
The correctional system is the default health care setting when treatment for drug addiction has failed, leading to other behaviors, said Tracie Gardner, senior vice president of policy advocacy at the Legal Action Center. Indeed, she said, a majority of incarcerated people—some 58 percent of state prisoners and 63 percent of sentenced jailed inmates—meet the criteria for drug dependence or addiction (Bronson et al., 2017). Yet, she noted that correctional settings represent challenging environments for the provision of care. Consequently, the risk of death from overdose for people coming out of correctional facilities is extraordinarily high, she said (Joudrey et al., 2019b). Gardner added that improving treatment for opioid use disorder within the criminal justice system has the potential to provide more broad information about the care of people within the correctional system.
CROSSCUTTING REGULATORY ISSUES THAT IMPACT CORRECTIONAL FACILITIES AND OTHER INSTITUTIONS
While most of the world has figured out that punishment does not work as a remedy for addiction, Josiah “Jody” Rich, professor of medicine and epidemiology at Brown University and a 28-year consultant to the Rhode Island Department of Corrections, pointed out that the criminal justice system remains stuck in the punishment mode. As an example, he said, the United States spends $182 billion per year on mass incarceration, but only $2.8 billion per year on treatment for opioid use disorder (OUD) (NIDA, 2021; Wagner and Rabuy, 2017).
More than 2 million people are behind bars each day in the United States, about two-thirds in prisons and one-third in jail, and more than 10 million people cycle in and out of correctional facilities each year, said Rich (Minton et al., 2021; Zeng, 2020). He added that nearly one in five of these people coming in and out of prisons and jails have OUD (Bronson et al., 2017). Because jail populations turn over much more frequently than prison populations, he suggested that jails present an opportunity to provide treatment for many more people with OUD.
Individuals with OUD tend to self-report more chronic conditions, higher levels of disabilities, severe mental illness, or co-occurring drug use, and have involvement in the criminal justice system compared with individuals with no opioid use (Winkelman et al., 2018). Indeed, said Rich, the definition of addiction is continued use despite adverse consequences. With OUD, people develop tolerance and withdrawal, which leads to a cycle of ever-increasing dosages and often, involvement in the criminal-legal system, said Rich. During incarceration, their use generally decreases because of the decreased availability of opioids, he said. When they are released to the community, they have lower tolerance and are set up for an overdose. Consequently, people coming out of correctional facilities are at much higher risk of fatal overdose in the first 2 weeks after release, said Rich (Binswanger et al., 2007; Bukten et al., 2017; Ranapurwala et al., 2015).
He added that incarceration disrupts supportive resources that could be protective against overdose. “So what we have is the highest risk population at the highest risk time,” said Rich, making it especially important to start treatment at this critical time. He advocated screening people entering the correctional system for OUD and either initiating treatment or continuing them on the treatment they have been receiving. Most critical, he said, is ensuring that they have connection to treatment in the community after release. “If we start people with treatment on the inside and have no provisions for them to get connected with treatment on the outside, we have not really helped them,” he said. Rich noted that while racial disparities in the criminal justice system itself also extend to treatment in the community, he suggested that if high-quality treatment could be expanded in correctional settings and linked to high-quality care in the community, some of those racial disparities might be offset.
Medication is the gold standard for OUD in the criminal justice system as in other settings, said Rich. Rikers Island in New York started a methadone program in 1987 and until recently was one of the only such programs in the country. In 2016, he helped start the first statewide comprehensive program in Rhode Island, which offers all three medications—methadone, buprenorphine, and naltrexone—as well as linkage to care in the community. Patients and clinicians work together to decide what medication is
best, said Rich. Surprisingly, when asked, most people knew which treatment they preferred: About half chose methadone, another half chose buprenorphine, and almost no one preferred naltrexone, he said.
Rich and colleagues have also launched a website called the Jail and Prison Opioid Project (JPOP)1 that collects, tracks, and shares data about medications for opioid use disorder (MOUD) programs in prisons and jails and serves as a repository for resources on implementing such programs. Data collected by JPOP indicate that about 10 percent (n = 634) of all correctional facilities offer any type of MOUD and about 40 percent of those offer methadone, at least to some patients, said Rich. Most of these programs collaborate with an outside opioid treatment program (OTP) to get their methadone, but 19 operate as an OTP themselves. To operate as their own OTP is an onerous process, said Rich, yet he suggested that many of them already have a full pharmacy that distributes controlled substances in a controlled environment.
Figure 6-1 shows the treatments provided by the different programs. Interestingly, in light of the Rhode Island program’s data showing that few patients prefer naltrexone, more than 200 programs offer naltrexone only. Rich suggested that the reason for this is that “naltrexone is a blocker so it appeals to the custody and control mentality, and it’s a monthly injection.” He added that people are generally started on naltrexone “on their way out the door” and that there is little evidence for it being successful in the long run.
In terms of regulatory changes needed to expand MOUD in correctional facilities, Rich noted that because regulations were not designed with these facilities in mind, many of them do not make sense. For example, he said, take-home doses are not an option for incarcerated people and some of the security regulations pertain only to facilities in the community. He asserted that a goal of methadone regulation revisions should be to encourage and facilitate expansion of methadone in correctional facilities and the connections to community programs after release. This is probably best addressed by revising clinical practice guidelines, he said. Other mechanisms Rich supports are reducing the obstacles for prisons to become OTPs, expanding how OTPs function in correctional settings, expanding the use of mobile units at correctional facilities, and enabling these facilities to have their own pharmacies with Drug Enforcement Administration (DEA) certification to distribute controlled substances. To expand community resources available after release, he advocated expanding the ability of pharmacies and physicians to provide methadone to patients.
Rich suggested developing regulatory structures for correctional facilities that parallel those used in hospitals, where people can be started on
___________________
1 To access the Jail & Prison Opioid Project website, go to https://prisonopioidproject.org (accessed April 11, 2022).
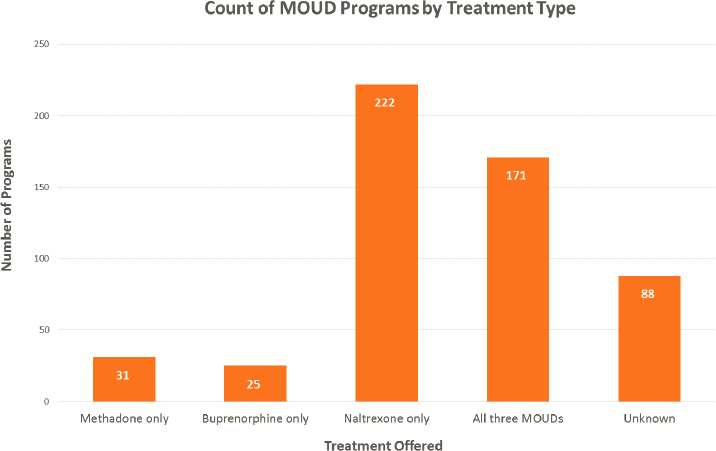
NOTE: MOUD = medications for opioid use disorder.
SOURCES: Presented by Josiah “Jody” Rich, March 3, 2022; Jail and Prison Opioid Project.
methadone, continue treatment, and link to community resources. He also recommended standardizing state regulations so they align with federal guidelines.
TRANSITIONING FROM INCARCERATION TO THE COMMUNITY
For people with OUD, the transition from incarceration to the community is a high-risk period associated with poor health outcomes, said Emily Wang, professor of medicine and public health at the Yale University School of Medicine and director of the SEICHE Center for Health and Justice. “A primary reason for this is that most return home without any access to safe housing, food, or gainful employment, and this is worsened by structural barriers that prevent people with criminal records from obtaining public assistance or applying for jobs,” she said. They also have limited access to quality health care for a variety of reasons arising from the fact that correctional health care is largely siloed from community health care,
said Wang. They may have to find their own doctor and reactivate their insurance, yet with criminal records, they face barriers to access, including stigma often exacerbated by racial discrimination, she said. In addition, parole and probation officers may prohibit them from being on MOUD. To help ensure that these individuals have access to primary care, Wang co-founded the Transitions Clinic Network,2 a consortium of 50 community health centers nationwide.
The crux of the Transitions Clinic Program are community health workers, people with histories of incarceration, who help patients navigate the health care and social support systems after release from incarceration, said Wang. For patients with OUD, this may include providing naloxone, clean needles, referrals to safe injection facilities, evidence-based pharmacotherapy, and counseling, as well as addressing the social determinants that augment drug use: lack of food, housing, and income, she said.
As an example of how this approach can help recently incarcerated patients, Wang told the story of a 55-year-old man with a longstanding history of OUD as well as hepatitis C. He had been on methadone but was forced to detox from it when he was incarcerated and vowed never to do that again, said Wang. The Transitions Clinic treated his hepatitis C and the community health worker helped him navigate the bureaucracy to obtain food and housing. He continued to use drugs and when he was rearrested, the clinic made sure his hepatitis C treatment was uninterrupted, said Wang. Released again, he showed up at the clinic with cravings and asked to start MOUD. Since then, he received methadone and then buprenorphine at different points in time, is cured of hepatitis C, and works full time. Wang attributed this success by the medical home that allowed the patient to “engage in care how and when he wants, on his terms, in partnership with the health care provider and a community health worker.”
Rich agreed that any kind of transfer in or out or between correctional facilities is usually the weak point in terms of health care provision and treatment of OUD. One reason, he said, is that people who are incarcerated do not know when they are getting out. “We tell people right up front, if you get out, go to the nearest OTP of this program (i.e., CODAC Behavioral Healthcare in Rhode Island) and they will dose you.” Wang noted, however, that most people do not have the kind of robust OTP infrastructure that is available in Rhode Island. Rich added that there are many ways people can fall out of care, from not having a bus pass to losing their ID. “We need to try and facilitate retention in care after the transition,” he said.
Wang added that while Medicaid restrictions, including the Inmate
___________________
2 To learn more about the Transitions Clinic Network, go to https://transitionsclinic.org (accessed April 12, 2022).
Exclusion Policy,3 contribute to the challenges for people transitioning out of corrections, this is not simply a Medicaid or methadone regulation issue. The point is to get people on methadone and keep them in care so they can thrive. “There are so many criminal justice policies that really constrain the patient’s engagement and retention in care—collateral consequences such as bans on the ability to get housing, food, and employment,” she said. In addition, as has been discussed by other workshop speakers, notably Magdalena Cerdá in Chapter 3, the most impactful way to improve the health of people with OUD would be to minimize their contact with the criminal justice system, said Wang. A host of system-level interventions could help achieve this, she said: minimizing drug testing; eliminating probation and parole revocation for drug use; lowering barriers for treatment with methadone, buprenorphine, and naltrexone; and providing strong social supports and resources for people to thrive in their communities when they return home after incarceration.
Bridging the Transition through Regulatory Action
Wang proposed several regulatory changes that might improve treatment of people following their release from incarceration and potentially help reduce the extremely high incidence of overdose and death among this population group.
- Eliminate or modify the Medicaid inmate exclusion policy, which prohibits the use of federal funds for medical care provided to an inmate of a public institution. The purpose of this policy was to prevent cost shifting to the federal government but is a major reason for the siloing of health care between corrections and community, said Wang. The Medicaid Reentry Act,4 currently under consideration in Congress with significant bipartisan support, would allow Medicaid to pay for health care of eligible incarcerated people starting 30 days prior to their release, said Wang. This care could include methadone and other services, she said. The Act would also provide access to care coordination, enabling a smooth transition for patients, and create federal oversight for correctional health care that receives Medicaid funding, she said (Khatri and
___________________
3 The Inmate Exclusion Policy excludes incarcerated individuals from receiving Medicaid. To learn more about health coverage for incarcerated people, go to https://www.healthcare.gov/incarcerated-people (accessed May 3, 2022).
4 The Medicaid Reentry Act of 2021 is under consideration in the Senate as S 285 and in the House of Representatives as HR 955. To learn more, go to https://www.congress.gov/bill/117th-congress/senate-bill/285/all-info and https://www.congress.gov/bill/117th-congress/house-bill/955 (accessed May 3, 2022).
- Winkelman, 2022). The Medicaid Reentry Act would also help bridge different payment systems such as Medicaid or other insurance, said Wang.
- Create sustainable financing mechanisms for community health workers. Wang said studies have shown that enabling Medicaid payments in correctional systems is a necessary first step, but not sufficient for engaging people with justice involvement into substance use or mental health treatment. Community health workers, especially those who have been incarcerated, are essential for building trust, eliminating stigma, and sustaining engagement of patients, said Wang. With stronger support, they could conduct “in-reach” into jails or prisons prior to release, meet patients, and coordinate release, she said. Data from the Transitions Clinic Network indicate that this in-reach approach substantially improves engagement. Multiple pathways within Medicaid are being explored as sources of sustainable funding for community health workers, said Wang.
- Allow for methadone prescription and dispensation in Federally Qualified Health Centers (FQHCs) and pharmacies. Joudrey and colleagues have analyzed drive times to the nearest OTP as it compares to drive times to FQHCs and pharmacies in five states with the highest overdose rates in the country (Joudrey et al., 2019a, 2020) (see Figure 6-2). In many counties in these five states, drive times to OTPs are greater than 60 minutes, but much less to FQHCs or pharmacies.
A STATE TRIAL COURT PERSPECTIVE
From the perspective of a judge who adjudicates cases of people with OUD charged with criminal offenses on the ground, the Honorable Michael Barrasse, president judge in the Lackawanna County, PA, Court of Common Pleas, the number one obstacle to MOUD in the criminal justice system is stigma. The criminal justice system is slow to change, he said. “It is adversarial and was never meant to be a change agent in dealing with behavioral health,” Judge Barrasse said.
As an example of stigma and misinformation within the justice system, Judge Barrasse pointed to a lawsuit5 recently filed in Pennsylvania, “The United States of America vs. the Unified Judicial System of Pennsylvania,” in which the Justice Department claimed that Pennsylvania has “unlawfully discriminated against individuals with opioid use disorder in its court
___________________
5 For more information regarding the lawsuit, go to https://www.justice.gov/crt/case/united-states-v-unified-judicial-system-pennsylvania (accessed May 9, 2022).
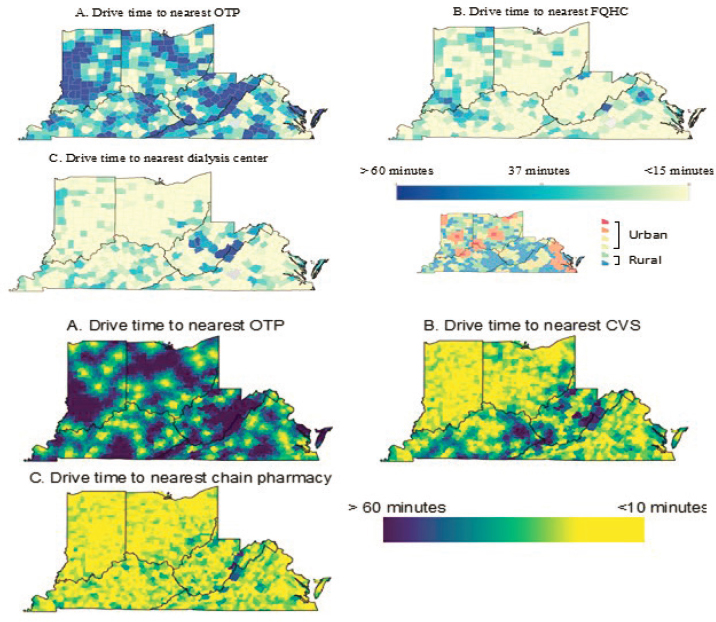
SOURCES: Presented by Emily Wang, March 3, 2022; Joudrey et al., 2019a, 2020.
supervision program, in violation of Title II of the ADA, by prohibiting or otherwise limiting the use of medication prescribed to treat their disability.” The complaint cited an administrative order issued by a judge for the Jefferson County Court of Common Pleas, requiring individuals under court supervision to be completely clean of any opioid-based treatment medication for 30 days or face revocation of their probation. The only exception was for pregnancy.
In issuing the order, the Jefferson County Court claimed, without scientific evidence, that “the vast majority, well in excess of 80 percent” of individuals who are prescribed opioid-based treatments, misuse those drugs regularly and that these treatments do not “appear to help the patients
in any way to become productive members of society.” The order further stated that “among the thousands of individuals who have been on probation while prescribed these drugs,” fewer than 15 have successfully completed treatment.6
Judge Barrasse cited this case because, he said, it provides a clear picture of the problem. “If this is the mentality, and this is what the beliefs are for those people that are running the court systems, no matter how you change regulations, we are going to have a very steep hill to climb to make changes,” he said.
Judge Barrasse added that the criminal justice system is particularly averse to methadone in comparison to buprenorphine and naltrexone. States have more restrictive policies for prescribing and distributing methadone, as well as inadequate pathways to obtain methadone upon release from incarceration, as has been discussed earlier. The vast majority of jails do not have methadone in their medication formularies and many local jails, which far outnumber federal prisons, have no MOUD under consideration in any form, said Judge Barrasse.
The criminal justice system depends on grants for funding, he said. He suggested two requirements for eligibility to receive federal grants:
- Individuals with OUD should be assessed for appropriate MOUD, including methadone, and a reason provided if they are denied. States, agencies, providers, and insurers who fail to follow this rule will be subject to prosecution by the Department of Justice Civil Rights Division for failure to comply with Title II of the Americans with Disabilities Act (ADA).
- Individuals with OUD deemed appropriate for methadone treatment should be provided with the same pathways to treatment as any other MOUD.
CIVIL RIGHTS LITIGATION TO ENABLE METHADONE TREATMENT IN INSTITUTIONS
As alluded to by Judge Barrasse, the ADA specifically requires that people with addictions receive access to treatment, including methadone, in jails, prisons, and other aspects of the criminal legal system such as courts,
___________________
6 For an overview of the evidence base for medications for opioid use disorder, please see the National Academies’ report titled “Medications for Opioid Use Disorder Saves Lives,” available at https://nap.nationalacademies.org/catalog/25310/medications-for-opioid-use-disorder-save-lives (accessed June 12, 2022). The report concluded “FDA-approved medications to treat opioid use disorder are effective and save lives” and “long-term retention on medication for opioid use disorder is associated with improved outcomes.”
parole, and probation, said Rachel Rollins, U.S. attorney for the District of Massachusetts. Yet, while disrupting treatment in the criminal legal system makes it far more likely that a person will commit further criminal offenses or overdose and die, Rollins said that 80 percent of jails and prisons in the United States do not allow methadone, and many court systems and judges have policies that prevent access to methadone. “Probation and parole boards sometimes go so far as to make not accessing methadone a condition of parole or probation,” she said.
The ADA has been in place since 1990, yet Rollins said the first investigation into these unlawful practices was in 2018. Greg Dorchak, assistant U. S. Attorney in Massachusetts, said, “It took nearly 28 years before federal entities really started working in this, but now the tide has turned and they are enforcing it.” He added that the ADA is not the only federal law that explicitly addresses discrimination against individuals with OUD. “So does the Fair Housing Act, section 504 of the Rehabilitation Act,7 amongst other statutes,” he said.
Dorchak said these statutes are designed not only to protect people with OUD, but also to address the barriers to providing treatment within the criminal justice system. He cited four ways that these laws protect the civil rights of people with OUD:
- Jails and prisons that do not maintain all three medications approved for OUD and provide them to individuals already receiving that treatment prior to entering their facility violate federal civil rights statutes, “just as they would have to be able to maintain somebody’s blood pressure medication or insulin [for] diabetes,” he said. He added that there are many ways they can provide these medications, for example, by contacting another entity that is an OTP.
- Parole and probation officers who order people off MOUD as a condition of their parole or probation also may be violating federal civil rights statutes when they are doing this as a blanket policy or practice.
- Skilled nursing facilities that refuse, as a blanket policy, admission to patients solely because they are on methadone or buprenorphine are violating civil rights statutes.
- Sober homes that reject people solely because they are receiving treatment with methadone or buprenorphine are violating federal civil rights statutes.
___________________
7 To learn more about Section 504 of the Rehabilitation Act of 1973, go to https://www.congress.gov/bill/117th-congress/senate-bill/285/all-info (accessed May 3, 2022).
Dorchak acknowledged that while this may sound simple, there are many policy and practical barriers that can slow compliance. It might take a day or a couple of weeks to convince an entity that by law, they have to comply; then it may take as much as a year for the facility to navigate the complex system and actually provide methadone inhouse, he said. Dorchak noted that it can be particularly difficult for smaller, rural jails and prisons, where there may not be any methadone providers nearby or where only a few people who need methadone or buprenorphine go through that facility. For example, he said, there’s no OTP on Martha’s Vineyard in Massachusetts, so someone incarcerated in the county jail there would have to receive guest dosing from an offsite OTP as a more long-term solution is developed. Skilled nursing facilities have the same issues, he said.
“It’s not so simple as flipping a switch,” said Dorchak. “It requires complex decisions and can be a logistical nightmare” for entities to navigate these legal and logistical hurdles. Moreover, he said, most people do not know these practices and barriers are unlawful and that despite the complexity, they will have to comply.
Dorchak described another complication in the laws pertaining to incarcerated people with OUD: There is a carve-out in the ADA that denies protection for people illegally using drugs and an exception to the carve-out, which is that current illegal drug use does not apply to the provision of health care. For example, if a person entering a correctional setting takes buprenorphine but is also using cocaine, the cocaine in their system does not mean they lose their ADA protections for the buprenorphine because that is the provision of health care, which is still protected. “Legal acrobatics,” said Gardner.
Rollins vowed that, as the chief federal law enforcement officer for the District of Massachusetts, she would make ADA enforcement a top priority and work with carceral facilities as well as nursing homes and hospitals to make all treatment options available and accessible. Moreover, she said, state departments of corrections and the federal Bureau of Prisons need to be educated about treatment of OUD and held accountable when they violate the law.
Potential strategies for improving treatment of OUD in and upon release from correctional settings proposed by individual workshop participants are summarized in Box 6-1.
This page intentionally left blank.














