
2
Overview of Hematopoietic Stem Cell Transplantation and Disability in the United States
To set the stage for the workshop, Fred Appelbaum, executive senior vice president and deputy director at the Fred Hutchinson Cancer Research Center, gave workshop participants a simple description of hematopoietic stem cell transplantation (HSCT) and defined some relevant terms. Every individual, said Appelbaum, starts as a single cell—a fertilized egg. In the first week after conception, this cell divides multiple times and forms a small ball of cells called a blastocyst. Within the blastocyst, there are cells called embryonic stem cells. These cells are “pluripotent,” which means that they can turn into any type of tissue in the body (e.g., brain, skin, bone). As the embryo grows, cells lose their pluripotency. By the time the child is born, each tissue contains its own population of adult stem cells. These cells are responsible for the repair and regeneration of a specific type of tissue; for example, skin stem cells repair skin and bone stem cells repair bone. These cells are “multipotent” because they can form different types of cells within the tissue type; for example, skin stem cells can form hair, epidermis, or sweat glands. Hematopoietic stem cells—the topic of this workshop—are cells responsible for forming all blood and immune cells in the body.
A hematopoietic stem cell transplant “has the potential to cure virtually every blood and immune-based disorder,” said Appelbaum. The first person ever cured through HSCT was treated in 1960 and is “alive and well” today, he said. HSCT is now performed more than 100,000 times each year worldwide, and the field of stem cell transplantation over the years has been both “challenging and fascinating.” In this session, experts gave an overview of HSCT, including its indications and expected outcomes.
UNDERSTANDING STEM CELL TRANSPLANTATION
Mary Horowitz, the chief scientific director of the Center for International Blood and Marrow Transplant Research (CIBMTR), said that HSCT is an intensive therapy used primarily for blood cancers, as well as bone marrow and immune deficiency disorders (D’Souza et al., 2020). The procedure generally involves administration of high doses of cytotoxic and/or immune suppressive therapy, followed by infusion of blood stem cells, to restore hematopoiesis (the formation of the cellular components of blood). HSCT aims to restore hematopoiesis that has been destroyed by the primary disease or the pretransplant therapy, or to provide an immune-mediated graft-vs.-malignancy effect. There are a variety of diseases that are treatable by HSCT, said Horowitz, including both malignant and nonmalignant diseases; however, more than 90 percent of transplants are directed at malignant diseases (see Table 2-1). There are other types of stem cells and other uses of hematopoietic stem cells, said Horowitz. Other uses of hematopoietic stem cells include immune modulation to facilitate kidney and other solid organ transplants, gene therapy for congenital diseases, and a number of therapies administered by diverse medical specialties. There are very few data on long-term effects of those therapies, Horowitz said, so they are not addressed in this workshop.
There are two major types of HSCT, said Horowitz. Autologous transplants are collected from the patient’s own bone marrow or bloodstream; this is an option when dose-intensification is the primary goal.1 Allogeneic transplants use cells from a family member, unrelated donor, or umbilical cord blood; this type of transplant has the potential for potent immune-mediated
TABLE 2-1 Diseases Treatable with Hematopoietic Stem Cell Transplantation
| Malignant Disease | Nonmalignant Disease |
|---|---|
|
|
SOURCE: As presented by Mary Horowitz, November 15, 2021.
___________________
1 Dose intensification is a regimen of radiation or chemotherapeutic agents that may be administered to a patient in conjunction with the HSCT procedure to help improve outcomes.
anticancer effects. The cells for transplant are collected either directly from the bone marrow or through apheresis after using drugs to mobilize cells out of the marrow into the bloodstream.2 Umbilical cord blood stem cells are collected from the placenta after delivery. Horowitz said that allogeneic transplants usually require close matching for human leukocyte antigens (HLA), which are cell surface proteins that are critical to immune responses.
Individuals inherit their HLA type from their parents, and given family size in the United States, only about 30 percent of patients will have an HLA-matched family member. The World Marrow Donor Association brings together nearly 40 million donors from around the globe, which significantly increases the chances of a patient finding a good match. However, she said, there is still no guarantee of a match for a patient; Whites have about an 80 percent chance, while African Americans only have a 30 percent chance. Fortunately, it is now possible to successfully pair donors and patients who have some degree of HLA mismatch. While the “gold standard” for a match is a matched relative, transplants can be performed with mismatched unrelated donors, mismatched haploidentical relatives, and with umbilical cord blood.
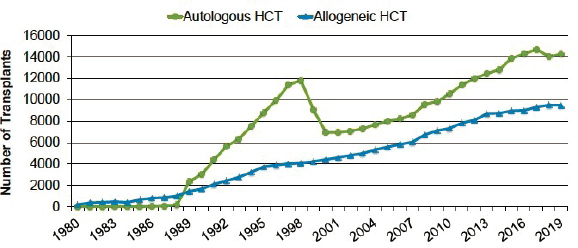
The number of transplant recipients in the United States has increased significantly over the past 30 years (Figure 2-1). Part of this increase, she said, is because of the increasing ability to perform transplants for older patients; nearly half of transplants are now in patients over age 60.
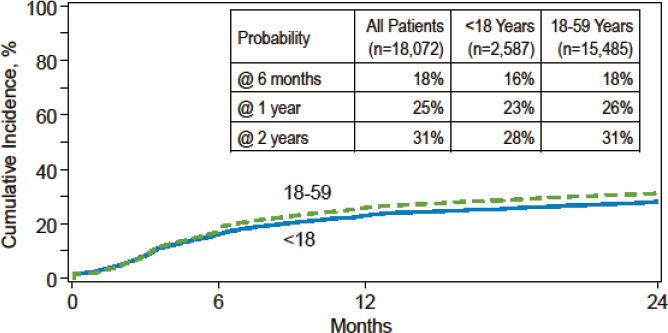
Among patients under age 60, 20 percent will die in the first year after an allogeneic transplant, and another 10 percent in the year after, said Horowitz. Although HSCT is an efficacious treatment, it is most often provided to patients diagnosed with hematologic malignancies. The risk of recurrence or
NOTE: HCT = hematopoietic cell transplantation.
SOURCES: As presented by Mary Horowitz, November 15, 2021; Phelan et al., 2020.
___________________
2 Apheresis refers to the process of separating the cellular and soluble components of blood using a machine.
progression of these malignancies is around 30 percent in the first 2 years (Figure 2-2). In addition, graft-versus-host disease (GVHD) is a major complication of transplantation and is an important cause of both early and late mortality and morbidity. GVHD occurs when immune cells in the graft recognize the recipient cells as foreign and initiate tissue injury, particularly of the skin, gut, and liver. Acute and chronic GVHD occur in 30 to 40 percent of patients. The use of posttransplant cyclophosphamide has improved the ability to perform mismatched related and unrelated donor transplants and is associated with lower rates of chronic GVHD, said Horowitz.
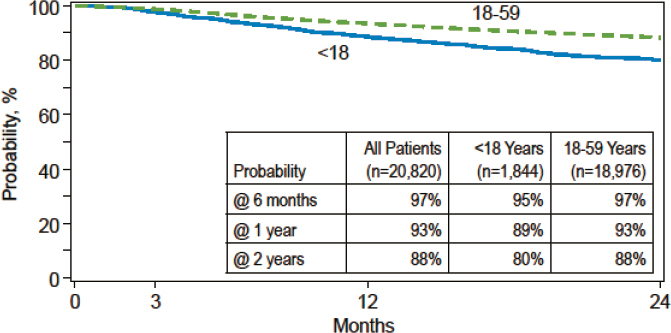
Patients who receive autologous transplants have better survival rates than allogeneic patients, with 90 percent surviving the first year and nearly 90 percent surviving 2 years (Figure 2-3). However, said Horowitz, the risk of disease progression persists after autologous transplants, and about 40 percent of patients will experience recurrence of the underlying malignancy or require ongoing maintenance therapy for malignancy.
SOURCES: As presented by Mary Horowitz, November 15, 2021; CIBMTR®. The views expressed in this publication are that of the authors and do not reflect the position of the Center for International Blood and Marrow Transplant Research.a
a CIBMTR® (Center for International Blood and Marrow Transplant Research) represents an international network of hematopoietic stem cell transplant centers that submit transplant-related data and collaborate on research studies. CIBMTR’s clinical database contains information from more than 585,000 patients. These data are freely available to research investigators in the medical and scientific communities. https://www.cibmtr.org/About/WhatWeDo/Pages/index.aspx (accessed March 6, 2022).
SOURCES: As presented by Mary Horowitz, November 15, 2021; CIBMTR®. The views expressed in this publication are that of the authors and do not reflect the position of the Center for International Blood and Marrow Transplant Research.
Although the use of HSCT has increased in recent years, said Horowitz, it is still underused. For example, only about 25 to 35 percent of patients with acute myeloidleukemia receive a transplant. While a transplant is not appropriate for every patient, the currentproportion is only about half of those who could benefit. Horowitz said that recent studies showing efficacy in comparison to nontransplant therapy and the ability to successfully use HLA-mismatched donors for allogeneic transplantation may result in the increased use of HSCT in some diseases. However, some new therapies, such as CAR T cells, may supplant the use of HSCT in other diseases. The rate of survival after a transplanthas also increased; while this is a positive trend, Horowitz said that it also increases the numberof people who require care for lingering functional disability after a transplant. In conclusion, Horowitz said that HSCT is an effective therapy for patients with a wide range of hematologicdisorders, but rates of mortality and morbidity following a transplant are stillsubstantial.
PATTERNS OF RECOVERY
Following Horowitz’s presentation, Stephanie Lee, a member of the FredHutchison Cancer Research Center, gave workshop participants an overview of the patterns ofrecovery seen after patients are treated with HSCT. The goals of such treatment, she said, are forpatients to be alive and free of disease, to have normal physical and mental functioning, to have agood quality of life, and to be able to return to their social roles (e.g., parent, worker). Ideally, saidLee, a
transplant would restore a patient’s life expectancy to what it would be without the diseaseor the transplant. Unfortunately, increased mortality rates persist in both the short andlong term after transplantation. For example, said Lee, patients who were free of the original disease 5 yearsafter transplantation still experienced a higher mortality rate up to 30 years after thetransplant, compared to their age- and sex-matched peers (Martin et al., 2010). This translates into about a30 percent decrease in life expectancy for transplant survivors. The causes of theselate deaths vary, said Lee, and include recurrent disease, second cancers, cardiovascularissues, infection, and chronicGVHD (Martin et al., 2010).
Another goal of HSCT is to restore physical and mental functioning. However, many patients are already disabled before transplantation because of chemotherapy and radiotherapy, she said, and as a result they are unable or not advised to go to work or school. Many patientshave comorbidities, frailty, and poor physical and mental health; these pretransplantcharacteristics are predictive of survival, complications, and transplant-related mortality, said Lee. Unlikesome other lifesaving medical procedures, such as heart and lung transplants, HSCT does notusually improve health while curingdisease.
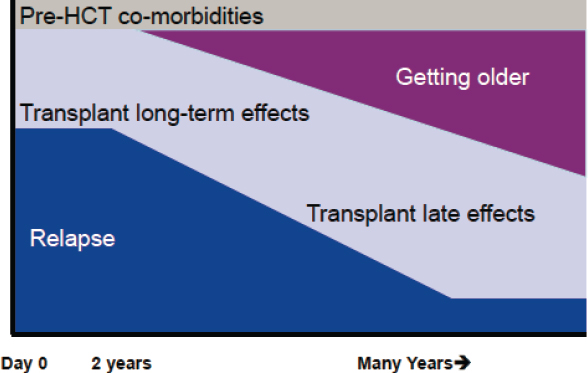
Posttransplant disability may be attributed to many things, said Lee, including pretransplant comorbidities, relapse, transplant long-term effects, transplant late effects, and getting older; the potential effect of each of these changes over time (Figure 2-4). The potential for relapse is highest in the first 2 years but persists for many years. Long-term effects are issues that begin during the transplant and persist, while late effects are issues that arise after the transplant but are attributable to it.
In the first year after HSCT, said Lee, three main factors determine a
SOURCE: As presented by Stephanie Lee, November 15, 2021.
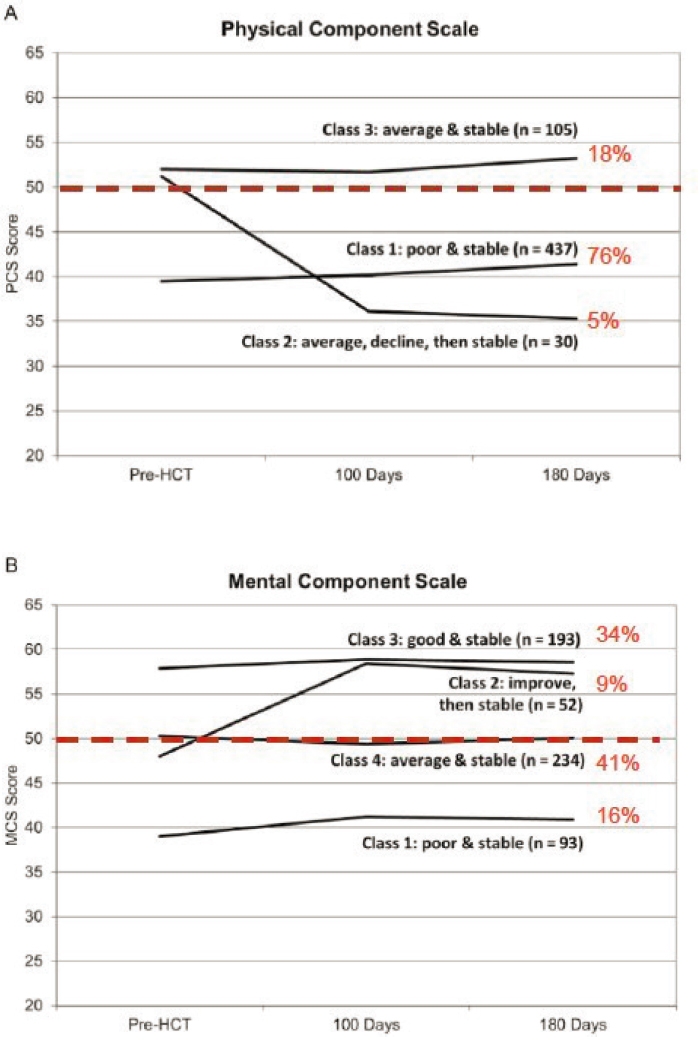
patient’s health and functioning: the toll the transplant takes, whether relapse occurs, and whether chronic GVHD develops. Few studies follow patients along the trajectory from pretransplant through recovery, said Lee, but some relevant data are available. A 2016 study (Jim et al., 2016) examined both physical and mental quality of life of patients in the 6 months following HSCT and found that patients could be grouped into distinct classes based on the trajectory of their recovery (Figure 2-5). For physical outcomes, 76 percent of patients had poor and stable quality of life, 18 percent were average and stable, and 5 percent began with average quality of life that declined and then remained stable. For mental health outcomes, 41 percent were average and stable, 34 percent were good and stable, 16 percent were poor and stable, and 9 percent began lower but then improved and remained stable. Another study (Wood et al., 2016) found that a decline in either physical or mental functioning by day 100 following a transplant was associated with a higher rate of mortality after day 100.
Patients who survive the first year following HSCT still contend with issues such asa high burden of medication, physical limitations, fatigue, depression, and late effects, saidLee. For example, in a survey of 118 patients who had received allogeneic transplants a year prior, the majority were still on multiple systemic medications, ranging from anti-infective agents(94 percent), prednisone (50 percent), hormones (27 percent), and antidepressants (26 percent) (Lee et al., 2009). Lee saidthat 71 percent were taking immune suppressants at 1 year, which is often used to determine whether patients are safe to return towork.
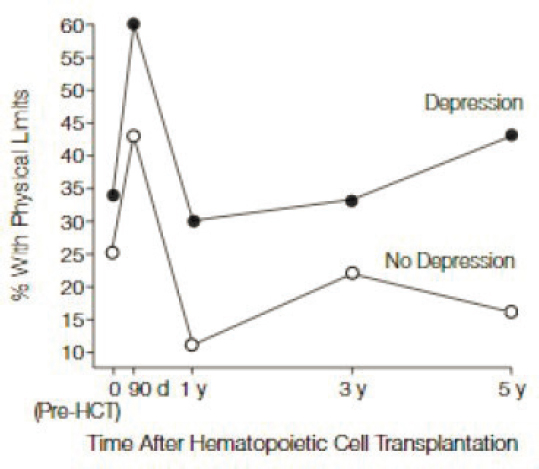
Lee shared data from a longitudinal study that analyzed quality of life and functionin transplant patients (Syrjala et al., 2004). The study found that the burden of physicallimitations peaked about 3 months after transplant, then improved by 1 year and remained high at 3years and 5 years posttransplant (Figure 2-6). The burden of physical limitations was higher for patients who experienced depression prior to the transplant. This study also examined the rateat which patients returned to work after HSCT; among survivors without recurrentmalignancy, about 84 percent returned to full-time work by 5years.
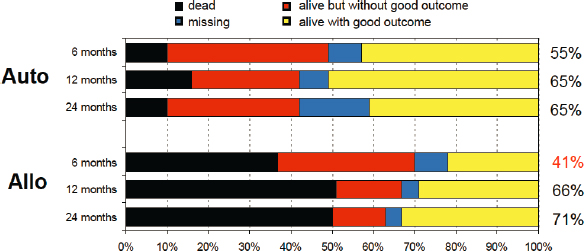
Some research, said Lee, has used self-reported measures of recovery to examinethe posttransplant trajectory. One older study (Lee et al., 2001) asked patients to rate their agreement with the statement “I have recovered from my transplant.” Patients whohad undergone autologous transplants were much more likely than patients receivingallogeneic transplants to report they had recovered by 6 months, but by 24 months, the populationsreported similar recovery rates of around 70 percent (Figure 2-7). The study also asked patients whetherthey had returned to school, work, or homemaking; by 24 months, around 70 percent ofpatients receiving autologous and allogeneic transplants reported a return to these roles. Asizable proportion of both populations of
SOURCES: As presented by Stephanie Lee, November 15, 2021; Jim et al., 2016.
NOTE: HCT = hematopoietic cell transplantation.
SOURCES: As presented by Stephanie Lee, November 15, 2021; Syrjala et al., 2004.
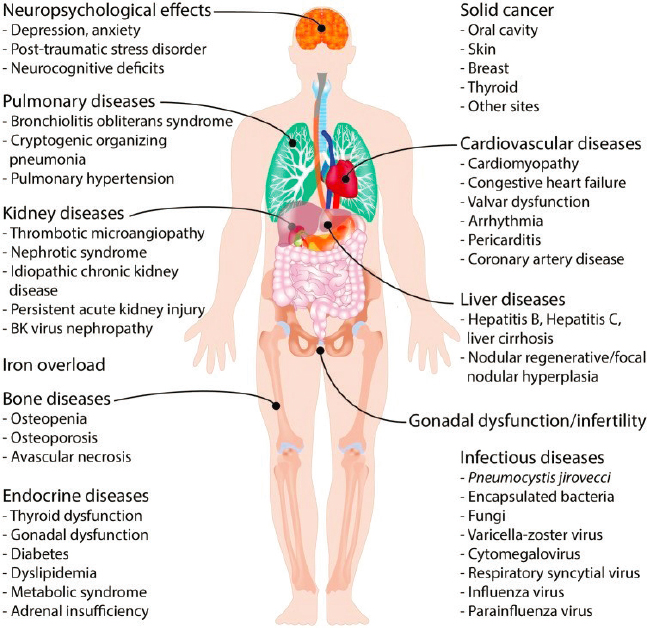
patients continued to be bothered by fatigue after atransplant; nearly half of the patients were bothered a lot or extremely bothered by fatigue at 6 months, and about a third continued to be bothered at 12 months. In addition to fatigue, Lee saidthat transplant survivors face a wide variety of late effects and comorbiditiesincluding neuropsychological effects, cancer, infection, and
NOTE: auto = autologous transplant; allo = allogeneic transplants
SOURCES: As presented by Stephanie Lee, November 15, 2021; Lee et al., 2001.
infertility (Figure 2-8); the cumulative incidence of these effects increases over time (Sun et al.,2010).
Comorbidities and fatigue are factors that can affect whether an individual returnsto work or school after a transplant, said Lee. Across multiple studies in different populationswith different study designs, around 50 to 80 percent of transplant survivors return to full- and part-time work (see Table 2-2). Predictors of not returning to work include fatigue, pain, cognitive dysfunction, comorbidities, and medical complications related to the transplant; inaddition, those with lower educational status, those who are older, and women are less likely toreturn. There are myriad causes of disability among transplant survivors, said Lee, and thesedisabilities can prevent or delay a return to work. Theseinclude:
- Physical dysfunction, such as lack of strength and stamina
SOURCES: As presented by Stephanie Lee, November 15, 2021; Inamoto and Lee, 2017.
TABLE 2-2 Studies Examining Return to Work After Hematopoietic Stem Cell Transplantation
| Design | Population | % Returning to Work; Risk Factors Associated with Work Status | Reference |
|---|---|---|---|
| Longitudinal | N = 88 (auto/allo) | 92% @ 5 years if full-time pre-HCT; female, physical dysfunction | Kirchhoff et al., 2010 |
| Longitudinal | N = 312 (auto/allo) | 74% @ 3 years; older autos with lower pre-HCT income, allos with chronic GVHD | Wong et al., 2020 |
| Longitudinal | N = 690, 79% auto | 62% @ 1 year; hospitalizations, relapse, pain, fatigue | Morrison et al., 2016 |
| Longitudinal | N = 152, allo | 47% @ 5 years; peripheral blood | Lee et al., 2016 |
| Cross-sectional survey | N = 203, > 5 year, 85% allo | 77% @ 12 years; older, living alone, physical/mental late effects, fatigue | Tichelli et al., 2017 |
| Cross-sectional survey | N = 1,048, ages 20–64, > 2 year allo DFS | 52–76% @ 5 years; female, older, part-time | Kurosawa et al., 2021 |
| CIBMTR study | N = 2,844 childhood HCT, 1985–2010, allo | 73% when 28–32 years old; RIC/NMA, older at HCT | Bhatt et al., 2019 |
| CIBMTR study | N = 1,365 young adults, 2008–2015, allo | 50% @ 1–3 years; female, multiple comorbidities, severe acute GVHD, relapse | Bhatt et al., 2021 |
NOTE: auto = autologous transplant; allo = allogeneic transplants; DFS = disease-free survival; GVHD = graft-versus-host disease; HCT = hematopoietic stem cell transplantation; RIC/NMA = reduced-intensity conditioning/nonmyeloablative (i.e., therapies given in conjunction with HSCT).
SOURCE: As presented by Stephanie Lee, November 15, 2021.
- Mental dysfunction, such as depression, anxiety, post-traumatic stress disorder
- Cognitive issues, such as memory problems
- Symptoms related to transplant or disease, such as fatigue, pain
- Comorbidities, such as diabetes, cardiovascular disease
- Risk of infections, particularly if experiencing GVHD or taking immunosuppressants
Following HSCT, patients may require frequent medical care, visits to clinics, and hospitalizations, which may lead to absenteeism. In addition, said Lee, many disabilities arenot visible to others, nor are they self-limited. As rates of transplantation among older andsicker patients increase and as “gentler” approaches to transplantation are implemented, said Lee, itis unclear whether these shifts will result in better overall health for transplant survivors, or whether they will result in more people surviving in poorhealth.
In conclusion, Lee emphasized the key points she had made duringher presentation:
- Many patients are already disabled beforetransplantation.
- Patients receiving autologous transplants recover more quickly and have fewerlate effects, but their self-reported health at 1 year is similar to patients whoreceived allogeneictransplants.
- Transplant patients have a high burden of comorbidities, ongoing medical care, and compromised function and quality of life. These effects improve with time butplateau with about 70 percent of survivors reporting goodrecovery.
- Around 50 to 80 percent of transplant survivors return to work orschool.
- Rates of posttransplant disability burden will rise as transplants are performed formore and sickerpatients.
DISCUSSION
Following the presentations, Appelbaum led panelists in a discussion by asking aseries of questions, some of which were posed by the workshopparticipants.
Q1: How much does HSCT improve survival compared to standard of care for patients with multiple myeloma?
Horowitz saidis very clear that autologous transplantation improves progression-free survivalafter multiple myeloma, and it isnow clearly “part of the armamentarium” for patients who can tolerate a transplant. Horowitz added that compared to standard of care, the question is not whether to perform a
transplant, it iswhen. Appelbaum added that while the advantage of transplantation compared to conventionaltherapy was clear in early randomized studies, there have been major advances in therapies formultiple myeloma in recent years. These advances have necessitated new studiescomparing transplantation to conventional therapy. Horowitz agreed but noted that thenontransplant approaches are also associated with significant disability and morbidity; they “each havetheir impacts,” shesaid.
Q2: Why are long-term outcomes so similar between autologous and allogeneic transplant patients? What are the long-term outcomes for patients who receive donations from mismatched unrelated donors, mismatched haploidentical relatives, or umbilical cord blood?
Appelbaum said that the data that Lee presented on the similarity in outcomesbetween patients receiving autologous and allogeneic transplants were surprising; he said he wouldhave expected patients undergoing autologous transplants to have better outcomes. Lee said there isa bias in the field that expects better outcomes from autologous transplants, but that the data donot reflect this. She opined that the similarities in outcomes could be attributable to a number offactors, including similarities in pretransplant treatments, similarities between thetransplants themselves, and similarities in comorbidities and health status. Horowitz added that inboth populations, some patients receiving HSCT have undergone multiple rounds of othertherapies before transplantation, which means that their functional status and well-being reflectthe cumulative effects of these pretransplanttherapies.
HSCT using non-HLA-matched donors is a more recent development, said Lee, sothere is a lack of long-term data on these populations. Horowitz said that while it is likely still bestto have a matched donor, the differences are “modest at best.” She said there is no reason tothink that long-term disability would be substantially different among thesepopulations.
Q3: What are the reasons that not all patients who should get a hematopoietic stem cell transplant are getting a transplant? What can be done to overcome this gap, and what are the implications for racial and ethnic minorities?
There are a number of reasons why patients are not getting transplants, said Horowitz;a major barrier is the fact that knowledge about successful transplants with mismatched donorshas not yet been disseminated in the oncology community. Other barriers are common for alltypes of intensive medical therapy; these include barriers of geography, lack of money orinsurance, and lack of a caregiver. Further, there are disparities in access to care based on race, ethnicity, andsocioeconomics.
Q4: How can we prevent or decrease disability after HSCT? Would these efforts be cost-effective? How much of the disability is predictable before transplant?
Appelbaum noted that there have been recent advances in transplant care, such asnew therapies for preventing GVHD. At the same time, HSCT is increasingly being offered tomore and older patients. Lee said that these factors could potentially result in an increase in theoverall number of patients who are disabled after HSCT. “Some of the patients that would have died5 or 10 years ago are surviving,” but they may be in poor health, she said. Currentdisability prevention efforts include better prophylaxis for GVHD, prehabilitation that aims atmaking patients stronger before a transplant, and aggressive rehabilitation after a transplant toimprove functional status.
Appelbaum asked about the cost-effectiveness of these efforts, andLee responded that “prevention is always better than cure.” She said she is pleased that there isa focus on outcomes such as quality of life, rather than a simple survival/nonsurvivaldichotomy. In terms of predicting posttransplant disability, Horowitz said that in general, poor quality of life before a transplant predicts poor quality of life after a transplant. Whenpatients have many comorbidities, or have undergone multiple aggressive treatments prior totheir transplant, they are more likely to be disabled after undergoing a transplant. Lee addedthat although this is true, the transplant itself has a significant effect on posttransplanthealth.
Q5: What would you tell a patient if he or she asked, “Why should I do a hematopoietic stem cell transplant?”
For many patients, said Appelbaum, transplantation is the only opportunity to cure. For example, patients with high-risk acute myeloid leukemia have “no chance for cure” oncethey have relapsed, other than HSCT. In other circumstances, he said, a transplant is used toextend life, but “at a cost.” Lee said although transplant survivors experience a number ofnegative effects, many of them rate their overall quality of life as good. When faced with the alternativeof death, many patients adapt to their “new normal” and find meaning and beauty in theirposttransplant life. Patients have told her “how thankful they are that they were able to havea transplant and see their grandkids and kids grow up.” Horowitz opined that only a smallminority of patients come to regret having a transplant. Most patients, she said, even if they cannotreturn to work, do return to a reasonable quality oflife.














