
1
Introduction
BACKGROUND
Women’s well-being and safety are often disproportionately negatively affected during disasters and public health emergencies (PHEs) (Thurston et al., 2021). International and domestic studies have reported that violence against women increases in the context of PHEs and disasters (Thurston et al., 2021). Multiple studies conducted in the United States after Hurricane Katrina, after the Deepwater Horizon oil spill, and throughout the COVID-19 pandemic have found increases in the prevalence and severity of intimate partner violence (IPV) against women in the aftermath of these events (First et al., 2017; Lauve-Moon and Ferreira, 2016; Viero et al., 2021). Women who experience IPV during a disaster or PHE are exposed to physical and psychological trauma due to IPV in addition to traumas from the PHE. With this in mind, the Health Resources and Services Administration’s (HRSA’s) Office of Women’s Health (OWH) identified a need to identify, highlight, and describe essential health care services related to IPV that should be prioritized and made available during PHEs. Thus, HRSA’s OWH contracted with the National Academies of Sciences, Engineering, and Medicine’s Health and Medicine Division to convene an expert multidisciplinary panel of 14 members to address the statement of work (see Box 1-1) and produce a report with recommendations and conclusions within an 18-month timeframe. The committee on Sustaining Essential Health Care Services Related to Intimate Partner Violence During Public Health Emergencies was formed and convened four in-person meetings and four virtual meetings in response to HRSA’s request.
BOX 1-1
Statement of Task and Charge to the Committee
An ad hoc committee of the National Academies of Sciences, Engineering, and Medicine shall develop a conceptual framework for delivering essential preventive and primary health care services related to Intimate Partner Violence (IPV) during public health emergencies (PHEs), using an all-hazards approach. The committee’s framework shall:
- Identify essential health care services related to IPV in non-PHEs (steady state) based on currently available evidence;
- Define essential health care services related to IPV in PHEs based on currently available evidence;
- Identify ways to prepare for and prioritize the provision of essential health care services related to IPV before PHEs;
- Describe health disparities related to IPV in PHEs;
- Identify innovations and best practices to prepare for and operationalize the equitable delivery of essential health care services related to IPV during PHEs;
- Identify promising practices in the prevention of IPV; and
- Develop strategies to overcome barriers faced by HRSA-supported and safety-net care settings in providing essential health care services related to IPV during PHEs, particularly for underserved populations.
STUDY APPROACH AND SCOPE
Defining Intimate Partner Violence
The committee adopted the Centers for Disease Control and Prevention’s (CDC’s) definition of intimate partner violence as abuse or aggression committed by a current or former intimate partner (Breiding et al., 2015). An intimate partner is a person with whom one has a close romantic and consensual physically intimate relationship and is characterized by regular interaction. IPV can include, but is not limited to, physical violence, sexual violence, stalking, psychological aggression, and reproductive coercion (ACOG, 2012; CDC, 2022). Physical violence or physical IPV refers to the intentional use of physical force to inflict injury (Breiding et al., 2015). Examples include but are not limited to pushing, grabbing, choking, hair pulling, the use of a weapon, the use of restraints, or coercing others to
commit such acts (Breiding et al., 2015). Sexual violence or sexual IPV refers to forcing a partner to take part in a sexual act without his or her consent or when the partner is not able to freely give consent and includes drug- or alcohol-facilitated acts and non-physical acts (Breiding et al., 2015). Some examples are forced sexual touching, rape, sexual coercion, sexting, or forcing sexual contact with a third party. Stalking is a pattern of repeated behavior that involves unsought attention and contact by a current or former intimate partner that creates a sense of fear for one’s safety or that of someone with a close relationship to the victim (Breiding et al., 2015). Some examples are following or repetitive phone calls or text messages. Psychological aggression or psychological IPV refers to using verbal and non-verbal communication to intentionally harm a partner mentally or emotionally or to wield control over a partner (ACOG, 2012; Breiding et al., 2015; CDC, 2022). Some examples include name-calling, isolation, degradation, reproductive coercion, or intentional deprivation of resources such as food, medication, health care, or economic resources. Psychological IPV often co-occurs with other forms of IPV. Reproductive coercion refers to actions that exert control over a partner’s reproductive health and can occur in the absence of physical or sexual violence (ACOG, 2012). Some examples include contraception sabotage, refusal to practice safe sex, forced pregnancy, forced pregnancy termination (either through forced abortion or infliction of injury with the intent to cause a miscarriage), and controlling access to reproductive health services (ACOG, 2012).
IPV is different from domestic violence (DV). DV is a broader category that refers to abuse or aggression committed by a family member or member of a household against another family member or member of a household (Merriam-Webster, 2023). DV may include IPV, but it also includes child abuse, elder abuse, and abuse or aggression between other family members or household members. Some organizations, researchers, reporting bodies, and legal jurisdictions use IPV and DV interchangeably, which can create challenges in interpreting data and research findings. The committee considered research and data specific to IPV. It only included references and data that referred to DV for consideration if the source’s definition of DV was limited to abuse and aggression between current or former intimate partners.
IPV should not be confused with interpersonal violence. Interpersonal violence is the intentional use of violence or aggression by an individual or small group of individuals against another individual or small group (Mercy et al., 2017).
Study Scope
The experience of IPV is not limited to women. However, to remain consistent with the guidance from the study sponsor, the committee limited
its focus to women (see next section for the committee’s definition of women) over the age of 13 who directly experience IPV. Additionally, consideration of health care services for individuals who engage in IPV, beyond those specifically addressed in prevention strategies, is beyond the scope of this study. The committee acknowledges that IPV is also directed at men, including transgender men, and there is a growing body of research into the effects of experiencing IPV on men. However, health care interventions specifically for men experiencing IPV are also beyond the scope of the study. Additionally, while elder abuse and child abuse are significant issues that can intersect with IPV, these issues also fall outside of the parameters of the statement of task. Undoubtedly, the pediatric health care setting represents a point of contact with the health care system for parents or adolescents to disclose that they are experiencing IPV (Randell and Ragavan, 2020). However, services for children witnessing IPV are beyond the scope of the statement of task. Of note, several studies have identified a parent’s concern about the safety of their children or losing custody of their children as a frequently reported barrier to IPV disclosure (Heron and Eisma, 2021). The committee considers essential health care services for the parent or caregiver experiencing IPV that reduce barriers to disclosure and IPV care by supporting the safety of their child or children. The committee also considers IPV in relationships among adolescents as detailed in the chapters that follow.
The committee acknowledges that the complex nature of addressing IPV may necessitate a broad array of supports and strategies to address the many effects of IPV as well as its root causes. However, the scope of this study is limited to health care services, which are defined later in this chapter. As such, when considering essential health care services for IPV, the committee limited its consideration to IPV care that is delivered in or referrable from a health care setting. The committee did consider a specific group of support services that are directed at protecting the immediate health and safety of women experiencing IPV and that often serve as an initial point of contact for women to access IPV-related care, including health care.
Women
The committee used an inclusive approach to define woman/women as the population of interest in this report. For the purpose of this report, woman/women encompass cisgender women, transgender women, and people whose gender identity is not exclusively male who are non-binary or otherwise gender expansive. This is a modified version of the approach used by the HRSA-funded Women’s Preventive Services Initiative (WPSI) (WPSI, 2022). The committee emphasizes that inclusion of people who are gender non-binary or otherwise gender expansive as part of the population they refer to when using the word woman throughout this report is done
with the intent of being inclusive of individuals whose gender identity is not exclusively male and not with the intent of disregarding the gender identity of those who are gender non-binary or otherwise gender expansive. Unfortunately, there is very little research in the literature about IPV in the gender non-binary or otherwise gender expansive population. This limited the frequency with which this population could be discussed specifically when discussing the research evidence throughout the report.
The Committee’s Approach
The committee conducted an extensive review of the literature pertaining to IPV and PHEs. This review included websites maintained by such organizations as the World Health Organization (WHO), United Nations, Futures Without Violence, National Resource Center on Domestic Violence, and multiple pertinent state and federal agencies. Committee members and project staff identified additional salient literature and information using traditional academic research methods and online searches throughout the course of the study. The committee also drew on information gleaned from presentations given by experts in the health effects of IPV; IPV in lesbian, gay, bisexual, transgender, and queer populations; IPV care delivery in American Indian and Alaska Native populations; individuals with lived experience of IPV; and individuals with lived experience providing IPV care during PHEs.
Conceptual Framework
The statement of task identified the value of an overarching conceptual framework to guide the committee’s process for identifying essential health care services related to intimate partner violence. The committee selected the Social Ecological Model (SEM) as the conceptual framework to guide their understanding of the health care needs of women experiencing IPV and to identify the essential health care services related to IPV (see Figure 1-1) (Bronfenbrenner, 1977; McLeroy et al., 1988). The model has been widely applied to public health and clinical health care services challenges, including IPV and public health disaster response (Bell et al., 2021; Di Napoli et al., 2019; Nyambe et al., 2016). The committee considered the effect of factors consistent with the scope of the study at each level of the SEM on the health care needs of women experiencing IPV and the essential health care services to address those needs.
Health care services are delivered in multiple settings within the health care system as well as in community settings outside of a defined health care system (Aday and Andersen, 1974). In some cases, people experiencing IPV may be referred to community-based care from the traditional health care
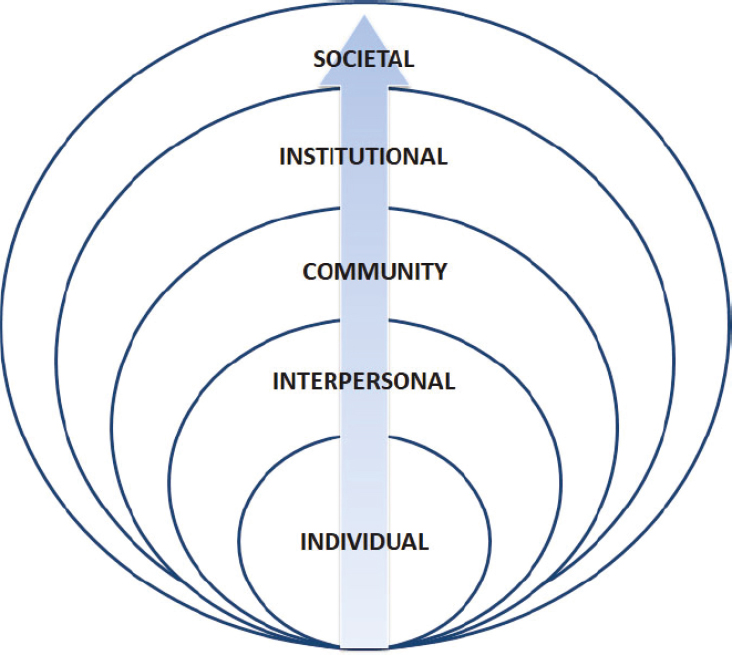
SOURCE: Concept from McLeroy et al., 1988. Figure adapted from NASEM report Getting to Zero Alcohol-Impaired Driving Fatalities: A Comprehensive Approach to a Persistent Problem (2018).
setting. In other cases, these community-based settings may be the initial site of care. The committee appreciates the value and interdependence of connections between the health care system and community-based care settings. The importance of these connections is further developed in the Care Coordination Model, which emphasizes high-quality referrals and transitions to outside resources for clinicians and patients (Wagner et al., 2014). Therefore, while this report is focused on health care services, the committee felt that it was important to acknowledge the role of community-based organizations in IPV-related care and emphasize the importance of warm referrals to that care.1
___________________
1 Warm referrals, or warm handoffs, are transfers of care between members of a health care team that occur with the patient’s permission, often with an in-person introduction. This approach can also be used when referring a patient to community-based services.
Determination Criteria for Essential Health Care Services for Intimate Partner Violence
The committee’s process for identifying essential health care services related to IPV was informed by an extensive review of evidence from several literature searches; recommendations from the U.S. Preventive Services Task Force (USPSTF), WPSI, and WHO; and insight gleaned from presentations to the committee by experts in IPV-related care. The committee notes that not all essential health care services related to IPV are delivered within the health care system or by clinicians. The committee identified the following criteria for essential health care services related to IPV:
- Evidence-based health care services that address the most common and most serious health outcomes related to experiencing IPV;
- Preventive services recommended by USPSTF and WPSI; and
- Specific support services required to meet the basic safety and housing needs of people experiencing IPV.
The committee recognizes that some of the essential health care services identified may currently be unavailable due to state-level restrictions placed on reproductive health care services and federal restrictions that may apply to the use of federal funding for such services. However, significant scientific evidence of increased risk for negative maternal and fetal health outcomes, including death, as well as elevated risk for increased severity or frequency of IPV and intimate partner homicide in the perinatal period support their inclusion (Black, 2011; D’Angelo et al., 2022; Dillon et al., 2013; Liu et al., 2016; Nelson et al., 2022; Roberts et al., 2014; Smith et al., 2023; Stubbs and Szoeke, 2022; Vicard-Olagne et al., 2022). These risks are discussed in further detail in Chapter 4 of the report.
Research Considerations
Evaluating studies of the effectiveness of IPV interventions requires understanding the complexities of conducting this type of research. In biomedical science and health care research, evidence is typically evaluated using hierarchical levels based on the inherent biases of specific study designs (Burns et al., 2011). While multiple classification systems exist, they consistently rank randomized controlled trials (RCTs) and systematic reviews of RCTs as the highest level of evidence and expert opinion and case series as the lowest (Burns et al., 2011). The quality (internal validity or risk of bias) of intervention studies is evaluated using criteria based on the study design components of RCTs, such as randomization, blinding, selection of appropriate measurements, control of confounding variables, and
loss to follow-up (Balshem et al., 2011; Higgins et al., 2023). These criteria apply primarily to interventions conducted in controlled settings where an intervention has low variance, such as drug trials. These criteria are not relevant to interventions that are ethically or operationally inappropriate for randomization, blinding, and other conditions of drug trials (Walshe, 2007). Most interventions for IPV fit into this latter group.
The committee understood several important challenges in conducting high-quality studies of IPV interventions. This research has been characterized as methodologically limited due to inconsistent randomization, inadequate control groups, no blinding, lack of long-term follow-up, or insufficient outcome measures (Zink and Putnam, 2005). Several issues specific to IPV research underlie these limitations.
First, the experience of IPV incorporates multiple confounding variables that can obscure the treatment effect of an IPV intervention (O’Campo et al., 2011). The most recent National Intimate Partner and Sexual Violence Survey results estimate that 63.3 percent of women had concerns for their safety during their lifetime because of IPV (Leemis et al., 2022). These issues differ for each individual and are often unanticipated and beyond their control. People experiencing IPV navigate complex and evolving circumstances related to their safety when they disclose IPV and seek care (Zink and Putnam, 2005). A study participant may experience a change in her or his safety during the study, requiring services that differ from the intervention to which the participant was randomized. Failure to modify the intervention would pose an unethical risk to the participant’s safety (Zink and Putnam, 2005). Moreover, people experiencing IPV may need to relocate for their safety, which disrupts the administration of the intervention, long-term follow-up, and outcome measurement.
IPV intervention studies rely on self-reported, unverified predictors (disclosure) and outcome variables that lack standardization (Zink and Putnam, 2005). Since many individuals experiencing IPV do not disclose when first asked, the IPV status of study participants may be inaccurate (Korab-Chandler et al., 2022). Study outcomes may also be inaccurate, particularly when participants are concerned about the legal or social repercussions of ongoing or escalating IPV. Additional attempts to verify IPV status and outcome data could violate confidentiality and cause harm (Zink and Putnam, 2005).
In most IPV intervention studies, the control group is provided with usual or alternate care for ethical reasons. However, these non-interventions could increase participants’ awareness of IPV, affect their use of services, and influence trial outcomes by creating a Hawthorne effect (i.e., the phenomenon that study participants change their behavior because of being involved in the study; see Franke and Kaul, 1978) (Nelson et al., 2012). As a result, differences between intervention and control groups may be diminished, and the effectiveness of the intervention may be underestimated.
The committee kept these challenges in mind throughout their consideration of the research evidence. Much of the research into effectiveness of different interventions for IPV had mixed results that were confounded by the variables discussed above. This limited the number of interventions that the committee could describe as effective based on the research evidence. However, the committee was able to identify several care models that it considered promising based on the committee’s expert opinion and their review of the evidence. Those are discussed in Chapters 5 and 7 of this report.
Guiding Principles
Person-First Language
The committee acknowledges that stigma creates barriers to care, and language contributes to stigma. The Veterans Health Administration’s Intimate Partner Violence Assistance Program uses person-first language as part of its approach to reducing the stigma associated with IPV (VA, 2021). Throughout this report, the terms woman or women or person or people experiencing IPV will be used instead of victim or battered spouse, and the term person or people engaging in IPV will be used instead of batterer or perpetrator.
Health Equity, Health Disparities, and Resilience
The committee sought to center health equity in developing a framework for delivering essential health care services related to IPV during PHEs. In the article “Systems of Power, Axes of Inequity: Parallels, Intersections, Braiding the Strands,” Camara P. Jones offers this description of health equity: “Health equity is assurance of the conditions for optimal health for all people. Achieving health equity requires valuing all individuals and populations equally, recognizing and rectifying historical injustices, and providing resources according to need. Health disparities will be eliminated when health equity is achieved” (Jones, 2014, p. S74). Populations adversely affected by health disparities include racially and ethnically minoritized populations, people with low incomes, populations residing in underserved rural areas, and sexual and gender minoritized populations (NIMHD, 2023).2 Some of these populations have been historically marginalized through discriminatory policies and systems that have led to intergenerational trauma, which may exacerbate health disparities. Many underserved communities lack access to quality health care services,
___________________
2 The term minoritized refers to the active marginalization of certain groups into minority status, as well as what that status has historically entailed.
including perinatal health care, perpetuating health disparities (Brigance, 2022). The committee acknowledges that the health care services identified as essential during steady state and PHE conditions are substantially less accessible or inaccessible in underserved communities (Frakt, 2019). These underserved communities often experience a lack of access to health care services during steady state conditions which resembles the lack of access encountered by wealthier, better resourced communities during disasters (Topchik et al., 2021).
Inadequate access to health care services is one of many factors that affect community resilience, or its ability to maintain its essential functions despite shocks or stressors, such as PHEs (Clark-Ginsberg et al., 2020). In public health, the evaluation of community resilience is frequently focused on using defined neighborhood characteristics to describe factors such as vulnerability or social capital, with improving resilience being defined as a positive outcome. However, these evaluations can overlook the adverse effects of the interdependence of neighborhoods that occur during disasters. The COVID-19 pandemic provided an example of the negative effect of this interdependence. During the pandemic, essential workers continued to work, frequently outside of their neighborhoods, providing services for those who could work from home in more affluent neighborhoods (Hong et al., 2021). Essential workers and the less affluent neighborhoods where they lived bore a heavier contagion rate than those more affluent neighborhoods (Hong et al., 2021; Maroko, 2020). The resilience of more affluent neighborhoods is often bolstered by the labor of those residing in other, less affluent neighborhoods during disasters. Committee members kept this in mind throughout their work. They sought to develop a framework for delivering essential primary care and preventive health care services related to IPV during PHEs that did not reinforce pre-existing health care disparities or improve access for one community at the expense of another.
PHEs, by their nature of overwhelming system capacities, lay bare inadequate resilience among communities and systems, as well as disparities between them. The COVID-19 pandemic highlighted the degree to which longstanding health disparities and economic inequality had undermined the resilience of many communities. It also revealed that many government and community institutions were not adequately equipped to meet the compounding needs of those under-resourced communities in the face of a global pandemic (OASH, 2022). This revelation was the impetus for development of the Federal Plan for Equitable Long-Term Recovery and Resilience.3 The interagency workgroup that developed the plan noted that, in light of the significant disparities that existed prior to the onset of the
___________________
3 See https://health.gov/our-work/national-health-initiatives/equitable-long-term-recovery-and-resilience (accessed August 25, 2023).
COVID-19 pandemic, recovery efforts should not seek to restore systems and communities to pre-pandemic conditions (OASH, 2022). Instead, they aimed to develop a long-term recovery plan that would improve community and national resilience, which included improving health and well-being. The committee notes that while recovery planning is beyond the scope of this project, the factors that undermine resilience and contribute to adverse outcomes in PHEs, such as health disparities, exacerbate the adverse outcomes of IPV (this is discussed in greater detail in Chapter 3).
Key Terminology
Public Health Emergency
In 2020, the National Academies consensus study report Evidence-Based Practice for Public Health Emergency Preparedness and Response defined the term public health emergency as “a situation with health consequences whose scale, timing, or unpredictability threatens to overwhelm routine capabilities” (NASEM, 2020, p. 43). This committee acknowledges that routine capabilities vary broadly across communities. Therefore, the committee modifies the definition of a PHE as follows: a situation with health consequences whose scale, timing, or unpredictability threatens to overwhelm the routine capabilities of the affected geographic area. The committee applies this definition to the term public health emergency throughout this report. The committee notes that this is different from a declared PHE. The committee acknowledges that the declaration of a disaster or PHE typically involves one or more statutes or other legal authorities, which vary from jurisdiction to jurisdiction. Within the confines of this report, the committee defines a declared PHE as a formal emergency or disaster declaration or determination made by federal, state, local, tribal, or territorial authorities in response to an actual or potential PHE, as defined above to account for those many varied statutes and legal authorities. This report will note specific statutory declarations when the specifics of those legal authorities are central to the committee’s findings, conclusions, or recommendations.
Steady State
In the context of this report, steady state refers to periods when a community’s routine capabilities have not been disrupted due to a PHE. It represents the period when health care systems, businesses, schools, support services, and community-based organizations are operating without impediment from a PHE or its aftermath. Infrastructure, homes, and other buildings are intact and functioning without damage from a PHE.
Health Care Services
The committee defines health care services as care delivered in or referrable from a health care setting. This is a modification of the description of primary care services that is used by the USPSTF Topic Prioritization Workgroup: care that can be delivered in or referred from the primary care setting (Barry et al., 2023). Referrable services are those targeted at addressing the immediate social risk factors and social needs of a person experiencing IPV in order to protect that person’s health and safety. Social risk factors are specific negative social conditions that have a negative effect on health at the individual level, such as housing instability (Alderwick and Gottlieb, 2019). Social needs reflect the social contributors to health, such as housing stability or access to food, that an individual has identified as a priority (Alderwick and Gottlieb, 2019). The committee acknowledges that the complex nature of addressing IPV may necessitate a broad array of supports and strategies to address the many effects of IPV as well as its root causes. However, the scope of this study is limited to health care services. As such, when considering essential health care services for IPV, the committee limited its consideration to IPV care that is delivered in or referrable from a health care setting.
Health Care System
The health care system is referred to throughout the report. For the purposes of this report, the health care system refers to the care delivery component, including individuals and institutions, clinicians, ancillary and support personnel, hospitals, and other health care facilities. The committee acknowledges that the U.S. health system is complex and involves an expansive variety of entities that are responsible for different aspects of health care, including financing, care delivery, regulation, and research. This report covers topics and makes recommendations that affect many elements and actors within the system. Throughout the report, entities of the U.S. health care system not included in the delivery component described above are referred to as different specified entities.
Prevention
The committee was asked to identify promising practices for the prevention of IPV. HRSA described three categories of public health prevention strategies applicable to IPV in its 2023–2025 HRSA Strategy to Address Intimate Partner Violence.4 Those three are:
___________________
4 See https://www.hrsa.gov/office-womens-health/addressing-intimate-partner-violence (accessed August 28, 2023).
- Primary prevention, defined as preventing IPV before it occurs;
- Secondary prevention, defined as immediately responding to occurrences of IPV; and
- Tertiary prevention, defined as responding to the long-term effects of IPV (HRSA, 2023).
All-Hazards Approach
The statement of task asks the committee to use an all-hazards approach to develop its conceptual framework. An all-hazards approach is an integrated approach to emergency preparedness planning that focuses on capacities and capabilities that are critical to prepare for, respond to, and recover from the full spectrum of emergencies or disasters, whether human-made or natural (CMS, 2017). The committee notes that their application of an all-hazards approach acknowledges that not all disasters and emergencies are identical, nor are their effects on different populations and communities (Benevolenza and DeRigne, 2018; Mendenhall et al., 2023).
Disaster Health Responders
For the purposes of this report, disaster health responders are the leaders and staff with expertise in public health and health care who are working and providing care in those settings during response to a PHE.
Emergency Personnel
For the purposes of this report, the term emergency personnel refers to general leads and staff within emergency management infrastructures deployed throughout the emergency environment, including social services and other entities supporting the emergency response.
IPV Care Providers
For the purposes of this report, IPV care providers refer to staff and administrators whose expertise and role are focused on providing care for people experiencing IPV in the health care, social services, and support services settings.
Social Services and Support Services
For the purposes of this report, the committee defines social services as services provided by government agencies that are targeted at addressing
the needs and promoting the well-being of individuals, families, and communities. Examples include programs operated by government agencies such as food and nutrition support programs, adult and child day care programs, and unemployment assistance programs. For the purposes of this report, the committee defines support services as services provided outside of the clinical health care setting by community-based organizations that are targeted at addressing the social needs and promoting the well-being of individuals and families.
Warm Referral
Warm referrals, or warm handoffs, as defined by the Agency for Healthcare Research and Quality, are transfers of care between members of a health care team that occur with the patient’s permission, often with an in-person introduction (AHRQ, 2017). Warm referrals have been used in many domains of patient care in a wide variety of settings, including for behavioral health treatment and in successful social needs screening and referral programs.
ORGANIZATION OF THE REPORT
Chapter 1 of this report explains the committee’s charge and approach to meeting that charge and defines key terminology and language used throughout the report. Chapter 2 describes IPV in the United States during steady state conditions, including prevalence, population-specific considerations, and factors affecting access to IPV-related care. Chapter 3 is organized into two parts. It begins with a high-level overview of core components of PHE response planning, including key related U.S. laws and regulations, existing federal frameworks and response resources, and a discussion of the interaction between PHEs and health disparities. The second part of Chapter 3 addresses the intersection of IPV with PHEs and discusses effects of PHEs on the prevalence and severity of IPV, the double-survivorship experience of those who have experienced both IPV and a PHE, barriers to accessing IPV-related care during PHEs, and existing guidance for providing health care related to IPV during PHEs. Chapter 4 discusses the most common and most serious health conditions related to experiencing IPV. Chapter 5 identifies the essential health care services related to IPV, the settings where care is typically delivered during steady state conditions, and promising models for IPV care during steady state conditions. Chapter 6 discusses the essential health care services related to IPV during PHEs and sustaining access to those services during PHEs, including a discussion of insights gleaned from international guidance and crisis standards of care, as well as approaches for addressing challenges in
sustaining access. Chapter 7 discusses the planning and delivery of essential health care services related to IPV during PHEs, including opportunities to integrate IPV care into existing systems and settings, promising models for IPV care during PHEs, key supply considerations, training for disaster health responders, and existing guidance related to sheltering. Chapter 8 presents all of the committee’s recommendations.
REFERENCES
ACOG. (American College of Obstetricians and Gynecologists). 2012. ACOG committee opinion no. 518: Intimate partner violence. Obstet Gynecol 119(2 Pt 1):412-417.
Aday, L. A., and R. Andersen. 1974. A framework for the study of access to medical care. Health Serv Res 9(3):208-220.
AHRQ (Agency for Healthcare Research and Quality). 2017. Warm handoff: Intervention. https://www.ahrq.gov/patient-safety/reports/engage/interventions/warmhandoff.html (accessed August 25, 2023).
Alderwick, H., and L. M. Gottlieb. 2019. Meanings and misunderstandings: A social determinants of health lexicon for health care systems. Milbank Q 97(2):407-419.
Balshem, H., M. Helfand, H. J. Schunemann, A. D. Oxman, R. Kunz, J. Brozek, G. E. Vist, Y. Falck-Ytter, J. Meerpohl, S. Norris, and G. H. Guyatt. 2011. Grade guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 64(4):401-406.
Barry, M. J., T. A. Wolff, L. Pbert, K. W. Davidson, T. M. Fan, A. H. Krist, J. S. Lin, I. R. MabryHernandez, C. M. Mangione, J. Mills, D. K. Owens, and W. K. Nicholson. 2023. Putting evidence into practice: An update on the U.S. Preventive Services Task Force methods for developing recommendations for preventive services. Ann Fam Med 21(2):165-171.
Bell, S. A., L. K. Krienke, S. Dickey, and R. G. De Vries. 2021. “Helping fill that gap”: A qualitative study of aging in place after disaster through the lens of home-based care providers. BMC Geriatr 21(1):235.
Benevolenza, M. A., and L. DeRigne. 2018. The impact of climate change and natural disasters on vulnerable populations: A systematic review of literature. Journal of Human Behavior in the Social Environment 29(2):266-281.
Black, M. C. 2011. Intimate partner violence and adverse health consequences. American Journal of Lifestyle Medicine 5(5):428-439.
Breiding, M. J., K. C. Basile, S. G. Smith, M. C. Black, and R. R. Mahendra. 2015. Intimate partner violence surveillance: Uniform definitions and recommended data elements. Version 2.0. Edited by Centers for Disease Control and Prevention. Atlanta, GA: National Center for Injury Prevention and Control.
Brigance, C., R. Lucas, E. Jones, A. Davis, M. Oinuma, K. Mishkin, and Z. Henderson. 2022. Nowhere to go: Maternity care deserts across the U.S. 2022 report. March of Dimes.
Bronfenbrenner, U. 1977. Toward an experimental ecology of human development. American Psychologist 514-531.
Burns, P. B., R. J. Rohrich, and K. C. Chung. 2011. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg 128(1):305-310.
CDC (Centers for Disease Control and Prevention). 2022. Fast facts: Preventing intimate partner violence. https://www.cdc.gov/violenceprevention/intimatepartnerviolence/fastfact.html (accessed October 5, 2022).
Clark-Ginsberg, A., B. McCaul, I. Bremaud, G. Caceres, D. Mpanje, S. S. Patel, and R. B. Patel. 2020. Practitioner approaches to measuring community resilience: The analysis of the resilience of communities to disasters toolkit. Int J Disaster Risk Reduct 50.
CMS (Centers for Medicare and Medicaid Services). 2017. Frequently asked questions emergency preparedness regulation: Clarifications on definitions. CMS.
D’Angelo, D. V., J. M. Bombard, R. D. Lee, K. Kortsmit, M. Kapaya, and A. Fasula. 2022. Prevalence of experiencing physical, emotional, and sexual violence by a current intimate partner during pregnancy: Population-based estimates from the pregnancy risk assessment monitoring system. J Fam Violence 38(1):117-126.
Di Napoli, I., F. Procentese, S. Carnevale, C. Esposito, and C. Arcidiacono. 2019. Ending intimate partner violence (IPV) and locating men at stake: An ecological approach. Int J Environ Res Public Health 16(9).
Dillon, G., R. Hussain, D. Loxton, and S. Rahman. 2013. Mental and physical health and intimate partner violence against women: A review of the literature. Int J Family Med 2013:313909.
First, J. M., N. L. First, and J. B. Houston. 2017. Intimate partner violence and disasters. Affilia 32(3):390-403.
Frakt, A. B. 2019. The rural hospital problem. JAMA 321(23):2271-2272.
Franke, R. H., and J. D. Kaul. 1978. The Hawthorne experiments: First statistical interpretation. American Sociological Review 43(5):623-643.
Heron, R. L., and M. C. Eisma. 2021. Barriers and facilitators of disclosing domestic violence to the healthcare service: A systematic review of qualitative research. Health Soc Care Community 29(3):612-630.
Higgins, J. P. T., J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Page, and V. A. Welch, eds. 2023. Cochrane handbook for systematic reviews of interventions, version 6.4. Cochrane. www.training.cochrane.org/handbook.
Hong, B., B. J. Bonczak, A. Gupta, L. E. Thorpe, and C. E. Kontokosta. 2021. Exposure density and neighborhood disparities in COVID-19 infection risk. Proc Natl Acad Sci U S A 118(13):e2021258118.
HRSA (Health Resources and Services Administration). 2023. 2023-2025 HRSA strategy to addressing intimate partner violence. Rockville, MD: HRSA.
Jones, C. P. 2014. Systems of power, axes of inequity: Parallels, intersections, braiding the strands. Med Care 52(10 Suppl 3):S71-S75.
Korab-Chandler, E., M. Kyei-Onanjiri, J. Cameron, K. Hegarty, and L. Tarzia. 2022. Women’s experiences and expectations of intimate partner abuse identification in healthcare settings: A qualitative evidence synthesis. BMJ Open 12(7):e058582.
Lauve-Moon, K., and R. J. Ferreira. 2016. An exploratory investigation: Post-disaster predictors of intimate partner violence. Clinical Social Work Journal 45(2):124-135.
Leemis, R. W., N. Friar, S. Khatiwada, M. S. Chen, M.-j. Kresnow, S. G. Smith, S. Caslin, and K. C. Basile. 2022. The national intimate partner and sexual violence survey: 2016/2017 report on intimate partner violence. Atlanta, GA: Centers for Disease Control and Prevention.
Liu, F., J. McFarlane, J. A. Maddoux, S. Cesario, H. Gilroy, and A. Nava. 2016. Perceived fertility control and pregnancy outcomes among abused women. J Obstet Gynecol Neonatal Nurs 45(4):592-600.
Maroko, A. R., D. Nash, and B. T. Pavilonis. 2020. COVID-19 and inequity: A comparative spatial analysis of New York City and Chicago hot spots. J Urban Health 97(4):461-470.
McLeroy, K. R., D. Bibeau, A. Steckler, and K. Glanz. 1988. An ecological perspective on health promotion programs. Health Educ Q 15(4):351-377.
Mendenhall, R., J. C. Shin, F. Adibu, M. M. Yago, R. Vandewalle, A. Greenlee, and D. S. Grigsby-Toussaint. 2023. Lessons (not) learned: Chicago death inequities during the 1918 influenza and COVID-19 pandemics. Int J Environ Res Public Health 20(7).
Mercy, J. A., S. D. Hillis, A. Butchart, M. A. Bellis, C. L. Ward, X. Fang, and M. L. Rosenberg. 2017. Interpersonal violence: Global impact and paths to prevention. In Disease control priorities, third edition (volume 7): Injury prevention and environmental health. Pp. 71-96.
Merriam-Webster. 2023. Domestic violence. In Merriam-Webster Dictionary. https://www.merriam-webster.com/dictionary/domestic%20violence (accessed April 20, 2023).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2018. Getting to zero alcohol-impaired driving fatalities: A comprehensive approach to a persistent problem. Edited by S. M. Teutsch, A. Geller and Y. Negussie. Washington, DC: The National Academies Press.
NASEM. 2020. Evidence-based practice for public health emergency preparedness and response. Edited by N. Calonge, L. Brown and A. Downey. Washington, DC: The National Academies Press.
Nelson, H. D., C. Bougatsos, and I. Blazina. 2012. Screening women for intimate partner violence: A systematic review to update the U.S. Preventive services task force recommendation. Ann Intern Med 156(11):796-808, W-279, W-280, W-281, W-282.
Nelson, H. D., B. G. Darney, K. Ahrens, A. Burgess, R. M. Jungbauer, A. Cantor, C. Atchison, K. B. Eden, R. Goueth, and R. Fu. 2022. Associations of unintended pregnancy with maternal and infant health outcomes: A systematic review and meta-analysis. JAMA 328(17):1714-1729.
NIMHD (National Institute on Minority Health and Health Disparities). 2023. HD pulse: An ecosystem of health disparities and minority health resources. https://hdpulse.nimhd.nih.gov/#def3 (accessed June 5, 2023).
Nyambe, A., G. Van Hal, and J. K. Kampen. 2016. Screening and vaccination as determined by the social ecological model and the theory of triadic influence: A systematic review. BMC Public Health 16(1):1166.
O’Campo, P., M. Kirst, C. Tsamis, C. Chambers, and F. Ahmad. 2011. Implementing successful intimate partner violence screening programs in health care settings: Evidence generated from a realist-informed systematic review. Soc Sci Med 72(6):855-866.
OASH (Office of the Assistant Secretary for Health). 2022. Equitable long-term recovery and resilience. https://health.gov/our-work/national-health-initiatives/equitable-long-term-recovery-and-resilience (accessed August 25, 2023).
Randell, K. A., and M. I. Ragavan. 2020. Intimate partner violence: Identification and response in pediatric health care settings. Clin Pediatr (Phila) 59(2):109-115.
Roberts, S. C., M. A. Biggs, K. S. Chibber, H. Gould, C. H. Rocca, and D. G. Foster. 2014. Risk of violence from the man involved in the pregnancy after receiving or being denied an abortion. BMC Med 12(1):144.
Smith, E. J., B. A. Bailey, and A. Cascio. 2023. Sexual coercion, intimate partner violence, and homicide: A scoping literature review. Trauma, Violence, & Abuse 25(1):341-353. https://doi.org/10.1177/15248380221150474.
Stubbs, A., and C. Szoeke. 2022. The effect of intimate partner violence on the physical health and health-related behaviors of women: A systematic review of the literature. Trauma, Violence, & Abuse 23(4):1157-1172.
Thurston, A. M., H. Stockl, and M. Ranganathan. 2021. Natural hazards, disasters and violence against women and girls: A global mixed-methods systematic review. BMJ Glob Health 6(4).
Topchick, M., T. Brown, M. Pinette, B. Balfour, and H. Kein. 2021. Rural communities at risk: Widening health disparities present new challenges in aftermath of pandemic. The Chartis Group.
VA (U.S. Department of Veterans Affairs). 2021. Intimate partner violence assistance program. https://www.socialwork.va.gov/IPV/About.asp (accessed May 1, 2023).
Vicard-Olagne, M., B. Pereira, L. Rouge, A. Cabaillot, P. Vorilhon, G. Lazimi, and C. Laporte. 2022. Signs and symptoms of intimate partner violence in women attending primary care in Europe, North America and Australia: A systematic review and meta-analysis. Fam Pract 39(1):190-199.
Viero, A., G. Barbara, M. Montisci, K. Kustermann, and C. Cattaneo. 2021. Violence against women in the COVID-19 pandemic: A review of the literature and a call for shared strategies to tackle health and social emergencies. Forensic Sci Int 319:110650.
Wagner, E. H., N. Sandhu, K. Coleman, K. E. Phillips, and J. R. Sugarman. 2014. Improving care coordination in primary care. Med Care 52(11 Suppl 4):S33-S38.
Walshe, K. 2007. Understanding what works–and why–in quality improvement: The need for theory-driven evaluation. Int J Qual Health Care 19(2):57-59.
WPSI (Women’s Preventive Services Initiative). 2022. Women’s preventive services initiative. https://www.womenspreventivehealth.org/wpsi-statements/ (accessed August 18, 2023).
Zink, T., and F. Putnam. 2005. Intimate partner violence research in the health care setting: What are appropriate and feasible methodological standards? J Interpers Violence 20(4):365-372.


















