
The New England Journal of Medicine
©Copyright, 1977, by the Massachusetts Medical Society
Volume 297 DECEMBER 1, 1977 Number 22
LEGIONNAIRES’ DISEASE
Description of an Epidemic of Pneumonia
DAVID W.FRASER, M.D., THEODORE R.TSAI, M.D., WALTER ORENSTEIN, M.D., WILLIAM E.PARKIN, D.V.M., DR. P.H., H.JAMES BEECHAM, M.D., ROBERT G.SHARRAR, M.D., JOHN HARRIS, M.D., GEORGE F.MALLISON, M.P.H., STANLEY M.MARTIN, M.S., JOSEPH E.MCDADE, PH.D., CHARLES C.SHEPARD, M.D., PHILIP S.BRACHMAN, M.D., AND THE FIELD INVESTIGATION TEAM*
Abstract An explosive, common-source outbreak of pneumonia caused by a previously unrecognized bacterium affected primarily persons attending an American Legion convention in Philadelphia in July, 1976. Twenty-nine of 182 cases were fatal. Spread of the bacterium appeared to be air borne. The source of the bacterium was not found, but epidemiologic analysis suggested that exposure may have occurred in the lobby of the headquarters hotel or in the area immediately surrounding the hotel. Person-to-person spread seemed not to have occurred. Many hotel employees appeared to be immune, suggesting that the agent may have been present in the vicinity, perhaps intermittently, for two or more years. (N Engl J Med 297:1189–1197, 1977)
NEW infectious diseases continue to be found with the aid of increasingly sophisticated laboratory methods for identifying microbial agents. Often, it is through investigation of an epidemic—as recently with Lassa fever1 and Ebola-virus disease2— that new organisms and new diseases are identified. The occurrence of an epidemic signals the need for an investigation of a previously unrecognized problem and presents a cluster of cases in which, by means of appropriate comparisons with controls, a common epidemiologic, clinical, and microbiologic thread can be sought. On the centennial of Koch’s discovery that bacteria caused anthrax, an explosive outbreak of pneumonia occurred in Pennsylvania, mostly in persons who had attended an American Legion convention. We describe the epidemic, the clinical illness and, in a companion paper,3 the evidence that it is caused by a bacterium not previously recognized as a cause of human disease.
|
|
Address reprint requests to the Center for Disease Control (attention of Dr. Fraser) Bacterial Diseases Division, Bureau of Epidemiology, Atlanta, GA 30333. |
BACKGROUND
The 58th annual convention of the American Legion, Department of Pennsylvania, was held in Philadelphia July 21–24, 1976. The headquarters of the convention was in Hotel A. During the same period, the 56th annual convention of the American Legion Auxiliary, Department of Pennsylvania, was also held in Philadelphia, with headquarters in Hotel B. Persons who attended the conventions included American Legion delegates, delegates of the Ladies Auxiliary, members of the families of Legion and Auxiliary delegates, and other Legionnaires with no formal role at the conventions.
Official activities of the American Legion Convention incuded meetings for all delegates, a parade, a testimonial dinner, a dance, committee meetings, regional caucuses and a breakfast. Unofficial activity centered around the Hotel A lobby, a sidewalk in front of the hotel and several hospitality rooms. Each of the 13 candidates for major office reserved a room or a suite of rooms in Hotel A to serve as a hospitality room for entertaining delegates. Each district and many of the local posts had their own hospitality rooms, which were scattered throughout several hotels. Liquor—most commonly beer and whiskey with or without mixers and ice—was served along with simple snacks.
Hotel A was constructed in 1904 and has been extensively modified and renovated since. Hotel guests were housed in approximately 700 rooms on the sec-
Reprinted with permission from Fraser, et al., The New England Journal of Medicine 297(22):1189–1197, Copyright 1977, Massachusetts Medical Society.
ond through 16th floors. The lobby floor, which is slightly above street level, included a registration desk, a counter for the sale of newspapers and sundries, several shops and airline offices, ladies’ and men’s rooms and two restaurants and lounges. Meeting rooms were on the first and 18th floors. The air-conditioning system consisted of two water chillers in the subbasement from which chilled water was circulated to approximately 60 air-handling units in the building.
METHODS
Case Definition
A case was considered Legionnaires’ disease if it met clinical and epidemiologic criteria. The clinical criteria required that a person have onset between July 1 and August 18, 1976, of an illness characterized by cough and fever (temperature of 38.9°C or higher) or any fever and chest x-ray evidence of pneumonia. To meet the epidemiologic criteria, a patient either had to have attended the American Legion Convention held July 21–24, 1976, in Philadelphia or had to have entered Hotel A between July 1 and the onset of the illness. A person was considered to have had Broad Street pneumonia if he met the clinical but not the epidemiologic criteria for Legionnaires’ disease but had been within one block of Hotel A between July 1 and the onset of illness. A person was considered to have seroconversion if there was a fourfold or greater rise in titer to 1:64 or higher by indirect fluorescent-antibody measurement using as antigen the unnamed gram-negative bacterium implicated as the cause of Legionnaires’ disease.3 A person was considered seropositive if he had a titer of 1:128 or greater by indirect fluorescent-antibody assay.
Case Finding
Information about cases was obtained through active and passive surveillance. After recognition on August 2 that an outbreak had occurred among those attending the American Legion Convention, the Pennsylvania Department of Health alerted local health officials to help in the investigation. State health officials also notified the Pennsylvania Medical Society, the Pennsylvania Osteopathic Association and the Hospital Association of Pennsylvania of a potential statewide epidemic. They requested co-operation in reporting potential cases, and, because of the statewide nature of the problem, the Pennsylvania Department of Health was made the center for planning and data collection.
Public-health nurses were instructed to search hospitals in their districts for hospitalized Legionnaires. They made daily rounds at local hospitals and reported date of onset of illness, clinical description, association with the convention and existence of secondary spread of illness. A telephone hot line was established in Philadelphia, and the public invited to report possible epidemic cases. News reports were scanned to identify additional cases.
Surveys
Eight epidemiologic surveys are discussed in this paper.
Hotel-guest survey. To assess the rate at which illness meeting the clinical criteria was occurring in hotel guests other than Legionnaires in Philadelphia, a telephone randomized survey was made of guests registered at four hotels between July 6 and August 7. The hotels surveyed included Hotels A and B as well as a center city hotel where a few Legionnaires stayed (Hotel C), and a hotel on the periphery of the city where no Legionnaires stayed (Hotel D). The overall completion rate was 67 per cent; however, there were considerable differences in completion rates within time periods for each hotel and between hotels. An additional group of 80 persons not attending the convention who were registered at Hotel A on July 23 were also selected for interview.
Hotel-employee survey. To determine if illness was affecting employees of the headquarters hotel, a review was made of unscheduled employees’ absences since July 1, and each employee who missed two or more days was interviewed concerning illness that might meet the case criteria. In addition, an approximate 25 per cent randomized sample of the estimated 400 employees of Hotel A was selected for telephone questioning. Also, an attempt was made to interview all persons who worked in the lobby.
Roommate survey. Fifty-nine roommates of 52 patients and 69 roommates of 68 control Legionnaires at Hotel A were queried about illness in the interval from July 21 to August 9, 1976.
Hospital survey. To determine if illness meeting the clinical criteria of disease was occurring apart from the American Legion Convention and Hotel A, emergency-room and admission records of patients seen from July 1 to August 9, 1976, in three hospitals serving center-city Philadelphia (Graduate Hospital, Pennsylvania Hospital and Thomas Jefferson University Hospital) were reviewed.
Pneumonia and influenza deaths. Deaths caused by pneumonia and influenza are routinely reported to the Philadelphia City Health Department as part of the national influenza surveillance system. Review was made of reported deaths in the interval from June 4 through September 24 for the years 1974, 1975 and 1976 among Philadelphia residents.
Legionnaire census. On August 9 a packet of two-page questionnaires regarding activities at the convention and subsequent illness was delivered to the commanders of each of the 1002 local American Legion posts in Pennsylvania. Each commander was asked to identify persons in or associated with his post who had attended the convention, to deliver a form to each person and to retrieve completed questionnaires; 3683 forms were returned by Legionnaires who had attended the convention. Of the 3580 who listed their convention status, 1849 (51.6 per cent) were delegates. Because 2274 delegates voted at the convention, it may be estimated that approximately 4400 persons attended the convention ![]() The responses of persons who reported having been well since the convention were compared with those of patients.
The responses of persons who reported having been well since the convention were compared with those of patients.
Case-control survey No. 1. A case-control survey, designed after completion and analysis of the Legionnaire census, was intended for all surviving male Legionnaires on the case list and a randomized sample of 202 men chosen from the Legionnaire census who indicated that they had been well since the convention (controls). Interviews were completed by telephone on August 17 with 147 control Legionnaires (73 per cent) and 113 case Legionnaires (91 per cent).
Case-control survey No. 2. An attempt was made to survey 56 case and 56 control Legionnaires in December, five months after the epidemic. The patients chosen were the surviving male delegates who had been hospitalized and were known to have had a temperature of 38.9°C or higher and radiographic evidence of pneumonia. Controls were matched for age and sex. Fifty-two case and age-matched control pairs were interviewed in person.
Other Technics
Various parts of the inanimate environment of Hotel A were sampled in August to determine if changes in the physical environment of the hotel might have taken place in temporal association with the Legionnaires’ convention. Weather records for Philadelphia were reviewed. Selected autopsies were attended by medical epidemiologists to supervise collection of appropriate specimens. Interviews were conducted with residents and workers in the area of Hotel A, with persons attending several other conventions and with officials of the American Legion. Two patients with Legionnaires’ disease who had had brief exposure were brought back to the scene of the convention and “walked through” their activities at the time. Medical epidemiologists attempted to interview in person and examine all suspect cases identified as of August 3. Hospital medical records of 94 and 147 hospitalized patients were obtained and reviewed.
Laboratory Methods
The Bureau of Laboratories of the Pennsylvania Department of Health co-ordinated local collection of specimens from all persons. Details of the laboratory aspects of the investigation are presented in a companion paper.3
RESULTS
Clinical Illness
Of the 182 patients, 147 (81 per cent) were hospitalized, and 29 (16 per cent) died. The typical illness began seven days after the Legionnaire had arrived at the convention and three days after he had returned home. Earliest symptoms were malaise, muscle aches and a slight headache. Within less than a day there was a rapidly rising fever associated with shaking chills. A nonproductive cough was common early, often with the onset of initial symptoms. Chest pain often accompanied the cough and was frankly pleuritic in a third of the cases. Dyspnea, abdominal pain and gastrointestinal symptoms also occurred in many of the patients. By the time a patient saw his physician, two or three days after onset of illness, the temperature had usually risen to 38.9 to 40.6°C, and examination of the chest disclosed some rales, without evidence of consolidation. One fifth of the patients became obtunded. In most cases the rest of the physical examination gave normal results.
From review of hospital records of 94 of the hospitalized patients it was found that 58 had a history of pre-existing illness including 10 with emphysema or other chronic pulmonary disease, 13 with hypertension, nine with arteriosclerotic cardiovascular disease, seven with peptic-ulcer disease and four with cancer. The admission urinalysis showed a ≥3+ test for protein in 20 per cent of the patients, and microscopic hematuria occurred in 10 per cent. Fifty-nine per cent had a white-cell count above 10,000 per cubic millimeter, but in only 20 per cent was it above 14,000 per cubic millimeter; 50 per cent had a shift to the left, with more than 5 per cent band forms. The initial white-cell count and the proportion of band forms were higher in those who died than in those who survived. A total count less than 2000 per cubic millimeter was seen in two persons who died and in one who survived; only two other patients had fewer than 6000 white cells per cubic millimeter. Erythrocyte sedimentation rate was greater than 80 mm per hour in 33 per cent of those in whom it was measured. Modest elevations of blood urea nitrogen, glutamic oxalacetic transaminase and alkaline phosphatase were commonly seen.
Radiographs of the chest were abnormal in 90 per cent. Patchy, interstitial infiltrates or areas of consolidation were most often seen early and usually progressed to more widespread consolidation. In nearly 50 per cent of the cases, pulmonary infiltrates remained unilateral. Effusions, when present, were usually minimal and did not present management problems. No cavitation was seen.
In most cases the illness progressed over two or three days, and in the survivors there was a remittent fever that broke by lysis. Cough commonly became productive during the course of the illness but was rarely purulent. Most patients were treated with oxygen. Inspired oxygen concentration greater than 40 per cent and mechanical ventilation were required in 20 per cent; these requirements were (not unexpectedly) associated with death. Shock occurred in 50 per cent of those who died and in none of those who recovered. Upper and lower gastrointestinal bleeding was not uncommon but may have been related to the stress of illness. Transient impairment of renal function was frequent and usually mild. In four cases renal failure required treatment with dialysis. One patient had evidence of preceding hypotension and clinical shock before onset of renal failure. Three patients were in renal failure on admission to the hospital and had no antecedent history of hypotension. Death occurred after a median of seven days after onset of illness. Risk of death was increased in older patients. In those who recovered, radiographic evidence of improvement appeared at a median of 10 days after onset of illness and lagged behind clinical resolution.
Individual patients seemed to improve after therapy with a variety of antibiotics was started, but, when cases were considered as a group, no antibiotic was clearly effective. The case-fatality ratio was higher in those treated with cephalothin (20/49) and steroids (14/25), and was intermediate in patients treated with aminoglycosides (9/25), chloramphenicol (3/10), ampicillin (10/41) and penicillin (6/30). Outcome was most favorable in patients given tetracycline (3/30) or erythromycin (2/18). The severity of illness at the time of hospital admission among patients in each treatment group was evaluated by a combination of clinical and laboratory features of prognostic value; this assessment showed the groups to be clinically comparable before therapeutic intervention. The timing of therapy did not confound evaluation of treatment efficacy except in moribund patients treated terminally with steroids.
Pathological findings are described in detail elsewhere.4 Characteristic findings were largely limited to the lungs, in which pneumonia and acute diffuse alveolar damage were seen.4 With a silver-impregnation stain, many bacilli were consistently seen in affected alveoli. Other stains commonly used did not demonstrate large numbers of bacilli. Serologic data appear in the paper by McDade et al.3 In summary, 91 per cent (101 of 111) of patients with Legionnaires’ disease from whom adequate serum specimens were obtained either showed seroconversion (56 per cent) or were seropositive only (35 per cent). Nine of 14 cases of Broad Street pneumonia in which adequate serum specimens were obtained four to seven months after the epidemic showed seroconversion or seropositivity.
Some Legionnaires had mild respiratory illness that did not meet the clinical criteria for Legionnaires’ disease. Of delegates responding to the Legionnaire census, 98 not meeting the criteria reported fever and either cough or a chest x-ray examination since the convention. No properly timed serum pairs are available from these persons. Serum specimens drawn on August 6 and September 1, 1976, from 21 Legionnaires who had attended the convention and who were subsequently perfectly well did not show a fourfold
change in titer. Mild respiratory illness not meeting the clinical criteria was not appreciably more common in registrants of Hotel A or B in the week of July 18–24 than in registrants of Hotels C or D (data not shown).
Person, Place and Time
Of the 182 cases meeting the clinical and epidemiologic definition of Legionnaires’ disease, 142 were in males. Patients ranged in age from three to 82 years; 75 per cent were 40 to 69 years old, with a mean of 54.7 years. One hundred and forty-nine had attended the American Legion Convention (Table 1). One case was in a hotel employee. Of the other 32 patients nine had attended the Eucharistic Congress (August 1–8, 1976), two a Candlemakers’ Convention (July 17–21, 1976), and one a Magicians’ Convention (July 14– 17); the others had no convention association. Eighty-four of the patients and 75 of the Legionnaire patients had stayed overnight at Hotel A.
The incidence rate of illness among those at the American Legion Convention, calculated from the Legionnaire census, was 4.0 per cent. Among delegates the rate was 6.8 per cent, among family members 6.3 per cent and among others attending the Legion convention 0.4 per cent (Table 1). Only two of the 17 family members who were ill (12 per cent) returned a
Table 1. Attack Rates of Legionnaires’ Disease among Persons at the American Legion Convention, July 21–24, 1976, According to Status.
|
CONVENTION STATUS |
ATTACK RATE (%) |
RESPONDENTS |
NO. OF CASES |
|
Delegate |
6.8 |
1,849 |
125 |
|
Auxiliary |
0.6 |
701 |
4 |
|
Family member |
6.3 |
268 |
17 |
|
Nondelegate |
0.4 |
762 |
3 |
|
Unknown |
0 |
103 |
0 |
|
Totals |
4.0 |
3,683 |
149 |
questionnaire in the Legionnaire census, as compared with 72 (58 per cent) of 125 delegates with illness, suggesting that completion rates in family members were lower than those in delegates. If there had been a fourfold underestimation of the denominator in family members, their actual attack rate would have been approximately 1.6 per cent—a rate closer to that of Auxiliary and other nondelegates. Incidence rates were 5.4 per cent for men and 1.9 per cent for women. Attack rate for delegates increased progressively with increasing age (Table 2). The homes of ill persons were scattered throughout Pennsylvania, and the rates of illness were similar for Legionnaires coming from Philadelphia or the remaining eastern, western, and central parts of the State (data not shown).
Thirty-nine persons met the criteria of Broad Street pneumonia. Ages of persons with Broad Street pneumonia ranged from 19 to 70 years, with a mean of 50.6 years. Twenty-four cases were in males. Five cases were fatal. Eight of these persons were known to have walked on the same side of Broad Street as Hotel A,
Table 2. Legionnaires’ Disease Attack Rates in American-Legion Delegates, According to Age and Residence at Hotel A or Elsewhere, July 21–24, 1976.
|
AGE (YR) |
HOTEL A RESIDENTS |
RESIDENTS ELSEWHERE |
TOTAL RESIDENTS |
||||||
|
|
ILL |
TOTAL |
% ILL |
ILL |
TOTAL |
% ILL |
ILL |
TOTAL |
% ILL |
|
<40 |
3 |
44 |
6.8 |
3 |
116 |
2.6 |
6 |
160 |
3.7 |
|
40–49 |
9 |
160 |
5.6 |
11 |
232 |
4.7 |
20 |
392 |
5.1 |
|
50–59 |
27 |
320 |
8.4 |
25 |
523 |
4.8 |
52 |
843 |
6.2 |
|
60–69 |
12 |
108 |
11.1 |
19 |
207 |
9.1 |
31 |
315 |
9.8 |
|
≥70 |
11 |
54 |
20.4 |
5 |
76 |
6.5 |
16 |
130 |
12.3 |
|
Unknown |
0 |
2 |
0 |
0 |
7 |
0 |
0 |
9 |
0 |
|
Totals |
62 |
688 |
9.0 |
63 |
1,161 |
5.4 |
125 |
1,849 |
6.8 |
13 on the other side of the street, and two on both sides of the street; information is not available on the other 16. Five persons admitted to some contact with Legionnaires during the convention; six had attended the Eucharistic Congress.
Illness meeting the clinical criteria was rare except in Hotels A and B in the week of the American Legion Convention (Table 3). Five persons who met the clinical criteria for a case of Legionnaires’ disease were found among registrants at Hotels C and D during the week surveyed, two during the week before the American Legion Convention, and three during the week of the convention. Three of the five entered Hotel A and met epidemiologic criteria for Legionnaires’ disease.
There was no evidence from the survey of hotel guests that an epidemic associated with hotel residence continued after the American Legion cohort. For Hotel A in the week of July 18–24, a supplementary sample was chosen of persons who had no known association with the convention. Including the supplementary group, illness in those who attended the convention (15 of 110) was more common than that in those who did not (one of 47) among registrants in Hotel A on the nights of July 21–23.
Only one of more than 400 employees, an air-conditioner repairman, met the case criteria with a temperature of 38.9°C and cough beginning on July 24 that required him to miss work for four days. His two children, three and four years old, had colds beginning on July 27, and his wife became ill on August 2. He recovered and did not see a physician or have a chest x-ray study. No serum specimens were available from him or his family. Nine other employees who worked in different locations in the hotel were known to have had minor colds but did not meet the case criteria.
Table 3. Illness Resembling Legionnaires’ Disease in Randomized Sampling of Guests in Four Philadelphia Hotels According to Week of Registration, July 6-August 7, 1976.
|
HOTEL |
7/6–7/10 |
7/11–7/17 |
7/18–7/24 |
7/25–7/31 |
8/1–8/7 |
|
A |
0/142/155* |
0/130/159 |
15/180/200 |
0/106/152 |
0/88/147 |
|
B |
— |
— |
5/144/200 |
— |
— |
|
C |
— |
1/70/85 |
2/100/160 |
0/95/140 |
0/78/160 |
|
D |
— |
1/90/151 |
1/84/150 |
0/92/151 |
0/58/154 |
|
*No. ill/no, interviewed/no, chosen for survey. |
|||||
The epidemic curve showed a rapid upswing in cases from July 22 to 25, followed by a plateau through July 28, and a somewhat slower decline through August 3; a scattering of cases were observed until August 16 (Fig. 1). The 149 cases in Legionnaires showed dense clustering in a narrow space of time, whereas the 33 cases in non-Legionnaires were clustered in two groups from July 24 to August 1 and August 9 to 16. The distribution of cases of Broad Street pneumonia was similar to that of Legionnaires’ disease.
The distribution in time of illnesses between July 1 and August 9 that were found in the hospital survey gave no evidence of an unusual incidence of disease about the time of the outbreak of Legionnaires’ disease (data not shown). There was no increase in the weeks of or after the outbreak in the number of persons diagnosed on death certificates in Philadelphia as having died from pnuemonia or influenza (data not shown).
Incubation Period
For the 72 patients with Legionnaires’ disease or Broad Street pneumonia who either were culture positive or showed seroconversion (Fig. 2), a comparison of date of onset with dates of possible exposure within one block of Hotel A permits an estimate of the possible or necessary range of incubation period. All but two cases could be explained by an incubation period of two to 10 days. The two exceptions (Cases 68 and 58) apparently had incubation periods of 16 and 26 days, respectively. The two are residents of the same town. 64 km from Philadelphia.
Time of Exposure
The 72 persons with Legionnaires’ disease or Broad Street pneumonia who were shown to have seroconversion or from whom the agent of Legionnaires’ disease was cultured, 67 attended the American Legion Convention or were in or in the vicinity of Hotel A in the interval July 1 through July 24 (Fig. 2). Single days of exposure on July 21, 22 and 23 were associated with seroconversion. Four other patients were in the vicinity in the first nine days of August. The person who was the last case (Case 58) was present in Philadelphia only on July 5 and fell ill 26 days later.
Place of Exposure
When responses of all ill and well Legionnaires were compared, attendance at each of many conven-
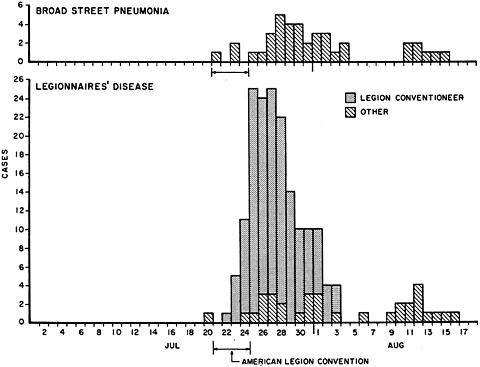
Figure 1. Dates of Onset of Illness in Cases of Legionnaires’ Disease and Cases of Broad Street Pneumonia in Philadelphia, July 1–August 18, 1976.
Dates of onset of two cases of Legionnaires’ disease are unknown.
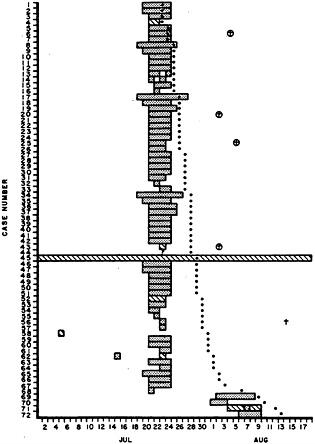
Figure 2. Days Spent at Hotel A or the American Legion Convention ![]() or Otherwise within One Block of Hotel A (▧) by Each of 72 Persons Who Met the Clinical Definition of Legionnaires’ Disease or Broad Street Pneumonia and Who Were Shown to Have Seroconversion or a Positive Culture for the Implicated Gram-Negative Bacterium.
or Otherwise within One Block of Hotel A (▧) by Each of 72 Persons Who Met the Clinical Definition of Legionnaires’ Disease or Broad Street Pneumonia and Who Were Shown to Have Seroconversion or a Positive Culture for the Implicated Gram-Negative Bacterium.
One person with an uncertain date of exposure within one block of Hotel A is shown (?). Also shown are dates of the onset of illness (●), of death (†) and of positive culture (○).
tion activities was associated with illness. These associations were with the typical activities of delegates and could have been expected because delegates formed the group at highest risk of disease. To avoid the confounding effect of the high risk for delegates, most subsequent analysis of places of exposure and modes of spread is restricted to Legionnaire delegates.
From the Legionnaire census, 62 (50 per cent) of 125 ill delegates resided at Hotel A as compared with 356 (35 per cent) of 1006 well delegates (P<0.01 by chi-square). Illness was not associated with residence at any other hotel. Cases did not cluster within Hotel A by location of bedroom.
Among delegates responding to the Legionnaire census, significantly more patients than controls attended hospitality room A on the 14th floor (P<0.05 by chi-square). All other rooms showed no significant differences between case and control delegates. The mean number of hospitality rooms attended by delegates determined from the Legionnaire census was 2.8 for ill delegates and 1.8 for well (P<0.02 by t-test). The difference was observed only for delegates who did not stay at Hotel A. No association was found between illness and consumption of specific foods or ice served in common in several hospitality rooms. Five of the 12 family members who were ill and from whom information was available and none of those who had Broad Street pneumonia attended hospitality rooms.
The mean number of minutes spent in the lobby of Hotel A by Legionnaire patients (delegates and non-delegates) was greater than that for controls, both for residents of Hotel A (259 and 142, respectively) and for Legionnaires who stayed elsewhere (133 and 86, respectively). Case delegates spent more time than controls in the lobby of Hotel A, both among residents of Hotel A (P=0.05 by Mann-Whitney test) and among delegates who stayed elsewhere (P<0.001 by Mann-Whitney test).
Case delegates who were serologically positive or had seroconversion spent more time on the average than control delegates in Hotel A on July 23 (82 per cent of case delegates and 54 per cent of controls spent more than six hours in the hotel on that day; P< 0.0001 by chi-square). On July 23, among these serologically confirmed case delegates, there was a linear trend for more time spent on the sidewalk in front of Hotel A as compared to controls (P=0.04 by chi-square). Among persons who watched the Legion parade on July 23, independent of hotel of residence, those with serologically confirmed cases were more likely than controls to have watched from the sidewalk directly in front of Hotel A (55 per cent vs. 26 per cent, P<0.01 by chi-square).
Single serum specimens were obtained from 61 employees of Hotel A on August 19 and 20, 1976. Indirect fluorescent-antibody titers to the agent of Legionnaires’ disease were <1:64–34, 1:64–17, 1:128–7, 1:256–2 and 1:1024–1. These titers contrast with those of 30 employees of the Pennsylvania State Health Laboratory in North Philadelphia, all of whom had titers <1:64. Among Hotel A employees, titers of ≥1:64 were found in a larger proportion of persons whose employment there had begun before 1975 (20 of 34, or 59 per cent) than in those who began work later (six of 25, or 24 per cent) (P<0.05 by chi-square). The date on which two persons started work was unknown. There was no association between titer and age, shift, type or location of work within the hotel, or illness between July 1 and August 19, 1976.
Mode of Transmission
Investigation of the mode of transmission included the following general categories: person-to-person, food, tobacco, alcohol, water, animals, ice, fomites and air.
Person-to-person. In the case-control survey No. 1, completed on August 17, 24 days after the end of the convention, none of the contacts (140 adults and 53 children) with Legionnaires’ disease who were interviewed had contracted illness that met the clinical criteria for a case. Similarly, among family contacts (143
adults and 68 children) of well attendants at the convention, none had had illness after the convention that met the clinical criteria.
There was no clustering of cases in rooms as might be expected if person-to-person spread occurred. Room-mates of patients had an attack rate of 8.5 per cent (five of 59) and those of controls an attack rate of 7.2 per cent (five of 69).
Food. Of the many food establishments in the area of Hotel A 28 restaurants and bars in the local area were selected for inquiry. No restaurant was found to be significantly associated with illness, nor was purchase of food from street vendors.
Two main American Legion events were associated with the distribution of food: a testimonial dinner and a breakfast. There were no significant differences in attendance between case and control delegates for either event and no difference in the proportion of case and control delegates who ate specific foods at the breakfast. No differences were found between the two groups in preferences for snack foods known to have been, served in hospitality rooms during the convention.
Tobacco. In 17 case-control pairs, in case-control survey No. 2, the case delegate smoked cigarettes at the time of the convention and the control delegate did not (Table 4). In five case-control pairs the converse
Table 4. History of Cigarette Smoking among Case and Control Pairs at the American Legion Convention, Philadelphia, July 1976.
|
CONTROLS |
CASES |
TOTALS |
|
|
|
Smoker |
Nonsmoker |
|
|
Smoker |
14 |
5 |
19 |
|
Nonsmoker |
17 |
16 |
33 |
|
Totals |
31 |
21 |
52 |
was true. The relative risk of illness associated with smoking was 3.4 and was significantly different from unity (chi-square=5.5, P<0.05, McNemar test). Survey of Philadelphia resident cases indicated that no cigarette brand predominated. The average number of cigarettes smoked was greater for case delegates who smoked than in controls who smoked. Cigar or pipe smoking was not associated with illness.
Alcohol. No statistically significant differences between case delegates and controls were found for the average number of alcoholic drinks, including beer, consumed each day during the convention. Nine ill Legionnaires, including five delegates of 90 questioned, indicated that they had had no alcoholic drinks during the convention. No association was found between illness and preference for beer, type of hard liquor, mixer or homemade liquor.
Water. In the Legionnaire census, delegates were asked whether they drank any water or consumed any ice at Hotel A: Forty-five of 69 ill delegates drank water as compared with 469 of 976 well delegate controls, a significant difference at the 0.01 level. The relation holds even when corrected for the number of days delegates spent at the hotel. Fifty-three (62 per cent) of 86 ill Legionnaires queried remembered drinking water at Hotel A. No significant association was found between consumption of ice and illness.
Other. No association was found between illness and contact with birds, mammals or souvenirs. Patients did not complain of insect bites. A hypothesis of airborne spread is difficult to test directly, but it is consistent with the observed association of illness with time spent in the lobby and on the sidewalk in front of the hotel. Several patients with Legionnaires’ disease and most with Broad Street pneumonia had only transient exposure in these areas and had no identifiable exposure there other than to air.
DISCUSSION
Between July 22 and August 3, 1976, there was a remarkable incidence of febrile respiratory disease among persons who had attended the American Legion Convention from July 21 to 24. From the age distribution of the Legionnaire group attending the convention and recent mortality statistics from Pennsylvania,5 it can be estimated that 60 deaths per year, or 1.2 per week, would be expected among the conventioneers. The excess number of deaths (26) that occurred in conventioneers between July 27 and August 16 is further evidence of the occurrence of an epidemic. The outbreak involved, in addition, other visitors to the headquarters hotel and persons who had walked within a block of the hotel, but the outbreak did not appear to be more widely spread in Philadelphia. Clinical, epidemiologic and laboratory results indicated that the large majority of cases that met the criteria for Legionnaires’ disease and for Broad Street pneumonia were in fact the same disease.
The shape of the epidemic curve, with its rapid upswing and the incubation period of two to 10 days, suggests a continuing common-source exposure. There is no evidence of spread from person to person. At a minimum, exposure appears to have occurred on July 22 and 23 and also sometime in each of the intervals August 1–3 and August 6–9. Two cases of apparent exposure in Philadelphia only before July 22 were unusual in that their apparent incubation periods were long (16 and 26 days). One could speculate that these patients may have been exposed after leaving Philadelphia, perhaps in their common home town, but there is no direct evidence to confirm that hypothesis. The highest risk of exposure is likely to have been during the time of the American Legion Convention. Whether or not a low-grade exposure was present from July 24 to 31 or after August 9 is unknown, but there is no evidence that the outbreak in the area continued after August, 1976. Serologic survey of the employees of Hotel A suggests the possibility of a low-grade or intermittent exposure to the same or a similar agent for several years.
The place of exposure cannot be defined with certainty, but the most reasonable hypothesis is that ex-
posure occurred within or in the immediate vicinity of Hotel A. Such a hypothesis is consistent with the observation that of delegates, those who stayed at Hotel A had a significantly higher rate of illness than those who did not, and that of the delegates who did not stay at Hotel A, those who fell ill spent more time on the average in Hotel A than those who stayed well.
The fact that cases occurred in persons who had been near, but not in, Hotel A (cases of Broad Street pneumonia) shows that in at least some cases, exposure occurred outside Hotel A, and suggests that exposure could have occurred on the streets or sidewalks around that hotel. Other evidence of exposure outside the hotel comes from the observation that serologically confirmed cases in delegates occurred more frequently in those who watched the parade from the sidewalk in front of Hotel A and that the length of time spent on the sidewalk was associated with illness. Exposure may well have occurred within Hotel A also. In the delegate group, there was a strong association between time spent in the lobby of Hotel A and risk of contracting the disease both for all cases and for those serologically confirmed. Initially, it seemed that the absence of noteworthy illness in employees who worked in the lobby of Hotel A was evidence against the lobby as a site of exposure. However, serologic survey of hotel employees suggests that a large proportion of them may have been immune. Twenty-nine per cent had a titer of 1:64—a titer that is just below that considered diagnostic of recent infection.3 The prevalence of this borderline titer in hotel employees is considerably higher than that observed in groups not associated with the outbreak of Legionnaires’ disease.3
It is unlikely that the place of exposure was in any of the main convention function rooms in Hotel A because attendance at those functions was not associated with illness. Similarly, bedrooms were unlikely places of exposure since roommates of patients were not at increased risk of illness and because there was no geographic clustering of bedrooms of cases in Hotel A. Because no hospitality room was said to have been visited by more than half the patients and because there was no striking association between attendance or food consumption and illness, the rooms are unlikely to have been the sites of exposure.
The mode of spread is not proved, although it was probably air borne. It is clear from the studies of families who did not come to the convention that secondary person-to-person spread was unusual or nonexistent. The possibility that the initial exposure at the convention was by person to person is not ruled out entirely, but the uniform attack rate across districts militates against the possibility. The failure to implicate a common meal at the convention, the street vendors, foods served at the hospitality rooms or any of the local coffee shops or restaurants argues against a food-borne outbreak.
The possibility of a water-borne illness is raised because patients were more likely than controls to state they drank water at Hotel A. However, 35 per cent of ill delegates and 38 per cent of all ill persons queried said that they never drank water at Hotel A. Furthermore, none of those who had Broad Street pneumonia drank water from Hotel A.
The occurrence in the summer would be consistent with spread by an arthropod vector, but bites were not noted by the ill patients.
If the exposure was air borne, the association of illness and time spent in the lobby might be explained. An air-borne agent might also have affected non-Legionnaires who were in the hotel only transiently and had no other apparently noteworthy exposure; it might also have exposed persons who walked near the hotel but did not enter it.
The source of the bacterium is not known, nor is the reason for the sudden appearance of the outbreak in late July and disappearance in mid-August. It does seem that exposure continued for 16 to 19 days, more intensively at first and then trailing off. Efforts are under way to determine if the bacterium can be found in local bird or rodent populations or in dust and dirt. The relatively high proportion of Hotel A employees —especially long-term employees—with indirect fluorescent-antibody titers of ≥1:64 suggests that exposure to the organism may have been present intermittently for several years. Serologic testing of employees of surrounding businesses is under way to assess the breadth of exposure.
Two previous outbreaks caused by this or a related bacterium also had the pattern of a continuing common-source air-borne exposure.6,7 In one, an air-conditioning system was instrumental in spreading the agent,6 but in the other the involved buildings were not air conditioned.7 In each of those outbreaks, nearby excavation was suspected as an inciting activity. In Philadelphia, however, no nearby excavation in July was identified. All three outbreaks occurred in the summer, but the implications of this apparent seasonality remain speculative.
Sporadic cases of pneumonia caused by this bacterium have been observed.3 To investigate the clinical characteristics, mode of spread and source of infection of sporadic cases, a case-control study of undiagnosed pneumonia has been organized in Pennsylvania, Ohio, Maryland, Connecticut, Delaware, Florida and the District of Columbia.
We are indebted to Calvin C.Edmonds, David A.Hall, Thomas Leonard, Robert L.Longenecker, John Kolnik, David Knorowski, Denis Lucy, M.D., Joel Mulder, Edward J.Powers, George Rogers, Jerry Shirah, Eleanor Streiff, R.N., M.P.H., public-health nurses of the Pennsylvania Department of Health, personnel of the City of Philadelphia—City Representatives Office, Department of Health, Licenses and Inspections Department, Manager Director’s Office, Police Department and Water Department—personnel of the Region III Office, DHEW, and the staff at the Center for Disease Control for assistance during the field investigation, to Robert A.Pollard and Phyllis A.Wingo for assistance in statistical analyses and to John V.Bennett, M.D., for advice and criticism.
REFERENCES
1. Frame JD, Baldwin JM Jr, Gocke DJ, et al: Lassa fever, a new virus disease of man from West Africa. I. Clinical description and pathological findings. Am J Trop Med Hyg 19:670–676, 1970
2. Johnson KM, Lange JV, Webb PA, et al: Isolation and partial characterization of a new virus causing acute haemorrhagic fever in Zaire. Lancet 1:569–571, 1977
3. McDade JE, Shepard CC, Fraser DW, et al: Legionnaires’ disease: isolation of a bacterium and demonstration of its role in other respiratory disease. N Engl J Med 297:1197–1203, 1977
4. Chandler FW, Hicklin MD, Blackmon JA: Demonstration of the agent of Legionnaires’ disease in tissue. N Engl J Med 297:1218–1220, 1977
5. 1974 Natality and Mortality Statistics: Pennsylvania annual report. Harrisburg, Pennsylvania Department of Health, 1976
6. Epidemic of obscure illness—Pontiac, Michigan. Morbid Mortal Weekly Rep 17:315–320, 1968
7. Institutional outbreak of pneumonia. Morbid Mortal Weekly Rep 14: 265–286, 1965









