
8
Financing Children’s Health Care
In 2019, children represented just under one-quarter of the U.S. population, yet only approximately 9 percent of total health care spending (Ortaliza et al., 2021). Expenditures for children’s health care services tend to be disproportionately distributed, with a relatively small share of children accounting for a majority of costs. Children with special health care needs are more likely to have persistently high health care costs than other children, indicating an ongoing need for intense services (Leininger at al., 2015; Liptak et al., 2006). In addition, spending on health care during childhood has been documented to improve health into adulthood and even subsequent generations, and investments in child health can be considered a long-term, multigenerational investment (East et al., 2023; Miller and Wherry, 2018; Wherry et al., 2018). Data from the 2019 National Ambulatory Medical Care Survey reported that while private insurance was the primary expected source of payment for most pediatric office-based physician visits (56 percent), Medicaid was the primary expected source of payment for 39 percent of pediatric office-based physicians’ visits (Ashman et al., 2023). Additionally, Weiss et al. (2022) found that nearly half of pediatric hospital stays were from children with Medicaid coverage in 2019, with approximately 61 percent of hospitalized infants (less than 1 year of age) covered by Medicaid.
Financing of children’s subspecialty care directly affects payments to health care institutions and providers, which impacts provider salary, practice decisions, and, ultimately, provider supply. In this way, financing of child health care affects access to pediatric subspecialty physician care. Financing and payment for specific services, providers, or practice models
also affect access, as lack of coverage or limited reimbursement may limit benefits, scope of practice, or innovations in care delivery. Therefore, while this chapter discusses the financing of children’s health care broadly, the focus is on the issues that are particularly challenging for pediatric subspecialty physicians.
FINANCING AND COVERAGE OF CHILDREN’S SUBSPECIALTY CARE
Specialty health care services for children in the United States are financed through a combination of private and public funds. Private funds include commercial health insurance that is primarily obtained through the parents’ employers and usually paid as an employment benefit. Other private funds include payments made directly by individuals, either for insurance or for services. Public financing is primarily through Medicaid or the Children’s Health Insurance Program (CHIP).1 Medicaid/CHIP funds are a combination of federal and state (and sometimes local) funds, and the federal government matches states’ spending, based on the Federal Medical Assistance Percentage (FMAP). The FMAP is based on a formula set in federal statute that accounts for a state’s per-capita income, relative to that of other states, with lower income states receiving a higher FMAP, and ranges from a minimum of 50 percent to a high of 77 percent in Mississippi in FY2024 (HHS, 2022). The federal government pays different FMAPs for some services, such as family planning or administrative services, or for specific populations (e.g., ACA expansion populations under the Patient Protection and Affordable Care Act [ACA]2 or children covered through CHIP) (MACPAC, 2023a,b). Increased FMAPs have been used by the federal government to provide incentives for states to expand Medicaid eligibility or benefits, to offset state spending and provide fiscal relief during economic downturns, and to finance federal initiatives or priorities that flow through Medicaid (MACPAC, 2023b; Rudowitz et al., 2020). Because Medicaid is an entitlement program, spending is open-ended, which means that the federal government must match allowable state expenditures and states must pay for covered services provided to covered individuals. While the federal government is allowed to accrue a deficit to cover entitlement spending, states generally must balance their budgets each year and cannot run a deficit on Medicaid spending (Rueben and Randall, 2017).
___________________
1 The Children’s Health Insurance Program was enacted in 1997 as a block grant program to reduce the number of uninsured children. To be eligible for CHIP, the child must not be eligible for Medicaid and not otherwise insured (CMS, 2023a).
2 The Patient Protection and Affordable Care Act of 2010, Public Law 111-148; 42 USC 18022 (March 23, 2010).
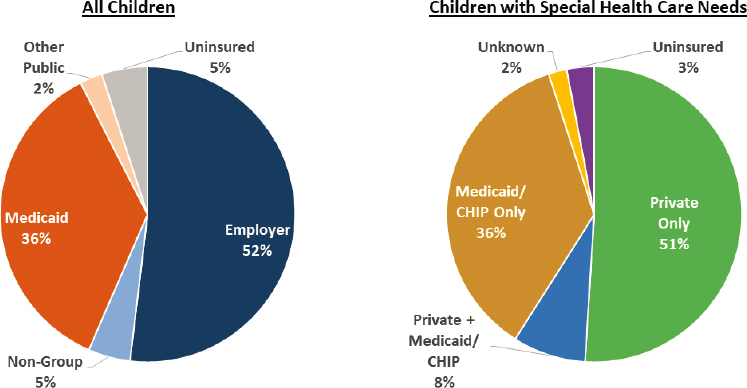
In 2021, the most recent full year for which data are available, half (52 percent) of all children (aged 0–18 years) were covered through private, employer-based insurance; approximately one-third (36 percent) through Medicaid/CHIP; 5 percent through other private insurance (e.g., ACA Marketplace coverage); and 2.5 percent through other public coverage (KFF, 2022a).3 In 2021, only 5 percent of children were uninsured (see Figure 8-1). Pediatric insurance coverage varies by state, reflecting both private coverage rates and variation in Medicaid eligibility levels for children. There are racial/ethnic differences across types of coverage, with more than half of Black, Hispanic, American Indian/Alaska Native, and Native Hawaiian/Other Pacific Islander children covered by Medicaid and CHIP (Artiga, 2022). Children with special health care needs represent a distinct subgroup that includes many children who require specialty care; 44 percent of this subgroup is covered by Medicaid, including 8 percent who have both Medicaid and private coverage (Williams and Musumeci, 2021).
Out-of-pocket payments made by families for cost sharing and uncovered services represent financing for a portion of children’s health care in the United States. In 2016–2017, more than 13 percent of parents reported that they made annual out-of-pocket health care expenses at or above $1,000 for their children’s care (Jones et al., 2021). Over time, as a greater share of children with private coverage are covered through high-deductible health plans,4 some families’ financial burden for health care costs has increased (KFF, 2022b; Larson et al., 2021).
Health care expenditures for children are skewed toward those with higher levels of medical needs, similar to the pattern observed for adults. Within Medicaid, overall, about 10 percent of pediatric-specific spending is for outpatient specialty services (not including behavioral health services); while the distribution of spending on outpatient specialty care was fairly consistent across higher and lower spending groups, spending levels for this service increased from $8 per member per month for the least expensive 80 percent of children to $768 per member per month for children in the top 1 percent of spenders (Kuo et al., 2015). Other work finds that outpatient specialty care is the second highest cost category among Medicaid-covered children with complex chronic conditions (second to pharmacy spending) (Ming et al., 2022) or medical complexity (second to inpatient spending)
___________________
3 Children with end-stage renal disease may qualify for Medicare coverage if their parents meet work history requirements and they need regular dialysis or have had a kidney transplant. In 2021, approximately 1,300 people under age 18 were covered by Medicare (CMS, 2023b).
4 “A developing body of evidence suggests that high-deductible health plans discourage families from seeking high-value and/or medically necessary medical services” (Price et al., 2020). This discouragement decreases inappropriate or excessive use, but also can restrict access to appropriate care (Agarwal et al., 2017; Brot-Goldberg et al, 2017; Price et al., 2020). See Chapter 2 for more information on financial accessibility to care.
1 See https://www2.census.gov/programs-surveys/cps/techdocs/cpsmar21.pdf (accessed June 30, 2023).
NOTES: Data for all children are for 2021 and include children aged 0–19; data for children with special health care needs (CSHCN) are for 2019 and include children aged 0–17. “In this analysis, individuals are sorted into only one category of insurance coverage using the following hierarchy: Medicaid: Includes those covered by Medicaid, Medical Assistance, Children’s Health Insurance Plan (CHIP), or any kind of government-assistance plan for those with low incomes or a disability, as well as those who have both Medicaid and another type of coverage, such as dualeligibles who are also covered by Medicare. Employer: Includes those covered by employer-sponsored coverage either through their own job or as a dependent in the same household. Other public: Includes those covered under the military or Veterans Administration as well as non-elderly Medicare enrollees. Non-group: Includes individuals and families that purchased or are covered as a dependent by non-group insurance. Uninsured: Includes those without health insurance and those who have coverage under the Indian Health Service only.”
SOURCES: KFF estimates for all children are based the Census Bureau’s March Current Population Survey (CPS: Annual Social and Economic Supplements)1, KFF (2022a); For CSHCN, KFF analysis of 2019 National Survey of Children’s Health (Williams and Musumeci, 2021).
(Berry et al., 2014). Similar patterns exist for children covered by other types of insurance, including private insurance.
The benefits covered by private and public health insurance vary substantially, both across states and across insurers. Since 2014, under the ACA most private plans are required to provide, at a minimum, “essential health benefits” that include pediatric services, including oral and vision care.5 However, some plans are exempt from these requirements, and private plans may still impose substantial cost sharing for these services. Private plans also may use limited provider networks as a strategy to manage costs. Medicaid benefits vary by state, although federal law requires all states to provide Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) services to children enrolled in Medicaid. Under EPSDT, states must provide regular medical, vision, hearing, and dental screening as well as services necessary to correct or ameliorate health conditions, regardless of whether these services are otherwise covered under the state’s Medicaid plan. Medicaid covers services not typically covered by private plans, such as non-emergency medical transportation, and long-term services as well as supports that may be required by children who have substantial health care needs. States that provide CHIP coverage through a separate (non-Medicaid) program may provide different benefits under these programs, but many states use a benefits package that is equivalent to Medicaid in separate CHIP programs.
Under both private and public health insurance, most children participate in managed care, under which financing flows to a managed care organization that in turn structures a care delivery system for enrollees. As of 2022, nearly half (49 percent) of people covered through employer-sponsored coverage were enrolled in a preferred provider organization, with nearly all of the rest enrolled in another type of managed care plan such as a health maintenance organization (12 percent), point-of-service plan (9 percent), or high-deductible plan coupled with a managed care plan (29 percent) (KFF, 2022b). As of July 2022, 41 states and the District of Columbia had contracts with Medicaid managed care organizations (Hinton et al., 2022). More than three-quarters of children covered by Medicaid (excluding CHIP) were enrolled in comprehensive managed care organizations, or health plans that cover comprehensive benefits including acute, primary, and specialty care, in 37 of the 41 states (Hinton and Raphael, 2023). Medicaid managed care plans include private for-profit, private non-profit, and public plans, but a small number of private for-profit firms (United Health Group, Centene, Molina, Aetna/CVS, and Elevance Health) account for the majority of Medicaid managed care enrollment (Klukoff et al., 2023).
___________________
5 The Patient Protection and Affordable Care Act of 2010, Public Law 111-148; 42 USC 18022 (March 23, 2010).
In states that have not implemented comprehensive Medicaid managed care, children may receive services on a fee-for-service basis or may be covered by limited service plans (e.g., prepaid inpatient health plans or prepaid ambulatory health plans) or primary care case management arrangements, under which a primary care provider is paid a small, monthly amount per member per month to provide case management services in addition to regular primary care. For children covered through Medicaid managed care, states must still ensure that they receive the full scope of Medicaid services (either through the managed care plan or through wrap-around services). In some cases, Medicaid managed care plans provide additional services beyond those covered in the state Medicaid plan (e.g., social needs services). States and Medicaid managed care plans are subject to federal regulations as a condition of federal matching payments, though states and plans maintain some flexibility in setting standards for network adequacy and payment within federal rules (and subject to federal approval).
The providers that are available to serve children covered by private or public insurance depend not only on the supply of providers in an area but also on contracting and provider enrollment rules. For Medicaid, providers must enroll with each state’s Medicaid program; within federal guidelines, states set standards and requirements for provider enrollment in Medicaid, which at a minimum, mirror Medicare enrollment rules (CMS, 2023c). Providers are not required to participate in Medicaid, and, as discussed elsewhere, may opt out of the program due to low payment rates or other issues. Medicaid managed care plans and private insurance plans contract with a network of providers to serve enrollees in their plans. Network adequacy—or whether health insurance networks include a sufficient number and distribution of providers to ensure access for enrollees—has been a longstanding policy issue across health care and for children’s health care access (MACPAC, 2015). State Medicaid agencies are responsible for developing, publicly posting, and enforcing quantitative network adequacy standards for both adult and pediatric specialists, in addition to other provider types.6 Metrics can include time and distance standards, provider-to-enrollee ratio, and wait time standards; states set their own standards and there are no federal minimums (Schneider and Corcoran, 2022). Some studies have examined network adequacy in the context of ACA Marketplace plans, with research on initial plan offerings in 2014, finding that such plans were more likely to have narrow networks (defined as <10% of available providers in an area being included in the insurance network) for pediatric versus adult specialists (Wong et al., 2017). More recent work has found that narrow networks in the ACA Marketplace have proliferated over time, leading to new proposed federal requirements for network adequacy
___________________
6Network Adequacy Standards § 438.68 (2020).
standards in this market (Pollitz, 2022). Recently proposed federal regulations governing Medicaid managed care would establish new standards for network adequacy and align these more closely with federal rules governing ACA Marketplace plans (Schneider, 2023).
PAYMENT RATES FOR CHILDREN’S SUBSPECIALTY CARE
Payment rates for children’s health care services are largely determined by health plans (in negotiation with providers) or set by state Medicaid programs. In private coverage and Medicaid managed care plans, payment rates take a broad range of forms, including traditional fee-for-service (under which providers are paid per individual service), bundled payments (in which payment is made for an episode of care or for a set of services that are often delivered together), payment models that place providers at risk (e.g., as monthly capitation payments), or pay-for-performance models (in which providers may be paid a bonus or face a penalty depending on whether they meet quality or outcome measures), among others (OECD, 2016). In more recent years, payers have also explored value-based payment models; see Chapter 7 for more information. Private commercial plans set payment rates based on negotiation or proprietary methods. Commercial payment rates are determined by a range of factors, including market forces, competition, and contracting rules. In many cases, commercial insurers pay providers using a method similar to Medicare, though providers in some areas may negotiate “multipliers” to increase rates or have sufficient market power to demand other methods (CBO, 2022). Medicaid rates are similarly determined by market factors but also are governed by additional factors, including state budgets and federal regulations.
Overall, states have substantial flexibility to determine fee schedules that govern fee-for-service Medicaid payment rates (and in some cases, as described below, Medicaid managed care rates), with federal requirements stipulating that payment levels be “consistent with efficiency, economy, and quality of care and sufficient to enlist enough providers so that services under the plan are available to beneficiaries at least to the extent that those services are available to the general population” (42 CFR § 447.204).7 Outside of this provision, known as the “equal access” provision, the federal government has over time issued some additional regulation or requirements for Medicaid payment. Under the Boren Amendment, enacted in 1980 and repealed in 1997, the federal government regulated Medicaid
___________________
7 CMS Requirements for Medicaid Program—Methods for Assuring Access to Covered Medicaid Services, 42 CFR § 447.204 (2016) Under federal law, federally qualified health centers, which focus on providing primary and preventive care, are paid on a prospective payment system (PPS) that reimburses clinics a set amount per visit (MACPAC, 2017a).
payments for institutional providers such as nursing homes and hospitals; as part of the Balanced Budget Act of 1997 that repealed the Boren Amendment, state agencies are required to use a public process to determine payment rates for institutional providers (MACPAC, 2023c; Miller, 2007). In 2015, CMS issued regulations governing Medicaid’s equal access provision, including requirements that states develop access monitoring review plans (AMRP), among other requirements, and that CMS approve any payment changes that could affect access (CMS, 2015). However, the 2015 rule explicitly excluded Medicaid managed care and demonstration programs, and it did not set federal standards for payment or access (CMS, 2015; Rosenbaum, 2015). States and stakeholders have questioned the utility of the AMRP process, and in 2019, CMS proposed to rescind the 2015 rule (CMS, 2019). While the recission was never finalized, in late spring 2023, CMS issued a notice of proposed rulemaking on Ensuring Access to Medicaid Services that acknowledged the limits to the 2015 rule (CMS, 2023d). CMS proposed requirements to “increase the transparency of FFS provider payment rates, update and standardize the requirements for states to submit documentation about proposed payment rate reductions or restructurings, and improve the public comment process for changes to payment rates” (CMS, 2023e). These new rules would require states to post Medicaid fee-for-service payment rates to a publicly accessible website, conduct analysis comparing Medicaid fee-for-service rates to Medicare, and provide documentation for any rate changes that meet certain thresholds of reduction relative to existing rates or Medicare rates (among other provisions) (Manatt Health, 2023).
Multiple legal cases have attempted to use the judicial system as a mechanism to require states to increase Medicaid payment rates, holding that low state payment levels were a failure to adhere to the equal access provision (Berman, 2018; Perkins, 2015; Staman, 2011). However, these cases have failed for a variety of reasons, including the question of whether the plaintiffs (typically providers) have standing or a cause of action to pursue the case. The recent Supreme Court case Health & Hospital Corporation of Marion County, Indiana v. Talevski could have further limited the use of the courts to enforce the equal access provision, as it decided “whether Medicaid beneficiaries can seek relief in federal court when they believe their rights are being violated by state officials” (Rudowitz and Sobel, 2022). In June 2023, the Supreme Court issued a 7-2 decision that reaffirmed the private right of action under Medicaid.8 However, the decision noted that not all federal laws create individual rights, and previous Supreme Court decisions have held that the Medicaid statute does not provide a private right of action for providers and beneficiaries to challenge
___________________
8Health and Hosp. Corp. of Marion Cnty. v. Talevski, No. 21-806 (U.S. Jun. 8, 2023).
payment rates in federal court, making the use of the court as a potential avenue for providers and enrollees to pursue enforcement of the equal access provision uncertain (Rosenbaum et al., 2023).
According to a review by the Medicaid and CHIP Payment and Access Commission (MACPAC):
State Medicaid programs that pay physicians on a direct, [fee-for-service] basis typically pay physicians and other clinicians using a fee schedule that establishes base payment rates for every covered service, as with Medicare and commercial payers. State Medicaid programs generally use one of three methods for establishing base payment rates (fee schedules): the resource-based relative value scale (RBRVS), a percentage of Medicare’s fee, or a state-developed fee schedule using local factors. (MACPAC, 2017b, 2022a)
The review found that 23 states used RBRVS, 15 set fees based on a percent of Medicare fees, and 12 used a fee schedule based on either market assessment or internal processes (MACPAC, 2017b). States also include a variety of adjustments to their fee schedules (e.g., adjustments to reflect geographic cost differences (e.g., urban versus rural) or adjustments to account for site of care (e.g., office versus hospital based); 25 states make upward adjustments for pediatric services. These adjustments, and the mechanisms that they are made by, vary by states. For example, certain primary care and preventive medicine services are compensated at a higher rate for individuals who are 17 or younger in California; rates for child patients are roughly 9 percent higher than those for adult patients. In Michigan, adjustments may be made for providers who care for children with special health care needs; the payment adjustment method determined by the Medical Services Administration is the lesser of the difference between the fee-for-service Medicaid fee screens and the average commercial rate, or the difference between the fee-for-service Medicaid fee screens and the physician’s customary charge. States also use a range of incentive payments within fee-for-service, including supplemental payments for academic medical centers (26 states). The review did not include specific information on other adjustments or payment policies for pediatric specialty care.
Payments through Medicaid managed care plans may be bound by state contracting requirements or payment floors. A 2017 survey of Medicaid managed care plans found that 51 percent of plans set physician rates based on state Medicaid fee schedule, 5 percent based on Medicare fee schedule, and the rest negotiated (38 percent) or set in some other way (6 percent) (Garfield et al., 2018). As of July 1, 2021, 16 states have a directed minimum fee schedule for providers (physicians or other professional services) covered by Medicaid managed care (Gifford et al., 2021). Certain payments under Medicaid managed care (e.g., state directed payments) are subject
to federal regulations and approval. In late spring 2023, CMS issued a proposed rule that would require states to submit an annual analysis that compares Medicaid managed care plan payment rates to Medicare for a limited number of services; the proposed rule also includes several provisions governing use of state-directed payments in Medicaid managed care (CMS, 2023d).
Adequacy of Payment Rates across Payers
A review by the Congressional Budget Office (CBO) concluded that, compared with public payers, commercial insurers face more upward pressure on prices and therefore pay higher rates and increase rates more quickly. The review also found that the ratio between commercial rates and Medicare rates for physician services was higher for specialty care (in which commercial insurance paid 144 percent of Medicare) than primary care (in which commercial insurance paid 117 percent of Medicare), though ratios varied widely by state and even metropolitan area within a state. While CBO did not include conclusions about whether rates were “adequate,” it did note that there is limited evidence of “cost shifting,” or higher commercial rates to providers to offset lower prices paid by public payers (CBO, 2022). Other work has reached a similar conclusion, though most research focuses on hospital cost shifting (Coughlin et al., 2021).
In comparison, there is a great deal of discussion about whether Medicaid rates are too low to cover providers’ and health systems’ costs and thereby contribute to cost-shifting from public to private payers or result in financial shortfalls for providers whose patient panels include a large share of Medicaid enrollees (e.g., pediatric primary care clinicians and subspecialists). While the preponderance of evidence, summarized below, shows that Medicaid payment rates are below other payers, there are some data challenges in directly comparing rates. Many private fee schedules are proprietary (including those used by Medicaid managed care plans) and are not currently publicly available. In addition, analysis of Medicaid fee schedules may not reflect actual payment (because final payment rates reflect a variety of adjustments); a Government Accountability Office study (2014a) that compared fee schedules to payments reported in claims data showed that “fee schedule rates [used in other analyses]…were rarely used in practice” due to adjustments. In some cases, actual payments were lower, reflecting adjustments downward for non-physician providers, though the study also found that payments were frequently higher, reflecting other adjustments including higher payments for services for children. Comparative analysis of fee schedules is also time-consuming and thus typically restricted to a subset of services or procedures, leading to limited insight into services specific to pediatrics in general or pediatric specialty care in particular. Analysis of
claims data can address some of these limitations, but are subject to other challenges, such as inclusion of out-of-pocket payments in assessment of payment for patients covered by private insurance or Medicare or inability to directly compare reimbursement at a service-versus-visit level.
Bearing these limitations in mind, recent studies that compare Medicaid and commercial payment based on claims data find that Medicaid payment is lower, with Medicaid fee-for-service payment lower than Medicaid managed care. A Government Accountability Office (2014b) review of 26 evaluation and management services showed that Medicaid fee-for-service and managed care were generally 27 to 65 percent lower than private insurance. In all but two states included in the analysis, Medicaid managed care payments were at or above Medicaid fee-for-service payments. The report further found that differences in evaluation and management services varied by site of care, with differences being largest in emergency care and smallest in office settings. A 2017 report of differences in payments for child visits to office-based physicians (based on the Medical Expenditure Panel Survey) concluded that the median Medicaid payment per visit was approximately 65 percent of the median payment for private insurance (the mean difference was larger, mainly due to some very high payment for some private visits) (Muhuri and Machlin, 2017). The study also found that differences were consistent across Census regions and consistent across specialties included, with differences for orthopedics being much higher than other specialties. Notably, the private payment rates included out-of-pocket payments (which were applicable in 58 percent of private visits), and the authors noted an inability to adjust for service intensity.
Comparisons of Medicaid and Medicare fee schedules similarly find Medicaid rates generally to be below Medicare, with some variation across states, specialties, or services. Few studies specifically examine services common in pediatric specialty care. The most recent analysis of Medicaid fee-for-service to Medicare fee ratios published by The Urban Institute found that the 2019 national average Medicaid-to-Medicare fee index was lower for primary care (0.67) than for obstetric care (0.80) or for other services (0.78), and only five states (i.e., Alaska, Delaware, Montana, Nebraska, and North Dakota) had average Medicaid fees equal to or higher than Medicare (Zuckerman et al., 2021). The service categories included in the analysis included limited services9 common to pediatric subspecialty care. Other studies that have examined orthopedic surgery (Lalezari et al., 2018), general surgery (Mabry et al., 2016), cochlear implants (Conduff
___________________
9 Other services include endoscopy, dilation and curettage, hysterectomy, cataract removal, tympanostomy, head computerized axial tomography, chest X-ray, pathology, ophthalmologic services, echocardiogram, pregnant uterus echography, and echocardiography (Zuckerman et al., 2021; supplemental materials).
and Coelho, 2017), and musculoskeletal radiology (Santiago et al., 2020) find that while there is most commonly a shortfall between Medicaid rates relative to Medicare, this conclusion does not hold in all states and all services. In other words, while many outcomes show Medicaid payments below Medicare, there was wide variation in the scale of the shortfall, and in some cases Medicaid rates were above Medicare.
COMPENSATION FOR PEDIATRIC MEDICAL SUBSPECIALTY PHYSICIANS
The following sections address the factors that contribute to physician compensation, including payment to physicians, payments to pediatric departments and hospitals, and administrative costs.
Payments to Physicians and the Resource-Based Relative Value Scale
Physician compensation is a factor of the financing system that structures the flow of funds within the health care system, payment rates, and structure of salary or compensation. As mentioned above, provider payment generally may be on a fee-for-service basis (in which providers are paid for each service they provide), a capitated or bundled basis (in which providers are paid a set amount for a population or package of services), a flat salary, an incentive basis (in which providers are paid or penalized according to certain quality goals or other outcomes), or through a combination of approaches.
Based on data from the maintenance of certification surveys for 2018–2022, most commonly pediatric subspecialists (32 percent) indicate that their primary work setting is an academic setting affiliated with a medical school or university, with the remainder working in a nongovernmental hospital or clinic (22 percent), multispecialty group practice (20 percent), or another setting (ABP, 2023).10 In addition, 57 percent of pediatric subspecialists hold a full-time academic position. Salaries for physicians in most academic settings (and private practices within large health care systems) are based on expected clinical productivity, and salaries for faculty members are often determined relative to national benchmarks (developed using data submitted by departments and schools across the country) (Schnapp et al., 2020; Weidemann et al., 2022). Traditionally, faculty compensation is determined using a formula for base salary, with additional rewards for
___________________
10 Calculated on the ABP dashboard by choosing “overall specialty status” under “select to crosstab results” and by choosing the 15 ABP-certified subspecialties under “GP/subspecialty certification filter.”
productivity, seniority, and leadership/administration. As noted in Chapter 5, pediatricians are among the lowest paid specialists, even among primary care specialties (Doximity and Curative, 2023), and pediatricians have significantly lower incentive bonuses as compared with other specialists (Martin, 2021). Incentive bonuses for pediatricians were relatively low, averaging $26,000; only psychiatrists reported a lower average bonus. See Chapter 5 for more information on salaries for pediatric subspecialists. See Box 8-1 for clinician perspectives on payment.
Faculty clinical productivity, which goes into both base salary as well as bonus payments, is often measured by work relative value units (RVUs). Developed in the early 1990s to set physician payment rates in Medicare,
the RVU system is “set nationally for a discrete piece of physician work and attempt to equilibrate aspects of care across specialties” (Schnapp et al., 2020). RVUs consist of three components: physician work RVUs; practice expense RVUs; and professional liability insurance RVUs:
- Physician work RVUs (wRVU): Account for the time, technical effort and skill, medical decision making, and mental stress required to provide a certain service;
- Practice expense RVUs: account for the non-physician labor, equipment, and building space; and
- Professional liability insurance RVUs: factor in the costs of malpractice premiums (Weidemann et al., 2022).
Although RVUs themselves are not monetary values, they can be multiplied by a conversion factor (dollars per RVU) to determine the amount of payment for a service (Weidemann et al., 2022). The Centers for Medicare & Medicaid Services (CMS) and most private payers have used the RVU system for physician payment since 1992 (Weidemann et al., 2022). As outlined in the 2021 National Academies of Sciences, Engineering, and Medicine (National Academies) report, Implementing High-Quality Primary Care, the resource-based relative value scale, and the process for updating it, have “contributed to the differences in compensation across specialties, the distribution of physicians across specialties, inefficient distortions in use, and inadequate beneficiary access to undervalued services” (NASEM, 2021, pg 291; MedPAC, 2018). In general, the system leads to lower payment for not only primary care, but also specialty care outside of surgical or procedural services. The report further asserts that because changes to Medicare’s fee schedule must be budget neutral, evaluation and management codes “have become passively devalued in the PFS [physician fee schedule] as their relative prices fall as a result of other service prices (including new technologies) increasing” (NASEM, 2021, pg.291). The National Academies report identified a variety of other factors contributing to this devaluation, including overestimation of work time for some procedures; lack of reevaluation of RVUs for these services; difficulty in the estimation of time, skill, and effort for evaluation and management services, among others. As a result, PFS is “oriented toward discrete, often procedural, technical services” (NASEM, 2021). Recent efforts to change misvalued codes resulted in significant upward revision for office visits (CMS, 2020). However, CMS efforts are hindered by “the lack of current, accurate, and objective data on clinician work time and practice expenses” (NASEM, 2021; GAO, 2015; Mulcahy et al., 2020; Wynn et al., 2015; Zuckerman et al., 2016). The multispecialty Relative Value Scale Update Committee, which includes members from 26 specialties, provides input to CMS for determining the
physician fee schedule for RVUs. However, despite the inclusion of only one pediatric representative on this committee, the determination of RVUs for all pediatric services is made primarily based on this input (Moore et al., 2008). Although the Relative Value Scale Update Committee provides recommendations, CMS makes all final decisions about payments and can accept or modify these recommendations, though CMS has historically deferred to nearly all the Relative Value Scale Update Committee’s recommendations (AMA, 2023; GAO, 2015; NASEM, 2021).
Current challenges with existing fee schedules are particularly problematic for pediatric subspecialty care. Because the RVU system is Medicare-driven, CMS acknowledges that it “underrepresent[s] or undervalue[s] some components of pediatric work” (AAP, 2008). As a result, the RVU system may overvalue services to adults (Massoumi et al., 2021; Weidemann et al., 2022). RVUs may undervalue the physician work input for pediatric care: Because children are accompanied by their parents, creating a triadic relationship, and may take more time to gain cooperation in the health care process than adult counterparts, services and procedures for children require more face-to-face time, more education, more information-giving and counseling, more emotional support, and more communication with child care facilities, schools, or absent parents, which can increase post-service time for an encounter (AAP, 2008; Lakshminrusimha et al., 2023). Furthermore, practice expenses for pediatric services may be higher than for adult care due to the need for more direct hands-on time by clinical staff, more case management, higher telephone call volume, and other factors (e.g., cost of supplies in multiple sizes for inpatient pediatric units). A study of pediatric nephrology payments noted that increases in fees for pediatric codes for dialysis were lower than those for adult dialysis, even though management of children on dialysis may be more time-consuming (Weidemann et al., 2022).
Furthermore, the weighting of the RVU system to procedure-based specialties persists in pediatric care, leading to differences in payment not only across pediatric subspecialties, but also between pediatric and adult specialists. An analysis of the application of the RVU system to pediatric nephrology noted that technological advances have generally increased efficiency for procedure-based practice (i.e., allowing more procedures in less time); they have decreased efficiency for non–procedure-based practice through the need for extensive documentation in the electronic record; and these documentation requirements are particularly burdensome for pediatric care (Weidemann et al., 2022). In addition, compared with adult specialists in the same field, pediatric specialists may have fewer procedures and thus lower RVU expectations, which partially accounts for salary levels. Recent analysis of productivity benchmarks for pediatric subspecialists found that the median productivity per 1.0 clinical full-time equivalent is
lower for many non-ICU pediatric medical subspecialists compared to their adult counterparts (Lakshminrusimha et al., 2023). Lower patient volumes, particularly for subspecialists who are not practicing in freestanding large children’s hospitals, also contributes to lower RVUs, as clinicians must be on call and cover services in between a predominantly outpatient schedule (Lakshminrusimha et al., 2023). Lower RVUs also affect RVU-based bonus payments available to providers. A study of pediatric rheumatology found that the RVU expectation for pediatric rheumatologists was about 70 percent of that for adult rheumatologists (Singer and Onel, 2019). The incentives in the RVU system and conclusion that the care of complex patients is “inadequately captured in the RVU model” (Weyand and Freed, 2020) also impact patient care by creating incentives for referrals, fewer “curbside” consultations, or focus on ongoing monitoring for patients whose acute issues have been resolved. See Box 8-2 for trainee and clinician perspectives on RVUs.
Payments to Pediatric Departments and Hospitals
Provider reimbursement is also a factor of the flow of funds within a department and institution. Department chairs have a significant role in setting salaries and incentives for clinical faculty as well as allocating the amount of time to be spent on research, patient care, education, and administration. In turn, department budgets are a function of professional fees collected, hospital agreements for time spent in administrative and operational functions, and other funds that flow to the department from the larger institution. (Departments within academic institutions also have other revenue sources, e.g., grants and teaching agreements.) Departments are part of the larger institution, which may also collect supplemental payments. These are not tied to a specific service, such as those targeted to graduate medical education (see Chapter 5 for more information about graduate medical education payments) or payments to support safety net providers.
Analysis of Medicaid payment rates shows that, like provider payment rates, base payments to hospitals are often below hospital costs of providing services to Medicaid beneficiaries, leading to what is known as the “Medicaid shortfall” (MACPAC, 2022b). While other payers may also pay below costs, a recent analysis found that underpayment to children’s hospitals (defined as payment below calculated costs) was more frequent for Medicaid compared with private payers (VonAchen et al., 2021). Medicaid disproportionate share (DSH) payments are supplemental payments intended to provide financial assistance to hospitals that serve a relatively high share of Medicaid or low-income patients, in part to offset the Medicaid shortfall (MACPAC, 2023d). DSH funds are allocated from the federal government to states, which then distribute funds to providers within broad federal guidelines. States may also make other supplemental Medicaid payments to hospitals through other mechanisms, including upper payment limits that “allow states to make up the difference between a reasonable estimate of what Medicare would pay and Medicaid payments” (in aggregate within a type and class of providers) (Rudowitz, 2020) and state directed payments (SDPs), under which a state directs a Medicaid managed care organization to pay providers certain rates or payment methodologies (MACPAC, 2022c).
Health care institutions that treat a relatively large share of patients covered by Medicaid may recoup some of the difference in reimbursement rates through supplemental payments. However, analysis finds that Medicaid DSH funds are poorly targeted, with “little meaningful relationship between DSH allotments and the number of uninsured individuals; the amounts and sources of hospitals’ uncompensated care costs; and the number of hospitals with high levels of uncompensated care that also provide
essential community services for low-income, uninsured, and vulnerable populations” (MACPAC, 2022b, pg. 105). MACPAC finds that, in some cases, supplemental payments may fully cover hospital costs, while in other cases, hospitals still face a shortfall relative to the cost of care for Medicaid patients (MACPAC, 2022b). Supplemental payments also typically flow to the institution and, depending on that institution’s policies, may or may not flow to pediatric subspecialty departments or providers.
Given the different role of Medicaid for varied patient populations as well as how RVUs affect reimbursement in different specialties, some institutions take steps to rebalance resources across departments or support services that provide capacity but are not profitable through funds flow. “Funds flow arrangements define the financial relationships between departments, medical centers, and university entities within a coordinated academic health system” (Josephson et al., 2020, pg. 785). The clinical revenue from hospitals and medical centers represents the majority of financial support to its associated entities. The revenue generated by clinical activities is usually allocated to clinical departments to cover the costs of the centralized faculty practice plan, including faculty compensation and employee benefits (Miller et al., 2012). “System” funds may then be redistributed across entities and departments to fund the academic or other underfunded activities that are central to the organization’s mission (Itri et al., 2017; Miller et al., 2012). Clinical departments that generate excess revenue may be used to support other departments that are not generating sufficient revenue to cover their own expenses. The allocation of funds among clinical departments is often negotiated among the department chair, the hospital, and the dean, and the dean may have the discretion to use the surplus generated by one department to cover the expenses of other clinical departments (Miller et al., 2012). Funds flow formulas may be based on the “shortfall” of payments per RVU needed to meet needs, calculations of FTEs needed to staff services, or some combination of both (Lakshminrusimha et al., 2022). There are a broad variety of arrangements, corporate structures, and relationships among affiliated entities. Financing within health care institutions has been described as a black box due to the seemingly randomness of typing specific revenue streams to concepts such as “knowledge” or “population health” (Miller et al., 2012).
Administrative Costs
A final aspect of reimbursement is administrative costs. Administrative burden on providers may result from a range of factors, including medical records, health insurance authorizations or referrals, care coordination, billing, or other factors. Much evidence shows that providers’ administrative burden in the United States is substantial and has increased in recent years
(Casalino et al., 2009; Erickson et al., 2017; Himmelstein et al., 2014; West et al., 2018). Administrative duties may be seen as a “hassle” for providers and may also affect payment, especially if these factors lead to denied claims or take time away from other billable activities (Dunn et al., 2023). Administrative burdens are a major contributor to “burnout” or job dissatisfaction (Apaydin, 2020; Frintner et al., 2020). To the extent that these administrative duties vary by specialty or payer, they also may influence physician practice or career decisions, as discussed below. While administrative burdens may be universal, there is some evidence that certain factors that particularly affect pediatric specialists lead to heavy administrative burdens. For example, research non-specific to pediatrics finds that, within an academic medical center, administrative costs are higher for specialty care compared with primary care (Tseng et al., 2018). Other research finds that insurance denial rates are higher in Medicaid compared with other payers, leading to lower payment for these patients, lending evidence to the idea that providers with a relatively higher share of Medicaid patients may face higher administrative costs (Dunn et al., 2023). This evidence builds on previous work showing that Medicaid reimbursement delays can offset increases in Medicaid reimbursement rates to the point that “increasing these rates may be insufficient to increase physicians’ participation unless accompanied by reductions in administrative burden” (Cunningham and O’Malley, 2009).
HOW FINANCING AND PAYMENT TIE TO PROVIDER SALARIES, PRACTICE DECISIONS, AND ACCESS TO CARE
Most studies that have examined the link between payment rates and provider availability have focused on Medicaid and used outcome measures such as appointment availability, insurance participation, or patient use. Several studies have examined the effect of the Medicaid primary care payment bump under ACA, which increased primary care rates to Medicare rates for 2 years in 2013 and 2014. Results are mixed, with most research finding increases in self-reported Medicaid participation (Tang et al., 2018), improvement in patient-reported difficulty finding a provider (Alexander and Schnell, 2019), and appointment availability for new patients (Candon et al., 2018; Polsky et al., 2015), but others finding no effect of the payment bump on Medicaid participation or service volume (Decker, 2018; Mulcahy et al., 2018). Other work has looked more generally at associations between Medicaid primary care payment rates and provider participation and found that states with higher average Medicaid payment rates have higher rates of appointment availability for new patients (Sharma et al., 2018) or physician participation in Medicaid (Holgash and Heberlein, 2019). Findings based on primary care may not be fully applicable to pediatric specialty
care, where physicians may be less likely to opt out of Medicaid due to the higher share of patients with this coverage type as well as policies of their institutions. There is more limited research that examines payment rates and provider availability among specialists. Other studies have found an association between Medicaid rates for dental care and access to dental services (Buchmueller et al., 2015; Chalmers and Compton, 2017).
While evidence points to a link between payment rates and provider availability or insurance participation, there is less direct evidence that in turn links payment rates to overall provider supply. Studies have examined how salary expectations (which are in part driven by payment rates) relate to career decisions among physicians. (See Chapter 5 for more on the influence of earning potential on career choices.)
While there is not a robust evidence base regarding the implications of a lack of parity between Medicare and Medicaid payments, the committee’s collective judgment is that the lack of parity is a major driver for the financial disincentives to pursuing a career in a pediatric subspecialty, which, in turn, contributes to access challenges for children. The general ethical rationale for parity between Medicaid and Medicare payment rates is that if Medicaid payment rates are too low, it may be difficult for health care providers to accept patients with Medicaid coverage. This limitation in access to high-quality care for children with Medicaid coverage could lead to disparities in access to care and health outcomes. As noted previously, comparisons of Medicaid and Medicare fee schedules generally find Medicaid rates to be less than Medicare, with some variation across states, specialties, or services. Given the large percentage of children on Medicaid, there are disproportionately larger adverse effects on reimbursement and compensation for pediatric care (as compared with adult care). These disparities in the compensation of health care providers can be considered unfair or unjust. Perrin et al. (2020) argued that “both the federal government and state governments haven’t consistently enforced the federal requirement that Medicaid provide payments that are high enough to ensure that people with Medicaid coverage have as much access to care as people with commercial insurance” (pg. 2597). The 2021 National Academies report on high-quality primary care also discussed Medicaid payment rates in the context of access to primary care:
As the nation’s second largest payer, with disproportionate numbers of children and high-needs beneficiaries, Medicaid needs a primary care strategy that addresses the low rates state Medicaid agencies and their contractors pay for primary care, which limits children’s access to it. CMS should lead this strategy, and its state partners should implement and enforce it. Reforming Medicaid to mirror Medicare’s payment standards may be the most straightforward path to ensuring equitable access to high-quality
primary care for its beneficiaries. Short of that, modifying federal access-to-care standards for state Medicaid programs can catalyze state and managed care organization payment and coverage policies to prioritize high-quality primary care. Meeting federal and accrediting bodies’ access standards will require states and their contracted managed care organizations to take the necessary actions, including increasing Medicaid rates for primary care and expanding primary care provider networks as needed. (NASEM, 2021)
During the committee’s public webinars, Sara Rosenbaum, Harold and Jane Hirsh Professor of Health Law and Policy and founding chair of the Department of Health Policy at George Washington University’s Milken Institute School of Public Health, testified about the significance of Medicaid rates for pediatric subspecialty care:
Even though there are all these complex reasons for access problems, you cannot get anywhere in my view until you have leveled the playing field on rates…it means a reasonably competitive rate…in the case of pediatrics, it is a much deeper issue than just what any individual provider gets paid because it obviously affects the entire structural soundness of pediatric subspecialties….It makes it that much harder to attract people into subspecialties where the financial stability of the subspecialty is open to question because so many children are publicly insured, and public payers just pay much lower rates….It is a foundational issue where the subspecialties are concerned. As far as I can tell and the same is true for adult subspecialties, adults just are not as prevalent [of a] part of the [Medicaid] population and therefore impact of high Medicaid dependence is not so much in evidence…everybody knows it is more complicated than rates. But everybody also knows that you cannot get anywhere without fixing the rates. You are really doing major damage in the case of pediatrics because of the role of Medicaid.…Medicaid is incomparable as a source of pediatric coverage, but the rate issue should be taken off the table and then we can go to work on the other access barriers.11
To address inequities in payment for pediatric subspecialty services, various mechanisms could be considered, that may differ by state. States can simply increase provider payment rates, as some states have done over time. For example, in FY2022, 16 states reported increasing payment rates for specialist physicians, and 17 states reported plans to do so in FY2023 (Hinton et al., 2022). While states that increase Medicaid payment rates will receive commensurate increased federal funds (based on the FMAP),
___________________
11 The webinar recording can be accessed at https://www.nationalacademies.org/event/11-14-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-meeting-4.
limits in state funds may restrict the ability of states to pursue this option. Further, the simplicity of this mechanism means states also may target provider payment rates for cuts as a cost-saving area during economic downturns (Smith et al., 2010). Some states have used supplemental federal funds previously to increase provider rates. For example, Gould and Honsberger (2022) reviewed how states used expanded federal funding to states’ Medicaid Home and Community-Based Services (HCBS) programs (including a one-year, 10-percentage-point FMAP bump to Medicaid HCBS) so states can use the increased federal funds to address payment. Five states have outlined their intention to raise rates paid to providers (direct support professionals for children and youth) for HCBS covered through specific waivers or state plan amendments; four states plan to raise rates paid for certain services to support in-demand specialty providers; Washington State proposed directing funds to managed care organizations to increase provider payments for wraparound mental health services for youth; and West Virginia proposed a temporary 70 percent increase in reimbursement rates for services covered under the state’s Children with Serious Emotional Disorder Waiver, which covers HCBS for youth with severe mental disorders (Gould and Honsberger, 2022). These mechanisms are not the only ones that could be successful in addressing inequities in payment for pediatric subspecialty services through supplemental federal funding but are listed only as examples.
During the committee’s public webinars, the impact of financing of children’s health on the pipeline and retention of pediatric subspecialists as well as the overall sustainability of children’s health care were highlighted by multiple speakers:
So much of this unfortunately comes down to finances….I work in a children’s hospital within an adult health care system. You have to constantly, constantly fight for children here….The reimbursement and opportunity for system margin, for example, is basically disincentivized for development of programs for children with complex needs, and it ultimately leads to downward pressure on salaries for pediatricians.12
– Stephanie Duggins Davis, Edward C. Curnen, Jr., Distinguished Professor and Chair for the Department of Pediatrics at the University of North Carolina at Chapel Hill
Academic medical centers are traditionally described as having this tripartite mission that resembles a three-legged stool…with clinical care, education, and research, all given equal importance. But I recently heard
___________________
12 The webinar recording can be accessed at https://www.nationalacademies.org/event/07-19-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-webinar-1.
a different analogy, and that is [that] the reality of the academic medical centers now resembles a tricycle with clinical revenue functioning as the big wheel sort of pulling the other two along. So, we really rely on the clinical margin to fund the research and education mission. Our problem in pediatrics is that the front wheel is not very big. We are an independent children’s hospital here, but when we looked at the clinical margin across the entire health system at Stanford, the Department of Pediatrics was less than 5 percent of that clinical margin—despite the fact that…we’re the second biggest department. So, the front wheel is not very big and it’s not very big because Medicaid and children’s health insurance programs reimburse physician services in pediatrics at much lower rates than Medicare…this has really important implications for physician compensation…it has huge implications for funding the education programs…if my front wheel of my tricycle was bigger, if we had Medicaid equity, funding the research and education mission would just be much more possible.13
– Mary Leonard, Arline and Pete Harman Professor and Chair of the Department of Pediatrics at Stanford University; director of the Stanford Maternal and Child Health Research Institute; and physician-in-chief of Lucile Packard Children’s Hospital
[Pediatrics is the] department that is thought of secondarily to all of the adult needs. It becomes the role of the department chair of pediatrics to fight that apathy toward children’s health, every day in our health systems…it is something that could be solved through putting children’s health first, starting with reimbursement….There is not as much margin as adult departments and surgical departments to continue allowing for research, training, and development of [physician–scientists]. What this leaves us with is a therapeutic pipeline for children that’s really threatened by not having enough bright new minds going into the field and really leaves out children when it comes to early adoption of novel therapies…with more investments into our pediatric clinical care, that big wheel of the tricycle, there could be more opportunity to think about diversifying careers in ways that are going to help us deliver better care, like focusing on quality, like focusing more on research, focusing more on our diversity and our health equity…the way that we fund health care so poorly from Medicaid is leading to segregated settings of care by payer. And that needs to be brought to light and done away with.14
– Sallie Permar, Nancy C. Paduano Professor and Chair of Pediatrics at Weill Cornell Medicine and pediatrician-in-chief at New York-Presbyterian/Weill Cornell Medical Center
___________________
13 The webinar recording can be accessed at https://www.nationalacademies.org/event/07-19-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-webinar-1.
14 The webinar recording can be accessed at https://www.nationalacademies.org/event/07-19-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-webinar-1.
I think a fair and equitable workforce will follow if we have an equitable reimbursement and finance system.15
– Harold Simon, Marcus Professor and Vice Chair, Department of Pediatrics, Emory University School of Medicine and Children’s Healthcare of Atlanta
KEY FINDINGS AND CONCLUSIONS
Key Findings
Finding #8-1: While rates of commercial coverage are similar between children and adults, Medicaid covers 35 percent of children and a higher share of children with complex medical needs. State Medicaid agencies have discretion in setting payment rates depending on state rules. Private insurers set payment rates based on market forces, negotiation, and other proprietary factors.
Finding #8-2: Comparisons of Medicaid and Medicare fee schedules generally find Medicaid rates to be less than Medicare, with some variation across states, specialties, or services.
Finding #8-3: Efforts to increase Medicaid payment rates through litigation under the equal access provision have been unsuccessful, the federal government has issued limited regulations to enforce the equal access provision, and there has been limited oversight of state payment rates.
Finding #8-4: Research studies have established a connection between payment levels and provider participation and children’s access to care.
Finding #8-5: Existing productivity-based fee schedules (i.e., RVUs) generally reward procedure-based subspecialties and undervalue the increased time needs per clinical interaction, increased pre- and post-service time, and higher practice expenses for most subspecialty care, especially pediatric subspecialty care.
Finding #8-6: There is some evidence that pediatric subspecialties generate less revenue compared with adult subspecialties, in part due to
___________________
15 The webinar recording can be accessed at https://www.nationalacademies.org/event/07-19-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-webinar-1.
insurance mix. As a result, salaries for pediatric subspecialists are often lower than for their adult medicine counterparts.
Finding #8-7: The exact methods through which pediatric subspecialists’ salaries are set are subject to complex, proprietary formulas that vary by institution.
Conclusions
Conclusion #8-1: Medicaid can be a mechanism to target investments in specific types of health care services for specific populations. Low Medicaid payments represent an underinvestment by federal and state governments in children’s health. States can raise Medicaid payment rates using matched state-federal funds, but limits on state finances or other pressures may prevent states from doing so.
Conclusion #8-2: The large percentage of children on Medicaid, especially those cared for by subspecialists, coupled with the low payment rates and RVUs, adversely affects reimbursement for pediatric care. This, in turn, results in lower salaries for most pediatric subspecialties compared with adult subspecialties and compared with private practice primary care (or general) pediatricians. The relatively lower salaries for pediatric subspecialties, particularly medical subspecialties, can influence the career decisions of trainees pursuing pediatrics and pediatric subspecialty training.
Conclusion #8-3: Payment rates are one of many inputs that influence access to pediatric subspecialists.
RECOMMENDATIONS
Expansions in insurance coverage over the past decades, including via CHIP, expanded Medicaid eligibility for children, and the Affordable Care Act, have successfully removed financial barriers to health care for most children. While Medicaid and CHIP provide affordable coverage for families, the low rates of reimbursement coupled with low RVUs contribute to comparatively lower salaries for pediatric subspecialists, especially medical subspecialists. As a result, as discussed in Chapter 4, lower salaries may create disincentives for individuals to pursue careers in pediatrics.
Therefore, to achieve a goal of reducing financial and payment disincentives, the committee provides the following recommendations:
RECOMMENDATION 8-1 To invest in children’s health and address the factors that contribute to limited access to pediatric subspecialty care, Congress should allocate additional federal funding to increase payment for pediatric services.
- Within 5 years, Congress should provide federal funds to states to increase Medicaid payment rates for pediatric services to achieve or exceed parity with Medicare payment rates.
These federal funds should be provided to all states, and the federally funded payment increases should be mandatory and apply to payments in managed care. The committee recognizes that this recommendation may be difficult to implement immediately but believes that it should be phased in as soon as possible—no later than within five years. The committee also recognizes that states can, and some have, increased payments for pediatric services themselves and encourages states to use their flexibility under Medicaid to address the payment challenges facing pediatric subspecialists. Medicaid is a policy lever that states can use in both fee-for-service and managed care settings. However, many states have not done so on their own, which is why the committee believes these mandatory, federal funds are needed.
RECOMMENDATION 8-2 The Centers for Medicare & Medicaid Services should prioritize attention to pediatric services in assigning relative value units that accurately reflect the time and resource use for pediatric subspecialty care.
REFERENCES
AAP (American Academy of Pediatrics). 2008. Application of the resource-based relative value scale system to pediatrics. Pediatrics 122(6):1395-1400.
ABP (American Board of Pediatrics). 2023. Results: Continuing certification (MOC) enrollment surveys for 2018 to 2022. https://www.abp.org/dashboards/results-continuing-certification-moc-enrollment-surveys-2018-2022 (accessed July 17, 2023).
Agarwal, R., O. Mazurenko, and N. Menachemi. 2017. High-deductible health plans reduce health care cost and utilization, including use of needed preventive services. Health Affairs 36(10):1762-1768.
Alexander, D., and M. Schnell. 2019 (unpublished). The impacts of physician payments on patient access, use, and health (wp-19-23).
AMA (American Medical Association). 2023. RVS Update Committee (RUC). https://www.ama-assn.org/about/rvs-update-committee-ruc/rvs-update-committee-ruc (accessed July 3, 2023).
Apaydin, E. 2020. Administrative work and job role beliefs in primary care physicians: An analysis of semi-structured interviews. SAGE Open 10(1): https://doi.org/10.1177/2158244019899092.
Artiga, S., L. Hill, and A. Damico. 2022. Health coverage by race and ethnicity, 2010–2021. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity/ (accessed April 21, 2023).
Ashman, J. J., L. Santo, and T. Okeyode. 2023. Characteristics of office-based physician visits, 2019. Hyattsville, MD: National Center for Health Statistics.
Berman, S. 2018. State Medicaid payment levels and the federal “equal access” statute. Pediatrics 141(1)e20173241. https://doi.org/10.1542/peds.2017-3241.
Berry, J. G., M. Hall, J. Neff, D. Goodman, E. Cohen, R. Agrawal, D. Kuo, and C. Feudtner. 2014. Children with medical complexity and Medicaid: Spending and cost savings. Health Affairs 33(12):2199-2206.
Brot-Goldberg, Z. C., A. Chandra, B. R. Handel, and J. T. Kolstad. 2017. What does a deductible do? The impact of cost-sharing on health care prices, quantities, and spending dynamics.* The Quarterly Journal of Economics 132(3):1261-1318.
Buchmueller, T. C., S. Orzol, and L. D. Shore-Sheppard. 2015. The effect of Medicaid payment rates on access to dental care among children. American Journal of Health Economics 1(2):194-223.
Candon, M., S. Zuckerman, D. Wissoker, B. Saloner, G. M. Kenney, K. Rhodes, and D. Polsky. 2018. Declining Medicaid fees and primary care appointment availability for new Medicaid patients. JAMA Internal Medicine 178(1):145-146.
Casalino, L. P., S. Nicholson, D. N. Gans, T. Hammons, D. Morra, T. Karrison, and W. Levinson. 2009. What does it cost physician practices to interact with health insurance plans? Health Affairs 28(Suppl 1):w533-w543.
CBO (Congressional Budget Office). 2022. The prices that commercial health insurers and Medicare pay for hospitals’ and physicians’ services. https://www.cbo.gov/system/files/2022-01/57422-medical-prices.pdf (accessed January 4, 2023).
Chalmers, N. I., and R. D. Compton. 2017. Children’s access to dental care affected by reimbursement rates, dentist density, and dentist participation in Medicaid. American Journal of Public Health 107(10):1612-1614.
CMS (Centers for Medicare & Medicaid Services). 2015. Final rule: Medicaid program; methods for assuring access to covered Medicaid services. https://www.federalregister.gov/documents/2015/11/02/2015-27697/medicaid-program-methods-for-assuring-accessto-covered-medicaid-services (accessed June 30, 2023).
CMS. 2019. Proposed rule: Medicaid Program; Methods for Assuring Access to Covered Medicaid Services-Rescission. https://www.federalregister.gov/documents/2019/07/15/2019-14943/medicaid-program-methods-for-assuring-access-to-covered-medicaid-services-rescission (accessed June 30, 2023).
CMS. 2020. Final rule and interim final rule: Medicare program; CY2021 payment policies under the physician fee schedule and other changes to Part B payment policies. https://www.govinfo.gov/content/pkg/FR-2020-12-28/pdf/2020-26815.pdf (accessed January 4, 2023).
CMS. 2023a. Program history. https://www.medicaid.gov/about-us/program-history/index.html (accessed April 26, 2023).
CMS. 2023b. Beneficiary enrollment. https://data.cms.gov/summary-statistics-on-beneficiaryenrollment/medicare-and-medicaid-reports/cms-program-statistics-medicare-total-enrollment (accessed July 17, 2023).
CMS. 2023c. Affordable Care Act Program Integrity Provisions. https://www.medicaid.gov/medicaid/program-integrity/affordable-care-act-program-integrity-provisions/index.html (July 10, 2023).
CMS. 2023d. Proposed rule: Medicaid Program; Ensuring Access to Medicaid Services. https://www.govinfo.gov/content/pkg/FR-2023-05-03/pdf/2023-08959.pdf (accessed June 30, 2023).
CMS. 2023e. Summary of Medicaid and CHIP Payment-Related Provisions: Ensuring Access to Medicaid Services (CMS 2442-P) and Medicaid and Children’s Health Insurance Program (CHIP) Managed Care Access, Finance, and Quality (CMS-2439-P). https://www.cms.gov/newsroom/fact-sheets/summary-medicaid-and-chip-payment-related-provisions-ensuring-access-medicaid-services-cms-2442-p#_ftnref1 (accessed June 30, 2023).
Conduff, J. H., and D. H. Coelho. 2017. Professional reimbursement by Medicaid for cochlear implants and related services. Otology & Neurotology 38(7):985-989.
Coughlin, T. A., H. Samuel-Jakubos, and R. Garfield. 2021. Sources of payment for uncompensated care for the uninsured. https://www.kff.org/report-section/sources-of-payment-for-uncompensated-care-for-the-uninsured-issue-brief (accessed January 4, 2023).
Cunningham, P. J., and A. S. O’Malley. 2009. Do reimbursement delays discourage Medicaid participation by physicians? Health Affairs 28(1):w17-w28.
Decker, S. L. 2018. No association found between the Medicaid primary care fee bump and physician-reported participation in Medicaid. Health Affairs 37(7):1092-1098.
Doximity and Curative. 2023. 2023 physician compensation report. https://press.doximity.com/reports/doximity-physician-compensation-report-2023.pdf (accessed May 5, 2023).
Dunn, A., J. D. Gottlieb, A. Shapiro, D. J. Sonnenstuhl, and P. Tebaldi. 2023. A denial a day keeps the doctor away. https://www.nber.org/papers/w29010 (accessed June 5, 2023).
East, C. N., S. Miller, M. Page, and L. R. Wherry. 2023. Multigenerational impacts of childhood access to the safety net: Early life exposure to Medicaid and the next generation’s health. American Economic Review 113(1):98-135.
Erickson, S. M., B. Rockwern, M. Koltov, and R. M. McLean. 2017. Putting patients first by reducing administrative tasks in health care: A position paper of the American College of Physicians. Annals of Internal Medicine 166(9):659-661.
Frintner, M. P., D. Kaelber, E. Kirkendall, C. Lehmann, and E. Lourie. 2020. U.S. pediatricians’ perspectives on reducing administrative tasks. https://www.aap.org/en/research/pediatrician-life-and-career-experience-study-places/results-and-publications/us-pediatricians-perspectives-on-reducing-administrative-tasks (accessed May 5, 2023).
GAO (U.S. Government Accountability Office). 2014a. Medicaid: Use of claims data for analysis of provider payment rates. Washington, DC: GAO.
GAO. 2014b. Medicaid payment comparisons of selected services under fee-for-service, managed care, and private insurance. Washington, DC: GAO.
GAO. 2015. Medicare physician payment rates: Better data and greater transparency could improve accuracy. Washington, DC: GAO.
Garfield, R., E. Hinton, C. Cornachione, and C. Hall. 2018. The Kaiser Family Foundation 2017 Survey of Medicaid Managed Care Plans. https://files.kff.org/attachment/Topline-and-Methodology-Kaiser-Family-Foundation-2017-Survey-of-Medicaid-Managed-Care-Plans (accessed January 4, 2023).
Gifford, K., A. Lashbrook, S. Barth, M. Nardone, E. Hinton, M. Guth, L. Stolyar, and R. Rudowitz. 2021. States respond to COVID-19 challenges but also take advantage of new opportunities to address long-standing issues: Results from a 50-state Medicaid budget survey for state fiscal years 2021 and 2022. https://www.kff.org/report-section/states-respond-to-covid-19-challenges-but-also-take-advantage-of-new-opportunities-to-address-long-standing-issues-provider-rates-and-taxes/ (accessed January 4, 2023).
Gould, Z., and K. Honsberger. 2022. Expanded federal investment in home and community-based services: State approaches to serve children and youth. https://nashp.org/expanded-federal-investment-in-home-and-community-based-services-state-approaches-to-serve-children-and-youth/ (accessed May 5, 2023).
HHS (U.S. Department of Health and Human Services). 2022. Federal financial participation in state assistance expenditures; federal matching shares for Medicaid, the Children’s Health Insurance Program, and aid to needy aged, blind, or disabled persons for October 1, 2023 through September 30, 2024. https://www.federalregister.gov/documents/2022/12/05/2022-26390/federal-financial-participation-in-state-assistance-expenditures-federal-matching-shares-for (accessed May 5, 2023).
Himmelstein, D. U., M. Jun, R. Busse, K. Chevreul, A. Geissler, P. Jeurissen, S. Thomson, M. Vinet, and S. Woolhandler. 2014. A comparison of hospital administrative costs in eight nations: U.S, costs exceed all others by far. Health Affairs 33(9):1586-1594.
Hinton, E., Guth, M., Raphael, J., Haldar, S., and R. Rudowitz. 2022. How the Pandemic Continues to Shape Medicaid Priorities: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2022 and 2023. https://files.kff.org/attachment/REPORT-How-the-Pandemic-Continues-to-Shape-Medicaid-Priorities-Results-from-an-Annual-Medicaid-Budget-Survey-for-State-Fiscal-Years-2022-and-2023.pdf (accessed July 10, 2023).
Hinton, E., and J. Raphael. 2023. 10 things to know about Medicaid managed care. https://www.kff.org/medicaid/issue-brief/10-things-to-know-about-medicaid-managed-care/ (accessed May 5, 2023).
Holgash, K., and M. Heberlein. 2019. Physician acceptance of new Medicaid patients. https://www.macpac.gov/wp-content/uploads/2019/01/Physician-Acceptance-of-New-Medicaid-Patients.pdf (accessed January 4, 2023).
Itri, J. N., A. Mithqal, and A. Krishnaraj. 2017. Funds flow in the era of value-based health care. Journal of the American College of Radiology 14(6):818-824.
Jones, J. R., M. D. Kogan, R. M. Ghandour, and C. S. Minkovitz. 2021. Out-of-pocket health care expenditures among United States children: Parental perceptions and past-year expenditures, 2016 to 2017. Academic Pediatrics 21(3):480-487.
Josephson, S. A., R. L. Sacco, J. M. Czech, R. N. Maher, C. S. Knutson, and L. B. Goldstein. 2020. Funds flow in academic neurology: A potential path to financial success. Neurology 94(18):785-791.
KFF. 2022a. Health insurance coverage of children 0-18 (CPS). https://www.kff.org/other/state-indicator/health-insurance-coverage-of-children-0-18-cps/?activeTab=graph¤tTimeframe=0&startTimeframe=2&selectedDistributions=medicaid&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed January 4, 2023).
KFF. 2022b. 2022 employer health benefits survey. https://www.kff.org/report-section/ehbs-2022-section-5-market-shares-of-health-plans/ (accessed January 4, 2023).
Klukoff, H., M. Lehan, and A. Schneider. 2023. Medicaid managed care financial results for 2022: Another big year for the big five. https://ccf.georgetown.edu/2023/02/22/medicaid-managed-care-financial-results-for-2022-another-big-year-for-the-big-five (accessed June 30, 2023).
Kuo, D. Z., M. Hall, R. Agrawal, E. Cohen, C. Feudtner, D. M. Goodman, J. M. Neff, and J. G. Berry. 2015. Comparison of health care spending and utilization among children with Medicaid insurance. Pediatrics 136(6):1521-1529.
Lakshminrusimha, S., S. Murin, J. D. Kirk, Z. Mustafa, T. R. Maurice, N. Sousa, J. Lee, and D. A. Lubarsky. 2022. “Funds flow” implementation at academic health centers: Unique challenges to pediatric departments. The Journal of Pediatrics 249:6-10.e14. https://doi.org/10.1016/j.jpeds.2022.01.058. Epub 2022 Feb 3. PMID: 35124013.
Lakshminrusimha, S., S. Murin, and D. A. Lubarsky. 2023. Low compensation for academic pediatric medical specialists: Role of Medicaid, productivity, work hours, and sex. The Journal of Pediatrics 255:1-6.
Lalezari, R. M., A. Pozen, and C. J. Dy. 2018. State variation in Medicaid reimbursements for orthopaedic surgery. Journal of Bone and Joint Surgery 100(3):236-242.
Larson, K., E. A. Gottschlich, W. L. Cull, and L. M. Olson. 2021. High-deductible health plans for U.S. children: Trends, health service use, and financial barriers to care. Academic Pediatrics 21(8):1345-1354.
Leininger, L. J., B. Saloner, and L. R. Wherry. 2015. Predicting high-cost pediatric patients: Derivation and validation of a population-based model. Medical Care 53(8):729-735.
Liptak, G. S., L. P. Shone, P. Auinger, A. W. Dick, S. A. Ryan, and P. G. Szilagyi. 2006. Short-term persistence of high health care costs in a nationally representative sample of children. Pediatrics 118(4):e1001-e1009.
Mabry, C. D., L. A. Gurien, S. D. Smith, and S. C. Mehl. 2016. Are surgeons being paid fairly by Medicaid? A national comparison of typical payments for general surgeons. Journal of the American College of Surgeons 222(4):387-394.
MACPAC (Medicaid and CHIP Payment and Access Commission). 2015. Provider Networks and Access: Issues for Children’s Coverage. https://www.macpac.gov/wp-content/uploads/2015/03/Provider-Networks-and-Access-Issues-for-Children%E2%80%99s-Coverage.pdf (accessed July 10, 2023).
MACPAC. 2017a. Medicaid payment policy for Federally Qualified Health Centers. https://www.macpac.gov/wp-content/uploads/2017/12/Medicaid-Payment-Policy-for-Federally-Qualified-Health-Centers.pdf (accessed July 10, 2023).
MACPAC. 2017b. State Medicaid fee-for-service physician payment policies. https://www.macpac.gov/publication/states-medicaid-fee-for-service-physician-payment-policies (accessed January 4, 2023).
MACPAC. 2022a. Provider payment under fee for service. https://www.macpac.gov/subtopic/provider-payment (accessed January 4, 2023).
MACPAC. 2022b. Annual analysis of disproportionate share hospital allotments to states. https://www.macpac.gov/publication/annual-analysis-of-disproportionate-share-hospital-allotments-to-states-3 (accessed April 7, 2023).
MACPAC. 2022c. Directed payments in Medicaid managed care. https://www.macpac.gov/wp-content/uploads/2022/06/June-2022-Directed-Payments-Issue-Brief-FINAL.pdf (accessed June 30, 2023).
MACPAC. 2023a. Matching rates. https://www.macpac.gov/subtopic/matching-rates/ (accessed April 6, 2023).
MACPAC. 2023b. Federal match rate exceptions. https://www.macpac.gov/federal-match-rate-exceptions (accessed April 6, 2023).
MACPAC. 2023c. Federal legislative milestones in Medicaid and CHIP. https://www.macpac.gov/reference-materials/federal-legislative-milestones-in-medicaid-and-chip/ (accessed May 10, 2023).
MACPAC. 2023d. Disproportionate share hospital payments. https://www.macpac.gov/subtopic/disproportionate-share-hospital-payments (accessed April 7, 2023).
Manatt Health. 2023. Proposed rules on Medicaid payments, access and quality: Implications for health care stakeholders. https://www.manatt.com/insights/webinars/proposed-rules-on-medicaid-payments-access-and-qu (accessed June 30, 2023).
Martin, K. 2021. Medscape pediatrician compensation report 2021. https://www.medscape.com/slideshow/2021-compensation-pediatrician-6013859 (accessed May 5, 2023).
Massoumi, R. L., C. P. Childers, and S. L. Lee. 2021. Underrepresentation of pediatric operations in the relative value unit updating process. Journal of Pediatric Surgery 56(6):1101-1106.
MedPAC (Medicare Payment Advisory Committee). 2018. June 2018 Report to the Congress: Medicare and the health care delivery system. Washington, DC: MedPAC.
Miller, E. A. 2007. Federal administrative and judicial oversight of Medicaid: Policy legacies and tandem institutions under the Boren amendment. Publius: The Journal of Federalism 38(2):315-342.
Miller, S., and L. R. Wherry. 2018. The long-term effects of early life Medicaid coverage. Journal of Human Resources: https://doi.org/10.3368/jhr.54.3.0816.8173R1.
Miller, J. C., G. E. Andersson, M. Cohen, S. M. Cohen, S. Gibson, M. A. Hindery, M. Hooven, J. Krakower, and D. H. Browdy. 2012. Perspective: Follow the money: The implications of medical schools’ funds flow models. Academic Medicine 87(12):1746-1751.
Ming, D. Y., K. A. Jones, M. J. White, J. E. Pritchard, B. G. Hammill, C. Bush, G. L. Jackson, and S. R. Raman. 2022. Healthcare utilization for Medicaid-insured children with medical complexity: Differences by sociodemographic characteristics. Maternal and Child Health Journal 26(12):2407-2418.
Moore, K. J., T. A. Felger, W. L. Larimore, and T. L. Mills. 2008. What every physician should know about the RUC. Family Practice Management 15(2):36.
Muhuri, P., and S. Machlin. 2017. Differences in payments for child visits to office-based physicians: Private versus Medicaid insurance, 2010 to 2015. In Statistical brief (Medical Expenditure Panel Survey (U.S.)). Rockville, MD: Agency for Healthcare Research and Quality.
Mulcahy, A. W., T. Gracner, and K. Finegold. 2018. Associations between the Patient Protection and Affordable Care Act Medicaid primary care payment increase and physician participation in Medicaid. JAMA Internal Medicine 178(8):1042-1048.
Mulcahy, A. W., K. Merrell, and A. Mehrotra. 2020. Payment for services rendered—updating Medicare’s valuation of procedures. New England Journal of Medicine 382(4):303-306.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2021. Implementing high-quality primary care: Rebuilding the foundation of health care. Edited by L. McCauley, R. L. Phillips, Jr., M. Meisnere, and S. K. Robinson. Washington, DC: The National Academies Press.
OECD (Organisation for Economic Co-operation and Development). 2016. Better ways to pay for health care. https://www.oecd.org/publications/better-ways-to-pay-for-health-care-9789264258211-en.htm (accessed May 5, 2023).
Ortaliza, J., M. McGough, E. Wager, G. Claxton, and K. Amin. 2021. How do health expenditures vary across the population? https://www.healthsystemtracker.org/chart-collection/health-expenditures-vary-across-population/#Proportion%20of%20individuals%20by%20health%20status,%202019 (accessed May 5, 2023).
Perkins, J. 2015. Armstrong v. Exceptional Child Care Center: Health care providers’ access to court is blocked. https://healthlaw.org/wp-content/uploads/2015/04/2015_04_27_Arm-strong_Summary_Rev.pdf (accessed May 5, 2023).
Perrin, J. M., G. M. Kenney, and S. Rosenbaum. 2020. Medicaid and child health equity. New England Journal of Medicine 383(27):2595-2598.
Pollitz, K. 2022. Network adequacy standards and enforcement. https://www.kff.org/health-reform/issue-brief/network-adequacy-standards-and-enforcement (accessed July 10, 2023).
Polsky, D., M. Richards, S. Basseyn, D. Wissoker, G. M. Kenney, S. Zuckerman, and K. V. Rhodes. 2015. Appointment availability after increases in Medicaid payments for primary care. New England Journal of Medicine 372(6):537-545.
Price, J., M. L. Brandt, M. L. Hudak, S. K. Berman, K. M. Carlson, A. P. Giardino, L. Hammer, K. Heggen, S. A. Pearlman, and B. G. Sood. 2020. Principles of financing the medical home for children. Pediatrics 145(1): e20193451.
Rueben, K.S., and M. Randall. 2017. Balanced budget requirements. https://www.urban.org/research/publication/balanced-budget-requirements (accessed July 17, 2023).
Rosenbaum, S. 2015. Medicaid and access to care: The CMS equal access rule. Health Affairs Blog.
Rosenbaum, S., Jost, T., Musimeci, M., and Somodevilla, A. 2023. A victory for Medicaid beneficiaries in Supreme Court’s Talevski decision. Health Affairs Forefront.
Rudowitz, R. 2020. What you need to know about the Medicaid fiscal accountability rule (MFAR). https://www.kff.org/medicaid/issue-brief/what-you-need-to-know-about-the-medicaid-fiscal-accountability-rule-mfar/#:~:text=States%20are%20limited%20in%20making,would%20pay%20and%20Medicaid%20payments. (accessed July 17, 2023).
Rudowitz, R., B. Corallo, and R. Garfield. 2020. How much fiscal relief can states expect from the temporary increase in the Medicaid FMAP? https://www.kff.org/coronavirus-covid-19/issue-brief/how-much-fiscal-relief-can-states-expect-from-the-temporary-increase-in-the-medicaid-fmap/ (accessed July 17, 2023).
Rudowitz, R., and L. Sobel. 2022. What is at stake for Medicaid in Supreme Court case Health & Hospital Corp v. Talevski? https://www.kff.org/policy-watch/what-is-at-stake-for-medicaid-in-supreme-court-case-health-hospital-corp-v-talevski/ (accessed April 7, 2023).
Santiago, C. C., D. C. Santiago, and R. Sebro. 2020. State variation in Medicaid and Medicare reimbursements in musculoskeletal radiology. Clinical Imaging 66:67-72.
Schnapp, L. M., M. J. Steiner, and S. D. Davis. 2020. Basic primer for finances in academic adult and pediatric pulmonary divisions. Chest 157(2):363-368.
Schneider, A. 2023. A closer look at the network adequacy provisions of CMS’s proposed Medicaid managed care rule. In Say Ahhh!: Georgetown University Health Policy Institute Center for Children and Families.
Schneider, A., and A. Corcoran. 2022. Standards for provider network adequacy in Medicaid and the marketplaces. In Say Ahhh!: Georgetown University Health Policy Institute Center for Children and Families.
Sharma, R., S. Tinkler, A. Mitra, S. Pal, R. Susu-Mago, and M. Stano. 2018. State Medicaid fees and access to primary care physicians. Health Economics 27(3):629-636.
Singer, N. G., and K. B. Onel. 2019. Challenges to practicing pediatric rheumatology. Rheumatic Disease Clinics 45(1):67-78.
Smith, V. K., K. Gifford, E. Ellis, R. Rudowitz, and L. Snyder. 2010. Hoping for economic recovery, preparing for health reform: A look at Medicaid spending, coverage and policy trends results from a 50-state Medicaid budget survey for state fiscal years 2010 and 2011. https://www.kff.org/wp-content/uploads/2013/01/8105.pdf (accessed July 10, 2023).
Staman, J. 2011. Medicaid reimbursement rate litigation: An overview of Douglas v. Independent Living Center of Southern California. https://www.everycrsreport.com/files/20110718_R41923_7b27132c1be30c4e727dc85ddc64e252795fd91d.pdf (accessed May 5, 2023).
Tang, S.-F. S., M. L. Hudak, D. M. Cooley, B. N. Shenkin, and A. D. Racine. 2018. Increased Medicaid payment and participation by office-based primary care pediatricians. Pediatrics 141(1): e20172570.
Tseng, P., R. S. Kaplan, B. D. Richman, M. A. Shah, and K. A. Schulman. 2018. Administrative costs associated with physician billing and insurance-related activities at an academic health care system. Journal of the American Medical Association 319(7):691-697.
VonAchen, P., D. Gaur, W. Wickremasinghe, M. Hall, D. M. Goodman, R. Agrawal, and J. G. Berry. 2021. Assessment of underpayment for inpatient care at children’s hospitals. JAMA Pediatrics 175(9):972-974.
Weidemann, D. K., I. Ashoor, D. Soranno, R. Sheth, C. Carter, and P. Brophy. 2022. Moving the needle toward fair compensation in pediatric nephrology. Frontiers in Pediatrics 10:849826. https://doi.org/10.3389/fped.2022.849826.
Weiss, A. J., L. Liang, and K. Martin. 2022. Overview of hospital stays among children and adolescents, 2019. https://hcup-us.ahrq.gov/reports/statbriefs/sb299-Hospital-Stays-Children-2019.jsp (accessed May 5, 2023).
West, C. P., L. N. Dyrbye, and T. D. Shanafelt. 2018. Physician burnout: Contributors, consequences and solutions. Journal of Internal Medicine 283(6):516-529.
Weyand, A. C., and G. L. Freed. 2020. Pediatric subspecialty workforce: Undersupply or over-demand? Pediatric Research 88(3):369-371.
Wherry, L. R., S. Miller, R. Kaestner, and B. D. Meyer. 2018. Childhood Medicaid coverage and later-life health care utilization. The Review of Economics and Statistics 100(2):287-302.
Williams, E., and M. Musumeci. 2021. Children with special health care needs: Coverage, affordability, and HCBS access. https://www.kff.org/medicaid/issue-brief/children-with-special-health-care-needs-coverage-affordability-and-hcbs-access (accessed January 4, 2023).
Wong, C. A., K. Kan, Z. Cidav, R. Nathenson, and D. Polsky. 2017. Pediatric and adult physician networks in Affordable Care Act marketplace plans. Pediatrics 139(4).
Wynn, B. O., L. F. Burgette, A. W. Mulcahy, E. N. Okeke, I. Brantley, N. Iyer, T. Ruder, and A. Mehrotra. 2015. Development of a model for the validation of work relative value units for the Medicare physician fee schedule. RAND Health Quarterly 5(1):5.
Zuckerman, S., K. Merrell, R. A. Berenson, S. Mitchell, D. Upadhyay, and R. Lewis. 2016. Collecting empirical physician time data: Piloting an approach for validating work relative value units. https://www.urban.org/sites/default/files/publication/87771/2001123-collecting-empirical-physician-time-data-piloting-approach-for-validating-work-relative-value-units_0.pdf (accessed January 4, 2023).
Zuckerman, S., L. Skopec, and J. Aarons. 2021. Medicaid physician fees remained substantially below fees paid by Medicare in 2019. Health Affairs 40(2):343-348.
This page intentionally left blank.


































