
Throughout the workshop, participants explored opportunities to address current regulatory barriers to methadone treatment within opioid treatment programs (OTPs), as discussed in Chapter 5. However, several workshop participants also argued that this alone will not alleviate current access barriers to treatment, sufficiently increase provider capacity, and meet the demand for care. In this chapter, workshop participants explore regulatory changes outside the structure of OTPs—for example, office-based and pharmacy-based dispensing—that have the potential to further improve medications for opioid use disorder (MOUD), said Gavin Bart, director of the Division of Addiction Medicine at Hennepin Healthcare and professor of medicine at the University of Minnesota Medical School. Potential regulatory changes that could help facilitate these innovations noted by individual workshop participants are listed in Box 7-1 at the end of the chapter. In considering expansions beyond OTPs, Brenda Davis provided a note of caution, saying, “As we think beyond the historic integrated
OTP model where patients receive a variety of medical services, medication, case management, counseling, and other support services all in one place, it is critical that we not throw away the good with bad.”
OFFICE-BASED METHADONE
Methadone treatment delivery in physician offices is not permitted in the United States without a Substance Abuse and Mental Health Services Administration (SAMHSA) exception, said Robert Schwartz. By contrast, he said, Australia, Canada, Great Britain, and other countries have permitted office-based methadone treatment and pharmacy collaboration for decades; office-based methadone treatment is available for stable patients as well as new and unstable patients, he said.
However, research on office-based methadone treatment has been limited, said Schwartz (McCarty et al., 2021). In the United States, “methadone medical maintenance” has been studied only in stable patients, he said. Among the advantages, patients experienced less stigma and had less interaction with drug-using patients, Schwartz added. He summarized published literature on office-based methadone treatment in stable patients from five case areas in the United States: Manhattan, Baltimore, the Bronx, Seattle, and a pilot study in rural Lancaster, PA. The minimum abstinence criteria in these studies ranged from 6 months to 5 years, although many patients had much longer periods of abstinence, said Schwartz. In Manhattan and Baltimore, methadone was provided by physicians, while pharmacies dispensed the methadone in the other three sites. The outcomes for these patients were excellent, with very high rates of treatment retention and a remarkably low percentage of positive drug tests, said Schwartz. To assess diversion, staff randomly called patients between visits and asked them to return unused methadone. All patients brought the correct amount of medication back to the clinic, said Schwartz.
Four randomized clinical trials comparing office-based medical maintenance to usual care at an OTP have also been reported in the United States (Drucker et al., 2007; Fiellin et al, 2001; King et al., 2006; Senay et al., 1993). In one of these studies, the physician’s office was in the OTP. Schwartz said that in all of these studies, there was no significant difference between the two care models in terms of treatment retention or percentage of positive drug tests. One study also showed a non-significant difference in clinical instability, defined as two consecutive positive weekly drug tests or testing negative for methadone (Fiellin et al., 2001). In this study, patient satisfaction was significantly higher among participants in the office-based condition, although physicians noted that managing methadone administration was burdensome and better handled by pharmacists.
Another study was a three-group randomized trial comparing office-based medical maintenance, office-based medical maintenance in the physi-
cian’s office in the OTP (rather than at the nursing station), and usual care in the OTP. Participants in the office-based condition received 28 take-home doses per month; those receiving usual care in the OTP got 5–6 doses per week (King et al., 2006). This study added treatment intensification criteria, where if a participant in the office-based condition had one positive drug test or one failed callback, they went back to the OTP for weekly counseling and drug testing and received only two take-homes per week. If they stopped having positive drug tests after 4 weeks, they were able to return to physician office–based visits and an increased number of take-homes. No significant differences were seen among groups in terms of meeting the criteria for intensified treatment, and most returned to their original treatment condition, said Schwartz. Participants in both office-based conditions reported significantly higher rates of new employment or social and family activities than those in the standard OTP group, he said.
Schwartz suggested several regulatory changes for new or unstable patients that could achieve the goals of increasing patient choice and increasing the number of people in treatment:
- Select and implement the best international approach for methadone medical maintenance using offices and pharmacies based on evidence of safety, efficacy, and impact on overdose deaths. The selected approach should include safe dose induction guidelines, direct methadone administration, take-home rules consistent with OTPs, and an evaluation protocol that compares outcomes to the standard OTP approach, said Schwartz.
- Leverage the Drug Addiction Treatment Act of 2000 (DATA 2000) buprenorphine waiver system1 and community health infrastructure and link physician offices with OTPs or addiction treatment specialists to enable implementation of office-based methadone medical maintenance, he added.
For stable patients, Schwartz said the goals should be to increase patient choice, reduce stigma, integrate care, and create openings for new OTP admissions. To achieve this, he suggested:
- Expanding medical maintenance under current regulations using available evidence, and providing states and care providers with information about best practices, payment guidance, and how to obtain exemptions.
___________________
1 To learn more about buprenorphine waivers available from SAMHSA as part of the Drug Addiction Treatment Act of 2000 (DATA 2000), go to https://www.samhsa.gov/medicationassisted-treatment/become-buprenorphine-waivered-practitioner (accessed April 14, 2022).
- Updating regulations to permit trained pharmacists with connections to office-based sites to administer and dispense methadone.
- Supplying methadone directly to dispensing sites to reduce bureaucratic issues and barriers.
- Aligning take-home rules for office-based sites with those used at OTPs.
INTERNATIONAL MODELS OF PHARMACY-BASED DISPENSING
The use of pharmacies for dispensing methadone (previously discussed in Chapter 5), while experimental in the United States, is widely used in other parts of the world, said Bart. However, the models used vary across countries, said Jane “Janie” Sheridan, associate director of the Centre for Addiction Research at the University of Auckland, New Zealand. For example, some jurisdictions limit pharmacy dispensing of methadone to only stable patients; some services require supervised dosing while others allow take-home doses; and costs to the patient may also vary, she said. Any type of pharmacy, ranging from independent small pharmacies to large chain pharmacies, may provide these services, although large pharmacies may have the capacity to treat larger numbers of patients as well as access to inhouse training resources, which may not be available at independent pharmacies, said Sheridan. Whatever size pharmacy is providing services, she emphasized that they should have a private area for dispensing and good communication channels between pharmacists and prescribing physicians.
Small independent pharmacies may be the only pharmacies available in some regional and rural areas and should not be ruled out, said Suzanne Nielsen, deputy director of the Monash Addiction Research Centre in Melbourne, Australia. She added that if a large chain pharmacy decides to stop offering methadone because of its insufficient remuneration, this can have a major impact on access. Thus, she said, attention should be paid to reimbursement mechanisms and other types of financial support to encourage pharmacies to provide methadone programs.
Research and experience provide information about the benefits and issues for both patients and pharmacists of expanding availability of methadone beyond the clinic to community pharmacies. For example, patient access can be improved and allow more flexibility (Anstice et al., 2009), and may afford anonymity given that patients could be going to the pharmacy for any reason, not necessarily for methadone, said Sheridan. Pharmacists report improved professional satisfaction (Fonseca et al., 2018), including from developing supportive relationships with their patients, and there are opportunities for undertaking specialized training, she said. However, there are several considerations for both patients and pharmacists. Sheridan said
patients report concerns about privacy (Neale, 1999; Neale et al., 2018), and stigma (Anstice et al., 2009; Matheson, 1998; Neale, 1999; Neale et al., 2018), and pharmacists have reported perceived concerns about safety, patient antisocial behavior (Fonseca et al., 2018; Matheson et al., 2002), and community resistance (Fonseca et al., 2018).
Training is key to ensuring the successful implementation of pharmacy-based methadone treatment, said Sheridan. This includes not only training pharmacists to recognize when a patient is intoxicated, for example, but also training around attitudes and stigma, and creating a safe environment where patients feel welcome. In the United Kingdom (UK), Sheridan had participated in “shared care training,” where within a local area, primary care physicians engaged in training along with pharmacists and clinic staff around the delivery of methadone. Pharmacy assistants, technicians, front-line workers, office-based prescribers, and reception staff were also offered training and given the opportunity to talk about their concerns and misgivings about methadone. These types of training events, as well as improving professional networks, could, in the future, provide an opportunity to discuss issues around inequity and culturally appropriate responses to different groups of people, Sheridan added.
In Australia, around 80 percent of patients receive community pharmacy dosing and about half of pharmacies provide these services, said Nielsen. About two-thirds of patients receive care, including prescriptions, in primary care settings; only about one-third are prescribed opioid agonist treatments in specialist clinics. Medication is provided directly from the government at no cost to pharmacies but no payment is available to cover staffing costs to provide dosing, which typically means that pharmacies charge a dispensing fee to patients to cover those costs (Tran et al., 2021). A 24-hour help line provides clinical advisory services to both pharmacists and prescribers, and other clinical supports are also provided by the state to community pharmacies.
Methadone is listed as a “schedule eight” controlled drug in Australia, representing the highest level of control, but the same level as for morphine, oxycodone, and buprenorphine, said Nielsen. In terms of the regulation of pharmacy methadone supply, specific requirements around prescribing and administering methadone are usually outlined in state policies and clinical guidelines. While methadone prescribers are accredited in Australia, pharmacy accreditation varies by state, and individual pharmacists are not usually accredited, although they are recommended to complete training that covers jurisdictional policies and clinical aspects of care, said Nielsen. Lastly, the state health department must provide approval before a patient can start methadone (i.e., a patient-prescriber specific “permit” that limits a patient to one prescriber).
In addition to the regulatory protections, Nielsen noted that another aspect that supports patient and community safety within the community pharmacy program is the use of supervised dosing. She noted that early experiences in Scotland and the UK demonstrated significant reductions in deaths due to overdose involving prescribed methadone when unsupervised dosing was replaced with supervised dosing” (Strang et al., 2010).
During the COVID-19 pandemic, Nielsen said unsupervised dosing was more widely used and managed well. To mitigate risks of unsupervised dosing, patients are carefully assessed to determine the level of unsupervised dosing that is appropriate. A period of stabilization is usually required before unsupervised doses are allowed, and other checks and balances are in place, said Nielsen.2 She added that some states dilute take-home doses to decrease the likelihood of injection (Lintzeris et al., 2002).
“To date we haven’t seen evidence that it [increased unsupervised dosing during the COVID-19 pandemic] has led to increased mortality or diversion,” Nielsen said (Coroners Court of Victoria, 2021), adding that unsupervised dosing requires targeting and flexibility. Sheridan agreed, adding, “It’s possible to be more flexible without having disastrous consequences. The key is really careful assessment of each patient to see what is and isn’t appropriate, and also making sure that each patient is receiving a therapeutic dose of methadone.”
A naturalistic study in Australia found that dosing in community pharmacies rather than clinics improves retention; however, a study in Canada found the opposite effect (Burns et al., 2009; Gauthier et al., 2018), said Nielsen. Recognizing the limitations of observational studies, she acknowledged that patients were not randomized to pharmacy versus clinic dosing. She added that to increase treatment capacity in regional areas and use prescriber time more efficiently, Australia is taking steps to extend the use of pharmacists even more. This includes by enabling pharmacists to go beyond dosing to providing other aspects of clinical care. A model of collaborative care was co-designed with pharmacists, prescribers, and consumers, where pharmacists oversee treatment within a treatment plan, working within state and national guidelines with pharmacist providing reviews using validated assessment tools, she said (Nielsen et al., 2021).
INNOVATIVE MODELS OF INITIATION UNDER EXISTING REGULATIONS—INPATIENT AND OUTPATIENT SETTINGS
Even with the existing regulatory framework, there are opportunities not currently being leveraged to treat patients outside of OTPs before link-
___________________
2 For more information on this guidance, go to https://www.health.vic.gov.au/drugs-andpoisons/pharmacotherapy-policy-in-victoria (accessed June 14, 2022).
ing them to OTPs, said Alexander Walley, professor of medicine at Boston University School of Medicine. Key to all of these “venue-based methadone initiations” is a trusting relationship between the initiation venue and the OTP, he said.
Direct Admission to an OTP from Detoxification Centers
At medically managed withdrawal programs, more commonly called detoxification centers or detoxes, many people seek treatment to reduce both their use of opioids and their overdose risk, said Walley. Yet paradoxically, detox is often followed by low treatment, high relapse, and high overdose death. For example, Walley and colleagues showed that between 2012 and 2014 in a cohort of 61,000 people in Massachusetts, MOUD treatment rose from 15 to 20 percent immediately after detox (Walley et al., 2020). In other words, most people do not receive treatment, he said. “This has implications because detox patients who do receive further treatment have better survival,” as shown in Figure 7-1, he said, adding that in his opinion, “detox without further treatment really equals malpractice.”
Instead of patients in detox being tapered from their initial methadone dose down to zero, they are titrated to control withdrawal symptoms and opioid cravings and then transferred to an OTP. Walley noted that these direct admissions will hinge on an existing, trusting relationship between
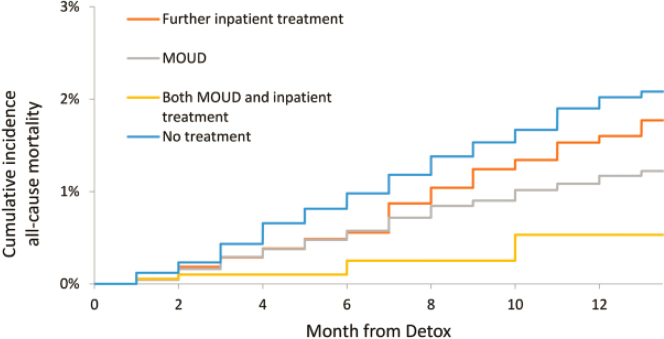
NOTE: MOUD = medications for opioid use disorder.
SOURCES: Presented by Alexander Walley, March 4, 2022; Walley et al., 2020.
the detox program and an OTP. At least one OTP that must accept patients initiated and titrated at a venue outside the OTP. Many detox programs are certified as OTPs and provide methadone, and therefore can serve as methadone induction centers, said Walley. He advocated for this model and noted that all detox centers in Massachusetts with methadone on their formulary are certified as OTPs.
Hospital Initiation of Methadone followed by Linkage to an OTP
While only federally certified and accredited OTPs can dispense methadone for the treatment of opioid use disorder (OUD), an exception allows a physician to administer methadone to maintain or detoxify a person as an incidental adjunct to medical or surgical treatment of conditions other than addiction.3 A study by Walley and colleagues showed that among patients who were initiated on medications for OUD or alcohol use disorder and then linked to outpatient addiction treatment, those linked to a methadone clinic achieved the highest rates of retention compared to buprenorphine and naltrexone through 6 months of follow-up (Trowbridge et al., 2017).
Delivery of Methadone in Outpatient Settings
A second exception to the requirement that only OTPs can dispense methadone for treatment of OUD is known as the “72-hour rule,” said Walley. This exception allows a physician not specifically registered to conduct a narcotic treatment program to administer but not prescribe methadone or other narcotic drugs for the purpose of relieving acute withdrawal. Only 1 day’s dose of medication at a time may be administered for no more than 3 days.4,5 This approach was used successfully at a low-barrier substance use disorder bridge clinic in Boston in March 2021, said Walley (Laks et al., 2021). In the following 6 months, of 138 patients seen at the bridge clinic under the 72-hour rule, 129 were referred to OTPs, 4 were referred to inpatient, 1 was sent to the hospital, and 4 were already enrolled at an OTP, said Walley. Moreover, he said, among those referred to either of their two main OTP partners, 87 percent were linked to the OTP and 58 percent were retained at the OTP at 1 month (Taylor et al., 2022).
___________________
3 Title 21 Code of Federal Regulations §1306.07 C.
4 Title 21 Code of Federal Regulations §1306.07 C.
5 A few weeks following the workshop, the Drug Enforcement Administration modified this rule to allow practitioners working in hospitals, clinics, and emergency rooms to request an exception allowing them to dispense a 3-day supply of medication. To learn more, go to https://www.dea.gov/press-releases/2022/03/23/deas-commitment-expanding-access-medication-assisted-treatment (accessed June 12, 2022).
Walley emphasized that all three of these venues see very high-risk patients. In another study, he and his colleagues have analyzed what they call the “critical encounter touch points” that lead to fatal overdoses. Opioid detoxification increased the risk of death 66-fold and non-fatal overdose increased the risk of death 111-fold compared to age-and-sex-matched individuals (Larochelle et al., 2019). “These are exactly the people that we need to make methadone accessible to because it is lifesaving and their risk is super high,” he said.
Walley suggested five concrete actions that could facilitate better use of these venue-based methadone initiations:
- Issue and promote guidance for OTP direct admission approaches that already exist under current regulations.
- Incentivize partnerships between OTPs and detox centers, hospitals, outpatient clinics, and emergency departments.
- Transform detox centers into induction venues via regulation and funding incentives.
- Redesign OTP intakes to be welcoming rather than a “gauntlet” for patients through (1) true treatment on demand; (2) starting methadone for withdrawal within an hour; (3) liberalizing dose titration and take-home access; and (4) integrating methadone into the rest of health care.
- Fund research that evaluates innovative methadone initiation approaches.
POTENTIAL NEW TREATMENT MODALITIES AND SETTINGS THAT COULD BE OPENED UP WITH REGULATORY CHANGES
In addition to these innovative opportunities that could be realized under existing regulations or expanded with regulatory changes, workshop speakers were encouraged to “think outside of the box,” said Bart. These novel types of settings provide opportunities to address racial and social inequities by making methadone more accessible, integrating community voices, and “lifting up the very people who have died unnecessarily during the drug overdose crisis,” said Ayana Jordan. Potential changes that could enhance methadone access for racial and ethnic minorities noted by individual workshop participants are listed in Box 7-2 at the end of the chapter.
Culturally Responsive Community-Driven Substance Use Recovery for Black and Latinx Populations
Black and Latinx people with OUD are dying at disproportionate rates, and have less access to effective treatment, said Jordan. “This is a serious
public health disparity that has not gotten the attention that White people have in dealing with their opioid use disorder,” she added. Jordan and Chyrell Bellamy of Yale University are leading an NIH U01 funded study, the Imani Breakthrough Project, which is centered on the experiences of Black and Latinx people, with a focus on community-based participatory research and community trust. The name Imani, which means faith in Swahili, was chosen by Black and Latinx community members who said they rely on their faith to break through and access recovery in dealing with OUD and other substance use disorders, said Jordan. Imani Breakthrough aims to promote health and healing for people in the community by creating a sense of unity and collective responsibility, she said (Bellamy et al., 2021).
Part one of Imani Breakthrough involves a 3-month group education component, with classes and activities devoted to wellness enhancements delivered in Black and Latinx churches. “We talk about the social determinants of health, which SAMHSA calls eight dimensions of wellness—spiritual, emotional, physical, financial, environmental, social, intellectual, and occupational dimensions—that are needed for someone to be successful in recovery,” said Jordan. In addition, a Citizens Enhancement Project6 focuses on the roles, responsibilities, relationships, resources, and rights that are essential components of citizenship. Jordan said this project has been shown to decrease substance use without access to any medication.
The second part of Imani Breakthrough provides 3 months of wraparound support and coaching, provided by Black and Latinx facilitators and people who use drugs, to address vulnerabilities in the social determinants of health, said Jordan.
The U017 itself has three aims, said Jordan, who uses the term medication for addiction treatment (MAT): (1) to evaluate the impact of Imani plus a church-based, telehealth, MAT option; (2) assess whether there are changes in substance use over time for Imani plus church-based, telehealth-provided MAT compared to Imani plus traditional referral and linkage for MAT; and (3) evaluate potential mediators and moderators of improvements that affect primary substance use disorder outcomes; for example, how choice of MAT treatment location and social determinants of health affect whether people stay in recovery.
All Imani participants get the full 24 weeks of intervention, but 1 month into the treatment each participant decides if they are interested in medi-
___________________
6 To learn more about the Citizens Enhancement Project, go to https://medicine.yale.edu/psychiatry/prch/research/comm_enhancement (accessed May 9, 2022).
7 For more information about the grant, go to https://clinicaltrials.gov/ct2/show/NCT05260047 (accessed June 14, 2022).
cation; if so, they are randomized to MAT delivered via telehealth in the church or referral to MAT in the community.
“All of our services have been informed by and are delivered by people who live in the community, people with lived experience, and trusted collaborators,” said Jordan. “We focus on harm reduction and choice, we emphasize mutual support, and we have intensive coaching to address the social determinants of health.”
She added that Imani values community partnerships as a way of connecting with “diverse communities within communities.” She noted that while being Black or Latinx has its own challenges, given the racism that permeates American society, “what extra stigmatization is added if you are non-gender conforming and Black or Latinx and have a substance use disorder and are engaging in methadone?” The different experiences of people with multiple stigmatized identities and the challenges faced by those who are undocumented or uninsured need to be better understood, said Jordan.
Jordan advocated for “#FreeMethadone” to increase access for Black and Latinx people and “reject the white supremacist organizing of methadone so it’s only in OTPs.” Her vision includes:
- Not requiring proof of insurance or other documentation to receive methadone.
- Allowing for telehealth prescribing of methadone in community settings (i.e., faith-based settings).
- Allowing for methadone to be given in primary care and community settings.
- Approving and extending the Opioid Treatment Access Act.
- Providing take-home dosing beyond 14 or 28 days when patients are stabilized.
Bridging Two Worlds: Methadone Treatment Consideration for American Indian/Alaska Native Communities
American Indian and Alaska Native peoples represent nearly 3 percent of the U.S. population and have one of the highest rates of opioid overdose mortality across all racial groups, said Kamilla Venner, a member of the Ahtna Athabascan tribe and professor of psychology at the University of New Mexico. She added that polysubstance use is present in many of these deaths. Most native peoples, about 78 percent, live outside of tribal areas, but about 22 percent live on reservations in tribal lands (U.S. Census Bureau, 2012).
Health inequities among American Indian and Alaska Native peoples are largely attributable to social determinants of health, said Venner. Lower median incomes, poverty rates nearly six times the national rate, and lower
rates of achieving a high school diploma combine with discrimination, racial historical trauma, and systemic racism to negatively impact mental and physical health, which may contribute to the overuse of opioids, she said. Venner added that the Indian Health Service (IHS) is chronically underfunded. She also noted some positive health behaviors among this population, such as higher than average rates of alcohol abstention and vaccination. Venner attributed these strengths to the fact that the U.S. government allowed the tribes to align messaging on these issues to cultural values such as “save our elders who are the knowledge keepers,” and “watch out for the community.”
To address the needs of American Indian and Alaska Native peoples, Venner said that the Office of National Drug Control Policy (ONDCP) needs to understand and deeply integrate a non-Western world view rooted in spirituality and traditional healing and work in equal partnership with tribal communities. This means, she said, “deeply engaging them, taking the time to get to know them and learn from their great wisdom, and then investing long term with them.” She added that the federal trust responsibility to Indian nations requires the United States to support tribal self-government and economic prosperity, protect Indian tribes, and respect their sovereignty.
Because of their sovereign nation status, federal and state regulations regarding methadone use do not apply to tribal nations, and different tribes have different approaches to treating OUD, said Venner. When dealing with a tribe that does not support the use of methadone, she approaches them with respect and a collaborative mindset to try to understand their position. If they are willing to engage in conversation, she may then have the opportunity to address misinformation about methadone treatment as well as the potential harmful outcomes when people are taken off methadone.
Venner suggested that there are aspects of evidence-based treatment that require cultural adaptation for American Indian and Alaska Native communities. For example, most evidence-based treatments are dyadic, involving only two people in the room, whereas a whole community may be involved in traditional healing. Evidence-based treatments are also stigmatized in this population, whereas traditional healing is admired; they tend to be secular rather than sacred; and they don’t explicitly include native culture, whereas traditional healing preserves and values culture, said Venner.
“If we just offer evidence-based treatment without any cultural adaptation, it might be viewed as a broken bridge or something that is not inviting or maybe even treacherous,” she said. “If we culturally tailor these evidence-based treatments, that bridge will look strong, inviting, and beautiful, and hopefully encourage more engagement and treatment.”
Regulatory barriers discussed throughout this workshop may be compounded for American Indian and Alaska Native peoples, said Venner. For
example, she noted that having daily in-person visits is challenging for people living in poverty; lack of privacy in receiving methadone can be stigmatizing and often is not humanistic.
National data also indicate that American Indian and Alaska Native peoples have less access to methadone, said Venner. For example, data from the National Survey on Substance Abuse Treatment Services showed that methadone was least likely to offered as a treatment for OUD if treatment was sought from an IHS clinic or if it was a tribally run clinic or a clinic with providers that speak the tribal language (SAMHSA, 2019). Facilities serving American Indian and Alaska Native peoples appeared to offer MOUD at typical rates, but were less likely to offer buprenorphine or methadone and more likely to offer naltrexone or vivitrol. Another survey showed that only 28 percent of facilities serving American Indian and Alaska Native peoples offered medication-assisted treatment for substance use disorder (Rieckmann et al., 2017). Payment barriers also limit access to methadone by American Indian and Alaska Native peoples, said Venner.
Venner suggested that to encourage engagement and overcome barriers of stigma within American Indian and Alaska Native communities, it may be helpful to frame methadone as a medicine and remember that they were some of the original pharmacists, using plants and herbs as medicine. She also advocated ensuring that providers, directors, and staff are themselves American Indian and Alaska Native or at the very least are knowledgeable and comfortable discussing culture; hiring American Indian and Alaska Native Elders as staff or cultural educators; and ensuring there is space for traditional services and cultural activities.
In developing such programs, Venner offered these suggestions:
- Consult and partner with American Indian and Alaska Native peoples.
- Learn from successful programs, such as the didgwálič Wellness Center in Anacortes, WA, which offers all services under one roof, including administering medication in a private room and providing medical, behavioral, and dental health care.
- Advocate for more resources for American Indians and Alaska Natives.
- Make sure assessments are valid for American Indians and Alaska Natives and that treatments are delivered in a culturally centered, appropriate way.
- Increase the availability of treatments, decrease restrictions, and incentivize the delivery of methadone in humane and culturally appropriate ways.
















