
5
Current Capital Asset Management at NIH
DETERMINING THE VALUE OF FACILITIES ON THE BETHESDA CAMPUS
As noted in Chapter 3, the National Institutes of Health (NIH) Intramural Research Program (IRP) annually performs over $3.7 billion in research, primarily at the Bethesda Campus, and employs over 3,600 research professionals and some 5,400 non-full-time-equivalent trainees. The campus’s facilities that house these research activities and personnel make it possible for NIH to accomplish its mission. Assessment of the value of these facilities in accomplishing the mission is essential for prioritization of investments in facilities.
Value of Real Property Assets
NIH real property falls under Executive Order 13327 (2004), which established the requirements for federal real property asset management, including a full inventory of real property assets, market valuation of those assets, and prioritized plans to improve the operational and financial management of those assets.1 The U.S. General Services Administration (GSA) administers the Federal Real Property Inventory Reporting, and recently updated the calculations of Replacement Value as follows (FPRC, 2018, p. 22):
Replacement Value is defined as the cost required to design, acquire and construct an asset to replace an existing asset of the same functionality, size, and in the same location using current costs, building codes, and standards. Neither the current condition of the asset nor the future need for the asset is a factor in the replacement value estimate.
- Numeric values reported for replacement value must be greater than zero.
- Failure to follow this guidance will result in inaccurate information on the FRPP condition index (CI), since CI is estimated based on replacement value.
___________________
1 Executive Order 13327 of February 4, 2004, Federal Real Property Asset Management, Federal Register 69(25):5897-5900.
- Replacement value must be reported for all owned and otherwise managed buildings and structures regardless of facility condition, type, or whether it has been identified for disposal. For otherwise managed property, the “unit” should be based on the size (square feet of space) as specified in the agreement. Replacement Value for building assets must be a numeric value greater than or equal to the asset’s square feet.
While the GSA recommends annually increasing the Replacement Value to reflect inflation, the functional replacement value (FRV) might more effectively reflect the value of the asset with respect to rapidly advancing research and development requirements. For example, the Current Replacement Value (CRV) of an existing surgical facility with limited floor-to-floor heights can be calculated from standard cost databases, but if the needs of the research program require additional floor-to-floor height plus more densely serviced communications and power lines to accommodate robotic assisted surgery research, the FRV may be tailored to more clearly reflect those additional costs. While it is the CRV that is widely used in calculating CI—indicating as it does the present condition of an asset—using the FRV for such purposes can offer an interesting comparison. A 2015 U.S. Government Accountability Office report notes that “GSA defines functional replacement value (FRV) as follows: FRV = Cost to replace the building’s function (office, warehouse, etc.) and not the cost to replace the building as an exact replica of itself” (GAO, 2015, p. 5).
As noted in the 2012 National Research Council (NRC) report Predicting the Outcomes of Investments in Maintenance and Repair of Federal Facilities, “the primary objective of portfolio-based facilities management is to ensure that facilities-related investments enable the organization’s mission” (p. 61). The report details several approaches that assess the value of facilities with respect to the risk of failure and the threat to achieving mission. For example, the Mission Dependency Index (MDI) assesses the damage from interruption or downtime from facility failure, which is used to prioritize investments. The U.S. Army Corps of Engineers developed the IMPACT simulation model to assess the impacts of delaying repairs on the service life of the equipment and consequent emergency repair cost (p. 64). The NRC report states:
Facilities program managers should understand and be able to communicate effectively the economic value of a component or system to a mission, and the cost of protecting its value. To do that, they will need to identify the types of deterioration or other adverse events that will lead to loss of mission, the vulnerabilities of facilities to adverse events, the potential loss of economic value if a failure occurs, the accumulation of potential losses until the system is repaired, and how vulnerabilities can cascade into additional failures. (p. 77)
Another agency that utilizes the MDI is NASA. NASA adopted the MDI in 2004 with the goal to better manage facilities’ risks and provide a better guide for investment and divesture decisions.2 This approach involves asking the user to honestly assess the capability of the organization to perform its mission when the asset is not available. This allows decisions about repair, replacement, or disposal of capital assets to include the key discussion about impacts on mission accomplishment due to potential adverse events. It should be noted that there are times when the duration of the interruption is very short or other locations are available to facilitate relocation with little impact to the mission. But when that is not the case, it may be very appropriate to direct capital assets into existing or new facilities to ensure mission accomplishment (NASA, 2010). This is further discussed in the section “Using CI for Decision Making,” below.
If the NIH capital asset management followed this approach, it could establish the value of the full functionality of its facilities in three ways:
- Assess the relevant IRP budget affected by facility downtime (such as from power failures) or loss of productivity (such as from water damage) related to emergency repairs;
___________________
2 NASA Facilities and Real Estate Division, “Notes on Using the Mission Dependency Index,” https://www.nasa.gov/offices/FRED/directives_and_requirements.
- Assess the potential value of the outcomes from the IRP research that are delayed, constrained, or cancelled due to facility downtime or emergency repairs; and
- Assess the impact on patient care (such as travel time and wait time, delays in receiving treatment, and rescheduling) due to facility downtime or emergency repairs.
A recent report by the Institute for Defense Analyses (Howieson et al., 2013) cites four examples of federal security labs (i.e., those labs that conduct national security research and development) for which the management explicitly calculates the cost of facility disruptions in its prioritization of capital asset investments relative to agency mission:
- MIT-LL [MIT Lincoln Laboratory] developed the disruption index to indicate the degree to which a new project or alternatives to the project would interrupt current operations and research programs.
- NRL [Naval Research Laboratory] evaluates the disruption to ongoing research program as another consideration when prioritizing facilities, equipment, and F&I [facilities and infrastructure] projects.
- JHU-APL [Johns Hopkins University Applied Physics Laboratory] measures impact to its mission as the risk associated with the continuity of its customers’ research programs.
- The Army’s MEDCOM established the Facility Experience Index to consider aesthetics when evaluating F&I projects. The aesthetics index is based on a questionnaire completed by facility managers and patients that are weighted 75 and 25 percent, respectively. Although the aesthetics index is applicable only to medical treatment facilities (as relevant to the public’s perception of the quality of their care), it provides an example of how MEDCOM is applying various concepts, methods, and tools to assess its F&I needs. (pp. 38-39)
PROCESS BY WHICH PROJECTS ARE PLANNED AND EVALUATED
Description of Process
NIH staff presented the organization, structure, and general process of the Facilities Working Group (FWG) and its subcommittees to the National Academies of Sciences, Engineering, and Medicine committee:3 “The FWG is responsible for evaluating NIH’s programmatic needs; balancing competing priorities; exploring alternative means of meeting NIH’s changing needs for capital facilities; and reconciling them into a rolling 5-year Strategic Facilities Plan [i.e., the B&F/NEF-Funded 5-Year Plan], an annual Buildings and Facilities (B&F) Plan, and an annual Leased Facilities Plan.”4 Membership in the FWG consists of 11 voting members and 1 nonvoting member. The group includes representation of IC directors, IC scientific directors, and executive officers from various ICs appointed by the Director of NIH for 3-year terms.5 Two subcommittees operate under the FWG, the Space Recommendation Board (SRB) and the Budget Committee. Under the SRB is a Research Facilities Advisory Committee (RFAC). The FWG advises the NIH Director and NIH Steering Committee on the planning, acquisition, development, and use of land and facilities. The NIH Steering Committee was formed to provide advice and recommendations on trans-NIH governance issues. This committee is chaired by the NIH Director, who appoints IC directors as members.6
The project list scored in the spring of 2018 indicates that all projects are the results of recommendations made by the Building and Space Plan Process. The spreadsheet, “B&F Project Prioritization Model for FY
___________________
3 D. Wheeland, P.E., Director, Office of Research Facilities, “Open Discussion with FWG and RFAC,” presentation to the committee, March 20, 2018.
4 NIH Office of Intramural Research, “Facilities Working Group,” https://oir.nih.gov/sourcebook/committees-advisory-ddir/facilities-working-group, accessed March 8, 2019.
5 Ibid.
6 NIH Office of the Chief Information Officer, “NIH Governance Groups,” reviewed December 20, 2017, https://ocio.nih.gov/ITGovPolicy/Pages/NIH-Governance-Groups.aspx.
TABLE 5.1 Point Distribution in the Buildings and Facilities Project Prioritization Model for Fiscal Year 2019-2023 (Total Score of 1,000)
| Criteria | Subcriteria | Points |
|---|---|---|
| Program impact |
Mission criticality and/or intramural program affected for IC project |
260 |
| Project impact |
Number of customers affected |
40 |
|
Building use |
15 | |
|
Returns lease space to government owned |
20 | |
| Functional obsolescence |
Building function to support current, approved program |
330 |
| Facility evaluation |
Building Condition Index |
15 |
|
Regulatory impact |
45 | |
|
Building systems risk of failure impacting life safety and critical mission functions |
222 | |
|
Sustainability |
30 | |
| Total |
Operating cost impact |
23 1,000 |
SOURCE: Dan Cushing, NIH Office of Research Facilities, “Projects Selection and Execution 2018 B&F Proposed Line Item Projects for Prioritization,” presentation to the committee, May 15, 2018.
2019-2023 (Total Score of 1,000),” provided by NIH—hereafter “B&F Prioritization Model”—contains the components and potential point distribution list in Table 5.1. The 1,000-point scoring mechanism for each project/proposal shown in Table 5.1 has the following components: 335 points focused on IC Program Impacts; 330 points focused on Functional Obsolescence; and 335 points focused on Facility Impacts.7 Simply stated, an evaluation with a high score means a potential adverse impact to the program and a greater risk of failure to building system/components including life safety and critical mission functions. Thus, a high score should lead to a high priority for the project to move forward.
The RFAC, the scientific director for remote campuses, and three executive officers review and score the Program Impact section. The Office of Research Facilities (ORF) B&F board reviews and scores the Facility Impacts section. The Functional Obsolescence section is scored by both groups.
Each of the subcriteria showing points in Table 5.1 has value guidance that is used by the scoring committee to select the potential portion of the available points for the subcriteria to apply to each project. As an example, the Facility Evaluation—Regulatory Impact (45 points) has four values:
| • Must be addressed within 2 years | 45 points |
| • Should be addressed within 3-5 years | 30 points |
| • Can be addressed in conjunction with new project | 7 points |
| • No regulatory impact | 0 points |
The specific regulatory issues and the magnitude of the issue, which might be expressed as the cost to correct, are not part of the evaluation. The only subcriterion that uses data is the building CI that results from the condition assessment process.
However, the B&F Prioritization Model does not weigh the key outcome of improved building CI with much importance. The maximum number of points for improving the building CI is 15 out of the 1,000-point total available for a project. Therefore, the condition index improvement, which translates to a reduction in Backlog of Maintenance and Repair (BMAR), represents only 1.5 percent of the total possible project score. The criteria for the 15 points available for the building CI are as follows:
___________________
7 D. Cushing, NIH Office Research Facilities, “Project Selection and Execution,” presentation to the committee, May 15, 2018.
| • CI below 65 or project will increase CI to >90 | 15 points |
| • CI between 65 and 85 or Central Utility Plant | 8 points |
| • CI over 85 or new construction | 0 points |
The U.S. Department of Agriculture (USDA) by contrast uses a degree of portfolio-level analysis of the BMAR to focus the capital investment strategy. The USDA Agricultural Research Service, Capital Investment Strategy, April 2012 (USDA, 2012) provides the ranking of each facility from worst to best based on the CI. All facilities are assigned a priority of 1 to 4 based on the importance of the research programs to the mission. These priorities are systematically evaluated by senior research program leaders. USDA then reviews, portfolio-wide, the combination of the facility’s CI rank with the highest priority research. This analysis drives the decisions on where the capital investment recommendations will focus, considering economic restraints.
NIH Bethesda Campus projects are categorized into three sections (A, B, or C). Section A projects have a complete program, environmental impacts, and cost estimate and are included in the Master Plan. Section B projects are those with incomplete documentation that would otherwise have been required for the projects’ inclusion in Section A. Those in Section C are minimally defined projects. Projects are considered for B&F funding if they have a high score and are in Section A. The timing of when projects progress through the planning and construction process is based on the availability of funds and the completion schedule of other projects.
One example with a low CI, placed in Section B due to an incomplete priority scoring index, is the replacement of Building 12. Building 12, which houses the data center, is slated for replacement in the Master Plan and currently has not been funded while awaiting completion of fiscal year (FY) 2018-2022 Priorities. The CI for the existing building is 51.7, which is extremely low for the campus, and the B&F Priority score for Functional Obsolescence section is currently 165 out of 330 possible points. This score is far less than one would expect for a building with such a low CI and that provides research services that are available to all ICs. Further, the building is at risk due to inadequate utility capacity, including an estimate showing inadequate generator power capacity by 2020, and chilled water-cooling capacity in 2017. A project to increase chilled water capacity has received funding and begun construction. From 2015 to 2017, the high-performance computing (HPC) system, Biowulf,8 has seen a net increase of users for HPC of 78 percent, principal investigators of 53 percent, CPU hours of 345 percent, and storage used of 100 percent. (Biowulf is discussed further in Chapter 3, in the section “Data Science Infrastructure and High-Performance Computing.”) It is surprising that a building with this kind of growing impact on research has not moved forward quickly with appropriate analysis into Section A due to its low CI score and potential infrastructure failures.9
Condition Index Assessment
The condition assessment contractor’s process is to initially gather aggregated system-level information to determine deferred maintenance and capital renewal. The primary focus is to determine the age of each system, compare the age to the industry standard life expectancy for each system and project estimated remaining life based on the comparison (age versus life expectancy), making adjustments to estimated remaining life based on visual condition observations or maintenance histories. This develops a data source that can be updated as systems age and building conditions change. The process includes an update by the contractor on a 4-year cycle based on field observations and updated condition information. System
___________________
8 A. Baxevanis, “BIOWULF High Performance Computing at NIH,” presentation to the committee, May 16, 2018.
9 NIH Center for Information Technology, “High-Performance Computing Services,” https://www.cit.nih.gov/service/high-performance-computing-services.
replacement costs are based on the industry cost estimating source RSMeans.10 The replacement cost of the systems is based on the current capacities and characteristics (in-kind). The costs are adjusted for factors such as geographic location (factors provided by RSMeans) and any factors NIH uses for construction on campus. Each year the BMAR and CI are recalculated based on the updates described above and inflation. The BMAR data provided by NIH includes a report that shows the projected increase in BMAR per year per building.11 The current year BMAR is used to calculate the current year CI, which is used in the project scoring process described above.
The BMAR that results from the assessment approach is used in a limited fashion to develop a small segment of the project scoring process. Approximately two-thirds of the annual B&F appropriation is used for smaller projects in the category of Repairs and Improvements. These projects are developed by the NIH facilities staff with knowledge of the day-to-day operations, as discussed in Chapter 4, in the section “Project Dashboard.” There is not a direct link to the BMAR in the development of these projects.
PLANNING ENVIRONMENT
Long-Range Planning Process
The long-range planning process at NIH is overseen by the NIH Director and driven by the aforementioned FWG and its subcommittees.
The Bethesda Campus Master Plan was issued in 2013 and completed the associated National Environmental Policy Act Record of Decision in 2015. This plan had input from the NIH Director and the FWG and provides guidance to the long-range planning process. It encompasses a number of the Director’s strategic themes for future improvements.12
The rolling 5-year B&F/NEF-Funded Plan described in the previous section includes projects that have been selected via the B&F Prioritization Model. Projects are “generally considered for funding if they score over 500 points” and have complete program, environmental and cost data.13 However, it appears that this threshold is not always used. For example, the FWG has placed a project (Building 40 Lab Addition) on the Projected Timelines with Funding even though it has a score of 250, which is well below the 500-point threshold for funding. This indicates that unrecorded factors must have been considered.
Project timing is dependent on availability of funds and when predecessor projects are complete (if applicable). This plan is reviewed and approved by the FWG.14 Projects seem to originate from those identified in the Master Plan, the Director’s thematic focus areas, functionally underperforming facilities (i.e., low-CI facilities), grass roots (as in the case of Biowulf high-performance computing and its associated facilities’ needs), or programmatically based on specific targets (e.g., the Porter Neuroscience Research Center project). In a more prospective vein, the IRP in June 2015 issued an implementation plan (NIH ACD, 2015) responding to the Advisory Committee to the Director report to the NIH Director on Long-Term Intramural Research Program Planning (NIH ACD, 2014). Both the implementation plan and the report look forward in terms of new areas of investigation and can inform the long-range facilities planning process.15
___________________
10 RSMeans “provides accurate and up-to-date cost information that helps owners, architects, engineers, contractors and others to precisely project and control the cost of both new building construction and renovation projects.” See http://www.rsmeans.com.
11 NIH Office of Research Facilities, “Running BMAR Tallies by Year and Building,” sent via e-mail, February 22, 2018.
12 D. Wheeland, NIH, “NIH Bethesda Master Plan,” presentation to the committee, March 20, 2018.
13 D. Wheeland, NIH, “Buildings and Facilities Scoring 2017,” presentation to NIH Facilities Working Group, June 14, 2017.
14 D. Cushing, NIH Office of Research Facilities, “Annual Budgets: Buildings and Facilities, Facilities Maintenance, and Process,” presentation to the committee, March 20, 2018.
15 M. Gottesman, M.D., “Facilities vis-à-vis Scientific Mission,” presentation to the committee, May 15, 2018.
As noted in the previous section, the B&F Prioritization Model sorts proposed projects into three tiers. Projects on the B&F Section A list can be funded using the baseline B&F funding, nonrecurring expense funds provided by the Department of Health and Human Services (HHS), specific emergency allocations (such as Biodefence [2003] and the American Recovery and Reinvestment Act [ARRA, 2009] from Congress)16 or one-time increases for major individual capital projects as line items approved by Congress (such as Building 50). Projects also can be funded using IC appropriated funds subject to a $3.5 million cap on individual projects and $45 million NIH-wide cap per year—the so-called special authority discussed in Chapter 4. Facilities’ nonemergency maintenance projects over $75,000 are handled by ORF using B&F funding. The B&F/NEF-Funded 5-Year Plan is reviewed annually by HHS. Project proposals that are considered for approval must have a Facility Project Approval Agreement.
There is no external (i.e., outside NIH or federal government) input into the long-range planning process. All the committees consist of senior employees of the ICs and Office of the Director. It is unclear if there is input from NIH personnel at more junior levels into the process.
Constraints and Challenges
As with most organizations, capital planning for the long range at NIH faces a number of challenges and constraints, some of which are unique to the Bethesda Campus:
- B&F funds have been essentially static for the past 20 years (around $128 million per annum), with a 5-year expiration (not X-year, or nonexpiring); this level of funding has not allowed the organization to keep up with inflation or to pool funding for larger capital expenditures. The B&F appropriation increased to $200 million for FY 2019.
- Over the past two decades, the funding stream has been sporadic for large capital expenditures from either special authority or through one-time appropriations (e.g., ARRA in 2009) or when certain projects are picked up by Congress (Biodefense in 2003).17 This sporadic funding stream does not allow a smooth and logical progression of projects. In some cases, the planning for a facility becomes obsolete before it is funded, leading to inefficiency. This also tends to lower morale among those who are performing the planning.
- The campus has a large backlog of deferred maintenance items, which at times lead to emergencies at specific facilities, and a continued growth in operation and maintenance costs at those facilities. It does not appear that the maintenance backlog is addressed in a systematic manner or is tied to the long-range plan. In other words, if the long-range plan is to demolish and replace an existing facility, one can question how decisions are made regarding further significant investment in that facility. Nor does it appear that ORF has sufficient flexibility in how it utilizes the B&F account to implement a program of preventative maintenance such as might decelerate the growth in BMAR.18 When the funding window for a project continues to be pushed back, the facility continues to degrade. An example of this is the Building 14/28 complex (vivarium), which may impact the ability to continue its accreditation, while operations and maintenance costs escalate. For example, in the past 5 years NIH has spent in excess of $19 million for renovations on this complex.19 (See Recommendation 4.3.)
___________________
16 D. Cushing, NIH Office of Research Facilities, “Annual Budgets: Buildings and Facilities Maintenance and Process,” March 20, 2018.
17 Ibid.
18 Studies of test portfolios of F&I show a positive net-present value for preventative maintenance. See, for example, Jones Lang Lasalle, “Determining the Economic Value of Preventive Maintenance,” https://gridium.com/wp-content/uploads/economic-value-of-preventative-maintenance.pdf, accessed July 24, 2019.
19 NIH Office or Research Facilities, “20180927 Bldg 14 28 and 12 obligations last five years” via e-mail September 27, 2018.
- The rapidly changing technological innovations and opportunities in medical research that NIH should pursue as part of its mission makes its ability to perform long-range planning more difficult. The solution to this dilemma is to build modularization and flexibility into all facilities looking at long-range needs, perhaps with the idea of turning over a majority of each new facility every 5 to 10 years to new requirements.
- The diverse mission requirements of 27 IC are a challenge when trying to balance the requirements of NIH, and the needs of the individual IC. The challenge of addressing agreements on expenditures is solvable, but requires a tremendous amount of communication, education (e.g., expenditures on shared core utilities), and input back into long-range plans. The long-range plan must be aligned to the strategic direction of NIH collectively and vice versa, taking a proactive approach.
- As discussed in Chapter 4, funds appropriated to the ICs, up to $3,500,000 per project, can be used to cover costs associated with altering, repairing, or improving NIH facilities. The funding ceiling for all ICs collectively cannot exceed $45,000,000. Historically, an average of roughly $35,000,000 has been spent on these types of projects.20 This number is admirable; however, it does leave some funding unspent, requires significant coordination to provide the funds for projects (as the moneys are held by the ICs and have to be released by them, which may generate a conflict of objectives), and reduces the amount of research that ultimately can be accomplished.
ASSESSING THE NEED FOR RENOVATION, REPLACEMENT, OR ADAPTIVE REUSE
The Utility of the NIH Condition Assessment and B&F Prioritization Model
The Government Accountability Office identified the following leading practices to manage deferred maintenance and repair backlogs:21
- Establish clear maintenance and repair objectives and set priorities among outcomes to be achieved.
- Identify assets that are mission-critical and mission-supportive.
- Conduct condition assessments as a basis for establishing appropriate levels of funding to reduce any deferred maintenance and repair backlog.
- Establish performance goals, outcome baselines, and performance measures.
- Identify the primary methods to be used for delivering maintenance and repair activities.
- Employ models for predicting the outcome of investments, analyzing trade-offs, and optimizing among competing investments.
- Align real property portfolios with mission needs; dispose of unneeded assets.
- Identify the types of risks posed by lack of timely investment.
- Structure budgets to identify funding allotted (1) for maintenance and repair and (2) to address any backlog of deferred deficiencies.
While NIH has a condition assessment process, not all of the leading practices are followed. As it relates to the capital investment strategy, it is not clear that NIH establishes performance goals, outcome baselines, and performance measures associated with projects. NIH does not predict the outcome of the investment and measure the success. A sampling of project documents did not show current operating costs and the anticipated new operating costs by square foot to set a benchmark to measure the success of the project in
___________________
20 D. Cushing, NIH Office of Research Facilities, “Annual Budgets: Buildings and Facilities Maintenance and Process,” presentation to the committee, March 20, 2018.
21 M. Armes, U.S. Government Accountability Office, “Federal Real Property Management Issues,” presentation to the committee, March 21, 2018.
reducing those costs after project completion. Based on the information provided, NIH’s use of the condition assessment information is very limited. The assessment data are used to develop the CI to assist in the score of a project and along with the BMAR provide information that supports reporting needs across the portfolio. However, the actual use of the assessment data in the planning process was not demonstrated.
The condition assessment provides little impact on the project scoring process as described and weighted. Improving the building condition index is described in the Master Plan as one of the key outcomes. However, the criteria for selecting a value uses only the change in CI, which shows that the results of the condition assessment has little to no utility in identifying facilities with the most need. As noted above, the committee received a presentation of the condition assessment data and CIs showing that Building 12 was in very poor condition (CI of 51.71) and recommended for demolition by the Master Plan Subcommittee22 as part of a larger scheme in that area of the campus to bring leased lab space onboard and to replace and modernize waste transfer and storage facilities (NIH ORF, 2013, pp. 5-20 and 5-24). Building 12 has recently had a significant investment, including one of $37 million for an uninterruptable power system (situated outside the building and thus movable), $5 million for increased cooling capacity, and $2.4 million for miscellaneous improvements.23 (This is in addition to investment in the information technology that resides in Building 12, part of NIH’s move into high-performance computing.)24 Despite what the BMAR and CI might imply about a building’s viability, the needs of the research program—for high-performance computing in this case—indicates that NIH is making significant investments in buildings recommended for demolition by the Master Plan.
The CI is a relative indicator of the condition of a facility when compared to similar facilities. The CI by itself does not discern between the criticality of the deferred maintenance or the system that is impacted in the facility. Therefore, one facility could have a CI that identifies that it is in worse condition than another. However, the facility with a better CI may have deferred maintenance concentrated in critical systems (e.g., HVAC, electrical, plumbing, roof) and thus represent greater risk. The NIH has not provided any portfolio-wide analysis showing a more in-depth look at the data and how it could inform their processes and plans.
As discussed in Chapter 4, in the section “Risk to Research and Patient Care Created by Outages and Disruptions,” NIH performed an analysis of risk associated with the Building 10 complex for some critical systems (i.e., mechanical, electrical, and distribution) and for the function and amount of space.25 This appears to be a specific example of using the condition information for the Building 10 complex to analyze risk. A formalized risk assessment using this approach could be extended to other facilities in the portfolio.
CI is calculated based on current year deferred maintenance and current replacement value. However, the planning process is at best a 5-year timeline. The condition assessment contractor hired by NIH provides reports that project the BMAR changes by year for the next 10 years. Therefore, the annual change in CI can also be projected. The committee believes that the current and projected CI could be used in the project scoring process to account for the length of time associated with the planning and funding process and any potential significant changes in BMAR during that period. This process would further define and prioritize the projects to which the $600 million suggested in Recommendation 4.1 would be applied.
The condition assessment process addresses the projected replacement of systems based on age and adjusted according to condition observations. The condition assessment process generates the BMAR and CI. The CI (15 points—1.5 percent) is the only data driven factor in the Facility Evaluation criteria in the B&F Prioritization Model (see Table 5.1). Other facility issues such as accessibility, environmental concerns, code compliance, operating cost savings (e.g., energy savings), and sustainability are not quantified by other specialized inspection services or studies. The B&F Prioritization Model uses the
___________________
22 D. Wheeland, NIH, “Bethesda Campus Master Plan,” presentation to the committee, March 21, 2018. Also see NIH ORF (2013), p. 5-29.
23 NIH, “1-10-19 Questions and Answers with Table,” via e-mail, January 11, 2019.
24 Stephanie Hixson, NIH, “Bioinformatics and High-Performance Computing,” presentation to the committee, May 16, 2018.
25 D. Cushing, NIH Office of Research Facilities, “Capital Projects on Deck, Shovel Ready & Emerging,” presentation to the committee, March 20, 2018.
subjectivity of the committee to score regulatory impact, sustainability, and operating cost impact rather than quantifiable measures that could drive the process such as the change in square foot operation costs potentially achieved by the project.
The functional obsolescence values in the scoring process subjectively rate how building systems support current program(s) located in the building. The analysis of functional obsolescence could be included in the condition assessment process to identify and quantify the requirements.
Committee’s Assessment
The NIH has developed many large construction and renovation projects based on the Master Plan and there are several system replacement projects on the funded project list, including the fire alarm reliability for the Clinical Center (CC) and emergency power to assure chilled water, which are more limited in scope. The funded projects and the projects in the planning phase are all needed. However, the committee was not able to discern that a specified standard process is used to determine which projects address the most important needs of the campus.
Throughout the committee’s interactions with NIH staff and in the various presentations to the committee, a number of recurring themes were voiced. These included the poor condition of the animal facilities, the lack of infrastructure to support data analytics and computing needs, constraints in the clinical facilities, the challenges of managing campus infrastructure projects, and the goal of reaching a CI for all facilities at the Bethesda Campus of 90 or above. Site visits to facilities by committee members confirmed the challenges facing NIH in these regards and their mission criticality. Chapter 3 of this report provides a description of the animal facilities, data infrastructure, and CC. Some examples of the challenges they face are provided below.
The animal facilities housed in Buildings 14B to 14H and 24 are contiguous, and due to their age and deteriorated condition could become a licensing problem absent appropriate intervention. These buildings house animals that are not located within a laboratory building and have a significant impact on the success of research across many institutes. The Division of Veterinary Resources manages most of these buildings. The average CI for these buildings is 78, and all but one is over 60 years old. Replacement of this complex of buildings will provide the opportunity to rightsize capacities, provide a modern mechanical-electrical-plumbing system, allow for redundancy in mechanical and electrical systems, and increase reliability and reduction in maintenance and energy costs. These facilities continue to experience critical failures in building performance—for example, during the weeks of December 28, 2017, to January 10, 2018, failures included seven days of HVAC failure in Building 14D, low/high temperature failures, and floods in surgery.26 The lack of essential mechanical infrastructure upgrades prevents the program from meeting basic NIH needs for the largest animal holding facility on campus. The long-term plans include replacement of the facility as part of the Center for Disease Research (CDR). The 2013 Comprehensive Master Plan—Bethesda Campus envisaged the North Development of the CDR for the existing 7 and 9 building sites, although the NIH Office of Research Facilities advises that the location of the CDR is being reevaluated.
The pursuit of this project should include review of all options for housing animals. NIH needs not only to consider replacement of the current Building 14/28 complex but also to look at other options. These include the acquisition of facilities beyond the current campus that would have less impact on future programmatic growth for other key NIH programs and consideration of third-party solutions that include leasing of existing facilities or outsourcing animal facilities to a third party. These kinds of options are often considered by other biomedical research organizations, and it is not assumed that one option is more viable than another.
Another project impacting the mission of many if not all NIH institutes is the computer center (Building 12 complex). As discussed earlier in this chapter, utilization of the computer center is growing dramatically,
___________________
26 S.M. Roberts, R.A., NIH, “Animal Facilities,” presentation to the committee, March 20, 2018.
and the current building has reached its limits for infrastructure needs. The need for a new facility includes the following criteria:
- Co-location of experts in the computational, statistical, and data sciences;
- Replacement of obsolete infrastructure to empower mission-critical computational and data science; and
- Support of current and emerging science with high-performance/flexible building infrastructure.
Like the animal facility, this project should look at all alternatives as well, but is faced with obstacles that are unique to high-speed computing. A location off site may not be practical due to high-speed dedicated data lines located under public rights-of-way, which can be costly to install and maintain. A formidable challenge for NIH is ensuring security of the data and site, which may make a remote location impractical. Another possibility is to contract with a third party to build and manage a new computing facility on campus.
Building 10, which houses the CC, was originally constructed in 1953, with a number of additions in the interim—including the new Mark O. Hatfield Clinical Research Center constructed in 2005. Portions of the Building 10 complex assigned to the CC have experienced serious deferred maintenance failures impacting mission accomplishment. Parts of the facility, including the existing surgical center, are functionally obsolete. Its ability to handle an increasing load of outpatient activities is limited and problematic. As a result, a number of the projects in Section A of the B&F 5-year plan are focused on improving the CC capabilities and functionality. Over $8.3 million in funds appropriated to ICs—applying the special authority of up to $3,500,000 per project—were used to cover costs associated with altering, repairing, or improving CC facilities during the past 5 years.27 As discussed in Chapter 4, in the section “Project Dashboard,” NIH has a listing of over 400 repair and improvement projects for future funding.
In FY 2017, $212 million of BMAR was attributable to the CC.28 Given that the CC is a “unique in the world facility” that provides strategic leverage for NIH and supports the ability of a large number of its ICs to accomplish their missions, failure of any CC capabilities is problematic to NIH.
The committee believes that NIH should continue its efforts to enhance campus infrastructure. Since the formation of a dedicated Utility Distribution Branch in 2013 to assess the current condition of the distribution system and respond to needed repairs and look long term for future projects (replacements), the campus has completed numerous commendable improvements. Examples of completed or underway projects include replacement of chillers in the Central Utility Plant, addition of emergency power generation for chilled water, electrical power reliability for the CC, a new chilled water storage facility (the Thermal Energy Storage system; Building 34 in Figure 4.2), and chilled water monitoring stations in the Central Plant for “real time” data on system performance. The committee believes efforts by this group should continue and be supported with sufficient funding to ensure improved systems reliability; however, these should be evaluated utilizing the Mission Dependency Index as discussed below.
Using CI for Decision Making
Comparable Methodologies
The contractor that NIH uses to perform the condition assessment and maintain the database of that information has several federal agency clients, as well as many research colleges and universities, hospital systems, and private research businesses. The process they use is very similar in nature to the primary approach that the Department of Defense (DoD) and the individual branches of the military use.
___________________
27 NIH, “1-10-19 Questions and Answers with Table,” via e-mail, January 11, 2019.
28 NIH Office of Research Facilities, “The Clinical Center Complex: History of Architectural and Engineering Development,” handout to the committee, March 20, 2018.
The BUILDER™ Sustainment Management System (SMS) is a web-based software application developed by ERDC’s [Engineering Research and Development Center’s] Construction Engineering Laboratory (CERL) to help civil engineers, technicians and managers decide when, where and how to best maintain building infrastructure. Because building assets are so vast and diverse, a “knowledge-based” philosophy drives the BUILDER™ SMS process. The process starts with the automated download of real property data, and then a more detailed system inventory is modeled and/or collected which identifies components and their key life cycle attributes (e.g., the age and material). From this inventory, Condition Index (CI) measures for each component are predicted based on its expected stage in the life-cycle.29
Using Condition Assessment Data and CI in Decision Making
NIH has developed many large construction and renovation projects based on the Master Plan from 2013 (fully described in Appendix H) and the rolling 5-year B&F Plan30 that is prepared annually and includes funded projects.31 There are several system replacement projects on the funded project list, including the fire alarm reliability for the CC and emergency power to ensure chilled water, that are more limited in scope. The committee accepts that all the funded projects, as well as the projects in the planning phase, are needed; however, the committee was unable to discern that a recognized and standardized process was used to determine whether and to what degree these projects address the most important needs of the campus.
The strength of using CI metrics is in identifying the buildings in poor condition in a significant portfolio of facilities. The National Park Service recognized that there are limitations to the CI as the only indicator of condition in developing their Life Cycle Business Practices (NPS, 2006). The CI is simply a relative indictor of condition within a group of homogeneous facilities. The wide variety of facility types combined with the significant level of the deferred maintenance required a more focused use of the condition assessment data. NPS developed a critical systems approach, including priority criteria for each deficiency that are based on risk to the facility and safety (minor, serious, and critical). Additionally, NPS identified the critical systems for each asset type. Therefore, the serious and critical deficiencies within critical systems informs the development of projects.
The NPS condition assessment identifies work required for facilities to comply with legislatively mandated requirements of accessibility, fire/structural, life safety, and code compliance. The existence and the cost of correcting these issues are considered during project development and scoring.
As described above, in the section “Process by Which Projects Are Planned and Evaluated,” there is an opportunity for NIH to utilize a Mission Dependency Index (MDI) to compare one building to another to prioritize their needed improvements based on “mission impact.” Strategically, this is particularly important when choices must be made between individual buildings for limited B&F funding. The same methodology can be used in the CI analysis by recognizing that not all infrastructure systems that support a building are equal—some may have a more serious impact on successful operation of the building. The two methodologies’ linkage is simple—CI considers the probability of infrastructure failure and MDI identifies the severity of the failure. This would be a way to prioritize the findings utilized in the Backlog of Maintenance and Repairs to allow a more strategic focus on system expenditures and repairs.
Likewise, the committee believes that efforts should be made to utilize the Mission Dependency Index concept to develop data across the Bethesda Campus portfolio to quantify the requirements to upgrade campus-wide facility and infrastructure systems to meet current and future programmatic needs. This then
___________________
29 See https://www.erdc.usace.army.mil/Media/Fact-Sheets/Fact-Sheet-Article-View/Article/476728/builder-sustainment-management-system/.
30 D. Cushing, NIH Office of Research Facilities, “Capital Projects: On Deck, Shovel Ready & Emerging,” presentation to the committee, March 20, 2018.
31 D. Cushing, NIH Office of Research Facilities, “Projects Selection and Execution 2018 B&F Proposed Line Item Projects for Prioritization,” presentation to the committee, May 15, 2018.
can guide the Utility Distribution Branch team in their program (see the above section, “The Utility of the NIH Condition Assessment and the B&F Prioritization Model”).
FINDINGS AND RECOMMENDATIONS
Finding: All federal agencies are required to maintain a facility Condition Index as part of their real property asset management. Federal agencies such as the U.S. Army Corps of Engineers, NASA, and the three federal security labs referenced in this chapter explicitly calculate the cost of facility disruptions in the prioritization of capital assets. NIH does not appear to do so currently.
Finding: NIH does not appear to have taken advantage of the capital asset management expertise existing in other federal agencies that manage large capital programs. NIH could utilize the expertise found in these agencies to improve its practices and procedures.
Finding: Building 12 housing the NIH computer center, the Building 14/28 Complex housing animals, and the Building 10 CC provide resources that are available to all institutes and centers, and any temporary loss of their functionality due to facility failures imposes a significant negative impact on operations and mission accomplishment. While the projects involving these facilities appear to be important, the committee believes that their priority should be confirmed by use of a model that is more objective-based.
Finding: While projects are generally considered for funding if they score over 500 points, there is an example of a project in Section A of the 5-Year NIH Buildings and Facilities Master Plan with a score of 250 points (Building 46A, Vaccine Research Center Addition). This leaves the impression that there are unrecorded subjective factors that came into play during the ranking process.
Recommendation 5.1: NIH should revise its Building and Facilities (B&F) prioritization model so that a significant portion of the 1,000-point scoring system (no less than one-third of the total points) includes the Condition Index and Mission Dependency Index as objective parameters. Using this revised model, NIH should reassess all current projects in the 5-year B&F plan. The balance of the $1.3 billion of funding (i.e., $600 million) should be prioritized based on this assessment. This assessment could also be used to determine the annual required funding set aside.
Recommendation 5.2: NIH should utilize the changes in the Building and Facilities prioritization model to complete an analysis of projects to modify or replace Building 12, the Building 14/28 complex, and various active or planned projects to renovate or replace portions of Building 10 occupied by the Clinical Center. If the analysis supports a high priority for these projects, then NIH should continue with efforts to move forward as quickly as possible with these projects.
Recommendation 5.3: NIH should seek out the federal agencies referenced in this report, along with other similar agencies, to determine if there are best practices that it can utilize. NIH should consider regular (e.g., quarterly) engagements with these agencies to review its Capital Asset Management Program, as well as how the engagement of key individuals from the institutes and centers (at all levels of the organization who are impacted by the program) and the private sector could enhance the success of NIH projects.
ANNEX 5.A: PREVENTATIVE MAINTENANCE MEASURES AND LIFE CYCLE COST ANALYSIS
Preventative Maintenance Measures
While NIH staff members spent little time on integration of maintenance activities into long-range planning during their presentations to the committee, it is worth mentioning that this may be an opportunity if NIH’s current efforts are not rigorous in this regard. Integration of maintenance into long-range planning would allow better optimization of funding opportunities, and at the same time inform the planning process from a prioritization perspective.
Underscoring the importance of preventative maintenance, experts have judged that 2 to 6 percent of an annual operating budget should be allocated to preventative maintenance to minimize a facility’s rate of degradation.1 Preventive maintenance both saves money and forestalls the need to replace a facility—which might otherwise require capital and time owing to time needed for evaluation and design to funding and implementation. Preventive maintenance especially helps reduce building failure and poor conditions that can negatively impact mission critical building operations, energy efficiency and employee morale.
According to one analyst (Hemmerdinger, 2014, p. 4), “such a comprehensive operations and maintenance program for energy and water systems, based on proactive, predictive maintenance and analytics, can save up to 20 percent per year on maintenance and energy costs, while increasing the projected lifetime of the building by several years.” The report, Operations and Maintenance Best Practices: A Guide to Achieving Operational Efficiency (FEMP, 2010, p. 5.4), Release 3.0, indicates that savings can be even greater for the best in class Predictive Maintenance programs:
- 10-times return on investment
- Reduction in maintenance costs: 25-35 percent
- Elimination of breakdowns: 70-75 percent
- Reduction in downtime: 35-45 percent
- Increase in production: 20-25 percent
Predictive maintenance can incur higher initial costs, for example, owing to funds needed for new software for capturing data on the condition of systems and equipment. It is further likely that additional staff or contractors would be required to make the needed repairs with attendant increase in maintenance costs. Ideally, the organization implementing predictive maintenance would have staff with the technical expertise to analyze the data coming out of the building management system and compare that information against optimal performance benchmarks. It is envisaged that using the predictive maintenance approach, repairs and improvements would be prioritized based on potential cost and mission impact. Supporters of this approach believe that predictive maintenance can extend the lifetime of a building by several years and deliver ancillary benefits such as “increased safety from properly maintained equipment, greater comfort and productivity for occupants, and better compliance with efficiency requirements” (Hemmerdinger, 2014, p. 7).
Designing for Minimum Life Cycle Costs
As with the topics of preventive maintenance measures and long-range planning, there was little discussion during presentations to the committee and follow-up question and answer sessions regarding life cycle cost analysis. This concept is integral to the Department of Defense (DoD) energy and nonenergy projects, as well as being outlined in guidelines by the Office of Management and Budget (OMB) Circular A-91.
___________________
1 P.S. Kimmel, AIA, IFMA Fellow, 2009, IFMA Benchmarking Report.
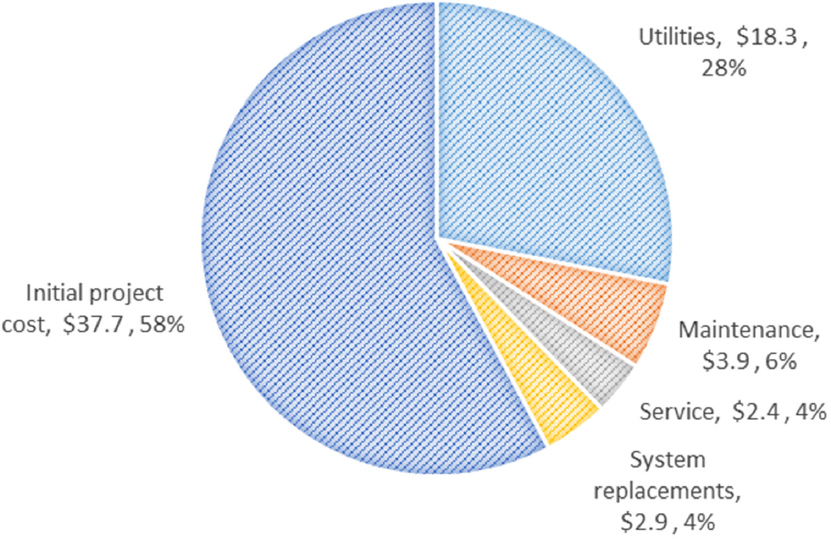
Life Cycle Cost Analysis (LCCA) “is a method of evaluating the cost-effectiveness of project design decisions.” LCCA
Properly accounts for many project cost variables. These include a wide variety of project costs (e.g., construction, operations, maintenance, replacements, utilities, etc.) [Figure 5.A.1]. They also encompass the time value of money, including a project-specific discount rate, inflation, and cost escalations for a variety of goods and services. … Performing an LCCA study involves (1) establishing objectives for the analysis, (2) determining the criteria for evaluating alternatives, (3) identifying and developing design alternatives, (4) gathering cost information, and (5) developing a life cycle cost for each alternative. (Stanford University, 2005, p. 12)
As described in the Whole Building Design Guide (WBDG) series of documents,2
LCCA can be applied to any capital investment decision in which relatively higher initial costs are traded for reduced future cost obligations. It is particularly suitable for the evaluation of building design alternatives that satisfy a required level of building performance but may have different initial investment costs, different operating and maintenance and repair costs, and possibly different lives. LCCA provides a significantly better assessment of the long-term cost-effectiveness of a project than alternative economic methods that focus only on first costs or on operating-related costs in the short run.
___________________
2 Sieglinde Fuller, NIST, September 19, 2016, “Life-Cycle Cost Analysis (LCCA),” http://www.wbdg.org/resources/life-cycle-cost-analysis-lcca, accessed March 8, 2019.
The WBDG further notes that3
LCCA can be performed at various levels of complexity. Its scope might vary from a “back-of-the-envelope” study to a detailed analysis with thoroughly researched input data, supplementary measures of economic evaluation, complex uncertainty assessment, and extensive documentation. The extensiveness of the effort should be tailored to the needs of the project.
WBDG further notes that for OMB projects,4
Office of Management and Budget (OMB) Circular A-94—Guidelines and Discount Rates for Benefit-Cost Analysis of Federal Programs, October 1992, applies to building-related benefit-cost or cost-effectiveness analyses of federal programs or policies that are not primarily concerned with energy or water conservation or renewable energy projects. Appendix C of Circular A-94, updated annually in February, provides the OMB discount rates.
LCCA, and likewise for Federal Energy Management Program (FEMP) projects5
The Federal Energy Management Program (FEMP) has published life-cycle costing rules and procedures [Code of Federal Regulations, Title 10, Part 436, Subpart A]. These FEMP rules are consistent with OMB rules. They are to be followed by all federal agencies, unless specifically exempted, in evaluating the cost-effectiveness of potential energy and water conservation projects and renewable energy projects for federally owned and leased buildings. NIST Handbook 135, Life-Cycle Costing for the Federal Energy Management Program, explains and amplifies the LCC rules of FEMP. The Annual Supplement to Handbook 135, Energy Price Indices and Discount Factors for Life-Cycle Cost Analysis [NIST, 2017b], updated annually on April 1, provides the FEMP discount rates. The same publication contains tables of discount factors for time periods up to 30 years, using either the OMB or FEMP discount rate. The FEMP discount factors also include the most recent energy price escalation rates projected by the Energy Information Administration (EIA). The discount factors are embedded in BLCC and other federal LCC computer programs.
For the DoD,6
The Tri-Services Memorandum of Agreement (MOA) on “Criteria/Standards for Economic Analyses/Life-Cycle Costing for MILCON Design” provides the guidelines for LCCA for DoD energy and non-energy projects.7 These guidelines are consistent with FEMP and OMB guidelines. However, the MOA recommends (but does not require) that cash flows are discounted from the middle of each year rather than from the end of each year as are cash flows of FEMP and OMB projects.
___________________
3 Ibid.
4 Ibid.
5 Ibid.
6 Ibid.
7 U.S. Army Corps of Engineers, U.S. Air Force, and U.S. Navy Facilities Command, March 18, 1991, “Memorandum of Agreement on Criteria/Standards for Economic Analyses/Life-Cycle Costing for MILCON Design,” https://www.wbdg.org/FFC/DOD/dod_moa_lcca.pdf.
















