
3
Understanding Patients with Traumatic Brain Injury
One of the essential features of quality health care is patient- or person-centeredness (IOM, 2001), a key feature of the optimized traumatic brain injury (TBI) system described in Chapter 8. To achieve a patient-centered system, it is necessary first to understand those who experience TBI: their journeys and the multiple dimensions—biological, psychological,
social, and ecological (contextual)—that feed into and help shape their experiences; the complex, dynamic interactions among these dimensions; and the associated inequities in access to care and in long-term outcomes.
THE PATIENT JOURNEY AND TBI PREVENTION, CARE, AND RECOVERY
The pathway toward addressing TBI starts with prevention (see Chapter 4). Although not the focus of this report, the committee emphasizes that the identification and implementation of effective strategies for reducing the numbers and severity of brain injuries that occur is the most effective way to reduce the burden of TBI.
Despite efforts at prevention, however, brain injuries will inevitably occur. Figure 3-1 depicts an overarching and generalized view of a person’s pathway from recognition of a potential injury through care; recovery; and return to community, work, and school environments. TBI is a complex condition with many unknowns. Some people completely recover over time, while in other people TBI becomes a chronic and often disabling disease.
The care journey for a person who experiences a TBI can involve different elements and care providers depending on the nature of the injury and the recovery process. Acute and longer-term elements may include the following:
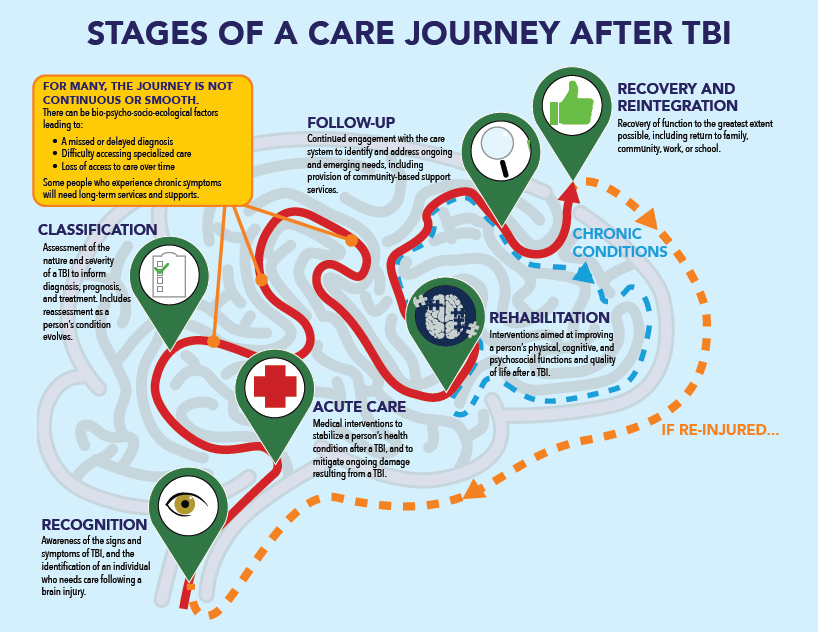
SOURCE: Graphic developed by Masai Interactive.
- Recognition and provision of early care or aid: In the context of a sports-related TBI, an athletic trainer or team physician on the field may make an initial assessment to guide a return-to-play decision. In the case of an event such as a vehicle crash, emergency aid may need to be provided at the scene until emergency medical services (EMS) personnel arrive. In a military context, a soldier or medic on the battlefield may provide early aid to an injured comrade.
- Prehospital EMS care to stabilize vital functions: In the civilian context, EMS personnel may be called on to stabilize the vital functions of a person who has experienced a TBI and transport them to a higher level of medical care, such as a local hospital emergency department (ED) or a trauma center. In the military trauma system, care may be provided by a forward surgical team or in a combat hospital. A person who experiences a suspected TBI that appears to be minor may receive no hospital-based care beyond an initial evaluation, perhaps coupled with guidance to rest and to seek follow-up should symptoms develop.
- Acute hospital care to address injuries: For someone who has experienced a TBI or concomitant injuries of a serious nature, this stage of care includes medical interventions provided in a hospital ED or intensive care unit, aimed at saving the person’s life and preventing further negative consequences of the injury. In the military, a person may be evacuated to a regional or U.S.-based military hospital able to provide more advanced levels of care.
- Rehabilitation and longer-term follow-up to minimize disability: Rehabilitation and longer-term follow-up can take many pathways and forms, depending on the nature of the injuries sustained. Rehabilitation interventions aim to improve a person’s function and quality of life after TBI. Delivery of this care may occur in both military and civilian and both inpatient and outpatient settings. In the military, post-acute rehabilitation therapies are provided through the Department of Veterans Affairs (VA).
- Recovery and reintegration into society and the workforce to the extent possible: The goal after TBI is for the person to return to independent living in their home or community and to work or school to the extent possible. A person who experiences a less serious TBI may recover fully, while someone who experiences a more severe injury may deal with ongoing, long-term symptoms and impairments, including a need to receive continued follow-up and rehabilitation care, as well as community-based patient and caregiver support services. In some cases, a person may experience another TBI, potentially starting the journey again.
A FRAMEWORK FOR UNDERSTANDING TBI: THE BIO-PSYCHO-SOCIO-ECOLOGICAL MODEL
Understanding the medical course of TBI is important, but to fully address effective TBI prevention and care requires a framework that is broader than a medical model of injury, given the multiple personal and social/environmental factors that affect the experience of and recovery from such an injury. Models that recognize the interactions among such factors have been applied to a variety of prevention and disease contexts and are required to understand TBI.
The Unique Array of Factors Brought by Each Individual to an Injury
Experienced clinicians, patients and patient advocates, and rehabilitation specialists know that a variety of preexisting and current attributes of the patient, including physiologi-
cal, interpersonal, and other critical factors, as well as family and community relationships, play key roles in how significant a TBI will be for the patient. In many cases, the role played by these attributes in determining the trajectory of immediate recovery; rehabilitation; and long-term physical, emotional, intellectual, spiritual, and social outcomes is as important as the nature of the injury itself.
Biomedical Aspects of a TBI
Biomedical aspects of a TBI include the nature of the forces and stresses acting on a person’s brain, the potential occurrence of traumatic hemorrhage and swelling, and the existence of co-occurring injuries. A person’s own physiological responses to the injury are also important in the context of their genetics and endocrine, metabolic, and immune systems. As described in Chapter 2, a majority of TBIs result in what have been termed “mild” injuries with less severe damage to the brain and lesser threats to long-term cognitive, motor, sensory, social, and psychological functions. A smaller number of TBIs have more consequential traumatic impacts and far-ranging effects.
Psychosocial and Ecological Aspects of a TBI
The role of factors beyond the nature of the physical injury lies within a construct that examines the “whole person” in relation to intersecting domains of physical and nonphysical personal characteristics, interpersonal family and immediate community relationships, and socioeconomic factors within the individual’s living environment. This construct was first formally described by Engel as the biopsychosocial model (Engel, 1977). Systems theory, including related socioecological models, similarly view health conditions through a framework that considers interactions among individual characteristics, interpersonal relationships, community settings, and wider societal policies, applying the model to prevention, public health, and clinical settings (see, e.g., Karriker-Jaffe et al., 2020; Register-Mihalik and Callahan, 2020; van Erp et al., 2019, and the Centers for Disease Control and Prevention’s [CDC’s] violence prevention efforts1). In the context of TBI, an expanded bio-psycho-socio-ecological (BPSE) model includes the wide and complex array of qualitative and quantitative elements of the living and inanimate network within which each human lives and flourishes. The ecological dimensions of TBI also encompass economic forces, recognizing that challenges in U.S. health care and social systems, such as a scarcity of rehabilitation venues and limited insurance coverage, can limit a person’s access to care.
TBIs are not the only illnesses or injuries whose management and outcomes of care are influenced by various elements of a BPSE model. Chronic pain, diabetes, asthma, cardiovascular disease, various cancers, stroke, and Alzheimer’s disease and other dementias are among the many chronic health conditions that share this range of influence. In fact, one could argue that no significant survivable injury, illness, or combat-related wound is free of the influence of BPSE factors. For all of these conditions, biological, psychological, social, and human ecological factors play significant roles in the patient’s degree of suffering, extent of functional capacity, and even length of survival, and must be assessed and addressed if these illnesses and injuries are to be managed optimally. Improvement in the patient’s condition depends on more than a short-term medical-surgical model of treatment, even in
___________________
1 See The Social-Ecological Model: A Framework for Prevention at https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html (accessed September 27, 2021).
the hands of the most talented clinicians employing the most advanced, state-of-the-art and science modalities.
The prism in Figure 3-2 represents these BPSE factors. The array of BPSE factors unique to each patient can “refract” that person’s trajectory after TBI, in some cases leading to outcomes that are better than initially anticipated and in some cases to outcomes that are worse. Collectively, these factors affect the process of recovery and the level of function ultimately achieved for an individual person. The BPSE construct is always present, but the balance of factors and their interactions can change over time for any one patient.
This multifactorial model of human health and well-being is increasingly being recognized as having a major effect at the population level. Direct clinical care may contribute only 20 percent of the overall well-being of a nation’s citizenry (Hood et al., 2016), with lifestyle and behavioral factors and social and physical determinants of health playing a more dominant role (NRC and IOM, 2013). Life expectancy, maternal–child health, and a variety of other objective measures of population health are strongly related to these factors, although no one factor plays a more dominant role than others in the U.S. population as a whole.
How the BPSE Framework Describes the Course of a Person’s Trajectory After TBI
A TBI can represent the start of a potentially lifelong experience with the long-term consequences of a brain injury, and one cannot predict with certainty at the time of the initial injury what the long-term effects of any one TBI might be for a given person. As reported by providers across the continuum of care, as well as patients and family members, the prism of the BPSE model plays an essential role in affecting outcomes and long-term function. An initial classification of a TBI in a range from less to more severe can be refracted into an array of outcomes, from very poor to very favorable. Illustrating this point, a person’s chances of immediate survival from the initial injury have been summarized by the comment, “Where you live actually can determine if you live.”2
Beyond immediate survival, people who live in rural communities or are injured in remote sites with austere resources for emergency response, evacuation to definitive care,
___________________
2 Robinson, J. 2021. TBI Care Gaps and Opportunities: Provider Perspectives on the Acute-Stage Continuum of Care. Panel discussion during virtual workshop for the Committee on Accelerating Progress in Traumatic Brain Injury Research and Care, March 18, 2021.
and access to intensive care treatment, as well as those who live in some urban communities where social determinants of health3 can affect well-being, are less likely to receive prompt, comprehensive, long-term care and rehabilitation after TBI relative to people without these impediments. Factors in American social and political life that have existed for the duration of the republic’s history and have contributed to institutional racism and stratification of educational, economic, employment, residential, and other opportunities have had a serious impact on the optimal management of TBI among disenfranchised groups, including people of color and Native Americans, the poor, and those living in rural areas.
How the Influence of the BPSE Prism and Engagement with an Effective Health Care System Affect a Person’s Experiences with TBI Across the Lifespan
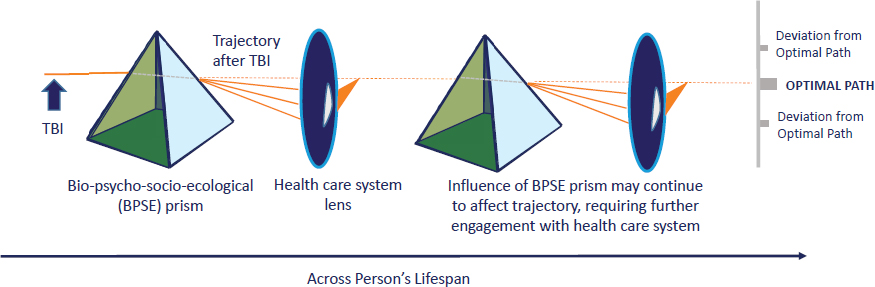
After a TBI has been sustained, an “ideal” or optimal treatment and rehabilitation pathway represents what is achievable for that person under the best of conditions. Any deviation from that ideal pathway results in an outcome that is less than optimal. The BPSE prism can steer a person’s recovery trajectory away from the ideal pathway, reflecting how the biological nature of the injury, psychological enablers or disablers, social influences (family, race, ethnicity, political, community, faith group, etc.), and the wider ecological environment all impact prospects for short-term survival and longer-term function and potential disability (see Figure 3-3).
In Figure 3-3, an effective health care system provides the lens that refocuses a person’s pathway back toward the best possible recovery trajectory. This health care lens encompasses diagnosis, treatment, rehabilitation, and reintegration. Ideally, the lens is able to recognize a deviation, identify requirements for achieving improved care and outcomes, and adjust a person’s course accordingly. A person with TBI may need to engage with the health care system multiple times over the course of their lifespan as post-TBI recovery evolves.
While BPSE factors play a role in all phases of TBI management and in the ultimate outcome for each patient, success in incorporating a full understanding of these factors into a patient’s clinical course and functional end state has been limited. Any fundamental advances in understanding TBI and in improving prevention, diagnosis, treatment, rehabilitation, and recovery will require integrating BPSE factors into the management scheme and research agenda for TBI, and engaging not only the medical system but also research, financial, educational, community support, and other key elements.
As explored in subsequent chapters, however, the current system for understanding and managing TBI does not function optimally for everyone. Challenges include the heterogeneity of TBI; the need for further research; gaps in the handoffs and transitions that occur along the continuum of care; the need for involvement of multiple types of care providers; the variety of data and payment systems involved in TBI care and research; and the diversity of organizations and communities in which people live, learn, work, and play.
INTERSECTION OF TBI WITH OTHER CONDITIONS
Confounding both acute and long-term diagnosis and management of TBI is the frequent coexistence of posttraumatic stress disorder (PTSD) and pain, especially chronic pain. This
___________________
3 Social determinants of health are “conditions in the places where people live, learn, work, and play that affect a wide range of health risks and outcomes,” including aspects of health care access and quality, education access and quality, social and community context, economic stability, and neighborhood and built environment (https://www.cdc.gov/socialdeterminants/about.html [accessed March 2, 2022]).
constellation, often termed the “polytrauma triad” (Cifu et al., 2013), occurs frequently in military service members who are injured or wounded in combat (Hoge et al., 2008). These comorbidities undoubtedly contribute as well to the difficulty of making an accurate diagnosis and designing optimal management for civilian victims of terrorist attacks, natural disasters, violent crimes, and motor vehicle crashes. Much work and controversy surround the attribution of symptoms of TBI and PTSD in the military setting. The principal symptoms of the two conditions overlap substantially in the absence of a penetrating head wound or severe crush injury, with headache alone being one of the few symptoms that accompany TBI but not PTSD. Large population studies have documented marked overlap between and among several comorbid conditions—notably TBI, PTSD, chronic pain, depression, and drug and alcohol abuse—in Veterans of military service (Cifu et al., 2013). Less severe forms of TBI, PTSD, and chronic pain are all clinical diagnoses largely, if not exclusively, reliant upon patient-reported subjective symptoms. This fact injects a level of uncertainty into these diagnoses and often complicates optimal management of the conditions, especially when adjudication of disability or health insurance benefits necessitates attribution for the symptoms involved.
Disparities and Inequities in TBI Outcomes and Access to Care
Equity and TBI
To realize a vision of optimal treatment for and recovery from TBI for all military and civilian populations, it will be necessary to understand and overcome inequities that exist in the current state of TBI treatment, support, and research. Broadly, health inequity arises from the confluence of (1) the interpersonal and systemic mechanisms that organize the distribution of power and resources differentially by individual and group identity, and (2) unequal allocation of power and resources, which is manifested in unequal social, economic, and environmental conditions—that is, the social determinants of health (NASEM, 2017).
Systemic inequities exist in the risk of sustaining a brain injury; access to timely and definitive treatment and recovery; and access to work, family, and community infrastructures that support long-term quality of life. As Chapter 2 documents, being male is associated with higher rates of TBI than is being female. Other studies have identified greater risks of expe-
riencing TBI associated with living in rural or high-poverty areas (Brown et al., 2019; Karb et al., 2016), or have identified higher rates of lifetime TBI among homeless or incarcerated populations, for example (Ferguson et al., 2012; Stubbs et al., 2020).
Inequities in outcomes after TBI have been associated with factors including race, ethnicity, biological sex, socioeconomic status, and others. Studies have documented inequities after TBI in access across the spectrum of care, from prehospital to rehabilitation, as evidenced by the examples that follow later in this chapter. A subset of patients with TBI experience a delayed recovery that can last for months or years after the injury, often with persistent functional impairments that can undermine their emotional health and quality of life (Haarbauer-Krupa et al., 2021). A host of factors have been linked to an increased likelihood of negative TBI-related outcomes, including the patient’s age, preinjury status (e.g., mental health, previous head injuries), presence of comorbidities, and propensity for resilience, as well as social and environmental factors related to gender and biological sex, race, ethnicity, socioeconomic status, insurance status, employment status, education status, and geographic location (Haarbauer-Krupa et al., 2021). The cognitive impairment that can result from TBI also presents barriers to self-advocacy and participation in and access to care (Dams-O’Connor et al., 2018).
All of these factors can interact to compound and exacerbate inequities in outcomes and access to care across different populations of TBI patients. However, although many of the causal factors leading to these disparities have been identified, those factors and the ways in which they interact are not yet fully understood. For example, Piatt (2021) identifies injury severity as the major contributing factor in a higher TBI mortality rate among Black relative to White children, with insurance status making only a small contribution. Lack of attention to social drivers—including structural racism, inequities, and bias—plays a role in poor access to quality TBI care and in particular, to rehabilitation and longer-term follow-up across the lifespan (Moore et al., 2019; NASEM, 2017). Access to rehabilitation services after acute care for a TBI is influenced as well by the individual patient’s characteristics, the behavior of the health care providers involved, processes of referral, and the broader context of the health care system (Foster and Tilse, 2003). Making progress toward mitigating the inequities detailed above will require considering all of these factors.
There are limited systematic, evidence-based, culturally resonant, and patient-centered interventions in the TBI realm. Research agendas need to address various types of inequities directly; help identify the affected populations; and, more important, build the evidence base for overcoming these inequities. Building this evidence base will require research of all types. Laboratory research is needed to ensure that animal and cell lines are representative of the diverse human populations suffering from TBI. Epidemiological research can identify populations suffering from inequities and evaluate approaches for overcoming them, while implementation and translational research can measure the impacts of intervention approaches. And policy research is needed to ensure that approaches found to be effective reach all populations affected by TBI.
Gender and Sex Differences in TBI Outcomes and Access to Care
Civilian Population
Although it has been established that women with TBI tend to experience worse outcomes than men, gender and sex differences in TBI outcomes have not yet been well characterized (Fabricius et al., 2020). This is largely because women have long been excluded from or greatly underrepresented in TBI preclinical studies and clinical trials, and many
studies that do include women are not stratified by sex (NINDS, 2017). Prevalence data are particularly lacking on TBI caused by intimate partner violence, often in the form of repetitive injuries and strangulation (NINDS, 2017). In 2019, PINK Concussions launched the Partner-Inflicted Brain Injury Task Force4 to foster collaboration between brain injury professionals and domestic violence/intimate partner violence professionals. In addition to the Pink Concussions effort, the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA) Consortium Intimate Partner Violence Working Group is a global collaboration working to collect data on this issue, advance understanding of the neurobehavioral and neurobiological effects, and characterize how TBIs related to intimate partner violence affect long-term health (Esopenko et al., 2021).
New avenues of research demonstrate differences in TBI by sex related to neuroanatomy, neural mechanisms, gonadal hormones, immunity response, and symptoms, underscoring the need for further research (NINDS, 2017). For instance, in women with TBI, hormonal factors can affect recovery outcomes (Haarbauer-Krupa et al., 2021). Social factors also shape the experiences of women who sustain a TBI or provide care for a TBI patient. A qualitative study exploring the lived experience of women with mild and moderate-to-severe TBIs found that their experiences during recovery and caregiving were highly shaped by their gender and gender expectations (Fabricius et al., 2020). In addition, there is evidence that, despite biological sex differences, extrinsic factors that, importantly, are modifiable by policy change or enhanced funding or both can improve outcomes for women, at least in the arena of sports-related concussion (Master et al., 2021).
Military Population
TBI has been called a signature injury of the wars in Iraq and Afghanistan (Tanielian et al., 2008). Although female service members tend to experience a lower rate of TBI compared with their male counterparts, they are more likely to report certain neurobehavioral symptoms after mild TBI (Bouldin et al., 2021; Gray et al., 2020; Haarbauer-Krupa et al., 2021; Kim et al., 2018). For instance, a study of Veterans of the conflicts in Afghanistan and Iraq (Operation Enduring Freedom and Operation Iraqi Freedom, respectively) who experienced TBI during deployment found that PTSD was the most commonly reported condition for both men and women, but that women were more likely to be diagnosed with depression, non-PTSD anxiety disorders, and PTSD with comorbid depression (Iverson et al., 2011). Other studies have yielded similar findings that female Veterans with mild TBI are likely to report neurobehavioral symptoms, are more frequently diagnosed with depression relative to their male counterparts, and are more likely to experience long-term postconcussion syndrome and to opt for non-VA health services (Cogan et al., 2020; Kim et al., 2018). It has been posited that female Veterans may experience more neurobehavioral symptoms in part because they are more likely to experience TBI secondary to interpersonal violence or sexual trauma, as well as because they are more likely to be screened for TBI than are men (Haarbauer-Krupa et al., 2021; Pugh et al., 2019). However, more research is needed on gender differences in the neurobehavioral sequelae of TBI, as female Veterans are not well represented in the existing literature. These issues are being explored in the Women Warriors Initiative, which was launched by the nonprofit Wounded Warrior Project.5
___________________
4 More information about the PINK Concussions Partner-Inflicted Brain Injury Task Force is available at https://www.pinkconcussions.com/violence (accessed August 3, 2021).
5 More information about the Women Warriors Initiative is available at https://www.woundedwarriorproject.org/media/tt0ftq4a/wwp-women-warriors-initiative-report-2021.pdf (accessed August 3, 2021).
Age Differences in TBI Outcomes and Access to Care
Children
Individual outcomes among children who experience TBI are shaped by a range of variables, including the type of injury, parenting style, intellectual ability, and socioeconomic factors (Haarbauer-Krupa et al., 2021). One study found higher lifetime prevalence of TBI among U.S. children in states with higher rates of private insurance and insurance adequacy, suggesting that children with less access to care are undercounted in TBI prevalence statistics (Haarbauer-Krupa et al., 2018). The authors also found a significant amount of variability in treatments for pediatric TBI. The experience of TBI can change the social and emotional life of adolescents; for instance, they may need to create new identities for themselves if they can no longer participate in athletics.6 Coordination between health systems and school systems is critical to ensuring that children continue to meet educational requirements during the TBI recovery process. However, parents of TBI patients are often overwhelmed and do not know how to help their children, as that information may not be readily available and may be difficult for parents to find (Haarbauer-Krupa et al., 2017).
Older Adults
Older adults (generally aged 65 and above) experience the highest rates of TBI-related hospitalization and death, as well as poor functional outcomes (Dams-O’Connor et al., 2013a). Older adults account for 10 percent of all patients with TBI, but 50 percent of deaths attributed to TBI (Stippler et al., 2012). An analysis of TBI trends in United States between 2007 and 2010 found that trauma center admissions increased by about 20–25 percent among adults aged ≥75 compared with the general population (Dams-O’Connor et al., 2013a). During that period, adults aged ≥65 with TBI tended to be White females with severe fall-related injuries. Compared with their younger adult counterparts, older adults tended to require more in-hospital procedures, longer hospital stays, and continued medical care. Older age also increased the likelihood of death in the hospital. Other studies have found that older compared with younger TBI patients tend to have worse functional outcomes (Marquez de la Plata et al., 2008), a greater likelihood of reinjury (Dams-O’Connor et al., 2013b), and more ED visits (Albrecht et al., 2016). Older adults with TBI do worse than younger adults even after mild TBI (Albrecht et al., 2016), and older age predicts worse functional trajectories after TBI post-inpatient rehabilitation (Howrey et al., 2017). Differences in outcome begin to appear even in patients aged 45–59 (Livingston et al., 2005; MRC CRASH Trial Collaborators et al., 2008). Additionally, a history of TBI may accelerate age at onset of cognitive impairment (Li et al., 2016).
Although older age has been clearly established as a strong risk factor for morbidity and mortality after TBI, the factors underlying these outcomes are not well understood. Clearly, however, the observation underscores the need to conceptualize TBI as a long-term condition in which pathophysiological processes interact with age-related changes (Griesbach et al., 2018). Some studies suggest that age moderates the relationship between injury severity and health outcomes, indicating that the effect of injury severity on functioning depends on the patient’s age at the time of injury. For instance, the fact that older patients with TBI have higher rates of mortality and worse functional outcomes compared with younger patients holds true despite their tendency to have apparently less severe head injuries (Susman et al., 2002). In
___________________
6 Patient Experiences with TBI Systems of Care. Panel discussion during virtual workshop for the Committee on Accelerating Progress in Traumatic Brain Injury Research and Care, March 16, 2021.
Marquez de la Plata and colleagues’ (2008) study of age and long-term recovery from TBI, older patients, despite having less severe TBI upon admission, had poorer functional status at discharge and less improvement at 1 year. Livingston and colleagues (2005) found that older TBI patients had poorer functional status at discharge and less improvement at 1 year compared with all other patients, despite less severe TBI upon admission (Livingston et al., 2005).
Given that TBI among older adults remains understudied, predicting outcomes and developing more effective treatment protocols for TBI in older adults will remain problematic in the absence of sufficient clinical data (Thompson et al., 2006). Age and TBI severity are inadequate prognostic markers, as many older adults can respond well to management and rehabilitative treatment (Gardner et al., 2018). However, there are no geriatric-specific TBI guidelines, and the performance of TBI prognostic models for geriatric patients is suboptimal (Dams-O’Connor et al., 2013a; Gardner et al., 2018). Moreover, older adults with TBI may be “misdiagnosed as having dementia and deemed not candidates for intensive rehabilitation.”7 There is clearly a need to develop geriatric-specific prognostic models and evidence-based geriatric TBI treatment and management guidelines.
Rural and Urban Differences in TBI Outcomes and Access to Care
As noted earlier, the care received by individual TBI patients may vary depending on where they live or receive care. For instance, one study evaluated differences in TBI mortality across urban and rural areas in the United States and found that the TBI fatality rate was 13 deaths per 100,000 persons higher in the most rural compared with the most urban areas (Brown et al., 2019). The median fatality rate from all causes of TBI was 23 percent higher in rural than in urban areas, with the greatest differences at the ends of the spectrum of metropolitan and nonmetropolitan counties (Brown et al., 2019).8Yue and colleagues (2020) found that the burden of TBI in terms of injury severity, outcomes, and survival is worse in rural than nonrural areas. Underlying factors include reduced or variable access to prehospital care, trauma centers, neurosurgical interventions, and rehabilitative services (Haarbauer-Krupa et al., 2021). Rural populations tend to experience longer delays in reaching care relative to urban populations, which affects long-term outcomes (Tiesman et al., 2007).
Individuals living in rural areas face unique challenges in accessing TBI care and achieving optimal outcomes. Rural areas are home to fewer people with access to fewer public resources compared with those living in nonrural areas. Thus, people in rural areas frequently rely on volunteer emergency response workforces and service providers. Furthermore, injuries occurring in rural areas often are sustained in remote settings with even more limited access to care. This remoteness is associated with greater delays in access to care, greater variability in hospital care capabilities, and the challenge of transporting patients to specialized trauma care when needed, as well as other economic and demographic challenges. For example, people living in remote areas may be older, less able to travel, or less able to afford travel for acute and post-acute care (Tiesman et al., 2007).
The term “rural” can be defined using various indices or criteria, but rural populations, however defined, frequently must contend with conditions of environmental austerity, such as geographic remoteness, isolation, and severe weather conditions. The similarities between
___________________
7 Connors, S. 2021. Family Impacts from TBI and Engagement in TBI Care. Panel discussion during virtual workshop for the Committee on Accelerating Progress in Traumatic Brain Injury Research and Care, March 16, 2021.
8 See Figure 3 from Brown and colleagues (2019), which compares TBI fatality rates per 100,000 persons in the United States by urban influence code. Garcia and colleagues (2017, p. 5) similarity report that “during 1999-2014, the age-adjusted death rates for unintentional injuries were approximately 50% higher in rural areas than urban areas.”
these challenges faced by rural populations and those faced by the armed forces may present an opportunity for collaboration among rural providers, special operations medical staff, and wilderness organizations to develop best practices for trauma care in austere conditions.
In terms of health systems and the experiences of rural and urban health care providers, urban providers practice in higher-resource settings where patients are typically closer to the point of care, and these providers have relatively frequent opportunities to practice and maintain skills in providing critical care. In contrast, rural providers practice in lower-resource settings where patients are often injured in remote settings far from the point of care, and these providers therefore have fewer opportunities to practice and maintain critical care skills. Moreover, there are very few neurosurgeons located in rural areas. Most trauma experts working in so-called rural settings in fact work in urban Level I or Level II trauma centers, that is, urban hubs that serve surrounding rural areas. Unfortunately, these providers often lack a comprehensive understanding of how trauma care is provided in truly rural settings or the experiences of providers in those settings. During 2020, for example, the committee learned that no members of the American College of Surgeons’ Rural Trauma Committee worked in a rural center. Similarly, the report A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths (NASEM, 2016a) mentions the term “rural” fewer than ten times, exemplifying the insufficient focus on rural trauma care systems.9
In fact, the typical conditions for highly rural trauma care are austere and often comparable to the conditions faced by deployed military personnel. Many medical centers in rural areas have fewer than 25 beds, and half of these centers are at least 75 miles from a Level I or II trauma center. Providers working in these rural settings have variable capability to treat severely injured patients, and data are sparse regarding the transfer of patients from rural settings to more capable trauma centers.10 Rural populations are doubly impacted by the lack of access to specialized trauma care. The current understanding of how best to treat TBI patients in rural settings is insufficient, and because these settings have reduced access to effective treatments, patients often do not receive the standard of care that is known to be effective in other settings.
In addition to the challenges associated with acute TBI care, access to post-acute and rehabilitative services is even more limited in rural areas. Comparing vocational rehabilitation outcomes between TBI survivors from rural versus urban settings, Johnstone and colleagues (2003) found that despite similar injury severity, neuropsychological test scores, and demographic characteristics, survivors residing in urban areas received significantly greater funds for basic needs required for full participation in the vocational rehabilitation program, as well as significantly more transportation assistance and on-the-job training.
The substantial burden of rural trauma highlights the need for additional study to evaluate the mechanisms of and possible solutions for the disparity between rural and urban trauma care and outcomes (Brown et al., 2019). Such studies might also have implications for trauma care in low- and middle-income countries.
A systematic approach to improved access to acute care for traumatic injuries in rural areas has been proposed.11 The starting point for such a system could be a notification system that, upon the reporting of an injury, would transmit SMS notifications to a dispatch center that would have up-to-date status and capacity information for all nearby hospitals.
___________________
9 Sidwell, R. 2021. Traumatic Brain Injury in the Rural Environment. Presentations and panel discussion during virtual workshop on Accelerating Progress in Traumatic Brain Injury Research and Care, March 16, 2021.
10 Ibid.
11 Ibid.
Patients could then be directed to the nearest appropriate center capable of delivering optimal care for a given patient.
Racial and Ethnic Differences in TBI Outcomes and Access to Care
Racial and ethnic differences have been linked to disparities and inequities in TBI prevalence, outcomes, and access to care. Many of the leading causes of TBI, such as road traffic crashes and violence, occur more frequently among populations of color relative to their White counterparts. Illustrating this point, the ED admission rate for the White population was 66 per 1,000 in 2019, compared with 74 per 1,000 for the non-White population (WISQARS, 2019 query).12 A retrospective cohort study of adults presenting to California EDs between 2005 and 2014, for example, found a 58 percent increase in TBI ED visits and a 34 percent decrease in the proportion of patients admitted to the hospital. Patients who were older adults, Black, and publicly insured had the highest visit rates (Hsia et al., 2018). Assaults, a leading cause of brain injury, occurred three times more often in Black people (10.7/1000) than in White people (3/1000) (WISQARS, 2019 query). Referral to inpatient posthospital care was lower for non-White patients and those without private insurance (Kane et al., 2014). Racial, ethnic, and socioeconomic disparities have also been identified among children who experience TBI. According to a 2006 study, among children under 10 in the United States who experienced a TBI related to a motor vehicle crash between 1995 and 2001, Black children experienced significantly higher rates of death and hospitalization compared with their White peers (Langlois et al., 2005).
A comprehensive literature review explored racial differences in post-TBI outcomes, as well as the potential causes of racial and ethnic disparities in TBI rehabilitation and postacute services (Gary et al., 2009). The review found that compared with their White counterparts, Black and Hispanic patients who experienced a TBI tended to have worse functional outcomes, were less integrated into their communities, were less likely to receive treatment, and were less likely to be employed. Black and Hispanic caregivers for people with TBI also reported experiencing greater burden, having more unmet needs, and using different types of coping strategies relative to White caregivers. The authors highlight emerging research that suggests racial and ethnic differences in TBI with respect to marital stability, emotional and neurobiological sequelae, and quality-of-life outcomes, although more research is needed to explore these associations.
Numerous studies have identified relationships of race and ethnicity to rehabilitation outcomes after TBI, including utilization of posthospital care, access to rehabilitation, functional status, community reintegration, and employment. This research has shown that survivors from racial and ethnic minority groups are significantly less likely to utilize posthospital health care after brain injury (Gao et al., 2018; Odonkor et al., 2021). For example, a study using data from the National Trauma Databank (NTDB) between 2012 and 2015 on more than 100,000 TBI survivors found that only 16.1 percent of Black patients and 12.5 percent of Hispanic patients with TBI had been discharged from acute care to inpatient rehabilitation, compared with 23.3 percent of White patients (Haines et al., 2019). Black survivors with TBI were more likely to be discharged from acute care to home and less likely to utilize outpatient physical medicine and rehabilitation (PM&R) services (Schiraldi et al., 2015). Compared with White TBI survivors, Hispanic survivors also experienced a lower likelihood of discharge to rehabilitation (Asemota et al., 2013;
___________________
12 WISQARS is CDC’s Web-based Injury Statistics Query and Reporting Systems, available at https://www.cdc.gov/injury/wisqars/index.html (accessed March 2, 2022).
Budnick et al., 2017; McQuistion et al., 2016) or posthospital care (Kane et al., 2014) and lower odds of discharge to high-level rehabilitation services despite similar insurance coverage (Meagher et al., 2015). Moreover, Black and Hispanic versus White survivors had poorer disability ratings, functional independence scores, and community reintegration (Arango-Lasprilla et al., 2007a,b; Hart et al., 2005), while Hispanic survivors were less likely to obtain employment or to receive on-the-job supports compared with European Americans (da Silva Cardoso et al., 2007).
Demographic data at the local and national levels are currently too limited to enable a full understanding of the needs of many minority communities. During the committee’s information-gathering workshop, for instance, Megan Moore from the University of Washington reported that there have been more than 400 studies on the impacts of structural inequities by race and ethnicity, but far fewer studies based on other facets of inequity.13 She noted that the literature on racial and ethnic differences in TBI often describes disparities in outcomes without adequately identifying the drivers of those disparities, and that even fewer address solutions. Research on these disparities is impeded by the pooling of many racial and ethnic groups in the TBI literature, resulting in gaps in personal/identity-related data. Moore stressed that more data are needed to support the research needed to fully understand these disparities by race and ethnicity, taking into account that not all disparities are differentially negative.14
To mitigate the underlying inequities that contribute to these disparate outcomes, it will be necessary to design interventions targeting post-acute care that are specifically tailored to these groups (Gary et al., 2009). At the patient and family level, interventions need to be shaped by an awareness of sociocultural conditions and traditions, as well as the impact of preinjury resilience on outcomes. At the provider level, interventions need to include cultural competency assessments and training that are specific to the needs of a diverse population of TBI patients. At the level of the health care system, strategies are needed for increasing the proportion of Black, Indigenous, and people of color (BIPOC) health care professionals who are part of multidisciplinary teams. To support these efforts, research will be needed to explore the foundational factors driving these disparities, such as discrimination and cultural incongruence (Moore et al., 2015).
Finally, resources for Black and Hispanic families facing TBI are limited, and it is often difficult to reach these communities, in part because they are not well represented in the TBI community. Information about TBI also needs to be made more broadly accessible by addressing language barriers, for example.
Examples of Other Factors Associated with Disparities After TBI
A variety of other pre- and postinjury social determinants of health, including unemployment, housing insecurity, and lack of health insurance, have been associated with disparities in TBI care and outcomes. Other factors, such as criminal history or substance abuse, may be stigmatized and can serve as additional barriers to TBI care and rehabilitation.
Unemployment
Preinjury unemployment among persons with mild TBI has been associated with decreases in functional outcomes and increases in postconcussion symptom reporting, psy-
___________________
13 Moore, M. 2021. Reducing disparities in traumatic brain injury. Presentation and panel discussion during virtual workshop on Accelerating Progress in Traumatic Brain Injury Research and Care, March 16, 2021.
14 Ibid.
chiatric symptoms, and PTSD 6 months after injury (Yue et al., 2018), while unemployment in survivors of severe TBI has been associated with lower 1-year outcome scores and more severe 8-year dysexecutive problems (Ruet et al., 2019). Several studies have also explored the intersection of employment status with racial and ethnic differences. In a sample of 3,468 White and 1,761 Black, Hispanic, Asian, and Native American persons with moderate to severe TBI, odds of unemployment at 1-year follow-up were twice as high among non-White versus White persons (Arango-Lasprilla et al., 2008). Another study found that, after controlling for preinjury status, age, education, injury mechanism, rehabilitation length of stay, and disability rating at discharge, non-White compared with White persons had 3.59 times greater odds of being unemployed than stably employed, 1.91 times greater odds of being unstably employed than stably employed, and 1.88 times greater odds of being unemployed than unstably employed (Arango-Lasprilla et al., 2009).
Housing Insecurity
TBI is often an unrecognized condition in persons experiencing housing insecurity. A systematic review and meta-analysis by Stubbs and colleagues (2020) found that the lifetime prevalence of TBI of any severity in homeless and marginally housed individuals was approximately 53 percent.
Lack of Health Insurance
A recent review of disparities in health insurance coverage and utilization of health services among U.S. TBI survivors (Gao et al., 2018) found that lack of insurance was associated with decreased use of posthospital care. Concerns about losing eligibility or coverage for disability benefits or care provided through such programs as Medicaid may also serve as disincentives for people with TBI to return to work. A meta-analysis of the U.S. labor market from 1990 to 2018 found that expanded eligibility for disability benefits was associated with reduced employment (McHale et al., 2020).
Lessons and Recommendations from Recent National Academies Reports Addressing Equity in Health Care
Several recent National Academies studies and workshops have explored strategies for advancing equity in health care systems (NASEM, 2016b, 2019a,b,c, 2021a,b). Although not directed specifically at TBI, many of the reflections and recommendations emerging from these sources are potentially applicable to efforts to increase equity in systems of care for TBI and may be worthy of consideration by the TBI community. These reflections and recommendations span a range of areas, including improving workforce education and performance monitoring, building interdisciplinary care teams, increasing access to care, forging institutional partnerships beyond health systems, reforming payment systems, and leveraging digital health technology and implementation science (see Box 3-1).
In 2017, the National Quality Forum published A Roadmap for Promoting Health Equity and Eliminating Disparities, highlighting four pillars: (1) identify priority disparity areas, (2) implement evidence-based interventions to reduce disparity, (3) invest in health equity performance measures, and (4) incentivize the reduction of disparities (NQF, 2017). These four pillars can also serve as a guiding structure for the design and implementation of strategies for reducing the impact of structural barriers and providing more equitable access to TBI care for those populations currently underserved. Adopting an equity lens to shape such efforts
will require awareness of assumptions that constrain the way people perceive, understand, and feel the world (NASEM, 2016b), ingrained viewpoints and expectations that must be changed to achieve a more inclusive perspective. In some contexts, health care inequity can be framed most effectively as a systemic and unsustainable issue of moral justice that affects all of society, not just particular minority groups, improvements in which will yield benefits for all. In other scenarios, it may be more appropriate to leverage a value-proposition argument for improving diversity, equity, and inclusion.
Lessons from Care Systems That Minimize Disparities
The early phases of assessment and acute management of TBI for military personnel and athletes on sports teams, such as those in the National Football League (NFL) and selected other professional sports leagues, provide lessons for minimizing the effect of disparities on immediate management at the site of injury, as well as on the quality and location of definitive emergency care.
Injuries to some of these individuals occur in the most dangerous, remote, and inaccessible places in the world. In battle zones where military service members are wounded, priority is given to mitigating the limitations of available health care capacity with evidence-based TBI protocols, extensive medical and nonmedical training, and timely evacuation and definitive care. Assessment, reporting, and rest protocols are an important component of early phases of TBI management for active duty service members.15 TBI is considered a potential risk for all service members deployed to war zones, engaged in training, or participating in sports programs, as well as for athletes in high-risk professional and university sports programs.16 As a consequence, potential TBIs in combat or on the playing field are treated aggressively, particularly given the attention to TBI resulting from the past two decades of war in Southwest Asia and increased focus on the long-term effects of concussions in athletics.
After acute TBI care, mid- and long-term management of the consequences of TBI is affected by access to and the nature of specialty care and institutional, community, and educational rehabilitation. In the management of sports-related concussion, such modifiable factors as early identification and follow-up with a specialist experienced in TBI are associated with faster recovery and improved outcomes (Desai et al., 2019; Kontos et al., 2020; Master et al., 2020). For military service members, a Transition and Care Management Program for Veterans who have served since the terrorist attacks of 9/11 extends comprehensive care into their transition to civilian life. The Department of Defense’s (DoD’s) military care system and the facilities and programs of the VA strive to ensure the availability of a system of care that encompasses prevention, early recognition and treatment of a potential TBI, and access to long-term rehabilitation.
Testimony during the committee’s information-gathering sessions included examples
___________________
15 DoD Instruction 6490.11, enacted in 2012 (DoD, 2019), provides policy guidance on management of concussion or “mild” TBI among deployed service members, and includes requirements for reporting, conduct of medical evaluations, and mandatory rest. For example, all service members must be assessed for a potential concussion after such circumstances as vehicle collisions or rollovers, exposure within 50 meters of an explosion, a blow to the head, or loss of consciousness. The military has also developed the Military Acute Concussion Evaluation-2 (MACE-2) screening tool (https://health.mil/Reference-Center/Publications/2020/07/30/Military-Acute-Concussion-Evaluation-MACE-2 [accessed August 24, 2021]).
16 The consensus statement of the Concussion in Sport Group recommends that “In all suspected cases of concussion, the individual should be removed from the playing field and assessed by a physician or licensed healthcare provider” (CISG, 2017, p. 839). The group has developed a standardized Sport Concussion Assessment Tool, now in its fifth edition, to aid in rapid evaluation (https://bjsm.bmj.com/content/bjsports/early/2017/04/26/bjsports-2017-097506SCAT5.full.pdf [accessed August 24, 2021]).
of optimal management of health challenges with lifelong impacts. Optimal management of stroke, for example, relies on prompt recognition of its occurrence, rapid transport to a facility capable of performing appropriate brain imaging studies, and thrombolytic/hemostatic intervention (Powers et al., 2019). Failure to take these steps may result in early death or prolonged disability. Recovery and rehabilitation after stroke requires a multidisciplinary approach with active family and patient support and community engagement to achieve optimal function for the patient. BPSE factors also play important roles in achieving an optimal management scheme for pain care, and a comprehensive national program is currently under way aimed at combining the efforts of basic and clinical researchers, clinicians, community health and health care organizations, patient advocacy groups, and public and private funding sources to reduce the impact of these factors.17
Similarly, optimal management of Alzheimer’s disease relies on prompt identification and multidisciplinary engagement (Bradley et al., 2015). These efforts may forestall the full impact of neurodegeneration and promote patient function, reduce family and community suffering, and lessen individual financial impacts and community economic costs as the disease progresses. As with stroke management, a multidisciplinary approach with active family and patient support, as well as community engagement, is needed to achieve optimal function for the patient and reduce long-term secondary and tertiary effects. The access of individual patients and their supportive families and friends to these collective services is a function of BPSE factors that are being addressed on a national scale.18
CONCLUSIONS
TBI needs to be viewed through the lens of a BPSE model. Outcomes from TBI are affected by factors beyond medical care, and TBI interacts strongly with other physical, psychological, and social conditions. Factors associated with disparities in TBI care and outcomes include geographic location, race and ethnicity, age, and gender, and current care and research systems do not function ideally for many patients and their families. A life-course approach to understanding and managing TBI is also required. A person who experiences TBI, of whatever initial severity, needs to be able to reengage with the health care system if new symptoms emerge or as needs change. These engagement points represent potential opportunities for intervention to refocus a patient’s post-TBI pathway toward more optimal recovery and outcomes.
REFERENCES
Albrecht, J. S., J. M. Hirshon, M. McCunn, K. T. Bechtold, V. Rao, L. Simoni-Wastila, and G. S. Smith. 2016. Increased rates of mild traumatic brain injury among older adults in US emergency departments, 2009-2010. Journal of Head Trauma Rehabilitation 31(5):E1-E7.
Arango-Lasprilla, J. C., M. Rosenthal, J. Deluca, E. Komaroff, M. Sherer, D. Cifu, and R. Hanks. 2007a. Traumatic brain injury and functional outcomes: Does minority status matter? Brain Injury 21(7):701-708.
___________________
17 See the VA program of team-based pain care, which draws on a biopsychosocial model of pain and uses a Stepped Care Model linking elements from self-care to care at specialized centers (https://www.va.gov/PAINMANAGEMENT/Providers/IntegratedTeambasedPainCare.asp [accessed August 25, 2021]). In addition, the National Institutes of Health (NIH)-DoD-VA Pain Management Collaboratory involves multiple workgroups conducting 11 multisite pragmatic clinical trials (https://painmanagementcollaboratory.org [accessed August 24, 2021]).
18 See, for example, the CDC website for information on the intersections of social determinants of health with Alzheimer’s’ disease (https://www.cdc.gov/aging/disparities/social-determinants-alzheimers.html [accessed August 24, 2021]). See also the Department of Health and Human Services’ Healthy People 2030 initiative to improve health and well-being (https://health.gov/healthypeople [accessed August 24, 2021]).
Arango-Lasprilla, J. C., M. Rosenthal, J. DeLuca, D. Cifu, R. Hanks, and E. Komaroff. 2007b. Functional outcomes from inpatient rehabilitation after traumatic brain injury: How do Hispanics fare? Archives of Physical Medicine and Rehabilitation 88(1):1-18.
Arango-Lasprilla, J. C., J. Ketchum, K. Williams, J. Kreutzer, C. Marquez de la Plata, T. O’Neil-Pirozzi, and P. Wehman. 2008. Racial differences in employment outcomes after traumatic brain injury. Archives of Phsyical Medicine and Rehabilitation 89(5):988-995.
Arango-Lasprilla, J. C., J. Ketchum, K. Gary, J. Kreutzer, T. O’Neil-Pirozzi, P. Wehman, C. Marquez de la Plata, and A. Jha. 2009. The influence of minority status on job stability after traumatic brain injury. Physical Medicine and Rehabilitation 1(1):41-49.
Asemota, A., B. George, C. Cumpsty-Fowler, A. Haider, and E. Schneider. 2013. Race and insurance disparities in discharge to rehabilitation for patients with traumatic brain injury. Journal of Neurotrauma 30(24):2057-2065.
Bouldin, E. D., A. A. Swan, R. S. Norman, D. F. Tate, C. Tumminello, M. E. Amuan, B. C. Eapen, C. P. Wang, A. Trevino, and M. J. Pugh. 2021. Health phenotypes and neurobehavioral symptom severity among post-9/11 veterans with mild traumatic brain injury: A chronic effects of neurotrauma consortium study. Journal of Head Trauma Rehabilitation 36(1):10-19.
Bradley, P., R. Akehurst, C. Ballard, S. Banerjee, K. Blennow, J. Bremner, K. Broich, J. Cummings, K. Dening, B. Dubois, W. Klipper, C. Leibman, V. Mantua, J. L. Molinuevo, S. Morgan, L. A. Muscolo, F. Nicolas, L. Pani, L. Robinson, P. Siviero, J. van Dam, J. Van Emelen, A. Wimo, M. Wortmann, and L. Goh. (2015). Taking stock: A multistakeholder perspective on improving the delivery of care and the development of treatments for Alzheimer’s disease. Alzheimer’s & Dementia 11(4):455-461.
Brown, J. B., M. Kheng, N. A. Carney, A. M. Rubiano, and J. C. Puyana. 2019. Geographical disparity and traumatic brain injury in America: Rural areas suffer poorer outcomes. Journal of Neurosciences in Rural Practice 10(1):10-15.
Budnick, H., A. Tyroch, and S. Milan. 2017. Ethnic disparities in traumatic brain injury care referral in a Hispanic-majority population. Journal of Surgical Research 215:231-238.
Cifu, D. X., B. C. Taylor, W. Carne, D. Bidelspach, N. Sayer, J. Scholten, and E. Campbell. 2013. Traumatic brain injury, posttraumatic stress disorder, and pain diagnoses in OIF/OEF/OND veterans. Journal of Rehabilitation Research and Development 50(9):1169-1176.
CISG (Concussion in Sport Group). 2017. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. British Journal of Sports Medicine 51:838-847.
Cogan, A. M., V. K. McCaughey, and J. Scholten. 2020. Gender differences in outcomes after traumatic brain injury among service members and veterans. PM&R: The Journal of Injury, Function, and Rehabilitation 12(3):301-314.
da Silva Cardoso, E., M. Romero, F. Chan, A. Dutta, and M. Rahimi. 2007. Disparities in vocational rehabilitation services and outcomes for Hispanic clients with traumatic brain injury: Do they exist? Journal of Head Trauma Rehabilitation 22(2):85-94.
Dams-O’Connor, K., J. P. Cuthbert, J. Whyte, J. D. Corrigan, M. Faul, and C. Harrison-Felix. 2013a. Traumatic brain injury among older adults at level I and II trauma centers. Journal of Neurotrauma 30(24):2001-2013.
Dams-O’Connor, K., L. E. Gibbons, J. D. Bowen, S. M. McCurry, E. B. Larson, and P. K. Crane. 2013b. Risk for late-life re-injury, dementia and death among individuals with traumatic brain injury: A population-based study. Journal of Neurology, Neurosurgery and Psychiatry 84(2):177-182.
Dams-O’Connor, K., A. Landau, J. Hoffman, and J. St De Lore. 2018. Patient perspectives on quality and access to healthcare after brain injury. Brain Injury 32(4):431-441.
Daugherty, J., D. Waltzman, K. Sarmiento, and L. Xu. 2019. Traumatic brain injury-related deaths by race/ethnicity, sex, intent, and mechanism of injury—United States, 2000–2017. Morbidity and Mortality Weekly Report 68(46):1050-1056.
Desai, N., D. J. Wiebe, D. Corwin, J. Lockyer, M. Grady, and C. L. Master. 2019. Factors affecting recovery trajectories in pediatric female concussion. Clinical Journal of Sport Medicine 29(5):361-367.
DoD (Department of Defense). 2019. Instruction 6490.11. DoD policy guidance for management of mild traumatic brain injury/concussion in the deployed setting. September 8, 2012. Incorporating Change 2, effective November 26, 2019.
Engel, G. 1977. The need for a new medical model: a challenge for biomedicine. Science 196 (4286):129-136.
Esopenko, C., J. Meyer, E. Wilde, A. Marshall, D. Tate, A. Lin, I. Koerte, K., et al. 2021. A global collaboration to study intimate partner violence-related head trauma: The ENIGMA consortium IPV working group. Brain Imaging and Behavior 15(2):475-503.
Fabricius, A. M., A. D’Souza, V. Amodio, A. Colantonio, and T. Mollayeva. 2020. Women’s gendered experiences of traumatic brain injury. Qualitative Health Research 30(7):1033-1044.
Ferguson, P. L., E. E. Pickelsimer, J. D. Corrigan, J. A. Bogner, and M. Wald. 2012. Prevalence of traumatic brain injury among prisoners in South Carolina. Journal of Head Trauma Rehabilitation 27(3):E11-E20.
Foster, M., and C. Tilse. 2003. Referral to rehabilitation following traumatic brain injury: A model for understanding inequities in access. Social Science & Medicine 56(10):2201-2210.
Gao, S., R. Kumar, S. Wisniewski, and A. Fabio. 2018. Disparities in health care utilization of adults with traumatic brain injuries are related to insurance, race and ethnicity: A systematic review. Journal of Head Trauma Rehabilitation 33(3):e40-e50.
Garcia, M. C., Faul, M., Massetti, G., Thomas, C. C., Hong, Y., Bauer, U. E., and M. F. Iademarco. 2017. Reducing potentially excess deaths from the five leading causes of death in the rural United States. Morbidity and Mortality Weekly Report Surveillance Summaries 66(2):1-7.
Gardner, R. C., K. Dams-O’Connor, M. R. Morrissey, and G. T. Manley. 2018. Geriatric traumatic brain injury: Epidemiology, outcomes, knowledge gaps, and future directions. Journal of Neurotrauma 35(7):889-906.
Gary, K. W., J. C. Arango-Lasprilla, and L. F. Stevens. 2009. Do racial/ethnic differences exist in post-injury outcomes after TBI? A comprehensive review of the literature. Brain Injury 23(10):775-789.
Gray, M., M. M. Adamson, R. C. Thompson, K. I. Kapphahn, S. Han, J. S. Chung, and O. A. Harris. 2020. Sex differences in symptom presentation and functional outcomes: a pilot study in a matched sample of veterans with mild TBI. Brain Injury 34(4):535-547.
Griesbach, G. S., B. E. Masel, R. E. Helvie, and M. J. Ashley. 2018. The impact of traumatic brain injury on later life: Effects on normal aging and neurodegenerative diseases. Journal of Neurotrauma 35(1):17-24.
Haarbauer-Krupa, J., A. Ciccia, J. Dodd, D. Ettel, B. Kurowski, A. Lumba-Brown, and S. Suskauer. 2017. Service delivery in the healthcare and educational systems for children following traumatic brain injury: Gaps in care. Journal of Head Trauma Rehabilitation 32(6):367-377.
Haarbauer-Krupa, J., A. H. Lee, R. H. Bitsko, X. Zhang, and M. J. Kresnow-Sedacca. 2018. Prevalence of parent-reported traumatic brain injury in children and associated health conditions. JAMA Pediatrics 172(11):1078-1086.
Haarbauer-Krupa, J., M. J. Pugh, E. M. Prager, N. Harmon, J. Wolfe, and K. C. Yaffe. 2021. Epidemiology of chronic effects of traumatic brain injury. Journal of Neurotrauma 8(23):3235-3247.
Haines, K., B. Nguyen, C. Vatsaas, A. Alger, K. Brooks, and S. Agarwal. 2019. Socioeconomic status affects outcomes after severity-stratified traumatic brain injury. Journal of Surgical Research 235:131-140.
Hart, T., J. Whyte, M. Polansky, G. Kersey-Matusiak, and R. Fidler-Sheppard. 2005. Community outcomes following traumatic brain injury: Impact of race and preinjury status. Journal of Head Trauma Rehabilitation 20(3):158-172.
Hoge, C. W., D. McGurk, J. Thomas, A. Cox, C. Engel, and C. Castro. 2008. Mild traumatic brain injury in U.S. Soldiers returning from Iraq. New England Journal of Medicine 358(5):453-463.
Hood, C. M., K. Gennuso, G. Swain, and B. Catlin. 2016. County health rankings: Relationships between determinant factors and health outcomes. American Journal of Preventive Medicine 50(2):129-135.
Howrey, B. T., J. E. Graham, M. R. Pappadis, C. V. Granger, and K. J. Ottenbacher. 2017. Trajectories of functional change after inpatient rehabilitation for traumatic brain injury. Archives of Physical Medicine and Rehabilitation 98(8):1606-1613.
Hsia, R. Y., A. J. Markowitz, F. Lin, J. Guo, D. Y. Madhok, and G. T. Manley. 2018. Ten-year trends in traumatic brain injury: A retrospective cohort study of California emergency department and hospital revisits and readmissions. BMJ Open 8(12):e022297.
IOM (Institute of Medicine). 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
Iverson, K. M., A. M. Hendricks, R. Kimerling, M. Krengel, M. Meterko, K. L. Stolzmann, E. Baker, T. K. Pogoda, J. J. Vasterling, and H. L. Lew. 2011. Psychiatric diagnoses and neurobehavioral symptom severity among OEF/OIF VA patients with deployment-related traumatic brain injury: A gender comparison. Women’s Health Issues 21(4 Suppl):S210-S217.
Johnstone, B., T. Price, T. Bounds, L. Schopp, M. Schootman, and D. Schumate. 2003. Rural/urban differences in vocational outcomes for state vocational rehabilitation clients with TBI. NeuroRehabilitation 18(3):197-203.
Kane, W. G., D. A. Wright, R. Fu, and K. F. Carlson. 2014. Racial/ethnic and insurance status disparities in discharge to posthospitalization care for patients with traumatic brain injury. Journal of Head Trauma Rehabilitation 29(6):E10-E17.
Karb, R. A., S. V. Subramanian, and E. W. Fleegler. 2016. County poverty concentration and disparities in unintentional injury deaths: A fourteen-year analysis of 1.6 million U.S. fatalities. PloS One 11(5):e0153516.
Karriker-Jaffe, K. J., J. Witbrodt, A. Mericle, D. Polcin, and L. A. Kaskutas. 2020. Testing a socioecological model of relapse and recovery from alcohol problems. Substance Abuse: Research and Treatment 14:1178221820933631.
Kim, L. H., J. Quon, F. Sun, K. Wortman, M. Adamson, and O. Harris. 2018. Traumatic brain injury among female veterans: A review of sex differences in military neurosurgery. Neurosurgical Focus 45(6):E16.
Kontos, A. P., K. Jorgensen-Wagers, A. M. Trbovich, N. Ernst, K. Emami, B. Gillie, J. French, C. Holland, R. Elbin, and M. Collins. 2020. Association of time since injury to the first clinic visit with recovery following concussion. JAMA Neurology 77(4):435-440.
Langlois, J. A., W. Rutland-Brown, and K. E. Thomas. 2005. The incidence of traumatic brain injury among children in the United States: Differences by race. Journal of Head Trauma Rehabilitation 20(3):229-238.
Li, W., S. L. Risacher, T. W. McAllister, and A. J. Saykin. 2016. Traumatic brain injury and age at onset of cognitive impairment in older adults. Journal of Neurology 263(7):1280-1285.
Livingston, D. H., R. F. Lavery, A. C. Mosenthal, M. M. Knudson, S. Lee, D. Morabito, G. T. Manley, A. Nathens, G. Jurkovich, D. B. Hoyt, and R. Coimbra. 2005. Recovery at one year following isolated traumatic brain injury: A western trauma association prospective multicenter trial. Journal of Trauma and Acute Care Surgery 59(6):1298-1304; discussion 1304.
Marquez de la Plata, C. D., T. Hart, F. M. Hammond, A. B. Frol, A. Hudak, C. R. Harper, T. M. O’Neil-Pirozzi, J. Whyte, M. Carlile, and R. Diaz-Arrastia. 2008. Impact of age on long-term recovery from traumatic brain injury. Archives of Physical Medicine and Rehabilitation 89(5):896-903.
Master, C. L., B. Katz, K. Arbogast, M. McCrea, T. McAllister, P. Pasquina, M. Lapradd, W. Zhou, S. Broglio, and CARE Consortium Investigators. 2020. Differences in sport-related concussion for female and male athletes in comparable collegiate sports: A study from the NCAA-DoD Concussion Assessment, Research and Education (CARE) Consortium. British Journal of Sports Medicine 55(24):1387-1394.
Master, C. L., B. P. Katz, K. B. Arbogast, M. A. McCrea, T. W. McAllister, P. F. Pasquina, M. Lapradd, W. Zhou, S. P. Broglio, and CARE Consortium Investigators. 2021. Differences in sport-related concussion for female and male athletes in comparable collegiate sports: a study from the NCAA-DoD Concussion Assessment, Research and Education (CARE) Consortium. British Journal of Sports Medicine 55:1387-1394.
McHale, P., A. Pennington, C. Mustard, Q. Mahood, I. Andersen, N. K. Jensen, B. Burström, K. Thielen, L. Harber-Aschan, A. McAllister, M. Whitehead, and B. Barr. 2020. What is the effect of changing eligibility criteria for disability benefits on employment? A systematic review and meta-analysis of evidence from OECD countries. PloS One 15(12):e0242976.
McQuistion, K., Zens, T., Jung, H. S., Beems, M., Leverson, G., Liepert, A., Scarborough, J., and S. Agarwal. 2016. Insurance status and race affect treatment and outcome of traumatic brain injury. Journal of Surgical Research 205(2):261-271.
Meagher, A., C. Beadles, J. Doorey, and A. Charles. 2015. Racial and ethnic disparities in discharge to rehabilitation following traumatic brain injury. Journal of Neurosurgery 122:599-601.
Moore, M., G. Robinson, R. Mink, K. Hudson, D. Dotolo, T. Gooding, A. Ramirez, D. Zatzick, J. Giordano, D. Crawley, and M. S. Vavilala. 2015. Developing a family-centered care model for critical care after pediatric traumatic brain injury. Pediatric Critical Care Medicine 16(8):758-765.
Moore, M., K. M. Conrick, M. Fuentes, A. Rowhani-Rahbar, J. Graves, D. Patil, M. Herrenkohl, B. Mills, F. Rivara, B. Ebel, and M. S. Vavilala. 2019. Research on injury disparities: A scoping review. Health Equity 3(1):504-511.
MRC CRASH Trial Collaborators, P. Perel, M. Arango, T. Clayton, P. Edwards, E. Komolafe, S. Poccock, I. Roberts, H. Shakur, E. Steyerberg, and S. Yutthakasemsunt. 2008. Predicting outcome after traumatic brain injury: Practical prognostic models based on large cohort of international patients. British Medical Journal 336(7641):425-429.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016a. A national trauma care system: Integrating military and civilian trauma systems to achieve zero preventable deaths after injury. Washington, DC: The National Academies Press.
NASEM. 2016b. Framing the dialogue on race and ethnicity to advance health equity. Washington, DC: The National Academies Press.
NASEM. 2017. Communities in action, pathways to health equity. Washington, DC: The National Academies Press.
NASEM 2019a. Health-focused public-private partnerships in the urban context. Washington, DC: The National Academies Press.
NASEM. 2019b. Improving access to and equity of care for people with serious illness. Washington, DC: The National Academies Press.
NASEM. 2019c. Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. Washington, DC: The National Academies Press.
NASEM. 2021a. Implementing high-quality primary care: Rebuilding the foundation of health care. Washington, DC: The National Academies Press.
NASEM. 2021b. The future of nursing 2020–2030: Charting a path to achieve health equity. Washington, DC: The National Academies Press.
NINDS (National Institute of Neurological Disorders and Stroke). 2017. Workshop summary: Understanding traumatic brain injury in women. https://www.ninds.nih.gov/sites/default/files/tbi_workshop_summary_-_december_18-19_2017_508c_0.pdf (accessed September 27, 2021).
NQF (National Quality Forum). 2017. A roadmap for promoting health equity and eliminating disparities: The four I’s for health equity. https://www.qualityforum.org/Publications/2017/09/A_Roadmap_for_Promoting_Health_Equity_and_Eliminating_Disparities__The_Four_I_s_for_Health_Equity.aspx (accessed September 27, 2021).
NRC and IOM (National Research Council and Institute of Medicine). 2013. U.S. health in international perspective: Shorter lives, poorer health. Washington, DC: The National Academies Press.
Odonkor, C., R. Esparza, L. Flores, M. Verduzco-Gutierrez, M. Escalon, R. Solinski, and J. Silver. 2021. Disparities in health care for black patients in physical medicine and rehabilitation in the United States: A narrative review. Physical Medicine and Rehabilitation 13(2):180-203.
Piatt, J. 2021. Racial disparities in mortality after severe traumatic brain injury in childhood: Mediators identified by Oaxaca-Blinder decomposition of trauma registry data. Injury Epidemiology 8(1):1.
Powers, W. J., A. Rabinstein, T. Ackerson, O. Adeoye, N. Bambakidis, K. Becker, J. Biller, M. Brown, B. Demaerschalk, B. Hoh, E. Jauch, C. Kidwell, T. Leslie-Mazwi, B. Ovbiagele, P. Scott, K. Sheth, A. Southerland, D. Summers, and D. L. Tirschwell. 2019. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 50(12):e344-e418.
Pugh, M. J., A. A. Swan, M. E. Amuan, B. C. Eapen, C. A. Jaramillo, R. Delgado, D. F. Tate, K. Yaffe, and C. P. Wang. 2019. Deployment, suicide, and overdose among comorbidity phenotypes following mild traumatic brain injury: A retrospective cohort study from the chronic effects of neurotrauma consortium. PLoS One 14(9):e0222674
Register-Mihalik, J. K., and C. E. Callahan. 2020. Postconcussion exertion evolution: Clinical and behavioral considerations. Current Sports Medicine Reports 19(4):151-156.
Ruet, A., E. Bayen, C. Jourdan, I. Ghout, L. Meaude, A. Lalanne, P. Pradat-Diehl, G. Nelson, J. Charanton, P. Aegerter, C. Vallat-Azouvi, and P. Azouvi. 2019. A detailed overview of long-term outcomes in severe traumatic brain injury eight years post-injury. Frontiers in Neurology 10.120. https://doi.org/10.3389/fneur.2019.00120.
Schiraldi, M., C. Patil, D. Mukherjee, B. Ugiliweneza, M. Nuño, S. Lad, and M. Boakye. 2015. Effect of insurance and racial disparities on outcomes in traumatic brain injury. Journal of Neurological Surgery 76(3):224-232.
Stippler, M., E. Holguin, and E. Nemoto. 2012. Traumatic brain injury in elders. Annals of Long-Term Care: Clinical Care and Aging 20(5):1-7.
Stubbs, J., A. Thornton, J. Sevick, N. Silverberg, A. Barr, W. Honer, and W. Panenka. 2020. Traumatic brain injury in homeless and marginally housed individuals: A systematic review and meta-analysis. Lancet Public Health 5(1):e19-e32.
Susman, M., S. M. DiRusso, T. Sullivan, D. Risucci, P. Nealon, S. Cuff, A. Haider, and D. Benzil. 2002. Traumatic brain injury in the elderly: Increased mortality and worse functional outcome at discharge despite lower injury severity. Journal of Trauma and Acute Care Surgery 53(2):219-223; discussion 223-224.
Tanielian, T., L. Jaycox, and D. M. Adamson. 2008. Invisible wounds of war. Santa Monica, CA: RAND Corporation.
Thompson, H. J., W. C. McCormick, and S. H. Kagan. 2006. Traumatic brain injury in older adults: Epidemiology, outcomes, and future implications. Journal of the American Geriatrics Society 54(10):1590-1595.
Tiesman, H., T. Young, J. C. Torner, M. McMahon, C. Peek-Asa, and J. Fiedler. 2007. Effects of a rural trauma system on traumatic brain injuries. Journal of Neurotrauma 24(7):1189-1197.
van Erp, R., I. Huijnen, M. Jakobs, J. Kleijnen, and R. Smeets. 2019. Effectiveness of primary care interventions using a biopsychosocial approach in chronic low back pain: A systematic review. Pain Practice 19(2):224-241.
Yue, J. K., J. W. Rick, M. R. Morrissey, S. R. Taylor, H. Deng, C. G. Suen, M. J. Vassar, M. C. Cnossen, H. F. Lingsma, E. L. Yuh, P. Mukherjee, R. C. Gardner, A. B. Valadka, D. O. Okonkwo, T. A. Cage, G. T. Manley, and TRACK-TBI Investigators, 2018. Preinjury employment status as a risk factor for symptomatology and disability in mild traumatic brain injury: A TRACK-TBI analysis. NeuroRehabilitation 43(2):169-182.
Yue, J. K., P. Upadhyayula, L. Avalos, and T. A. Cage. 2020. Rural-urban disparities and considerations. Brain Sciences 10(3):135.
This page intentionally left blank.
























