4
Opportunity Gaps in the Physical Health and Health Care Experienced by Young Children and Their Parents
This chapter focuses on the drivers of opportunity gaps related to the physical health and health care experienced by young children and their parents. Physical health is a key determinant of children’s ability to participate and thrive in educational settings. Yet there are vast disparities in physical health in the United States. From prenatal and infant health to adolescent health, children from low-income, racial/ethnic minority, and rural backgrounds are more likely to experience health problems. While differences in health care access and quality explain some of these disparities, they are strongly rooted in structural racism and discrimination, as well as underinvestment in economically disadvantaged urban and rural areas (Oberg et al., 2016). Among immigrant children, while those in the first generation are often of lower socioeconomic status but healthier than U.S.-born children on average (the so-called immigrant paradox), the average masks heterogeneity, with worse outcomes among particularly vulnerable groups, such as undocumented children or refugees. Moreover, this paradox often fades by the second generation (Perreira & Allen, 2021).
We also wish to make clear that, by addressing physical and mental health in separate chapters, we do not wish to imply a false dichotomy between the two. We fully recognize the emerging science of brain health as integral to physical health and contextual experiences. Indeed, it is our view that the mental health of children and youth is an essential part of their overall health and a necessary cornerstone of lifelong well-being; we regard neither physical nor mental health as being more or less important than the other, and stress that both are needed to ensure optimal health for children.
Yet opportunity gaps exist in both areas, and ensuring that children thrive will require gaining a comprehensive and global understanding of the status of children’s physical and mental health (Laraque-Arena & Stein, 2021).
The first section of this chapter takes a detailed look at drivers of opportunity gaps in health and health outcomes. The discussion starts by examining prenatal conditions and care for mothers. In the United States, one-fifth of all lower-income women of childbearing age lack access to health insurance, leaving them physically and financially vulnerable and without access to pre- or interconception care. These conditions are exacerbated in certain states that have not extended state-level benefits. As a result, 15% of women in the United States lack quality prenatal care (Osterman & Martin, 2018). The discussion then turns to access to preventive and curative health care for young children, as well as the role of proper nutrition and access to sufficient food in children’s well-being. Informing this discussion is an increase in recent decades in research identifying the effects of increased food availability and improved nutrition (at all stages of life, but especially in infancy) on the well-being of both children and adults.
In addition to health care and nutrition, this section addresses social and structural causes of poor health among children. For example, poverty helps determine the well-being of young children—for example, by contributing to poor housing conditions, which in turn can lead to increased risk of asthma and other adverse health outcomes.
Safe and healthy environments are another important component of the well-being of young children, representing a key structural determinant of health. The discussion of this issue focuses in particular on the benefits of physical safety and freedom from harm and danger and their role in the opportunity gaps experienced by young children. In one study, approximately 37% of U.S. children were found to have experienced physical assault in the past year; 51.4% had experienced physical assault in their lifetime; and 24.5% and 38.3%, respectively, had witnessed violence in the past year or in their lifetime (Finkelhor et al., 2015). Indeed, gun violence is the leading cause of death among U.S. children, recently overtaking injuries from motor vehicle crashes (Goldstick, Cunningham, & Carter, 2022; Lee et al., 2022). With more than 25% of all children witnessing an act of violence in their home, school, or community and more than 5% witnessing a shooting, the importance of understanding and addressing the physical and mental impacts of this exposure to violence is clear (Finkelhor et al., 2009).
The second section of this chapter reviews existing research on potential solutions to some of the drivers of the opportunity gaps in physical health and health care. It describes existing program interventions,
including some introduced during the COVID-19 pandemic, that have been shown to improve these conditions for young children and their mothers.1
DRIVERS OF OPPORTUNITY GAPS IN HEALTH AND HEALTH OUTCOMES
Theoretical and empirical work in the field of life-course epidemiology has consistently shown that prenatal and early-life conditions, including powerful social and structural factors, can affect children’s physical health later in life (Kuh et al., 2003; Ben-Schlomo, Mishra, & Kuh, 2014). Gaps in opportunities related to health begin before birth and can have both short-term and lifelong consequences for well-being. These gaps are influenced by myriad factors, including access to health care and adequate nutrition, poverty, neighborhood safety, and environmental factors, and are exacerbated by racism, segregation, implicit and explicit bias, and stigma (Adler & Stewart, 2010).
Conditions Prior to Birth and Pregnancy
Adverse outcomes in the perinatal period experienced by children and women/birthing people as a result of often preventable pregnancy and birth complications can have lifelong consequences for children’s health and well-being. Most babies in the United States are born healthy and on track for normal physical and cognitive development, but those who are not may need substantial resources and care—not just to survive infancy but to meet the challenges beyond (National Institute of Child Health and Human Development, 2012). Premature birth occurs before the 37th week of pregnancy, a time during which the development of the brain and other organs still benefits substantially from the intrauterine environment (March of Dimes, 2021). Premature birth increases the likelihood of low birthweight (less than 2,500 grams), and can predispose children to breathing and feeding difficulties, vision and hearing problems, developmental delays, and learning disabilities, among other health issues, over the life course (National Institute of Child Health and Human Development, 2012).
Thus gaps in opportunities that emerge before a child is born can have lifelong effects on outcomes. Research is clear that a pregnant person’s access to health insurance can influence the use and timing of prenatal care; that adequate prenatal care is associated with healthier birth outcomes, such as a longer period of gestation and healthier birthweight (Creanga et
___________________
1 The committee uses the terms “woman” and “mother” in this report; however, we recognize that the terms “pregnant woman,” “woman,” “mother,” and “maternal” may not reflect how some pregnant individuals or others seeking reproductive health care may identify.
al., 2014; Ely & Driscoll, 2019); and that healthier birth outcomes can in turn have substantial benefits for the subsequent health and well-being of the developing child.
While the United States does well on some measures of health according to the Organisation for Economic Co-operation and Development (OECD; e.g., rates of death from heart attack and stroke are below OECD levels), it is important to understand the differences in health expenditures between the United States and OECD countries. In general, the richer a country is, the more resources it devotes to health care as citizens’ demands for care increase. However, the United States is also the biggest outlier among the G7 countries in health spending relative to outcomes, with some mortality and morbidity measures falling below the OECD average (e.g., life expectancy is 2 years below the OECD average, and 43% of U.S. children between the ages of 5 and 9 are overweight compared with the OECD average of 31.4% (OECD, 2019, 2022). Unfortunately, an alarming number of people of childbearing age, particularly those with lower incomes, lack access to health insurance, receive inadequate prenatal care, give birth to children who are preterm and of low birthweight, and experience higher rates of infant mortality and maternal mortality and morbidity (a topic discussed further below). These adverse conditions that emerge in the perinatal period are typically more prevalent for people of color, particularly Black birthing people and their infants, and result largely from long-standing oppression and discrimination within health systems (Hoyert & Miniño, 2020; Martin et al., 2019). These early opportunity gaps can widen opportunity gaps and outcomes over the life course.
Maternal Access to Health Insurance
Birthing persons’ access to health care and health insurance is vital for their own health, particularly during the perinatal period, and for the health of their children. In the United States, however, more than 16.7% of lower-income women of childbearing age lack access to health insurance (Prenatal-to-3 Policy Impact Center, 2020), leaving them physically and financially vulnerable and without access to pre- or interconception care.
The lack of access to health insurance among lower-income people of childbearing age, particularly people of color, has historical roots in the development and rollout of Medicaid—the primary insurer for births to lower-income birthing people. Medicaid was launched in 1965 and was originally provided only to people eligible to receive cash benefits through the Aid to Families with Dependent Children (AFDC) program, or “welfare.” In the 1960s, the AFDC program largely excluded families of color, especially in Southern states, because of racist rules that excluded agricultural and domestic workers. Administration of benefit levels and eligibility
for Medicare, the medical insurance program responsible largely for supporting the elderly, occurs at the federal level. By contrast, the administration of Medicaid is left to the states. With minimal federal oversight, states have been allowed to determine income eligibility thresholds, services covered, and reimbursement rates, and these program elements have varied considerably nationwide, with Southern states largely restricting access (Nolen, Beckman, & Sandoe, 2020). Once eligibility has been determined, moreover, continuous coverage for the year is not guaranteed, and even temporary increases in family income can result in loss of coverage and disruption of health care access.
In 2014, the Supreme Court ruled that states could determine whether to implement the expansion of Medicaid in the Affordable Care Act, which provides Medicaid insurance to all individuals with incomes up to 138% of the federal poverty level (FPL). This expansion of Medicaid has reduced the rates of uninsured women of childbearing age significantly, increasing access to and utilization of health care (Kaiser Family Foundation, 2022). To date, however, 12 states have failed to adopt Medicaid expansion, and these states have disproportionately high populations of people of color. In these nonexpansion states, no childless adults are eligible for Medicaid, and the income eligibility threshold for parents varies from a low of 17% of the FPL in Texas to 100% of the FPL in Wisconsin, leaving millions of parents and prospective parents without access to health insurance, a resource that promotes healthier birth outcomes and health across the lifespan.
The percentage of women who lack health insurance is much higher in states that have not expanded Medicaid. In Texas, for example, one of the 12 states that have not expanded Medicaid as part of the Affordable Care Act, nearly half (48.9%) of low-income women aged 19–44 lack health insurance—the highest uninsurance rate in the country (Prenatal-to-3 Policy Impact Center, 2020). These women would be eligible for Medicaid if the state expanded the program, but as noted, under the state rules, no childless adults are eligible for Medicaid, and parents must earn less than 17% of the FPL to qualify. By contrast, fewer than 4% of similar women in the District of Columbia lack health insurance. Not only has the District expanded Medicaid, but it provides coverage to parents with incomes up to 221% of the FPL rather than the 138% required by the Medicaid expansion (Prenatal-to-3 Policy Impact Center, 2020).
In addition, in nearly all states, including Texas, Medicaid income eligibility thresholds for pregnant people are higher than they are for parents or childless adults (in Texas, the threshold for pregnant people is 204% of the FPL, and in the District of Columbia it is 324% of the FPL). And in most states, new parents lose access to Medicaid pregnancy coverage 60 days postpartum. Health insurance is therefore lacking for many new parents, particularly those who cannot remain on traditional Medicaid or buy
insurance on the Marketplace (which is unavailable to those with incomes below 138% of the FPL). The American Rescue Plan Act of 2021 allowed states to provide continuous health coverage for up to a year for postpartum birthing people, but to date, few states have fully implemented that policy (American Public Health Association, 2021). Thus many mothers are left without access to health care when they themselves are still at high risk for postpartum conditions, such as depression, that may affect their ability to care for their child.
Uninsurance rates also vary considerably by race and ethnicity. In particular, lower-income Hispanic women of childbearing age (38.5%) are twice as likely to be uninsured as Black (19.1%) or White (17%) women. This disparity is due in part to eligibility restrictions related to immigration status for many state and federal safety net policies and less generous employer benefits for Hispanic women in low-wage jobs (Prenatal-to-3 Policy Impact Center, 2020).
Maternal Access to Adequate Prenatal Care
Related to access to health insurance is access to quality prenatal care, which in turn is linked to healthier birth outcomes and better health for the mother. Access to quality maternity care is a critical component of maternal health and positive birth outcomes, especially in light of the high rates of maternal mortality and severe maternal morbidity in the United States. Yet nearly 15% of women in the United States—ranging from a low of 5% of births in Rhode Island to nearly 25% in New Mexico—do not receive adequate prenatal care. The lack of quality prenatal care can be attributed to the lack of access to health care and health insurance coverage, as well as the limited availability of prenatal programs in an area or region of the country.
The percentage of Black women who do not receive adequate prenatal care (20.1%) is twice as high as the percentage for White women (9.9%; March of Dimes, 2022). This discrepancy is one of the drivers of the stark differences in birth outcomes between Black women and women of other races/ethnicities. Compared with their White and Hispanic counterparts, for example, the proportion of Black babies born preterm (Box 4-1) is 50% higher, and Black babies are more than twice as likely to be born at low birthweight.
Maternity care deserts are counties in which access to maternity health care services is limited or absent as a result of either lack of services or barriers to a woman’s ability to access those services (March of Dimes, 2022). More than 2.2 million women of childbearing age live in maternity care deserts (1,095 counties), with no hospital or birth center offering obstetric care and no obstetric provider (March of Dimes, 2022). In 2017, almost
150,000 babies were born to women living in maternity care deserts, while an additional 4.8 million women of childbearing age lived in counties with limited access to maternity care (March of Dimes, 2022).
Congress recently reintroduced a sweeping package of 12 maternal health–related bills aimed at addressing racism and racial inequities that disproportionately affect pregnant and birthing people in the United States. The “Momnibus” aims to invest in training a cadre of perinatal health providers to improve upon and better address the significant disparities in maternal and infant health outcomes. For example, although midwives are widely recognized around the world as the primary source of maternal health care, they account for only 8% of U.S. birth workers (Scientific American Editors, 2019; Batstone, 2021). Midwives are health care professionals who may be part of the birth care team or stand alone in providing prenatal, delivery, and postpartum care. States that have policies to allow direct-entry midwives—credentialed midwives who are not registered nurses—and certified nurse midwives to practice may increase access to care, especially in underresourced areas (March of Dimes, 2022). Midwifery care, coordinated with care from a physician, can help reduce medical interventions that contribute to the risk of maternal mortality and morbidity in initial and subsequent pregnancies, lower costs, and potentially improve the health of mothers and babies (American College of Nurse-Midwives, 2021). The maternal care team may also include doulas, nonclinical professionals who support women emotionally and physically during the perinatal period, including birth and postpartum. Increased access to doula care can help improve birth outcomes and reduce the higher rates of maternal morbidity and mortality among women of color in the United States.
Troubling as well is that the rate of infant mortality among Black babies (10.8 per 100 births) is twice the national average (5.6 per 100 births; Ely & Driscoll, 2019). Black mothers are also more than twice as likely to die in childbirth or experience severe maternal morbidity, regardless of education level or socioeconomic status (Centers for Disease Control and Prevention [CDC], 2022). Adverse birth outcomes reflect the trauma resulting from discrimination and racism that many Black women have experienced across their life course, as well as their disproportionately lower access to financial security (Alhusen et al., 2016).
Where babies are born is also predictive of their birth outcomes; for example, babies born in Mississippi are nearly twice as likely to be born preterm and nearly three times as likely to die in the first year of life compared with those born in New Hampshire. Again, these differences in opportunities and outcomes are largely a result of state policy choices, such as those discussed previously with regard to Medicaid expansion. Those states that have declined to expand Medicaid are often the same states with weak safety net programs and consequently higher poverty rates, resulting in a
combination of forces that exacerbate adverse birth outcomes for marginalized families.
The Medical Home and Developmental Screening
For children, the lack of primary and preventive health services can impact not only physical health but also mental health, social-emotional development, and academic outcomes (Polacheck & Gears, 2020). Preventive (or “well-child”) care—including standard vaccinations and flu shots, as well as chronic disease screenings—is an important complement to primary care for physical development and long-term well-being (Regalado & Halfon, 2001; Hagan, Shaw, & Duncan, 2017). Yet obstacles due to the lack of access and health care coverage and to institutional biases reduce the quantity and quality of both primary and preventive care for young children. Also of note, recent data from the Centers for Medicare & Medicaid Services show downward trends in health care utilization during the COVID-19 pandemic for the nearly 40 million children enrolled in Medicaid and the Children’s Health Insurance Program (Centers for Medicare & Medicaid Services [CMS], 2020a; Polacheck & Gears, 2020), driven by stay-at-home orders in states across the nation.
The Medical Home
The medical home is an approach to providing comprehensive primary care that facilitates partnerships among patients, clinicians, and families. The pediatric health care/medical home is a model of care that promotes holistic care of children and their families whereby each patient/family has an ongoing relationship with a health care professional (National Association of Pediatric Nurse Practitioners, 2009). A medical home combines place, process, and people. It is not a building, house, or hospital, but an approach to providing comprehensive primary care. The pediatric clinician can help the family and patient access and coordinate specialty care, other health care services, educational services, in- and out-of-home care, family support, and other public and private community services that are important to the overall health of the child and family. Providing a medical home means addressing both the medical and nonmedical needs of the child and family (American Academy of Pediatrics, 2015).
The medical home is significantly associated with positive child health outcomes regardless of household income. However, children living below versus those living above the FPL are at greater risk of lacking access to a medical home (Anker et al., 2018). Parental perceptions and experiences of having a medical home differ by socioeconomic status and race/ethnicity (Diao et al., 2017). And as with health care utilization generally, the
percentage of children having access to a medical home visit and/or receiving well-child visits decreased during the COVID-19 pandemic. Well-child visits began to decrease in March 2020, reaching their lowest point of the year in April 2020, reflecting a 47.3% decrease compared with 2018–2019. Visit rates rebounded to 2018–2019 levels in June 2020, reaching a peak in September 2020 and remaining at levels nearly equal to those of 2018–2019 during October–December 2020. In January–March 2021, visits dipped below baseline, with the largest decrease in January 2021 (−9.2%; Kujawski et al., 2022).
Developmental Screening
National guidelines for child preventive care visits recommend that children have 10 preventive care visits from birth to 3 years of age (Hagan, Shaw, & Duncan, 2017). Prior to preschool entry at age 3, child preventive care visits may serve as the only opportunity to screen for, identify, and intervene on a range of social, developmental, and health concerns that can have significant impacts on a child’s health and well-being. Yet for many children, particularly those living in poverty, this critical opportunity is often missed, in many cases because of uninsurance or underinsurance or challenges in accessing care, such as those related to transportation and parental work schedules (Bethell et al., 2004, 2011; Halfon et al., 2004; Chung et al., 2006; Norlin et al., 2011).
Routine health care—in particular, well-child visits—is essential for child health and development and can be an important component of lifelong health. When children fall behind on immunizations, they run the risk of developing vaccine-preventable diseases (Santoli et al., 2020). Regular developmental screenings under Early and Periodic Screening, Diagnosis and Treatment guidelines offer an opportunity for pediatric providers to screen for and diagnose physical or cognitive delays early so that early intervention services can be provided (CMS, 2020b). Likewise, failure to identify emerging social-emotional concerns and mental health conditions in childhood or adolescence may result in worsening symptoms over time, potentially leading to increased distress for the child, as well as the need for high-cost inpatient or residential care (Golberstein, Wen, & Miller, 2020). School-based health care and nursing care are a dependable source of pediatric health care for children. When many schools were at least partly closed at the beginning of the COVID-19 pandemic, children and adolescents who previously depended on in-person, school-based mental health care—including a disproportionate number from racial/ethnic minority groups and low-income households—no longer had access to those services (Ali et al., 2019; Golberstein, Wen, & Miller, 2020; Polacheck & Gears, 2020).
Poverty and Health Care
According to a recent National Academies report, poverty has a negative effect on a range of child outcomes in a number of domains (National Academies, 2019). Outcomes related to physical health include low birthweight, structural changes in brain development, child maltreatment, adverse childhood experiences, worse physical health, mental health problems, and increased risky behaviors.
Children and families living in poverty are more likely than their better-resourced counterparts to have needs left unaddressed after a preventive care visit, often as a result of greater social, psychosocial, developmental, and health education and guidance needs that outstrip the 15–20 minutes available for a preventive care visit (Olson et al, 2004; Bethell et al., 2011; Halfon et al., 2011; Norlin et al., 2011; Freeman & Coker, 2018). Pediatric health care visits have traditionally focused on regular immunizations, assessment of growth and developmental milestones, and anticipatory guidance for parents on child development and preventive care to reduce risk for injuries and promote social-emotional learning. Emphasis is increasing, however, on the importance of addressing health-related social needs and social determinants of health within health care through screening; coordinated referrals; colocated and integrated services (including integrated mental health care); and efforts to address institutional and interpersonal racism in medical care through revisions to medical education, leadership development pathways, and policies and protocols (Gottlieb, Sandel, & Adler, 2013).
Beginning at birth, racial and ethnic minorities and those of lower socioeconomic status have poorer access to health care (Flores, 2010). Rural areas are also particularly challenged in terms of health care access, in part because of the difficulty of attracting and retaining high-quality medical providers, as well as transportation and financial difficulties that impede access to care (Douthit et al., 2015). Health care for children is often facilitated through relationships between clinical systems and caregivers, and the broader social context impacts families’ engagement with the health care system. For example, since health insurance in the United States is linked to employment or place of residence, with no universal coverage, when parents of children in low-income families change jobs or move, the children’s care is often fragmented and disjointed.
Currently, medical care is delivered inequitably. Children of color and lower-income families are more likely to receive fragmented services, episodic and limited care, or care that is not culturally or linguistically competent. These children are also less likely to have a medical home. These inequities are greater for children with learning difficulties and developmental disabilities. Exacerbating these inequities are growing rates of childhood
overweight and obesity; mental health and behavioral health challenges; and neurodevelopmental conditions, including autism spectrum disorders (Shonkoff et al., 2012).
Racism and Culturally Responsive Care
Racism is a pervasive stressor, which, like other stressors that operate through physiological pathways, may challenge one’s ability to adapt and may increase health risks (Cohen, Kessler, & Gordon, 1997; McEwen, 2005). The National Academy of Medicine report Vibrant and Healthy Kids provides an extensive review of stress, traumatic stress, adverse childhood experience, and positive buffers. According to that report:
A large body of recent research provides insights into the mechanism by which early adversity in the lives of young children and their families can change the timing of sensitive periods of brain and other organ system development and impact the “plasticity” of developmental processes. Decades of research in the neurobiological sciences have found that responses to pre- and postnatal early life stress are rooted in genetic and environmental interactions that can result in altered molecular and cellular development that impacts the assembly of circuits during sensitive periods of development. There are biologic and physiologic systems involved in cognitive and emotional development that are more sensitive to early disturbances (critical periods) that activate stress response networks, such as the frontal cortex, hippocampus, amygdala, and the hypothalamicpituitaryadrenal axis, provided a basis for both short- and long-term functional consequences of early life stress. (National Academies, 2019, p. 7)
Because racism involves prejudicial attitudes, discriminatory treatment, systemic barriers, and internalized oppression due to an immutable personal characteristic fundamental to identity, it can be especially threatening to well-being (Landrine & Klonoff, 1996; Myers, Lewis, & Dominguez, 2003; Williams & Mohammed, 2009), and although most research focuses on direct targets, racism can also have unintended victims. As described by Harrell (2000) regarding racism-related stress for people of color, vicarious racism includes indirect exposure to the prejudice and discrimination experienced by friends, family, and strangers, which can be distressing and may also affect health. Because children develop within the context of their families and wider social environments (Bronfenbrenner, 1979) and are in critical phases of development, they may be particularly vulnerable to the adverse consequences of vicarious racism (Dominguez et al., 2008)—specifi-cally the perceived threats to maltreatment of persons in their environment (Cohen, Kessler, & Gordon, 1997; Kelly, Bécares, & Nazroo, 2013; Priest
et al., 2013). In addition, evidence suggests that perceived racism—the subjective experience of discrimination or prejudice—may lead to negative biopsychosocial effects, such as psychological and physiological stress, and other negative health outcomes, such as depression and elevated blood pressure (Clark et al., 1999).
Racism is an established social determinant of children’s mental and physical health (Pachter & Coll, 2009). Stress that occurs continually or is triggered by multiple sources not only shapes children’s later emotional lives as adults but also affects their physical health and longevity. Race-based traumatic stress associated with direct or indirect (vicarious) social forces and interpersonal or group dynamics (Harrell, 2000) has been linked to anxiety, poor immune functioning, poor sleep, and impaired daily activity (Menakem, 2017).
Racism as it relates to health care has been shown to contribute to the overall health disparities seen among communities of color. Structural or institutional racism results in decreased access to health care and fewer resources for education, often leading to lower health literacy and fewer health care providers of color. Despite progress in treating and preventing many diseases overall, health disparities continue to exist across different groups, with Black individuals experiencing higher rates of diabetes, obesity, asthma, and hypertension compared with their White counterparts (National Center for Health Statistics [NCHS], 2018, 2020; CDC, 2020; Matthew, Clark, & McDavid, 2021).
It must be acknowledged that health care providers contribute to health disparities. Clinicians and health professional students may lack understanding of White privilege and how racism is perpetuated through policies, protocols, practices, and systems, as well as interpersonally. Inequities can be exacerbated by medical teams with limited numbers of members who have lived experiences similar to those of patients from marginalized populations, as well as by a lack of diversity in ethnic and cultural backgrounds among those in decision-making roles. In addition, families may be less likely to access the health care system if they have not received culturally and linguistically appropriate care in the past or if they face additional challenges due to language, transportation issues, cost, and communication (National Academies, 2017). The intersection of race and poverty, especially profound in the context of residential racial segregation (Schickedanz & Coker, 2016; Williams et al., 2010), adds to the problem. Some research has revealed bias and prejudice among pediatric clinicians with respect to caring for lower-income families, reflecting a lack of understanding and training regarding the effects of poverty on children, failure to confront their own personal prejudices and biases, and stigma often attendant to working with low-income families. This research also revealed that providers found it difficult to apply typical diagnostic frameworks to children from low-income families (Smith et al., 2011, 2013).
Relational Health
Caregiver and parenting practices are critical to children’s physical, cognitive, and social-emotional health. Relational health—or bidirectional relationships between family members and emotional connectedness—begins in infancy in the parent–child bond and is closely associated with attachment and a number of developmental outcomes, including language development and mental health through adulthood (Bethell et al., 2019; Madigan et al., 2019). Father–child and mother–child relational health are viewed as equally important for health (Roby et al., 2021). In both traditional and nontraditional family structures, other family relationships (e.g., with siblings, grandparents, aunts, and uncles) also are critical for child development. Similarly, teachers and other adult mentors in educational settings can play important roles in promoting child health. The negative consequences of the lack of a responsive parent–child or other adult–child relationship are exacerbated in the context of adversity (Hambrick, Brawner, & Perry, 2019).
Since early relational health is so critical for healthy child development, it has become a key area of focus for both preventive and targeted interventions aimed at improving children’s outcomes. Parenting and parent–child relationships therefore represent a central consideration in developmental–behavioral pediatrics. Given that parenting occurs within the context of the greater social and built environments, it is important to address how the stressors of poverty and racism impact the resources, both material and emotional, that parents can devote to their children.
Adultification
Childhood is a social construct that intersects with the social construct of race. As discussed in Chapter 3, relative to their White peers, Black children are more likely to be misperceived as older and more developmentally mature than they are. Beginning at age 5, Black girls are more likely to be viewed as more adult-like, with less need for nurturing, comfort, support, or protection, and to receive harsher punishments (Epstein, Blake, & González, 2017). From age 10, Black boys are viewed as less innocent, misperceived as older, and subject to police violence if accused of a crime (Goff et al., 2014). Research has demonstrated that in general, Black children and youth are more likely than their White peers to receive a punitive response to childlike behavior (Dumas & Nelson, 2016).
Adultification is a term used to describe these differential perceptions of children associated with race (Epstein, Blake, & González, 2017). In this form of implicit bias, the social constructs of childhood and race intersect in a way that disadvantages children of color. A second form of adultification that has been observed in low-resource environments is socialization
of children such that they take on more adult responsibilities at younger ages (Burton, 2007). During enslavement, Black children were dehumanized and viewed as chattel, valued on the basis of their ability to work, subjected to brutal forms of punishment, separated from caregivers, and disallowed access to play and to experiencing the world as children (King, 2005). This historical legacy of slavery informs patterns seen today.
Children are afforded unique protections based on social perceptions of innocence associated with understanding of their social and psychological development, as well as moral principles and laws intended to safeguard them from harsh penalties and levels of culpability and responsibility applied to adults. Adultification can result in losing the freedom to engage in the world as children and access to rights and protections of childhood under the law. The misperception that Black children are more mature, and therefore more accountable for their behavior, may help account for disparate outcomes by race in education, social welfare, and juvenile justice (Ocen, 2015).
Perceptions of children of color as more developmentally mature and the association of those perceptions with the way they are treated ultimately have implications for their social, emotional, and physical health. In one study, Black children aged 5–14 were found to be 31% less likely than their White peers to receive medication in the preoperative period to minimize anxiety, although this association was not observed for children younger than 5 and older than 14 (Baetzel et al., 2019). Other studies found that Black children were more likely to be physically restrained in the emergency department compared with their White counterparts (Tolliver et al., 2022), and were less likely to receive any form of analgesia for moderate pain and less likely to receive opioids for severe pain (Goyal et al., 2015), a disparity discussed further below. It is plausible that adultification informs one form of implicit bias that is associated with such disparate treatment and with physical health outcomes. Implicit racial bias toward Black children has been demonstrated at levels similar to those directed at Black adults (Johnson et al., 2017) and has been shown to impact pain management in pediatrics (Sabin & Greenwald, 2012), although other studies have yielded mixed evidence regarding the impact of implicit bias on clinical decision making (Dehon et al., 2017; Voepel-Lewis & Nafiu, 2017).
Researchers and clinicians alike have argued that raising awareness about the prevalence of adultification by tracking data and implementing quality improvement practices to identify adultification and racism, including coding of encounters that are concerning for these forms of discrimination, can help raise awareness among providers, improve recognition of adultification, and help drive intentional efforts to reduce this form of implicit bias (Koch & Kozhumam, 2021, 2022). Providers can support parents in understanding the implications of these perceptions for their children,
particularly with respect to encounters with police, educators, and health care providers. “The talk” has been popularized as a strategy for caregivers, educators, and clinicians to help children learn protective strategies for police encounters (Maroney & Zuckerman, 2018), although data showing that these strategies are effective are currently not available. “The talk” may also be based in an expectation that Black children can prematurely assume adult roles and responsibilities in the face of institutional racism, a view that may incur a developmental benefit or toll (Burton, 2007).
Antiracism and Dismantling Race-based Medicine
As the discussion in the last chapter has demonstrated, racism, a system of advantage whereby opportunities and values are assigned on the basis of socially constructed categories of “race,” has been identified as a root cause of health and health care inequities (Jones, 2001). Racism operates on multiple levels—interpersonal, institutional, structural, and systemic—although it is perpetuated and reinforced at the structural level. Achieving health equity will therefore require addressing institutional, structural, and systemic racism in health care and public health, and race-based medicine is one area in which systemic racism manifests. It is also worth noting that, while pediatricians have often served as lead clinician in the pediatric medical home, a team-based approach to child health has emerged by which primary care is reconfigured to address access issues. This approach involves the incorporation of mental health in primary care and the medical home, along with an increased role for other health professionals, such as nurse practitioners, school nurses, nurse midwives, social workers, psychologists, doulas, and frontline staff.
History of Race in Medicine
The belief that Black and White individuals have fundamental biological differences was propagated by slaveholders to justify slavery and by scientists and physicians to justify unethical and inhumane medical research conducted on Black people (Cartwright, 1851, as cited in Guillory, 1968; Washington, 2006; Owens, 2017). Today, assumptions about athleticism associated with race/ethnicity are based in beliefs about racial genetics. Although biological conceptions of racial differences are not strongly associated with racist attitudes, they are associated with acceptance of racial inequities as endemic (Williams and Eberhardt, 2008).
The 1985 Report of the Secretary’s Task Force on Black and Minority Health, commonly known as the Heckler Report, documented racial inequities in health. Unequal Treatment, a groundbreaking report of the Institute of Medicine (now known as the National Academy of Medicine),
documented racial/ethnic disparities in the quality of care, demonstrating that for almost all diseases among hundreds reviewed, Black Americans received less effective care than their White counterparts even when such factors as insurance and socioeconomic status were matched (Institute of Medicine [IOM], 2003). Implicit bias in the form of unconscious racial stereotypes related to personal and cultural experiences and limited interracial or intercultural engagement is common among health care providers, mirroring the general population (Chapman, Kaatz, & Carnes, 2013; Ansell & McDonald, 2015). Implicit bias is thought to influence administrative decisions on insurance plans accepted, neighborhoods for establishing offices, and selection and inclusion of diverse students in medical education and training and among faculty (Ansell & McDonald, 2015).
Mounting evidence confirms that race is not a reliable proxy for genetic differences. Yet despite these advances in research, the use of race as a proxy for biological and genetic differences with clinical significance has remained embedded in medical practice, education, training, and research.
Diagnostic Algorithms
Diagnostic algorithms and practice guidelines that correct for a patient’s race or ethnicity continue to be in common use in clinical medicine (Vyas, Eisenstein, & Jones, 2020), taught in medical education, and included in medical board examinations (Amutah et al., 2021). Race-adjusted clinical algorithms guide clinical decisions and operationalize racism in clinical medicine by directing attention and resources to White patients to the detriment of racial and ethnic minorities (Vyas, Eisenstein, & Jones, 2020). Many of these guidelines offer no rationale for the use of race/ethnicity (Vyas, Eisenstein, & Jones, 2020), or when investigated are found to be rooted in race- and class-based biases and assumptions (Braun, 2014).
Diagnostic algorithms that include race/ethnicity lower estimates of success for people of color, and their use to guide care can exacerbate inequities in health care and outcomes. The vaginal birth after cesarean (VBAC) algorithm, for example, predicts risk associated with a vaginal delivery among those who have had a previous cesarean section. The VBAC calculator was informed by a prior research study that identified variables correlated with VBAC success, including insurance type (Landon et al., 2005). It incorporates two race-based correction factors—one for African American women and another for Hispanic women—that subtract from the overall likelihood of successful VBAC, and these women are therefore assigned a lower chance of success (Vyas, Eisenstein, & Jones, 2020). While this algorithm incorporates race/ethnicity as a correction factor, it does not incorporate other factors, such as insurance type, that were correlated with VBAC success in the referenced study. In the United States, women of color
have higher rates of cesarean section in comparison with their White counterparts, as well as three to four times higher rates of maternal mortality and morbidity.
Medical Education
Evidence suggests that medical students and trainees hold false beliefs about fundamental biological and genetic differences by race. The content of medical school curricula reinforces this misperception (Tsai et al., 2016), and this misrepresentation can propagate bias (see Table 4-1; Tsai et al., 2016; Nieblas-Bedolla et al., 2020; Amutah et al., 2021). This misrepresentation can take the form of race-based clinical guidelines; data that tend to associate minoritized populations with increased incidence of disease in the absence of context; association of disease with particular racial groups, which can lead to diagnostic bias; and presentation of racial/ethnic differences in disease burden without addressing the broader social context (Amutah et al., 2021). Race/ethnicity also appears routinely in question banks used to prepare for the United States Medical Licensing Examination (Ripp & Braun, 2017).
Action Steps to Reform Medical Education
The portrayal and misuse of race in medical curricula has been explored, and revisions have been suggested (Amutah et al., 2021). Recommendations include (1) standardizing the language used to describe race/ethnicity; and (2) building relevant medical competencies, such as structural competency, which includes recognizing structures that shape clinical interactions and developing structural interventions (Metzl & Hansen, 2014; Stonington et al., 2018). Training in structural competency can help providers understand the structural and social forces, policies, and historical processes that affect health. More equitable and antiracist care practices could be supported if providers had a deeper understanding of structural and institutional racism and interpersonal discrimination and their impacts on health, clinical encounters, and conditions. To date, however, literature conceptualizing structural racism has not been adequately integrated into medical education, and the majority of empirical studies of racism have focused on interpersonal discrimination rather than structural racism (Bailey et al., 2017).
Implicit Bias
Research has established that the majority of U.S. physicians and medical students have the kinds of implicit biases discussed above that privilege
TABLE 4-1 Misrepresentation of Race in Preclinical Curricula
| Domain | Description | Representative Examples |
|---|---|---|
| Semantics | Using imprecise and nonbiologic labels that inaccurately conflate race and ancestry | Widespread use of “Caucasian,” “Black,” “African American,” and “Asian” as labels to denote biologic differences between patients |
| Describing a Nigerian patient as “African American” in a clinical vignette | ||
| Prevalence without context | Presenting racial/ethnic differences in disease burden without contextualization | Teaching students that “Black” patients have higher rates of asthma than “White” patients without reference to the effects on asthma prevalence of residential segregation and unequal access to high-quality housing and health care |
| Teaching students that “Black” patients have higher rates of hospital readmission without any discussion of the underlying causes of these disparities | ||
| Race-based diagnostic bias | Presentation of links between racial groups and particular diseases | Priming students to view sickle cell disease as affecting only Black people rather than as common in populations at risk for malaria |
| Pathologizing race | The tendency to link minorities with increased disease burden | In a slide showing the incidence of 13 types of brain tumors in Black patients and White patients, using the title “Incidence rates are higher among Blacks than among Whites,” even though 10 of the tumors occurred more frequently in White patients |
| Race-based clinical guidelines | Teaching of guidelines that endorse the use of racial categories in the diagnosis and treatment of diseases | Teaching students to use different first-line antihypertensive drugs in Black patients than in White patients, without any exposure to literature that questions these practices and misleading interpretations of information |
SOURCE: Excerpted from Amutah et al., 2021.
White patients (Haider et al., 2011), with significant proportions of medical students and trainees holding false beliefs about biological differences by race (Hoffman et al., 2016). As noted previously, implicit bias, stereotyping, and prejudice among health care professionals influence inequities in diagnosis, treatment, and care by race/ethnicity (Chapman, Katz, & Carnes, 2013; Hall et al., 2015; FitzGerald & Hurst, 2017), including among common pediatric diagnoses (Sabin & Greenwald, 2012). Medical students who hold such false beliefs were found to be more likely to rate pain lower and make less accurate treatment recommendations for Black versus White patients (Hoffman et al., 2016). Research has documented that Black patients,
including children, not only are less likely to receive pain medication but also receive lower quantities and experience greater delays in administration even though they self-report similar levels of pain (Goyal et al., 2015; Singhal, Tien, & Hsia, 2016). Yet despite the disparities resulting from the inequities embodied in diagnostic algorithms and manifest in differential treatment, medical education and clinical practice have been slow to evolve to reflect race as a social construct rather than a biological category, and racism as a systemic factor in shaping social experiences that have biological consequences.
Efforts of Medical Associations and Other Organizations to Confront Systemic Racism
In recent years, medical associations, such as the American Medical Association (AMA), have acknowledged the role of racism in perpetuating health inequities and harms in communities that have historically been marginalized (O’Reilly, 2020; Madara, 2021; Tanne, 2021), and have adopted policies aimed at embedding racial justice and advancing equity in their work (Maybank et al., 2022). In 2021, the AMA adopted guidelines designed to confront systemic racism (American Medical Association, 2021).
The American Academy of Pediatrics (AAP) has recently taken steps to dismantle race-based medicine in clinical practice and medical education. To that end, it is examining and eliminating inaccurately applied “race corrections” or “race adjustment factors” that result in differential approaches to disease management and disparate clinical outcomes. The AAP recently retired clinical guidelines that linked race, as a biologic proxy, to urinary infections in children (Wright et al., 2022). Presently, the AAP is addressing the use of race in guidelines for newborn jaundice. In May 2022, it released a policy statement, “Eliminating Race-Based Medicine,” that calls for scrutiny and revision of the suite of clinical guidelines, algorithms, educational materials, textbooks, and literature used to guide clinical practice and for medical education (Wright et al., 2022). And some have called on other prominent health organizations, such as the National Institutes of Health, to examine ways of dismantling racism through research infrastructure (Bear et al., 2022).
Nutrition
It is well known that proper nutrition plays a major role in physical development, and young children are the age group most vulnerable to deficits in nutrition given the important developmental changes that occur during the early years of life. The consequences of poor nutrition may plague children into adolescence and adulthood through stunting and poor
cognitive development (De Sanctis et al., 2021; Galler et al., 2021; Pizzol et al., 2021). Existing programs and tax credit policies play an important role in improving nutrition for the poorest children, and recent extensions to these programs may help achieve significant progress toward reducing child hunger and poor nutrition.
Recent decades have seen an increase in research aimed at identifying the effect of increased food availability and improved nutrition on child (and adult) well-being. The techniques used for these studies have leveraged the delayed rollout of programs within the United States to identify the effect of certain U.S. federal and state programs on nutrition outcomes (Almond, Hoynes, & Whitmore Schanzenbach, 2011). For example, increasing evidence indicates that the consumption of nutritious foods during the prenatal period affects the general health and well-being of children and may play a role in their cognitive and physical development (Guan et al., 2021).
Although access to adequate and nutritious food affects development across the life course, it is particularly important for the preconception, prenatal, and early childhood periods. Furthermore, the period from conception to 2 years of age (about the first 1,000 days) is especially critical, as the brain undergoes significant developmental changes during this period that may not be possible later in life (Schwarzenberg et al., 2018). In addition to macronutrients (protein, fat, and glucose), certain micronutrients (zinc, copper, iodine, iron, and selenium) and vitamins and cofactors (vitamin B6, vitamin B12, vitamin A, vitamin K, folate, and choline) are particularly important for healthy early brain development (IOM, 1990; Georgieff, Brunette, & Tran, 2015; Cusick & Georgieff, 2016; Schwarzenberg et al., 2018; National Academies, 2019). Adequate nutrition during later stages of childhood may also play a role in child development. Beyond the above developmental effects, children living in extreme poverty may suffer from insufficient amounts of food that can result in stunting, wasting, or other growth inhibition or delays. Stunting reflects long-term deprivation of nutritious foods, while wasting is the result of more acute periods of food deprivation (Food and Agriculture Organization of the United Nations et al., 2021). Stunting may be indicative of permanent cognitive and/or physical disabilities for children that persist into adulthood.
In addition, poor dietary habits early in life may lead to consumption of foods higher in fat and sugar, which in turn may increase the risk of diabetes (Wen et al., 2014). These habits may be formed in households with little access to nutritious foods because those foods cost more to purchase or prepare, or because supermarkets with these foods are not located conveniently in urban or rural settings.
Food Insecurity for Households with Children
Food insecurity is a pervasive problem in the United States, especially for households with children. The U.S. Department of Agriculture defines food insecurity as a lack of consistent access to enough food for an active and healthy life. In 2016, for example, 13 million (1 in 6) U.S. children were food insecure; 85% of counties with high child food insecurity were rural. Table 4-2 provides a sense of the problem of food insecurity in the United States (National Academies, 2019).
Whereas nutritious foods are important sources of energy, fiber, protein, and key minerals and vitamins needed for healthy development, adequate food is more a measure of whether sufficient quantities of food are available for individuals and households over long periods of time in a sustained manner. Households often face a trade-off between (more costly) nutritious food and adequate quantities of food. Here again, disparities persist within the United States. Although evidence has shown the link between maternal and infant nutrition and children’s health and developmental outcomes, access to affordable nutritious food is often more likely to be limited for low-income communities and communities of color (National Academies, 2019).
Safe and Healthy Environments
As discussed previously, young children exist within the contexts of their families and neighborhoods, including the places where they live, learn, and play, and these environments need to be safe and healthy if children are to achieve optimal physical health, growth, and development. Health-promoting neighborhoods provide the physical and social conditions and community resources—social, economic, environmental, and
TABLE 4-2 Food Insecurity by Selected Household Characteristics
| Type of Household | Percentage of All Households (%) |
|---|---|
| Households with children | 12.5 |
| Households with children under 6 | 12.9 |
| Households with children headed by a single woman | 24.3 |
| Non-Hispanic Black households | 19.8 |
| Hispanic households | 16.2 |
| Non-Hispanic White households | 7.0 |
| Households with income below the federal poverty threshold | 32.1 |
SOURCE: Data from U.S. Department of Agriculture, 2022.
cultural—that enable young children to be healthy (CDC, 2009; National Academies, 2017). The Child Opportunity Index is a tool used to describe and quantify the neighborhood conditions experienced by U.S. children, ranking them from lowest to highest with regard to the opportunity they provide. Child Opportunity Scores rank all 72,000 neighborhoods in the United States from one to 100 according to this metric (Diversity Data Kids, 2019, Box 1-2). Child Opportunity Scores are also available for metro areas for use in assessing their level of opportunity overall and by race and ethnicity. The opportunity gap between very low- and very high-opportunity neighborhoods represents differences along important dimensions of neighborhood environment. Access to green space, for example, varies widely. In very low-opportunity neighborhoods, almost half of children (48%) lack access to parks and playgrounds, while in very high-opportunity neighborhoods, this is the case for fewer than a quarter of children (22%). As discussed previously, access to nature and to safe places to play is critical for children’s health and well-being (Acevedo-Garcia et al., 2019).
After reviewing some methodological considerations regarding the association between neighborhood and child health, this section looks at two specific aspects of neighborhoods thought to be linked most directly with young children’s physical health: freedom from environmental contaminants and safety and freedom from violence.
Methodological Considerations
It is important to note that the evidence the committee presents on the association between neighborhoods and child health is complex, and the existing literature is fraught with methodological challenges and pitfalls. For example, associations between neighborhood characteristics and child health may vary based on individual-level characteristics, such as a child’s race or immigration status, and effect estimates may be sensitive to the selection of covariates included in models (Paczkowski & Galea, 2010; Auchincloss et al., 2013; Meijer, Bloomfield, & Engholm, 2013; Blair et al., 2014). Given the correlation among different neighborhood factors—such as poverty, racial segregation, housing quality, and environmental contaminants—it is also difficult to separate out the effects of any single neighborhood factor. In addition, results vary widely depending on how a specific health outcome or neighborhood characteristic is measured, and many studies capture only limited subsets of neighborhood factors. As a result, it is difficult to identify specific interventions focused on altering specific neighborhood characteristics to target specific high-risk subgroups. Also, given that true randomized controlled trials are often unethical or infeasible in this realm, causal connections between neighborhood conditions and child health are challenging to validate (Oakes, 2004; Oakes et
al., 2015; Glass & Bilal, 2016; Jeffries et al., 2019). For example, existing studies may suffer from selection bias by which unhealthy versus healthy families are more likely to live in disadvantaged neighborhoods.
A handful of studies have overcome some of these methodological limitations. For example, the Moving to Opportunity study randomized families to receive a voucher to move to a low-poverty neighborhood. Analyses of the Moving to Opportunity study have found that children who moved to low-poverty neighborhoods when they were younger were more likely to experience positive social outcomes (e.g., college attendance) later in life, while children who moved at older ages experienced worse outcomes (Chetty, Hendren, & Katz, 2016). The Moving to Opportunity study also showed that girls experienced improved mental health (e.g., decreased risk of major depression), while boys experienced worse outcomes (e.g., increased rates of posttraumatic stress disorder) (Kessler et al., 2014). Yet despite the strength of its randomized study design, the Moving to Opportunity study could not tease apart which aspects of the neighborhood environment mattered, or why this differed for children of different ages and genders. Moreover, the number of physical health conditions examined was limited, and the sample was relatively small (4,604 families, with 98% of households headed by women), restricted to only five U.S. cities, and enrolled in the mid-1990s. Therefore, it may be necessary to address this issue with a broader range of quasi-experimental and observational studies, which of course would have to be interpreted cautiously.
In recent years, an increasing number of quasi-experimental studies have leveraged natural experiments in which families are quasi-randomly assigned to neighborhoods of different levels of disadvantage so the effects of neighborhood characteristics on health can be examined. For example, several studies have found negative health effects of neighborhood disadvantage among refugees quasi-randomly assigned to more deprived neighborhoods in Denmark and Sweden (White et al., 2016; Hamad et al., 2020; Raphael et al., 2020), including increased mental health problems among children (Foverskov et al., 2022). Other studies have examined the effects of the built environment on cardiometabolic disease among older adults forcibly displaced and quasi-randomly assigned to neighborhoods in the wake of the 2011 Great East Japan Earthquake and Tsunami (Shiba et al., 2020). Unfortunately, few of these quasi-experimental studies have focused on child health, and the circumstances underlying the natural experiment, including those just cited, are often “unnatural,” hinging on quasi-random variation generated by natural disasters or policies that typically are not generalizable (Hamad, 2020). Nevertheless, quasi-experimental studies provide a balance between randomized studies (which are challenging and/or unethical to conduct and yet methodologically rigorous) and observational studies (which are easier to conduct but can suffer from confounding/-
endogeneity), and future research could identify natural experiments with which to focus on child health in the context of U.S. settings in particular.
Environmental Contaminants
Child well-being is affected by environmental determinants related to pollutants and contaminants in the water; the air; and other aspects of a young child’s home, school, and play areas. Environmental contaminants have repeatedly been found to be associated with poor health throughout the life course, and the prenatal and early childhood periods represent particularly sensitive developmental windows in which individuals may be especially vulnerable to their effects. Young children may be exposed to thousands of potential contaminants, including through the air they breathe, the water they drink and use, the food they eat, and the consumer products with which they come into contact (Giudice, Woodruff, & Conry, 2017). While these substances may be present in the environment naturally, many are released through human-based processes such as manufacturing, fossil fuel use, and waste disposal (Di Renzo et al., 2015). This section looks at two specific subsets of contaminants—allergens and pollutants that cause asthma, and lead that affects neurological development and cognition—as well as evidence on environmental contaminants more generally.
Allergens/pollutants and asthma
Asthma is the most common chronic lung disease in U.S. children (Zahran et al., 2018). It is a serious health condition characterized by inflammation of the lungs and chronic respiratory symptoms such as shortness of breath and coughing, especially with physical activity. Not only does asthma impair quality of life and increase health care utilization, but it also contributes to more than 10.5 million missed days of school annually among U.S. children.
Poor housing conditions can lead to increased risk of asthma in several ways. Research has found links between asthma and cockroaches, dust mites, dampness, and mold (IOM, 2000; Wu & Takaro, 2007; Rauh, Landrigan, & Claudio, 2008). Other work has found an association of higher density of housing code violations and worse public housing conditions with increased risk of health care utilization related to exacerbation of asthma (Beck et al., 2014; Kersten et al., 2014).
Lead
Exposure to lead, even in small amounts, is associated with lower IQ and test scores, as well as increased incidence of impulsivity and attention-deficit/hyperactivity disorder (Needleman et al., 1979, 1990; Rauh, Landrigan, & Claudio, 2008; Leventhal & Newman, 2010; Muller, Sampson, & Winter, 2018). Such effects are thought to persist through to later in childhood and have been linked with high adolescent body mass index, impulsivity, anxiety, and depression, as well as lower earnings and criminal activity
in adulthood (Kim & Williams, 2017; Winter & Sampson, 2017). Exposure to lead among pregnant mothers has been linked with adverse birth outcomes, possibly through transmission to the fetus (Taylor, Golding, & Emond, 2015). Consistent with prior research on disparities, Black children in these studies have more elevated blood lead levels (BLLs) relative to White children (Miranda et al., 2009). In one study, only one in four Black children had a BLL of 3 micrograms per deciliter (μg/dL) or less, compared with almost half of White children. In a study of BLL and third-grade test scores, non-Hispanic Black students had a mean BLL of 7.7 μg/dL—more than twice that of non-Hispanic White students (3.7 μg/dL; Evens et al., 2015; National Center for Healthy Housing, 2013). Box 4-2 provides an example of how policy changes related to lead exposure succeeded in improving academic performance in children and reducing community-level inequality in Massachusetts.
Other environmental contaminants
Numerous other environmental contaminants have been linked to adverse health outcomes at birth and in early childhood. Chemicals from heavy metals and pesticides to carbon monoxide and ozone are thought to affect neurological development and
contribute to endocrine disruption, with wide-ranging negative effects on asthma as well as on child growth and development, obesity, sexual anatomy, and kidney disorders (Cox et al., 1989; Kalter, 2003; Vandenbergh, 2004; Diamanti-Kandarakis et al., 2009; Nakamura et al., 2012; Manikkam et al., 2013; Di Renzo et al., 2015; Gore et al., 2015; Webb et al., 2016; Weidemann, Weaver, & Fadrowski, 2016; Giudice, Woodruff, & Conry, 2017). The effects of hundreds of contaminants remain untested. Therefore, these contaminants may have both immediate impacts on health and wellness and long-term effects on chronic disease, educational attainment and achievement, and mortality.
Opportunity gaps related to environmental contaminants
As the evidence reported above demonstrates, children experience differing levels of exposure to environmental contaminants, such as lead and those that place them at risk of asthma. Exposures vary across an income and race gradient rooted in decades of discriminatory policies and programs. Children whose families have lower incomes and live in substandard housing are more likely to live in greater proximity to known sources of such contaminants, as are children from racial/ethnic minority and immigrant (particularly Latino) groups as a result of the chronic effects of structural racism (Oberg, Colianni, & King-Schultz, 2016; American College of Obstetricians and Gynecologists Committee on Obstetric Practice, 2021). Studies from the United States and other high-income countries also suggest that residence in urban versus rural areas affects the types and quantities of pollutants to which people are exposed (Northridge et al., 2003; Hendryx, Fedorko, & Halverson, 2010; Hulin, Caillaud, & Annesi-Maesano, 2010).
An example is particulate matter 2.5 micrometers or less in diameter (PM2.5), which places children at higher risk of asthma. People living in poverty and people of color are exposed to significantly higher levels of PM2.5 compared with White individuals (Mikati et al., 2018). Another study found that White individuals experience a “pollution advantage” more generally in that they have 17% less exposure to air pollution on average when the amount to which they are exposed is compared with the amount for which they are responsible; conversely, Black and Latino Americans experience 56% and 64% excess exposure, respectively, when the same comparison is made (National Academies, 2019; Tessum et al., 2019). These inequities persist even as exposure to pollution on average is declining as a result of increased regulation and a shift in population density away from polluted areas. The net result is large racial and socioeconomic disparities in the prevalence of asthma in the United States. Prevalence is highest among Black people (11.1% compared with 8.2% in the population overall), and Black individuals are more than three times more likely than White individuals to visit an emergency department for asthma care (Akinbami, Moorman, & Liu, 2011). And while child deaths from asthma
are rare, they are roughly 10 times more likely for Black than for White children (Pate et al., 2021).
Similarly, while more than half a million U.S. children aged 1–5 have BLLs above the reference range according to the most recent prevalence estimates (from 1999 to 2010), this risk is not distributed equally across all groups of children (Wheeler & Brown, 2013). Black children are more than twice as likely as their White peers to have a BLL above 5 µg (5.6% vs. 2.4%), and those who live in poverty or have Medicaid coverage are nearly eight times as likely to have elevated BLLs (Wheeler & Brown, 2013). Even after correcting for risk factors and other variables, such as housing, socioeconomic, status, and age, Black versus White children nationwide have BLLs 1.8 to 5.6 times higher within each risk factor subgroup (Yeter, Banks, & Aschner, 2020).
The primary reason for differential exposures to environmental contaminants is proximity to sources of pollutants, such as traffic and roadways, industrial facilities, power plants, and natural gas wells, that repeatedly have been associated with worse health outcomes for children, including adverse birth outcomes and asthma in particular (Ahmad et al., 2001; Hopenhayn et al., 2003; Tsai et al., 2004; Salam, Islam, & Gilliland, 2008; Clark et al., 2010; Pénard-Morand et al., 2010; Currie & Walker, 2011; Padula et al., 2012; Miranda et al., 2013; Ha et al., 2015; Woodward, Finch, & Morgan, 2015; Casey et al., 2016; Harris et al., 2016; Alexander & Currie, 2017; Fleisch et al., 2017). Proximity to sources of pollutants is in turn determined by other, more upstream risk factors, most notably family poverty, neighborhood poverty and disadvantage, and residential segregation driven by structural racism in housing policies, discussed in turn below.
Families that live in poverty are naturally less likely to be able to afford housing that is high quality (e.g., free of lead and asbestos) and located farther from sources of pollutants (Sandel et al., 2004; Rauh, Landrigan, & Claudio, 2008). Living in older housing also means that outdoor pollutants are more likely to enter the home (Houston et al., 2016). Thus lower-income neighborhoods are more likely to have higher levels of ambient air pollution, while at the same time they have fewer air quality monitoring resources (Stuart, Mudhasakul, & Sriwatanapongse, 2009; Houston et al., 2016).
Like family poverty, neighborhood poverty and disadvantage, experienced disproportionately by families of color, is associated with poor-quality housing and a higher risk of lead contamination (Baek et al., 2021). Although lead paint was banned in 1978, exposure remains high among children living in older homes (particularly in the Northeastern and Midwestern United States), where the paint can peel and be ingested, and
among those living close to certain types of manufacturing sites (Rauh, Landrigan, & Claudio, 2008; Muller, Sampson, & Winter, 2018).
Residential segregation is a persistent feature of U.S. neighborhoods, driven by historical racist practices and policies such as redlining and discriminatory banking practices (National Academies, 2017). Although these policies are no longer entrenched in the legal system, their effects are persistent and demonstrated by the continued segregation of many U.S. neighborhoods. These patterns have contributed to the higher levels of poverty and disadvantage experienced by segregated Black neighborhoods because of their limited access to health-promoting resources, including those for children (Acevedo-Garcia et al., 2007, 2008), as well as their greater likelihood of being in proximity to potential pollutants and environmental hazards and of having poor-quality housing (National Academies, 2019).
Safe and Violence-free Environments
Children need environments in which to grow, develop, and thrive that are safe with respect to prevention of unintentional injuries, as well as exposure to violence—whether that exposure is primary (i.e., direct victimization by adults or peers) or secondary (i.e., witnessing violence in the home or community). Young children’s exposure to violence in their home or neighborhood is likely to create additional obstacles to their long-term well-being.
Maltreatment
Statistics reported for federal fiscal year 2019 document 656,000 victims of child abuse and neglect nationally, which equates to a national rate of 8.9 victims per 1,000 children in the population. The Centers for Disease Control and Prevention (CDC) estimates that in 2019, about 1 in 7 children were affected by maltreatment, and 1,840 of these children died as a result (Department of Health and Human Services, Administration for Children and Families, & Administration on Children, Youth and Families, Children’s Bureau, 2021). The youngest children are the most vulnerable to maltreatment: nationally, more than one-quarter (28.1%) of victims are aged 0–2 years. Among school-based children, African American students, students who qualify for free/reduced-price lunch (i.e., those from families with low incomes), students living in relatively high-poverty areas, and students attending urban schools all have an elevated likelihood of being investigated by Child Protective Services for suspected child maltreatment (Jacob & Ryan, 2018). Maltreatment in early childhood is associated with significantly worse academic outcomes, even after controlling for school, neighborhood, race, and other key demographics (Jacob & Ryan, 2018). The total lifetime economic cost associated with child maltreatment in terms of worse outcomes, lower educational
attainment, lower probability of employment, and high disability rates was estimated to be about $428 billion in 2015.
The Nurse-Family Partnership (NFP) is often cited as an effective intervention for preventing child abuse and neglect. This program provides nurse home visits to pregnant women with no previous live births, most of whom are: (1) low income, (2) unmarried, and (3) teenagers. The nurses visit the women once or twice per month during their pregnancy and the first two years of their children’s lives (Arnold Ventures, 2020). Data on the outcomes of the program in Elmira, New York, and Memphis, Tennessee, show that it reduced verified incidences of abuse and reduced hospitalizations for injuries in young children. Treatment families reported statistically significant decreases in child abuse/neglect and domestic violence and improvements in home learning environments compared with control families.
Injuries
Injuries are a leading cause of death among children in the United States, and data on these deaths reveal prominent racial disparities (CDC, 2021). According to a CDC report based on data from 2000–2009, American Indian/Alaska Native children had the highest death rate from injuries at 30.4 per 100,000 in 2000 and 23.8 per 100,000 in 2009—nearly double the rates among Black children (16.2 and 12.8, respectively), the population with the next-highest rate in 2009 (Gilchrist, Ballesteros, & Parker, 2012). There is also a more than sixfold gap between the lowest and highest rates across states (from 4.0 per 100,000 in Massachusetts to 25.1 per 100,000 in Mississippi).
The impact of injury and injury severity on academic outcomes can be substantial. Following an injury, a young person’s ability to learn and concentrate can be interrupted, future learning can be affected, and injuries resulting in physical disability have been shown to negatively influence cognitive skills (Ewing-Cobbs et al., 2006; Vu, Babikian, & Asarnow, 2011; Fulton et al., 2012; Kingery et al., 2017; Prasad, Swank, & Ewing-Cobbs, 2017; Treble-Barna et al., 2017). Aside from problems with cognitive performance, seriously injured young people may also experience psychological and physical health problems that can adversely affect their academic performance (Foster et al., 2019a,b). Results of one large population-based study (involving more than 150,000 injured children) suggest that while some young people may fully recover after their injury, others may experience ongoing adverse effects on their school-based academic performance. Overall, injured young people demonstrate poorer performance on school assessments, with increasing injury severity having a greater negative impact. In addition, one study found that injured young people had almost twice the risk of not completing high school compared with their uninjured matched peers (Mitchell et al., 2021).
Exposure to violence
Exposure to violence is disturbingly prevalent among U.S. children. Data from the National Survey of Children’s Exposure
to Violence (2013–2014) show that 37.3% of children had experienced physical assault in the past year; 51.4% had experienced physical assault in their lifetime; and 24.5% and 38.3% had witnessed violence in the past year and in their lifetime, respectively (Finkelhor et al., 2015). Black children have the highest exposure to violence in their communities—9.5% among children aged 5–12, compared with 6.9% for White and 5.7% for Hispanic children (Ullmann, Weeks, & Madans, 2021). Boys are at higher risk than girls.
Opportunity gaps related to safety and exposure to violence
Several factors may explain the above disparities in young children’s exposure to violence; they include individual, family, and place-based risk factors. On an individual level, babies under 1 year old experience higher rates of injuries and maltreatment (CDC, 2014, 2021). Children with disabilities also are at increased risk, having more than three times greater odds of being victims of violence compared with their peers without disabilities (Jones et al., 2012). In these latter cases, it is likely that increased family conflict and parenting challenges contribute to the greater risk.
At the family level, poverty and structural racism lead to higher levels of chronic stress that may contribute to greater family tensions, which in turn have been found to be associated with increased levels of child maltreatment and violence (Jewkes, 2002; Foster, Brooks-Gunn, & Martin, 2007; Stith et al., 2009). Families living in poverty and parents with limited educational attainment may also be less able to acquire health-promoting resources that can protect against injuries, such as the ability to afford or properly install car seats or to perform adequate childproofing in the home. Similarly, as noted earlier, poverty and structural racism may affect the ability to afford high-quality housing, which is more likely to have appropriate safety measures in place (Reading, Haynes, & Shesnassa, 2005).
Place-based characteristics also contribute to potentially unsafe environments. In addition to the issues with housing quality mentioned above, disadvantaged neighborhoods tend to be the recipients of poor urban planning, with roadways and traffic patterns contributing to traffic injuries (Morency et al., 2012). As noted previously, the distribution of health-promoting community characteristics is racially and socially patterned as a result of historical segregation, placing low-income children and children of color at high risk of exposure to such hazards. The geographic disparities across states discussed above also suggest that aspects of the social and physical environments may play a role, including exposure to place-based hazards (e.g., vehicle-miles traveled, exposure to water settings, urban versus rural environment) and differences in public policy (e.g., gun legislation; Ullmann, Weeks, & Madans, 2021). Additional research is needed to clarify what aspects of disadvantaged neighborhoods are most important to address in this regard (Newgard et al., 2011).
Finally, police brutality, especially in segregated Black, Latino, and Indigenous communities, is a significant driver of health problems in these populations. Beyond police-inflicted violence, these community tensions can also worsen mental health problems among residents, as well as affect downstream outcomes relevant to child health, such as prenatal outcomes among Black women (Alang et al., 2017).
Gun violence is now the leading cause of death for all children and teens aged 1–19 (Figure 4-1). According to the CDC, nearly two-thirds of the 4,368 U.S. children up to age 19 who were killed by guns in 2020 were homicide victims (CDC, 2020). In that year, by comparison, motor vehicle crashes, formerly the leading cause of death for children aged 1 and above, killed nearly 4,000 children. While mass shootings garner the attention of the public and policy makers, routine gunfire kills more children each week than died in the Columbine, Sandy Hook, and Parkland massacres combined. Here, too, there are stark racial disparities. Black children and teens are four times more likely than their White peers to die from gun violence.
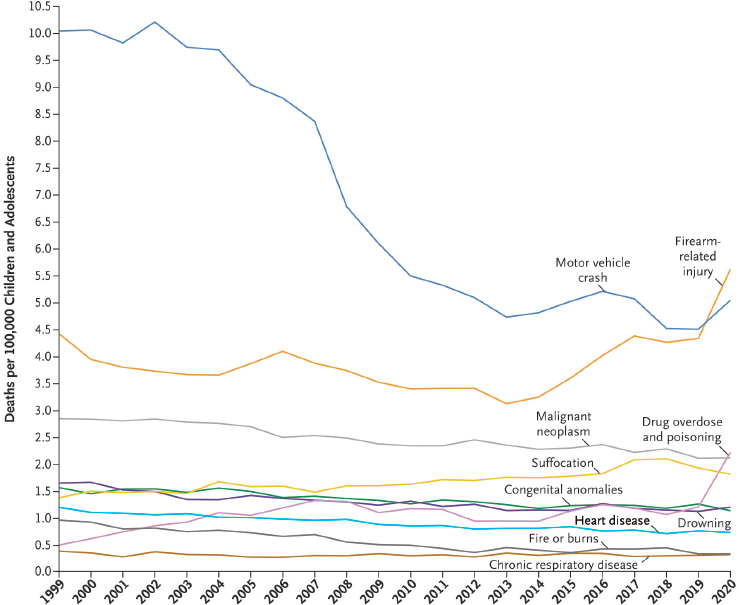
SOURCE: Goldstick, Cunningham, & Carter, 2022.
U.S. mortality rates among children due to gun violence are the highest across high-income countries and are thought to be due to this country’s having the least restrictive gun policies, higher rates of gun ownership, and types of guns available to the public. Differences in state-level gun control policies are also associated with differences in firearm-related morbidity and mortality among children (Rudolph et al., 2015; Raifman et al., 2020).
The consequences of gun violence are pervasive, affecting entire communities in addition to families and children. More than 25% of children witnessed an act of violence in their home, school, or community during 2009, and more than 5% witnessed a shooting. Beyond gun regulation, then, it is essential to address the impact on those who have been injured and traumatized by such violence (Finkelhor et al., 2009; Children’s Defense Fund, 2022; Collins and Swoveland, 2022; Goldstick, Cunningham, & Carter, 2022).
While the majority of children who experience injuries or are exposed to violence recover, they often suffer short- and long-term consequences (Schneeberg et al., 2016). Long-term consequences may include impacts on their physical health (e.g., physical disability, asthma, blood pressure), mental health (e.g., posttraumatic stress disorder, sleep disorders), and cognitive health (e.g., cognitive performance, attention disorders). Some of these effects are direct consequences of the injury or violence itself, while others are due to missing school during recovery, and still others are mediated by the impact of stress on dysregulation of biological pathways involving the hypothalamic-pituitary-adrenal axis and autonomous nervous system (Brunton, 2013; Provençal & Binder, 2015; Theall et al., 2017; McGowan and Matthews, 2018; van den Bergh, Dahnke, & Mennes, 2018). Moreover, children exposed to one incident of violence are more likely to be exposed again, including to other forms of violence (Finkelhor, Ormrod, & Turner, 2007; Finkelhor et al., 2009, 2015).
ADDRESSING OPPORTUNITY GAPS IN PHYSICAL HEALTH AND HEALTH CARE
Opportunity gaps in the physical health and health care of young children can be addressed through efforts focused on poverty reduction, access to pediatric and family health care, antiracism and dismantling of race-based medicine, screening for social influences on health, alternative models for delivering health care, and safe and violence-free environments.
Poverty Reduction
As described throughout previous sections of this chapter, poverty is a major contributor to various opportunity gaps for young children—for
example, by affecting housing quality, access to health care, and educational settings. Poverty reduction is therefore a major promising focus of efforts to reduce these gaps. According to a prior National Academies report on child poverty (National Academies, 2019), three general sets of forces affect poverty: (1) demographics (e.g., parental age and household size), (2) the economy (e.g., labor markets), and (3) government policy. While the first two forces are challenging to address through interventions, studies of government policy demonstrate promising avenues for programs aimed at reducing child poverty. The above National Academies report reviews in detail the evidence behind such policies and practices, and we briefly summarize them here.
Among those federal governmental programs specifically designed to address poverty are the earned income tax credit, the child tax credit, and the Supplemental Nutrition Assistance Program, which provide cash or in-kind transfers to low-income families, and all of which have been shown to reduce poverty and improve child health outcomes. The temporary expansion of the child tax credit in response to the COVID-19 pandemic had a significant impact on poverty alleviation, reducing child poverty by about 30% and decreasing food insufficiency, with implications for the well-being of many of the nation’s most vulnerable children. This expansion has expired, although several states are considering their own child tax credits (Shafer et al., 2022). Indeed, state and local governments have been active in policy making to reduce child poverty, including state supplements to the federal earned income tax credit and programs designed to increase take-up and use of benefits. Nongovernmental organizations have also been active players in pursuing poverty reduction, including by funding research and programs focused on understanding and addressing determinants of low take-up of safety net benefits.
Access to Pediatric and Family Health Care
Research demonstrates that healthy child development begins prior to conception and is dependent upon a strong prenatal foundation. Research has shown, for example, that a family’s access to high-quality resources for limiting chronic stress reduces the risk for disrupted development and can alleviate disparities based on race/ethnicity and socioeconomic status (National Academies, 2019). To address psychosocial adversities and social determinants of health within the medical home, providers need culturally competent care models, mental health expertise on the team, and training in screening for and addressing psychosocial adversity (Bair-Merritt et al., 2015). In addition, medical homes need to link intentionally with community-based resources and centralized, colocated community services
to optimize transitions in care, promote care coordination, and address health-related social needs (Garg et al., 2012).
Antiracism and Dismantling of Race-based Medicine
Medical providers who receive ongoing training in culturally and linguistically competent care are better able to provide appropriate care to diverse populations (National Academies, 2017). Health care systems can prioritize efforts to address inequities in health and institutional and structural racism by continually reviewing policies, protocols, and strategies, as well as promoting antiracist practices and working to develop trustworthy institutions.
Race-based medicine is a clear driver of opportunity gaps in medical treatment and care. Antiracism is an active practice that involves learning about how racism is constructed, operationalized, and perpetuated and working to dismantle those systems. A number of steps could be taken to dismantle race-based medicine, some of which were discussed earlier in this chapter. They include abandoning the use of race in clinical algorithms and incorporating more complex and nuanced understandings of racism and its impact on health outcomes. In addition, reform of standardized examinations and board exams for medical professionals could eliminate testing on race-based guidelines and racial heuristics. Medical institutions, medical societies, and health care providers could work to advance their recognition of racism in medical research, education, training, and practice, and implement infrastructure for accountability in this regard and motivation to contribute to change. Providers could use clear language to describe racism and racial justice and serve as role models in their own efforts to reduce racial bias.
Screening for Social Influences on Health
The long-term impacts of social adversities on population health are increasingly acknowledged, as is the importance of screening for “health-related social needs” to address social determinants of health (Billioux et al., 2017). Screening for these needs in the pediatric setting holds particular promise for its primary prevention power (Gottlieb, Sandel, & Adler, 2013).
Effective screening is indispensable if pediatric health care providers are to identify and address health-related social needs, thereby helping to prevent and mitigate the health effects of social adversity for families, for children, and for the adults that children will become. These efforts include screening for both risk and protective factors, engaging families and communities in developing screening tools and protocols, establishing person-centered screening priorities for health-related social needs, ensuring that screening is conducted by staff members trained in strengths-based
approaches, recognizing that screening is not risk-free for families, and acknowledging family-level risks in a broader historical context (Chung et al., 2016; Andermann, 2018; Flacks & Boynton-Jarrett, 2018; Gears et al., 2021). In addition, providers can ensure that they have the tools to make appropriate referrals to social and other community services if screening results in the identification of such nonmedical needs.
Alternative Models for Delivering Health Care
Group visits for preventive care, in which a group format is used for six to eight families with similarly aged children, have been studied for nearly 50 years (Osborn & Woolley, 1981; Dodds et al., 1993; Rice & Slater, 1997; Taylor, Davis, & Kemper, 1997a,b; Taylor & Kemper, 1998; Jones et al., 2018; Gullett et al., 2019; Fenick et al., 2020). Group visits have also been suggested in systematic and narrative reviews as an effective alternative format for preventive care for young children, particularly for low-income families (Coker et al., 2013; Oldfield, Rosenthal, & Coker, 2020). In group visits, families receive preventive care in a supportive group setting; have more time with providers than they would in an individual visit; and are more likely to have their social, behavioral, and developmental needs addressed (Oldfield, Rosenthal, & Coker, 2020). Yet despite the evidence of effectiveness for group visits, this format for child preventive care has not been widely implemented. There remains a critical need for research comparing models for delivering primary care and examining their impact on racial/ethnic and socioeconomic inequities in preventive care utilization and health outcomes.
Safe and Violence-free Environments
Given the numerous risk factors that place children at higher risk of exposure to unsafe environments, individual and family interventions are unlikely to be sufficient; multilevel societal interventions and policies are needed.
At the family level, counseling and support to alleviate family tension can help reduce the risk of interpersonal violence. In addition, counseling in a health care setting can educate families about restraints for children in vehicles, firearm safety, drowning risks, and other aspects of home safety. Interventions can also address the upstream determinants of family conflict, such as poverty and unemployment, through policies to increase income and promote labor force participation. As noted earlier, for example, the child tax credit and earned income tax credit have been found to improve household resources and reduce child injuries and neglect (Hamad
& Rehkopf, 2016; Klevens et al., 2017; Averett & Wang, 2018; Rostad et al., 2020; Kovski et al., 2022).
At the community level, increasing the supply of high-quality affordable housing can help improve the safety of homes (National Academies, 2019). Additionally, school and health care systems can serve as anchor institutions to help address the root causes of unsafe environments, including housing insecurity, blight, and crime, by supporting neighborhood development (Sharkey, Torrats-Espinosa, & Takyard, 2017; Kelleher, Reece, & Sandel, 2018). Urban planning can improve road safety and prevent traffic and pedestrian deaths among children. Also at the community level, evidence-based programs for young people can be implemented, such as those that include tutoring or mentoring, sports, cognitive-behavioral therapy, and summer jobs, which randomized controlled trials have shown lead to decreased involvement in crime and violence (National Academies, 2019). Finally, to address police brutality that children may witness, better data are needed on the epidemiology of deaths and injuries at the hands of police to inform possible interventions, such as demilitarization or decriminalizing of such behaviors as loitering (Krieger et al., 2015; Alang et al., 2017).
At the policy level, there are multiple ways to address risk factors farther upstream at the population level. To address traffic injuries, for example, policy makers could enact legislation to reduce speed limits, while policies targeting playground injuries could include legislation and enforcement of appropriate standards to reduce risk. Government could also test new Medicaid payment models that would engage providers and other community organizations in addressing housing safety concerns, especially those focused on young children (National Academies, 2019). The World Health Organization’s World Report on Child Injury Prevention provides additional detail on evidence-based interventions for each of the primary types of injury, including those that are beyond the scope of the present report (Peden et al., 2008).
CONCLUSIONS
Healthy birth, medical care, nutrition, and safe and healthy environments are key determinants in ensuring that children have optimal physical health. In all of these cases, however, notable disparities exist by race/ethnicity, income, rural versus urban residence, and immigration status.
In the prenatal period, adverse outcomes experienced by children and birthing people are often due to preventable pregnancy and birth complications, inadequate access to health insurance, and suboptimal prenatal care. These outcomes can have lifelong consequences for children’s health and well-being. Early life, including the in utero and even preconception periods, includes critical points during which exposures can influence the trajectory
of physical health. Gaps in opportunities intertwine and build on each other over the life course and across generations. Economic insecurity, for example, drives adverse birth outcomes, which then become determinants of later-life challenges that can impact educational experiences.
Proper nutrition plays a large role in physical development, and young children are the most vulnerable to nutrition deficits given the important developmental changes that occur during the first years of life. Existing programs and tax credit policies play an important role for the poorest children, and recent extensions to these programs may help reduce child hunger and poor nutrition. Children also need safe environments in which to grow, develop, and thrive. They need to have stable and secure housing. Their homes and places of play and schooling need to be free from contaminants (e.g., lead) and allergens (e.g., mold), and from exposure to violence and unsafe conditions.
As noted in other chapters of this report, access to high-quality care and programs that can aid in meeting the above needs can vary significantly from state to state. Programs administered at the state level, such as Medicaid, have differing criteria for eligibility that limit access in ways that affect both parents and children. Lack of access to adequate health care in the early years reduces opportunities to screen for, identify, and intervene on a number of health and developmental concerns. Failure to provide these opportunities early in life can lead to worse outcomes or exacerbate health issues that are cause for concern. Children of color and those from lower-income households are more likely to experience these opportunity gaps. The COVID-19 pandemic and related policies, such as school closures, exacerbated these disparities, because of both the disproportionate burden of disease experienced by low-income communities and people of color and the further limitations placed on access to key material and psychosocial resources among marginalized groups.
Stable access to quality health care is essential for child health and development. For young children, health care involves communication and relationships between clinical systems and caregivers. It is important to understand, however, that the broader social and political context impacts engagement with the health care system for families. Critical to a child’s optimal physical health and development are equitable access to a stable medical home, one that provides health promotion and preventive care and is patient and family centered, and a social context that supports child, caregiver, and family well-being. Also essential to the development and well-being of children in their early years is having healthy and well-cared-for parents. The absence of these conditions lays the foundation for opportunity gaps in physical and cognitive well-being in the early years that can persist into adolescence and adulthood.
REFERENCES
Abel, K.M., Wicks, S., Susser, E.S., Dalman, C., Pedersen, M.G., Mortensen, P.B., & Webb, R.T. (2010). Birth weight, schizophrenia, and adult mental disorder: Is risk confined to the smallest babies? Archives of General Psychiatry, 67(9), 923–30. https://doi.org/10.1001/archgenpsychiatry.2010.100
Acevedo-Garcia, D., McArdle, N., Tosypuk, T.L., Lefkowitz, B., & Krimgold, B.K. (2007). Children left behind: How metropolitan areas are failing America’s children. Harvard School of Public Health and the Center for the Advancement of Health. Available: https://escholarship.org/uc/item/28t4f2p4
Acevedo-Garcia, D., Osypuk, T.L., McArdle, N., & Williams, D.R. (2008). Toward a policy-relevant analysis of geographic and racial/ethnic disparities in child health. Health Affairs, 27(2), 321–33. https://doi.org/10.1377/hlthaff.27.2.321
Acevedo-Garcia, D., McArdle, N., Noelke, C., Huber, R., Huntington, N., & Sofer, N. (2019). The child opportunity gap: Inequities in child opportunity within metros. Brandeis University. Available: https://www.diversitydatakids.org/research-library/data-visualization/child-opportunity-gap
Adler, N.E., & Stewart, J. (2010). Health disparities across the lifespan: Meaning, methods, and mechanisms. Annals of the New York Academy of Sciences, 1186(1), 5–23. https://doi.org/10.1111/j.1749-6632.2009.05337.x
Ahmad, S.A., Sayed, M.H., Barua, S., Khan, M.H., Faruquee, M.H., Jalil, A., Hadi, S.A., & Talukder, H.K. (2001). Arsenic in drinking water and pregnancy outcomes. Environmental Health Perspectives, 109(6), 629–31. https://doi.org/10.1289/ehp.0110962
Akinbami, L.J., Moorman, J.E., & Liu, X. (2011). Asthma prevalence, health care use, and mortality: United States, 2005–2009. National Health Statistics Reports, 32. Washington, DC: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics.
Alang, S., McAlpine, D., McCreedy, E., & Hardeman, R. (2017). Police brutality and black health: Setting the agenda for public health scholars. American Journal of Public Health, 107(5), 662–5. https://doi.org/10.2105/AJPH.2017.303691
Alexander, D., & Currie, J. (2017). Is it who you are or where you live? Residential segregation and racial gaps in childhood asthma. Journal of Health Economics, 55, 186–200. https://doi.org/10.1016/j.jhealeco.2017.07.003
Alhusen, J.L., Bower, K.M., Epstein, E., & Sharps, P. (2016). Racial discrimination and adverse birth outcomes: An integrative review. Journal of Midwifery & Women’s Health, 61(6), 707–20. https://doi.org/10.1111/jmwh.12490
Ali, M.M., West, K., Teich, J.L., Lynch, S., Mutter, R., & Dubenitz, J. (2019). Utilization of mental health services in educational setting by adolescents in the United States. Journal of School Health, 89(5), 393–401. https://doi.org/10.1111/josh.12753
Almond, D., & Currie, J. (2010). Human capital development before age five. (Working Paper No. 15827). National Bureau of Economic Research. Available: https://www.nber.org/papers/w15827
Almond, D., Hoynes, H., & Whitmore Schanzenbach, D. (2011). Inside the war on poverty: The impact of food stamps on birth outcomes. The Review of Economics and Statistics, 93(2), 387–403. http://www.jstor.org/stable/23015943
American Academy of Pediatrics. (2015). A medical home where everybody knows your name: What is a medical home? HealthyChildren. Available: https://healthychildren.org/English/family-life/health-management/Pages/A-Medical-Home-Where-Everybody-Knows-Your-Name.aspx
American College of Nurse-Midwives. (2021). Congress reintroduces black maternal health “momnibus” legislative package. Available: https://www.midwife.org/congress-reintroduces-black-maternal-health-momnibus-legislative-package
American College of Obstetricians and Gynecologists Committee on Obstetric Practice. (2021). Reducing prenatal exposure to toxic environmental agents. Opinion No. 832. Obstetrics and Gynecology, 138(1), e40–54. https://doi.org/10.1097/AOG.0000000000004449
American Medical Association. (2021). AMA adopts guidelines that confront systemic racism in medicine. (Press Release). Available: https://www.ama-assn.org/press-center/press-releases/ama-adopts-guidelines-confront-systemic-racism-medicine
American Public Health Association. (2021). Expanding Medicaid coverage for birthing people to one year postpartum. (Policy No. LB21-02). Available: https://www.apha.org/Policies-and-Advocacy/Public-Health-Policy-Statements/Policy-Database/2022/01/07/Expanding-Medicaid-Coverage-for-Birthing-People-to-One-Year-Postpartum
Amutah, C., Greenidge, K., Mante, A., Munyikwa, M., Surya, S.L., Higginbotham, E., Jones, D.S., Lavizzo-Mourey, R., Roberts, D., Tsai, J., & Aysola, J. (2021). Misrepresenting race—The role of medical schools in propagating physician bias. New England Journal of Medicine, 384(9), 872–8. https://doi.org/10.1056/NEJMms2025768
Andermann, A. (2018). Screening for social determinants of health in clinical care: Moving from the margins to the mainstream. Public Health Reviews, 39(1), 1–17. https://doi.org/10.1186/s40985-018-0094-7
Anker, B., Tripodis, Y., Long, W.E., & Garg, A. (2018). Income disparities in the association of the medical home with child health. Clinical Pediatrics, 57(7), 827–34. https://doi.org/10.1177/0009922817733697
Ansell, D.A., & McDonald, E.K. (2015). Bias, black lives, and academic medicine. New England Journal of Medicine, 372(12), 1087–9. https://doi.org/10.1056/NEJMp1500832
Arnold Ventures. (2020). Social programs that work review: Evidence summary for the nurse family partnership. Available: https://evidencebasedprograms.org/document/nurse-family-partnership-nfp-evidence-summary
Auchincloss, A.H., Mujahid, M.S., Shen, M., Michos, E.D., Whitt-Glover, M.C., & Diez Roux, A.V. (2013). Neighborhood health-promoting resources and obesity risk (the multi-ethnic study of atherosclerosis). Obesity, 21(3), 621–8. https://doi.org/10.1002/oby.20255
Averett, S., & Wang, Y. (2018). Effects of higher EITC payments on children’s health, quality of home environment, and noncognitive skills. Public Finance Review, 46(4), 519–57. https://doi.org/10.1177/1091142116654965
Baek, M., Outrich, M.B., Barnett, K.S., & Reece, J. (2021). Neighborhood-level lead paint hazard for children under 6: A tool for proactive and equitable intervention. International Journal of Environmental Research and Public Health, 18(5), 2471. https://doi.org/10.3390/ijerph18052471
Baetzel, A., Brown, D.J., Koppera, P., Rentz, A., Thompson, A., & Christensen, R. (2019). Adultification of black children in pediatric anesthesia. Anesthesia and Analgesia, 129(4), 1118–23. https://doi.org/10.1213/ANE.0000000000004274
Bailey, Z.D., Krieger, N., Agénor, M., Graves, J., Linos, N., & Bassett, M.T. (2017). Structural racism and health inequities in the USA: Evidence and interventions. Lancet, 389(10077), 1453–63. https://doi.org/10.1016/S0140-6736(17)30569-X
Bair-Merritt, M.H., Mandal, M., Garg, A., & Cheng, T.L. (2015). Addressing psychosocial adversity within the patient-centered medical home: Expert-created measurable standards. The Journal of Primary Prevention, 36(4), 213–25. https://doi.org/10.1007/s10935-015-0390-7
Batstone, K. (2021). The Momnibus Act: Improving black maternal health outcomes by increasing doula and midwifery accessibility. National Women’s Health Network. Available: https://nwhn.org/the-momnibus-act-improving-black-maternal-health-outcomes-by-increasing-doula-and-midwifery-accessibility/
Bear, K., Braveman, P., Dixon-Roman, E., Iruka, I.U., Laraque-Arena, D., LaVeist, T., Murray, V.M., Rodriguez, L.J., & Taylor, S. (2022). Dismantling systemic racism and advancing health equity throughout research infrastructures. NAM Perspectives. National Academy of Medicine. Available: https://nam.edu/dismantling-systemic-racism-and-advancing-health-equity-throughout-research/
Beck, A.F., Huang, B., Chundur, R., & Kahn, R.S. (2014). Housing code violation density associated with emergency department and hospital use by children with asthma. Health Affairs, 33(11), 1993–2002. https://doi.org/10.1377/hlthaff.2014.0496
Bélanger, R., Mayer-Crittenden, C., Minor-Corriveau, M., & Robillard, M. (2018). Gross motor outcomes of children born prematurely in northern Ontario and followed by a neonatal follow-up programme. Physiotherapy Canada, 70, 1–7. https://doi.org/10.3138/ptc.2017-13
Ben-Shlomo, Y., Mishra, G., & Kuh, D. (2014). Life course epidemiology. Handbook of Epidemiology. Springer. Available: https://doi.org/10.1007/978-0-387-09834-0_56
Bertagnolli, M., Luu, T.M., Lewandowski, A.J., Leeson, P., & Nuyt, A.M. (2016). Preterm birth and hypertension: Is there a link? Current Hypertension Reports, 18(4), 28. https://doi.org/10.1007/s11906-016-0637-6
Bethell, C., Reuland, C.H., Halfon, N., & Schor, E.L. (2004). Measuring the quality of preventive and developmental services for young children: National estimates and patterns of clinicians’ performance. Pediatrics, 113(6 Suppl), 1973–83. https://doi.org/10.1542/peds.113.S5.1973
Bethell, C., Reuland, C., Schor, E., Abrahms, M., & Halfon, N. (2011). Rates of parent-centered developmental screening: Disparities and links to services access. Pediatrics, 128(1), 146–55. https://doi.org/10.1542/peds.2010-0424
Bethell, C., Jones, J., Gombojav, N., Linkenbach, J., & Sege, R. (2019). Positive childhood experiences and adult mental and relational health in a statewide sample: Associations across adverse childhood experiences levels. JAMA Pediatrics, 173(11), e193007, 1–10. https://doi.org/10.1001/jamapediatrics.2019.3007
Bhutta, A.T., Cleves, M.A., Casey, P.H., Cradock, M.M., & Anand, K.J. (2002). Cognitive and behavioral outcomes of school-aged children who were born preterm: A meta-analysis. Journal of the American Medical Association, 288(6), 728–37. https://doi.org/10.1001/jama.288.6.728
Billioux, A., Verlander, K., Anthony, S., & Alley, D. (2017). Standardized screening for health-related social needs in clinical settings: The accountable health communities screening tool. Discussion Paper. NAM Perspectives. National Academy of Medicine. https://doi.org/10.31478/201705b
Blair, A., Ross, N.A., Gariepy, G., & Schmitz, N. (2014). How do neighborhoods affect depression outcomes? A realist review and a call for the examination of causal pathways. Social Psychiatry and Psychiatric Epidemiology, 49(6), 873–87. https://doi.org/10.1002/oby.20255
Bonamy, A.K., Holmström, G., Stephansson, O., Ludvigsson, J.F., & Cnattingius, S. (2013). Preterm birth and later retinal detachment: A population-based cohort study of more than 3 million children and young adults. Ophthalmology, 120(11), 2278–85. https://doi.org/10.1016/j.ophtha.2013.03.035
Bower, K.M., Geller, R.J., Perrin, N.A., & Alhusen, J. (2018). Experiences of racism and preterm birth: Findings from a pregnancy risk assessment monitoring system, 2004 through 2012. Womens Health Issues, 28(6), 495–501. https://doi.org/10.1016/j.whi.2018.06.002
Braun, L. (2014). Breathing race into the machine: The surprising career of the spirometer from plantation to genetics. University of Minnesota Press. https://doi.org/10.5749/minnesota/9780816683574.001.0001
Braveman, P., Dominguez, T.P., Burke, W., Dolan, S.M., Stevenson, D.K., Jackson, F.M., Collins, J.W., Driscoll, D.A., Haley, T., Acker, J., Shaw, G.M., McCabe, E.R.B., Hay, W.W., Thornburg, K., Acevedo-Garcia, D., Cordero, J.F., Wise, P.H., Legaz, G., Rashied-Henry, K., Frost, J., Verbiest, S., & Waddell, L. (2021). Explaining the black-white disparity in preterm birth: A consensus statement from a multi-disciplinary scientific work group convened by the March of Dimes. Frontiers in Reproductive Health, 3. https://doi.org/10.3389/frph.2021.684207
Bronfenbrenner, U. (1979). Contexts of child rearing: Problems and prospects. American Psychologist, 34(10), 844–50. https://doi.org/10.1037/0003-066X.34.10.844
Brunton, P.J. (2013). Effects of maternal exposure to social stress during pregnancy: Consequences for mother and offspring. Reproduction, 146(5), R175–89. https://doi.org/10.1530/REP-13-0258
Burd, L., Severud, R., Kerbeshian, J., & Klug, M.G. (1999). Prenatal and perinatal risk factors for autism. Journal of Perinatal Medicine, 27(6), 441–50. https://doi.org/10.1515/JPM.1999.059
Burton, L. (2007). Childhood adultification in economically disadvantaged families: A conceptual model. Family Relations, 56(4), 329–45. https://doi.org/10.1111/j.1741-3729.2007.00463.x
Casey, J.A., Savitz, D.A., Rasmussen, S.G., Ogburn, E.L., Pollak, J., Mercer, D.G., & Schwartz, B.S. (2016). Unconventional natural gas development and birth outcomes in Pennsylvania, USA. Epidemiology, 27(2), 163–72. https://doi.org/10.1097/EDE.0000000000000387
Centers for Disease Control and Prevention (CDC). (2009). Healthy places terminology. Available: https://www.cdc.gov/healthyplaces/terminology.htm
———. (2014). Child maltreatment: Facts at a glance. Available: https://www.cdc.gov/violen-ceprevention/pdf/childmaltreatment-facts-at-a-glance.pdf
———. (2020). Health of Black or African American non-Hispanic population. Available: https://www.cdc.gov/nchs/fastats/black-health.htm
———. (2021). Injuries among children and teens. Available: https://www.cdc.gov/injury/features/child-injury/index.html
———. (2022). Working together to reduce black maternal mortality. Available: https://www.cdc.gov/healthequity/features/maternal-mortality/index.html#print
Centers for Medicare & Medicaid Services (CMS). (2020a). CMS issues urgent call to action following drastic decline in care for children in Medicaid and Children’s Health Insurance Program due to COVID-19 pandemic. (Press Release). Available: https://www.cms.gov/newsroom/press-releases/cms-issues-urgent-call-action-following-drastic-decline-care-children-medicaid-and-childrens-health
———. (2020b). Early and periodic screening, diagnostic, and treatment. Available: https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-treatment/index.html
Chapman, E.N., Kaatz, A., & Carnes, M. (2013). Physicians and implicit bias: How doctors may unwittingly perpetuate health care disparities. Journal of General Internal Medicine, 28(11), 1504–10. https://doi.org/10.1007/s11606-013-2441-1
Chetty, R., Hendren, N., & Katz, L.F. (2016). The effects of exposure to better neighborhoods on children: New evidence from the moving to opportunity experiment. American Economic Review, 106(4), 855–902. https://doi.org/10.1257/aer.20150572
Chung, E.K., Siegel, B.S., Garg, A., Conroy, K., Gross, R.S., Long, D.A., Lewis, G., Osman, C.J., Messito, M.J., & Wade, R. Jr. (2016). Screening for social determinants of health among children and families living in poverty: A guide for clinicians. Current Problems in Pediatric and Adolescent Health Care, 46(5), 135–53. https://doi.org/10.1016/j.cppeds.2016.02.004
Chung, P.J., Lee, T.C., Morrison, J.L., & Schuster, M.A. (2006). Preventive care for children in the United States: Quality and barriers. Annual Review of Public Health, 27, 491–515. https://doi.org/10.1146/annurev.publhealth.27.021405.102155
Children’s Defense Fund. (2022). Gun violence prevention. Available: https://www.childrens-defense.org/policy/policy-priorities/gun-violence-prevention
Clark, N., Demers, P., Karr, C., Koehoorn, M., Lencar, C., Tamburic, L., & Brauer, M. (2010). Effect of early life exposure to air pollution on development of childhood asthma. Environmental Health Perspectives, 118, 284–90. https://doi.org/10.1289/ehp.0900916
Clark, R., Anderson, N.B., Clark, V.R., & Williams, D.R. (1999). Racism as a stressor for African Americans: A biopsychosocial model. American Psychologist, 54(10), 805.
Cohen, S., Kessler, R., & Gordon, L.U. (1997). Measuring stress: A guide for health and social scientists. Oxford, England: Oxford University Press.
Coker, T.R., Windon, A., Moreno, C., Schuster, M.A., & Chung, P.J. (2013). Well-child care clinical practice redesign for young children: A systematic review of strategies and tools. Pediatrics, 131(1 Suppl), S5–25. https://doi.org/10.1542/peds.2012-1427c
Collins, J., & Swoveland, E. (2022). The impact of gun violence on children, families, & communities. Children’s Voices, 23(1). Child Welfare League of America. Available: https://www.cwla.org/the-impact-of-gun-violence-on-children-families-communities/
Commonwealth of Massachusetts. (2022). Childhood lead poisoning prevention program (CLPPP). Available: https://www.mass.gov/orgs/childhood-lead-poisoning-prevention-program
Costa, D.L. (2004). Race and pregnancy outcomes in the twentieth century: A long-term comparison. The Journal of Economic History, 64(4), 1056–86. https://www.jstor.org/stable/3874989
Cox, C., Clarkson, T.W., Marsh, D.O., Amin-Zaki, L., Tikriti, S., & Myers, G.G. (1989). Dose-response analysis of infants prenatally exposed to methyl mercury: An application of a single compartment model to single-strand hair analysis. Environmental Research, 49(2), 318–32. https://doi.org/10.1016/S0013-9351(89)80075-1
Creanga, A.A., Bateman, B.T., Kuklina, E.V., & Callaghan, W.M. (2014). Racial and ethnic disparities in severe maternal morbidity: A multistate analysis, 2008–2010. American Journal of Obstetrics and Gynecology, 210(5), 435.e431–8. https://doi.org/10.1016/j.ajog.2013.11.039
Crump, C., Winkleby, M.A., Sundquist, K., & Sundquist, J. (2011). Risk of diabetes among young adults born preterm in Sweden. Diabetes Care, 34(5), 1109–13. https://doi.org/10.2337/dc10-2108
Crump, C., Howell, E.A., Stroustrup, A., McLaughlin, M.A., Sundquist, J., & Sundquist, K. (2019a). Association of preterm birth with risk of ischemic heart disease in adulthood. JAMA Pediatrics, 173(8), 736–43. https://doi.org/10.1001/jamapediatrics.2019.1327
Crump, C., Sundquist, J., Winkleby, M.A., & Sundquist, K. (2019b). Preterm birth and risk of chronic kidney disease from childhood into mid-adulthood: National cohort study. British Medical Journal, 365, l1346. https://doi.org/10.1136/bmj.l1346
Currie, J., & Walker, R. (2011). Traffic congestion and infant health: Evidence from E-Zpass. American Economic Journal: Applied Economics, 3(1), 65–90. Available: https://www.aeaweb.org/articles?id=10.1257/app.3.1.65
Cusick, S.E., & Georgieff, M.K. (2016). The role of nutrition in brain development: The golden opportunity of the “first 1000 days.” The Journal of Pediatrics, 175, 16–21. https://doi.org/10.1016/j.jpeds.2016.05.013
De Sanctis, V., Soliman, A., Alaaraj, N., Ahmed, S., Alyafei, F., & Hamed, N. (2021). Early and long-term consequences of nutritional stunting: From childhood to adulthood. Acta Biomedica: The Official Journal of the Society of Medicine and Natural Sciences of Parma, 92(1), e2021168. https://doi.org/10.23750/abm.v92i1.11346
Dehon, E., Weiss, N., Jones, J., Faulconer, W., Hinton, E., & Sterling, S. (2017). A systematic review of the impact of physician implicit racial bias on clinical decision making. Academic Emergency Medicine: Official Journal of the Society for Academic Emergency Medicine, 24(8), 895–904. https://doi.org/10.1111/acem.13214
Department of Health and Human Services, Administration for Children and Families, & Administration on Children, Youth and Families, Children’s Bureau. (2021). Child Maltreatment 2019. Available: https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2019.pdf
Di Renzo, G.C., Conry, J.A., Blake, J., DeFrancesco, M.S., DeNicola, N., Martin, J.N. Jr., McCue, K.A., Richmond, D., Shah, A., Sutton, P., Woodruff, T.J., van der Poel, S.Z., & Giudice, L.C. (2015). International Federation of Gynecology and Obstetrics opinion on reproductive health impacts of exposure to toxic environmental chemicals. International Journal of Gynecology & Obstetrics, 131(3), 219–25. https://doi.org/10.1016/j.ijgo.2015.09.002
Diamanti-Kandarakis, E., Bourguignon, J.P., Giudice, L.C., Hauser, R., Prins, G.S., Soto, A.M., Zoeller, R.T., & Gore, A.C. (2009). Endocrine-disrupting chemicals: An endocrine society scientific statement. Endocrine Reviews, 30(4), 293–342. https://doi.org/10.1210/er.2009-0002
Diao, K., Tripodis, Y., Long, W.E., & Garg, A. (2017). Socioeconomic and racial disparities in parental perception and experience of having a medical home, 2007 to 2011–2012. Academic Pediatrics, 17(1), 95–103. https://doi.org/10.1016/j.acap.2016.07.006
Diversity Data Kids. (2019). What is child opportunity? Brandeis University, diversitydatakids.org. Available: https://www.diversitydatakids.org/research-library/research-brief/what-child-opportunity
Dodds, M., Nicholson, L., Muse, B. III, & Osborn, L.M. (1993). Group health supervision visits more effective than individual visits in delivering health care information. Pediatrics, 91(3), 668–670.
Dominguez, T.P., Dunkel-Schetter, C., Glynn, L.M., Hobel, C., & Sandman, C.A. (2008). Racial differences in birth outcomes: The role of general, pregnancy, and racism stress. Health Psychology, 27(2), 194–203. https://doi.org/10.1037/0278-6133.27.2.194
Dong, Y., & Yu, J.L. (2011). An overview of morbidity, mortality and long-term outcome of late preterm birth. World Journal of Pediatrics, 7(3), 199–204. https://doi.org/10.1007/s12519-011-0290-8
Douthit, N., Kiv, S., Dwolatzky, T., & Biswas, S. (2015). Exposing some important barriers to health care access in the rural USA. Public Health, 129(6), 611–20. https://doi.org/10.1016/j.puhe.2015.04.001
Dumas, M.J., & Nelson, J.D. (2016). (Re)Imagining black boyhood: Toward a critical framework for educational research. Harvard Educational Review, 86(1), 27–47. https://doi.org/10.17763/0017-8055.86.1.27
Ely, D.M., & Driscoll, A.K. (2019). Infant mortality in the United States, 2017: Data from the period linked birth/infant death file. National Vital Statistics Reports, 68(10), 1–20.
Epstein, R., Blake, J., & González, T. (2017). Girlhood interrupted: The erasure of black girls’ childhood. Center on Poverty and Inequality, Georgetown Law. Available: https://genderjusticeandopportunity.georgetown.edu/wp-content/uploads/2020/06/girlhood-interrupted.pdf
Evens, A., Hryhorczuk, D., Lanphear, B., Lewis, D., Forst, L., & Rosenberg, D. (2015). The effect of childhood lead exposure on school performance in Chicago Public Schools: A population-based retrospective cohort study. Environmental Health: A Global Access Science Source, 14, 21. https://doi.org/10.1186/s12940-015-0008-9
Evensen, K.A., Steinshamn, S., Tjønna, A.E., Stølen, T., Høydal, M.A., Wisløff, U., Brubakk, A.M., & Vik, T. (2009). Effects of preterm birth and fetal growth retardation on cardiovascular risk factors in young adulthood. Early Human Development, 85(4), 239–45. https://doi.org/10.1016/j.earlhumdev.2008.10.008
Ewing-Cobbs, L., Prasad, M.R., Kramer, L., Cox, C.S., Jr., Baumgartner, J., Fletcher, S., Mendez, D., Barnes, M., Zhang, X., & Swank, P. (2006). Late intellectual and academic outcomes following traumatic brain injury sustained during early childhood. Journal of Neurosurgery, 105(4 Suppl), 287–96. https://doi.org/10.3171/ped.2006.105.4.287
Fenick, A.M., Leventhal, J.M., Gilliam, W., & Rosenthal, M.S. (2020). A randomized controlled trial of group well-child care: Improved attendance and vaccination timeliness. Clinical Pediatrics, 59(7), 686–91. https://doi.org/10.1177/0009922820908582
Finkelhor, D., Ormrod, R.K., & Turner, H.A. (2007). Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse & Neglect, 31(5), 479–502. https://doi.org/10.1016/j.chiabu.2006.03.012
Finkelhor, D., Turner, H., Ormrod, R., Hamby, S., & Kracke, K. (2009). Children’s exposure to violence: A comprehensive national survey. National Survey of Children’s Exposure to Violence. Office of Justice Programs, Department of Justice. Available: https://www.ojp.gov/pdffiles1/ojjdp/227744.pdf
Finkelhor, D., Turner, H.A., Shattuck, A., & Hamby, S.L. (2015). Prevalence of childhood exposure to violence, crime, and abuse: Results from the national survey of children’s exposure to violence. JAMA Pediatrics, 169(8), 746–54. https://doi.org/10.1001/jamapediatrics.2015.0676
FitzGerald, C., & Hurst, S. (2017). Implicit bias in healthcare professionals: A systematic review. BMC Medical Ethics, 18(1), 19. https://doi.org/10.1186/s12910-017-0179-8
Flacks, J., & Boynton-Jarrett, J.R. (2018). A strengths-based approach to screening families for health-related social needs. Center for the Study of Social Policy. Available: https://cssp.org/resource/strengths-based-approaches-screening-families-final/
Fleisch, A.F., Luttmann-Gibson, H., Perng, W., Rifas-Shiman, S.L., Coull, B.A., Kloog, I., Koutrakis, P., Schwartz, J.D., Zanobetti, A., Mantzoros, C.S., Gillman, M.W., Gold, D.R., & Oken, E. (2017). Prenatal and early life exposure to traffic pollution and cardiometabolic health in childhood. Pediatric Obesity, 12(1), 48–57. https://doi.org/10.1111/ijpo.12106
Flores, G. (2010). Technical report—Racial and ethnic disparities in the health and health care of children. Pediatrics, 125(4), e979–1020. https://doi.org/10.1542/peds.2010-0188
Food and Agriculture Organization of the United Nations, International Fund for Agricultural Development, United Nations Children’s Fund, World Food Programme, & World Health Organization. (2021). The state of food security and nutrition in the world. Transforming food systems for food security, improved nutrition and affordable healthy diets for all. https://doi.org/10.4060/cb4474en
Foster, H., Brooks-Gunn, J., & Martin, A. (2007). Poverty/socioeconomic status and exposure to violence in the lives of children and adolescents. The Cambridge handbook of violent behavior and aggression, 664–87. Cambridge, UK: Cambridge University Press.
Foster, K., Mitchell, R., Van, C., Young, A., McCloughen, A., & Curtis, K. (2019a). Resilient, recovering, distressed: A longitudinal qualitative study of parent psychosocial trajectories following child critical injury. Injury, 50(10), 1605–11. https://doi.org/10.1016/j.injury.2019.05.003
Foster, K., Mitchell, R., Young, A., Van, C., & Curtis, K. (2019b). Parent experiences and psychosocial support needs 6 months following paediatric critical injury: A qualitative study. Injury, 50(5), 1082–8. https://doi.org/10.1016/j.injury.2019.01.004
Foverskov, E., White, J., Frøslev, T., Sørenson, H., & Hamad, R. (2022). Risk of psychiatric disorders among refugee children and adolescents living in disadvantaged neighborhoods. Journal of the American Medical Association: Pediatrics, 176(11), 1107–14. https://doi.org/10.1001/jamapediatrics.2022.3235
Freeman, B.K., & Coker, T.R. (2018). Six questions for well-child care redesign. Academic Pediatrics, 18(6), 609–19. https://doi.org/10.1016/j.acap.2018.05.003
Fulton, J.B., Yeates, K.O., Taylor, H.G., Walz, N.C., & Wade, S.L. (2012). Cognitive predictors of academic achievement in young children 1 year after traumatic brain injury. Neuropsychology, 26(3), 314–22. https://doi.org/10.1037/a0027973
Gale, C.R., & Martyn, C.N. (2004). Birth weight and later risk of depression in a national birth cohort. British Journal of Psychiatry, 184, 28–33. https://doi.org/10.1192/bjp.184.1.28
Galler, J.R., Bringas-Vega, M.L., Tang, Q., Rabinowitz, A.G., Musa, K.I., Chai, W.J., & Valdés-Sosa, P.A. (2021). Neurodevelopmental effects of childhood malnutrition: A neuroimaging perspective. NeuroImage, 231, 117828. https://doi.org/10.1016/j.neuroimage.2021.117828
Garg, A., Sandel, M., Dworkin, P.H., Kahn, R.S., & Zuckerman, B. (2012). From medical home to health neighborhood: Transforming the medical home into a community-based health neighborhood. The Journal of Pediatrics, 160(4), 535–6. Available: https://www.bmc.org/sites/default/files/About_Us/MAG/health-neighborhood.pdf
Gears, H., Casau, A., Buck, L., & Yard, R. (2021). Accelerating child health care transformation: Key opportunities for improving pediatric care. Center for Health Care Strategies. Available: https://www.nationalcomplex.care/wp-content/uploads/2022/06/AcceleratingChild-Health-Care-Transformation-Key-Opportunities-for-Improving-Pediatric-Care.pdf
Georgieff, M.K., Brunette, K.E., & Tran, P.V. (2015). Early life nutrition and neural plasticity. Development and Psychopathology, 27(2), 411–23. https://doi.org/10.1017/S0954579415000061
Gilchrist, J., Ballesteros, M., & Parker, E.M. (2012). Vital signs: Unintentional injury deaths among persons aged 0–19 years—United States, 2000–2009. Morbidity and Mortality Weekly Report, 61, 270–6. Available: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6115a5.htm
Giudice, L., Woodruff, T., & Conry, J. (2017). Reproductive and developmental environmental health. Obstetrics, Gynaecology & Reproductive Medicine, 27(3), 99–101. https://doi.org/10.1097/GCO.0b013e3283404e59
Glass, T.A., & Bilal, U. (2016). Are neighborhoods causal? Complications arising from the ‘stickiness’ of ZNA. Social Science & Medicine, 166, 244–53. https://doi.org/10.1016/j.socscimed.2016.01.001
Goff, P.A., Jackson, M.C., Di Leone, B.A.L., Culotta, C.M., & DiTomasso, N.A. (2014). The essence of innocence: Consequences of dehumanizing black children. Journal of Personality and Social Psychology, 106(4), 526. https://doi.org/10.1037/a0035663
Golberstein, E., Wen, H., & Miller, B.F. (2020). Coronavirus disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatrics, 174(9), 819–20. https://doi.org/10.1001/jamapediatrics.2020.1456
Goldstick, J.E., Cunningham, R.M., & Carter, P.M. (2022). Current causes of death in children and adolescents in the United States. New England Journal of Medicine, 386(20), 1955–6. https://www.nejm.org/doi/full/10.1056/NEJMc2201761
Gore, A.C., Chappell, V.A., Fenton, S.E., Flaws, J.A., Nadal, A., Prins, G.S., Toppari, J., & Zoeller, R.T. (2015). Executive summary to EDC-2: The Endocrine Society’s second scientific statement on endocrine-disrupting chemicals. Endocrine Reviews, 36(6), 593–602. https://doi.org/10.1210/er.2015-1093
Gottlieb, L., Sandel, M., & Adler, N. (2013). Collecting and applying data on social determinants of health in health care settings. The Journal of the American Medical Association: Internal Medicine, 173(11), 1017–20. https://doi.org/10.1001/jamainternmed.2013.56
Goyal, M.K., Kuppermann, N., Cleary, S.D., Teach, S.J., & Chamberlain, J.M. (2015). Racial disparities in pain management of children with appendicitis in emergency departments. The Journal of the American Medical Association: Pediatrics, 169(11), 996–1002. https://doi.org/10.1001/jamapediatrics.2015.1915
Guan, A., Hamad, R., Batra, A., Bush, N., Tylavsky, F., & LeWinn, K. (2021). The revised WIC food package and child development: A quasi-experimental study. Pediatrics 147(2), e20201853. https://doi.org/10.1542/peds.2020-1853
Guillory, J.D. (1968). The pro-slavery arguments of Dr. Samuel A. Cartwright. Louisiana History: The Journal of the Louisiana Historical Association, 9(3), 209–27. https://www.jstor.org/stable/4231017
Gullett, H., Salib, M., Rose, J., & Stange, K.C. (2019). An evaluation of CenteringParenting: A group well-child care model in an urban federally qualified community health center. The Journal of Alternative and Complementary Medicine, 25(7), 727–32. https://doi.org/10.1089/acm.2019.0090
Ha, S., Hu, H., Roth, J., Kan, H., & Xu, X. (2015). Associations between residential proximity to power plants and adverse birth outcomes. American Journal of Epidemiology, 182(3). https://doi.org/10.1093/aje/kwv042
Hagan, J.F., Shaw, J.S., & Duncan, P.M. (2017). Bright futures: Guidelines for health supervision of infants, children and adolescents. (4th ed.). American Academy of Pediatrics. Available: https://downloads.aap.org/AAP/PDF/Bright%20Futures/BF4_Introduction.pdf
Haider, A.H., Sexton, J., Sriram, N., Cooper, L.A., Efron, D.T., Swoboda, S., Villegas, C.V., Haut, E.R., Bonds, M., Pronovost, P.J., & Lipsett, P.A. (2011). Association of unconscious race and social class bias with vignette-based clinical assessments by medical students. The Journal of the American Medical Association, 306(9), 942–51. https://doi.org/10.1001/jama.2011.1248
Halfon, N., Regalado, M., Sareen, H., Inkelas, M., Reuland, C.H., Glascoe, F.P., & Olson, L.M. (2004). Assessing development in the pediatric office. Pediatrics, 113(6 Suppl), 1926–33. https://doi.org/10.1016/j.acap.2010.08.008
Halfon, N., Stevens, G.D., Larson, K., & Olson, L.M. (2011). Duration of a well-child visit: Association with content, family-centeredness, and satisfaction. Pediatrics, 128(4), 657–64. https://doi.org/10.1542/peds.2011-0586
Hall, W.J., Chapman, M.V., Lee, K.M., Merino, Y.M., Thomas, T.W., Payne, B.K., Eng, E., Day, S.H., & Coyne-Beasley, T. (2015). Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: A systematic review. American Journal of Public Health, 105(12), e60–76. https://doi.org/10.2105/AJPH.2015.302903
Hamad, R. (2020). Natural and unnatural experiments in epidemiology. Epidemiology, 31(6), 768–70. https://doi.org/10.1097/EDE.0000000000001242
Hamad, R., & Rehkopf, D.H. (2016). Poverty and child development: A longitudinal study of the impact of the earned income tax credit. American Journal of Epidemiology, 183(9), 775–84. https://doi.org/10.1093/aje/kwv317
Hamad, R., Öztürk, B., Foverskov, E., Pedersen, L., Sørensen, H.T., Bøtker, H.E., & White, J.S. (2020). Association of neighborhood disadvantage with cardiovascular risk factors and events among refugees in Denmark. The Journal of the American Medical Association: Network Open, 3(8), e2014196. https://doi.org/10.1001/jamanetworkopen.2020.14196
Hambrick, E.P., Brawner, T.W., & Perry, B.D. (2019). Timing of early-life stress and the development of brain-related capacities. Frontiers in Behavioral Neuroscience, 13. https://doi.org/10.3389/fnbeh.2019.00183
Hamilton, B.E., Martin., J.A., & Osterman, M.J.K. (2020). Births: Provisional data for 2019. (Report No. 008). Vital Statistics Rapid Release. Available: https://www.cdc.gov/nchs/data/vsrr/vsrr-8-508.pdf
Harrell, S.P. (2000). A multidimensional conceptualization of racism-related stress: Implications for the well-being of people of color. American Journal of Orthopsychiatry, 70(1), 42–57. https://doi.org/10.1037/h0087722
Harris, M.H., Gold, D.R., Rifas-Shiman, S.L., Melly, S.J., Zanobetti, A., Coull, B.A., Schwartz, J.D., Gryparis, A., Kloog, I., Koutrakis, P., Bellinger, D.C., Belfort, M.B., Webster, T.F., White, R.F., Sagiv, S.K., & Oken, E. (2016). Prenatal and childhood traffic-related air pollution exposure and childhood executive function and behavior. Neurotoxicology and Teratology, 57, 60–70. https://doi.org/10.1016/j.ntt.2016.06.008
Hendryx, M., Fedorko, E., & Halverson, J. (2010). Pollution sources and mortality rates across rural-urban areas in the United States. The Journal of Rural Health, 26(4), 383–91. https://doi.org/10.1111/j.1748-0361.2010.00305.x
Heron, M. (2019). Deaths: Leading causes for 2017. National Vital Statistics Reports, 68(6), 1–77. Available: https://stacks.cdc.gov/view/cdc/79488
Hoffman, K.M., Trawalter, S., Axt, J.R., & Oliver, M.N. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the National Academy of Sciences of the United States of America, 113(16), 4296–301. https://doi.org/10.1073/pnas.1516047113
Hopenhayn, C., Ferreccio, C., Browning, S.R., Huang, B., Peralta, C., Gibb, H., & Hertz-Picciotto, I. (2003). Arsenic exposure from drinking water and birth weight. Epidemiology, 14(5), 593–602. https://doi.org/10.1097/01.ede.0000072104.65240.69
Houston, D., Dang, A., Wu, J., Chowdhury, Z., & Edwards, R. (2016). The cost of convenience: Air pollution and noise on freeway and arterial light rail station platforms in Los Angeles. Transportation Research Part D: Transport and Environment, 49, 127–37. https://doi.org/10.1016/j.trd.2016.09.011
Hoyert, D.L., & Miniño, A.M. (2020). Maternal mortality in the United States: Changes in coding, publication, and data release, 2018. National Vital Statistics Reports, 69(2), 1–18. https://stacks.cdc.gov/view/cdc/84769
Hulin, M., Caillaud, D., & Annesi-Maesano, I. (2010). Indoor air pollution and childhood asthma: Variations between urban and rural areas. Indoor Air, 20(6), 502–14. https://doi.org/10.1111/j.1600-0668.2010.00673.x
Institute of Medicine (IOM). (1990). Nutrition during pregnancy: Part I: Weight gain, Part II: Nutrient supplements. The National Academies Press. https://doi.org/10.17226/1451
———. (2000). Clearing the air: Asthma and indoor air exposures. The National Academies Press. https://doi.org/10.17226/9610.
———. (2003). Unequal treatment: Confronting racial and ethnic disparities in health care. The National Academies Press. https://doi.org/10.17226/12875.
Jacob, B., & Ryan, J. (2018). How life outside of school affects student performance in school. Brookings Institution. Available: https://www.brookings.edu/research/how-life-outside-of-a-school-affects-student-performance-in-school/
Jeffries, N., Zaslavsky, A.M., Diez Roux, A.V., Creswell, J.W., Palmer, R.C., Gregorich, S.E., Reschovsky, J.D., Graubard, B.I., Choi, K., & Pfeiffer, R.M. (2019). Methodological approaches to understanding causes of health disparities. American Journal of Public Health, 109(S1), S28–33. https://doi.org/10.2105/AJPH.2018.304843
Jewkes, R. (2002). Intimate partner violence: Causes and prevention. The Lancet, 359(9315), 1423–9. https://doi.org/10.1016/S0140-6736(02)08357-5
Johnson, T.J., Winger, D.G., Hickey, R.W., Switzer, G.E., Miller, E., Nguyen, M.B., Saladino, R.A., & Hausmann, L.R. (2017). Comparison of physician implicit racial bias toward adults versus children. Academic Pediatrics, 17(2), 120–6. https://doi.org/10.1016/j.acap.2016.08.010
Jones, C.P. (2001). Invited commentary: “Race”, racism, and the practice of epidemiology. American Journal of Epidemiology, 154(4), 299–304. https://doi.org/10.1093/aje/154.4.299
Jones, K.A., Do, S., Porras-Javier, L., Contreras, S., Chung, P.J., & Coker, T.R. (2018). Feasibility and acceptability in a community-partnered implementation of CenteringParenting for group well-child care. Academic Pediatrics, 18(6), 642–9. https://doi.org/10.1016/j.acap.2018.06.001
Jones, L., Bellis, M.A., Wood, S., Hughes, K., McCoy, E., Eckley, L., Bates, G., Mikton, C., Shakespeare, T., & Officer, A. (2012). Prevalence and risk of violence against children with disabilities: A systematic review and meta-analysis of observational studies. The Lancet, 380(9845), 899–907. https://doi.org/10.1016/S0140-6736(12)60692-8
Kaijser, M., Edstedt Bonamy, A.K., Akre, O., Cnattingius, S., Granath, F., Norman, M., & Ekbom, A. (2009). Perinatal risk factors for diabetes in later life. Diabetes, 58(3), 523–6. https://doi.org/10.2337/db08-0558
Kaiser Family Foundation. (2022). Medicaid postpartum coverage extension tracker. Available: https://www.kff.org/medicaid/issue-brief/medicaid-postpartum-coverage-extension-tracker
Kajantie, E., Osmond, C., Barker, D.J.P., & Eriksson, J.G. (2010). Preterm birth—A risk factor for type 2 diabetes? The Helsinki birth cohort study. Diabetes Care, 33(12), 2623–5. https://doi.org/10.2337/dc10-0912
Kalter, H. (2003). Teratology in the 20th century: Environmental causes of congenital malformations in humans and how they were established. Neurotoxicology and Teratology, 25(2), 131–282. https://doi.org/10.1016/S0892-0362(03)00010-2
Kelleher, K., Reece, J., & Sandel, M. (2018). The healthy neighborhood, healthy families initiative. Pediatrics, 142(3), e20180261. https://doi.org/10.1542/peds.2018-0261
Kelly, Y.J., Bécares, L., & Nazroo, J.Y. (2013). Associations between maternal experiences of racism and early child health and development: Findings from the UK Millennium Cohort Study. Journal of Epidemiology & Community Health, 67, 35–41. https://doi.org/10.1136/jech-2011-200814
Kerkhof, G.F., Breukhoven, P.E., Leunissen, R.W., Willemsen, R.H., & Hokken-Koelega, A.C. (2012a). Does preterm birth influence cardiovascular risk in early adulthood? Journal of Pediatrics, 161(3), 390–6. https://doi.org/10.1016/j.jpeds.2012.03.048
Kerkhof, G.F., Willemsen, R.H., Leunissen, R.W., Breukhoven, P.E., & Hokken-Koelega, A.C. (2012b). Health profile of young adults born preterm: Negative effects of rapid weight gain in early life. Journal of Clinical Endocrinology & Metabolism, 97(12), 4498–506. https://doi.org/10.1210/jc.2012-1716
Kersten, E.E., LeWinn, K.Z., Gottlieb, L., Jutte, D.P., & Adler, N.E. (2014). San Francisco children living in redeveloped public housing used acute services less than children in older public housing. Health Affairs, 33(12), 2230–7. https://doi.org/10.1377/hlthaff.2014.1021
Kessler, R.C., Duncan, G.J., Gennetian, L.A., Katz, L.F., Kling, J.R., Sampson, N.A., Sanbonmatsu, L., Zaslavsky, A.M., & Ludwig, J. (2014). Associations of housing mobility interventions for children in high-poverty neighborhoods with subsequent mental disorders during adolescence. Journal of the American Medical Association, 311(9), 937–47. https://doi.org/10.1001/jama.2014.607
Kim, M.A., & Williams, K.A. (2017). Lead levels in landfill areas and childhood exposure: An integrative review. Public Health Nursing, 34(1), 87–97. https://doi.org/10.1111/phn.12249
King, W. (2005). Afterword: African American children in contemporary society. In African American Childhoods. Palgrave Macmillan. https://doi.org/10.1007/978-1-349-73165-7_11
Kingery, K.M., Narad, M.E., Taylor, H.G., Yeates, K.O., Stancin, T., & Wade, S.L. (2017). Do children who sustain traumatic brain injury in early childhood need and receive academic services 7 years after injury? Journal of Developmental & Behavioral Pediatrics, 38(9), 728–35. https://doi.org/10.1097/DBP.0000000000000489
Klevens, J., Schmidt, B., Luo, F., Xu, L., Ports, K.A., & Lee, R.D. (2017). Effect of the Earned Income Tax Credit on hospital admissions for pediatric abusive head trauma, 1995–2013. Public Health Reports, 132(4), 505–11. https://doi.org/10.1177/0033354917710905
Koch, A., & Kozhumam, A. (2021). Addressing adultification of black pediatric patients in the emergency department: A framework to decrease disparities. Health Promotion Practice, 23(4), 555–9. https://doi.org/10.1177/15248399211049207
———. (2022). Adultification of black children negatively impacts their health: Recommendations for health care providers. Nursing Forum, 57(5), 963–67. https://doi.org/10.1111/nuf.12736
Kovski, N.L., Hill, H.D., Mooney, S.J., Rivara, F.P., Morgan, E.R., & Rowhani-Rahbar, A. (2022). Association of state-level earned income tax credits with rates of reported child maltreatment, 2004–2017. Child Maltreatment, 27(3), 325–33. https://doi.org/10.1177/1077559520987302
Krieger, N., Chen, J., Waterman, P., Kiang, M., & Feldman, J. (2015). Police killings and police deaths are public health data and can be counted. PLoS Medicine, 12, e1001915. https://doi.org/10.1371/journal.pmed.1001915
Kuh, D., Ben-Shlomo, Y., Lynch, J., Hallqvist, J., & Power, C. (2003). Life course epidemiology. Journal of Epidemiology and Community Health, 57(10), 778–83. https://doi.org/10.1136/jech.57.10.778
Kujawski, S.A., Yao, L., Wang, H.E., Carias, C., & Chen, Y.T. (2022). Impact of the COVID-19 pandemic on pediatric and adolescent vaccinations and well child visits in the United States: A database analysis. Vaccine, 40(5), 706–13. https://doi.org/10.1016/j.vaccine.2021.12.064
Landon, M.B., Leindecker, S., Spong, C.Y., Hauth, J.C., Bloom, S.L., Varner, M.W., Moawad, A.H., Caritis, S.N., Harper, M., Wapner, R.J., Sorokin, Y., Miodovnik, M., Carpenter, M.W., Peaceman, A.M., O’Sullivan, M.J., Sibai, B.M., Langer, O., Thorp, J.M., Ramin, S.M., . . . & Gabbe, S.G. (2005). The MFMU Cesarean Registry: Factors affecting the success of trial of labor after previous cesarean delivery. American Journal of Obstetrics and Gynecology, 193(3), 1016–23. https://doi.org/10.1016/j.ajog.2005.05.066
Landrine, H., & Klonoff, E.A. (1996). The schedule of racist events: A measure of racial discrimination and a study of its negative physical and mental health consequences. Journal of Black Psychology, 22(2), 144–68. https://doi.org/10.1177/00957984960222002
Laraque-Arena, D., & Stein, R.E. (2021). Integrating mental health in the comprehensive care of children and adolescents: Prevention, screening, diagnosis and treatment. Pediatric Medicine, 4, 21. https://doi.org/10.21037/pm-21-36
Larsson, H.J., Eaton, W.W., Madsen, K.M., Vestergaard, M., Olesen, A.V., Agerbo, E., Schendel, D., Thorsen, P., & Mortensen, P.B. (2005). Risk factors for autism: Perinatal factors, parental psychiatric history, and socioeconomic status. American Journal of Epidemiology, 161(10), 916–25. https://doi.org/10.1093/aje/kwi123
Lee, L.K., Fleegler, E.W., Goyal, M.K., Doh, K.F., Laraque-Arena, D., & Hoffman, B.D. (2022). Firearm-related injuries and deaths in children and youth. Pediatrics, 150(6). e2022060071. https://doi.org/10.1542/peds.2022-060071
Leventhal, T., & Newman, S. (2010). Housing and child development. Children and Youth Services Review, 32(9), 1165–74. https://doi.org/10.1016/j.childyouth.2010.03.008
Linnet, K.M., Wisborg, K., Agerbo, E., Secher, N.J., Thomsen, P.H., & Henriksen, T.B. (2006). Gestational age, birth weight, and the risk of hyperkinetic disorder. Archives of Disease in Childhood, 91(8), 655–60. https://doi.org/10.1136/adc.2005.088872
Madara, J.L. (2021). Reckoning with medicine’s history of racism. The American Medical Association. Available: https://www.ama-assn.org/about/leadership/reckoning-medicine-s-history-racism
Madigan, S., Prime, H., Graham, S.A., Rodrigues, M., Anderson, N., Khoury, J., & Jenkins, J.M. (2019). Parenting behavior and child language: A meta-analysis. Pediatrics, 144(4), e20183556. https://doi.org/10.1542/peds.2018-3556
Manikkam, M., Tracey, R., Guerrero-Bosagna, C., & Skinner, M.K. (2013). Plastics derived endocrine disruptors (BPA, DEHP and DBP) induce epigenetic transgenerational inheritance of obesity, reproductive disease and sperm epimutations. PLoS One, 8(1), e55387. https://doi.org/10.1371/journal.pone.0055387
March of Dimes. (2021). 2021 March of Dimes report card. Available: https://www.marchofdimes.org/2021-march-dimes-report-card
———. (2022). Momnibus. Available: https://www.marchofdimes.org/momnibus
Marlow, N., Wolke, D., Bracewell, M.A., & Samara, M. (2005). Neurologic and developmental disability at six years of age after extremely preterm birth. New England Journal of Medicine, 352(1), 9–19. https://doi.org/10.1056/NEJMoa041367
Maroney, T., & Zuckerman, B. (2018). “The talk,” physician version: Special considerations for African American, male adolescents. Pediatrics, 141(2). https://doi.org/10.1542/peds.2017-1462
Martin, J.A., Hamilton, B.E., Osterman, M.J.K., & Driscoll, A.K. (2019). Births: Final data for 2018. National Vital Statistics Reports, 68(13), 1–47. Available: https://stacks.cdc.gov/view/cdc/82909
Mathai, S., Cutfield, W.S., Derraik, J.G., Dalziel, S.R., Harding, J.E., Robinson, E., Biggs, J., Jefferies, C., & Hofman, P.L. (2012). Insulin sensitivity and β-cell function in adults born preterm and their children. Diabetes, 61(10), 2479–83. https://doi.org/10.2337/db11-1672
Matthew, A.J., Clark, M.A, & McDavid, L.M. (2021). Combating racism: The role of the pediatrician. Pediatric Research, 90, 708–10. https://doi.org/10.1038/s41390-020-01345-x
Maybank, A., De Maio, F., Lemos, D., & Derige, D.N. (2022). Embedding racial justice and advancing health equity at the American Medical Association. The American Journal of Medicine, 135(7), 803–5. https://doi.org/10.1016/j.amjmed.2022.01.058
McEwen, B.S. (2005). Stressed or stressed out: What is the difference? Journal of Psychiatry & Neuroscience, 30(5), 315–8.
McGowan, P.O., & Matthews, S.G. (2018). Prenatal stress, glucocorticoids, and developmental programming of the stress response. Endocrinology, 159(1), 69–82. https://doi.org/10.1210/en.2017-00896
Meijer, M., Bloomfield, K., & Engholm, G. (2013). Neighbourhoods matter too: The association between neighbourhood socioeconomic position, population density and breast, prostate and lung cancer incidence in Denmark between 2004 and 2008. Journal of Epidemiology and Community Health, 67(1), 6–13. https://doi.org/10.1136/jech-2011-200192
Menakem, R. (2017). My grandmother’s hands: Racialized trauma and the pathway to mending our hearts and bodies. Las Vegas, NV: Central Recovery Press.
Metzl, J.M., & Hansen, H. (2014). Structural competency: Theorizing a new medical engagement with stigma and inequality. Social Science & Medicine (1982), 103, 126–33. https://doi.org/10.1016/j.socscimed.2013.06.032
Mikati, I., Benson, A.F., Luben, T.J., Sacks, J.D., & Richmond-Bryant, J. (2018). Disparities in distribution of particulate matter emission sources by race and poverty status. American Journal of Public Health, 108(4), 480–5. https://doi.org/10.2105/AJPH.2017.304297
Miranda, M.L., Kim, D., Reiter, J., Overstreet Galeano, M.A., & Maxson, P. (2009). Environmental contributors to the achievement gap. Neurotoxicology, 30(6), 1019–24. https://doi.org/10.1016/j.neuro.2009.07.012
Miranda, M.L., Edwards, S.E., Chang, H.H., & Auten, R.L. (2013). Proximity to roadways and pregnancy outcomes. Journal of Exposure Science & Environmental Epidemiology, 23(1), 32–8. https://doi.org/10.1038/jes.2012.78
Mitchell, R.J., Cameron, C.M., McMaugh, A., Lystad, R.P., Badgery-Parker, T., & Ryder, T. (2021). The impact of childhood injury and injury severity on school performance and high school completion in Australia: A matched population-based retrospective cohort study. BMC Pediatrics, 21(1), 426. https://doi.org/10.1186/s12887-021-02891-x
Morency, P., Gauvin, L., Plante, C., Fournier, M., & Morency, C. (2012). Neighborhood social inequalities in road traffic injuries: The influence of traffic volume and road design. American Journal of Public Health, 102(6), 1112–9. https://doi.org/10.2105/AJPH.2011.300528
Muller, C., Sampson, R.J., & Winter, A.S. (2018). Environmental inequality: The social causes and consequences of lead exposure. Annual Review of Sociology, 44(1), 263–82. https://doi.org/10.1146/annurev-soc-073117-041222
Myers, H., Lewis, T., & Dominguez, T. (2003). Stress, coping, and minority health: Biopsychosocial perspective on ethnic health disparities. Handbook of racial and ethnic minority psychology, 377–400. Thousand Oaks, CA: SAGE Publications.
Nakamura, K., Itoh, K., Dai, H., Han, L., Wang, X., Kato, S., Sugimoto, T., & Fushiki, S. (2012). Prenatal and lactational exposure to low-doses of bisphenol A alters adult mice behavior. Brain Development, 34(1), 57–63. https://doi.org/10.1016/j.braindev.2010.12.011
National Academies of Sciences, Engineering, and Medicine (National Academies). (2017). Communities in action: Pathways to health equity. The National Academies Press. https://doi.org/10.17226/24624
———. (2019). Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. The National Academies Press. https://doi.org/10.17226/25466
National Association of Pediatric Nurse Practitioners. (2009). NAPNAP position statement on pediatric health care/medical home: Key issues on delivery, reimbursement, and leadership. Journal of Pediatric Health Care, 23(3), A23–4.
National Center for Healthy Housing. (2013). Issue brief: Childhood lead exposure and educational outcomes. Available: https://nchh.org/resource-library/Childhood_Lead_Exposure.pdf.
National Center for Health Statistics (NCHS). (2018). Health, United States 2018. Department of Health and Human Services. Available: https://www.cdc.gov/nchs/data/hus/hus18.pdf#Highlights(2018)
———. (2020). NCHS Data on racial and ethnic disparities. Department of Health and Human Services. Available: https://www.cdc.gov/nchs/data/factsheets/factsheet_disparities.pdf
National Institute of Child Health and Human Development. (2012). The long-lasting effects of preterm birth. Department of Health and Human Services. Available: https://www.nichd.nih.gov/newsroom/resources/spotlight/012612-effects-preterm-birth
Needleman, H.L., Gunnoe, C., Leviton, A., Reed, R., Peresie, H., Maher, C., & Barrett, P. (1979). Deficits in psychologic and classroom performance of children with elevated dentine lead levels. New England Journal of Medicine, 300(13), 689–95. https://doi.org/10.1056/nejm197903293001301
Needleman, H.L., Schell, A., Bellinger, D., Leviton, A., & Allred, E.N. (1990). The long-term effects of exposure to low doses of lead in childhood: An 11-year follow-up report. New England Journal of Medicine, 322(2), 83–8. https://doi.org/10.1056/NEJM199001113220203
Newgard, C.D., Schmicker, R.H., Sopko, G., Andrusiek, D., Bialkowski, W., Minei, J.P., Brasel, K., Bulger, E., Fleischman, R.J., Kerby, J.D., Bigham, B.L., Warden, C.R., & Resuscitation Outcomes Consortium Investigators. (2011). Trauma in the neighborhood: A geospatial analysis and assessment of social determinants of major injury in North America. American Journal of Public Health, 101(4), 669–77. https://doi.org/10.2105/AJPH.2010.300063
Nieblas-Bedolla, E., Christophers, B., Nkinsi, N.T., Schumann, P.D., & Stein, E. (2020). Changing how race is portrayed in medical education: Recommendations from medical students. Academic Medicine: Journal of the Association of American Medical Colleges, 95(12), 1802–6. https://doi.org/10.1097/ACM.0000000000003496
Nolen, L.T., Beckman, A.L., & Sandoe, E. (2020). How foundational moments in Medicaid’s history reinforced rather than eliminated racial health disparities. Health Affairs Blog. Lown Institute. Available: https://lowninstitute.org/headlines/how-foundational-moments-in-medicaids-history-reinforced-rather-than-eliminated-racial-health-disparities/
Nomura, Y., Brooks-Gunn, J., Davey, C., Ham, J., & Fifer, W.P. (2007). The role of perinatal problems in risk of co-morbid psychiatric and medical disorders in adulthood. Psychological Medicine, 37(9), 1323–34. https://doi.org/10.1017/S0033291707000736
Norlin, C., Crawford, M.A., Bell, C.T., Sheng, X., & Stein, M.T. (2011). Delivery of well-child care: A look inside the door. Academic Pediatrics, 11(1), 18–26. https://doi.org/10.1016/j.acap.2010.12.008
Northridge, M.E., Stover, G.N., Rosenthal, J.E., & Sherard, D. (2003). Environmental equity and health: Understanding complexity and moving forward. American Journal of Public Health, 93(2), 209–14. https://doi.org/10.2105/ajph.93.2.209
Oakes, J.M. (2004). The (mis)estimation of neighborhood effects: Causal inference for a practicable social epidemiology. Social Science & Medicine, 58(10), 1929–52. https://doi.org/10.1016/j.socscimed.2003.08.004
Oakes, J.M., Andrade, K.E., Biyoow, I.M., & Cowan, L.T. (2015). Twenty years of neighborhood effect research: An assessment. Current Epidemiology Reports, 2(1), 80–7. https://doi.org/10.1007/s40471-015-0035-7
Oberg, C., Colianni, S., & King-Schultz, L. (2016). Child health disparities in the 21st century. Current Problems in Pediatric and Adolescent Health Care, 46(9), 291–312. https://doi.org/10.1016/j.cppeds.2016.07.001
Ocen, P.A. (2015). (E)rasing childhood: Examining the racialized construction of childhood and innocence in the treatment of sexually exploited minors. UCLA Law Review, 62(6). Available: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2692829
Oldfield, B.J., Rosenthal, M.S., & Coker, T.R. (2020). Update on the feasibility, acceptability, and impact of group well-child care. Academic Pediatrics, 20(6), 731–2. https://doi.org/10.1016/j.acap.2020.02.029
Olson, L.M., Inkelas, M., Halfon, N., Schuster, M.A., O’Connor, K.G., & Mistry, R. (2004). Overview of the content of health supervision for young children: Reports from parents and pediatricians. Pediatrics, 113(6 Suppl), 1907–16. https://doi.org/10.1542/peds.113.S5.1907
Organisation for Economic Co-operation and Development (OECD). (2019). Health at a glance 2019: United States. Available: https://www.oecd.org/unitedstates/health-at-a-glance-united-states-EN.pdf
———. (2022). Understanding differences in health expenditure between the United States and OECD countries. Available: https://www.oecd.org/health/Health-expenditure-differences-USA-OECD-countries-Brief-July-2022.pdf
O’Reilly, K.B. (2020). AMA: Racism is a threat to public health. American Medical Association. Available: https://www.ama-assn.org/delivering-care/health-equity/ama-racism-threat-public-health
Osborn, L.M., & Woolley, F.R. (1981). Use of groups in well child care. Pediatrics, 67(5), 701–6.
Osterman, M.J.K., & Martin, J.A. (2018). Timing and adequacy of prenatal care in the United States, 2016. National Vital Statistics Reports, 67(3), 1–14. Available: https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_03.pdf
Owens, D.C. (2017). Medical bondage: Race, gender, and the origins of American gynecology. University of Georgia Press. https://doi.org/10.2307/j.ctt1pwt69x
Pachter, L.M., & Coll, C.G. (2009). Racism and child health: A review of the literature and future directions. Journal of Developmental & Behavioral Pediatrics, 30(3), 255–63. https://doi.org/10.1097/DBP.0b013e3181a7ed5a
Paczkowski, M.M., & Galea, S. (2010). Sociodemographic characteristics of the neighborhood and depressive symptoms. Current Opinion in Psychiatry, 23(4), 337–41. https://doi.org/10.1097/YCO.0b013e32833ad70b
Padula, A.M., Humblet, O., Mortimer, K., Lurmann, F., & Tager, I. (2012). Exposure to air pollution during pregnancy and pulmonary function growth in the faces lite cohort A49. Presented at the American Thoracic Society 2012 International Conference, May 20. https://doi.org/10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A1725
Parkinson, J.R., Hyde, M.J., Gale, C., Santhakumaran, S., & Modi, N. (2013). Preterm birth and the metabolic syndrome in adult life: A systematic review and meta-analysis. Pediatrics, 131(4), e1240–63. https://doi.org/10.1542/peds.2012-2177
Pate, C.A., Zahran, H.S., Qin, X., Johnson, C., Hummelman, E., & Malilay, J. (2021). Asthma surveillance—United States, 2006–2018. Morbidity and Mortality Weekly Report Surveillance Summaries, 70(5), 1–32. http://dx.doi.org/10.15585/mmwr.ss7005a1
Patton, G.C., Coffey, C., Carlin, J.B., Olsson, C.A., & Morley, R. (2004). Prematurity at birth and adolescent depressive disorder. British Journal of Psychiatry, 184, 446–7. https://doi.org/10.1192/bjp.184.5.446
Peden, M., Oyegbite, K., Ozanne-Smith, J., Hyder, A.A., Branche, C., Rahman, A., Rivara, F., & Bartolomeos, K. (Eds.). (2008). WHO guidelines approved by the guidelines review committee. World report on child injury prevention. Geneva, Switzerland: World Health Organization.
Pénard-Morand, C., Raherison, C., Charpin, D., Kopferschmitt, C., Lavaud, F., Caillaud, D., & Annesi-Maesano, I. (2010). Long-term exposure to close-proximity air pollution and asthma and allergies in urban children. European Respiratory Journal, 36(1), 33. https://doi.org/10.1183/09031936.00116109
Perreira, K.M., & Allen, C.D. (2021). The health of Hispanic children from birth to emerging adulthood. Annals of the American Academy of Political and Social Science, 696(1), 200–22. https://doi.org/10.1177/00027162211048805
Pizzol, D., Tudor, F., Racalbuto, V., Bertoldo, A., Veronese, N., & Smith, L. (2021). Systematic review and meta‐analysis found that malnutrition was associated with poor cognitive development. Acta Pædiatrica, 110(10), 2704–10. https://doi.org/10.1111/apa.15964
Polacheck, S., & Gears, H. (2020). COVID-19 and the decline of well-child care: Implications for children, families, and states. Center for Health Care Strategies. Available: https://www.chcs.org/resource/covid-19-and-the-decline-of-well-child-care-implications-for-children-families-and-states
Prasad, M.R., Swank, P.R., & Ewing-Cobbs, L. (2017). Long-term school outcomes of children and adolescents with traumatic brain injury. Journal of Health Trauma Rehabilitation, 32(1), e24–32. https://doi.org/10.1097/HTR.0000000000000218
Prenatal-to-3 Policy Impact Center. (2020). Prenatal-to-3 state policy roadmap 2020: Building a strong and equitable prenatal-to-3 system of care. Lyndon B. Johnson School of Public Affairs, University of Texas at Austin. Available: https://pn3policy.org/wp-content/uploads/2020/09/Prenatal-to-3-State-Policy-Roadmap-2020.pdf
Priest, N., Paradies, Y., Trenerry, B., Truong, M., Karlsen, S., & Kelly, Y. (2013). A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Social Science & Medicine, 95, 115–27. https://doi.org/10.1016/j.socscimed.2012.11.031
Provençal, N., & Binder, E.B. (2015). The effects of early life stress on the epigenome: From the womb to adulthood and even before. Experimental Neurology, 268, 10–20. https://doi.org/10.1016/j.expneurol.2014.09.001
Raifman, J., Larson, E., Barry, C., Siegel, M., Ulrich, M., Knopov, A., & Galea, S. (2020). State handgun purchase age minimums in the US and adolescent suicide rates: Regression discontinuity and difference-in-differences analyses. British Medical Journal, 370, m2436. https://doi.org/10.1136/bmj.m2436
Ramírez-Vélez, R., Correa-Bautista, J.E., Villa-González, E., Martínez-Torres, J., Hackney, A.C., & García-Hermoso, A. (2017). Effects of preterm birth and fetal growth retardation on life-course cardiovascular risk factors among schoolchildren from Colombia: The Fuprecol study. Early Human Development, 106–107, 53–8. https://doi.org/10.1016/j.earlhumdev.2017.02.001
Raphael, E., White, J.S., Li, X., Cederin, K., Glymour, M.M., Sundquist, K., Sundquist, J., & Hamad, R. (2020). Neighborhood deprivation and mental health among immigrants to Sweden. Epidemiology, 31(3), e25–7. https://doi.org/10.1097/EDE.0000000000001160
Rauh, V.A., Landrigan, P.J., & Claudio, L. (2008). Housing and health. Annals of the New York Academy of Sciences, 1136(1), 276–88. https://doi.org/10.1196/annals.1425.032
Reading, R., Haynes, R., & Shesnassa, E. (2005). Neighborhood influences on child injury risk. Children, Youth and Environments, 15(1), 165–85. Available: https://www.jstor.org/stable/10.7721/chilyoutenvi.15.1.0165
Regalado, M., & Halfon, N. (2001). Primary care services promoting optimal child development from birth to age 3 years: Review of the literature. Archives of Pediatrics and Adolescent Medicine, 155(12), 1311–22. https://doi.org/10.1001/archpedi.155.12.1311
Reyes, J.W. (2011). Childhood lead and academic performance in Massachusetts. (Working Paper No. 11-3). New England Public Policy Center at the Federal Reserve Bank of Boston. Available: http://www.bostonfed.org/economic/neppc/wp/2011/neppcwp113.htm
Rice, R.L., & Slater, C.J. (1997). An analysis of group versus individual child health supervision. Clinical Pediatrics, 36(12), 685–9. https://doi.org/10.1177/000992289703601203
Ripp, K., & Braun, L. (2017). Race/ethnicity in medical education: An analysis of a question bank for step 1 of the United States medical licensing examination. Teaching and Learning in Medicine, 29(2), 115–22. https://doi.org/10.1080/10401334.2016.1268056
Roby, E., Piccolo, L.R., Gutierrez, J., Kesoglides, N., Raak, C., Mendelsohn, A., & Canfield, A. (2021). Father involvement in infancy predicts behavior and response to chronic stress in middle childhood in a low-income Latinx sample. Developmental Psychobiology, 63(5), 1449–65. https://doi.org/10.1002/dev.22081
Rostad, W.L., Klevens, J., Ports, K.A., & Ford, D.C. (2020). Impact of the United States Federal Child Tax Credit on childhood injuries and behavior problems. Children and Youth Services Review, 109, 104718. Available: https://stacks.cdc.gov/view/cdc/87308
Rudolph, K.E., Stuart, E., Vernick, J., & Webster, D. (2015). Association between Connecticut’s permit-to-purchase handgun law and homicides. American Journal of Public Health, 105(8), e49–54. https://doi.org/10.2105/AJPH.2015.302703
Sabin, J.A., & Greenwald, A.G. (2012). The influence of implicit bias on treatment recommendations for 4 common pediatric conditions: Pain, urinary tract infection, attention deficit hyperactivity disorder, and asthma. American Journal of Public Health, 102(5), 988–95. https://doi.org/10.2105/AJPH.2011.300621
Saigal, S., & Doyle, L.W. (2008). An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet, 371(9608), 261–9. https://doi.org/10.1016/S0140-6736(08)60136-1
Salam, M.T., Islam, T., & Gilliland, F.D. (2008). Recent evidence for adverse effects of residential proximity to traffic sources on asthma. Current Opinion in Pulmonary Medicine, 14(1), 3–8. https://doi.org/10.1097/MCP.0b013e3282f1987a
Sandel, M., Phelan, K., Wright, R., Hynes, H.P., & Lanphear, B.P. (2004). The effects of housing interventions on child health. Pediatric Annals, 33(7), 474–81. https://doi.org/10.3928/0090-4481-20040701-14
Santoli, J.M., Lindley, M.C., DeSilva, M.B., Kharbanda, E.O., Daley, M.F., Galloway, L., Gee, J., Glover, M., Herring, B., Kang, Y., Lucas, P., Noblit, C., Tropper, J., Vogt, T., & Weintraub, E. (2020). Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration—United States, 2020. Morbidity and Mortality Weekly Report, 69(19), 591–3. https://doi.org/10.15585/mmwr.mm6919e2
Schendel, D., & Bhasin, T.K. (2008). Birth weight and gestational age characteristics of children with autism, including a comparison with other developmental disabilities. Pediatrics, 121(6), 1155–64. https://doi.org/10.1542/peds.2007-1049
Schickedanz, A., & Coker, T.R. (2016). Surveillance and screening for social determinants of health-where do we start and where are we headed? Current Problems in Pediatric and Adolescent Health Care, 46(5), 154–6. https://doi.org/10.1016/j.cppeds.2016.02.005
Schneeberg, A., Ishikawa, T., Kruse, S., Zallen, E., Mitton, C., Bettinger, J.A., & Brussoni, M. (2016). A longitudinal study on quality of life after injury in children. Health and Quality of Life Outcomes, 14(1), 120. https://doi.org/10.1186/s12955-016-0523-6
Schwarzenberg, S.J., Georgieff, M., Committee on Nutrition, Daniels, S., Corkins, M., Golden, N., Kim, J., Lindsey, C.W., & Magge, S. (2018). Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics, 141(2), e20173716. https://doi.org/10.1542/peds.2017-3716
Scientific American Editors. (2019, February 1). The U.S. needs more midwives for better maternity care. Policy. Scientific American. Available: https://www.scientificamerican.com/article/the-u-s-needs-more-midwives-for-better-maternity-care
Shafer, P.R., Gutiérrez, K., Ettinger de Cuba, S., Bovell-Ammon, A., & Raifman, J. (2022). Association of the implementation of Child Tax Credit advance payments with food insufficiency in US households. JAMA Network Open, 5(1), e2143296. https://doi.org/10.1001/jamanetworkopen.2021.43296
Sharkey, P., Torrats-Espinosa, G., & Takyar, D. (2017). Community and the crime decline: The causal effect of local nonprofits on violent crime. American Sociological Review, 82(6), 1214–40. https://doi.org/10.1177/0003122417736289
Shiba, K., Hanazato, M., Aida, J., Kondo, K., Arcaya, M., James, P., & Kawachi, I. (2020). Cardiometabolic profiles and change in neighborhood food and built environment among older adults: A natural experiment. Epidemiology, 31(6), 758–67. https://doi.org/10.1097/EDE.0000000000001243
Shonkoff, J.P., Garner, A.S., Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, & Section on Developmental and Behavioral Pediatrics. (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129(1), e232–46. https://doi.org/10.1542/peds.2011-2663
Singhal, A., Tien, Y.Y., & Hsia, R.Y. (2016). Racial-ethnic disparities in opioid prescriptions at emergency department visits for conditions commonly associated with prescription drug abuse. PLoS One, 11(8), e0159224. https://doi.org/10.1371/journal.pone.0159224
Smith, L., Mao, S., Perkins, S., & Ampuero, M. (2011). The relationship of clients’ social class to early therapeutic impressions. Counselling Psychology Quarterly, 24(1), 15–27. https://doi.org/10.1080/09515070.2011.558249
Smith, L., Li, V., Dykema, S., Hamlet, D., & Shellman, A. (2013). “Honoring somebody that society doesn’t honor”: Therapists working in the context of poverty. Journal of Clinical Psychology, 69(2), 138–51. https://doi.org/10.1002/jclp.21953
Stith, S.M., Liu, T., Davies, L.C., Boykin, E.L., Alder, M.C., Harris, J.M., Som, A., McPherson, M., & Dees, J.E.M.E.G. (2009). Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior, 14(1), 13–29. https://doi.org/10.1016/j.avb.2006.03.006
Stonington, S.D., Holmes, S.M., Hansen, H., Greene, J.A., Wailoo, K.A., Malina, D., Morrissey, S., Farmer, P.E., & Marmot, M.G. (2018). Case studies in social medicine—Attending to structural forces in clinical practice. New England Journal of Medicine, 379(20), 1958–61. https://doi.org/10.1056/NEJMms1814262
Stuart, A.L., Mudhasakul, S., & Sriwatanapongse, W. (2009). The social distribution of neighborhood-scale air pollution and monitoring protection. Journal of the Air & Waste Management Association, 59(5), 591–602. https://doi.org/10.3155/1047-3289.59.5.591
Tanne, T. (2021). American Medical Association confronts its racist past with plan for a more equal future. BMJ, 373(1314). http://dx.doi.org/10.1136/bmj.n1314
Taylor, C.M., Golding, J., & Emond, A.M. (2015). Adverse effects of maternal lead levels on birth outcomes in the ALSPAC study: A prospective birth cohort study. British Journal of Obstetrics and Gynaecology, 122(3), 322–8. https://doi.org/10.1111/1471-0528.12756
Taylor, J.A., & Kemper, K.J. (1998). Group well-child care for high-risk families: Maternal outcomes. Archives of Pediatrics & Adolescent Medicine, 152(6), 579–84. https://doi.org/10.1001/archpedi.152.6.579
Taylor, J.A., Davis, R.L., & Kemper, K.J. (1997a). Health care utilization and health status in high-risk children randomized to receive group or individual well child care. Pediatrics, 100(3), e1. https://doi.org/10.1542/peds.100.3.e1
———. (1997b). A randomized controlled trial of group versus individual well child care for high-risk children: Maternal-child interaction and developmental outcomes. Pediatrics, 99(6), e9. https://doi.org/10.1542/peds.99.6.e9
Tessum, C.W., Apte, J.S., Goodkind, A.L., Muller, N.Z., Mullins, K.A., Paolella, D.A., Polasky, S., Springer, N.P., Thakrar, S.K., Marshall, J.D., & Hill, J.D. (2019). Inequity in consumption of goods and services adds to racial-ethnic disparities in air pollution exposure. Proceedings of the National Academy of Sciences of the United States of America, 116(13), 6001–6. https://doi.org/10.1073/pnas.1818859116
Theall, K.P., Shirtcliff, E.A., Dismukes, A.R., Wallace, M., & Drury, S.S. (2017). Association between neighborhood violence and biological stress in children. JAMA Pediatrics, 171(1), 53–60. https://doi.org/10.1001/jamapediatrics.2016.2321
Tikanmäki, M., Tammelin, T., Sipola-Leppänen, M., Kaseva, N., Matinolli, H.M., Miettola, S., Eriksson, J.G., Järvelin, M.R., Vääräsmäki, M., & Kajantie, E. (2016). Physical fitness in young adults born preterm. Pediatrics, 137(1). https://doi.org/10.1542/peds.2015-1289
Tolliver, D.G., Lee, L.K., Patterson, E.E., Monuteaux, M.C., & Kistin, C.J. (2022). Disparities in school referrals for agitation and aggression to the emergency department. Academic Pediatrics, 22(4), 598–605. https://doi.org/10.1016/j.acap.2021.11.002
Treble-Barna, A., Schultz, H., Minich, N., Taylor, H.G., Yeates, K.O., Stancin, T., & Wade, S.L. (2017). Long-term classroom functioning and its association with neuropsychological and academic performance following traumatic brain injury during early childhood. Neuropsychology, 31(5), 486–98. https://doi.org/10.1037/neu0000325
Tsai, J., Ucik, L., Baldwin, N., Hasslinger, C., & George, P. (2016). Race matters? Examining and rethinking race portrayal in preclinical medical education. Academic Medicine, 91(7), 916–20. https://doi.org/10.1097/ACM.0000000000001232
Tsai, S.S., Yu, H.S., Chang, C.C., Chuang, H.Y., & Yang, C.Y. (2004). Increased risk of preterm delivery in women residing near thermal power plants in Taiwan. Archives of Environmental Health, 59(9), 478–83. https://doi.org/10.1097/ACM.0000000000001232
Ullmann, H., Weeks, J.D., & Madans, J.H. (2021). Disparities in stressful life events among children aged 5–17 years: United States, 2019. National Center for Health Statistics Data Brief, 416. Centers for Disease Control and Prevention. Available: https://www.cdc.gov/nchs/products/databriefs/db416.htm
U.S. Department of Agriculture. (2022). Household food security in the United States in 2021. Available: https://www.ers.usda.gov/publications/pub-details/?pubid=104655
van den Bergh, B.R.H., Dahnke, R., & Mennes, M. (2018). Prenatal stress and the developing brain: Risks for neurodevelopmental disorders. Development and Psychopathology, 30(3), 743–62. https://doi.org/10.1017/S0954579418000342
Vandenbergh, J.G. (2004). Animal models and studies of in utero endocrine disruptor effects. Institute for Laboratory Animal Research Journal, 45(4), 438–42. https://doi.org/10.1093/ilar.45.4.438
Voepel-Lewis, T., & Nafiu, O.O. (2017). Reflecting on racial disparities in pediatric care: Can perianesthesia care nurses make a difference? Journal of PeriAnesthesia Nursing, 32(6), 668–70. https://doi.org/10.1016/j.jopan.2017.09.002
Vu, J.A., Babikian, T., & Asarnow, R.F. (2011). Academic and language outcomes in children after traumatic brain injury: A meta-analysis. Exceptional Children, 77(3), 263–81. https://doi.org/10.1177/001440291107700301
Vyas, D.A., Eisenstein, L.G., & Jones, D.S. (2020). Hidden in plain sight—Reconsidering the use of race correction in clinical algorithms. The New England Journal of Medicine, 383(9), 874–82. https://doi.org/10.1056/NEJMms2004740
Washington, H.A. (2006). Medical apartheid: The dark history of medical experimentation on black Americans from colonial times to the present. New York, NY: Doubleday Books.
Webb, E., Hays, J., Dyrszka, L., Rodriguez, B., Cox, C., Huffling, K., & Bushkin-Bedient, S. (2016). Potential hazards of air pollutant emissions from unconventional oil and natural gas operations on the respiratory health of children and infants. Reviews on Environmental Health, 31(2), 225–43. https://doi.org/10.1515/reveh-2014-0070
Weidemann, D.K., Weaver, V.M., & Fadrowski, J.J. (2016). Toxic environmental exposures and kidney health in children. Pediatric Nephrology, 31(11), 2043–54. https://doi.org/10.1007/s00467-015-3222-3
Wen, X., Kong, K.L., Eiden, R.D., Sharma, N.N., & Xie, C. (2014). Sociodemographic differences and infant dietary patterns. Pediatrics, 134(5), e1387–98. https://doi.org/10.1542/peds.2014-1045
Wheeler, W., & Brown, M.J. (2013). Blood lead levels in children aged 1–5 years—United States, 1999–2010. Morbidity and Mortality Weekly Report, 62(13), 245–8. Available: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6213a3.htm
White, J.S., Hamad, R., Li, X., Basu, S., Ohlsson, H., Sundquist, J., & Sundquist, K. (2016). Long-term effects of neighbourhood deprivation on diabetes risk: Quasi-experimental evidence from a refugee dispersal policy in Sweden. The Lancet Diabetes & Endocrinology, 4(6), 517–24. https://doi.org/10.1016/S2213-8587(16)30009-2
Williams, D.R., & Mohammed, S.A. (2009). Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine, 32(1), 20–47. https://doi.org/10.1007/s10865-008-9185-0
Williams, D.R., Mohammed, S.A., Leavell, J., & Collins, C. (2010). Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities. Annals of the New York Academy of Sciences, 1186, 69–101. https://doi.org/10.1111/j.1749-6632.2009.05339.x
Williams, K., Helmer, M., Duncan, G.W., Peat, J.K., & Mellis, C.M. (2008). Perinatal and maternal risk factors for autism spectrum disorders in New South Wales, Australia. Child: Care, Health and Development, 34(2), 249–56. https://doi.org/10.1111/j.1365-2214.2007.00796.x
Williams, M.J., & Eberhardt, J.L. (2008). Biological conceptions of race and the motivation to cross racial boundaries. Journal of Personality and Social Psychology, 94(6), 1033–47. https://doi.org/10.1037/0022-3514.94.6.1033
Winter, A.S., & Sampson, R.J. (2017). From lead exposure in early childhood to adolescent health: A Chicago birth cohort. American Journal of Public Health, 107(9), 1496–501. https://doi.org/10.2105/AJPH.2017.303903
Woodward, N., Finch, C.E., & Morgan, T.E. (2015). Traffic-related air pollution and brain development. AIMS Environmental Science, 2(2), 353–73. https://doi.org/10.3934/environsci.2015.2.353
Wright, J. L., Davis, W.S., Joseph, M.M., Ellison, A.M., Heard-Garris, N.J., & Johnson, T.L. (2022). Eliminating race-based medicine. Pediatrics, 150(1), e2022057998. https://doi.org/10.1542/peds.2022-057998
Wu, F., & Takaro, T.K. (2007). Childhood asthma and environmental interventions. Environmental Health Perspectives, 115(6), 971–5. https://doi.org/10.1289/ehp.8989
Yeter, D., Banks, E.C., & Aschner, M. (2020). Disparity in risk factor severity for early childhood blood lead among predominantly African-American black children: The 1999 to 2010 US NHANES. International Journal of Environmental Research and Public Health, 17(5), 1552. https://doi.org/10.3390/ijerph17051552
Zahran, H., Bailey, C., Damon, S., Garbe, P., & Breysse, P. (2018). Vital signs: Asthma in children—United States, 2001–2016. Morbidity and Mortality Weekly Report, 67(5), 149–55. Available: https://www.cdc.gov/mmwr/volumes/67/wr/mm6705e1.htm?s_cid=mm6705e1_w