
“Our methadone system is unique to the U.S. and evolved through the accident of our history and politics,” said Helena Hansen, professor of psychiatry and chair of the research theme in translational social science and health equity at the University of California at Los Angeles David Geffen School of Medicine, and moderator of the first workshop session. Moreover, she said, “Understanding how that happened helps us to see that our current regulations could be otherwise.”
THE EARLY YEARS OF METHADONE MAINTENANCE REGULATION AND THE POLITICS OF STIGMA AND RACIALIZATION
According to Samuel Kelton Roberts, associate professor of history, sociomedical sciences, and African American and African diaspora studies at Columbia University, methadone maintenance1 is one of the most closely regulated medical protocols. “Perhaps not entirely by coincidence, it is also one of the most stigmatized, controversial, and misunderstood,” he said. Stigma alienates patients from treatments such as methadone maintenance, said Roberts. Black patients are particularly affected by a trifecta of stigmas—being Black, having an opioid use disorder, and being a methadone patient—which, combined with the history of medical abuses against people of color, has engendered a culture of mistrust, he said. Roberts’ ideas are further developed in the commissioned paper that can be found in Appendix C.
Methadone emerged as a maintenance treatment modality for heroin dependence in the mid-1960s. Mark Parrino, added that opioid treatment programs (OTPs) came into existence because of a rejection by the medical community to treat this particular patient population.
By 1972, the Food and Drug Administration (FDA) and the Drug Enforcement Administration (DEA) had instituted severe regulations that restricted access, said Roberts. These regulations were designed primarily to prevent methadone from being diverted to the street, he said. For example, patients were required to receive medication under close supervision at federally approved clinics and submit to regular urine testing. Some states also employed coercive tactics, such as requiring participation in a methadone program in order to receive public benefits or to obtain release from prison, said Roberts. Physicians were also subject to close scrutiny and were required to have complicated security systems to prevent diversion.
“When the FDA created this restrictive environment and Congress bifurcated authority between DEA and what would ultimately be SAMHSA,”
___________________
1 Methadone maintenance treatment was the term used most frequently in the historical period discussed here. The preferred term today is medication for opioid use disorder (MOUD).
recalled Parrino, “I will tell you without any reservation that it was sort of akin to the Wild West prior to the implementation of the regulations.”
Roberts said policies instituted at that time affect how methadone treatment is viewed. When a treatment is heavily regulated, he said, people assume that it is dangerous. Another common criticism of methadone is that it is portrayed as a “false cure,” merely substituting one drug for another, said Roberts.
Public mistrust of methadone as a useful medical intervention increased when many politicians began promoting it more for its ability to reduce crime than for its therapeutic potential, said Roberts. Regulations were also instituted against a backdrop of increasing calls from Black grassroots organizations for community involvement in policy decisions relevant to the Black community. Yet, local community health and antipoverty organizations were excluded from policy discussions, increasing the alienation of those communities and contributing to the perception that methadone could be weaponized as an agent of social control and even genocide, said Roberts.
CURRENT BARRIERS TO ACCESS, INITIATION, AND RETENTION IN METHADONE TREATMENT
With an understanding of the historical backdrop to methadone regulations in the United States, several workshop participants discussed the effects of those regulations on health inequities, including social barriers to treatment, and considerations for special populations. Those populations include minoritized groups; people with low income; elderly individuals; people involved in the criminal justice system; pregnant women; lesbian, gay, bisexual, transgender, queer, intersex, asexual and all sexual and gender minority (LGBTQIA+) individuals; and individuals with HIV/AIDS.
Racial and Ethnic Minorities: High Risks, High Barriers
Opioid overdose death rates have skyrocketed in the past 20 years in all racial and ethnic groups, with the greatest increase among Black Americans in the past 10 years, said Magdalena Cerdá, professor and director of the Center for Opioid Epidemiology and Policy at the Department of Population Health, New York University Grossman School of Medicine (Friedman et al., 2022). The COVID-19 pandemic has exacerbated the crisis further, she said. In 2021, more than 100,000 people died from opioid overdoses, with particularly high increases among racially minoritized groups, especially Black Americans, followed by people of Asian and Hispanic ancestry (Baumgartner and Radley, 2022) (see Figure 3-1).
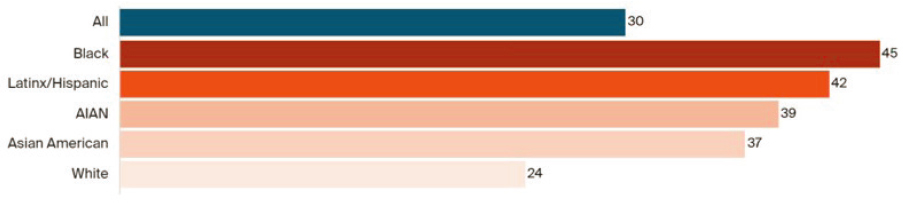
NOTE: AIAN = American Indian/Alaska Native.
SOURCES: Presented by Magdalena Cerdá, March 3, 2022; Baumgartner and Radley, 2022; CDC, 2021.
Cerdá noted that studies have shown that increased access to medications for opioid use disorder (MOUD) has the power to substantially reduce overdose rates. “What is particularly tragic is that racially minoritized individuals, who are experiencing some of the greatest rises in overdose rates today, have less access to medications for opioid use disorder,” said Cerdá.
In a study comparing the number of people who meet the criteria for OUD with those who actually receive treatment, Cerdá and colleagues documented a huge gap, as well as disparities in who gets access to treatment (this study is under review). Other studies have shown similar inequities across racial lines, said Cerdá (Wu et al., 2016). Indeed, one study showed that White patients are more likely to be referred to a medical professional and receive medication as part of their treatment plan, and less likely to leave against medical advice or be terminated by the facility than are racially minoritized patients (Entress, 2021). Regions with large Black and Hispanic populations have also been shown to have reduced access to hospitals that offer medication-based treatment (Chang et al., 2022).
Looking specifically at access to methadone and buprenorphine, Cerdá noted additional examples of racial patterning, with racially minoritized individuals having lower access to buprenorphine, which she called a “more flexible form of care” (Schiff et al., 2020). Whereas buprenorphine can be accessed through a primary care provider or psychiatrist with a prescription that can be picked up at a pharmacy and consumed in the comfort of their own home, access to methadone is much more difficult, said Cerdá. Access to methadone requires people to attend a licensed OTP as often as 6 days per week, said Cerdá. They sometimes must stand in line outside waiting for treatment. “This is in itself a highly stigmatized, punitive approach to getting access to treatment,” said Cerdá.
Geographical differences in access to buprenorphine and methadone treatment also contribute to racial patterning, said Cerdá. A study in New York City by Helena Hansen and colleagues showed that between 2004 and 2013, buprenorphine treatment increased across all areas, with a significantly higher increase in areas with the highest income and lowest percentage of Black, Hispanic, and lower income residents. By contrast, methadone use was concentrated in areas of high poverty and a higher concentration of Black and Hispanic residents, said Cerdá (Hansen et al., 2016). Cerdá and colleagues observed a similar pattern when they analyzed data from more than 3,000 counties across the United States. Methadone was more likely to be available in counties with highly segregated Black populations, whereas buprenorphine was more likely to be available in highly segregated White communities (Goedel et al., 2020).
Cerdá suggested that to reduce racial and ethnic inequalities in access to MOUD, regulatory and social barriers need to be dismantled. The first regulatory barrier she cited is the restriction of methadone to specialized
licensed programs. This limits access because people are often required to travel far from home to get treatment. She noted that this is a particularly acute problem for rural populations. Second, Cerdá said, requiring people to attend a facility to access care can be challenging for low-income people in particular, who must balance this requirement against the realities of childcare and non-flexible jobs. Requiring facilities to provide counseling presents another regulatory barrier because it makes it difficult to fully staff opioid treatment programs, resulting in a limited number of facilities licensed to provide methadone, Cerdá added.
Social barriers include affordability (including the cost of copays), insurance and Medicaid-imposed limits on the duration and dose of treatment for methadone, and prior authorization requirements, said Cerdá. Beyond these factors related to the cost of treatment, other social barriers to methadone treatment include stigma, discrimination in health care settings, lack of culturally responsive and respectful care, and the inequalities present in the criminal justice system. “We know that there are racial and ethnic inequalities in arrests and incarceration,” said Cerdá. “At the same time, we know that for every day spent incarcerated, the likelihood of initiating and being retained in treatment decreases substantially.”
Cerdá suggested policy solutions that could reduce racial and ethnic inequalities in access to MOUD. She cited a study showing that after the implementation of the Affordable Care Act, Black patients were more likely to access MOUD, particularly in states that expanded Medicaid coverage. Other policies that could broaden access to MOUD include integrating methadone into office-based treatment,2 particularly in primary care, and allowing for telehealth prescribing and pharmacy dispensing of methadone, said Cerdá. She noted that during the COVID-19 pandemic, telehealth prescribing and pharmacy dispensing were allowed for buprenorphine. The Opioid Treatment Access Act of 2022 (HR 62793 and S 36294), introduced in the U.S. Senate by Edward Markey (D-MA) and Rand Paul (R-KY), and in the U.S. House of Representatives by Donald Norcross (D-NJ) and David Trone (D-MD), would help to achieve these goals.
Finally, Cerdá suggesting making permanent the federal requirement that Medicaid cover all medications for OUD; enacting policies to reduce copays and prior authorization requirements by commercial insurance; and expanding the possibility of using community settings to dispense methadone, including mobile units and harm reduction programs.
___________________
2 Outpatient treatment services provided outside of licensed OTPs by primary care or general health prescribers with a Drug Addiction Treatment Act (DATA) waiver.
3 To learn more about HR 6279, the Opioid Treatment Access Act of 2022, go to https://www.congress.gov/bill/117th-congress/house-bill/6279/text (accessed May 2, 2022).
4 To learn more about S 3629, the Opioid Treatment Access Act of 2022, go to https://www.govinfo.gov/app/details/BILLS-117s3629is (accessed May 2, 2022).
Pregnancy and Parenting: A Critical Time for People with OUD
Pregnancy is a critical moment for addressing OUD because there is near-universal health insurance for pregnant people and motivation to protect their baby-to-be, said Mishka Terplan, medical director at Friends Research Institute and adjunct faculty at the University of California, San Francisco. He added that methadone and buprenorphine are the safest and most effective medications for OUD during pregnancy and improve outcomes.
However, for people with OUD, “we oftentimes abandon support during pregnancy, in particular postpartum,” said Terplan. He maintained that this distinction results from a federal statute that is misaligned with the normal physiology of pregnancy, the realities of the postpartum period, and the right and dignity of parenting. He explained that during pregnancy, as the metabolism of most people shifts toward rapid or ultrarapid metabolism, increasing methadone doses may be needed, particularly later in gestation. Once-daily dosing and restrictions against take-home doses, which could enable patients to split doses over the day, may lead to overmedication following dosing and undermedication the rest of the day, he said.
Terplan also linked treatment attrition caused by the lack of or non-continuation of health insurance or Medicare to the marked increase in maternal deaths in the United States. “Overdose is one of the leading causes of maternal death in the United States, and most of these deaths happen in the postpartum period,” he said. Some of this increase in overdose deaths postpartum is due to treatment attrition, which in the case of methadone may result from discontinuation of health insurance or Medicaid after giving birth, said Terplan. Standard prenatal care also often ignores the “fourth trimester,” that is, the 1-year postpartum period, he said.
Finally, he cited the proliferation of punitive state policies related to substance use in pregnancy as a driver of worse obstetric outcomes, higher rates of neonatal abstinence syndrome, and low birthweight and preterm delivery. These punitive policies are due to an increase in restrictive reproductive health policies at the state level, he said. For example, states that have restricted abortion access are more likely to collapse substance use in pregnancy with child abuse, even though he said the assumption that OUD or using drugs during pregnancy is associated with abuse or neglect is not supported by the literature. These same states are also more likely to arrest, prosecute, and convict pregnant people who miscarry while using drugs or give birth to an infant who develops symptoms of withdrawal to opioids.
Substance use is also the primary driver of increased foster care placements in the United States, added Terplan, noting that there are marked racial inequities in the child welfare system, driven in large part by primary health care providers. Terplan’s research has shown that the rate of
screened-in reports5 from medical professionals has increased markedly over the past decade, particularly for Black infants, followed by Alaska Natives and American Indian infants and other minoritized populations. “The child welfare system on the whole is a system of surveillance, not of support,” said Terplan.
Yet, he maintained that while a huge amount is known about early childhood development and how to support children in their development, the child welfare system and foster placement in particular interfere with that greatly. Instead of focusing on drugs and whether someone has a positive drug test, he suggested the need to “flip the script, to acknowledge what we all agree upon, which is that all children should be raised in stable communities devoid of violence so that they can thrive and reach their full potential.” Until the focus is changed from drug enforcement to early childhood development, some form of discrimination and stigma is going to be inherent,” said Terplan.
He advocated loosening OTP regulations to address the needs of pregnant and parenting people. Split dosing (i.e., dividing a prescribed daily dose of methadone into two or more administrations in the course of one day) is just one example of how regulatory change could result in better pregnancy outcomes. More generally, Terplan supported efforts to provide integrated child and family friendly reproductive health services at treatment sites.
At the federal level, he noted that the Child Abuse Prevention and Treatment Act (CAPTA)6 is currently undergoing reauthorization, providing an opportunity for states to decouple substance use disorder from child abuse; to roll back punitive policies; and to implement legislation grounded in basic bioethical principles.
Unique Barriers for LGBTQIA+ Individuals and People Living with HIV
LGBTQIA+ individuals, including or as well as those living with HIV, comprise communities with unique health disparities and inequities, including in the realm of substance use disorders, said Alex Keuroghlian, associate professor of psychiatry at Harvard Medical School and director of the Division of Education and Training at The Fenway Institute. Fenway Health was founded more than 50 years ago as a historically LGBTQIA+focused health center, said Keuroghlian. The National LGBTQIA+ Health
___________________
5 A “screened-in report” is a report to state child protection agencies that will be followed up with an investigation.
6 To learn more about CAPTA, go to www.acf.hhs.gov/cb/law-regulation/child-abuse-prevention-and-treatment-act-capta (accessed March 28, 2022).
Education Center at the Fenway Institute7 offers educational programs, resources and consultation to health care organizations, he said. Among these resources are best practice guidelines for addressing opioid use disorders among LGBTQIA+ people.8
Keuroghlian cited several examples of the impact of the opioid epidemic on this population:
- Data from SAMHSA indicate that there is a higher incidence of prescription pain medication misuse among sexual minority people, and research also shows that sexual minority youth misuse prescription pain medication earlier in life than do their sexual majority counterparts, said Keuroghlian (Kecojevic et al., 2012).
- Men who have sex with men (MSM) also have higher perceived stress levels associated with higher opioid misuse (Kecojevic et al., 2015), and non-medical opioid use among MSM is associated with risky behaviors such as condomless sexual intercourse and sharing of syringes (Zule et al., 2016).
- Transgender and gender-diverse middle and high school students report increased use of prescription pain medication compared with cisgender teens, and adults on Medicare report increased levels of chronic pain, which puts them at higher risk for opioid use disorder, said Keuroghlian. In addition, when transgender and gender-diverse individuals pursue gender-affirming surgery, they are often prescribed opioids to manage their pain.
- Keuroghlian and colleagues have also shown that among transgender and gender-diverse adults, the increased prevalence of substance use is associated with intimate partner violence, posttraumatic stress disorder (PTSD), public accommodations discrimination, unstable housing, and sex work; all are viewed as downstream effects of chronic gender minority stress (Keuroghlian et al., 2015).
“This is an oppressed minoritized population with a massive built-in exposure to opioids,” said Keuroghlian. “We’re increasingly having conversations with public health officials and policy makers to try to mitigate the adverse public health impact of exposure.”
Keuroghlian said the health inequities experienced by LGBTQIA+ people must be understood in the context of a minority stress framework. From
___________________
7 To learn more about the National LGBTQIA+ Health Education Center, go to https://www.lgbtqiahealtheducation.org (accessed March 24, 2022).
8 The publication “Addressing Opioid Use Disorder among LGBTQ Populations” is available for download at https://www.lgbtqiahealtheducation.org/publication/addressingopioid-use-disorder-among-lgbtq-populations.
early childhood through adolescence and adulthood, LGBTQIA+ individuals experience a high level of external stigma-related stress in the form of everyday discrimination, victimization, microaggressions, and outright violence, said Keuroghlian. He noted that there is also an intersectional component to this stigma-related stress. For example, he said the Federal Bureau of Investigation has reported that African American transgender women have among the highest incidence of hate crimes in the United States.
For many people, this external stigma-related stress may lead to disruptions in psychological processes, coping skills, emotional regulation, interpersonal functioning, and protective cognitive structures and beliefs. These disruptions, combined with medical mistrust due to the historical mistreatment of LGBTQIA+ individuals in health care systems, may result in distressing beliefs, such as that their lives will never improve, or that no one can be trusted. External stigma-related stress combined with similar internal stress, such as internalized homophobia or transphobia, may also lead to an increased prevalence of behavioral health problems and depression, anxiety, PTSD, and substance use disorders, said Keuroghlian. These stressors, in turn, can lead to decreased engagement in health care, resulting in physical health problems.
Keuroghlian and colleagues have used this minority stress framework to understand the evidence on opioid use and misuse among LGBTQIA+ people and suggest behavioral health interventions using a trauma-informed approach (Girouard et al., 2019). He added that while minority stress can present as a crisis, it can also provide an opportunity to cultivate resilience and learn adaptive coping skills. However, Keuroghlian emphasized that addressing OUD in this population will require not just cultivating resilience, but more importantly, making policy and structural changes.
For example, MOUD is an important tool for treating opioid use disorders in LGBTQIA+ people, but it is not sufficient, said Keuroghlian. He advocated incorporating behavioral health approaches such as cognitive behavioral therapy, delivered in a culturally responsive manner grounded in the minority stress framework and tailored for LGBTQIA+ people. Such care would focus on minority stress-specific triggers for cravings, such as identity-related discrimination and victimization, expectations of rejection, identity concealment, and internalized homophobia/transphobia (Girouard et al., 2019).
Framing substance use disorders as barriers to personal health goals may also be useful. For example, Keuroghlian said he has found that the most compelling reason people give for maintaining abstinence from opioids is that they want to pursue gender-affirming surgery and know the surgeon would require this in order to perform the procedure with good surgical outcomes. In addition, culturally responsive biobehavioral approaches for transgender people should address medically unmonitored
hormone use, particularly in Black, Indigenous, and People of Color, who often have less access to gender-affirming medical care.
Keuroghlian emphasized the importance of delivering methadone-related care in environments that are inclusive, affirming, and welcoming to the identities of LGBTQIA+ peoples (Goldhammer et al., 2021). Progress has been made in this regard through the use of electronic health records, he said. Since 2016, the Bureau of Primary Healthcare9 has required all Federally Qualified Health Centers (FQHCs), nearly 1,400,10 to report sexual orientation and gender identity data (Keuroghlian, 2021). “This allows us to engage in population health management and also improves culturally responsive addiction care at health centers nationally,” he said, noting that more standardized data collection across health systems could improve this even further. He added that city-level non-discrimination policies related to sexual orientation and gender identity increase the completeness of reported data (Almazan et al., 2021). “So there’s a real relationship between nondiscrimination laws and collection of this important demographic data to be able to provide culturally responsive tailored care,” said Keuroghlian.
Keuroghlian noted that many of the challenges discussed in providing methadone care to LGBTQIA+ people also extend to people living with HIV. He and his colleagues have implemented clinic-based and mobile buprenorphine interventions for this population in recent years. A similar implementation science approach is needed to evaluate and scale up such interventions in the methadone space.
Challenges for Older Adults with OUD
Current policies regarding dosing, take-homes, and where methadone can be dispensed also fail older adults with OUD, said Ximena Levander, assistant professor of medicine and clinical investigator at Oregon Health & Science University. She gave two examples, which highlight the challenges faced by older adults.
In the first example, a 60-year-old man being treated with methadone for chronic severe pain had turned to heroin when the primary care clinic where he had been treated closed and he was unable to find another clinic where he could receive methadone treatment. Levander saw him at an OTP after he had developed a severe OUD. He asked not to exceed 60 milligrams of methadone once per day because he experienced sedation at higher doses that limited his ability to function normally. However, at night when the
___________________
9 To learn more about the Bureau of Primary Healthcare, go to https://bphc.hrsa.gov (accessed March 27, 2022).
10 For more information about Federally Qualified Health Centers, go to https://bphc.hrsa.gov/about-health-centers (accessed June 14, 2022).
morning methadone dose wore off, he continued to use heroin. This led to a positive urine drug test for opioids and ineligibility for take-home doses.
Older adults are at increased risk of having musculoskeletal pain as well as co-occurring conditions that limit their ability to safely receive methadone treatment under current guidelines or those that make receiving methadone treatment prohibitively challenging, said Levander. For example, these co-occurring conditions may result in reduced mobility or cognitive impairment, making it difficult to get to an appointment even if they remember it, she said. Each co-occurring condition also increases the risk of polypharmacy, said Levander, noting that there is an extensive list of medications that interact with methadone. Moreover, the metabolism of methadone changes significantly with age. The result, she said, is that chronic pain may be better treated with methadone dosed two or three times per day depending on how it is metabolized and how it works on opioid receptors. Side effects from methadone treatment that may also be a significant concern in older adults include heart arrhythmias, respiratory depression, worsening constipation, urinary retention, and sedation, often increasing their risk for falls and injury.
Physical limitations and access challenges were a particular problem for the second patient Levander described. She was a frail 58-year-old woman with multiple medical conditions including severe opioid use disorder, which was being treated at an OTP with 80 milligrams of methadone per day. She was hospitalized with a severe heart infection called endocarditis, which caused a blood clot that caused a spinal infarct and bilateral paralysis in her legs. Her doctors recommended discharge to a skilled nursing facility (SNF), but no such facility was found that could dispense her methadone. To facilitate discharge to the SNF, there was an attempt to switch her to buprenorphine, which she was unable to tolerate. Levander recalled, “Given no options for rehabilitation, she was transitioned to comfort care and eventually died in the hospital on methadone.”
This patient highlights the devastation that can result from barriers to treatment in a SNF faced by patients on methadone, said Levander. Indeed, she said, a research study found that many nursing facilities violate Americans with Disabilities Act (ADA) laws by rejecting patients for post-acute facility placement (Kimmel et al., 2021). This is discussed further in Chapter 6.
Levander mentioned several policy changes that could have prevented the tragic outcome this woman experienced. For example, while current policies require daily dosing regardless of a person’s living situation, the controlled environment of a SNF could have been able to accommodate split dosing at more appropriate levels.
Other system gaps and potential policy changes discussed by Levander and other individual participants in this workshop session are summarized
in Box 3-1. These include changes to Medicare reimbursement guidelines. Levander said Medicare historically did not cover treatment in an OTP, requiring patients to self-pay if they wanted to stay on methadone or if unable to pay, to transition off methadone. The Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities (SUPPORT) Act of 201811 expanded addiction treatment coverage for Medicare and Medicaid. In addition, Medicare Managed Care and Advantage Plans as well as private insurance may limit coverage through requirements for cost sharing and prior authorizations. Levander advocated including methadone as a preferred drug by Medicare Part D to promote reforms such as providing methadone through pharmacies, doctors’ offices, and hospitals for older adults.
Training in addiction treatment across all population groups is also critical, said Levander. “Our patients deserve to be treated by people who are trained to provide them with the best evidence-based care in a non-stigmatizing and compassionate way,” she said. Keuroghlian echoed that point, noting the need for medical education reform and integration of addiction medicine into the standard curriculum at schools of medicine, nursing, and social work. He suggested that this is already happening in schools across the country, as medical educators have become more cognizant of social determinants of health and equity.
___________________
11 To learn more about the SUPPORT Act and other federal regulations that pertain to medication-assisted treatment for OTPs, go to https://www.samhsa.gov/medication-assistedtreatment/statutes-regulations-guidelines (accessed April 6, 2022).
This page intentionally left blank.
















