5
Essential Health Care Services for Intimate Partner Violence
ESSENTIAL HEALTH CARE SERVICES RELATED TO INTIMATE PARTNER VIOLENCE
The committee defines health care services as care delivered in or referrable from a health care setting. Therefore, essential health care services related to intimate partner violence (IPV) refer to essential care delivered in or referrable from a health care setting. This reflects the committee’s understanding that the health consequences of IPV may require care that extends beyond the traditional health care system. Essential health care services related to IPV include those that address the most prevalent and serious physical and behavioral health conditions related to IPV, which are discussed in Chapter 4. Essential health care services related to IPV also facilitate identification of IPV, protect the safety of the person experiencing IPV (and their children if needed), and meet their basic needs for food and shelter.
Essential Explained
The committee’s process for identifying essential health care services related to IPV in steady state conditions was informed by an extensive review of high-quality evidence from several literature searches; recommendations from the U.S. Preventive Services Task Force (USPSTF), the Women’s Preventive Services Initiative (WPSI), and the World Health Organization (WHO); and insight gleaned from a commissioned paper and presentations to the committee by experts in IPV-related care.
The committee identified the following criteria for identifying essential health care services related to IPV:
- Evidence-based health care services that address the most common and most serious health outcomes related to experiencing IPV;
- Preventive services recommended by USPSTF and WPSI; and
- Specific support services required to meet the basic safety and housing needs of people experiencing IPV.
Essential Intimate Partner Violence–Related Health Care Services
The many adverse health effects related to experiencing IPV do not occur in isolation. Women experiencing IPV need care for multiple physical and psychological conditions concurrently. The list of essential health care services in the recommendation below should not be considered exhaustive. Each woman’s experience of IPV is different, as are her needs for health care services related to IPV.
Recommendation 1: The committee recommends that the Health Resources and Services Administration and all U.S. health care systems classify the following as essential health care services related to intimate partner violence (IPV):
- Universal IPV screening and inquiry
- Universal IPV education
- Safety planning
- Forensic medical examinations
- Emergency medical care
- Treatment of physical injuries
- Gynecologic and reproductive health care, including all forms of Food and Drug Administration-approved contraception and pregnancy termination
- Screening and treatment of sexually transmitted infections and HIV
- Treatment for substance use disorders and addiction care
- Pharmacy and medication management
- Obstetric care, including perinatal home visits
- Primary and specialty care
- Mental health care
- Support services, including shelter, nutritional assistance, and child care
- Dental care
Universal Screening and Education
Screening in health care generally refers to delivering preventive health services that identify a condition or risk for a condition to patients without signs or symptoms of the condition being screened, as opposed to diagnosing patients with indications of the condition. Universal screening for IPV includes all patients, regardless of the presence of signs, symptoms, or health conditions related to IPV, to identify those with subclinical experiences of previous or ongoing IPV and those at risk for future IPV. The goal of IPV screening in health care settings is to provide support and patient specific interventions, including referrals, that reduce exposure to IPV and improve health outcomes. Screening for IPV is included for coverage under preventive service mandates of the Patient Protection and Affordable Care Act (ACA).1
Periodic universal screening for IPV is an established standard of routine preventive health care for women aged 13 years and older in the United States. The USPSTF recommends screening all women of reproductive age for IPV and providing ongoing support services to women who have a positive screening outcome or referring them to those services (USPSTF et al., 2018). The WPSI recommends screening adolescents and adults with biological or other identification as a woman at least annually and providing women with—or referring them to—intervention and support services if needed (WPSI, 2022). The WPSI recommendation notes that intervention services “include, but are not limited to, counseling, education, harm reduction strategies, and referral to appropriate supportive services” (WPSI, 2022, p. 52). The second part of both the USPSTF and WPSI screening recommendations highlight that providing or referring women to support services is a critical component of screening for IPV.
Routine screening is usually implemented during primary care and maternity care visits, although it also occurs in other settings. Screening in health care settings is generally acceptable to women when done privately and safely, and some prefer self-administered methods, including computerized screening (Ahmad et al., 2009; Kapur and Windish, 2011; MacMillan et al., 2006). A coding guide developed by the WPSI assists clinical practices with coding and billing for IPV screening services. The coding guide includes ICD-10 codes, coding scenarios, and Medicare and Medicaid resources (WPSI, 2022).2
Screening generally involves the administration of a validated screening instrument composed of a brief set of questions that may include questions about physical, sexual, and psychological abuse (see Table 5-1).
___________________
1 Patient Protection and Affordable Care Act, Public Law 118-148, 111th Congress (March 23, 2010).
2 ICD-10 refers to International Classification of Diseases, 10th edition.
TABLE 5-1 Validated Tools for Screening for IPV
| Measure | Components | Sensitivity; specificity |
|---|---|---|
| Hurt/Insult/Threaten/Scream tool (HITS) | Four items (hurt, insult, threaten, scream), 5-point Likert scale, self-report or clinician administered survey; score ranges from 4 to 20 points, ≥10 indicates abuse. | 86%; 99% |
| Ongoing Violence Assessment Tool (OVAT) | Four items (threaten, beaten, would like to kill you, no respect), dichotomous scale; score ranges from 0 to 4. | 86%; 83% |
| Partner Violence Screen (PVS) | Three items (past physical violence, perceived personal safety), dichotomous scale, clinician administered; score ranges from 0 to 3, ≥1 indicates IPV. | 49–71%; 80–94% |
| Woman Abuse Screening Tool (WAST) | Eight items (physical, sexual, emotional abuse), 3-point response scale (0 = never, 1 = sometimes, 2 = often); scores range from 0 to 16, and ≥4 indicates exposure to IPV. Short form includes two questions about tension in the relationship and how arguments are resolved. | 47–88%; 89–96% |
| Slapped, Threatened, and Throw (STaT) Measure | Three items (pushed or slapped; threatened with violence; partner has thrown, broken, or punched things), dichotomous, self-report scale; score ranges from 0 to 3. | 96%; 75% |
| Abuse Assessment Screen (AAS) | Five items (sexual coercion, lifetime abuse, current abuse, abuse during pregnancy), dichotomous scale, clinician administered survey; scores range from 0 to 5, with any positive response considered a positive screen. | 92%; 55% |
| Humiliation, Afraid, Rape, Kick (HARK) Tool | Four items (humiliation, afraid, rape, kick), dichotomous scale, self-report survey, adapted from AAS; scoring ranges from 0 to 4. | 81%; 95% |
| Ongoing Abuse Screen (OAS) | Five items (threaten, beaten, would like to kill you, no respect), dichotomous scale; scores range from 0 to 5. | 60%; 90% |
SOURCE: Feltner et al., 2018.
Some instruments, such as the Ongoing Violence Assessment Tool, focus on physical violence and personal safety (Feltner et al., 2018). In contrast, others, such as the Women Abuse Screening Tool, include additional types of abuse (Feltner et al., 2018). Most instruments identify current IPV or IPV occurring within the previous 12 months, while some collect information about past IPV, such as the Abuse Assessment Screen (AAS) (Feltner et al.,
2018). Validated instruments may not apply to all patient populations, such as non-English speakers, and other screening approaches may be necessary.
Screening tools have also been developed to specifically assess IPV lethality or the risk of intimate partner homicide (Campbell, 1986; Campbell et al., 2009; Echeburúa et al., 2009; López-Ossorio et al., 2019; Messing et al., 2013, 2017, 2020). Sensitivity, specificity, and reliability for these metrics are mixed (Garcia-Vergara et al., 2022; Messing et al., 2017). They are not evaluated or included in the USPSTF or WPSI screening recommendations.
IPV screening may be appropriate for patients and settings outside those specified in routine screening recommendations. These include screening in emergency departments, orthopedic clinics, and other health care settings where IPV-related conditions commonly present but may go unrecognized. In these cases, the use of IPV screening instruments may extend beyond universal screening to detect IPV in the context of coexisting health conditions associated with IPV.
Some researchers and practitioners have raised concerns that screening for IPV may cause harm to women (Chisholm et al., 2017; McLennan and MacMillan, 2016). Potential harms discussed in the literature include opportunity costs regarding other health services, child protection investigation, false positives, increased abuse, retaliation, labeling, and stigma (Feltner et al., 2018; McLennan and MacMillan, 2016). However, a USPSTF evidence review did not find evidence that IPV screening presents a statistically significant risk of harm (Feltner et al., 2018). A separate Cochrane review also found no evidence that screening for IPV poses a significant risk of harm (O’Doherty et al., 2015). However, both reviews indicated that there were few robust studies examining the harms of screening and noted methodological heterogeneity across the literature (Feltner et al., 2018; O’Doherty et al., 2015).
The perinatal period is a critical time to offer screening and health care for IPV. Women access health care more frequently during this period and are more likely to implement suggested health behaviors than in other situations. Therefore, screening during regular perinatal care is important, and attention to the health effects and care needs related to IPV in this population is necessary. Despite the recommendation from the USPSTF calling for universal screening for those of reproductive age, screening practices remain inconsistent throughout perinatal care. Analysis of data from the 2016–2019 Pregnancy Risk Assessment Monitoring System found that of the respondents who reported experiencing physical IPV during pregnancy and received prenatal care, 25.5 percent (n = 1,326, N = 6,124) were not screened for IPV at any prenatal care visits (Kozhimannil et al., 2023).3
___________________
3 Additional context has been added to the sentence to ensure an accurate representation of the data presented, after initial release of the report.
Within the group of people receiving prenatal care, those who lived in rural districts and those who were covered through private insurance were less likely to be screened for IPV than those in urban areas and those covered through Medicaid (Kozhimannil et al., 2023). Universal screening for IPV in the health care setting not only aids in identifying those who are at risk of or experiencing IPV but can lead to interventions to improve maternal and fetal outcomes. There is a particularly large window of opportunity for screening during perinatal care, as pregnant and postpartum people typically have more regular office visits with their clinicians and have the chance to build trusting relationships with their clinicians during this time (Alhusen et al., 2015). Not all IPV screening assessments screen for physical, psychological, and sexual violence (Chisholm et al., 2017). The American College of Obstetricians and Gynecologists provides guidance for IPV screening in the perinatal period (ACOG, 2012).
Universal education involves offering information about healthy relationships, the intersections of IPV and health, and relevant supports and services during all clinical encounters (McKay, 2021). This approach addresses a limitation of screening often noted by advocates—that a woman experiencing IPV must be ready to disclose in order to receive information about IPV and relevant resources (McKay, 2021). Research directed at identifying barriers to IPV disclosure has highlighted the role of knowledge about IPV and available supports in disclosure and help seeking. A systematic review of 29 studies investigating barriers to disclosing IPV found that two of the most commonly reported reasons women reported for not disclosing IPV during screening were a lack of knowledge about IPV and a lack of awareness of available services to support them (Robinson et al., 2021). This was echoed by Ravi and colleagues in their systematic review of 24 studies investigating facilitators of formal help seeking among people experiencing IPV (Ravi et al., 2022). By highlighting that this information may be relevant to themselves or someone they know, clinicians and front line responders can reduce feelings of shame and isolation that some women experience. A core component of essential health care services is ensuring that information about IPV (including how a public health emergency [PHE] may escalate abusive behaviors in a relationship) is readily available in all settings where individuals seek help.
Safety Planning
Safety planning is the process of collaborating with the woman experiencing IPV to empower her to develop strategies that increase safety by increasing her situational awareness of IPV-related risks (Sabri et al., 2021). The process is centered on the woman experiencing IPV and informed by her identified concerns and priorities. Once those are identified, planning
includes identifying and connecting the woman to resources consistent with her needs (Sabri et al., 2021). In some situations, the person experiencing IPV may not want to or may not feel that they can leave an abusive relationship. Research has found that in situations where the person engaging in IPV is highly dangerous, the act of leaving the relationship may increase the woman’s level of danger (Campbell et al., 2003, 2009). In that situation, safety planning focuses on strategies to enhance her safety and reduce risk while remaining in the relationship (Sabri et al., 2021). The literature has identified elements of safety plans that are most effective, including:
- Assessing individual needs and circumstances;
- Providing education about the different forms of IPV;
- Helping women identify their safety risks;
- Developing concrete safety plans;
- Directly connecting women to resources and support services;
- Establishing long-term support, including continued safety check-ins during follow-up IPV care and services;
- Focusing on empowerment to enhance women’s safety strategies and strengthening support networks to help manage safety threats; and
- Including interventions to address co-occurring conditions, including mental health issues, substance use, and sexual risk behaviors that may put them at risk for sexually transmitted infections (STIs), including HIV (Sabri et al., 2021).
TREATMENT OF CONDITIONS RELATED TO ACUTE INTIMATE PARTNER VIOLENCE
Injuries to the Head, Neck, and Face
Treatment for injuries to the head, neck, and face require different essential health care services depending on the severity of the injury. Fractures to the head, neck, and face can be life-threatening and require emergency medical care to stabilize the fracture and address any associated airway obstruction, spinal cord injury, brain injury, or secondary trauma that can affect vision, hearing, speaking, or jaw function (Chouinard et al., 2016; Jose et al., 2016). These fractures may require surgical intervention, and all fractures will require post-reduction follow-up in the form of specialty medical care. Soft tissue injuries to the head, neck, and face will require treatment for acute trauma and may require surgical intervention and follow-up specialty medical care.
Women with a traumatic brain injury (TBI) related to IPV require multiple health care services and may seek care in a variety of settings. Many
of the acute injuries associated with TBI, such as skull fracture, cervical fracture, and intracranial hemorrhage, require emergency medical care and may require surgical intervention (Galgano et al., 2017; Taylor et al., 2017). Women who have sustained an IPV-related TBI may also require hospitalization, depending on the severity of the TBI and associated injuries (Taylor et al., 2017). Women who have sustained an IPV-related TBI may initially seek care for another concomitant physical injury, such as an extremity fracture or dental injury (Ellis et al., 2019; Turkstra et al., 2023). Women who have experienced an IPV-related TBI will require multiple essential health care services, including primary and specialty medical care, mental health care, and pharmacy/medication management to support recovery and long-term management of chronic TBI sequelae. The cognitive sequelae of TBI, such as impaired judgement and executive function deficits, can make it difficult for women with IPV-related TBI to complete both simple everyday tasks and more complex tasks, such as those that may be necessary to access health care or support services, or to separate from a person using IPV (Haag et al., 2022).
Women who sustain a TBI or hypoxic brain injuries due to IPV-related strangulation can reasonably be expected to experience acute and chronic adverse physical, psychological, and cognitive effects that are similar to those associated with sustaining a TBI not due to strangulation (Anderson and Archiniegas, 2010; Valera et al., 2022). As a result, the same categories of IPV-related essential health care services are required for women that have survived IPV-related strangulation.
Musculoskeletal Injuries
Women experiencing IPV-related musculoskeletal injuries will have differing essential health care service needs depending on the severity of their injuries. Severe acute injuries such as dislocations and some fractures are associated with an elevated risk for dangerous complications, such as damage to adjacent vasculature, and require emergency medical care. Those injuries as well as other musculoskeletal injuries require specialty medical care. A growing body of research suggests that a large number of women experiencing IPV-related musculoskeletal injuries seek care in outpatient orthopedic clinics and fracture clinics, highlighting the importance of this setting to essential IPV health care services (Logue et al., 2021; Sprague et al., 2013a,b; Velonis et al., 2019).
Gynecologic and Reproductive Health Issues
Women experiencing IPV have complex gynecologic and reproductive health problems that require multiple essential health care services related
to IPV. Emergency medical care is required for severe gynecologic injuries and infections. Gynecologic and reproductive health services, screening and treatment for STIs and HIV, and primary and specialty medical care are needed to address IPV-related injuries, infections, and other disorders. Those services may be delivered in a variety of settings, including primary care clinics, obstetric and gynecology clinics, and other medical specialty clinics such as oncology, family planning, and reproductive health clinics.
Women experiencing reproductive coercion or an unplanned pregnancy related to IPV have unique needs for essential health care services related to IPV. They need gynecologic and reproductive health care services, which include all forms of FDA-approved contraception. Access will reduce the likelihood of unintended pregnancy, particularly in light of the well-documented barriers to accessing some forms of contraception, such as emergency contraception, for those experiencing IPV (Bergmann and Stockman, 2015; Gee et al., 2009; Miller et al., 2014; Smith et al., 2022). In light of the substantial risks to maternal and infant health as well as increased risk to women’s safety associated with an IPV-related unintended pregnancy, the essential gynecologic and reproductive health care services related to IPV include pregnancy termination when the woman and her health care professional determine that is appropriate (Auger et al., 2022; Mogos et al., 2016; Nelson et al., 2022; Smith et al., 2023). Some adverse health effects related to unintended pregnancy and IPV are serious and can be life threatening, requiring emergency medical care. Additionally, individuals who experience IPV-related unplanned pregnancies also need access to obstetric care for both standard pregnancy care and to address the adverse health effects associated with IPV and unplanned pregnancy.
Additionally, women experiencing IPV-related sexual assault require several essential health care services related to IPV. They should have access to treatment for physical injuries sustained during the assault and, depending on the severity of their injuries, may need emergency medical care. Their care needs will vary, from needing primary care to needing specialty clinical care, depending on the nature of the injuries or disorders. The needs of women experiencing IPV-related sexual assault include access to gynecologic and reproductive health care services to address both acute and chronic gynecologic injuries and disorders. They also need access to STI and HIV screening and treatment. Mental health care is also important for addressing the psychological trauma associated with experiencing violent acts, such as rape. This array of services should also be available for women who have been raped by an intimate partner. They have time-sensitive needs for essential health care services. Emergency contraception should be available to reduce the risk of unintended pregnancy within 5 days of the rape (Basile et al., 2018; Smith et al., 2023). Additionally, it is possible that a woman who has experienced IPV rape will not know the HIV and STI status of
her partner, which makes access to STI and HIV screening and treatment, including post-exposure prophylaxis, an urgent need (Gilmore et al., 2022).
The forensic medical examination, also referred to as a sexual assault medical forensic examination, is an essential health care service related to IPV that facilitates access to time-sensitive care needs related to IPV sexual assault and rape (Gilmore et al., 2021). Individuals who undergo a sexual assault forensic medical examination at a facility with a sexual assault nurse examiner (SANE) also receive crucial medical care, including STI and HIV testing and prophylaxis, as well as emergency contraception (Gilmore et al., 2021). SANEs have specialized training in evaluating and caring for a person who has experienced sexual assault using a trauma-informed approach (Thiede and Miyamoto, 2021). SANE-led care is associated with a high quality of care as well as with more thorough examinations, high-quality evidence collection, and more positive prosecutorial outcomes (Thiede and Miyamoto, 2021). In addition to sexual assault, forensic medical examinations for people who have experienced IPV can be used to document injuries from physical IPV, including strangulation (Pritchard et al., 2017).
In May 2023, the U.S. Department of Justice’s Office on Violence Against Women released a National Protocol for Intimate Partner Violence Medical Forensic Examinations (DOJ, 2023). The protocol emphasizes the importance of a warm handoff of the person experiencing IPV to service providers and community-based organizations, in which the clinician connects the individual to the appropriate resource instead of simply providing a telephone number or website address (DOJ, 2023). The protocol also stresses that IPV care providers need to engage in a trauma-informed approach when caring for people experiencing IPV. According to the protocol, a medical forensic examination for people experiencing IPV includes:
- Medical forensic history gathering,
- Comprehensive physical assessment,
- Treatment of injuries,
- Provision of care for other health concerns identified during the examination,
- Sample and evidence collection,
- Photographic documentation of findings,
- Written documentation of the patient encounter, and
- Safety and discharge planning, including targeted referrals based on the patient’s specific needs. (DOJ, 2023)
Chronic Pain
Chronic pain is a complex condition that is further confounded in the setting of experiencing IPV. Its complex nature requires individualized and
multimodal treatment. These include, but are not limited to, treatment of traumatic physical injuries, gynecologic and reproductive health care, mental health care, pharmacy/medication management, and primary care and specialty medical care.
Mental and Behavioral Health
Given the substantial adverse effects that experiencing IPV has on mental and behavioral health, mental health care is an essential health care service related to IPV. Women experiencing IPV and substance use disorder have broad needs for essential health care services related to IPV, including access to substance use treatment and addiction care, pharmacy/medication management, mental health care, STI and HIV testing and treatment, primary and specialty medical care, and emergency medical care. The syndemic of IPV, substance abuse, and HIV among women in the United States is well documented in the literature (González-Guarda et al., 2011; Meyer et al., 2011; Vavala et al., 2022). Therefore, the essential health care services related to IPV for substance use and HIV are likely to be needed concurrently.
INTIMATE PARTNER VIOLENCE HEALTH CARE ACCESS AND DELIVERY
Essential health care services for IPV are delivered in multiple settings across health care systems, including primary care, practices related to women’s health (e.g., Planned Parenthood), perinatal-specific care settings, and settings supported by federal funding. Community-based care settings also serve to provide many of these essential services. One analysis of survey data from 3,333 women in Washington state and Idaho found that women experiencing IPV reported at least 20 percent more health care utilization than those that had not reported experiencing IPV, even after their experiences of IPV have ended (Rivara et al., 2007). Given the higher frequency of health care use among women experiencing IPV, primary care and other specialty care professionals can play an important role in interrupting IPV and promoting women’s health and well-being.
A systematic review of IPV interventions in primary care found that most of the reviewed studies (10 of 17) recruited women from reproductive health care settings in obstetrics–gynecology and family planning (Bair-Merritt et al., 2014). Most of the interventions were conducted entirely in the primary care office setting. Most interventions included outside office contact, including case management, phone calls, and home visits. The interventions ranged in length from 10 minutes to 16 hours (eight 2-hour weekly sessions). Nonphysicians delivered the majority of the care, which focused on empowerment, empathetic listening, discussion of the cycle of
violence and safety, and referral to community-based resources. It is important to note that none of the interventions were conducted in a pediatric setting. Since more than one in six youth in the United States report being exposed to IPV as children, much still needs to be learned about youth interventions (Hamby et al., 2011).
As noted earlier, because essential health care services for IPV encompass a wide range of health care settings, specialties, resources, and personnel, services interface not only with the patient and health system but also with the community and society. Patients access health care services for IPV through multiple pathways (see Figure 5-1). Most health care services are accessed through the health care system itself, including health care provided by first responders, community health workers, and telemedicine programs, in addition to clinics and hospitals.
Health Care System Settings
IPV is associated with increased health care utilization (Rivara et al., 2007). Care for patients experiencing IPV involves clinicians and staff across various settings in health care systems, including outpatient primary care clinics, specialty clinics, emergency and urgent care settings, and inpatient facilities.
Emergency department (ED) staff and clinicians routinely serve women who have experienced IPV. A review of nationwide insurance claims data found that women with a documented history of experiencing IPV had 4.5 times more ED visits than those without a documented history of IPV (Kishton et al., 2022). Several studies have noted high reported rates of IPV, including reproductive coercion, among women seeking care in family planning and women’s health clinics (Miller et al., 2014; Rickert et al., 2002). In these settings, women with IPV are more likely to seek emergency contraception, treatment for STIs, and pregnancy tests (Kazmerski et al., 2015; Miller et al., 2010). In an analysis of survey data collected in eight Canadian and U.S. orthopedic fracture clinics, the prevalence of IPV within the past year was 18 percent and the lifetime prevalence was 40 percent (Sprague et al., 2013a). Clinicians serving those with chronic health conditions may see patients whose conditions are directly related to IPV or exacerbated by new episodes of IPV. In contrast, chronic conditions associated with IPV are common. However, they may go undetected or under-treated in the health care system (Wilson et al., 2007).
Clinicians in diverse settings, especially those in which confidentiality is ensured are likely to encounter adolescents who have experienced IPV (Miller et al., 2010). However, adolescents are unlikely to mention relationship or sexual abuse as the reason for their visit. Instead, they may present with trauma symptoms, injuries, or mental health problems. They
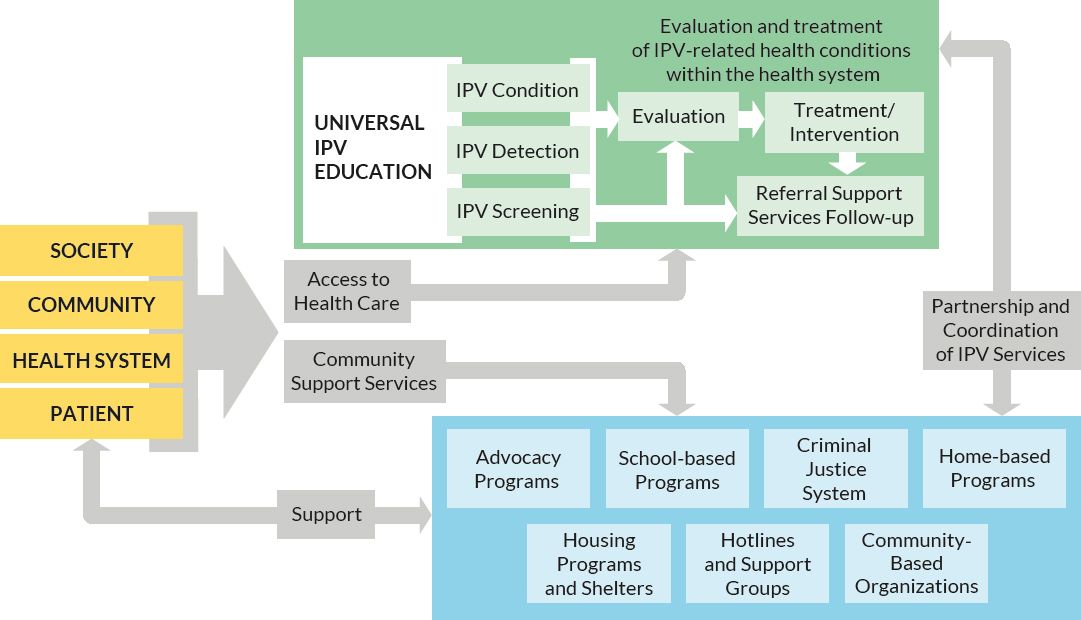
NOTES: Patients access health care services through multiple pathways, including treatment of recognized IPV-related health conditions (e.g., acute trauma from IPV assault). IPV is typically detected during the course of health care (e.g., injury identified during a maternity care visit) or through inquiry (e.g., routine IPV screening without current signs or symptoms).
may also present with nonspecific complaints, such as recurrent headaches, poor sleep, abdominal pain, or fatigue (Miller et al., 2010). Requests for pregnancy or STItesting and emergency contraception may suggest that relationship abuse or sexual violence has occurred.
Clinical settings that provide pediatric care are confidential and safe spaces that can support parents and caregivers experiencing IPV who may be more likely to seek care for their children than for themselves (Ragavan and Miller, 2022). Studies in pediatric care settings during the COVID-19 pandemic found that parents reported partners engaging in IPV employed coercive control tactics including social isolation, manipulating child custody, taking stimulus money, and a myriad of other tactics (Kourti et al., 2023; Ragavan et al., 2022). The American Academy of Pediatrics has encouraged pediatric clinicians to engage in training and education about IPV and to consider incorporating universal IPV education into their practices (Thackeray et al., 2023).
Positive and Negative Experiences in Health Care Settings
In its recently released 2023–2025 Strategy to Address Intimate Partner Violence, HRSA notes that an equitable, community-driven approach necessitates seeking input from communities and individuals being served (HRSA, 2023a). People who have experienced IPV can provide critical feedback on developing, funding, implementing, and evaluating services and programs to prevent and respond to IPV. Centering community voices in preparation for public health emergencies ensures that programs are relevant and responsive to community priorities, assets, and challenges. Simultaneously, culturally responsive care and attention to health equity in clinical practices can reduce health disparities experienced by populations disproportionately affected by IPV.
Experiences of Patients
A systematic review of studies of health care for IPV in emergency departments identified several factors contributing to positive and negative experiences with clinicians (Duchesne et al., 2022). Patients reported positive experiences with clinicians who were nonjudgmental and compassionate, validated their experience, and focused on the whole person and not just specific injuries. In addition, the health care system provided access to effective resources and referrals and delivered timely and private care (Duchesne et al., 2022). Patients also identified factors contributing to a negative experience, such as clinicians who minimized patients’ concerns; seemed unconcerned, judgmental, or blaming; were uncomfortable with IPV; and lacked knowledge or experience with IPV. Ways in which health
care systems have failed to adequately support patients included lacking adequate referrals or services, making the patient feel hopeless, and allowing the partner engaging in IPV to stay in the exam room (Duchesne et al., 2022). In negative encounters, patients experienced long wait times and felt belittled or stereotyped. Negative experiences related to system- and clinician-level factors can lead to avoidance and distrust of the health care system, as illustrated in Figure 5-2. These effects can drive patients experiencing IPV away from the health care settings that could help them. Alternatively, factors related to positive experiences can improve engagement with the health care system.
Experiences of Clinicians
Health care professionals in emergency departments have identified positive and negative factors associated with providing high-quality care for people experiencing IPV. Positive factors include being knowledgeable and well-equipped to care for patients experiencing IPV, having supportive policies and protocols, providing adequate time and private clinical space, and collaborating with a trained interdisciplinary team (Duchesne et al., 2022). Negative factors reported by clinicians included reluctance to address the
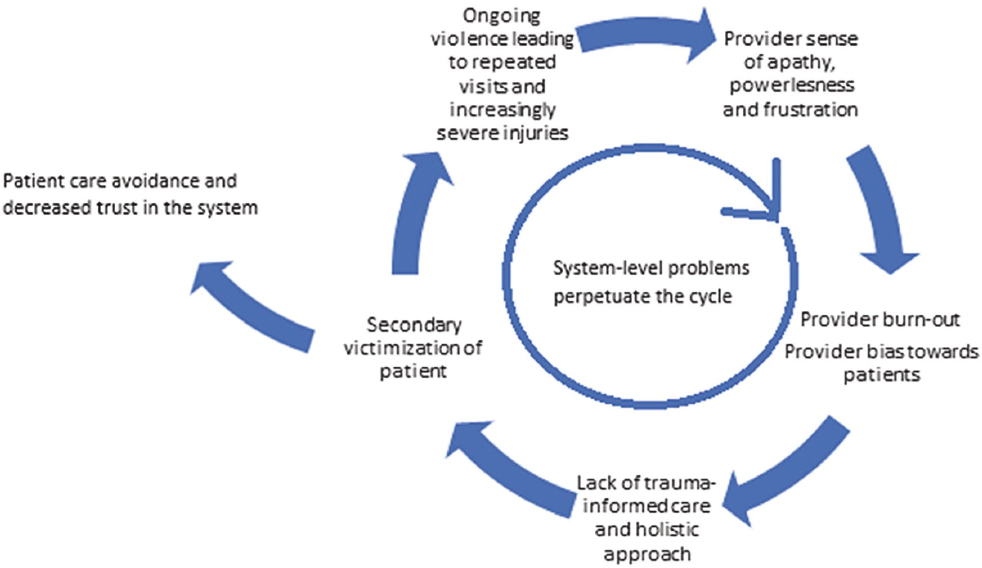
NOTE: Patients seeking care for IPV may encounter negative experiences in the health care system related to multiple system-level and health care provider–level factors.
SOURCE: Duchesne et al. (2022).
complexity of IPV in the context of acute care; beliefs that IPV was a social not medical issue and outside their scope; frustration and powerlessness when patients returned to violent environments; lack of training, infrastructure, and support services; working in under-resourced environments; and personal stereotypes and biases about IPV. Many of these issues were also described in studies of barriers to effective IPV interventions in other settings (Rivas et al., 2019).
Patient Preferences in Intimate Partner Violence Care
Studies with women who have experienced IPV indicate that most want clinicians to talk to them about IPV in a safe and private setting, to discuss the possibility of IPV exposure without pushing for disclosure, and to offer tangible medical and social resources for support (Chang et al., 2005; Feder et al., 2006). Patients may not connect the symptoms they are experiencing, such as recurrent headaches, pain, heart palpitations, and insomnia, to stressors associated with IPV. Printed information about linkages between challenging relationships and personal health and information about available supports can be helpful for patients and can help build trust with the practitioner and practice (Miller et al., 2017).
A meta-synthesis of qualitative data focused on women’s experiences and expectations of disclosing IPV experiences to a clinician highlighted the importance of delivering woman-centered care (Tarzia et al., 2020). The authors reviewed 31 manuscripts and identified four critical areas related to women’s expectations of health care professionals after disclosing IPV. These included emotional connection through kindness and care, recognition and understanding of women’s experiences, action and advocacy (doing more than listening), and giving women choice and control in making their own decisions. Similarly, a study of people who have experienced IPV asked what they wanted from professionals in a helping role. Study participants identified three key characteristics: preserving respect for autonomy, offering support and information about existing resources (regardless of disclosure), and not pushing for disclosure (Chang et al., 2005).
Community-Based Care Settings
Community-based services play an important role in addressing IPV. Many IPV-related health care services are provided outside health care systems (e.g., hospitals, clinics, and primary care). In some cases, people experiencing IPV may be referred to community-based care from the health care system. In other cases, these community-based settings may be the first site of care. Additionally, community-based services can provide the primary response to IPV for individuals who do not access health care or do
not disclose their experiences to clinicians. Examples of such community-based services include:
- Advocacy programs, which help people experiencing IPV navigate the legal system or access supports such as housing, education, counseling, financial planning, and job placement (Shorey et al., 2014). Advocacy programs may be community-based organizations or may be housed in domestic violence shelters or law schools.
- Criminal justice system, including police and legal offices, enables people experiencing IPV to obtain civil protection orders (Shorey et al., 2014). Some police departments have programs in which individuals with expertise in domestic violence accompany officers on calls of reported IPV to provide crisis intervention and referrals to support services (Shorey et al., 2014).
- Housing programs, which can include crisis violence shelters (also referred to as safe houses), transitional supportive housing, and permanent housing. Shelters, in addition to providing food and a place to live, may also offer counseling, advocacy services, and supports for children of people experiencing IPV, including transportation to and from school and tutoring (Shorey et al., 2014).
- Assistance hotlines, such as the National Domestic Violence Hotline, national and local sexual assault or rape crisis hotlines, the StrongHearts Native Helpline, National Dating Abuse Helpline, and others (NCADV, n.d.).
- Home-based care programs, which are typically associated with home visitation programs for maternal and infant care (Sharps et al., 2016).
- Peer-led support groups (Shorey et al., 2014).
Researchers have examined the effectiveness of community-based approaches for IPV. However, these studies have limitations that make comparison of the effectiveness of different interventions difficult. Individual studies vary in the types of outcomes that are measured, making accurate comparison difficult. Analysis of these studies through the lens of the many challenges associated with conducting IPV intervention research is critical. While inconsistencies in study design make it difficult to determine whether one intervention is more effective than another, it is apparent that community-based interventions play a key role in providing care for women experiencing IPV.
Domestic Violence Advocacy Programs
Many community-based domestic violence advocacy programs serve individuals and families experiencing IPV. These programs often use an empowerment model with a gendered approach by contextualizing IPV within gender oppression (Kasturirangan, 2008). They partner with clients to identify goals, assess risk and engage in safety planning, and connect clients to needed community resources. The resources often include opportunities for individuals experiencing IPV to connect with one another through support groups and other strategies for promoting social support (Kasturirangan, 2008). Offering individuals affected by IPV social support has been found to contribute to improvements in mental health (Ogbe et al., 2020).
Shelters and Housing Programs
Shelters and other housing programs are important for people experiencing IPV. Women who have experienced IPV are at greater risk of experiencing homelessness and housing insecurity than women who have not (Adams et al., 2021; Gilroy et al., 2016; Pavao et al., 2007). Housing insecurity has been linked to worse outcomes with regard to physical safety and mental health (Gilroy et al., 2016; Rollins et al., 2012). Shelters also allow people experiencing IPV to separate from the person perpetrating the violence.
Critical IPV services are also provided in shelters and other housing programs, spanning emergency, transitional, and permanent housing. Advocacy services are often delivered through IPV shelters and housing programs (Shorey et al., 2014). Although leaders in the field have defined these services as critical in the response to IPV, more studies are needed to evaluate the impact of housing interventions on outcomes for people experiencing IPV (Klein et al., 2021).
Nurse-Family Partnership Home Visit Programs
Nurse–Family Partnership programs are home visitation programs in which nurses provide health promotion interventions for new mothers. This model has positively affected infants and mothers, including showing promise for reducing IPV (Olds and Yost, 2020). Various adaptations of nurse-led interventions delivered at home for mothers, including the Domestic Violence Enhanced Home Visitation Program, have demonstrated promise for improving identification and intervention for mothers experiencing IPV and reducing IPV over time (Burnett et al., 2021; Sharps et al., 2016).
School- and College-Based Health Centers
An estimated 6.3 million students have received services from a school-based health center (SBHC), most of which are located in underserved, low-resource neighborhoods (Love et al., 2019). Features of these centers include access to services for students without health insurance, confidential psychosocial assessments occur routinely, and students can connect with other students through peer-to-peer outreach (Britto et al., 2001; Clayton et al., 2010; Gibson et al., 2013; Juszczak et al., 2003). Adolescent relationship abuse is prevalent among youth seeking care in SBHCs (Miller et al., 2015). IPV is not uncommon among women attending college (Coker et al., 2016; Sutherland et al., 2021). Many of these women seek care at college health and counseling centers (Grace et al., 2023). College health and counseling centers are also helpful as a confidential setting for offering preventive services and connecting survivors to supports and safety.
Federally Supported Care Settings
Several federal programs have been established to meet the needs of under-resourced communities. These include Federally Qualified Health Centers and centers for family planning and reproductive health supported by Title X provisions.
Federally Qualified Health Centers
Federally Qualified Health Centers (FQHCs) are critical sites in the health care safety net. Typically, FQHCs serve medically underserved areas or populations and offer services on a sliding scale to individuals who have low incomes or are uninsured (HRSA, 2023b). In 2022, 66 percent of patients seen at HRSA health centers had incomes at or below the federal poverty level, and 18 percent were uninsured (HRSA, 2023b). FQHCs offer a range of primary health care services to adults and children, referrals to specialty care, and support services such as health education, translation, and transportation that address the social determinants of health. Many FQHCs provide dental care, mental health services, and substance use services. Services may be provided for free or on a sliding scale basis. HRSA requires that FQHCs be governed by a board of directors that includes community members. HRSA’s strategy for addressing IPV identifies four priorities for staff and its network of clinics:
- Train the health care and public health workforce to address IPV at community and health-system levels;
- Develop partnerships to raise awareness about IPV within HRSA and the U.S. Department of Health and Human Services (HHS);
- Increase access to high-quality IPV-informed health care services across all populations; and
- Address gaps in knowledge about IPV risks, impacts, and interventions (HRSA, 2023a).
Additionally, one of HRSA’s National Training and Technical Assistance Partners, Health Partners on IPV and Exploitation, offers training to health centers about addressing IPV.4 The training addresses providing trauma-informed services, developing partnerships, policy development, IPV prevention and identification, and referral to support services. Training is also available about IPV among specific populations, including adolescents, pregnant people, victims of human trafficking, and unhoused individuals.
Title X Network of Clinicians
Title X5 is the federal program administered by the Office of Population Affairs (OPA) that supports the delivery of family planning and related health services to individuals with low incomes. The program is implemented through grants awarded to various organizations, including health departments, family planning clinics, community health centers, and nonprofit agencies, which award subgrants to family planning clinics and other entities that offer family planning services for free or on a sliding scale. In 2021, Title X funds supported more than 3,000 service sites across the United States (Fowler et al., 2022).
Title X–funded clinics serve a diverse population and include many historically underserved communities. Nationally in 2021, 85 percent (1,419,731) of the program’s family planning clients were female, 65 percent (1,080,935) had incomes below the poverty level, over one-third (36 percent; 594,416) were uninsured, and 15 percent (255,554) were under 20 years of age. In 2021, more than half (58 percent; 958,762) of clients were White, 25 percent (418,397) were Black, 2 percent (30,637) were Asian, 1 percent (19,349) were American Indian/Alaska Native, and 1 percent (13,195) were Native Hawaiian or Pacific Islander. In addition, 38 percent (626,784) were Hispanic or Latino (OASH, 2022).
The tenets of the Title X program include maintaining confidentiality, advancing equity, and delivering client-centered and trauma-informed care (HHS, 2021). These tenets are consistent with key characteristics of quality IPV-related care. In addition to funding the delivery of family planning
___________________
4 https://healthpartnersipve.org/ (accessed August 28, 2023).
5 Title X of the Public Health Service Act 42 USC § 300 to 300a-6.
services, the OPA and the Centers for Disease Control and Prevention (CDC) developed the Quality Family Planning Services Recommendations, which provide clinical recommendations for family planning and related services (Gavin et al., 2017). The guidelines specifically recommend that clinicians consider the impact of IPV on contraceptive use, access, and needs (Gavin et al., 2017). Oral contraceptives are the most commonly used reversible contraceptive among women in the United States, and extended supply has been associated with higher continuation rates and lower rates of unintended pregnancy (Judge-Golden et al., 2019; White and Westhoff, 2011).
Staff at family planning clinics often have extensive experience caring for people who have experienced IPV, particularly sexual violence and reproductive coercion. Title X family planning clinics provide a range of essential health care services related to IPV, including FDA-approved contraceptive methods and contraceptive counseling; cervical cancer screening; testing, referrals, and prevention education for STIs and HIV; and diagnosis, counseling, and referrals for pregnancy (Fowler et al., 2022). Smith and colleagues conducted a scoping review and analysis of data from the Colorado Family Planning Initiative (CFPI) and the Colorado National Violent Deaths Reporting System from 2009–2015 (Smith et al., 2023). This analysis demonstrated promising findings for a family planning centered approach to reducing the rates of intimate partner homicide related to unplanned pregnancy (Smith et al., 2023). From 2009 to 2015, the CFPI provided 36,762 long-acting reversible contraceptives (LARCs) to women. LARCs are discrete, tamper resistant, and usable without coordination from other partners. Smith and colleagues (2023) found that, over the same time period, intimate partner homicide in Colorado had a net decline as compared with the 5 years prior to LARC distribution (Smith et al., 2023).
EXISTING AND PROMISING MODELS FOR INTIMATE PARTNER VIOLENCE CARE
Telehealth and Digital Interventions
Telehealth describes health care services delivered using communication technology to supplement or replace in-person visits. These technologies most often include telephone, e-mail, or video, which can be synchronous (i.e., occur at the same time for all participants) or asynchronous (i.e., occur at different times). While telehealth has been well integrated into various health care practices, its use expanded greatly during the COVID-19 pandemic (Acharya et al., 2023; McBain et al., 2023; Uscher-Pines et al., 2023). This increase in telehealth use was also demonstrated for IPV services (Krishnamurti et al., 2021).
Telehealth can have a role in providing IPV care when privacy and safety are assured. A recent systematic review of trials comparing interventions for IPV services using telehealth versus usual care showed similar outcomes for each group. The systematic review included 2,663 women in six randomized controlled trials (RCTs) and one nonrandomized trial investigating telehealth strategies for delivery of women’s health and IPV care in the United States (Cantor et al., 2023). The trials enrolled women with positive responses to IPV screening questions or recent IPV experiences (Ford-Gilboe et al., 2020; Gilbert et al., 2015; Glass et al., 2017; Hegarty et al., 2019; Koziol-McLain et al., 2018; McFarlane et al., 2004; Saftlas et al., 2014). Telehealth interventions varied across trials and included personalized online tools, interactive websites, or telephone-based support to supplement or replace in-person care for IPV (Ford-Gilboe et al., 2020; Gilbert et al., 2015: Glass et al., 2017; Hegarty et al., 2019; Koziol-McLain et al., 2018; McFarlane et al., 2004; Saftlas et al., 2014). The outcomes also varied across trials. Compared with usual care, telehealth interventions for IPV services resulted in similar rates of repeat IPV, symptoms of depression, fear of partner, coercive control, self-efficacy, post-traumatic stress disorder, and safety behaviors in studies assessing these outcomes (Cantor et al., 2023). The studies did not adequately evaluate potential harms, but they did note barriers to telehealth including limited internet access, digital literacy, technical challenges, and confidentiality concerns (Cantor et al., 2023). Given the small body of studies in this area, more research is needed to understand access barriers and safety concerns among women experiencing IPV when accessing telehealth medical services.
Futures Without Violence offers a guide for community health centers and advocacy programs about how to best prepare for a telehealth visit while keeping the continuity of care for people who have or are experiencing IPV.6 The guidance highlights preparing a script to integrate information about IPV throughout the call, prioritizing confidentiality, offering universal education, and offering encouragement as key factors to incorporate during a visit (Futures Without Violence, n.d.). Telehealth visits may not always be a safe place to discuss IPV as others may be in the same room or able to hear the conversation. Futures Without Violence offers some suggested language to help navigate conversations and ensure safety for the patient (Futures Without Violence, n.d.).
___________________
6 https://healthpartnersipve.org/telehealth-covid-19-intimate-partner-violence-and-human-trafficking/ (accessed August 25, 2023).
App-Based Interventions for Identifying Risk and Connecting to Resources
App-based interventions are emerging as an important strategy for addressing IPV. A longitudinal study of an app-based screening and safety planning program, MyPlan, found it to be effective for improving safety behaviors and reducing IPV among young adults over time (Glass et al., 2022). During the COVID-19 pandemic, when individuals needed to shelter in place, an app-based intervention that screened for IPV and provided support services appeared to show promise (Krishnamurti et al., 2021).
Programs in Primary Care Settings
Health Care Can Change From Within is a systems-change intervention aimed at improving the identification of women experiencing IPV and caring for their health and well-being (Hamberger et al., 2014). Results of an 18-month longitudinal study of the intervention among women patients seeking care in four different Midwestern primary care clinics showed that the intervention increased IPV inquiry, discussion, and disclosure compared with usual care. Women in intervention clinics made fewer doctor visits and received more prescriptions over time. Notably, researchers did not observe between group differences in levels of physical abuse, psychological abuse, use of safety behaviors, connection to the community, patient-reported satisfaction, or quality of health. However, over the course of the study, both the intervention and usual care groups showed a significant increase in safety behaviors and were less likely to experience severe physical or minor violence, suggesting that participating in the research may have affected both groups (Hamberger et al., 2014).
Multisector Partnerships and Coordinated Community Responses
Multisector partnerships are vital for addressing major public health problems and are relevant for addressing IPV. Multisector partnerships with a clear purpose and structures that support coordination, information sharing, and evaluation have been found to be central to effective public health efforts (Wiggins et al., 2021).
Several multisector models that address IPV appear promising. There are indications that this approach fosters survivorship and growth among people experiencing IPV (Gwinn et al., 2007; Hellman et al., 2021). These vary from local to statewide efforts and are intended to improve the coordination of needed services for individuals and families affected by IPV. Often referred to as Coordinated Community Responses (CCRs), these include the critical role of advocates who ensure that clients have access to a wide
range of services, such as advocacy, shelter, and legal protection (Shorey et al., 2014). Although there is no standard protocol for CCRs, they typically involve a coordinating council with representatives from across sectors and services that form relationships among one another and can identify and fill in service gaps (Shorey et al., 2014). Similarly, statewide initiatives, such as Project Catalyst, have engaged leaders from primary care, public health, and domestic violence coalitions and have demonstrated improved collaboration between health centers and domestic violence agencies (Brown et al., 2023).7
Domestic Violence and Health Care Partnership
The Domestic Violence and Health Care Partnership initiative, sponsored by Blue Shield of CA Foundation and Futures Without Violence, offers a model for collaboration between community health care centers (including FQHCs) and victim service agencies.8 The demonstration project focused on strategies for improving the health care delivery system’s capacity to collaborate with victim service agencies to address IPV. This included formal referral processes for patients identified in health care settings to rapidly connect with advocacy services and for survivors seeking care in advocacy agencies to receive health care expeditiously (Miller-Walfish et al., 2021).
Integrating Intimate Partner Violence Care into HIV Clinics
Integrating IPV screening, care, and delivery services into HIV clinics can facilitate reductions in repeat or co-occurring victimization (Marshall et al., 2018). Recognizing the critical need for integrated IPV–HIV services, in 2012 the White House established an Interagency Federal Working Group to address issues involving the intersection of IPV and HIV prevention and care (White House, 2013). One of the working group’s tasks was to coordinate government agency efforts to integrate sexual and reproductive health services with gender-based violence services and HIV/AIDS services (White House, 2013).
Currently, few states have guidelines for integrating IPV screening into HIV prevention and care. Published guidelines set forth by the New York State Department of Health indicate that domestic violence risk assessment is a standard of care. This guidance notes that “domestic violence as a standard of care” means that discussing domestic violence is encouraged
___________________
7 https://www.futureswithoutviolence.org/health-2/project-catalyst/ (accessed August 28, 2023).
8 https://blueshieldcafoundation.org/grants/legacy-projects/domestic-violence-health-care-partnerships-0 (accessed August 28, 2023).
during pretest counseling for HIV and domestic violence risk assessment is required during post-test counseling of HIV-infected individuals (NYSDOH, 2013). However, the extent to which these guidelines have been implemented or evaluated is unknown.
The Women’s HIV Program at the University of California, San Francisco is one of the few HIV clinics that provide integrated IPV–HIV care guided by trauma-informed care principles identified by the Center for Health Care Strategies (Center for Health Care Strategies, 2018; Dawson-Rose et al., 2019). The delivery of trauma-informed care includes the below core components:
- A foundation based in trauma-informed principles and a team approach,
- An empowering environment that supports a sense of calm and safety,
- Education about the health effects of current and past trauma, and
- Inquiry about and response to recent and prior trauma that integrates on-site or community-based resources and care (Machtinger et al., 2019).
Patients in the Women’s HIV Program receive universal education about healthy and unhealthy relationships, how IPV affects health, and resources such as a safety card created by Futures Without Violence. Patients who disclose being in an abusive relationship are immediately seen by a clinic social worker who can create a safety plan and connect them with IPV resources as needed. Researchers are still collecting and analyzing data to determine the outcomes of this unique care model.
Some of the limited intervention efforts that have taken place to date have provided domestic violence advocates with HIV prevention knowledge to facilitate prevention and care for women with experiences of IPV. An example of one such effort was a small pilot study of a group-based two-session HIV prevention education intervention for domestic violence advocates conducted in Mississippi (Willie et al., 2022). Key components of the intervention included education on the IPV–HIV relationship, HIV prevention for IPV survivors (e.g., pre-exposure prophylaxis [PrEP]), the barriers that women with experiences of IPV face, and the benefits of PrEP for women with experiences of IPV (Willie et al., 2022). Compared with pre-intervention, investigators found improvements both immediately and at 3 months post-intervention in advocates’ knowledge about PrEP and reported self-efficacy for several HIV prevention and information-sharing behaviors all increased (Willie et al., 2022). However, due to high staff turnover, while the pilot began with 25 participants, only 9 were retained by the 3-month post-intervention point.
Veterans Administration Intimate Partner Violence Program
The Veterans Health Administration (VHA) began formally encouraging IPV screening in Veterans Affairs (VA) medical centers in 2014 and issued a national directive calling for routine IPV screening and provision of interventions throughout VHA facilities in 2019 (Miller et al., 2022; Rossi et al., 2020). The VA’s Intimate Partner Violence Assistance Program (IPVAP), which began in 2014, provides comprehensive, trauma-informed, recovery-oriented services to veterans, their intimate partners, and VA staff experiencing IPV (Iverson et al., 2022; Rossi et al., 2020). Connecting all individuals who screen positive for IPV in VHA facilities with interventions and supports is a key component of IPVAP (Iverson et al., 2022; Rossi et al., 2020).
All women veterans seeking health services in a VA center are asked about IPV using the five item Extended-Hurt/Insult/Threaten/Scream (E-HITS) screener along with a sexual violence screening question (Miller et al., 2022). A 2022 study analyzing VHA administrative data from 2014 to 2020 investigated the reach of the program and the prevalence of positive screens among women ages 18–44 (Miller et al., 2022). The analysis found that the deployment of IPVAP was associated with a steady increase in the number of women screened for IPV in VHA primary care settings (Miller et al., 2022). The analysis also found that the average percentage of women aged 18–44 who screened positive was 8.1 percent (Miller et al., 2022).
Each VA facility and most units within large VA facilities have an IPV Assistance Program Coordinator (referred to as an IPV Champion)—a staff member assigned to make sure staff are trained in the use of the protocol, help clinicians with particularly challenging cases, and compile reports of screening (Adjognon et al., 2021; Iverson et al., 2019, 2022). At early adoption sites, these IPV Champions were integral in implementing the IPVAP, particularly the screening component (Adjognon et al., 2021; Iverson et al., 2019). In addition to training and supporting staff, IPV Champions develop relationships with community-based organizations, which develops the resources available for veterans experiencing IPV (Adjognon et al., 2021). They also collaborate with their counterparts across the VA to develop clinical guidelines and adapt risk assessment and management processes for diverse populations, including groups minoritized by race, ethnicity, lesbian, gay, bisexual, transgender, or queer status, and immigration status (Adjognon et al., 2021). Studies investigating implementation of IPVAP across VA facilities have highlighted the IPV Champion as a key factor in its success (Adjognon et al., 2021; Rossi et al., 2020).
Recovering from IPV through Strengths and Empowerment (RISE) is an evidence-based, trauma-informed, person-centered, brief psychosocial counseling intervention for people experiencing IPV that has been piloted
at several VHA facilities (Iverson et al., 2022). RISE focuses on understanding individuals’ values and supporting them in improving their general self-efficacy and personal empowerment. It is designed to maximize flexibility, choice, and autonomy to better meet both patient and clinician needs (Iverson et al., 2022). Modules in the intervention include safety planning, education about the warning signs of IPV and its adverse health effects, coping and self-care skills, building social support, improving decision-making skills, and connecting to resources (Iverson et al., 2022). Evaluations of the pilot program in the literature have had promising findings. A 2022 analysis of data from a cohort of 45 patients who participated in the pilot program found a statistically significant decrease in depressive symptoms and high participant satisfaction scores (Iverson et al., 2022). A randomized clinical trial investigated outcomes of RISE versus “enhanced care as usual” among 59 women recruited from an urban VHA hospital (Iverson et al., 2021). Women who participated in RISE had greater increases in empowerment and self-efficacy than those who received enhanced care as usual (Iverson et al., 2021).
Care Models for Intimate Partner Violence in the Perinatal Period
Women experiencing IPV in the perinatal period require many of the essential health care services related to IPV. Women experiencing perinatal IPV need additional obstetric care and specialty medical care to address the multiple adverse health effects of experiencing IPV in the perinatal period. Some adverse health effects associated with perinatal IPV are life threatening, such as preeclampsia, and require emergency medical services. These women also need treatment for traumatic physical injuries due to IPV. Women experiencing IPV in the perinatal period also require mental health care to address the psychological effects of perinatal IPV. Referrals to treatments, interventions, and additional resources are imperative during the perinatal period, as people are most likely to adopt interventions when receiving perinatal care as compared with other care contexts (Hahn et al., 2018).
Perinatal home visit programs using interventions focused on Dutton’s empowerment model have shown promising results in decreasing the incidence of IPV. One example is the Domestic Violence Enhanced Home Visitation Program (DOVE) (Sharps et al., 2016). The DOVE program is a brochure-based intervention developed to be integrated and implemented within existing home visit programs. Nurses or community health workers are trained to use the DOVE brochure to share information and resources about IPV during their home visits and can modify this intervention to meet the individual woman’s needs. The DOVE brochure includes educational information about the cycle of violence; the Danger Assessment,
which assesses the woman’s risk for intimate partner homicide; options available to the woman; safety planning information that is consistent with the context and level of danger; community-specific IPV resources; and national hotline information (Sharps et al., 2016). A pragmatic trial of the DOVE intervention found that participants in the group that received the DOVE intervention experienced a greater decrease in IPV than those that did not receive the DOVE intervention (Sharps et al., 2016). The greater reduction in IPV was sustained at 2 years postpartum, despite the intervention ending 3 months postpartum (Sharps et al., 2016). Prior research on home visit programs found that the nurses and community health workers felt underprepared to assist a woman if she disclosed that she was experiencing IPV (Dyer and Abildsco, 2019). Programs such as DOVE offer needed guidance for those conducting home visits, providing them with resources for supporting the pregnant or postpartum person experiencing IPV.
Existing Intimate Partner Violence Prevention Guidance and Strategies
CDC developed evidence-based prevention strategies with the greatest potential to prevent IPV for communities and states (Table 5-2) (Niolon et al., 2017). These include strategies for teaching safe and healthy relationship skills and engaging influential adults and peers in IPV education and prevention programs. Strategies for disrupting the developmental pathway toward IPV include early childhood programs, parenting programs, and
TABLE 5-2 CDC IPV Prevention Strategies
| Risk or Protective Factors* | Strategy | Approach |
|---|---|---|
|
Teach safe and healthy relationship skills |
|
| Engage influential adults and peers |
|
|
| Risk or Protective Factors* | Strategy | Approach |
|---|---|---|
|
Disrupt the developmental pathway toward partner violence |
|
|
Create protective environments |
|
|
Strengthen economic supports for families |
|
|
Support survivors to increase safety and lessen harms |
|
*Risk and protective factors may apply to multiple strategies.
SOURCE: Niolon et al. (2017).
treatment for at-risk children, youth, and families. Strategies for creating protective environments, including schools, work, and neighborhoods, could reduce IPV risk related to established risk factors. Services for supporting survivors that increase safety and reduce harm provide an additional secondary prevention strategy. Together, these strategies provide a comprehensive plan for IPV prevention that particularly targets prevention at the community level.
Promoting Healthy Families and Communities
Primary prevention of IPV is crucial for preventing IPV and its consequences across the lifespan and for promoting healthy families and communities. One of the key ways to accomplish this is by promoting healthy, respectful, and nonviolent relationships. Initiatives in this area include social–emotional learning programs for youth and programs that focus on forming healthy couple relationships before violence occurs. Safe Dates is a school-based program designed to promote healthy relationships that in a randomized controlled trial (RCT) was found to reduce the likelihood of engaging in teen dating violence among participants without a history of engaging in abuse and prevent teen relationship violence (Foshee et al., 2004). Expect Respect Support Groups is another evidence-based intervention designed for teens who are at high risk for teen relationship violence and have a history of exposure to violence (Reidy et al., 2017). A study of the program in 36 Texas high schools found that among boys, participation in the program was associated with a decrease in psychological and sexual teen dating violence (Reidy et al., 2017). Healthy relationship programs for couples, such as the Prevention and Relationship Enhancement Program, can be helpful for addressing factors such as relationship satisfaction and anger management among adult couples and have shown evidence of preventing later-life IPV (Anderson et al., 2013; Braithwaite and Fincham, 2014; Markman et al., 1993).
There are several promising programs targeted at bystander education. One example is Coaching Boys Into Men, a program that trained high school coaches to educate their male athletes in grades 9–12 in healthy relationship skills (Miller et al., 2013). A cluster-randomized controlled trial of 2,006 student athletes at 16 California schools found that athletes who received the coach-led education reported they were less likely to laugh at or go along with peers’ abusive behaviors. However, the study did not find a difference between the intervention and control group for intention to intervene in observed IPV, recognition of abusive behaviors, or gender-equitable attitudes (Miller et al., 2013). Bystander programs among college students, such as Bring in the Bystander and the Green Dot program, aim to educate and empower college students to engage in reactive and proactive responses to IPV and to reduce the likelihood of assault (Coker et al.,
2015; Moynihan et al., 2015). Analyses of the outcomes of these programs have found mixed results, particularly in long-term follow ups. However, lessons learned through studies of these programs represent an opportunity for future intervention development.
Results from research conducted outside the United States have had promising findings regarding the effect of interventions at the community level that focus on addressing the effect of gender inequities on IPV prevalence. For example, the SASA! Study, an RCT conducted in Uganda that investigated a multilevel community intervention designed to prevent violence against women and reduce HIV risk, found that after 3 years of intervention programming, women in participating communities were less likely to report experiencing physical IPV in the past year (Abramsky et al., 2016).
Healing-Centered Engagement
Healing-centered engagement (HCE) is a holistic approach that emphasizes the importance of culture to well-being and integrates empowering the individual that has experienced trauma to understand their strengths and take an active role in their healing with an understanding of healing as a collective experience (Gupta, 2021). HCE approaches have shown promise in studies of application of the intervention with youth and adults from minoritized populations (Condon et al., 2022; Maleku, et al., 2022; Pearce et al., 2019). Clinicians and other frontline health workers could benefit from learning about a community’s history, its collective trauma experiences, and how to use strengths-based approaches to encourage patients and clients to problem solve together. A healing-centered approach that focuses on universal education shifts away from an overemphasis on disclosure to building a trusting relationship with the patient that is compassionate, relational, and centers the autonomy and strengths of patients.
Universal Prevention and Harm Reduction Education
Universal prevention and harm reduction education related to IPV during clinical encounters shifts the emphasis away from eliciting a disclosure and mitigates against the assumption that a “no” response to a screening question about abuse means the patient has not experienced or is not currently experiencing violent or controlling behaviors. This approach has been evaluated in reproductive, college, and adolescent health settings and has been shown to increase patients’ knowledge of resources and strategies for harm reduction and to reduce reproductive coercion and abuse victimization among adolescent and young adult women (Miller et al., 2011, 2015, 2016, 2020).
Firearm Violence Prevention
Women are more likely to be shot and killed by a male intimate partner than they are to be killed by a stranger (Sorenson, 2017; Sorenson and Schut, 2018). A 2020 meta-analysis of results from 17 studies investigating risk factors for intimate partner homicide found that the greatest risk factor for women to experience intimate partner homicide was the person engaging in IPV having direct access to a firearm (Spencer and Stith, 2020). Extreme-risk protection orders, also known as red flag laws, may provide an avenue for health professionals to intervene in situations where they determine that an individual poses a significant risk of IPV-related gun violence. In Maryland,9 Colorado,10 Hawaii,11 Michigan,12 and New York,13 as well as the District of Columbia,14 a medical, mental health, or other health professional may initiate a court petition that could ultimately authorize law enforcement officials to temporarily remove firearms from a person who poses a significant danger of firearm violence to themselves or others.15 Requirements governing who is qualified to file a petition vary by state. For example, to initiate a petition in Maryland, the clinician must have examined the individual who poses a threat.16 To initiate a petition in Colorado, the clinician must have examined either the individual who poses a threat or that individual’s child within 6 months. In the District of Columbia, any mental health professional who is in a position to state facts in support of the risk assessment may initiate a petition.17 In several other states, health professionals are ineligible to file a petition but may advise patients of their right to do so.
Preventing Intimate Partner Violence Among Adolescents
Efficacious, easily implementable, and scalable interventions for preventing adolescent relationship abuse are essential for promoting adolescent health and wellness (Piolanti and Foran, 2022). Core components of evidence-based and research-informed IPV prevention programs for adolescents include gender equity transformative programming, adult social supports and mentoring, parent–adolescent communication, promoting social norms to protect against violence, bystander interventions, and creating
___________________
9 Maryland Code Ann. Pub. Safety § 5-601(e).
10 Colorado Revised Statutes, title 13, article 14.5.
11 Hawaii Revised Statutes §134-67.
12 Michigan Public Act 38 of 2023.
13 New York Civil Practice Law and Rules article 63-a § 6340-6348.
14 District of Columbia Code § 7-2510.
15 List of states and laws current as of August 2023.
16 Maryland Code Ann. Pub. Safety § 5-601(e).
17 District of Columbia Code § 7-2510.
protective environments (Finnie et al., 2022; Niolon et al., 2019). Several interventions and strategies have demonstrated positive effects, including family-, community-, and school-based prevention programs (Basile et al., 2016; Niolon et al., 2019). Open parent–adolescent communication is associated with less exposure to and use of adolescent relationship abuse (Kast et al., 2016; Ombayo et al., 2019). School- and clinic-based education and assessment programs can increase youth recognition of abusive behaviors (Finnie et al., 2022; Foshee et al., 2004). The School Health Center Healthy Adolescent Relationships Program (SHARP) is a provider-delivered, brief universal education and counseling intervention created to be used with all students seeking care in school-based health centers (Miller et al., 2015). The intervention was designed to be inclusive of all gender and sexual identities and clinic visit types, and it addresses a range of adolescent relationship abuse, including cyber dating abuse and reproductive coercion (Miller et al., 2015). A study of 939 students aged 14–19 found that those who received the SHARP intervention and filled out surveys 3 months after a clinic visit demonstrated greater recognition of sexual coercion and reduced victimization (Miller et al., 2015).
ADDRESSING HEALTH DISPARITIES AND BARRIERS SPECIFIC TO PEOPLE EXPERIENCING INTIMATE PARTNER VIOLENCE
Individual-Level Barriers
Individual-level barriers—sociodemographic characteristics that intersect culture and behavior—affect the delivery of essential services for IPV. Women in some communities are often pressured to maintain the privacy of IPV experiences to avoid community shame and adhere to traditional gender norms. This barrier is compounded by insufficient accessibility of IPV resources within those communities (Schmidt et al., 2023). Nuanced cultural differences within racial and ethnic groups (e.g., African American and Caribbean Black women) can hinder access to IPV services. Women who are immigrants or refugees often express confidentiality concerns related to inadequate access to linguistically appropriate services (Guruge and Humphreys, 2009). Women who are immigrants also experience confusion over their legal rights, social isolation, and disparities in economic and social resources (between a woman and her partner), further impeding IPV service use (Stockman et al., 2015). Intersecting racial, ethnic, and gender stereotypes (e.g., the strong Black woman) contribute to decreased use of formal essential services (Bent-Goodley, 2007; Monterrosa, 2021). Cultural stigmas or ideologies that delegitimize experiences of IPV and that promote acceptance of violence as a norm combined with various stereotypes collectively reduce the uptake of services (Overstreet and Quinn, 2013; Stockman et al., 2014).
General feelings of social disconnectedness and hopelessness can also serve as barriers for Black women with IPV experiences who also have had a history of involvement with the legal system (Gutowski et al., 2023). The interaction of behavioral health problems (e.g., substance use) with IPV may create additional barriers to engagement with needed services (Ponce et al., 2014).
Some women experiencing IPV distrust service organizations, the health care system, and the legal system, among other essential services. This is often rooted in intergenerational trauma related to historical events involving abuse and atrocities against certain populations (e.g., forced sterilization among American Indian/Alaska Native women) and discriminatory practices embedded in services and service delivery (Robinson et al., 2021; Stockman et al., 2015). In general, a less representative physician workforce can reduce patient trust in the medical system and in their personal physician. This, in turn, may lead to worse health outcomes (Mcintosh-Clarke et al., 2019; Schoenthaler et al, 2014; Snyder et al., 2023). IPV services that are culturally specific or culturally tailored are not broadly available (Guruge and Humphreys, 2009; Kulkarni, 2018). Moreover, access to specialized IPV services is lacking for marginalized women, including those with disabilities (e.g., the deaf community) and women who identify as LBTQ+ (Calton et al., 2016; Mastrocinque et al., 2017). Client/patient–provider communication can also be less than optimal for women, which can create barriers to both disclosure and connection to the essential health care services that match their needs (Stockman et al., 2015).
LBTQ+ women face unique barriers while seeking essential services for IPV. Stigma can present a barrier to disclosure (Ard and Makadon, 2011; Calton et al., 2016; Scheer et al., 2020). In particular, the fear of being outed, or having their identity revealed to others such as family, friends, coworkers, or medical professionals, may pose a strong barrier to disclosure (Ollen et al., 2017; Porsch et al., 2022; Scheer et al., 2023). This stigma is sometimes reinforced via bias from physicians and other resources, which reduces both disclosure and the effectiveness of services (Calton et al., 2016; Guadalupe-Diaz and Jasinski, 2017).
Transgender women also report stigma and discrimination as barriers to disclosing IPV (Gray et al., 2023; Kurdyla et al., 2021). In particular, transgender women have reported experiencing discrimination when seeking access to gendered shelters (Ezie, 2023; James et al., 2016). They are far less likely to report or seek help from help-giving resources, including police officers, hotlines, shelters, or legal support when compared to cisgendered individuals. When reporting or seeking help after an IPV experience, transgender women are far more likely to report to friends, family, or a mental health professional (Kurdyla et al., 2021).
Other individual-level factors may influence access to IPV care. For example, given that animal maltreatment is a strategy that partners
engaging in IPV use to control and intimidate their partners, concern for the safety of pets can be a barrier to disclosure and care seeking. Access to shelters that allow women experiencing IPV to bring their pets can reduce this barrier (Campbell and Glass, 2009; Collins et al., 2018). Concern surrounding animal abuse can delay women from entering a shelter. A study conducted in Utah found that 22.8 percent (N=101, n=23) of women who had entered a shelter delayed going due to concern for their pets (Ascione et al., 2007). Some studies have noted that women have left shelters to check on pets or returned to abusive relationships because their pet was still with the partner who engaged in IPV (Barrett et al., 2020). An analysis of data from a Canadian survey of 128 human services professionals and 43 veterinarians and other animal welfare professionals noted that respondents emphasized the need for pet-friendly IPV shelters and long-term housing options (Giesbrecht, 2022). Having a safety plan and alternative resources for housing a pet is an important barrier to be addressed when women are seeking shelter services (Hageman et al., 2018).
Additionally, there is a general lack of availability and accessibility of essential IPV services for women who are homeless or marginally housed, reside in rural geographic or low-income areas, or reside in tribal communities or reservations (Edwards, 2015; Jock et al., 2022; Ponce et al., 2014; Rodriguez et al., 2009). Lack of resources, including transportation and child care, can pose additional challenges to accessing essential IPV services, further contributing to preexisting disparities (Robinson et al., 2021; Wadsworth et al., 2018). IPV care approaches that prioritize women’s sense of agency, culture, and mutual respect while acknowledging experiences of cumulative trauma can help reduce their barriers to accessing IPV-related care.
Health Care Deserts
Health care provider maldistribution, in which the distribution of clinicians does not match the health care needs of a geographic area, has led to health care deserts across the United States. These health care deserts have created additional barriers for people experiencing IPV to access needed care.
Primary Care Clinicians
A large body of literature reports that the nation faces a worsening shortage in the availability of primary care clinicians, including physicians and nurses, who are major providers of preventive services, including screening and education for IPV. The challenges and burnout presented by the COVID-19 pandemic have hastened and exacerbated workforce shortages, which have been building for several years.
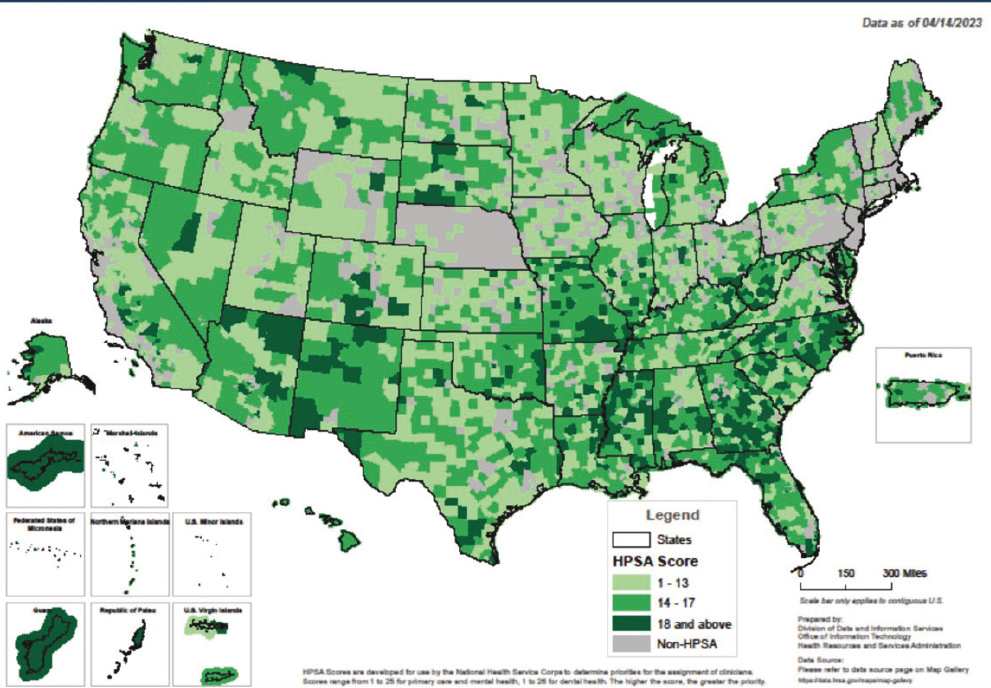
SOURCE: HRSA (2023e).
HRSA (2023a) estimates that 100 million people live in a federally designated Health Professional Shortage Area for primary care services, and these gaps are expected to grow (see Figure 5-3). HRSA (2023d) projects that between 2020 and 2035, the supply of primary care physicians will grow by 12 percent, but demand will grow by 16 percent.18 HRSA projects a 13 percent increase in supply for general internal physicians, short of the expected 24 percent increase in demand19 between 2020 and 2035 (HRSA, 2023d). The Bureau of Labor Statistics projects approximately 193,100 job openings for registered nurses annually between 2022 and 2032 (BLS, 2023). Clinician shortages are spread unevenly and are particularly pronounced in rural areas, which have had longstanding challenges with provider recruitment and retention as well as with hospital closures.
___________________
18 Projection data as of September 13, 2023.
19 Projection data as of September 13, 2023.
Maternity Care Professionals
The March of Dimes categorizes maternity care deserts as counties that have no hospitals or birth centers offering obstetric care and no obstetricians/gynecologists (OB-GYNs) or certified nurse midwives providing deliveries (Brigance et al., 2022). Their analysis used data from HRSA, the CDC National Center for Health Statistics, and the U.S. Census Bureau (see Figure 5-4). In 2022 approximately one-third (35.6 percent) of counties in the United States were classified as maternity care deserts, and another 11.9 percent were considered to have low access to maternity care (Brigance et al., 2022). As with primary care, shortages in the perinatal workforce are particularly stark in rural communities, especially the most remote areas. More than half of rural counties do not have obstetric services, and more than half of women who live in rural communities must travel at least 30 minutes to reach a hospital that offers obstetric care services (Brigance et al., 2022; Hung et al., 2017). Gaps in maternity care have been associated with increases in emergency department births and preterm births (Kozhimannil et al., 2020; Wallace et al., 2021).
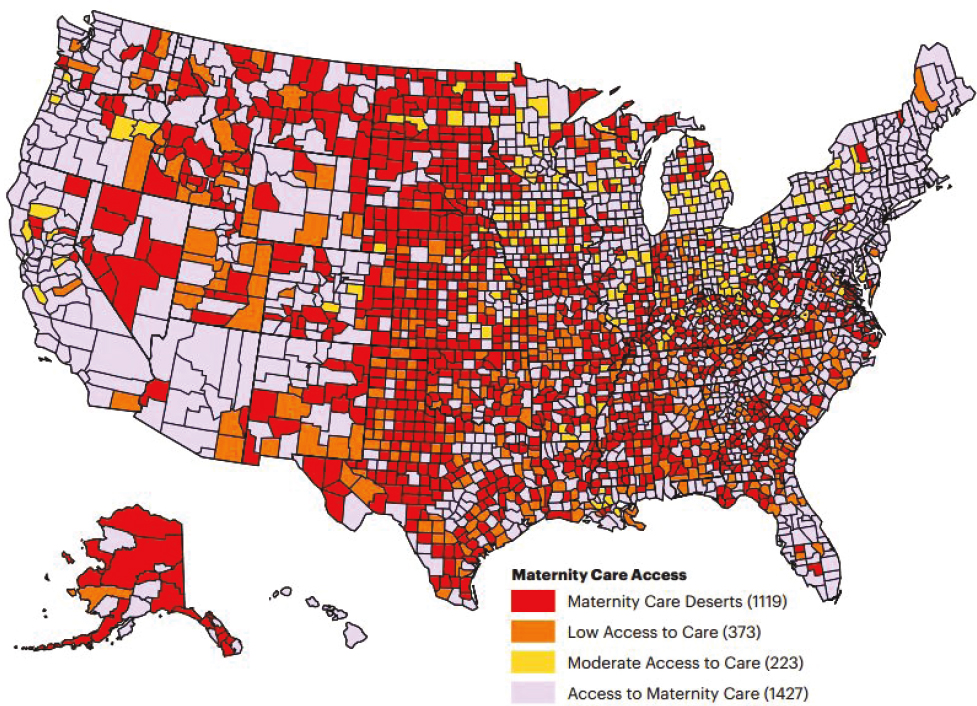
SOURCE: Brigance, C., R. Lucas, E. Jones, A. Davis, M. Oinuma, K. Mishkin, and Z. Henderson. 2022. Nowhere to Go: Maternity Care Deserts Across the U.S. (Report No. 3). March of Dimes. https://www.marchofdimes.org/research/maternity-care-deserts-report.aspx (accessed August 25, 2023).
Sexual and Reproductive Health Care Professionals
In some regions there are major shortages and gaps in the availability and distribution of clinicians providing the full range of sexual and reproductive health care. Contraception is a fundamental element of women’s health care, and federal law20 requires full coverage of contraceptives for those with private insurance or Medicaid. Additionally, the federal Title X program, administered by the Office of Population Affairs, provides free and low-cost contraceptives at approximately 3,000 sites across the United States (Fowler et al., 2022). Despite these protections, not all individuals have ready access to the full range of contraceptive options. A study analyzing data from 2019 found that many counties and states in the United States lack a clinic that provides comprehensive contraception services under Title X (Smith et al., 2022). This translates to millions without access to this care (Smith et al., 2022). The rapidly changing regulatory environment in the wake of the Supreme Court ruling in Dobbs v. Jackson Women’s Health Organization21 makes it challenging to estimate how many people lack access to comprehensive contraception services under Title X at the time of this report. For women who are uninsured, most of whom are low-income, out-of-pocket costs may make contraception unaffordable. Given that according to an analysis of data from the 2022 KFF Women’s Health Survey, 90 percent of female respondents reported using contraception at some point and 76 percent of respondents reported using more than one method over the course of their lifespan, access to the full range of methods is an important aspect of women’s control over their family planning and reproductive health (Frederiksen et al., 2022).
In addition to the shortages and uneven distribution of clinicians, there are gaps in the availability of some services. In 2020, a nationally representative survey of OB-GYNs found that just over a quarter (28 percent) work at practices that provide gender-affirming care, including hormone therapy or surgery (Weigel et al., 2021). While the vast majority of OB-GYNs reported that they felt somewhat or very prepared to meet the sexual reproductive health care needs of patients who are lesbian, gay, bisexual, and queer, only about half (56 percent) felt the same about providing care to transgender patients (Weigel et al., 2021). Shortages are particularly stark for abortion services. Abortion care is delivered primarily in outpatient clinics, but there are vast differences in clinic availability across the country. As noted earlier in this report, pregnancy coercion and interference with contraception are associated with unintended pregnancies among women
___________________
20 Patient Protection and Affordable Care Act, Public Law 118-148, 111th Congress (March 23, 2010).
21 Dobbs, State Health Officer of the Mississippi Department of Health et al. v. Jackson Women’s Health Organization et al. 597 US_ (2022).
experiencing IPV. Pregnancy testing and abortion services are essential for those who experience sexual IPV and reproductive coercion (Grace and Anderson, 2018). The June 2022 Supreme Court ruling in Dobbs v. Jackson Women’s Health Organization22 overturned the precedents in Roe v. Wade23 and Planned Parenthood v. Casey.24 It eliminated the longstanding federal standards regarding abortion access. As of August 2023, abortion is banned in 15 states (KFF, 2023a). No clinicians offer abortion in these states except for under a minimal set of circumstances (KFF, 2023a). An additional 10 states have gestational limits ranging from 6 to 22 weeks as of August 2023 (KFF, 2023a). Several other states have a variety of regulations such as mandatory waiting periods, restrictions on the use of telehealth, and restrictions on the type of provider that can prescribe the medications used in medication abortion (KFF, 2023b). The lack of abortion availability is widest in the South and Plains states, where many states have banned or imposed gestational limits on abortion.
This lack of abortion access in large swaths of the country poses significant barriers for pregnant people experiencing IPV who are seeking an abortion, particularly people who have low incomes and some communities of color, who, on average, have fewer resources to travel to obtain care (Pleasants et al., 2022; Rader et al, 2022). Many would need to travel out of state to obtain this essential service, which will likely be even more challenging during a PHE (Pleasants et al., 2022; Rader et al., 2022). Those seeking an abortion without a partner’s knowledge have even more limited access after the Dobbs ruling.
Sexual Assault Nurse Examiners
Sexual Assault Nurse Examiners (SANEs) play an important role in providing care for individuals who have experienced IPV-related sexual assault. SANEs are trained to provide “comprehensive and compassionate specialty care to sexual assault survivors” (Hollender et al., 2023, p. 1). Sexual assault forensic medical examinations may be performed by clinicians who have not been trained to perform these exams (GAO, 2016). However, researchers have found that patients are more likely to accept services offered from SANEs, they report feeling more cared for, and are more likely to be offered pregnancy tests and emergency contraception (Chandramani et al., 2020; Hollender et al., 2023). A nationwide survey of
___________________
22 Dobbs, State Health Officer of the Mississippi Department of Health et al. v. Jackson Women’s Health Organization et al. 597 US_ (2022).
23 Jane Roe, et al., Appellants v. Henry Wade 410 U.S. 113 (1973).
24 Planned Parenthood of Southeastern Pennsylvania, et al. v. Casey, Governor of Pennsylvania, et al. 505 U.S. 833 (1992).
315 advocates from 119 sexual assault crisis centers across 44 states about emergency department preparedness to care for people who experience sexual assault found that the presence of a SANE was associated with an increased likelihood of availability of post-discharge resources (Chalmers et al., 2023). While data on the exact number of SANEs across the United States is limited, several studies conducted at the local and state level have highlighted a shortage of SANEs across the country, particularly in rural areas (GAO, 2016; Mitchell et al., 2022; Miyamoto et al., 2021; Morris et al., 2022; Thiede and Miyamoto, 2021). A 2016 Government Accountability Office (GAO) report noted that state officials from all six of the states included in their research reported that the number of SANEs in their respective states did not meet the need for exams (GAO, 2016). The GAO report said that several state officials offered examples to illustrate the SANE shortage in their respective states. For example, in rural western Colorado, someone who has been sexually assaulted may need to travel over an hour to reach a facility that has a SANE available, and in Nebraska they may need to drive 2 or more hours (GAO, 2016). This shortage represents a serious barrier to care access for women experiencing sexual IPV. The shortage of SANE workers was elevated in March 2022 when President Biden signed the Supporting Access to Nurse Exams (SANE) Act into law as part of the Violence Against Women Reauthorization Act of 202225 with the goal to increase access to SANE care. This law is intended to help address the SANE shortage by providing funding for SANE salaries in rural, tribal, and underserved communities, establish regional training centers, provide additional funding for pediatric SANEs, and provide funding for mobile SANE units (Hanson, 2023).
Mental Health Professionals
Women that experience IPV have substantial needs for mental health care, including behavioral health care such as substance abuse treatment. In 2023, there were 166 million people residing in areas classified as mental health provider shortage areas according to tracking by HRSA (HRSA, 2023c).26 As illustrated in Figure 5-5, most of the United States has some degree of mental health professional shortage. With few exceptions, large metropolitan areas are less likely to have a shortage than rural areas. HRSA’s national-level projections of supply adequacy for
___________________
25 Violence Against Women Reauthorization Act of 2022, Public Law 117-103 Division W, 117th Congress (March 15, 2022).
26 The providers included in HRSA’s data for mental health providers include adult psychiatrists, addiction counselors, child psychiatrists, marriage and family therapists, mental health counselors, psychiatric nurse practitioners, psychiatric physician assistants, psychologists, school counselors, and social workers.
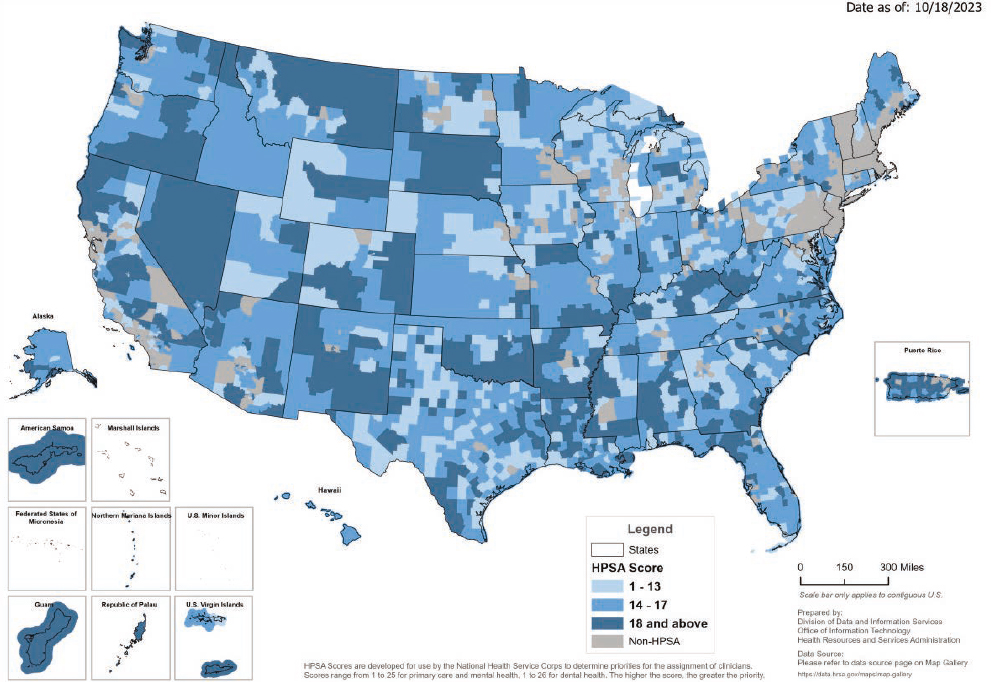
SOURCE: HRSA (2023e).
mental health providers indicate likely shortages by 2035 of many of the professions that care for women who experience IPV, including adult psychiatry, child and adolescent psychiatry, psychologists, addiction counselors, mental health counselors, and under some scenarios, marriage and family therapists (HRSA, 2022). Prior to the COVID-19 pandemic, rural mental health and substance abuse treatment providers had begun efforts to use telehealth to increase access (Uscher-Pines et al., 2020; Vakkalanka et al., 2022). The COVID-19 pandemic and associated policy changes brought about a substantial increase in use of telehealth for mental health and substance abuse treatment. However, barriers associated with the digital divide, including lack of internet access and technological devices needed to access the internet (i.e., smartphones or laptop computers) have perpetuated mental health access barriers for people in both urban and rural settings (Summers-Gabr, 2020). In addition to shortages, a systematic review including 20 studies found that mental health providers lacked in-depth training on IPV and felt underprepared when working with someone who had experienced IPV (Sutton et al., 2021).
Adolescent Care Professionals
Accessibility to comprehensive adolescent care remains a major barrier for youth across the country, especially those who are immigrants, are uninsured, live in a rural area, or live in a neighborhood with a concentrated disadvantage. Even with federal and state insurance coverage for minors, including increases in receipt of care with the Patient Protection and Affordable Care Act (ACA), fewer than half of adolescents in the United States receive well visits (Adams et al., 2019).
POLICY AND REGULATORY CONSIDERATIONS
Referral and Financing
One challenge for providing the entire constellation of services that people experiencing IPV might need is financing and payment, which tends to be siloed between buckets of services. Most women are covered by private insurance or Medicaid, which has broad coverage for many medical care services but limited coverage for abortion services. The federal Hyde Amendment27 blocks certain federal funds from being used to pay for abortion outside of the exceptions for rape, incest, or when the pregnancy is determined to endanger the pregnant person’s life. This has resulted in severely limited coverage of abortion under Medicaid and other federal programs, including the Indian Health Service (IHS) and the federal employees’ health benefits program (Liu and Shen, 2022). Under private insurance, several states also impose restrictions on the circumstances under which private insurance plans can cover abortion services (Guttmacher Institute, 2023).
Health insurance coverage is also limited for nonmedical support services, such as transportation and housing, which are essential for some people experiencing IPV. Some models may be promising for integrated coverage. The state of North Carolina’s Medicaid program is operating the Healthy Opportunities pilot program, which allows for reimbursement of some non-medical services that address specific social needs and are linked to health or health outcomes, including safe housing, transportation, food, and interpersonal safety for state Medicaid enrollees that are considered high need (NCDHHS, n.d.).
___________________
27 Hyde Amendment Public Law 94-439 § 209 94th Congress, September 30, 1976 (original). Most recently enacted version Public Law 117-103. Div. H, §§ 506–507, 117th Congress, March 15, 2022.
Confidentiality and Privacy Requirements
Privacy and confidentiality requirements present challenges for integrated service models in a steady state context. For example, medical–legal partnerships, which “address the health-harming social and legal needs of patients and communities by integrating the expertise of health care, public health, and legal professionals,” face legal impediments to sharing data among members of interprofessional care teams (Mantel and Knake, 2018, p. 184). During a PHE, barriers to data sharing may be exacerbated by the displacement and disruption of access to mechanisms for secure communication. For example, during a hurricane, health care facilities may lose power, and communications systems may be affected (Horahan et al., 2014). At the same time, barriers to data sharing may be eased by orders suspending privacy regulations pursuant to federal or state declarations. During the federally declared PHE for COVID-19 under Section 319 of the Public Health Services Act,28 the HHS Secretary exercised authority to waive sanctions and penalties against covered hospitals for failure to comply with specific provisions of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule.29
Confidentiality and accessibility are critical for adolescent health services. Adolescents are generally amenable to having trusted adults, including parents and caregivers, involved in important health care decisions. However, the ability to seek care confidentially is a well-documented factor that increases the likelihood of an adolescent receiving needed health care, including preventive services and behavioral health treatment (Ford et al., 2004). Although great variability exists in laws governing consent for adolescent patients, some protections exist in all U.S. states for some provision of confidential care, generally in reproductive and sexual health and behavioral health.
Title X Regulations
Title X30 regulations require participating clinics to provide pregnant clients with non-directive pregnancy options counseling. At the same time, it is prohibited to use Title X funds for the provision of abortion services. The program does allow for the co-location of family planning and abortion services. However, in 2019 regulations were revised to require Title X-funded clinicians to maintain strict physical and financial separation of abortion services. This resulted in a large decline in the network of Title X clinicians and in the number of clients served (Fowler et al., 2022). Those regulations were revoked, but an ongoing legal challenge seeks to reinstate the ban on
___________________
28 Public Health Service Act 42 USC 247d §319.
29 Health Insurance Portability and Accountability Act of 1996 Privacy Rule 45 CFR Part 160 and Subparts A and E of Part 164.
30 Title X of the Public Health Service Act 42 USC § 300 to 300a-6.
abortion counseling and referral and disqualify family planning sites that provide abortion services (Frederiksen et al., 2021). This ongoing threat could eventually compromise the Title X network of clinicians and reduce access to clinicians with expertise in making family planning services available to people experiencing IPV.
Payment and Insurance Challenges
Access to essential health care services related to IPV depends in part on insurance coverage of those services, availability of in-network clinicians to deliver them, and laws ensuring or restricting access to certain services regardless of insurance coverage or prevailing clinical standards of care. These matters vary by insurance type, service type, and geographic jurisdiction.
Rates of Coverage and Enrollment Challenges
According to a KFF analysis of data from the 2021 American Community Survey, among nonelderly adult women ages 19–64, 60 percent were covered by private employer–sponsored group health plans; private nongroup plans covered 8 percent; 18 percent relied on Medicaid coverage; 3 percent relied on Medicare, military, or other public programs; and 11 percent were uninsured (as of 2021) (KFF, 2023c). This analysis found that coverage patterns were similar among women and teenage girls of reproductive age (15–49). In 2021, 58 percent were covered by employer-sponsored group health plans, one in five were covered by Medicaid (21 percent), and one in ten were uninsured (11 percent) (KFF, 2023c).
Experiencing IPV may qualify an individual to initiate or change type of health insurance, with associated changes in the network of clinicians from whom the individual may seek covered services. Under the ACA,31 health insurers and self-insuring employers are prohibited from refusing to issue or renew coverage or charging higher premiums based on an applicant’s history of conditions arising from experiencing domestic violence, pregnancy, and other health status–related factors.
In March 2020, at the outset of the COVID-19 pandemic, the Families First Coronavirus Response Act32 was enacted into federal law. The law required that states keep people continuously enrolled in the Medicaid program through the end of the COVID-19 PHE in exchange for increased
___________________
31 Patient Protection and Affordable Care Act, Public Law 118-148, 111th Congress (March 23, 2010).
32 Families First Coronavirus Response Act, Public Law 116-127, 116th Congress (March 18, 2020).
federal funding. Research has found that Medicaid enrollment grew during the PHE partly because of this policy (Benitez and Dubay, 2022; Mandal et al., 2022). With the end of the COVID-19 PHE, many states have restarted administrative verifications of Medicaid eligibility, and many people have already been disenrolled from the program. Given the intense health needs of many people experiencing IPV, maintaining stable coverage is vital for connecting to and receiving health care services. States can employ policies and practices that facilitate access to coverage for people experiencing IPV, such as partnering with IPV service agencies for outreach and streamlining enrollment processes to minimize paperwork requirements (Wagner, 2021).
Restrictive provider networks may limit access to health care services for individuals enrolled in private insurance plans (group or nongroup) and those enrolled in privatized Medicaid managed care plans (which cover the majority of Medicaid recipients) or privatized Medicare plans (GAO, 2022). Health plans establish provider networks through contracts with clinicians and facilities. When enrollees seek care from out-of-network clinicians, their health plan may deny coverage or charge higher out-of-pocket costs. Health plan provider networks are often geographically limited (GAO, 2022). Therefore, it is reasonable to assume that displacement due to IPV or a PHE may hinder access to affordable health care services.
Access to Abortion Services
Access to abortion services varies by insurance type and jurisdiction. As previously noted, a federal restriction known as the Hyde Amendment33 prohibits using certain federal funds to cover abortion services. This greatly limits access for individuals covered by Medicaid, Medicare, and IHS (Liu and Shen, 2022). Several states have restricted coverage of abortion services by private health plans. However, these restrictions on benefit design are preempted by the federal Earned Retirement Income Security Act34 and therefore do not apply to health plans sponsored by employers who self-insure. Since the Supreme Court’s 2022 ruling in Dobbs v. Jackson Women’s Health Organization,35 several states have also restricted the provision of abortion services regardless of insurance.
___________________
33 Hyde Amendment Public Law 94-439 § 209 94th Congress, September 30, 1976 (original). Most recently enacted version Public Law 117-103. Div. H, §§ 506–507, 117th Congress, March 15, 2022.
34 Earned Retirement Income Security Act of 1974. Public Law 93-406, amended through Public Law 117-328, 117th Congress, (December 29, 2022).
35 Dobbs, State Health Officer of the Mississippi Department of Health et al. v. Jackson Women’s Health Organization et al. 597 US_ (2022).
Required Coverage for Services
Federal and state governments ensure or restrict access to health care through various means. One approach is to require health plans to cover certain types of services, such as preventive care. Health plan benefits are regulated by overlapping federal and state laws, which vary by insurance type and service. In addition, government agencies may be required to ensure no-cost provision of certain services regardless of insurance status. Finally, states may restrict or prohibit the provision of certain types of services, such as abortion, even if the services are deemed essential under prevailing clinical standards of care.
Federal law requires most private health plans and some Medicaid plans to cover IPV screening. A provision in the ACA requires most private health plans to cover the total cost of certain preventive services, including those that receive an A or B rating from the USPSTF, which HRSA recommends via the Women’s Preventive Services Initiative (WPSI).36 WPSI recommends screening adolescents and women for interpersonal and domestic violence at least annually and, when needed, providing or referring for initial intervention services (including, but not limited to, counseling, education, harm reduction strategies, and referral to appropriate supportive services).37 A separate provision in the ACA requires Medicaid Alternative Benefit Plans (which cover all Medicaid enrollees eligible as part of the ACA’s expansion population and other enrollees in some states) to cover the same slate of preventive services as private plans. States may opt to cover these services in their traditional Medicaid plans with financial assistance from the federal government but are not required to do so.
In addition to screening for IPV, the preventive services recommended by USPSTF and WPSI include many important services for caring for women experiencing IPV. These include the full range of FDA-approved contraceptives for women, STI screenings, well-woman visits, screening for depression and anxiety, and a broad range of pregnancy-related tests and services.
___________________
36 42 USC § 300gg–13; see also https://www.kff.org/health-reform/report/preventive-services-tracker/ (accessed August 25, 2023). The same provision also requires most private health plans to cover services that receive an A or B rating from USPSTF, including IPV screening for women of reproductive age. In 2023 this requirement was vacated by a federal district court order applicable to all benefit design mandates triggered by USPSTF recommendations issued after 2010; however, the requirement to cover WPSI-recommended services is not currently affected by this ruling (see Braidwood Management Inc., et al. v. Xavier Becerra et al. 666 F.Supp.3d 613 [5th Cir. 2023]).
37 WPSI defines interpersonal and domestic violence as including physical violence, sexual violence, stalking and psychological aggression (including coercion), reproductive coercion, neglect, and the threat of violence, abuse, or both.
Out-of-Pocket Expenses
While preventive services are covered without cost sharing, the health consequences of IPV can be severe, and many people who experience IPV have significant care needs beyond preventive services. As a result, many face substantial out-of-pocket expenses. According to data from the 2016–2017 NISVS, 35 percent of women had injuries from IPV during their lifetimes (Leemis et al., 2022). Common injuries include bruises, scratches, cuts, and black eyes. Furthermore, 28 percent reported mental or emotional harm related to IPV during their lifetime (Leemis et al., 2022). Analysis of 2016–2017 NISVS data found 13.9 percent of women reported needing medical care due to IPV related injuries during their lifetime (Leemis et al., 2022). This care can be costly. A 2007 study found that women who experienced IPV had higher utilization of primary care, specialty visits, and prescription medications (Rivara et al., 2007). Another analysis using 2014 costs estimated that a woman experiencing IPV would have an additional $65,165 in medical costs during her lifetime (Peterson et al., 2018).
In cases of sexual assault, the Violence Against Women Act (VAWA)38 requires states, local governments, and IHS to ensure no-cost access to medical forensic exams, regardless of insurance status (Hanson, 2023). However, services ancillary to the evidence-gathering portion of the medical forensic exam—such as treatment for injuries, pregnancy testing, and emergency contraception—are not required under VAWA-mandated programs. The no-cost provision of these ancillary services is governed by state law, which varies from jurisdiction to jurisdiction (Ramaswamy et al., 2022). These services may be covered by insurance, possibly without cost-sharing, depending on how the services are classified and the type of insurance the individual has, as described above. In correspondence with the New England Journal of Medicine, researchers noted that many patients are still charged out-of-pocket fees when they seek care for sexual violence in emergency departments (Dickman et al., 2022).
Challenges with Confidentiality
Another challenge with insurance, particularly private insurance, is confidentiality. Private insurers typically send beneficiaries billing statements that enumerate the health services they received and the associated costs. For people experiencing IPV, this can be dangerous, particularly if the patient received services that the partner opposes, such as contraception
___________________
38 Violence Against Women Reauthorization Act of 2019, H.R. 1585, 116th Cong., 1st Session (April 10, 2019), H. Rept. 116-21.
or abortion. HIPAA39 does allow patients to request that explanation of benefits statements are kept confidential, but enforcement has been uneven (English and Lewis, 2016). Similarly, some states have added confidentiality protections, but these are limited and do not cover most people with private insurance (English et al., 2012).
CHAPTER SUMMARY
Essential health care services related to IPV are those that address the most prevalent and serious physical health issues related to IPV, behavioral health issues related to IPV, and those that facilitate disclosure of IPV, protect the safety of the person experiencing IPV (and their children if needed), and meet these individuals’ basic needs for food and shelter. They are delivered in a variety of settings within and outside of the traditional health care system. Community-based support services are an important component of care delivery for essential health care services related to IPV. Health care deserts, particularly for primary care, maternal and reproductive health care, adolescent care, and SANEs, create barriers to accessing essential health care services related to IPV. Additional barriers to accessing essential health care services related to IPV include state-level restrictions on reproductive health care, limitations on insurance coverage, and inadequate availability of culturally and linguistically appropriate care.
REFERENCES
Abramsky, T., K. M. Devries, L. Michau, J. Nakuti, T. Musuya, N. Kyegombe, and C. Watts. 2016. The impact of SASA!, a community mobilisation intervention, on women’s experiences of intimate partner violence: Secondary findings from a cluster randomised trial in Kampala, Uganda. Journal of Epidemiology and Community Health 70(8):818-825.
Acharya, M., M. M. Ali, C. J. Hayes, C. A. Bogulski, E. F. Magann, and H. Eswaran. 2023. Trends in telehealth visits during pregnancy, 2018 to 2021. JAMA Netw Open 6(4):e236630.
ACOG (American College of Obstetricians and Gynecologists). 2012. ACOG committee opinion no. 518: Intimate partner violence. Obstet Gynecol 119(2 Pt 1):412-417.
Adams, E. N., H. M. Clark, M. M. Galano, S. F. Stein, A. Grogan-Kaylor, and S. GrahamBermann. 2021. Predictors of housing instability in women who have experienced intimate partner violence. J Interpers Violence 36(7-8):3459-3481.
Adams, S. H., M. J. Park, L. Twietmeyer, C. D. Brindis, and C. E. Irwin, Jr. 2019. Young adult preventive healthcare: Changes in receipt of care pre- to post-affordable care act. J Adolesc Health 64(6):763-769.
___________________
39 Health Insurance Portability and Accountability Act of 1996, Public Law 104-91, 104th Congress (August 21, 1996).
Adjognon, O. L., J. E. Brady, M. R. Gerber, M. E. Dichter, A. R. Grillo, A. B. Hamilton, S. W. Stirman, and K. M. Iverson. 2021. Getting routine intimate partner violence screening right: Implementation strategies used in Veterans Health Administration (VHA) primary care. The Journal of the American Board of Family Medicine 34(2):346-356.
Ahmad, F., S. Hogg-Johnson, D. E. Stewart, H. A. Skinner, R. H. Glazier, and W. Levinson. 2009. Computer-assisted screening for intimate partner violence and control: A randomized trial. Ann Intern Med 151(2):93-102.
Alhusen, J. L., E. Ray, P. Sharps, and L. Bullock. 2015. Intimate partner violence during pregnancy: Maternal and neonatal outcomes. J Womens Health (Larchmont) 24(1):100-106.
Anderson, C. A., and D. B. Arciniegas. 2010. Cognitive sequelae of hypoxic-ischemic brain injury: A review. NeuroRehabilitation 26(1):47-63.
Anderson, J. R., S. M. Stith, M. D. Johnson, M. M. Strachman-Miller, Y. Amanor-Boadu, and D. J. Linkh. 2013. Multi-couple group and self-directed prep formats enhance relationship satisfaction and improve anger management skills in Air Force couples. American Journal of Family Therapy 41(2):121-133.
Ard, K. L., and H. J. Makadon. 2011. Addressing intimate partner violence in lesbian, gay, bisexual, and transgender patients. J Gen Intern Med 26(8):930-933.
Ascione, F. R., C. V. Weber, T. M. Thompson, J. Heath, M. Maruyama, and K. Hayashi. 2007. Battered pets and domestic violence: Animal abuse reported by women experiencing intimate violence and by nonabused women. Violence Against Women 13(4):354-373.
Auger, N., N. Low, G. E. Lee, A. Ayoub, and T. M. Luu. 2022. Pregnancy outcomes of women hospitalized for physical assault, sexual assault, and intimate partner violence. J Interpers Violence 37(13-14):NP11135.
Bair-Merritt, M. H., A. Lewis-O’Connor, S. Goel, P. Amato, T. Ismailji, M. Jelley, P. Lenahan, and P. Cronholm. 2014. Primary care-based interventions for intimate partner violence: A systematic review. Am J Prev Med 46(2):188-194.
Barrett, B. J., A. Fitzgerald, R. Stevenson, and C. H. Cheung. 2020. Animal maltreatment as a risk marker of more frequent and severe forms of intimate partner violence. J Interpers Violence 35(23-24):5131-5156.
Basile, K. C., S. DeGue, K. Jones, K. Freire, J. Dills, S. G. Smith, and J. L. Raiford. 2016. Stop SV: A technical package to prevent sexual violence. National Center for Injury Prevention and Control (U.S.). Division of Violence Prevention.
Basile, K. C., S. G. Smith, Y. Liu, M. J. Kresnow, A. M. Fasula, L. Gilbert, and J. Chen. 2018. Rape-related pregnancy and association with reproductive coercion in the US. American Journal of Preventive Medicine 55(6):770-776.
Benitez, J. A., and L. Dubay. 2022. COVID-19-related Medicaid enrollment in Medicaid expansion and non-expansion states. Health Services Research 57(6):1321-1331.
Bent-Goodley, T. B. 2007. Health disparities and violence against women: Why and how cultural and societal influences matter. Trauma Violence Abuse 8(2):90-104.
Bergmann, J. N., and J. K. Stockman. 2015. How does intimate partner violence affect condom and oral contraceptive use in the United States?: A systematic review of the literature. Contraception 91(6):438-455.
BLS (Bureau of Labor Statistics). 2023. Occupational outlook handbook. https://www.bls.gov/ooh/healthcare/registered-nurses.htm (accessed September 13, 2023).
Braithwaite, S. R., and F. D. Fincham. 2014. Computer-based prevention of intimate partner violence in marriage. Behaviour Research Therapy 54:12-21.
Brigance, C., R. Lucas, E. Jones, A. Davis, M. Oinuma, K. Mishkin, and Z. Henderson. 2022. Nowhere to go: Maternity care deserts across the U.S. 2022 report. March of Dimes.
Britto, M. T., B. K. Klostermann, A. E. Bonny, S. A. Altum, and R. W. Hornung. 2001. Impact of a school-based intervention on access to healthcare for underserved youth. J Adolesc Health 29(2):116-124.
Brown, R. B., S. Miller-Walfish, S. Scott, A. Ali, A. Marjavi, E. Miller, and E. A. McGuier. 2023. Cross-sector collaboration in project catalyst: Creating state partnerships to address the health impact of intimate partner violence. Prev Med Rep 33:102204.
Burnett, C., J. Crowder, L. J. Bacchus, D. Schminkey, L. Bullock, P. Sharps, and J. Campbell. 2021. “It doesn’t freak us out the way it used to”: An evaluation of the domestic violence enhanced home visitation program to inform practice and policy screening for IPV. Journal of Interpersonal Violence 36(13-14):NP7488-NP7515.
Calton, J. M., L. B. Cattaneo, and K. T. Gebhard. 2016. Barriers to help seeking for lesbian, gay, bisexual, transgender, and queer survivors of intimate partner violence. Trauma Violence Abuse 17(5):585-600.
Campbell, J. C. 1986. Nursing assessment for risk of homicide with battered women. Advances in Nursing Science 8(4):36-51.
Campbell, J., and N. Glass. 2009. Safety planning, danger, and lethality assessment. In Intimate partner violence: A health-based perspective. New York, NY: Oxford University Press. Pp. 319-334.
Campbell, J. C., D. Webster, J. Koziol-McLain, C. Block, D. Campbell, M. A. Curry, F. Gary, N. Glass, J. McFarlane, C. Sachs, P. Sharps, Y. Ulrich, S. A. Wilt, J. Manganello, X. Xu, J. Schollenberger, V. Frye, and K. Laughon. 2003. Risk factors for femicide in abusive relationships: Results from a multisite case control study. Am J Public Health 93(7):1089-1097.
Campbell, J. C., D. W. Webster, and N. Glass. 2009. The danger assessment: Validation of a lethality risk assessment instrument for intimate partner femicide. J Interpers Violence 24(4):653-674.
Cantor, A. G., H. D. Nelson, M. Pappas, C. Atchison, B. Hatch, N. Huguet, B. Flynn, and M. McDonagh. 2023. Telehealth for women’s preventive services for reproductive health and intimate partner violence: A comparative effectiveness review. J Gen Intern Med 38(7):1735-1743.
Center for Health Care Strategies. 2018. Incorporating patients’ voices at the women’s HIV program: University of California, San Francisco. https://www.traumainformedcare.chcs.org/incorporating-patients-voices-at-the-womens-hiv-program-university-of-californiasan-francisco/ (accessed September 11, 2023).
Chalmers, K., M. Hollender, L. Spurr, R. Parameswaran, N. Dussault, J. Farnan, S. Oyola, and K. Carter. 2023. Emergency department preparedness to care for sexual assault survivors: A nationwide study. West J Emerg Med 24(3):629-636.
Chandramani, A., N. Dussault, R. Parameswaran, J. Rodriguez, J. Novack, J. Ahn, S. Oyola, and K. Carter. 2020. A needs assessment and educational intervention addressing the care of sexual assault patients in the emergency department. J Forensic Nurs 16(2):73-82.
Chang, J. C., P. A. Cluss, L. Ranieri, L. Hawker, R. Buranosky, D. Dado, M. McNeil, and S. H. Scholle. 2005. Health care interventions for intimate partner violence: What women want. Womens Health Issues 15(1):21-30.
Chisholm, C. A., L. Bullock, and J. E. J. Ferguson, 2nd. 2017. Intimate partner violence and pregnancy: Screening and intervention. Am J Obstet Gynecol 217(2):145-149.
Chouinard, A.-F., M. J. Troulis, and E. T. Lahey. 2016. The acute management of facial fractures. Current Trauma Reports 2:55-65.
Clayton, S., T. Chin, S. Blackburn, and C. Echeverria. 2010. Different setting, different care: Integrating prevention and clinical care in school-based health centers. Am J Public Health 100(9):1592-1596.
Coker, A. L., B. S. Fisher, H. M. Bush, S. C. Swan, C. M. Williams, E. R. Clear, and S. DeGue. 2015. Evaluation of the green dot bystander intervention to reduce interpersonal violence among college students across three campuses. Violence Against Women 21(12):1507-1527.
Coker, A. L., D. R. Follingstad, H. M. Bush, and B. S. Fisher. 2016. Are interpersonal violence rates higher among young women in college compared with those never attending college? Journal of Interpersonal Violence 31(8):1413-1429.
Collins, E. A., A. M. Cody, S. E. McDonald, N. Nicotera, F. R. Ascione, and J. H. Williams. 2018. A template analysis of intimate partner violence survivors’ experiences of animal maltreatment: Implications for safety planning and intervention. Violence Against Women 24(4):452-476.
Condon, M. C., D. Charlot-Swilley, and T. Rahman. 2022. At the feet of storytellers: Equity in early relational health conversations. Infant Ment Health J 43(3):390-409.
Dawson-Rose, C., Y. P. Cuca, M. Shumway, K. Davis, and E. L. Machtinger. 2019. Providing primary care for HIV in the context of trauma: Experiences of the health care team. Womens Health Issues 29(5):385-391.
Dickman, S. L., G. Himmelstein, D. U. Himmelstein, K. Strandberg, A. McGregor, D. McCormick, and S. Woolhandler. 2022. Uncovered medical bills after sexual assault. N Engl J Med 387(11):1043-1044.
DOJ (Department of Justice). 2023. A national protocol for intimate partner violence medical forensic examinations. Washington, DC: US Department of Justice.
Duchesne, E., A. Nathoo, M. Walker, and S. A. Bartels. 2022. Patient and provider emergency care experiences related to intimate partner violence: A systematic review of the existing evidence. Trauma Violence Abuse 24(5):2901-2921. https://doi.org/10.1177/15248380221118962.
Dyer, A. M., and C. G. Abildso. 2019. Impact of an intimate partner violence training on home visitors’ perceived knowledge, skills, and abilities to address intimate partner violence experienced by their clients. Health Educ Behav 46(1):72-78.
Echeburúa, E., J. Fernández-Montalvo, P. de Corral, and J. J. López-Goñi. 2009. Assessing risk markers in intimate partner femicide and severe violence: A new assessment instrument. Journal of Interpersonal Violence 24(6):925-939.
Edwards, K. M. 2015. Intimate partner violence and the rural-urban-suburban divide: Myth or reality? A critical review of the literature. Trauma Violence Abuse 16(3):359-373.
Ellis, T. W., S. Brownstein, K. Beitchman, and J. Lifshitz. 2019. Restoring more than smiles in broken homes: Dental and oral biomarkers of brain injury in domestic violence. Journal of Aggression, Maltreatment & Trauma 28(7):838-847.
English, A., and J. Lewis. 2016. Privacy protection in billing and health insurance communications. AMA J Ethics 18(3):279-287.
English, A. G., R. B. Gold, E. Nash, and J. Levine. 2012. Confidentiality for individuals insured as dependents: A review of state laws and policies. Guttmacher Institute.
Ezie, C. 2023. Dismantling the discrimination to incarceration pipeline for trans people of color. University of St. Thomas Law Journal 19.
Feder, G. S., M. Hutson, J. Ramsay, and A. R. Taket. 2006. Women exposed to intimate partner violence: Expectations and experiences when they encounter health care professionals: A meta-analysis of qualitative studies. Arch Intern Med 166(1):22-37.
Feltner, C., I. Wallace, N. Berkman, C. E. Kistler, J. C. Middleton, C. Barclay, L. Higginbotham, J. T. Green, and D. E. Jonas. 2018. Screening for intimate partner violence, elder abuse, and abuse of vulnerable adults: Evidence report and systematic review for the US preventive services task force. JAMA 320(16):1688-1701.
Finnie, R. K. C., D. L. Okasako-Schmucker, L. Buchanan, D. Carty, H. Wethington, S. L. Mercer, K. C. Basile, S. DeGue, P. H. Niolon, J. Bishop, T. Titus, S. Noursi, S. A. Dickerson, D. Whitaker, S. Swider, P. Remington, and Community Preventive Services Task Force. 2022. Intimate partner and sexual violence prevention among youth: A community guide systematic review. Am J Prev Med 62(1):e45-e55.
Ford, C., A. English, and G. Sigman. 2004. Confidential health care for adolescents: Position paper for the Society for Adolescent Medicine. J Adolesc Health 35(2):160-167.
Ford-Gilboe, M., C. Varcoe, K. Scott-Storey, N. Perrin, J. Wuest, C. N. Wathen, J. Case, and N. Glass. 2020. Longitudinal impacts of an online safety and health intervention for women experiencing intimate partner violence: Randomized controlled trial. BMC Public Health 20(1):260.
Foshee, V. A., K. E. Bauman, S. T. Ennett, G. F. Linder, T. Benefield, and C. Suchindran. 2004. Assessing the long-term effects of the safe dates program and a booster in preventing and reducing adolescent dating violence victimization and perpetration. Am J Public Health 94(4):619-624.
Fowler, C. I., J. Gable, and B. Lastaer. 2022. Family planning annual report 2021 national summary. Rockville, Maryland: Health and Human Services.
Frederiksen, B., I. Gomez, and A. Salganicoff. 2021. Rebuilding Title X: New regulations for the federal family planning program. https://www.kff.org/womens-health-policy/issue-brief/rebuilding-title-x-new-regulations-for-the-federal-family-planning-program/ (accessed July 26, 2023).
Frederiksen, B., U. Ranji, M. Long, K. Diep, and A. Salganicoff. 2022. Contraception in the United States: A closer look at experiences, preferences, and coverage. https://www.kff.org/womens-health-policy/report/contraception-in-the-united-states-a-closer-look-at-experiences-preferences-and-coverage/ (accessed September 13, 2023).
Futures Without Violence. n.d. Telehealth, COVID-19, intimate partner violence, and human trafficking: Increasing safety for people surviving abuse. Edited by Futures Without Violence: IPV Health Partners.
Galgano, M., G. Toshkezi, X. Qiu, T. Russell, L. Chin, and L. R. Zhao. 2017. Traumatic brain injury: Current treatment strategies and future endeavors. Cell Transplant 26(7):1118-1130.
GAO (Government Accountability Office). 2016. Sexual assault: Information on training, funding, and the availability of forensic examiners. Washington, DC: U.S. Government Accountability Office.
GAO. 2022. Private health insurance: State and federal oversight of provider networks varies. Washington, DC: U.S. Government Accountability Office.
Garcia-Vergara, E., N. Almeda, F. Fernández-Navarro, and D. Becerra-Alonso. 2022. Risk assessment instruments for intimate partner femicide: A systematic review. Frontiers in Psychology 13.
Gavin, L., K. Pazol, and K. Ahrens. 2017. Update: Providing quality family planning services - recommendations from CDC and the U.S. Office of Population Affairs, 2017. MMWR Morb Mortal Wkly Rep 66(50):1383-1385.
Gee, R. E., N. Mitra, F. Wan, D. E. Chavkin, and J. A. Long. 2009. Power over parity: Intimate partner violence and issues of fertility control. Am J Obstet Gynecol 201(2):148 e141-e147.
Gibson, E. J., J. S. Santelli, M. Minguez, A. Lord, and A. C. Schuyler. 2013. Measuring school health center impact on access to and quality of primary care. J Adolesc Health 53(6):699-705.
Giesbrecht, C. J. 2022. Animal safekeeping in situations of intimate partner violence: Experiences of human service and animal welfare professionals. J Interpers Violence 37(17-18):NP16931-NP16960.
Gilbert, L., S. A. Shaw, D. Goddard-Eckrich, M. Chang, J. Rowe, T. McCrimmon, M. Almonte, S. Goodwin, and M. Epperson. 2015. Project wings (women initiating new goals of safety): A randomised controlled trial of a screening, brief intervention and referral to treatment (SBIRT) service to identify and address intimate partner violence victimisation among substance-using women receiving community supervision. Crim Behav Ment Health 25(4):314-329.
Gilmore, A. K., A. E. Jaffe, C. K. Hahn, L. E. Ridings, K. Gill-Hopple, G. B. Lazenby, and J. C. Flanagan. 2021. Intimate partner violence and completion of post-sexual assault medical forensic examination follow-up screening. J Interpers Violence 36(13-14):5991-6004.
Gilmore, A. K., G. McKee, J. C. Flanagan, R. M. Leone, D. W. Oesterle, C. M. Kirby, N. Short, and K. Gill-Hopple. 2022. Medications at the emergency department after recent rape. Journal of Interpersonal Violence 37(15-16):NP12954-NP12972.
Gilroy, H., J. McFarlane, J. Maddoux, and C. Sullivan. 2016. Homelessness, housing instability, intimate partner violence, mental health, and functioning: A multi-year cohort study of IPV survivors and their children. Journal of Social Distress and the Homeless 25(2):86-94.
Glass, N. E., N. A. Perrin, G. C. Hanson, T. L. Bloom, J. T. Messing, A. S. Clough, J. C. Campbell, A. C. Gielen, J. Case, and K. B. Eden. 2017. The longitudinal impact of an internet safety decision aid for abused women. Am J Prev Med 52(5):606-615.
Glass, N. E., A. Clough, J. T. Messing, T. Bloom, M. L. Brown, K. B. Eden, J. C. Campbell, A. Gielen, K. Laughon, K. T. Grace, R. M. Turner, C. Alvarez, J. Case, J. Barnes-Hoyt, J. Alhusen, G. C. Hanson, and N. A. Perrin. 2022. Longitudinal impact of the myPlan app on health and safety among college women experiencing partner violence. J Interpers Violence 37(13-14):NP11436-NP11459.
Gonzalez-Guarda, R. M., A. L. Florom-Smith, and T. Thomas. 2011. A syndemic model of substance abuse, intimate partner violence, HIV infection, and mental health among Hispanics. Public Health Nurs 28(4):366-378.
Grace, K. T., and J. C. Anderson. 2018. Reproductive coercion: A systematic review. Trauma Violence Abuse 19(4):371-390.
Grace, K. T., M. R. Decker, C. N. Holliday, J. Talis, and E. Miller. 2023. Reproductive coercion in college health clinic patients: Risk factors, care seeking and perpetration. J Adv Nurs 79(4):1464-1475.
Gray, S., and K. M. R. Sizemore, Jonathon. 2023. Coping strategies as a moderator for the association between intimate partner violence and depression and anxiety symptoms among transgender women. Int. J. Environ. Res. Public Health 20(11).
Guadalupe-Diaz, X. L., and J. Jasinski. 2017. “I wasn’t a priority, I wasn’t a victim”: Challenges in help seeking for transgender survivors of intimate partner violence. Violence Against Women 23(6):772-792.
Gupta, R. C., K. A. Randell, and M. D. Dowd. 2021. Addressing parental adverse childhood experiences in the pediatric setting. Adv Pediatr 68:71-88.
Guruge, S., and J. Humphreys. 2009. Barriers affecting access to and use of formal social supports among abused immigrant women. Can J Nurs Res 41(3):64-84.
Gutowski, E. R., S. Freitag, S. Zhang, M. P. Thompson, and N. J. Kaslow. 2023. Intimate partner violence, legal systems and barriers for African American women. J Interpers Violence 38(1-2):NP1279-NP1298.
Guttmacher Institute. 2023. Regulating insurance coverage of abortion. https://www.guttmacher.org/state-policy/explore/regulating-insurance-coverage-abortion (accessed August 16, 2023).
Gwinn, C., G. Strack, S. Adams, and R. Lovelace. 2007. The Family Justice Center Collaborative Model. St. Louis University Public Law Review 27(1):79-120.
Haag, H., D. Jones, T. Joseph, and A. Colantonio. 2022. Battered and brain injured: Traumatic brain injury among women survivors of intimate partner violence—a scoping review. Trauma, Violence, & Abuse 23(4):1270-1287.
Hageman, T. O. N., L. Langenderfer-Magruder, T. Greene, J. H. Williams, J. St. Mary, S. E. McDonald, and F. R. Ascione. 2018. Intimate partner violence survivors and pets: Exploring practitioners’ experiences in addressing client needs. Families in Society 99(2):134-145.
Hahn, C. K., A. K. Gilmore, R. O. Aguayo, and A. A. Rheingold. 2018. Perinatal intimate partner violence. Obstet Gynecol Clin North Am 45(3):535-547.
Hamberger, L. K., B. Ambuel, C. E. Guse, M. B. Phelan, M. Melzer-Lange, and A. Kistner. 2014. Effects of a systems change model to respond to patients experiencing partner violence in primary care medical settings. Journal of Family Violence 29(6):581-594.
Hamby, S., D. Finkelhor, H. Turner, and R. Ormrod. 2011. Children’s exposure to intimate partner violence and other family violence. Edited by U.S. Department of Justice. Office of Justice Programs.
Hanson, E. J. 2023. The 2022 Violence Against Women Act Reauthorization, Congressional Research Service reports. Washington, DC: Congressional Research Service.
Hegarty, K., L. Tarzia, J. Valpied, E. Murray, C. Humphreys, A. Taft, K. Novy, L. Gold, and N. Glass. 2019. An online healthy relationship tool and safety decision aid for women experiencing intimate partner violence (i-decide): A randomised controlled trial. Lancet Public Health 4(6):e301-e310.
Hellman, C. M., C. Gwinn, G. Strack, M. Burke, R. T. Munoz, S. R. Brady, N. Aguirre, and Y. Aceves. 2021. Nurturing hope and well-being among survivors of domestic violence within the family justice center model. Violence and Victims 36(5):651-666.
HHS (Department of Health and Human Services). 2021. Ensuring access to equitable affordable, client-centered, quality family planning services. Federal Register 86(192).
Hollender, M., E. Almirol, M. Meyer, H. Bearden, and K. Stanford. 2023. Sexual assault nurse examiners lead to improved uptake of services: A cross-sectional study. Western Journal of Emergency Medicine 24(5).
Horahan, K., H. Morchel, M. Raheem, and L. Stevens. 2014. Electronic health records access during a disaster. Online J Public Health Inform 5(3):232.
HRSA (Health Resources and Services Administration). 2022. Behavioral health workforce projections, 2020-2035. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/Behavioral-Health-Workforce-Projections-Factsheet.pdf (accessed August 16, 2023).
HRSA. 2023a. 2023-2025 HRSA strategy to address intimate partner violence. Rockville, Maryland: Health Resources and Services Administration.
HRSA. 2023b. 2022 health center data. https://data.hrsa.gov/tools/data-reporting/programdata/national/table?tableName=Full&year=2022 (accessed September 11, 2023).
HRSA. 2023c. Health workforce shortage areas. https://data.hrsa.gov/topics/health-workforce/shortage-areas (accessed August 21, 2023).
HRSA. 2023d. Workforce projections. https://data.hrsa.gov/topics/health-workforce/workforce-projections (accessed September 13, 2023).
HRSA. 2023e. Map gallery. https://data.hrsa.gov/maps/map-gallery (accessed August 21, 2023).
Hung, P., C. E. Henning-Smith, M. M. Casey, and K. B. Kozhimannil. 2017. Access to obstetric services in rural counties still declining, with 9 percent losing services, 2004-14. Health Aff (Millwood) 36(9):1663-1671.
Iverson, K. M., O. Adjognon, A. R. Grillo, M. E. Dichter, C. A. Gutner, A. B. Hamilton, S. W. Stirman, and M. R. Gerber. 2019. Intimate partner violence screening programs in the Veterans Health Administration: Informing scale-up of successful practices. J Gen Intern Med 34(11):2435-2442.
Iverson, K. M., S. B. Danitz, D. R. Shayani, D. Vogt, S. W. Stirman, A. B. Hamilton, C. T. Mahoney, M. R. Gerber, and M. E. Dichter. 2021. Recovering from intimate partner violence through strengths and empowerment: Findings from a randomized clinical trial. J Clin Psychiatry 83(1).
Iverson, K. M., S. B. Danitz, S. K. Low, J. A. Knetig, K. W. Doyle, and L. E. Bruce. 2022. Recovering from Intimate Partner Violence through Strengths and Empowerment (RISE): Initial evaluation of the clinical effects of rise administered in routine care in the US Veterans Health Administration. International Journal of Environmental Research and Public Health 19(14).
James, S. E., J. L. Herman, S. Rankin, M. Keisling, L. Mottet, and M. Anafi. 2016. The report of the 2015 U.S. Transgender Survey.
Jock, B. W. I., G. Dana-Sacco, J. Arscott, M. E. Bagwell-Gray, E. Loerzel, T. Brockie, G. Packard, V. M. O’Keefe, C. E. McKinley, and J. Campbell. 2022. “We’ve already endured the trauma, who is going to either end that cycle or continue to feed it?”: The influence of family and legal systems on Native American women’s intimate partner violence experiences. J Interpers Violence 37(21-22):NP20602-NP20629.
Jose, A., S. A. Nagori, B. Agarwal, O. Bhutia, and A. Roychoudhury. 2016. Management of maxillofacial trauma in emergency: An update of challenges and controversies. J Emerg Trauma Shock 9(2):73-80.
Judge-Golden, C. P., K. J. Smith, M. K. Mor, and S. Borrero. 2019. Financial implications of 12-month dispensing of oral contraceptive pills in the veterans affairs health care system. JAMA Intern Med 179(9):1201-1208.
Juszczak, L., P. Melinkovich, and D. Kaplan. 2003. Use of health and mental health services by adolescents across multiple delivery sites. J Adolesc Health 32(6 Suppl):108-118.
Kapur, N. A., and D. M. Windish. 2011. Optimal methods to screen men and women for intimate partner violence: Results from an internal medicine residency continuity clinic. J Interpers Violence 26(12):2335-2352.
Kast, N. R., M. E. Eisenberg, and R. E. Sieving. 2016. The role of parent communication and connectedness in dating violence victimization among Latino adolescents. J Interpers Violence 31(10):1932-1955.
Kasturirangan, A. 2008. Empowerment and programs designed to address domestic violence. Violence Against Women 14(12):1465-1475.
Kazmerski, T., H. L. McCauley, K. Jones, S. Borrero, J. G. Silverman, M. R. Decker, D. Tancredi, and E. Miller. 2015. Use of reproductive and sexual health services among female family planning clinic clients exposed to partner violence and reproductive coercion. Maternal and Child Health Journal 19:1490-1496.
KFF (Kaiser Family Foundation). 2023a. Abortion in the United States dashboard. https://www.kff.org/womens-health-policy/dashboard/abortion-in-the-u-s-dashboard/ (accessed August 24, 2023).
KFF. 2023b. The availability and use of medication abortion. https://www.kff.org/womenshealth-policy/fact-sheet/the-availability-and-use-of-medication-abortion/ (accessed August 24, 2023).
KFF. 2023c. State profiles for women’s health. https://www.kff.org/interactive/womens-healthprofiles/?activeState=United%20States&activeCategory=coverage (accessed August 25, 2023a).
Kishton, R., L. Sinko, R. Ortiz, M. N. Islam, A. Fredrickson, N. E. Sheils, J. Buresh, P. F. Cronholm, and M. Matone. 2022. Describing the health status of women experiencing violence or abuse: An observational study using claims data. J Prim Care Community Health 13:21501319221074121.
Klein, L. B., B. R. Chesworth, J. R. Howland-Myers, C. F. Rizo, and R. J. Macy. 2021. Housing interventions for intimate partner violence survivors: A systematic review. Trauma Violence Abuse 22(2):249-264.
Kourti, A., A. Stavridou, E. Panagouli, T. Psaltopoulou, C. Spiliopoulou, M. Tsolia, T. N. Sergentanis, and A. Tsitsika. 2023. Domestic violence during the COVID-19 pandemic: A systematic review. Trauma Violence Abuse 24(2):719-745.
Kozhimannil, K. B., J. D. Interrante, M. K. S. Tuttle, and C. Henning-Smith. 2020. Changes in hospital-based obstetric services in rural US counties, 2014-2018. JAMA 324(2):197-199.
Kozhimannil, K. B., V. A. Lewis, J. D. Interrante, P. L. Chastain, and L. Admon. 2023. Screening for and experiences of intimate partner violence in the United States before, during, and after pregnancy, 2016-2019. American Journal of Public Health 113(3):297-305.
Koziol-McLain, J., A. C. Vandal, D. Wilson, S. Nada-Raja, T. Dobbs, C. McLean, R. Sisk, K. B. Eden, and N. E. Glass. 2018. Efficacy of a web-based safety decision aid for women experiencing intimate partner violence: Randomized controlled trial. J Med Internet Res 19(12):e426.
Krishnamurti, T., A. L. Davis, B. Quinn, A. F. Castillo, K. L. Martin, and H. N. Simhan. 2021. Mobile remote monitoring of intimate partner violence among pregnant patients during the COVID-19 shelter-in-place order: Quality improvement pilot study. Journal of Medical Internet Research 23(2):e22790.
Kulkarni, S. 2018. Intersectional trauma-informed intimate partner violence (IPV) services: Narrowing the gap between IPV service delivery and survivor needs. Journal of Family Violence 34(1):55-64.
Kurdyla, V., A. M. Messinger, and M. Ramirez. 2021. Transgender intimate partner violence and help-seeking patterns. Journal of Interpersonal Violence 36(19-20):NP11046-NP11069.
Leemis, R. W., N. Friar, S. Khatiwada, M. S. Chen, M.-j. Kresnow, S. G. Smith, S. Caslin, and K. C. Basile. 2022. The National Intimate Partner and Sexual Violence Survey: 2016/2017 report on intimate partner violence. Atlanta, GA: Centers for Disease Control and Prevention.
Liu, E. C., and W. W. Shen. 2022. The Hyde Amendment: An overview. Congressional Research Service Reports.
Logue, T. C., N. C. Danford, E. C. Bixby, M. M. Levitsky, and M. P. Rosenwasser. 2021. Neck and back sprain and hand flexor tendon repair are more common in victims of domestic violence compared with patients who were not victims of domestic violence: A comparative study of 1,204,596 patients using the National Trauma Data Bank. JAAOS Global Research & Reviews 5(9).
López-Ossorio, J. J., J. L. González-Álvarez, I. Loinaz, A. Martínez-Martínez, and D. Pineda. 2020. Intimate partner homicide risk assessment by police in Spain: The dual protocol VPR5.0-H. Psychosocial Intervention 30(1):47-55. https://doi.org/10.5093/pi2020a16.
Love, H. E., J. Schlitt, S. Soleimanpour, N. Panchal, and C. Behr. 2019. Twenty years of school-based health care growth and expansion. Health Aff (Millwood) 38(5):755-764.
Machtinger, E. L., K. B. Davis, L. S. Kimberg, N. Khanna, Y. P. Cuca, C. Dawson-Rose, M. Shumway, J. Campbell, A. Lewis-O’Connor, M. Blake, A. Blanch, and B. McCaw. 2019. From treatment to healing: Inquiry and response to recent and past trauma in adult health care. Womens Health Issues 29(2):97-102.
MacMillan, H. L., C. N. Wathen, E. Jamieson, M. Boyle, L. A. McNutt, A. Worster, B. Lent, M. Webb, and McMaster Violence Against Women Research Group. 2006. Approaches to screening for intimate partner violence in health care settings: A randomized trial. JAMA 296(5):530-536.
Maleku, A., B. Subedi, Y. K. Kim, H. Haran, and S. Pyakurel. 2022. Toward healing-centered engagement to address mental well-being among young Bhutanese-Nepali refugee women in the United States: Findings from the cultural leadership project. Journal of Ethnic & Cultural Diversity in Social Work:1-19.
Mandal, B., N. Porto, D. E. Kiss, S. H. Cho, and L. S. Head. 2022. Health insurance coverage during the COVID-19 pandemic: The role of Medicaid expansion. J Consum Aff 57(1):296-319.
Mantel, J., and R. Knake. 2018. Legal and ethical impediments to data sharing and integration among medical legal partnership participants. Annals of Health Law 27(2):183-204.
Markman, H. J., M. J. Renick, F. J. Floyd, S. M. Stanley, and M. Clements. 1993. Preventing marital distress through communication and conflict management training: A 4- and 5-year follow-up. J Consult Clin Psychol 61(1):70-77.
Marshall, K. J., D. N. Fowler, M. L. Walters, and A. B. Doreson. 2018. Interventions that address intimate partner violence and HIV among women: A systematic review. AIDS Behav 22(10):3244-3263.
Mastrocinque, J. M., D. Thew, C. Cerulli, C. Raimondi, R. Q. Pollard, Jr., and N. P. Chin. 2017. Deaf victims’ experiences with intimate partner violence: The need for integration and innovation. J Interpers Violence 32(24):3753-3777.
McBain, R. K., J. Cantor, M. F. Pera, J. Breslau, D. M. Bravata, and C. M. Whaley. 2023. Mental health service utilization rates among commercially insured adults in the US during the first year of the COVID-19 pandemic. JAMA Health Forum 4(1). https://doi.org/10.1001/jamahealthforum.2022.4936.
McFarlane, J., A. Malecha, J. Gist, K. Watson, E. Batten, I. Hall, and S. Smith. 2004. Increasing the safety-promoting behaviors of abused women: In this study, a telephone intervention for victims of intimate-partner violence showed efficacy for 18 months. AJN The American Journal of Nursing 104(3):40-50.
Mcintosh-Clarke, D. R., M. N. Zeman, H. A. Valand, and R. K. Tu. 2019. Incentivizing physician diversity in radiology. Journal of the American College of Radiology 16(4, Part B):624-630.
McKay, T. E., M. L. Kan, J. Landwehr, and E. Miller. 2021. When disclosure isn’t the goal: Exploring responses to partner violence victimization screening and universal education among youth and adults. Journal of Family Violence 37(3):487-504.
McLennan, J. D., and H. L. MacMillan. 2016. Routine primary care screening for intimate partner violence and other adverse psychosocial exposures: What’s the evidence? BMC Family Practice 17(1):103.
Messing, J. T., Y. Amanor-Boadu, C. E. Cavanaugh, N. E. Glass, and J. C. Campbell. 2013. Culturally competent intimate partner violence risk assessment: Adapting the danger assessment for immigrant women. Social Work Research 37(3):263-275.
Messing, J. T., J. Campbell, J. Sullivan Wilson, S. Brown, and B. Patchell. 2017. The lethality screen: The predictive validity of an intimate partner violence risk assessment for use by first responders. Journal of Interpersonal Violence 32(2):205-226.
Messing, J. T., J. Campbell, K. Dunne, and S. Dubus. 2020. Development and testing of the danger assessment for law enforcement (da-le). Social Work Research 44(3):143-156.
Meyer, J. P., S. A. Springer, and F. L. Altice. 2011. Substance abuse, violence, and HIV in women: A literature review of the syndemic. J Womens Health (Larchmt) 20(7):991-1006.
Miller, E., M. R. Decker, A. Raj, E. Reed, D. Marable, and J. G. Silverman. 2010. Intimate partner violence and health care-seeking patterns among female users of urban adolescent clinics. Maternal and Child Health Journal 14:910-917.
Miller, E., M. R. Decker, H. L. McCauley, D. J. Tancredi, R. R. Levenson, J. Waldman, P. Schoenwald, and J. G. Silverman. 2011. A family planning clinic partner violence intervention to reduce risk associated with reproductive coercion. Contraception 83(3):274-280.
Miller, E., D. J. Tancredi, H. L. McCauley, M. R. Decker, M. C. D. Virata, H. A. Anderson, B. O’Connor, and J. G. Silverman. 2013. One-year follow-up of a coach-delivered dating violence prevention program: A cluster randomized controlled trial. Am J Prev Med 45(1):108-112.
Miller, E., H. L. McCauley, D. J. Tancredi, M. R. Decker, H. Anderson, and J. G. Silverman. 2014. Recent reproductive coercion and unintended pregnancy among female family planning clients. Contraception 89(2):122-128.
Miller, E., S. Goldstein, H. L. McCauley, K. A. Jones, R. N. Dick, J. Jetton, J. G. Silverman, S. Blackburn, E. Monasterio, L. James, and D. J. Tancredi. 2015. A school health center intervention for abusive adolescent relationships: A cluster RCT. Pediatrics 135(1):76-85.
Miller, E., D. J. Tancredi, M. R. Decker, H. L. McCauley, K. A. Jones, H. Anderson, L. James, and J. G. Silverman. 2016. A family planning clinic-based intervention to address reproductive coercion: A cluster randomized controlled trial. Contraception 94(1):58-67.
Miller, E., H. L. McCauley, M. R. Decker, R. Levenson, S. Zelazny, K. A. Jones, H. Anderson, and J. G. Silverman. 2017. Implementation of a family planning clinic-based partner violence and reproductive coercion intervention: Provider and patient perspectives. Perspect Sex Reprod Health 49(2):85-93.
Miller, E., K. A. Jones, A. J. Culyba, T. Paglisotti, N. Dwarakanath, M. Massof, Z. Feinstein, K. A. Ports, D. Espelage, J. Pulerwitz, A. Garg, J. Kato-Wallace, and K. Z. Abebe. 2020. Effect of a community-based gender norms program on sexual violence perpetration by adolescent boys and young men: A cluster randomized clinical trial. JAMA Network Open 3(12):e2028499.
Miller, C. J., K. Stolzmann, M. E. Dichter, O. L. Adjognon, J. E. Brady, G. A. Portnoy, M. R. Gerber, S. Iqbal, and K. M. Iverson. 2022. Intimate partner violence screening for women in the Veterans Health Administration: Temporal trends from the early years of implementation 2014-2020. J Aggress Maltreat Trauma a:1-19.
Miller-Walfish, S., J. Kwon, C. Raible, A. Ali, J. H. Bell, L. James, and E. Miller. 2021. Promoting cross-sector collaborations to address intimate partner violence in health care delivery systems using a quality assessment tool. J Womens Health (Larchmt) 30(11):1660-1666.
Mitchell, S. A., L. A. Charles, and N. Downing. 2022. Increasing access to forensic nursing services in rural and underserved areas of Texas. J Forensic Nurs 18(1):21-29.
Miyamoto, S., E. Thiede, L. Dorn, D. F. Perkins, C. Bittner, and D. Scanlon. 2021. The Sexual Assault Forensic Examination Telehealth (SAFE-T) Center: A comprehensive, nurse-led telehealth model to address disparities in sexual assault care. J Rural Health 37(1):92-102.
Mogos, M. F., W. N. Araya, S. W. Masho, J. L. Salemi, C. Shieh, and H. M. Salihu. 2016. The feto-maternal health cost of intimate partner violence among delivery-related discharges in the United States, 2002-2009. J Interpers Violence 31(3):444-464.
Monterrosa, A. E. 2021. How race and gender stereotypes influence help-seeking for intimate partner violence. J Interpers Violence 36(17-18):NP9153-NP9174.
Morris, A., S. Goletz, and J. Friona. 2022. Indiana sexual assault nurse examiner training initiative: Positive impacts for medical forensic care. J Forensic Nurs 18(3):146-155.
Moynihan, M. M., V. L. Banyard, A. C. Cares, S. J. Potter, L. M. Williams, and J. G. Stapleton. 2015. Encouraging responses in sexual and relationship violence prevention: What program effects remain 1 year later? J Interpers Violence 30(1):110-132.
National Coalition Against Domestic Violence. n.d. Resources. https://ncadv.org/RESOURCES (accessed May 8, 2023).
Nelson, H. D., B. G. Darney, K. Ahrens, A. Burgess, R. M. Jungbauer, A. Cantor, C. Atchison, K. B. Eden, R. Goueth, and R. Fu. 2022. Associations of unintended pregnancy with maternal and infant health outcomes: A systematic review and meta-analysis. JAMA 328(17):1714-1729.
Niolon, P. H., M. C. Kearns, J. Dills, K. Rambo, S. M. Irving, T. L. Armstead, and L. K. Gilbert. 2017. Preventing intimate partner violence across the lifespan: A technical package of programs, policies, and practices. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Niolon, P. H., A. M. Vivolo-Kantor, A. J. Tracy, N. E. Latzman, T. D. Little, S. DeGue, K. M. Lang, L. F. Estefan, S. R. Ghazarian, W. L. K. McIntosh, B. Taylor, L. L. Johnson, H. Kuoh, T. Burton, B. Fortson, E. A. Mumford, S. C. Nelson, H. Joseph, L. A. Valle, and A. T. Tharp. 2019. An RCT of dating matters: Effects on teen dating violence and relationship behaviors. Am J Prev Med 57(1):13-23.
North Carolina Department of Health and Human Services. Healthy opportunities. https://www.ncdhhs.gov/about/department-initiatives/healthy-opportunities (accessed August 25, 2023).
NYSDOH (New York State Department of Health). 2013. Guidelines for integrating domestic violence screening into HIV counseling, testing, referral & partner notification. https://www.health.ny.gov/diseases/aids/providers/regulations/domesticviolence/guide.htm (accessed May 8, 2023).
OASH (Office of the Assistant Secretary for Health). 2022. Equitable long-term recovery and resilience. https://health.gov/our-work/national-health-initiatives/equitable-long-term-recovery-and-resilience (accessed August 20, 2023).
O’Doherty, L., K. Hegarty, J. Ramsay, L. L. Davidson, G. Feder, and A. Taft. 2015. Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev 2015(7):CD007007.
Ogbe, E., S. Harmon, R. Van den Bergh, and O. Degomme. 2020. A systematic review of intimate partner violence interventions focused on improving social support and mental health outcomes of survivors. PLoS ONE 15(6):e0235177.
Olds, D., and E. Yost. 2020. Developing the nurse-family partnership. Designing Evidence-Based Public Health and Prevention Programs. London, UK: Routledge. Pp. 173-193.
Ollen, E. W., V. E. Ameral, K. Palm Reed, and D. A. Hines. 2017. Sexual minority college students’ perceptions on dating violence and sexual assault. J Counseling Psych 64(1):112-119.
Ombayo, B., B. Black, and K. M. Preble. 2019. Adolescent–parent communication among youth who have and have not experienced dating violence. Child and Adolescent Social Work Journal 36(4):381-390.
Overstreet, N. M., and D. M. Quinn. 2013. The intimate partner violence stigmatization model and barriers to help-seeking. Basic Applied Soc Psych 35(1):109-122.
Pavao, J., J. Alvarez, N. Baumrind, M. Induni, and R. Kimerling. 2007. Intimate partner violence and housing instability. Am J Prev Med 32(2):143-146.
Pearce, M. E., K. Jongbloed, L. Demerais, H. MacDonald, W. M. Christian, R. Sharma, N. Pick, E. M. Yoshida, P. M. Spittal, and M. B. Klein. 2019. “Another thing to live for”: Supporting HCV treatment and cure among indigenous people impacted by substance use in Canadian cities. Int J Drug Policy 74:52-61.
Peterson, C., M. C. Kearns, W. L. McIntosh, L. F. Estefan, C. Nicolaidis, K. E. McCollister, A. Gordon, and C. Florence. 2018. Lifetime economic burden of intimate partner violence among U.S. adults. Am J Prev Med 55(4):433-444.
Piolanti, A., and H. M. Foran. 2022. Efficacy of interventions to prevent physical and sexual dating violence among adolescents: A systematic review and meta-analysis. JAMA Pediatr 176(2):142-149.
Pleasants, E. A., A. F. Cartwright, and U. D. Upadhyay. 2022. Association between distance to an abortion facility and abortion or pregnancy outcome among a prospective cohort of people seeking abortion online. JAMA Netw Open 5(5):e2212065.
Ponce, A. N., M. S. Lawless, and M. Rowe. 2014. Homelessness, behavioral health disorders and intimate partner violence: Barriers to services for women. Community Ment Health J 50(7):831-840.
Porsch, L. M., M. Xu, C. B. Veldhuis, L. A. Bochicchio, S. S. Zollweg, and T. L. Hughes. 2022. Intimate partner violence among sexual minority women: A scoping review. Trauma, Violence, & Abuse 24(5):3014-3036. https://doi.org/10.1177/15248380221122815.
Pritchard, A. J., A. Reckdenwald, and C. Nordham. 2017. Nonfatal strangulation as part of domestic violence: A review of research. Trauma, Violence, & Abuse 18(4):407-424.
Rader, B., U. D. Upadhyay, N. K. R. Sehgal, B. Y. Reis, J. S. Brownstein, and Y. Hswen. 2022. Estimated travel time and spatial access to abortion facilities in the US before and after the Dobbs v Jackson women’s health decision. JAMA 328(20):2041-2047.
Ragavan, M. I., and E. Miller. 2022. Healing-centered care for intimate partner violence survivors and their children. Pediatrics 149(6).
Ragavan, M. I., L. Risser, V. Duplessis, S. DeGue, A. Villaveces, T. P. Hurley, J. Chang, E. Miller, and K. A. Randell. 2022. The impact of the COVID-19 pandemic on the needs and lived experiences of intimate partner violence survivors in the United States: Advocate perspectives. Violence Against Women 28(12-13):3114-3134.
Ramaswamy, A., B. Frederiksen, M. Rae, U. Ranji, A. Salganicoff, and D. McDermott. 2022. Rebuilding Title X: New regulations for the federal family planning program. https://www.kff.org/womens-health-policy/issue-brief/out-of-pocket-charges-for-rape-kits-and-services-for-sexual-assault-survivors/ (accessed August 20, 2023).
Ravi, K. E., S. R. Robinson, and R. V. Schrag. 2022. Facilitators of formal help-seeking for adult survivors of IPV in the United States: A systematic review. Trauma Violence Abuse 23(5):1420-1436.
Reidy, D. E., K. M. Holland, K. Cortina, B. Ball, and B. Rosenbluth. 2017. Evaluation of the expect respect support group program: A violence prevention strategy for youth exposed to violence. Prev Med 100:235-242.
Rickert, V. I., C. M. Wiemann, S. D. Harrykissoon, A. B. Berenson, and E. Kolb. 2002. The relationship among demographics, reproductive characteristics, and intimate partner violence. American Journal of Obstetrics and Gynecology 187(4):1002-1007.
Rivara, F. P., M. L. Anderson, P. Fishman, A. E. Bonomi, R. J. Reid, D. Carrell, and R. S. Thompson. 2007. Healthcare utilization and costs for women with a history of intimate partner violence. Am J Prev Med 32(2):89-96.
Rivas, C., C. Vigurs, J. Cameron, and L. Yeo. 2019. A realist review of which advocacy interventions work for which abused women under what circumstances. Cochrane Database of Systematic Reviews 6.
Robinson, S. R., K. Ravi, and R. J. Voth Schrag. 2021. A systematic review of barriers to formal help seeking for adult survivors of IPV in the United States, 2005-2019. Trauma Violence Abuse 22(5):1279-1295.
Rodriguez, M., J. M. Valentine, J. B. Son, and M. Muhammad. 2009. Intimate partner violence and barriers to mental health care for ethnically diverse populations of women. Trauma Violence Abuse 10(4):358-374.
Rollins, C., N. E. Glass, N. A. Perrin, K. A. Billhardt, A. Clough, J. Barnes, G. C. Hanson, and T. L. Bloom. 2012. Housing instability is as strong a predictor of poor health outcomes as level of danger in an abusive relationship: Findings from the SHARE study. J Interpers Violence 27(4):623-643.
Rossi, F. S., M. Shankar, K. Buckholdt, Y. Bailey, S. T. Israni, and K. M. Iverson. 2020. Trying times and trying out solutions: Intimate partner violence screening and support for women veterans during covid-19. J Gen Intern Med 35(9):2728-2731.
Sabri, B., S. Tharmarajah, V. P. S. Njie-Carr, J. T. Messing, E. Loerzel, J. Arscott, and J. C. Campbell. 2021. Safety planning with marginalized survivors of intimate partner violence: Challenges of conducting safety planning intervention research with marginalized women. Trauma, Violence, and Abuse 23(5):1728-1751. https://doi.org/10.1177/15248380211013136.
Saftlas, A. F., K. K. Harland, A. B. Wallis, J. Cavanaugh, P. Dickey, and C. Peek-Asa. 2014. Motivational interviewing and intimate partner violence: A randomized trial. Ann Epidemiol 24(2):144-150.
Scheer, J. R., M. Lawlace, C. J. Cascalheira, M. E. Newcomb, and S. W. Whitton. 2023. Help-seeking for severe intimate partner violence among sexual and gender minority adolescents and young adults assigned female at birth: A latent class analysis. J Interpers Violence 38(9-10):6723-6750.
Scheer, J. R., A. Martin-Storey, and L. Baams. 2020. Help-seeking barriers among sexual and gender minority individuals who experience intimate partner violence victimization. In Intimate partner violence and the LGBT+ community: Understanding power dynamics. Edited by B. Russell. Cham: Springer International Publishing. Pp. 139-158.
Schmidt, M., S. K. Kedia, P. J. Dillon, and K. H. Howell. 2023. Challenges to help-seeking among women of color exposed to intimate partner violence. J Interpers Violence 38(13-14):8088-8113.
Schoenthaler, A., E. Montague, L. Baier Manwell, R. Brown, M. D. Schwartz, and M. Linzer. 2014. Patient–physician racial/ethnic concordance and blood pressure control: The role of trust and medication adherence. Ethnicity & Health 19(5):565-578.
Sharps, P. W., L. F. Bullock, J. C. Campbell, J. L. Alhusen, S. R. Ghazarian, S. S. Bhandari, and D. L. Schminkey. 2016. Domestic violence enhanced perinatal home visits: The DOVE randomized clinical trial. J Womens Health (Larchmont) 25(11):1129-1138.
Shorey, R. C., V. Tirone, and G. L. Stuart. 2014. Coordinated community response components for victims of intimate partner violence: A review of the literature. Aggress Violent Behav 19(4):363-371.
Smith, C. W., R. J. Kreitzer, K. A. Kane, and T. M. Saunders. 2022. Contraception deserts: The effects of Title X rule changes on access to reproductive health care resources. Politics & Gender 18(3):672-707.
Smith, E. J., B. A. Bailey, and A. Cascio. 2023. Sexual coercion, intimate partner violence, and homicide: A scoping literature review. Trauma Violence Abuse 25(1):341-353. https://doi.org/10.1177/15248380221150474.
Snyder, J. E., R. D. Upton, T. C. Hassett, H. Lee, Z. Nouri, and M. Dill. 2023. Black representation in the primary care physician workforce and its association with population life expectancy and mortality rates in the US. JAMA Network Open 6(4):e236687-e236687.
Sorenson, S. B. 2017. Guns in intimate partner violence: Comparing incidents by type of weapon. J Womens Health (Larchmont) 26(3):249-258.
Sorenson, S. B., and R. A. Schut. 2018. Nonfatal gun use in intimate partner violence: A systematic review of the literature. Trauma Violence Abuse 19(4):431-442.
Spencer, C. M., and S. M. Stith. 2020. Risk factors for male perpetration and female victimization of intimate partner homicide: A meta-analysis. Trauma Violence Abuse 21(3):527-540.
Sprague, S., K. Madden, S. Dosanjh, K. Godin, J. C. Goslings, E. H. Schemitsch, and M. Bhandari. 2013a. Intimate partner violence and musculoskeletal injury: Bridging the knowledge gap in orthopaedic fracture clinics. BMC Musculoskelet Disord 14(1):23.
Sprague, S., M. Bhandari, G. J. Della Rocca, J. C. Goslings, R. W. Poolman, K. Madden, N. Simunovic, S. Dosanjh, and E. H. Schemitsch. 2013b. Prevalence of abuse and intimate partner violence surgical evaluation (PRAISE) in orthopaedic fracture clinics: A multinational prevalence study. Lancet 382(9895):866-876.
Stockman, J. K., M. B. Lucea, R. Bolyard, D. Bertand, G. B. Callwood, P. W. Sharps, D. W. Campbell, and J. C. Campbell. 2014. Intimate partner violence among African American and African Caribbean women: Prevalence, risk factors, and the influence of cultural attitudes. Glob Health Action 7:24772.
Stockman, J. K., H. Hayashi, and J. C. Campbell. 2015. Intimate partner violence and its health impact on ethnic minority women [corrected]. J Womens Health (Larchmt) 24(1):62-79.
Summers-Gabr, N. M. 2020. Rural-urban mental health disparities in the United States during COVID-19. Psychol Trauma 12(S1):S222-S224.
Sutherland, M. A., H. C. Fantasia, M. K. Hutchinson, and J. Katz. 2021. Individual and institutional predictors of IPV/SV screening in college health centers. J Interpers Violence 36(3-4):1330-1355.
Sutton, A., H. Beech, B. Ozturk, and D. Nelson-Gardell. 2021. Preparing mental health professionals to work with survivors of intimate partner violence: A comprehensive systematic review of the literature. Affilia 36(3):426-440.
Tarzia, L., M. A. Bohren, J. Cameron, C. Garcia-Moreno, L. O’Doherty, R. Fiolet, L. Hooker, M. Wellington, R. Parker, J. Koziol-Mclain, G. Feder, and K. Hegarty. 2020. Women’s experiences and expectations after disclosure of intimate partner abuse to a healthcare provider: A qualitative meta-synthesis. BMJ Open 10(11):e041339.
Taylor, C. A., J. M. Bell, M. J. Breiding, and L. Xu. 2017. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths - United States, 2007 and 2013. MMWR Surveillance Summaries 66(9):1-16.
Thackeray, J., N. Livingston, M. I. Ragavan, J. Schaechter, E. Sigel, Council on Child Abuse and Neglect, Council on Injury, Violence, and Poison Prevention. 2023. Intimate partner violence: Role of the pediatrician. Pediatrics 152(1).
Thiede, E., and S. Miyamoto. 2021. Rural availability of sexual assault nurse examiners (SANES). J Rural Health 37(1):81-91.
Turkstra, L. S., K. Salanki, E. MacIntyre, N. Kim, J. Jin, S. Sprague, T. Scott, and M. Bhandari. 2023. What is the prevalence of intimate partner violence and traumatic brain injury in fracture clinic patients? Clin Orthop Relat Res 481(1):132-142.
Uscher-Pines, L., J. Cantor, H. A. Huskamp, A. Mehrotra, A. Busch, and M. Barnett. 2020. Adoption of telemedicine services by substance abuse treatment facilities in the U.S. J Subst Abuse Treat 117:108060.
Uscher-Pines, L., C. M. McCullough, J. L. Sousa, S. D. Lee, A. J. Ober, D. Camacho, and K. A. Kapinos. 2023. Changes in in-person, audio-only, and video visits in California’s federally qualified health centers, 2019-2022. JAMA 329(14):1219-1221.
USPSTF (U.S. Preventive Services Task Force), S. J. Curry, A. H. Krist, D. K. Owens, M. J. Barry, A. B. Caughey, K. W. Davidson, C. A. Doubeni, J. W. Epling, Jr., D. C. Grossman, A. R. Kemper, M. Kubik, A. Kurth, C. S. Landefeld, C. M. Mangione, M. Silverstein, M. A. Simon, C. W. Tseng, and J. B. Wong. 2018. Screening for intimate partner violence, elder abuse, and abuse of vulnerable adults: US Preventive Services Task Force final recommendation statement. JAMA 320(16):1678-1687.
Vakkalanka, J. P., M. M. Nataliansyah, K. A. S. Merchant, L. J. Mack, S. Parsons, N. M. Mohr, and M. M. Ward. 2022. Telepsychiatry services across an emergency department network: A mixed methods study of the implementation process. American Journal of Emergency Medicine 59:79-84.
Valera, E. M., J. C. Daugherty, O. C. Scott, and H. Berenbaum. 2022. Strangulation as an acquired brain injury in intimate-partner violence and its relationship to cognitive and psychological functioning: A preliminary study. Journal of Head Trauma Rehabilitation 37(1):15-23.
Vavala, G., Q. Wang, S. Jimenez, W. E. Ramos, M. A. Ocasio, A. Romero-Espinoza, R. Flynn, R. Bolan, M. I. Fernandez, P. Doan, E. M. Arnold, D. Swendeman, W. S. Comulada, and J. D. Klausner. 2022. Substance use, violence, and sexual risk among young cis-gender women placed at high-risk for human immunodeficiency virus infection. AIDS Behav 26(9):3008-3015.
Velonis, A. J., P. O’Campo, J. J. Rodrigues, and P. Buhariwala. 2019. Using implementation science to build intimate partner violence screening and referral capacity in a fracture clinic. J Eval Clin Pract 25(3):381-389.
Wadsworth, P., C. Kothari, G. Lubwama, C. L. Brown, and J. Frank Benton. 2018. Health and health care from the perspective of intimate partner violence adult female victims in shelters: Impact of IPV, unmet needs, barriers, experiences, and preferences. Fam Community Health 41(2):123-133.
Wagner, A. L., S. Sheinfeld Gorin, M. L. Boulton, B. A. Glover, and J. D. Morenoff. 2021. Effect of vaccine effectiveness and safety on COVID-19 vaccine acceptance in Detroit, Michigan, July 2020. Hum Vaccin Immunother 17(9):2940-2945.
Wallace, M., L. Dyer, E. Felker-Kantor, J. Benno, D. Vilda, E. Harville, and K. Theall. 2021. Maternity care deserts and pregnancy-associated mortality in Louisiana. Womens Health Issues 31(2):122-129.
Weigel, G., B. Frederiksen, U. Ranji, and A. Saiganicoff. 2021. Obgyns and the provision of sexual and reproductive health care: Key findings from a national survey. https://www.kff.org/womens-health-policy/report/obgyns-and-the-provision-of-sexual-and-reproductive-health-care-key-findings-from-a-national-survey/#:~:text=The%20vast%20majority%20of%20OBGYNs%20provided%20most%20forms%20of%20hormonal,and%20resources%20to%20address%20psychosocial (accessed September 13, 2023).
White House. 2013. Addressing the intersection of HIV/AIDS, violence against women and girls, & gender–related health disparities. https://obamawhitehouse.archives.gov/sites/default/files/docs/vaw-hiv_working_group_report_final_-_9-6--2013.pdf (accessed August 21, 2023).
White, K. O., and C. Westhoff. 2011. The effect of pack supply on oral contraceptive pill continuation: A randomized controlled trial. Obstet Gynecol 118(3):615-622.
Wiggins, B., K. Anastasiou, and D. N. Cox. 2021. A systematic review of key factors in the effectiveness of multisector alliances in the public health domain. Am J Health Promot 35(1):93-105.
Willie, T. C., L. Sharpless, M. Monger, T. S. Kershaw, W. B. Mahoney, and J. K. Stockman. 2022. Enhancing domestic violence advocates’ ability to discuss HIV pre-exposure prophylaxis (PREP): Feasibility and acceptability of an educational intervention. Womens Health (Lond) 18:17455065211070548.
Wilson, K. S., M. R. Silberberg, A. J. Brown, and S. D. Yaggy. 2007. Health needs and barriers to healthcare of women who have experienced intimate partner violence. Journal of Women’s Health 16(10):1485-1498.
WPSI (Women’s Preventive Services Initiative). 2022. Women’s Preventive Services Initiative 2022 coding guide. American College of Obstetricians and Gynecologists.
This page intentionally left blank.