 5% without CARES funding) (Kaufman Hall, 2021). Notably, health systems with diversified revenue streams (e.g., health plan operations) and payment models (e.g., capitation) were able to partially offset some losses (Liss, 2021; Bannow, 2020). Nevertheless, the sector overall experienced significant financial impacts. Additionally, while health care has historically been considered “recession proof,” the jobs recovery continues to lag, with net layoffs exceeding 110,000 jobs in U.S. hospitals alone as of September 2020 (BLS, 2020). The key drivers of the pandemic-induced financial impact include shifts in payer mix (e.g., expansion in self-pay and Medicaid patient segments due to the abrupt rise in unemployment), the lost revenue from delays and cancellations of scheduled, non-emergent procedures (a key revenue stream for care delivery systems), and the ancillary expenditures for pandemic preparedness and response. Together, these factors led to a 14% increase in expenses per discharge and a 6% decline in outpatient revenue during 2020, reflecting the financial difficulties for the sector as a whole (Kaufman Hall, 2021).
Care Delays and Cancellations
While American hospitals possess moderate excess capacity (average occupancy of 62% at baseline), the anticipated demand from COVID-19 suggested that hospitals would need to create additional inpatient capacity (Song and Ferris, 2018). To generate additional capacity, conserve supplies, and reduce the exposure risk for patients and staff, CMS recommended on March 18, 2020 that most elective surgeries and non-essential procedures be cancelled or delayed during the public health emergency (CMS, 2020b). Federal action was followed by executive orders from dozens of states and the District of Columbia (ACS, 2020). While well-intentioned and appropriate, these actions carried several challenges and financial consequences.
First, the meaning of “elective” was misinterpreted during the ensuing implementation of public health guidance. Although the defining characteristic of an “elective” procedure is that it is a scheduled operation, policymakers and the lay public conflated “elective” with “optional” (e.g., cosmetic surgery). While care deferrals and cancellations certainly freed up inpatient capacity, this imprecision in messaging may have delayed time-sensitive care (e.g., tumor biopsies, operable cancers, ischemic heart disease) and also created a backlog of millions of procedures (e.g., joint replacements, cataracts removal) which is forecasted to take months, if not years, to resolve (Berlin et al., 2020; Brindle et al., 2020).
Second, the cancellation or deferral of vast numbers of procedures and outpatient services had a profound effect on health systems’ financial health. The volume-based payment system generally provides better reimbursement relative to cost for procedural than consultative services (Bai and Zare, 2020; Gondi and Chokshi, 2020; Khullar et al., 2020). Cancellations also generally affected hospitals’ more profitable service lines (e.g., complex surgeries), with approximately 30% of inpatient revenue attributed to elective procedures (Khullar et al., 2020). Likewise, the 6% decline in outpatient revenue during 2020 negatively impacted the sector, as hospital revenue today is generally evenly distributed across both inpatient and outpatient service lines (Kaufman Hall, 2021; Khullar et al., 2020). Consequently, the volume declines which resulted from both governmental mandates and patient choices resulted in significant shortfalls in operating revenue, even at health systems where intensive care units were at capacity due to COVID-19, with rural hospitals and CAHs experiencing particularly severe impacts (Khullar et al., 2020).
Additional Pandemic-Related Expenditures
In addition to declining revenue streams due to service disruptions, care delivery organizations also incurred additional expenditures due to the resources and staffing costs associated with the pandemic response. Demand for many pandemic essentials (e.g., medication, PPE, labor) far outpaced supply, requiring many organizations to pay hefty premiums to replenish their stocks in anticipation of additional cases. For example, market research found key supplies (e.g., N95 respirators, nitryl gloves) in April 2020 to carry markups in excess of 1,000% of pre-COVID-19 pricing (SHOPP, 2020). Likewise, drug expenses per adjusted discharge increased by 62% during April 2020 for select critical care medicines which went into shortage (Kaufman Hall, 2020b). Beyond line-item costs, care delivery organizations also incurred additional expenses from the reconfiguration of facilities and staffing workflows for the pandemic response (Capstone Headwaters, 2021; Kaufman Hall, 2020b). Overall, non-labor expenses increased by 14% and supply expenses by 13% in 2020, illustrating the added costs from the COVID-19 response (Kaufman Hall, 2021).
While the $175 billion which Congress appropriated through the CARES Act offered health systems temporary financial relief, the long-term financial outlook for health systems remains unclear, particularly with the persistence of high COVID-19 caseloads and the uncertain time frame for the full return to pre-pandemic non-COVID-19 utilization levels. Additionally, the criteria and distribution system for financial relief required amendments, as the original methodology was anchored to historical levels of Medicare fee-for-service payments, creating inequities in allocation. This experience illustrates the need
for more transparent and targeted approaches that account for the unique context of different health systems (e.g., safety net institutions) (Socker et al., 2020).
Supply Chain
COVID-19 has exposed significant vulnerabilities in the global health care supply chain. These vulnerabilities preceded the pandemic, with the FDA documenting the periodic lapses of medical equipment, essential supplies, and pharmaceuticals. The drivers of supply chain vulnerability during COVID-19 include:
- Baseline shortages of medical products;
- The geographic consolidation of manufacturing; and
- The lack of incentives for health systems to maintain excess capacity (see Table 3-2).
Baseline Shortages
Many medical products were already in shortage prior to COVID-19. For example, the FDA reported 51 new drug shortages during 2019, with agency intervention required to prevent another 154 new shortages over the course of the calendar year (FDA, 2020b). Yet while FDA documentation of supply chain
TABLE 3-2 | Drivers of Supply Chain Vulnerability
| Theme | Challenges | Example |
|---|---|---|
| Baseline Shortages |
|
|
|
|
|
| Geographic Consolidation |
|
|
| Misaligned Incentives |
|
|
deficiencies is helpful, the agency’s reports are a lagging indicator given that health systems experience difficulties in obtaining critical items well before the FDA publishes data on shortages. For example, surveys of hospital pharmacists found that 69% reported more than 50 shortages for their facility before the pandemic (Hantel et al., 2019).
Given these existing shortages, it is no wonder that the supply chains quickly collapsed under pandemic-induced demand. For example, after randomized controlled trials found dexamethasone, a common and inexpensive steroid, substantially reduced mortality among hospitalized COVID-19 patients, hospital demand in the U.S. increased by 610% while the fill rate declined to 54% (Silverman, 2020; The RECOVERY Collaborative Group, 2020). Such an outcome was not unforeseen, considering that dexamethasone has been in shortage since February 2019 (FDA Drug Shortages, 2020). The challenges are magnified for devices, as prior to the passage of the CARES Act the FDA did not possess the same mandate to proactively collect and report data regarding device shortages as it did for drugs (FDA, 2020c).
The U.S. does maintain reserves of essential medicines and key medical devices and equipment in the Strategic National Stockpile (SNS) for use during emergency situations. However, the SNS has long been underfunded and lacked appropriate procedures for efficient and coordinated distribution (Gerstein, 2020). For example, reserve PPE in the SNS was not replenished after the 2009 H1N1 pandemic (Reinhard and Brown, 2020). Likewise, the approximately 12,000 ventilators in the SNS at the beginning of the COVID-19 outbreak were considered insufficient to meet patient needs in March 2020. While the federal government and health systems did take steps to address these challenges, the presence of baseline shortages created significant barriers for effective emergency response from the outset of the pandemic.
Geographic Consolidation
The American health care system’s heavy reliance on overseas manufacturers and its predilection toward maintaining lower inventory, which under normal circumstances enables cost savings and efficiencies, became critical weaknesses during a pandemic that fueled global demand for products. Indeed, the supply chains for the overwhelming majority of medical product classes today are offshored. For example, FDA officials in 2019 testimony to Congress noted that the majority of manufacturing facilities for active pharmaceutical ingredients (72%) and finished dosage form (53%) were located outside of the U.S. (Woodcock, 2019). Likewise, the majority of factories which manufacture PPE are located in China, which also acquired a significant portion of the global supply at the beginning of the pandemic (Bradsher and Alderman, 2020).
The concentration of manufacturing capacity offshore is the result of labor cost advantages on the part of international producers, which have both enabled such manufacturers to scale their operations and also rendered it challenging for producers from more costly geographies (e.g., the U.S.) to compete. The resulting narrowing of the number of suppliers renders the market more vulnerable to supply shocks and pricing instability (as was the case for COVID-19) and has also been tied to gaps in quality. For example, the FDA’s interagency task force on drug shortages identified the leading causes of supply chain vulnerabilities to include a reliance on low-price clauses by group purchasing organizations (GPOs) during contract negotiations and immature quality management systems (e.g., incentives for compliance rather than continuous improvement) (FDA, 2019).
Misaligned Incentives
With rising cost pressures, health systems have gravitated over the last two decades toward more efficient strategies that lower supply chain costs while optimizing quality, such as just-in-time manufacturing, just-in-time distribution, and just-in-time delivery (Khorasani et al., 2020). The advent of GPOs during this same period of time led the distribution of medical supplies to become increasingly consolidated and efficient, but may have also reduced excess production capacity in the system.
While health system innovations (e.g., retrofitting medical devices to meet patient needs) and public-private partnerships (e.g., PPE donation drives, 3D print exchange curated by the National Institutes of Health) helped to address shortages, the overall challenges during COVID-19 illustrate the need to consider new strategies that allow for far greater medical supply surge capacity.
Workforce
An important focus for health systems was reconfiguring staffing workflows for pandemic response. This process not only highlighted existing challenges in the workforce (e.g., staffing shortages, limited flexibility of existing models) but also spotlighted the pervasive challenge of burnout among health professionals. Key workforce challenges are as follows.
Staffing Shortages
Increased demand for care during COVID-19 highlighted gaps in staffing supply for health systems in general and across select clinical domains (e.g., critical care) and care sites (e.g., post-acute care). Many of these shortages preceded the pandemic. For example, analyses performed by the U.S. Department
of Health and Human Services project multiple states to have deficits exceeding 10,000 nurses by 2030 (HHS, 2017). Such shortages—which are attributed to a number of factors including burnout-induced turnover and the dearth of nurse educators—undermine health systems’ capacity for general inpatient care, leading care delivery organizations to increasingly rely on traveling clinicians to fill in gaps at baseline (Galewitz, 2015). Researchers have also reported an association between staffing shortages and poor health outcomes for inpatient care (Griffiths et al., 2018). High volumes of hospitalizations during COVID-19 illustrate the consequences of these preexisting workforce gaps, with health system demand for nurses regularly outpacing available local and national supply throughout the pandemic (McLernon, 2020).
The staffing shortages for general inpatient care are even more pronounced in specific specialties and care sites. For example, while a significant number of COVID-19 patients required admission to the Intensive Care Unit (ICU), only half of all acute care hospitals in the U.S. had any intensivists at all according to the Society for Critical Care Medicine, creating challenges for managing admission volume (SCCM, 2019). Capacity gaps became a persistent issue during COVID-19, with ICU occupancy approaching nearly 80% in January 2021—well above the pre-pandemic baseline of 63% (Kaufman Hall, 2021). While the growing use of advanced practice providers (e.g., nurse practitioners, physician assistants) has helped to fill staffing gaps, shortages have persisted in part due to the uneven distribution of labor across the country (Flynn, 2018). Indeed, while the number of registered nurses (RNs) primarily practicing in critical care settings has increased in recent years, current staffing levels continue to lag behind system needs (Smiley et al., 2018).
Many facilities have in turn become chronically understaffed, particularly in the post-acute care setting. For example, nursing homes have been understaffed for years, with CMS in 2018 issuing one-star ratings to nearly 1,400 facilities due to staffing shortages (approximately 9% of all nursing homes) (Rau, 2018; Spanko, 2018). The longstanding shortage of nursing home staff can be attributed to many factors, including inadequate salaries and poor working conditions (BLS, 2019). These capacity gaps, coupled with the increasing use of contract workers in the industry, created challenges during the pandemic due to the susceptibility of postacute care facilities to COVID-19 outbreaks, with 21% of U.S. nursing homes reporting staff shortages during the summer of 2020 (McGarry et al., 2020).
Training and Flexibility
Staffing gaps are also overlaid with skill gaps, particularly in critical care. For example, baseline education programs for advanced practice providers offer little
exposure to critical care, and dedicated fellowship opportunities have limited seats and funding (SCCM, 2019). The pandemic has also highlighted the challenges that health systems face at efficiently retraining and redeploying staff in response to episodic demand. For example, many health systems relied on locum tenens to meet staffing needs during COVID-19. This response is an outgrowth of pre-pandemic patterns, in which the majority of health care facilities now routinely utilize temporary physicians and nurses, particularly in the acute care specialties. However, the need for temporary physicians tends to be concentrated with select specialties; for example, demand for locum tenens in emergency medicine and anesthesiology has tripled over the past decade (Staff Care, 2020). These trends illustrate the need for more flexible workflows and internal capacity for cross-training across specialties to meet health system needs, as well as the need to address chronic issues such as limited funding for health professions education and nationwide nursing shortages.
Workforce Well-Being
A significant area of focus for health systems prior to COVID-19 was addressing growing rates of burnout among health professionals. The National Academy of Medicine’s (NAM’s) 2019 report on the subject highlighted the multifactorial nature of burnout (e.g., documentation burden and administrative requirements) and the important role of health systems in developing a supportive workplace environment that fosters the health and well-being of their staff (NASEM, 2019). Emerging evidence illustrates the toll of COVID-19 on the physical, mental, and emotional health of health professionals. Distressingly, burnout has only exacerbated existing inequities within the health system. For example, women—who represent the majority of frontline health care workers—accounted for the majority of COVID-19 cases among health care workers, and also bore a disproportionate burden of added personal responsibilities during the pandemic (e.g., childcare, school closures) (CDC, 2020a). Health systems are increasingly evaluating systems-level solutions to support the health care workforce, including addressing long-standing issues around work-life integration and gender inequities in representation and personal responsibilities (Brubaker, 2020).
System and Community-Wide Coordination
COVID-19 required stakeholders from across multiple sectors to collaborate, share resources, and develop joint strategies for pandemic response. However, systems did not always have relationships with the relevant entities prior to the pandemic, which created challenges for communication. Furthermore, the
preexisting technical infrastructure in many facilities was often outdated and lacked the capacity for the facile exchange of data and information. Challenges encountered in system- and community-wide coordination are explored below.
Coordination Across Systems
Many health systems in America span multiple provider types, communities, regions, and even states. However, as reported in a spring 2020 survey of AMC leaders, facilities and organizations within these systems often continue to operate in a decentralized manner, which in many cases created challenges for communication, resource sharing, and protocol development. These challenges also manifested in coordination with other sectors. For example, the organization of public health in America varies significantly across the country, with some states employing a centralized model while others delegating most decision-making authority to local health agencies. Coordination with public health was further complicated by the heterogeneity in health department resources and capabilities in the U.S., as well as the lack of strong federal guidance and leadership (Haffajee and Mello, 2020).
Data Sharing
Health systems faced challenges receiving and sharing data with public agencies, with specific barriers associated with standardizing data elements (e.g., for demographic information) and integrating with electronic health records (CDC, 2020b; Holmgren et al., 2020). Health systems also experienced significant challenges with data reporting at the national level. The midsummer migration of hospital data reporting systems for COVID-19 created tremendous technical difficulties, imposed transition costs, and resulted in missing or erroneous data (Tahir and Roubein, 2020a). Following implementation, 15% of hospitals remained missing from the database, and many were only able to provide half of the requested information, further compromising the accuracy and reliability of national disease surveillance reports (Tahir and Roubein, 2020b). These technical hurdles created challenges for data sharing beyond disease surveillance; for example, health systems were limited in their ability to communicate timely information about bed capacity and supply stocks in order to efficiently coordinate referrals, plan health services, and allocate resources.
PRIORITY ACTIONS AND POLICY CONSIDERATIONS
The root causes of many of the challenges described in the prior section precede COVID-19. Consequently, health systems are analyzing the challenges
manifest in the pandemic as opportunities for improvement. In particular, systems are looking at new ways to address gaps in financing, infrastructure, and coordination to improve the sector’s overall efficiency as well as enhance preparedness for future emergencies. Sustaining and scaling these best practices will require policy, regulatory, and in some cases legislative, changes. Of course, solutions are far from universal; the heterogeneity of the care delivery sector will require nuanced improvement initiatives that reflect the context of specific subsectors (e.g., rural hospitals, safety net hospitals). This section outlines several priority areas and policy considerations for sector-wide improvement. The key domains for transformation include:
- Enhancing the financial resiliency of health systems;
- Providing for surge capacity in the medical supply chain for care delivery organizations;
- Investing in new workforce support and development programs and staffing models;
- Improving health system flexibility and built-in capacity for inpatient care;
- Building upon renewed commitments and taking concrete actions to address health inequities;
- Addressing subsector-specific challenges for baseline operations and emergency preparedness; and
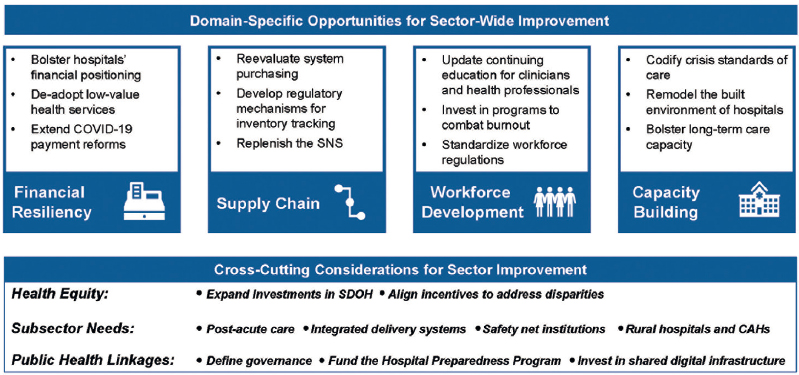
- Fostering linkages between health systems, community-based providers and public health departments (see Figure 3-4).
Enhancing Financial Resiliency
The pandemic exposed the precarious financial foundations of America’s health systems. While federal relief dollars and reimbursement flexibilities helped to soften the pandemic’s blow, the ongoing financial impact of COVID-19 (e.g., from increased operating costs, delayed or canceled care, growth in uncompensated care, and bad debt due to pandemic-induced loss of employer-sponsored insurance) should prompt exploration of opportunities to improve the sector’s financial resiliency. At the operational level, health systems are likely to take steps to reinforce the resilience of their business model. For example, health systems may expand their efforts to diversify their revenue streams, including not only vertical businesses beyond direct provision of health services (e.g., supply chain collaboratives, laboratory companies) but greater collaboration with payers on risk-based arrangements. Likewise, with the concurrent decline in high-margin elective procedures and outpatient services severely affecting hospital credit ratings, systems moving forward may opt to reduce costs and capital investments to conserve cash, in some cases to avoid violating financial covenants.
At the policy level, health systems are uncertain whether the care models developed during the pandemic will be followed by the financial incentives and reimbursement infrastructure needed to truly become mainstays in care delivery. For example, telehealth and HaH programs have both existed for years and possess a rich body of evidence supporting their efficacy; however, they lacked uptake prior to the pandemic due to gaps in reimbursement driven by public and private payer concerns about ‘supply induced demand,’ which is now being examined through the lens of the pandemic (NCQA, 2020). COVID-19 caused most major payers to temporarily enhance payments, enabling health systems to deploy these innovations at unprecedented scale (e.g., reimbursing virtual visits at parity). However, most of these regulatory flexibilities will expire at the conclusion of the public health emergency. Although regulators and legislators have signaled a willingness to make flexibilities such as telehealth permanent, questions remain about potential thresholds on payment, metrics for quality, and guardrails for fraud and abuse (Ross, 2020; Wicklund, 2020). Policymakers will also need to address concerns about patient privacy and challenges for data governance. Similar considerations apply to other delivery innovations. For example, to sustain the expansion of and interest in HaH programs during the pandemic, regulators will need to develop new pathways for reimbursing home-based hospitalizations to account for the potential savings yielded from HaH models (NCHS, 2020; Nundy and Patel, 2020). Furthermore, with CMS flexibilities allowing hospitals to perform site relocations for outpatient services without incurring reductions
in reimbursement, regulators will need to provide clarity on the future of site-neutral payments and provide technical assistance and oversight for providers implementing home-based care solutions (Bekelman et al., 2020).
Beyond delivery models, the pandemic also provides health systems with an opportunity to address existing inefficiencies in health care financing. For example, deferred care can provide an opportunity to support the de-adoption of low-value and wasteful services (e.g., inappropriate screenings), building on programs such as the Choosing Wisely initiative of the American Board of Internal Medicine Foundation (Kim et al., 2020a; Powers et al., 2020; Rosenberg et al., 2015). Likewise, health systems could build on new partnerships with other sectors to address administrative inefficiencies around payment and care coordination.
Priority actions to enhance sector-wide financial resiliency for health systems are summarized in Box 3-1.
Strengthening National and Health System Supply Chains
COVID-19 focused care delivery organizations’ attention on the limited surge capacity in the U.S. health care supply chain. From the elevated infection risk for staff due to the paucity of PPE, to persistent gaps in testing capacity due to supply shortages, to the dearth of medical supplies (e.g., swabs, syringes) and essential medicines, the pandemic has illustrated the need to reconceptualize health care supply chains as a critical national infrastructure.
At the organizational level, health systems may consider emergency supply options where just-in-time production is utilized, and the industry may reevaluate the contractual obligations of GPOs, with a particular focus on surge capacity guarantees (Devaiah et al., 2020). Health systems may seek to diversify
their vendors, develop new protocols for crisis situations, and enhance oversight of waste and inventory. Hospitals in particular may express increased interest in collaborative initiatives and regional resource-sharing programs, building on previous coalitions to address shortages of essential medicines (CivicaRx, 2020). Likewise, health systems may seek to build on regional models for disaster medical response to improve coordination of key medical supplies across local facilities during emergency situations (Mitchell et al., 2020).
At the national level, policies and practices that will enhance supply chain surge capacity include identifying the raw materials and manufactured products that are currently in short supply, as well as inventorying similar and substitutive materials that are currently not in shortage, and delineating the necessary inventory levels for both categories of items that are needed for health systems to function under both normal and crisis conditions. To support this endeavor, regulators could consider creating a low-burden mechanism for tracking essential materials (e.g., a National Drug Code identifier system for consumable medical supplies) that is paired with clear protocols for communication about inventory status across health systems, manufacturers, and regulators. As regulators and health systems work to map supply chains and forecast inventory, policymakers could also perform analyses of potential geographic bottlenecks to identify nodes in the supply chain which may be vulnerable to disruption (e.g., from political events, natural disasters). Policymakers will need to develop incentives to support product diversification, particularly for supply chains that are currently dominated by a single manufacturer. The Defense Production Act of 1950 should be readily leveraged to assess, replenish, and enhance the distribution of critical health care stockpiles (The White House, 2021). In parallel, preparations for future public health emergencies will require increased funding for the SNS, as well as updates to protocols for resource allocation during emergency situations and mechanisms for monitoring inventory turnover (e.g., from use in an emergency, or for when products become obsolete or expired). Lastly, at the state and federal level, anti-price gouging statutes can be extended to encompass health care supplies following emergency declarations.
Priority actions for strengthening medical supply chains for health systems are summarized in Box 3-2.
Investing in Workforce Development
The pandemic illustrates the advantages of staffing protocols and training that are responsive to episodic demand, as well as the benefits of support systems that promote health and well-being across the workforce.
From an operational perspective, COVID-19 has highlighted how flexible staffing and training approaches can better position health systems for the redeployment of staff. For example, to address staffing needs in critical care, cross-training of physicians, nurses, and other health professionals to work in critical settings was essential for filling capacity gaps. Health systems, with the support of accrediting bodies, could foster preparedness by supporting the development of systems of continuing medical education that incorporate annual updates for critical care (e.g., dedicated yearly rotations, simulation training). Likewise, health systems could streamline the future redeployment of staff by standardizing care processes as much as possible within health systems to reduce the risk of errors.
Beyond staffing models, health systems are reaffirming their commitment to supporting the health and well-being of health professionals given both the existing trends for burnout and the significant strain of the pandemic. Approaches to guide system leaders and policymakers are provided in the 2019 NAM consensus study on clinician well-being, as well as other sources (The Blue Ridge Academic Health Group, 2019). Bolstering support systems within health care organizations to support mental health and building on pandemic-era flexibilities to address sources of burnout (e.g., the documentation burden) could further improve the resilience of the health care workforce (NASEM, 2019). For example, greater attention to work-life balance—particularly in light of the disproportionate impact of the pandemic on female health care workers—could include strategies such as expansions to paid leave, temporary housing, emergency funds for unforeseen expenses, and improvements in the accessibility and affordability of childcare for health care workers.
Lastly, investing in workforce development will also require actions from regulators and professional societies. With COVID-19 illustrating the value of sharing staff across state lines during surge periods, rapid recruitment during future emergencies could be supported by improving the uniformity of guidelines
for scope of practice and developing a national database with information on training, certification, and other experience factors.
Priority actions for workforce development are summarized in Box 3-3.
Building Capacity for Patient Care
While health systems met the challenge of surge capacity through unprecedented collaboration and innovation, the COVID-19 experience reveals the importance of identifying new approaches to rapidly and sustainably expanding inpatient care capacity during public health emergencies. Given the role that appropriate rationing of critical care resources might have to play in these crisis settings, experts should also evaluate whether the crisis standards of care that were implemented during COVID-19, including the triggers for activation and the guidelines for specific situations (e.g., allocations of scare ventilator resources), were optimized or require improvements (Hick et al., 2020). Additionally, elevated awareness following the pandemic of the limited supply of health care resources at baseline—and the often unequal distribution of those resources across the population—may prompt a broader reflection on existing inequities and gaps in access to types of health services and products.
Health systems could evaluate the host of operational innovations used to manage episodic demand during COVID-19, with special consideration of those practices that are likely to be useful and sustainable for the future. At the facility level, infrastructure changes such as the development of select inpatient rooms as “universal rooms” capable of conversion for critical care needs, or the construction of entire units with negative pressure ventilation, can anticipate future surges in patients with infectious diseases. Inpatient capacity guidelines at state and local levels could facilitate the construction of public health surge capacity,
with considerations for public funding, building codes, and certificate-of-need guidance to support emergency capacity. Clinicians and hospitals could play a key role in identifying evidence-based practices to inform the development of these guidelines. Furthermore, state, local, and federal programs could be developed with incentives in support of construction that allows for surge capacity, such as private patient rooms that are sufficiently large for double occupancy, with additional oxygen lines and other capabilities, as well as cameras and videoconferencing technology installed in hallways and other locations outside of patient rooms to minimize the frequency of health professionals entering patients’ rooms to reduce contamination and conserve PPE.
Priority actions for health system capacity building are summarized in Box 3-4.
Renewing Commitments to Health Equity
COVID-19 has laid bare the systemic disparities in health outcomes in the U.S. across race, ethnicity, and socioeconomic strata. Nationwide, investments for improving health require additional focus on SDoH to address the environmental drivers of health inequity in America (e.g., housing stability, food insecurity, economic stability, social and community context) (CDC, n.d.; Healthy People 2030, n.d.). Expanding on the kinds of multi-sectoral partnerships identified in the National Academies of Sciences, Engineering, and Medicine 2017 report on Pathways to Health Equity may provide a path forward for investments in the root causes of poor health (NASEM, 2017).
However, actualizing goals to addressing health disparities and structural racism will require sustainable financing systems that support equity-oriented activities. Consequently, payment systems that support delivery models with defined and measurable objectives for closing the outcomes gap for care quality and outcomes will be needed. Policymakers could explore creative mechanisms for pooling funds and investing in community needs, while regulators could advance their support for innovative models such as Accountable Health Communities and
health insurance benefit designs that provide explicit support for SDoH (CMS, 2020c).
Lastly, while this subsection provides examples of specific equity-oriented actions, it should be noted that each of the priority actions highlighted in this paper can and should be approached through the lens of health equity—from the disproportionate financial impact of the pandemic on health systems serving marginalized populations to the unequal distribution of pandemic stressors among the health care workforce.
Priority actions for health system capacity building are summarized in Box 3-5.
Addressing Subsector-Specific Challenges
Care delivery in the U.S. is distributed across a complex matrix of providers and facilities, and each unit of care delivery experienced unique challenges during the COVID-19 pandemic. This section outlines the priority areas for specific health system subsectors.
Post-Acute Care
Post-acute care—which include care settings such as inpatient rehabilitation facilities, long-term care hospitals, and SNFs—has been a key area of focus during the pandemic.
First, post-acute care settings have accounted for a disproportionate number of U.S. COVID-19 deaths (Barnett and Grabowski, 2020; Miller, 2020a; New York Times, 2020). The challenges for health systems (e.g., financial impact, supply shortages, staffing gaps) have been magnified in this subsector. For example, 20% of SNFs continued to report severe PPE shortages throughout the summer months of 2020 (McGarry et al., 2020). Likewise, the decline in short-term Medicare admissions placed downward pressure on unit reimbursement
for nursing homes, severely impacting the finances of postacute care providers (Silver-Greenberg and Harris, 2020). Improving the financial stability of postacute care to withstand this kind of public health emergency will require a broad set of strategies, ranging from coverage reform for long-term care, reimbursement alignment across payers, improved standards for supply and staff capacity, and training and infrastructure for infection control (Grabowski, 2020). For example, nursing home deaths and cases have been negligible in Hong Kong, which has required all facilities to maintain a one-month supply of PPE following the 2003 outbreak of Severe Acute Respiratory Syndrome (Khazan, 2020).
Second, COVID-19 has exposed the pre-pandemic gaps in post-acute care capacity, with the “long haul” effects of COVID-19 illustrating the importance of developing a more robust infrastructure for rehabilitative care. With average SNF occupancy rates exceeding 85% prior to the pandemic, the system had little spare capacity to accommodate COVID-19 survivors during the pandemic (Grabowski and Joynt Maddox, 2020). While health systems in recent years have worked to develop in-house rehabilitation capacity due to challenges with timely access to postacute care, such efforts were complicated during the pandemic by staffing gaps and PPE shortages. Shoring up post-acute care capacity for COVID-19 and beyond will require a range of compensation and workplace improvements to meet staffing needs, as well as new investments in alternatives to institutional post-acute care that leverage technology and home care solutions.
Integrated Delivery Systems
Integrated delivery systems, which are networks of health care facilities and programs that align incentives and resources, have played a critical role during the pandemic response, from serving as hubs for COVID-19 care to pioneering innovations in testing and infection control and continuing to deliver complex and necessary non-COVID-19 care (e.g., transplants, cancer care) (Enthoven, 2009). However, integrated delivery systems also faced notable challenges with regards to operations and financing.
First, for AMCs, the pandemic created unique challenges for medical student and resident education. Many AMCs transitioned preclinical instruction to virtual formats, suspended medical student clerkships and away rotations, offered pathways to early graduation to supplement frontline health care workers, and adopted a phased approach for managing resident involvement in COVID-19 care to optimize care planning and PPE conservation (Kim et al., 2020b; Murphy, 2020; Whelan et al., 2020). Pedagogical innovations during COVID-19, coupled with the transformation of care delivery during the pandemic, may foster long-term changes in medical education. Additionally, the staffing shortages exposed
by the pandemic, particularly in rural and underserved communities, may prompt reforms of education financing. For example, given nursing shortages during COVID-19, policymakers may consider building on the Graduate Nursing Education Demonstration project, which increased graduation rates of advanced practice RNs by 67% over a 6-year period (Jones-Schenk and Leavitt, 2020; CMS, 2019). Likewise, legislators are experiencing renewed calls for reforms to graduate medical education (GME) financing—which capped Medicare support for residency positions in 1997—as well as financing programs such as the National Health Service Corps (Heisler, 2018; IOM, 2014).
Second, the pandemic has illustrated the value of integrated leadership and centrally coordinated decision-making for integrated delivery systems, which occupy a growing geographic and economic footprint of the nation’s health care system, but often are decentralized in their oversight and governance. To cover the cost of uncompensated care and myriad other subsidized services, from behavioral health services to teaching and research, nearly all health systems depend on specific high-margin service lines (Johnston, 2019). The pandemic may prompt integrated delivery systems and policymakers to consider financing reforms that address the uneven distribution of funding for the essential services provided by these institutions. Furthermore, the prominent role of integrated delivery systems in providing public health and scientific leadership during the pandemic (e.g., guideline creation, medical countermeasure development) may motivate greater collaboration with health departments and federal, state, and local officials to improve public health infrastructure (e.g., data infrastructure), combat care inequities (e.g., resource coordination), and enhance research and development capacity (e.g., clinical trial networks) (Shapiro and Rothman, 2020).
Safety Net Institutions
The role of safety net institutions—which are entities providing a significant level of care to the uninsured, Medicaid, and other vulnerable populations—is likely to increase as pandemic-induced layoffs affect health insurance coverage for millions of Americans (Stolberg, 2020; IOM, 2000). Such institutions already operate on narrow margins due to the instability of public financing and the financial burden of providing uncompensated care (Khullar and Chokshi, 2018; Felland et al., 2016). Yet the pandemic has also illustrated the critical importance of safety net institutions to drive innovation in care delivery, from coordinating with health departments to spearheading efforts during the pandemic to address patients’ non-medical needs such as housing insecurity and support for self-isolation.
Increased support for safety net systems will be imperative as the health system recovers from COVID-19. Financial support geared toward addressing gaps in
health equity would help to address the full scope of needs for the marginalized populations which safety net systems serve (Elnahal, 2020). This support can be coupled to the broader adoption of population-based payment systems—which have been successfully trialed at several institutions—and could help improve the financial stability of safety net systems. Additionally, the “braiding and blending” of health and social funds could enhance interdependencies with the public health system (Butler et al., 2020; Stine et al., 2017).
Rural Hospitals and CAHs
Health care in rural America was already in crisis prior to the pandemic, with nearly 40% of all rural hospitals at risk of closure (Miller, 2020b). Challenges abound, such as the gaps in reimbursement due to poor reimbursement rates across public and private payers and low occupancy rates compared to other hospitals nationwide (Kacik, 2018). COVID-19 imposed additional pressures on these structural inadequacies, with already narrow (and often negative) rural margins further contracted under service cancellations, payment rates compromised by Medicaid cuts, and additional pandemic-related expenditures (e.g., for PPE) incurred without commensurate improvements in revenue (Diaz et al., 2020).
The aftermath of the pandemic will require substantive efforts in order to restore financial stability to rural hospitals. For example, CMS recently announced the Community Health Access and Rural Transformation (CHART) Model to support delivery transformation and financial stability in rural areas (CMS, 2020d). Other ongoing reforms, such as the HHS Rural Action Plan, provide promising opportunities to address longstanding disparities in health care access and outcomes (HHS, 2020a). Importantly, the vibrancy of rural hospitals requires fundamental infrastructure investments, such as expanded broadband to ensure rural providers benefit from the transition to telehealth. Payment reforms such as low-volume adjustments could help improve the financial stability of rural facilities, while building on GME pilots such as the Teaching Health Center program could help support workforce development in rural areas (AHA, 2020c; Barclift et al., 2016).
Priority areas for each subsector are summarized in Box 3-6.
Fostering Linkages with Public Health
The pandemic has illustrated the urgent need to develop greater functional integration between health systems and public health departments. Such linkages require governance structures, physical infrastructure, and dedicated funding. Additionally, policy guidance and support for cross-sector coordination is
especially timely as health systems navigate how they can best leverage their delivery network and clinical infrastructure to support COVID-19 vaccination campaigns in their local and state jurisdictions.
First, clear governance structures demarcating the responsibilities for stakeholders from each sector are needed to streamline coordination for emergency situations. Health system and health department capabilities vary widely across the U.S., and many health departments are chronically underfunded. This heterogeneity in resources contributes to variability in emergency response, with health systems often developing add-on functions in regions with underdeveloped public health infrastructure. For example, in some states, health systems helped to coordinate the distribution of COVID-19 therapies such as remdesivir and were intimately involved in the development of the micro-plans for COVID-19 vaccine distribution. Likewise, some health systems played an active role in supporting testing, tracing, and disease surveillance. Actors across the system will need to work together to proactively define key functions and the attribution of responsibilities. Consequently, in the aftermath of the pandemic, health systems and health departments should coordinate to review models of successful partnerships during COVID-19, identify protocols for crisis situations (e.g., designation of dedicated emergency response centers), and define key elements for information sharing (e.g., bed capacity, medical supplies) (Liebman and Patel, 2020; NHRN, 2020; PA Media, 2020).
Second, robust linkages will require investments in shared infrastructure, particularly around technology and data systems. The challenges with data
integrity during COVID-19 have only reaffirmed the need for interoperability both across health systems and between care delivery organizations. The Office of the National Coordinator for Health IT could build on its 2020 interoperability rule to address regulatory issues regarding patient privacy and data interoperability and define standardized approaches for the collection and reporting of common data elements (e.g., demographic information) (Savage et al., 2020). Importantly, efforts to promote interoperability for health systems must also be paired with guidance and resources to modernize shared technical infrastructure for public health. For example, legislators could consider expanding the CDC’s “Digital Bridge” program. Moreover, ongoing review of the performance of “meaningful use” requirements should include health system integration with public health services (CDC, 2019).
Third, expanded purviews and partnerships aimed at emergency preparedness will require appropriate resources. This includes the Hospital Preparedness Program, for which funding levels have declined from $515 million in 2003 to $276 million in 2020, and should include a review of the program’s mandate and functions (HHS, 2020b; Watson et al., 2017). The Assistant Secretary for Preparedness and Response should also consider reviewing the performance of the Hospital Preparedness Program during COVID-19 and ensure the program is appropriately reformed and resourced to address both short-term (e.g., natural disasters) and sustained public health emergencies.
Priority areas for improving coordination between health systems and public health are summarized in Box 3-7.
CONCLUSION
Health systems have been foundational to America’s response to COVID-19, focused first and foremost on providing care to infected patients while navigating challenges ranging from capacity gaps to supply chain shortages. Yet the pandemic has also highlighted how the multifaceted role of health systems today includes functions beyond care delivery. For example, hospitals partnered with organizations across the health system to support public health functions ranging from testing, contact tracing, and more recently, vaccination, as well as working to address the non-medical needs and inequities exacerbated by the pandemic for marginalized populations.
While health systems have played a key role in the pandemic response, COVID-19 has significantly impacted multiple aspects of health system operations, ranging from tremendous financial uncertainty to inadequate resources to meet the needs of patients during persistent waves of outbreaks. Different care delivery organizations across the sector also had distinct experiences, from the unique pressures on postacute care facilities to the cross-sector coordination led by integrated delivery systems. Many of the vulnerabilities exposed by the pandemic represent longstanding challenges for health systems, from shortages of key personnel (e.g., the critical care workforce) to the lack of centralized coordination for the medical product supply chain. Although health systems adapted throughout the pandemic to meet the needs of patients, from introducing innovative new delivery models such as virtual care platforms and Hospital at Home programs to rethinking staffing workflows and entering new cross-sector partnerships, the overall pandemic experience highlights opportunities for the sector to not only improve long-term preparedness for public health emergencies but also the effectiveness of baseline operations.
This discussion paper has sought to capture the experiences of hospitals and health systems during the COVID-19 pandemic and identify opportunities to leverage the lessons of COVID-19 to support performance improvements to the sector more broadly. Although the public health emergency remains ongoing, this review of the experience and evidence to date is applicable for both navigating the next phase for the pandemic and identifying priority actions for upcoming policy reforms. Key policy considerations include enhancing financial resiliency, creating surge capacity in the medical supply chain, investing in new workforce support and development programs and staffing models, improving flexibility and built-in capacity for inpatient care, building upon renewed commitments to address health inequities, addressing subsector-specific challenges, and fostering linkages between health systems and other sectors such as public health. Regulators and system leaders can leverage these lessons to guide the recovery from COVID-19 and the response to future public health emergencies, strengthening the health system’s capacity to address the population health challenges of the 21st century.
REFERENCES
Agency for Healthcare Research and Quality (AHRQ). 2018. Compendium of U.S. Health Systems, 2018. Available at: https://www.ahrq.gov/chsp/data-resources/compendium-2018.html (accessed February 28, 2021).
AHRQ. 2017. Snapshot of U.S. Health Systems, 2016. Available at: https://www.ahrq.gov/sites/default/files/wysiwyg/snapshot-of-us-health-systems-2016v2.pdf (accessed November 5, 2020).
American College of Surgeons (ACS). 2020. COVID-19: Executive Orders by State on Dental, Medical, and Surgical Procedures. Available at: https://www.facs.org/covid-19/legislative-regulatory/executive-orders (accessed October 24, 2020).
American Hospital Association (AHA). 2020a. Community Collaboration During COVID-19: Reaching Hmong and Latino Residents in a Rural Setting. Available at: https://www.aha.org/system/files/media/file/2020/10/aha-cs-ascension-1020_final.pdf (accessed October 24, 2020).
AHA. 2020b. Hospitals and Health Systems Continue to Face Unprecedented Financial Challenges due to COVID-19. Available at: https://www.aha.org/system/files/media/file/2020/06/aha-covid19-financial-impact-report.pdf (accessed October 24, 2020).
AHA. 2020c. Rural Hospital Systems Letter. Available at: https://www.aha.org/system/files/media/file/2020/08/aha-president-trump-urging-additional-support-rural-hospitals-health-systems-letter-8-31-20.pdf (accessed October 24, 2020).
AHA. 2019. Evolving Care Models. Available at: https://www.aha.org/system/files/media/file/2019/04/MarketInsights_CareModelsReport.pdf (accessed November 5, 2020).
Bai, G. and H. Zare. 2020. Hospital Cost Structure and the Implications on Cost Management During COVID-19. Journal of General Internal Medicine 35(9):2807-2809.
Bannow, T. 2020. System-Owned Health Plans Provide Financial Buffer Against Pandemic. Available at: https://www.modernhealthcare.com/finance/system-owned-health-plans-provide-financial-buffer-against-pandemic (accessed November 24, 2020).
Barclift, S. C., E. J. Brown, S. C. Finnegan, E. R. Cohen, and K. Klink. 2016. Teaching Health Center Graduate Medical Education Locations Predominantly Located in Federally Designated Underserved Areas. Journal of Graduate Medical Education 8(2):241-243. https://doi.org/10.4300/JGME-D-15-00274.1.
Barnett, M. L., and D. C. Grabowski. 2020. Nursing Homes Are Ground Zero for COVID-19 Pandemic. JAMA. https://doi.org/10.1001/jamahealthforum.2020.0369.
Bekelman, J. E., E. J. Emanuel, and A. S. Navathe. 2020. Outpatient Treatment at Home for Medicare Beneficiaries During and After the COVID-19 Pandemic. JAMA 324(1):21-22. https://doi.org/10.1001/jama.2020.9017.
Berlin, G., D. Bueno, K. Gibler, and J. Schulz. 2020. Cutting Through the COVID-19 Surgical Backlog. Available at: https://www.mckinsey.com/~/media/McKinsey/Industries/Healthcare-%20Systems%20and%20Services/Our%20Insights/Cutting%20through%20the%20COVID%2019%20surgical%20backlog/Cutting-through-the-COVID-19-surgicalbacklog.pdf?shouldIndex=false (accessed October 24, 2020).
Boston Consulting Group. 2020. Payer and Provider Collaboration and Vertical Integration. Available at: https://www.bcg.com/en-gb/industries/healthcarepayers-providers/payer-provider-collaboration-vertical-integration (accessed November 8, 2020).
Bradsher, K., and L. Alderman. 2020. The World Needs Masks. China Makes Them, but Has Been Hoarding Them. March 13, New York Times. Available at: https://www.nytimes.com/2020/03/13/business/masks-china-coronavirus.html (accessed October 24, 2020).
Brigham and Women’s Hospital. 2020. Statement for Media Regarding COVID-19 Cluster. Available at: https://www.brighamandwomens.org/about-bwh/newsroom/press-releases-detail?id=3684 (accessed October 24, 2020).
Brindle, M. E., G. Doherty, K. Lillemoe, and A. Gawande. 2020. Approaching Surgical Triage During the COVID-19 Pandemic. Annals of Surgery 272(2):40-42. https://doi.org/10.1097/SLA.0000000000003992.
Brubaker, L. 2020. Women Physicians and the COVID-19 Pandemic. JAMA 324(9):835-836. https://doi.org/10.1001/jama.2020.14797.
Bureau of Labor Statistics (BLS). 2020. The Employment Situation—September 2020. Available at: https://www.bls.gov/news.release/pdf/empsit.pdf (accessed October 24, 2020).
BLS. 2019. Occupational Employment and Wages, May 2019. Available at: https://www.bls.gov/oes/current/oes311131.htm (available February 28, 2021).
Butler, S. M., T. Higashi, and M. Cabello. 2020. Budgeting to Promote Social Objectives: A Primer on Braiding and Blending. Available at: https://www.brookings.edu/research/budgeting-to-promote-social-objectives-a-primer-on-braiding-and-blending/ (accessed October 24, 2020).
Capstone Headwaters. 2021. Healthcare Staffing in High Demand as COVID-19 Stresses Healthcare Providers. Available at: https://capstoneheadwaters.com/sites/default/files/Capstone%20Headwaters%20Healthcare%20Staffing%20M%26A%20Coverage%20Report%20January%202021.pdf (accessed February 28, 2021).
Centers for Disease Control and Prevention (CDC). 2020a. Characteristics of Health Care Personnel with COVID-19—United States, February 12–April 9, 2020. MMWR 69(15):477-481. Available at: https://www.cdc.gov/mmwr/volumes/69/wr/mm6915e6.htm (accessed February 28, 2021).
CDC. 2020b. Surveillance Strategy Report—How Sharing Data Digitally Benefits Health. Available at: https://www.cdc.gov/surveillance/innovation/sharing-data-digitally.html (accessed October 24, 2020).
CDC. 2019. Public Health and Promoting Interoperability Programs. Available at: https://www.cdc.gov/ehrmeaningfuluse/public_health_option.html (accessed October 24, 2020).
CDC. n.d. Social Determinants of Health: Know What Affects Health. Available at: https://www.cdc.gov/socialdeterminants/index.htm (accessed February 28, 2021).
CivicaRx. 2020. Civica Update: Civica Rx Partners on COVID-19 Response and “End-to-End” U.S. Based Generic Drug Manufacturing. Available at: https://civicarx.org/civica-update-civica-rx-partners-oncovid-19-response-and-end-to-end-u-s-based-generic-drug-manufacturing/ (accessed October 24, 2020).
Centers for Medicare & Medicaid Services (CMS). 2020a. CMS Announces Comprehensive Strategy to Enhance Hospital Capacity Amid COVID-19 Surge. Available at: https://www.cms.gov/newsroom/press-releases/cms-announces-comprehensivestrategy-enhance-hospital-capacity-amid-covid-19-surge (accessed February 28, 2021).
CMS. 2020b. CMS Releases Recommendations on Adult Elective Surgeries, Non-Essential Medical, Surgical, and Dental Procedures During COVID-19 Response. Available at: https://www.cms.gov/newsroom/press-releases/cms-releases-recommendationsadult-elective-surgeries-non-essential-medicalsurgical-and-dental (accessed October 24, 2020).
CMS. 2020c. Accountable Health Communities Model Fact Sheet. Available at: https://innovation.cms.gov/media/document/ahc-fact-sheet-2020-prelimfindings (accessed October 24, 2020).
CMS. 2020d. CHART Model. Available at: https://innovation.cms.gov/innovation-models/chart-model (accessed October 24, 2020).
CMS. 2019. The Graduate Nurse Education Demonstration Project: Final Evaluation Report. Available at: https://innovation.cms.gov/files/reports/gne-finaleval-rpt.pdf (accessed October 24, 2020).
Cohen, J. K. 2020. Hospitals Retool Contact-Tracing Processes for Staff Amid COVID-19. July 7, Modern Healthcare. Available at: https://www.modernhealthcare.com/operations/hospitals-retool-contact-tracing-processes-staff-amid-covid-19 (accessed October 24, 2020).
Devaiah, A., M. Wijaranakula, C. Kommuru, and R. M. Conti. 2020. Medical Product Procurement in a Time of Federalism: The COVID-19 Challenge. Health Affairs Blog. https://doi.org/10.1377/hblog20200515.360276.
Diaz, A., K. R. Chhabra, and J. W. Scott. 2020. The COVID-19 Pandemic and Rural Hospitals—Adding Insult to Injury. Health Affairs Blog. https://doi.org/10.1377/hblog20200429.583513.
Ehnes, C., C. D. Dauner, and T. Dougherty. 2020. 10 Things to Expect from the New Hospital Price Transparency Rule. Health Affairs Blog. https://doi.org/10.1377/hblog20200304.157067.
Elnahal, S. 2020. Advance Equity by Investing in America’s Healthcare Safety Net. July 7, Modern Healthcare. Available at: https://www.modernhealthcare.com/opinion-editorial/commentaryadvance-equity-investing-americas-healthcaresafety-net (accessed October 24, 2020).
Enthoven, A. C. 2009. Integrated Delivery Systems:The Cure For Fragmentation. American Journal of Managed Care 15(10):S284-S290.
U.S. Food and Drug Administration (FDA). 2020a. In Vitro Diagnostics EUAs. Available at: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/vitro-diagnostics-euas (accessed October 24, 2020).
FDA. 2020b. Report on Drug Shortages for Calendar Year 2019. Available at: https://www.fda.gov/media/139613/download (accessed November 8, 2020).
FDA. 2020c. Food and Drug Administration Safety and Innovation Act (FDASIA). Available at: https://www.fda.gov/regulatory-information/selected-amendments-fdc-act/food-and-drug-administration-safety-and-innovation-act-fdasia#supplychain (accessed October 24, 2020).
FDA. 2019. Drug Shortages; Root Causes and Potential Solutions. Available at: https://www.fda.gov/media/131130/download (accessed October 24, 2020).
FDA Drug Shortages. 2020. Dexamethasone Sodium Phosphate Injection. Available at: https://www.accessdata.fda.gov/scripts/drugshortages/dsp_ActiveIngredientDetails.cfm?AI=Dexamethasone%20Sodium%20Phosphate%20Injection&st=c&tab=tabs-1 (accessed October 24, 2020).
Felland, L., P. Cunningham, A. Doubleday, and C. Warren. 2016. Effects of the Affordable Care Act on Safety Net Hospitals. Available at: https://aspe.hhs.gov/system/files/pdf/255491/SafetyNetHospital.pdf (accessed October 24, 2020).
Flynn, M. 2018. Gulf Between Nursing Shortage, Surplus to Expand by 2030. Available at: https://skillednursingnews.com/2018/10/gulf-nursing-shortagesurplus-expand-2030/ (accessed November 8, 2020).
Furukawa, M. F., L. Kimmey, D. J. Jones, R. M. Machta, J. Guo, and E. C. Rich. 2020. Consolidation of Providers Into Health Systems Increased
Substantially, 2016–18. Health Affairs 39(8):1321-1325. https://doi.org/10.1377/hlthaff.2020.00017.
Furukawa, M., L. Kimmey, D. J. Jones, R. M. Machta, J. Guo, and E. Rich. 2019. Consolidation and Health Systems in 2018: New Data from the AHRQ Compendium. Health Affairs Blog. https://doi.org/10.1377/hblog20191122.345861.
Galewitz, P. 2015. Demand for Travel Nurses Hits a 20-Year High. Available at: https://eu.usatoday.com/story/news/2015/05/24/kaiser-growth-traveling-nurses/27708517/ (accessed December 8, 2020).
Gerstein, D. M. 2020. The Strategic National Stockpile and COVID-19. Available at: https://www.rand.org/pubs/testimonies/CTA530-1.html (accessed October 24, 2020).
Goldhill, O. 2020. ‘People are going to die’: Hospitals in half the states are facing a massive staffing shortage as COVID-19 surges. November 19, STAT News. Available at: https://www.statnews.com/2020/11/19/covid19-hospitals-in-half-the-states-facing-massive-staffing-shortage/ (accessed February 28, 2021).
Gondi, S., and D. A. Chokshi. 2020. Financial Stability as a Goal of Payment Reform—A Lesson from COVID-19. JAMA Forum. https://doi.org/10.1001/jamahealthforum.2020.1012.
Gooch, K. 2020. 17 States Where Hospitals Are Largest Employers. May 12, Becker’s Hospital Review. Available at: https://www.beckershospitalreview.com/workforce/17-states-where-hospitals-are-largest-employers.html (accessed October 24, 2020).
Grabowski, D. C. 2020. Strengthening Nursing Home Policy for the Postpandemic World: How Can We Improve Residents’ Health Outcomes and Experiences? Available at: https://www.commonwealthfund.org/publications/issue-briefs/2020/aug/strengthening-nursing-home-policy-postpandemic-world (accessed October 24, 2020).
Grabowski, D. C., and K. E. Joynt Maddox. 2020. Postacute Care Preparedness for COVID-19: Thinking Ahead. JAMA 323(20):2007–2008. https://doi.org/10.1001/jama.2020.4686.
Griffiths, P., A. Maruotti, A. R. Saucedo, O. C. Redfern, J. E. Ball, J. Briggs, C. Dall’Ora, P. E. Schmidt, and G. B. Smith. 2018. Nurse Staffing, Nursing Assistants, and Hospital Mortality: Retrospective Longitudinal Cohort Study. BMJ Quality and Safety 1-9. http://dx.doi.org/10.1136/bmjqs-2018-008043.
Haffajee, R. L. and M. M. Mello. 2020. Thinking Globally, Acting Locally – The U.S. Response to COVID-19. New England Journal of Medicine 382:e75. https://doi.org/10.1056/NEJMp2006740.
Hantel, A., M. Siegler, F. Hlubocky, K. Colgan, and C. K. Daugherty. 2019. Prevalence and Severity of Rationing During Drug Shortages. JAMA Internal Medicine 179(5):710-711. https://doi.org/10.1001/jamainternmed.2018.8251.
Healthy People 2030. n.d. Social Determinants of Health. Available at: https://health.gov/healthypeople/objectives-and-data/social-determinantshealth (accessed February 28, 2021).
Heisler, E. J. 2018. The National Health Service Corps. Available at: https://fas.org/sgp/crs/misc/R44970.pdf (accessed October 24, 2020).
U.S. Department of Health and Human Services (HHS). 2020a. HHS Details Multiple COVID-19 Testing Statistics as National Test Volume Surges. Available at: https://www.hhs.gov/about/news/2020/07/31/hhs-details-multiple-covid-19-testing-statistics-as-national-test-volume-surges.html#:~:text=Expanding%20capacity%3A%20HHS%20continuously%20works,days%20(from%20specimen%20pickup) (accessed October 24, 2020).
HHS. 2020b. FY2021 Budget in Brief. Available at: https://www.hhs.gov/sites/default/files/fy-2021-budgetin-brief.pdf (accessed November 21, 2020).
HHS. 2017. Supply and Demand Projections of the Nursing Workforce: 2014-2030. Available at: https://bhw.hrsa.gov/sites/default/files/bhw/nchwa/projections/NCHWA_HRSA_Nursing_Report.pdf (accessed December 8, 2020).
Herman, C. O. 2020. Hospitals help skilled nursing facilities with COVID. July 28, The Daily Item. Available at: https://www.dailyitem.com/news/lifestyles/health/hospitals-help-skilled-nursing-facilities-with-covid/article_19e8dce8-79ef-582e-b551-fe8a15481633.html (accessed November 8, 2020).
Hick, J. L., D. Hanfling, M. K. Wynia, and A. T. Pavia. 2020. Duty to Plan: Health Care, Crisis Standards of Care, and Novel Coronavirus SARS-CoV-2. NAM Perspectives. Discussion Paper. National Academy of Medicine. Washington, DC. https://doi.org/10.31478/202003b.
Holmgren, A. J., N. C. Apathy, and J. Alder-Milstein. 2020. Barriers to Hospital Electronic Public Health Reporting and Implications for the COVID-19 Pandemic. Journal of the American Medical Informatics Association 27(8):1306-1309. https://doi.org/10.1093/jamia/ocaa112.
Horwitz, L. I., C. Chang, H. N. Arcilla, and J. R. Knickman. 2020. Quantifying Health Systems’ Investment in Social Determinants of Health, By Sector, 2017–19. Health Affairs 39(2):192-198. https://doi.org/10.1377/hlthaff.2019.01246.
Institute of Medicine (IOM). 2014. Graduate Medical Education That Meets the Nation’s Health Needs. Washington, DC: The National Academies Press. https://doi.org/10.17226/18754.
IOM. 2000. America’s Health Care Safety Net: Intact But Endangered. Washington, DC: The National Academies Press. https://doi.org/10.17226/9612.
Jeffery, M. M., G. D’Onofrio, H. Paek, T. F. Platts-Mills, W. E. Soares III, J. A. Hoppe, N. Genes, B. Nath, and E. R. Melnick. 2020. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First
Months of the COVID-19 Pandemic in the US. JAMA Internal Medicine 180(10):1328-1333. https://doi.org/10.1001/jamainternmed.2020.3288.
Johnson, S. R. 2020. 4 Ways Hospitals Are Improving COVID-19 Testing Lab Efficiency. September 9, Modern Healthcare. Available at: https://www.modernhealthcare.com/care-delivery/4-ways-hospitals-are-improving-covid-19-testing-lab-efficiency (accessed October 24, 2020).
Johnston, S. C. 2019. Academic Medical Centers: Too Large for Their Own Health? JAMA 322(3):203-204. https://doi.org/10.1001/jama.2019.6834.
Jones-Schenk, J., and M. O. Leavitt. 2020. Go National to Solve the Country’s Looming Nursing Shortage. September 4, STAT News. Available at: https://www.statnews.com/2020/09/04/go-national-to-solve-looming-nursing-shortage/ (accessed October 24, 2020).
Kacik, A. 2018. ‘If we had to drive to Albuquerque or Las Vegas she might not have made it.’ Modern Healthcare. Available at: https://www.modernhealthcare.com/indepth/rural-hospitals-look-forhelp-to-survive/ (accessed October 24, 2020).
Kaufman Hall. 2021. National Hospital Flash Report: January 2021. Available at: https://www.kaufmanhall.com/ideas-resources/research-report/national-hospital-flash-report-january-2021 (accessed February 28, 2021).
Kaufman Hall. 2020a. The Effect of COVID-19 on Hospital Financial Health. Available at: https://www.aha.org/system/files/media/file/2020/07/KH-COVID-Hospital-Financial-Health_FINAL.pdf (accessed October 24, 2020).
Kaufman Hall. 2020b. National Expense Observations. Available at: https://flashreports.kaufmanhall.com/expense-may-2020 (accessed October 24, 2020).
Keeley, C., J. Jimenez, H. Jackson, L. Boudourakis, R. J. Salway, N. Cineas, Y. Villanueva, D. Bell, A. B. Wallach, D. B. Schwartz, I. Mendez-Justiniano, and T. G. Long. 2020. Staffing Up for the Surge: Expanding the New York City Public Hospital Workforce During the COVID-19 Pandemic. Health Affairs 39(8):1426-1430. https://doi.org/10.1377/hlthaff.2020.00904.
Kennedy, C. S. 2020. Contact Tracing Essential to Limiting COVID-19’s Spread. Baptist is Doing its Own to Keep Hospital Workers Safe. July 21, Memphis Commercial Appeal. Available at: https://eu.commercialappeal.com/story/news/health/2020/07/21/covid-19-contact-tracing-memphis-shelby-county-baptist-hospitals/5474957002/ (accessed October 24, 2020).
Khazan, O. 2020. The U.S. Is Repeating Its Deadliest Pandemic Mistake. July 6, The Atlantic. Available at: https://www.theatlantic.com/health/archive/2020/07/us-repeating-deadliest-pandemic-mistake-nursing-home-deaths/613855/ (accessed October 24, 2020).
Khorasani, S. T., J. Cross, and O. Maghazei. 2020. Lean Supply Chain Management in Healthcare: A Systematic Review and Meta-Study. International Journal of Lean Six Sigma 11(1):1-34. https://doi.org/10.1108/IJLSS-07-2018-0069.
Khullar, D. 2020. ‘Adrenaline, Duty, and Fear’: Inside a New York Hospital Taking on the Coronavirus. April 3, The New Yorker. Available at: https://www.newyorker.com/science/medical-dispatch/new-yorks-hospitals-take-on-the-coronavirus (accessed October 24, 2020).
Khullar, D., A. M. Bond, and W. L. Schpero. 2020. COVID-19 and the Financial Health of US Hospitals. JAMA 323(21):2127-2128. https://doi.org/10.1001/jama.2020.6269.
Khullar, D., Z. Song, and D. A. Chokshi. 2018. Safety-Net Health Systems At Risk: Who Bears The Burden Of Uncompensated Care? Health Affairs Blog. https://doi.org/10.1377/hblog20180503.138516.
Kim, D. D., D. A. Ollendorf, P. J. Neumann, and M. Fendrick. 2020a. Crisis Into Opportunity: Can COVID-19 Help Set a Path to Improved Health Care Efficiency? The American Journal of Managed Care 26(9):369-370. https://doi.org/10.37765/ajmc.2020.88412.
Kim, C. S., J. B. Lynch, S. Cohen, S. Neme, T. O. Staiger, L. Evans, S. A. Pergam, C. Liu, C. Bryson-Cahn, and T. H. Dellit. 2020b. One Academic Health System’s Early (and Ongoing) Experience Responding to COVID-19: Recommendations From the Initial Epicenter of the Pandemic in the United States. Academic Medicine. https://doi.org/10.1097/ACM.0000000000003410.
King, R. 2020. More Hospitals Turn to In-House Tests to Handle Surge of COVID-19 Patients. March 29, Fierce Healthcare. Available at: https://www.fiercehealthcare.com/hospitals-health-systems/more-hospitals-turn-house-tests-to-handle-surge-covid-19-patients (accessed October 24, 2020).
Kliff, S. 2019. Surprise Medical Bills, the High Cost of Emergency Department Care, and the Effects on Patients. JAMA Internal Medicine 179(11):1457-1458. https://doi.org/10.1001/jamainternmed.2019.3448.
Koonin, L. M., B. Hoots, C. A. Tsang, Z. Leroy, K. Farris, B. T. Jolly, P. Antall, B. McCabe, C. B. R. Zelis, I. Tong, and A. M. Harris. 2020. Trends in the Use of Telehealth During the Emergence of the COVID-19 Pandemic — United States, January–March 2020. MMWR 69(43):1595-1599. http://dx.doi.org/10.15585/mmwr.mm6943a3.
Kurtzman, L. 2020. UCSF Partners with State to Develop Public Health Workforce for COVID-19 Response. Available at: https://www.ucsf.edu/news/2020/05/417346/ucsf-partners-state-develop-public-health-workforce-covid-19-response (accessed October 24, 2020).
Laughlin, A. I., M. Begley, T. Delaney, L. Zinck, L. M. Schuchter, J. Doyle, S. Mehta, J. E. Bekelman, and C. A. Scott. 2020. Accelerating the Delivery of Cancer Care at Home During the COVID-19 Pandemic. NEJM Catalyst. https://catalyst.nejm.org/doi/full/10.1056/cat.20.0258.
Liebman, D., and N. Patel. 2020. To Save Staff And Supplies, Designate Specialized COVID-19 Referral Centers. Health Affairs Blog. https://doi.org/10.1377/hblog20200324.547284.
Liss, S. 2021. COVID-19 puts squeeze on Kaiser Permanente’s 2020 financials. February 8, Healthcare Dive. Available at: https://www.healthcaredive.com/news/covid-19-puts-squeeze-on-kaiserpermanentes-2020-financials/594690/ (accessed February 28, 2021).
Lord, R. 2020. UPMC Could Captain Nursing Home COVID Response Under Bill it Helped to Write. Available at: https://www.publicsource.org/upmccould-captain-nursing-home-covid-response-under-bill-it-helped-to-write/ (accessed November 8, 2020).
Matsuo, T., D. Kobayashi, F. Taki, F. Sakamoto, Y. Uehara, N. Mori, and T. Fukui. 2020. Prevalence of Health Care Worker Burnout During the Coronavirus Disease 2019 (COVID-19) Pandemic in Japan. JAMA Network Open 3(8):e2017271. https://doi.org/10.1001/jamanetworkopen.2020.17271.
McGarry, B. E., D. C. Grabowski, and M. L. Barnett. 2020. Severe Staffing and Personal Protective Equipment Shortages Faced by Nursing Homes During the COVID-19 Pandemic. Health Affairs 39(10):1812-1822. https://doi.org/10.1377/hlthaff.2020.01269.
McLean Hospital. 2020. McLean Establishes Anti-Racist, Justice, and Health Equity Oversight Committee. Available at: https://www.mcleanhospital.org/news/mclean-establishes-anti-racist-justice-and-health-equity-oversight-committee (accessed October 25, 2020).
McLernon, L. M. 2020. COVID-Related Nursing Shortages Hit Hospitals Nationwide. Available at: https://www.cidrap.umn.edu/news-perspective/2020/11/covid-related-nursing-shortages-hit-hospitals-nationwide (accessed December 8, 2020).
Megerian, C. 2020. Expanding Our Commitment to Confronting Racism. Available at: https://www.uhhospitals.org/for-clinicians/articles-and-news/articles/2020/07/Expanding-Our-Commitment-to-Confronting-Racism (accessed October 24, 2020).
Mehrotra, A., M. Chernew, D. Linetsky, H. Hatch, and D. Cutler. 2020a. The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges. May 19, The Commonwealth Fund. Available at: https://www.commonwealthfund.org/publications/2020/apr/impact-covid-19-outpatient-visits (accessed February 28, 2021).
Mehrotra, A., M. Chernew, D. Linetsky, H. Hatch, D. Cutler, and E. C. Schneider. 2020b. The Impact of the COVID-19 Pandemic on Outpatient Care: Visits Return to Prepandemic Levels, but Not for All Providers and Patients. October 15, The Commonwealth Fund. Available at: https://www.commonwealthfund.org/publications/2020/oct/impact-covid-19-pandemic-outpatient-care-visits-return-prepandemic-levels (accessed February 28, 2021).
mHealth Fairview. 2020. Tackling COVID-19 and Health Equity. Available at: https://www.mhealth.org/blog/2020/june-2020/tackling-covid-19-and-health-equity-partnership-brings-testing-to-eastside (accessed October 24, 2020).
Michigan Medicine Headlines. 2020. Michigan Medicine Commits to Anti-Racism. Available at: https://mmheadlines.org/2020/07/michigan-medicine-commits-to-anti-racism/ (accessed October 25, 2020).
Miller, A. M. 2020a. Nursing Home Residents and Workers Make Up a Third of Coronavirus Deaths. May 9, Business Insider. Available at: https://www.businessinsider.com/one-third-of-us-coronavirus-deaths-nursing-home-residents-workers-2020-5?r=US&IR=T (accessed October 24, 2020).
Miller, H. D. 2020b. Saving Rural Hospitals and Sustaining Rural Healthcare. Available at: http://www.chqpr.org/downloads/Saving_Rural_Hospitals.pdf (accessed October 24, 2020).
Mitchell, S. H., E. M. Bulger, H. C. Duber, A. L. Greninger, T. D. Ong, S. C. Morris, L. D. Chew, T. M. Haffner, V. L. Sakata, and J. B. Lynch. 2020. Western Washington State COVID-19 Experience: Keys to Flattening the Curve and Effective Health System Response. Journal of the American College of Surgeons 231(3):316-324. https://doi.org/10.1016/j.jamcollsurg.2020.06.006.
Moghadas, S. M., A. Shoukat, M. C. Fitzpatrick. C. R. Wells, P. Sah, A. Pandey, J. D. Sachs, Z. Wang, L. A. Meyers, B. H. Singer, and A. P. Galvani. 2020. Projecting Hospital Utilization During the COVID-19 Outbreaks in the United States. Proceedings of the National Academy of Sciences 117(16):9122-9126. https://doi.org/10.1073/pnas.2004064117.
Murphy, B. 2020. COVID-19: How the Virus Is Impacting Medical Schools. Available at: https://www.ama-assn.org/delivering-care/public-health/covid-19-how-virus-impacting-medical-schools (accessed October 24, 2020).
National Academies of Sciences, Engineering, and Medicine (NASEM). 2019. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. Washington, DC: The National Academies Press. https://doi.org/10.17226/25521.
NASEM. 2017. Communities in Action: Pathways to Health Equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/24624.
National Center for Health Statistics (NCHS). 2020. Health Expenditures. Available at: https://www.cdc.gov/nchs/fastats/health-expenditures.htm (accessed October 24, 2020).
National Center for Quality Assurance (NCQA). 2020. Taskforce on Telehealth Policy (TTP) Findings and Recommendations. Available at: https://www.ncqa.org/wp-content/uploads/2020/09/20200914_Taskforce_on_Telehealth_Policy_Final_Report.pdf (accessed February 28, 2021).
National Healthcare Safety Network (NHSN). 2020. Current Hospital Capacity Estimates – Snapshot. Available at: https://www.cdc.gov/nhsn/covid19/report-patient-impact.html (accessed November 8, 2020).
New York Times. 2020. About 38% of U.S. Coronavirus Deaths Are Linked to Nursing Homes. Available at: https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html (accessed October 24, 2020).
Northwest Healthcare Response Network (NHRN). 2020. Regional COVID-19 Coordination Center Operational Framework. Available at: http://www.wsha.org/wp-content/uploads/Regional-COVID-19-Coordination-Center-Operational-Framework_Final_2020_03_27.pdf (accessed November 8, 2020).
Nundy, S., and K. K. Patel. 2020. Hospital-at-Home to Support COVID-19 Surge—Time to Bring Down the Walls? JAMA Health Forum. https://doi.org/10.1001/jamahealthforum.2020.0504.
NYC Health + Hospitals. 2020. In Recognition of National Physician Suicide Awareness Day, NYC Health + Hospitals Provides Update on Staff Mental Health Services, DoD Partnership. Available at: https://www.nychealthandhospitals.org/pressrelease/systemprovides-update-on-employee-mental-health-services-after-covid19-peak/ (accessed November 8, 2020).
Office of Inspector General (OIG). 2020. Hospital Experiences Responding to the COVID-19 Pandemic: Results of a National Pulse Survey March 23-27, 2020. Available at: https://oig.hhs.gov/oei/reports/oei-06-20-00300.pdf (accessed October 24, 2020).
PA Media. 2020. Department Of Human Services Announces Health Systems And Academic Medical Centers Selected For Regional Response Health Collaboration Program. Available at: https://www.media.pa.gov/pages/DHS_details.aspx?newsid=569 (accessed November 8, 2020).
Paavola, A. 2020. 29 health systems declare racism a public health crisis, vow to fight it. September 29, Beckers Hospital Review. Available at: https://www.beckershospitalreview.com/hospital-management-administration/39-health-systems-declare-racism-a-public-health-crisis-vow-to-fight-it.html (accessed February 28, 2021).
Podulka, J., and J. Blum. 2020. Regulatory Changes to Medicare in Response to COVID-19. August 4, The Commonwealth Fund. Available at: https://www.commonwealthfund.org/publications/issuebriefs/2020/aug/regulatory-changes-medicareresponse-covid-19 (accessed February 28, 2021).
Powers, B. W., S. H. Jain, and W. H. Shrank. 2020. De-adopting Low Value Care: Evidence, Eminence, and Economics. JAMA 324(16):1603-1604. https://doi.org/10.1001/jama.2020.17534.
Pradhan, R. 2020. As Problems Grow With Abbott’s Fast COVID Test, FDA Standards Are Under Fire. June 22, Kaiser Health News. Available at: https://medcitynews.com/2020/06/as-problems-grow-with-abbotts-fast-covid-test-fda-standards-are-under-fire/ (accessed October 24, 2020).
Rau, J. 2018. ‘It’s Almost Like a Ghost Town.’ Most Nursing Homes Overstated Staffing for Years. July 7, New York Times. Available at: https://www.nytimes.com/2018/07/07/health/nursing-homesstaffing-medicare.html (accessed November 8, 2020).
Reinhard, B., and E. Brown. 2020. Face Masks in National Stockpile Have Not Been Substantially Replenished Since 2009. March 10, The Washington Post. Available at: https://www.washingtonpost.com/investigations/face-masks-in-national-stockpile-have-not-been-substantially-replenishedsince-2009/2020/03/10/57e57316-60c9-11ea-8baf-519cedb6ccd9_story.html (accessed October 24, 2020).
Rosenberg, A., A. Agiro, M. Gottlieb, J. Barron, P. Brady, Y. Liu, C. Li, and A. DeVries. 2015. Early Trends Among Seven Recommendations from the Choosing Wisely Campaign. JAMA Internal Medicine 175(12):1913-1920. https://doi.org/10.1001/jamainternmed.2015.5441.
Ross, C. 2020. ‘I can’t imagine going back’: Medicare leader calls for expanded telehealth access after COVID-19. June 9, STAT News. Available at: https://www.statnews.com/2020/06/09/seema-vermatelehealth-access-covid19/ (accessed October 24, 2020).
Savage, M., A. Neinstein, and J. Adler-Milstein. 2020. Measure The Impact Of The ONC’s New Interoperability Rules Now. Health Affairs Blog. https://doi.org/10.1377/hblog20200701.58142.
Shapiro, S. D., and P. B. Rothman. 2020. How Academic Health Systems Can Move Forward Once COVID-19 Wanes. JAMA 323(23):2377-2378. https://doi.org/10.1001/jama.2020.8002.
Silver-Greenberg, J. and A. J. Harris. 2020. ‘They Just Dumped Him Like Trash’: Nursing Homes Evict Vulnerable Residents. July 23, The New York Times. Available at: https://www.nytimes.com/2020/06/21/business/nursing-homes-evictions-dischargescoronavirus.html (accessed February 28, 2021).
Silverman, E. 2020. Hospitals See Shortages of a Cheap Steroid That One Study Says Helps COVID-19 Patients. June 26, STAT News. Available at: https://www.statnews.com/pharmalot/2020/06/25/covid19-coronavirus-dexamethasone-shortages/ (accessed October 24, 2020).
Sitammagari, K., S. Murphy, M. Kowalkowski, S.-H. Chou, M. Sullivan, S. Taylor, J. Kearns, T. Batchelor, C. Rivet, C. Hole, T. Hinson, P. McCreary, R. Brown, T. Dunn, Z. Neuwirth, and A. McWilliams. 2021. Insights from Rapid Deployment of a “Virtual Hospital” as Standard Care During the COVID-19 Pandemic. Annals of Internal Medicine. https://doi.org/10.7326/M20-4076.
Smiley, R. A., P. Lauer, C. Bienemy, J. G. Berg, E. Shireman, K. A. Reneau, and M. Alexander. 2018. The 2017 National Nursing Workforce Survey. Journal of Nursing Regulation 9(3):S1-S88. https://doi.org/10.1016/S2155-8256(18)30131-5.
Society for Critical Care Medicine (SCCM). 2019. The Multidisciplinary Critical Care Workforce: An Update from SCCM. Available at: https://www.sccm.org/Communications/Critical-Connections/Archives/2019/The-Multidisciplinary-Critical-Care-Workforce-An (accessed November 8, 2020).
Society for Healthcare Organization Procurement Professionals (SHOPP). 2020. COVID-19 PPD Cost Analysis. Available at: http://cdn.cnn.com/cnn/2020/images/04/16/shopp.covid.ppd.costs.analysis_.pdf (accessed October 24, 2020).
Socker, E., A. Spratt, and M. E. Miller. 2020. Distributing Provider Financial Aid to Create a More Efficient, Equitable System. Health Affairs Blog. https://doi.org/10.1377/hblog20201006.416650.
Song, Z., and T. G. Ferris. 2018. Baby Boomers and Beds: a Demographic Challenge for the Ages. Journal of General Internal Medicine 33:367-369. https://doi.org/10.1007/s11606-017-4257-x.
Spanko, A. 2018. CMS Hits 1,400 Nursing Homes with One-Star Reviews Over Staffing Concerns. Available at: https://skillednursingnews.com/2018/07/cmshits-1400-nursing-homes-one-star-reviews-staffing-concerns/ (accessed November 8, 2020).
Staff Care. 2020. 2020 Survey of Temporary Physician Staffing Trends. Available at: https://www.staffcare.com/uploadedFiles/staffcare2020surveyPDF.pdf (accessed November 8, 2020).
Stine, N., D. A. Chokshi, J. Knudsen, M. Cunningham, and R. Wilson. 2017. How America’s Largest Safety-Net Health System Built A High-Performing Medicare ACO. Health Affairs Blog. https://doi.org/10.1377/hblog20171106.437941.
Stolberg, S. G. 2020. Millions Have Lost Health Insurance in Pandemic-Driven Recession. July 13, New York Times. Available at: https://www.nytimes.com/2020/07/13/us/politics/coronavirus-healthinsurance-trump.html (accessed October 24, 2020).
Tahir, D., and R. Roubein. 2020a. Trump’s End Run Around CDC Brings Threat of Fewer Drugs for Hospitals. July 22, POLITICO. Available at: https://www.politico.com/news/2020/07/22/trump-hospital-data-cdc-drugs-379038 (accessed October 24, 2020).
Tahir, D., and R. Roubein. 2020b. Trump Plots Broad Health Data Overhaul After Troubled Rollout of COVID-19 Database. August 19, POLITICO. Available at: https://www.politico.com/news/2020/08/19/trump-plots-broad-health-data-overhaul-aftertroubled-rollout-of-covid-19-database-398403 (accessed October 24, 2020).
Texas Medical Center. 2020. Coronavirus (COVID-19) Updates. Available at: https://www.tmc.edu/coronavirus-updates/ (accessed October 24, 2020).
The Blue Ridge Academic Health Group. 2019. The Behavioral Health Crisis: A Road Map for Academic Health Center Leadership in Healing Our Nation. Available at: http://whsc.emory.edu/blueridge/publications/archive/Blue%20Ridge%202019-2020-FINAL.pdf (accessed December 3, 2020).
The COVID Tracking Project. n.d. The Long-Term Care COVID Tracker. Available at: https://covidtracking.com/nursing-homes-long-term-care-facilities (accessed February 28, 2021).
The RECOVERY Collaborative Group. 2020. Dexamethasone in Hospitalized Patients with COVID-19 — Preliminary Report. New England Journal of Medicine 384:693-704. https://doi.org/10.1056/NEJMoa2021436.
The SCAN Foundation. 2018a. New Opportunities for Serving Complex Care Populations in Medicare Advantage. Available at: https://www.thescanfoundation.org/media/2019/08/2018-12-12_New-Opportunities-for-Serving-Complex-Care-Populations-in-MA.pdf (accessed February 28, 2021).
The SCAN Foundation. 2018b. Ten Questions to Better Understand and Serve Your Complex Care Population. Available at: https://www.thescanfoundation.org/publications/ten-questions-to-better-understand-and-serve-your-complex-care-population-2/ (accessed February 28, 2021).
The White House. 2021. Executive Order on a Sustainable Public Health Supply Chain. Available at: https://www.whitehouse.gov/briefing-room/presidential-actions/2021/01/21/executive-order-a-sustainable-public-health-supply-chain/ (accessed February 28, 2021).
Tsai, T. C., B. H. Jacobson, and A. K. Jha. 2020. American Hospital Capacity and Projected Need for COVID-19 Patient Care. Health Affairs Blog. https://doi.org/10.1377/hblog20200317.457910.
Tupponce, J. 2020. Taking the Facts About COVID-19 to the African-American Faith Community. Available at: https://www.vcuhealth.org/news/covid-19/taking-the-facts-about-covid-19-to-the-african-american-faith-community (accessed October 24, 2020).
University of California, San Francisco (UCSF). 2020. Resources to Support Your Mental Health During the COVID-19 Outbreak and Climate Crises. Available at: https://psychiatry.ucsf.edu/copingresources (accessed November 8, 2020).
VUMC Reporter. 2020. Transcript: Dr. Jeff Balser Announces a New Anti-Racism Task Force and Gives an Update on VUMC’s Leadership Role in the COVID-19 Battle. Available at: https://news.vumc.org/2020/09/22/transcript-dr-jeff-balser-announces-a-new-anti-racism-task-force-and-gives-an-update-on-vumcs-leadership-role-in-the-covid-19-battle/ (accessed October 24, 2020).
Watson, C. R., M. Watson, and T. K. Sell. 2017. Public Health Preparedness Funding: Key Programs and Trends From 2001 to 2017. American Journal of Public Health 107(2):S165-S167. https://doi.org/10.2105/AJPH.2017.303963.
Whelan, A., J. Prescott, G. Young, V. M. Catanese, and R. McKinney. 2020. Guidance on Medical Students’ Participation in Direct In-person Patient Contact Activities. Available at: https://www.aamc.org/system/files/2020-08/meded-August-14-Guidance-on-Medical-Students-on-Clinical-Rotations.pdf (accessed October 24, 2020).
Wicklund, E. 2020. Congress Aims to Keep Telehealth Momentum Going Beyond the COVID-19 Crisis. Available at: https://mhealthintelligence.com/news/congress-aims-to-keep-telehealth-momentum-going-beyond-the-covid-19-crisis (accessed October 24, 2020).
Weissman, G. E., A. Crane-Droesch, C. Chivers, T. B. Luong, A. Hanish, M. Z. Levy, J. Lubken, M. Becker, M. E. Draugelis, G. L. Anesi, P. J. Brennan, J. D. Christie, C. M. Hanson, M. E. Mikkelsen, and S. D. Halpern. 2020. Locally Informed Simulation to Predict Hospital Capacity Needs During the COVID-19 Pandemic. Annals of Internal Medicine. https://doi.org/10.7326/M20-1260.
Woodcock, J. 2019. Securing the U.S. Drug Supply Chain: Oversight of FDA’s Foreign Inspection Program. Available at: https://energycommerce.house.gov/sites/democrats.energycommerce.house.gov/files/documents/Updated%20Testimony%20-%20Woodcock%20%28FDA%29%2020191210.pdf (accessed October 24, 2020).
AUTHOR INFORMATION
Jeffrey Balser, MD, PhD, is President and CEO of Vanderbilt University Medical Center. Jaewon Ryu, MD, JD, is President and CEO of Geisinger. Michelle Hood, MHA, is Executive Vice President and COO of the American Hospital Association. Gary Kaplan, MD, is Chairman and CEO of Virginia Mason Health System. Jonathan Perlin, MD, PhD, is President, Clinical Services and Chief Medical Officer of HCA Healthcare. Bruce Siegel, MD, MPH, is President and CEO of America’s Essential Hospitals.
ACKNOWLEDGMENTS
This paper was supported in part by a grant from The SCAN Foundation—advancing a coordinated and easily navigated system of high-quality services for older adults that preserve dignity and independence. For more information, visit www.TheSCANFoundation.org.
The authors would like to acknowledge Steve Levin and the Chartis Group for their contributions to this paper.
This paper benefited from the thoughtful input of Andrew Bindman, Kaiser Permanente; Terry Fulmer, The John A. Hartford Foundation; Patricia Gabow, University of Colorado School of Medicine and Denver Health (former); and Mukesh Jain, Harrington Discovery Institute and University Hospitals Health System.
Jennifer Lee, Kushal Kadakia, and C. Stephen Chukwurah from the National Academy of Medicine; Anaeze Offodile from the University of Texas MD Anderson Cancer Center; and Marcelo Cerullo from Duke University provided valuable support to the development of this paper.
CONFLICT OF INTEREST DISCLOSURES
Jeffrey Balser discloses that he receives compensation as a member of the board of Varian Medical Systems and is an unpaid member of the board for the Center for Medical Interoperability.
This page intentionally left blank.


















































