2
Children’s Health Care Needs and Access to Subspecialty Care
Pediatric subspecialty physicians fill a major role for children with health conditions that occur too infrequently for primary care clinicians to gain and maintain sufficient, up-to-date clinical knowledge; for common conditions with high disease severity; or for conditions that require technical procedures and use specialized equipment and procedures. Children’s rapid development renders them particularly vulnerable as delays in addressing health needs or deferring care altogether may lead to harmful effects both during childhood and much later as adults, particularly if they occur during critical periods of development. For example, high blood pressure in childhood and adolescence has been associated with morbidity at older ages (due to heart and kidney disease) and premature death (Leiba et al., 2019; Franks et al., 2010; Yang et al., 2020). Given the low prevalence of individual conditions, pediatric subspecialists see enough cases concentrated from a very large population to give them the experience needed to diagnose and treat these conditions effectively. However, while children have relatively high rates of access for common preventive care such as well-child visits (CDC, 2020), their access to care for rarer conditions may be more complicated. A well-functioning health system needs to be organized to ensure good access to care for both common and uncommon acute and chronic health problems. While this chapter discusses some issues of access to health care in general, a framework is presented for understanding access to pediatric subspecialty physician care specifically in the context of the changing health care needs of infants, children, and adolescents.
FRAMEWORK
Ensuring access to high-quality pediatric subspecialty care benefits the health and well-being of millions of children both for children themselves and the adults they will become. As seen in Figure 2-1, the committee developed a framework to help understand the connection between pediatric subspecialty care and children’s health, including demand and need for
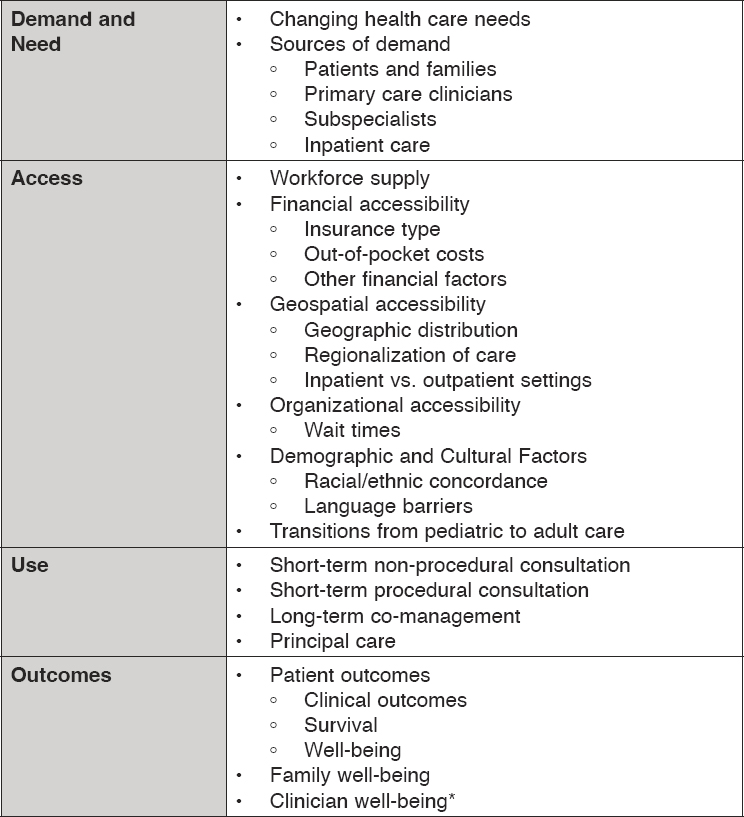
NOTES: *Clinician outcomes of job satisfaction and well-being are discussed in Chapter 5. While consultation typically refers to a short-term situation and referral may imply a long-term scenario for co-management or shifting of care management, the committee generally uses the term referral to apply to both situations.
SOURCE: Committee generated.
services; access to care; use of subspecialty services; and patient, family, and provider outcomes.
DEMAND AND NEED
Understanding the need for health care is an important step toward quantifying demand for health care and its future trends. The process of obtaining subspecialty care begins with a perceived need—that is, demand for these services. An individual who thinks they need a service has a demand for it. However, demand is not the same as need. Demand relates to the desire to receive health care while need refers to the capacity to benefit from health care, meaning that the care is effective in “improving, maintaining, or slowing the deterioration of health” (Rodriguez Santana et al., 2023). Need may be recognized by an individual, their health care team, or both. One of the core functions of primary care is recognition of new health problems and selection of the most appropriate treatment setting for the care of that problem or the ruling out of health problems that may require subspecialty care.
For example, consider this hypothetical example drawn from the collective experience of the authoring committee: a primary care physician evaluates a patient with a history of chronic diarrhea, weight loss, and intermittent abdominal pain. The physician is concerned about possible celiac disease, and initial testing supports this presumptive diagnosis; the patient has a need for subspecialty care to definitively make this diagnosis and provide consultation on nutritional management and best available treatments. The patient will benefit from long-term co-management between the primary care clinician and pediatric gastroenterologist, who provides episodic consultation over time related to progression and optimal treatments. In an alternative hypothetical example of a healthy child who is growing and developing well but has infrequent hard stools, a primary care physician makes a diagnosis of constipation and counsels the family that the constipation will likely resolve with hydration, dietary changes, and over-the-counter medication. However, the family remains concerned and self-refers to a pediatric gastroenterologist. This patient has demand, but likely no need for subspecialty care. Thus, demand is a belief that care is required, while need refers to a capacity to benefit from a particular type of health care service.
Patients can have needs, but no demand (i.e., unmet need). The patient with likely celiac disease described above had a need for subspecialty care, but may have deferred treatment if they experienced disincentives to seeking such care, such as high deductibles or long wait times. Patients can also have demand, but no need, which leads to overuse of services. In both cases, patients may experience harm. A high-functioning health system will align demand with need as much as possible.
The Changing Health Care Needs of Infants, Children, and Adolescents
Over the past two decades, there have been significant changes in the physical, mental, and behavioral health needs of the pediatric population. For example, among American infants, children, and adolescents:
- In 2017–2020, obesity affected 19.7 percent of children aged 2–19 (Stierman et al., 2021), up from 13.9 percent of children in 1999–2000 (Sanyaolu et al., 2019). Early studies show significant increases in weight and body mass index among children during the COVID-19 pandemic (Lange et al., 2021; Woolford et al., 2021).
- In 2015–2017, 17.8 percent of children aged 3–17 had a developmental disability (up from 16.2 percent in 2009 to 2011) (Zablotsky et al., 2019).
- In 2001–2017, the prevalence of type 2 diabetes among children aged 10–19 years doubled (from 0.34 to 0.67 per 1,000) (Lawrence et al., 2021).
- Between 2016 and 2020, there were significant increases in anxiety (27 percent increase) and depression (24 percent increase) in children (Lebrun-Harris et al., 2022).
- From 2009 to 2019, the percentage of pediatric mental health hospitalizations with attempted suicide, suicidal ideation, or self-injury diagnoses increased from 30.7 percent to 64.2 percent (Arakelyan et al., 2023).
Overall, serious congenital conditions that were previously lethal or disabling are now treatable and even curable, thanks to scientific innovations. For example, immunizations have eradicated or significantly reduced a number of deadly infections, such as diphtheria, smallpox, measles, bacterial meningitis, pertussis, and many other diseases (CDC, 2022). On the other hand, today’s children experience a wide variety of chronic, often lifelong, illnesses (Anderson and Horvath, 2002; Gerteis et al., 2014; Van Cleave et al., 2010; Wise, 2007). Although the most common health conditions that affect children today are acute and recurrent illnesses (e.g., otitis media, respiratory viral illnesses, gastroenteritis), a growing proportion of children are affected by long-term (i.e., expected to last more than one year) medical and behavioral health conditions. Additionally, there are a sizable number of children afflicted with less common diseases, such as nephrotic syndrome, congenital heart disease, sickle cell disease, cystic fibrosis, muscular dystrophy, and complications associated with premature birth. Rare diseases comprise a clinically heterogeneous group of disorders, each one occurring in fewer than 200,000 persons in the United States. They are
commonly diagnosed during childhood (70 percent have an exclusive pediatric onset), are frequently genetic in origin, and can have deleterious effects on both immediate and long-term health (Nguengang Wakap et al., 2020). Children also have a variety of mental, behavioral, and social care needs.
A variety of terms have been used to describe the complex care needs of some children, including chronic illness, special health care needs, and medical complexity. Although all have somewhat different definitions, of these types of health care, needs are rising and create challenges for care coordination, referral, and the time needed for subspecialists to assess and treat these patients.
Chronic Conditions
More than one-third (38 percent) of children in middle childhood and adolescence have at least one chronic health condition (CAHMI, 2023a). Many of these individuals are affected by mental health and neurodevelopmental conditions such as anxiety, depression, attention deficit hyperactivity disorder (ADHD), and developmental delay. Others are affected by common chronic medical conditions such as asthma, headaches, and allergies.
Chronic pediatric conditions traditionally have been conceptualized as stratified by physical or mental health conditions, but over the past decades there has been greater awareness of the comorbidity of physical and mental health conditions (Berg et al., 2017; Bright et al., 2016; Butwicka et al., 2016; Muskens et al., 2017; Rankin et al., 2016; Rubinstein et al., 2018). In children with physical and mental health comorbidities, mental health issues may make care and control of the medical condition like diabetes difficult unless both are treated together. An important note, however, is that while children with chronic conditions have worse general health (including function and symptom burden) than those without chronic conditions, life satisfaction appears the same for both groups (Blackwell et al., 2019; Forrest et al., 2022). Therefore, pediatric subspecialty care can help children with chronic conditions to maintain and optimize their quality of life by maximizing their function and minimizing symptom burden.
Children and Youth with Special Health Care Needs
Children [and youth]1 with special health care needs (CYSHCN) is purposively broadly defined as “those who have or are at risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally” (McPherson et al., 1998). While the “at
___________________
1 Originally defined as children with special health care needs.
risk” component of this definition has not been adequately quantified or measured, it is important to acknowledge that CYSHCN status can change over time and patients may require services to prevent a chronic condition among those at risk. Special health care needs can include “physical, intellectual, and developmental disabilities, as well as long-standing medical conditions such as asthma, diabetes, a blood disorder, or muscular dystrophy” (CDC, 2021). In 2019-2020, about 20 percent of U.S. children had a special health care need, with needs being more prevalent in non-Hispanic Black children and children with multiple adverse childhood experiences (HRSA, 2022). In 2019–2020, 32.2 percent of CYSHCN received care from a specialist2 doctor compared with 7.4 percent of non-CYSHCN (CAHMI, 2023b). CYSHCN were nearly four times more likely to have unmet health care needs in the past year compared with non-CYSHCN and more likely to have unmet needs across every type of need, the largest gap being observed in mental health care. The most commonly reported reasons for unmet need included cost (49 percent) and appointment availability (54 percent). Fewer than two-thirds of CYSHCN and their families had adequate insurance to cover the needed services and less than a quarter received health care transition planning to adult care (HRSA, 2022).
Mental Health
Mental and behavioral health conditions are prevalent among the children cared for by pediatric subspecialists, particularly children with chronic medical conditions (Reardon et al., 2020). The severity of mental health conditions occurs on a continuum, from mild conditions that do not necessarily require any treatment, to more severe conditions that can cause impairment. Many disorders typically start in early childhood, although symptoms may not be recognized until later (Amminger et al., 2011; Kessler et al., 2005; Schimmelmann et al., 2007; Shear et al., 2006).
Globally, mental health disorders among children and adolescents contribute to disability and self harm (Kyu et al., 2016). Approximately one in six U.S. children have a diagnosable mental, behavioral, or developmental disorder (Cree et al., 2018; Whitney and Peterson, 2019). The most common disorders among children and adolescents (aged 3–17) are ADHD, anxiety, disruptive behavior problems, and depression (Bitsko et al., 2022; Ghandour et al., 2019). In 2016, nearly 10 percent of U.S. children had a diagnosis of ADHD (Danielson et al., 2018). In 2020, one in 36 children met the case definition for autism (up from one in 59 in 2014) (Baio et al.,
___________________
2 In the National Survey of Children’s Health, specialist doctors were defined as “doctors like surgeons, heart doctors, allergy doctors, skin doctors, and others who specialize in one area of health care.”
2018; Maenner et al., 2023). One-fifth (20 percent) of adolescents (aged 12–17) experienced a major depressive episode between 2013 and 2019, and more than one-third (37 percent) reported “persistently feeling sad or hopeless in the past year” (Bitsko et al., 2022). Some conditions commonly occur together. For example, about 74 percent of children with depression also have anxiety (CDC, 2023). Suicide rates among children and adolescents aged 10–24 years have increased dramatically since 2007—reaching nearly 0.11 percent in 2018 (Curtin, 2020). Physical and mental health comorbidities are also common in children (Chavira et al., 2008; Merikangas et al., 2015; Romano et al., 2021). Transgender and non-binary youth are at increased risk for depression, suicidality, and self-harm (Connolly et al., 2016; Price-Feeney et al., 2020; Rimes et al., 2019).
The COVID-19 pandemic increased mental health risks in children and adolescents, particularly those from disadvantaged backgrounds (Fegert et al., 2020; NASEM, 2023). Children in the United States were more likely to experience anxiety or depression during the first year of the pandemic (as compared with previous years), with 5.6 million children diagnosed with anxiety and 2.4 million children diagnosed with depression in 2020 (AECD, 2022; Lebrun-Harris et al., 2022). From 2019 to 2020, there was a 21 percent year-over-year increase in diagnoses of behavior or conduct problems (Lebrun-Harris et al., 2022). In addition, the disruption of schooling for most children in 2020–2021 due to the states’ and communities’ response to the pandemic has had and will likely continue to have serious consequences for children for a number of years (NASEM, 2023). For example, the rate of teen suicide and the burden of pediatric mental health problems increased during the COVID-19 pandemic (Charpignon et al., 2022; Yard et al., 2021).
Even before the COVID-19 pandemic, improving access to and quality of child mental health care has been a national priority area (Hoagwood and Olin, 2002; Hogan, 2003; NRC and IOM, 2004; Stroul and Friedman, 1986) supported by evidence that the child mental health care system is often inaccessible, ineffective, and inequitable (Coker et al., 2016; Danielson et al., 2018; Epstein et al., 2014; Kalb et al., 2019; Whitney and Peterson, 2019; Zima et al., 2010). Among children and adolescents aged 3–17 years, about 10 percent had received mental health services, and nearly 8 percent had taken medication for their disorder (Bitsko et al., 2022). However, while evidence based-treatments (e.g., psychotherapy, parent training, applied behavior analysis, psychotropic medications) are effective for common child mental health disorders (AHRQ, 2017, 2022; Cheung et al., 2013; Fristad and MacPherson, 2014; Müller et al., 2014; Slocum et al., 2014), nearly half (49.4 percent) of children with a mental health disorder do not receive needed treatment or counseling (Whitney and Peterson, 2019). Treatment status can also vary by disorder. For example, nearly 80
percent of children with depression report receiving treatment within the past year, but only 59 percent of children with anxiety reported receiving treatment (Ghandour et al., 2019). The adverse consequences of untreated or inadequately treated mental health disorders include increased child risk for suicide (Siffel et al., 2020), school failure (Finning et al., 2019; Kuriyan et al., 2013; Loe and Feldman, 2007), and traumatic injury (Brunkhorst-Kanaan et al., 2021; Chang et al., 2018a). Furthermore, nearly 10 percent of U.S. pediatric hospitalizations are for a primary mental health diagnosis, and rates continue to rise (Bardach et al., 2014). Among hospitalizations, the most frequent and costly diagnoses are depression (44 percent; $1.33 billion), bipolar disorder (18 percent; $702 million), and psychosis (12 percent; $540 million) (Bardach et al., 2014). The 10-year rise in U.S. children’s hospitalizations was five times greater for mental health diagnoses compared with other conditions, costing $1.6 billion (Zima et al., 2016). Following COVID-19 school closure orders, among 44 U.S. children’s hospitals, hospitalizations for suicide attempt or self-injury rose by 42 percent (Zima et al., 2022).
Source of Demand for Subspecialty Care
Subspecialty consultation and referral demand can be driven by patients, families, or primary care clinicians who perceive a need for consult with a subspecialist. Demand for subspecialty services also results from patient visits to emergency departments, between subspecialists themselves (cross-referral), or from subspecialty-generated return appointments.
Patients and Families
Patients and families may induce demand by directly seeking subspecialty care (self-referral) or consult with their primary care clinician about the need for referral to a subspecialist. Primary care clinicians report that patient/parent pressure is a common reason for a referral (Kaul et al., 2015; Kunin et al., 2018; Little et al., 2004), and as a result, they may refer in order to maintain patient satisfaction, which is often incentivized by health systems. For example, “readiness to refer your child to another physician in a timely manner?” is included as a question to rate professional competence on a validated standardized questionnaire for patient satisfaction in the pediatric outpatient setting (Bitzer et al., 2012). In a survey of pediatricians, 4 in 10 reported that they sometimes or often made unnecessary referrals to specialists based on patient request (Kaul et al., 2015). Patient demand for subspecialty care may also increase via self-referral if there is constrained access to primary care or if they feel that referral for care of a particular problem is inevitable. Ray et al. (2016) identified five desired outcomes for
subspecialty referrals: improved current health status, improved long-term health outcomes, increased knowledge and understanding of their disease and/or treatment, informed family expectations for care goals, and reduced anxiety regarding changes in their child’s health status. During one of the committee’s public webinars, LaToshia Rouse, birth and postpartum doula (Birth Sisters Doula Services), patient and family engagement consultant, and parent to children who have needed subspecialty care, stated:
I would love to have a system that would allow me to go when I needed to go, but also have those telehealth system[s] when it was necessary. Some appointments could have been an e-mail. Some appointments could have been a test or a chart message. But some of them, I need you to see this, I need to see you.3
Primary Care Clinicians
Primary care clinicians may believe a subspecialty referral is needed if the health condition is rare and they lack the necessary expertise, they need advice on diagnosis or treatment for a complex problem, the patient needs a technical procedure, the patient needs ancillary services provided by a subspecialty team, or the patient has not responded to conventional therapy in primary care settings. An important determinant of primary care physicians’ subspecialty referral behavior, which drives demand, is the breadth of their service provision. As the number of pediatric subspecialties has grown, many pediatricians may refer for conditions they might have treated themselves in the past. Pediatricians may also refer to subspecialists in response to disincentives to initiate care for certain patients such as lack of time to invest in patients with complex care needs and fear of malpractice for “failure to refer” (Pho, 2012).
Subspecialists
Subspecialists induce demand largely due to follow-up or return visits. One older study found that 75 percent of visits to medical subspecialists for children were for continuing care, with just 25 percent reported to be for new patients, and 73 percent of all visits resulted in a specialist request for a follow-up visit (Valderas et al., 2009). There is limited evidence to guide decision making on the frequency and timing of return subspecialty visits, resulting in wide practice variation. Administrative quotas for visit and
___________________
3 The webinar recording can be accessed at https://www.nationalacademies.org/event/07-19-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-webinar-1.
procedure volume may incentivize specialists to induce demand, although the extent to which this occurs is unknown and merits examination.
Subspecialists can create additional demand by cross-referring to other specialists and converting primary care clinician-requested, short-term consults into longer term co-managed care, which often makes primary care clinicians’ coordination of the referral more challenging. Some specialist-induced demand is necessary, such as during diagnostic evaluations and to ascertain treatment responsiveness. On the other hand, some follow-up visits may be unnecessary, or may be more appropriately performed in primary care settings. (For more on primary care–subspecialty collaboration and referrals, see Chapter 7.)
Hospitalization and Inpatient Consultations
Inpatient pediatric subspecialty consultation is not well described in the literature, but existing studies indicate there is likely wide variation in consultative practice related to patient, provider, and system factors (Darby et al., 2019; Kern-Goldberger et al., 2023; Sump et al., 2020). In children with medical complexity, inpatient consultations may decrease length of stay, cost of care, and subsequent hospitalizations (Mosquera et al., 2021). However, there are likely opportunities to be more judicious with inpatient consultation (Kern-Goldberger et al., 2021). Parallels exist to primary care consultation, including challenges ensuring clear communication between a primary inpatient clinician and the pediatric subspecialty consultant, consultations at the request of families, and because of medicolegal concerns (Kern-Goldberger et al., 2021).
ACCESS TO SUBSPECIALTY CARE
Access can be evaluated from the vantage of patients/families (how easy or difficult it is to obtain care), providers (organization of subspecialty care to make it available for patients), or the health system (how its financing and organization influence the equitable distribution of subspecialty services). Access can also be evaluated across multiple dimensions of experience: geospatial accessibility (e.g., location of providers), financial accessibility (e.g., out-of-pocket costs, insurance design), organizational accessibility (e.g., wait times), and equity (e.g., whether patients’ opportunities to access subspecialty services are based on need, rather than socially determined characteristics). Chapter 7 provides more insights on access to care due to challenges at the primary care–subspecialty interface (i.e., consultation and referral between primary care clinicians and pediatric subspecialists). See Box 2-1 for family and clinician perspectives on access to subspecialty care.
Geospatial Accessibility
Patients and families are responsible for getting to the subspecialist and they may experience difficulty in traveling there because of the geographic distribution of subspecialists.4 At the health-system level, the geospatial
___________________
4 Technological innovations like telehealth may help reduce this access barrier for some patients, but not all. See Chapter 7 for more information on strategies and technologies to ensure equitable patient access to pediatric expertise.
distribution per population is a key factor. Turner et al. (2020) found that the number of pediatric subspecialists in the United States increased by 77 percent between 2003 and 2019, with increases varying across subspecialties. During the same period, the number of children in the United States remained the same, but the changing population density of children varied across the country (see Figure 2-2).
Driving Distance and Regionalization of Care
Driving distance is typically presented as a measure of geographic accessibility. Between 2003 and 2019, the mean driving distance for children decreased among all pediatric subspecialties, but the benefits of increased numbers of subspecialists on travel distance were not uniformly distributed across the United States or by subspecialty (Turner et al., 2020). Depending on the subspecialty, an estimated 1 million to 39 million children (2 to 53 percent) resided 80 miles or more from a subspecialist (Turner et al., 2020). Analyses by the American Board of Pediatrics also show variation in mean driving distance to care by subspecialty (ABP, 2023). However,
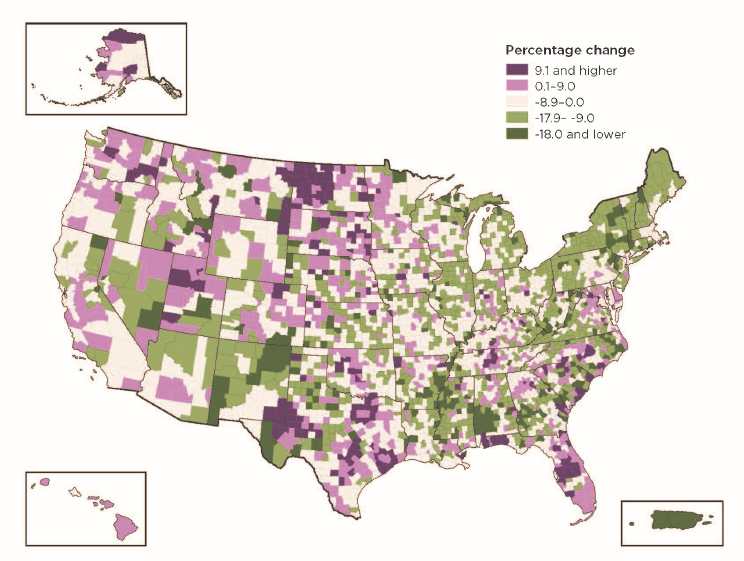
SOURCE: U.S. Census Bureau, 2020. Modified and reprinted with permission from U.S. Census Bureau.
driving distance may not be an accurate representation of the challenges patients and families face in receiving subspecialty care. For example, these measurements may not take certain sites of care into account such as outreach clinics from larger academic medical centers; in part, these locations may not be accounted for because there is limited data on their locations and use (Freed, 2021; Turner et al., 2022). During one of the committee’s public webinars, Joanna Lewis, pediatric residency program director and director for mobile health services at Advocate Children’s Hospital in Park Ridge, IL, described her program, which uses partnerships with hospitals and health systems to create multi-specialty pediatric ambulatory hubs (e.g., school-based health center, mobile unit) that provide local access to care.5
It is likely not a fair expectation for all children to live within a short distance of every type of subspecialist. As noted by Mayer (2006), “the practice locations of pediatric subspecialists parallel the geographic distribution of children in the United States.” The committee recognizes that more rural communities, for example, will not likely support full subspecialty practices, and so traveling for subspecialty care will likely always be necessary for various populations. Factors contributing to the regionalization of subspecialists include “that highly specialized physicians would be unlikely to have enough patients to attend to in any single community” and that access to technologies and other resources for care would be more available in centralized care centers (Gans et al., 2013). Furthermore, concentration of subspecialty care into centralized pediatric care centers leads to a higher volume of experience with rarer conditions and is associated with better outcomes (as compared to centers that see fewer cases per condition) (Howell et al., 2007; Khan et al., 2015; Lasswell et al., 2010; Michelson et al., 2018; Myers et al., 2019). Associated with regionalization, partnerships between larger hospital and community-based settings can help improve access to care for some subspecialties. For example, neonatal intensive care units are typically tiered according to the intensity of care they provide; as a result, some less complicated services may be provided in community-based settings, allowing for partnerships between facilities to provide comprehensive care (Stark et al., 2023). Outreach clinics, as described above, may also help extend the reach of centralized subspecialty care. Finally, when it comes to geographic distribution, accessibility to pediatric subspecialists, especially for rural and frontier communities, may be more directly impacted by lack of transportation or the unavailability of telehealth options, including reliable broadband access (Cortelyou-Ward et
___________________
5 The webinar recording can be accessed at https://www.nationalacademies.org/event/09-06-2022/the-pediatric-subspecialty-workforce-and-its-impact-on-child-health-and-well-being-webinar-2.
al., 2020; Marcin et al., 2016; Wolfe et al., 2020). (See Chapter 7 for more on the use of telehealth.)
Hospital Settings
Although most children receive pediatric subspecialty care in outpatient settings, inpatient care is another important access point for children who require pediatric subspecialty care. Overall, pediatric hospitalizations are decreasing, but children are admitted with increasing acuity and complexity of illness (Berry et al., 2013; Elixhauser, 2008; Horak et al., 2019; Witt et al., 2014). In addition, children are less likely to be cared for in non-academic, community hospitals, but instead are admitted to academic medical centers that offer tertiary care (i.e. comprehensive care across a wide range of conditions) (França and McManus, 2017). This change in care setting, driven in part by chronicity and complexity of illness as well as other health policies, resulted in an emerging trend in community hospitals closing their inpatient pediatric units, necessitating a shift in inpatient pediatric care to regional, tertiary-care children’s hospitals (Krugman and Rauch, 2022). Closure of inpatient pediatric units impacts access to pediatric subspecialty inpatient care, but also limits outpatient pediatric subspecialty care in those communities as well (Chang, 2018; França and McManus, 2018; Krugman and Rauch, 2022; VonAchen et al., 2022). Wider implications including patient outcomes and cost of care are not yet clear.
Financial Accessibility
Cost of care, insurance status, and insurance design can impact whether and how quickly patients can obtain subspecialty care due to limited networks, high out-of-pocket payments, and broader financing issues that affect access. See Chapter 8 for more information on the financing of children’s health care.
Barriers due to Insurance Type and Status
While all children may experience challenges in access to subspecialty care, these challenges may be magnified based on the specific type of insurance (i.e., Medicaid, Children’s Health Insurance Program [CHIP], private) and insurance status (i.e., insured versus uninsured). In general, being insured improves access to subspecialty care (Davidoff et al., 2005; Skinner and Mayer, 2007). Indeed, expansions in insurance coverage over the past decades, including expanded Medicaid eligibility for children, CHIP, the Affordable Care Act, and other changes have been successful in removing
the barrier of uninsurance for 95 percent of U.S. children (Tolbert et al., 2022).
In an older study by Bisgaier and Rhodes (2011), 66 percent of callers to specialty clinics were denied appointments when they reported Medicaid/CHIP insurance compared with 11 percent of callers who reported having commercial insurance. Among 89 clinics that accepted Medicaid/CHIP and private insurance, callers indicating Medicaid/CHIP enrollment were given on average a 22-day longer wait time. In a similar study, Bisgaier and colleagues (2012) found that callers with Medicaid/CHIP experienced lower rates of denial for appointments if the specialty clinic was affiliated with an academic medical center. However, callers with Medicaid/CHIP were given a 40-day longer wait time on average by these academic specialty clinics than callers with private insurance. Additionally, a meta-analysis of appointment availability audit studies that examined both pediatric and adult patients found that patients with Medicaid insurance experienced more difficulty securing an appointment for specialty care compared with primary care (Hsiang et al., 2019).
For both adults and children, Timbie et al. (2019) found that difficulty obtaining new patient specialty visits reported by community health centers varied by insurance type, with most respondents reporting difficulty for patients with no insurance (84 percent) or Medicaid (57 percent). The community health centers that reported difficulty obtaining specialty care for their patients insured by Medicaid rated several barriers as often or always contributing to poor access, including barriers related to “payment, coverage, and availability of appointments, including low Medicaid payment rates for specialists (78 percent), few specialists in Medicaid managed care organization (MCO) networks accepting new patients (69 percent), lack of Medicaid coverage for telemedicine (49 percent), and Medicaid MCOs’ administrative requirements for obtaining specialist consults (49 percent)” (Timbie et al., 2019). More research is needed to determine whether these denial trends have improved, worsened, or stayed the same over the past decade, and whether there are different rates for children and adults.
Difficulties in Cross State Access due to Insurance Policies
For some patients, the distance to the closest pediatric subspecialist or academic medical center is much shorter in a neighboring state compared to one within their own state, particularly in certain rural areas. For these patients and families, an out-of-state hospital is often the closest and most convenient option, ensuring they can receive cutting-edge care while lessening their transportation burdens (Meyer, 2021). While the issue of out-of-state care affects all populations, it is particularly relevant in the field of pediatrics. A review examining Medicaid payment for out-of-state hospital
services found that children’s hospitals serve a higher share of patients from out of state than any other type of hospital, with nearly 90 percent of children’s hospitals treating Medicaid patients that reside outside of their state compared to just under 60% of short-term acute care hospitals (MACPAC, 2020).
Health insurance may pose a barrier to accessing care out of state. Some health insurance plans may not cover out-of-state care or may have greater out-of-pocket costs if the out-of-state care is not considered in-network; this varies by type of insurance (e.g., commercial, or public) and by type of plan (e.g., Health Management Organizations, Preferred Provider Organizations, Exclusive Provider Organizations, Point of Service Plans) (Aetna, 2023).6 (See Chapter 8 for more information on network adequacy and narrow networks.) In Medicaid, federal law requires states to cover out-of-state services under certain circumstances, including a medical emergency; cases in which the beneficiary’s health would be at risk if they were required to travel to the state of residence; situations where services or resources are more readily available in another state; or instances where it is common practice for Medicaid recipients in a particular locality to use medical resources in another state (42 CFR § 431.52; MACPAC, 2020). However, administrative challenges may hinder provider availability to provide out-of-state care. Both clinicians and out-of-state hospitals must enroll with the patient’s home state Medicaid program and fulfill screening requirements. The specific requirements, as well as the time needed for screening and enrolling out-of-state providers, vary widely from state to state in terms of their approach, operational processes, application procedures, and verification timelines (GAO 2019; MACPAC, 2020; Manetto et al., 2020).7 Providers are routinely asked to enroll and re-enroll in multiple out-of-state Medicaid programs, and these administrative measures may result in delays in care (Manetto et al., 2020).
In addition, pediatric patients with Medicaid insurance may face additional obstacles in accessing out-of-state services due to state Medicaid regulations that restrict or limit out-of-state payments. States have some flexibility in determining reimbursement rates for out-of-state hospitals that may affect providers’ willingness to serve out-of-state Medicaid beneficiaries. For physician services covered under fee-for-service Medicaid, 26 of 36 states for which information could be found pay the in-state rate to out-of-state providers; of the remaining ten states, three use the in-state rate
___________________
6 Both health maintenance organizations and exclusive provider organizations have closed networks, meaning nonemergency care from out-of-network providers generally is not covered (Pollitz, 2022).
7 All states implemented Section 1135 waivers to allow out-of-state providers with equivalent licensing in another state to provide care to Medicaid enrollees during the pandemic, though many states have let those waivers lapse. For more information, see Chapter 7.
as a floor for out-of-state payment (MACPAC, 2017). For payment under Medicaid managed care, plans set reimbursement rates (Meyer, 2021). Some states have established different payment rates for out-of-state hospitals located in specific geographical areas. For example, Vermont’s Medicaid state plan designates some hospitals in neighboring states as “out-of-state in-network hospitals” (border hospitals) and pays them the same rate as in-state hospitals due to their close proximity and the general practice of Vermont residents to receive care at these hospitals (DVHA 2023), while making lower payments to other out-of-state hospitals that are not designated as border hospitals (MACPAC, 2020). Similar policies are being considered by other states, particularly for children’s hospitals in neighboring states, with the aim of achieving near-parity with in-state facilities (Meyer, 2021).
In 2021, CMS issued guidance outlining best practices to ensure that children with complex medical conditions receive prompt care out of state when medically necessary, including (1) states should pursue an abbreviated timeline for provider screening and enrollment, (2) states should promote access to telehealth services from out-of-state providers, and (3) states should establish economic and efficient provider payment rates to “ensure access to care and services available under the state plan and, under certain circumstances, provide coverage and payment when services are provided by out-of-state providers who serve children with medically complex conditions, consistent with section 1902(a)(30)(A) of the Act and 42 CFR § 431.52. States use a variety of payment methods to set rates paid to out-of-state providers and these methods should be clearly described in the Medicaid state plan” (CMS, 2021). CMS also released guidance in 2022 on a new Medicaid health home benefit for children with medically complex conditions that includes providing access to the full range of pediatric specialty and subspecialty medical services, including services from out-of-state providers (CMS, 2022). (See Chapter 7 for more information.)
Out-of-Pocket Costs
Children forgo or reduce service use in response to various cost-sharing mechanisms such as health plan deductibles and co-payments, a finding first reported by the classic RAND Health Insurance Experiment (Leibowitz et al., 1985). Over the past 15 years, while the proportion of children insured has expanded, there has been a steady growth in the number of children enrolled in high-deductible health plans. A data analysis commissioned by this committee from HealthCore found that use of high-deductible plans increased from 0.5 percent of the study population with commercial insurance in 2006 to 26 percent in 2021.8 (See Chapter 3 for more on this data
___________________
8 Commissioned HealthCore data analysis can be accessed in the Public Access File.
analysis.) This increase was also reported by Larson et al. (2021); using data from the National Health Interview Survey, Larson and colleagues found that the proportion of children with private insurance who were enrolled in these plans increased from 18 percent in 2007 to 49 percent in 2018 (Larson et al., 2021). That study defined these plans as those with a minimum deductible of $2,700 per family per year. They also found that compared with children with conventional private insurance, those with high-deductible health plans were more likely to forgo needed medical care and reported problems paying medical bills. More work is needed to understand how these plans are shaping children’s use of needed subspecialty care.
Another attribute of health plans that can increase costs of care for children is the composition of the provider network. Many plans include tiers of cost sharing, with reduced costs for using providers within a defined network and higher out-of-pocket costs for those providers who are out of network. Children with rare or complex diseases are more likely to need specialized providers who are not within a plan’s network. A recent study of children enrolled in commercial insurance found that those with complex chronic diseases were most likely to obtain out-of-network care, incurring markedly higher costs (Xu et al., 2022).
Other Financial Factors
Other patient and family financial factors may influence accessibility to care. For example, the ability to receive care may be influenced by the ability to take time off work to attend a medical visit (and the associated lost wages), the cost for child care for other children in the family, and transportation costs (Chang et al., 2018b). Additionally, little is known about how financial incentives inherent in alternative physician payment systems influence subspecialists’ decisions about use of specialized technology, frequency of follow-up visits, and availability of visits.
Organizational Accessibility
How subspecialty care is organized within a health care system contributes to the accessibility of that care, a dimension that can be monitored to some degree by appointment wait times. Most clinics monitor appointment wait time, often operationalized as the time to first visit for new patients. The number of subspecialists, the proportion of their time spent in clinical care, the balance of new versus follow-up visits, model of care (e.g., use of advanced practice registered nurses and generalists within the clinic), subspecialist-induced demand for follow-up, and the appointment system itself all influence appointment wait times. However, the relative
contribution of each of these factors to overall pediatric subspecialty access is currently unknown.
In a survey of 8,583 pediatric medical subspecialists conducted from 2012 to 2015, 10 percent of respondents reported typical wait times of longer than 8 weeks, with highest levels reported for developmental-behavioral pediatrics (50 percent), neurology (30 percent), endocrinology (23 percent), and rheumatology (16 percent) (Rimsza et al., 2018). Long wait times to see a specialist are associated with increased chances of not attending the first visit with a specialist for a new health problem and forgoing needed care (Stephens et al., 2019).
One possible reason for the longer wait times in some subspecialties may be the changing epidemiology of pediatric disorders, noted earlier in this chapter. For example, it is possible that a contributing factor to the long wait times for subspecialties such as developmental-behavioral pediatrics and child neurology is the increasing number of children with diagnosed neurodevelopmental disorders (Visser et al., 2014), some of whom may be children who were born and survive at a greater severity of prematurity.
In 2017, the Children’s Hospital Association surveyed 40 children’s teaching hospitals to highlight the specialties with the longest appointment wait times and vacancies (i.e., staffing shortages) at their institutions (CHA, 2017). Developmental pediatrics, child and adolescent psychiatry, and pediatric neurology were ranked as the specialties with the largest shortages affecting ability to deliver care. The specialties with the longest appointment wait times included genetics (21 weeks), developmental pediatrics (19 weeks), pain management and palliative care (12 weeks), and child and adolescent psychiatry (10 weeks). See Chapter 7 for more on referral innovations to reduce wait times.
Accessibility Related to Demographic and Cultural Factors
A variety of demographic and cultural factors (e.g., race/ethnicity, language, gender identity, educational level) can influence a person’s ability to access needed health care. Studies of implicit bias in health care (in general) show that “biases are likely to influence diagnosis and treatment decisions and levels of care in some circumstances” (FitzGerald and Hurst, 2017, p.1). While the literature base on these influences specific to pediatric medical subspecialty care is limited, the following sections provide an overview of several demographic and cultural factors that can influence access to care.
Racial and Ethnic Disparities in Access
As noted by Flores and Lin (2013), “minority children continue to experience multiple disparities in medical and oral health and healthcare.”
In particular, they noted that all minoritized groups (except for Asian/Pacific Islander) had difficulty accessing specialty care (as compared with White children). Disparities by race and ethnicity persist for children’s access to general and subspecialty physical and mental health care (Alberto et al., 2019; Burdick et al., 2023; Rodgers et al., 2022). For example, in one study of children with medical complexity insured by Medicaid, Black non-Hispanic and Hispanic children had lower outpatient visit rates as compared with White non-Hispanic children (Ming et al., 2022). Another study of children with ADHD concluded that “disparities in ADHD treatment among children from racial–ethnic minority populations may be driven primarily by disparities in access rather than in utilization.” (Yang et al., 2022). (See Chapter 6 for more on diversity in research.)
Racial and ethnic disparities in access to care may be related to the fact that some patients have indicated a preference for racial/ethnic concordance in their health care practitioners (i.e., someone of their own rate or ethnicity), and racial/ethnic concordance has been associated with reduction in health care disparities and increased patient satisfaction (Alberto et al., 2021; Greenwood et al., 2020; Takeshita et al., 2020). However, the diversity of the pediatric health care workforce in general, and the pediatric subspecialty workforce specifically, does not reflect the diversity of the population it serves. (See Chapter 4 for more on workforce diversity.)
Immigration Status
Some limited evidence shows that immigration status may be associated with barriers to needed health care in general, such as policies that limit access to insurance (Perreira and Pedroza, 2019). This may be particularly important for pregnant women who are ineligible for Medicaid (because of their immigration status) and as a result receive inadequate prenatal care. Insurance eligibility expansions have been associated with increased use of prenatal care (Drewry et al., 2015; Fuentes-Afflick et al., 2006).
Language Barriers
Language-specific barriers can affect the ability of children to access needed subspecialty care (Cohen and Christakis, 2006; Flower et al., 2021; St. Amant et al., 2018; Wojcik et al., 2023; Yu et al., 2004). Particular challenges include lack of bilingual interpreters and difficulty for the child’s parents in communicating over the phone. Language concordance care has been defined as “the provision of health care in a shared non-dominant minority language” (Lor and Martinez, 2020). In general, language concordance has been associated with levels of trust and patient satisfaction, but
has mixed evidence for its impact on health outcomes (Hsueh et al., 2021; Lor and Martinez, 2020). In pediatrics specifically, language concordance, including the use of interpreters, has been associated with greater satisfaction, improved communication, and enhanced understanding (Dunlap et al., 2015; Gutman et al., 2018; Jaramillo et al., 2016). In addition, studies show underrepresentation of non-English-speaking children or children of non-English-speaking parents in pediatric research (Aristizabal et al., 2015; Chen et al., 2023).
Transitioning from Pediatric to Adult Care
Many adolescents with chronic conditions experience fragmented care as they transition from pediatric to adult subspecialty care and may receive care from pediatric clinicians into adulthood (Lebrun-Harris et al., 2018; McManus et al., 2020). The transition from child to adult medical and behavioral health care often is associated with poor outcomes among young adults, with challenges including discontinuities in care, differences between the child/adolescent and adult health systems, a lack of available adult clinicians, difficulties in breaking the bond with pediatric clinicians, lack of payment for transition support, a lack of training in childhood-onset conditions among adult clinicians, the failure of pediatric clinicians to prepare adolescents for an adult model of care, and a lack of communication between pediatric and adult clinicians and systems of care (NASEM, 2015). In terms of pediatric specialty care, only 17 percent of youth with special health care needs and 14 percent of youth without special health care needs receive anticipatory guidance on transition preparation from their health care providers (Lebrun-Harris et al., 2018).
While the transition of care to adult clinicians is complex and requires the cooperation of patients and their families, clinicians play an essential role in successful transition (White et al., 2018). Got Transition’s Six Core Elements of Health Care Transition™ 3.0 is the widely adopted approach based on a report from a coalition that included the Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians (White et al., 2020). The Six Core Elements define the basic components of a structured transition process and include customizable sample tools for each core element, with tailoring to the type of practice facilitating the health care transition and type of condition (see Table 2-1).
Many well-described barriers to transition of care exist at the clinician level, particularly the lack of coordination between pediatric and adult clinicians at the time of transition. The list of potential clinician-level barriers to transition is extensive (see Box 2-2).
TABLE 2-1 Summary of Six Core Elements approach for pediatric and adult practices
| Practice or Provider | #1: Transition and/or care policy | #2: Tracking and monitoring | #3: Transition readiness and/or orientation to adult practice | #4: Transition planning and/or integration into adult approach to care or practice | #5: Transfer of care and/or initial visit | #6: Transition completion or ongoing care |
|---|---|---|---|---|---|---|
| Pediatric | Create and discuss with youth and/or family | Track progress of youth and/or family transition preparation and transfer | Conduct transition readiness assessments | Develop transition plan, including needed readiness assessment skills and medical summary, prepare youth for adult approach to care, and communicate with new clinician | Transfer of care with information and communication including residual pediatric clinician’s responsibility | Obtain feedback on the transition process and confirm young adult has been seen by the new clinician |
| Adult | Create and discuss with young adult and guardian, if needed | Track progress of young adult’s integration into adult care | Share and discuss welcome and FAQs with young adult and guardian, if needed | Communicate with previous clinician, ensure receipt of transfer package | Review transfer backage, address young adult’s needs and concerns at initial visit, update self-care assessment and medical summary | Confirm transfer completion with previous clinician, provide ongoing care with self-care skill building and link to needed specialists |
NOTE: Clinicians who care for youth and/or young adults throughout the lifespan can use both the pediatric and adult sets of core elements without the transfer process components.
SOURCES: White et al., 2020. Copyright ©2014–2023 GOT TRANSITION®.
Certain types of pediatric patients face additional barriers. For example, an analysis of 2017 National Electronic Health Records Survey data found that pediatricians are more likely to accept Medicaid insurance than adult clinicians (MACPAC, 2021). This raises questions about how difficult it is for pediatric patients with Medicaid insurance to transition to adult care. Understanding these use patterns is critical when implementing transition of care programs.
USE OF SUBSPECIALTY CARE
Use of subspecialty care indicates whether a service is received; it does not say whether the service was needed or the quality of that service provision. Pediatric subspecialists assist children and their families by attending to health problems referred to them, providing advice, performing procedures, and sharing in the care of patients with unstable health conditions. Four types of referrals encapsulate these responsibilities: (1) short-term non-procedural consultation for diagnostic or treatment advice; (2) short-term procedural consultation for a specific diagnostic evaluation (e.g., echocardiogram, allergy testing) or management (e.g., endoscopy for a gastrointestinal bleed); (3) longer term co-management in which they share care for the health problem with primary care clinicians; and (4) principal care, which involves co-management with the specialist providing all the care for a given problem (Forrest, 2009). See Chapter 3 for data analyses on the use of pediatric subspecialty care and Chapter 7 for more on the primary care–subspecialist interface, including referral.
OUTCOMES OF SUBSPECIALTY CARE
Advances in pediatric care in general have led to dramatic improvements in the health and well-being of children (see Chapter 1). Measuring quality of care, including clinical outcomes, can be difficult in subspecialty pediatrics given the low prevalence of many of the conditions addressed by subspecialists, the impact of different developmental stages among pediatric patients, and the challenges of demonstrating long-term impact of care (Schuster, 2015). Evidence from small studies of individual subspecialties suggests that pediatric subspecialists are more likely to perform comprehensive assessments and adhere to evidence-based guidelines of care for a particular disorder, compared with care by non-specialists (Cloutier et al., 2018; Conway et al., 2006; Feldman et al., 2015; Hudgins et al., 2021; McCulloh et al., 2012). Evidence on clinical outcomes from subspecialty care (as compared to non-specialty care or no care) is limited. Specific examples from individual studies include:
- Survival from pediatric non-traumatic cardiac arrest in pediatric emergency departments was higher than in general emergency departments (Michelson et al., 2018).
- Five-year survival rates for pediatric leukemias were significantly lower (46.4 percent versus 75.1 percent) for patients not treated at a pediatric cancer center (Howell et al., 2007).
- Lung transplantation in children was associated with better survival when performed at pediatric centers as opposed to adult centers, even if the volume at the adult centers (including adult transplantation) was higher (Khan et al., 2015).
- There is some evidence of better outcomes when surgery is performed by a pediatric surgeon as compared to general surgeons (Borenstein et al., 2005; Evans and van Woerden, 2011).
Medical advances in the twentieth century and more recently have resulted in more children with complex medical needs surviving past infancy, increasing the need for timely access to pediatric subspecialty care (Lonetti et al., 2019; Oh et al., 2022; Siegel et al., 2020). For example, between 2002 and 2016, death rates decreased for some childhood cancers such as pediatric leukemias and lymphomas (Siegel et al., 2020). Survival rates for children with acute myeloid leukemia are now at 70 percent (Lonetti et al., 2019). Yet despite these gains, the impact on survival varies by type of disorders, type of treatment, and sociodemographic characteristics. For example, from 2001 to 2015, survival from pediatric cancers were highest among females, those aged 15 to 19 years, non-Hispanic Whites, and those residing in counties in the top 25 percent by economic status (Siegel et al., 2020). According to Yohe et al. (2019), “overall survival rates for pediatric patients with high-risk or relapsed rhabdomyosarcoma have not improved
significantly since the 1980s.” Advanced heart failure in children with congenital heart disease is uncommon but increasing and is associated with significant morbidity, mortality, and resource use, with approximately one in five affected children not surviving to hospital discharge (Burstein et al., 2019). Moreover, children’s all-cause mortality rates in the United States are increasing, although much of this is attributable to increases in injury-related deaths, including gun violence (Woolf et al., 2023).
KEY FINDINGS AND CONCLUSIONS
Key Findings
Finding #2-1: There have been significant changes in the physical, mental, and behavioral health status of the U.S. pediatric population, which drives need and demand for subspecialty care.
Finding #2-2: Children’s health needs are becoming increasingly more complex.
Finding #2-3: There are factors beyond provider supply that impact access to needed pediatric subspecialty care, including patient/family factors (e.g., insurance and out-of-pocket costs, time availability, broadband access, and transportation), subspecialty provider factors (e.g., provider network, care model), and health system-level factors (e.g., reimbursement model, geospatial distribution of clinicians, and equity).
Finding #2-4: Demand for subspecialty care is driven by patients and families (including self-referral), primary care clinicians (for short-term consultation or long-term co-management), and subspecialists themselves (for return visits or for cross-referral to other subspecialists).
Finding #2-5: Children covered by Medicaid, rural children, and children with chronic illness or special health care needs often face increased access barriers to pediatric subspecialty care.
Finding #2-6: The financial viability to support a practice in some locations, such as rural areas (given the lower prevalence of many disorders cared for by subspecialists), contributes to the geographic distribution of subspecialists.
Finding #2-7: The increase in closings of both rural and urban hospitals, and diminished pediatric services within non-children’s hospitals,
further exacerbates the problem of limited access to pediatric subspecialty care.
Finding #2-8: High-volume experience with children is associated with improved health outcomes.
Finding #2-9: Demographic and cultural factors such as racial/ethnic concordance, language, and immigration status can influence access to care.
Conclusions
Conclusion #2-1: Pediatric medical subspecialists play a pivotal role in enhancing the survival and health of children with chronic conditions and complex health care needs.
Conclusion #2-2: Children’s use of subspecialty care is influenced by a complex and interconnected mix of patient, family, community, provider, and health system factors.
Conclusion #2-3: Regionalization of medical subspecialty care is logical given the lower prevalence of conditions requiring subspecialty care and the technologies and resources available in centralized centers of care.
Conclusion #2-4: The pediatric workforce and the health care system more generally need to be nimble in their ability to be responsive to the changing health care needs of infants, children, and adolescents.
Conclusion #2-5: A systematic approach to monitoring children’s changing health needs and access to pediatric primary and subspecialty care is needed to inform interventions to improve equity in subspecialty care as well as to prepare the optimal workforce to be able to address those needs.
RECOMMENDATION
The needs of children in the twenty-first century differ from the needs of those in the twentieth century. More attention is needed to ensure optimal access, coordination, and impact on the health and well-being of infants, children, and adolescents. The Agency for Healthcare Research and Quality (AHRQ) produces an annual report on health care quality and disparities (AHRQ, 2023). Similarly, improved monitoring of children’s changing health needs and demands, access to care, disparities, and trends
in the pediatric workforce are all essential to inform future workforce planning efforts. Understanding these trends will help determine the appropriate education and training needed to prepare the pediatric workforce to work collaboratively toward meeting children’s health care needs and which subspecialties should be prioritized for different interventions or programs (e.g. loan repayment) and inform innovative models of care to improve access. Therefore, in order to achieve a goal of promoting collaboration and effective use of services between pediatric primary care clinicians and subspecialty physicians, the committee provides the following recommendation:
RECOMMENDATION 2-1 The Agency for Healthcare Research and Quality should submit a biennial report to the Secretary of the Department of Health and Human Services summarizing the changing demands and needs for pediatric primary and subspecialty care, status of access to that care, and disparities in receipt of those services. This report should include information on the pediatric generalist and subspecialist workforce broadly (including data on clinicians from backgrounds underrepresented in medicine).
REFERENCES
ABP (American Board of Pediatrics). 2023. Estimated driving distance to visit a pediatric subspecialist. https://www.abp.org/content/estimated-driving-distance-visit-pediatric-subspecialist (accessed April 21, 2023).
AECD (Annie E. Casey Foundation). 2022. 2022 KIDS COUNT data book. https://www.aecf.org/resources/2022-kids-count-data-book (accessed December 22, 2022).
Aetna. 2023. HMO, POS, PPO, EPO and HDHP with HSA: What’s the difference? https://www.aetna.com/health-guide/hmo-pos-ppo-hdhp-whats-the-difference.html (accessed July 14, 2023).
AHRQ (Agency for Healthcare Research and Quality). 2017. Anxiety in children. https://effectivehealthcare.ahrq.gov/products/anxiety-children/research-2017 (accessed May 2, 2023).
AHRQ. 2022. Attention deficit hyperactivity disorder: Diagnosis and treatment in children and adolescents. https://effectivehealthcare.ahrq.gov/products/attention-deficit-hyperactivity-disorder/protocol (accessed May 2, 2023).
AHRQ. 2023. National Healthcare Quality and Disparities Reports. https://www.ahrq.gov/research/findings/nhqrdr/index.html (accessed May 5, 2023).
Alberto, C. K., J. Kemmick Pintor, R. M. McKenna, D. H. Roby, and A. N. Ortega. 2019. Racial and ethnic disparities in provider-related barriers to health care for children in California after the ACA. Global Pediatric Health 6:1-9.
Alberto, C. K., J. Kemmick Pintor, A. Martinez-Donate, L. P. Tabb, B. Langellier, and J. P. Stimpson. 2021. Association of maternal-clinician ethnic concordance with Latinx youth receipt of family-centered care. JAMA Network Open 4(11):e2133857.
Amminger, G. P., L. P. Henry, S. M. Harrigan, M. G. Harris, M. Alvarez-Jimenez, H. Herrman, H. J. Jackson, and P. D. McGorry. 2011. Outcome in early-onset schizophrenia revisited: Findings from the early psychosis prevention and intervention centre long-term follow-up study. Schizophrenia Research 131(1-3):112-119.
Anderson, G., and J. Horvath. 2002. Chronic conditions: Making the case for ongoing care. http://www.partnershipforsolutions.org/DMS/files/chronicbook2002.pdf (accessed April 13, 2023).
Arakelyan, M. S. Freyleue, D. Avula, J. L. McLaren, A. J. O’Malley, and J. K. Leyenaar. 2023. Pediatric mental health hospitalizations at acute care hospitals in the U.S., 2009-2019. JAMA 329(12):1000-1011.
Aristizabal, P., J. Singer, R. Cooper, K. J. Wells, J. Nodora, M. Milburn, S. Gahagan, D. E. Schiff, and M. E. Martinez. 2015. Participation in pediatric oncology research protocols: Racial/ethnic, language and age-based disparities. Pediatric Blood & Cancer 62(8):1337-1344.
Baio, J., L. Wiggins, D. L. Christensen, M. J. Maenner, J. Daniels, Z. Warren, M. KurziusSpencer, W. Zahorodny, C. R. Rosenberg, and T. White. 2018. Prevalence of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, United States, 2014. MMWR Surveillance Summaries 67(6):1.
Bardach, N. S., T. R. Coker, B. T. Zima, J. M. Murphy, P. Knapp, L. P. Richardson, G. Edwall, and R. Mangione-Smith. 2014. Common and costly hospitalizations for pediatric mental health disorders. Pediatrics 133(4):602-609.
Berg, A. T., H. H. Altalib, and O. Devinsky. 2017. Psychiatric and behavioral comorbidities in epilepsy: A critical reappraisal. Epilepsia 58(7):1123-1130.
Berry, J. G., M. Hall, D. E. Hall, D. Z. Kuo, E. Cohen, R. Agrawal, K. D. Mandl, H. Clifton, and J. Neff. 2013. Inpatient growth and resource use in 28 children’s hospitals: A longitudinal, multi-institutional study. JAMA Pediatrics 167(2):170-177.
Bisgaier, J., and K. V. Rhodes. 2011. Auditing access to specialty care for children with public insurance. New England Journal of Medicine 364(24):2324-2333.
Bisgaier, J., D. Polsky, and K. V. Rhodes. 2012. Academic medical centers and equity in specialty care access for children. Archives of Pediatrics and Adolescent Medicine 166(4):304-310.
Bitsko, R. H., A. H. Claussen, J. Lichstein, L. I. Black, S. E. Jones, M. L. Danielson, J. M. Hoenig, S. P. Davis Jack, D. J. Brody, S. Gyawali, M. J. Maenner, M. Warner, K. M. Holland, R. Perou, A. E. Crosby, S. J. Blumberg, S. Avenevoli, J. W. Kaminski, and R. M. Ghandour. 2022. Mental health surveillance among children—United States, 2013-2019. Morbidity and Mortality Weekly Report 71(Suppl 2):1-42.
Bitzer, E. M., S. Volkmer, M. Petrucci, N. Weissenrieder, and M.-L. Dierks. 2012. Patient satisfaction in pediatric outpatient settings from the parents’ perspective—the child zap: A psychometrically validated standardized questionnaire. BMC Health Services Research 12(1):347.
Blackwell, C. K., A. J. Elliott, J. Ganiban, J. Herbstman, K. Hunt, C. B. Forrest, and C. A. Carmago, Jr. 2019. General health and life satisfaction in children with chronic illness. Pediatrics 143(6):e20182988.
Borenstein, S. H., T. To, A. Wajja, and J.C. Langer. 2005. Effect of subspecialty training and volume on outcome after pediatric inguinal hernia repair. Journal of Pediatric Surgery 40(1):75-80.
Bright, M. A., C. Knapp, M. S. Hinojosa, S. Alford, and B. Bonner. 2016. The comorbidity of physical, mental, and developmental conditions associated with childhood adversity: A population based study. Maternal and Child Health Journal 20:843-853.
Brunkhorst-Kanaan, N., B. Libutzki, A. Reif, H. Larsson, R. V. McNeill, and S. Kittel-Schneider. 2021. ADHD and accidents over the life span—a systematic review. Neuroscience & Biobehavioral Reviews 125:582-591.
Burdick, K. J., L. K. Lee, R. Mannix, M. C. Monuteaux, M. P. Hirsh, and E. W. Fleegler. 2023. Racial and ethnic disparities in access to pediatric trauma centers in the United States: A geographic information systems analysis. Annals of Emergency Medicine 81(3):325-333.
Burstein, D. S., P. Shamszad, D. Dai, C. S. Almond, J. F. Price, K. Y. Lin, M. J. O’Connor, R. E. Shaddy, C. E. Mascio, and J. W. Rossano. 2019. Significant mortality, morbidity and resource utilization associated with advanced heart failure in congenital heart disease in children and young adults. American Heart Journal 209:9-19.
Butwicka, A., W. Fendler, A. Zalepa, A. Szadkowska, M. Zawodniak-Szalapska, A. Gmitrowicz, and W. Mlynarski. 2016. Psychiatric disorders and health-related quality of life in children with type 1 diabetes mellitus. Psychosomatics 57(2):185-193.
CAHMI (Child and Adolescent Health Measurement Initiative). 2023a. 2020 National Survey of Children’s Health (NSCH) data query: Indicator 1.9: Does this child have current or lifelong health conditions? https://www.childhealthdata.org/browse/survey/results?q=8838&r=1 (accessed April 21, 2023).
CAHMI. 2023b. 2020 National Survey of Children’s Health (NSCH) data query: Indicator 4.5: During the past 12 months, did this child see a specialist other than a mental health professional? https://www.childhealthdata.org/browse/survey/results?q=9391&r=1&g=1000 (accessed April 21, 2023).
CDC (Centers for Disease Control and Prevention). 2020. QuickStats: Percentage of children aged <18 years who received a well-child checkup in the past 12 months, by age group and year—National Health Interview Survey, United States, 2008 and 2018. https://www.cdc.gov/mmwr/volumes/69/wr/mm6908a5.htm (accessed April 20, 2023).
CDC. 2021. Children and youth with special healthcare needs in emergencies. https://www.cdc.gov/childrenindisasters/children-with-special-healthcare-needs.html#:~:text=Children%20and%20youth%20with%20special%20healthcare%20needs%20(CYSHCN)%2C%20also,than%20their%20typically%20developing%20peers (accessed April 21, 2023).
CDC. 2022. Diseases you almost forgot about (thanks to vaccines). https://www.cdc.gov/vaccines/parents/diseases/forgot-14-diseases.html (accessed December 22, 2022).
CDC. 2023. Data and statistics on children’s mental health. https://www.cdc.gov/childrens-mentalhealth/data.html (accessed May 5, 2023).
CHA (Children’s Hospital Association). 2017. Pediatric workforce shortages persist https://glin.com/files/documents/bulletin_board/chgme_workforce_shortage_fact_sheet.pdf (accessed April 21, 2023).
Chang, H.- K., J.-W. Hsu, J.-C. Wu, K.-L. Huang, H.-C. Chang, Y.-M. Bai, T.-J. Chen, and M.-H. Chen. 2018a. Traumatic brain injury in early childhood and risk of attention-deficit/hyperactivity disorder and autism spectrum disorder: A nationwide longitudinal study. The Journal of Clinical Psychiatry 79(6):21226.
Chang, L. V., A. N. Shah, E. R. Hoefgen, K. A. Auger, H. Weng, J. M. Simmons, S. S. Shah, and A. F. Beck on behalf of the H2O Study Group. 2018b. Lost earnings and nonmedical expenses of pediatric hospitalizations. Pediatrics 142(3):e20180195.
Chang, W. W. 2018. The rapidly disappearing community pediatric inpatient unit. https://www.the-hospitalist.org/hospitalist/article/170115/pediatrics/rapidly-disappearing-community-pediatric-inpatient-unit (accessed April 13, 2023).
Charpignon, M.-L., J. Ontiveros, S. Sundaresan, A. Puri, J. Chandra, K. D. Mandl, and M. S. Majumder. 2022. Evaluation of suicides among U.S. adolescents during the COVID-19 pandemic. JAMA Pediatrics 176(7):724-726.
Chavira, D. A., A. F. Garland, S. Daley, and R. Hough. 2008. The impact of medical comorbidity on mental health and functional health outcomes among children with anxiety disorders. Journal of Developmental and Behavioral Pediatrics 29(5):394-402.
Chen, A., S. Demaestri, K. Schweiberger, J. Sidani, R. Wolynn, D. Chaves-Gnecco, R. Hernandez, S. Rothenberger, E. Mickievicz, J. D. Cowden, and M. I. Ragavan. 2023. Inclusion of non-English speaking participants in pediatric research: A review. JAMA Pediatrics 177(1):81-88.
Cheung, A. H., N. Kozloff, and D. Sacks. 2013. Pediatric depression: An evidence-based update on treatment interventions. Current Psychiatry Reports 15:1-8.
Cloutier, M. M., P. M. Salo, L. J. Akinbami, R. D. Cohn, J. C. Wilkerson, G. B. Diette, S. Williams, K. S. Elward, J. M. Mazurek, J. R. Spinner, T. A. Mitchell, and D. C. Zeldin. 2018. Clinician agreement, self-efficacy, and adherence with the guidelines for the diagnosis and management of asthma. Journal of Allergy and Clinical Immunology: In Practice 6(3):886-894.e4.
CMS (Centers for Medicare & Medicaid Services). 2021. Guidance on coordinating care provided by out-of-state providers for children with medically complex conditions. https://www.medicaid.gov/federal-policy-guidance/downloads/cib102021.pdf (accessed April 18, 2023).
CMS. 2022. Re: Health homes for children with medically complex conditions. https://www.medicaid.gov/federal-policy-guidance/downloads/smd22004.pdf (accessed April 18, 2023).
Cohen, A. L., and D. A. Christakis. 2006. Primary language of parent is associated with disparities in pediatric preventive care. The Journal of Pediatrics 148(2):254-258.
Coker, T. R., M. N. Elliott, S. L. Toomey, D. C. Schwebel, P. Cuccaro, S. Tortolero Emery, S. L. Davies, S. N. Visser, and M. A. Schuster. 2016. Racial and ethnic disparities in ADHD diagnosis and treatment. Pediatrics 138(3):e20160407.
Connolly, M. D., M. J. Zervos, C. J. Barone II, C. C. Johnson, and C. L. M. Joseph. 2016. The mental health of transgender youth: Advances in understanding. Journal of Adolescent Health 59(5):489-495.
Conway, P. H., S. Edwards, E. R. Stucky, V. W. Chiang, M. C. Ottolini, and C. P. Landrigan. 2006. Variations in management of common inpatient pediatric illnesses: Hospitalists and community pediatricians. Pediatrics 118(2):441-447.
Cortelyou-Ward, K. D., N. Atkins, A. Noblin, T. Rotarius, Ph. White, and C. Carey. 2020. Navigating the digital divide: Barriers to telehealth in rural areas. Journal of Health Care for the Poor and Underserved 31(4):1546-1556.
Cree, R. A., R. H. Bitsko, L. R. Robinson, J. R. Holbrook, M. L. Danielson, C. Smith, J. W. Kaminski, M. K. Kenney, and G. Peacock. 2018. Health care, family, and community factors associated with mental, behavioral, and developmental disorders and poverty among children aged 2-8 years—United States, 2016. Morbidity and Mortality Weekly Report 67(50):1377-1383.
Curtin, S. 2020. State suicide rates among adolescents and young adults aged 10-24: United States, 2000–2018. National Vital Statistics Reports 69(11):1-10.
Danielson, M. L., R. H. Bitsko, R. M. Ghandour, J. R. Holbrook, M. D. Kogan, and S. J. Blumberg. 2018. Prevalence of parent-reported ADHD diagnosis and associated treatment among U.S. children and adolescents, 2016. Journal of Clinical Child & Adolescent Psychology 47(2):199-212.
Darby, J. B., N. Tamaskar, S. Kumar, K. Sexson, M. de Guzman, M. E. M. Rocha, and S. T. Shulman. 2019. Variability in Kawasaki disease practice patterns: A survey of hospitalists at pediatric hospital medicine 2017. Hospital Pediatrics 9(9):724-728.
Davidoff, A., G. Kenney, and L. Dubay. 2005. Effects of the State Children’s Health Insurance Program expansions on children with chronic health conditions. Pediatrics 116(1):e34-e42.
Drewry, J., B. Sen, M. Wingate, J. Bronstein, E. M. Foster, and M. Kotelchuck. 2015. The impact of the State Children’s Health Insurance Program’s unborn child ruling expansions on foreign-born Latina prenatal care and birth outcomes, 2000–2007. Maternal and Child Health Journal 19(7):1464-1471.
Dunlap, J. L., J. D. Jaramillo, R. Koppolu, R. Wright, F. Mendoza, and M. Bruzoni. 2015. The effects of language concordant care on patient satisfaction and clinical understanding for Hispanic pediatric surgery patients. Journal of Pediatric Surgery 50(9):1586-1589.
DVHA (Department of Vermont Health Access). 2023. Provider network info. https://dvha.vermont.gov/providers/provider-network-info (accessed July 14, 2023).
Elixhauser, A. 2008. Statistical Brief #56: Hospital stays for children, 2006. https://hcup-us.ahrq.gov/reports/statbriefs/sb56.jsp (accessed April 20, 2023).
Epstein, J. N., K. J. Kelleher, R. Baum, W. B. Brinkman, J. Peugh, W. Gardner, P. Lichtenstein, and J. Langberg. 2014. Variability in ADHD care in community-based pediatrics. Pediatrics 134(6):1136-1143.
Evans, C., and H. C. van Woerden. 2011. The effect of surgical training and hospital characteristics on patient outcomes after pediatric surgery: A systematic review. Journal of Pediatric Surgery 46(11):2119-2127.
Fegert, J. M., B. Vitiello, P. L. Plener, and V. Clemens. 2020. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child and Adolescent Psychiatry and Mental Health 14(20). https://doi.org/10.1186/s13034-020-00329-3.
Feldman, H. M., N. J. Blum, A. E. Gahman, and J. Shults. 2015. Diagnosis of attention-deficit/hyperactivity disorder by developmental pediatricians in academic centers: A DBPnet study. Academic Pediatrics 15(3):282-288.
Finning, K., O. C. Ukoumunne, T. Ford, E. Danielsson-Waters, L. Shaw, I. R. De Jager, L. Stentiford, and D. A. Moore. 2019. The association between child and adolescent depression and poor attendance at school: A systematic review and meta-analysis. Journal of Affective Disorders 245:928-938.
FitzGerald, C. and S. Hurst. 2017. Implicit bias in healthcare professionals: A systematic review. BMC Medical Ethics 18:19.
Flores, G., and Lin, H. 2013. Trends in racial/ethnic disparities in medical and oral health, access to care, and use of services in U.S. children: Has anything changed over the years? International Journal for Equity in Health 12(10). https://doi.org/10.1186/1475-9276-12-10.
Flower, K. B., S. Wurzelmann, C. Tucker, C. Rojas, M. E. Díaz-González de Ferris, and F. Sylvester. 2021. Spanish-speaking parents’ experiences accessing academic medical center care: Barriers, facilitators and technology use. Academic Pediatrics 21(5):793-801.
Forrest, C. B. 2009. A typology of specialists’ clinical roles. Archives of Internal Medicine 169(11):1062-1068.
Forrest, C. B., J. Schuchard, C. Bruno, S. Amaral, E. D. Cox, K. E. Flynn, P. S. Hinds, I. Huang, M. D. Kappelman, J. A. Krishnan, R. B. Kumar, J. Lai, A. S. Paller, W. Phipatanakul, L. E. Schanberg, K. Sumino, E. R. Weitzman, and B. B. Reeve. 2022. Self-reported health outcomes of children and youth with 10 chronic diseases. Journal of Pediatrics 246:207-212.e.1. https://doi.org/10.1016/j.jpeds.2022.02.052.
França, U. L., and M. L. McManus. 2017. Availability of definitive hospital care for children. JAMA Pediatrics 171(9):e171096.
França, U. L., and M. L. McManus. 2018. Trends in regionalization of hospital care for common pediatric conditions. Pediatrics 141(1):e20171940.
Franks, P. W., R. L. Hanson, W. C. Knowler, M. L. Sievers, P. H. Bennett, and H. C. Looker. 2010. Childhood obesity, other cardiovascular risk factors, and premature death. New England Journal of Medicine 362:485-493.
Freed, G. L. 2021. Editorial: The pediatric subspecialty workforce is more complex than meets the eye. JAMA Pediatrics 175(10):1006-1008.
Fristad, M. A., and H. A. MacPherson. 2014. Evidence-based psychosocial treatments for child and adolescent bipolar spectrum disorders. Journal of Clinical Child & Adolescent Psychology 43(3):339-355.
Fuentes-Afflick, E., N. A. Hessol, T. Bauer, M. J. O’Sullivan, V. Gomez-Lobo, S. Holman, T. E. Wilson, and H. Minkoff. 2006. Use of prenatal care by Hispanic women after welfare reform. Obstetrics and Gynecology 107(1):151-160.
Gans, D., M. Battistelli, M. Ramirez, L. Cabezas, and N. Pourat. 2013. Assuring children’s access to pediatric subspecialty care in California. Los Angeles, CA: UCLA Center for Health Policy Research.
GAO (U.S. Government Accountability Office). 2019. CMS oversight should ensure state implementation of screening and enrollment requirements. Report no. GAO-20-8. Washington, DC: GAO. https://www.gao.gov/products/GAO-20-8 (accessed July 14, 2023).
Gerteis, J., D. Izrael, D. Deitz, L. LeRoy, R. Ricciardi, T. Miller, and J. Basu. 2014. Multiple chronic conditions chartbook. Rockville, MD: Agency for Healthcare Research and Quality. pp. 7-14.
Ghandour, R. M., L. J. Sherman, C. J. Vladutiu, M. M. Ali, S. E. Lynch, R. H. Bitsko, and S. J. Blumberg. 2019. Prevalence and treatment of depression, anxiety, and conduct problems in U.S. children. The Journal of Pediatrics 206:256-267.e3.
Greenwood, B. N., R. R. Hardeman, L. Huang, and A. Sojourner. 2020. Physician–patient racial concordance and disparities in birthing mortality for newborns. Proceedings of the National Academy of Sciences 117(35):21194-21200.
Gutman, C. K., L. Cousins, J. Gritton, E. J. Klein, J. C. Brown, J. Scannell, and K. C. Lion. 2018. Professional interpreter use and discharge communication in the pediatric emergency department. Academic Pediatrics 18(8):935-943.
Hoagwood, K., and S. S. Olin. 2002. The NIMH Blueprint for Change Report: Research priorities in child and adolescent mental health. Journal of the American Academy of Child and Adolescent Psychiatry 41(7):760-767.
Hogan, M. F. 2003. The President’s New Freedom Commission: Recommendations to transform mental health care in America. Psychiatric Services 54(11):1467-1474.
Horak, R. V., J. F. Griffin, A. Brown, S. T. Nett, L. M. Christie, M. L. Forbes, S. Kubis, S. Li, M. N. Singleton, J. T. Verger, B. P. Markovitz, J. P. Burns, S. A. Chung, A. G. Randolph, and the Pediatric Acute Lung Injury and Sepsis Investigator’s (PALISI) Network. 2019. Growth and changing characteristics of pediatric intensive care 2001–2016. Critical Care Medicine 47(8):1135-1142.
Howell, D. L., K. C. Ward, H. D. Austin, J. L. Young, and W. G. Woods. 2007. Access to pediatric cancer care by age, race, and diagnosis, and outcomes of cancer treatment in pediatric and adolescent patients in the state of Georgia. Journal of Clinical Oncology 25(29):4610-4615.
HRSA (Health Resources and Services Administration). 2022. Children and youth with special health care needs: NSCH data brief June 2022. https://mchb.hrsa.gov/sites/default/files/mchb/programs-impact/nsch-data-brief-children-youth-special-health-care-needs.pdf (accessed December 22, 2022).
Hsiang, W. R., A. Lukasiewicz, M. Gentry, C.-Y. Kim, M. P. Leslie, R. Pelker, H. P. Forman, and D. H. Wiznia. 2019. Medicaid patients have greater difficulty scheduling health care appointments compared with private insurance patients: A meta-analysis. INQUIRY: The Journal of Health Care Organization, Provision, and Financing 56:0046958019838118.
Hsueh, L., A. T. Hirsh, G. Maupome, and J. C. Stewart. 2021. Patient–provider language concordance and health outcomes: A systematic review, evidence map, and research agenda. Medical Care Research and Review 78(1):3-23.
Hudgins, J. D., M. I. Neuman, M. C. Monuteaux, J. Porter, and K. A. Nelson. 2021. Provision of guideline-based pediatric asthma care in U.S. emergency departments. Pediatric Emergency Care 37(10):507-512.
Jaramillo, J., E. Snyder, J. L. Dunlap, R. Wright, F. Mendoza, and M. Bruzoni. 2016. The Hispanic clinic for pediatric surgery: A model to improve parent–provider communication for Hispanic pediatric surgery patients. Journal of Pediatric Surgery 51(4):670-674.
Kalb, L. G., E. K. Stapp, E. D. Ballard, C. Holingue, A. Keefer, and A. Riley. 2019. Trends in psychiatric emergency department visits among youth and young adults in the U.S. Pediatrics 143(4):e20182192.
Kaul, S., A. C. Kirchhoff, N. E. Morden, C. S. Vogeli, and E. G. Campbell. 2015. Physician response to patient request for unnecessary care. American Journal of Managed Care 21(11):823-832.
Kern-Goldberger, A. S., N. M. Money, J. S. Gerber, and C. P. Bonafide. 2021. Inpatient subspecialty consultations: A new target for high-value pediatric hospital care? Hospital Pediatrics https://doi.org/10.1542/hpeds.2021-006165.
Kern-Goldberger, A. S., E. M. Dalton, I. R. Rasooly, M. Congdon, D. Gunturi, L. Wu, Y. Li, J. S. Gerber, and C. P. Bonafide. 2023. Factors associated with inpatient subspecialty consultation patterns among pediatric hospitalists. JAMA 6(3):e232648.
Kessler, R. C., P. Berglund, O. Demler, R. Jin, K. R. Merikangas, and E. E. Walters. 2005. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry 62(6):593-602.
Khan, M. S., W. Zhang, R. A. Taylor, E. D. McKenzie, G. B. Mallory, M. G. Schecter, D. L. S. Morales, J. S. Heinle, and I. Adachi. 2015. Survival in pediatric lung transplantation: The effect of center volume and expertise. The Journal of Heart and Lung Transplantation 34(8):1073-1081.
Krugman, S. D., and D. Rauch. 2022. An unexpected shortage: Hospital beds for children. https://www.healthaffairs.org/do/10.1377/forefront.20220615.615247 (accessed April 13, 2023).
Kunin, M., E. Turbitt, S. A. Gafforini, L. A. Sanci, N. A. Spike, and G. L. Freed. 2018. General practitioner referrals to paediatric specialist outpatient clinics: Referral goals and parental influence. Journal of Primary Health Care 10(1):76-80.
Kuriyan, A. B., W. E. Pelham, B. S. Molina, D. A. Waschbusch, E. M. Gnagy, M. H. Sibley, D. E. Babinski, C. Walther, J. Cheong, and J. Yu. 2013. Young adult educational and vocational outcomes of children diagnosed with ADHD. Journal of Abnormal Child Psychology 41:27-41.
Kyu, H. H., C. Pinho, J. A. Wagner, J. C. Brown, A. Bertozzi-Villa, F. J. Charlson, L. E. Coffeng, L. Dandona, H. E. Erskine, and A. J. Ferrari. 2016. Global and national burden of diseases and injuries among children and adolescents between 1990 and 2013: Findings from the Global Burden of Disease 2013 study. JAMA Pediatrics 170(3):267-287.
Lange, S. J., L. Kompaniyets, D. S. Freedman, E. M. Kraus, R. Porter, H. M. Blanck, and A. B. Goodman. 2021. Longitudinal trends in body mass index before and during the CO-VID-19 pandemic among persons aged 2–19 years—United States, 2018–2020. Morbidity and Mortality Weekly Reports 70(37):1278-1283.
Larson, K., E. A. Gottschlich, W. L. Cull, and L. M. Olson. 2021. High-deductible health plans for U.S. children: Trends, health service use, and financial barriers to care. Academic Pediatrics 21(8):1345-1354.
Lasswell, S. M., W. D. Barfield, R. W. Rochat, and L. Blackmon. 2010. Perinatal regionalization for very low-birth-weight and very preterm infants: A meta-analysis. JAMA 304(9):992-1000.
Lawrence, J. M., J. Divers, S. Isom, S. Saydah, G. Imperatore, C. Pihoker, S. M. Marcovina, E. J. Mayer-Davis, R. F. Hamman, L. Dolan, D. Dabelea, D. J. Pettitt, and A. D. Liese for the SEARCH for Diabetes in Youth Study Group. 2021. Trends in prevalence of type 1 and type 2 diabetes in children and adolescents in the U.S., 2001–2017. Journal of the American Medical Association 326(8):717-727.
Lebrun-Harris, L. A., M. A. McManus, S. M. Ilango, M. Cyr, S. B. McLellan, M. Y. Mann, and P. H. White. 2018. Transition planning among U.S. youth with and without special health care needs. Pediatrics 142(4):e20180194.
Lebrun-Harris, L. A., R. M. Ghandour, M. D. Kogan, and M. D. Warren. 2022. Five-year trends in U.S. children’s health and well-being, 2016-2020. JAMA Pediatrics 176(7):e220056. https://doi.org/10.1001/jamapediatrics.2022.0056.
Leiba, A., B. Fishman, G. Twig, D. Gilad, E. Derazne, A. Shamiss, T. Shohat, O. Ron, and E. Grossman. 2019. Association of adolescent hypertension with future end-stage renal disease. JAMA Internal Medicine 179(4):517-523.
Leibowitz, A., W. G. Manning, Jr., E. B. Keeler, N. Duan, K. N. Lohr, and J. P. Newhouse. 1985. Effect of cost-sharing on the use of medical services by children: Interim results from a randomized controlled trial. Pediatrics 75(5):942-951.
Little, P., M. Dorward, G. Warner, K. Stephens, J. Senior, and M. Moore. 2004. Importance of patient pressure and perceived pressure and perceived medical need for investigations, referral, and prescribing in primary care: Nested observational study. BMJ 328(7437):444.
Loe, I. M., and H. M. Feldman. 2007. Academic and educational outcomes of children with ADHD. Journal of Pediatric Psychology 32(6):643-654.
Lonetti, A., A. Pession, and R. Masetti. 2019. Targeted therapies for pediatric AML: Gaps and perspective. Frontiers in Pediatrics 7:463.
Lor, M., and G. A. Martinez. 2020. Scoping review: Definitions and outcomes of patient–provider language concordance in healthcare. Patient Education and Counseling 103(10):1883-1901.
MACPAC (Medicaid and CHIP Payment and Access Commission). 2017. State Medicaid fee-for-service physician payment policies. https://www.macpac.gov/publication/states-medicaid-fee-for-service-physician-payment-policies (accessed January 4, 2023).
MACPAC. 2020. Medicaid payment policy for out-of-state hospital services. https://www.macpac.gov/wp-content/uploads/2020/01/Medicaid-Payment-Policy-for-Out-of-State-Hospital-Services.pdf (accessed July 12, 2023).
MACPAC. 2021. Physician acceptance of new Medicaid patients: Findings from the National Electronic Health Records Survey. https://www.macpac.gov/wp-content/uploads/2021/06/Physician-Acceptance-of-New-Medicaid-Patients-Findings-from-the-National-Electronic-Health-Records-Survey.pdf (accessed April 13, 2023).
Maenner, M. J., Z. Warren, A. R. Williams, E. Amoakohene, A. V. Bakian, D. A. Bilder, M. S. Durkin, R. T. Fitzgerald, S. M. Furnier, M. M. Hughes, C. M. Ladd-Acosta, D. McArthur, E. T. Pas, A. Salinas, A. Vehorn, S. Williams, A. Esler, A. Grzybowski, J. Hall-Lande, R. H. N. Nguyen, K. Pierce, W. Zahorodny, A. Hudson, L. Hallas, K. C. Mancilla, M. Patrick, J. Shenouda, K. Sidwell, M. DiRienzo, J. Gutierrez, M. H. Spivey, M. Lopez, S. Pettygrove, Y. D. Schwenk, A. Washington, and K. A. Shaw. 2023. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2020. Morbidity and Mortality Weekly Report 72(2):1-14.
Manetto, N., J. Greenberg, and C. Reddy. 2020. Policies to enhance care of out-of-state pediatric Medicaid beneficiaries. In Health Affairs Blog. https://www.healthaffairs.org/content/forefront/policies-enhance-care-out-of-state-pediatric-medicaid-beneficiaries (accessed July 12, 2023).
Marcin, J. P., U. Shaikh, and R. H. Steinhorn. 2016. Addressing health disparities in rural communities using telehealth. Pediatric Research 79(1):169-176.
Mayer, M. L. 2006. Are we there yet? Distance to care and relative supply among pediatric medical subspecialties. Pediatrics 118(6):2313-2321.
McCulloh, R. J., S. Smitherman, S. Adelsky, M. Congdon, J. Librizzi, K. Koehn, and B. Alverson. 2012. Hospitalist and nonhospitalist adherence to evidence-based quality metrics for bronchiolitis. Hospital Pediatrics 2(1):19-25.
McManus, M., P. White, A. Schmidt, M. Barr, C. Langer, K. Barger, and A. Ware. 2020. Health care gap affects 20% of United States population: Transition from pediatric to adult health care. Health Policy OPEN 1:100007.
McPherson, M., P. Arango, H. Fox, C. Lauver, M. McManus, P. W. Newacheck, J. M. Perrin, J. P. Shonkoff, and B. Strickland. 1998. A new definition of children with special health care needs. Pediatrics 102(1):137-139.
Merikangas, K. R., M. E. Calkins, M. Burstein, J. He, R. Chiavacci, T. Lateef, K. Ruparel, R. C. Gur, T. Lehner, H. Hakonarson, and R. E. Gur. 2015. Comorbidity of physician and mental disorders in the Neurodevelopmental Genomics Cohort Study. Pediatrics 135(4):e927-e938.
Meyer, H. 2021. Families with sick kids on Medicaid seek easier access to out-of-state hospitals. NPR.
Michelson, K. A., J. D. Hudgins, M. C. Monuteaux, R. G. Bachur, and J. A. Finkelstein. 2018. Cardiac arrest survival in pediatric and general emergency departments. Pediatrics 141(2):e20172741. https://doi.org/10.1542/peds.2017-2741.
Ming, D. Y., K. A. Jones, M. J. White, J. E. Pritchard, B. G. Hammill, C. Bush, G. L. Jackson, and S. R. Raman. 2022. Healthcare utilization for Medicaid-insured children with medical complexity: Differences by sociodemographic characteristics. Maternal and Child Health Journal 26:2407-2418.
Mosquera, R. A., E. B. C. Avritscher, C. Pedroza, C. S. Bell, C. L. Samuels, T. S. Harris, J. C. Eapen, A. Yadav, M. Poe, R. L. Parlar-Chun, J. Berry, and J. E. Tyson. 2021. Hospital consultation from outpatient clinicians for medically complex children: A randomized clinical trial. JAMA Pediatrics 175(1):e205026.
Müller, H., S. Laier, and A. Bechdolf. 2014. Evidence-based psychotherapy for the prevention and treatment of first-episode psychosis. European Archives of Psychiatry and Clinical Neuroscience 264:17-25.
Muskens, J. B., F. P. Velders, and W. G. Staal. 2017. Medical comorbidities in children and adolescents with autism spectrum disorders and attention deficit hyperactivity disorders: A systematic review. European Child & Adolescent Psychiatry 26(9):1093-1103.
Myers, S. R., C. C. Branas, B. French, M. L. Nance, and B. G. Carr. 2019. A national analysis of pediatric trauma care utilization and outcomes in the United States. Pediatric Emergency Care 35(1):1-7.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015. Investing in the health and well-being of young adults. Washington, DC: The National Academies Press.
NASEM. 2023. Addressing the long-term effects of the COVID-19 pandemic on children and families. Edited by T. R. Coker, J. A. Gootman, and E. P. Backes. Washington, DC: The National Academies Press.
Nguengang Wakap, S., D. M. Lambert, A. Olry, C. Rodwell, C. Gueydan, V. Lanneau, D. Murphy, Y. Le Cam, and A. Rath. 2020. Estimating cumulative point prevalence of rare diseases: Analysis of the Orphanet database. European Journal of Human Genetics 28(2):165-173.
NRC and IOM (National Research Council and Institute of Medicine). 2004. Children’s health, the nation’s wealth: Assessing and improving child health. Washington, DC: The National Academies Press.
Oh, S. H., I. S. Jeong, D. Y. Kim, J. M. Namgoong, W. K. Jhang, S. J. Park, D. H. Jung, D. B. Moon, G. W. Song, G. C. Park, T. Y. Ha, C. S. Ahn, K. H. Kim, S. Hwang, S. G. Lee, and K. M. Kim. 2022. Recent improvement in survival outcomes and reappraisal of prognostic factors in pediatric living donor liver transplantation. Liver Transplantation 28(6):1011-1023.
Perreira, K. M., and J. M. Pedroza. 2019. Policies of exclusion: Implications for the health of immigrants and their children. Annual Review of Public Health 40:147-166.
Pho, K. 2012. Why more primary care doctors are referring patients to specialists. https://www.kevinmd.com/2012/01/primary-care-doctors-referring-patients-specialists.html (accessed April 20, 2023).
Pollitz, K. 2022. Network adequacy standards and enforcement. https://www.kff.org/health-reform/issue-brief/network-adequacy-standards-and-enforcement/ (accessed July 10, 2023).
Price-Feeney, M., A. E. Green, and S. Dorison. 2020. Understanding the mental health of transgender and nonbinary youth. Journal of Adolescent Health 66(6):684-690.
Rankin, J., L. Matthews, S. Cobley, A. Han, R. Sanders, H. D. Wiltshire, and J. S. Baker. 2016. Psychological consequences of childhood obesity: Psychiatric comorbidity and prevention. Adolescent Health, Medicine and Therapeutics 7:125-146.
Ray, K. N., L. E. Ashcraft, J. M. Kahn, A. Mehrotra, and E. Miller. 2016. Family perspectives on high-quality pediatric subspecialty referrals. Academic Pediatrics 16(6):594-600.
Reardon, J. L., P. Lembeck, T. Murray, and P. Weiss. 2020. Mental health in the pediatric subspecialties: Physicians’ beliefs and confidence in providing care. Academic Pediatrics 20(7):E53-E54.
Rimes, K. A., N. Goodship, G. Ussher, D. Baker, and E. West. 2019. Non-binary and binary transgender youth: Comparison of mental health, self-harm, suicidality, substance use and victimization experiences. International Journal of Transgenderism 20(2-3):230-240.
Rimsza, M. E., H. S. Ruch-Ross, C. J. Clemens, W. B. Moskowitz, and H. J. Mulvey. 2018. Workforce trends and analysis of selected pediatric subspecialties in the United States. Academic Pediatrics 18(7):805-812.
Ringberg, U., N. Fleten, and O. H. Førde. 2014. Examining the variation in GPs’ referral practice: A cross-sectional study of GPs’ reasons for referral. British Journal of General Practice 64(624):e426-e433.
Rodgers, C. R. R., M. W. Flores, O. Bassey, J. M. Augenblick, and B. Le Cook. 2022. Racial/ethnic trends in children’s mental health care access and expenditures from 2010–2017: Disparities remain despite sweeping policy reform. Journal of the American Academy of Child & Adolescent Psychiatry 61(7):915-925.
Rodriguez Santana, I., A. Mason, N. Gutacker, P. Kasteridis, R. Santos, and N. Rice. 2023. Need, demand, supply in health care: Working definitions, and their implications for defining access. Health Economics, Policy and Law 18(1):1-13.
Romano, I., C. Buchan, L. Baiocco-Romano, and M. A. Ferro. 2021. Physical–mental multimorbidity in children and youth: A scoping review. BMJ Open 11:e043124.
Rubinstein, T. B., A. M. Davis, M. Rodriguez, and A. M. Knight. 2018. Addressing mental health in pediatric rheumatology. Current Treatment Options in Rheumatology 4:55-72.
Sanyaolu, A., C. Okorie, X. Qi, J. Locke, and S. Rehman. 2019. Child and adolescent obesity in the United States: A public health concern. Global Pediatric Health https://doi.org/10.1177/2333794X19891305.
Schimmelmann, B. G., P. Conus, S. Cotton, P. D. McGorry, and M. Lambert. 2007. Pretreatment, baseline, and outcome differences between early-onset and adult-onset psychosis in an epidemiological cohort of 636 first-episode patients. Schizophrenia Research 95(1-3):1-8.
Schuster, M. A. 2015. Measuring quality of pediatric care: Where we’ve been and where we’re going. Pediatrics 135(4):748-751.
Shear, K., R. Jin, A. M. Ruscio, E. E. Walters, and R. C. Kessler. 2006. Prevalence and correlates of estimated DSM-IV child and adult separation anxiety disorder in the national comorbidity survey replication. American Journal of Psychiatry 163(6):1074-1083.
Siegel, D. A., L. C. Richardson, S. J. Henley, R. J. Wilson, N. F. Dowling, H. K. Weir, E. W. Tai, and N. Buchanan Lunsford. 2020. Pediatric cancer mortality and survival in the United States, 2001–2016. Cancer 126(19):4379-4389.
Siffel, C., M. DerSarkissian, K. Kponee-Shovein, W. Spalding, Y. M. Gu, M. Cheng, and M. S. Duh. 2020. Suicidal ideation and attempts in the United States of America among stimulant-treated, non-stimulant-treated, and untreated patients with a diagnosis of attention-deficit/hyperactivity disorder. Journal of Affective Disorders 266:109-119.
Skinner, A. C., and M. L. Mayer. 2007. Effects of insurance status on children’s access to specialty care: A systematic review of the literature. BMC Health Services Research 7(1):194.
Slocum, T. A., R. Detrich, S. M. Wilczynski, T. D. Spencer, T. Lewis, and K. Wolfe. 2014. The evidence-based practice of applied behavior analysis. The Behavior Analyst 37:41-56.
St. Amant, H. G., S. M. Schrager, C. Peña-Ricardo, M. E. Williams, and D. L. Vanderbilt. 2018. Language barriers impact access to services for children with autism spectrum disorders. Journal of Autism and Developmental Disorders 48(2):333-340.
Stark, A. R., D. M. Pursley, L. Papile, E. C. Eichenwald, C. T. Hankins, R. K. Buck, T. J. Wallace, P. G. Bondurant, and N. E Faster. 2023. Standards for levels of neonatal care: II, III, and IV. Pediatrics 151(6):e2023061957.
Stephens, M. R., A. S. Murthy, and P. J. McMahon. 2019. Wait times, health care touchpoints, and nonattendance in an academic pediatric dermatology clinic. Pediatric Dermatology 36(6):893-897.
Stierman, B., J. Afful, M. D. Carroll, T. Chen, O. Davy, S. Fink, C. D. Fryar, Q. Gu, C. M. Hales, J. P. Hughes, Y. Ostchega, R. J. Storandt, and L. J. Akinbami. 2021. National Health and Nutrition Examination Survey 2017–March 2020 prepandemic data files—Development of files and prevalence estimates for selected health outcomes. National Health Statistics Reports No. 158.
Stroul, B. A., and R. M. Friedman. 1986. A system of care for severely emotionally disturbed children and youth. https://www.ojp.gov/pdffiles1/Digitization/125081NCJRS.pdf (accessed May 1, 2023).
Sump, C. A., T. L. Marshall, A. J. Ipsaro, S. J. Patel, D. C. Warner, P. W. Brady, and P. A. Hagedorn. 2020. Uncertain diagnoses in a children’s hospital: Patient characteristics and outcomes. Diagnosis 8(3):353-357.
Takeshita, J., S. Wang, A. W. Loren, N. Mitra, J. Shults, D. B. Sin, and D. L. Sawinski. 2020. Association of racial/ethnic and gender concordance between patients and physicians with patient experience ratings. JAMA Open Network 3(11):2024583.
Timbie, J. W., A. M. Kranz, A. Mahmud, and C. L. Damberg. 2019. Specialty care access for Medicaid enrollees in expansion states. American Journal of Managed Care 25(3):e83-e87.
Tolbert, J., P. Drake, and A. Damico. 2022. Key facts about the uninsured population. https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/#:~:text=1%20Nonelderly%20adults%20are%20more%20likely%20to%20be,risk%20of%20being%20uninsured%20than%20White%20people.%20 (accessed May 2, 2023).
Turner, A., T. Ricketts, and L. K. Leslie. 2020. Comparison of number and geographic distribution of pediatric subspecialists and patient proximity to specialized care in the U.S. between 2003 and 2019. JAMA Pediatrics 174(9):852-860.
Turner, A., T. Ricketts, and L. K. Leslie. 2022. Revisiting complexities in the pediatric subspecialty workforce. JAMA Pediatrics 176(1):98-99.
U.S. Census Bureau. 2020. The next generation—percent change among the under 18 population: 2010 to 2019. https://www.census.gov/library/visualizations/2020/comm/map-popest-under-18.html (accessed April 21, 2023).
Valderas, J. M., B. Starfield, C. B. Forrest, L. Rajmil, M. Roland, and B. Sibbald. 2009. Routine care provided by specialists to children and adolescents in the United States (2002–2006). BMC Health Services Research 9(1):221.
Van Cleave, J., S. L. Gortmaker, and J. M. Perrin. 2010. Dynamics of obesity and chronic health conditions among children and youth. Journal of the American Medical Association 303(7):623-630.
Vernacchio, L., J. M. Muto, G. Young, and W. Risko. 2012. Ambulatory subspecialty visits in a large pediatric primary care network. Health Services Research 47(4):1755-1769.
Visser, S. N., M. L. Danielson, R. H. Bitsko, J. R. Holbrook, M. D. Kogan, R. M. Ghandour, R. Perou, and S. J. Blumberg. 2014. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. Journal of the American Academy of Child & Adolescent Psychiatry 53(1):34-46.e2.
VonAchen, P., M. M. Davis, J. Cartland, A. D’Arco, and K. Kan. 2022. Closure of licensed pediatric beds in health care markets within Illinois. Academic Pediatrics 22(3):431-439.
White, P. H., W. C. Cooley, Transitions Clinical Report Authoring Group, American Academy of Pediatrics, American Academy of Family Physicians, American College of Physicians, A. D. A. Boudreau, M. Cyr, B. E. Davis, D. E. Dreyfus, E. Forlenza, A. Friedland, C. Greenlee, M. Mann, M. McManus, A. I. Meleis, and L. Pickler. 2018. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics 142(5):e20182587.
White, P., A. Schmidt, J. Shorr, S. Ilango, D. Beck, and M. McManus. 2020. Six Core Elements of Health Care Transition 3.0. https://www.gottransition.org/6ce/?integrating-full-package (accessed April 28, 2023).
Whitney, D. G., and M. D. Peterson. 2019. U.S. national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediatrics 173(4):389-391.
Wise, P. H. 2007. The future pediatrician: The challenge of chronic illness. The Journal of Pediatrics 151(5 Suppl):S6-S10.
Witt, W. P., A. J. Weiss, and A. Elixhauser. 2014. Statistical Brief #187: Overview of hospital stays for children in the United States, 2012. https://www.hcup-us.ahrq.gov/reports/stat-briefs/sb187-Hospital-Stays-Children-2012.jsp (accessed April 20, 2023).
Wojcik, M. H., M. Bresnahan, M. C. del Rosario, M. M. Ojeda, A. Kritzer, and Y. S. Fraiman. 2023. Rare diseases, common barriers: Disparities in pediatric clinical genetics outcomes. Pediatric Research 93(1):110-117.
Wolfe, M. K., N. C. McDonald, and G. M. Holmes. 2020. Transportation barriers to health care in the United States: Findings from the National Health Interview Survey, 1997–2017. American Journal of Public Health 110(6):815-822.
Woolf, S. H., E. R. Wolf, and F. P. Rivara. 2023. The new crisis of increasing all-cause mortality in U.S. children and adults. Journal of the American Medical Association 329(12):975-976.
Woolford, S. J., M. Sidell, X. Li, V. Else, D. R. Young, K. Resnicow, and C. Koebnick. 2021. Changes in body mass index among children and adolescents during the COVID-19 pandemic. Journal of the American Medical Association 326(14):1434-1436.
Xu, W. Y., Y. Li, C. Song, S. Bose-Brill, and S. M. Retchin. 2022. Out-of-network care in commercially insured pediatric patients according to medical complexity. Medical Care 60(5):375-380.
Yang, L., C. G. Magnussen, L. Yang, P. Bovet, and B. Xi. 2020. Elevated blood pressure in childhood or adolescence and cardiovascular outcomes in adulthood: A systematic review. Hypertension 75:948-955.
Yang, K. G., M. W. Flores, N. J. Carson, and B. Le Cook. 2022. Racial and ethnic disparities in childhood ADHD treatment access and utilization: Results from a national study. Psychiatric Services https://doi.org/10.1176/appi.ps.202100578.
Yard, E., L. Radhakrishnan, M. F. Ballesteros, M. Sheppard, A. Gates, Z. Stein, K. Hartnett, A. Kite-Powell, L. Rodgers, J. Adjemian, D. C. Ehlman, K. Holland, N. Idaikkadar, A. IveyStephenson, P. Martinez, R. Law, and D. M. Stone. 2021. Emergency department visits for suspected suicide attempts among persons aged 12–25 years before and during the COVID-19 pandemic—United States, January 2019–May 2021. Morbidity and Mortality Weekly Report 70(24):888-894.
Yohe, M. E., C. M. Heske, E. Stewart, P. C. Adamson, N. Ahmed, C. R. Antonescu, E. Chen, N. Collins, A. Ehrlich, R. L. Galindo, B. E. Gryder, H. Hahn, S. Hammond, M. E. Hatley, D. S. Hawkins, M. N. Hayes, A. Hayes-Jordan, L. J. Helman, S. Hettmer, M. S. Ignatius, C. Keller, J. Khan, D. G. Kirsch, C. M. Linardic, P. J. Lupo, R. Rota, J. F. Shern, J. Shipley, S. Sindiri, S. J. Tapscott, C. R. Vakoc, L. H. Wexler, and D. M. Langenau. 2019. Insights into pediatric rhabdomyosarcoma research: Challenges and goals. Pediatric Blood & Cancer 66(10):e27869.
Yu, S. M., R. M. Nyman, M. D. Kogan, Z. J. Huang, and R. H. Schwalberg. 2004. Parent’s language of interview and access to care for children with special health care needs. Ambulatory Pediatrics 4(2):181-187.
Zablotsky, B., L. I. Black, M. J. Maenner, L. A. Schieve, M. L. Danielson, R. H. Bitsko, S. J. Blumberg, M. D. Kogan, and C. A. Boyle. 2019. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics 144(4):e20190811.
Zima, B. T., R. Bussing, L. Tang, L. Zhang, S. Ettner, T. R. Belin, and K. B. Wells. 2010. Quality of care for childhood attention-deficit/hyperactivity disorder in a managed care Medicaid program. Journal of the American Academy of Child & Adolescent Psychiatry 49(12):1225-1237. e1-e11.
Zima, B. T., J. Rodean, M. Hall, N. S. Bardach, T. R. Coker, and J. G. Berry. 2016. Psychiatric disorders and trends in resource use in pediatric hospitals. Pediatrics 138(5):e20160909.
Zima, B. T., J. B. Edgcomb, J. Rodean, S. D. Cochran, C. A. Harle, J. Pathak, C.-H. Tseng, and R. Bussing. 2022. Use of acute mental health care in U.S. children’s hospitals before and after statewide COVID-19 school closure orders. Psychiatric Services 73(11):1202-1209.