
3
Intimate Partner Violence and Public Health Emergencies
PUBLIC HEALTH EMERGENCIES
The committee defines a public health emergency (PHE) for the purposes of this report as a situation with health consequences whose scale, timing, or unpredictability threatens to overwhelm the routine capabilities of the affected geographic area. Examples include infectious disease outbreaks; extreme weather events such as hurricanes, heat waves, or wildfires; earthquakes; and technological disasters such as mass power outages, nuclear incidents, or oil spills.
Terms and Approaches
Five Phases
The five phases or steps of emergency management are prevention, mitigation, preparedness, response, and recovery (DHS, 2015). Prevention refers to activities undertaken to avoid these incidents. Mitigation involves reducing emergencies’ or disasters’ impacts and consequences (DHS, 2015). Preparedness refers to actions designed to develop resilience and the capability to respond to and recover from the effects of an incident. It involves planning, training, and educational activities (DHS, 2015). Mitigation and preparedness need to occur in advance of an incident. The response phase refers to activities undertaken during and immediately after an incident to address its impact directly (DHS, 2015). The recovery phase involves restoration efforts during the longer-term aftermath of an event (DHS,
2015). These five phases are used throughout the field of emergency management to guide efforts to address PHEs of all magnitudes.
All-Hazards Approach
An all-hazards approach, as defined by the Centers for Medicare & Medicaid (CMS), “is an integrated approach to emergency preparedness planning that focuses on capacities and capabilities that are critical” in order to prepare for, respond to, and recover from the full spectrum of emergencies or disasters, whether human-made or natural (CMS, 2017). The International Federation of the Red Cross and Red Crescent formally defines disasters as “serious disruptions to the functioning of a community that exceeds its capacity to cope using its own resources” (IFRC, 2023, para. 1). The shock of a disaster disrupts the health, well-being, and functioning of communities. This includes damage to infrastructure—such as the loss of electrical power or public transportation, supply shortages, and damage to buildings and homes. Notably, the functionality of health care systems may be affected, contributing to a lack of access to health care for the local community (Bayntun, 2012; Bell et al., 2020).
All-hazards planning is based on two core premises:
- Potential hazards, threats, and vulnerabilities have been assessed in advance and plans are in place to address these; and
- A uniform approach to response and recovery will be employed regardless of the hazard that occurs.
In other words, an all-hazards approach seeks to be ready for any disaster. The process includes the development of capacities and capabilities essential for effective disaster preparedness for all types of emergencies and disasters (CMS, 2016; FEMA, 2021). However, an all-hazards approach also includes planning specific to the locale of the service provider. It accounts for the different types of hazards that could potentially occur in a given community (FEMA, 2021).
Actors and Roles in Public Health Emergency Response
Initially, all disaster response is local in nature and consists of local emergency services supplemented by state and volunteer entities. All states and territories, as well as some tribal and local governments, have adopted statutes to guide and empower government leaders to respond to PHEs. Provisions relevant to PHEs may be found in statutes developed in preparation for natural disasters, disease outbreaks, civil unrest, and general emergencies. In addition, federal laws provide guidance and authority to
federal officials concerning how to support PHE preparedness, response, and recovery.
The response to PHEs may involve different actors and roles depending on the nature of the event and the jurisdiction’s organizational structure. In the public sector, federal and state, local, tribal, and territorial (SLTT) governments may be involved. At each of these levels, the response is typically led by the jurisdiction’s emergency management official. The emergency manager works under the direction of the chief executive—the president and one or more governors as well as local executives, such as mayors or county executives. In addition, state, territorial, city, and county health officers and agencies as well as officials and agencies responsible for other sectors—such as transportation, housing, agriculture, and others—may also be involved.
At the federal level, key entities involved in PHE response include the cabinet-level departments, especially the Department of Homeland Security (DHS) and the Department of Health and Human Services (HHS), as well as the plethora of sub-entities formed within each department. For example, under DHS, the Federal Emergency Management Agency (FEMA) is responsible for coordinating the response to emergencies and disasters that overwhelm SLTT governments. Under the HHS umbrella, a variety of entities play key roles. The Administration for Strategic Preparedness and Response (ASPR) is responsible for “medical and public health preparedness for, response to, and recovery from disasters and other public health emergencies” (ASPR, n.d.). CMS administers the two largest federal health care programs. The Centers for Disease Control and Prevention (CDC) provides technical and financial support to state and territorial governments for monitoring, controlling, and preventing disease outbreaks and injuries. The Food and Drug Administration (FDA) ensures that drugs, biologics, and medical devices (including some forms of personal protective equipment) are safe and effective. In turn, each of these sub-departmental agencies is populated by additional layers of centers, programs, and offices devoted to particular functions or areas of concern.
In 2008, the World Health Organization recommended that jurisdictions adopt a “whole of society” approach to pandemics (and later, other PHEs), which involves ensuring that partners from across all sectors and functions of society are engaged across all five phases of PHE management (WHO, 2009). This has been echoed through the FEMA publication A Whole Community Approach to Emergency Management: Principles, Themes, and Pathways for Action (FEMA, 2011).
U.S. Laws and Regulations Concerning Emergency Response
Several federal laws are principally relevant to PHE response. The Public Health Service Act1 (PHSA) and its amending legislation2 authorizes various federal emergency declarations, including PHE declarations, Emergency Use Authorization (EUA) declarations, and Pandemic Readiness and Emergency Preparedness Act3 (PREP) declarations. The Social Security Act4 (SSA) includes requirements applicable to Medicare and Medicaid, among other health care regulations. The Robert T. Stafford Disaster Relief and Emergency Assistance Act5 (Stafford Act) and National Emergencies Act6 (NEA) authorize emergency and major disaster declarations.
The most relevant federal declarations to ensure access to essential health care services related to IPV during a PHE are made under Section 319 of the PHSA and the various declarations available under the Stafford Act. A Section 3197 PHE declaration allows HHS and its multiple sub-agencies, including CMS, to suspend or waive specific federal requirements, including requirements rising out of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule, various conditions of clinic and clinician participation in Medicare, and various requirements applicable to state Medicaid programs, among other federal regulations.
The president may issue two distinct declarations under the Stafford Act when federal assistance is needed to supplement state, tribal, and local efforts and capabilities: an emergency declaration or a major disaster declaration. Both declarations authorize the distribution of federal relief funds and various forms of direct assistance, but the scope of assistance available under a major disaster declaration is broader than that under an emergency declaration. A state governor or tribal chief executive may only request a disaster declaration and accompanying federal assistance, but the president may issue a declaration unilaterally when an emergency exists for which the primary responsibility rests with the federal government.
___________________
1 Public Health Service Act 42 USC 247d.
2 See: Public Readiness and Emergency Preparedness (PREP) Act of 2005, Public Law 109-148, 109th Congress (December 30, 2005); Pandemic All-Hazards Preparedness Act, Public Law 109-417, 109th Congress (December 19, 2006); Pandemic and All-Hazards Preparedness Reauthorization Act (PAHPRA), Public Law 113-5, 113th Congress (March 13, 2013); Pandemic and All-Hazards Preparedness and Advancing Innovation Act (PAHPAIA), Public Law 116-22, 116th Congress (January 3, 2019), Public Health Service Act, Public Law 356, 117th Congress (January 25, 2023).
3 Public Readiness and Emergency Preparedness Act of 2005, Public Law 109-148, 109th Congress (December 30, 2005).
4 Social Security Act 42 USC § 1320b-5.
5 Robert T. Stafford Disaster Relief and Emergency Assistance Act, Public Law 100-707, 100th Congress (May 22, 1974) (November 23, 1988).
6 National Emergencies Act, Public Law 94-412, 94th Congress (September 14, 1976).
7 Public Health Service Act 42 USC 247d § 319.
During declared federal emergencies and disasters, federal authorities collaborate with SLTT authorities to provide emergency and disaster assistance, which may include services and supplies as well as financial assistance. Emergency declarations also act as triggers for provisions under other laws, which allow officials powers that they would not have in steady state conditions. The most well-known of these is found in Section 1135 of the SSA.8 This authority allows federal officials to temporarily waive or modify requirements under Medicare, Medicaid, and the Children’s Health Insurance Program during declared disasters and emergencies. Such 1135 waivers are designed to ensure the stability and availability of health care services during emergencies.
In March 2020, CMS issued an 1135 waiver modifying the requirements for clinicians under the Emergency Medical Treatment and Active Labor Act9 (EMTALA) (Brown, 2021). EMTALA ordinarily requires covered medical facilities to screen, stabilize, and appropriately transfer patients presenting to their emergency departments. This mandate, which is a condition for a clinician’s participation in Medicare, protects patients regardless of their ability to pay, documentation status, citizenship status, or other circumstances. COVID-19-era 1135 waivers allowed medical facilities to refer patients to alternative locations for screening, including those that were off site. Facilities were also allowed to transfer patients before they were fully stabilized.
During a declared PHE, federal officials may also exercise authorities available under various steady state provisions. For example, the SSA provides the basis for an Emergency Preparedness Rule applicable to health care institutions participating in CMS-funded programs (e.g., Medicare and Medicaid) (CMS, 2016). The PHSA10 includes communicable disease control powers that are not conditioned on an emergency declaration, such as the power to take measures deemed necessary by the HHS Secretary to prevent or mitigate the spread of communicable disease across international, state, or territorial borders.
CMS Emergency Preparedness Rule
The CMS Emergency Preparedness Requirements for Medicare and Medicaid Participating Providers and Suppliers Final Rule (EP rule) has particular relevance to PHE planning relevant to ensuring access to essential intimate partner violence (IPV) health care services. In 2016, this rule came into effect for all health care institutions participating in CMS-funded
___________________
8 Social Security Act Section 1135 42 USC § 1320b-5.
9 Social Security Act Section 1867 42 USC § 1395dd.
10 Public Health Service Act 42 USC § 264.
programs (Medicare and Medicaid) (CMS, 2016). The rule mandated the documentation of annual disaster response training; drill exercises; and plans for communicating how to contact local, state, and federal emergency preparedness officials (CMS, 2016). Examples of health care institutions subject to the EP rule and relevant to this report are hospitals, nursing homes, Federally Qualified Health Centers, community mental health centers, psychiatric residential treatment facilities, religious nonmedical health care institutions, and intermediate care facilities for individuals with intellectual disabilities (CMS, 2016).
The EP rule was designed to promote preparedness at the health care organization level, leaving flexibility to the organization in determining the amount and depth of training, drilling, and demonstrating competencies. This flexibility could be used to encourage preparedness activities among facilities with specific IPV care responsibilities.
Effects of Emergency Declarations
A PHE or disaster declaration can rapidly change legal requirements for health care delivery and financing. State emergency and disaster management declarations typically empower a governor to adopt reasonable and necessary measures for protecting life and property and bringing the situation under control. In some states, such as California and Oregon, these powers are far-reaching and may include the entirety of the state’s police powers.11 Disaster declarations open the door for funding and organizational support for the health care entities affected by a disaster, resources without which health care institutions may be unable to mount an effective response (ASPR, 2021a).
At the federal level, the president may issue an NEA12 declaration, which authorizes federal agencies to waive or suspend requirements and obligations under federal law. These remain in place for 1 year and may be renewed. The HHS Secretary may issue a declaration authorizing FDA to issue EUAs to facilitate the availability and use of medical countermeasures needed during PHEs. Section 564 of the Federal Food, Drug, and Cosmetic Act13 authorizes the FDA to issue EUAs for medical countermeasures, including personal protective equipment (PPE), diagnostics, therapeutics, and vaccines. EUAs allow the use of a countermeasure before it has met full FDA approval for the specific emergency use in question. Instead, the regulatory procedure for an EUA only requires federal officials to demonstrate that a current emergency justifies its issuance. Additionally, the HHS
___________________
11 Cal. Gov. Code § 8627; Or. Rev. Stat. § 401.168(1).
12 National Emergencies Act 50 USC 1601, 1621, 1622.
13 Federal Food, Drug, and Cosmetic Act Section 564 21 USC § 360bbb-3.
Secretary may issue a PREP Act14 declaration that limits liability for medical countermeasures provided during this time.
Indian Health Service and Tribal Emergency Preparedness
American Indian and Alaska Native (AI/AN) tribes have a unique relationship with the U.S. government. Based on treaties, laws, and court decisions, each of the federally recognized tribal nations maintain a government-to-government relationship with the U.S. federal government. With limited exceptions, state and local governments throughout the United States do not exercise authority over tribal governments (Hershey, 2019). These unique relationships are recognized within the American emergency preparedness and response structure at the federal level through amendments to the Stafford Act.15 These amendments allow tribal governments to declare emergencies and request presidential disaster declarations independent of the states. Additionally, FEMA policy16 recognizes the unique relationship between the tribal governments and the federal government and emphasizes specific consultations with tribal nations on issues that impact them (FEMA, 2020).
Given the diversity of AI/AN populations, it is difficult and potentially inappropriate to comprehensively identify the specific emergency preparedness and response challenges they face. Instead, the challenges many AI/AN individuals face are better understood through their general health risks and care limitations. These health factors are compounded due to the often-remote locations of most reservations. The emergency response services available to tribal members are often provided, similar to non-tribal neighbors, through a patchwork of federal (i.e., the Indian Health Service), state, local, and private providers (Genovesi, 2014). These providers, and the communities they serve, face challenges common to rural health care, including insufficient staffing, limited infrastructure, long travel times and distances, and challenging access to certain areas (Genovesi, 2014). In addition, AI/AN communities face the risk of morbidity and mortality and certain disease burdens at rates significantly higher than the national average (Hershey, 2019). This combination of increased risks and service delivery limitations makes the consistent delivery of high-quality care a particularly acute challenge when faced with PHEs.
___________________
14 Department of Defense, Emergency Supplemental Appropriations to Address Hurricanes in the Gulf of Mexico, and Pandemic Influenza Act, Public Law 109-148 Division C: Public Readiness and Emergency Preparedness (PREP) Act of 2005 § 2, 109th Congress (December 30, 2005).
15 See Sandy Recovery Improvement (SRIA) Act of 2013, Public Law 113-2, 113th Congress (January 29, 2013).
16 Federal Emergency Management Agency (FEMA) Policy 101-002-02.
The Indian Health Service (IHS) is an HHS agency that provides health services to AI/AN populations with the goal of “ensur(ing) that comprehensive, culturally appropriate personal and public health services are available and accessible to American Indian and Alaska Native people” (IHS, n.d.). Care in tribal communities is delivered primarily by IHS-supported facilities and, since 1976,17 in tribal-operated health care entities (referred to as 638 clinics). These facilities provide comprehensive primary care and support services in remote and underserved settings on tribal lands where they are typically the only health care professionals available in the area. In general, IHS clinicians function in a manner similar to health care professionals throughout the United States, building relationships and providing appropriate referrals to patients based on need and services available in the community (IHS, 2017). In a PHE, these entities are the essential health care organizations providing a comprehensive range of health and supportive services, including support and care to individuals experiencing IPV.
Federal Frameworks for Disaster Response
The federal government has established multiple overlapping frameworks and systems for accomplishing defined functions to prepare for and recover from disasters. Under the auspices of the Stafford Act, the PHSA, and other agency authorities, the National Response Framework coordinates federal agency responses to PHEs and other disasters, including providing guidance for organizational structures and preparedness (DHS, 2019a). The National Incident Management System includes and expands beyond federal agencies to support all public and private entities to implement an effective emergency response (FEMA, 2017). The National Response Framework delineates 15 Emergency Support Functions (ESFs), which provide the mechanism for coordination among federal agencies (DHS, 2019a). For example, ESF 8, Public Health and Medical Services, is coordinated by HHS and includes diverse partners such as the federal departments of Energy, Labor, and Defense; the U.S. Postal Service; and the American Red Cross (DHS, 2019a). Many of these agencies have primary or supporting roles in other ESFs. ESF 8 specifically addresses public health and medical services capabilities and is intended to coordinate health and health care in SLTTs and across federal agencies (DHS, 2019a). See Appendix A for additional information about ESFs.
The National Disaster Recovery Framework (NDRF) is a companion to the National Response Framework and provides a roadmap for promoting
___________________
17 Indian Self-determination and Education Assistance Act, Public Law 93-638, 93rd Congress (January 4, 1975)
successful disaster recovery, particularly from large-scale or catastrophic incidents (DHS, 2016). It provides guidance for coordinating the authorities and missions of federal agencies under the Stafford Act, PHSA, and other applicable statutes. The NDRF may be applied to an incident without a federal emergency or disaster declaration. It provides a flexible structure for disaster recovery managers to work in a unified manner and is intended to foster resilience in U.S. communities (DHS, 2016). Under the NDRF, Recovery Support Functions (RSFs) facilitate local stakeholder participation and promote intergovernmental and public–private partnerships (DHS, 2016). Each RSF is directed by designated federal agencies and supported by public and private entities at national, state, tribal, and local levels. Federal agencies gather pertinent specialists and stakeholders for planning during steady state conditions and then coordinate with the same individuals during post-disaster recovery to execute RSFs (DHS, 2016).
The multiplicity and overlap of these frameworks and functions have resulted in confusion among clinicians and members of the public alike. FEMA sought to reduce confusion when it introduced its Community Lifelines Implementation Toolkit, which enables the “continuous operation of critical government and business functions and are essential to human health and safety or economic security” (FEMA, 2023b). The Lifelines represent “the most fundamental services in the community that, when stabilized, enable all other aspects of society to function” (FEMA, 2023a). All eight lifelines in Figure 3-1 are interdependent and essential to enabling uninterrupted government and business functions essential to human health and safety or economic security (FEMA, 2023b). For example, the Health and Medical Lifeline includes objectives for restoring medical care, public health, patient movement, medical supply chain, and fatality management.
Disaster Response Resources
Much of the human resources operational capacity for larger-scale PHE response is focused at the federal level. Volunteer organizations such as the American Red Cross and faith-based organizations also play an important role. Disaster health responder teams need basic capacities to safely deploy in a PHE: rapid mobility, self-containment, self-sufficiency, and multidisciplinary team composition. These teams are often required to deploy within hours of a disaster or stage in a nearby location when a disaster is expected. These teams are expected to be able to independently set up and staff a field hospital and provide health care within hours of arriving on site. Teams usually arrive with adequate equipment, supplies, food, and water to last at least 72 hours (Weiner and Rosman, 2019). Several federal agencies have structures and plans that can help provide human resources, equipment, and protection for deploying disaster teams.
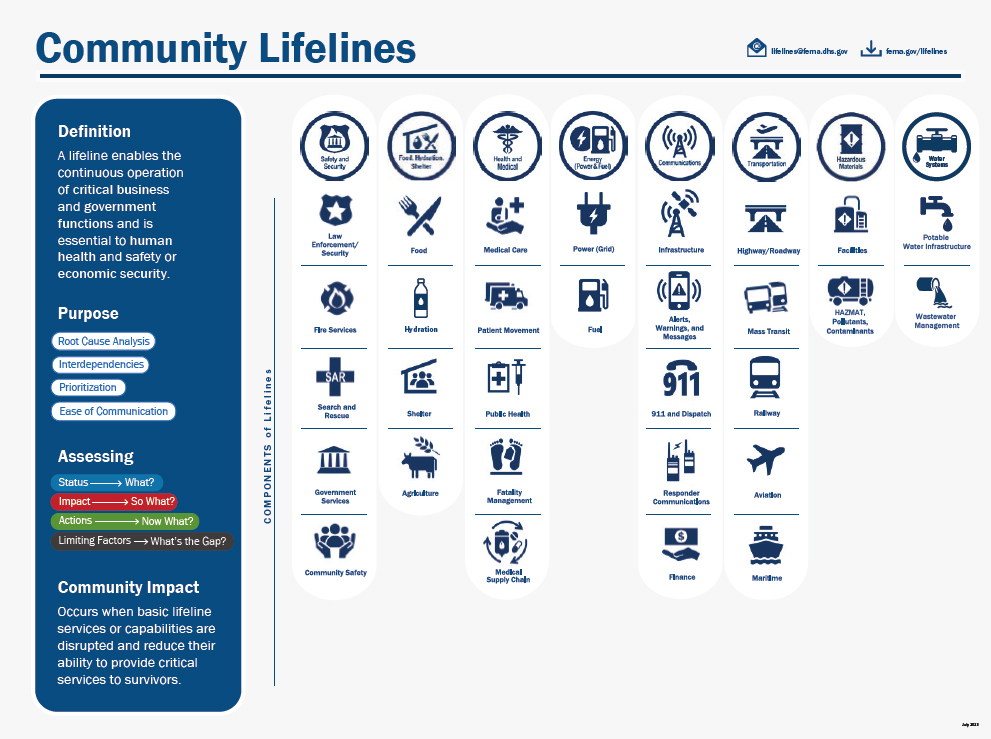
SOURCE: FEMA (2023b).
Additional protections are required for essential health care workers to continue providing care for people experiencing IPV during a PHE. This may include nonpharmaceutical interventions and supplies, such as PPE (gowns, masks, respirators), and pharmaceutical interventions, such as vaccination and pre- and post-exposure prophylaxis. Ensuring the safety of the IPV workforce is essential for maintaining their ability to support those affected by the PHE.
The National Disaster Medical System
The purpose of the National Disaster Medical System (NDMS), overseen by ASPR, is to support SLTTs during PHEs by supplementing existing health and medical systems and response capabilities (ASPR, 2021b). Disaster Medical Assistance Teams (DMATs) are comprised of health care clinicians that provide rapid-response health care when health needs due to disasters or PHEs overwhelm SLTT health resources (ASPR, 2021b). DMAT teams provide patient care in numerous settings and scenarios, including triage and pre-hospital care, general emergency medical care, general
medical care, hospital decompression, patient movement and transfer support, and mass prophylaxis and vaccinations (ASPR, 2021b).
Public Health Emergency Response Strike Teams
Public Health Emergency Response Strike Teams are active duty officers with the U.S. Public Health Service (USPHS) who serve as first responders in the event of disasters and PHEs (USPHS, 2022). These teams are designed to deploy rapidly to regional, national, and global emergencies. When not deployed, they support staffing gaps across USPHS-staffed facilities (USPHS, 2022).
Veterans Health Administration
In addition to providing services to veterans during PHEs, the fourth mission of the Veterans Health Administration (VHA) includes providing support to nonveteran civilians during times of crisis. Employees of the VHA may be deployed or diverted from their usual roles to provide health care support during federally declared disasters. During disasters, the VHA supports the NDMS (VA, 2021).
Health Care Coalitions
ASPR developed the Hospital Preparedness Program and its associated Health Care Coalitions (HCCs) as part of the response to the September 11, 2001, terror attacks and subsequent anthrax attacks (West Region Health Care Coalition, 2023). The purpose of HCCs is to ensure that local communities can respond to emergencies in an integrated, smooth, and timely manner (ASPR, 2016). Composed of geographically related health care and response organizations, HCCs are generally considered the regional organization supporting health care readiness (ASPR, 2016). They are vital for bridging the gap between public health and the health care community (IOM, 2015). The function of this group often depends on the context of the given community. Generally, HCCs are expected to organize stakeholders, medical supplies, real-time communication retrieval, and trained personnel. HCCs are critical for providing logistical guidance during disasters and safeguarding communities from preventable harm (ASPR, 2021b).
A vital role of HCCs is establishing relationships across health care entities on blue-sky days to ensure that effective communications are in place before a disaster event. HCCs also serve as a resource to local and regional health care organizations regarding preparedness planning, including coordinating medical response and surge exercises (ASPR, 2016). This
unique organizational role could position HCCs as a conduit for ensuring a greater emphasis on IPV care in PHEs, whether through developing and deploying specific protocols or by including IPV scenarios in drills and tabletop exercises.
Emergency Management Assistance Compact
The Emergency Management Assistance Compact (EMAC)18 was created to better provide support in resource-limited conditions and the communities affected by disasters by providing an avenue for assistance between states during disaster declarations. It was signed into law in 1996 under Public Law 104-321. All 50 states and multiple territories have become members via legislation. EMAC’s design is intentionally straightforward, allowing responsive action for sharing staff, equipment, and other supplies to support response and recovery in other states. Its governance structure supports building and maintaining relationships across federal and SLTT entities and professional organizations to encourage open communication and sharing of resources. A core strength of EMAC is its ability to move nearly any resource from one state to another (EMAC, 2023).
Building on the successes of EMAC could be an avenue for collaboratively designing and implementing a system that coordinates access to essential IPV resources through existing protocols and agreements. For example, EMAC supports using and disseminating mission-ready packages, which are “specific response and recovery capabilities that are organized, developed, trained, and exercised prior to an emergency or disaster” (GOHSEP, 2023). Developing a tailored mission-ready package could be of value to IPV care in PHEs.
Public Health Emergencies and Health Disparities
The scientific and lay literature has demonstrated that historically and structurally marginalized populations experience worse outcomes during disasters and PHEs (NASEM, 2019). Specifically, the interaction of weather- and climate-related disasters with the built environment causes damage to critical infrastructure that is essential for the health of communities, such as access to food, water, shelter, health care, transportation, and electrical power (Michaud and Kates, 2017). The current-day consequences associated with structural racism19 can also influence this interaction. Widening
___________________
18 Emergency Management Assistance Compact, Public Law 104-321, 104th Congress, (October 19, 1996).
19 Structural racism refers to the ways in which systems such as housing, health care, and education affect and reinforce biases and the discriminatory distribution of resources.
social inequalities, increasing urbanization, and rapid population growth—particularly in coastal areas—further predispose certain groups to disaster-related disparities (Raker et al., 2020).
After a disaster, disruptions in access to health care can be devastating for the 60 percent of American adults living with at least one chronic condition (CDC, 2022). Individuals with chronic health conditions may depend on medical equipment using electrical power, from refrigerators to keep insulin chilled to dialysis to continuous positive airway pressure machines. The careful adherence to the medical treatments needed to keep health conditions under control, such as medication regimens, may be at risk following a PHE. Additionally, mental health practices, substance use disorder treatment practices, health care centers, and dialysis services may experience operational interruptions, and transportation to alternative sources of care may not be possible. Such PHE-related disruptions have been associated with increased hospitalizations among those with chronic and comorbid conditions (Bell et al., 2022). Furthermore, research has described challenges in long-term health care access—specifically the availability of health care professionals—in disaster-affected communities with socioeconomic disparities (Bell et al., 2020).
Older adults are also vulnerable to poor health outcomes during disasters. While age itself does not make an individual at risk, social isolation, frailty, chronic and comorbid diseases (as described above), and cognitive impairment—all issues common to older adults—do. The acute disruption of a disaster can exacerbate these potential vulnerabilities for older adults. Almost 50 percent of deaths attributed to Hurricane Katrina were among adults aged 75 and older (Brunkard et al., 2008). Living through a hurricane has been associated with increased mortality among older adults with dementia, a highly vulnerable group that needs caregiver support for situational awareness during a disaster (Bell et al., 2023).
Racial and ethnic disparities continue to mount after PHEs, despite being documented for decades (Fothergill, 1999). A recent review of multiple studies of heat, extreme cold, hurricanes, flooding, and wildfires finds evidence that minoritized populations, including Black, Hispanic, Native American, Pacific Islander, and Asian communities, are generally at higher risk of climate-related health impacts than are White communities (Berberian et al., 2022). Multiple studies describe racial and ethnic disparities in mental health outcomes after hurricane and flood events, including high rates of depression, anxiety, and post-traumatic stress disorder (Alexander et al., 2017; Ali et al., 2017; Flores, 2020; Ma et al., 2021). While White individuals made up 68 percent of total disaster and extreme weather mortality in a recent study, mortality per 100,000 rates among Black individuals were 1.87 times higher than among White individuals, and for non-Hispanic AI/AN populations mortality per 100,000 was 7.34 times higher (Sharpe and Wolkin,
2022). Extreme heat has also been associated with higher all-cause mortality in the United States, with a greater increase noted among older adults and non-Hispanic Black individuals (Khatana et al., 2022).
Figure 3-2 and Figure 3-3 display Columbia University’s Natural Hazards Index (NHI) and CDC’s Social Vulnerability Index (SVI), respectively. The NHI shows hazard exposure data at the census tract level for 14 types of natural disasters (NCDP, 2023). The SVI measures the “potential negative effects on communities caused by external stresses on human health” (ATSDR, 2023). Together, these graphics illustrate that the geographic regions that are most socially vulnerable, particularly the Southern and Western United States, are also disproportionately exposed to natural hazards and disasters. In other words, historically and structurally marginalized populations face more harm from natural disasters, but they are also more likely to face them.
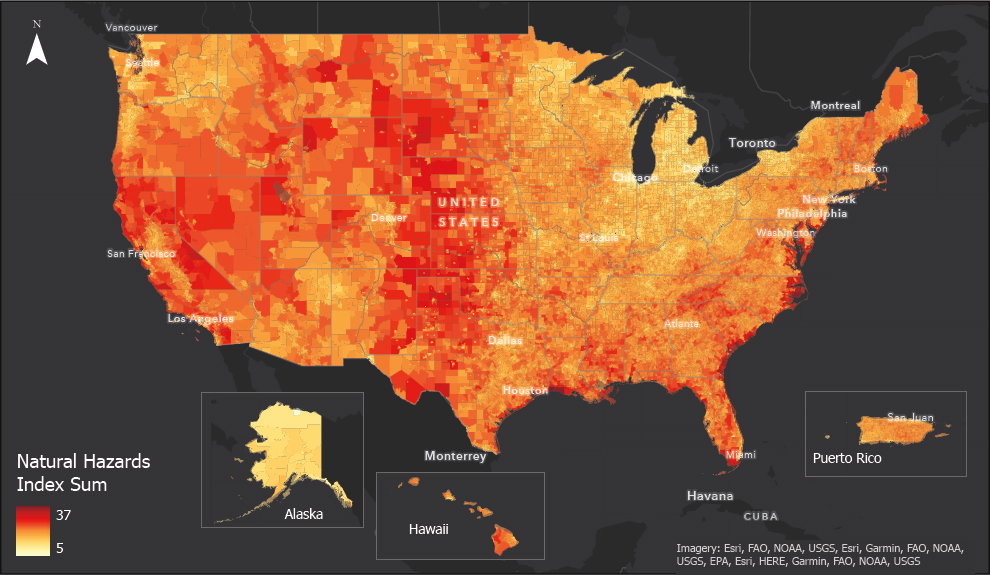
Notes: For detailed documentation including available hazard layers by region, data interpretation and limitations, and views of individual hazard layers, visit the Natural Hazards Index project homepage with live map application at https://bitly.com/hazardsindex. This tool is a hazards map, not a risk map and can be used as a planning tool but does not factor in local mitigation and preparedness efforts or population exposure.
SOURCE: Columbia Climate School National Center for Disaster Preparedness 2023.
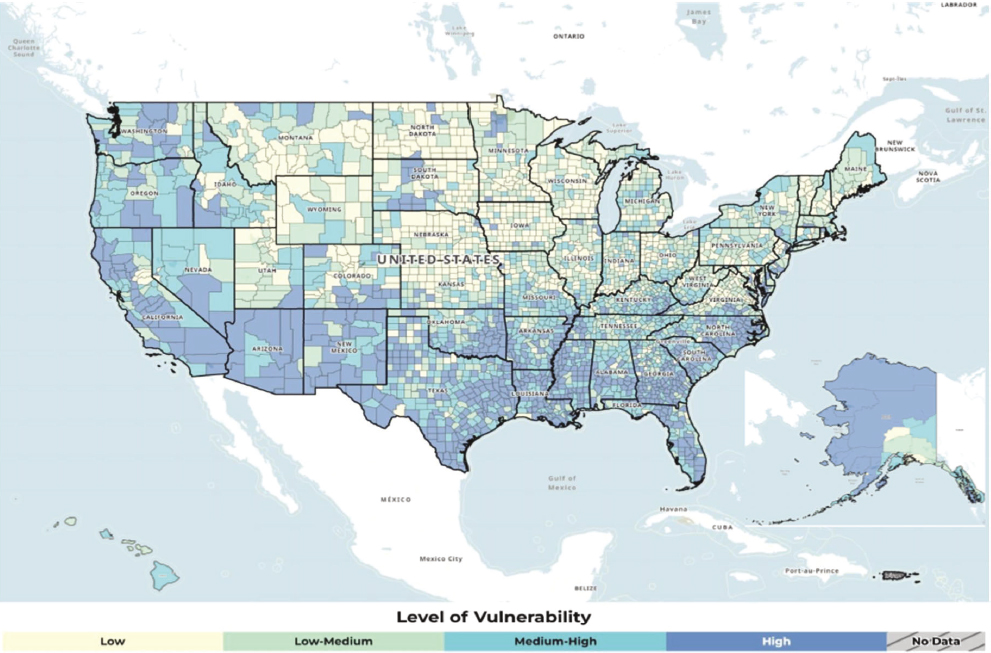
SOURCE: ATDSR, 2023.
INTERSECTION OF PUBLIC HEALTH EMERGENCIES AND INTIMATE PARTNER VIOLENCE
Effects of Public Health Emergencies on the Prevalence and Severity of Intimate Partner Violence
PHEs are a time of increased prevalence and severity of IPV. The causes and pathways for these effects overlap and tend to exacerbate inequities. Access to resources and support becomes more challenging for those experiencing IPV. Women experiencing IPV during PHEs can face additional safety risks because of disruptions in the normal function of some government services and lines of communication for measures such as orders of protection. Some mitigation or support efforts focused on the PHE, such as shelter-in-place orders and social distancing, may inadvertently worsen situations for survivors. Those experiencing IPV may be further isolated by abusive partners and structural barriers emerging during the PHE, such as a lack of support services, making it more challenging to connect with care.
Intimate Partner Violence During the COVID-19 Pandemic
The most recent surveillance data and research related to IPV during PHEs comes from the COVID-19 pandemic. The increase in IPV during the COVID-19 pandemic, particularly during the earlier periods of the pandemic, received attention in the media and among the IPV care professionals, advocates, and others who provide care and support for individuals experiencing IPV (Evans et al., 2020; Gupta and Aviva, 2020). Researchers have examined data from IPV hotlines, hospitals and other health care settings, IPV support service providers, and surveys to gain insight into IPV during the COVID-19 pandemic.
In a study by Ragavan and colleagues (2022), victim service advocates shared multiple tactics used to control, frighten, or manipulate IPV survivors. Abusive partners sought to isolate their partners during stay-at-home orders and social distancing that occurred during the COVID-19 pandemic. The inability to seek respite from a violent relationship through work or other activities with friends and family created further stress for survivors of IPV (Ragavan et al., 2022). The advocates explained that blocking or turning off cell phones or internet service was used as a form of coercive control that added to isolation. They also found that partners may withhold health insurance, information about the pandemic, and protective materials including hand sanitizer, as additional ways to create dependence and fear (Ragavan et al., 2022).
Hospital-based studies may not accurately reflect the experiences of those at elevated risk for IPV, as these individuals may not be presenting to hospital settings during infectious disease-related PHEs such as the COVID-19 pandemic. Thus, a systematic review by Beiter and colleagues (2021) found mixed evidence of increases in violent trauma reported by hospitals; two of three studies reported increases in IPV-related trauma as a proportion of all traumas. Gosangi and colleagues (2021) examined health records and clinical and radiological data for patients at a large urban academic medical center in the United States. They found that the number of patients reporting IPV decreased in 2020, but they observed an increased incidence of physical IPV, with a greater number of deep injuries per victim. Some hospital-based studies during the COVID-19 pandemic found reductions in overall emergency room use and IPV-related admissions (Muldoon et al., 2021).
In contrast, a study from a single-site trauma center (using interrupted time-series analysis) found that the IPV incidence nearly doubled compared with before the pandemic (Smith et al., 2022). Smith and colleagues (2022) described a 17 percent increase in IPV-related injury admissions in the weeks following the start of the COVID-19 pandemic shelter-in-place order. Avalos and colleagues (2023) noted a 38 percent increase in the first month of the pandemic in unsafe and unstable living situations among pregnant women.
Holland and colleagues (2021) reported on cross-sectional data from CDC’s National Syndromic Surveillance Program that were collected before and during the COVID-19 pandemic. These data, which capture about 70 percent of emergency department encounters in the United States, showed decreases in IPV-related visits to the emergency department during the pandemic (Holland et al., 2021). This underscores the dramatic shifts in care seeking at emergency departments that occurred as a result of the pandemic (Holland et al., 2021). Many studies noted the likelihood of under-reporting and undercounting IPV due to fear of infection and limited hospital and community resources.
A nationally representative online survey in 2020 during the pandemic assessed physical and psychological IPV. An analysis of the results found that people who were infected with COVID-19 or who lost employment were more likely to use and experience IPV (Davis et al., 2021). Similarly, in a cross-sectional online survey in the spring of 2020, 18 percent of respondents reported IPV, with increased odds of experiencing IPV among those with employment or income change due to the pandemic than those without change (Jetelina et al., 2021). Furthermore, IPV worsened in severity among those experiencing physical and sexual IPV (Jetelina et al., 2021).
In an anonymous online survey conducted from May 2020 through July 2020 focusing specifically on lesbian, gay, bisexual, transgender, and queer (LGBTQ+) adults (N=1,090), those who had experienced IPV in their relationship prior to the COVID-19 pandemic (n=98) reported increasing frequency of IPV since the pandemic began (Stults et al., 2022). More than 18 percent of those LGBTQ+ individuals reported an increase of IPV frequency, with 45.9 percent reporting that the instances stayed the same (Stults et al., 2022). A general population online survey of women, transgender, and nonbinary individuals in Michigan in July and August of 2020 found that nearly 10 percent of respondents had reported new or more frequent IPV since the start of the pandemic (Peitzmeier et al., 2022). This study also highlighted key demographic differences for those who identified as sexual/gender minorities, younger, urban or suburban, pregnant, had disabilities, or had less educational attainment, demonstrating that these groups were more likely to report incidents of IPV or exacerbated IPV since the start of the pandemic (Peitzmeier et al., 2022).
According to nationally representative data from the Adolescent Behavior and Experiences Survey (conducted from January to June 2021 among more than 7,000 respondents), 1 in 12 female-identified respondents had experienced non-dating sexual violence, 12.5 percent had experienced sexual dating violence, and 7.7 percent had experienced physical dating violence (Krause et al., 2023).
Intimate Partner Violence During Heat Waves
Extreme heat events can also disrupt routine capabilities. Heat-related health problems can lead to patient volume surges that overwhelm first responders and health care systems (Sanz-Barbero et al., 2018). Patient surges can be compounded by extreme heat or humidity that limits the function of some medical equipment and the first responders themselves. Excessive heat can also exacerbate relationship tensions and contribute to increased aggressive or violent behavior in some people (Sanz-Barbero et al., 2018). Heat waves and prolonged exposure to high temperatures can have serious physiological and psychological repercussions, such as increased irritability, discomfort, and sleep disruption (Vida et al., 2012). When these variables are combined with other stressors, they can exacerbate conflicts and raise the possibility of violence within partnerships.
Extreme heat has been linked to an upsurge in IPV (Henke and Hsu, 2020). Increases in police reports of domestic abuse (including IPV) phone calls and requests for access to shelters have also been documented during episodes of extreme heat (Rotton and Cohn, 2001; Sanz-Barbero et al., 2018). The impact of this violence extends throughout time, with varied lag periods depending on the violence indicators studied. The latency between temperature rising and aggression could be important in establishing strategies to avert catastrophic consequences of IPV (Sanz-Barbero et al., 2018).
Intimate Partner Violence During Hurricanes and Other Storms
A rapid review of 12 studies examining the relationship between IPV and disasters suggests increased severity and frequency of IPV during pandemics and natural disasters (Brabete et al., 2021). Anastario and colleagues (2009) reported increases in the lifetime prevalence of gender-based violence and IPV in the 2 years after Hurricane Katrina, with associated increases in depressive symptoms and suicidal ideation.
Intimate Partner Violence During Technological Disasters
Technological disasters are caused by the breakdown or malfunction of a technological system (Lindsey et al., 2021). They may occur spontaneously due to a natural disaster, mechanical malfunction, human error, or intentional attacks. Technological disasters include blackouts, hazardous waste incidents, oil spills, nuclear or radiological events, and cyberattacks. In addition to the unique logistical pressures presented by technological disasters, evidence shows that they substantially harm survivors’ mental health (Longmuir and Agyapong, 2021; Osofsky et al., 2011; Rubin and Rogers, 2019). Women have been shown to be particularly affected by these
harms during technological disasters (Rung et al., 2016). Technological disasters also have unique and gendered resilience dynamics (Ferreira et al., 2018; Lightfoot et al., 2020).
There is little evidence on the prevalence of IPV during technological disasters. However, women who experienced exposure to the Deepwater Horizon oil spill were twice as likely to have experienced both emotional and physical IPV (Lauve-Moon and Ferreira, 2017).
Double Survivorship
Women experiencing IPV during PHEs experience double survivorship, in the form of enduring IPV (one survivorship experience) within the context of a PHE (another survivorship). Women with current or previous experiences of IPV are often called survivors because they experience psychological and physical trauma and injuries, and they are encouraged to be empowered to recover from their situation (Alexenko et al., n.d.). Given that IPV can result in severe injuries and homicide, the concept of survivor also helps to communicate that individual’s ability to outlive that situation. Similarly, individuals experiencing a PHE are also often referred to as survivors because they have been exposed to psychological and physical trauma and injuries related to the event or circumstance of that PHE and have stayed alive (e.g., lived through a disaster, war, or pandemic). Similar terms are used in these different survivorship experiences when referring to necessary resources such as shelter. It is important to consider the context of these resources—for example, whether shelter is needed because of the IPV, PHE, or both—when considering essential services for this population.
Survivors of IPV and PHEs often experience similar sequelae related to their experiences that when combined, are likely to have a cumulative or synergistic effect on their experience of trauma. For example, symptoms of post-traumatic stress disorder (PTSD) are among the most common consequences of IPV and are also common in a PHE such as a natural disaster (Golding et al., 1999; Lai et al., 2017). Research shows that individuals with a history of trauma and PTSD are more likely to have a more severe traumatic stress response in the context of a new stressor and trauma exposure. For example, poly-victimization and exposure to multiple types of child maltreatment have been associated with increased severity of PTSD among pregnant women (Carney et al., 2023). Similarly, female veterans experiencing IPV are likely to have experienced other forms of trauma (e.g., military sexual assault), thus compounding the burden of IPV (Rossi et al., 2020).
Trauma exposure related to PHEs likely exacerbates the risk for IPV. Research conducted in Africa using the Uppsala Conflict Dataset documented that an increase in the frequency and severity of IPV was associated with an increase in the number of battles an individual had experienced (Le
and Nguyen, 2022). Similarly, a study of married couples in refugee camps found that IPV exposure among women was associated with increased exposure to war events and the associated psychopathology among their male partners (Goessmann et al., 2019).
Studies of other emergencies have also suggested a link between trauma exposure and IPV risk. One study examining conflict tactics between postpartum women and their partners after Hurricane Katrina found that women who experienced damage to their home or property during the storm were more likely to report experiencing one or more of physical, mental, or sexual violence from their partner (Harville et al., 2011). Similar results were reported after the 2010 earthquake in Haiti. Women who resided in the hardest hit areas of Haiti were more likely to report physical and sexual IPV (Weitzman and Berhman, 2016). Weitzman and Behrman (2016) also found that women who lost a household member, lived in a displacement camp, or whose households were affected by the subsequent Haitian cholera outbreak were more likely to report IPV.
Given the prevalence of IPV and the potential for cumulative trauma during and after a PHE, screening for both IPV and stress responses is needed. However, clinicians should be cautious and use appropriate timing when screening for traumatic and stress responses. For example, receiving a new diagnosis of HIV could constitute another traumatic event for women seeking care for IPV (Williams et al., 2017). On the other hand, some women have reported that comprehensive services during IPV screening and treatment have provided peace of mind and helped them move forward (Gonzalez-Guarda et al., 2021). Similarly, women may have different responses to the cumulative traumas of a PHE and IPV. Therefore, it is crucial to keep the experience of double survivorship in mind when screening for IPV during PHEs. Screening for IPV during PHEs using a trauma-informed approach and being guided by the perspective of the person experiencing IPV facilitates collaborative development of strategies that are feasible, acceptable, and safe (CDC, 2020). Services for women experiencing IPV during PHEs should apply these principles of trauma-informed care and empower those individuals to define their own needs and preferences, set their own goals, and make their own choices about the services they receive, with a focus of promoting physical, psychological, and emotional safety (CDC, 2020). Clinicians may need to seek out opportunities to revisit IPV screening if women report that they are currently unable to discuss their experiences.
Barriers to Accessing Intimate Partner Violence Care During Public Health Emergencies
Barriers to accessing care during PHEs include damage to health care facilities, displacement of survivors and health care staff, dysfunctional
health care systems during disasters, and staff burnout. Additionally, as mentioned earlier, regulatory and other measures taken to mitigate the risks associated with PHEs may result in unintended barriers to care. These barriers compound the challenges people experiencing IPV encounter when in need of care during steady state conditions. Officials may institute policies that limit certain health care services during PHEs to reserve limited supplies and staff for the care of individuals with the most severe conditions or injuries. For example, officials and health care system leaders cancelled surgeries and other procedures that were considered elective during the COVID-19 pandemic when hospitals were at risk of being overwhelmed with infected patients (CovidSurg Collaborative, 2020). This limited the health care services that could be provided to people experiencing IPV during those times (see Box 3-1).
In the past, PHEs have been disruptive to substance use treatment programs and hindered access to mental health services. Disruption to substance use treatment can lead to withdrawal symptoms, and potential relapse (Rutkow et al., 2012). Post Hurricane Katrina emergency shelters were reported to be ill equipped to assist those who had been receiving substance use care, leaving those individuals without the necessary proper treatment (Rutkow et al., 2012).
BOX 3-1
Effect of the COVID-19 Pandemic on Health Services Delivery
“The anterior cruciate ligament is a major ligament in the knee that is commonly sprained or torn. Those types of sprains happen in women that have been victims of intimate partner violence. Those types of injuries were felt to be more elective than urgent for care. So while we were able to address most fractures in a fairly expeditious timeframe, other injuries got put on the back burner. Also, non-hospital-based clinics for non-trauma orthopedic surgeons may have been shut down completely depending on the municipality.”
—Gregory Della Rocca,
University of Missouri-Columbia
Department of Orthopaedic Surgery
SOURCE: Della Roca, G. 2023. Orthopaedic surgeons’ roles in the identification and management of injuries related to intimate partner violence. Presented at Sustaining Essential Health Care Services Related to Intimate Partner Violence During Public Health Emergencies Meeting #3B, Washington, D.C.
Shelter-in-place or stay-at-home orders are issued at local, state, tribal, or federal levels because of PHEs such as pandemics, chemical hazards, or winter storms (DHS, 2019b). These orders are put in place to protect people in the affected area from an external hazard. During PHEs involving infectious respiratory diseases, as with COVID-19, officials may also enact physical distancing rules to reduce the spread of illness (NASEM, 2020). While effective at reducing the spread of contagious respiratory viruses, this strategy also creates challenges for IPV shelters (see Box 3-2).
The PHE and the immediate emergency response can create conditions that serve as physical barriers that disrupt the delivery of IPV care services. Disasters ranging from blizzards to wildfires can damage infrastructure critical to delivering care for people experiencing IPV. Road closures due to damage or obstruction from water, snow, or debris can limit or prevent staff and the people needing services from getting to facilities. While hospitals typically have generator support to provide backup power for a limited period in case of power outages, this is often not the case for outpatient facilities, social service facilities, and community-based organizations. Damage to facilities can limit or completely disrupt the provision of services, particularly during the early hours or, in some cases, days of a PHE.
Immigration documentation status can create challenges for accessing IPV-related health care services during a PHE. People who are undocumented are not eligible for government-sponsored insurance programs (e.g., Medicaid or Medicare) and may not meet eligibility requirements for government-supported prevention and support services that are limited to citizens during a PHE (KFF, 2023). For example, during the COVID-19 pandemic, U.S. workers without documentation often worked in essential jobs (construction,
BOX 3-2
Effect of Distancing Orders on IPV Shelters
“Sharing a room became a big problem. We had to have only one family per room, which had a very significant impact on our occupancy level.”
—Ivon Mesa,
Community Action and Human Services Department,
Miami-Dade County
SOURCE: Mesa, I. 2023. Miami Dade County Violence Prevention and Intervention Division. Presented at Sustaining Essential Health Care Services Related to Intimate Partner Violence During Public Health Emergencies Meeting 2, Irvine, CA.
food production, health care) but could not access COVID-19 economic relief (Disney et al., 2022). Additionally, individuals may have been reluctant to access COVID-19 food and housing assistance because they feared doing so would have a negative effect on their applications for residency or citizenship, even if they were eligible for these services (e.g., free testing and vaccinations) (Disney et al., 2022). In much the same way, documentation status can be a real or perceived barrier to accessing care and social services for IPV (Parson et al., 2016; Valdovinos et al., 2021). The disproportionate adverse effects that PHEs have on people without documentation can increase levels of stress and trauma, which may also worsen the severity and frequency of IPV within those populations.
Interventions to address IPV during PHEs may be improved by considering the intersectional ways in which marginalized groups may be at greater risk for experiencing IPV. For example, acculturative stress—the stress associated with adapting to a new culture and context for immigrant groups—is a known contributor to IPV (Cao et al., 2023; Kim, 2019). Family-level stressors, such as disagreements among family members related to cultural practices and an inability to center family needs, appear to be the most influential form of acculturative stress in predicting IPV risk (Cao et al., 2013; Cervantes et al., 2016). In general, interventions that address family stressors and differences in cultural values and perspectives among family members appear promising in improving health outcomes (Leite et al., 2023).
Accessing IPV-related health care services during PHEs requires a workforce to deliver that care. The COVID-19 pandemic placed extreme stress on the U.S. health care workforce, exposing its fragility, a lack of preparedness, and the starkly limited operational capacity for providing basic health care during a national crisis (NASEM, 2020). This increased the likelihood of first responders and other health care professionals exiting the workforce (Hendrickson et al., 2022). This was highlighted in an analysis of data collected from a survey of New York state physicians, nurse practitioners, and physician assistants first in April 2020, then repeated with the same clinicians in February 2021, which found that more than a third of respondents considered leaving their profession at least once monthly (N=978, 35.6%; 95% CI: 31.9–39.4%) (DiMaggio et al., 2023). The insights gleaned during the COVID-19 pandemic and other PHEs create an opportunity to address the ongoing barriers to accessing IPV care during disasters—as well as to address existing underlying challenges exposed by these disasters—to better support those affected by IPV. This includes managing the urgent need to shift from the current reactive approach to disasters to a proactive one. For health care organizations in disaster-affected areas, many of which are under-resourced, addressing mitigation and preparedness while still being in response or recovery mode is an enormous challenge. The 2022
Federal Plan for Equitable Long-Term Recovery and Resilience for Social, Behavioral, and Community Health20 provides several recommendations that could be beneficial for addressing these challenges.
Support Services
Community-based organizations, neighborhood associations, community outreach workers, and other support service providers are critical for addressing social drivers of health during steady state periods. In the context of PHEs, such community partners, usually trusted community members, can be vital partners (Gilmore et al., 2020). These groups are uniquely positioned to carry out essential functions, including the rapid mobilization of community health champions within harder-to-reach populations, building trust with the emergency response system, communication about available resources and mitigation of risk, data collection for surveillance and tracking, and guiding local response protocols (Gilmore et al., 2020). Although not always specific to IPV, these community partnerships provide vital services that mitigate the risk of poor outcomes for people experiencing IPV. Community-based service providers for IPV can provide critical feedback on developing, funding, implementing, and evaluating services and programs to prevent and respond to IPV during PHEs. Including community voices in preparation for PHEs ensures that the programs are relevant and responsive to community priorities, assets, and challenges. Simultaneously, culturally responsive care and attention to health equity in clinical practices during PHE response can reduce health disparities experienced by populations disproportionately affected by IPV during PHEs.
The increased intensity of IPV during PHEs highlights the need to prioritize support services that ensure the safety of these women (Gosangi et al., 2021). Among people experiencing IPV, access to safer housing (e.g., domestic violence shelters), advocacy services, and counseling have been found to increase a sense of safety (Bennett et al., 2004; Campbell and Glass, 2009; Sullivan, 2012). Economic, housing, and food resources, which aggravate stress in existing abusive relationships, are often disrupted during a PHE (Gilroy et al., 2016; Ricks et al., 2016; Tur-Prats, 2021). Consequently, support services that ensure access to food, water, and shelter can be a primary strategy for preventing the escalation of IPV during a PHE.
In studies conducted among advocacy and service provision organizations during the COVID-19 pandemic, advocates and administrators of victim service and child welfare agencies described using many workarounds and strategies to continue their work (also see Box 3-3) (Garcia et al., 2022;
___________________
20 https://health.gov/our-work/national-health-initiatives/equitable-long-term-recovery-and-resilience (accessed August 28, 2023).
BOX 3-3
IPV Service Providers’ Adaptations During the COVID-19 Pandemic
“…in 2020 a lot really had changed. In our county, we all had to shelter in place beginning, I think it was March 16th, 2020, when all of our school districts were ordered to go to work remotely from home. We really needed to continue our outreach and prevention work because now students weren’t physically at school, so the ability for mandated reporters to identify things sooner, or for students who were more comfortable in person and, maybe, sharing things with school staff, that all had now changed when we all went to distance learning. So some of the trainings that we provided that year—and actually ongoing even into 2021, part of 2022—is these considerations for COVID. They talked about text chat lines that might be more helpful than call-in numbers, because as we know, our students usually tend to be more comfortable doing chat lines.”
—Charisma De Los Reyes,
Student Wellness and Student Culture Department,
San Diego County Office of Education
“COVID brought a lot of challenges and concerns that our home visitors expressed about being able to see our clients. A lot of times, what we heard during COVID is that it was really important for the home visitor to have eyes on the family, because that’s something they typically could do. So that was a challenge. However, virtual visits were done, phone calls were done, and then they were creative sometimes, too, during COVID. They would just drive to the outside of the house and do a lesson on the lawn or do social distancing where they could visit and provide whatever information that family might need at that time.”
—Lisa Martin,
Johns Hopkins University
Center for Indigenous Health
“When the pandemic hit, it opened up opportunities that we have been fighting for for a really long time, like the ability to have phone visits, like the ability to coordinate care virtually, or having shorter visits, having more customized care because of what we could do. All of a sudden, access to care opened up for some of our survivors who had never been able to access care.”
—Anita Ravi,
PurpLE Health Foundation
Renov et al., 2022). Advocates needed to adjust their approaches and communication strategies to address and support safety. Virtual service provision was often a key strategy for increasing access to support services (Garcia et al., 2022; Ragavan et al., 2020a,b, 2022; Renov et al., 2022). IPV agencies connected rapidly and informally with other community organizations (e.g., grocery stores, food banks, and aid groups) to help share services and increase awareness of support services. At times, larger (or more well-resourced or experienced) agencies reached out to assist smaller, less connected agencies and to advocate on their behalf for additional resources (Garcia et al., 2022; Renov et al., 2022). Administrators noted a need for flexibility in the administration (and subsequent use) of disaster relief funds to adapt to the changing landscape and better support clients and staff. Additionally, culturally affirming organizations often experienced compounding impacts on their time without receiving equitable compensation (Garcia et al., 2022). Staff and administrators were also personally affected by the pandemic, with disruptions in school, child care, and employment, all contributing to burnout (Garcia et al., 2022; Renov et al., 2022).
EXISTING GUIDANCE FOR INTIMATE PARTNER VIOLENCE HEALTH CARE DURING PUBLIC HEALTH EMERGENCIES
The committee sought to identify existing, widely available guidance or standard protocols for disaster and emergency responders specific to IPV care during PHEs in the United States. In order for a resource to be considered widely available, it had to be public-facing and free to access. These efforts identified federal resources that included general guidance and suggested actions with varying levels of detail but had little success in identifying public-facing standard protocols. Researching federal agency protocols, guidance, and training programs explicitly addressing IPV during PHEs and disasters often required multiple keyword searches of individual documents identified following lengthy searches of numerous sections of various agency websites. In order for guidance to be practical, it should be easily accessed by those who need it, such as busy emergency planners and health care clinic leaders, as well as those working on the front lines during PHE response. Some state emergency operations plans echoed a common theme from various federal guidance items that encouraged emergency responders to have phone numbers for domestic violence hotlines and shelters available.21 Notably, most guidance referred to domestic violence
___________________
21 For example, see the emergency operations plans found on the emergency management department websites for Kentucky (https://kyem.ky.gov/programs/Pages/State-ESP-and-EOP.aspx) and Arizona (https://dema.az.gov/emergency-management/preparedness/planning-branch) (accessed April 2023).
instead of explicitly addressing IPV. In instances when IPV and domestic violence overlap, these resources may offer valuable information and protocols. However, guidance focused on domestic violence often frames IPV in the context of families with children and relationships with both partners residing in the same home. This can lead planners and disaster health responders to overlook the possibility of IPV in families that do not have children, couples that do not live together, or former intimate partners.
The most recent version of FEMA’s Developing and Maintaining Emergency Operations Plans: Comprehensive Preparedness Guide 101 encourages emergency planners to “identify and describe the actions that will be taken to provide alternate shelter accommodations for evacuees from domestic violence shelters” (FEMA, 2021, p. C-17). FEMA’s planning guidance for evacuation and shelter-in-place for SLTT partners includes a brief discussion of important considerations for evacuating people who have experienced IPV (DHS, 2019b). The guidance suggests that evacuation site managers post phone numbers for the National Domestic Violence Hotline and for local IPV/domestic violence (DV) shelters in visible places in emergency shelters. It also lists alternative accommodations for residents when an IPV/DV shelter must be evacuated, including other IPV/DV shelters, a safe home of a family member or friend, or time-limited placement in a motel or hotel (DHS, 2019b). The guidance encourages disaster planners to include IPV/DV shelter staff on planning teams. Of note, the guide also highlights the importance of ensuring the confidentiality of records from IPV/DV shelters to protect the safety of residents. However, it does not offer guidance to support shelters in that task (DHS, 2019b).
The Public Health Emergency Response Guide for State, Local, and Tribal Public Health Directors from the CDC is designed to provide guidance for the first 24 hours of an emergency (CDC, 2011). CDC’s most recent Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health, last updated in 2019, mentions the need to include community-based organizations in planning and the need to prioritize the development of behavioral health services for families (CDC, 2019). However, it does not explicitly address capabilities to support people experiencing IPV (CDC, 2019). Likewise, the most recent version of CDC’s Public Health Workbook to Define, Locate, and Reach Special, Vulnerable, and At-Risk Populations in an Emergency does not mention people experiencing IPV as an at-risk population (CDC, 2010).
The HHS Administration for Children and Families collaborated with ASPR to create a fact sheet for first responders about supporting pregnant people who have experienced IPV or sexual violence during disasters (HHS, 2017). The document identifies several unique needs for these individuals and provides contact information for national hotlines but has only limited
IPV-specific guidance. The fact sheet suggests that first responders refresh their training in case they need to deliver a baby; encourages them to facilitate private conversations with a nurse or advocate; and suggests that they promote access to continued clinical care, healthy foods and baby items, clean water and formula or breastfeeding supplies, and an emergency birth plan (HHS, 2017).
The HHS Maternal-Child Health Emergency Planning Toolkit notes the potential for increased IPV after an emergency. It emphasizes the need to ensure continuity of services and support to keep someone experiencing IPV separate from the person engaging in IPV (ASPR, 2021). The toolkit includes a recommendation that encourages first responders, health care professionals, and social service providers to use a trauma-informed approach for those they encounter who may have experienced “abuse” but does not explicitly refer to IPV (ASPR, 2021).
The National Resource Center on Domestic Violence’s online information center, VAWnet, includes a Disaster and Emergency Preparedness and Response collection.22 The majority of resources and information in the collection are targeted at informing and preparing domestic violence and sexual violence organizations for disasters. The collection includes a down-loadable participant guide for a 2014 course for disaster response workers (Sarabandi, 2018). The guide offers information about domestic violence (but does not mention IPV specifically), including the effect of disasters on people experiencing domestic violence, screening scripts, guidance for responding to disclosure, guidance for assessing the level of risk, and critical components and considerations for safety planning. It also includes a section that explains vicarious trauma, compassion fatigue, and burnout. That document was the most comprehensive discussion of domestic violence for first responders that our research identified. Of note, this document was found through a link on VAWnet. This website is familiar to those working in IPV care. However, it is not likely to be familiar to those outside the field, including emergency planners and health care practice administrators. This may be why committee members with disaster response expertise were unfamiliar with this document.
CHAPTER SUMMARY
PHE management and response is governed by an ecosystem of laws and agencies across federal and SLTT jurisdictions. Declared emergencies activate certain powers for officials, allow for modification of specific regulations, and make funding available to support response. Federal
___________________
22 https://vawnet.org/sc/disaster-and-emergency-preparedness-and-response (accessed June 30, 2023).
frameworks provide guidance for PHE planning and response and collaboration between federal and SLTT agencies and volunteer organizations active in disasters.
PHEs do not affect all people equally. Populations that experience health inequities are more likely to be disproportionately affected by PHEs. These populations are also more likely to be disproportionately affected by IPV. PHEs worsen the frequency and severity of IPV. Ensuring access to care and support services for IPV becomes even more critical during PHEs.
REFERENCES
Alexander, A. C., J. Ali, M. E. McDevitt-Murphy, D. R. Forde, M. Stockton, M. Read, and K. D. Ward. 2017. Racial differences in posttraumatic stress disorder vulnerability following Hurricane Katrina among a sample of adult cigarette smokers from New Orleans. J Racial Ethn Health Disparities 4(1):94-103.
Alexenko, N., J. Satinsky, and M. Simmons. n.d. Victim or survivor: Terminology from investigation through prosecution. https://sakitta.rti.org/toolkit/index.cfm?fuseaction=tool&tool=80 (accessed August 25, 2023).
Ali, J. S., A. S. Farrell, A. C. Alexander, D. R. Forde, M. Stockton, and K. D. Ward. 2017. Race differences in depression vulnerability following Hurricane Katrina. Psychol Trauma 9(3):317-324.
Anastario, M., N. Shehab, and L. Lawry. 2009. Increased gender-based violence among women internally displaced in Mississippi 2 years post-Hurricane Katrina. Disaster Med Public Health Prep 3(1):18-26.
ASPR (Administration for Strategic Preparedness and Response). n.d. ASPR program offices. https://aspr.hhs.gov/AboutASPR/ProgramOffices/Pages/ProgramOffice.aspx (accessed August 17, 2023).
ASPR. 2016. 2017-2022 health care preparedness and response capabilities. Edited by Office of the Assistant Secretary for Preparedness and Response. Rockville, Maryland: U.S. Department of Health and Human Services.
ASPR. 2021. HHS maternal-child health emergency planning toolkit, public health emergency. U.S. Department of Health and Human Services.
ASPR. 2021. Medical assistance. https://www.phe.gov/Preparedness/support/medicalassistance/Pages/default.aspx (accessed August 25, 2023).
ATDSR (Agency for Toxic Substances and Disease Registry). 2023. CDC/ATDSR social vulnerability index. https://www.atsdr.cdc.gov/placeandhealth/svi/index.html#:~:text=Social%20vulnerability%20refers%20to%20the,human%20suffering%20and%20economic%20loss (accessed August 25, 2023).
Avalos, L. A., G. T. Ray, S. E. Alexeeff, S. R. Adams, M. B. Does, C. Watson, and K. C. Young-Wolff. 2023. Association of the COVID-19 pandemic with unstable and/or unsafe living situations and intimate partner violence among pregnant individuals. JAMA Netw Open 6(2):e230172.
Bayntun, C. 2012. A health system approach to all-hazards disaster management: A systematic review. PLoS Curr 4:e50081cad55861d.
Beiter, K., E. Hayden, S. Phillippi, E. Conrad, and J. Hunt. 2021. Violent trauma as an indirect impact of the COVID-19 pandemic: A systematic review of hospital reported trauma. Am J Surg 222(5):922-932.
Bell, S. A., K. Klasa, T. J. Iwashyna, E. C. Norton, and M. A. Davis. 2020. Long-term healthcare provider availability following large-scale hurricanes: A difference-in-differences study. PLoS ONE 15(11):e0242823.
Bell, S. A., J. P. Donnelly, W. Li, and M. A. Davis. 2022. Hospitalizations for chronic conditions following hurricanes among older adults: A self-controlled case series analysis. J Am Geriatr Soc 70(6):1695-1703.
Bell, S. A., M. L. Miranda, J. P. W. Bynum, and M. A. Davis. 2023. Mortality after exposure to a hurricane among older adults living with dementia. JAMA Netw Open 6(3):e232043.
Bennett, L., S. Riger, P. Schewe, A. Howard, and S. Wasco. 2004. Effectiveness of hotline, advocacy, counseling, and shelter services for victims of domestic violence: A statewide evaluation. J Interpers Violence 19(7):815-829.
Berberian, A. G., D. J. X. Gonzalez, and L. J. Cushing. 2022. Racial disparities in climate change-related health effects in the United States. Curr Environ Health Rep 9(3):451-464.
Brabete, A. C., L. Wolfson, J. Stinson, N. Poole, S. Allen, and L. Greaves. 2021. Exploring the linkages between substance use, natural disasters, pandemics, and intimate partner violence against women: A rapid review in the context of COVID-19. Sexes 2(4):509-522.
Brown, H. L. 2021. Emergency care EMTALA alterations during the COVID-19 pandemic in the United States. J Emerg Nurs 47(2):321-325.
Brunkard, J., G. Namulanda, and R. Ratard. 2008. Hurricane Katrina deaths, Louisiana, 2005. Disaster Med Public Health Prep 2(4):215-223.
Campbell, J., and N. Glass. 2009. Safety planning, danger, and lethality assessment. In Intimate partner violence: A health-based perspective. New York, NY: Oxford University Press. Pp. 319-334.
Cao, J., S. G. Silva, M. Quizhpilema Rodriguez, Q. Li, A. M. Stafford, R. C. Cervantes, and R. M. Gonzalez-Guarda. 2023. Acculturation, acculturative stress, adverse childhood experiences, and intimate partner violence among Latinx immigrants in the US. J Interpers Violence 38(3-4):3711-3736.
Carney, J. R., L. E. Miller-Graff, T. R. Napier, and K. H. Howell. 2023. Elucidating the relations between adverse childhood experiences, age of exposure to adversity, and adult posttraumatic stress symptom severity in pregnant women. Child Abuse Negl 136:105995.
CDC (Centers for Disease Control and Prevention). 2010. Public health workbook to define, locate, and reach special, vulnerable, and at-risk populations in an emergency. Centers for Disease Control and Prevention.
CDC. 2011. Public health emergency response guide for state, local, and tribal public health directors version 2.0. U.S. Department of Health and Human Services.
CDC. 2019. Public health emergency preparedness and response capabilities: National standards for state, local, tribal, and territorial public health. U.S. Department of Health and Human Services.
CDC. 2020. Infographic: 6 guiding principles to a trauma-informed approach. https://www.cdc.gov/orr/infographics/6_principles_trauma_info.htm (accessed August 25, 2023).
CDC. 2022. About chronic diseases. https://www.cdc.gov/chronicdisease/about/index.htm (accessed September 6, 2023).
Cervantes, R. C., D. G. Fisher, A. M. Padilla, and L. E. Napper. 2016. The Hispanic stress inventory version 2: Improving the assessment of acculturation stress. Psychol Assess 28(5):509-522.
CMS (Centers for Medicare & Medicaid Services). 2016. Emergency preparedness requirements for Medicare and Medicaid participating providers and suppliers. Federal Register 81(180):63859-64044.
CMS. 2017. Frequently asked questions (FAQs): Emergency preparedness regulation. Centers for Medicare & Medicaid Services.
COVIDSurg Collaborative. 2020. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br J Surg 107(11):1440-1449.
Davis, M., O. Gilbar, and D. M. Padilla-Medina. 2021. Intimate partner violence victimization and perpetration among U.S. adults during the earliest stage of the COVID-19 pandemic. Violence Vict 36(5):583-603.
DHS (Department of Homeland Security). 2015. National preparedness goal. 2nd ed. Washington, DC: Federal Emergency Management Agency.
DHS. 2016. National disaster recovery framework. 2nd ed. Washington, DC: Federal Emergency Management Agency.
DHS. 2019a. National response framework. 4th ed. Washington, DC: Federal Emergency Management Agency.
DHS. 2019b. Planning considerations: Evacuation and shelter-in-place: Guidance for state, local, tribal, and territorial partners. Washington, DC: Federal Emergency Management Agency.
DiMaggio, C., E. Susser, S. Frangos, D. Abramson, H. Andrews, C. Hoven, M. Ryan, and G. Li. 2023. The New York state COVID-19 healthcare personnel study: One-year followup of physicians, nurse practitioners, and physician assistants, 2020-2021. Public Health Rep 138(3):518-525.
Disney, L., J. Koo, S. Carnes, and L. Warner. 2022. Essential but excluded: Using critical race theory to examine COVID-19 economic relief policies for undocumented US workers. J Hum Rights Soc Work 7(3):225-235.
EMAC (Emergency Management Assistance Compact). 2023. What is EMAC? https://www.emacweb.org/index.php/learn-about-emac/what-is-emac (accessed February 3, 2023).
Evans, M. L., M. Lindauer, and M. E. Farrell. 2020. A pandemic within a pandemic—intimate partner violence during COVID-19. N Engl J Med 383(24):2302-2304.
FEMA (Federal Emergency Management Agency). 2011. A whole community approach to emergency management: Principles, themes, and pathways for action. Washington, DC: U.S. Department of Homeland Security.
FEMA. 2017. National incident management system. https://www.fema.gov/emergencymanagers/nims (accessed August 25, 2023).
FEMA. 2020. FEMA tribal policy (rev. 2). Washington, DC: U.S. Department of Homeland Security.
FEMA. 2021. Developing and maintaining emergency operations plans: Comprehensive preparedness guide 101 version 3.0. Washington, DC: U.S. Department of Homeland Security.
FEMA. 2023a. Community lifelines fact sheet. Washington, DC: U.S. Department of Homeland Security.
FEMA. 2023b. Community lifelines implementation toolkit version 2.1. Washington, DC: U.S. Department of Homeland Security.
Ferreira, R. J., F. Buttell, and K. Elmhurst. 2018. The deepwater horizon oil spill: Resilience and growth in the aftermath of postdisaster intimate partner violence. Journal of Family Social Work 21(1):22-44.
Flores, A. B., T. W. Collins, S. E. Grineski, and J. Chakraborty. 2020. Disparities in health effects and access to health care among Houston area residents after Hurricane Harvey. Public Health Rep 135(4):511-523.
Fothergill, A., E. G. Maestas, and J. D. Darlington. 1999. Race, ethnicity and disasters in the United States: A review of the literature. Disasters 23(2):156-173.
Garcia, R., C. Henderson, K. Randell, A. Villaveces, A. Katz, F. Abioye, S. DeGue, K. Premo, S. Miller-Wallfish, J. C. Chang, E. Miller, and M. I. Ragavan. 2022. The impact of the COVID-19 pandemic on intimate partner violence advocates and agencies. J Fam Violence 37(6):893-906.
Genovesi, A. L., B. Hastings, E. A. Edgerton, and L. M. Olson. 2014. Pediatric emergency care capabilities of Indian health service emergency medical service agencies serving American Indians/Alaska Natives in rural and frontier areas. Rural Remote Health 14(2):2688.
Gilmore, B., R. Ndejjo, A. Tchetchia, V. de Claro, E. Mago, A. A. Diallo, C. Lopes, and S. Bhattacharyya. 2020. Community engagement for COVID-19 prevention and control: A rapid evidence synthesis. BMJ Glob Health 5(10).
Gilroy, H., J. McFarlane, J. Maddoux, and C. Sullivan. 2016. Homelessness, housing instability, intimate partner violence, mental health, and functioning: A multi-year cohort study of IPV survivors and their children. Journal of Social Distress and the Homeless 25(2):86-94.
Goessmann, K., H. Ibrahim, L. B. Saupe, A. A. Ismail, and F. Neuner. 2019. The contribution of mental health and gender attitudes to intimate partner violence in the context of war and displacement: Evidence from a multi-informant couple survey in Iraq. Soc Sci Med 237:112457.
GOHSEP (Governor’s Office of Homeland Security and Emergency Preparedness). 2023. IMAC and EMAC. https://gohsep.la.gov/RESPOND/REQUEST-RESOURCES/IMACEMAC#:~:text=Mission%20Ready%20Packages%20(MRPs)%20are,can%20help%20make%20this%20happen (accessed August 25, 2023).
Golding, J. M. 1999. Intimate partner violence as a risk factor for mental disorders: A meta-analysis. Journal of Family Violence 14(2):99-132.
Gonzalez-Guarda, R. M., J. Williams, D. Lorenzo, and C. Carrington. 2021. Desired characteristics of HIV testing and counseling among diverse survivors of intimate partner violence receiving social services. Health Soc Work 46(2):93-101.
Gosangi, B., H. Park, R. Thomas, R. Gujrathi, C. P. Bay, A. S. Raja, S. E. Seltzer, M. C. Balcom, M. L. McDonald, D. P. Orgill, M. B. Harris, G. W. Boland, K. Rexrode, and B. Khurana. 2021. Exacerbation of physical intimate partner violence during COVID-19 pandemic. Radiology 298(1):E38-E45.
Gupta, A., and S. Aviva. 2020. For abused women, a pandemic lockdown holds dangers of its own. New York Times, March 24 (updated October 8, 2021). https://www.nytimes.com/2020/03/24/us/coronavirus-lockdown-domestic-violence.html (accessed August 25, 2023).
Harville, E. W., C. A. Taylor, H. Tesfai, X. Xu, and P. Buekens. 2011. Experience of Hurricane Katrina and reported intimate partner violence. J Interpers Violence 26(4):833-845.
Hendrickson, R. C., R. A. Slevin, K. D. Hoerster, B. P. Chang, E. Sano, C. A. McCall, G. R. Monty, R. G. Thomas, and M. A. Raskind. 2022. The impact of the COVID-19 pandemic on mental health, occupational functioning, and professional retention among health care workers and first responders. J Gen Intern Med 37(2):397-408.
Henke, A., and L.-c. Hsu. 2020. The gender wage gap, weather, and intimate partner violence. Review of Economics of the Household 18(2):413-429.
Hershey, T. B. 2019. Collaborating with sovereign tribal nations to legally prepare for public health emergencies. J Law Med Ethics 47(2_suppl):55-58.
HHS (U.S Department of Health and Human Services). 2017. First responders: Support for pregnant survivors of abuse or rape during disasters. https://asprtracie.hhs.gov/MasterSearch?qt=support+for+pregnant+survivors+of+abuse (accessed August 25, 2023).
Holland, K. M., C. Jones, A. M. Vivolo-Kantor, N. Idaikkadar, M. Zwald, B. Hoots, E. Yard, A. D’Inverno, E. Swedo, M. S. Chen, E. Petrosky, A. Board, P. Martinez, D. M. Stone, R. Law, M. A. Coletta, J. Adjemian, C. Thomas, R. W. Puddy, G. Peacock, N. F. Dowling, and D. Houry. 2021. Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID-19 pandemic. JAMA Psychiatry 78(4):372-379.
IFRC (International Federation of Red Cross and Red Crescent Societies). 2023. What is a disaster. https://www.ifrc.org/our-work/disasters-climate-and-crises/what-disaster#:~:text=Disasters%20are%20serious%20disruptions%20to,and%20\vulnerability%20of%20a%20community (accessed August 27, 2023).
IHS (Indian Health Service). n.d. Agency overview. https://www.ihs.gov/aboutihs/overview/ (accessed August 21, 2023).
IHS. 2017. Indian health manual. Rockville, Maryland: U.S. Department of Health and Human Services.
IOM (Institute of Medicine). 2015. Healthy, resilient, and sustainable communities after disasters: Strategies, opportunities, and planning for recovery. Washington, DC: The National Academies Press.
Jetelina, K. K., G. Knell, and R. J. Molsberry. 2021. Changes in intimate partner violence during the early stages of the COVID-19 pandemic in the USA. Inj Prev 27(1):93-97.
KFF. 2023. Health coverage and care of immigrants. https://www.kff.org/racial-equity-andhealth-policy/fact-sheet/health-coverage-and-care-of-immigrants/ (accessed September 6, 2023).
Khatana, S. A. M., R. M. Werner, and P. W. Groeneveld. 2022. Association of extreme heat and cardiovascular mortality in the United States: A county-level longitudinal analysis from 2008 to 2017. Circulation 146(3):249-261.
Kim, C. 2019. Social isolation, acculturative stress and intimate partner violence (IPV) victimization among Korean immigrant women. International Journal of Intercultural Relations 72:87-95.
Krause, K. H., S. DeGue, G. Kilmer, and P. H. Niolon. 2023. Prevalence and correlates of non-dating sexual violence, sexual dating violence, and physical dating violence victimization among US high school students during the COVID-19 pandemic: Adolescent behaviors and experiences survey, United States, 2021. Journal of Interpersonal Violence 38(9-10):6961-6984.
Lai, B. S., R. Lewis, M. S. Livings, A. M. La Greca, and A. M. Esnard. 2017. Posttraumatic stress symptom trajectories among children after disaster exposure: A review. J Trauma Stress 30(6):571-582.
Lauve-Moon, K., and R. J. Ferreira. 2017. An exploratory investigation: Post-disaster predictors of intimate partner violence. Clinical Social Work Journal 45(2):124-135.
Le, K., and M. Nguyen. 2022. War and intimate partner violence in Africa. SAGE Open 12(2):21582440221096427.
Leite, R. O., V. Pavia, M. A. Kobayashi, T. Kyoung Lee, G. Prado, S. E. Messiah, and S. M. St. George. 2023. The effects of parent-adolescent acculturation gaps on adolescent lifestyle behaviors: Moderating role of family communication. J Lat Psychol 11(1):21-39.
Lightfoot, E. S., A. E. Lesen, and R. J. Ferreira. 2020. Gender and resilience in gulf coast communities: Risk and protective factors following a technological disaster. International Journal of Disaster Risk Reduction 50:101716.
Lindsey, A. B., M. Donovan, S. Smith, H. Radunovich, and M. Gutter. 2021. Impacts of technological disasters. IFAS Extension. University of Florida. https://edis.ifas.ufl.edu/publication/FY1230 (accessed August 25, 2023).
Longmuir, C., and V. I. O. Agyapong. 2021. Social and mental health impact of nuclear disaster in survivors: A narrative review. Behav Sci (Basel) 11(8):113.
Ma, C., T. E. Smith, and R. R. Iversen. 2021. Mental illness prevalence and disparities among Hurricane Sandy survivors: A 2-year retrospective. Disaster Med Public Health Prep 15(5):579-588.
Michaud, J., and J. Kates. 2017. Public health in Puerto Rico after Hurricane Maria. KFF Issue Briefs, November 17. https://www.kff.org/mental-health/issue-brief/public-healthin-puerto-rico-after-hurricane-maria/ (accessed August 25, 2023).
Muldoon, K. A., K. M. Denize, R. Talarico, D. B. Fell, A. Sobiesiak, M. Heimerl, and K. Sampsel. 2021. COVID-19 pandemic and violence: Rising risks and decreasing urgent care-seeking for sexual assault and domestic violence survivors. BMC Med 19(1):20.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. Building and measuring community resilience: Actions for communities and the Gulf Research Program. Washington, DC: The National Academies Press.
NASEM. 2020. Rapid expert consultation on understanding causes of health care worker deaths due to the COVID-19 pandemic (December 10, 2020). Washington, DC: The National Academies Press.
NCDP (National Center for Disaster Preparedness). 2023. US Natural Hazards Index v2.0. https://ncdp.columbia.edu/library/mapsmapping-projects/us-natural-hazards-index/ (accessed August 25, 2023).
Osofsky, H. J., J. D. Osofsky, and T. C. Hansel. 2011. Deepwater horizon oil spill: Mental health effects on residents in heavily affected areas. Disaster Med Public Health Prep 5(4):280-286.
Parson, N., R. Escobar, M. Merced, and A. Trautwein. 2016. Health at the intersections of precarious documentation status and gender-based partner violence. Violence Against Women 22(1):17-40.
Peitzmeier, S. M., L. Fedina, L. Ashwell, T. I. Herrenkohl, and R. Tolman. 2022. Increases in intimate partner violence during COVID-19: Prevalence and correlates. J Interpers Violence 37(21-22):NP20482-NP20512.
Ragavan, M. I., A. J. Culyba, F. L. Muhammad, and E. Miller. 2020a. Supporting adolescents and young adults exposed to or experiencing violence during the COVID-19 pandemic. J Adolesc Health 67(1):18-20.
Ragavan, M. I., R. Garcia, R. P. Berger, and E. Miller. 2020b. Supporting intimate partner violence survivors and their children during the COVID-19 pandemic. Pediatrics 146(3).
Ragavan, M. I., L. Risser, V. Duplessis, S. DeGue, A. Villaveces, T. P. Hurley, J. Chang, E. Miller, and K. A. Randell. 2022. The impact of the COVID-19 pandemic on the needs and lived experiences of intimate partner violence survivors in the United States: Advocate perspectives. Violence Against Women 28(12-13):3114-3134.
Raker, E. J., M. C. Arcaya, S. R. Lowe, M. Zacher, J. Rhodes, and M. C. Waters. 2020. Mitigating health disparities after natural disasters: Lessons from the risk project. Health Aff (Millwood) 39(12):2128-2135.
Renov, V., L. Risser, R. Berger, T. Hurley, A. Villaveces, S. DeGue, A. Katz, C. Henderson, K. Premo, J. Talis, J. C. Chang, and M. Ragavan. 2022. The impact of the COVID-19 pandemic on child protective services caseworkers and administrators. Child Abuse Negl 130(Pt 1):105431.
Ricks, J. L., S. D. Cochran, O. A. Arah, J. K. Williams, and T. E. Seeman. 2016. Food insecurity and intimate partner violence against women: Results from the California women’s health survey. Public Health Nutr 19(5):914-923.
Rossi, F. S., M. Shankar, K. Buckholdt, Y. Bailey, S. T. Israni, and K. M. Iverson. 2020. Trying times and trying out solutions: Intimate partner violence screening and support for women veterans during COVID-19. J Gen Intern Med 35(9):2728-2731.
Rotton, J., and E. G. Cohn. 2001. Temperature, routine activities, and domestic violence: A reanalysis. Violence Vict 16(2):203-215.
Rubin, G. J., and M. B. Rogers. 2019. Behavioural and psychological responses of the public during a major power outage: A literature review. International Journal of Disaster Risk Reduction 38:101226.
Rung, A. L., S. Gaston, E. Oral, W. T. Robinson, E. Fontham, D. J. Harrington, E. Trapido, and E. S. Peters. 2016. Depression, mental distress, and domestic conflict among Louisiana women exposed to the Deepwater Horizon oil spill in the watch study. Environ Health Perspect 124(9):1429-1435.
Rutkow, L., J. S. Vernick, R. Mojtabai, S. O. Rodman, and C. N. Kaufmann. 2012. Legal challenges for substance abuse treatment during disasters. Psychiatric Services 63(1):1-9.
Sanz-Barbero, B., C. Linares, C. Vives-Cases, J. L. Gonzalez, J. J. Lopez-Ossorio, and J. Diaz. 2018. Heat wave and the risk of intimate partner violence. Sci Total Environ 644:413-419.
Sarabandi, N. 2018. Curriculum: Intersection of domestic violence and natural disasters. https://nnedv.org/resources-library/curriculum-intersection-domestic-violence-naturaldisasters/ (accessed February 15, 2023).
Sharpe, J. D., and A. F. Wolkin. 2022. The epidemiology and geographic patterns of natural disaster and extreme weather mortality by race and ethnicity, United States, 1999-2018. Public Health Rep 137(6):1118-1125.
Smith, R. N., A. Nyame-Mireku, A. Zeidan, A. Tabaie, C. Meyer, V. Muralidharan, R. Kamaleswaran, K. Williams, A. Grant, J. Nguyen, S. Hurst, D. Hanos, E. Benjamin, R. Sola, Jr., and D. P. Evans. 2022. Intimate partner violence at a level-1 trauma center during the COVID-19 pandemic: An interrupted time series analysis. Am Surg 88(7):1551-1553.
Stults, C. B., K. D. Krause, R. J. Martino, M. Griffin, C. E. LoSchiavo, S. G. Lynn, S. A. Brandt, D. Tan, N. Horne, G. Lee, J. Wong, and P. N. Halkitis. 2022. Sociodemographic characteristics, depressive symptoms, and increased frequency of intimate partner violence among LGBTQ people in the United States during the COVID-19 pandemic: A brief report. Journal of Gay & Lesbian Social Services 35(2):258-270.
Sullivan, C. M. 2012. Domestic violence shelter services: A review of the empirical evidence. Domestic Violence Evidence Project. https://www.dvevidenceproject.org/wp-content/themes/DVEProject/files/research/DVShelterResearchSummary10-2012.pdf.
Tur-Prats, A. 2021. Unemployment and intimate partner violence: A cultural approach. Journal of Economic Behavior & Organization 185:27-49.
USPHS (U.S. Public Health Service). 2022. Public health emergency response strike team. https://www.usphs.gov/pherst (accessed August 25, 2023).
VA (Veterans Affairs Office of Emergency Management). 2021. Comprehensive emergency management program. https://www.va.gov/VHAEMERGENCYMANAGEMENT/CEMP/index.asp (accessed August 25, 2023).
Valdovinos, M. G., S. D. Nightingale, and M. Vasquez Reyes. 2021. Intimate partner violence help-seeking for Latina undocumented immigrant survivors: Feminist intersectional experiences narrated through testimonio. Affilia 36(4):533-551.
Vida, S., M. Durocher, T. B. M. J. Ouarda, and P. Gosselin. 2012. Relationship between ambient temperature and humidity and visits to mental health emergency departments in Québec. Psychiatric Services 63(11):1150-1153.
Weiner, D. L., and S. L. Rosman. 2019. Just-in-time training for disaster response in the austere environment. Clinical Pediatric Emergency Medicine 20(2):95-110.
Weitzman, A., and J. A. Behrman. 2016. Disaster, disruption to family life, and intimate partner violence: The case of the 2010 earthquake in Haiti. Sociological Science 3:167-189.
West Region Health Care Coalition. 2023. History of health care coalitions. https://www.westregionhcc.com/firm-history (accessed August 25, 2023).
WHO (World Health Organization). 2009. Whole of society pandemic readiness: WHO guidelines for pandemic preparedness and response in the non-health sector. Geneva, Switzerland: WHO Press.
Williams, J. R., R. M. Gonzalez-Guarda, and V. Ilias. 2017. Trauma-informed decision-making among providers and victims of intimate partner violence during HIV testing: A qualitative study. J Assoc Nurses AIDS Care 28(5):819-831.
This page intentionally left blank.




































