5
Child and Maternal Health
Child health is an important driver of intergenerational mobility. Children whose families live in poverty experience worse health early in life than children growing up in higher-income families, and this disparity worsens as they age. Better health in childhood promotes greater educational attainment and leads to better health in adulthood, both of which are important determinants of earnings—a key driver of mobility out of poverty.
Evidence reviewed in this chapter demonstrates that child health has a strong causal connection with future earnings. Moreover, the United States has seen significant reductions both in child mortality, an important measure of child health, and in the association between income and child health (called the income “gradient”), particularly in the case of child mortality (Currie & Schwandt, 2016). Multiple public programs have contributed to these improvements, underscoring the effectiveness of public investments in child health. However, the United States continues to be characterized by higher child mortality rates than other high-income countries, and the income-based gaps in child health, although smaller than they used to be, remain large, suggesting scope for additional investments.
In its investigation of the role child health plays in intergenerational poverty and whether further public investments in child health can effectively increase intergenerational mobility, this chapter begins with a discussion of differences in child health across incomes and racial/ethnic groups. It then presents evidence on the importance of child health as a key determinant of adult earnings. In so doing, the chapter is organized around three main determinants of child health: access to medical care (i.e., family planning services, health insurance coverage, mental health care, and
public care providers such as school-based clinics and the Indian Health Services; environmental influences, including pollution, stress and violence; and nutrition.
After presenting the evidence regarding the importance of the three factors, we discuss promising interventions for which there is evidence of direct impacts on both child health and future earnings.
HEALTH DIFFERENCES ACROSS INCOME, RACIAL, AND ETHNIC GROUPS
Children growing up in households with incomes below the poverty line are born in worse health than other children. This disparity in health increases as they age (Case et al., 2002), culminating in a strong relationship between childhood poverty and adult health (Figure 5-1). In the United States, adults who spent their early childhoods in low-income families are nearly three times more likely than those from higher-income families to rate their adult health as “fair” or “poor” and four times more likely to report health-related restrictions on their daily activities. They are also 30% more likely to have been born with low birthweight, and they report more psychological distress in adulthood.
The links to adult health begin in childhood. Children living in poverty are twice as likely as other children to be hospitalized, miss 22% more school because of sickness, are 18% more likely to have asthma, and are 33% more likely to have a mental health condition (Figure 5-2). They are also 3.5 times more likely to have high blood lead levels (Braveman et al., 2010; Larson & Halfon, 2010; Wood, 2003) and suffer worse oral health (Seirawan et al., 2012). While these disparities in child health by parental income are present in other developed nations, they are more pronounced in the United States (Chen et al., 2016).
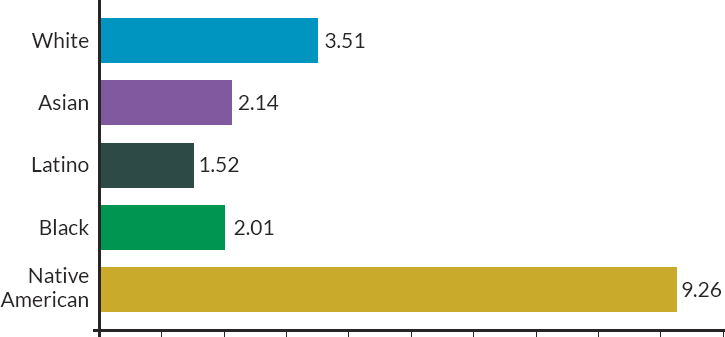
There are important racial/ethnic differences in child health as well. The rate of preterm and low-birthweight births is 50% higher among Black families relative to White families and 30% higher for Native American families (Figure 5-3). Significant disparities are also observed for maternal mortality and for infant and child mortality. In particular, Black and Native American children have considerably higher mortality than all other groups in every age category (infancy, childhood, and adolescence). These disparities in child health are apparent across a range of other measures, including prevalence of asthma and limitations on amount of play, which are similar for Latino and White children but 50% higher for Black children (Mehta et al., 2013). Interestingly, Black and Latino children with asthma are much more likely than White children to visit the emergency room, a result that
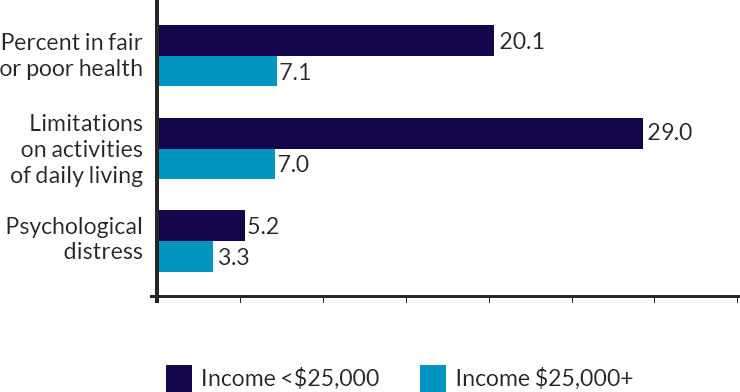
NOTES: Income is measured between the prenatal year and age 2 and is expressed in 2010 dollars. Adult health responses are averaged between ages 30 and 41. Percent in fair or poor health is based on a subjective health rating scale asking respondents whether their current health is excellent, very good, good, poor, or fair. Limitations on activities is measured by the Activity of Daily Living scale and multiplied by 100. Psychological distress is measured by the Kessler Screening Scale for Psychological Distress. All differences are p < .001.
SOURCE: Data from Ziol-Guest et al. (2012), based on data from the Panel Study of Income Dynamics.
is consistent with racial/ethnic differences in the prevalence and severity of this condition but also in access to care. One measure along which Black children fare better than White or Latino youth, and much better than Native American youth, is suicide, as discussed later, though rates of suicide among Black youth have recently grown more quickly.1 These racial/ethnic differences in child health translate into adult disparities in health, with significant labor market consequences. Differences in income across racial groups contribute to, but cannot fully explain, these racial/ethnic disparities in health and suggest that poverty alleviation efforts alone will not close these gaps.
___________________
1 It is important to note that health outcomes for American Indian children are often difficult to measure for multiple reasons, as detailed elsewhere (Stratford, 2018).
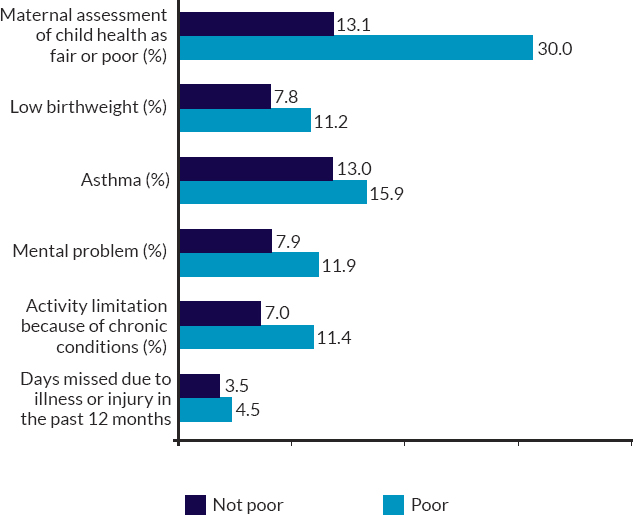
NOTES: Low birthweight is defined as birthweight of less than 2,500 grams (or 5.5 pounds). “Mental problem” includes learning disability, developmental delay, Down syndrome, and autism. “Poverty” is measured by the Official Poverty Measure.
SOURCE: Data from Currie (2009), based on data reported in the National Health Interview Survey 2001–2005.
Sources of the observed racial and ethnic disparities in child health beyond income include exposure to pollution and violence, as well as access to high-quality medical care. Regarding the former, a history of residential segregation by race has resulted in Black children being more likely to live in highly polluted areas (Jbaily et al., 2022; Kodros, 2022; Woo et al., 2019). Regarding disparate access to high-quality medical care, there are multiple causes. Child health insurance coverage does not differ appreciably for Black and White children, largely because of the Medicaid program. Rates of uninsurance are much higher for the Native American and Latino population.2 Other important sources of disparate access to medical care include differences in geographic access, distrust of the medical system based on past injustices, and racial discordance between patient and provider (Alsan & Wannamkaer, 2018; Alsan et al., 2019). Programs
___________________
2 Native American and Latino children have rates of uninsurance that are 13.3% and 8.6%, respectively, compared with 5.4% overall as of 2021 (U.S. Census Bureau, 2022).
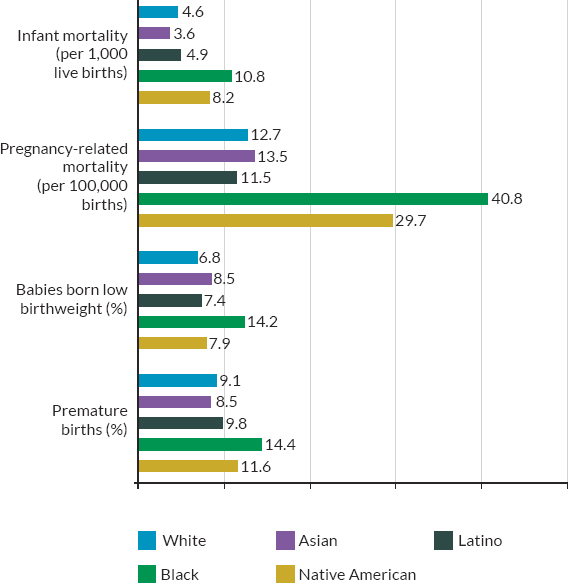
NOTES: Infant mortality statistics are from 2018. Maternal mortality statistics are from 2007 to 2016. Both rates of low birthweight and premature births are from 2020. Infant mortality is defined as the death of an infant before their first birthday. Low birthweight is defined as birthweight of less than 2,500 grams (or 5.5 pounds). Premature birth is defined as birth prior to 37 weeks gestation.
SOURCE: Kaiser Family Foundation (2023).
and policies that fail to address such sources are unlikely to eliminate racial/ethnic gaps in child health.
HOW HEALTH AFFECTS THE ECONOMIC MOBILITY OF CHILDREN
There are many reasons why child health might vary with parental income that would not necessarily imply the causal relationship needed to establish that health is a driver of intergenerational poverty. To isolate the causal impact of parental income on child health, researchers have relied upon natural experiments, including changes in policy that can raise or
lower family income, keeping all other characteristics constant. For example, work based on expansions in tax credits to low-income working families through the Earned Income Tax Credit (EITC) show that this increase in family income during pregnancy significantly improved newborn health (Hoynes et al., 2015). Taking advantage of variation in the earned income of workers between strong and weak labor markets, researchers have found that an additional dollar in earnings yields greater gains in child health at lower levels of family income (Doyle et al., 2007).
Where might these connections between family income and child health come from? A direct route runs from child health to adult health, which in turn affects future earnings via disability, employment, and wages. That is, healthy children grow up to become healthy adults who are more productive in the labor market, generating greater earnings and reducing reliance on public programs. Evidence for this is based on comparisons of siblings (who share the same family and neighborhood environment) showing that less healthy siblings are more likely to grow up to be unhealthy adults and to work less, earn less, and have less income (J. Smith, 2007, 2009; Stephens & Toohey, 2022). Other evidence relies on expansions to Medicaid, the public health insurance program for low-income families in the United States, which improved access to medical care but kept other family characteristics unchanged. Not only did Medicaid expansions improve child health (Currie & Gruber, 1997), but also the effects were long-lasting, reducing adult disability and improved earnings in adulthood (Brown et al., 2020).3
An indirect route is based on the facts that child health can affect cognitive development and schooling, which in turn also affect adult earnings. This evidence is likewise based on sibling comparisons and Medicaid expansions. An example of the former includes a comparison of twin siblings born in Norway between 1967 and 1997 documenting that the twin with higher birthweight (an important marker of prenatal health) grew up to score higher on IQ tests, complete more schooling, and earn more than their lower-weight twin (Black et al., 2007). Other work has confirmed this relationship in U.S. data (Conley & Bennett, 2000, 2001; Royer, 2009). The above-mentioned Medicaid expansions have also been shown to improve educational attainment.
Why does parental income matter for child health? One channel, alluded to above, is access to health insurance and medical care, which is lower for families living in poverty. But there are other ways in which parental income affects child health. Child, and ultimately adult, health is a function of the child’s health at birth, and all subsequent adverse “shocks”
___________________
3 Medicaid expansions for families have also been found to improve financial well-being by reducing medical debt, which has led to reduced borrowing and even evictions (Allen et al., 2019; Baicker et al., 2013; Hu et al., 2018).
to and investments in the child’s health (Currie, 2009). Shocks might include exposure to pollution, food insecurity, stress, and violence, all of which are more common for families living below poverty. There is also evidence that, conditional on an exposure or medical condition, income is protective (Case et al., 2002; Currie & Stabile, 2003). In other words, poverty magnifies the adverse impacts of such shocks on child health. This can also be true even when children have access to medical care. As an example, in an RCT for cancer treatment at a major cancer institute where children received equivalent, high-quality medical care, 5-year survival rates were significantly lower for children from neighborhoods with high poverty rates (Bona et al., 2021). Though the subject of ongoing work, the researchers have hypothesized that this disparity is likely attributable to a combination of worse underlying health prior to diagnosis and treatment, greater barriers to treatment adherence, or increased stress among the families experiencing poverty.
ACCESS TO HEALTH CARE: FAMILY PLANNING, MEDICAID, INDIAN HEALTH SERVICES, AND MENTAL HEALTH SERVICES
Access to Family Planning Services
Low-income families currently have the highest fertility rates, the lowest use of contraception, and the highest unmet need for family planning services. Eighteen percent of sexually active low-income women (below 200% of the Federal Poverty Line [FPL]) report that they are not using contraception even though they are not trying to conceive, compared with 14% nationally (Frederiksen, 2021). This finding is consistent with that of unintended pregnancies, which are higher among women who are adolescents, low-income, racial/ethnic minorities, or single. Those with unintended pregnancies have delayed prenatal care access and have higher rates of preterm birth, an important marker of newborn health with long-term consequences (Haider et al., 2013).
The causal research on the impact of access to family planning services has established that family planning services improve the short- and long-term outcomes of affected families. Bailey (2013) estimates the impact of Title X, the federal legislation in the 1970s that increased financial access to family planning services for low-income mothers, on the long-term outcomes of mothers and their children. To do so, she takes advantage of the roll-out of Title X across counties and over time by comparing the outcomes of families that gain local access to Title X before others. She finds that within a given county, children born after the roll-out of Title X were more likely to complete high school and college, had 2% higher earnings
as adults, and were 7.4% less likely to live in families with incomes below the poverty line than children born before roll-out (Bailey et al., 2019).
This reduction in poverty caused by access to family planning services operates in part through improved economic outcomes for mothers. Women who gained legal access to family planning services in their early childbearing years earned 5% to 11% more per year in their mid-40s than those who did not (Bailey et al., 2012). In other more recent work comparing the outcomes of women who sought an abortion just before reaching the gestational limit for legal abortion with those who just exceeded the gestational limit (and therefore did not receive an abortion), researchers have found that those denied an abortion experience a large increase in financial distress that persists for at least 10 years (Miller et al., 2023).
Access to family planning services also leads to delays in childbearing and reductions in teen parenting. Severe funding cuts to the family planning program in Texas in 2011–2013 led to a 3.4% increase in the teen birth rate, or 2,200 additional teen births over 4 years (Packham, 2017). Estimating the impact of teen parenting on child outcomes is complicated by the fact that teen mothers tend to be drawn from the most disadvantaged families. To address this, researchers have relied on “sister comparisons,” comparing the children of sisters, one of whom gave birth as a teen and one who did not. Unfortunately, U.S. data for this kind of analysis is largely inadequate due to the small sample sizes of surveys and a lack of long-term follow-up information. Exploiting the wealth of administrative data available in Scandinavian countries such as Norway that enable such an analysis, researchers have found that compared with the child of a sister who delayed childbearing, a child born to a teenaged mother completes fewer years of schooling and has lower long-term earnings (Aizer et al., 2022).
Health Insurance Coverage During Pregnancy and Childhood Through Medicaid
A major source of health insurance for low-income families is the Medicaid program, a means-tested public health insurance program that is funded via a combination of federal and state funds. Medicaid has expanded significantly over time since its establishment in 1966 as part of the War on Poverty.4 Medicaid covered 17.5 million children in 1995, and by
___________________
4 In 1966, when Medicaid was founded, the program covered only those families enrolled in the Aid to Families with Dependent Children (AFDC) program. Between 1985 and 1990, Medicaid expanded eligibility to low-income pregnant women and children who were not enrolled in AFDC. In 1997, as part of the State Children’s Health Insurance Program, states could further expand Medicaid eligibility, and finally the 2014 Affordable Care Act (ACA) further increased Medicaid eligibility in those states that opted into the ACA.
2019 this number had doubled to 36 million. Medicaid is a major source of coverage for pregnancy, covering 42% of all births in 2019.
Pregnancy and Post-Partum Care
Even with Medicaid expansions, women with lower socioeconomic status are still significantly less likely to have continuous health insurance for their pregnancies (Admon et al., 2021). If one considers preconception and post-partum coverage as well, only 40% of low-income pregnant women have continuous coverage over this period. This lack of continuous coverage during pregnancy is due to significant churn in the Medicaid program combined with post-partum coverage being limited to only 2 months. Recent legislation made permanent the 12-month extended post-partum coverage option provided by the American Rescue Plan Act in 2021 and utilized by 23 states. Although the option is too new to generate evidence on long-term outcomes, evaluation of the program in Texas suggests it improved access to care, especially contraceptive, preventive, and behavioral health services, and reduced short-interval pregnancies in the first year (Wang et al., 2022).
Childhood
Historic expansions in eligibility for the Medicaid program among children have contributed to significant declines in rates of uninsurance for low-income children over time. For children with household incomes below the poverty line, the share with health insurance rose from 60% in 1987 to 85% by 2012 (Buchmuller et al., 2016). Despite the large expansions in Medicaid, there are still disparities in child health insurance coverage by income, race, and ethnicity.
Children below 250% of the FPL have an uninsurance rate of 7.7%, compared with 3.8% for those above 250% of the FPL. Broken down by race and ethnicity, uninsurance rates are much higher for Native American (13.8%) and Latino children (9.2%) than they are for White and Black children.
Among children who lack health insurance, two-thirds are eligible for Medicaid but not enrolled, suggesting that efforts to increase health insurance coverage by targeting the already eligible and simplifying enrollment and re-enrollment processes are likely to be highly effective. Indeed, increases in the uninsurance rate of low-income children between 2018 and 2020 have been linked to changes in federal guidance that increased administrative requirements for reenrollment (Arbogast et al., 2022). Other work has identified administrative barriers as important in explaining low take-up of public programs, including health insurance (Aizer, 2007; Herd
& Moynihan, 2019; Sugar et al., 2021). Finally, work showing that among children eligible for Medicaid, those whose parents are also eligible are more likely to be enrolled, which suggests that parental ineligibility for Medicaid also contributes to lack of child take-up (Dubay & Kenney, 2003).
A large body of rigorous research links Medicaid expansions in pregnancy and childhood with better health at birth and throughout childhood and even improved future labor market outcomes. To establish this, researchers have taken advantage of the roll-out of Medicaid expansions for pregnant women and children in the late 1980s and early 1990s. The federal government increased Medicaid eligibility levels, but states had discretion in the timing of these expansions as well as the size of the expansion. Examining this variation in the timing of the Medicaid expansions across the states, researchers have linked expanded Medicaid eligibility to improved birthweight and child health (Currie & Gruber, 1996a, 1996b). Given the established causal relationship between newborn health and future economic outcomes, it is not surprising that researchers have also linked these Medicaid expansions in childhood to higher school attainment and earnings later in life (Brown et al., 2020). Expanding Medicaid access to older children is also beneficial: childhood Medicaid expansions reduced the mortality of Black children ages 15–18 by 13% to 20% (Wherry & Meyer, 2016). Recent research has established further intergenerational effects: Access to Medicaid in-utero improves the newborn health of the next generation (East et al., forthcoming).5
Lacking continuous coverage including preconception and post-partum is associated with worse health outcomes for new mothers and their children, including maternal deaths, one-third of which occur in the post-partum period (Johnston et al., 2021). Medicaid expansions through the ACA are associated with lower maternal mortality, with the effects concentrated among non-Latino Black mothers and in later maternal deaths (Eliason, 2020).
Access to Publicly Provided Health Care via the Indian Health Service (IHS)
Native American children experience the worst health along many measures and are more likely to be uninsured than the rest of the U.S. population. Infant mortality, for example, was 60% higher for the Native
___________________
5 Medicaid was introduced in the late 1960s and early 1970s and disproportionately improved the health of low-income mothers and children. Subsequent Medicaid expansions have been shown to have reduced disability and receipt of disability transfers and mortality (Goodman Bacon, 2021).
SOURCE: Centers for Disease Control and Prevention (2023).
American population than it was for the United States overall. Youth suicide is also highest among this group (see Figure 5-4). Access to health care likely contributes to this disparity, as Native American children are more than twice as likely to be uninsured (14%) as U.S. children overall (Roygardner et al., 2019). Native American children are unique in that they are also served by the IHS, a direct provider of health care services.6 However, according to the U.S. Department of Human Health and Services:
Funding for IHS addresses only an estimated 48.6% of the health care needs of Native American children and has historically been subject to year-by-year discretionary allocations from Congress, which creates substantial long-term uncertainty in funding and makes it challenging to maintain and modernize needed health care infrastructure (Office of the Assistant Secretary for Planning and Evaluation, 2022, p. 1).
Given the growing body of research linking access to medical care during childhood and the prenatal period to children’s long-term health
___________________
6 Not all Native Americans are eligible for services from the IHS. Out of every 5.7 Native Americans, 2.7 are eligible. They include those who reside in geographic areas covered by the IHS.
and economic status, the inability to adequately serve all eligible Native American children likely contributes to the intergenerational poverty of the Native American populations.
Access to Mental Health Care
One in five young people in the United States has a mental health disorder that will persist into adulthood, with mental illnesses that emerge before adulthood costing 10 times more than those emerge later in life (Lee et al., 2014). The five most common mental health disorders emerging in childhood and adolescence are attention deficit hyperactive disorder, conduct disorder, anxiety and mood disorders, schizophrenia, and substance use disorder. Mental health conditions are more prevalent among children with family incomes persistently below the poverty line and with children making transitions into poverty (Fitzimons et al., 2017; Wadsworth & Achenbach, 2005). Moreover, mental health conditions are an important predictor of adult earnings. Multiple studies have linked attention deficit hyperactive disorder and other mental health conditions in childhood with worse adult economic outcomes, including employment, earnings, and welfare use (Currie et al., 2010; Fletcher, 2014; Smith & Smith, 2010).
Between 2016 and 2020, anxiety, depression, and behavior and conduct problems increased among children (Lebrun-Harris et al., 2022), with a pronounced increase in depression, suicidal thoughts, and substance use during the COVID-19 pandemic (Mayne et al., 2021). It is important to note that these increases were largely the continuation of an alarming trend in rising rates of depression, suicide, and substance use among adolescents in the United States. In contrast to declines in child and youth mortality more generally, youth suicide rates have increased significantly over time for all racial/ethnic groups, with higher increases among Native American and White youth. Importantly, the method of suicide has shifted to include more use of firearms, which are deadlier.
Substance use disorders, such as the use of marijuana and alcohol, and overdoses among teens also increased during the pandemic (FAIR Health, 2021; Romm et al., 2022). Substance use can have long-term consequences as both the frequency and quantity of substance use during adolescence are strongly associated with a risk of heavy use and misuse in adulthood (Moss et al., 2014; Windle & Zucker, 2010). Substance use during adolescence and young adulthood is associated with neurocognitive and psychological impairment and increased risk for academic underachievement, chronic physical disease, and poor mental health outcomes (Atherton et al., 2016; M. Kim et al., 2017), which in turn lead to adult disabilities.
Mental health conditions are more highly predictive of school outcomes than physical health conditions (Currie & Stabile, 2006). This is also true for outcomes related to employment, marriage, and income in adulthood, with some estimates suggesting that childhood mental health conditions are associated with a 28% decline in earnings at age 50 (Goodman et al., 2011). Adolescents with serious mental health disorders or substance use disorders have seven times greater risk of criminal justice encounters (Prince & Wald, 2018). However, establishing a causal link is complicated by confounding factors.
Some of the strongest evidence of a causal link between mental health and important medium- and longer-term outcomes emerged from two studies based on natural experiments. Examining the timing of school shootings and comparing short- and long-term outcomes of children exposed to a school shooting with similar children living nearby but not directly exposed, researchers established that fatal school shootings result in an immediate increase in prescriptions to treat depression and anxiety that persists over time (Rosin Slater et al., 2020). Using this same setting, researchers have in turn linked this to reduced high school graduation, college enrollment and completion, and earnings and employment at ages 24–26 (Cabral et al., 2021). Together, these two studies point to a causal link between mental health in adolescence and future educational and economic outcomes. Though low-income children are not more likely to be exposed to a school shooting, they are more likely to be exposed to violence and to have mental health conditions. We draw upon the research on school shootings in order to highlight the likely causal relationship between low-income children’s greater exposure to violence, mental health conditions, and worse future economic outcomes.
Conversely, a separate study linked treatment for depression in adolescence with positive schooling outcomes. A natural experiment caused by a 2004 Food and Drug Administration (FDA) decision to issue warnings on antidepressive medications for teenagers provides evidence on long-term academic impacts of adolescent treatment of depression with selective serotonin reuptake inhibitors. The FDA warning resulted in a significant drop in the use of antidepressants among teenagers, which in turn resulted in a significant decline in school outcomes among those affected (Busch et al., 2014).
Treatment for mental health conditions can be effective (see Appendix for more details), but despite this, many children fail to receive treatment for mental health disorders. A 2016 survey covering 50,000 children in the United States found that of those with a mental health disorder, nearly half did not receive needed treatment from a mental health professional, with significant variation across the United States (Whitney & Peterson, 2019). Surveys suggest that lack of treatment stems from a combination of internal
(e.g., limited mental health knowledge, perceived stigma) and external (e.g., costs and the availability of mental health providers) causes (Radez et al., 2021). With 35% of the U.S. population living in an area with a shortage of mental health professionals, it is unsurprising that adolescents often have to wait 1 to 3 months for an appointment with a provider of adolescent psychiatric care (Steinman et al., 2015), with greater barriers to access for racial/ethnic minority individuals (Cook et al., 2016).
Conclusion 5-1: Improving the health of children experiencing poverty has been shown to improve economic status in adulthood as measured by future educational attainment, employment, earnings, and reduced reliance on public assistance. Two important mechanisms include access to family planning services and health insurance coverage in pregnancy and childhood, both of which are key to improving the short- and long-term health and economic outcomes of children. Yet many low-income families are still without health insurance coverage or access to family planning services. This is due in part to administrative barriers that reduce child Medicaid enrollment, the fact that Medicaid coverage for pregnancy often ends 2 months post-partem, an Indian Health Service that serves only half the eligible population, and declines in funding for Title X over time. For access to mental health, additional barriers include lack of providers.
ENVIRONMENTAL INFLUENCES AS A DRIVER: POLLUTION, STRESS, AND VIOLENCE
Pollution
A strong causal link has been established between child health and exposure to pollution, particularly during the in-utero period, based on both epidemiological and quasi-experimental methods (Currie et al., 2011b). More recently, this research has been extended to show causal impacts of childhood exposure to pollution on adult outcomes and even the health of the next generation (Colmer & Voorheis, 2022; Isen et al., 2017). Pollutants that have been the subject of the most study include air pollution (particulate matter [PM] 2.5) and lead. While other pollutants may exert a strong impact on child health, there is less research establishing this connection, in part due to limitations in the number and kind of pollutants that are regularly measured and monitored.7
___________________
7 For example, the Toxic Release Inventory (TRI) requires firms to disclose their use and emissions of listed chemicals. The lists have grown sharply over time as additional research establishes their negative impact on health.
Due in large part to federal action, childhood exposure to pollution (both air pollution and lead) has declined considerably over time. As overall pollution has fallen, so too have income and racial disparities in exposure to pollution, though disparities remain (Bell & Ebisu, 2012; Currie et al., 2023; Jbaily al., 2022; Liu et al., 2015). The major sources of pollution are stationary sources, such as power plants, refineries, and industrial facilities, and mobile sources, such as cars, buses, and planes, which pollute areas near major roadways, along with residual lead (and other toxins) that remains in the environment. Low-income and racial/ethnic minority families have historically been (and continue to be) exposed to more pollution due to the high degree of residential segregation by income and race in the United States, and the concentration of polluting sources in low-income, high racial/ethnic minority neighborhoods (Alexander & Currie, 2017; Teye et al., 2021). For example, children living in more racially segregated cities are exposed to twice the pollution, as measured by fine particulate matter (PM 2.5), than those in less segregated cities, and this difference increases to tenfold when one considers exposure to more toxic metals (Kodros et al., 2022).
Multiple federal policy efforts have been shown to have effectively reduced pollution and improved child health. These include the Clean Air Act (CAA) of 1970 and its 1990 amendments, the federal ban of lead from gasoline and paint, which dramatically reduced the amount of lead in the environment in the decade between 1976 and 1986, and the federal cleanup of Superfund sites, abandoned hazardous waste sites. We discuss the evidence linking each of these policy efforts to reduced pollution and to important short- and long-term outcomes for children. We follow this with a discussion of the evidence on other sources of pollution that are more common and widespread, such as automobile exhaust.
The CAA and its amendments dramatically reduced exposure to particulate matter by roughly 70% between 1970 and 1990.8 Researchers have linked the CAA and its amendments to important short- and long-term outcomes for children. To do so, they took advantage of variation across local areas in whether they were subject to the new CAA rules regarding acceptable pollution levels. Those areas subject to the new pollution limits saw dramatic declines in air pollution levels after the CAA, while those already “in attainment” (i.e., within the new limit for pollution levels) saw no to little appreciable decline in pollution. Reductions in pollution induced
___________________
8 In 1990, the Environmental Protection Agency (EPA) estimated that between 1970 and 1990, “Americans received 20 dollars of value in reduced risk of death, illness and other adverse effects for every one dollar spent to control air pollution” (EPA, 1996). It is estimated that the CAA amendments of 1990 prevented more than 230,000 early deaths (mostly adult deaths) and reduced the number of lost school days by 5.4 million by 2020.
by the CAA were found to improve infant health (Chay and Greenstone, 2003a, 2003b) as measured by infant mortality. More recently, researchers have linked the CAA to long-term outcomes. Children born after the CAA in areas that saw a steep decline in air pollution were found to have increased employment and earnings at age 30, driven in part by reductions in those with earnings in the bottom of the distribution, consistent with declines in disability (Isen et al., 2017, for the 1970 CAA and Colmer et al., 2022, for the 1990 amendments).
Lead is another major source of pollution that has been found to negatively affect child development, with long-term consequences. Recent research has taken advantage of naturally occurring variation in exposure to lead—as a result of federal and local policies that have sought to reduce exposure—to generate causal impacts. It has found that providing incentives to landlords to remediate lead in homes reduced children’s blood lead levels and increased child test scores in reading and math, especially among low-income and racial/ethnic minority households (Aizer et al., 2018). Moreover, work shows that remediating lead paint in homes increases their value (Billings & Schnepel, 2017). Examining variation in exposure to lead over time due to the de-leading of gasoline, by federal mandate, which disproportionately reduced lead levels in children living near roadways, researchers have documented reduced in-school disciplinary infractions, juvenile detention, and adult crime (Aizer & Currie, 2019; Groqvist et al., 2020), important predictors of adult earnings.
However, air pollution and toxic chemicals including lead are still present in the environment. For example, PM 2.5 (fine particulate matter that poses the greatest risk to health), while declining continuously between 1970 and 2016, increased by nearly 6% between 2016 and 2018 (Clay et al., 2021). Likewise, lead, while continuing to decline, still remains in the environment. It is present in water because of lead drinking pipes, is concentrated in the air and the soil near roadways, and remains in homes built before 1978. As a result, low-income and racial/ethnic minority children who are more likely to live near roads and in older homes are still more likely to be exposed to air pollution and other toxic substances including lead than their more advantaged counterparts.
A third area where federal policy has reduced exposure to pollution is the Superfund program. The program, established in 1980, allocates resources to abating the most hazardous sites in the United States. Twenty-one million Americans, 7% of all children under the age of 5, were living within a mile of a Superfund site as of 2020. This population is disproportionately living in poverty and is disproportionately Black and Latino (EPA, 2020). Research has linked Superfund clean-up with improved infant health and student test scores (Currie et al., 2011a; Persico et al., 2020), as
discussed in Appendix C: Chapter 5. Other long-term benefits are likely but have not yet been the subject of research.
Other sources of pollution that are more common and generally below federally determined limits (e.g., automobile exhaust, pollution from coal-fired plants, release of toxic chemicals from manufacturing facilities) have also been linked to important outcomes in children, both short- and medium-term. The installation of EZ-pass tolls on New Jersey and Pennsylvania highways significantly reduced exhaust and air pollution around toll plazas. Researchers linked this decline in pollution with improved infant health, as measured by an 11% and 12% reduction in prematurity and low birthweight, respectively (Currie & Walker, 2011). Public transportation is another important source of pollution for urban populations. A recent study estimated the impact of EPA transit bus emissions standards on infant health. Examining EPA requirements that new buses meet increasingly lower PM thresholds, Ngo (2017) took advantage of variation in bus fleet vintage over the period 1990–2009 in New York City to estimate the impact of proximity to pollutants on infant health. Mothers exposed to the oldest buses gave birth to newborns nearly 100 grams lighter. Still other research, using quasi-random variation induced by declines in coal-based energy production over time and across areas, has linked pollution with child test scores (Gilraine & Zheng, 2022). Given the similar magnitudes of the short-run impacts of the CAA of 1970 and these more common sources of pollution today, it is reasonable to assume they likely have similar long-term consequences given the link between newborn health, child school performance, and long-term outcomes. However, this has not yet been directly established.
Finally, children in families living below poverty and Black children are more likely to live near one of the 300,000 facilities that emit toxic chemicals, known as toxic release inventory sites (Perlin et al., 1999). There is research linking childhood exposure to toxic chemicals at these sites to short-term and (though more preliminarily) to long-term outcomes, including educational attainment and wages. This evidence is discussed in Appendix C: Chapter 5.
Increased Stress in Utero and During Childhood
Lower-income families are exposed to more stressful events than other families, and repeated exposure to stress can result in a greater allostatic role, the physiological response to the body’s neuroendocrine response to stress (Taylor & Seeman, 1999). This can result in the development of maladaptive behaviors and adverse physical and mental health outcomes in childhood (McLoyd, 1997, 1998). Over time, this can make the child more vulnerable to future stressors (Boyce et al., 2021; Shonkoff & Garner, 2012;
Taylor et al., 1997). Stress can affect children indirectly as well, through parental exposure to stress. Parental stress can harm children either by changing parental behavior or through “prenatal programming,” the process by which exposure to environmental influences in utero can affect fetal development, with long-term implications for health and development. In this chapter we focus on in-utero exposure to stress and its impact on offspring outcomes not because it is more important than childhood exposure, but because the finite nature of the in-utero period makes it easier to control for potential confounding, enabling causal inference.
In animal studies, experimental exposure in utero to elevated levels of stress and the stress hormone cortisol leads to worse outcomes for offspring (Harris & Seckl, 2011). Evidence of a causal impact of in-utero stress on child outcomes is new and somewhat mixed, with some work finding negative effects on cognitive development, mental health, and educational attainment (Aizer et al., 2016b; Persson & Rossin-Slater, 2018; Torche, 2018), and another study finding no effect (Black et al., 2016). These studies are based on sibling comparisons in which one sibling is exposed to high levels of maternal stress in-utero and the other is not. There is causal evidence that income transfers via the EITC reduce maternal stress (Evans & Garthwaite, 2014), underscoring the role that poverty and income can play in perpetuating elevated stress in families experiencing poverty.
Researchers have identified racism and discrimination as additional sources of stress faced by Black, Latino and Native American families in the United States (Collins et al., 2014; Nam et al., 2022; Paradies et al., 2015; Sawyer et al., 2012). This has been confirmed in lab experiments in which human subjects are brought into a lab and some are subjected to racist stimuli, which generates a heightened physiological stress response, including increased blood pressure and heart rate, relative to control subjects who are not subjected to the stimuli (e.g., Sawyer et al., 2012). Researchers have long hypothesized that higher rates of stress from racial discrimination may explain the worse child and maternal health outcomes experienced by Black mothers that cannot be explained by differences in income and education (see Braveman et al., 2021).
Establishing a causal link is challenging, as it is difficult to isolate the impact of stress from the stressor itself. Recent work has sought to do so using a somewhat idiosyncratic source of stress: formal complaints of excessive police force in women’s neighborhoods. Black women living in neighborhoods with excessive-use-of-force complaints are 1.2 times as likely to have a preterm birth and 1.4 times as likely to develop cardiovascular disease as women in the same neighborhood before and after an incident, or neighborhoods with otherwise equivalent levels of neighborhood disadvantage and crime. The negative effects for Black women were larger and more precise than those for White women. These results are unchanged
when one limits comparisons to two births to the same mother at different points in time, further reducing the possibility of confounding (Freedman et al., 2022). This finding is consistent with discrimination resulting in greater stress and worse health among Black families. While this has not yet been linked with long-term outcomes of the child, indirect evidence suggests that it likely will have long-term consequences given the relationship between newborn health and long-term outcomes.
Underlying sources of stress in the lives of low-income and racial/ethnic minority families include uncertainty, income volatility, victimization, and discrimination, among others. Policies and interventions that promote stability and reduce discrimination have the potential to reduce stress and improve health, particularly newborn health, an important determinant of adult economic outcomes.9 So too do policies that reduce violence and victimization, as discussed briefly below and in greater detail in the chapter on neighborhood crime.
Greater Exposure to Violence, Especially Gun Violence
Children living in poverty are more likely to be exposed to violence in their communities and their homes (Sedlak et al., 2010). Being a victim of violence affects child health directly through increased mortality and morbidity. Firearm-related injury has risen significantly over time and is now the primary cause of death among children in the United States, surpassing motor vehicle accidents and accounting for 20% of all child deaths (Figure 5-5). There are significant disparities by income and race. Youth in counties with the highest poverty rates had firearm-related mortality rates that were nearly five times higher than those living in counties with the lowest poverty rates (Barrett et al., 2022) and Black children experienced rates of firearm-related deaths (12 per 100,000) that were nearly six times higher than the rates among White children and three times higher than those among Native American children in 2021 (Kaiser Family Foundation, 2022).
Evidence shows that even indirect exposure to neighborhood or family violence (i.e., witnessing or knowing victims of violence) can result in significant long-term harm related to physical and mental health, problem behaviors, and poor academic performance and educational attainment (for reviews see Osofsky, 1999; Rivara et al., 2019; Sharkey, 2018; for more evidence see Bor et al., 2018, and Chapter 9). Perhaps the best evidence of a causal impact of exposure to gun violence on children’s long-term outcomes is the work linking school shootings to short-term mental health outcomes
___________________
9 Practitioners and researchers have developed interventions to reduce the stress response in affected families. However, the evidence linking such interventions to the short- or long-term social and economic outcomes of children is not yet sufficiently developed.
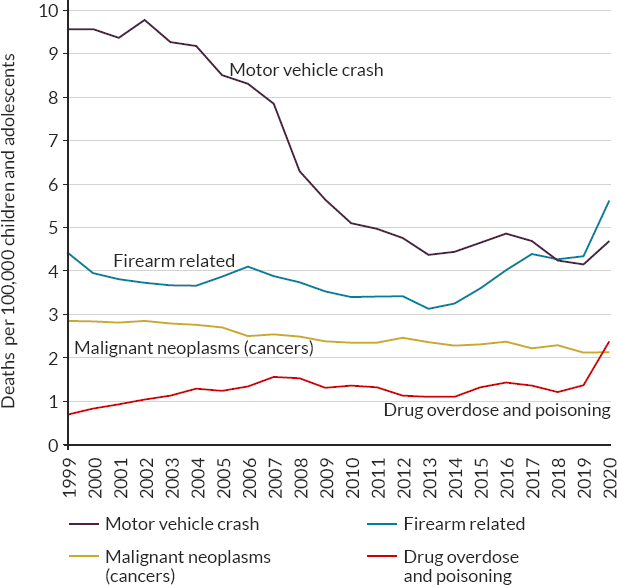
NOTE: Death rates are reported per 100,000.
SOURCE: Adapted from Goldstick et al. (2022) using data from the Centers for Disease Control and Prevention (n.d.).
and long-term economic outcomes. That research addresses confounding in exposure to violence by examining the timing of school shootings and comparing children living closest to the affected schools, and therefore exposed, with those living slightly further away and therefore similar but not exposed themselves (Cabral et al., 2021; Rosin Slater et al., 2020).
To the extent that exposure to violence leads to premature death as well as stress to those indirectly exposed, thereby contributing to intergenerational poverty, we discuss interventions to reduce violence in Chapter 9, which discusses crime and the criminal justice system.
Conclusion 5-2: A child’s environment (pollution, stress, and violence) exerts a strong influence on child health and development, with long-term economic consequences. Federal regulation of pollution has led
to significant improvements in infant and child health and, ultimately, adult income. Due in large part to federal action, disparities in exposure to pollution by income, race, and ethnicity have declined significantly over time. While child mortality has been falling over time, firearm-related violence is on the rise and is now the leading cause of death among all children in the United States, with significant disparities by income, race, and ethnicity. Direct exposure to violence or victimization resulting in premature death and disability, as well as indirect exposure resulting in increased stress, anxiety, and depression with long-term consequences, both contribute to the intergenerational persistence of poverty.
NUTRITION AND FOOD INSECURITY AS A DRIVER
Adequate nutrition during infancy and early childhood (first 1,000 days), the most critical and rapid time for neuronal proliferation, is essential for growth, health, and development for children to reach their fullest potential as adults (Schwarzenberg et al., 2018). Malnutrition, which includes both undernutrition, or the inadequate provision or intake of micro- and/or macronutrients, and overweight or obesity, or the provision/intake of excessive calories, both lead to unhealthy nutritional status.
Many low-income communities and racial/ethnic minority individuals are more likely than others to experience food insecurity, meaning a lack of adequate access to affordable, high-quality, nutritious food (Coleman-Jensen et al., 2022). Food insecurity is defined by the U.S. Department of Agriculture (USDA) as “a household-level economic and social condition of limited or uncertain access to adequate food” and is monitored through regular household surveys by the USDA (2021). Children living in households experiencing food insecurity might not have food insecurity themselves, as parents often compensate. Though household food insecurity has fallen for all groups over time (see Figure 5-6), it is still the case that children in poverty are twice as likely (28% vs. 14%) to live in a household that has experienced food insecurity. As compared with White children, Black children are 3.5 times more likely and Latino children almost 3 times more likely to live in a household that has experienced food insecurity.
Food insecurity during childhood is associated with worse physical health (Gunderson & Kreider, 2009; Thomas et al., 2019) and mental health (McIntyre et al., 2013), lower academic achievement in childhood (Jyoti et al., 2005), and worse psychological distress and physical health during adulthood (Fertig, 2019). Although the evidence linking food insecurity to overweight and obesity is clear for adults, the evidence for the association in children is mixed (St. Pierre et al., 2022). It is important
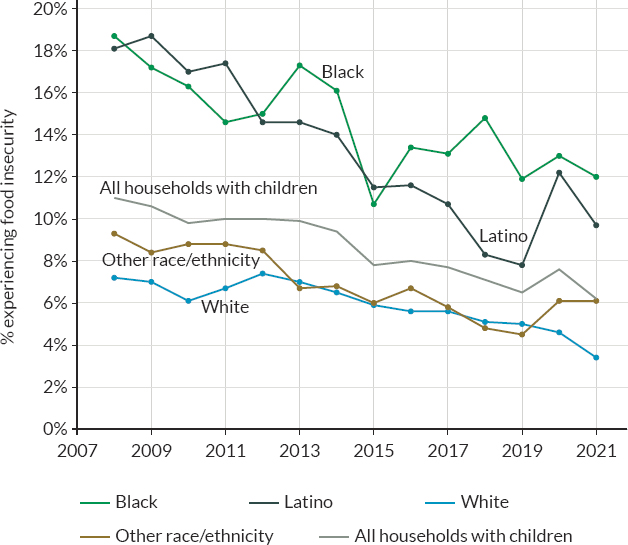
SOURCE: Calculated by USDA, Economic Research Service, using Current Population Survey Food Insecurity Supplement data. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/interactive-charts-and-highlights/#disability
to note that most of this evidence is based on comparisons of children in food-secure and -insecure households controlling for family background characteristics.
To establish the causal impact of nutrition in utero and during childhood on short- and long-term outcomes, researchers have taken advantage of policy changes that increased low-income families’ access to federal nutrition programs (see Box 5-1 for a description of the main programs). Examining the initial roll-out of the federal Supplemental Nutrition Assistance Program (SNAP) during the 1960s and 1970s, researchers have compared the short- and long-term outcomes of children born before and after SNAP became available in their county of birth. The staggered nature of the roll-out allows researchers to compare the long-term outcomes of children born in the same county before and after SNAP became available but also compare those born in same the year but in different counties, one with SNAP
and one not yet with SNAP. Researchers have found that SNAP availability led to improvements in newborn health, improved child outcomes, reductions in poverty, reductions in criminal activity, and improved economic and health outcomes in adulthood (Almond et al., 2011; M. Bailey et al., 2020; Barr & Smith, 2023; Hoynes & Schanzenbach, 2015; Hoynes et al., 2011, 2016). This body of research did not determine the comparative role of SNAP’s nutritional and general economic supplementation.10
One might be concerned, however, that evidence on the long-term benefits of SNAP availability based on the 1960s and 1970s might not generalize to the experience of children in a more recent setting. The current nutritional status of children may differ, and the impact of the creation of the SNAP program may be larger than the impact of marginal increases in SNAP benefit levels. One way to assess this is to compare results for child and adult health based on the roll-out of SNAP in the 1960s and 1970s with evidence from a more recent period. A study based on the period 1996–2003, during which the state of California first eliminated and then restored SNAP eligibility for immigrant parents, shows moderate medium-term effects associated with increases in SNAP benefit levels that are very similar to the effect sizes from the historic roll-out of SNAP (East, 2018; see Appendix C: Chapter 5 for details). This evidence suggests that SNAP benefits today are likely to have similar long-term positive benefits for children as they did in the 1970s.
The Special Supplemental Nutrition Program for Women, Infants and Children (WIC), the other major federal food program for children, is also associated with better nutrition, dietary intake, food security, and health, including birth outcomes. To estimate a causal impact of WIC receipt during pregnancy on newborn health, Currie and Rajani (2015) compared the health of newborns born to the same mother who received WIC for one pregnancy but not the other. In this way, Currie and Rajani controlled for underlying differences in mothers who did and did not use WIC but could otherwise bias estimated effects. She documents significant improvements in newborn health under WIC, as measured by birthweight. This is an important finding given that birthweight is causally associated with educational attainment and later economic outcomes (Black et al., 2007; Royer, 2009).
Despite the positive impact of federal nutrition programs on children, many pregnant individuals and children do not benefit from them. There are two main reasons: lack of take-up among the eligible (relevant for WIC, less
___________________
10 The issue of the “fungibility” of resources from cash and in-kind programs is a general one. In the SNAP studies cited above, we do not know whether cash payments equal in value to the SNAP payments would have generated the same benefits for children. Similar issues arise with housing vouchers (Jacob et al., 2015) and the Medicaid program benefits reviewed above.
BOX 5-1
Federal Food Programs Serving Children
The Supplemental Nutrition Assistance Program (SNAP), formerly known as “food stamps,” is a federal program that provides nutrition benefits to low-income individuals and families below 130% of the Federal Poverty Level (FPL) that are used at participating stores to purchase food. The maximum monthly benefit for a family of four in 2023 is $939. One in five children received SNAP benefits in 2017.
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) provides nutritious foods to supplement the diets of low-income pregnant and lactating individuals as well as infants and children up to age 5 who are at nutritional risk, and also provides information on healthy eating and referrals to health care. Families with incomes below 100% or 185% of the FPL (depending on the state) are eligible for WIC. WIC serves half of all infants in the United States, but take-up falls as children age, declining from 98% to 26% from infancy to age 4.
The National School Lunch Program provides free lunches to children in families below 130% of the FPL and reduced-cost lunch to children between 130% and 185% of the FPL. In the fiscal year 2020, the program provided 2.46 billion free or reduced-price lunches to school children.
so for SNAP), and reduced eligibility in the immigrant population (more relevant for SNAP), as discussed in Appendix C: Chapter 5.
One thing that does not appear to influence child nutrition among low-income families is geographic proximity to high-quality, nutritious foods (i.e., the problem of “food deserts”). While low-income families are more likely to live in food deserts, their nutrition does not improve when high-quality supermarkets enter the local market or when they move to “healthier” neighborhoods (Allcott et al., 2019).
Conclusion 5-3: Today, children living in poverty are still more likely to reside in households that experience food and nutrition insecurity than their better-off counterparts. Evidence from the introduction of the Supplemental Nutrition Assistance Program (SNAP) program in the 1960s and 1970s suggests that food supplements for children in low-income families, both in utero and during childhood, can contribute to intergenerational mobility, improving child health and ultimately future adult health and earnings. Evidence on the impact of SNAP from a more recent period shows similar effects on child health, at least in the short to medium term, suggesting that long-term outcomes of enhancing child nutrition today may be similarly effective in promoting intergenerational mobility. Barriers to take-up in the Supplemental Nutrition
Program for Women, Infants, and Children program eligibility among immigrant families limit the ability of children in the United States to benefit from federal nutrition programs.
INTERVENTIONS INVOLVING CHILDREN’S HEALTH
Our discussion of potential mechanisms focuses on child health interventions for which there is strong direct evidence that they will improve adult earnings and increase mobility. These include the family planning and Medicaid interventions. With regard to pollution, there is direct evidence that reductions in pollution improve child health and future earnings, but many of the current sources of pollution differ from historical sources on which the direct evidence is based, influencing the types of interventions we explore. Finally, the direct evidence on child nutrition is based on historical data, the roll-out of the food stamp program in the 1960s. There is no evidence from more recent time periods of effects of nutrition programs in childhood on adult earnings, but the evidence on medium-term effects of nutrition programs in more recent periods are similar in magnitude to the medium-term effects of the historical program, suggesting that longer-term effects are also likely to be similar.
As discussed in Chapter 1, we characterize the direct evidence for some of the programs or policies as “strong” and denote them with an “*.” This indicates that the program’s or policy’s impact on intergenerational poverty is supported by random-assignment evaluation evidence that has been replicated across several sites or by compelling quasi-experimental evidence based on national or multi-state data or a scaled-up program. We also considered evidence to be direct if strong post-1990 evidence of impacts on pre-adult mediators is coupled with strong pre-1990 evidence on long-run adult impacts in the same domain.
Increasing Access to Health Care Based on Direct Evidence
Family Planning
The main sources of funding for family planning are private health insurance, Medicaid, and the Title X Family Planning program. Recently, low-income families’ access to family planning services has declined due to changes in both public programs. Given the strong causal evidence linking mothers’ access to family planning services to improvements in their children’s long-term outcomes, including teen childbearing, the committee developed the following ideas to increase access to family planning services among low-income families:
- Increase funding for Title X family planning programs from its current level of $286 million per year to at least $500 million per year. Were Title X funds to have increased with inflation since the program’s inception in the 1970s, funding today would be slightly more than $1 billion. However, the significant increases in Medicaid coverage since Title X’s inception suggest that more modest funding for the program is needed to maintain access.
- Ensure that Medicaid beneficiaries have access to family planning services. Because all Medicaid beneficiaries are eligible for family planning services from any willing qualified provider, the Centers for Medicare & Medicaid Services (CMS) could ensure that these requirements are being met in all states.
Medicaid
Strong direct evidence has shown that Medicaid expansions during the prenatal period and childhood lead to better health, greater educational attainment, and higher earnings later in life. With 2.8 million children currently eligible for Medicaid but uninsured, enrolling those already eligible through outreach and continuous enrollment requirements is the most effective way to increase health insurance coverage for low-income families (Kaiser Family Foundation, 2024). The committee developed the following ideas to increase Medicaid enrollment among low-income women and children:
- Expand access to Medicaid with continuous 12-month eligibility and 12-month post-partum coverage even if the family experiences a temporary change in income during the year.
- Make the federal continuous eligibility requirements following pregnancy from 60 days to 12 months mandatory instead of optional. The annual cost of this nationwide was estimated at $466 million in Fiscal Year 2022, increasing to $786 million by Fiscal Year 2030 (Congressional Budget Office, 2020).
Improving the Environment Based on Direct Evidence
Reducing Maternal and Child Exposure to Pollution
Strong direct evidence has shown improvements in child health and increases in adult earnings stemming from the 1970 CAA and its 1990 amendments, as well as the de-leading of gasoline and paint. The current challenges to reducing children’s exposure to pollution, going forward, include the increasingly local phenomenon of pollution, the EPA’s inability to
monitor very local and common pollution sources, the high levels of indoor air pollution that are not monitored by the EPA, and climate change, which is disproportionately affecting low-income communities and communities of color (EPA, 2022). To address this, the committee developed the following ideas:
- The EPA could work with local communities to develop and maintain more local monitoring of air quality using less expensive technologies.
- The federal government, through the CDC and EPA, could provide information and resources to state and local governments to encourage the most efficient lead monitoring and abatement activities and provide appropriate funding.
Reducing Gun Violence
Direct-evidence studies have established that gun violence is both a crime issue and a health issue. That evidence and interventions to address are detailed in Chapter 9.
Improving Nutrition Based on Direct Evidence
Supplemental Nutrition Assistance Program
Numerous studies have shown that the SNAP programs promote intergenerational mobility out of poverty. Changes to several federal policies could address these gaps in coverage and increase food security among low-income children:
- To increase food security for children, remove the 5-year waiting period of SNAP eligibility for legal permanent-resident parents.
- To ensure that all children are adequately covered, eliminate the proration of SNAP benefits for children with undocumented parents.
HEALTH INTERVENTIONS BASED ON INDIRECT EVIDENCE
Increasing Access to Medical Care Among Native American Families
There is no direct evidence linking the IHS to adult poverty, However, the direct evidence on Medicaid likely applies to IHS as both operate by increasing access to medical care. In order to meet the considerable unmet
health care needs of Native American children, there is a need to increase funding for the IHS to levels that would adequately support the provision of services to all eligible children:
- To provide care to all mothers and children eligible for IHS services, increase federal funding to eliminate the funding gap for direct health care services. In 2018, that gap was estimated to cost approximately $7.8 billion.
Increasing Access to Mental Health Care
Given the established link between child mental health and reduced educational and labor market outcomes and the evidence showing significant barriers to receiving care among youth, the CDC could pilot multiple ways to increase child and adolescent access to mental health care, including these:
- Establish and/or expand school-based health clinics so that they include more mental health providers.
- Pilot telehealth access for children and youth in underserved areas.
As noted previously, barriers to youth receiving mental health care include the constrained supply of mental health providers, which can result in either a lack of willing providers or, even if providers are available, long wait times. To increase the number of mental health and substance use disorder providers available to serve youth, the federal government could consider the following:
- Increase funding for physician residency and fellowship positions in psychiatry and expand Medicare’s Health Professional Shortage Area bonus program to attract more mental health providers to underserved areas.
- Expand funding for pediatric mental health integration and support mental health care telehealth access programs.
- The Government Accountability Office could be directed to report on Medicaid payment rates for mental health services compared with medical and surgical services across multiple states and, if justified, raise payment rates for the former.
Reducing Child Exposure to Pollution
Resources provided to the CDC and the EPA would enable agencies to:
- Develop guidelines and recommendations for schools to follow based on their needs and resources to increase the monitoring of air quality in indoor settings and reduce indoor air pollution, particularly in schools. Partnerships could be established between the CDC and the EPA, the states, and local schools, so that air filtration systems are installed/improved as indicated.11
- Issue more stringent EPA regulations of air pollution from vehicles, especially public transportation in dense areas.
- Strengthen EPA monitoring of Toxic Release Inventory (TRI) sites and consider regulating them to reduce children’s exposure to toxic chemicals.
Increasing Child Nutrition via WIC
Several steps could be taken to increase WIC enrollment among low-income women and children and eligibility for children who do not yet have access to school meals:
- Infant certification could be extended to 2 years to prevent churn and increase participation rates within the first 1,000 days. The cost estimate is $380 million.
- Adjunctive eligibility could be allowed for infants, children, and pregnant and post-partum individuals in households that participate in CHIP, Head Start, Early Head Start, or the Food Distribution Program on Indian Reservations. The committee was unable to develop a cost estimate for this policy change.
- Remote services could be provided, including virtual appointments through telephone and video conferencing, as well as remote benefits issuance. Based on COVID-19 changes to WIC rules, the committee estimates the additional cost of continuing remote services to be $53.8 million.
___________________
11 Gilraine (2023) shows that air filtrations in schools reduced pollution and led to a 0.20 standard deviation increase in test scores. While this has not yet been linked with long-term outcomes, the evidence linking outdoor air pollution to greater mobility likely generalizes to the indoor setting.