
3
Considerations for Staffing, Effects on the Workforce, and Future Trends
As Mehta mentioned earlier in the workshop series, while many traditionally consider “stuff” to be the limited resource within health care, such as oxygen, ventilators, blood, or drugs, it is often “staff” shortages that cause issues and lead to considerations for shifting to contingency or crisis standards of care (CSC) modes. Staffing shortages and their accompanying challenges have been encountered throughout the pandemic across sectors, making this notion painfully clear. In this chapter, the speakers highlight some of the key staffing challenges encountered throughout the COVID-19 pandemic, discuss specific issues with nurses and emergency medical services (EMS) personnel, and present potential short- and long-term solutions and best practices that have been employed over the last few years to attempt to mitigate some of the staffing shortfalls felt in various areas. Speakers discussed some of the changes enacted through emergency measures that should remain even after the crisis ends. Finally, invited speakers reflected on the ongoing nursing crisis in particular and discussed ways to improve the profession for the future.
EFFECTS OF COVID-19 ON THE WORKFORCE
Asha Devereaux, senior medical officer, Sharp Coronado Hospital, highlighted first responders, nurses, and doctors as the key stakeholders for the discussion. She shared a disaster response framework showing the continuum of care from conventional to contingency to crisis (see Figure 3-1).
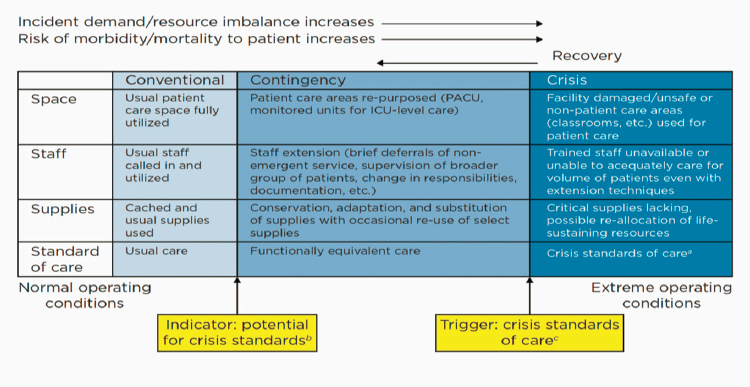
SOURCE: Asha Devereaux presentation, October 11, 2021.
The original developers of this CSC framework envisioned indicators between the conventional and contingency phases that would help determine when the change was coming, and then triggers to know when to shift into crisis phase. This is not what happens in reality, she said. Instead, the lines are much more blurred and uncertain. Devereaux noted that even before the pandemic, there were staffing shortages, antiquated hiring and staffing mechanisms, a failure to view nurses as key talent within an organization, scope-of-practice policies lacking flexibility, and unusual payment structures financing the nursing workforce. The speakers discussed some of these issues and their contribution to staffing challenges in a crisis.
The Consequences of Moral Injury
Intuitively, there are many lessons learned, from many events, on how to move into CSC and how to address those crises, said Jeanette Ives Erickson, chief nurse emerita, Massachusetts General Hospital. Painting a picture of the country in February 2020, Erickson said, “We didn’t know what we didn’t know.” However, pretty quickly, many ancillary services or nonessential surgeries and care delivery were cancelled, and those health workers found themselves thrown into an emergency response with varying levels of training. She concluded that the concept of intact teams was lost. She echoed Devereaux’s concerns about the workforce shortages that existed even before the pandemic and said that now there is a projected worldwide shortfall of 18 million health workers by 2030, mostly in low- and lower-middle income countries (WHO, n.d.).
She reviewed some of the current issues with the health care workforce, noting that 30 percent are considering leaving their profession, and nearly 60 percent reported experiencing negative effects on their mental health as a result of their work throughout the pandemic (Kirzinger et al., 2021). Erickson emphasized that it is imperative that clinician burnout be given more attention as many of them have become cynical, exhausted, and have little sense of personal accomplishment this long into the pandemic. What is needed in this current moment, she said, is the courage to push on behalf of the workforce to build new systems and structures and invest in people. Erickson concluded that the real worry is about people in general and their moral distress and suffering, and that this is the bigger issue that demands attention.
Staffing Challenges across Sectors
Cynda Hylton Rushton, professor of clinical ethics, School of Nursing at Johns Hopkins University, built on Erickson’s presentation, referencing the importance of the moral burden for the health care workforce. If you are the person deciding which person is seen first and who needs care the most, in an emergency room full of patients who need care, knowing that your decisions may likely cause harm to someone, it weighs heavily on you, she said, and it can lead to an accumulation of moral residue and suffering. She added that the pandemic has made this issue a chronic and unrelenting experience, a corrosive form of moral suffering, not just an episodic issue when there is a busy day. Rushton reported that 32 percent of clinicians and 38 percent of nurses had clinically significant symptoms of moral injury, showing how pervasive these consequences are (Rushton et al., 2021). She explained that moral injury is associated with posttraumatic stress disorder, increased depression, medical errors, and suicidal thoughts, creating another layered burden for clinicians, in addition to physical and psychological exhaustion.
While she appreciated the difficulty in distinguishing between the different standards of care, Rushton said that most clinicians have been operating in the contingency phase. But lacking regulatory and legal protections, they have been left to make individual allocation decisions without the benefit of a triage team or guidelines about how to resolve difficult ethical questions. She noted that this piece has been missing from this effort. She recalled her own time spent creating elegant allocation schemes for ventilators, blood, and drugs but realized they did not put the same effort into navigating the best ways to allocate human resources.
In the United States there are roughly one million EMS clinicians working in EMS agencies, said Gamunu Wijetunge, EMS specialist, Office of EMS, National Highway Traffic Safety Administration. In the course of
1 year, they typically respond to about 40 million events and 9-1-1 calls. Prior to the pandemic, it was common for clinicians to work at multiple positions, but this practice expanded during COVID-19 with clinicians working at many different locations, which has resulted in a strain on the 9-1-1 portion of EMS. In 2009, HHS led a nationwide assessment of state pandemic plans, revealing that there was no real planning for treatment of patients without transporting them to the hospital (HHS, 2009). Wijetunge explained that in his opinion, this was largely owing to reimbursement policy dating back decades, and that laws and regulations did not allow for “treat and refer.”
Andrew Garrett, associate professor at George Washington University’s School for Medicine and Health Sciences and senior advisor at the Office of the Assistant Secretary for Preparedness and Response (ASPR) at HHS, commented that the typical surge staffing model relied on by health care in most disasters has been a source of constraint in the pandemic. He highlighted two main practices within the model, saying often times the workforce just works harder and faster to get through it, thinking it will only last days or weeks, and then if that does not work, they borrow resources from other sources. Both of these practices have become problematic during a long-term pandemic, whether talking about personnel at a local hospital level or regional or state trade of an EMS compact. He explained that the pandemic has broken this all-hazards model that has worked fairly well up until now, and it has become clear that novel solutions, beyond those in the normal repertoire, are now needed.
Garrett said that workers cannot just work harder and faster to get it done; instead, we need to reimagine how crises and disasters are thought about and planned for in the United States, moving away from the short-term, high-impact disasters and shifting toward longer, more drawn out public health crises. Additionally, on top of the demands of 2020 and the pandemic, the rest of the world did not go away, Garrett noted. The year 2020 saw many large hurricanes that were added to the pandemic challenges, and staff and resources that would typically be needed for those responses became even more difficult to access and strained systems to the breaking point (Garrett, 2020).
Coming off of another week in the ICU at his hospital, Ryan Maves, professor of infectious disease, Wake Forest School of Medicine, said that stepping back as an attending physician and looking at the workforce implications of the current situation, he found two things most striking. The first was team cohesion, as there have been lots of shifts in where providers work and a lot of nurses moving because of travel agency work. As a result, he said there is a lack of continuity in busier hospitals, so every day it seems like you are working with a new team. He stated that one of the strengths of working in critical care typically is the mutual trust among
everyone on the team. You know what each person’s strengths are, and you know you can depend on them in stressful situations But with the current situation, care teams are meeting new people every day, and that mutual trust is lost. It influences efficiency when, for example, staff are actively decompensating patients, because one provider may not know what a nurse on the team knows, or the intubating process might be different, and this is an ongoing challenge.
The second factor he found striking, also alluded to by Anuj Mehta, is not a lack of physical beds, but a lack of people to staff them. Everyone is shifting their scopes of practice to try and optimize the workforce and pushing patients out into wards under care of staff that would never normally be expected to manage this level of patient severity, he explained, and this has a real effect on patient safety. There are benefits, as the system adapts over time and people learn new skills, but while that is happening, it can be extremely disruptive to have providers running around in three places with ICU nurses also functioning in the emergency department. He pointed out that typically within an ICU there are multiple different stakeholders on the team responsible for different procedures and tasks that they specialize in. He explained that this flexibility is not available anymore, and the pool of people to draw from has become smaller and smaller. At what point does the word disaster no longer apply, Maves asked, and at what point does this just become the way the world works?
Implications of Overburdened Staff and Lack of Team Culture
After the speakers’ remarks, Devereaux asked about the structural impediments to communication of strain or stress. For example, in Florida during the height of the surge, doctors had gag orders placed on them for asking for help, and clinicians have been fired for vocally calling for assistance. What are some challenges in this area? Rushton agreed it was certainly a problem, and while violence against health care workers was present before, it has only escalated during the pandemic. Health care work is interconnected with societal injustice and structural disadvantages, she said, and many people are angry and outraged at different things. Previously there was a level of safety at your workplace, but now, no one feels safe. Rushton shared that we may be seeing the erosion of societal trust. In her work, the most common theme around moral injury was broken trust and the sense of betrayal. For example, institutions say that there are resources for clinicians to address mental health issues, but there is a culture that is associated with stigma and shame for those clinicians to admit that they need help.
Erickson added to the discussion about the lack of team cohesion by explaining that the continuous movement of staff between various clinical settings and between various teams leads to questions of safety. She pon-
dered on how best to respond to the moment while ensuring the health care workforce remains safe. She pointed to the importance of taking a pause and getting back to the basic principle of human connection, and added that safety huddles throughout the day should be built into the structures and routine practices for care delivery.
Prior to the pandemic, there was an increasing focus on safety culture within EMS, said Wijetunge. He noted the ongoing need brought about by the pandemic to be more people centered and team centered, so patient and provider safety as well as mental health issues are being prioritized. More broadly, he added that one of the lessons learned is the critical need for more cross-sector collaboration, so EMS, public health, health care, and emergency management are all working closely together, with the challenges clearly outlined. Garret agreed that the health care system was thought of as much more integrated than it truly is, and existing fractures became highly magnified when the pandemic began.
There are cultural barriers to discussing the problems in EMS, said Garrett. He explained that typically an ambulance picks up a patient and drops them off at the hospital, and that the system evolved that way because of how these services are paid for in the United States. He added that if these everyday problems cannot be fixed, it will be difficult to implement even better models when there is a disaster. He suggested reimagining what the health care system looks like, from prehospital integrated health care to all specialties, with a “one coordinated fight” kind of approach to dealing with these major national catastrophes.
Devereaux asked about the lack of disaster preparedness and how that contributes to moral injury. Maves responded that the notion of triage is something that is well trained for in the military, and in that context people understand that in situations of austere resources, the priority should be to achieve the greatest good for the greatest number of people. However, this concept has only been in the civilian world for the last 18 months with constant triaging in health care. Maves believed that the pandemic opened up a window where the health care workforce can be trained in the concept of resource limitation, integrating it into a better appreciation for palliative care. He added that despite the circumstances, it is important to understand that even CSC are “standards of care,” and there is always an ability to provide some care.
He noted that although health care workers always want to do more, it is important for them to accept that sometimes a certain level of care is what is available. He acknowledged that education will help better prepare providers for these decisions, but it will not be sufficient to remove the moral burden, and it will take a long time for the clinical community to get used to this idea. Rushton agreed that the moral burden will not be erased and that there is a need to better understand how to help people carry it
without so much cost to themselves. She concluded that the process needed to be rehumanized and the focus shifted towards what is needed to better support both the people being cared for and those providing care.
PROMISING STAFFING STRATEGIES AND FUTURE DIRECTIONS
Lisa Rowen, chief nurse executive, University of Maryland Medical System, highlighted key strategies for managing staffing and workforce challenges across three time frames: today (immediate), short term (1–3 months), and longer term (greater than 3 months) (see Figure 3-2).
She suggested using technology for inpatient observation, such as teleobservation, instead of having a human observing the patient for safety. She explained this would allow for a more optimal use of both nurses and certified nurse assistants, because they do not have to stay in one room and deal with donning and doffing of personal protective equipment (PPE). She noted that staffing strategies have been the same for decades across the country; there are opportunities to streamline and optimize documentation and to deliver care so that it provides for and supports staff so they can gain time back in their day. There are also opportunities to create innovative roles, such as a “mobility tech,” that can be filled by exercise physiology graduates who are interested in the work instead of certified nursing assistants, who are often difficult to recruit. Finally, for long-term strategies, she shared that providers can optimize how they order care and treatment to avoid lengthening the time nurses spend providing that care and treatment. Additionally, some providers are creating an integrated, innovative model
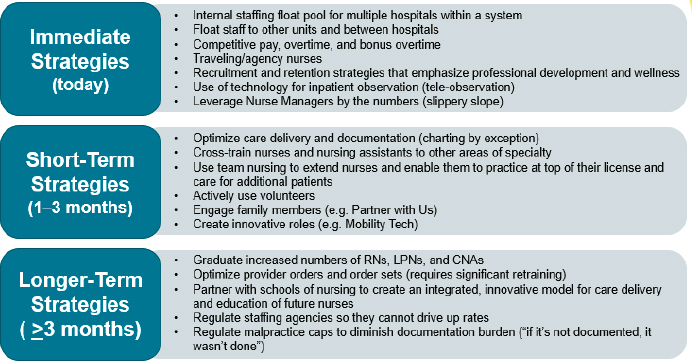
SOURCE: Lisa Rowen presentation, October 11, 2021.
for care delivery and education by partnering with schools of nursing to align their clinical setting with the new education standards.
California completed its CSC concept of operations in 2020 after being put on hold, said Howard Backer, medical director, California Medical Assistance Teams, California EMSA, and the state turned out to be a miniature model of the country given the variety of surge needs and outcomes during COVID-19. He reported three main areas of managing surge: regulatory support, surge missions, and staffing models. All the interventions had an effect on staffing, whether they were direct or indirect.
The first step to manage surge is through regulatory support, he said, including declarations and regulatory or executive orders that may come from the governor, health officer, or EMS director in a state. Examples of this include expanded nurse–patient ratios, expanded scope of practice for EMS, licensing for retired or out-of-state providers, and a vaccine mandate for health care workers. Next, he explained, they had multiple surge missions that affected hospitals, such as through skilled nursing facilities support, alternate care sites, and load balancing across institutions, which was often challenging because of the amount of high-flow oxygen that ambulances needed to carry to support patients during transport. Finally, he reviewed some of their staffing models for this support, which included California’s Disaster Medical Assistance Teams, which were highly mobile and flexible, as well as the National Guard, students, and retired personnel. He concluded by stating that this range of strategies used in California is what allowed them to stay out of the CSC phase, though he acknowledged they did go right up to the threshold of entering CSC.
Using Technology for Staffing
For technological solutions to staffing, Alistair Erskine, chief digital health officer, Mass General Brigham Hospital, shared that technology played a critical role across all environments of Mass General. Even for phone and online chat options, his hospital was able to quickly develop low-code or no-code algorithms, which could be adapted throughout the day, to advise patients and change the route of care and where people were being directed based on the hospitals’ staffing capacities and bed availability. A second strategy was to have patients help, using patient portals and augmented capacity to be able to schedule visits using online tools and remove the burden from phone calls by embedding the virtual visits directly into provider workflow and the patient portal.
To avoid hospitalization of patients, the hospital also had virtual observation units where patients who typically would have been admitted were discharged home with a pulse oximeter and monitored virtually by staff. For acute care interventions, Erskine said that after ICUs were overwhelmed
in Boston during the first wave, staff realized the solution was to form a virtual ICU. The hospital needed a dashboard for ICU awareness, so Erskine’s staff virtualized the consultation of the ICU doctor and remote monitoring across the hospital system. Medical isolation was also an important issue to overcome, so the hospital purchased tablets for every hospitalized patient and converted rooms to video and audio, which, similar to Rowen’s strategies, saved nursing time in donning and doffing PPE.
Staffing shortages in medical surgery led to making virtual rounds, so there was a much smaller team in hospital, he explained. But this way, even staff who had been exposed and needed to be quarantined could still work remotely and safely write notes and place orders. The hospital also needed to conduct COVID-19 testing and vaccinations for staff, so a portal was created for employees that included daily scheduling of testing and shots and another dashboard was created for staff awareness. This also included a mental health app to support staff.
One thing that was missing, Erskine noted, was a scalable, automated communication strategy for patients, as the outreach for patients missed the opportunity to gather responses from them about their treatment. They tried to manually identify high-risk patients to prioritize invitations to schedule a COVID-19 test or vaccination but realized that using the EMR transactional system to do so was very work intensive. A consumer relationship management tool that many retail organizations use could do this in a much more efficient and streamlined way, he said, so they are now in the process of creating that.
Supporting Health Care Workers
Alexander Niven, associate professor in pulmonary and critical care medicine at the Mayo Clinic, proposed potential solutions to the epidemic of burnout in health care workers that has occurred since March 2020. It is important to highlight the balance between resilience and workplace stressors, he said, as this was tilted in the wrong direction even prior to the pandemic. This imbalance is forcing health care workers into situations where they are regularly engaging in nonfunctional overreaching, which translates to increased burnout and errors. An important part of the conversation that is often left out are the stabilizing influences that can come from the quantity and quality of work, Niven explained, and the influences of cultural support within teams and health care organizations. Those elements are out of individuals’ direct control, and the scope goes beyond the individual. If left unaddressed, he underlined the potential damage to care that is delivered to patients and the potential damage done to the system in terms of lower-quality care, medical errors, decreased productivity, and increased turnover and costs (see Figure 3-3).
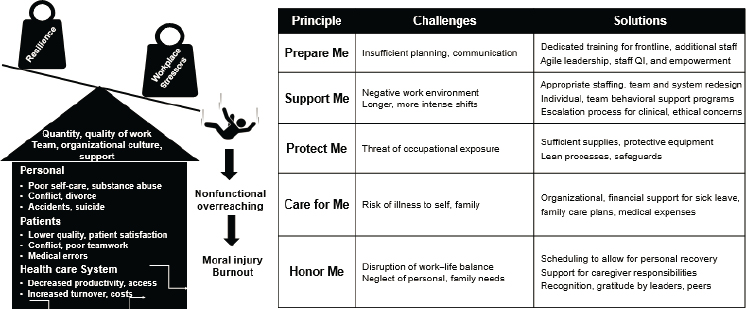
SOURCE: Alexander Niven presentation, October 11, 2021.
All of these ramifications underline the moral imperative that needs to be added to this existing dashboard for the learning health care system to improve, stated Niven. Dashboards already exist to look at safety, quality, cost, and performance on a regular basis; adding validated measures for staff burnout to that dashboard and monitoring it regularly would require marginal additional commitments. Also displayed in Figure 3-3, Niven shared some challenges and solutions based on a series of interprofessional focus groups conducted by Stanford University early in the pandemic. People are able to focus on delivering high-quality care when they do not have to worry about their own safety and security, Niven said. Creating organizational support structures that include sick leave, family care plans, caregiver assistance, and allowing a scheduling system that does allow for recovery can significantly help mitigate staff burnout.
Discussion on Structural Impediments to Staffing
While some have proposed increasing the number of new nurses and graduates as a solution to these challenges, a participant asked if these new recruits are just being put into the same environment that is causing current staff to leave. Rowen responded that the biggest reason staff are feeling burned out and demoralized is the lack of staff and other team members to share the burden of patient care. Nursing is typically a 90 percent female workforce, and 70 percent of them have either children or parents they are caring for, with the COVID-19 crisis amplifying those needs. Rowen added that she believes the travel nurse industry greatly reduced the number of nurses available to staff hospitals and clinics, in part because those agen-
cies were able to offer elevated pay rates, as high as $275/hour (salaried nurses would make two-thirds of that), and it became difficult for hospitals and health care centers to retain their staff and compete with these rates. However, she does believe that graduating more nurses and putting them in acute care settings will rebalance the equation, because the need for travel nurses lessens and more nurses will be in positions at the bedside. Early in the pandemic, Devereaux noted that many providers were furloughed or sidelined from work, which is what contributed to increased numbers in these alternate agencies or workforces.
Highlighting a related question, Devereaux asked if the health care workforce is lumped in as a resource, like a ventilator, that can be driven into CSC. She asked whether it was the right way to think about staff. Niven responded that humans are more than just a resource. He reiterated the importance of interpersonal relationships and shared his experience in creating a high-performing health care team. These concepts cross the gap between the bedside and the digital environment being created. He stated that human beings are naturally going to look for personal security and family security first, which are reasonable core values and should be considered by health systems if they want to retain a highly skilled and seasoned workforce. Without that, he continued, there will be a loss of manpower and constant turnover and staff churn, which degrades overall workflow and quality. Erskine added that those health care workers will need to adapt to the technology system and system of care, which involves training and electronic learning to bring the person up to speed, and this will take additional time and effort.
Devereaux asked how funding has become a challenge for staffing solutions and what the concerns might be. Rowen responded that paying high rates for certain services, like travel nursing, takes money away from what we can do about pay rates and benefits for internal staff. Hospitals are directing a huge amount of funding toward this temporary, mobile workforce instead of investing in loyal workers, committed to an institution, she continued. Backer added that in California there have been several mentions about the importance of highly functional teams. While this is easier to do with long-term staff, in a disaster you have to be more creative and bring in staff from many different sources—sometimes blending national, state, local, and occasionally military backgrounds. He added this may need to become a part of normal daily options for health care systems.
Health care is under stress at the best of times, and it could just take a bad flu season to use all the resources of a hospital and require tents and additional surge staffing. The State of California found that during the first few waves of COVID-19, the state covered all the costs for staffing. When the state tried to wean recipients off of state funding and send them to contract agencies to maintain the added capacity, he noted there was a
lot of resistance, so it had to be a very gradual process. Another point of response is that there were different compositions of teams, and Backer said EMS personnel are a good way of supplementing health care teams because they are flexible. Backer concluded that paramedics cannot replace nurses but they complement them quite well in an acute care setting. But once a hospital changes back from crisis and contingency to standard conventional care, then often the regulation exemptions and the territoriality of professional societies and unions returns and brings challenges to the mixed staffing models.
Emergency Changes That Should Become Standard
Devereaux raised another question: which of the changes seen recently in health care should remain permanent? Rowen replied that during the crisis hospitals changed what was required for documentation and charting and moved to exceptions for charting. Clinicians then assumed things were okay unless it was documented that something was not done. This change flipped how we document, she said, and it actually saves a lot of time, so we are now moving toward making this our standard practice. Erskine added that patient expectation also changed significantly regarding virtual care. There is no putting the “genie back in the bottle.” Knowing the level of convenience and reduced costs that come with virtual care, he predicted that this trend will likely persist. But there may need to be ongoing legislation about what can and cannot be done. Erskine noted that this idea was taken from the retail industry and applied appropriately in the health care space to let patients self-serve and have health care become less of a black box, while making providers more available at the patient’s schedule. This is a good change that should persist, he added.
Niven stated that from his standpoint, his organization broke down many siloes regarding staffing individual work areas and was able to maximize capacity and capabilities both within and outside the organization. His organization also recognized, especially in COVID-19 ICUs, that bedside care with PPE demands was extremely difficult, so it used the increased demand for electronic health resources as an opportunity to rotate staff and expand the pool of workers who can engage in those services to give them a break from the extremely burdensome PPE. Backer added that the long-term nature of this response has ingrained the emergency management concepts and practices deeply into the health care system. Not only do health systems and facilities know how to go into emergency mode and request resources, he said, but the process has become more embedded into common knowledge. Rowen also noted that her organization focused on team member wellness throughout the past 20 months, which has been appreciated. Management and leadership teams were prioritized, and this
will be something that will continue, as the health of all team members is prioritized moving forward.
REFLECTIONS ON THE NURSING CRISIS AND FUTURE DIRECTIONS
Tener Goodwin Veenema, contributing scholar and professor of nursing at Johns Hopkins Center for Health Security, presented some final reflections on the current nursing crisis throughout the country. The most dangerous thing that can be done, she argued, is to go back to normal and business as usual. She called for transformational change to create and sustain safer and more supportive workplace settings. This should include taking care of employees and humanizing workplace settings, designing systems to treat people with respect and value, and build the trust needed in order to build those trusted teams. Health care systems, hospitals, and other settings need to acknowledge nurses as talent, she said, just like any other workforce that needs to be recruited, developed, and maintained. She listed various ideas to improve the crisis, shown in Box 3-1.
COVID-19 has reopened old wounds in terms of professional hierarchies and lack of a voice within nursing, Veenema stated. She added that the value of nursing has long been obscured by hospital accounting practices that treat nurses more as undifferentiated labor costs. Additionally, while many traveling nurses are very committed and put their own health at risk in order to work, that system is adversely affecting the nursing workforce overall. She pointed to the existence of perverse payment structures that perpetuate this fragmented and disjointed system and concluded that there was a need to investigate how the nurses of this country can be better served.
In terms of understanding moral injury and supporting health care workers, Niven highlighted a final gap: there is no data regarding respiratory therapists, EMTs, or other allied health workers. That is something that needs to be understood and measured if solutions are to be found. Erskine added that people have realized health care is very labor dependent, but there are some places and processes that are amenable to technological solutions. It is incumbent on us to understand which aspects can be automated and how to share in decision making to augment care, he explained. Rowen added that there is a duty to partner with schools, whether nursing, medicine, or others, and “do it differently.” As students and interns are integrated into clinical settings, the model of care needs to be morphed into something different and more sustainable, she said, so students get a better bedside education and current staff get better support within various settings. Backer added that even the best facilities and hard infrastructure cannot provide health care without staff. While equipment and ventilators can be shifted around easily, staff cannot, and it remains the number one needed element, he said.














