
The first workshop, held April 8, 2022, featured an introductory session about global demographic changes, five presentations that described datasets for dietary assessment of older adults, and a panel discussion with the workshop speakers. The datasets and surveys discussed included nutritionDay,1 the Baltimore Longitudinal Study on Aging and InChianti Study, National Health and Nutrition Examination Survey (NHANES), National Health and Aging Trends Study (NHATS), and Longitudinal Aging Study Amsterdam (LASA).
INTRODUCTION: CHANGING DEMOGRAPHICS
Heather Keller, University of Waterloo (UW) and Schlegel-UW Research Institute for Aging, presented a brief overview of global demographic trends to illustrate the timeliness and importance of discussing the role of diet in healthy aging. She shared maps from the United Nations (UN) Population Division that illustrate the rapid aging of the world’s population. The first map distinguished countries based on the percentage of their population aged 65 and older (Figure 2-1). In 1950, that was only 5–10 percent in almost all countries, whereas nearly 70 years later, it comprises more than 10 percent and up to 25–30 percent in many countries.
In addition to the rapid aging of populations worldwide, Keller continued, an increase in life expectancy at age 65 has occurred in many countries, and the gap between countries on this metric has narrowed overall (UN DESA Population Division, 2019). The UN projections of life expectancy at birth for individuals born between 2025 and 2030 indicate that much
___________________
1www.nutritionday.org (accessed September 14, 2022).
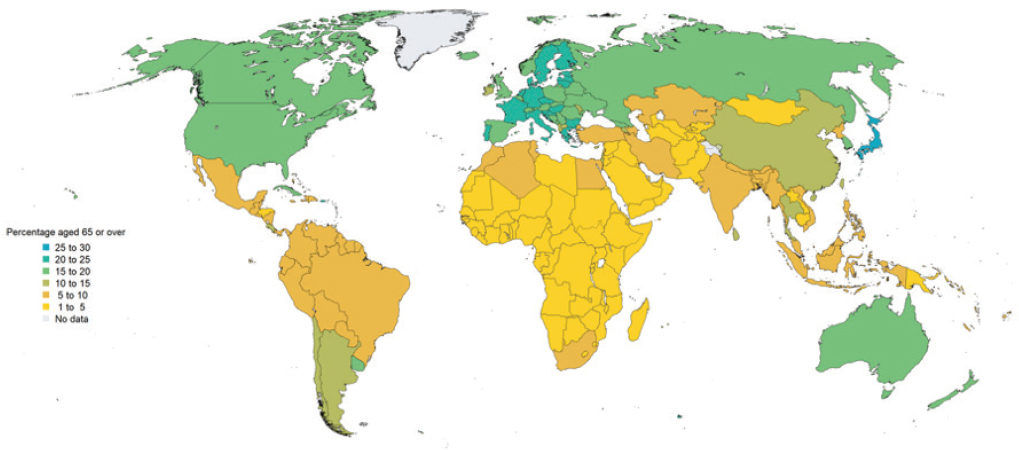
SOURCE: Presented by Heather Keller on April 8, 2022 (UN DESA Population Division, 2019).
of the world will be expected to live beyond 70, and a sizable proportion will be expected to live beyond 80 (UN DESA Population Division, 2019). Keller underscored the importance of considering the impact of these shifts on population health, and she highlighted the role of diet in healthy aging. According to a study that put forth nine habits for longevity (Buettner and Skemp, 2016), two of them are directly related to diet—eat plants and stop eating when 80 percent full.
Keller relayed that the World Health Organization (WHO) has recognized demographic changes and designated 2021–2030 as a “decade of healthy aging.” In its baseline report on healthy aging, WHO described it as a “process of developing and maintaining functional ability that enables well-being in older age” (WHO, 2021), which Keller said essentially equates functional ability with not being frail. Diet is closely connected with frailty, a condition that often overlaps with sarcopenia and malnutrition. Frailty can result from a variety of contributing factors, and diet probably plays a role (WHO, 2021).
NUTRITIONDAY
Dorothee Volkert, Friedrich-Alexander-University of Erlangen-Nürnberg, discussed nutritionDay, a worldwide, 1-day cross-sectional audit on nutrition care held annually in hospitals and nursing homes. NutritionDay is an awareness initiative that was adopted to improve knowledge about disease-related malnutrition and nutrition care and improve patient safety by monitoring quality of nutrition care globally. Its vision is to achieve standardized nutritional assessment in all institutions and a discussion of malnutrition as a public health concern at the political level. Institutions are invited to participate for free, and standardized questionnaires are available for local nursing staff to collect data and enter them in a joined online database.
Volkert focused on the nursing home setting for the nutritionDay initiative, explaining that the focus is on older adult residents, in contrast to the hospital settings, where patients of all ages can participate. She shared examples of nursing home questionnaires—one for collecting information about the institution, including characteristics such as unit size and nutritional routines; another for collecting information about individual residents; and a third for 6-month follow-up data collection, which tracks mortality, hospital admissions, and falls. Only three questions on the resident questionnaire are concerned with nutrition and food intake, and they ask about intake during a given day, the past week, and the past 3 months.
She highlighted the large size of the nutritionDay database as a strength and the absence of energy and nutrient intake information as a limitation. Between 2007 (the year the initiative commenced) and 2015, that more than 30,000 residents from 20 countries were represented in the nursing
home database, with an additional 10,000 residents from 17 countries participating from 2016 to 2020 (when a shorter version of the questionnaires was in use). The initiative’s database is available for analysis with a signed data use agreement and accepted research proposal submitted to the nutritionDay office. Volkert noted that data analysis may be performed by the nutritionDay office in Vienna or by researchers themselves. Several publications using the dataset are available, such as a descriptive analysis of indicators for reduced food intake (Schindler et al., 2016); research on prevalence and associated factors for low food intake in hospital patients from different medical specialties (Bohne et al., 2022); and an annual report highlighting that around one-third of nursing home residents ate half or less of the lunch meal on the annual assessment (Tarantino et al., 2022).
Volkert added a few comments about dietary assessment in institutions serving older adults. Such settings typically contain physically and/or mentally impaired populations, which makes self-assessment of dietary intake via recall or records infeasible. On a positive note, the meal plan and menus are well known, with mostly standardized portions. Volkert suggested that nursing home staff perform dietary assessment using either plate diagrams to estimate the proportion of a meal or specific food items consumed, estimated food records, or weighed records—which are the gold standard but also the most laborious.
BALTIMORE LONGITUDINAL STUDY ON AGING AND INCHIANTI STUDY
Luigi Ferrucci, National Institute on Aging at the National Institutes of Health (NIH), shared data from the Baltimore Longitudinal Study on Aging (BLSA) and Invecchiare in Chianti (“aging in the Chianti area” [InChianti]) study. Ferrucci believed that nutrition is “the culprit of how we age”—aging and health are surely affected by food consumed throughout the lifetime.
Ferrucci described the dietary assessment component of the BLSA. This cohort study collected 3–7-day dietary records among a relatively healthy population between 1984 and 1992 and again between 1994 and 2003. The time and labor intensiveness of this practice led to its replacement with food frequency questionnaires (FFQs) in 2003, which is completed by the respondent or administered by an interviewer via phone or in person. BLSA examines respondents’ adherence to three dietary patterns (and diet quality) that have been associated with positive health outcomes: Mediterranean, Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND), and Alternate Healthy Eating Index (AHEI).
Ferrucci shared data on the percentage of BLSA participants with “high adherence” (i.e., top tertile based on a score that considers consumption frequency of various food groups and key nutrients) to one of these three dietary patterns (Figure 2-2). He pointed out a substantial age effect that is
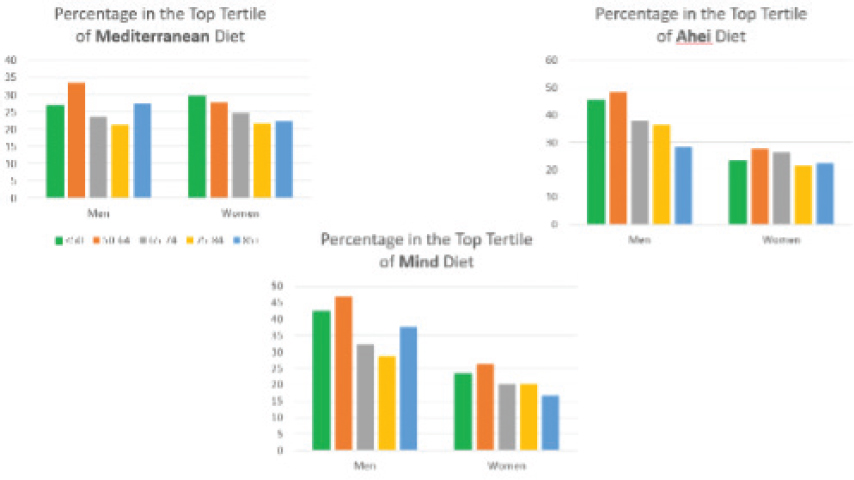
SOURCE: Presented by Luigi Ferrucci on April 8, 2022.
seemingly sex dependent—women have an increasingly lower likelihood of high adherence to Mediterranean or MIND diets as age increases.
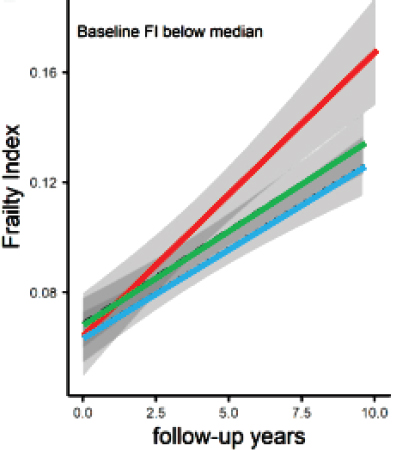
Ferrucci shared data on the relationships between varying levels of adherence to a Mediterranean-style diet and the health outcomes of mobility decline and frailty. In one cross-sectional analysis, all three tertiles of adherence (high, medium, and low) to the diet at baseline were nearly identical in terms of score for a key metric of mobility decline; but, over time, participants with low adherence showed a significant reduction in mobility compared to those with high adherence (Milaneschi et al., 2011). Another cross-sectional analysis demonstrated that higher adherence is inversely associated with developing frailty in community-dwelling older men and women (Talegawkar et al., 2012).
Ferrucci indicated that longitudinal data provide consistent results, which he illustrated with findings from a cohort study that observed accelerated frailty among participants with baseline frailty index (FI) measures below the median and low adherence to the Mediterranean diet during a 10-year follow-up period (Figure 2-3).
Another longitudinal study examined adherence to a Mediterranean diet and cognitive decline among participants in the InChianti study. During a follow-up period of nearly 20 years, Ferrucci reported that an accelerated decline in cognitive function was observed among participants who had low
SOURCE: Presented by Luigi Ferrucci on April 8, 2022 (Tanaka et al., 2021).
adherence (Tanaka et al., 2018). This effect seemed to be mostly attributable to intakes of vegetables, fish, legumes, and fruit and nuts.
Ferrucci also mentioned data on the relationship between varying levels of adherence to a MIND intervention diet and physical function and grip strength in older adults. He shared evidence of an accelerated decline in physical health among participants in the lowest tertile of adherence (Talegawkar et al., 2022).
According to Ferrucci, reporting bias is a challenge of dietary assessment. To address this, his group is working to evaluate dietary intake using blood and urine biomarkers. Ferrucci shared a study that found a strong correlation between total urinary polyphenol and mortality but a null effect between the two when total dietary polyphenol was calculated on a participant-reported questionnaire (Zamora-Ros et al., 2013). He suggested that the best approach is probably a combination of self-reported and objective dietary assessment tools.
Ferrucci moved on to potential mechanisms by which the different diets affect health outcomes. One effect is certainly epigenetic, given evidence indicating that consuming fish, fruits, and vegetables; moderating alcohol intake; high socioeconomic status and level of education; and regular physical activity were associated with a “slower epigenetic clock” (a slower progression of aging; Quach et al., 2017). In contrast, central obesity, high triglyceride and low HDL cholesterol values, high systolic blood pressure, presence of inflammatory markers, dysregulated insulin function/elevated glucose levels, and meat consumption were associated with faster epigenetic aging.
Another mechanism by which diet affects health is the metabolites that are produced as a result of dietary intakes, Ferrucci continued, and the Mediterranean, MIND, and AHEI diets similarly affect metabolomic biomarkers (Tanaka et al., 2022), which other researchers have also observed. Different dietary patterns have different effects on many metabolites, and he stated that dietary intervention to target any single metabolite is misguided.
Ferrucci shared evidence to demonstrate that for the MIND and AHEI dietary patterns, metabolomic signature strongly mediated the association between dietary pattern and frailty index—60–80 percent of the outcome was driven by metabolomic signatures produced by the intervention diet (Tanaka et al., 2022). These findings are important because they indicate that metabolite presence and levels can be an objective measure of dietary quality.
NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY
Shinyoung Jun, National Cancer Center in Korea, shared findings from the NHANES, a nationally representative survey operated by the National Center for Health Statistics (NCHS) at the Centers for Disease Control and Prevention. NHANES has been a continuous program since 1999 and collects cross-sectional data from approximately 5,000 people annually, with a target population of noninstitutionalized, civilian residents in the 50 states and the District of Columbia. Jun explained that the sampling method is a multistage, stratified, clustered design with sampling domains that aim to reliably represent age, sex, income, and race and Hispanic origin subgroups.
Jun described NHANES’ extensive data collection methods. Participants first complete an in-home interview during which they provide sociodemographic information, disclose any medical conditions, and answer questions about diet behaviors and food security and food assistance program participation. They also provide containers and labels for any dietary supplements used during the past 30 days, along with the frequency, dose, and amount of each. During a second phase of data collection, participants complete a physical examination at the NHANES mobile examination center that includes body measurements, a blood draw, clinical examinations, and a 24-hour dietary recall. A second 24-hour dietary recall is collected by telephone 3–10 days later. Both recalls query participants about intake of foods, beverages, and dietary supplements. Jun explained that dietary data processing begins when NHANES interviewers type responses into computers for direct transmission to NCHS databases, where coders process the data into information about dietary supplement use and food and beverage consumption. Dietary supplement use is converted to nutrient intake from supplements using the NHANES dietary supplement database, and food and beverage consumption is converted to nutrient intakes using the U.S. Department of Agriculture (USDA) Food and Nutrition Database for Dietary Studies.
Dietary supplement use is high among older adults (60+ years old), with the majority using at least one (Figure 2-4). Most supplement users reported multiple products, with the most common being multivitamin and minerals, vitamin D, omega-3, B-complexes, calcium and vitamin D, and vitamin C (Gahche et al., 2017).
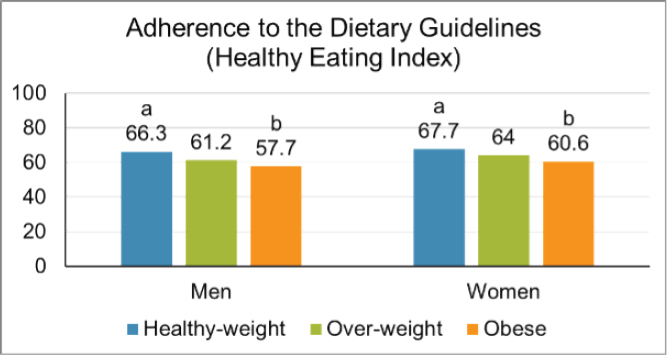
Jun stated that when only foods and beverages (and not dietary supplements) are considered, dietary quality (as measured by adherence to the Healthy Eating Index [HEI]) is generally low. Her team’s assessment of nutrition status by body weight status among older adults (≥60 years of age) who completed both 24-hour dietary recalls for NHANES found that the mean HEI scores were lower among those with obesity (body mass
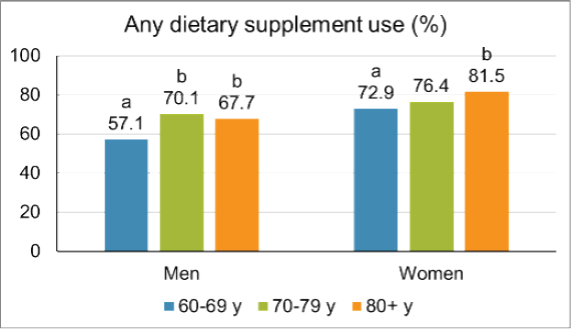
NOTE: Letters (a) and (b) at the top of the columns indicate significant differences from each other.
SOURCE: Presented by Shinyoung Jun on April 8, 2022 (Gahche et al., 2017).
index [BMI] ≥30 kg/m2) than those at a healthy weight (BMI 18.5–24.9 kg/m2) (Figure 2-5).
Jun pointed out that a strength of NHANES is that total usual nutrient intake estimation (from both dietary supplements and foods and beverages) is possible: “usual nutrient intake” is a long-term, average intake that can be compared to recommended levels, such as the dietary reference intakes, and “total usual nutrient intake” is the usual intakes from both diet (foods and beverages) and supplements. Long-term intake is difficult to measure, but can be estimated from short-term measures by applying statistical techniques. At least one 24-hour recall from all participants and a second 24-hour recall from a subsample is needed to derive usual nutrient intake from diet, and a combination of a 30-day dietary supplement frequency questionnaire plus the two 24-hour recalls may be the ideal way to capture usual nutrient intake from dietary supplements (Bailey et al., 2019; Cowan et al., 2020).
Jun shared her research estimating total usual intake for several nutrients designated as underconsumed by the Dietary Guidelines for Americans. Many older adults were found to be at risk of inadequate intake for several of those (which include calcium, magnesium, zinc, folate, vitamin B6, vitamin B12, vitamin C, and vitamin D), but including dietary supplements considerably reduced the proportion of those at risk (Jun et al., 2020). Jun noted that women who had obesity had a higher risk of inadequacy for calcium, magnesium, vitamin B6, and vitamin D (as did men with obesity,
SOURCE: Presented by Shinyoung Jun on April 8, 2022 (Jun et al., 2020).
for magnesium) compared with women who had a healthy weight. This finding implies that obesity may coexist with micronutrient inadequacy, despite a common assumption that people with obesity have adequate or excessive food intakes and thus must have adequate micronutrient intake.
Another finding from the same research, Jun continued, was that health risks may cluster in certain population subgroups. About 40 percent of U.S. older adults have obesity, and in addition to the coexistence of obesity with lower dietary quality and micronutrient inadequacy, other risks included self-reported fair or poor overall health, five or more prescription medications used, limitations in activities of daily living, metabolic risk factors, osteoporosis, and participation in the Supplemental Nutrition Assistance Program (SNAP).
Jun listed challenges of using NHANES dietary data, which are cross-sectional and thus lacking temporality. In her view, the biggest challenge is that the data are self-reported and therefore subject to recall bias, which might become magnified among older adults who are experiencing cognitive decline. Proxy reporters may supplement a respondent’s reporting, but that has its own limitations. Jun highlighted that data from participants older than 80 are top-coded for privacy, which makes characterizing the “oldest old” challenging. In addition, NHANES targets noninstitutionalized older adults and requires participants to come to the mobile examination center, which may attract a relatively healthy older adult population. Another challenge is the need to regularly update the dietary supplement database to keep pace with the dynamic market for these products.
Jun ended by listing strengths of the NHANES dietary data collection methods. Its ability to produce nationally representative estimates makes it suitable for informing health policy and programs, and the wealth of sociodemographic and health information collected can enable identification of vulnerable subgroups. In-home interview in tandem with a product inventory for dietary supplement intake is a useful method to reduce recall bias, because interviewers check the labels and bottles. Recall bias can also be addressed by use of biomarkers, whereby blood and urine samples are used to produce biomarker information that may calibrate self-reported dietary intake if the nutrient of interest has a potential or known biomarker.
NATIONAL HEALTH AND AGING TRENDS STUDY
Rose Ann DiMaria-Ghalili, Drexel University, explained how her research team used data from the NHATS to produce robust estimates of malnutrition in community-dwelling older adults at a national level. She began by stating that older adults are at risk for malnutrition due to contributors such as physiological changes associated with aging, medications, dietary changes, social conditions, economic factors, and chronic health conditions. In hospitals, malnutrition or nutrition risk affects 12–72 percent of older adults depending on diagnostic criteria used, and some larger datasets of U.S. inpatient samples indicate that patients coded for malnutrition in this setting tend to be 65 and older and have greater infection rates, lengths of stay, costs, and morbidity and mortality rates. Older adults with a malnutrition diagnosis are more likely to be admitted to the hospital from and to be discharged to a skilled nursing facility (Corkins et al., 2014; DiMaria-Ghalili and Nicolo, 2014, p. 3; Heersink et al., 2010).
Turning to the prevalence of malnutrition among U.S. community-dwelling older adults, DiMaria-Ghalili said that gaps remained because a nationally representative sample with this information is not known. About a decade ago, data were collected using an adapted Mini Nutritional Assessment (MNA) as part of the Southeast Pennsylvania Household Health Survey, and 6 percent of such adults were malnourished and 54 percent were at risk (DiMaria-Ghalili et al., 2013). An opportunity to obtain such information on a national level became available in the years following, she said, by conducting a secondary analysis of the NHATS longitudinal cohort.
DiMaria-Ghalili provided a brief overview of the NHATS study, funded by the National Institute on Aging, which is a nationally representative sample of Medicare beneficiaries 65+ that began in 2011 to study late-life disability trends and trajectories. Participants complete in-person assessments and answer questions about medical, social, functional, and technology domains. NHATS collected dried blood samples containing inflammatory
biomarkers during its seventh round of data collection in 2017, which her group obtained special permission to use.
To explain how her team assessed malnutrition among NHATS participants, DiMaria-Ghalili recapped the six topics assessed in the MNA:2 food intake, weight loss, mobility, psychological stress or acute disease, neuropsychological problems (dementia or depression), and BMI. She explained that her group identified items in the NHATS survey that aligned with the MNA, which allowed them to construct a derived MNA from the survey data. The resulting MNA screening score could calculate derived nutrition status score: 12–14 points is normal, 8–11 points is at risk for malnutrition, and 0–7 points is malnourished (Guigoz, 2006; Kaiser et al., 2009; Rubenstein et al., 2001; Vellas et al., 2006). The research team also examined other variables, such as sociodemographic factors (gender, age, living arrangement), health status (self-rated health, chronic conditions, falls, hospitalization), food security, and inflammation.
DiMaria-Ghalili discussed the research sample size and findings: 4,472 participants were included, after exclusion based on factors such as living in a nursing home. After applying weights to the sample, it represents 31 million U.S. older adults in 2017. Based on the MNA-derived screening score, 68 percent were normal, 26 percent were at risk for malnutrition, and about 6 percent were malnourished. DiMaria-Ghalili elaborated on characteristics of participants who were more likely to have malnutrition, which she said included older age (relative to the sample), female gender, living alone in the community, and living in (non-nursing-home) residential care, such as assisted living. No difference was observed by race or ethnicity.
Findings were also stratified by self-reported health-related variables, which indicated that individuals with malnutrition were more likely to self-report their health as fair or poor, have more chronic conditions, and report both falls and hospitalizations in the past year. These results are consistent with findings about malnutrition risk factors among older adults. When nutritional status was examined by food security, individuals with malnutrition were more likely to use Meals on Wheels but no differences in nutrition status were observed based on other food security questions, such as skipping meals due to lack of money or participating in federal food assistance programs.
DiMaria-Ghalili highlighted her study’s assessment of inflammatory markers and malnutrition, noting that a reason for heightened interest in diagnosing malnutrition is based on the inflammatory aspects of the condition. NHATS collected two biomarkers of inflammation, C-reactive protein (hsCRP) and interleukin-6 (IL-6), via dried blood samples. These specimens made it possible for the research team to calculate that compared
___________________
2www.mna-elderly.com (accessed September 14, 2022).
with individuals with normal nutrition status, individuals with malnutrition were more likely to have hsCRP levels above the median, and those at nutritional risk were more likely to have IL-6 levels above the median. In other words, older adults who have or are at risk for malnutrition also have inflammation.
DiMaria-Ghalili shared a few conclusions. Despite the limitation of deriving nutrition status based on NHATS items mapped to the MNA, the study’s results indicate that malnutrition is not limited to the hospital setting and that an interrelationship exists between malnutrition and inflammation in older adults. She espoused interdisciplinary approaches to address malnutrition in community-dwelling older adults to promote healthy aging and suggested that future work examine the impact of malnutrition on health outcomes and relationship to physical performance.
THE LONGITUDINAL AGING STUDY AMSTERDAM
Marjolein Visser, Vrije Universiteit Amsterdam, discussed assessment of dietary intake in older adults participating in the LASA. This nationally representative sample from the Netherlands includes more than 5,000 participants and uses a multidisciplinary approach that focuses on physical, cognitive, psychological, and social aging over time. The first cohort of approximately 3,100 people was recruited in 1992, and a new cohort of approximately 1,000 people has been added to enrich the sample every 10 years (in 2002 and 2012) as well as a migrant cohort (in 2013) of the first generation of Turkish and Moroccan people in the Netherlands (Hoogendijk et al., 2016, 2020; Huisman et al., 2011). Visser recounted that nutritional status was an area of focus from the beginning, but dietary assessment was not performed until 2014–2015. The resulting data have been used to examine a number of relationships, such as dietary patterns and depression, protein intake and functional outcomes and sarcopenia, and dietary protein intake and overall diet sustainability.
Visser explained that individuals in the study were invited to participate in ancillary studies—more than 1,400 out of approximately 2,000 eligible individuals completed an FFQ. This response rate of 68.9 percent was higher than the response rate in the national dietary survey, and she attributed nonresponses to people who are either very frail or relatively young, active, and short on time. The FFQ was offered on paper or digitally, she said, and about half of the sample completed it online. The online questionnaires had fewer missing data than the paper questionnaires, Visser added, because respondents skipped pages on the latter.
She described the FFQ, which queried respondents on frequencies and portion sizes of nearly 240 food items during the prior 4 weeks. Participants could indicate consumption amounts using standard units (e.g., slices of
bread) and household units (e.g., tablespoons) and by selecting pictures that represented their typical consumption. She explained that questionnaires were excluded if they had missing items or reported implausibly high energy intakes. However, those with implausibly low energy intakes were not excluded, as is often done with FFQs. This decision was made because the 24-hour recall data for a subset of participants indicated that many older people have habitually low energy intakes. The 24-hour recall data were available because some participants who completed the FFQ were selected for three 24-hour recalls as part of a validation study. The FFQ was developed for a wide age range, so the researchers wanted to assess whether it would also be valid in a sample comprised exclusively of older people.
Visser shared the methodology for the three 24-hour recalls; two were performed on weekdays and the third on a weekend. Prior to the first recall, participants received information about best practices for measuring food quantities using frequently used kitchenware and a picture book with portion sizes. During the interviews—which were unscheduled so as not to influence intake on the interview day—interviewers asked participants to reference the picture book. Eighty-eight individuals with an average age of 71.9 were included in the sample, which was deemed sufficiently representative of the total FFQ sample (Visser et al., 2020).
Visser discussed the validation results for macronutrients, a selection of micronutrients, and a selection of food groups. For energy and macronutrients, the group-level bias was small, and the quintile agreement was moderate to high (i.e., most individuals were ranked in the same or adjacent quintiles of intake on both the FFQ and the 24-hour recall). For most micronutrients and food groups, the Pearson’s correlation coefficients were moderate, and for all the micronutrients and most food groups, quintile agreement was moderate to high. An exception was legumes and fish because the FFQ overestimated intake of those food groups and they are not well captured in 24-hour dietary recalls due to infrequent consumption and low daily intake.
Relative to other Dutch FFQ validation studies conducted in younger adults, Visser indicated similar or only slightly lower Pearson’s correlations. This suggests that FFQs are as valid in older adults, and the validity of the FFQ is similar to that of FFQs in older adults from other countries. She also noted that conducting 24-hour recalls by phone is less affected by the participant’s visual or physical limitations as compared with an FFQ.
Visser shared the study’s methods for assessing dietary supplement intake. In several survey waves, specific supplement use was queried via interviewer-administered questions at home. This led to suboptimal recording of information, such as failure to report specific vitamins, such as vitamin D, that were part of multivitamin supplements. In more recent waves of the survey, all dietary supplements were recorded in the same
way as medication use (participants provided all bottles and containers of prescribed and nonprescribed supplements used during the past 2 weeks, and interviewers recorded label information [brand name, dose, concentration, etc.]). It would seem that this method easily lends itself to calculating intake of nutrients through supplements, but it is more challenging than it may seem. Despite an annual updating of the Dutch Supplement Database with new brands, labels, and concentrations, it is still a challenge to obtain their true intake. As true dietary supplements are often not included in the database, people may face difficulty or make errors when inputting them. This challenge led Visser’s team to develop an algorithm to ensure the best estimate of nutrient intake from dietary supplements among older adults (Figure 2-6).
PANEL DISCUSSION WITH SPEAKERS
Following the six presentations, speakers answered questions from the workshop planning committee and attendees about a variety of topics related to dietary assessment of older adults: using biological specimens to assess dietary intake, assessing and addressing inflammation, assessing supplement use, stratifying cohorts by age beyond 80 years, using technology, issues associated with clinical populations, priority metrics to collect in clinical settings, and vision for future dietary assessment practices.
Using Biological Specimens to Assess Dietary Intake
In response to a question about the utility of biological specimens for enhancing dietary assessment methods, Ferrucci stated that the science of evaluating dietary intake through biomarkers is advancing. He encouraged routine use of biomarker data, such as metabolomic assessment reports, in clinical settings to evaluate dietary quality of older adults. The costs could be reasonable if done at a large scale, and collecting objective markers of intake would be less burdensome on providers and patients than asking them to complete traditional dietary assessment instruments. DiMaria-Ghalili urged consideration of how to bridge the gap of what is feasible in research settings versus clinical practice, noting that advances in knowledge and tools are gradually broadening the scope of what is possible in health care settings. Visser added that different assessment methods and biomarkers are needed to produce estimates of how well an individual’s diet aligns with recommended dietary patterns versus intake of single nutrients, to which Regan Bailey, session moderator, commented that triangulating
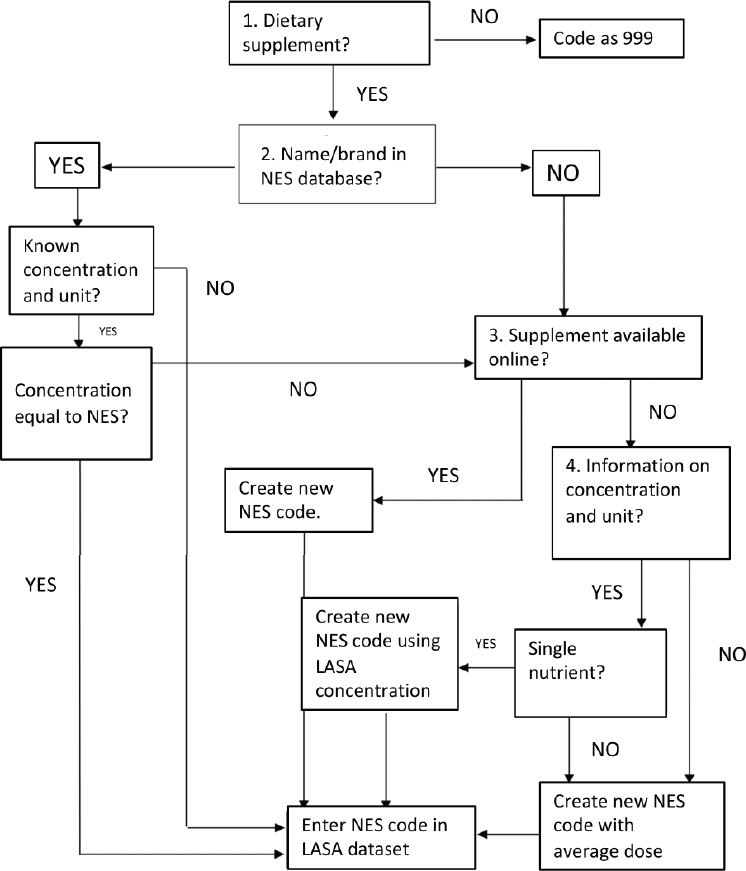
NOTE: NES = Dutch supplement database; LASA = Longitudinal Aging Study Amsterdam.
SOURCE: Presented by Marjolein Visser on April 8, 2022.
exposure from several complementary methods of assessment is a viable approach.
Assessing and Addressing Inflammation
Another question related to biomarkers was how to consider inflammation when assessing dietary intakes of older adults, given its effect on nutrient digestion and absorption. Ferrucci emphasized that inflammatory status is affected by diet and physical activity, stress, and other factors, and despite accumulation of high-quality evidence about inflammatory biomarkers and their relationship to health outcomes, they are rarely measured in practice. He urged researchers to consider how inflammation—chronic or acute—might affect older adults’ nutritional requirements, referencing the increased protein requirement in the context of high inflammation due to its effects on muscle protein synthesis. Jun agreed, suggesting that because dietary reference intakes are designed for healthy people, they may need to be revised (evidence permitting) for the many individuals with multiple chronic conditions that promote an inflammatory state. Volkert added that because inflammation impairs appetite, it is important to identify strategies to improve food intake. Ferrucci raised the possibility of dietary strategies to block inflammation and ensuing disease, urging research to identify nutrition interventions.
Assessing Supplement Use
Visser replied to a question about strategies to assess supplement use in older adults; open-ended recall via questionnaire is much less effective than asking participants to provide the actual bottles. Researchers can then query participants about dose and copy information from the label about brand, nutrient content, and ingredients (this information may also be contained in databases used for dietary assessment studies), although she cautioned that label (or database) information may not always match the actual contents due to factors such as deterioration over time or changes in formulation without updates to the label (or database).
Stratifying Cohorts by Age Beyond 80 Years
A workshop participant asked about the value of separating study cohorts into further age-defined subgroups after 80 to observe differences in health outcomes DiMaria-Ghalili confirmed that NHATS data are available for individuals over 80 and could be stratified beyond that point, but for NHATS and other studies, some of these data may be restricted and less accessible for analysis. Keller shared that examining cohorts by 5-year
age subgroups (e.g., 80–85, 86–90) could help focus analysis and might be considered moving forward.
Using Technology
Keller recalled Visser’s comment about the positive uptake of a digitally based FFQ in one of her studies and asked what advice she would give to others interested in using technology for dietary assessment of older adults. Visser elaborated that half of participants voluntarily opted to complete the FFQ digitally, which she attributed to a high prevalence of Internet use in the Netherlands across socioeconomic groups. She urged others to consider rates of Internet use by demographic groups in a study’s geographic area, lest results be biased by different rates in certain age or income groups, for example.
Issues Associated with Clinical Populations
Keller asked the speakers to consider approaches to improve dietary assessment in clinical populations, which are vulnerable to malnutrition and frailty. Ferrucci raised the issue of anorexia among aging clinical populations, stating that low food intake and appetite, along with declining weight, is often associated with depression. He suggested that assessment tools consider anorexia and its risk factors, including those that might seem trivial, such as the ability to chew and swallow easily. Visser called attention to the seemingly opposite issue of obesity in older adults, which she said is often overlooked and also often associated with low protein intake. Volkert added that the ability to self-report food intake depends on cognitive ability, physical status, and frailty status, and she wondered if research had examined the validity of dietary assessment in the oldest old (>80) in residential settings. Bailey and Jun pointed out that NHANES has a subset of participants 80 and older, which they thought could be compared to older adults in the 60- and 70-year ranges. DiMaria-Ghalili suggested that waves of data collection with U.S. longitudinal cohorts incorporate nutrition measures to generate standardized measures across study populations.
Priority Metrics to Collect in Clinical Settings
Ferrucci responded to a related question about which metrics should be prioritized for collection in clinical settings, remarking that this question is “enormously complex.” He observed that free-living older adult populations have been more well studied than those in nursing homes or residential assisted-living facilities, which vary widely in how they are operated. Researchers and clinicians could contact the people who care directly
for residents in those facilities to understand how things work there and what questions should be part of a dietary assessment. He urged a continued focus on disease prevention through good nutrition and attention to existing problems, such as anorexia. Volkert provided a list of measures to assess, including appetite (i.e., desire to eat), weight, and recent weight history. DiMaria-Ghalili suggested that because of the overlap among common conditions in older adults (e.g., malnutrition, sarcopenia, frailty, cachexia), it may be helpful to use an appropriate metric to help differentiate conditions so that intervention and treatment can be provided accordingly (noting that some treatments may be suitable to address more than one condition). Visser mentioned that body weight is often monitored at nursing homes in the Netherlands to watch for malnutrition, but measures of diet quality, such as fruit and vegetable intake, are important but rarely collected. Keller shared that in her experience assessing food intake in long-term care populations, more than half of participants did not meet dietary intake recommendations for one-third of vitamins assessed (Keller et al., 2018). Lack of knowledge may be part of the problem, Visser suggested, referencing her research that indicated unawareness among older adults of protein sources (e.g., one-third of the sample thought that tomato contained more protein than an equivalent weight of beef) and recommended intake amounts (e.g., many people in the sample thought that one meal per day with a good protein source was adequate) (Visser et al., 2021).
Opportunities for Future Dietary Assessment Practices
The final question asked speakers to describe one change they would like to see in nutrition assessment for older adults. DiMaria-Ghalili said she would like nutrition screening or assessment to be added to the Medicare annual wellness exam. In Ferrucci’s dream world, people would think about and recognize how their current dietary choices shape their future health and experiences; young people tend to think that their food choices do not matter, but evidence indicates that early life choices accumulate to have an impact on health and disease as one ages. Visser agreed and added that she would want people to realize that it is never too late to adopt healthier eating habits and that doing so has immediate benefits. Jun imagined that technological advances in assessment methods, such as image-based approaches, could greatly reduce the burden of current methods. A newer approach that Visser said she would like to see expanded is a version of ecological momentary assessment, whereby participants receive messages in an app at random times of the day for weeks and are prompted to enter what they consumed in the past hour. This is a relatively low-burden approach, with satisfactory validity data.
REFERENCES
Bailey, R. L., K. W. Dodd, J. J. Gahche, J. T. Dwyer, A. E. Cowan, S. Jun, H. A. Eicher-Miller, P. M. Guenther, A. Bhadra, P. R. Thomas, N. Potischman, R. J. Carroll, and J. A. Tooze. 2019. Best practices for dietary supplement assessment and estimation of total usual nutrient intakes in population-level research and monitoring. Journal of Nutrition 149(2):181–197.
Bohne, S. E. J., M. Hiesmayr, I. Sulz, S. Tarantino, R. Wirth, and D. Volkert. 2022. Recent and current low food intake—prevalence and associated factors in hospital patients from different medical specialities. European Journal of Clinical Nutrition 76(10):1440–1448.
Buettner, D., and S. Skemp. 2016. Blue zones: Lessons from the world’s longest lived. American Journal of Lifestyle Medicine 10(5):318–321.
Corkins, M. R., P. Guenter, R. A. DiMaria-Ghalili, G. L. Jensen, A. Malone, S. Miller, V. Patel, S. Plogsted, H. E. Resnick, and American Society for Parenteral and Enteral Nutrition. 2014. Malnutrition diagnoses in hospitalized patients: United States, 2010. Journal of Parenteral and Enteral Nutrition 38(2):186–195.
Cowan, A. E., S. Jun, J. A. Tooze, K. W. Dodd, J. J. Gahche, H. A. Eicher-Miller, P. M. Guenther, J. T. Dwyer, A. J. Moshfegh, D. G. Rhodes, A. Bhadra, and R. L. Bailey. 2020. Comparison of 4 methods to assess the prevalence of use and estimates of nutrient intakes from dietary supplements among U.S. adults. Journal of Nutrition 150(4):884–893.
DiMaria-Ghalili, R. A., Y. L. Michael, and A. L. Rosso. 2013. Malnutrition in a sample of community-dwelling older Pennsylvanians. Journal of Aging Research & Clinical Practice 2(1):39–45.
DiMaria-Ghalili, R. A., and M. Nicolo. 2014. Nutrition and hydration in older adults in critical care. Critical Care Nursing Clinics of North America 26(1):31–45.
Gahche, J. J., R. L. Bailey, N. Potischman, and J. T. Dwyer. 2017. Dietary supplement use was very high among older adults in the United States in 2011–2014. Journal of Nutrition 147(10):1968–1976.
Guigoz, Y. 2006. The Mini Nutritional Assessment (MNA) review of the literature—what does it tell us? Journal of Nutrition, Health & Aging 10(6):466–485; discussion 485–487.
Heersink, J. T., C. J. Brown, R. A. DiMaria-Ghalili, and J. L. Locher. 2010. Undernutrition in hospitalized older adults: Patterns and correlates, outcomes, and opportunities for intervention with a focus on processes of care. Journal of Nutrition for the Elderly 29(1):4–41.
Hoogendijk, E. O., D. J. Deeg, J. Poppelaars, M. van der Horst, M. I. Broese van Groenou, H. C. Comijs, H. R. Pasman, N. M. van Schoor, B. Suanet, F. Thomese, T. G. van Tilburg, M. Visser, and M. Huisman. 2016. The Longitudinal Aging Study Amsterdam: Cohort update 2016 and major findings. European Journal of Epidemiology 31(9):927–945.
Hoogendijk, E. O., D. J. H. Deeg, S. de Breij, S. S. Klokgieters, A. A. L. Kok, N. Stringa, E. J. Timmermans, N. M. van Schoor, E. M. van Zutphen, M. van der Horst, J. Poppelaars, P. Malhoe, and M. Huisman. 2020. The Longitudinal Aging Study Amsterdam: Cohort update 2019 and additional data collections. European Journal of Epidemiology 35(1):61–74.
Huisman, M., J. Poppelaars, M. van der Horst, A. T. Beekman, J. Brug, T. G. van Tilburg, and D. J. Deeg. 2011. Cohort profile: The Longitudinal Aging Study Amsterdam. International Journal of Epidemiology 40(4):868–876.
Jun, S., A. E. Cowan, A. Bhadra, K. W. Dodd, J. T. Dwyer, H. A. Eicher-Miller, J. J. Gahche, P. M. Guenther, N. Potischman, J. A. Tooze, and R. L. Bailey. 2020. Older adults with obesity have higher risks of some micronutrient inadequacies and lower overall dietary quality compared to peers with a healthy weight, National Health and Nutrition Examination Surveys (NHANES), 2011–2014. Public Health Nutrition 23(13):2268–2279.
Kaiser, M. J., J. M. Bauer, C. Ramsch, W. Uter, Y. Guigoz, T. Cederholm, D. R. Thomas, P. Anthony, K. E. Charlton, M. Maggio, A. C. Tsai, D. Grathwohl, B. Vellas, C. C. Sieber, and M. N. A.-International Group. 2009. Validation of the Mini Nutritional Assessment Short-Form (MNA-SF): A practical tool for identification of nutritional status. Journal of Nutrition, Health & Aging 13(9):782–788.
Keller, H. H., C. Lengyel, N. Carrier, S. E. Slaughter, J. Morrison, A. M. Duncan, C. M. Steele, L. Duizer, K. S. Brown, H. Chaudhury, M. N. Yoon, V. Boscart, G. Heckman, and L. Villalon. 2018. Prevalence of inadequate micronutrient intakes of Canadian long-term care residents. British Journal of Nutrition 119(9):1047–1056.
Milaneschi, Y., S. Bandinelli, A. M. Corsi, F. Lauretani, G. Paolisso, L. J. Dominguez, R. D. Semba, T. Tanaka, A. M. Abbatecola, S. A. Talegawkar, J. M. Guralnik, and L. Ferrucci. 2011. Mediterranean diet and mobility decline in older persons. Experimental Gerontology 46(4):303–308.
Quach, A., M. E. Levine, T. Tanaka, A. T. Lu, B. H. Chen, L. Ferrucci, B. Ritz, S. Bandinelli, M. L. Neuhouser, J. M. Beasley, L. Snetselaar, R. B. Wallace, P. S. Tsao, D. Absher, T. L. Assimes, J. D. Stewart, Y. Li, L. Hou, A. A. Baccarelli, E. A. Whitsel, and S. Horvath. 2017. Epigenetic clock analysis of diet, exercise, education, and lifestyle factors. Aging 9(2):419–446.
Rubenstein, L. Z., J. O. Harker, A. Salva, Y. Guigoz, and B. Vellas. 2001. Screening for undernutrition in geriatric practice: Developing the Short-Form Mini-Nutritional Assessment (MNA-SF). Journals of Gerontology, Series A, Biological Sciences and Medical Sciences 56(6):M366–372.
Schindler, K., M. Themessl-Huber, M. Hiesmayr, S. Kosak, M. Lainscak, A. Laviano, O. Ljungqvist, M. Mouhieddine, S. Schneider, M. de van der Schueren, T. Schutz, C. Schuh, P. Singer, P. Bauer, and C. Pichard. 2016. To eat or not to eat? Indicators for reduced food intake in 91,245 patients hospitalized on nutritionDays 2006–2014 in 56 countries worldwide: A descriptive analysis. American Journal of Clinical Nutrition 104(5):1393–1402.
Talegawkar, S. A., S. Bandinelli, K. Bandeen-Roche, P. Chen, Y. Milaneschi, T. Tanaka, R. D. Semba, J. M. Guralnik, and L. Ferrucci. 2012. A higher adherence to a Mediterranean-style diet is inversely associated with the development of frailty in community-dwelling elderly men and women. Journal of Nutrition 142(12):2161–2166.
Talegawkar, S. A., Y. Jin, E. M. Simonsick, K. L. Tucker, L. Ferrucci, and T. Tanaka. 2022. The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet is associated with physical function and grip strength in older men and women. American Journal of Clinical Nutrition 115(3):625–632.
Tanaka, T., S. A. Talegawkar, Y. Jin, M. Colpo, L. Ferrucci, and S. Bandinelli. 2018. Adherence to a Mediterranean diet protects from cognitive decline in the Invecchiare in Chianti study of aging. Nutrients 10(12).
Tanaka, T., S. A. Talegawkar, Y. Jin, S. Bandinelli, and L. Ferrucci. 2021. Association of adherence to the Mediterranean-style diet with lower frailty index in older adults. Nutrients 13(4).
Tanaka, T., S. A. Talegawkar, Y. Jin, J. Candia, Q. Tian, R. Moaddel, E. M. Simonsick, and L. Ferrucci. 2022. Metabolomic profile of different dietary patterns and their association with frailty index in community-dwelling older men and women. Nutrients 14(11).
Tarantino, S., M. Hiesmayr, I. Sulz, and nDay Working Group. 2022. NutritionDay worldwide annual report 2019. Clinical Nutrition ESPEN 49:560–667.
UN (United Nations) DESA Population Division. 2019. World population prospects 2019. https://population.un.org/wpp/publications/files/wpp2019_highlights.pdf (accessed September 14, 2022).
Vellas, B., H. Villars, G. Abellan, M. E. Soto, Y. Rolland, Y. Guigoz, J. E. Morley, W. Chumlea, A. Salva, L. Z. Rubenstein, and P. Garry. 2006. Overview of the MNA—its history and challenges. Journal of Nutrition, Health & Aging 10(6):456–463; discussion 463–465.
Visser, M., L. E. M. Elstgeest, L. H. H. Winkens, I. A. Brouwer, and M. Nicolaou. 2020. Relative validity of the Helius Food Frequency Questionnaire for measuring dietary intake in older adult participants of the Longitudinal Aging Study Amsterdam. Nutrients 12(7).
Visser, M., Y. Hung, and W. Verbeke. 2021. Protein knowledge of older adults and identification of subgroups with poor knowledge. Nutrients 13(3).
WHO (World Health Organization). 2021. Decade of healthy ageing: Baseline report.
Zamora-Ros, R., M. Rabassa, A. Cherubini, M. Urpi-Sarda, S. Bandinelli, L. Ferrucci, and C. Andres-Lacueva. 2013. High concentrations of a urinary biomarker of polyphenol intake are associated with decreased mortality in older adults. Journal of Nutrition 143(9):1445–1450.
This page intentionally left blank.
























