
4
Implementation of Precision and Personalized Nutrition
Presenters in this session of the workshop provided academic, regulatory, and industry perspectives on opportunities and challenges in the implementation of precision and personalized nutrition. Robin McKinnon, U.S. Food and Drug Administration (FDA), moderated the session’s six presentations and an ensuing panel discussion.
WILL PRECISION NUTRITION HELP IN ACHIEVING GREATER HEALTH EQUITY?
Christina Roberto, University of Pennsylvania, discussed challenges to the potential of precision nutrition to achieve greater health equity. She began by disclosing that her answer to the question in her presentation’s title was a skeptical “maybe.” Roberto stressed that precision nutrition has tremendous potential to offer people targeted guidance based on their individual disease risks and biological responses to diet. At the same time, she asserted, while the idea of being able to provide tailored nutrition advice to individuals is appealing, doing so requires understanding the complex interplay among biological factors, food environments, and other systems-level forces that affect health (Rodgers and Collins, 2020). Although these factors are acknowledged in discussions of precision nutrition, she argued, those conversations tend to focus on individual-level factors. Roberto emphasized the importance of broader thinking because those factors interact with many environmental- and systems-level forces that influence food choices.
Roberto provided an example of environmental- and systems-level effects via maps indicating differences in life expectancy in different neighborhoods of Philadelphia. She pointed to 20-year gaps in life expectancy between some neighborhoods distinguished by income levels and population demographics.1 These gaps are not all diet-driven, she maintained, but diet-related chronic diseases contribute to disproportionate rates of chronic disease and mortality in low-income neighborhoods. According to Roberto, this observation highlights the importance of applying precision nutrition in a way that does not widen income and racial/ethnic disparities.
Roberto described “a vicious cycle of unhealthy dietary habits” whereby environmental drivers of food intake exploit biological, psychosocial, and social and economic vulnerabilities that contribute to overconsumption of unhealthy foods, driving preferences and demand for those foods (Roberto et al., 2015). She pointed out that nearly two-thirds of U.S. adults have a diet-related chronic disease, and many people do not adhere to dietary recommendations—even simple messages, such as “eat more fruits and vegetables”—that have been consistent for decades. On a scale of 0–100, where 100 indicates adherence to all food group and nutrient intake components of the Dietary Guidelines for Americans, Americans have fluctuated between a score of 56 and 60 each year since at least 2005 (USDA and HHS, 2020). Roberto expressed her doubt that targeted nutrition advice will solve that problem because lack of knowledge is not the only and often not the main barrier to healthful eating.
Roberto discussed the challenges of communicating nutrition messages to the public and achieving behavior change. Beginning with an explanation from basic psychology, she highlighted that people have limited memories and that it takes effort to process information. She explained that psychologists tend to think about two systems with which people think and make decisions and judgments: system 1 comprises fast, automatic, effortless actions based on associations and emotions; system 2 comprises slow, controlled, effortful actions based on reason and logic (Kahneman, 2003). She pointed out that most food decisions are made with system 1 and shared a research example to illustrate human limitations in terms of recalling and implementing nutrition messages.
In Roberto’s example, researchers assessed the memorability and actionability of the personalized guideline from the 2005 food pyramid (“MyPyramid”), which a person could generate from a website to learn
___________________
1 From Mapping Life Expectancy: Philadelphia, available here: https://societyhealth.vcu.edu/work/the-projects/mapsphiladelphia.html (accessed October 11, 2021).
how many servings from each food group should be eaten daily (Ratner and Riis, 2014). They compared MyPyramid with the Half Plate Guideline, a simple message instructing people to fill half their plate with fruits and vegetables. Study subjects were first assessed for their motivation to follow nutritional guidelines, and were then randomized to view either the MyPyramid or Half Plate message. When asked to provide open-ended recall immediately after viewing the message, Roberto reported, 85 and 19 percent, respectively, recalled Half Plate and MyPyramid perfectly. Motivation to follow the Half Plate Guideline was higher than motivation to follow MyPyramid among both the low- and high-motivated groups as assessed at baseline. When the study was replicated and outcomes were assessed 1 month later, Roberto continued, 62 and 0.7 percent, respectively, recalled the recommended food group servings in Half Plate and MyPyramid correctly (Riis and Ratner, 2011). In Roberto’s view, a key takeaway from this research is that simple guidelines have tremendous recall advantages. She acknowledged that the recall burden is reduced with technologies that can remind people of advice they have been given, but expressed concern about increasing population disparities by relying on such technologies, given that mobile devices and health apps are most likely to be used by younger, educated women (Carroll et al., 2017).
Roberto also raised concern about precision nutrition being exploited for profit. She contended that food products are already exploited in this way, using the example of a fruit juice drink bearing multiple marketing messages, such as nutrient content claims, natural ingredient claims, and fruit and vegetable imagery. On the topic of profits, Roberto suggested that online shopping could be a positive or negative source of personalized marketing of foods. She noted that some retailers are already organizing their offerings by dietary preferences and using customers’ browsing and purchasing data to recommend similar products, adding that this can be beneficial if the products are healthy foods but could exacerbate poor eating habits if the foods are unhealthy.
Roberto ended her remarks by referring to a framework for achieving health equity (Figure 4-1), which she proposed incorporating into the precision nutrition conversation. This framework, she explained, emphasizes the importance of developing interventions that aim to increase healthy options and/or reduce deterrents to unhealthy behaviors while also incorporating considerations related to social disadvantage and social determinants of health (Kumanyika, 2019). She appealed for “meeting people where they are” and pursuing strategies for making precision nutrition tools accessible for people with few resources.
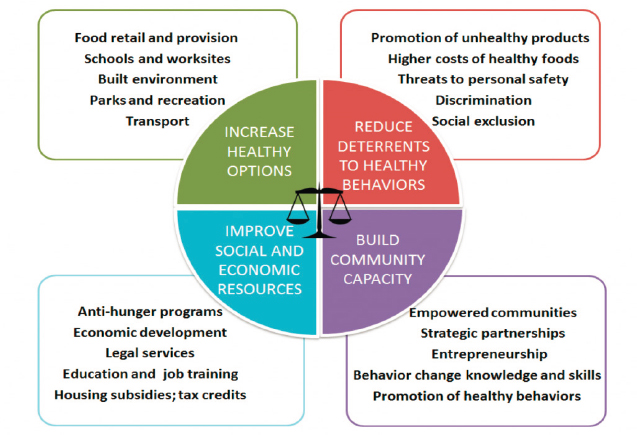
SOURCES: Presented by Christina Roberto on August 12, 2021; Kumanyika, 2017.
CHALLENGES TO IMPLEMENTING PRECISION NUTRITION
Peter Lurie, Center for Science in the Public Interest, prefaced his presentation by expressing excitement about the science underlying precision nutrition technologies, while cautioning that exciting science alone is not enough to improve public health. He argued that government has a role in supporting translation of the science into public health gains, but contended that current structures available to the government are inadequate to that task. Lurie supported this view by describing the history of precision medicine, whose promise, he stated, has been impeded for several decades. According to Lurie, some of that promise is finally being realized, but historically, the hype has exceeded what has been delivered.
Lurie suggested that one way to measure the increased focus on precision medicine at the FDA is by examining a category of products called companion diagnostics—diagnostic tests used as a companion to a therapeutic drug, biologic, or device. He noted that most FDA-approved companion diagnostic devices are for various cancers, and that these diagnostics can fall into a “regulatory vacuum” at the agency. He added that this is the case in particular for a subset of diagnostics called laboratory-developed tests (LDTs), a type of test for which the sample is collected in one location and submitted to another location for analysis.
According to Lurie, the FDA has exercised its enforcement authority over LDTs infrequently, in part because of industry assertions that they are subject to adequate oversight under the Comprehensive Laboratory Improvement Act (CLIA). But Lurie pointed out that the CLIA regulates laboratories, not tests, which he characterized as a problem that leads to a number of deficiencies in LDT oversight: a lack of evidence supporting the clinical validity of tests (i.e., how to use, interpret, and label a test and determine for whom it is indicated); inadequate adverse event reporting; lack of premarket review of performance data; unsupported manufacturer claims; inadequate product labeling because the focus is on the laboratory instead of the test; and an uneven playing field that he said results when some companies get premarket approval from the FDA and address these deficiencies while others do not. In 2020, the Secretary of Health and Human Services issued a memorandum stating that LDTs must be addressed individually in separate regulatory actions (to include Federal Register notices and comment periods), which Lurie maintained for practical purposes “is another way of saying there will be no regulation at all.”
Lurie then gave three examples from what he said is a longer list of problematic LDTs, starting with an ovarian cancer screening test that detected a genetic variant thought to increase cancer risk and predict therapeutic response. A large independent study failed to confirm the variant’s association with the suspected mutations, he recounted, meaning the test’s detection of the variant’s presence could effectively be a false positive that could lead to unnecessary surgery. A second problematic LDT, he continued, is a collection medium for the human papillomavirus test that is prone to false negatives for cancerous strains of the virus, presenting the risk of untreated cervical cancer. And a third example is an autism biomarker test that Lurie said lacks scientific basis but is used to develop a treatment plan for patients who screen positive (FDA, 2015).
Another complicating factor in FDA regulation, in Lurie’s view, is its “general wellness” policy, stating that the agency does not intend to regulate general wellness products that (1) are intended to maintain or encourage a general state of health or healthy activity, and (2) present a low safety risk to users and other persons. Wellness products tend to fall into two categories, Lurie continued: those that do not make reference to treating, diagnosing, or preventing diseases or conditions (although such claims as “helps maintain a healthy weight” are permitted) and those that do not make reference to reducing risk of disease or helping people live with diseases or conditions unless the product is generally accepted as doing so (such as by tracking calories to reduce risk of type 2 diabetes). Many personalized nutrition offerings fall into these categories, he observed, making them exempt from premarket review of safety and adverse event reporting, and from having to prove that they follow good manufacturing processes, for example.
Lurie next described three types of claims about food that are permitted by FDA as another element of its regulation relevant to precision nutrition. First are health claims, which characterize the relationship between a substance and a disease and require “significant scientific agreement” and FDA preapproval before being used on food labels. Second are qualified health claims, which are similar but require a lower standard of evidence (“credible evidence”). Finally, structure/function claims describe a food’s effect on the normal structure or function of the body and require “competent and reliable scientific evidence,” as well as a disclaimer stating that the claim was not evaluated by FDA, and the product is not intended to diagnose, treat, cure, or prevent disease.
Lurie shared images of webpages for several personalized nutrition products that use these claims. Many appear to be structure/function claims, he observed, but he expressed doubt about the quality of the underlying evidence demonstrating support for and promotion of health. He cited as one example a test that measures one marker of immune response to nearly 100 foods, and suggests which foods to consider for an elimination diet. Whether that single marker of immune response is related to allergy and warrants avoiding certain foods is unsubstantiated, he asserted. Another example is a statement on a company’s website that according to Lurie appeared to stray into health claim territory without apparent FDA approval. Lurie noted that FDA sends companies warning letters for food and supplement misbranding, and has sent more than 20 such letters each year for the past few years. If the agency had adequate resources, he contended, it would send many more such letters.
Lurie ended his presentation by appealing for better science and better regulation around precision nutrition. He argued that identifying a biological marker purported to be associated with increased risk of a disease is not equivalent to saying that intervening on that marker would have a measurable impact on a person’s health, and that even if it were, intervention based on a personalized as opposed to a general approach would not necessarily make sound public health sense. The challenge is to identify when personalization versus a population-based approach makes most sense, he submitted, and he stressed that the choice between the two should be guided by which will have the most public health impact.
REGULATORY CHALLENGES AND OPPORTUNITIES FOR PRECISION NUTRITION
Robert Califf, Verily and Google Health, provided a regulatory perspective on challenges and opportunities for precision nutrition, informed by his experience as FDA’s deputy commissioner for medical products and tobacco (2015–2016) and commissioner of food and drugs (2016–2017).
FDA’s mission is to preserve and protect the public health, he explained, making it a regulatory agency, a science agency, and a public health agency with the disciplines of science, medicine, public health, policy, and law simultaneously at play. He noted that the agency regulates human and veterinary drugs, biological products, medical devices, cosmetics, tobacco products, and radiation-emitting products, and asserted that the principles used to regulate those various products are often transferable to its regulation of food.
Although FDA is a science-based organization, Califf emphasized that it is also tasked with making decisions, even when more research would be helpful to clarify an optimal choice. He likened FDA’s role to that of a referee making decisions with guidance from a rulebook, comprised of laws made by Congress, that it is responsible for interpreting and enforcing. The consequences of its actions are profound, he underscored, because the products it regulates represent about 20 percent of the U.S. economy and directly affect public health and patient well-being.
Califf discussed what he termed a “deteriorating” state of health among the U.S. public. The United States has the lowest life expectancy among the top 18 high-income countries worldwide (Ho and Hendi, 2018), he reported, and has lost even more ground on this metric in the wake of COVID-19, so that the gap in life expectancy between the United States and other high-income countries is now approaching 5 years (Woolf et al., 2021). The top 10 causes of death are dominated by chronic diseases, he added, with dietary factors being among the top risk factors driving death and disability (GBD 2019 Diseases and Injuries Collaborators, 2020).
Califf then highlighted a positive note in the context of the country’s disappointing state of health—that the current data environment offers new capability to understand biology and behavior. As salient characteristics of the new data environment he cited real-time access to massive amounts of data, made possible by new methods of data storage; the ubiquity and liquidity of data; little to no delay in access to data; and the ability to analyze data rapidly to gain insights and develop guidance. Califf referenced the opportunity to intervene on a person’s smartphone as an example of a capability that is a product of the new data environment and offers tremendous opportunity for providing precision nutrition guidance. The data-saturated environment enables integration of comprehensive health data, which he said is valuable both for assessing the entire human being and its interacting components and for generating evidence to inform public health decisions.
Califf’s comment about the value of comprehensive health data led to his next point: that individual biomarkers are unlikely to predict a food’s effect on health except in cases of specific nutritional deficiencies. He explained that for a biomarker of one measurement to serve as a surrogate (i.e., a substitute for a clinical endpoint), substantial evidence must
exist to support that designation. The vast majority of biomarkers are not valid surrogates, he pointed out, because they exist in a milieu of biological complexity that provides many opportunities for error in predicting a health outcome. For this reason, he cautioned against making unsubstantiated claims that intermediate biomarkers will affect health in a predictable way. He referred attendees to the BEST (Biomarkers, EndpointS, and other Tools) Resource, a joint FDA–National Institutes of Health (NIH) project to develop a glossary of harmonized terminology for biomarkers and endpoints (FDA–NIH Biomarker Working Group, 2016).
In closing, Califf elaborated on the risk of intervening on surrogate endpoints represented by single biomarkers. He asserted that surrogates can be misleading by either overestimating or underestimating an intervention’s effect on clinical outcomes (Fleming and DeMets, 1996), pointing out that an intervention can affect the biomarker of interest, the outcome of interest, or some other biological process in many unimagined ways. He expressed the hope that the emerging field of systems biology will provide unprecedented insights into the complex, multidimensional interplay of biological processes. According to Califf, the effect of food on health is a prime example of this complexity because many nutrients and substances interact simultaneously, each affecting multiple pathways and each with a potential impact on health. He added that biomarker tests—including those used for developing personalized nutrition guidance—need to be reliable and reproducible across multiple laboratories and clinical settings, and to maintain adequate sensitivity and specificity before the data they yield can be used in subsequent evaluation steps. Otherwise, he stressed, personalized recommendations could cause harm that might not be apparent until many years later.
LESSONS LEARNED ABOUT COMMERCIALIZING PERSONALIZED NUTRITION
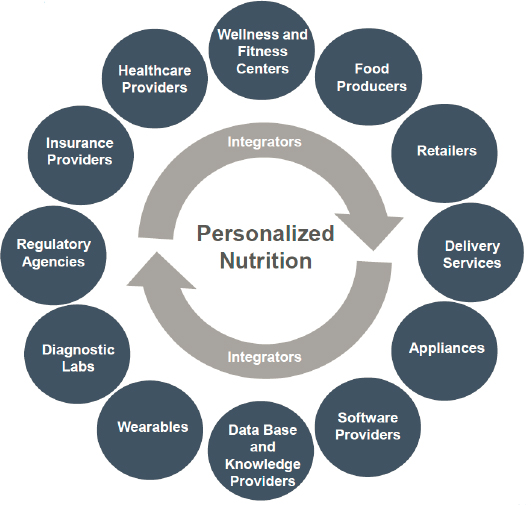
Joshua Anthony, Nlumn,2 shared lessons learned from his experience in the field. He began by observing that a variety of providers are rushing to understand how they can fit into the rapidly growing ecosystem of the personalized nutrition market (Figure 4-2), but they often make the mistake of putting themselves and their brand at the center when seeking to implement personalized nutrition. Instead, he said, it is critical to begin with consumers and examine their needs, behaviors, and values.
Anthony shared a series of insights about the profiles of people seeking personalized, food-based approaches to managing their health and wellness.
___________________
2 Nlumn is a consulting company that works with food, nutrition, and health technology companies to help them compete in the personalized nutrition and health marketplace.
SOURCE: Presented by Joshua Anthony on August 12, 2021.
They hold widely different views about what health means, he noted, partly because of their different needs and partly because of their varying access to information or misinformation. Many people are turning away from experts and embracing scientific controversy, he observed, and seeking self-affirming information or groups aligned with their beliefs. He suggested the term “subjective personalization” to describe this behavior, which he said includes frequent shifting between different eating styles (e.g., ketogenic diet, intermittent fasting) to gain the different purported health benefits promised by each. A smaller proportion of consumers are seeking objective, data-driven personalization, Anthony continued. The challenge with this segment of consumers, he maintained, is that their expectations for the ability of online tools and wearables to help tailor their diet and behaviors are often ahead of the science supporting them, and very few providers have published results demonstrating improved health and functional outcomes.
Anthony described consumer expectations in the context of the current scientific landscape. Expectations for personalized nutrition’s delivery of benefit solutions are broad and inconsistent, he asserted, ranging from managing chronic disease risk, to improving digestive health or joint pain, to maintaining sustained energy and reducing stress levels. Despite these
differing expectations, he said, several common themes emerge in characterizing an ideal personalized nutrition consumer.
The ideal personalized nutrition consumer, Anthony continued, is highly motivated and goal oriented; a digitally savvy data tracker seeking objective advice based on personalized data who is willing and able to follow prescriptive lifestyle advice and prepared to manage and act on that information. With higher levels of education and socioeconomic status, he maintained, these individuals are relatively healthy and wealthy, highlighting the challenge of getting personalized nutrition solutions to populations of lower socioeconomic status.
Anthony next described a model of personalized nutrition that supports creating and sustaining engagement with a wide variety of potential users (Figure 4-3).
He explained that this model calls for first selecting the optimal health outcome of interest for the consumer, while collecting an objective, validated measure of health or function is the next step. The consumer’s result for that measure, he continued, leads to personalized recommendations for improving health and lifestyle, which are intended to drive the behavior change necessary to achieve the desired outcome. The cyclical, continuous nature of the process supports engagement through reassessment and new advice, he added, as the consumer sets new outcome goals as health and functional needs change.
Anthony then described how providers can use the four aspects of the personalized nutrition engagement model to help design personalized nutrition offerings. When selecting a health outcome, he proposed focusing on a specific goal or benefit, which he said would allow solution providers to identify how their offerings can best deliver to fill one or more user need
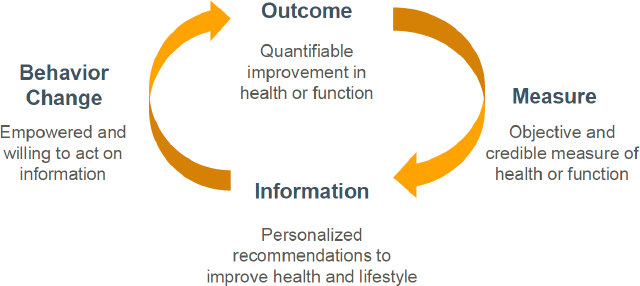
SOURCES: Presented by Joshua Anthony on August 12, 2021; modified from Adams et al., 2020. Reprinted with permission from Oxford University Press.
gaps (gaps between desired user benefit and the current state). Anthony reiterated that user expectations are often ahead of the science, and that companies can differentiate their products and services by focusing on aspects of their program for which proof is provided by the existing evidence.
When assessing health or function, Anthony advised using validated diagnostic methods and measures (whether the metric is biological, behavioral, or sociological in nature); communicating instructions clearly to promote the collection of high-quality, accurate results; clarifying how the data will be used and how the measure is linked to a relevant benefit for the user’s health; and being open to switching between validated diagnostic technologies to obtain a more robust assessment and avoid reliance on a specific technology that could become outdated.
Personalized recommendations based on a user’s health assessment results will be more likely to drive behavior change, Anthony argued, if they are communicated consistent with the user’s skill and experience. To enable behavior change, he continued, acknowledging and respecting user needs and preferences sets the tone for greater receptivity to objective suggestions for change. Small, frequent interactions offer opportunities to provide feedback and a reason to believe that change can be achieved, he observed, adding that the type and frequency of feedback are best personalized to the user. People still want a real person behind the technology, he maintained, noting that many programs use registered dietitians in this role as they can provide nutrition expertise and serve as behavior change mediators.
Anthony then discussed the state of the science of personalization. Companies can differentiate themselves by committing to evidence-based practices, he said, but most companies lack published data to support their program and its purported outputs. He added that companies may say that their program is supported by thousands of different studies, but usually this refers to research done by others. According to Anthony, personalized nutrition will be successful when it delivers health and functional benefits to users that go beyond one-size-fits-all approaches and are sustained over time (e.g., more than 12 months). In his view, most programs that are more rooted in science are just at the point where they are delivering or starting to show some health and functional benefits to users, but have yet to demonstrate that those benefits are sustainable and superior to outcomes from broader approaches.
Anthony concluded with three key takeaways for implementing personalized nutrition programs: identify a clear, compelling user-need gap to define the ideal consumer for the program instead of starting with the technology; build an engagement cycle around the ideal consumer and that person’s user experience, so that users’ inputs are commensurate with the outputs they receive; and continue to develop the program’s proof points instead of relying solely on secondary sources for support.
COMMUNICATING THE BENEFITS OF PERSONALIZED NUTRITION SOLUTIONS TO CONSUMERS
Martin Hahn, Hogan Lovells, U.S., LLP, discussed the future challenge of communicating the benefits of personalized nutrition solutions to the public while maintaining compliance with the current regulatory framework, which he said is not well designed to convey some of the industry’s technological capabilities.
Hahn provided context for FDA’s role in regulating food by explaining that it regulates products based on their intended use. Such use, he elaborated, determines whether a product is regulated as a drug or a dietary supplement, for example, and what types of claims it is permitted to carry. He briefly reiterated the various types of claims that products can bear, starting with disease claims for products intended to diagnosis, cure, mitigate, treat, or prevent disease. This type of claim will subject the product to regulation as an unapproved new drug or biologic, he explained, which he said is rational but can become complicated when the objective is to classify and communicate about nutritional interventions that purport to have a beneficial effect on disease. Echoing Lurie, he went on to say that health claims and qualified health claims are about reducing the risk of developing a disease, and structure/function claims are limited to the effect of the product on the body’s structure or function.
Hahn pointed out what he called a paradox of structure/function claims—that many of them imply disease prevention. He provided examples of two approved structure/function claims—“calcium builds strong bones” and “whole oats support heart health”—implying reduced risk for osteoporosis and coronary heart disease, respectively. Despite support from competent, reliable scientific evidence, Hahn pointed out, these claims have the potential to convey a message that may not have been intended.
In Hahn’s view, claims involve a tremendous tension between effectively conveying the intended message to consumers and remaining within regulatory guardrails. He identified as a related issue the need to ensure that statements made in advertising are both truthful and not misleading, which he explained is determined by the Federal Trade Commission (FTC). To make this determination, he said, FTC considers both explicit and implied messages conveyed by claims, meaning that companies are responsible for substantiating all reasonable interpretations of a claim with competent, reliable scientific evidence. For example, he elaborated, a cosmetic that is promoted as “age defying” may be supported by evidence that it increases skin elasticity, but if a certain threshold of consumers believe that the claim means the product will prevent wrinkles (when evidence does not exist to support this statement), the claim can be deemed false and misleading. This requirement creates further tension, he observed, in attempting to develop
the short, pithy structure/function claims that many marketers insist are ideal for communicating to consumers.
Hahn next discussed challenges to communicating the benefits of personalized and precision nutrition. Communications must be truthful and not misleading, he emphasized, supported by competent, reliable scientific evidence for both explicit and reasonably implied claims. In Hahn’s view, the evidence base for personalized nutrition is close to but not quite at the level needed to claim that certain types of diets will produce benefits for certain people with specific diseases and conditions. But, he stressed, when personalized nutrition technology reaches that point and communications about demonstrated health improvements are being developed for consumers, it will be important to have a regulatory structure that allows for communicating those benefits without unintended regulatory consequences.
Hahn then provided a series of examples to support his contention that the current regulatory system is not well suited to allowing the benefits of personalized nutrition technologies to be communicated without risking allegations of misleading consumers or being regulated in a way that is inconsistent with their intended use. As an example, he noted that a genetic analysis used to identify a diet that can help a healthy individual reduce the risk of developing diabetes could be communicated through an FDA-approved health claim, but if the genetic analysis is used to identify a diet that reduces insulin dependence for an individual with diagnosed diabetes, it is communicating a treatment effect and warrants a disease claim, which would trigger filing of the product as a drug. The new drug approval process is lengthy and expensive, he said, and could stifle innovation because it is not a viable option for many of the personalized nutrition technologies currently under way. A less risky structure/function claim could be made for a product, he added (e.g., that it supports blood glucose levels within normal ranges), but such a claim would not communicate the full benefits of the technology and likely would not attract as much consumer interest. In another example, he observed communicating a product’s ability to alter the microbiome in a way that reduces the length and severity of the common cold would be making a disease claim, whereas making a structure/function claim such as “supports immune function” would be less risky but would not communicate in a clear, effective manner because it would underpromise the expected benefit.
Hahn urged stakeholder discussion toward developing a strategy for supporting a regulatory structure that would allow personalized nutrition technologies to advance and, when they have a sufficient evidence base, for clearly and effectively communicating their benefits to target populations without risking unintended regulatory consequences. Such a strategy, he posited could involve considering new legislation to give the FDA the authority to develop a new regulatory framework for personalized nutrition
solutions, or adapting existing regulatory frameworks, such as those governing foods for special dietary uses or medical foods.
INCORPORATING PRECISION NUTRITION INTO FOOD-BASED AND NUTRIENT-BASED GUIDELINES
Patsy Brannon, Cornell University, discussed challenges and opportunities for incorporating precision nutrition into food- and nutrient-based guidelines for public health (such as the Dietary Reference Intakes [DRIs] and the Dietary Guidelines for Americans [USDA and HHS, 2020]), as well as into recommendations for individuals. She began by contrasting these two types of guidelines. Public health guidelines inform population-based policies and regulatory actions, such as federal nutrition programs, nutrition labeling, and population-level dietary intake assessments, she clarified, whereas individualized recommendations tailor nutrient and dietary intake, dietary patterns, and dietary intake assessment for a specific person. Public health guidelines are implemented through national outreach and education, policies and regulation, fortification, and population monitoring and assessment, she continued, which she acknowledged come with limitations resulting from their one-size-fits-all approach, but pointed out are necessary because it is not feasible to develop individualized recommendations for an entire population. Individualized recommendations are implemented through what Brannon called a “tech model” (an individual interacting with supported technology); a “hybrid model” (which adds a health professional to the supported technology); or a “self-directed model” (involving the individual’s actions), which she suggested would entail individuals picking and choosing information from a variety of digital sources at the risk of taking in misinformation.
Public health guidelines must account for population-wide variation in individual needs, risks, preferences, and behaviors, Brannon observed, whereas individualized recommendations can be tailored to each of these aspects. She pointed out that moderate- to high-strength evidence is needed to support public health guidelines because of the risk to the population with lower levels of evidence quality. Turning to individualized recommendations, she suggested that they should be supported by at least moderate-strength evidence in either the tech model or hybrid model, but a lower level of evidence might be adequate for the self-directed model given the way individuals gather their information. Finally, she drew a distinction between public health guidelines, which are not directed at people with diseases that require medical nutrition therapy or that alter nutrition needs because of malabsorption, dialysis, disability, or altered mobility, and individualized recommendations, which may be able to include these individuals.
Brannon next reviewed the expanded DRI model, highlighting that it now includes the concept of chronic disease risk reduction (CDRR). She pointed out that chronic disease outcomes are no longer considered in determining either the estimated average requirement (EAR) or adequate intake for a nutrient, which are now based on an adequacy outcome, or the tolerable upper level (UL) for a nutrient, which is now based on toxicological outcomes. The notion of distribution of need is embedded in the expanded model, Brannon observed, noting that in a normal distribution of need, the EAR meets the needs of 50 percent of the population, while the recommended daily allowance (RDA) meets the needs of 97.5 percent of the population. She added, however, that an individual might have a need different from the RDA but still be included in the distribution of risk and need of the DRI framework.
Brannon explained that the formalization of chronic disease risk in the expanded DRI model can convey the potential for a variety of relationships to exist between such risk and dietary intake. To illustrate this point, she contrasted sodium, for which the risk of chronic disease increases as intake increases, and omega-3 fatty acids, for which the risk of chronic disease may decrease as intake increases. There could be other chronic diseases for which risk increases with intakes that are either too low or too high, she added, but in any case, the CDRR level is set to minimize chronic disease risk across the population.
Turning to the type of evidence needed to select adequacy and/or toxicity outcomes for a nutrient, Brannon explained that for adequacy, the indicator of nutrient status (i.e., biomarker) must be on the causal pathway to the clinical deficiency outcome of interest. Such outcomes relate to deficiency disorders, she elaborated, but the biomarkers can relate to effect (e.g., bone mineral density for calcium), exposure (e.g., red blood cell levels for folate), or mechanisms and functional outcomes (e.g., enzyme activity for thiamin). For adequacy and toxicity outcomes, respectively, the relationship between nutrient intake and the associated deficiency disorder or toxicologic effect must be supported by direct evidence. For adequacy, she continued, high certainty of causal and intake–response relationships is required (i.e., demonstrated by randomized controlled trials (RCTs), metabolic balance studies, or depletion/repletion studies).
Although the approach for setting DRI values requires examining the totality of the evidence using a rigorous, systematic review approach, Brannon pointed out that there are only 12 nutrients (total fat, omega-3 and omega-6 fatty acids, biotin, choline, vitamin K, pantothenic acid, chromium, fluoride, manganese, sodium, and potassium) for which the distribution of need is not yet understood, primarily because no adequacy outcome has been identified. Precision nutrition thus has an opportunity, she proposed, to help build stronger reference intake values for these nutrients as research leads to the identification of biomarkers of adequacy and their variance.
Brannon then clarified that DRIs for adequacy or toxicity are needed when the deficiency or toxicity of an essential nutrient is caused by that one nutrient, is prevented by nutritional interventions, and affects everyone if intake is inadequate or excessive. In contrast, she maintained, DRIs for CDRR purposes are not warranted without sufficient evidence of a relationship between the nutrient or a naturally occurring food substance and the risk of chronic disease. She added that such risk varies by individual, age, life stage, and various “omics,” indicating the importance of systems biology approaches for understanding the relationships between chronic disease and nutrient intakes. Such relationships can be relative and/or small, she continued, are often related to many individual and environmental factors, and are only partly ameliorated by nutrition interventions. According to Brannon, precision nutrition has an opportunity to identify surrogate outcomes for chronic disease, even though having specific clinical disease outcomes is ideal (but difficult because discovering these outcomes requires longitudinal research).
Brannon also discussed the process for validating a surrogate outcome (i.e., intake of a nutrient, food, or dietary pattern) for chronic disease. First, the surrogate outcome must be on the causal pathway to disease, which she noted can be determined by observational and small interventional studies. Second, it must be concordant with changes in a health outcome that occur with a specific nutritional intervention, must be demonstrated in rigorous clinical trials, and must explain a clinically significant proportion of response to the nutritional intervention. Finally, it must accurately predict the effect of the nutritional intervention on the clinical outcome in rigorous clinical trials.
Brannon suggested that as precision nutrition advances, consideration be given to the evidence requirements for selecting chronic disease outcomes detailed in the Guiding Principles for Developing Dietary Reference Intakes Based on Chronic Disease Outcomes (NASEM, 2017) and applied by the DRI committee for sodium and potassium. She clarified that there must be at least moderate strength of evidence (based on GRADE [Grading of Recommendations Assessment, Development and Evaluation] methodology, a structured approach for evaluating the strength of evidence) for a causal association between the nutrient and a single specific chronic disease outcome or a single qualified surrogate outcome. She noted that the nature and substance of the evidence may vary from what is required to demonstrate adequacy, such that more evidence may come from observational studies than from RCTs, for example. Should that be the case, she said, there is lower certainty of a causal relationship because of the inherently greater risk of various types of bias with observational research.
Brannon next discussed an opportunity for precision nutrition to determine population subgroups with specific nutrient needs, including subgroups with distinctly different distributions of the requirement for a
nutrient and response to its intake and subgroups of responders and nonresponders to a nutrient. As an example of the latter, Brannon pointed out that the 2019 DRI committee for sodium and potassium noted the need to identify sodium-sensitive individuals through determination of “rare and common genetic variants” (NASEM, 2019). Subgroups may need to follow specific dietary patterns to mitigate risk of chronic disease, she continued, but evidence must be moderate to high for the causal association between dietary pattern and disease risk, as well as for the intake–response relationship. She identified as another opportunity for precision nutrition helping to fill the research gap of defining a “healthy population” when the prevalence of chronic disease is high. Doing so would promote better-informed public health guidelines for nutrients and dietary patterns, she argued, and enhance understanding of variance within a healthy population.
Brannon next raised the issue of whether individual algorithms can be linked to public health guidelines. She observed that a major challenge in both clinical and dietetics practice is the difficulty of confirming an individual’s specific nutrient requirements, although she stressed that this challenge does not invalidate the typical public health population approach of basing recommendations on a normal distribution of nutrient requirements. At the same time, she said, differences in individual needs could create opportunities for both adequacy and chronic disease DRIs and for the Dietary Guidelines (USDA and HHS, 2020) to be more tailored to individuals, although the strength of evidence required for such tailoring remains to be determined.
Brannon pointed out that individual guidelines based on precision nutrition also raise the issue of efficacy versus effectiveness. She affirmed that some precision nutrition approaches have demonstrated efficacy, but suggested that the effectiveness of these findings may be subject to bias due to self-selection of participants. She encouraged consideration of theories of behavior change—such as the health belief model, theory of planned behavior, transtheoretical model (stages of change), and precaution adoption process model—that could provide insight into characteristics of participants, such as perceptions of health risks and of avoiding those risks, perceived control over one’s health, and degree of motivation and readiness to change.
To end her presentation, Brannon highlighted four questions. First, how can we develop blended models that address the needs for both population food- and nutrient-based guidelines and individualized precision nutrition recommendations? Second, what is an effective strategy for communicating both types of guidelines? Third, how do we ensure equitable access for people at highest risk of poor health (e.g., individuals with low incomes, lack of health insurance, food insecurity, lack of housing, low health literacy)? And fourth, how do we ensure that practitioners receive an appropriate scope and depth of training to implement individual guidelines?
PANEL DISCUSSION
Health Claims for Targeted Populations
An audience member observed that existing FDA-approved nutrition-related health claims apply to the general population, and asked whether health claims for precision nutrition interventions would require claims for targeted populations. Califf said he did not see a reason for the FDA to allow a product to carry a health claim for the general population with respect to a benefit that applies only to a targeted population. Lurie agreed that a health claim should not exceed the evidence supporting it. He added that practically speaking, companies might not want to make restricted claims because doing so would limit the target audience for their products. Hahn contended that not allowing a claim for a targeted population would represent a missed opportunity, and suggested that designated medical foods (which are designed to address an individual’s unique needs resulting from a disease) could carry these types of claims. Lurie countered that the medical foods pathway is unattractive from a commercialization point of view because it requires a physician intermediary.
Preventing Erosion of Public Trust in Precision and Personalized Nutrition Solutions
An audience member alluded to the erosion of consumer trust in public health guidance during the COVID-19 pandemic and asked how to avoid the same response to personalized nutrition solutions. Califf underscored the importance of maintaining scientific integrity in messages aimed at connecting emotionally with consumers to effect behavior change. Anthony appealed for building trust and transparency with consumers by being honest about the strengths and limitations of a personalized nutrition solution. Brannon alluded to the challenge of communicating to the public about evolving science and public health topics when guidance may change as additional evidence becomes available. Lurie agreed and added that the pace of evolution in scientific understanding is not commensurate with the pace of new claims circulating through the Internet, and that the regulatory process for policing claims and bringing enforcement action against false claims is quite slow.
Incorporating Social Determinants of Health in Precision and Personalized Nutrition Models
Brannon agreed with an audience member’s comment that it is important to incorporate social determinants of health into precision nutrition
models, and suggested that also incorporating constructs from behavior change theory can help predict consumer success with uptake of recommendations. For example, asking people about their perceived barriers to change can inform how they will respond to personalized nutrition guidance. Roberto agreed that incorporating social determinants of health is critical for ensuring that people receive recommendations that are not only matched to their biological attributes but also actionable in their cultural, community, and economic contexts. Califf pointed out that behavioral attributes are just as measurable as biological attributes, and that a common practice in advertising is to segment populations by behavioral phenotypes. He warned that if a product’s profit is higher in one population segment than another, it introduces risk that the unprofitable segment may not be included in research unless a requirement for inclusive research designs exists.
N-of-1 Study Designs
In response to an audience member’s question about the role of n-of-1 study designs in personalized nutrition, Califf replied that n-of-1 is a great design when the objective is to assess an intervention’s short-term effects in an individual. He noted, however, that a primary risk with this design is drawing incorrect conclusions because short-term changes in a biomarker are often not predictive of the overall long-term outcome. In Lurie’s view, n-of-1 designs are most useful when the mechanism of action is clearly defined and outcome measures are objective. Anthony suggested that the strongest evidence from n-of-1 study designs comes from crossover studies, and Califf contended that subjective outcomes are appropriate in n-of-1 studies if a crossover design with a placebo is used. Roberto advocated for studying broad groups in any research design that is used, pointing out that if at baseline, more narrowly defined study populations are already healthier than groups not included in the study, relationships will look stronger for any positive health effects observed in response to the nutrition intervention being studied.
Developing Blended Models to Address Population and Individual Needs
Brannon speculated as to whether public health models could provide general recommendations while also stating that additional guidance for tailoring certain recommendations was available for people with specific characteristics. This approach would apply in the case of sodium, she said in reference to Hilliard’s presentation earlier in the workshop, for which a subset of the African American population had much lower needs relative to other population groups.
Anthony suggested that “personalized nutrition” is the term that will best resonate with consumers, whereas “precision nutrition” may be construed as narrowly focused on measurement of biomarkers hitting specific targets for nutrient intake. He suggested that the latter is unnecessarily prescriptive and does not account for the personal preferences, beliefs, and values that influence an individual’s food choices.
Applying Personalized Nutrition to Family Meals
An audience member asked the speakers how they envision implementation of personalized nutrition at the family level, when each family member may have different food plans. Lurie responded that a great deal of work would be required to customize meals for each family member, and suggested that increased precision could also increase complexity and confusion. He noted that people sometimes accept degrees of imprecision because such messaging is simpler, and proposed that increased precision in nutrition guidance is not necessarily worth the potential risk of increased confusion until stronger data are available to support the associated health benefits. Califf added that food access and availability influence the degree to which people are able to follow specific dietary guidance. Roberto suggested that it would be helpful to have pre-prepared, good-tasting, convenient meal solutions for people who do not always have time to prepare customized meals for their families. Brannon pointed out that when certain family members have special dietary needs, the family often chooses meals with components that can easily be adapted for those needs. These families would likely find it helpful to work with a registered dietitian or other expert, she proposed, so they could learn how to translate special dietary needs into food choices and recipes. And according to Anthony, one family member’s special dietary needs or preferences can encourage food exploration by other family members.
Personalized Nutrition’s Potential to Improve Food Access
Hahn speculated whether personalized nutrition recommendations could promote increased access to healthy foods in underserved communities. Lurie pointed out that in the pharmaceutical market, drugs developed for targeted populations are sold at a higher price point relative to drugs for broader populations. People are willing to pay more for something they believe is tailored to their specific needs, he proposed, but added that higher prices also restrict access to those products. Califf noted that certain grocery stores are intentionally located in higher-income areas and suggested that greater transparency about retailer siting could lead people to demand more equitable distribution of retail food venues. Brannon cautioned against
the use of unnecessarily restrictive messaging that leads people to believe, for example, that they must choose fresh forms of fruits and vegetables. Minimally processed canned and frozen produce is as nutritious as fresh varieties, she pointed out, and its affordability and shelf stability make it more accessible for people with limited resources. To clarify, she added that more flexible guidance helps people make choices that address the various factors they must weigh when making food choices. Anthony suggested that increased personalization may increase food waste, but the foods that do not meet one group’s personalized plans could be minimally processed into other foods that meet another group’s needs (rather than being discarded). Although this approach could help improve food access, he cautioned that it could result in the appearance that one population is getting “seconds.”
Exciting Aspects of Precision and Personalized Nutrition
Before concluding the panel discussion, McKinnon invited the six speakers to share aspects of the precision and personalized nutrition field that are particularly exciting to them. Hahn responded that the science is advancing to the point of being actionable. The science is fascinating, Roberto agreed, and added that it is spurring conversations about related environmental, political, economic, and social issues that are introduced by precision and personalized nutrition opportunities. Lurie echoed Roberto’s thoughts and added that he was encouraged to be discussing these issues while the technology is still emerging, rather than having to manage misinformation and unintended consequences down the road. Califf expressed excitement about the opportunities to measure behavioral and environmental factors and their interactions, and Anthony highlighted the potential to combine those measures with biological measures in a systems approach that can make personal nutrition solutions more widely accessible. Finally, Brannon voiced hope for the prospect of translating the effective aspects of personalized nutrition platforms into innovative solutions for implementing public health guidelines.
This page intentionally left blank.






















