
MEDICAL MEMORANDA
Formalin Asthma in Hospital Staff
D.J.HENDRICK, D.J.LANE
British Medical Journal, 1975, 1, 607–608
Few cases of airways obstruction attributable to inhaled formaldehyde have been reported, though it has been suggested that the presence of formaldehyde contributes to the aggravation of chest diseases caused by air pollution (Kotin and Falk, 1964). Occupational “formalin asthma” has been described in a worker in a match factory (Vaughan, 1939) and in workers employed in the tanning and rubber industries (Popa et al., 1969). We report here the use of inhalation provocation tests to investigate the relevance of inhaled formalin fumes to airways obstruction in two hospital staff members continually exposed to this substance in the course of their work.
Case 1
This patient was a 41-year-old nursing sister who began working with formalin in a renal dialysis unit in 1969. She developed a persistent dry cough and episodic attacks of wheezing within a few months which were not improved when she stopped smoking. On two occasions wheezing began four to five hours after exposure for five to 20 minutes to spilled undiluted formalin B.P.C. (34–38% solution of formaldehyde in water w/w). There were no other obvious provoking factors. In 1973 her wheezing, accompanied by increasing breathlessness and rhinitis, became persistent and her cough became productive. Treatment with antibiotics and bronchodilators brought little relief and in June 1973 she was obliged to take sick leave, during
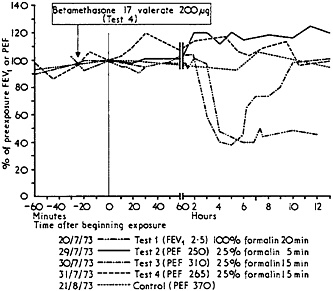
FIG. 1—Case 1. Results of inhalation provocation tests. Values in parentheses are readings obtained immediately before each exposure.
|
|
Chest Clinic, Churchill Hospital, Oxford OX3 7LJ D.J.HENDRICK, M.B., M.R.C.P., Senior Registrar D.J.LANE, D.M., M.R.C.P., Consultant Physician |
which she slowly recovered. A chest x-ray film showed inflammatory changes in the apical segment of the right lower lobe. The haemoglobin was 13·4 g/dl and the W.B.C. was 13·1×109/1 (13 100/mm3), of which 2·1×109/1 (2100/mm3) were eosinophils. Routine skin prick tests with 12 common allergens proved negative.
Inhalation provocation tests were begun one month later, when she was receiving no medication. She simulated occupational exposure by “painting” formalin on identical cardboard pieces on different mornings within a confined space. A nose clip prevented her recognizing 25% but not 100% formalin. Ventilatory function was monitored by measurement of forced expiratory volume in one second (FEV1) using a dry spirometer (Vitalograph) or peak expiratory flow (PEF) using a Wright’s meter. The results, expressed as % change, are shown in fig. 1. The late asthmatic reaction seen in test 1 persisted for some days and like that of test 3 showed little objective response to inhaled salbutamol. It was inhibited by prior inhalation of betamethasone 17-valerate 200 µg (test 4). There was no febrile response or significant change in W.B.C. or eosinophil count after any of these tests.
After these studies extractor fans were fitted to the dialysis unit, and undiluted formalin was handled more carefully. The nurse avoided unnecessary exposure and, in particular, no longer cleared up spilled undiluted formalin herself. With these measures her symptoms were completely relieved and she needed no medication.
Case 2
A 59-year-old pathologist had suffered mild asthma as a child and hay fever from the age of 19. Airways obstruction had recurred in 1970 and been slowly progressive ever since. He smoked a pipe and had worked with formalin continually for 17 years. He thought that prolonged exposures worsened his symptoms during the evening after. Routine investigations showed an eosinophilia of 1·19×109/1 (1188/mm3), and a skin-prick test produced a positive reaction to grass pollen. There was no other abnormality.
Inhalation provocation tests were conducted as in case 1. Increasing exposures to formalin produced no febrile or haematological response and no significant change in the pattern of ventilatory function from that shown on a control day (fig. 2). The exposure of test 4 was thought to have exceeded the daily maximum encountered naturally in the course of his work. He may consequently be regarded as a control to case 1.
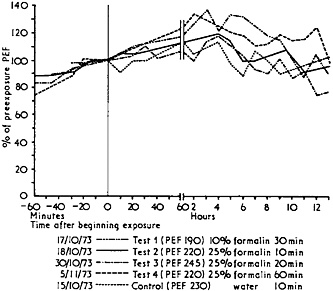
FIG. 2—Case 2. Results of inhalation provocation tests. Values in parentheses are readings obtained immediately before each exposure.
Reprinted with permission from Hendrick and Lane, BMJ 1(5958):607–8, Copyright 1975, BMJ Publishing Group.
Comment
The value of inhalation provocation tests as an adjunct to a carefully taken occupational history in the investigation of airways obstruction is well illustrated by these two cases. The suspected aetiological role of formalin was confirmed in one patient but excluded in the other. As a result measures of environmental control were introduced where appropriate, with good effect.
The responses observed in case 1 seemed to be specific asthmatic reactions to formalin fumes. They began between two and four hours after exposure was begun. The greater the exposure the longer the reaction persisted, though the maximum percentage fall in ventilatory function was similar, provided exposure was sufficiently prolonged to provoke a positive response. Similar late asthmatic reactions have been described after the inhalation of fumes of other chemicals, including tolylene di-isocyanate (Pepys et al., 1972) and aminoethyl ethanolamine (Sterling, 1967; Pepys and Pickering, 1972). Such reactions may be inhibited by the prior inhalation of corticosteroid aerosols (Pepys et al., 1974), and this was confirmed in our patient though subsequent treatment did not in the event prove
We thank the medical illustration department, Radcliffe Infirmary, for the illustrations.
References
Kotin, P., and Falk, H.L. (1964). Annual Review of Medicine, 15, 233.
Pepys, J., et al. (1972). Clinical Allergy, 2, 225.
Pepys, J., and Pickering, C.A.C. (1972). Clinical Allergy, 2, 197.
Pepys, J., et al. (1974). Clinical Allergy, 4, 13.
Popa, V., et al. (1969). Diseases of the Chest, 56, 395.
Sterling, G.M. (1967). Thorax, 22, 533.
Vaughan, W.T. (1939). The Practice of Allergy, p. 677. St. Louis, Mosby.


