7
Implications and Considerations for Design of Interventions to Improve Infant and Young Child Feeding Behavior in the United States
In this chapter, the committee describes conclusions drawn from the literature identified in the scoping review as well as from additional information on the considerations important in designing infant and young child feeding interventions. At the request of the sponsor, the committee described factors (such as financial or human resources, barriers and facilitators, as well as measurable and standardized indicators) needed to scale interventions and affect infant and young child feeding behavior and the potential of the interventions to reduce inequities and complement existing federal-level programs. The committee then discusses the role of building off existing systems and infrastructure, collecting and applying standardized indicators, reaching underserved populations, and final considerations and opportunities for future actions.
BUILDING FROM EXISTING SYSTEMS AND INFRASTRUCTURE: OPPORTUNITIES AND CHALLENGES
Distinct opportunities and challenges to harnessing existing programs and harmonizing strategies exist across the settings and systems reviewed by the committee, including health care; early care and education (ECE); university cooperative extension (CE); the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); and home visiting programs. The expansion and harmonization of existing supports for complementary feeding in the United States across settings would facilitate families with young children receiving consistent messages
about complementary feeding and responsive feeding. The opportunities and challenges specific to each setting identified by the committee are described in the following sections, followed by those that apply across settings.
Health Care
As noted in Chapter 3, recent national survey data suggest that more than 95 percent of U.S. children have health insurance coverage (Conmy et al., 2023), and as of 2018, more than 90 percent of young children ages 0–4 years old receive a well-child checkup at least annually (CDC, 2020). As of June 2021, 40 million children (nearly 50 percent) in the United States are insured either through Medicaid or the Children’s Health Insurance Program (CHIP), with the vast majority insured through Medicaid (Alker and Brooks, 2022). Furthermore, between 2019–2021, more than 98 percent of pregnant individuals received prenatal care (Martin and Osterman, 2023). The expenditures for the health care ecosystem are greater than the funds available for the other settings included in this report (Gibbs and Malik, 2022).
Among studies in this report examining interventions conducted in the health care system, five of the six U.S. studies and one study from Canada used pediatric office or clinic visits to deliver interventions to influence dietary choices and eating behavior in the first 2 years of life (French et al., 2012; Maguire et al., 2010; Messito et al., 2020; Sanghavi, 2005; Schroeder et al., 2015; Taveras et al., 2011). The other U.S. study (Fiks et al., 2017) recruited from an obstetric clinic and delivered the intervention electronically. Importantly, four of the six U.S. studies enrolled participants in health care settings serving primarily individuals with public insurance or low-income communities (Fiks et al., 2017; French et al., 2012; Messito et al., 2020; Sanghavi, 2005), which are populations of high relevance for public health interventions. The 10 health care setting studies conducted outside the United States and Canada often enrolled participants outside of pediatric clinics (e.g., parent groups, home visits) and largely studied well-educated populations (Cameron et al., 2014; Campbell et al., 2013; Daniels et al., 2012, 2013, 2014, 2015; Fildes et al., 2015; Globus et al., 2019; Hesketh et al., 2020; Magarey et al., 2016; Maguire et al., 2010; Spence et al., 2013, 2014; van Grieken et al., 2017; Vlasblom et al., 2020; Zheng et al., 2022) or did not report socioeconomic status (SES) (de Franchis et al., 2022; Hoffmann et al., 2021; Morandi et al., 2019). Consideration of factors such as the characteristics of the study population, the settings where the participants were enrolled in and completed the study, and the country in which the study was conducted are important in considering the implications of study findings in the health care sector, as health care infrastruc-
ture and social, cultural, and other factors can vary widely by population and geographic location.
As described in Chapter 3, preventive health care for U.S. children ages 0–24 months is determined by Bright Futures guidelines from the American Academy of Pediatrics (AAP, 2023) and by the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit of Medicaid, for children enrolled in Medicaid (Commonwealth Fund, 2005). Counseling on what to feed and how to feed in the first 2 years of life is aligned with the EPSDT requirement to provide anticipatory guidance regarding healthy lifestyles, and data suggest that it is common for pediatricians to provide brief guidance about limiting juice, avoiding sugar-sweetened beverages (SSB) and consuming a variety of fruits and vegetables daily (Boundy et al., 2020; VanFrank et al., 2018). Limited time is typically spent on nutrition counseling during well-child visits, with one small study reporting approximately 2–8 minutes of nutrition counseling per visit (Kaar et al., 2019).
Given the number of components required by EPSDT and Bright Futures and the brevity of most well-child visits, physicians are under significant time constraints to complete all services. In the United States, more than 80 percent of well-child visits last fewer than 20 minutes (Halfon et al., 2011; Konrad et al., 2010). Thus, only a few trials included in this review studied counseling interventions provided primarily by pediatricians, none of which were in the United States (de Franchis et al., 2022; Morandi et al., 2019). Most trials studied interventions provided by other health professionals, such as registered dietitians, social workers, or psychologists, either alone (Cameron et al., 2014; Campbell et al., 2013; Daniels et al., 2012, 2013, 2014, 2015; Dodd et al., 2014, 2018; Fiks et al., 2017; Fildes et al., 2015; Globus et al., 2019; Hesketh et al., 2020; Magarey et al., 2016; Messito et al., 2020; Spence et al., 2013, 2014; Zheng et al., 2022) or in concert with a pediatrician (French et al., 2012; Schroeder et al., 2015; Taveras et al., 2011; van Grieken et al., 2017; Vlasblom et al., 2020). Beneficial effects on what to feed and on how to feed were noted both from interventions delivered by physicians and from interventions delivered by other health care personnel, suggesting that further studies focused on interventions delivered by registered dietitians, psychologists, social workers or other health professionals might facilitate future implementation. However, in the United States, these professionals are not routinely available in most settings providing preventive health care to children nor are they consistently reimbursed by public and private health care payers.
While only one of the included studies (Fiks et al., 2017) reported adherence data, it is known that adherence to well-child visits is low for U.S. children overall and even lower for those with adverse social determinants of health (SDOH), placing them at increased risk for adverse outcomes (Abdus and Selden, 2022). Among the 10 preventive visits rec-
ommended in the first 2 years, the 15-month-old and 18-month-old visits are the most likely to be missed (Wolf et al., 2018).
The inclusion of community health workers and peer counselors in well-child visits can improve the cultural sensitivity of the information communicated and expand linguistic competency (CMS, 2021). These efforts would have the potential to reduce the overwhelming burden of nutrition-related chronic disease on the health care system. Furthermore, augmentation of services by community health workers or peer counselors would greatly enhance the feasibility of population-wide nutrition education in the health care setting (Burt and Sisselman-Borgia, 2020). Taking all these factors into account and because the review identified beneficial effects on feeding from both interventions delivered by physicians and interventions delivered by other health care personnel, the effectiveness and scalability of nutrition counseling interventions could be improved by their delivery by registered dietitians, psychologists, or other health or social support professionals, along with community health workers and other trained paraprofessionals. Limited insurance coverage for nutrition counseling interventions provided by registered dietitians, psychologists, and other health and social support professionals and paraprofessionals presents a barrier to broader access to these services (Aspry et al., 2018). The covered services vary by service, provider type, insurance type, state, and plan. Services covered under Medicaid vary by state, with registered dietitian and community health worker services currently covered only in some states (AND, n.d.; MACPAC, 2022) and, in some cases, only for specific clinical indications (Petrin et al., 2014). Broader insurance coverage for these individuals, such as through Medicaid and CHIP, would greatly facilitate addressing cultural and social factors, including SDOH, during dissemination of nutrition recommendations and help to extend interventions within areas that have significant health care workforce shortages (RHIhub, 2023).
The committee concludes that healthy eating interventions involving the U.S. health care system are of particular interest given the health care system’s potential to reach nearly all young children and their parent/caretaker through prenatal care and regular well-child visits. Expanding state Medicaid and CHIP coverage of counseling interventions by registered dietitians, psychologists, or social workers, augmented by community health workers or peer counselors, could reduce physician burden, and improve intervention adherence, since these professionals and paraprofessionals may be able to operate more flexibly and spend more time with families than physicians.
Early Care and Education
According to the Centers for Disease Control and Prevention (CDC), ECE settings can help young children build a foundation for healthy liv-
ing (CDC, 2023b). Children who attend ECE programs can consume one-half to two-thirds of their daily calorie intake while in care, making ECE programs key settings for the development of healthy habits (Benjamin-Neelon, 2018).
The studies identified within the scoping review in this setting all involved publicly- and privately-funded child care centers; however, many children ages 0 to 24 months receive care from home-based child care providers. Many of these studies focused on repeated exposure to healthy foods and had positive outcomes. In the ECE setting, intervention opportunities for repeated exposure to healthy foods are abundant, as are opportunities to engage and educate parents through center-based care. More research can help to improve understanding of how to best support the involvement of home-based care providers with repeated exposure as well as other complementary feeding interventions.
The Child and Adult Care Food Program (CACFP) is the largest federal nutrition program in the U.S. ECE system and, as noted in Chapter 3, it provides reimbursements for nutritious meals and snacks served to eligible children at participating child care centers and family child care homes (FNS, n.d.). Studies suggest that centers and homes that participate in CACFP provide healthier foods and beverages than those that do not participate in the program (Chriqui et al., 2020; Cotwright et al., 2019; Dave et al., 2022; Erinosho et al., 2018; Gurzo et al., 2020; Kenney et al., 2020, 2023; Ritchie et al., 2012; Zaltz et al., 2020) and that, on average, children’s diets are healthier in ECE settings than at home (i.e., children consumed more energy and less fruits, vegetables, and milk outside of ECE settings) (Robson et al., 2015). However, only one of the five studies the committee reviewed in the ECE setting was conducted in the United States (Clark et al., 2009), and it did not assess CACFP as a stand-alone intervention. Moreover, while participation in CACFP among family child care homes varies across states, it has been declining nationwide (FRAC, 2019; USDA, 2022a). Barriers to CACFP participation by child care providers include perceptions that the nutrition requirements, monitoring and paperwork required are too challenging given the amount of reimbursement and support provided by the program (Andreyeva et al., 2022; Erinosho et al., 2022; Heinz et al., 2022; Jana et al., 2023; Lee et al., 2022).
While CACFP nutrition standards cover the specific types and amounts of food groups provided at up to three meals or snacks per day, many children eat more than three times while in a full day of child care, and the CACFP standards do not apply to foods and beverages served outside of the reimbursed meals and snacks (Korenman et al., 2013). While CACFP also provides guidance and resources on best practices for feeding young children, these additional recommendations are optional to implement and focus primarily on what to feed, rather than how to feed,
young children (Kline, 2016). Furthermore, while one of the ECE studies reviewed by the committee found that repeated exposure of young children to novel vegetables while in child care was effective in helping young children to eat more vegetables (Caton et al., 2013), repeated exposure to novel vegetables is not currently addressed by CACFP resources, for example (FNS, 2023d).
Responsive parenting/feeding guidelines tailored to health care providers, WIC professionals, and ECE providers have been developed for the U.S. context (AAP, 2011; Sigman-Grant et al., 2017). However, the extent to which these guidelines are implemented by ECE providers who are responsible for feeding multiple children simultaneously, is unclear. As also discussed by the 2020 National Academies report Feeding Infants and Children from Birth to 24 Months: Summarizing Existing Guidance, guidance on responsive feeding could be incorporated into future CACFP and state nutrition requirements (NASEM, 2020). CACFP could be strengthened by including resources and requirements related to how to feed in addition to what to feed, providing more guidance on nutrition to ECE providers, and increasing the number of reimbursable meals/snacks offered under the program that are required to meet nutrition guidelines.
As described in Chapter 3, Early Head Start (EHS) is a center or home-based program administered by the U.S. Department of Health and Human Services (HHS) to promote school readiness for children ages 0–3 in families with low-income (ACF, n.d.-a). While there has not been an assessment of the impacts of program participation on dietary outcomes, Head Start sites have been found to provide healthier meals and snacks than most other types of child care (Ritchie et al., 2012). Of note, the one study the committee identified that was conducted as part of CE was conducted in an EHS center (as discussed below) (Horodynski and Stommel, 2005). The National Center on Parent, Family, and Community Engagement has developed evidence-based practices for Early Head Start/Head Start and other ECE settings across the country (CSSP, n.d.). This existing infrastructure could help with translating complementary feeding interventions into ECE settings, since community and parent engagement are essential.
Outside of CACFP, there are no federal nutrition requirements for ECE settings. Some states require all licensed ECE centers or licensed and license-exempt homes to follow CACFP nutrition standards or to have instituted additional nutrition requirements, while others do not (Adams and Hernandez, 2021). However, state policies are typically not comprehensive, and monitoring and enforcement challenges remain (Benjamin et al., 2009; Benjamin-Neelon et al., 2017; Lee et al., 2021; Public Health Law Center, n.d.). States also vary in the amount, if any, of nutrition training that child care providers must complete before becoming licensed. For example, in 2016, California mandated that newly licensed child care
providers complete 1 hour of nutrition training out of 16 total hours of required training (California State Assembly Bill, 2013).
Challenges to scalability and implementation of programs or interventions on what to feed and how to feed exist in ECE settings. HHS’s newly launched National Early Care and Education Workforce Center reported that as of February 2023, the child care sector had lost almost 80,000 jobs (about 7.5 percent of its workforce) since the COVID-19 pandemic (ACF, 2023). It noted that ECE workers are among the lowest-paid workforces in the country, despite the skills and expertise they possess to support the development of young children (ACF, 2023; Coffey, 2022). Family child care providers tend to make even less money than child care center providers; yet home-based care is used at higher rates by Hispanic and Black families, rural families, families with low incomes, and parents with lower educational attainment (HHS, 2019). Of note, none of the studies identified by the committee were conducted in family child care homes. In addition to inadequate staffing, staff compensation, and staff training, a lack of time has been identified as a barrier to implementing health interventions in ECE settings (Asada et al., 2023). The new ECE Workforce Center will support research and technical assistance for states, communities, territories, and Tribal nations to improve both the recruitment and retention of a diverse and qualified workforce across ECE programs (ACF, 2023).
The committee concludes that the existing infrastructure of both CACFP and EHS could be enhanced to improve translation of complementary feeding interventions in ECE settings. Strategies that fund and support ECE providers of all types to adopt CACFP meal patterns, routinize the introduction of new healthy foods into the diets of children under age 2 years, and involve parents in menu planning such that similar healthy foods are included in family meals would be well positioned to impact complementary feeding outcomes. Barriers to ECE providers introducing new foods to children, such as the potential for increased food waste, and therefore cost, should be addressed. CACFP, for example, provides reimbursement for up to two meals and snacks per day, but not necessarily cover the costs of all foods provided. Research is needed to understand ECE barriers to the provision of healthful foods in ECE settings and the impact of interventions in family child care homes and thus to help ensure equity in improving what and how to feed young children.
University Cooperative Extension
Academics and educators within the CE system, along with the public health departments and other community organizations with whom they collaborate, have substantial expertise and experience providing nutrition education and implementing policy, systems, and environmental change efforts through the Supplemental Nutrition Assistance Program–Educa-
tion (SNAP-Ed) and the Expanded Food and Nutrition Education Program (EFNEP) to improve dietary intake and health in populations with low incomes. Moreover, the CE system exists in land-grant universities in every state and territory, including the District of Columbia. Curricula to address infant and toddler nutrition have been developed for these programs (e.g., see Eating Smart, Being Active,1 Families Eating Smart and Moving More,2 and Food Smarts for Adults3). Of note, while both EFNEP and SNAP-Ed collect annual program evaluation data to assess reach and outcomes, this funding cannot be used for research (NIFA, n.d.; UNC, 2022), which may help to explain why the committee identified few published studies involving CE.
CE interventions may be most effective when engaged with the other settings described in this report. This was exemplified by the one CE-led study reviewed by the committee, where group lessons were provided to parents and young children in an ECE setting (Early Head Start) coupled with individualized counseling delivered via home visits. This multicomponent intervention improved parental knowledge and self-efficacy on what and how to feed young children (Horodynski and Stommel, 2005). Moreover, CE academics and educators have the potential to implement many of the interventions categorized by the committee as outside of the prespecified settings. Such interventions included repeated exposure to novel foods, marketing messaging, and more comprehensive interventions for feeding young children. CE engagement outside of the prespecified settings would also allow program delivery curriculums to target diverse audiences and would facilitate the grounding of programs in sound behavior change embedded in socio-ecological conceptual frameworks that take equity into account from early life (Kumanyika, 2019; Skouteris et al., 2021).
The committee concludes that university cooperative extension is ideally positioned to integrate messaging across settings, working with home visiting programs, health care, WIC, and other sectors. Intentional partnerships between cooperative extension academics and educators and settings focused on complementary feeding of children under age 2 years could improve nutrition education and training options for caregivers, early childhood educators, and paraprofessionals such as community health workers, and could have a significant impact on complementary feeding interventions.
___________________
1 See https://eatingsmartbeingactive.colostate.edu/eating-smart-%e2%80%a2-being-active/about/description (accessed June 27, 2023).
2 See https://snapedtoolkit.org/interventions/programs/families-eating-smart-and-moving-more-fesmm (accessed June 27, 2023).
3 See https://snapedtoolkit.org/interventions/programs/food-smarts (accessed June 27, 2023).
WIC
As noted in Chapter 3, infants and young children with household incomes at or below 185 percent of the federal poverty level (FPL) who are at nutrition risk are eligible for WIC (USDA, 2020). The program reaches nearly 82 percent of eligible infants less than 12 months old and nearly 57 percent of eligible toddlers of ages 12–23 months (FNS, 2023b) with supplemental healthy foods and beverages, nutrition education, human milk feeding support, and health/social service referrals (Oliveira and Frazão, 2015).
Although few WIC studies (n=2) met the eligibility criteria for inclusion in this scoping review of promising interventions around complementary feeding, the WIC program, through the provision of healthy first foods paired with human milk feeding support and nutrition education, is itself already a highly impactful complementary feeding intervention for infants and young children under age 2 years. There is extensive published literature on WIC and program impacts, including a recent systematic review of maternal and child health outcomes associated with program participation (Caulfield et al., 2022). WIC participation has been shown to have an impact on numerous outcomes, including improved diet quality of infants and young children (Anderson et al., 2022; Au et al., 2019; Weinfield et al., 2020) and healthier growth trajectories following the 2009 improvements to the WIC food packages (Chaparro et al., 2019a,b, 2020).
WIC already has a broad reach, and its breastfeeding and nutrition education are needed by new caregivers (FNS, 2023a), regardless of income level. Few Americans in any demographic groups have diets that are aligned with the U.S. Dietary Guidelines for Americans (FNS, 2023b). The WIC workforce includes a highly diverse collection of registered dietitians and nutrition professionals and paraprofessionals whose exclusive focus is on optimizing healthy nutritional outcomes for pregnant and postpartum women and children under age 5. A recent study of WIC participants from across the United States found that 95 percent of caregivers report that the education, information, and advice they get from WIC is a reason they continue to participate in the program (Borger et al., 2022). WIC nutrition education is designed to support any family with young children. For those higher-income families who do not qualify for WIC food benefits, the WIC food list can serve as a shopping list of healthy foods appropriate for young children so that all families with young children in the United States can “eat like WIC” (Caulfield et al., 2022). In fact, the labeling of WIC foods in food retailers already occurs in many regions, making healthy WIC foods easy for families to identify and offering a potential marketing strategy for expanding familiarity of WIC foods for all.
Co-location of WIC and health care settings has the potential to benefit both ecosystems by facilitating referrals across settings and improving both WIC participation and preventive care use among the WIC-eligible population. The geographic co-location of WIC and health care services could also help to increase access to registered dietitians, social workers, or psychologists in clinical settings.
The committee concludes that locating WIC services in health care settings would allow for optimal co-location of services and enhanced staffing of registered dietitians, social workers, or psychologists in clinical settings. In addition, given the positive impact and broad reach of WIC to the populations with low incomes across the United States, a promising strategy for consideration is expanding access to WIC’s nutrition education and nutrition support to those of all income levels. Thus, exploring appropriate funding approaches to expand the reach of WIC nutrition education and human milk feeding support to families with incomes above the 185 percent of the federal policy level income threshold has great potential for optimizing complementary feeding for all families in the United States.
Home Visiting
As noted in Chapter 3, U.S. early childhood home visiting programs provide a variety of health-, education-, and social support-oriented services to families with pregnant individuals and/or children ages 0–5 years old (NHVRC, n.d.-b). Evidence-based home visiting programs are available across all 50 U.S. states; Washington, DC; Tribal communities; and U.S. territories (Ingalls et al., 2019; NHVRC, n.d.-a; Rosenstock et al., 2021) and are accessible within about 62 percent of zip codes in the United States (NHVRC, n.d.-a). The services offered, the target audience, the professionals or paraprofessionals delivering the content, and the duration, frequency, and modality (in-person or virtual) of the home visits vary across home visiting models. Not all home visiting programs in the United States currently deliver child nutrition content or have documented positive impact in the child health domain (HHS, 2022, n.d.-a).
Notwithstanding the variability in content of current home visiting models, after reviewing the studies included in this scoping review (see Appendix E), the committee determined that most U.S. home visiting models could incorporate and deliver the infant and young child feeding interventions identified in the review. Ten of the 12 home visiting studies reviewed tested interventions consistent with typical home visiting activities (e.g., one-on-one delivery of education, counseling, skill-building, and goal setting content and resources to caregivers) (Cloutier et al., 2018; Harris et al., 2020; Hernandez et al., 2022; Hohman et al., 2017, 2020; LoRe et al., 2019; Rosenstock et al., 2021; Savage et al., 2016, 2018; Tussing-Humphreys
et al., 2019). Six of these 10 studies were conducted in the United States, with 5 of those including predominantly Black caregivers (Hernandez et al., 2022; LoRe et al., 2019; Tussing-Humphreys et al., 2019) or Black and Hispanic caregivers (Cloutier et al., 2018), or Navajo (Rosenstock et al., 2021). Analogous to the heterogeneity of home visiting programs in the United States, the included studies varied with respect to who delivered the education or counseling and the frequency and duration of the intervention visits in the studies, potentially justifying flexibility during a scale-up process. Two U.S. home visiting studies, Family Spirit Nurture and INSIGHT (Harris et al., 2020; Hohman et al., 2017, 2020; Ingalls et al., 2019; Rosenstock et al., 2021; Savage et al., 2016, 2018), were highlighted in this report as informative studies because of the strength of their design and evaluation and evidence of impact on some feeding outcomes of interest. Three studies emphasized the importance of cultural concordance between the individuals delivering the home visiting content and caregivers (Hernandez et al., 2022; Rosenstock et al., 2021; Tussing-Humphreys et al., 2019) and co-design of the curriculum with the community to ensure cultural sensitivity (Rosenstock et al., 2021).
Home visiting staff could use their professional experience to further adapt the content and delivery based on their program infrastructure and the cultural and linguistic needs of the populations that they serve. Documenting any adaptations will allow for the impact of adapted curricula to be examined through implementation research and/or quality improvement projects. An additional question for further research is whether nutrition content can be effectively delivered virtually in the home visiting setting. The home visiting intervention studies reviewed in this report delivered content in-person, but many U.S. home visiting programs are incorporating virtual service delivery options (NHVRC, n.d.-c). Other studies included in this scoping review demonstrate the potential of virtual approaches.
Similar to the case with interventions in a medical setting, home visitors have many content areas to cover within their curricula. As with the ECE setting, additional efforts are needed to recruit, train, and fairly compensate the home visiting workforce to sustain high-quality home visiting programs that can effectively deliver nutrition content to caregivers (HRSA, n.d.; Sandstrom et al., 2020). Unlike the other settings discussed thus far, the biggest barrier to leveraging home visiting to deliver infant and young child feeding interventions is its limited reach within the U.S. population. Despite nearly $350 million in federal and state investment in the home visiting infrastructure (HFA, n.d.), U.S. family engagement with home visiting is low. Only about 1–3 percent of the approximately 18 million potentially eligible families in the United States are estimated to have contact with a home visiting program (NHVRC, 2019). More intensive
efforts to identify eligible families and recruit and retain them in home visiting programs could help to increase participation (HHS, 2023). A more integrated approach across home visiting, health care, ECE, CE, and WIC settings could be mutually beneficial, as home visitors can provide families with intensive, hands-on, long-term support across many overlapping areas of focus, including responsive parenting and feeding practices, child development, food security, and economic and social stability.
The committee concludes that home visiting programs could feasibly implement many of the interventions identified as efficacious in this scoping review. There is the opportunity for home visiting programs to expand their involvement in the delivery of complementary feeding interventions in the United States To facilitate this, multiple settings (e.g., health care, ECE, CE, WIC) could collaborate to develop, distribute, and provide training on interactive what to feed and how to feed modules for U.S. home visiting programs and to refer families to home visiting programs. Expanded referrals to home visiting programs from multiple settings could increase the proportion of families that engage with home visiting services, improving the services’ reach and potential impact on child health outcomes. In addition, guidance and support for home visitors could enhance the nutrition content of home visiting curricula and help home visitors balance delivery of nutrition content against other priorities in their curricula during home visits.
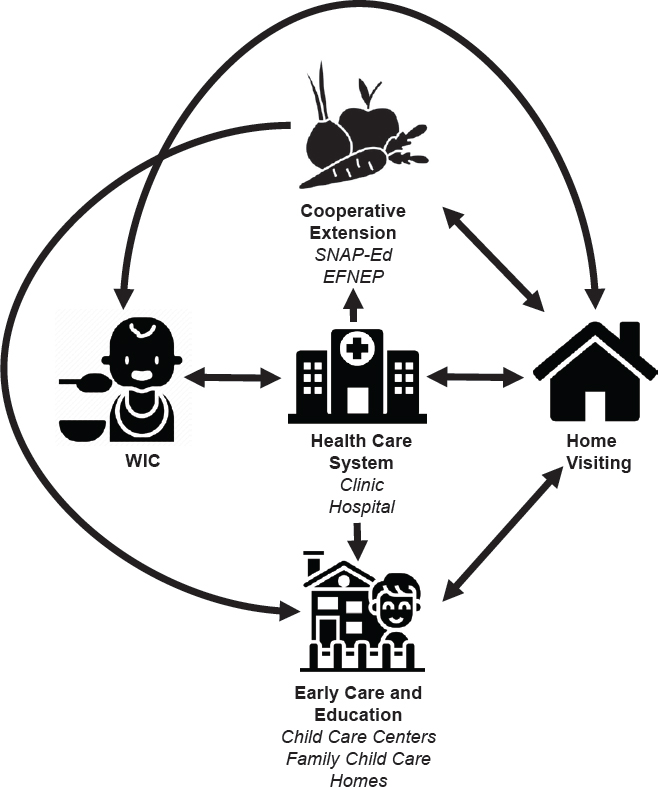
Connections Across Settings and Systems
As noted in Chapter 6, several of the interventions tested by the studies under review here required coordination of program implementation across multiple settings. While there are currently connections across many of the settings and systems (see Figure 7-1) described in this report via referral and other processes, there still is a recognized need to improve these linkages. Collaboration across systems may vary at the community or state level, depending on how much effort has been made to establish and maintain communication across settings and systems. There is the potential for the health care system to be a hub for connections across systems, especially given the near-universal participation in the health care system and the Joint Commission requirements that patients be screened for social determinants of health (e.g., food insecurity) and provided with information about community resources and supports (Joint Commission, 2022). Home visiting is similarly situated to be a hub across these systems, but, as noted above, fewer U.S. families engage with home visiting than with primary health care.
Strengthening collaboration across the settings and systems could help advance progress toward the common goals of promoting responsive parenting, healthy child growth and development, and improving family health outcomes and health equity across the U.S. population. As interventions are translated and scaled up within the United States, it will be important to
consider how to facilitate and improve connections across these settings and systems as part of evaluation and quality improvement efforts. There are clear opportunities to enhance the focus on complementary feeding in each setting through the expansion of funding to support the workforce necessary for such efforts and the integration of nutrition into existing initiatives.
COLLECTION AND APPLICATION OF STANDARDIZED INFANT AND YOUNG CHILD FEEDING OUTCOMES
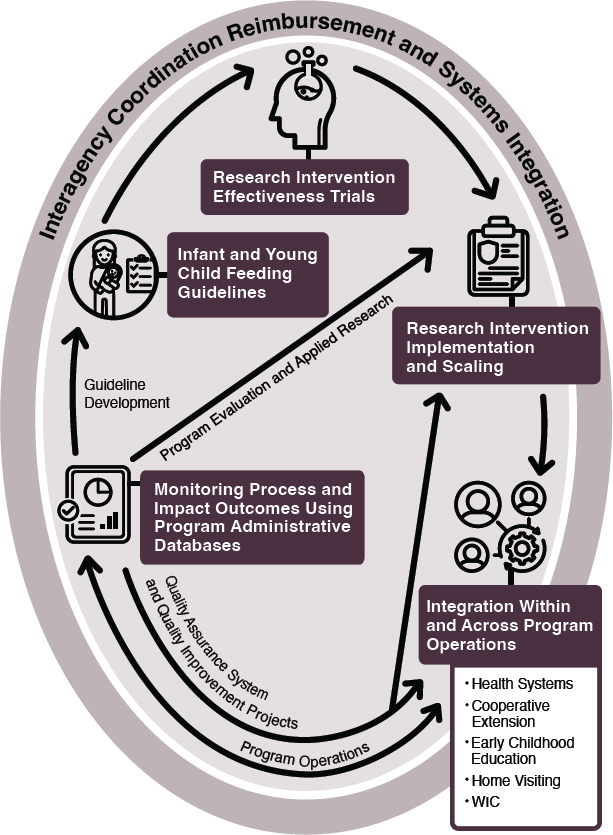
The collection of a harmonized set of process and impact outcomes across the settings described in this report would have several practical implications. The routine collection, analysis, and reporting of a consistent set of process outcomes evaluating service delivery and impact outcomes assessing caregiver implementation of recommendations related to what to feed and how to feed infants and young children could be used to inform day-to-day medical, early childhood educator and program operations; quality assurance systems and quality improvement projects; applied research and program evaluation efforts; and future infant and young
child feeding guidelines (see Figure 7-2). It will be important for all programmatic evaluation to include at least some objective assessment of patient outcomes related to nutrition, such as weight-for-length z-score or body mass index (BMI) z-score.
Both this report and the 2020 National Academies report scoping existing guidelines for feeding infants and young children can be used to guide outcome selection for future interventions (NASEM, 2020). The current report presents evidence that complementary feeding interventions increased child consumption of fruits and vegetables, improved caregiver responsive feeding behaviors, and decreased child consumption of SSBs and snacks high in added sugar or salt. The interventions shown to be beneficial in effectiveness trials should be prioritized. Including outcomes that provide an objective assessment of what-to-feed and how-to-feed recommendations from recognized authorities highlighted in the 2020 National Academies report could also be beneficial (Atkinson et al., 2021; Jimenez et al., 2021; NASEM, 2020; Pérez-Escamilla et al., 2021).
As described in this report (see Chapters 3, 4, and Appendix E), there are many ways to measure complementary feeding impact outcomes,
requiring varying degrees of time and skill both for program personnel to administer and for caregivers to complete. Outcomes related to what to feed can be evaluated using standardized and validated approaches to assessing dietary intake by self-report (e.g., 24-hour dietary recalls, food frequency questionnaires, individual questions about intake of specific foods) or can be evaluated by objective measures such as observed food intake. How to feed, or responsive feeding behaviors (e.g., identification of hunger and satiation cues, nurturing and stimulating verbalizations, not forcing the child to eat, family meals, child repeated exposure to new foods, and caregiver encouragement of self-feeding and self-regulation), can be measured by direct observations (live or via video) and/or caregiver self-report of the child’s feeding behaviors. Although the research studies on complementary feeding interventions reviewed in this report used many different approaches, the predominant approach was caregiver self-report via questionnaires. While it may be feasible for program personnel to collect self-reported information via questionnaire, many research questionnaires may be too long and complex to use as part of standard operations. The identification and broad adoption of short questionnaires that have been evaluated for validity and that can accurately capture intakes of fruits, vegetables, and foods to avoid and assess caregiver responsive feeding behaviors can make monitoring and evaluation efforts across systems more practical and useful. Examples of questionnaires include those developed by Townsend et al. for use in EFNEP/SNAP-Ed interventions (Ontai et al., 2016, 2019; Townsend et al., 2018, 2020). The collection of existing data on objective measures such as child growth may also be possible and could be facilitated by collaborative efforts across settings. Identifying key impact outcomes and validating the tools that can be used to assess them across settings and platforms is a critical next step.
All of the settings already use data systems to track operations and support service delivery to infants and young children and their families. For example, electronic medical records are now used by most health care delivery settings for the purposes of documenting medical care, and WIC and home visiting programs use administrative databases to enable timely enrollment and follow-up of the families served (Lin et al., 2019). However, despite the availability of these data systems, the information captured related to what to feed outcomes is inconsistent across providers, states, and systems (Pérez-Escamilla and Segura-Pérez, 2020). In addition, although all settings use data systems that track health indicators, these systems are generally setting-specific and communication across data systems for children who are served in multiple settings is very limited. Examples of process outcomes that could potentially be informative include tracking waitlists, number and duration of appointments,
whether certain core topics are discussed with caregivers, and whether caregivers are satisfied with the services they receive. Tracking similar process outcomes across settings could help to identify gaps in services and to estimate the total contact time and the infant and young child feeding messaging that families receive from these sources.
To complement an ongoing monitoring and evaluation approach, more intensive collection of complementary feeding outcomes could occur with subsets of participants on a periodic or as needed basis, as has been done to enhance evaluation of child nutrition programs and WIC (FNS, 2022). These more intensive evaluations could also collect comprehensive cost information to allow for the calculation of economic outcomes such as cost-effectiveness and cost-benefit (Adams et al., 2019).
The committee concludes that the development of consensus complementary feeding impact outcomes and measurement tools and integration of these tools into the everyday operations of the settings discussed in the report will allow for systemwide changes to improve complementary feeding and infant and early childhood nutrition in the United States. Improved interagency collaboration within and across the settings described in this report (see Figure 7-2) and across states to capture, share, and report the same key impact outcomes would allow for more effective evaluation and improve U.S. complementary feeding efforts. Improved harmonization of process outcomes documenting service implementation could also strengthen implementation and improvement efforts. Efforts to develop innovative data strategies to facilitate data sharing across settings and minimize administrative burden would be well placed. Monitoring and evaluation efforts that include identification of disparities in access to services, program impact, and outcomes measures by race/ethnicity, parental education level, and SES could be used to drive program refinements that improve health equity.
REACHING UNDERSERVED POPULATIONS
It is a priority of the sponsor and the committee that any complementary feeding intervention or strategy maximize the potential for equitable reach to diverse populations, which is why the sponsor requested the committee to describe ways that interventions could reach underserved populations and improve equity. The previous chapters have detailed studies that provide promising interventions around complementary feeding in early childhood. However, most of these studies enrolled primarily White populations of relatively high income and education, making it difficult to know how these interventions might translate to culturally, racially, ethnically, economically, linguistically, and geographically diverse populations. It should also be noted that several of these studies took place outside the United States, where programs and services available differ from the U.S. context.
Health equity is a priority for the U.S. government, as indicated in Healthy People 2030: “Healthy People 2030 has a strong focus on eliminating health disparities and creating equitable opportunities for people to live healthy lives” (HHS, n.d.-b). Healthy People 2030 further indicates a commitment to “advance health equity, increase health literacy, and address SDOH in communities across the nation” (HHS, n.d.-b). Health equity and SDOH also align strongly with the priorities of the study sponsor, CDC. CDC has taken multiple steps to ensure that efforts to address SDOH are built into their work (CDC, 2022), including the development of six pillars that support the integration of equity considerations and provide a useful framework for aligning the studies reviewed in previous chapters to maximize equitable outcomes for all children (see Box 7-1).
A crucial step in future work to implement complementary feeding interventions will be to ensure that the strategies that have been shown to work effectively in more highly resourced populations can be implemented in less-resourced ones. This will likely require additional
resources and the appropriate input and vetting from families with the fewest resources, and who are the most marginalized and underrepresented in society. Families and communities with few resources are often overlooked but are most able to devise effective solutions that meet their needs. Strategically embedding CDC’s pillars of partnership and collaboration and community engagement into interventions from the very early stages of planning and translation of research interventions into practice will help to maximize the chance that the interventions will be successful with historically and currently underrepresented populations. Aligning with all six CDC SDOH pillars will ensure interventions address SDOH.
At the center of the work on complementary feeding, and also a focus of the previous chapters, is the evidence surrounding the important behaviors related to what to feed and how to feed. Interventions that fail to consider the diverse social determinants that influence what and how to feed—ranging from diversity in basic access to healthy, affordable food options to cultural norms and practices around feeding—are unlikely to be successful at achieving optimal outcomes across diverse populations. It is unlikely that a one-size-fits-all model of intervention will equitably reach or impact families and communities across the United States, given the rich diversity of cultural and linguistic backgrounds and daily lived experiences in the U.S. population. Similarly, not all families or communities may require the same intensity of intervention, nor will they necessarily respond to the same messaging. However, from the challenge of identifying uniquely impactful interventions to meet myriad needs comes the opportunity to identify strategies that hold promise in their ability to adhere to an evidence base while also being able to adapt to the input of the target communities. Many elements of the interventions noted in the earlier chapters of this report hold that promise.
As an example, the INfant Feeding, Activity, and Nutrition Trial (INFANT) study is an early life family-centered behavioral intervention designed to improve dietary, physical activity, and screen time outcomes among children and caregivers with the ultimate goal of reducing childhood obesity incidence in the state of Victoria in Australia. INFANT targeted behaviors in four domains for children (infant feeding, food provision, dietary intake, physical activity, and sedentary behaviors) and four domains for parents (dietary intake, physical activity, sedentary behaviors, and overall well-being). The original trial targeted first-time parents and used behavioral change techniques, including goal setting, problem solving, and self-monitoring (Campbell et al., 2008). As the INFANT trial is being scaled-up for broader implementation across the region, modifications are being made to reflect the need for a population-based intervention to flexibly adapt while also maintaining its evidence base (Marshall et al., 2022). By incorporating feedback from stakeholders, the scaled-up
version expands its target population, adapts the number and duration of sessions, and broadens the type of personnel delivering the intervention and the modalities in which the intervention is delivered (e.g., online modalities in addition to face to face).
In addition, other studies offer the opportunity to consider how aspects of interventions can be adapted to meet the needs of more diverse populations. The COVID-19 pandemic brought about rapid changes in remote and digital service delivery methods. While their long-term impacts have not been examined, the proliferation of digital strategies creates new and engaging ways to increase reach to and engagement of underserved populations (MacMillan Uribe et al., 2023). As noted by MacMillan Uribe et al. (2023), “while a ‘digital divide’ exists with some [digital technologies], like desktop/laptop ownership and home broadband internet access, most people own smart phones (≥ 76 percent) or use social media (≥ 65 percent), regardless of income, race and ethnicity, or age” (p. 391). Thus, the digital technologies noted throughout this report (such as texting within the WIC SMS study) hold great promise for both customizability and reach to less-resourced families, especially in concert with ongoing efforts to subsidize internet access for families with low-income and improve internet infrastructure in rural U.S. and Tribal communities (FCC, 2023; White House, 2022). Studies both before and during the pandemic, for example, suggest that remote options for receiving nutrition counseling and information are both feasible and acceptable to WIC populations (Anderson and Whaley, 2023; Au et al., 2016, 2022; Bensley et al., 2011; Ritchie et al., 2021).
The committee concludes that the successful implementation of complementary feeding interventions in underserved populations will require partnership, collaboration, and community engagement with the target populations throughout the research, implementation, and scale-up processes. The most effective interventions will adapt to the needs and input of the target communities, while adhering to the evidence base.
ADDITIONAL CONSIDERATIONS
Barriers to the effectiveness of any nutrition intervention in the United States include food insecurity, unhealthy food marketing, and poor nutrition literacy. These three issues are cross-cutting and apply to interventions implemented in all settings considered in this report.
Food Insecurity
Despite the positive impacts of WIC and SNAP programs, food insecurity remains common in the United States, with 12.5 percent of families with children being food insecure (USDA, 2023). Food insecurity is defined
by the U.S. Department of Agriculture (USDA) as access to adequate food needed for active, healthy living that is limited by a lack of money or other resources (USDA, 2022b). Food insecurity during childhood can have a lifelong influence on dietary intake patterns, leading to increased intake of energy dense foods, lower consumption of fruits and vegetables, and other unhealthy dietary behaviors (Landry et al., 2019). Nutrition education interventions may not be as effective when families do not have access to or cannot afford healthy foods. Food insecurity has been associated with caregiver reluctance to repeatedly offer novel foods that may not be eaten (Daniel, 2016) but findings are mixed on the association between food insecurity and controlling or pressured caregiver feeding practices (Arlinghaus and Laska, 2021). An intervention that decreases food insecurity, as done with WIC, might be an effective way to improve complementary feeding.
The committee concludes that for the anticipatory guidance, nutrition education, and brief targeted feeding interventions reviewed in this report to be most effective, they should also assess and address food insecurity.
Food Marketing
Food marketing is ubiquitous in the United States. In 2015, $77 million was spent on advertising for foods that specifically targeted infants and toddlers (Rudd Center, 2016). These advertised foods were generally less healthy than the variety of fruits, vegetables, and iron-containing foods that are recommended (Harris and Pomeranz, 2020; Harris et al., 2017). For example, in 2015, companies spent $17 million to promote toddler milks in the United States (Rudd Center, 2016). These products contain added sugars and are more expensive than the plain whole milk recommended for children ages 1 to 2 years old (Choi et al., 2020; Harris et al., 2017). Families with young children are besieged by food advertising virtually everywhere they go, through a variety of media including television, print, and social media. In the United States, food advertising is regulated by the Federal Trade Commission in conjunction with the U.S. Food and Drug Administration. A variety of approaches toward regulating food advertising have been attempted with varying success (Taillie et al., 2019); none have been studied in a way that met inclusion criteria for this review. The one marketing message study reviewed by the committee showed that exposure to a brief counter-marketing video can change parent attitudes about beverages that are appropriate for young children (Harris et al., 2022), and the communication strategy study demonstrated that mass media communications can change parents’ knowledge and food purchases (Verrall et al., 2006).
The committee concludes that counter-marketing and mass media communications strategies directed at families with young children is a promising intervention deserving of further study, with evaluation over longer time periods.
Nutrition Literacy
The goal of complementary feeding is to gradually introduce solid foods so that by the time children are 2 years old they are eating similarly to the rest of the family, as families eat together and children model the behaviors of others. An inherent challenge, however, is that most Americans do not eat a healthy diet (e.g., as recommended by the 2020–2025 Dietary Guidelines for Americans [USDA and HHS, 2020]).
Nutrition (or food) literacy includes attributes such as nutrition knowledge, food purchasing and preparation skills, and self-efficacy (Azevedo Perry et al., 2017). Nutrition literacy for caregivers of young children also includes knowledge of developmentally appropriate nutrition needs and what and how to feed young children 6–24 months old. It also should include skills to identify credible sources of information to combat the misinformation readily available online. Nutrition literacy is important as one determinant of diet quality (Gibbs et al., 2016; Taylor et al., 2019). In the United States, few parents and others who care for young children receive nutrition education regarding their own eating habits outside of the WIC setting. Notably, while the United States has a school meals program that includes nutrition standards to ensure healthy meals and some nutrition education occurs in U.S. schools (NCES, n.d.), the United States is among a minority of nations that does not include nutrition education as a required part of the K–12 school curriculum (UNESCO, 2023). According to the CDC, children attending U.S. schools receive less than 8 hours of formal health and nutrition education per year (CDC, 2023a). WIC, SNAP-Ed, and EFNEP help households with low incomes eat healthier, but not all parents have access to these programs. While national expenditures on SNAP-Ed and EFNEP in fiscal year 2017 reached, respectively, $404 million and $51 million (GAO, 2019), this funding is small compared with the nearly $2.54 billion spent in advertising by the food industry, most of which promotes unhealthy food (Finlay et al., 2022; Potvin Kent et al., 2022; Rudd Center, n.d.).
It is important to consider the nutrition literacy of caregivers of young children in designing any intervention to improve nutrition (Gibbs, 2016). However, few of the interventions reviewed include a focus on the dietary habits of the family. Professional training on nutrition is also limited. ECE professionals may receive nutrition education prior to becoming licensed, but the amount and content of this education is limited and not standardized (ACF, n.d.-b). Universities and colleges do not require nutrition as part of the general education curriculum. While some health care providers receive training on nutrition, it is also variable and not required by many schools or programs (Crowley et al., 2019).
The committee concludes that considering the nutrition literacy of caregivers and professionals in the design of interventions aimed at improving child
feeding practices behaviors is necessary. Adapting the content accordingly will allow for interventions to better reach a wide range of caregivers and families. Nutrition literacy for caregivers of young children includes understanding the developmentally appropriate nutrition needs of and what and how to feed young children 6–24 months old, as well as skills to identify credible sources to combat misinformation. In addition, interventions that address the age-appropriate feeding practices and eating behaviors of young children and the dietary habits of the whole family may be best positioned to sustainably improve dietary intakes of young children.
GOING FORWARD: FINAL CONSIDERATIONS
The existing literature contains many studies that have examined interventions aimed at improving nutrition for infants and young children. Based on this scoping review, the committee did not identify any one specific intervention that could be immediately scaled in the United States. However, the committee can offer guidance on what such successful interventions might look like. Many interventions were conducted in controlled clinical or research settings without their effectiveness and potential for translation and scalability being assessed in practical, real-life settings, with the INFANT study being a notable exception. In addition, nearly two-thirds of the publications were from outside the United States, with interventions occurring in different cultural, legal, and political contexts. Collectively, the evidence-based interventions identified were based on messaging that was highly consistent with the “what to feed” aspects of the 2020–2025 Dietary Guidelines for Americans (USDA and HHS, 2020) recommendations focusing on children under 2 years of age and the “how to feed” aspects of the responsive feeding framework (Pérez-Escamilla et al., 2021).
INFANT was the most scaled-up program identified. Its development and testing provide a strong model for carefully orchestrating the process of translating findings from a randomized controlled trial (RCT) to widespread implementation of an intervention in the community. Although the applicability of the INFANT intervention to the U.S. population is unknown, the scale-up process utilized for the INFANT model is highly applicable in the United States. The INFANT intervention was family-centered and relied on group sessions with parents, taking advantage of existing Australian programs and contact opportunities through the health care system. The INFANT intervention was delivered by diverse health professionals including dietitians, nurses, and parenting skills instructors. In the United States, it is possible to envision an INFANT-like program delivered through WIC, CE (SNAP-Ed or EFNEP), child care centers (including EHS), or well-child visits, and it could be
particularly effective if these systems were coordinated with each other through a multiagency coordinating body including agencies such as CDC, USDA, HHS, and the Administration for Children and Families. Such coordination will be especially important in designing an intervention that ensures generalizability to the U.S. population and that is centered in equity.
Such an integrated, coordinated approach could be facilitated by the new White House National Strategy on Hunger, Nutrition, and Health which calls for strengthening the links between food assistance programs and health care and education systems starting in early life (EOP, 2022). An example of the implementation of this strategy is the now strong national- and state-level support for the co-design and scale-up of produce-prescription programs for patients across the life-course (Mozaffarian et al., 2022). These programs are already being tested in partnership with WIC and SNAP-Ed programs and can include innovative maternal, infant, and young child feeding evidence-based curricula focusing on what and how to feed infants and young children (Harris et al., 2020; Hohman et al., 2017, 2020; Savage et al., 2016, 2018), taking cultural preferences and the SDOHs into account (Ingalls et al., 2019; Rosenstock et al., 2021).
The Family Spirit Nurture home visiting intervention also holds promise as an intervention that could be readily scaled in the United States, pending the findings from the second RCT. There is a strong existing home visiting infrastructure in place through the Johns Hopkins Bloomberg School of Public Health, with affiliates trained to implement the Family Spirit home visiting model in 130 U.S. communities (primarily rural and reservation-based) across 21 U.S. states (Ingalls et al., 2019; JHU, n.d.; Rosenstock et al., 2021). Since Family Spirit is delivered in primarily rural and reservation-based communities that have experienced historical and present-day marginalization, the scaling of this community-co-designed, culturally sensitive infant and young child feeding intervention could have important health equity implications. The INSIGHT home visiting intervention also demonstrated efficacy with respect to many nutrition outcomes and is potentially scalable, although its delivery by nurses is not consistent with many existing home visiting models in the United States. Nevertheless, adaptation of its content for delivery by paraprofessionals and other home visitors would be possible and could potentially be done in a way that centered on equity.
There were also other interventions conducted across settings that had promising components that could be part of multicomponent “packages” of interventions delivered across systems to address what and how to feed infants and young children. For example, there were interventions that highlighted the potential to reach families using social media (e.g.,
Facebook groups) (Fiks et al., 2017), via interactive mobile applications (Campbell et al., 2008), and with two-way text messaging (Gibby et al., 2019; Macchi et al., 2022; Palacios et al., 2018). To achieve health equity, these interventions would need to be pursued in tandem with ongoing efforts to improve internet access and infrastructure for marginalized populations in the United States.
In chapter 6, the committee describes factors for consideration in scaling infant and young child feeding interventions. As the INFANT program has shown, translational trials and implementation monitoring and evaluation are crucial when going to scale. Following a similar approach in the United States would help to ensure that effective programs can be properly adapted to diverse contexts, while maintaining their effectiveness and promoting health equity based on implementation frameworks that take equity into account (Brownson et al., 2021). It will be important for the United States to add additional, harmonized infant and young child feeding indicators that address dietary intake and responsive feeding practices to data collection systems across settings and to its broader infant and young child feeding monitoring systems (Pérez-Escamilla et al., 2021). Currently, such infant and young child feeding monitoring systems focus mainly on monitoring human milk feeding and commercial infant formula indicators (Vaz et al., 2021).
All families with infants and young children can benefit from access to credible information on best feeding practices. Because healthy eating behaviors are established early in the life course, widespread implementation of best practices for feeding infants and young children can establish an important strong foundation for U.S. population health in the long term, in concert with continued efforts later in the life course. The implementation and sustainment of large-scale, effective, population-wide infant and young child feeding programs across the settings identified in this report would help make progress toward this goal. For this reason, intergovernmental agency collaboration on workforce development, internet and technology infrastructure, evaluation and program improvement, and efforts to increase funding levels and options and reimbursement for this work is essential. It is also important for both public and private health insurance actors to be engaged with this effort, as was called for in the White House National Strategy on Hunger, Nutrition, and Health (EOP, 2022).
The committee concludes that although a specific, scalable intervention model was not identified, there were several interventions with promising elements that could be part of a multicomponent constellation of interventions delivered across settings and systems to address what and how to feed infants and young children. The settings and corresponding systems that were examined—health care, ECE,
CE, home visiting, and WIC—are critically important to leverage. No one system is currently equipped or adequately funded to reach all children up to age 2 years in the United States, but the existing complementary feeding supports available for some families in the United States could be expanded and harmonized such that all families with young children receive consistent messages about complementary feeding and responsive feeding across multiple settings. The effective scaling of any intervention requires consideration of implementation science and equity principles. Securing permanent funding for program implementation; supporting personnel recruitment, training, and retention; and considering integration of virtual options across the settings highlighted in this report will be key for sustainability.
SUMMARY
This chapter provided the committee’s conclusions, based on its scoping review, related to design of interventions to improve infant and young child feeding behavior in the United States. It addressed opportunities and challenges to build from existing ecosystems in each of the systems reviewed by the committee and connections across settings and systems. It discussed the collection and application of standardized infant and young child feeding outcomes and ways to reach underserved populations with complementary feeding interventions. Additional considerations, including food insecurity, food marketing, and nutrition literacy were also addressed.
Overall, this report addresses the committee’s Statement of Task (see Chapter 1, Box 1-1) by providing the results of its scoping review and assessment of the peer-reviewed published literature and other publicly available information on interventions aimed at improving infant and young child feeding behaviors. As dictated by the sponsor, the review was limited to developed countries or U.S.-specific contexts and interventions occurring in health care, ECE, and CE settings and those that complement existing federal-level programs. This report summarizes the available evidence and provides information on possible interventions that could be scaled up or implemented at a community or state level. Using the committee’s learnings to develop, implement, and scale complementary feeding programs for infants and children should improve current and future infant and young child nutrition and health outcomes for years to come.
REFERENCES
AAP (American Academy of Pediatrics). 2011. Caring for our children: National health and safety performance standards: Guidelines for early care and education programs. 3rd edition. Washington, DC: American Public Health Association.
AAP. 2023. American Academy of Pediatrics’ schedule of well-child care visits. AAP, Bright Futures. https://www.aap.org/en/practice-management/bright-futures/bright-futures-family-centered-care/well-child-visits-parent-and-patient-education (accessed August 21, 2023).
Abdus, S., and T. M. Selden. 2022. Well-child visit adherence. JAMA Pediatrics 176(11):1143–1145.
ACF (Administration for Children and Families). 2023. HHS launches the first national early care and education workforce center. https://www.acf.hhs.gov/media/press/2023/hhs-launches-first-national-early-care-and-education-workforce-center (accessed July 21, 2023).
ACF. n.d.-a. Head Start and Early Head Start. https://childcare.gov/consumer-education/head-start-and-early-head-start (accessed August 22, 2023).
ACF. n.d.-b. Staff qualifications and required training. https://childcare.gov/consumer-education/staff-qualifications-and-required-trainings (accessed August 23, 2023).
Adams, G., and F. Hernandez. 2021. The child and adult care food program and home-based child care providers: Expanding participation. Washington, DC: Urban Institute.
Adams, K. P., J. A. Lee, E Piltch, and E. Y. Jimenez. 2019. An introduction to economic analysis of food security and nutrition interventions. Journal of the Academy of Nutrition and Dietetics 119(5):856–864.
Alker, J., and T. Brooks. 2022. Millions of children may lose Medicaid: What can be done to help prevent them from becoming uninsured? Washington, DC: Georgetown University Health Policy Institute, Center for Children and Families. https://ccf.georgetown.edu/2022/02/17/millions-of-children-may-lose-medicaid-what-can-be-done-to-help-prevent-them-from-becoming-uninsured (accessed August 6, 2023).
AND (Academy of Nutrition and Dietitics). n.d. Medicaid. https://www.eatrightpro.org/career/payment/medicaid (accessed July 21, 2023).
Anderson, C. E., and S. E. Whaley. 2023. Use of interactive texting is associated with higher odds of continued WIC participation during the COVID-19 pandemic. Journal of the Academy of Nutrition and Dietetics, May 12. Online ahead of print. https://doi.org/10.1016/j.jand.2023.05.008.
Anderson, C. E., C. E. Martinez, L. D. Ritchie, C. Paolicelli, A. Reat, C. Borger, and S. E. Whaley. 2022. Longer Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) participation duration is associated with higher diet quality at age 5 years. Journal of Nutrition 152(8):1974–1982.
Andreyeva, T., X. Sun, M. Cannon, and E. L. Kenney. 2022. The Child and Adult Care Food Program: Barriers to participation and financial implications of underuse. Journal of Nutrition Education and Behavior 54(4):327–334.
Arlinghaus, K. R., and M. N Laska. 2021. Parent feeding practices in the context of food insecurity. International Journal of Environmental Research and Public Health 18(2):366.
Asada, Y., S. Lin, L. Siegel, and A. Kong. 2023. Facilitators and barriers to implementation and sustainability of nutrition and physical activity interventions in early childcare settings: A systematic review. Prevention Science 24(1):64–83.
Aspry, K. E., L. Van Horn, J. A. S. Carson, J. Wylie-Rosett, R. F. Kushner, A. H. Lichtenstein, S. Devries, A. M. Freeman, A. Crawford, and P. Kris-Etherton. 2018. Medical nutrition education, training, and competencies to advance guideline-based diet counseling by physicians: A science advisory from the American Heart Association. Circulation 137(23):e821–e841.
Atkinson, S. A., E. Y. Jimenez, and R. Pérez-Escamilla. 2021. Evidence gaps and research needs in current guidance on feeding children from birth to 24 months. Applied Physiology, Nutrition, and Metabolism 46(3):294–297.
Au, L. E., S. Whaley, K. Gurzo, M. Meza, and L. D. Ritchie. 2016. If you build it they will come: Satisfaction of WIC participants with online and traditional in-person nutrition education. Journal of Nutrition Education and Behavior 48(5):336–342.
Au, L. E., C. Paolicelli, K. Gurzo, L. D. Ritchie, N. S. Weinfield, K. R. Plank, and S. E. Whaley. 2019. Contribution of WIC-eligible foods to the overall diet of 13- and 24-month-old toddlers in the WIC Infant and Toddler Feeding Practices Study-2. Journal of the Academy of Nutrition and Dietetics 119(3):435–448.
Au, L. E., S. E. Whaley, C. A. Hecht, M. M. Tsai, C. E. Anderson, A. M. Chaney, N. Vital, C. E. Martinez, and L. D. Ritchie. 2022. A qualitative examination of California WCI participants’ and local agency directors’ experiences during the coronavirus disease 2019 pandemic. Journal of the Academy of Nutrition and Dietetics 122(12):2218–2227.
Azevedo Perry, E., H. Thomas, H. R. Samra, S. Edmonstone, L. Davidson, A. Faulkner, L. Petermann, E. Manafò, and S. I. Kirkpatrick. 2017. Identifying attributes of food literacy: A scoping review. Public Health Nutrition 20(13):2406–2415.
Benjamin, S. E., E. M. Taveras, A. L. Cradock, E. M. Walker, M. M. Slining, and M. W. Gillman. 2009. State and regional variation in regulations related to feeding infants in child care. Pediatrics 124(1):e104–e111.
Benjamin-Neelon, S. E. 2018. Position of the Academy of Nutrition and Dietetics: Benchmarks for nutrition in child care. Journal of the Academy of Nutrition and Dietetics 118(7):1291–1300.
Benjamin-Neelon, S. E., S. Gonzalez-Nahm, E. Grossman, M. L. Davis, B. Neelon, A. Ayers Looby, and N. Frost. 2017. State variations in infant feeding regulations for child care. Pediatrics 140(6):e20172076.
Bensley, R. J., J. V. Anderson, J. J. Brusk, N. Mercer, and J. Rivas. 2011. Impact of internet vs traditional Special Supplemental Nutrition Program for Women, Infants, and Children nutrition education on fruit and vegetable intake. Journal of the American Dietetic Association 111(5):749–755.
Borger, C., T. Zimmerman, J. DeMatteis, B. Gollapudi, S. Whaley, L. Ritchie, L. Au, and L. May. 2022. WIC Infant and Toddler Feeding Practices Study-2: Fifth year report. Alexandria, VA: USDA-FNS.
Boundy, E. O., A. Fisher Boyd, H. C. Hamner, B. Belay, J. L. Liebhart, J. Lindros, S. Hassink, and M. P. Frintner. 2020. U.S. pediatrician practices on early nutrition, feeding, and growth. Journal of Nutrition Education and Behavior 52(1):31–38.
Brownson, R. C., S. K. Kumanyika, M. W. Kreuter, and D. Haire-Joshu. 2021. Implementation science should give higher priority to health equity. Implementation Science 16(1):28.
Burt, K. G., and A. Sisselman-Borgia. 2020. How community health workers can improve workforce diversity and dietary outcomes. Nutrition Today 55(5):254–259.
California State Assembly Bill No. 290. 2013. Child day care: Childhood nutrition training. https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201320140AB290 (accessed August 21, 2023).
Cameron, A. J., K. Ball, K. D. Hesketh, S. A. McNaughton, J. Salmon, D. A. Crawford, S. Lioret, and K. J. Campbell. 2014. Variation in outcomes of the Melbourne Infant Feeding, Activity, and Nutrition trial (InFANT) program according to maternal education and age. Preventive Medicine 58:58–63.
Campbell, K., K. Hesketh, D. Crawford, J. Salmon, K. Ball, and Z. McCallum. 2008. The Infant Feeding Activity and Nutrition Trial (INFANT): An early intervention to prevent childhood obesity: Cluster-randomised controlled trial. BMC Public Health 8:103.
Campbell, K. J., S. Lioret, S. A. McNaughton, D. A. Crawford, J. Salmon, K. Ball, Z. McCallum, B. E. Gerner, A. C. Spence, A. J. Cameron, J. A. Hnatiuk, O. C. Ukoumunne, L. Gold, G. Abbott, and K. D. Hesketh. 2013. A parent-focused intervention to reduce infant obesity risk behaviors: A randomized trial. Pediatrics 131(4):652–660.
Caton, S. J., S. M. Ahern, E. Remy, S. Nicklaus, P. Blundell, and M. M. Hetherington. 2013. Repetition Counts: Repeated exposure increases intake of a novel vegetable in UK pre-school children compared to flavour–flavour and flavour–nutrient learning. British Journal of Nutrition 109(1):2089–2097.
Caulfield, L. E., W. L. Bennett, S. M. Gross, K. M. Hurley, S. M. Ogunwole, M. Venkataramani, J. L. Lerman, A. Zhang, R. Sharma, and E. B. Bass. 2022. Maternal and child outcomes associated with the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Rockville, MD: Agency for Healthcare Research and Quality.
CDC (Centers for Disease Control and Prevention). 2020. Quickstats: Percentage of children aged <18 years who received a well-child checkup in the past 12 months, by age group and year—National Health Interview Survey, United States, 2008 and 2018. https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6908a5-h.pdf (accessed July 21, 2023).
CDC. 2022. What is CDC doing to address social determinants of health? https://www.cdc.gov/about/sdoh/cdc-doing-sdoh.html (accessed June 27, 2023).
CDC. 2023a. Healthy eating learning opportunities and nutrition education. https://www.cdc.gov/healthyschools/nutrition/school_nutrition_education.html (accessed July 21, 2023).
CDC. 2023b. Nutrition and physical activity. https://www.cdc.gov/earlycare/nutrition/index.html (accessed July 21, 2023).
Chaparro, M. P., C. E. Anderson, C. M. Crespi, S. E. Whaley, and M. C. Wang. 2019a. The effect of the 2009 WIC food package change on childhood obesity varies by gender and initial weight status in Los Angeles County. Pediatric Obesity 14(9):e12526.
Chaparro, M. P., C. M. Crespi, C. E. Anderson, M. C. Wang, and S. E. Whaley. 2019b. The 2009 Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food package change and children’s growth trajectories and obesity in Los Angeles County. American Journal of Clinical Nutrition 109(5):1414–1421.
Chaparro, M. P., C. E. Anderson, C. M. Crespi, M. C. Wang, and S. E. Whaley. 2020. The new child food package is associated with reduced obesity risk among formula fed infants participating in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) in Los Angeles County, California, 2003–2016. International Journal of Behavioral Nutrition and Physical Activity 17(1):18.
Choi, Y. Y., A. Ludwig, and J. L. Harris. 2020. U.S. toddler milk sales and associations with marketing practices. Public Health Nutrition 23(6):1127–1135.
Chriqui, J. F., J. Leider, R. M. Schermbeck, A. Sanghera, and O. Pugach. 2020. Changes in Child and Adult Care Food Program (CACFP) practices at participating childcare and education centers in the United States following updated national standards, 2017–2019. Nutrients 12(9):2818.
Clark, A., J. Anderson, E. Adams, S. Baker, and K. Barrett. 2009. Assessing an infant feeding web site as a nutrition education tool for child care providers. Journal of Nutrition Education and Behavior 41(1):41–46.
Cloutier, M. M., J. F. Wiley, C. L. Kuo, T. Cornelius, Z. Wang, and A. A. Gorin. 2018. Outcomes of an early childhood obesity prevention program in a low-income community: A pilot, randomized trial. Pediatric Obesity 13(1):677–685.
CMS (Centers for Medicare & Medicaid Services). 2021. On the front lines of health equity: Community health workers. Centers for Medicare & Medicaid Services. https://www.cms.gov/files/document/community-health-worker.pdf (accessed July 21, 2023).
Coffey, M. 2022. Still underpaid and unequal: Early childhood educators face low pay and a worsening wage gap. Center for American Progress. https://www.americanprogress.org/article/still-underpaid-and-unequal (accessed August 6, 2023).
Commonwealth Fund. 2005. EPSDT: An overview. https://www.commonwealthfund.org/publications/other-publication/2005/sep/epsdt-overview (accessed July 3, 2023).
Conmy, A. B., C. Peters, N. De Lew, and B. D. Sommers. 2023. Children’s health coverage trends: Gains in 2020–2022 reverse previous coverage losses. Issue brief No. HP-2023-07. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services. https://aspe.hhs.gov/sites/default/files/documents/77d7cc41648a371e0b5128f0dec2470e/aspe-childrens-health-coverage.pdf (accessed August 6, 2023).
Cotwright, C. J., H. Bradley, N. Celestin, S. Drake, K. Love, and L. Birch. 2019. Beverage policy implementation by Child and Adult Care Food Program participation and program type: A statewide examination in Georgia. Childhood Obesity 15(3):185–193.
Crowley, J., L. Ball, and G. J. Hiddink. 2019. Nutrition in medical education: A systematic review. The Lancet Planetary Health 3(9):e379–e389.
CSSP (Center for the Study of Social Policy). n.d. National Center on Parent, Family, and Community Engagement: Family engagement is essential to high quality early care and education. https://cssp.org/our-work/project/national-center-for-parents-family-and-community-engagement/#outcomes (accessed July 17, 2023).
Daniel, C. 2016. Economic constraints on taste formation and the true cost of healthy eating. Social Science & Medicine 148:34–41. https://doi.org/10.1016/j.socscimed.2015.11.025.
Daniels, L. A., K. M. Mallan, D. Battistutta, J. M. Nicholson, R. Perry, and A. Magarey. 2012. Evaluation of an intervention to promote protective infant feeding practices to prevent childhood obesity: Outcomes of the NOURISH RCT at 14 months of age and 6 months post the first of two intervention modules. International Journal of Obesity 36(1):1292–1298.
Daniels, L. A., K. M. Mallan, J. M. Nicholson, D. Battistutta, and A. Magarey. 2013. Outcomes of an early feeding practices intervention to prevent childhood obesity. Pediatrics 132(1):e109–e118.
Daniels, L. A., K. M. Mallan, D. Battistutta, J. M. Nicholson, J. E. Meedeniya, J. K. Bayer, and A. Magarey. 2014. Child eating behavior outcomes of an early feeding intervention to reduce risk indicators for child obesity: The NOURISH RCT. Obesity (Silver Spring, Md.) 22(5):E104–E111.
Daniels, L. A., K. M. Mallan, J. M. Nicholson, K. Thorpe, S. Nambiar, C. E. Mauch, and A. Magarey. 2015. An early feeding practices intervention for obesity prevention. Pediatrics 136(1):e40–e49.
Dave, J. M., T. A. Chen, M. Almohamad, and S. Cotto-Moreno. 2022. Dietary intake among children attending childcare centers: Impact of the new CACFP meal guidelines. Nutrients 14(16):3394.
de Franchis, R., L. Bozza, P. Canale, M. Chiacchio, P. Cortese, A. D’avino, M. De Giovanni, M. Dello Iacovo, A. D’onofrio, A. Federico, N. Gasparini, F. Iaccarino, G. Romano, R. Spadaro, M. Tedesco, G. Vitiello, A. Antignani, S. Auricchio, V. Valentino, F. De Filippis, D. Ercolini, and D. Bruzzese. 2022. The effect of weaning with adult food typical of the Mediterranean diet on taste development and eating habits of children: A randomized trial. Nutrients 14(12):2486.
Dodd, J. M., D. Turnbull, A. J. McPhee, A. R. Deussen, R. M. Grivell, L. N. Yelland, C. A. Crowther, G. Wittert, J. A. Owens, and J. S. Robinson. 2014. Antenatal lifestyle advice for women who are overweight or obese: Limit randomised trial. BMJ 348:g1285.
Dodd, J. M., J. Louise, A. R. Deussen, A. J. McPhee, J. A. Owens, and J. S. Robinson. 2018. Prenatal diet and child growth at 18 months. Pediatrics 142(3):e20180035.
EOP (Executive Office of the President). 2022. Biden–Harris administration National Strategy on Hunger, Nutrition, and Health. Washington, DC: Executive Office of the President of the United States.
Erinosho, T., A. Vaughn, D. Hales, S. Mazzucca, Z. Gizlice, and D. Ward. 2018. Participation in the Child and Adult Care Food Program is associated with healthier nutrition environments at family child care homes in Mississippi. Journal of Nutrition Education and Behavior 50(5):441–450.
Erinosho, T., B. Jana, K. Loefstedt, M. Vu, and D. Ward. 2022. Facilitators and barriers to family child care home participation in the U.S. Child and Adult Care Food Program (CACFP). Preventive Medicine Reports 30:102022.
FCC (Federal Communications Commission). 2023. Affordable connectivity program. https://www.fcc.gov/acp (accessed July 3, 2023).
Fiks, A. G., R. S. Gruver, C. T. Bishop-Gilyard, J. Shults, S. Virudachalam, A. W. Suh, M. Gerdes, G. K. Kalra, P. A. DeRusso, A. Lieberman, D. Weng, M. A. Elovitz, R. I. Berkowitz, and T. J. Power. 2017. A social media peer group for mothers to prevent obesity from infancy: The Grow2Gether randomized trial. Childhood Obesity 13(5):356–368.
Fildes, A., C. Lopes, P. Moreira, G. Moschonis, A. Oliveira, C. Mavrogianni, Y. Manios, R. Beeken, J. Wardle, and L. Cooke. 2015. An exploratory trial of parental advice for increasing vegetable acceptance in infancy. British Journal of Nutrition 114(2):328–336.
Finlay, A., E. Robinson, A. Jones, M. Maden, C. Cerny, M. Muc, R. Evans, H. Makin, and E. Boyland. 2022. A scoping review of outdoor food marketing: Exposure, power and impacts on eating behaviour and health. BMC Public Health 22(1):1431.
FNS (Food and Nutrition Service). 2022. Current data collections. https://www.fns.usda.gov/ops/current-data-collections (accessed June 27, 2023).
FNS. 2023a. HEI scores for Americans https://www.fns.usda.gov/CNPP/hei-scores-americans (accessed July 17, 2023).
FNS. 2023b. National and state level estimates of WIC eligibility and program reach in 2020. https://www.fns.usda.gov/wic/eligibility-and-program-reach-estimates-2020 (accessed July 17, 2023).
FNS. 2023d. Nutrition education for CACFP. https://www.fns.usda.gov/cacfp/nutrition-and-nutrition-education (accessed August 22, 2023).
FNS. n.d. Child and Adult Care Food Program. https://www.fns.usda.gov/cacfp (accessed July 17, 2023).
FRAC (Food Research and Action Center). 2019. Child and Adult Care Food Program: Participation trends 2018. Food Research and Action Center. https://frac.org/wp-content/uploads/CACFP-participation-trends-2018.pdf (accessed August 6, 2023).
French, G. M., L. Nicholson, T. Skybo, E. G. Klein, P. M. Schwirian, L. Murray-Johnson, A. Sternstein, I. Eneli, B. Boettner, and J. A. Groner. 2012. An evaluation of mother-centered anticipatory guidance to reduce obesogenic infant feeding behaviors. Pediatrics 130(3):e507–e517.
GAO (U.S. Government Accountability Office). 2019. Nutrition education: USDA actions needed to assess effectiveness, coordinate programs, and leverage expertise. Washington, DC: GAO.
Gibbs, H., and R. Malik. 2022. Child care spending generates massive dividends. https://www.americanprogress.org/article/child-care-spending-generates-massive-dividends (accessed July 17, 2023).
Gibbs, H. D., A. R. Kennett, E. H. Kerling, Q. Yu, B. Gajewski, L. T. Ptomey, and D. K. Sullivan. 2016. Assessing the nutrition literacy of parents and its relationship with child diet quality. Journal of Nutrition Education and Behavior 48(7):505–509.
Gibby, C. L. K., C. Palacios, M. Campos, R. E. Graulau, and J. Banna. 2019. Acceptability of a text message-based intervention for obesity prevention in infants from Hawai’i and Puerto Rico WIC. BMC Pregnancy and Childbirth 19(1):291.
Globus, I., Y. Latzer, O. Pshetatzki, C. Shani Levi, R. Shaoul, I. Elad, and G. S. Rozen. 2019. Effects of early parent training on mother–infant feeding interactions. Journal of Developmental and Behavioral Pediatrics 40(2):131–138.
Gurzo, K., D. L. Lee, K. Ritchie, S. Yoshida, E. Homel Vitale, K. Hecht, and L. D. Ritchie. 2020. Child care sites participating in the federal Child and Adult Care Food Program provide more nutritious foods and beverages. Journal of Nutrition Education and Behavior 52(7):697–704.
Halfon, N., G. D. Stevens, K. Larson, and L. M. Olson. 2011. Duration of a well-child visit: Association with content, family-centeredness, and satisfaction. Pediatrics 128(4):657–664.
Harris, J. L., and J. L. Pomeranz. 2020. Infant formula and toddler milk marketing: Opportunities to address harmful practices and improve young children’s diets. Nutrition Reviews 78(10):866–883.
Harris, J. F.-M., F. Frances, W. Frazier, K. Haraghey, S. Kalnova, M. Romo-Palafox, N. Seymour, G. Rodriguez-Arauz, and M. B. Schwartz. 2017. Baby food facts: Nutrition and marketing of baby and toddler food and drinks. UConn Rudd Center for Food Policy and Obesity.
Harris, H. A., S. Anzman-Frasca, M. E. Marini, I. M. Paul, L. L. Birch, and J. S. Savage. 2020. Effect of a responsive parenting intervention on child emotional overeating is mediated by reduced maternal use of food to soothe: The INSIGHT RCT. Pediatric Obesity 15(1):e12645.
Harris, J. L., L. Phaneuf, and F. Fleming-Milici. 2022. Effects of sugary drink countermarketing videos on caregivers’ attitudes and intentions to serve fruit drinks and toddler milks to young children. American Journal of Public Health 112(S):S807–S816.
Heinz, H., D. Bell, J. Martinez, M. Cunningham, B. Maunders, and E. Y. Jimenez. 2022. New Mexico sponsors identify time and money as factors affecting home-based provider child and adult care food program engagement. Journal of Nutrition Education and Behavior 54(10):947–956.
Hernandez, E., J. A. Lavner, A. M. Moore, B. K. Stansfield, S. R. H. Beach, J. J. Smith, and J. S. Savage. 2022. Sleep SAAF responsive parenting intervention improves mothers’ feeding practices: A randomized controlled trial among African American mother–infant dyads. International Journal of Behavioral Nutrition and Physical Activity 19(1):129.
Hesketh, K. D., J. Salmon, S. A. McNaughton, D. Crawford, G. Abbott, A. J. Cameron, S. Lioret, L. Gold, K. L. Downing, and K. J. Campbell. 2020. Long-term outcomes (2 and 3.5 years post-intervention) of the INFANT early childhood intervention to improve health behaviors and reduce obesity: Cluster randomised controlled trial follow-up. International Journal of Behavioral Nutrition and Physical Activity 17(1):95.
HFA (Healthy Families America). n.d. Supporting home visiting: A guide to state and federal funding. Chicago: Healthy Families America.
HHS (U.S. Department of Health and Human Services). 2019. The decreasing number of family child care providers in the United States. https://www.acf.hhs.gov/occ/news/decreasing-number-family-child-care-providers-united-states (accessed July 11, 2023).
HHS. 2022. Early childhood home visiting models: Reviewing evidence of effectiveness. Washington, DC: Administration for Children and Families, Office of Planning, Research, and Evaluation. https://www.mathematica.org/publications/early-childhood-home-visiting-models-reviewing-evidence-of-effectiveness (accessed August 6, 2023).
HHS. 2023. Understanding and expanding the reach of home visiting (HV-REACH): 2021–2024. https://www.acf.hhs.gov/opre/project/understanding-and-expanding-reach-home-visiting (accessed July 11, 2023).
HHS. n.d.-a. Effects shown in research—Child health domain. https://homvee.acf.hhs.gov/outcomes/child%20health/In%20Brief (accessed July 17, 2023).
HHS. n.d.-b. Healthy People 2030: Building a healthier future for all. https://health.gov/healthypeople (accessed July 11, 2023).
Hoffmann, J., J. Günther, L. Stecher, M. Spies, K. Geyer, R. Raab, D. Meyer, K. Rauh, and H. Hauner. 2021. Infant growth during the first year of life following a pregnancy lifestyle intervention in routine care—Findings from the cluster-randomised GeliS trial. Pediatric Obesity 16(2):e12705.
Hohman, E. E., I. M. Paul, L. L. Birch, and J. S. Savage. 2017. INSIGHT responsive parenting intervention is associated with healthier patterns of dietary exposures in infants. Obesity 25(1):185–191.
Hohman, E. E., J. S. Savage, L. L. Birch, and I. M. Paul. 2020. The Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting intervention for firstborns affects dietary intake of secondborn infants. Journal of Nutrition 150(8):2139–2146.
Horodynski, M. A., and M. Stommel. 2005. Nutrition education aimed at toddlers: An intervention study. Pediatric Nursing 31(5):364–372.
HRSA (Health Resources and Services Administration). n.d. Strengthening the MIECHV home visiting workforce: A checklist for staff recruitment and staff retention. https://mchb.hrsa.gov/sites/default/files/mchb/programs-impact/strengthening-miechv-workforce.pdf (accessed August 6, 2023).
Ingalls, A., S. Rosenstock, R. Foy Cuddy, N. Neault, S. Yessilth, N. Goklish, L. Nelson, R. Reid, and A. Barlow. 2019. Family Spirit Nurture (FSN)—A randomized controlled trial to prevent early childhood obesity in American Indian populations: Trial rationale and study protocol. BMC Obesity 6:18.
Jana, B., K. Loefstedt, M. Vu, D. Ward, and T. Erinosho. 2023. “It has a lot to do with the cumbersome paperwork”: Barriers and facilitators of center-based early care and education program participation in the Child and Adult Care Food Program. Journal of the Academy of Nutrition and Dietetics 123(8):1173–1186.
JHU (Johns Hopkins University). n.d. Family Spirit affiliates in over 20 states serving over 130 communities. https://www.jhsph.edu/research/affiliated-programs/family-spirit/becoming-a-family-spirit-affiliate/our-affiliates/index.html (accessed July 7, 2023).
Jimenez, E. Y., R. Pérez-Escamilla, and S. A. Atkinson. 2021. Existing guidance on feeding infants and children from birth to 24 months: Implications and next steps for registered dietitian nutritionists. Journal of the Academy of Nutrition and Dietetics 121(4):647–654.
Joint Commission. 2022. New requirements to reduce health care disparities. The Joint Commission. https://www.jointcommission.org/-/media/tjc/documents/standards/r3-reports/r3_disparities_july2022-6-20-2022.pdf (accessed August 6, 2023).
Kaar, J. L., J. L. Hanson, S. A. Caskey, S. Jimenez, L. Lane, N. F. Krebs, and D. A. Thompson. 2019. Beyond nutrition knowledge and tools—What do pediatric providers really need? Medical Science Educator 29(1):307–314.
Kenney, E. L., M. K. Poole, H. Cory, and A. L. Cradock. 2020. Impact of changes to the Child and Adult Care Food Program on children’s dietary intake in family child care homes. Public Health Nutrition 23(11):2016–2023.
Kenney, E. L., K. Tucker, R. S. Plummer, C. Mita, and T. Andreyeva. 2023. The Child and Adult Care Food Program and young children’s health: A systematic review. Nutrition Reviews. Mar 7:nuad016.
Kline, A. 2016. Optional best practices to further improve nutrition in the CACFP. CACFP 15–2016. https://www.fns.usda.gov/cacfp/optional-best-practices-further-improve-nutrition-cacfp (accessed August 6, 2023).
Konrad, T. R., C. L. Link, R. J. Shackelton, L. D. Marceau, O. von dem Knesebeck, J. Siegrist, S. Arber, A. Adams, and J. B. McKinlay. 2010. It’s about time: Physicians’ perceptions of time constraints in primary care medical practice in three national healthcare systems. Medical Care 48(2):95–100.
Korenman, S., K. S. Abner, R. Kaestner, and R. A. Gordon. 2013. The Child and Adult Care Food Program and the nutrition of preschoolers. Early Childhood Research Quarterly 28(2):325–336.
Kumanyika, S. K. 2019. A framework for increasing equity impact in obesity prevention. American Journal of Public Health 109(10):1350–1357.
Landry, M. J., A. E. van den Berg, F. M. Asigbee, S. Vandyousefi, R. Ghaddar, and J. N. Davis. 2019. Child-report of food insecurity is associated with diet quality in children. Nutrients 11(7):1574.
Lee, D. L., R. Traseira, S. Navarro, N. Frost, S. E. Benjamin-Neelon, A. L. Cradock, K. Hecht, and L. D. Ritchie. 2021. Alignment of state regulations with breastfeeding and beverage best practices for childcare centers and family childcare homes, United States. Public Health Reports 136(1):79–87.
Lee, D. L., E. Homel Vitale, S. K. Marshall, C. Hecht, L. T. Beck, and L. D. Ritchie. 2022. Child and Adult Care Food Program participation benefits, barriers and facilitators for independent child care centers in California. Nutrients 14(21):4449.
Lin, V., S. H. Shaw, and K. Maxwell. 2019. Administrative data sources to address early care and education policy-relevant research questions. Washington, DC: OPRE; HHS.
LoRe, D., C. Y. Y. Leung, L. Brenner, and D. L. Suskind. 2019. Parent-directed intervention in promoting knowledge of pediatric nutrition and healthy lifestyle among low-SES families with toddlers: A randomized controlled trial. Child: Care, Health and Development 45(4):518–522.
Macchi, A. K., J. Banna, S. Moreira, M. Campos, and C. Palacios. 2022. Effect of a short messaging service (SMS) intervention delivered to caregivers on energy, nutrients, and food groups intake in infant participants of the WIC program. Frontiers in Public Health 10:986330.
MacMillan Uribe, A. L., E. W. Duffy, B. Enahora, P. Githinji, J. McGuirt, and G. L. Tripicchio. 2023. Digital technology in nutrition education and behavior change: Opportunities and challenges. Journal of Nutrition Education and Behavior 55(6):391–392.
MACPAC (Medicaid and CHIP Payment and Access Commission). 2022. Medicaid coverage of community health worker services. Medicaid and CHIP Payment and Access Commission issue brief. https://www.macpac.gov/wp-content/uploads/2022/04/Medicaid-coverage-of-community-health-worker-services-1.pdf (accessed August 6, 2023).
Magarey, A., C. Mauch, K. Mallan, R. Perry, R. Elovaris, J. Meedeniya, R. Byrne, and L. Daniels. 2016. Child dietary and eating behavior outcomes up to 3.5 years after an early feeding intervention: The NOURISH RCT. Obesity 24(7):1537–1545.
Maguire, J. L., C. S. Birken, S. Jacobson, M. Peer, C. Taylor, A. Khambalia, M. Mekky, K. E. Thorpe, and P. Parkin. 2010. Office-based intervention to reduce bottle use among toddlers: TARGet Kids! Pragmatic, randomized trial. Pediatrics 126(2):e343–e350.
Marshall, S., B. J. Johnson, K. D. Hesketh, K. J. Campbell, K. Fraser, P. Love, E. Denney-Wilson, J. Salmon, Z. Callum, and R. Laws. 2022. Mapping intervention components from a randomized controlled trial to scale-up of an early life nutrition and movement intervention: The INFANT program. Frontiers in Public Health 10:1026856. https://doi.org/10.3389/fpubh.2022.1026856.
Martin, J. A, and M. J. K. Osterman. 2023. Changes in prenatal care utilization: United States, 2019–2021. National Vital Statistics Reports 72(4). May 4. Hyattsville, MD: National Center for Health Statistics. https://stacks.cdc.gov/view/cdc/125706 (accessed August 8, 2023).
Messito, M. J., M. W. Katzow, A. L. Mendelsohn, and R. S. Gross. 2020. Starting early program impacts on feeding at infant 10 months age: A randomized controlled trial. Childhood Obesity 16(S):S4–S13.
Morandi, A., M. Tommasi, F. Soffiati, F. Destro, L. Fontana, F. Grando, G. Simonetti, C. Bucolo, E. Alberti, L. Baraldi, A. Chiriacò, N. Ferrarese, G. Frignani, M. Pasqualini, V. Rossi, C. Siciliano, A. M. Zuccolo, G. Matticchio, V. Vettori, D. Danieli, L. Guarda, M. Iuliano, F. Raimo, S. Sirpresi, E. Trevisan, S. Vinco, and C. Maffeis. 2019. Prevention of Obesity in Toddlers (PROBIT): A randomised clinical trial of responsive feeding promotion from birth to 24 months. International Journal of Obesity 43(1):1961–1966.
Mozaffarian, D., H. M. Blanck, K. M. Garfield, A. Wassung, and R. Petersen. 2022. A food is medicine approach to achieve nutrition security and improve health. Nature Medicine 28(11):2238–2240.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2020. Feeding infants and children from birth to 24 months: Summarizing existing guidance. Washington, DC: The National Academies Press.
NCES (National Center for Education Statistics). n.d. Nutrition education in public elementary and secondary schools. https://nces.ed.gov/surveys/frss/publications/96852 (accessed July 11, 2023).
NHVRC (National Home Visiting Resource Center). 2019. Exploring home visiting’s unmet need: Comparing who could benefit to who is served. https://nhvrc.org/wp-content/up-loads/NHVRC-Brief-120919-FINAL.pdf.
NHVRC. n.d.-a. About home visiting: Location and reach. https://nhvrc.org/yearbook/2022-yearbook/about-home-visiting/location-reach (accessed August 6, 2023).
NHVRC. n.d.-b. What is home visiting? https://nhvrc.org/what-is-home-visiting (accessed July 21, 2023).
NHVRC. n.d.-c. Who is being served by emerging models? https://nhvrc.org/yearbook/2022-yearbook/who-is-being-served/by-emerging-models (accessed July 21, 2023).
NIFA (National Institute of Food and Agriculture). n.d. EFNEP-related research. https://www.nifa.usda.gov/grants/programs/capacity-grants/efnep/efnep-related-research (accessed August 22, 2023).
Oliveira, V., and E. Frazão. 2015. The WIC program: Background, trends, and economic issues, 2015 edition. Washington, DC: U.S. Department of Agriculture, Economic Research Service.
Ontai, L. L., S. L. Sitnick, M. K. Shilts, and M. S. Townsend. 2016. My Child at Mealtime: A visually enhanced self-assessment of feeding styles for low-income parents of preschoolers. Appetite 99:76–81.
Ontai, L. L., C. Sutter, S. Sitnick, M. K. Shilts, and M. S. Townsend. 2019. My Child at Mealtime parent self-assessment of food related behaviors: Validation with mealtime behaviors. Appetite 136:62–69.
Palacios, C., M. Campos, C. Gibby, M. Meléndez, J. E. Lee, and J. Banna. 2018. Effect of a multi-site trial using short message service (SMS) on infant feeding practices and weight gain in low-income minorities. Journal of the American College of Nutrition 37(7):605–613.
Pérez-Escamilla, R., and S. Segura-Pérez. 2020. Can a pragmatic responsive feeding scale be developed and applied globally? Maternal and Child Nutrition 16(3):e13004.
Pérez-Escamilla, R., E. Y. Jimenez, and K. G. Dewey. 2021. Responsive feeding recommendations: Harmonizing integration into dietary guidelines for infants and young children. Current Developments in Nutrition 5(6).
Petrin, C., K. Prakash, S. Kahan, and M. Gallagher. 2014. Medicaid fee-for-service treatment of obesity interventions. Stop Obesity Alliance. George Washington University.
Potvin Kent, M., F. Hatoum, D. Wu, L. Remedios, and M. Bagnato. 2022. Benchmarking unhealthy food marketing to children and adolescents in Canada: A scoping review. Health Promotion and Chronic Disease Prevention in Canada 42(8):307–318.
Public Health Law Center. n.d. Child care licensing laws for nutrition, active play and screen time—Snapshot: Maryland. https://www.publichealthlawcenter.org/sites/default/files/PHLC-Maryland-HER-State-Summary.pdf (accessed July 21, 2023).
RHIhub. 2023. Rural healthcare workforce. https://www.ruralhealthinfo.org/topics/health-care-workforce (accessed July 10, 2023).
Ritchie, L. D., M. Boyle, K. Chandran, P. Spector, S. E. Whaley, P. James, S. Samuels, K. Hecht, and P. Crawford. 2012. Participation in the Child and Adult Care Food Program is associated with more nutritious foods and beverages in child care. Childhood Obesity 8(3):224–229.
Ritchie, L., D. Lee, L. Sallack, C. Chauvenet, G. Machell, L. Kim, L. Song, and S. Whaley. 2021. Multi-state WIC participant satisfaction survey: Learning from program adaptations during COVID. National WIC Association. https://media.nwica.org/nwamulti-state-wic-participant-satisfaction-surveynationalreportfinal.pdf (accessed August 6, 2023).
Robson, S. M., J. C. Khoury, H. J. Kalkwarf, and K. Copeland. 2015. Dietary intake of children attending full-time child care: What are they eating away from the child-care center? Journal of the Academy of Nutrition and Dietetics 115(9):1472–1478.
Rosenstock, S., A. Ingalls, R. Foy Cuddy, N. Neault, S. Littlepage, L. Cohoe, L. Nelson, K. Shephard-Yazzie, S. Yazzie, A. Alikhani, R. Reid, A. Kenney, and A. Barlow. 2021. Effect of a home-visiting intervention to reduce early childhood obesity among Native American children: A randomized clinical trial. JAMA Pediatrics 175(2):133–142.
Rudd Center. 2016. Baby food facts. UCONN Rudd Center. https://uconnruddcenter.org/wp-content/uploads/sites/2909/2020/09/Baby-Food-FACTS-fourpager_FINAL.pdf (accessed July 21, 2023).
Rudd Center. n.d. Food marketing. https://uconnruddcenter.org/research/food-marketing (accessed June 27, 2023).
Sandstrom, H., D. Genua, C. Lou, and S. Benatar. 2020. Home visiting career trajectories: Snapshot of home visitors’ qualifications, job experiences, and career pathways. Washington, DC: Office of Planning, Research, and Evaluation.
Sanghavi, D. M. 2005. Taking well-child care into the 21st century: A novel, effective method for improving parent knowledge using computerized tutorials. Archives of Pediatrics & Adolescent Medicine 159(5):482–485.
Savage, J. S., L. L. Birch, M. Marini, S. Anzman-Frasca, and I. M. Paul. 2016. Effect of the INSIGHT responsive parenting intervention on rapid infant weight gain and overweight status at age 1 year: A randomized clinical trial. JAMA Pediatrics 170(8):742–749.
Savage, J. S., E. E. Hohman, M. E. Marini, A. Shelly, I. M. Paul, and L. L. Birch. 2018. INSIGHT responsive parenting intervention and infant feeding practices: Randomized clinical trial. International Journal of Behavioral Nutrition and Physical Activity 15(1):64.
Schroeder, N., B. Rushovich, E. Bartlett, S. Sharma, J. Gittelsohn, and B. Caballero. 2015. Early obesity prevention: A randomized trial of a practice-based intervention in 0–24-month infants. Journal of Obesity 2015:795859.
Sigman-Grant, M., R. Pérez-Escamilla, S. Segura-Pérez, and M. Lott. 2017. Feeding infants and young toddlers: Using the latest evidence in child-care settings. https://www.fns.usda.gov/cacfp/optional-best-practices-further-improve-nutrition-cacfp (accessed July 10, 2023).
Skouteris, H., H. J. Bergmeier, S. D. Berns, J. Betancourt, R. Boynton-Jarrett, M. B. Davis, K. Gibbons, R. Pérez-Escamilla, and M. Story. 2021. Reframing the early childhood obesity prevention narrative through an equitable nurturing approach. Maternal & Child Nutrition 17(1):e13094.
Spence, A. C., S. A. McNaughton, S. Lioret, K. D. Hesketh, D. A. Crawford, and K. J. Campbell. 2013. A health promotion intervention can affect diet quality in early childhood. Journal of Nutrition 143(1):1672–1678.
Spence, A. C., K. J. Campbell, D. A. Crawford, S. A. McNaughton, and K. D. Hesketh. 2014. Mediators of improved child diet quality following a health promotion intervention: The Melbourne InFANT program. International Journal of Behavioral Nutrition and Physical Activity 11:137.
Taillie, L. S., E. Busey, F. M. Stoltze, and F. R. Dillman Carpentier. 2019. Governmental policies to reduce unhealthy food marketing to children. Nutrition Review 77(11):787–816.
Taveras, E. M., K. Blackburn, M. W. Gillman, J. Haines, J. McDonald, S. Price, and E. Oken. 2011. First Steps for Mommy and Me: A pilot intervention to improve nutrition and physical activity behaviors of postpartum mothers and their infants. Maternal and Child Health Journal 15(8):1217–1227.
Taylor, M. K., D. K. Sullivan, E. F. Ellerbeck, B. J. Gajewski, and H. D. Gibbs. 2019. Nutrition literacy predicts adherence to healthy/unhealthy diet patterns in adults with a nutrition-related chronic condition. Public Health Nutrition 22(12):2157–2169.
Townsend, M. S., M. K. Shilts, D. M. Styne, C. Drake, L. Lanoue, and L. Ontai. 2018. An obesity risk assessment tool for young children: Validity with BMI and nutrient values. Journal of Nutrition Education and Behavior 50(7):705–717.
Townsend, M. S., M. K. Shilts, L. Lanoue, C. Drake, D. M. Styne, L. Woodhouse, and L. Ontai. 2020. Obesity risk assessment tool among 3–5 year olds: Validation with biomarkers of low-grade chronic inflammation. Childhood Obesity 16(S1):S23–S32.
Tussing-Humphreys, L., J. L. Thomson, M. Goodman, and A. Landry. 2019. Enhanced vs standard parents as teacher curriculum on factors related to infant feeding among African American women. Southern Medical Journal 112(1):512–519.
UNC. 2022 Center for Health Promotion and Disease Prevention. Appendix C. Evaluation methods. https://snapedtoolkit.org/framework/appendices/appendix-e-evaluation-methods (accessed August 22 2023).
UNESCO (United Nations Educational, Scientific and Cultural Organization). 2023. Ready to learn and thrive: School health and nutrition around the world. Paris, France: United Nations.
USDA (U.S. Department of Agriculture). 2020. WIC program. https://www.ers.usda.gov/topics/food-nutrition-assistance/wic-program.aspx (accessed July 21, 2023).
USDA. 2022a. Child and Adult Care Food Program. https://www.ers.usda.gov/topics/food-nutrition-assistance/child-nutrition-programs/child-and-adult-care-food-program (accessed May 2, 2023).
USDA. 2022b. Food security and nutrition assistance. https://www.ers.usda.gov/data-products/ag-and-food-statistics-charting-the-essentials/food-security-and-nutrition-assistance (accessed July 14, 2023).
USDA and HHS (Department of Health and Human Services). 2020. Dietary Guidelines for Americans, 2020–2025. https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed August 10, 2023).
van Grieken, A., E. Vlasblom, L. Wang, M. Beltman, M. M. Boere-Boonekamp, M. P. L’Hoir, and H. Raat. 2017. Personalized web-based advice in combination with well-child visits to prevent overweight in young children: Cluster randomized controlled trial. Journal of Medical Internet Research 19(7):e268.
VanFrank, B. K., S. Park, J. L. Foltz, L. C. McGuire, and D. M. Harris. 2018. Physician characteristics associated with sugar-sweetened beverage counseling practices. American Journal of Health Promotion 32(6):1365–1374.
Vaz, J. S., M. F. S. Maia, P. A. R. Neves, T. M. Santos, L. P. Vidaletti, and C. Victora. 2021. Monitoring breastfeeding indicators in high-income countries: Levels, trends and challenges. Maternal and Child Nutrition 17(3):e13137.
Verrall, T., L. Napash, L. Leclerc, S. Mercure, and K. Gray-Donald. 2006. Community-based communication strategies to promote infant iron nutrition in northern Canada. International Journal of Circumpolar Health 65(1):65–78.
Vlasblom, E., A. van Grieken, M. Beltman, M. P. L’Hoir, H. Raat, and M. M. Boere-Boonekamp. 2020. Parenting support to prevent overweight during regular well-child visits in 0–3 year old children (BBOFT+ program), a cluster randomized trial on the effectiveness on child BMI and health behaviors and parenting. PLOS ONE 15(8):e0237564.
Weinfield, N. S., C. Borger, L. E. Au, S. E. Whaley, D. Berman, and L. D. Ritchie. 2020. Longer participation in WIC is associated with better diet quality in 24-month-old children. Journal of the Academy of Nutrition and Dietetics 120(6):963–971.
White House. 2022. Bipartisan infrastructure law rural playbook: A roadmap for delivering opportunity and investments in rural America. https://www.whitehouse.gov/build/re-sources/rural (accessed July 11, 2023).
Wolf, E. R., C. J. Hochheimer, R. T. Sabo, J. DeVoe, R. Wasserman, E. Geissal, D. J. Opel, N. Warren, J. Puro, J. O’Neil, J. Pecsok, and A. H. Krist. 2018. Gaps in well-child care attendance among primary care clinics serving low-income families. Pediatrics 142(5):e20174019.
Zaltz, D. A., A. A. Hecht, R. R. Pate, B. Neelon, J. R. O’Neill, and S. E. Benjamin-Neelon. 2020. Participation in the Child and Adult Care Food Program is associated with fewer barriers to serving healthier foods in early care and education. BMC Public Health 20(1):856.
Zheng, M., K. D. Hesketh, S. A. McNaughton, J. Salmon, D. Crawford, A. J. Cameron, S. Lioret, and K. J. Campbell. 2022. Quantifying the overall impact of an early childhood multi-behavioural lifestyle intervention. Pediatric Obesity 17(3):e12861.
This page intentionally left blank.