
2
Intimate Partner Violence in Steady State Conditions
PREVALENCE OF INTIMATE PARTNER VIOLENCE
Intimate partner violence (IPV) is common among women in the United States. It affects women of all races and ethnicities, all levels of income, and all sexualities and gender identities, regardless of whether they live in rural, suburban, or urban areas. The Centers for Disease Control and Prevention (CDC) National Intimate Partner and Sexual Violence Survey (NISVS) is the most commonly used tool in the field of IPV research for estimating the prevalence of IPV in the United States. NISVS is a nationally representative random-digit-dial telephone survey. Data are collected from non-institutionalized English- and Spanish-speaking adult women who completed the survey. The most recent NISVS, conducted in 2016–2017 (N=15,152 women), estimated that 47.3 percent of women have experienced IPV in the form of contact sexual violence, physical violence, or stalking; and 49.4 percent have experienced psychological aggression by an intimate partner in their lifetimes (see Table 2-1) (Leemis, 2022). The past 12 months prevalence was 7.3 percent for experiencing any form of IPV, with 3.2 percent of women experiencing contact sexual violence, 4.5 percent experiencing any physical violence, 2.5 percent experiencing stalking, and 6.7 percent experiencing psychological abuse. A higher percentage of Black (12.3 percent), Hispanic (7.2 percent), and multiracial women (17.4 percent) women respondents reported a past-year experience of IPV, compared with only 6 percent of White women (Leemis, 2022). Prevalence rates of IPV are useful for identifying populations and characteristics associated with higher levels of IPV and related
TABLE 2-1 Lifetime Prevalence by Victimization Type for U.S. Women from the National Intimate Partner and Sexual Violence Survey: 2016–2017 Reporta
| Victimization Typeb | Lifetime Prevalence Percentagec |
|---|---|
| Total Nd | 15,152 |
| Any contact sexual violence, physical violence, and/or stalking | 47.3 |
| Psychological aggression | 49.4 |
| Physical violence | 42.0 |
| Contact sexual violence | 19.6 |
| Stalking | 13.5 |
a Definitions used in the survey: Physical violence includes a range of behaviors from slapping, pushing, or shoving to severe acts that include being hit with a fist, kicked, hurt by pulling hair, slammed against something, choked, beaten, burned on purpose, or use of a weapon. Contact sexual violence includes rape, being made to penetrate someone else, sexual coercion, and unwanted sexual contact. Stalking refers to a pattern of harassing or threatening tactics used by people engaging in IPV that is both unwanted and causes fear or safety concerns in the woman experiencing abuse. Psychological aggression includes expressive aggression (e.g., name-calling, insulting, or humiliating an intimate partner) and coercive control (e.g., monitoring, controlling, or threatening an intimate partner).
b The summation of the percentage of respondents for each victimization type is different from the total percentages of respondents because respondents may have experienced multiple victimization types.
c All percentages are weighted to the U.S. non-institutionalized English- or Spanish-speaking adult population.
d N=number of respondents.
SOURCE: Leemis et al. (2022).
health conditions, guiding appropriate screening and interventions, and designing effective prevention efforts.
Lifetime prevalence rates of IPV are also high for all women, with the highest rates in American Indian or Alaska Native (AI/AN; 57.7 percent), non-Hispanic Black (53.6 percent), and multiracial groups (63.8 percent) (see Table 2-2) (Leemis, 2022). In addition to population-based survey data, such as those reported in NISVS, police-reported IPV rates are two to three times higher among Black and Hispanic women than among White women (Lipsky et al., 2009).
Prevalence estimates from NISVS survey results are the most referenced, but they are not the only source of information about IPV prevalence. Clinic and other site-based surveys have examined the prevalence of different forms of IPV in various demographic and geographic groups. However, the research methodology differs across studies, which limits comparisons. Many surveys, including different years of the NISVS, differ in terms of the
| Lifetime Prevalence | Total | Hispanic | Non-Hispanic, Black | Non-Hispanic, White | Asian or Pacific Islander | American Indian or Alaska Native | Multiracial |
|---|---|---|---|---|---|---|---|
| Na | 15,152 | 2,197 | 1,864 | 9,879 | 849 | 91 | 257 |
| Any contact sexual violence, physical violence, and/or stalking percentageb | 47.3 | 42.1 | 53.6 | 48.4 | 27.2 | 57.7 | 63.8 |
a N=number of respondents
b All percentages are weighted to the U.S. non-institutionalized English- or Spanish-speaking adult population.
SOURCE: Leemis et al. (2022).
terminology used related to IPV, demographic categories, and approaches to data collection. This makes it difficult to compare data and findings across studies. CDC released the first version of its Intimate Partner Violence Surveillance: Uniform Definitions and Recommended Data Elements in 1999 with the goal of improving consistency in IPV surveillance research (Breiding et al., 2015a; Saltzman et al., 1999). CDC released its second version of Intimate Partner Violence Surveillance: Uniform Definitions and Recommended Data Elements in 2015 with updated and added terminology, again with the intention of improving data gathering for IPV surveillance. This tool provides recommended uniform definitions, guidance about data elements for record-based and survey surveillance, and recommended data elements (RDEs). The uniform definitions can be used both in the clinic for documentation or data collection and in research, including survey data collection. The RDEs included in the guidelines address four types of violence: physical, sexual, stalking, and psychological. Each RDE has a corresponding definition or description, type of surveillance for which it is recommended, and coding instructions. The majority of the RDEs focus on collecting data about the most recent incidence of IPV as well as the very first experience of IPV but could be used to gather further information (Breiding et al., 2015a). While the CDC document is not all-encompassing, broader application of its guidance would greatly improve the usefulness of data collected in clinical and research settings, including surveys.
POPULATION-SPECIFIC CONSIDERATIONS
As noted earlier in this chapter, some populations are disproportionately affected by IPV. The committee found that many of those populations are under-represented in the IPV research literature, including those discussed in this section. The populations and considerations included in this section are those for which the committee identified adequate evidence to support an informed discussion. Additionally, the committee prioritized considerations that were most relevant to the study’s statement of task.
American Indian and Alaska Native Women
There are currently 574 federally recognized American Indian and Alaska Native (AI/AN) tribes in the United States (BIA, 2022). The committee recognized that these tribes are distinct entities with unique languages, traditions, and structures and sought to avoid treating them as a monolith. This report refers to specific tribes when information is available. Unfortunately, tribal affiliation is rarely reported in studies relevant to IPV.
Data Collection
Much of the epidemiologic data and analysis about AI/AN populations, including IPV-related data, are subject to important methodological limitations. These include racial misclassification, in which individuals are incorrectly classified as a different race or ethnicity instead of AI/AN (Petrosky et al., 2021; Yellow Horse and Huyser, 2021). The demographic information section of forms in many states and in surveys often does not allow for the selection of multiple races or does not include a category for AI/AN (Yellow Horse and Huyser, 2021). This limits the response option to other and aggregates that data with the data of the rest of the respondents that are placed in the other category (Huyser et al., 2021). Also, in statistical analysis, data from a very small group are frequently combined with data from another group that, while smaller than other groups, is much larger than the very small group; such as the case with aggregating data from Asian American and Pacific Islander populations (Korngiebel et al., 2015). In this case, data from the smaller group, Native Hawaiians and other Pacific Island populations, can be obscured by data from the much larger group, Asian Americans (Korngiebel et al., 2015). These limitations result in inaccurate findings.
Violent crimes against AI/AN women are under-reported, which adds additional opacity to an understanding of the prevalence of violence inflicted by current and former intimate partners (BIA, n.d.). This is highlighted by the epidemic of missing and murdered Indigenous women and girls. An examination of reports of missing AI/AN women and girls found that in 2016 there were 5,712 reports of missing AI/AN women and girls in the U.S. Department of Justice federal missing persons database (BIA, n.d.). However, only 116 of those cases were logged in the National Missing and Unidentified Persons System, which serves as the national information clearinghouse for missing, unidentified, and unclaimed person cases (BIA, n.d.).
Prevalence of Intimate Partner Violence Among American Indian/Alaska Native Women
AI/AN women are a population that experiences exceptionally high rates of IPV. The 2016–2017 analysis of the NISVS found that 57.7 percent of non-Hispanic AI/AN women in the survey had experienced IPV in the form of physical violence, contact sexual violence, or stalking in their lifetime (Leemis et al., 2022). Among 230 undergraduate students self-identifying as AI/AN attending 20 medium- and large-sized universities across the United States, 28.9 percent reported having experienced any violence from a current or past intimate partner in the previous 6 months (Edwards et al., 2023). A study funded by the National Institute of Justice found that 66.4 percent of AI/AN women (N=2,473, n=1,642) had experienced psychological
aggression from an intimate partner during their lifetime (Rosay, 2016). This study also found that AI/AN women experiencing IPV were 1.5 times more likely than non-Hispanic White women to be physically injured due to IPV and 2.3 times more likely to need medical care. AI/AN women were also 2.5 times more likely to lack access to needed IPV services (Rosay, 2016). Among AI/AN women, IPV is associated with poorer physical and mental health (Fedina et al., 2022; Stockman et al., 2015). Economic inequalities among these women are a salient predictor of IPV health outcomes, which demographic and geographic contexts may compound (Fedina et al., 2022). A CDC National Violent Death Reporting System analysis of AI/AN homicides in 34 states and the District of Columbia from 2003 to 2018 found that the suspect in murders of AI/AN women was most likely to be a current or former intimate partner in 38.4 percent of reported cases (Petrosky et al., 2021).
Sociological Factors
In the literature, the substantially higher rates of IPV in AI/AN populations have been attributed to historical violence, including forced relocation, traumas inflicted through residential schools, retraction of tribal sovereignty and associated economic rights leading to economic deprivation, and jurisdictional uncertainty, which contributes to a lack of legal consequences for people engaging in IPV (Fedina et al., 2022; Wahab and Olson, 2004). Studies have noted that exposure to intergenerational violence contributes to the normalization of IPV (Jock et al., 2022). AI/AN women have reported that contextual factors contributing to IPV include controlling relationships, losing a sense of priorities, using children as manipulation tools, socioeconomic stress, family pressures, and restricting relationships (McKinley and Liddell, 2022). Additional challenges include living in remote, rural areas that limit access to support or the ability to leave a dangerous relationship, or living in areas that isolate AI/AN women from their extended family, community ties, and culture (Gauthier et al., 2021; Raponi et al., 2023). Language barriers, fear of losing custody of children, lack of culturally congruent services, inconvenient location of services, and economic stress and its consequences also limit help seeking for AI/AN women experiencing IPV (Fedina et al., 2022; Wahab and Olson, 2004).
Pregnant and Postpartum Women
Prevalence of Intimate Partner Violence in the Perinatal Period
Studies comparing IPV prevalence before and during pregnancy have had mixed findings, with some reporting a decline during pregnancy
and others reporting an increase, particularly under conditions of an unwanted pregnancy or paternal uncertainty (Cizmeli, 2018; Saltzman et al., 2003). A study using Pregnancy Risk Assessment Monitoring System (PRAMS) data from 16 states from 1996 to 1998 found a prevalence rate of 5.3 percent (N=64,994, n=3,444) for physical abuse during pregnancy (Saltzman et al., 2003). Studies using clinic-based data for IPV in the perinatal period usually consider more than one type of IPV and have found higher prevalence rates (Hahn et al., 2018). Perinatal IPV rates were 16.4 percent (N=104) for physical IPV and 73 percent (N=104) for psychological IPV in a review of studies using clinic-based data (Flanagan et al., 2015; Hahn et al., 2018). A large global systematic review found that for reported IPV prevalence during pregnancy in North America, physical violence occurred at a rate of 9 percent (11 studies, N=11,204), psychological abuse occurred at a rate of 28.6 percent (eight studies, N=9,680), and sexual IPV occurred at a rate of 8.9 percent (five studies, N=942) (Román-Gálvez et al., 2021). An analysis of PRAMS data from six states in 2016–2018 found that women younger than age 25 experienced both psychological and physical IPV at a higher rate than those in an older age range during pregnancy (D’Angelo et al., 2022). The analysis found that AI/AN, mixed race, and Black women experienced emotional violence at a higher rate than White women throughout the perinatal period (D’Angelo et al., 2022). This analysis also found that AI/AN and Black women experienced physical violence during pregnancy at higher rates than White women (D’Angelo et al., 2022). Few U.S.-based studies reported rates of sexual IPV during the perinatal period. However, a study of 104 southern Appalachian women found that 20.2 percent experienced sexual abuse at the hands of a current or former intimate partner during the perinatal period (Bailey and Daugherty, 2007).
An analysis of PRAMS data for 43,811 persons who had a live birth between 2018 and 2020 highlighted the role of sociodemographic factors and disability status of those experiencing IPV during the perinatal period (Alhusen et al., 2023). The analysis found that the odds of experiencing IPV during the perinatal period were higher for those who had less than a college education, had a household income less than 200 percent of the federal poverty level, or identified as White (Alhusen et al., 2023). The study also found that the odds of experiencing perinatal IPV were twice as high for women with at least one disability as compared to those without a disability (Alhusen et al., 2023).
Intimate Partner Violence Screening in the Perinatal Period
While the nature of perinatal care, which involves multiple visits with a clinician during that period, provides greater opportunity for IPV detection,
screening rates are generally inconsistent and suboptimal (IPV screening is discussed further in Chapter 5) (ACOG, 2012). Data related to physical IPV from the 2016 to 2019 PRAMS (N=158,338) indicated that 65.7 percent of respondents reported not being screened for IPV before pregnancy, 29.7 percent reported not being screened during pregnancy, and 48 percent reported not being screened for IPV during the postpartum period (Kozhimannil et al., 2023). Of the 3.5 percent of women in the dataset reporting physical IPV in the perinatal period, 58.7 percent reported not being screened for IPV before pregnancy, 26.9 percent reported not being screened during pregnancy, and 48.3 percent reported not being screened after pregnancy (Kozhimannil et al., 2023). The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics Bright Futures Guidelines recommend that clinicians discuss IPV during perinatal appointments (Hagan et al., 2017).
Perinatal Intimate Partner Homicide
The most severe outcome of abuse from a current or former intimate partner during the perinatal period is death. In an analysis of data from 2003 to 2007 from the National Violent Death Reporting System (NVDRS), 42.4 percent (N=139, n=59) of pregnancy-related homicides were found to have been carried out by an intimate partner (Campbell et al., 2021). A systematic review of research investigating intimate partner homicide during pregnancy or postpartum also concluded that current or former intimate partners were most frequently the perpetrator of the murder (Noursi et al., 2020). Additionally, in a case-control study, severe physical IPV during pregnancy (described in the study as women being “beaten”) was a risk factor for intimate partner homicide, while less severe IPV was not (Campbell, 2003). Another analysis of NVDRS data found that suicide, although less frequent than homicide, was also a common cause of maternal mortality highly associated with IPV (Palladino et al., 2011).
Adolescent Girls
Teen dating violence (also referred to as adolescent dating abuse or dating abuse) includes emotional, physical, sexual, or economic abuse by an intimate or sexual partner, which can occur in person, via social media, or texting (McCauley et al., 2014). Examples of adolescent relationship abuse are similar to those for IPV in adults and include monitoring a partner’s cell phone, telling partners what they can wear, limiting social interactions, refusing to use condoms, preventing contraceptive use, coercing sexual behaviors (including insisting on receiving nude or seminude photos from a partner), coercing a partner to use substances, and other controlling behaviors (Scott et al., 2023).
Reports on teen dating violence in the adolescent girl population demonstrate that violence and abuse are not uncommon in adolescent relationships. Among teens (ages 12–18) who have dated, 69 percent (N=1,804) report ever having experienced physical, psychological, or sexual relationship abuse (Taylor and Mumford, 2016). Many adults report that they first experienced IPV before age 25 (Breiding et al., 2014; Leemis et al., 2022). Several studies, including CDC’s Youth Risk Behavior Surveillance System, document that female respondents reported significantly higher prevalence of either physical or sexual dating violence than male respondents (20.9 vs. 10.4 percent; N=9,900) (Vagi et al., 2015).
Youth who experience marginalization and social disadvantage have had a higher reported prevalence of IPV in the literature. An evaluation of differences in the prevalence of relationship abuse among youth suggests higher prevalence among Black/African American and Hispanic youth, including experiences of reproductive coercion (Miller et al., 2014).
Black Women
Non-Hispanic Black women experience some of the highest rates of IPV when compared to other racial and ethnic groups. Most recent data from the NISVS reported non-Hispanic Black women have a lifetime prevalence of IPV of 53.6 percent (Leemis, 2022). An analysis of 2003–2017 data from the National Violent Death Reporting System found that pregnancy-related intimate partner homicide (IPH) rates were three times higher for Black woman than White or Hispanic women (Kivisto et al., 2022). Despite this, published research specifically addressing IPV and Black women is limited. Studies investigating rates of reproductive coercion have reported that Black women are subjected to this form of abuse at higher rates than White, Hispanic, and Asian women (Alexander et al., 2021). Studies investigating severe IPV and IPH in Black women have identified some common themes. These researchers have noted that Black women may delay contacting law enforcement due to concerns related to historically prejudicial treatment during interactions with law enforcement or fear of unjust treatment of their partner during or after arrest (Harper, 2022; Vil et al., 2022). Researchers have also highlighted that while studies have suggested that Black women may underutilize formal IPV services, many also lack access to these services in their community (Vil et al., 2022)
LBTQ Populations
The prevalence data for IPV experienced by the lesbian, bisexual, transgender, and queer (LBTQ) population varies, but is generally higher than that for the general population. A systematic review of 14 studies that
investigated the prevalence and correlates of IPV in same-sex relationships of self-identified lesbians found that IPV prevalence ranged from 9.6 to 51.5 percent (Badenes-Ribera, 2016). A majority of the included studies found that reported lifetime physical IPV for these women ranged from 40 to 50 percent and psychological IPV ranged from 18 percent to 84 percent (Badenes-Ribera, 2016). A systematic review of 85 articles found that compared with cisgender individuals, transgender individuals were 1.7 times more likely to experience any IPV, 2.2 times more likely to experience physical IPV, and 2.5 times more likely to experience sexual IPV (Peitzmeier et al., 2020). A systematic review including nine studies looking specifically at bisexuality and IPV found that in three of those studies, women who identified as bisexual had an increased risk of experiencing IPV (Corey et al., 2023).
IPV in sexual minority women is associated with poorer physical health and mental health outcomes, including stress, depression, anxiety, alcohol abuse, and emotional regulation difficulties (Porsch et al., 2022). IPV also increases overall health care costs for LBTQ people experiencing abuse (Porsch et al., 2022). There are several minority stressors that affect those in the LBTQ community, including stigma, facing prejudice and discrimination, internalized homophobia, and concealment of sexual identity, which can contribute to poor mental health outcomes (Porsch et al., 2022). Providing trauma-informed care for LBTQ IPV survivors can increase their empowerment to begin working toward safety and recovery (Scheer and Poteat, 2021).
Rural Populations
Women who experience IPV and reside in rural areas face unique challenges related to geographic isolation. Research investigating geographic differences in the prevalence of IPV has had mixed findings. However, comparison of findings is limited by variations in the types of data collection methods, inconsistent distinctions between definitions of different regions, and different types of regional mapping.
A systematic review of 32 studies comparing frequency of IPV by locale found that the prevalence of IPV was similar regardless of urban or rural location (Edwards, 2015). The authors noted that the five studies included that used National Crime Victimization Survey data reported prevalence rates that were similar or greater for urban women compared with rural and suburban women (Edwards, 2015). A study of more specific geographic regions (urban core, suburban, exurban, small town, and dispersed rural)—found that those residing in small towns, defined as “the urbanized portions of nonmetropolitan counties,” were at higher risk of IPV (DuBois, 2022).
Women experiencing IPV in rural and remote communities are more likely to have worse mental and physical health outcomes, including intimate partner homicide (AbiNader, 2020; Edwards, 2015). They are likely to stay longer with a partner engaging in IPV, more likely to experience torture, and more likely to be shot by a partner engaging in IPV than women living in urban areas (Hart and Klein, 2013). Women living in rural areas are at a disadvantage regarding accessing IPV-related resources. A cross-sectional clinic-based survey of 1,478 women in Iowa found that the average distance to the nearest IPV resource for rural women was substantially greater than the distance for urban women (29.4 to 29.6 miles versus 6.5 miles) (Peek-Asa et al., 2011). Researchers have suggested that women experiencing IPV who live in rural areas may have worse physical and mental health outcomes due to inadequate availability, accessibility, and quality of IPV resources in their area (Edwards, 2015; Peek-Asa et al., 2011; Reckdenwald et al., 2017). Faith-based organizations are often the most likely place for women experiencing IPV in rural communities to find services (Hart and Klein, 2013).
ADDITIONAL CONSIDERATIONS
Disability
A secondary analysis of data from the 2010 NISVS found that women with a disability (N= 9,086, n=2,162) were substantially more likely than women without a disability (N= 9,086, n=6,924) to report each type of IPV measured, including rape (1.7 vs. 0.4 percent), sexual violence other than rape (4.5 vs. 1.8 percent), physical violence (7.1 vs. 3.3 percent), stalking (6.5 vs. 2.1 percent), psychological aggression (21.0 vs. 12.2 percent), and control of reproductive or sexual health (2.4 vs. 1.4 percent) (Breiding and Armour, 2015b). There is a limited body of research about IPV and women with disabilities. An analysis of PRAMS data from 2018 to 2020 found that women with disabilities experienced much higher prevalence of abuse from a current or former intimate partner (N=3,024) than those with no disabilities (N=70,813) both before (9.5 versus 2.4 percent) and during pregnancy (5.8 versus 1.7 percent) (Alhusen et al., 2023). An analysis of data from the 2001–2005 National Epidemiologic Survey of Alcohol and Related Conditions found that both physical and mental disabilities were significantly associated with experiencing IPV (Hahn et al., 2014).
Women living with disabilities experience higher levels of poverty and social isolation, and may be more likely to stay with a partner engaging in IPV if that person is providing their physical or financial care (Breiding and Armour, 2015). There are added barriers for women with disabilities related to disclosing and seeking care for IPV because the partner engaging in IPV may be providing transportation or communication assistance,
which hinders one’s ability to reach out for help when experiencing IPV (Breiding and Armour, 2015).
Immigration Status
Disparities related to immigration status can adversely affect the physical and mental health outcomes of IPV, particularly for racial and ethnic minority women (Stockman et al., 2015). Hispanic and Asian immigrant women experiencing IPV face significant social, cultural, structural, and political barriers to communication with IPV care providers which affect their help-seeking behaviors related to IPV (Stockman et al., 2015). Acculturative stress, the stress of adapting to a new context in the United States, has been demonstrated to be among the strongest predictors of experiencing IPV among Hispanic women who are immigrants (Cao et al., 2023; González-Guarda et al., 2012).
Immigrant populations, especially those arriving through irregular or extra-legal immigration routes, are particularly at risk for experiencing IPV (Salgado and Gurm, 2020). These women face unique barriers to reporting IPV related to the perceived threat that law enforcement involvement may lead to deportation and concerns about public charge status that may affect permanent legal status determination (Ballard et al., 2019).
Housing and Food Insecurity
IPV contributes to homelessness and housing insecurity for women and their children (Adams et al., 2021; Fraga Rizo et al., 2022). Women who reported recent housing or food insecurity were significantly more likely to experience all forms of IPV than women without housing or food insecurity (Breiding et al., 2017). Additionally, lack of access to safe and affordable housing is a barrier for women experiencing IPV to leave a partner engaging in abuse (Decker et al., 2022; Pavao et al., 2007). An analysis of data from the 2003 California Women’s Health Survey (N=3,619), found that women who had experienced IPV in the previous year were almost four times more likely to have reported housing instability than women who had not experienced IPV (adjusted OR=3.98, 95% CI: 2.94–5.39) (Pavao et al., 2007). Higher rates of housing, food, and health care insecurity have been observed among women who identified as Black/African American, Hispanic, AI/AN, and other racial and ethnic minority groups (Fedina et al., 2022).
Reducing housing insecurity may help prevent IPV revictimization. A quasi-experimental evaluation of on-site transitional housing and community-based rehousing was conducted to meet the safety and stability needs of individuals made homeless because of IPV. Both IPV revictimization
and housing instability had significantly improved by the 6-month follow-up point (p<0.001) (Decker et al., 2022).
Substance Use
Women using illicit drugs may be at greater risk of experiencing IPV (Testa et al., 2003). Among 414 women enrolled in methadone maintenance treatment programs in New York City, 88 percent reported having experienced physical and sexual IPV during their lifetime (El-Bassel et al., 2004). Nearly 50 percent reported having experienced physical or sexual IPV in the previous 6 months, and slightly more than 20 percent indicated that the physical or sexual IPV experienced in the past 6 months was severe (El-Bassel et al., 2004). Lifetime prevalence estimates of IPV among women with opioid use disorders range from 36 (N=114, n=41) to 94 percent (N=406, n=381) (Stone and Rothman, 2019). Women who used heroin were twice as likely to experience IPV and 2.7 times more likely to report IPV-related injury than those who did not report using heroin (El-Bassel et al., 2005).
The evidence related to the relationship between alcohol use in women and experiencing IPV is mixed and shows no clear causal relationship. Some studies have shown an association between alcohol use and experiencing IPV (Temple and Freeman, 2011; Testa et al., 2003; White and Chen, 2002). However, after reviewing the literature, Capaldi et al. (2012) suggested that the relationship may not be strong because substance use tends to co-occur with other risk factors for experiencing IPV. Moreover, the temporal direction of this association has not been consistently demonstrated (Dardis et al., 2021; Devries et al., 2014; Keller et al., 2009). Some studies have found that there is no significant association between alcohol use in women and experiencing IPV (Sabina et al., 2017; Thompson and Kingree, 2006).
HIV Infection
Women living with HIV infection are more likely than the general population to experience IPV, and women in IPV relationships are more likely to acquire HIV and other sexually transmitted infections (Campbell et al., 2008; Marshall et al., 2018). State-level IPV prevalence is positively associated with higher rates of state-level HIV diagnosis among women (Willie et al., 2018). Researchers have suggested that increased rates of HIV infection among women who experience IPV may be due to these women being sexually assaulted by a male partner with an HIV infection, directly affecting their HIV susceptibility (Dunkle and Decker, 2013; Li et al., 2014; Maman et al., 2000; Stockman et al., 2013). Additionally, women in relationships with controlling partners may not be able to
negotiate safer sex practices. Finally, the chronic stress and trauma related to experiencing IPV may negatively affect the immune system (Campbell et al., 2008). While the literature has not shown a direct mechanical association, this may make these women more susceptible to acquiring sexually transmitted infections (Campbell et al., 2008). In an examination of data from the National Epidemiologic Survey on Alcohol and Related Conditions, among 13,928 women in a relationship in the last year, 11.8 percent of cases of HIV infection among women were attributable to past-year IPV (Sareen et al., 2009).
Involvement in Sex Work
Women involved in sex work may face increased vulnerability to IPV and barriers to reporting IPV and accessing health care. In a convenience sample of 346 HIV-negative, drug-involved women in relationships recruited in New York City, women reporting sex trading were three times as likely to report recent severe physical or sexual IPV than women who did not report sex trading, after accounting for sociodemographic factors (Jiwatram-Negrón and El-Bassel, 2019).
A couples-based study of 214 women engaged in sex work explored the context in which IPV occurred (Ulibarri et al., 2019). In this study, couples reported that conflict arose over the financial need for women to engage in sex work, men’s inability to provide for female partners, men feeling uncomfortable that their female partners had sex with other men as part of work, and relationship power dynamics (women being considered head of the household due to higher income than a partner). They also reported conflict while under the influence of drugs or while going through drug withdrawal (Ulibarri et al., 2019).
RISK FACTORS FOR PEOPLE ENGAGING IN INTIMATE PARTNER VIOLENCE
While this report focuses on women experiencing IPV, research on factors associated with IPV risk has concentrated on characteristics associated with people engaging in IPV. Understanding risk and protective factors for people engaging in IPV is fundamental to IPV prevention. In addition, recognizing these factors can guide responses to public health emergencies by focusing on risk factors that are likely to worsen during and in the wake of an emergency.
Multiple factors are associated with an increased likelihood for engaging in IPV and have been classified by CDC as occurring at the individual, relationship, community, and society levels (see Figure 2-1) (Capaldi et al., 2012; CDC, 2021). These risk and protective factors may be contributing
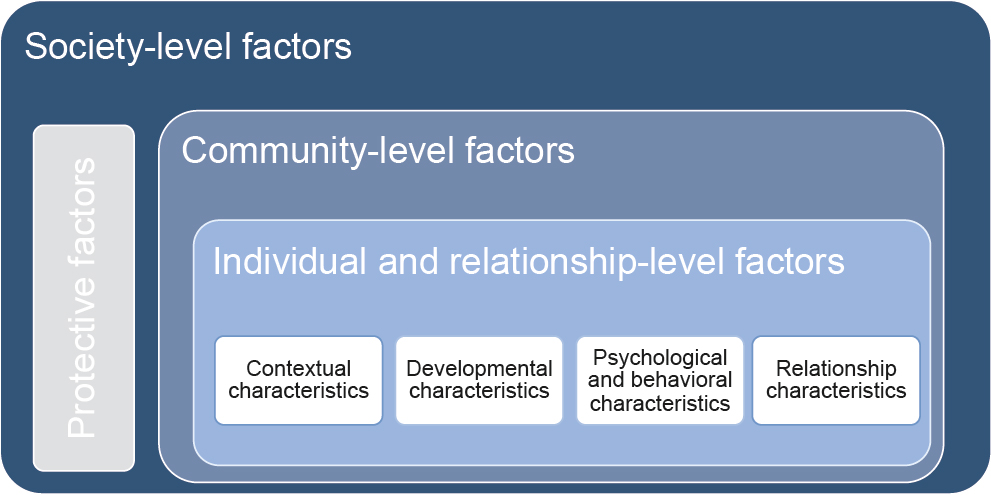
NOTE: Multiple factors are associated with IPV. These include individual, relationship, community, and societal factors. Factors that increase the likelihood of IPV may be contributing factors and not direct causes.
factors to—not direct causes of—IPV, and they commonly include combinations of factors operating at different levels (e.g., coexisting individual- and community-level factors).
Individual- and relationship-level risk factors identified in observational studies relevant to the general U.S. population are listed in Table 2-3. Individual-level factors include contextual characteristics, such as low education or income, young age, and economic stress (e.g., unemployment). Developmental characteristics include a history of demonstrating previous physically abusive behavior, experiencing or witnessing physical or emotional abuse or violence in childhood, experiencing poor parenting, and having parents with less than a high school education (Capaldi et al., 2012; CDC, 2021). Psychological and behavioral characteristics include low self-esteem, aggressive or delinquent behavior, depression, suicide attempts, antisocial or borderline personality, and heavy alcohol and drug use. Also included in this category are beliefs in strict gender roles and hostility toward women (Capaldi et al., 2012).
Community-level risk factors include high poverty rates, unemployment, violence, and crime (Table 2-4). Communities with easy access to drugs and alcohol, limited educational and economic opportunities, low community involvement among residents, and a lack of sanctions against IPV are also at higher risk. Society-level risk factors include cultural norms that support traditional gender roles, gender inequality, and aggression toward others. Income inequality and weak policies or laws related to
TABLE 2-3 Individual- and Relationship-Level Risk Factors for Engaging in IPV
| Contextual characteristics |
Low education or income |
|
Young age |
|
|
Economic stress, such as unemployment |
|
| Developmental characteristics |
History of being physically abusive |
|
History of physical or emotional abuse in childhood |
|
|
History of experiencing physical discipline as a child |
|
|
History of experiencing poor parenting as a child |
|
|
Parents with less than a high school education |
|
|
Witnessing violence between parents as a child |
|
| Psychological and behavioral characteristics |
Low self-esteem |
|
Aggressive or delinquent behavior |
|
|
Depression and suicide attempts |
|
|
Anger and hostility |
|
|
Heavy alcohol and drug use |
|
|
Lack of nonviolent social problem-solving skills |
|
|
Antisocial personality traits and conduct problems |
|
|
Poor behavioral control and impulsiveness |
|
|
Traits associated with borderline personality disorder |
|
|
Emotional dependence and insecurity |
|
|
Belief in strict gender roles, such as male dominance and aggression in relationships |
|
|
Having few friends and being isolated from other people |
|
|
Hostility toward women |
|
|
Attitudes accepting or justifying violence and aggression |
|
| Relationship characteristics |
Relationship conflicts, including jealousy, possessiveness, tension, divorce, or separation |
|
Dominance and control of the relationship by one partner over the other |
|
|
Families experiencing economic stress |
|
|
Unhealthy family relationships and interactions |
|
|
Association with antisocial and aggressive peers |
SOURCES: Modified from Capaldi et al. (2012); CDC (2021).
health, educational, economic, and social needs also contribute to risk for people engaging in IPV.
The absence of risk factors is associated with a lower likelihood of people engaging in IPV. Protective factors specifically identified in studies include strong social support networks; neighborhood collective efficacy; coordination of resources and services among community agencies; and access to housing, medical care, and economic and financial help (CDC, 2021).
TABLE 2-4 Community- and Society-Level Risk Factors and Protective Factors for Engaging in IPV
| Community factors |
High rates of poverty and limited educational and economic opportunities |
|
High unemployment rates |
|
|
High rates of violence and crime |
|
|
Neighbors do not know or look out for each other, and residents have low community involvement |
|
|
Easy access to drugs and alcohol |
|
|
Weak community sanctions against IPV |
|
| Societal factors |
Traditional gender norms and gender inequality |
|
Cultural norms that support aggression toward others |
|
|
Societal income inequality |
|
|
Weak health, educational, economic, and social policies or laws |
|
| Protective factors |
Strong social support networks and stable, positive relationships with others |
|
Neighborhood collective efficacy, meaning residents feel connected to each other and are involved in the community |
|
|
Coordination of resources and services among community agencies |
|
|
Communities with access to safe, stable housing |
|
|
Communities with access to medical care and mental health services |
|
|
Communities with access to economic and financial help |
SOURCES: Modified from Capaldi et al. (2012); CDC (2021).
FACTORS INFLUENCING DISCLOSURE
Barriers to Disclosure
There are several reasons commonly cited by women experiencing IPV to not disclose that they are experiencing IPV to a clinician, including shame and fear of the consequences of reporting, such as retaliation (Heron et al., 2021; Othman et al., 2014). Also, they may not believe a clinician has time or interest in addressing IPV (Narula et al., 2012; Spangaro et al., 2011). People experiencing IPV also cited a lack of awareness of the range of services and supports available to them as a reason they did not disclose (Ravi et al., 2022). Additionally, cultural and religious norms and values can influence a woman’s disclosure decision (Hulley et al., 2023).
Parents experiencing IPV may be concerned about the effects of disclosure on their children. Children are present or otherwise members of the household in 59–76 percent of cases of IPV reported to the police (Campbell et al., 2020; Ernst et al., 2006; McDonald et al., 2006). Child maltreatment co-occurs with as many as 30–40 percent of IPV cases (Appel and Holden, 1998; Hamby et al., 2010). Children’s experience of witnessing IPV can have long-term adverse effects on their physical and mental health
(Artz et al. 2014; Carpenter and Stacks, 2009; Evans et al., 2008; Felitti, 2009; Kitzmann et al., 2003; Tiyyagura et al., 2018; Vu et al., 2016). While disclosure is a potential way for mothers and their children to separate from these dangerous conditions, the perceived risk of retaliation can be a substantial barrier (Buttell and Ferreira, 2020). Qualitative studies have found that parents experiencing IPV also fear retaliation against their children if they disclose (Cerulli et al., 2014; Meyer, 2010). Another commonly cited concern for parents regarding disclosure of IPV is the possibility that their clinician will file a report of child abuse. This may lead to actions by child protective services, such as removing the child from the home. Most states require clinicians and government employees to report suspected child abuse (Children’s Bureau, 2019). Additionally, most states and territories require clinicians to report several types of crime-related injuries, and some states have laws requiring reporting domestic violence in general (Lizdas et al., 2019). Fear of losing custody of their children is a commonly reported barrier for women experiencing IPV who are considering disclosure (DeVoe and Smith, 2003; Heron and Eisma, 2021; Lippy et al., 2019; Varcoe and Irwin, 2004).
Child-related barriers are compounded by additional issues for some populations. Immigration documentation status may also affect the decision to disclose IPV, as some women may not disclose because of a fear of deportation (Kelly, 2009). Women with disabilities are also particularly deterred from disclosure due to biases against them in custody decisions (Ballan et al., 2014; Ortoleva and Lewis, 2012).
While some barriers to IPV disclosure are shared by most women experiencing IPV, some populations face additional challenges that increase their hesitancy to disclose that they are experiencing IPV. A systematic review of 47 articles found that Black women often encounter unique barriers to disclosing IPV that are rooted in harmful racist stereotypes (Hulley et al., 2023; Waller et al., 2022). This reinforces their concern that they will not be believed if they disclose (Hulley et al., 2023; Waller et al., 2022). Other studies have noted that pressure stemming from cultural beliefs about protecting family honor in Latin American and South Asian populations can discourage women in these populations from disclosing IPV (Hulley et al., 2023). In one qualitative study of 83 participants in AI/AN communities, some women who experienced IPV explained that the intergenerational experience of violence can contribute to the normalization of abusive behavior within the family, including intimate partners (Jock et al., 2022). That normalization can make AI/AN people experiencing IPV less likely to disclose because they perceive IPV as normal (Jock et al., 2022). Additionally, some respondents indicated that such intergenerational experiences of violence were related to historical oppression of their communities (Jock et al., 2022).
Stigma and systematic inequities have acted as barriers to disclose for those in the LBTQ population (Calton et al., 2016). Due to existing discrimination toward sexual minorities, there may be reluctance to seek help out of fear of further discrimination. There also may be hesitation to disclose incidents of IPV if the individual has been selective about who they share their sexual orientation with, therefore the fear of being outed may hinder one’s likelihood of seeking help (Calton et al., 2016).
CHAPTER SUMMARY
Lifetime IPV prevalence is high for all women in the United States. Frequent inconsistencies in terminology and data collection in IPV epidemiological research limit comparison and applicability of the data. Prevalence rates for women reporting they have experienced IPV are higher among some populations. Understanding the prevalence of IPV, the populations most at risk, factors associated with people engaging in IPV, and barriers to disclosure can enable planning that ensures that the health care needs of women experiencing IPV are addressed, whether during steady state conditions or public health emergencies. The next chapter provides an overview of public health emergencies and discusses their impact on IPV prevalence and access to IPV related health care.
REFERENCES
AbiNader, M. A. 2020. Correlates of intimate partner homicide in the rural United States: Findings from a national sample of rural counties, 2009–2016. Homicide Studies 24(4):353-376.
ACOG (American College of Obstetricians and Gynecologists). 2012. ACOG committee opinion no. 518: Intimate partner violence. Obstet Gynecol 119(2 Pt 1):412-417.
Adams, E. N., H. M. Clark, M. M. Galano, S. F. Stein, A. Grogan-Kaylor, and S. GrahamBermann. 2021. Predictors of housing instability in women who have experienced intimate partner violence. J Interpers Violence 36(7-8):3459-3481.
Alexander, K. A., T. C. Willie, R. McDonald-Mosley, J. C. Campbell, E. Miller, and M. R. Decker. 2021. Associations between reproductive coercion, partner violence, and mental health symptoms among young black women in Baltimore, Maryland. J Interpers Violence 36(17-18):NP9839-NP9863.
Alhusen, J. L., G. Lyons, K. Laughon, and R. B. Hughes. 2023. Intimate partner violence during the perinatal period by disability status: Findings from a united states population-based analysis. J Adv Nurs 79(4):1493-1502.
Appel, A. E., and G. W. Holden. 1998. The co-occurrence of spouse and physical child abuse: A review and appraisal. Journal of Family Psychology 12(4):578-599.
Artz, S., M. A. Jackson, K. R. Rossiter, A. Nijdam-Jones, I. Géczy, and S. Porteous. 2014. A comprehensive review of the literature on the impact of exposure to intimate partner violence for children and youth. International Journal of Child, Youth and Family Studies 5(4):493-587.
Badenes-Ribera, L., A. Bonilla-Campos, D. Frias-Navarro, G. Pons-Salvador, and I. B. H. Monterde. 2016. Intimate partner violence in self-identified lesbians: A systematic review of its prevalence and correlates. Trauma Violence Abuse 17(3):284-297.
Bailey, B. A., and R. A. Daugherty. 2007. Intimate partner violence during pregnancy: Incidence and associated health behaviors in a rural population. Matern Child Health J 11(5):495-503.
Ballan, M. S., M. B. Freyer, C. N. Marti, J. Perkel, K. A. Webb, and M. Romanelli. 2014. Looking beyond prevalence: A demographic profile of survivors of intimate partner violence with disabilities. J Interpers Violence 29(17):3167-3179.
Ballard, J., M. Witham, and M. Mittal. 2019. Chapter 6: Intimate partner violence among immigrants and refugees. In Immigrant and refugee families. 2nd Ed ed.
BIA (Bureau of Indian Affairs). 2022. Tribal leaders directory. https://www.bia.gov/service/tribal-leaders-directory (accessed 2023).
BIA. n.d. Missing and murdered indigenous people crisis. https://www.bia.gov/service/mmu/missing-and-murdered-indigenous-people-crisis (accessed 2023).
Breiding, M. J., and B. S. Armour. 2015. The association between disability and intimate partner violence in the United States. Ann Epidemiol 25(6):455-457.
Breiding, M. J., S. G. Smith, K. C. Basile, M. L. Walters, J. Chen, and M. T. Merrick. 2014. Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization—National Intimate Partner and Sexual Violence Survey, United States, 2011. MMWR Surveill Summ 63(8):1-18.
Breiding, M. J., K. C. Basile, S. G. Smith, M. C. Black, and R. R. Mahendra. 2015. Intimate partner violence surveillance: Uniform definitions and recommended data elements. Version 2.0. Edited by Centers for Disease Control and Prevention. Atlanta, GA: National Center for Injury Prevention and Control.
Breiding, M. J., K. C. Basile, J. Klevens, and S. G. Smith. 2017. Economic insecurity and intimate partner and sexual violence victimization. Am J Prev Med 53(4):457-464.
Buttell, F., and R. J. Ferreira. 2020. The hidden disaster of COVID-19: Intimate partner violence. Psychol Trauma 12(S1):S197-S198.
Calton, J. M., L. B. Cattaneo, and K. T. Gebhard. 2016. Barriers to help seeking for lesbian, gay, bisexual, transgender, and queer survivors of intimate partner violence. Trauma Violence Abuse 17(5):585-600.
Campbell, A. M., R. A. Hicks, S. L. Thompson, and S. E. Wiehe. 2020. Characteristics of intimate partner violence incidents and the environments in which they occur: Victim reports to responding law enforcement officers. Journal of Interpersonal Violence 35(13-14):2583-2606.
Campbell, J., S. Matoff-Stepp, M. L. Velez, H. H. Cox, and K. Laughon. 2021. Pregnancy-associated deaths from homicide, suicide, and drug overdose: Review of research and the intersection with intimate partner violence. J Womens Health (Larchmt) 30(2):236-244.
Campbell, J. C., M. L. Baty, R. M. Ghandour, J. K. Stockman, L. Francisco, and J. Wagman. 2008. The intersection of intimate partner violence against women and HIV/AIDS: A review. Int J Inj Contr Saf Promot 15(4):221-231.
Campbell, J. C., D. Webster, J. Koziol-McLain, C. Block, D. Campbell, M. A. Curry, F. Gary, N. Glass, J. McFarlane, C. Sachs, P. Sharps, Y. Ulrich, S. A. Wilt, J. Manganello, X. Xu, J. Schollenberger, V. Frye, and K. Laughon. 2003. Risk factors for femicide in abusive relationships: Results from a multisite case control study. Am J Public Health 93(7):1089-1097.
Cao, J., S. G. Silva, M. Quizhpilema Rodriguez, Q. Li, A. M. Stafford, R. C. Cervantes, and R. M. Gonzalez-Guarda. 2023. Acculturation, acculturative stress, adverse childhood experiences, and intimate partner violence among Latinx immigrants in the U.S. J Interpers Violence 38(3-4):3711-3736.
Capaldi, D. M., N. B. Knoble, J. W. Shortt, and H. K. Kim. 2012. A systematic review of risk factors for intimate partner violence. Partner Abuse 3(2):231-280.
Carpenter, G. L., and A. M. Stacks. 2009. Developmental effects of exposure to intimate partner violence in early childhood: A review of the literature. Children and Youth Services Review 31(8):831-839.
CDC (Centers for Disease Control and Prevention). 2021. Risk and protective factors for perpetration. https://www.cdc.gov/violenceprevention/intimatepartnerviolence/riskprotectivefactors.html (accessed August 18, 2023).
Cerulli, C., C. L. Kothari, M. Dichter, S. Marcus, J. Wiley, and K. V. Rhodes. 2014. Victim participation in intimate partner violence prosecution: Implications for safety. Violence Against Women 20(5):539-560.
Children’s Bureau. 2019. Mandatory reporters of child abuse and neglect. https://www.childwelfare.gov/pubPDFs/manda.pdf (accessed 2023).
Cizmeli, C., M. Lobel, K. K. Harland, and A. Saftlas. 2018. Stability and change in types of intimate partner violence across pre-pregnancy, pregnancy, and the postpartum period. Womens Reprod Health (Phila) 5(3):153-169.
Corey, J., M. Duggan, and A. Travers. 2023. Risk and protective factors for intimate partner violence against bisexual victims: A systematic scoping review. Trauma Violence Abuse 24(4):2130-2142.
D’Angelo, D. V., J. M. Bombard, R. D. Lee, K. Kortsmit, M. Kapaya, and A. Fasula. 2022. Prevalence of experiencing physical, emotional, and sexual violence by a current intimate partner during pregnancy: Population-based estimates from the pregnancy risk assessment monitoring system. J Fam Violence 38(1):117-126.
Dardis, C. M., S. E. Ullman, L. M. Rodriguez, E. A. Waterman, E. R. Dworkin, and K. M. Edwards. 2021. Bidirectional associations between alcohol use and intimate partner violence and sexual assault victimization among college women. Addictive Behaviors 116:106833.
Decker, M. R., K. T. Grace, C. N. Holliday, K. G. Bevilacqua, A. Kaur, and J. Miller. 2022. Safe and stable housing for intimate partner violence survivors, Maryland, 2019-2020. Am J Public Health 112(6):865-870.
DeVoe, E. R., and E. L. Smith. 2003. Don’t take my kids: Barriers to service delivery for battered mothers and their young children. Journal of Emotional Abuse 3(3-4):277-294.
Devries, K. M., J. C. Child, L. J. Bacchus, J. Mak, G. Falder, K. Graham, C. Watts, and L. Heise. 2014. Intimate partner violence victimization and alcohol consumption in women: A systematic review and meta-analysis. Addiction 109(3):379-391.
DuBois, K. O. 2022. Rural isolation, small towns, and the risk of intimate partner violence. J Interpers Violence 37(5-6):NP2565-NP2587.
Dunkle, K. L., and M. R. Decker. 2013. Gender-based violence and HIV: Reviewing the evidence for links and causal pathways in the general population and high-risk groups. Am J Reprod Immunol 69(Suppl 1):20-26.
Edwards, K. M. 2015. Intimate partner violence and the rural-urban-suburban divide: Myth or reality? A critical review of the literature. Trauma Violence Abuse 16(3):359-373.
Edwards, K. M., S. Lim, M. Huff, R. Herrington, L. Leader Charge, and H. Littleton. 2023. Rates and correlates of intimate partner violence among indigenous college students: A multi-campus study. Journal of Interpersonal Violence 38(11-12):7852-7866.
El-Bassel, N., L. Gilbert, V. Frye, E. Wu, H. Go, J. Hill, and B. L. Richman. 2004. Physical and sexual intimate partner violence among women in methadone maintenance treatment. Psychol Addict Behav Jun;18(2):180-183.
El-Bassel, N., L. Gilbert, E. Wu, H. Go, and J. Hill. 2005. Relationship between drug abuse and intimate partner violence: A longitudinal study among women receiving methadone. American Journal of Public Health 95(3):465-470.
Ernst, A. A., S. J. Weiss, and S. Enright-Smith. 2006. Child witnesses and victims in homes with adult intimate partner violence. Acad Emerg Med 13(6):696-699.
Evans, S. E., C. Davies, and D. DiLillo. 2008. Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggression and Violent Behavior 13(2):131-140.
Fedina, L., Y. Shyrokonis, B. Backes, K. Schultz, L. Ashwell, S. Hafner, and A. Rosay. 2022. Intimate partner violence, economic insecurity, and health outcomes among American Indian and Alaska Native men and women: Findings from a national sample. Violence Against Women 29(11):2060-2079. https://doi.org/10.1177/10778012221127725.
Felitti, V. J. 2009. Adverse childhood experiences and adult health. Acad Pediatr 9(3):131-132.
Flanagan, J. C., K. C. Gordon, T. M. Moore, and G. L. Stuart. 2015. Women’s stress, depression, and relationship adjustment profiles as they relate to intimate partner violence and mental health during pregnancy and postpartum. Psychol Violence 5(1):66-73.
Fraga Rizo, C., L. B. Klein, B. Chesworth, R. J. Macy, and R. Dooley. 2022. Intimate partner violence survivors’ housing needs and preferences: A brief report. J Interpers Violence 37(1-2):958-972.
Gauthier, G. R., S. C. Francisco, B. Khan, and K. Dombrowski. 2021. Social integration and domestic violence support in an indigenous community: Women’s recommendations of formal versus informal sources of support. J Interpers Violence 36(7-8):3117-3141.
Hagan, J. F., J. S. Shaw, and P. M. Duncan. 2017. Bright futures: Guidelines for health supervision of infants, children, and adolescents [pocket guide]. 4th ed. American Academy of Pediatrics.
Hahn, C. K., A. K. Gilmore, R. O. Aguayo, and A. A. Rheingold. 2018. Perinatal intimate partner violence. Obstet Gynecol Clin North Am 45(3):535-547.
Hahn, J. W., M. C. McCormick, J. G. Silverman, E. B. Robinson, and K. C. Koenen. 2014. Examining the impact of disability status on intimate partner violence victimization in a population sample. Journal of Interpersonal Violence 29(17):3063-3085.
Hamby, S., D. Finkelhor, H. Turner, and R. Ormrod. 2010. The overlap of witnessing partner violence with child maltreatment and other victimizations in a nationally representative survey of youth. Child Abuse Negl 34(10):734-741.
Harper, S. B. 2022. “I’m just like, you know what, it’s now or never”: Exploring how women of color experiencing severe abuse and homicide risk journey toward formal help-seeking. Journal of Interpersonal Violence 37(15-16):NP13729-NP13765.
Hart, B. J., and A. F. Klein. 2013. Practical implications of current intimate partner violence research for victim advocates and service providers. Washington, DC: U.S. Department of Justice Office of Justice Programs.
Heron, R. L., and M. C. Eisma. 2021. Barriers and facilitators of disclosing domestic violence to the healthcare service: A systematic review of qualitative research. Health Soc Care Community 29(3):612-630.
Hulley, J., L. Bailey, G. Kirkman, G. R. Gibbs, T. Gomersall, A. Latif, and A. Jones. 2023. Intimate partner violence and barriers to help-seeking among Black, Asian, minority ethnic and immigrant women: A qualitative metasynthesis of global research. Trauma, Violence, & Abuse 24(2):1001-1015.
Huyser, K. R., A. J. Y. Horse, A. A. Kuhlemeier, and M. R. Huyser. 2021. COVID-19 pandemic and indigenous representation in public health data. Am J Public Health 111(S3):S208-S214.
Jiwatram-Negrón, T., and N. El-Bassel. 2019. Overlapping intimate partner violence and sex trading among high-risk women: Implications for practice. Women & Health 59(6):672-686.
Jock, B. W. I., G. Dana-Sacco, J. Arscott, M. E. Bagwell-Gray, E. Loerzel, T. Brockie, G. Packard, V. M. O’Keefe, C. E. McKinley, and J. Campbell. 2022. “We’ve already endured the trauma, who is going to either end that cycle or continue to feed it?”: The influence of family and legal systems on Native American women’s intimate partner violence experiences. Journal of Interpersonal Violence 37(21-22):NP20602-NP20629.
Keller, P. S., M. El-Sheikh, M. Keiley, and P. J. Liao. 2009. Longitudinal relations between marital aggression and alcohol problems. Psychol Addict Behav 23(1):2-13.
Kelly, U. A. 2009. “I’m a mother first”: The influence of mothering in the decision-making processes of battered immigrant Latino women. Research in Nursing & Health 32(3):286-297.
Kitzmann, K. M., N. K. Gaylord, A. R. Holt, and E. D. Kenny. 2003. Child witnesses to domestic violence: A meta-analytic review. J Consult Clin Psychol 71(2):339-352.
Kivisto, A. J., S. Mills, and L. S. Elwood. 2022. Racial disparities in pregnancy-associated intimate partner homicide. J Interpers Violence 37(13-14):NP10938-NP10961.
Korngiebel, D. M., M. Taualii, R. Forquera, R. Harris, and D. Buchwald. 2015. Addressing the challenges of research with small populations. Am J Public Health 105(9):1744-1747.
Kozhimannil, K. B., V. A. Lewis, J. D. Interrante, P. L. Chastain, and L. Admon. 2023. Screening for and experiences of intimate partner violence in the United States before, during, and after pregnancy, 2016–2019. Am J Public Health 113(3):297-305.
Leemis, R. W., N. Friar, S. Khatiwada, M. S. Chen, M.-j. Kresnow, S. G. Smith, S. Caslin, and K. C. Basile. 2022. The National Intimate Partner and Sexual Violence Survey: 2016/2017 report on intimate partner violence. https://www.cdc.gov/violenceprevention/pdf/nisvs/nisvsreportonipv_2022.pdf
Li, Y., C. M. Marshall, H. C. Rees, A. Nunez, E. E. Ezeanolue, and J. E. Ehiri. 2014. Intimate partner violence and HIV infection among women: A systematic review and meta-analysis. J Int AIDS Soc 17(1):18845.
Lippy, C., S. N. Jumarali, N. A. Nnawulezi, E. P. Williams, and C. Burk. 2019. The impact of mandatory reporting laws on survivors of intimate partner violence: Intersectionality, help-seeking and the need for change. Journal of Family Violence 35(3):255-267.
Lipsky, S., R. Caetano, and P. Roy-Byrne. 2009. Racial and ethnic disparities in police-reported intimate partner violence and risk of hospitalization among women. Women’s Health Issues 19(2):109-118.
Lizdas, K., A. O’Flaherty, N. Durborow, A. Marjavi, and A. Ali. 2019. Compendium of state and US territory statutes and policies on domestic violence and health care. Edited by Futures Without Violence. 4th ed. https://ipvhealth.org/wp-content/uploads/2019/09/Compendium-4th-Edition-2019-Final-small-file.pdf.
Maman, S., J. Campbell, M. D. Sweat, and A. C. Gielen. 2000. The intersections of HIV and violence: Directions for future research and interventions. Soc Sci Med 50(4):459-478.
Marshall, K. J., D. N. Fowler, M. L. Walters, and A. B. Doreson. 2018. Interventions that address intimate partner violence and HIV among women: A systematic review. AIDS and Behavior 22:3244-3263.
McCauley, H. L., R. N. Dick, D. J. Tancredi, S. Goldstein, S. Blackburn, J. G. Silverman, E. Monasterio, L. James, and E. Miller. 2014. Differences by sexual minority status in relationship abuse and sexual and reproductive health among adolescent females. J Adolesc Health 55(5):652-658.
McDonald, R., E. N. Jouriles, S. Ramisetty-Mikler, R. Caetano, and C. E. Green. 2006. Estimating the number of American children living in partner-violent families. J Fam Psychol 20(1):137-142.
McKinley, C. E., and J. L. Liddell. 2022. “Why I stayed in that relationship”: Barriers to indigenous women’s ability to leave violent relationships. Violence Against Women 28(14):3352-3374.
Meyer, S. 2010. Seeking help to protect the children?: The influence of children on women’s decisions to seek help when experiencing intimate partner violence. Journal of Family Violence 25(8):713-725.
Miller, E., H. L. McCauley, D. J. Tancredi, M. R. Decker, H. Anderson, and J. G. Silverman. 2014. Recent reproductive coercion and unintended pregnancy among female family planning clients. Contraception 89(2):122-128.
Narula, A., G. Agarwal, and L. McCarthy. 2012. Intimate partner violence: Patients’ experiences and perceptions in family practice. Fam Pract 29(5):593-600.
Noursi, S., J. A. Clayton, J. Campbell, and P. Sharps. 2020. The intersection of maternal morbidity and mortality and intimate partner violence in the United States. Current Women’s Health Reviews 16(4):298-312.
Ortoleva, S., and H. Lewis. 2012. Forgotten sisters—a report on violence against women with disabilities: An overview of its nature, scope, causes and consequences. Northeastern University School of Law Research Paper 104-2012.
Othman, S., C. Goddard, and L. Piterman. 2014. Victims’ barriers to discussing domestic violence in clinical consultations: A qualitative enquiry. J Interpers Violence 29(8):1497-1513.
Palladino, C. L., V. Singh, J. Campbell, H. Flynn, and K. J. Gold. 2011. Homicide and suicide during the perinatal period: Findings from the national violent death reporting system. Obstet Gynecol 118(5):1056-1063.
Pavao, J., J. Alvarez, N. Baumrind, M. Induni, and R. Kimerling. 2007. Intimate partner violence and housing instability. Am J Prev Med 32(2):143-146.
Peek-Asa, C., A. Wallis, K. Harland, K. Beyer, P. Dickey, and A. Saftlas. 2011. Rural disparity in domestic violence prevalence and access to resources. J Womens Health (Larchmt) 20(11):1743-1749.
Peitzmeier, S. M., M. Malik, S. K. Kattari, E. Marrow, R. Stephenson, M. Agenor, and S. L. Reisner. 2020. Intimate partner violence in transgender populations: Systematic review and meta-analysis of prevalence and correlates. Am J Public Health 110(9):e1-e14.
Petrosky, E., L. M. Mercer Kollar, M. C. Kearns, S. G. Smith, C. J. Betz, K. A. Fowler, and D. E. Satter. 2021. Homicides of American Indians/Alaska Natives—national violent death reporting system, United States, 2003-2018. MMWR Surveill Summ 70(8):1-19.
Porsch, L. M., M. Xu, C. B. Veldhuis, L. A. Bochicchio, S. S. Zollweg, and T. L. Hughes. 2022. Intimate partner violence among sexual minority women: A scoping review. Trauma Violence Abuse 24(5):3014-3036.
Raponi, M. B. G., P. C. Condeles, N. F. Azevedo, and M. T. Ruiz. 2023. Prevalence and risk factors for intimate partner violence and indigenous women: A scoping review. Int J Nurs Pract e13159.
Ravi, K. E., S. R. Robinson, and R. V. Schrag. 2022. Facilitators of formal help-seeking for adult survivors of IPV in the United States: A systematic review. Trauma Violence Abuse 23(5):1420-1436.
Reckdenwald, A., A. Yohros, and A. Szalewski. 2017. Health care professionals, rurality, and intimate femicide. Homicide Studies 22(2):161-187.
Roman-Galven, S., S. Martin-Pelaez, B. M. Fernandez-Felix, J. Zamora, K. S. Khan, and A. Bueno-Cavanillas. 2021. Worldwide prevalence of intimate partner violence in pregnancy. A systematic review and meta-analysis. Frontiers in Public Health 9:73859.
Rosay, A. B. 2016. Violence against American Indian and Alaska Native women and men. NIJ Journal (277).
Sabina, C., J. L. Schally, and L. Marciniec. 2017. Problematic alcohol and drug use and the risk of partner violence victimization among male and female college students. Journal of Family Violence 32(3):305-316.
Salgado, G., and B. Gurm. 2020. Chapter 21: Relationship violence (IPV) in immigrant and refugee communities, Making sense of a global pandemic: Relationship violence & working together towards a violence free society. Kwantlen Polytechnic University.
Saltzman, L. E., J. L. Fanslow, P. M. McMahon, and G. A. Shelley. 1999. Intimate partner violence surveillance: Uniform definitions and recommended data elements. Version 1.0. Atlanta, GA: Centers for Disease Control and Prevention. National Center for Injury Prevention and Control.
Saltzman, L. E., C. H. Johnson, B. C. Gilbert, and M. M. Goodwin. 2003. Physical abuse around the time of pregnancy: An examination of prevalence and risk factors in 16 states. Matern Child Health J 7(1):31-43.
Sareen, J., J. Pagura, and B. Grant. 2009. Is intimate partner violence associated with HIV infection among women in the United States? General Hospital Psychiatry 31(3):274-278.
Scheer, J. R., and V. P. Poteat. 2021. Trauma-informed care and health among LGBTQ intimate partner violence survivors. Journal of Interpersonal Violence 36(13-14):6670-6692.
Scott, S., D. R. Lavage, G. Acharya, L. Risser, S. G. Bocinski, E. A. Walker, K. A. Randell, M. I. Ragavan, and E. Miller. 2023. Experiences of exploitation and associations with economic abuse in adolescent dating relationships: Findings from a US cross-sectional survey. Journal of Trauma & Dissociation 1-17.
Spangaro, J. M., A. B. Zwi, and R. G. Poulos. 2011. “Persist. Persist.”: A qualitative study of women’s decisions to disclose and their perceptions of the impact of routine screening for intimate partner violence. Psychology of Violence 1(2):150.
Stockman, J. K., M. B. Lucea, and J. C. Campbell. 2013. Forced sexual initiation, sexual intimate partner violence and HIV risk in women: A global review of the literature. AIDS Behav 17(3):832-847.
Stockman, J. K., H. Hayashi, and J. C. Campbell. 2015. Intimate partner violence and its health impact on disproportionately affected populations, including minorities and impoverished groups. J Womens Health (Larchmt) 24(1):62-79.
Stone, R., and E. F. Rothman. 2019. Opioid use and intimate partner violence: A systematic review. Current Epidemiology Reports 6(2):215-230.
Taylor, B. G., and E. A. Mumford. 2016. A national descriptive portrait of adolescent relationship abuse: Results from the national survey on teen relationships and intimate violence. J Interpers Violence 31(6):963-988.
Temple, J. R., and D. H. Freeman, Jr. 2011. Dating violence and substance use among ethnically diverse adolescents. J Interpers Violence 26(4):701-718.
Testa, M., J. A. Livingston, and K. E. Leonard. 2003. Women’s substance use and experiences of intimate partner violence: A longitudinal investigation among a community sample. Addict Behav 28(9):1649-1664.
Thompson, M. P., and J. B. Kingree. 2006. The roles of victim and perpetrator alcohol use in intimate partner violence outcomes. Journal of Interpersonal Violence 21(2):163-177.
Tiyyagura, G., C. Christian, R. Berger, D. Lindberg, and S. I. Ex. 2018. Occult abusive injuries in children brought for care after intimate partner violence: An exploratory study. Child Abuse Negl 79:136-143.
Ulibarri, M. D., M. Salazar, J. L. Syvertsen, A. R. Bazzi, M. G. Rangel, H. S. Orozco, and S. A. Strathdee. 2019. Intimate partner violence among female sex workers and their noncommercial male partners in Mexico: A mixed-methods study. Violence Against Women 25(5):549-571.
Vagi, K. J., E. O’Malley Olsen, K. C. Basile, and A. M. Vivolo-Kantor. 2015. Teen dating violence (physical and sexual) among US high school students: Findings from the 2013 National Youth Risk Behavior Survey. JAMA Pediatr 169(5):474-482.
Varcoe, C., and L. G. Irwin. 2004. “If I killed you, I’d get the kids”: Women’s survival and protection work with child custody and access in the context of woman abuse. Qualitative Sociology 27:77-99.
Vil, N. M. S., M. Sperlich, J. Fitzpatrick, E. Bascug, and J. Elliott. 2022. “I thought it was normal:” perspectives of Black nursing students from high-risk IPV communities on causes and solutions to IPV in the Black community. Journal of Interpersonal Violence 37(13-14):NP12260-NP12283.
Vu, N. L., E. N. Jouriles, R. McDonald, and D. Rosenfield. 2016. Children’s exposure to intimate partner violence: A meta-analysis of longitudinal associations with child adjustment problems. Clin Psychol Rev 46:25-33.
Wahab, S., and L. Olson. 2004. Intimate partner violence and sexual assault in Native American communities. Trauma Violence Abuse 5(4):353-366.
Waller, B. Y., J. Harris, and C. R. Quinn. 2022. Caught in the crossroad: An intersectional examination of African American women intimate partner violence survivors’ help seeking. Trauma Violence Abuse 23(4):1235-1248.
White, H. R., and P. H. Chen. 2002. Problem drinking and intimate partner violence. J Stud Alcohol 63(2):205-214.
Willie, T. C., J. K. Stockman, R. Perler, and T. S. Kershaw. 2018. Associations between intimate partner violence, violence-related policies, and HIV diagnosis rate among women in the United States. Ann Epidemiol 28(12):881-885.
Yellow Horse, A. J., and K. R. Huyser. 2022. Indigenous data sovereignty and COVID-19 data issues for American Indian and Alaska Native tribes and populations. J Popul Res (Canberra) 39(4):527-531.


























