
PATIENT STORY: MALLORY SMITH
“We’re losing the battle against bacteria,” stated Diane Shader Smith (Mother of the late Mallory Smith, author of Salt in My Soul, and AMR advocate). According to Shader Smith, despite years of messaging on the part of scientists and thought leaders, the issue has not penetrated the American consciousness the way it needs to. Shader Smith, whose daughter, Mallory, died in 2017 due to an antibiotic-resistant bacterial infection, emphasized that it is critical to hear the voices and understand the experiences of people living with and dying from AMR. Shader Smith suggests that storytelling is one way to get there.
Mallory was diagnosed with cystic fibrosis at the age of three. She had a happy childhood with no significant health challenges until she was colonized by Burkholderia cenocepacia, an opportunistic bacteria that commonly infects immunocompromised patients, at the age of 12. Suddenly, as her mother put it, “Mallory had an expiration date.” By high school, Mallory was in and out of the hospital, each time needing IV antibiotics for weeks to months. Despite her health challenges, Mallory was a typical, high-achieving teenager who got straight As and played three varsity sports. However, in the second half of her senior year, Mallory got very sick. She ended up attending her high school prom and was voted prom queen. Unfortunately, a student threw a smoke bomb into the venue, searing Mallory’s lungs, and she began coughing up blood.
These experiences instilled in Mallory a profound understanding of how precarious life is, said Shader Smith. Over the coming years, she was hospitalized repeatedly. These visits followed the same routine: cultures were taken, antibiotics were prescribed, drug susceptibility tests were performed, and antibiotic cocktails were adjusted. Shader Smith said that based on her lay understanding, antibiotic use is what leads to resistance. Better diagnostics could have helped Mallory.
AMR is a “complex, unpredictable, irreversible, progressive, painful, suffocating, choking weed,” said Shader Smith. As Mallory’s body deteriorated, her mind sharpened and she honed her writing skills. She spent the next 10 years documenting what it was like to live with a drug-resistant bacteria. Mallory graduated from Stanford University and wrote her first book, but AMR continued to wreak havoc on her life. Eventually, said Shader Smith, the only option left for Mallory was a lung transplant. Her insurance company initially denied the transplant; she was finally approved because her family “knew someone who knew someone.” Shader Smith said that skewed social and economic policies and care practices made things easier for Mallory than for others, and Mallory wanted to use her privilege and power of the pen to expose these injustices. While waiting for her transplant, Mallory wrote, “I want to maintain dignity to whatever
extent possible, to receive whatever lifesaving tactic is appropriate, to be able to communicate in some way, to have the blinds open for natural light, to have calming music to listen to, to have my mom or dad with me always. I want to live.”
The call for a lung transplant finally came, and despite a grueling recovery, Mallory celebrated her 25th birthday without supplemental oxygen. It was a happy time, said Shader Smith, and they dared to dream about a new life. However, a few weeks later, the B. cenocepacia infection returned, and Mallory was out of options. Mallory’s father reached out to Stephanie Strathdee, an epidemiologist who had used phages to help save her husband (Macpherson, 2021). Strathdee amplified the call on Twitter and pleaded with researchers around the globe for help in finding phage matches. Mallory was on a ventilator but scribbled a note to her loved ones: “Can’t talk at all, but so grateful you are all here for the hardest part.” A phage match was found, and Mallory became the first patient in the United States with cystic fibrosis to receive phage therapy. “We were filled with hope,” said Shader Smith, but the next morning the family had to make the “gut-wrenching decision” to remove Mallory from life support. The autopsy revealed that the therapy had started to work but not in time to save Mallory’s life.
Mallory’s writings were published posthumously as Salt in My Soul, which led to a documentary of the same name (Smith, 2019; 3Arts Entertainment, 2022). The Lancet published the largest study to date about superbugs at the same time the New York Times referred to Salt in My Soul as an awareness raising tool about the possibilities of bacterial phages (Antimicrobial Resistance Collaborators, 2022; Kenigsberg, 2022). “The seeds of my advocacy were planted by Mallory,” said Shader Smith. Mallory’s writing has enabled Shader Smith to share the patient voice, raise awareness, advocate for phage therapy, and address the need for better diagnostics. Shader Smith has taken on this advocacy role in a variety of settings, speaking at medical schools, bookstores, community events, conferences, Capitol Hill, and the White House. “I’m not a doctor, a scientist, a lobbyist, or a paid publicist,” said Shader Smith, “just a grieving mom trying to make sense of the world and my place in it.”
PANEL DISCUSION
Bioethics Perspective
Nicholas Evans (Chair, Associate Professor, University of Massachusetts, Lowell) observed that discussions about AMR rarely include a focus on bioethics or justice. Evans referenced several decades’ worth of National Academies’ publications on AMR and found no mention of “health equity.”
He did find one mention of “justice” in the context of AMR, but it was in a small subsection of a larger report about infectious disease research. A search on PubMed, said Evans, reveals only 16 articles that discuss bioethics and antimicrobial resistance. Evans suggested a few reasons for this gap. First, there may already be moral clarity on the issue of AMR; as he put it, “Antimicrobial resistance is bad. We should fix it.” Second, the field of bioethics has not historically focused on infectious disease. More recently, there have been bioethics discussions in areas of infectious disease, but they have tended to emphasize high-profile pathogens such as SARS or Ebola. The third reason, said Evans, is that AMR has received little public attention in general and for this reason may not be a priority for bioethicists. The published literature that addresses AMR mainly explores issues of distributive justice; that is, certain groups of people have access to antimicrobial medications while other groups have limited access.
In the context of rapid diagnostic development and use, Evans identified three pressing bioethical issues:
- Use of AMR diagnostics in research
- Diagnostic data and sample sharing
- Cost and access
Use of AMR diagnostics in research
In the United States, Federal Policy for the Protection of Human Subjects (‘Common Rule’) defines research as “a systematic investigation, including research development, testing, and evaluation, designed to develop or contribute to generalizable knowledge” (45 CFR, §46.102l). Public health surveillance activities are exempted from this policy. Evans argued that research using AMR diagnostics should be considered under the Common Rule given that diagnostics can be used to track the movement and evolution of resistant pathogens, thus contributing to generalizable knowledge. Evans recognized that this shift in policy would require diagnostics researchers to engage with an institutional review board (IRB), which can be a cumbersome process. To facilitate the process, there would need to be better data management, data harmonization, and data standards in place for rapid diagnostics for AMR. Elevating AMR diagnostics to research status under the Common Rule, said Evans, could open opportunities for product development pipelines and standard setting for treating drug-resistant bacterial infections.
Diagnostic data and sample sharing
In past public health efforts, there has been a lack of consistent attention and commitment to domestic and international data and sample sharing, said Evans. For example, during the 2006 avian influenza pandemic,
Indonesia decided to withhold avian influenza A H5N1 samples from the WHO due to concerns about global inequities and lack of access to vaccines for developing countries (Fidler, 2008). Another example was seen when Sierra Leone was unable to retrieve Ebola virus disease samples from the United Kingdom due to national security restrictions (Evans et al., 2020). Data and sample sharing are core concerns when it comes to global health equity and justice, said Evans, and ensuring access to results and samples is critical for controlling infectious disease and AMR.
Cost and access
Evans highlighted that the key equity drivers for AMR are cost and access as bioethicists regard AMR as an issue of distributive justice. Evans further explained that the cause of AMR is largely an issue of unequal distribution of resources: antibiotics are often overprescribed in wealthy countries and underprescribed in poor countries (Selgelid, 2007). This inequity represents a failure of market-based healthcare allocation. Equity concerns may also arise for diagnostics that are not affordable or universal in design. Evans argued that it is essential to encourage collaboration across nations and public health authorities so that diagnostics are ethically designed and implemented in a manner that can be delivered at any point-of-care globally.
Research Perspective
AMR is an ongoing pandemic and like all pandemics there are equity issues in terms of who gets resources and how those resources are distributed at the national- and community-levels, said Daniel Bausch (Director of Emerging Threats & Global Health Security, FIND, The Global Alliance for Diagnostics). People who are disenfranchised and on the margins of society are nearly always the ones who suffer the most, however, Bausch offered four potential ways to address some of these inequities.
First, there is a need for effective messaging, both to the public and political leaders. Bausch noted that progress is often driven by constituents demanding change. For example, patient advocacy led to progress in HIV research and development. Despite powerful stories like the ones shared at this workshop, this has largely not happened for AMR. There is a need to build a constituency that will come together, speak frankly with political leaders, and give AMR the attention it deserves.
Second, there is a need to move beyond the concept of binary diagnostics—tests that indicate whether or not a patient has a particular disease. Bausch said that when patients are told they do not have a disease—whether Ebola or COVID-19—they might be happy for a moment but then the focus turns to figuring out what they do have. There are new
diagnostic tools that will help with this issue, but these products must be available at a price point that makes them globally accessible.
Third, said Bausch, it is critical that systems for detecting and addressing AMR are integrated into routine health systems. Parallel systems are often established during outbreaks but become obsolete once the outbreak is resolved. Instead, surveillance should be built into existing systems and sustained in a way that offers value for patients, clinicians, and the public health enterprise.
Finally, there is a need to build equity into health systems to reduce vulnerabilities and inequities. For example, Bausch advocated that manufacturing be distributed around the world so that product pipelines are not dependent on just a few countries, and that health coverage and access to care should be universal.
Public Health Perspective
“Profound inequities are woven into the U.S. healthcare and public health systems,” said Melinda Pettigrew (Professor of Epidemiology and Interim Dean, Yale School of Public Health) and these inequities are inextricably linked to structural factors and social determinants of health and can manifest across the trajectory of care. Inequitable outcomes in health can be a result of inequitable access to care, including a lack of fair and just access to diagnostics. Data that would help elucidate and identify disparities in AMR are not routinely collected, but there are some cases of well-documented disparities. For example, rates of gonorrhea vary by race and ethnicity and disproportionately impact members of certain racial and ethnic groups (Lieberman et al., 2021). Pettigrew pointed to employment, access to care, housing, health literacy, and behavioral factors that can alter an individual’s exposure and risk for AMR infection. Some of these behaviors, said Pettigrew, are highly stigmatized, putting individuals at extra risk and influencing how they interact with the public health and healthcare system.
According to Pettigrew, in order to address health inequities, the first step is to identify groups that are at risk and to better understand the drivers and mechanisms behind these inequities. For example, race is a major driver of health inequities. Pettigrew stressed that it is important to identify the mechanisms, which could be socially constructed as well as biology- or genetic-based. For instance, if there are differences between men and women in terms of treatment efficacy, this could be due to a difference based on biology or how men and women interact with the healthcare system and what options they are offered. These types of questions are not always explicitly asked, and they are not always appropriately addressed.
While there are organizations working to improve health equity, Pettigrew emphasized a need for more work, particularly in the AMR space. There is a need to better quantify and characterize the intersection between AMR and inequities and carry out studies that enroll participants who are representative of the populations that bear the burden of disease, she said. In 1993, the NIH was given explicit authority to direct investigators of funded research to improve representation in trials with respect to gender, race, and ethnicity, but these policies do not apply to private industry. The FDA requires sponsors of new drug applications to present efficacy and safety data by gender, age, and racial subgroups, and in 2014, the FDA published an Action Plan for encouraging more inclusive trial participation.1 However, after decades of voluntary and aspirational initiatives, there remains a lack of diverse representation in clinical trials, said Pettigrew.
Draft legislation passed by the U.S. House of Representatives in June 2022 would require study sponsors to submit a diversity action plan, including a description of how they plan to increase access for certain demographic groups.2 However, these provisions would not fully resolve the barriers to diverse participation, including restrictive eligibility criteria, costs associated with participation, and limited outreach. Pettigrew said there is also a need for federal incentives, standards for diversity in research standards, and post-marketing surveillance to monitor effectiveness.
Access and Innovation Perspective
In 2019, 255,000 people in Sub-Saharan Africa died because of AMR and over half were children under 5, said Anthony So (Professor of the Practice; Director, Innovation + Design Enabling Access (IDEA) Initiative, Johns Hopkins Bloomberg School of Public Health) (Antimicrobial Resistance Collaborators, 2022). At the same time, the 2022 Mapping Antimicrobial Resistance and Antimicrobial Use Partnership (MAAP) project (MAAP, 2022) found that laboratory services were largely inaccessible:
- Only 1.3% of the 50,000 medical laboratories in the 14 countries studied conducted bacteriology testing;
- In 8 out of 14 countries studied, bacteriology labs were geographically accessible to less than 50% of the population;
- 80% of the 205 labs surveyed performed fewer than 1000 antimicrobial susceptibility tests per year.
___________________
1 See https://www.fda.gov/media/89307/download (accessed January 23, 2023).
2Consolidated Appropriations Act, 2023, Public Law 117-328, 117th Cong., 2d sess. (December 29, 2022).
For patients in resource-limited settings, the barriers to access extend across the entire value chain, said So. On the development end, there are challenges with the value proposition for investing in a point-of-care diagnostics suited for resource-limited settings. Once a product is on the market, it may be priced out of reach and healthcare workers may opt for antibiotics because there is no available diagnostic nearby. These barriers to equitable access at the technology, financial, and structural levels are deeply intertwined. Both push and pull incentives can be used to address barriers and increase access. So identified a need for strategic thought on how push incentives—paying for the inputs of R&D—and pull incentives—paying for the outputs of R&D—can work to build the innovation ecosystem and contribute to the access that is needed globally. Pull incentives, however, typically benefit groups that already have capital to run the race for a prize. To address this, the Longitude Prize on Antimicrobial Resistance, a prize competition for innovation in point-of-care diagnostics, offered discovery awards to provide seed funding for teams to get their ideas off the ground.3 There is a need for more effort on push incentives to encourage those who may have an alternative approach that is focused on low- and middle-income countries (LMIC).
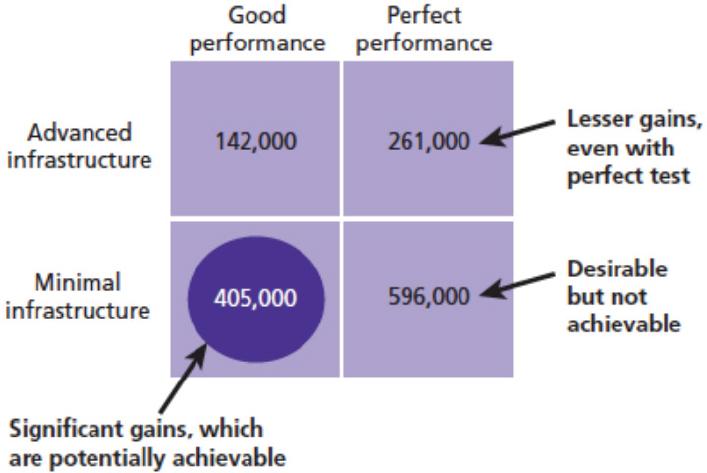
Bringing diagnostics into the healthcare systems of LMIC often requires tradeoffs between efficiency and accuracy. So shared a table (Figure 5-1) that demonstrates the tradeoffs in implementing a diagnostic for bacterial pneumonia. Implementing a test that has perfect performance but requires advanced infrastructure would result in fewer lives saved than a test with good performance that can be used in environments with minimal infrastructure. So emphasized that care must be taken to avoid the perception of double standards and to navigate regulatory approval for diagnostics that are designed for conditions of minimal infrastructure.
Even when diagnostic technology is effective and affordable, said So, there can still be unintended consequences from implementing it. For example, a clinical algorithm applied by healthcare workers to manage patients presenting with fever used a combination of respiratory rate and rapid diagnostic tests for malaria to determine if antibiotic treatment, not just antimalarial treatment, were needed (Mukanga et al., 2012). He explained that some providers did not prescribe antibiotics when the malaria test was positive, even if the respiratory rate was high enough to diagnose pneumonia, but providers would also prescribe antibiotics when the respiratory rate was normal and the malaria test was negative; So suggested this overuse may have stemmed from the healthcare provider’s interest in providing some kind of treatment to the pediatric patient. To help ensure equitable results from diagnostics, So suggested wraparound implementation
___________________
3 See https://longitudeprize.org/ (accessed January 23, 2023).
SOURCE: Presented by Anthony So, October 14, 2022; Burgess et al., 2007. See https://www.rand.org/pubs/research_briefs/RB9293.html (accessed March 1, 2023).
research to improve our understanding of what happens when technologies are deployed.
There are important lessons that can be learned from previous experiences in AMR diagnostics, said So. The GeneXpert System was an important advance that allowed for diagnoses of tuberculosis and rifampicin resistance. The technology platform is proprietary and pricey at around $17,000 per machine; test cartridges are just under $10 at the volume-discounted price. Public funders contributed over $250 million to its development, said So (Gotham et al., 2021). With this type of investment, should funders have insisted on an interoperable platform rather than a proprietary one? Should funders have insisted on more transparency on pricing? These types of questions, said So, can help better assess fair return on public financing in the future.
So shared the details of two innovations that were motivated by equity considerations, both of which were supported by Doctors without Borders (Médecins Sans Frontières or MSF). Antibiogo is an AI-based mobile app that is designed to help interpret AST, particularly where trained technicians may not be available.4 The Mini-Lab is a core laboratory system
___________________
4 See https://antibiogo.org/ (accessed January 23, 2023).
designed for rapid setup in field settings, from conflict-ridden areas to refugee camps.5 Both of these developments approach innovation with equity and accessibility built into design.
In conclusion, So shared three final thoughts. First, a systems perspective would enable strategic consideration of how to nurture dual markets in high-income countries and resource-limited markets that support equitable and sustainable access to diagnostics. For example, diagnostic platforms could serve to monitor and track emerging infections in health care settings as well as monitor prevalence of pathogens in wastewater. Second, there is a need to consider how to bundle the development, use, and reimbursement of diagnostics with drugs to lower costs and improve treatment. Finally, said So, diagnostics should be considered as part of a “best buy bargain” to address AMR. He said that “no one blinks” when billions are spent in public financing for new drugs, but there is a need to consider the opportunity costs of such funding if effectively deployed on complementary technologies like diagnostics. AMR-related complications in the Organization for Economic Co-operation and Development (OECD) and European Union (EU) countries are estimated to cost up to $3.5 billion each year; investing just $2 per capita per year in a comprehensive public health package, including diagnostics, to tackle AMR would avert 47,000 deaths per year in OECD countries and would pay for itself in under a year (OECD, 2018).
DISCUSSION
Gathering evidence and turning evidence into action
Evans described three barriers to gathering data necessary to understanding the extent of disproportionate impacts of AMR. First, the fragmentation of the health system makes it difficult to collect data in sufficiently high levels of granularity, and then share data among researchers, administrators, and other stakeholders. Second, there are competing and incompatible platforms for storing data, which exacerbates the difficulties of producing and sharing. Third, many labs simply do not have the capacity to collect these types of data. Pettigrew added that while collecting and managing data are challenges, it is important to first identify the types of data that are being collected and those that should be collected. Many of our definitions and labels are ill-defined and not always useful; for example, when considering the impact of race on AMR, is it the biological aspects or sociocultural determinants that matter? Collecting data using standard definitions will help identify who is at risk and where resources are needed but will not address the underlying mechanisms. Other data points that may be useful—such as insurance status or socioeconomic status—are very
___________________
5 See https://fondation.msf.fr/en/projects/mini-lab (accessed January 23, 2023).
challenging to collect, particularly within healthcare systems. In addition, there is a need to improve the diversity of those who participate in studies by addressing barriers to access and lack of trust. Despite these challenges, however, Pettigrew said “we have to start somewhere.” It would be beneficial to have macro-level data on race and ethnicity to assess disparities and identify groups that need special attention.
So said that as important as collecting data is, it does not always translate into increased action. For example, a study published in The Lancet said that 1.27 million people per year are dying of drug resistant bacterial infections, and the World Bank estimates that if AMR goes unchecked, 24 million people will be forced into extreme poverty by 2030 (Antimicrobial Resistance Collaborators, 2022; World Bank, 2017). Unfortunately, these numbers have not been enough to move policy makers to provide the necessary and commensurate resources. Addressing inequity cannot be done through data alone; sometimes it requires “putting a face to inequity.” Stories of people like Mallory Smith are so important to helping the public understand the scope of threat that AMR poses. Additionally, said So, there is a need to translate and communicate data in ways that are simple, straightforward, and lead to actionable results. AMR comprises a constellation of issues rather than one specific disease, meaning it can be particularly difficult to garner support and get results.
Bausch agreed that while better data are needed, it would be naïve to think data alone could spur action. In addition, equity arguments alone will not make the case; Bausch noted that there are data about inequities in multiple areas of health, but global resources are limited and economic constraints exist. What is needed, he said, are real-world political and economic arguments and a constituency of people who will demand change from decision makers. The “unfortunate reality” of our system is that politicians are looking for things that will benefit them and get them votes. Political cycles are short, so politicians need clear economic arguments about short-term benefits.
Shader Smith agreed with So that putting a face to the disease is critical for getting decision makers on board. Whether it is her daughter Mallory, patients with Valley Fever, or amputees, decision makers need to be able to see and understand the real-world impact on individual people. In addition, Shader Smith said, AMR discussions tend to happen in an echo chamber that is full of “alphabet soup” (i.e., acronyms). While these discussions are useful for sharing information, people on the outside of the echo chamber, or without specialized medical knowledge, are largely unaware of the problem or potential solutions.
Diversifying clinical trials
So encouraged stakeholders to consider diversity within a global context. He pointed out that depending on the setting, a diagnostic or
treatment may play out very differently. Based on experiences during the ongoing COVID-19 pandemic, clinical trials tend to rely on existing infrastructure, which may not overlap with places of diverse populations. Unless the clinical trials infrastructure extends into more diverse communities, said So, AMR researchers will continue to only “look at the light under the lamp post.”
Bausch said the entire system of research, development, and deployment of drugs and diagnostics is “haphazard” and “disjointed” with different stakeholders, barriers, and incentives at each step along the way. As a result, it is difficult for people to see the value in clinical trials, particularly for something like AMR. In contrast, his experience enrolling patients in a trial for an Ebola vaccine in the Democratic Republic of the Congo was relatively straightforward because there was an ongoing Ebola outbreak. There is a need to communicate the value of clinical trials and for people to see there is value for themselves and their communities in participating in research.
One marginalized group that is not often talked about, said Evans, is the community of people with disabilities. AMR-related issues appear to be more likely for people who have a disability or chronic disease (e.g., cystic fibrosis, amputee). These individuals are generally empowered to want to engage in the research process, he said, in part because medical care is a lifeline that allows them to live their lives as fully as possible. There is an urgent need for research that examines the interactions between AMR and different kinds of chronic conditions, comorbidities, and disabilities.
Pettigrew said that it can be difficult to know which populations should be included in a clinical trial. For example, if an infection is six times more prevalent in one population than another, should the enrollment reflect this ratio or should it reflect census data? Should trials focus the people who are most impacted by a condition or address more generalizable questions?
Incorporating diversity and equity from the beginning
A virtual participant asked panelists to comment on how considerations for diversity and equity can be intentionally incorporated from the very beginning of the development process for AMR diagnostics. Pettigrew responded that the first step is to look at the diversity of the field itself. “We all approach the world and research problems and challenges with our own lens based on our own experiences,” so if there are not enough diverse investigators running trials, there will not be diverse trial participants. In terms of barriers to trial participation, Pettigrew said that investigators need to consider issues such as access to the trial site, reimbursement for travel, and taking time off work. In addition, she agreed with Bausch that people need to see the value in participating in a trial. People need to understand the potential impact of AMR on themselves and their communities, and
they need to believe that their communities will benefit from the trial. For example, she said, trials where a product is tested in community A but will be used in community B are not useful.
Bausch agreed and said that investigators should be realistic and concrete about the benefits for clinical trial participants, rather than framing participation as a general benefit to humankind. The development process takes time, so investigators should be honest when engaging trial participants and communities. Evans referred to his earlier example of Indonesia withholding avian flu samples because they believed their nation would not benefit from the research (Fidler, 2008). This example drives home the importance of ensuring that research is designed in a way to benefit the populations participating in a trial.
So added that it can be challenging to enroll diverse populations if they will not be able to afford or benefit from a given technology. One approach for addressing this issue could be to design and target rapid diagnostics for use in resource-limited settings rather than trying to adapt technologies once they have been developed for a higher resource setting. Evans added that fundamental design principles in addition to price points, trial participation, and other issues, should include engagement from people who have a disability or chronic disease.
Building momentum and public engagement
As speakers have noted, said Kester, it can be challenging to build momentum and public engagement behind the issue of AMR because it is such a broad and variable condition. Visible diseases like polio or Ebola are more likely to get traction, whereas AMR is a hidden epidemic. Bausch and Evans underscored the value of consistent and focused messaging. Speaking from a marketing perspective, Shader Smith posited that if a popular and accessible platform, such as the Today Show, had an amputee, a cystic fibrosis patient, and a caregiver of a deceased patient share their stories, this could be a powerful way to educate and reach people. Shader Smith pointed out the need for a global marketing plan that includes people from outside of the insulated community of existing AMR experts and stakeholders. The discussions at this workshop are important, said Shader Smith, but it is essential that the messaging be spread into the general public.
This page intentionally left blank.














