
Federal regulations governing opioid use disorder (OUD) treatment, including the COVID-19 emergency allowances, have had both intended and unintended impacts, said Kenneth Stoller, associate professor in the department of psychiatry and behavioral sciences at the Johns Hopkins University School of Medicine. In addition, as discussed in Chapter 4, state laws may conflict with access and best treatment practice, he said.
The current opioid treatment program (OTP) system was established to provide a comprehensive approach to a complex disorder in a population that frequently has many social, medical, and mental health struggles in addition to misuse of opioids and other drugs, said Stoller. During the online open discussion period, Susan Staats Combs agreed, noting that many OTPs work earnestly to reduce stigma and help patients with an array of issues that led them to the clinic in the first place. “We help patients in every facet of their life,” she added. Yet, regulatory constraints and a com-
plex set of accreditation standards may stymie service delivery and limit access to certain populations, said Stoller. For example, these barriers can discourage the opening of smaller sized OTPs in areas of great need, such as rural areas. Regulations and accreditation standards have been added layer upon layer over time, creating a complicated multilayered system that results in OTPs spending more time attending to those regulations rather than caring for patients, said Stoller. By limiting access to “comprehensive, high quality, and safe treatment from well-trained professionals,” he said, excessive controls could push methadone treatment toward unregulated and unaccredited office-based practices that would not provide the comprehensive treatment needed to help patients achieve recovery.
To improve access to quality and safe treatment for OUD, regulatory innovations are needed that are supported by evidence and best practices, said Stoller. Changes are needed that increase flexibility and make the opening of new programs and the operation of existing programs easier, while continuing to hold programs accountable for using the most proven and patient-centered practices and ensuring the safe use of methadone, he said. Among these innovations, pharmacy-based dispensing, mobile units, and expanding the reach of the OTP as a hub site are discussed in this chapter.
FEDERAL STATUTES AND REGULATIONS THAT GOVERN OPIOID TREATMENT PROGRAMS
The regulatory structures that surround policy issues presented by OUD and other pressing social problems start with the statutes produced by Congress, said Bridget Dooling, research professor with the George Washington University Regulatory Studies Center. These statutes provide federal agencies such as Department of Health and Human Services (HHS) with the authority to govern, which they do by producing regulations at the federal level, adding that Congress also creates and funds those agencies. Both statutes and regulations are law, said Dooling, but it is important to recognize that only Congress can change statutes. “On the flip side, it’s a missed opportunity if we fail to recognize places where Congress has given an agency authority that it’s not using,” she said.
Potential to Extend Pandemic Flexibilities
With a grant from the Pew Charitable Trusts, Dooling and her colleague Laura Stanley have explored whether certain pandemic flexibilities such as those concerning take-home supplies of methadone could be legally extended after the pandemic ends. Dooling explained that the Substance Abuse and Mental Health Services Administration (SAMHSA) issues rules that govern how OTPs operate, and the rule is that patients must come to
the OTP almost every day to get their doses. The opportunity to receive take-homes, she said, is the exception, not the rule. As Yngvild Olsen described in Chapter 4, at the beginning of the pandemic, SAMHSA issued a modification to the rule that allowed states to request exceptions allowing stable patients to receive 28 days of take-home doses and less stable patients to receive 14 days of take-home doses if the OTP believed the patient could handle these take-homes safely. The definition of “stable” and “less stable” were left open to interpretation, said Dooling.
“The pandemic shifted something fundamental,” said Dooling, but understandably, people were concerned that SAMHSA would retract the flexibility when the pandemic ends. Dooling and Stanley set out to examine whether the law required that flexibility to end or whether it was a policy choice. “Our findings were stunning,” she said. “We found that SAMHSA has a high degree of authority to make regulatory changes without going to Congress to change the law.” Under the Controlled Substances Act, she said, the secretary of HHS has the authority to establish standards that spell out who qualifies for this kind of treatment. SAMHSA thus had the authority to make the take-home flexibilities permanent, said Dooling.
SAMHSA has stated that once the pandemic emergency ends, the take-home flexibility will stay in place for 1 year, said Dooling. “This will hopefully be enough time to get through the rulemaking process to make this flexibility stick,” she said, adding that many studies have documented how the take-home flexibilities have worked in practice (as noted in Chapter 4 by Noa Krawczyk). “My advice is for SAMHSA to move as quickly as possible to build a record showing what we’ve learned from the take-home supplies available during this pandemic and to get a proposed rule as soon as possible,” said Dooling.
She added, “The breadth of SAMHSA’s authority also makes me wonder what else needs to be changed and how it should be changed to facilitate better patient care using harm reduction techniques.” For example, the OTP model is part of the current regulations, but is not required by statute. She advocated for SAMHSA, the Drug Enforcement Administration (DEA), Congress, and state and local regulators to make it easier to pilot new ways of treatment. She also argued that bringing about regulatory change will require sustained attention with someone overseeing the activity, perhaps in the Office of National Drug Control Policy (ONDCP) or elsewhere in the White House. Noting that there are longstanding disagreements about the trade-offs between law enforcement and public health, this person should be a “deft policy maker who can guide the process, have hard conversations, and move the ball forward.”
“We know so much more about addiction and opioids than we used to,” she said. “Let’s bring the reg[ulation]s up to speed so they aren’t holding people back from the care that they need.”
PHARMACY DISPENSING AS AN EXTENSION OF OTPs
When the regulations for methadone treatment were finalized in 1972, they made it illegal to prescribe methadone for OUD outside of OTPs, said Robert Brooner, a senior research scientist at the Friends Research Institute and emeritus professor at the Johns Hopkins School of Medicine. Yet, he said there is a large and rapidly growing consensus of the need to increase access to methadone for OUD both within and outside of OTPs. Robert Schwartz, a senior research scientist at Friends Research Institute, said an underused and often overlooked aspect of current OTP regulations is the possibility for an OTP to act as a hub, with pharmacies, physician offices, mobile units, or other “medication units” to serve as spokes.
Moreover, as Schwartz noted, dispensing and administering medication is explicitly what pharmacies do extremely well, adding that they are experienced in maintaining, storing, and accounting for doses of controlled substances. Given how quickly COVID vaccinations were brought to scale so quickly in pharmacies, Schwartz expressed support for using pharmacies for the delivery of methadone. Using the same dose administration and dispensing guidance as is used by OTPs, he maintained that medication and take-homes could be dispensed safely in pharmacies.
One important rationale for this approach is to mitigate a shortage of physicians specializing in treating addiction, said Li-Tzy Wu, professor of psychiatry and behavioral sciences at Duke University School of Medicine. She cited a 2012 study that demonstrated a substantial gap between those needing treatment for OUD and the treatment capacity available at that time (Jones et al., 2015) (see Figure 5-1). Wu added that licensed pharmacists are medication therapy management experts and are widely available even in rural areas.
Brooner has been working on a National Institute on Drug Abuse–(NIDA-)funded study to investigate pharmacy administration of methadone for patients being managed in an OTP. OTPs provide a natural laboratory in which to study how to collaborate with pharmacies as a bridge to making methadone more readily available even outside of an OTP, said Brooner.
Two small studies conducted in the late 1960s and early 1970s showed mixed results including reduced drug use, said Brooner (Bowden et al., 1976). More than 45 years elapsed before two studies of pharmacy dispensing of methadone were completed by Brooner and Wu (Wu et al., 2022).
Brooner’s 3-month, non-randomized, single-arm pilot study was designed to evaluate the feasibility of having an OTP physician prescribe methadone and a community pharmacy dispense and administer it (Brooner et al., 2022). There were many delays in starting the project, said Brooner: about 15 months to obtain the necessary exceptions from DEA, followed by additional time to obtain the SAMHSA waiver, a support letter from
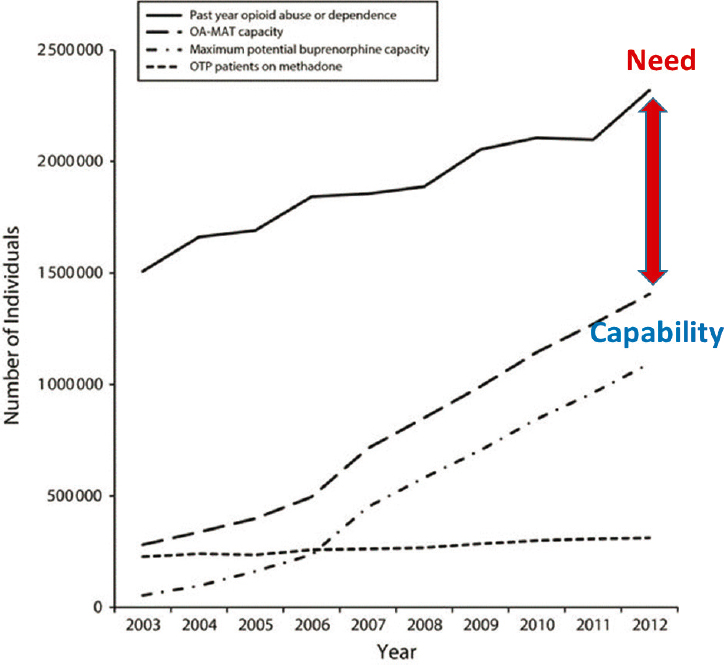
NOTE: OA-MAT = opioid agonist medication-assisted treatment; OTP = opioid treatment program.
SOURCES: Presented by Li-Tzy Wu, March 4, 2022; adapted from Jones et al., 2015.
the state methadone authority in Maryland, and institutional review board (IRB) approval from Johns Hopkins University. By then the COVID-19 pandemic had shut down operations at many health care institutions, and subject recruitment was suspended for several months. Finally, in October 2020, recruitment began and was completed in less than 3 months. Patients were required to be stable, that is, on an unchanging dose of methadone between 20 and 90 milligrams for at least 6 months, able to demonstrate at least 80 percent attendance at counseling sessions, employed or in a community volunteer position, and between the ages of 18 and 66. Eleven
patients were enrolled and 10 completed the trial, resulting in 91 percent retention. Participants self-reported zero days of opioid use and had zero opioid positive urine specimens; they also reported very high levels of satisfaction, according to Brooner.
Brooner emphasized that this study was conducted in highly stable patients who had long periods of abstinence. Additional studies are needed, he said, to determine if people with less stability and shorter durations of treatment would do as well. Federal and state approvals are needed to extend this work to other OTPs and conduct demonstration projects that enroll patient with shorter periods of stability and use telehealth for evaluations, counseling, and behavioral interventions, he said. Brooner also advocated extending this pharmacy-dispensing approach to office-based buprenorphine practices and projects where safety, implementation, and efficacy studies can be done. Brooner added that it will be important to work with Medicaid, Medicare, and commercial insurers to recognize prescribed methadone for OUD as an accepted benefit in pharmacy coverage plans.
Wu discussed another pilot study in which the prescribing OTP physician provides remote supervision of the patient’s care, plus electronic prescribing, through a collaborative practice agreement. Wu’s pilot study, described below, provides preliminary evidence of a potentially powerful way to expand access—a model that has already been used successfully in other countries, as is discussed later in Chapter 7.
Wu and colleagues have conducted two studies that demonstrate how a team-based care model pairing physicians with pharmacists may address access barriers to medications for opioid use disorder (MOUD). The first of these studies included three buprenorphine treatment clinics in North Carolina (Wu et al., 2021). For the 71 patients enrolled in the study, their buprenorphine care was transferred from their physician to a pharmacist for 6 months. During this time, physicians provided clinical guidance and/or coaching to pharmacists and continued to prescribe buprenorphine and determine dosage, while the pharmacists dispensed buprenorphine after checking the Prescription Drug Monitoring Program (PDMP),1 conducted dose reconciliation and patient education, and monitored other health issues and safety events, said Wu. The study was very successful, she said, with very high adherence and retention, low numbers of positive drug tests, no safety events, and high patient and physician/pharmacist satisfaction ratings. Wu added that pharmacist compliance with checking the PDMP was also very high.
___________________
1 The Prescription Drug Monitoring Program (PDMP) tracks controlled substance prescriptions to understand the behavior of the epidemic and to identify inappropriate prescribing trends. For more information, go to https://www.cdc.gov/drugoverdose/pdmp/index.html (accessed April 14, 2022).
Based on the success of this study, Wu and colleagues launched another pilot study to test a proof of concept about community pharmacy administration and dispensing of methadone, plus e-prescribing (Wu et al., 2022). She noted that while there are only approximately 1,800 SAMHSA-certified OTPs, there are approximately 67,753 community pharmacies in the United States (Qato et al., 2017). Leveraging the large network of community pharmacies could thus expand the number of methadone dispensing sites and address transportation and cost barriers that result in lower retention rates, reduced quality of life, and sometimes a patient’s inability to keep a job, said Wu.
The pilot study had three components: a collaborative practice agreement between the pharmacists and OTP physicians, electronic prescribing of methadone from the OTP physician to the pharmacy, and a methadone visit checklist to document pharmacist-provided intervention and check fidelity. After receiving exemption approval from DEA, SAMHSA, and the North Carolina State Opioid Treatment Authority to allow prescribing of methadone, and from the Duke Health IRB to undertake the study, 20 patients were enrolled in the 3-month study. They continued to receive routine care at the OTP and returned to the OTP to continue methadone treatment after the study ended.
In terms of outcomes, treatment adherence was 100 percent, retention 80 percent (two patients withdrew because of work-related issues, one due to pregnancy, and one due to a non-study-related hospitalization), no illicit opioid use, 100 percent compliance with psychosocial counseling attendance, no safety issues, and 100 percent pharmacists checked with PDMP in all 207 pharmacy visits (Wu et al., 2022). Satisfaction among participants was also very high.
The next step, said Wu, will be randomized controlled studies, including in diverse populations and various geographical locations, comparing pharmacy-based and OTP approaches in terms of efficacy, effectiveness, and implementations. Changes may also be needed in policies regarding pharmacy and pharmacist training, accreditation, and payment for pharmacist-provided care involving methadone treatment, she added.
Pharmacy-based dispensing of methadone has the potential to also address inequities in the current system, added Ayana Jordan, an addiction psychiatrist and the Barbara Wilson Associate Professor of Psychiatry at New York University Grossman School of Medicine. Achieving this will not only focus on how to present the option [methadone] to minoritized communities including how to ensure methadone is consistently stocked and available, but also ensure that minoritized pharmacists and pharmacy assistants are involved in these discussions, she said.
From the perspective of an OTP owner, Susan Staats Combs noted during the open discussion period online that in Alabama, OTPs are required
to have an in-house pharmacy, resulting in high costs and many hardships. While the in-house pharmacists are considered co-workers, she noted that the added issues of involving them in each patient’s case, including granting them access to the patient’s records and involving them in decision making, has been overwhelming and needs to be taken in consideration when considering pharmacy-based dispensing.
MOBILE MEDICATION UNITS—A DEMONSTRATION PROJECT IN NEW JERSEY
In New Jersey, mobile medication units that dispense methadone are now available in six municipalities to extend the reach of OTPs, said Valerie Mielke, assistant commissioner of the Division of Mental Health and Addiction Services in New Jersey’s Department of Human Services. The mobile vans (which are more like buses) all have DEA approval, are licensed by the state, and have separate SAMHSA certifications, even though they are linked and connected with brick-and-mortar OTP sites, she said. They were funded as part of the New Jersey Medication Assisted Treatment Initiative (MATI) through a $10 million appropriation to the Division of Addiction Services to make inpatient and outpatient treatment available for individuals with substance use disorder, said Mielke.
“It’s an innovative strategy that enables us to deliver treatment services directly to the neighborhoods where they are most needed,” she said. In addition, it allows treatment to be provided within the existing continuum of care and within the public health paradigm. Services are provided in a client-centered, recovery-oriented manner that values and respects individual choices and embraces the harm reduction philosophy,2 added Mielke.
To receive services at the mobile vans, individuals must meet MATI eligibility requirements, including low income and a history of injectable drug use, opioid dependence within the past year, or a positive test for opioids, said Mielke. They also cannot be enrolled concurrently in another opioid medication treatment program or be under the care of a prescriber of suboxone, she added. Medicare, Medicaid, and some private insurance plans can be billed for services.
The MATI vans are able to provide outpatient services as well as walk-in care, said Mielke, noting that many individuals are referred by New Jersey’s sterile syringe access program. People in residential treatment may also be referred to the vans. Some individuals receiving treatment through this program are also able to live in permanent supportive housing developed as part of the initiative.
___________________
2 Harm reduction is a key pillar of the HHS Overdose Prevention Strategy. To learn more, go to https://www.samhsa.gov/find-help/harm-reduction (accessed April 9, 2022).
One of the mobile medication vans has been repurposed to dispatch and make medication and counseling services available to people who are incarcerated at the Atlantic County Correctional Facility, said Mielke. She said that Project Kickstart, now about 6 years old, has served approximately 1,600 individuals. About 1,400 of these individuals have been released from the correctional facility on MOUD and 82 percent of those individuals continued treatment at a brick-and-mortar clinic site after release, she said.
New Jersey’s experience with mobile vans suggests that other states can consider initiating low-threshold, low-demand access programs such as in areas where individuals who are homeless gather or where individuals have difficulty accessing treatment, or in rural settings, said Mielke. These vans can also be a part of an emergency management strategy, she said. For example, during Hurricane Sandy in 2012, mobile vans were dispatched to areas where people were having trouble getting to OTPs.
Mark Parrino added that other states such as New York and Rhode Island are moving in the direction of developing van services. New mobile van guidance from DEA went into effect in July 2021. The next month SAMHSA sent a letter3 to OTPs and state opioid treatment authorities indicating that funding was available for vans if OTPs were interested, he said. Because the vans may cost as much as $250,000 each with special adjustments and additions, this funding stream is critical, said Parrino.
Mielke’s advice to states considering mobile medication programs included choosing a vehicle other than a bus because they found that if the bus broke down, services had to be halted. Instead, she suggested retrofitting a box truck with a separate cab, so that if something happens to the cab, another cab could be rented and services could continue. She also advised starting a public awareness campaign before introducing the mobile vans. Some communities did not want mobile vans in their neighborhoods and had misperceptions about the individuals served there. She added that funding is available for these vans because a recent guidance allows SAMHSA block grant funds to be used to purchase vehicles.
OTPs AS HUB SITES IN SYSTEMIC EXPANSION
According to Parrino, SAMHSA issued guidance in September 2021 outlining the kinds of services that could be provided through two different entities: (1) mobile vans functioning under the aegis of OTPs, and (2) non-mobile units, which are fixed site units. He noted that fixed site units need to be approved by state authorities, SAMHSA, and DEA, but regulations governing mobile vans associated with the OTPs, through the DEA
___________________
3 To view the letter, go to https://www.samhsa.gov/sites/default/files/2021-letter-stateauthorities-mobile.pdf (accessed May 9, 2022).
regulatory apparatus discussed by Kristi O’Malley in Chapter 3, do not need additional DEA approval—it is built into the process.
Parrino suggested that in addition to using a mobile van to extend the reach of an OTP, the OTP could also serve as a hub site with multiple vans acting as the spokes. He added that one of these spokes could provide access to treatment in correctional facilities if the facility wishes to engage in that opportunity, similar to the Project Kickstart program in New Jersey that Mielke mentioned.
To enable any of these innovations, SAMHSA and the state opioid treatment authorities will need to work collaboratively, said Parrino, because some of the challenges lie within the states. For example, state or county zoning ordinances may prohibit an OTP in certain areas. In addition, he advocated for states to adopt Medicaid reimbursement mechanisms that provide access to reimbursement for the full services offered through the OTP, similar to those adopted by Medicare. “This is not just a simple policy statement, but must be coordinated with the states and even within counties,” he said. Moreover, he noted that the federal government needs to address OTPs’ concerns that even if they wish to expand access, they may be unable to find trained personnel.
OTHER STRATEGIES TO EXPANDING ACCESS THROUGH OTPs DISCUSSED BY INDIVIDUAL WORKSHOP PARTICIPANTS
In addition to the approaches described earlier in the chapter, several individual workshop participants in this session considered other strategies that could help expand access to methadone at OTPs, as well as several potential regulatory changes aimed at reducing some of the barriers to methadone access that people with OUD may encounter (see Box 5-1).
Incentivizing pro-recovery behaviors. Stoller noted that contingency management, such as paying people for pro-recovery behaviors like attendance to treatment, has often been effective, but its implementation has been limited by provider fears that it could be considered in conflict with federal laws governing inducements for treatment. New Jersey has been looking into implementing such a strategy, said Mielke. Brooner added that because counseling interventions may take some time to become optimally effective, incentivizing the ongoing attendance of patients may help retain patients during this gap between delivery of service and patient recognition of its effectiveness.
Eliminating or changing accreditation requirements. Stoller suggested that accreditation bodies also play an important role in limiting access to treatment. Accreditation is used in many regulatory systems to transfer oversight responsibility from a federal agency, in this case SAMHSA, to a third party, said Dooling. However, she noted that there is no requirement
in the Controlled Substances Act to use an accreditation model. She suggested that accreditation should be looked at in the context of the entire landscape of regulations in terms of how it works to serve patients. Dooling used the metaphor of pebbles in a stream to explain how individual requirements that may seem beneficial on their own can accumulate over time until they become onerous, in the same way that pebbles thrown into a stream can build up to block the stream’s flow.
Parrino added that from the American Association for the Treatment of Opioid Dependence’s (AATOD’s) point of view, the requirement that OTPs meet onerous accreditation standards creates inequities because those standards do not apply to other office-based practices. “It goes to the issue of having [a] bifurcated system of care,” he said.
Allowing hospitals and other institutions to initiate methadone treatment. Other systemic adjustments are needed to expand access, said Parrino. For example, Stoller mentioned that hospitals can freely administer methadone or other opioids to patients without involving an OTP as long as it is for no more than 3 days, or if the primary diagnosis for the hospitalization is something other than OUD. But hospitals, skilled nursing facilities, rehabilitation centers, and other entities cannot initiate MOUD unless they have specific authority to do so, said Parrino. Changing this would require DEA to work in conjunction with SAMHSA to modify the regulations on how they provide oversight, he said.
Easing restrictions for patients under 18 to obtain methadone. Stoller advocated eliminating the requirement that patients under 18 have two failed detox attempts. However, Brooner noted that in practice many programs have already moved away from these specific requirements and shifted closer to documenting only that the patient has a current OUD to be eligible for treatment. “42 CFR in those specific areas should reflect what the field already knows, and that is incorporate this more rational, reasonable requirement that we’re providing, ordering, or prescribing methadone for a person who has a clear and present opioid use disorder,” said Brooner.
Expanding exceptions to the 1-year history of opioid addiction requirement for patient admission. Stoller also advocated for expanding exceptions to the requirement that a person must be currently addicted to an opioid and has been so for at least 1 year before admission. He noted that there are only a few exceptions4 to this requirement. Parrino added that this is
___________________
4 Exceptions include “patients released from penal institutions with a documented history of opioid use disorder (within 6 months after release), for pregnant patients (program physician must certify pregnancy), and for previously treated patients (up to 2 years after discharge).” For more information regarding the federal guidelines for OTPs, go to https://store.samhsa.gov/product/Federal-Guidelines-for-Opioid-Treatment-Programs/PEP15-FEDGUIDEOTP (accessed May 9, 2022).
part of the policy recommendations AATOD released in September 2021,5 which suggest that clinical judgment should be used to determine stability in treatment, but that the time requirement should be eliminated.
Expanding the use of telehealth and reducing the frequency of urine drug screens. AATOD has also recommended the use of telehealth induction of methadone through OTPs. Mielke agreed, noting that the expanded use of telehealth during the pandemic as well as relaxation of the frequency of urine drug screens resulted in more patients accessing OTP services and staying in treatment. “I think the most important thing is getting individuals into treatment and helping support their recovery,” she said.
___________________
5 To learn more about AATOD’s policy recommendations, go to http://www.aatod.org/wpcontent/uploads/2022/03/Regulatory-Reform-and-Policy-Initiatives-for-OTPs-in-a-Post-COVID-19-World-09302021.pdf (accessed May 9, 2022).
This page intentionally left blank.














