
6
Improving Procurement, Acceptance, and Use of Deceased Donor Organs
“Our vision of the transplant ecosystem is patient centered, designed to improve organ failure and patient survival by doing four things: Improving organ availability, maximizing use, achieving high-quality outcomes, and fostering innovation.”
—A. Osama Gaber, President, American Society of Transplant Surgeons, Houston Methodist Department of Surgery, testimony to the committee during July 15, 2021 public listening session
The U.S. organ transplantation system is dependent on many factors, as discussed in this chapter, but most importantly, it depends on the generosity of individuals and their families who, at the time of death, make the decision to donate organs to someone they have never met. The success of this system is founded on and maintained by the public’s trust in that system—both trust in the end-of-life decision-making process and trust in the process of providing transplants to patients who need them. In the context of evolving organ allocation and distribution policies and new organ procurement organization (OPO) regulations, there are notable tensions in the donation and transplant community that have resulted in the task of this report. After analyzing the performance of the organ transplantation and donation system—and OPOs and transplant centers in particular—and reviewing the scientific literature and publicly available data, the committee found that the current organ transplantation system, similar to other systems, is perfectly designed to achieve the results it gets (Berwick, 1996; IOM, 2006). That is, the results of the organ transplantation system, in terms of procuring, allocating, distributing, and transplanting organs into waiting recipients, are precisely the results permitted by the features of the system. The current deficiencies in the organ transplantation system present opportunities for improvement. Data on the performance of system components (e.g., OPOs and transplant centers) reveals significant shortfalls in the degree to which the potential transplant recipient is at the center of the decision-making process, but there are effective ways to address these shortfalls.
This chapter analyzes the performance data of OPOs and transplant centers with a focus on opportunities to standardize and bring innovations and best practices to OPOs and transplant centers nationwide. Inadequacies in OPO and transplant center performance are currently
detracting from getting the best organ for, and to, the right recipient in the most efficient and equitable manner. This chapter discusses the sources and types of data in the organ transplantation system and opportunities for standardization to improve understanding of system performance; the committee analyzed this evidence through a systems perspective and the underlying principle that putting the patient at the center of system improvements is always best.
There are two key areas with high variability in performance and therefore great room for improvement that are a major focus of this chapter: (1) OPO pursuit and procurement of donation after circulatory determination of death (DCDD) donors,1 and (2) transplant centers accepting and using more of the deceased donor organs offered to individuals on the waiting list. The committee’s identification of these two key areas was influenced by these striking statistics on performance: (1) An over five-fold variation exists across the nation’s OPOs in terms of recovery of DCDD donors, and (2) the 2019 transplant center rates at which organs were recovered for transplant but not transplanted (i.e., the nonuse rate)2 ranged from 20 percent for kidneys, 10 percent for livers, 6.5 percent for lungs, to 0.85 percent for hearts (Israni et al., 2021; SRTR, 2021) That is, one in five deceased donor kidneys are procured but not used (Israni et al., 2021; SRTR, 2021). Furthermore, there are organs offered and declined before they are ever procured, so the number of potentially transplantable organs that are not used for transplant may be even higher. To increase efficiency, the organ transplantation system must prioritize the use of already available organs, while simultaneously expanding the donor pool in all ways possible, especially including procurement and use of more DCDD donors to meet the needs of those on the transplant waiting list.
In all systems, including the organ transplantation system, variations exist for any number of reasons and are not, in and of themselves, an indicator of poor performance (NQF, 2021). However, meaningful performance comparisons are only possible, and variations explained, when standardized measures are used. Although an abundance of data has been collected on the organ transplantation system, the committee found that large, core segments of data are not standardized. For instance, while all 57 OPOs collect a variety of data related to the processes of organ donation in their geographic area, standardization of those data is lacking. Also, as discussed in Chapter 4, there are no national standards for how to train OPO staff on communication skills in compassion and cultural sensitivity, despite evidence suggesting that OPO staff were missing opportunities to increase the supply of available deceased donor organs and equalize regional variations in donation and transplantation rates (Traino et al., 2017).
This lack of standardization limits efforts in identifying causes of system variation. Despite the knowledge and sharing of many best practices for OPOs and transplant centers, underperformance and a lack of systemwide adherence will become further entrenched without the implementation of reliable process and outcome measures. All stakeholders benefit when variations are readily discernible, promoting both continuous improvement initiatives and the transfer of best practices among donor hospitals, OPOs, and transplant centers (Lynch et al., 2021).
INCREASING DECEASED ORGAN DONATION AND PROCUREMENT
As transplantation has become a treatment modality for end-stage organ failure of all types, the gap has continued to widen between the national waiting list and the number of available deceased organ donors. The National Academies have been called on in the past
___________________
1Donation after circulatory death (DCD) is the most well-known term, but the committee uses the more precise term donation after circulatory determination of death (DCDD). Historically, this was also known as non–heart-beating cadaveric donation.
2 This report uses the term nonuse rate; this is equivalent to the more commonly used discard rate.
to provide advice on ways to increase deceased organ donation in the United States (see Appendix B). National efforts in the years since the National Organ Transplant Act (NOTA)—and especially since the Organ Donation and Transplant Breakthrough Collaborative was initiated in 2003—have resulted in the widespread sharing of proven practices among all 57 OPOs (Shafer et al., 2008) and hundreds of the nation’s largest trauma centers where most donors originate. These efforts, and others, have resulted in a steady growth in the rate of deceased organ donation: the total number of deceased donors increased annually between 2010 and 2020 from 7,943 to 12,588 donors, and organ donation from deceased donors grew 39 percent between 2015 and 2020 (OPTN, 2021a). In 2020, the United States led the world in the deceased organ donor rate with 38.03 donors per million population (IRODaT, 2021). However, this committee did not conduct an analysis of differential death rates across countries or of the ways that differences in the cause of death could impact international comparisons. Relative to other high-income countries, the United States has disproportionately high numbers of drug overdose deaths (Ho, 2019), gun deaths (Grinshteyn and Hemenway, 2019), suicides (The Commonwealth Fund, 2020), and fatal car accidents (WHO, 2018). These differences, which may contribute to more potential donors per million population in the United States compared with other countries, deserve further research.
OPO REGULATORY FRAMEWORK AND PERFORMANCE METRICS
As described earlier in this report, OPOs have the responsibility for identifying potential organ donors, receiving authorization for deceased donor donation, providing support to donor families, clinically managing organ donors, allocating and procuring organs, and confirming that organs reach the transplant hospital (CMS, 2020a). In addition, OPOs provide professional and public education on organ donation. Therefore, organ donation is most closely linked to OPO performance, but the use of organs by transplant centers creates an interconnectedness between OPO and transplant center behaviors. For instance, the willingness of transplant centers to accept different types of organs has often driven OPO practices of pursuing medically complex, older, or DCDD donors. If a transplant center has been unwilling to accept and use organs from medically complex donors, then the OPO has been unlikely to pursue procuring these types of donors (Yu et al., 2020). With the advent of broader distribution of organs to transplant candidates, and as evidenced by increases in DCDD donation, many OPOs have proven to be more willing to pursue these donors and transplant centers are more willing to use the organs.
The formal system and structure of OPOs as regulated nonprofit monopolies was created under NOTA with regulatory authority assigned to the Centers for Medicare & Medicaid Services (CMS). CMS conducts surveys of OPOs every 4 years and evaluates whether they meet CMS conditions for coverage for recertification. There are currently 57 OPOs, each assigned to their own donation service area (DSA). Although an OPO has never been decertified, decertification would require the OPO’s geographic area—its DSA—to be opened to competition from other OPOs qualified to compete. On a monthly basis, the Scientific Registry of Transplant Recipients (SRTR) receives data collected from OPOs by the United Network for Organ Sharing (UNOS), contracted to act as the Organ Procurement and Transplantation Network (OPTN). The OPO data include the number of deaths reported by hospitals within their DSAs, the number of those deaths meeting standardized definitions of “eligible” or “imminent” deaths,3 the frequency with which deceased individuals become donors, and the
___________________
3 The definitions “eligible” and “imminent” are still in OPTN policies, but have been removed in the new OPO regulations.
number of organs that are successfully placed for transplant (SRTR, 2022a). Program-specific data for all OPOs are available on the SRTR website.
OPO performance measures are widely recognized as insufficient, largely because each OPO self-reports their outcomes in a nonstandardized way, making valid comparisons of OPO performance nearly impossible. For years, some within and beyond the OPO community requested defined, standardized performance regulations. In November 2020, CMS issued a long-awaited Final Rule that updates the conditions for coverage to evaluate OPOs on the outcomes of new measures of the donation rates and transplantation rates (CMS, 2020a). OPO performance on the new outcome measures will be publicly released each year, and OPOs will face increased competition under the new measures. At the end of each 4-year recertification cycle, DSAs for Tier 2 and Tier 3 OPOs will be opened for competition; the new CMS measures will be implemented in August 2022, and full application and enforcement will begin in 2026 (CMS, 2020a) (see Box 6-1 for key provisions).
This committee’s charge includes consideration of the following:
“self-reported donation metrics (e.g., “eligible deaths”) and the impact on estimates of the true donor supply….and the development of a new, standardized, objective, and verifiable donation metric to permit the transplant community to evaluate DSAs and OPOs and establish best practices” (see Chapter 1).
The revisions to the CMS Final Rule were a matter of much debate by stakeholders in the organ transplantation system. One area of particular relevance to this report is the reliance on death certificate data for the donation rate measure. In theory, death certificate data could be considered independent of bias, as it is not self-reported by OPOs, and able to provide a larger picture of the number of potential deceased donors. However, death certificates do not require the listing of secondary diagnoses, which may include medical conditions that would preclude deceased donation, such as cancer or an infectious disease like COVID19. Without these secondary diagnoses, a deceased person who would never be medically acceptable for donation could be inadvertently counted in the donation rate denominator, negatively affecting the OPO’s performance metrics under the proposed donation rate metric. Additionally, the reliability and accuracy of death certificate data is a challenge. The percent of death certificates inaccurately or incompletely reporting cause of death or having other significant errors ranges from 25 to 50 percent (Gill and DeJoseph, 2020; McGivern et al., 2017; POGO, 2021; Pritt et al., 2005; Wexelman et al., 2013). Also, death certificate data often do not become available until 1 to 2 years after the death occurred, a problem when considering the need to evaluate OPO performance in a timely manner. Notwithstanding these concerns, some authors indicate that irregularities in death certificate data would not impact the reporting of eligible donor deaths since stroke, trauma, and drug overdose deaths constitute a large portion of organ donors, and these conditions are rarely miscategorized on death certificates (Karp and Segal, 2021).
An alternative source of data suggested during the CMS comment period as a more accurate source of data for calculating donor potential is ventilated death data from hospitals’ electronic health records (EHRs). These hospital data refer to whether the patient died on a ventilator, a medical requirement for organ donation to occur. This is a key data point which is not specified on death certificates (UNOS, 2020). Advocates for this metric suggest that in the future these hospital-level patient data could come from individual patient EHRs upon referral of the donor to the OPO. However, some authors, including a former U.S. chief data scientist, have noted that ventilated death definitions are not standardized and there is currently no reporting mechanism or automated system to capture the relevant information,
thereby requiring manual review of patient medical records using complex definitions and patient-specific details. Among other problems, the authors suggest this complexity in using ventilated death definitions leaves the data vulnerable to manipulation and inaccuracy (Karp et al., 2020).
During consideration of the new OPO performance metrics, CMS reported that commenters raised concerns about the burden on donor hospitals if data on ventilated deaths were required for reporting. CMS agreed that requiring these additional reporting requirements or combining disparate data sources to estimate donor potential via ventilated deaths “could not be obtained by reasonable efforts” but would continue to be evaluated as new data sources become available (CMS, 2020b). In December 2021, CMS also issued a request for information regarding, among other parts of the organ donation process, input on data collection of patient-level data, underscoring the urgency in making accurate assessments of organ donor potential and suggesting there is room for ongoing clarity and improvement in current regulations (CMS, 2021).
In the end, the committee agreed that no single metric—whether based on death certificates or ventilated deaths data—would be adequate to fully understand and assess the performance of the interconnected parts of the organ transplantation system. Rather, performance measures in multiple domains are needed to assess the performance of donor hospitals, OPOs, and transplant centers in achieving overall system performance goals (see Recommendation 12 in Chapter 7 for greater discussion of the metrics that could populate a standardized dashboard of performance metrics). As organ donation, procurement, and transplantation practices evolve, performance metrics will need to evolve accordingly. For example, if donor care units are adopted by all OPOs in the United States, as recommended in this report (see Recommendation 11 later in this chapter), this would constitute a significant change in procurement practices that may warrant reconsideration of the performance measures used to assess OPO functionality given the new standard of practice. The committee believes that the organ transplantation system’s consideration of these issues should be informed by the experience of organizations such as the National Quality Forum that have demonstrated specific expertise in evaluating performance metrics across complex systems.
Box 6-2 provides the committee’s rationale for an integrated and holistic approach to the measurement and assessment of OPO performance.
Conclusion 6-1: The CMS OPO performance metrics taking effect in 2022 will provide standardization and allow for more meaningful reporting on system performance. However, timely, verifiable, and currently available data—ideally hospital patient-level data—would provide the most accurate assessment of deceased donor potential.
KEY AREA FOR IMPROVEMENT FOR OPOS: DONATION AFTER CIRCULATORY DETERMINATION OF DEATH
While there are many factors related to increasing the organ supply, the more than fivefold variation of DCDD donors by OPOs across the country provides a striking example that significant improvements are possible and needed in this area. The committee reviewed levels of achievement by the highest performers in the system to provide valuable insight into the possibilities within the existing statutory, regulatory, and clinical practice-based elements of the transplantation system to increase deceased organ donation.
Historical Perspective
Early transplant programs obtained organs either from healthy, living, related donors or from deceased donors who were declared dead by cardiopulmonary criteria. A determination of death by neurological criteria, although a legal option in the sense that state laws allowed clinicians to make determinations of death according to their own practice and custom, was not generally accepted historically as clinicians were reluctant to pronounce death in a patient who had continued heart function. These deceased donors provided kidneys most frequently, although there were some successful attempts to transplant other solid organs (IOM, 1997). In 1981, the National Conference of Commissioners on Uniform State Laws, the entity that promulgates many uniform laws, published the Uniform Determination of Death Act that was adopted very quickly by almost all 50 states. As more donors were being declared dead by neurological criteria, the number of donors declared by circulatory criteria decreased significantly, and virtually all DCDD donation in the United States came to a standstill.
In response to a 1997 request from the U.S. Department of Health and Human Services (HHS), the Institute of Medicine (IOM) studied ways to increase the availability of organs while ensuring the ethically and medically sound treatment of donor patients before and after death. The IOM study concluded that organ recovery after circulatory death provided an opportunity to increase the availability of organs to individuals on the waiting list (IOM, 1997). The release of the IOM report correlated with subsequent increases in DCDD, with OPOs and transplant centers developing protocols and supporting infrastructure to expand the practice of DCDD in the continuum of quality end-of-life care. A national focus in the pursuit of DCDD dona-
tion developed during the 2003 Health Resources and Services Administration-sponsored Organ Donation Breakthrough Collaborative, when a national benchmark of 10 percent of deceased donors being recovered through DCDD was established.4 While DCDD donors have increased overall, the adoption of DCDD protocols has been uneven across the United States and OPOs exhibit significant variation in their pursuit of and success with DCDD.
Some variation in procurement of DCDD organs could be related to challenges in determining death, particularly for the donation of hearts after cardiac death (Veatch, 2008). There is also consideration of variability in “hands-off” rules—that is, the time for which the decedent’s condition is considered irreversible. The committee did not conduct an in-depth analysis of these issues, but notes that under current regulatory and ethical regimes, there exists an opportunity to continue and support the upward trend of DCDD organ procurement and transplantation.
Current State of DCDD Donation and Transplantation
Since DCDD donation has been tracked by the OPTN, the consistent pursuit of DCDD donors and use by transplant centers began to systematically increase in 2004, precipitated by the Organ Donation and Transplantation Breakthrough Collaborative (Figure 6-1).
Despite these overall increases in DCDD procurement, today there is five-fold variation in the recovery of DCDD organs across the system. To analyze the variability in DCDD performance across OPOs, it is important to understand the variability in use of DCDD organs by transplant centers and the interconnected nature of OPO and transplant center behaviors and performance. Figure 6-2 shows the growth in the use of DCDD organs by transplant centers.
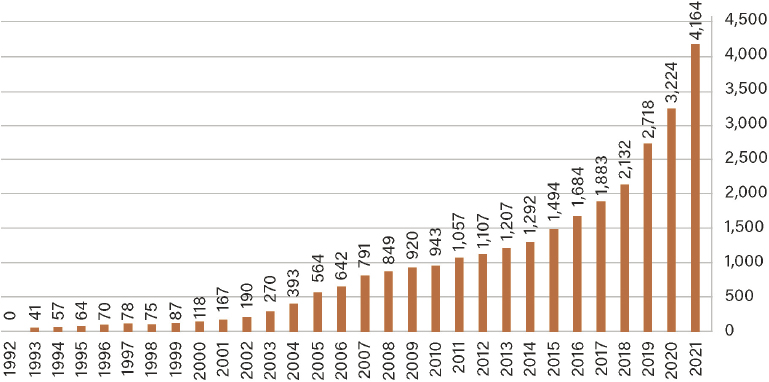
NOTE: DCDD donors n = 28,281; All DCDD + non-DCDD donors n = 250,461; DCDD donor percentage = 11.3%.
SOURCE: Based on OPTN data as of January 10, 2022. https://optn.transplant.hrsa.gov/data/view-datareports/national-data (accessed January 10, 2022).
___________________
4 A version of the program continues today as the Donation and Transplantation Community of Practice, managed by the alliance. See https://www.organdonationalliance.org/about (accessed December 23, 2021).
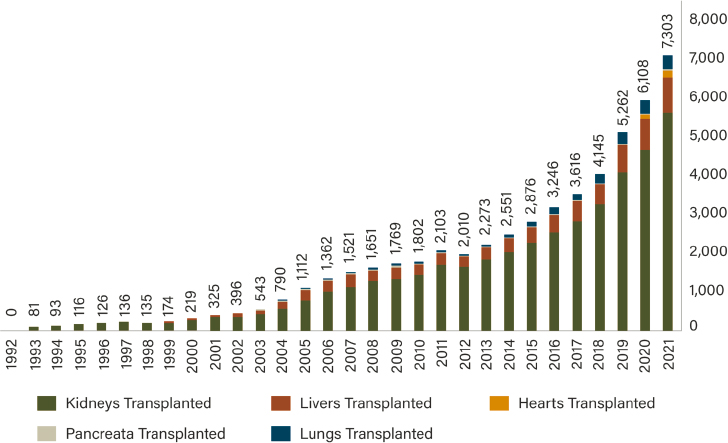
NOTE: Total DCDD transplants since 1992 = 53,844; total kidneys transplanted = 43,029; total livers transplanted = 7,856; total hearts transplanted = 327; total pancreata transplanted = 569; total lungs transplanted = 2,063.
SOURCE: Based on OPTN data as of January 10, 2022. https://optn.transplant.hrsa.gov/data/view-datareports/national-data (accessed January 10, 2022).
Figure 6-3 shows the considerable variation in the proportion of DCDD donors procured at each of the 57 OPOs in 2021,5 from a low of 11 percent to a high of 53 percent of all deceased donors within the OPO.
The committee’s analysis of SRTR data for 226 out of the 240 transplant centers that had complete data from 2019 to 2021 revealed significant variation in the likelihood of transplant with a DCDD kidney across U.S. transplant centers. A small but statistically significant increasing trend was observed in use of DCDD transplants (odds ratio = 1.16, 95% confidence interval = 1.13, 1.18, P < .0001); the overall observed percentages were 16.2 percent in 2019, 17.4 percent in 2020, and 19.9 percent in 2021.6
The likelihood that a donated kidney came from a DCDD donor ranges from 1 in 45 donated kidneys at low-performing centers to 1 in 1.4 donated kidneys at high-performing centers. As discussed later in this chapter, while the possibility of acceptance of DCDD kidneys is often discussed at listing, the rate at which a transplant center accepts and uses medically complex organs, such as DCDD, is not usually discussed or made transparent to patients and families at the time of listing. As evidenced by the variation in procurement and use of DCDD organs across the country, an individual’s access to a transplant can be greatly affected by the behaviors of the OPO and transplant center serving them.
___________________
5 On the OPTN website, LifeLink of Puerto Rico does not have a DCDD row and did not report any 2021 DCDD data. See https://optn.transplant.hrsa.gov/data/view-data-reports/national-data (accessed January 14, 2022). Saade et al. (2005) provides a brief history of donation and transplantation in Puerto Rico.
6 Based on committee analysis of OPTN data provided by SRTR; empirical Bayes estimates of the odds and 95% confidence intervals based on a mixed-effects logistic regression.
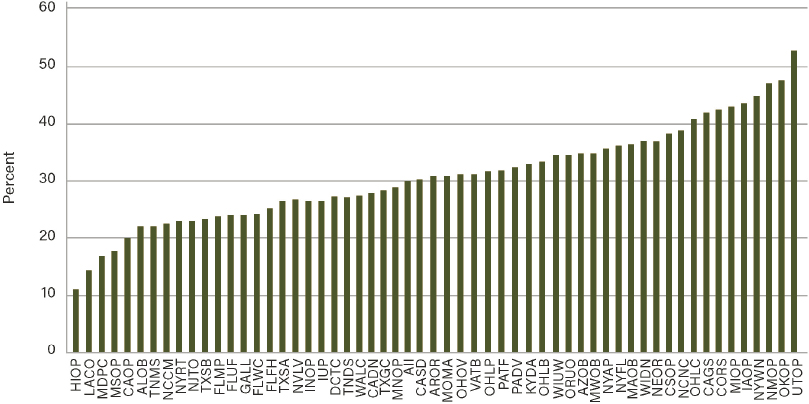
NOTES: All donation services donors n = 13,817. National average for all donation services areas in 2021 = 30 percent. DSA identifiers are identified by OPTN codes: the first two letters are the state where the OPO is headquartered, and the second two letters are related to what was submitted to CMS upon the original application. The full list of OPOs with key information can be found here: https://optn.transplant.hrsa.gov/about/search-membership/?memberType=Organ%20Procurement%20Organizations&organType=%27AL%27&state=0®ion=0 (accessed January 25, 2022). PRLL DCDD donor percentage is not included in this figure.
SOURCE: Based on OPTN data as of January 10, 2022. https://optn.transplant.hrsa.gov/data/view-datareports/national-data (accessed January 10, 2022).
Special Considerations of DCDD Organs
Outcomes following transplantation with organs from DCDD donors are much improved when compared to remaining on the transplant waiting list without access to an organ. However, there are increased care requirements, higher costs, institutional difficulties, and stigmas related to use of DCDD organs that also must be considered. For kidney recipients, DCDD kidneys are associated with higher rates of delayed graft function (temporary requirement of dialysis after transplantation) compared with donation after neurological determination of death (DNDD) kidneys (Kim et al., 2020; Lia et al., 2021; van der Windt et al., 2021). DCDD lung transplant recipients may have a higher rate of renal dysfunction following transplantation, which could add to hospitalization length and potentially cost (Verzelloni Sef et al., 2021). For liver transplant recipients, the use of DCDD organs has traditionally been associated with increased risk of ischemic cholangiopathy, a devastating diagnosis that can result in multiple procedures, hospitalizations, and ultimately retransplant. The rates of ischemic cholangiopathy seem to be decreased with use of normothermic perfusion, but data are still forthcoming. Similarly, DCDD heart transplant has occurred in the setting of normothermic perfusion. Each of these potential complications is associated with increased costs of patient care for the transplant center and increased morbidity for the recipient. Some of these negative outcomes are being mitigated by normothermic perfusion and new pumping and
perfusion approaches, but this technology is still novel and expensive (Padilla et al., 2021; Pearson et al., 2021). A new analysis of 136 individuals receiving heart transplants with DCDD hearts showed favorable outcomes and suggested an opportunity to increase adult heart transplantation volumes with DCDD hearts (Madan et al., 2022). Pagani (2022) notes that if DCDD heart transplantation continues to increase, clinical, economic, and ethical issues will need to be considered in order to construct a paradigm in which broader adoption of DCDD heart transplantation is possible. For example, the use of DCDD hearts will likely require changes in procedures and protocols for procuring these organs—including greater collaboration among thoracic and abdominal transplant procurement teams—as well as an increase in resources, as ex vivo perfusion equipment can cost $270,000, not including the time and materials required to use the console (Pagani, 2022).
Not only are transplant costs of care higher, there can also be higher costs for both OPOs and transplant centers in pursuit of DCDD donors. Not all DCDD donors have organs recovered because of variability in warm ischemic time, which leads to increased resource use for the OPO, and even the transplant centers pursuing these organs, potentially without any resultant organs. Additionally, while the committee feels strongly that every organ counts and is critical to pursue, DCDD donors yield fewer organs than DNDD donors, so the costs and efforts for recovery often result in fewer organs. Besides the direct costs to the OPO and transplant centers pursing the DCDD organs, there are added intangible burden and indirect costs from such things as staffing workload, administrative burden, and burnout that have not yet been comprehensively studied but may need to be considered (Kress et al., 2009). At the same time, there are OPOs and transplant centers that are successful high users of DCDD organs whose models should be shared, adapted, and used within the wider transplant community (see Chapter 7 for quality improvement initiatives). While there is the potential for increased costs to the patient, the transplant centers, and OPOs for procurement and use of DCDD organs, the pursuit and use of these organs is necessary to increase transplantation accessibility for all and improve patient outcomes.
Relationship Between DCDD and DNDD Organs
There are important differences between DCDD and DNDD organs that complicate their procurement, use, and transplantation. DCDD donation requires circulatory cessation within a defined period of time. Prior to the increase in extra-renal transplantation of DCDD organs, 60 minutes warm ischemic time was acceptable (Kotloff et al., 2015). That time frame has shortened to 20–30 minutes as longer periods of warm time have been demonstrated to affect transplant outcomes, especially in liver transplantation (Kalisvaart et al., 2021). Predictive tools have had variable success in assessing the probability of circulatory cessation within defined time frames.
Determining neurological death is complex as well, and DNDD accounts for only approximately 2 percent of adult and 5 percent of pediatric in-hospital deaths in the United States (Greer, 2021). As with DCDD donor potential, standardized assessment of DNDD potential based on hospital-level data would be beneficial to better understand donor potential for each pathway of donation. The committee discussed concerns that the growth in DCDD was not at the expense of DNDD donors, and that it is not unusual for a DCDD donor to progress to DNDD status during the evaluation period. Growth in the recovery of organs from DNDD donors is also possible while increasing the recovery of DCDD donors. Attention is warranted to ensure that increases in DCDD procurements do not decrease DNDD procurement volume.
Summary of DCDD Procurement and Transplantation
If the significant variations in DCDD procurement across the nation are not narrowed, there are life-threatening consequences for waiting recipients in the geographic areas served by low-performing OPOs and transplant centers with low use of DCDD organs. Overall system performance shows that the percentage of DCDD procured by the 57 OPOs of all deceased donors in 2021 was approximately 30 percent DCDD, and the highest-performing OPOs had approximately 53 percent of deceased donors from DCDD (see Figure 6-3). If all OPOs procured approximately 50 percent of donor organs from DCDD, it would be possible to double the number of DCDD donors overall to more than 6,000 donors, substantially increasing the supply of deceased donor organs for recipients on the waiting list. These key facts, together with the proven ability of the OPO and transplant community to achieve systematic improvement based on the experience of the highest performers in the system, inform the recommended national goals on DCDD outlined in Chapter 2. With the advent of normothermic perfusion of extra-renal organs in the last 3 years, utilization of livers, hearts, and lungs has increased and there are promising results for organ utilization and patient outcomes (Shah, 2021).
Opportunities to Improve Recovery of Other Medically Complex Organs
In addition to DCDD organs, there are opportunities and initiatives to improve the recovery of other medically complex organs that were once considered off-limits, including from older donors, hepatitis C donors, HIV-positive donors, and donors with COVID-19. Organ recipients and their clinicians have always had to carefully weigh the costs and benefits of accepting medically complex organs: understanding the risk–benefit ratio of accepting and transplanting a less than perfect organ must be assessed against the possibility of receiving no transplant at all (see section on shared decision making).
Older Donors
An area for opportunity and growth of the U.S. organ supply is ensuring recovery and use of organs that are donated from older donors. However, a recent review found that older donor age is associated with worse outcomes for liver, kidney, pancreas, heart, and lung transplantation; the donor age from which the negative survival effects start to become significant varies between organs (Dayoub et al., 2018). More organ-specific research on older deceased donors is needed. At the April 16, 2021 public webinar International Examples of Organ Procurement, Allocation, & Distribution,7 Axel Rahmel, of Deutsche Stiftung Organ Transplantation, presented Lessons from Eurotransplant and described a successful “old for old” program where donors above 65 are preferentially allocated to recipients above 65; additionally, Beatriz Domínguez-Gil, of Organización Nacional de Trasplantes, presented data on the average age of deceased donors in Spain, with more than 50 percent over age 60, more than 30 percent over age 70, and more than 9 percent over age 80 (see section on international lessons learned for more information).
___________________
7 See https://www.nationalacademies.org/event/04-16-2021/a-fairer-and-more-equitable-cost-effective-andtransparent-system-of-donor-organ-procurement-allocation-and-distribution-meeting-6 (accessed January 14, 2022).
Hepatitis C Donors
The notion of knowingly giving an organ from an infected donor to an immunosuppressed transplant recipient may initially seem unthinkable. However, increased understanding of the diseases caused by certain pathogens, as well as the availability of new drugs to treat or prevent infections, mean that these medically complex organs can now be used successfully. In recent years, organ recipients treated prophylactically with new, highly effective hepatitis C virus (HCV) medications were protected from infection after receiving organs from HCV-infected donors for kidneys, hearts, lungs, and livers (Bethea at al., 2021; Madhusoodanan, 2021; Woolley et al., 2019). Transplanting kidneys from donors infected with HCV into patients without the virus was shown to have promising outcomes in recent single-center and multicenter studies (Goldberg et al., 2017; Sise et al., 2020). Additionally, the opioid epidemic has correlated with an increase in the supply of deceased organ donors, many of them infected with HCV; further research on HCV-positive donors is an important opportunity for increasing access to organs, particularly kidneys, for transplantation by using organs that were not often used in the past.
HIV-Positive Donors
In transplant centers around the world, kidneys from deceased HIV-positive donors are increasingly being used for HIV-positive recipients, but the numbers are low. After they were pioneered in South Africa in 2008, surgeons have reported follow-up on 51 transplants. Since 2013, 25 have been reported in the United States (Thornton, 2021). Given advances in antiretroviral therapy, there are opportunities to explore transplanting HIV-infected organs to non–HIV positive recipients on the waiting list (Thornton, 2021).
Donors Positive for COVID-19
While longitudinal studies have not been conducted owing to the novelty of COVID-19, there has been some early success in transplanting otherwise healthy organs from SARSCoV-2-infected donors. One such study analyzed 10 kidney transplants from five deceased donors with new detection of SARS-CoV-2 RNA during donor evaluation in early 2021; with 8–16 weeks of follow-up, outcomes for all 10 patients and allografts had no signs or symptoms of donor-derived SARS-CoV-2 infection (Koval et al., 2021). More research is needed to understand the opportunities for organs transplanted from donors positive for COVID-19.
Conclusion 6-2: Opportunities exist to improve the recovery of medically complex organs from older donors, hepatitis C donors, HIV-positive donors, and donors positive for COVID-19. While there are also challenges in transplant center acceptance of these organs, the challenges are similar to DCDD in terms of OPO recovery of these organs.
Lessons from International Deceased Donor Organ Transplantation Systems
There are potential lessons to be gleaned from international deceased donor organ transplantation systems with a successful emphasis on equity. For example, Spain has implemented a comprehensive strategy to increase organ availability that may be instructive for improving organ availability in the United States (Matesanz et al., 2011). Spain’s
efforts include earlier referral of potential deceased donors to transplant coordination teams, benchmarking to identify success factors in donation after neurological death, family-based approaches and care methods for transplantation, and additional training for health care professionals (Matesanz et al., 2011). Other successful elements of the Spanish model include concerted efforts in professional training, active public outreach and engagement, and investment in infrastructure at the federal level. It has been proposed that a more aggressive approach to organ acceptance may benefit kidney transplant candidates in the United States.
A cohort study analyzing the use of deceased donor kidneys in the United States and France found that the kidney nonuse rate in the United States is nearly twice that of France (Aubert et al., 2019). Furthermore, a multicenter study of French donation centers found that donor kidney histology assessment, or biopsy, during allocation did not provide substantial incremental value in determining organ quality (Reese et al., 2021). Thus, the authors contended that many kidneys discarded in the United States owing to abnormal biopsies could instead be used to benefit patients on transplant waiting lists (see section on kidney biopsies for more information).
Conclusion 6-3: Greater than five-fold variation exists in the recovery of DCDD donors by OPOs across the country. Variation also exists in DCDD organ transplant rates by transplant centers across the country. Other nations transplant more DCDD donors than the United States with good outcomes. The committee concludes that an increase in the number of DCDD organs procured by OPOs, coupled with improved organ offer acceptance and use practices of transplant centers, would yield a significant number of organs for waiting candidates. With the innovation of ex vivo organ perfusion for liver, heart, and lungs, there is an increased opportunity to expand the donor pool with DCDD donation and increase the organs available that were not previously considered for transplant.
TRANSPLANT CENTER REGULATORY FRAMEWORK AND PERFORMANCE METRICS
Each of the approximately 250 transplant programs in the United States is subject to oversight by two federal entities. First, CMS has a long-term regulatory oversight perspective and the ability to decertify a transplant center if outcomes are not met.8 Second, the OPTN uses its committee structure and responsibility for implementing NOTA and the OPTN Final Rule to frequently consider data on transplant center performance and to take corrective actions for individual transplant centers if needed.
CMS Oversight of Transplant Centers
All transplant programs are housed within a hospital and since 2007 must comply with Medicare and specific hospital conditions of participation governing data submission, clinical experience, outcome, and process requirements for transplanting heart, lung, liver, kidney, pancreas, or intestine (CMS, 2020c). CMS relies on onsite evaluation of transplant programs, as well as data from the OPTN, to evaluate a transplant program’s compliance with Medicare requirements. Transplant programs are required to maintain patient and graft
___________________
8 CMS only has oversight over transplant programs that are certified for participation in Medicare. This is not a requirement, and there may be some transplant programs that are not certified by CMS. The OPTN has oversight over all transplant programs.
survival rates within CMS tolerance limits. In 2016, evidence indicated that transplant centers responded to the conditions of participation by removing sicker patients awaiting liver transplant to avoid harming the transplant center’s performance according to CMS standards. The study also found that conditions of participation did not significantly affect 1-year posttransplant mortality as intended (Dolgin et al., 2016). In 2016, CMS noted that “we are concerned that transplant programs may avoid using certain available organs that they believe might adversely affect the program’s outcome statistics” and revised its guidelines to broaden the acceptable “standard level” to include outcomes between 150 and 185 percent of the risk-adjusted expected number (CMS, 2016, p. 1).
OPTN Oversight of Transplant Centers
The OPTN also has a role in overseeing transplant programs and requiring corrective action as needed. The OPTN Membership and Professional Standards Committee (MPSC), operating on behalf of the OPTN Board, is responsible for monitoring OPTN member compliance with membership criteria, OPTN policies, and the 2020 Final Rule. The SRTR contractor provides statistical and analytical support to the OPTN, as well as support in areas such as policy formulation and evaluation, system performance metrics, and economic analysis (SRTR, 2022a). SRTR’s mission is to keep transplant programs, OPOs, policy makers, organ donors and families, and the public informed about the current state of solid organ transplantation in the United States. This is in alignment with the Final Rule, which states that the OPTN and SRTR “make available to the public timely and accurate program-specific information on the performance of transplant programs” and identify transplant programs and OPOs with better or worse outcomes.9
SRTR developed a five-tier outcome assessment system to present pre- and posttransplant performance metrics to make it easier for the public to understand and compare the outcomes of different transplant programs (SRTR, 2022b). Assessments are presented for three metrics: (1) survival on the waiting list (i.e., waiting list mortality rate), (2) getting a transplant faster (i.e., transplant rate), and (3) 1-year organ survival (i.e., first-year graft survival) (SRTR, 2022b). The SRTR performance assessment methodology calculates center performance for each statistic, producing a program score between 0 and 1 that is converted to one of five tier assignments, with higher scores and tiers indicating likely better performance (SRTR, 2022b). Transplant program-specific reports and OPO-specific reports are produced semiannually. CMS and the OPTN MPSC use the SRTR performance assessment methodology for 1-year organ survival to review transplant program performance (Kasiske et al., 2016).10
Incentives in Transplant Center Performance
It is the committee’s belief and experience that transplant providers intend to act in the best interests of their patients to review organ offers, accept the best organ for that patient, and perform a successful transplant. As indicated above, there is evidence to suggest that some transplant providers might be rejecting good organ offers that could benefit the recipient because of a reluctance to perform riskier surgeries (meaning procedures with either
___________________
9 OPTN Final Rule 121.11(b)(iv), 2021.
10 New transplant center performance metrics were approved by the OPTN Membership and Professional Standards Committee with implementation planned to begin in June 2022. See Chapter 7 for additional information, as well as https://optn.transplant.hrsa.gov/media/yctffgt2/20211206-bp-mpsc-enhnc-tx-prgrm-prfrmnc-mntrng-syst.pdf (accessed February 15, 2022).
medically complex organs or less than ideal patients) for fear it could damage the transplant center’s statistics (Yasinski, 2016). As discussed earlier in this report, the OPTN oversight mechanisms for the organ transplantation system begin only at the time a patient is added to the waiting list. As one component of the system, transplant centers are currently only accountable for the patients that receive a transplant.
The current five-tier assessment system for transplant centers creates incentives and associated behaviors of transplant centers that are inconsistent with the Final Rule. If transplant programs are evaluated in terms of maximizing waiting list survival and 1-year organ survival, they will be incentivized to only accept what they believe to be the highest-quality organs and list the least severely ill patients. While this behavior may result in increased performance according to 1-year posttransplant survival, it will result in decreased survival benefit for patients who remain on the waiting list compared to receiving a transplant. Transplantation of more medically urgent patients who have decreased waiting list survival, yet still have excellent posttransplant survival, could save more lives. There is also concern that the current transplant center performance metrics will lead to increases, or at least not decreases, in the already high organ nonuse rate, and continued lack of equity for minority populations who, for example, have twice the accrued dialysis time upon entry to the waiting list.
Although CMS no longer uses 1-year posttransplant survival for either the patient or the graft as a metric for transplant center certification, publicly available data on transplant center performance relies heavily on this statistic (Yasinski, 2016). Every 6 months, the SRTR releases a publicly available assessment of each transplant center in the country, using 1-year posttransplant survival rates for patients or grafts as a key metric (Yasinski, 2016). However, the difference between performance tiers for transplant programs is often just a single point or two.
Some suggest that the current incentives for transplant centers push providers to keep older, sicker patients off the waiting list even if they would benefit from transplant, because transplanting these patients could be riskier than transplanting younger, healthier patients. Another way to correct poor performance ratings under the current system is for a transplant center to dramatically reduce the number of transplants performed. Reducing the number of transplants can increase posttransplant survival rates and therefore the center’s rankings, allowing the center to remain in business. However, this approach limits access to lifesaving transplants to patients that a transplant center would have treated just a year or so before.
Conclusion 6-4: The organ transplantation system is not accountable to all patients who need an organ transplant. A shift is needed toward policies that engender accountability to all patients in need of a transplant.
Conclusion 6-5: There is a need to create new performance metrics for transplant centers that go beyond one-dimensional evaluations of 1-year patient and graft survival. There is an opportunity to further improve transplant center performance metrics in order to capture factors that are critically important to patients, such as time waiting before transplant, likelihood of survival on the waiting list prior to transplant, and overall added benefit of the transplant in terms of survival over remaining on the waiting list. There is also a need for an independent assessment of any proposed performance metrics before adoption by the government, which would include a focus on equity in access to transplant referral and evaluation, as well as equity in access to transplant once evaluated and added to the waiting list.
KEY AREA FOR IMPROVEMENT FOR TRANSPLANT CENTERS: ORGAN USE
As noted throughout this report, the organ donation and transplantation system in the United States is the largest and most sophisticated system of its kind in the world. Countless hours and resources are expended by thoughtful and dedicated professionals to ensure compliance with NOTA and the Final Rule, to create organ allocation policies that are based on sound medical judgment, to seek to achieve the best use of donated organs, and to aim to achieve equitable allocation of organs among patients through distribution over as broad a geographic area as feasible and in order of decreasing medical urgency.11 Using the combination of donor and candidate information, the OPTN computer system generates a “match run,” which is a rank-order list of candidates to be offered each organ that is unique to each donor and each organ (UNOS, 2021a). The candidates who appear highest in the ranking are those who are in most urgent need of the transplant, and/or those most likely to have the best chance of survival if transplanted. While this process is well defined by policy, the actual acceptance and transplantation of an available organ to a recipient is much more complicated.12
The successful treatment of end-stage organ failure through transplantation continues to fuel demand for deceased donor organs, with the waiting list outpacing the number of transplants performed. However, in practice, many recovered organs are not used (SRTR, 2021). SRTR data show that in 2019, 14.3 percent of all recovered organs were not transplanted, an increase from the 13.2 percent reported in both 2017 and 2018 (Israni et al., 2021). There has been little movement in improving overall nonuse of recovered organs, and in 2019, 4,460 kidneys, 345 pancreata, 874 livers, 5 intestines, 31 hearts, and 338 lungs were not used compared to lower numbers in 2018—3,755 kidneys, 278 pancreata, 707 livers, 3 intestines, 23 hearts, and 317 lungs were procured but not transplanted (Israni et al., 2021). Thus, the nonuse problem is increasing in severity.
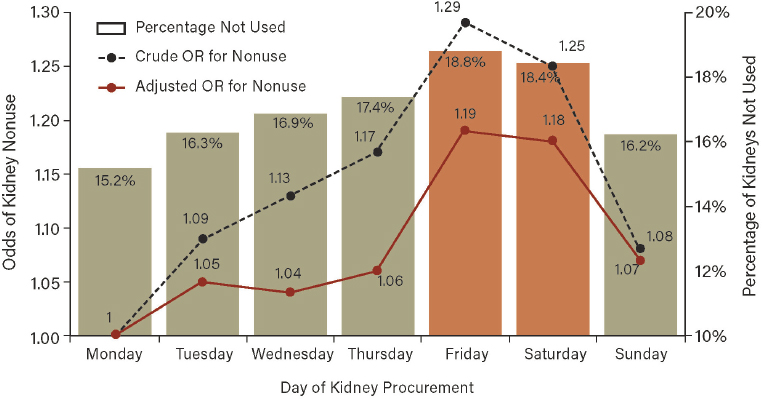
Compounding the problem of nonuse of organs is the size of the waiting list. The waiting list for kidneys is six times longer than the number of transplants performed, the liver waiting list is three times longer than the number of transplants performed, and the heart and lung waiting lists are double the number of transplants performed (OPTN, 2021a). Combining the year over year increase in the nonuse of recovered organs with organ demand exceeding supply, there is significant room for improvement in this area, especially in regard to kidneys, which represent 84.7 percent of the waiting list in February 2022.13 As of September 2021, the proportion of kidneys from deceased donors that were recovered for transplant but ultimately not transplanted remains at approximately 20 percent (OPTN, 2021a; Stewart et al., 2017), with a projected 2021 rate of 23 percent (see Figure 6-4). This is representative of an upward trend, with a 91.5 percent increase in nonuse of deceased donor kidney between 2000 to 2015, despite organ quality remaining stable (King et al., 2021; Mohan et al., 2018).
___________________
11 63 FR 16332 Apr. 2, 1998, see https://www.ecfr.gov/current/title-42/chapter-I/subchapter-K/part-121 (accessed January 27, 2022).
12 Patients and members of the public consider placement on the transplant waiting list to be an implicit promise of fair, unbiased treatment under a transparent allocation scheme; current practice may not be living up to that promise in a variety of ways (Segev et al., 2008).
13 As of February 3, 2022, there were 90,315 candidates waiting for a kidney transplant out of a total of 106,616 candidates waiting for any type of organ transplant. 90,135/106,616 = 84.7 percent. https://optn.transplant.hrsa.gov/data/view-data-reports/national-data (accessed February 3, 2022).
As depicted in Figure 6-4, the nonuse of organs has increased, even as OPOs increased the number of donors over the same period (Mohan et al., 2021; OPTN, 2021a). This increase in nonuse of kidneys has sometimes been attributed to risk-averse behavior by transplant providers worried about the effect of transplanting medically complex organs, or concern over the effect of transplanting sicker patients, on the transplant center 1-year posttransplant survival metric. Although a factor, this explanation alone does not justify the variation seen in organ use and acceptance practices across transplant centers.
Mohan et al. (2021) reviewed data from 2000 to 2015 that confirmed an overlap in the quality of kidneys that are transplanted with those that are not used (Figure 6-5). While the nonuse of some kidneys may be unavoidable, the data suggest there are opportunities to facilitate increased use. Nonused kidneys are most likely to come from older, higher body mass index, black, female donors with comorbidities of diabetes and hypertension. The organ nonuse rate for livers increased from 8.6 percent in 2018 to 9.6 percent in 2019, driven by increased nonuse of grafts from donors aged 55 years or older and, to a lesser extent, those of donors aged 30–54 years. Livers recovered from DCDD donors remained four times more likely to not be used than livers recovered from DNDD donors (29.9 percent versus 7.1 percent, respectively) (Kwong et al., 2021; SRTR, 2019).
Conclusion 6-6: Two facets of the organ transplantation system are in tension. Priority on each organ waiting list is based on formal, publicly announced policies, and organs are allocated by match-run algorithms; on the other hand, a patient’s access to an organ offered depends on how the transplant professionals in the program caring for the patient exercise the discretion that the system gives them regarding when to accept or reject an organ for transplantation. This divergence—which is not transparent either to the general public or to all patients on the waiting list—has implications for equitable treatment of all patients, for adherence to the ethical principles of autonomy and beneficence, and for trust in the system.

SOURCE: Mohan et al., 2021.
NOTE: 2021 rate is based on annualized OPTN data projected based on the first 8 months of 2021.
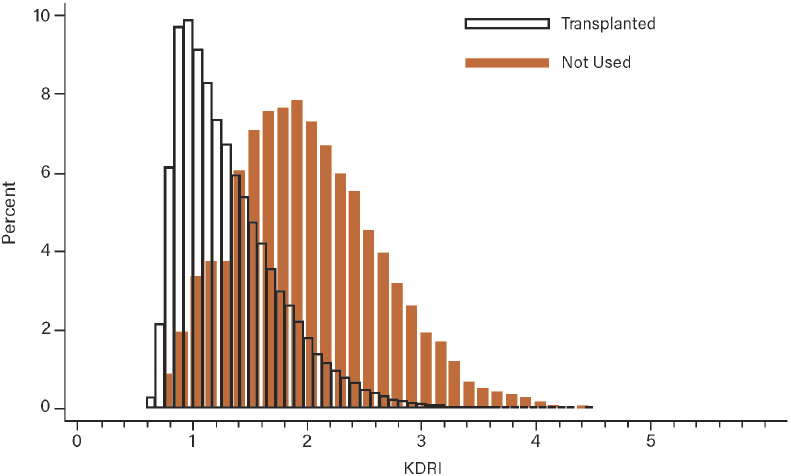
NOTES: Percentage is calculated using data from 2000 through 2015. KDRI = kidney donor risk index.
SOURCE: Mohan et al., 2018.
The Challenges of Use and Reasons for Nonuse
Policy prescriptions—administrative or organizational solutions within transplant programs—must mitigate against the ongoing increase in nonuse (King et al., 2019), and waiting patients should be informed of operational factors that are not related to organ supply that may affect their access to organs. There are numerous factors that may affect nonuse that are touched on briefly below.
Donor Quality
Donor quality alone cannot explain the steady increase over time in the organ nonuse rate. Using a donor utilization index, Brennan et al. (2019) assessed 182 transplant centers’ use practices with kidneys perceived as having a high risk from 2010 to 2016, and found that there was significant variation by OPTN region, revealing geographic trends in kidney use and nonuse. Similarly, an examination of regional changes in donor heart acceptance patterns found differences in acceptance and use patterns by geographic area, and suggested that these variations may reflect differences between transplant centers’ willingness to accept donor hearts with higher risk,14 differences in OPOs’ cardiac evaluation and allocation practices, or a combination of both (Khush et al., 2015). When all organ allocation and distribution policies are fully migrated to the continuous distribution model, it will be
___________________
14 In June 2020, the Centers for Disease Control and Prevention published a U.S. Health Service Guideline stating a change in terminology from increased risk donor to risk criteria present for acute HIV, HBV and HCV infection. See https://www.cdc.gov/mmwr/volumes/69/rr/rr6904a1.htm?s_cid=rr6904a1_w (accessed February 15, 2022).
important to continue monitoring the weight of the effects on organ acceptance and nonuse rates of policies not grounded in geography.
Transplant center size and regional competition may affect the variability of the nonuse rate. Volk et al. (2011) found that the transplant centers performing the most transplants and those with competing centers in their OPO were more likely to use increased risk organs,15 particularly among recipients with lower Model for End-Stage Liver Disease (MELD) scores. Transplant centers using increased risk organs had equivalent waiting list mortality rates but tended to have higher posttransplant mortality. Future research on assessing the variabilities of nonuse rates across transplant centers, as well as potential interventions, is needed.
While the problem of demand exceeding the supply is a global issue, the deceased donor kidney nonuse rate in the United States is high relative to other similarly developed countries (Mohan et al., 2018; Stewart et al., 2017). By comparison, the nonuse rate in the United States is nearly twice that of France (Aubert et al., 2019). In fact, in a 2019 study, researchers found that 62 percent of kidneys not used in the United States would be successfully transplanted in France (Aubert et al., 2019). Sometimes, selectivity can also be a reason for organ nonuse rates. Li et al. (2021) reviewed the use of kidneys during the COVID-19 pandemic in 2020 and found that transplant centers that continued transplantation during the first surge used lower Kidney Donor Profile Index (KDPI) kidneys, while allowing the nonuse rate to rise. However, some of the high nonuse rate in the United States could be skewed by the common practice of recovering organs before obtaining transplant center acceptance. This is contrary to practices in areas such as the United Kingdom where “recovering [an organ] is conditional on acceptance. Hence, the United Kingdom discard rate reflects post-acceptance dynamics whereas U.S. [nonuse] rates reflect possibilities as well as kidneys that were recovered but not accepted by any U.S. transplant center” (Ibrahim et al., 2020). In the United States, donor hearts are not recovered until accepted for transplant, while kidneys are often recovered without acceptance for transplant and sometimes before the offers are sent to transplant centers. This could be an explanation for why nonuse rates are lower for hearts than other organs in the United States.
Organ Biopsies
Mohan et al. (2018) analyzed the reported reasons for nonuse in over 36,000 kidney offers from 2000 to 2015, and “biopsy findings” made up 38 percent of responses, making it the most commonly cited reason for nonuse. Other commonly cited reasons for nonuse include
- “no recipient located,” meaning an OPO was unable to find a willing transplant center to accept the organ (15 percent);
- “poor organ function” (10 percent);
- “donor history” (8 percent);
- “anatomical abnormalities” (7 percent); and
- “organ damage” (4 percent).
For over 20 years, biopsies have been the most frequently cited reason for kidney nonuse, accounting for one-third of all kidneys not used (Stewart et al., 2017). There is growing evidence that biopsies may not significantly augment the prediction of outcomes beyond
___________________
15 The phrase increased risk refers to the donor characteristics that could place the potential recipient at increased risk of disease transmission. See https://optn.transplant.hrsa.gov/governance/public-comment/guidance-on-phs-increased-risk-donor-organs (accessed February 15, 2022).
estimates using clinical criteria (e.g., age and KDPI) (Reese et al., 2021). This is a growing concern given that over 50 percent of all kidneys removed for transplant undergo biopsy. Lentine et al. (2021) called for a randomized controlled trial of biopsy use to determine if and when a procurement biopsy should be used in the decision to accept or decline an organ offer. The OPTN’s Kidney Transplantation Committee has approved a Donor Criteria to Require Kidney Biopsy proposal for public comment in early 2022 (OPTN, 2021b).
In a retrospective study of prospectively collected data from the UNOS Standard Transplant Analysis and Research database, Steggerda et al. (2020) reviewed biopsies from deceased organ donors between 2006 and 2015 in order to consider higher macrosteatosis thresholds for liver transplantation. While it was a limited study, the results were able to identify a threshold macrosteatosis level for safe transplantation and characterize the donor and recipient factors that contribute to short- and long-term graft survival among steatotic allografts in the modern transplant era.
Health Care Use and Organizational Issues
There are organizational and systemic factors that extend beyond organ quality that appear to also be contributing to the high rate of nonuse of deceased donor organs in the United States.
Weekend Effect of Nonuse
There has been compelling research on the “weekend effect” for kidneys and livers. In SRTR data from 2000 to 2013, and compared with weekday kidneys, organs procured on weekends were significantly more likely to not be used (odds ratio: 1.16; 95% confidence interval: 1.13–1.19), even after adjusting for organ quality (adjusted odds ratio: 1.13; 95% confidence interval: 1.10–1.17) (see Figures 6-6 and 6-7) (King et al., 2019; Mohan et al., 2016). Program structure and staffing, particularly during weekends and in smaller programs,
NOTE: OR = odds ratio.
SOURCE: Mohan et al., 2016.
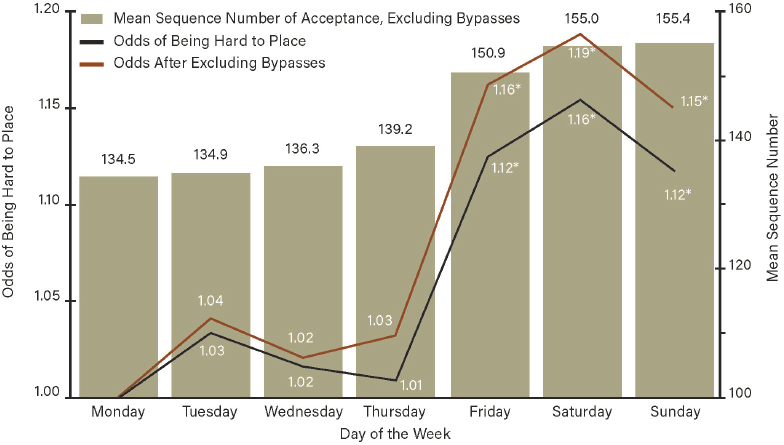
NOTES: Day of the week refers to the day of the first offer for the kidney. Automatically bypassed offers are not included in the “excluding bypasses” calculations. Compared with kidneys offered on Mondays, kidneys offered on Fridays, Saturdays, and Sundays had a higher mean sequence number of accepted offer and adjusted odds of becoming a hard-to-place kidney (reference is Monday; adjusted for Kidney Donor Profile Index). P ≤ .001.
SOURCE: King et al., 2019.
affects kidney use and ultimately affects a patient’s chances of receiving a transplant (King et al., 2019). This is unacceptable for a lifesaving surgical procedure such as transplantation.
Carpenter et al. (2019) observed that livers available for likely-weekend transplants were 11 percent more likely to be not used than their weekday counterparts, despite no differences in organ quality. This effect size was consistent and remained even after adjusting for other variables relating to donor, organ, and other factors. Rates of liver biopsy, macrosteatosis on biopsy, HCV-positive seropositivity, and donor risk factors were similar for both weekend and weekday transplants (Carpenter et al., 2019).
Operations Management
Contributing to the “weekend effect” are hospital surgical scheduling and flow challenges where an entire science of operations management would help alleviate this universal issue. Systematic attention to operations management issues in nurse staffing, availability of rooms for surgical procedures, and availability of hospital beds posttransplant require collaboration and process change across the entire hospital enterprise. Litvak et al. (2021) describe an effective strategy to improve hospital efficiency, the quality of care, and timely access to care for emergent and urgent surgeries by classifying the time and resource needs of surgical patients and smoothing the flow of surgical admissions over all days of the week.
When organ nonuse is attributed to hospital operational management limitations rather than clinical quality or patient readiness, the result is a less equitable, less transparent, and less efficient organ transplantation system.
Conclusion 6-7: Nonuse of organs is higher on Fridays, Saturdays, and Sundays. This weekend effect can be mitigated through appropriate planning and surgical scheduling management, including issues related to nurse staffing, availability of hospital beds for patients receiving a transplant, and the availability of surgical units.
The science of operations management has been used successfully to smooth surgical scheduling and better manage flow in multiple hospitals, including the Mayo Clinic of Florida, Boston Medical Center, Cincinnati Children’s Hospital Medical Center, and Toronto’s University Health Network (Litvak et al., 2021; Ryckman et al., 2009; Smith et al., 2013). This method requires first separating hospital resources (e.g., operating rooms) used for elective and unscheduled procedures and then ensuring that similar numbers of elective admissions occur in different hospital wards each day (Litvak and Fineberg, 2013).
Implementing proven processes to smooth surgical scheduling makes it possible for hospitals to have operating rooms, surgical staffing, ICU rooms, and other resources available to systematically deal with urgent, unscheduled surgeries when they arise (Litvak and Fineberg, 2013). Offers of lifesaving organs on Fridays, Saturdays, and Sundays provide a compelling example of the need for hospitals to properly plan for and ensure the availability of surgical capacity. A number of strategies to implement surgical schedule smoothing across hospitals with transplant centers could be used, including but not limited to systematic quality improvement to spread this known best practice; financial or payment incentives to hospitals that use these methods to ensure access to lifesaving, urgent surgical procedures such as transplants; and Conditions of Participation and/or Interpretive Guidelines by CMS surveyors to ensure that hospitals are properly managing surgical schedules to ensure access to emergency surgeries like transplants. In addition to ongoing commitment from hospital leaders, regulatory systems will need to support efforts to keep hospitals from overcrowding and improve patient morbidity and mortality (Kelen et al., 2021).
Not only does hospital flow affect the scheduling of organ transplants, it can also affect the timing of the organ donor procurement surgery. It is not uncommon for organ donor cases to be “bumped” to accommodate trauma or elective surgeries. The delay in the surgical recovery of deceased organs can lead to deterioration of organ function, making the organ less likely to be transplanted. An innovative solution for organ recovery are OPO-managed donor care units that do not depend on surgical suite availability and that offer improved transplant outcomes (see section on donor care units later in this chapter).
Waiting List Management
Organ transplant waiting list management has become increasingly complex across all organ types, but especially in the kidney population. Large transplant programs report upwards of 1,000 or more kidney patients on their waiting list, underscoring the importance of assessing for transplant readiness, communication of waiting list status, and patient education. Husain et al. (2018) found that in the years 2008 through 2015, between 14 and 20 percent of deceased donor kidneys that were eventually transplanted were first offered to one or more deceased candidates, contributing to less efficiency in the process of organ offers, and perhaps contributing to organ nonuse. Understanding that kidneys are offered to
deceased individuals on the waiting list is exactly the type of situation that undermines public trust in the organ transplantation system.16 See Chapter 5 for more information.
KEY AREA FOR IMPROVEMENT FOR TRANSPLANT CENTERS: ORGAN OFFER ACCEPTANCE
The U.S. organ transplantation system was built and designed primarily to maximize the ability of transplant centers and surgeons to exercise choice in accepting and transplanting organs. As stated earlier in this chapter, the system is perfectly designed to achieve the results it gets. For example, currently less than 1 percent of kidney offers are accepted (0.76 percent) (SRTR, 2021). Over 1.5 million offers were made to place the approximately 23,000 kidneys transplanted in 2019 (SRTR, 2021).
Understanding and improving variation in the acceptance of offered organs can decrease the nonuse rate if offers are purposefully made to programs likely to accept them. Standardizing and spreading best practices and improving allocation system efficiency will lead to a more fair, equitable, and transparent system. These opportunities are more fully outlined in Chapter 2 on goal setting and in Chapter 7 on quality improvement.
Each organ is “offered” to multiple transplant centers based on the formalized allocation systems previously designed and discussed in Chapter 5. The offers for a single organ are sent out sequentially based on a patient-by-patient basis to the transplant center where the patient is listed for transplant.
At the time of the organ offer, a transplant center assesses both the organ and the patient and determines if the organ is suitable for transplant for that patient at that moment at that center. A center can decline or accept an organ for each of its eligible patients in the sequence determined by the match run, or it can decline for all patients at their center. Reasons for offer declines are often multifactorial and are denoted by the center using refusal codes (discussed in detail below). The code categories include donor and candidate matching, organ specific, candidate specific, histocompatibility related, disease transmission risk, donor specific, and logistics, among other reasons (UNOS, 2021b). Like organ nonuse rates, the acceptance rates of organ offers vary significantly across transplant centers, and while the data are well documented, the behaviors that influence the decision-making process of accepting or declining an organ offer are less transparent and not well understood. The goal of allocation policy is to identify the best candidate for that organ and to have the transplant occur in a timely and efficient manner. Transplant centers receive many primary offers of organs for candidates on their waiting lists, and the offer may or may not be the best organ for that particular patient. There are significant data showing wide variation in acceptance rates across all organ types that result in inefficiency, potentially increasing the rates of nonused organs. Additionally, most of the primary organ offers are not accepted (Wolfe et al., 2007).
Mohan et al. (2021) present data that show the variability of nonuse that directly affects the probability of getting a kidney transplant within 3 years, and SRTR data confirm the variation in organ offer acceptance rates across all organs (King et al., 2020). This type of variation in performance across transplant centers results in severe consequences for those on waiting lists, including death. Organ offer acceptance ratios vary by more than 400 percent for kidneys, with similar levels of variation for other organ types (see Figure 6-8).
___________________
16 This text was modified after release of the report to clarify the findings of the study by Husain et al. (2018).
Variation in offer acceptance practices across transplant programs is larger than variation in other transplant program performance metrics, such as first-year outcomes, 3-year outcomes, waiting list mortality rate, or transplant rate. SRTR data suggest that there are programs accepting offers at rates about 80 percent lower than expected (ratios below 0.2), while other programs accept at rates 3.5 to 6 times the expected rate. These variations in organ offer acceptance practices reveal major differences in transplant center organ acceptance behavior, which impacts equitable access to transplant for waiting patients and can impact the efficient placement and ultimate acceptance of available organs. Figure 6-8 below details the variation in offer acceptance rates for all organ types, even after SRTR adjustments in the rates to account for differences in characteristics of candidates on their waiting list, quality of the offered organ, and geographic factors.
Choi et al. (2020) found that the rate at which U.S. heart transplant centers accepted a first-rank offer for a candidate on their waiting list varied significantly from 12.3 to 61.5 percent, with lower organ offer acceptance rates being associated with an increased risk of waiting list mortality. Additionally, another study observed marked variability in center practices regarding accepting livers allocated to the highest-priority patients, and that patients’ odds of dying on the waiting list without a transplant were significantly increased by center-level decisions to decline organs (Goldberg et al., 2016). Mulvihill et al. (2020) also found that among 65 transplant centers, organ offer acceptance rates for lungs varied significantly, from 9 to 67 percent.
King et al. (2020) found geographic disparities in rates of kidney transplantation and concluded that practices in transplant centers versus differences in local organ supply and
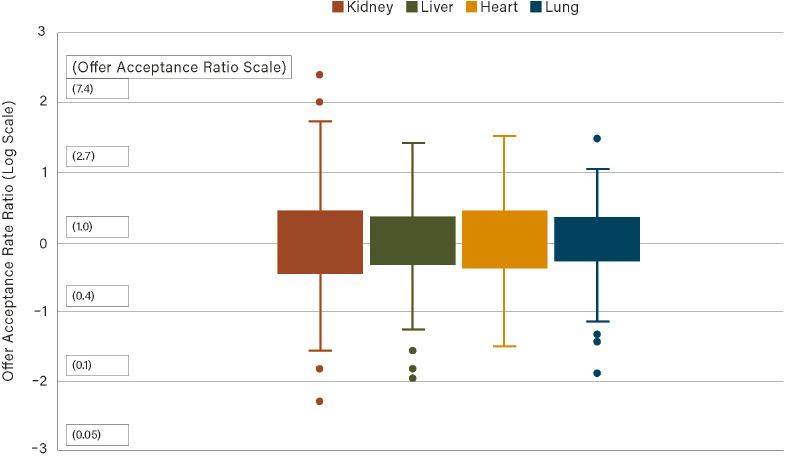
NOTE: The boxplots describe variation in offer acceptance practices within kidney, liver, heart, and lung transplant programs. Variation generally ranges from offer acceptance rate ratios of approximately 0.10 (90% lower offer acceptance rate than expected) to a high of approximately 5 (400% higher offer acceptance rate than expected). Offers between January 1 and December 31, 2020, were evaluated.
SOURCE: Scientific Registry of Transplant Recipients. Request for Information. Requested on October 5, 2021.

NOTES: Probabilities are for the average patient (man, nonblack, PRA < 98%, no diabetes, nonobese, mean age and dialysis vintage at listing in the region). Each dot represents one center, and each color outline represents one OPTN region. Gray bars represent the 95% confidence intervals around each center’s probability. Nationwide PrTx is the probability of deceased donor transplant within 3 years for all kidney transplant candidates in the United States added to the waiting list in 2015 in a national model.
SOURCE: King et al., 2020.
demand are unclear. Figure 6-9 compares the probability of receiving a deceased donor kidney transplant within 3 years of waiting list placement across centers. The variation is across all centers in the United States with a 16-fold variance between centers. Waiting patients at transplant centers with low offer acceptance rates have only a 4 percent chance of getting a transplant within 3 years. Conversely, patients waiting at transplant centers with high offer acceptance rates have a 65 percent chance of getting a transplant within 3 years (King et al., 2020). This is an inequitable and unacceptable level of variation in behavior and performance. Additionally, Figure 6-10 illustrates an up to 10-fold variation existing between transplant centers working with the same local organ supply (King et al., 2020). The authors suggest that large disparities between centers for likelihood of receiving a timely transplant may be related to center-level practice variations rather than geographic differences in underlying organ supply or patient case mix (King et al., 2020). These data challenge the conventional wisdom that variations in organ supply are the principal reason for geographic inequities in the ability of patients to get a transplant; instead, it points to the conclusion that the variations are largely a function of transplant center offer acceptance practices. As significant differences exist in the decision to accept an organ for transplant, standardizing center-level offer acceptance practices to the levels
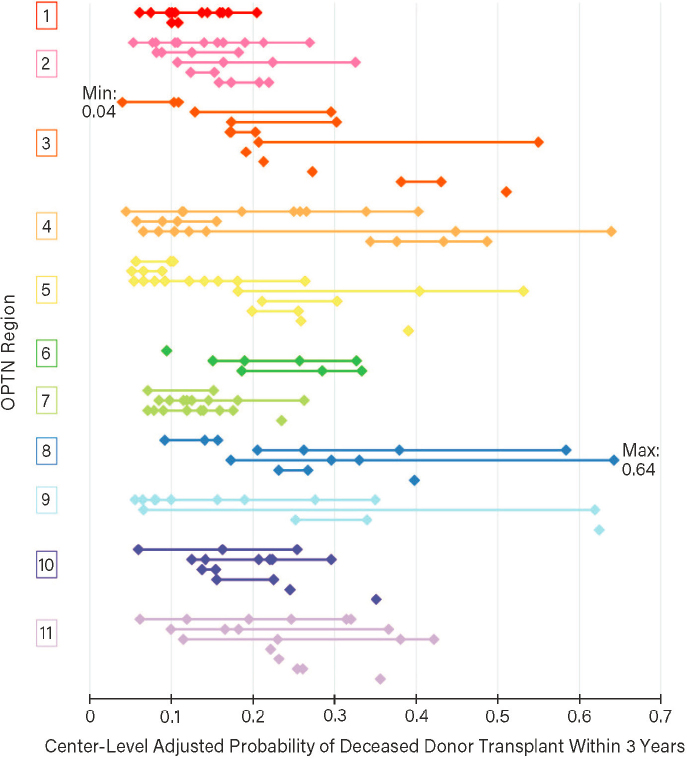
NOTES: Each point represents one transplant center, and each level along the y axis represents one of the 58 DSAs, grouped by OPTN region. Each horizontal line illustrates the range in probability of transplant between centers in a given DSA. DSA = donation service area.
SOURCE: King et al., 2020.
achieved by high-performing centers through further intervention has the potential to minimize waiting list mortality.
On average, patients who die waiting for a kidney had offers for 16 kidneys that were ultimately transplanted into other patients, indicating that many transplant centers refuse viable kidney offers on behalf of those on the waiting list (Husain et al., 2019).
It is important to note that programs have the option to apply broad organ offer filters (see section that follows on organ offer filters), ensuring that they do not receive organ offers that they believe they will not use. These programs do not get offers for organs in the filtered category for any of their patients. Programs applying filters may have higher organ offer acceptance rates than programs not utilizing filters because the “filtered”
offers are not used in calculations of organ offer acceptance rates. Therefore, organ offer acceptance rates may not fully reflect accessibility to organs for patients on the waiting list at a particular center. As more organ offer filter options are developed, the interplay between filters, organ offer acceptance rates, and patient outcomes should be further evaluated.
Understanding Organ Offer Tools
Refusal Codes
Selectivity can be a reason for organ nonuse rates, and better information will inform understanding of the low rates of organ offer acceptance. The OPTN Final Rule requires transplant programs to provide the OPTN with “reasons for refusal” of organ offers made to candidates registered at their programs. The OPTN Policy 18.3, Recording and Reporting the Outcomes of Organ Offers,17 accordingly requires these reasons to be reported to the OPTN. Based on community feedback that codes from 2004 were outdated, too vague, and required clarification, new codes went into effect in December 2021. By providing more relevant and granular options, the insights gathered will improve upon the current list by reducing the overuse of the refusal code “donor age or quality,” which accounted for 66 percent of the primary refusal reasons entered between July 2019 and June 2020.18 These new codes are intended to provide better data for quality improvement, for retrospective reviews, and for deciding in real time whether to accept or decline an organ. The utility of the codes for these purposes depends upon transplant centers accurately reporting the reasons they refused the offered organ.
Organ Offer Filters
Organ offer filters were first introduced by the OPTN in 2007 as a way to increase the efficiency of organ placement and to reduce the number of nonused kidneys. The concept was operationalized as a voluntary project where filters allowed a transplant center to screen out donor characteristics that would have little likelihood of being accepted for transplant, either for an individual patient or their entire waiting list. Filter settings include a broad range of characteristics, including medical history, intravenous drug use, age, history of diabetes, cold ischemia time, and pathway for determination of death (DCDD vs. DNDD).
In an analysis of organ offer filters from 2007 to 2019 in 175 kidney programs, King et al. (2022) noted that centers demonstrate a “fear of missing out” that has created less efficiency in the system, with very few centers having both restrictive filter settings and high offer acceptance. Over time, there has been an increase in the consideration of donors with a history of IV drug usage; however, more centers are unwilling to consider HCV+ donors, despite evidence in the safety of using these organs (see section on hepatitis C donors).
There are opportunities for refinement as current organ offer filters are not optimized to the fullest extent to increase organ allocation efficiency (Mohan et al., 2021) (see Box 6-3). In addition to whether a kidney transplant center optimizes the tool in organ
___________________
17 See https://optn.transplant.hrsa.gov/media/4639/update_to_refusal_codes_mini-brief.pdf (accessed January 14, 2022) and 42 C.F.R. §121.7(b)(4).
18 Based on OPTN data as of September 18, 2020. See https://optn.transplant.hrsa.gov/media/4639/update_to_refusal_codes_mini-brief.pdf (accessed February 16, 2022).
acceptance practices, how the tool is structured and collected is not synchronized with available data analysis files, making it more difficult to understand how settings may impact actual transplant outcomes. The ability for a transplant center to bypass organ offers also raises the question about the variability in access to transplant for patients on the waiting list.
Expedited Placement of Organs
Expedited placement can reduce delays in allocation by routing less-than-ideal organs to transplant centers with a proven willingness to use these organs (Mohan and Schold, 2021). Under the current system expedited placement (sometimes called “accelerated placement” or “out-of-sequence” allocation) allows an OPO to indicate exceptional circumstances in order to deviate from the policy-mandated match run that dictates patient priority for organ offers on the waiting list. When there are suboptimal donor characteristics related to donor disease or recovery-related issues, OPOs may turn to this discretionary tool of expedited placement to avoid nonuse of the organ (Giorgakis and Mathur, 2020; King et al., 2022). Expedited organ placement has been an important tool in organ allocation for many years as it allows OPOs to quickly place organs they believe are at risk of not being used for transplantation.
The committee heard testimony from international programs that have successful expedited placement strategies.19 For example, both the Eurotransplant rescue allocation system
___________________
19 See https://www.nationalacademies.org/event/04-16-2021/a-fairer-and-more-equitable-cost-effective-andtransparent-system-of-donor-organ-procurement-allocation-and-distribution-meeting-6 (accessed February 16, 2022).
and the UK Kidney Fast Track Scheme incorporate considerable flexibility for participating centers and have resulted in more than 50 percent of the organs that enter these pathways being transplanted (Callaghan et al., 2017).
While expedited placement can increase the use of organs, the necessary policy development and practice improvements to support expedited placement have generally lagged. Results remain to be evaluated for an expedited liver placement policy that went into effect in March 2021, providing guidance for OPOs and transplant centers, and instituting a consistent practice across the country for access to expedited offers. The 2019-2020 Kidney Accelerated Placement project implemented by the OPTN Organ Center offered kidneys with a high KDPI to transplant programs that had a history of accepting them. An evaluation of the project revealed there was no statistically significant change in the percentage of organ offer acceptances (Noreen et al., 2021).
Data suggest that a small number of transplant programs attract a large percentage of kidneys that are allocated through expedited placement. King et al. (2022) found that while the overall proportion of transplants from out-of-sequence allocation has remained stable over time, there are two outlier OPOs that use this discretionary tool more frequently than others. There are many reasons why OPOs may feel pressure to use out-of-sequence allocation—wide variation in local donation rates, donor quality, and transplant center acceptance behaviors are a few reasons (King et al., 2022). Expedited placement has the potential to result in disparities that result from routing organs only to transplant centers with greater resources, as well as concerns about further advantaging patients who have the means to be on multiple waiting lists in different areas of the country (Kinkhabwala et al., 2013; Mohan and Schold, 2021; Washburn and Olthoff, 2012). Out-of-sequence allocation is one tool for improving organ use rates and further study is warranted to understand if out-of-sequence allocation is associated with more successful and efficient organ placement and lower rates of organ nonuse. Perhaps most importantly, as out-of-sequence allocation relies on informal relationships between organizations and potentially concentrates a higher number of organs in a few transplant centers, the impact on disparities and equity will need to be closely monitored (King et al., 2022).
Key challenges to increase offer acceptances are noted in Box 6-4.
Conclusion 6-8: Too many deceased donor organs are procured but not transplanted each year. It is too easy for transplant centers to decline usable organs, and accountability for transplant center decision making is lacking. As demand for organs consistently exceeds supply, the continued underuse of available, usable, donated organs requires priority action.
Summary of Maximizing Use
In a review of the data, the committee finds strong evidence that supports the need for improvement on many fronts in order to decrease the nonuse rate and involve patient preferences in the consideration of organ offers. While not all of the currently unused organs could be used, the persistence of this rate over time diminishes the fairness, equity, and transparency of the organ transplantation system.
The wide variation in nonuse and organ offer acceptance rates is the result of a combination of many factors that are within the control of the transplant center, as well as resulting from operational practices and behaviors that are not supported by evidence of geography, organ supply, or patient complexity. These operational issues must be resolved to improve the fairness, equity, and transparency of the organ transplantation system. The committee acknowledges that there are some factors, such as the medical complexities of an organ offer, that are not within the control of the transplant center. Many transplant centers are top per-
formers and have found medical and operational solutions that are effective and maximize organ use. Donated organs that could be transplanted are not used for several reasons, prime among which is that the time involved each time an organ is offered but then rejected can reduce the viability of the organ, and the people to whom the organ is offered subsequently may regard it as undesirable because others have rejected it. Thus, greater use of donated organs depends on increasing the speed with which suitable organs are accepted by, and transplanted into, the patients to whom they are allocated and offered (see Box 6-5).
Conclusion 6-9: Some transplant programs state that they reject some medically complex organs because transplantation teams believe that transplants using such organs will negatively affect their program’s performance metrics, as evaluated by 1-year patient and graft survival, which can result in financial penalties. Overcoming this problem involves both adjusting measures to better identify high-quality performance and conveying to teams how they can transplant medically complex organs without adversely affecting their performance data (e.g., by sharing the techniques used by programs that have actually improved their metrics while accepting many medically complex organs).
Patient Shared Decision Making
Shared decision making is a model of patient-centered care that enables and encourages people to play a role in the medical decisions that affect their health (AHRQ, 2020). There are opportunities to increase patient shared decision making in order to improve the fairness, equity, cost-effectiveness, and transparency of the nation’s organ transplantation system. Ensuring patients are aware of all organs offered to them but declined by their transplant centers, and the reasons for the decline, will strengthen the patient-centered care that is an essential part of quality health care delivery.
Relevant Reports
The National Academies (then IOM) led the development of important work to address patient safety in U.S. hospitals with its landmark To Err Is Human report (IOM, 2000). This report provided the foundation for a new and sustained national movement to improve safety in hospitals and still today has implications for ways to improve the organ transplantation system in the United States. Crossing the Quality Chasm (IOM, 2001) quickly followed with a review of the health care delivery system, specifically the provision of preventive, acute, chronic, and end-of-life health care for individuals. The theme of increasing patient involvement resulted in a recommendation that health care processes should be redesigned to
share knowledge and the free flow of information, that patients should have unfettered access to their own medical information and to clinical knowledge. Furthermore, that clinicians and patients should communicate effectively and share information (IOM, 2001, p. 8).
Most recently, the World Health Organization has incorporated patient and family engagement as a key element to improve patient safety and for health care system improvement (WHO, 2021). These reports brought to light that patients were mostly unaware that hospital safety and health care quality were something to be concerned about, and most medical professionals were unaware of the scope of the problem. To the extent it was encountered, it was not discussed.
Although shared decision making has been examined in numerous clinical settings, it
has received little attention from the organ transplantation system (Gordon et al., 2013). This chapter has discussed the need for transparency, where reasons for the thousands of organs recovered but not transplanted annually are not well understood.20 When and why transplant centers accept or decline an organ offer is often opaque to the patients who are depending on transplant centers to make appropriate decisions for their circumstances (Mohan and Schold, 2021). This is especially important because on average, patients who die waiting for a kidney had offers for 16 kidneys that were ultimately transplanted into other patients (Husain et al., 2019). The decision to take an offered kidney or wait for a “better” one is complex and individual to the specific patient and donated kidney pair. Characteristics of each patient—such as age and time on the waiting list—as well as characteristics of each donated kidney are variable and influence the outcome of any transplantation.
Acknowledging and incorporating patient preferences is important to facilitate decisions about whether accepting a specific kidney is the best choice for that patient. For most patients with significant waiting times, taking a higher KDPI kidney when it is offered leads to better survival benefit as compared to remaining on dialysis and waiting for a “better” offer. Figure 6-11 shows estimated survival for three scenarios: transplantation now, waiting and then undergoing transplantation with a lower KDPI kidney, and waiting indefinitely without transplantation. For this example, the hypothetical patient is 55 years old, does not have diabetes, has been on dialysis for 3.5 years, and has waited 809 days on the waiting list. In this case, accepting a 60 percent KDPI kidney now would increase survival by 57.5 days on
___________________
20 See Chapter 3 for more information on increased transparency related to public trust and patient decision making, and see Chapter 5 on optimizing data for patient review in organ offers.
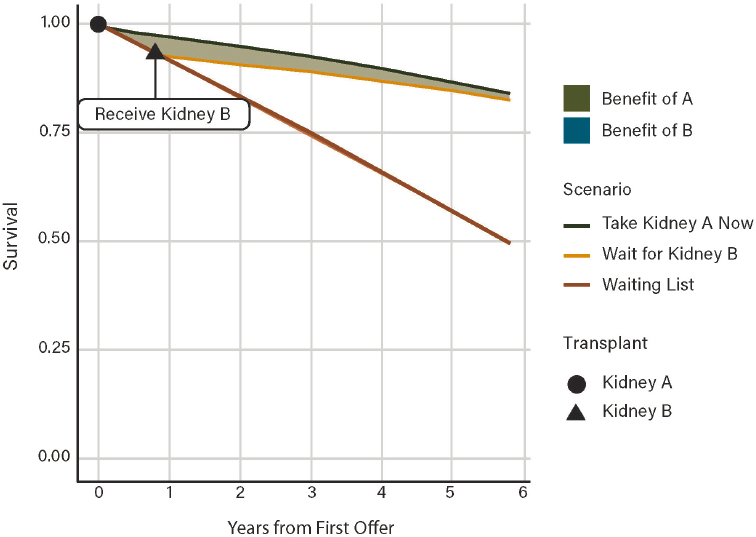
SOURCE: Parker et al., 2021.
average within the first 5 years following transplant, compared to waiting an additional 300 days for a 15 percent KDPI kidney. The probability the patient would die while waiting for the 15 percent KDPI kidney is 7 percent.
Figure 6-11 was created using one example of a web application to assist providers and patients in this type of shared decision making.21 Use of this or a similar app would allow patients to evaluate the difference in survival benefit associated with accepting a higher KDPI organ today versus waiting for an organ with lower KDPI at some point in the future. These parameters can be discussed in advance of an organ offer and updated over time as the patient remains on the waiting list and may experience changes in their preferences.
Shared decision making enables and encourages individuals to play a pivotal role in the medical decisions that affect their health, and the organ transplantation system can do this better with a focus on patient-centered care.
___________________
21 Available at https://wparker-uchicago.shinyapps.io/DDKT_survival_benefit_compare (accessed November 17, 2021).
DONOR CARE UNITS
In 2001, a significant innovation in the process of organ donation and recovery took place when Mid-America Transplant, the OPO located in St. Louis, Missouri, built a freestanding donor care unit (DCU),22 and began transferring organ donors declared dead by neurological criteria for the purposes of donor medical management and organ procurement. Over the next 20 years, 11 OPOs built and managed free-standing DCUs that serve donation service areas ranging from heavily metropolitan to large rural geographies.
The original rationale for OPOs to build and manage DCUs has not changed: to increase the number of organs transplanted, improve and manage OPO cost-effectiveness, provide consistent and reliable organ donor processes, and enhance safety for local transplant teams (Englesbe and Merion, 2009; Moazami et al., 2007). Having dedicated space where medically managing and treating organ function in a deceased organ donor is a singular organizational focus means that donation can take place without the challenges and time constraints of a busy intensive care unit in either acute care hospitals
___________________
22 DCUs are also known as “Organ Recovery Centers,” “Organ Procurement Organization Facilities,” “Organ Procurement Centers,” and “Specialized Donor Care Facilities.”
or hospitals with less familiarity with organ donation. Similarly, the ability to rely on an operating room time that is not dependent on bumping scheduled cases, or delayed because of unexpected trauma cases makes the donation process more reliable and consistent. Moving the organ donor and not the DSA surgical team provides a level of safety that has become increasingly important. Finally, the ability for an OPO to improve cost-effectiveness related to donor management and surgical recovery remains a key factor in controlling costs.
Description and Use of Donor Care Units
In general, a DCU is a facility built and managed by an OPO, under the guidance of the OPO’s medical director, for the purposes of medically managing organ function and recovering organs for transplantation from deceased organ donors.23 Because of legal requirements under state statute for hospital licensure, only donors declared dead by neurological criteria can be transferred to a DCU and not DCDD donors. After death is declared by neurological criteria in acute care or critical access hospitals, authorization for donation by the donor or surrogate decision maker has been obtained, the donor is hemodynamically stable, and approval for transfer has been given, the donor is moved by ground or air transport to the DCU. In the DCU, donor management takes place in a critical care setting where staff, monitored beds, and sophisticated imaging and diagnostic equipment such as X-ray, bronchoscopy, CT scanner, heart catheter, and point-of-care laboratory services are available onsite. The organ recovery procedure takes place in the same facility where large, state-of-the-art operating rooms can easily accommodate the multiple teams necessary for the surgical recovery of organs from multiorgan donors. With the advent of machine preservation for abdominal and thoracic organs, DCUs often house the equipment used to rehabilitate organs prior to transplantation. The ability to live stream the surgical procedure for distant surgeons and/or medical examiner/coroner/law enforcement via built-in high-resolution video cameras has provided a level of virtual hands-on experience not widely available in hospitals. Importantly, dedicated space is available for donor families to be with their loved ones, if they choose.
Models of Donor Care Units
There are three distinct models of donor care units primarily in use across the country: OPO-managed DCUs (“free-standing recovery centers”), partnerships with community hospitals, and partnerships with transplant centers.
OPO-Managed DCUs
OPO-managed DCUs, also known as free-standing recovery centers or organ procurement centers, are similar in structure, staffing, and available equipment to other DCUs, but they may differ in size of the facility and are located in the OPO building. Currently, there
___________________
23 Pediatric donor transfer practice varies by OPO due to equipment requirements. See Brockmeier presentation at the February 14, 2021, virtual workshop: https://www.nationalacademies.org/event/02-04-2021/a-fairer-and-more-equitable-cost-effective-and-transparent-system-of-donor-organ-procurement-allocation-and-distribution-a-virtualworkshop (accessed January 27, 2022).
are OPO-managed DCUs in 11 cities in United States.24 From a staffing perspective, OPO staff are trained to perform all donor management and testing procedures.
Partnerships with Community Hospitals
One large metropolitan OPO has developed a hybrid model of a DCU where, through an agreement with a community hospital, critical care beds and operating rooms are designated for donor management and the surgical recovery of organs. The staffing model for this type of DCU is similar to the donation process in donor hospitals—hospital staff provide bedside care and the OPO staff medically manage the donor.
Partnerships with Transplant Centers
The advent of transplant hospitals building in-house capabilities came about initially as a result of the interpretation of the transplant center cost report, and subsequently, as a way to increase Medicare reimbursement for the transplant center. In this model, donors declared dead (by DCDD or DNDD criteria) within the transplant center may be moved to a dedicated bed or a dedicated space within the transplant center. It is also possible for the transplant center to have agreements with non–transplant center donor hospitals where, like the other models, after the declaration of death by neurological criteria, those donors are transferred from referring hospitals throughout the DSA to the DCU housed in the transplant center. The transplant hospital may assume all responsibility for staffing, or the OPO staff may provide those services.
Key Benefits of Donor Care Units
DCUs have proven to be beneficial for both donor hospitals and donor families. In the DCU facility, private space for donor families include sleeping accommodations, internet access, restrooms, televisions, and landline use. Donor families are given the option to say their good-byes at the hospital, or move to the DCU. Under either scenario, “honor walks” and flag raising ceremonies still take place in the hospital ICU and all efforts are made to ensure that donation does not delay funeral ceremonies. Postdonation surveys consistently report high satisfaction with the DCU experience by donor families, with average results of 9.75 out of 10 for overall satisfaction (Doyle et al., 2016). Transferring donors to a DCU benefits hospitals by opening up bed space in busy ICUs and relieves staff in smaller hospitals who are less familiar with the donation process due to the infrequency of donation events. As mentioned earlier in this chapter, a DCU allows for stability in setting operating room times that will not be changed due to emergency admissions or other surgeries “bumping” organ procurement cases.
Importantly, DCUs have been cost effective in managing organ acquisition charges. The OPO pays a prorated reimbursement to donor hospitals that covers charges prior to the donor
___________________
24 These include Mid-America Transplant, St. Louis, MO (2001); Gift of Life Michigan, Ann Arbor, MI (2010), Donor Alliance, Denver, CO (2012); Center for Organ Recovery & Education, Pittsburgh, PA (2014); Mississippi Organ Recovery Agency, Jackson, MS (2017); LifeBanc, Cleveland, OH (2017); One Legacy, Los Angeles, CA (2017); Louisiana Organ Procurement Agency, New Orleans, LA (2018); and Southwest Transplant Alliance, Dallas, TX (Under Construction). See Brockmeier presentation at the February 14, 2021, virtual workshop: https://www.nationalacademies.org/event/02-04-2021/a-fairer-and-more-equitable-cost-effective-and-transparent-systemof-donor-organ-procurement-allocation-and-distribution-a-virtual-workshop (accessed January 27, 2022).
being transferred. After transfer to the DCU, the OPO assumes all expenses, which have been demonstrated to be lower than hospital charges. One OPO reported the average cost of donor recoveries between 2009 and 2014 51 percent lower when donors are transferred (hospital charges $33,161 compared to DCU costs of $16,153) (Doyle et al., 2016).
Several reports by the St. Louis group document a consistent and sustainable increase in organs transplanted, most notable with a 71 percent increase in lung transplantation when comparing two time periods (2001–2007 vs. 2009–2016) (Chang et al., 2018). From 2009 to 2014, the organ yield at the DCU was 6 percent higher in Standard Criteria Donors and 18 percent higher in Extended Criteria Donors (these donor categories are no longer used) compared to the national average of hospital recoveries (Doyle et al., 2016).
In addition to increased organ yield and decreased costs of organ procurements, DCUs have the potential to address provider burnout, the transplant surgery pipeline, and surgeon travel and allow for increased daytime operating (Doyle et al., 2016; Lindemann et al., 2019). Given the high-risk nature of air and ground transport to distant donor hospitals within a DSA, DCUs also provide an important element of greater safety for local transplant teams (Doyle et al., 2014). DCUs also have great potential for clinical research in organ donation, given the collaborative environment that encourages academic inquiry and because a relatively uncommon population is referred to a single center (Bery et al., 2021; Marsolais et al., 2017).
An additional and unexpected benefit has been the increased collaboration between the OPOs with DCUs and the transplant centers in their DSA. The decision to build a DCU is one that requires careful collaboration between the OPO, donor hospitals, and transplant centers. The committee heard testimony of how OPOs garner support from stakeholders in their DSA in order for the DCU to be successful, and monitor satisfaction of hospital critical care staff, administration, physicians, and donor families to ensure that needs and expectations are met. Based on committee testimony and shared satisfaction data, there have been no reported adverse effects to the donation culture within donor hospitals or any negative effect to donor families (Doyle et al., 2016).
Potential Challenges of DCUs
With the emergence of DCUs, several concerns have been raised, including support from acute care and critical access hospitals to transfer donors, care of the donor family, and donor family satisfaction. Initially, medical and nursing staff expressed concern about losing a connection with the donation process; however, the implementation of high touch ceremonies that include hospital staff (e.g., honor walks, flag raisings) have kept physician and nursing engagement high. As mentioned previously, care of the donor family has not been impacted by the presence of DCUs and donor families consistently report high satisfaction with their organ donation experience (Doyle et al., 2016). While OPO-managed DCUs routinely survey donor family and donor hospital satisfaction, it is unclear if the same analysis is conducted by DCUs with partnerships in community hospitals and transplant centers and more qualitative data are needed.
Given the benefits covered in this section, why have the other 37 DSAs not incorporated a DCU? Challenges to wider application of DCUs include the OPO not being geographically located adjacent to major donor hospitals and transplant centers, transplant centers refusing to transfer donors due to significant cost report implications for reimbursement, perceptions by OPOs and their Boards that the undertaking in staff training and financial outlay is too difficult to manage given the size of the OPO, and loss of revenue to local hospitals. It may be that in parts of the country, regional DCUs would be an option to help mitigate these
challenges, but the committee recognizes that they may seem daunting when initially considered. Standardizing and spreading best practices of established DCUs will help mitigate these challenges.
Committee Considerations
The financial arrangements surrounding the three DCU models described above include complex reimbursement structures negotiated between the relevant parties (OPOs, transplant centers, donor hospitals) and primarily, CMS. CMS has historically reimbursed donor
hospitals that are also transplant centers for usable organs recovered from deceased donors at their facility. Currently, if a declared deceased donor at a donor hospital that is also a transplant center is transferred to a DCU for organ procurement, the transplant center can no longer receive reimbursement for recovering those organs and organs procured at a DCU are not counted toward the Medicare organ ratio, leading to a loss in Medicare reimbursement (Lindemann et al., 2019). This committee discussed that the potential for a significant financial effect on a transplant center’s cost report has limited the willingness and ability of some transplant centers to transfer donors to DCUs and that changes in CMS or other reimbursement structures related to transferring donors to a DCU may be needed. For example, language around “excising organs” in the transplant center’s cost report could be reconsidered to “identification and declaration (or pronouncement) of death.” CMS may also consider ensuring that adequate volume exists within the OPO service area to ensure the efficient and safe operation of a DCU. In addition, capital investment, staff resourcing, and staff training would be important considerations in developing requirements for DCUs.
A December 2021 CMS Request for Information seeks public comments on a number of components of the transplantation system, including DCUs (referred to as organ recovery facilities by CMS). CMS expresses interest in learning about these facilities and the benefits and risks, particularly from a donor family and patient advocate perspective. As this committee discussed, and CMS also raises, it is possible that there will be a need for new specific health and safety requirements (possibly akin to ambulatory care center requirements) that would apply to DCUs.25
In developing Recommendation 11 below, the committee considered who is best to design, establish, and manage a DCU, and felt that OPOs were better suited for the responsibility of continuity of care with the deceased donor process. The committee concluded that CMS should review payment incentives for transplant centers such that the transplant center is neither financially punished nor excessively rewarded for performing deceased donor organ management and surgical recovery.
Conclusion 6-10: Donor care units are an innovation in organ procurement and provide an opportunity to bring consistency and high-quality care to donor organ procurement and the donor family care experience.
___________________
25 See Federal Register Vol. 86, No. 230, of Friday, December 3, 2021. Request for Information; Health and Safety Requirements for Transplant Programs, Organ Procurement Organizations, and End-Stage Renal Disease Facilities (discussion of organ recovery facilities begins on page 68603). https://www.federalregister.gov/documents/2021/12/03/2021-26146/request-for-information-health-and-safety-requirements-for-transplant-programs-organ-procurement (accessed January 28, 2022).
REFERENCES
AHRQ (Agency for Health Care Research and Quality). 2020. The SHARE Approach—Essential steps of shared decisionmaking: Quick reference guide. https://www.ahrq.gov/health-literacy/professional-training/shared-decision/tools/resource-1.html (accessed January 26, 2022).
Aubert, O., P. P. Reese, B. Audry, Y. Bouatou, M. Raynaud, D. Viglietti, C. Legendre, D. Glotz, J.-P. Empana, X. Jouven, C. Lefaucheur, C. Jacquelinet, and A. Loupy. 2019. Disparities in acceptance of deceased donor kidneys between the United States and France and estimated effects of increased US acceptance. JAMA Internal Medicine 179(10):1365-1374.
Berwick, D. M. 1996. A primer on leading the improvement of systems. BMJ Clinical Research 312(7031):619-622. Bery, A., G. Marklin, A. Itoh, D. Kreisel, T. Takahashi, B. F. Meyers, R. Nava, B. D. Kozower, H. Shepherd, G. A. Patterson, and V. Puri. 2021. Specialized donor care facility model and advances in management of thoracic organ donors. Annals of Thoracic Surgery. https://doi.org/10.1016/j.athoracsur.2020.12.026.
Bethea, E., A. Arvind, J. Gustafson, K. Andersson, D. Pratt, I. Bhan, M. Thiim, K. Corey, P. Bloom, J. Markmann, H. Yeh, N. Elias, S. Kimura, L. A. Dageforde, A. Cuenca, T. Kawai, K. Safa, W. Williams, H. Gilligan, M. Sise, J. Fishman, C. Kotton, A. Kim, C. C. Rogers, S. Shao, M. Cote, L. Irwin, P. Myoung, and R. T. Chung. 2020. Immediate administration of antiviral therapy after transplantation of hepatitis C-infected livers into uninfected recipients: Implications for therapeutic planning. American Journal of Transplantation 20(6):1619-1628.
Brennan, C., S. A. Husain, K. L. King, D. Tsapepas, L. E. Ratner, Z. Jin, J. D. Schold, and S. Mohan. 2019. A donor utilization index to assess the utilization and discard of deceased donor kidneys perceived as high risk. Clinical Journal of the American Society of Nephrology 14(11):1634-1641.
Callaghan, C. J., L. Mumford, L. Pankhurst, R. J. Baker, J. A. Bradley, and C. J. E. Watson. 2017. Early outcomes of the new UK deceased donor kidney fast-track offering scheme. Transplantation 101(12):2888-2897.
Carpenter, D. J., M. C. Chiles, E. C. Verna, K. J. Halazun, J. C. Emond, L. E. Ratner, and S. Mohan. 2019. Deceased brain dead donor liver transplantation and utilization in the United States: Nighttime and weekend effects. Transplantation 103(7):1392-1404.
Chang, S. H., D. Kreisel, G. F. Marklin, L. Cook, R. Hachem, B. D. Kozower, K. R. Balsara, J. M. Bell, C. Frederiksen, B. F. Meyers, G. A. Patterson, and V. Puri. 2018. Lung focused resuscitation at a specialized donor care facility improves lung procurement rates. Annals of Thoracic Surgery 105(5):1531-1536.
Choi, A. Y., M. S. Mulvihill, H.-J. Lee, C. Zhao, M. Kuchibhatla, J. N. Schroder, C. B. Patel, C. B. Granger, and M. G. Hartwig. 2020. Transplant center variability in organ offer acceptance and mortality among U.S. patients on the heart transplant waitlist. JAMA Cardiology 5(6):660-668.
CMS (Centers for Medicare & Medicaid Services). 2016. Solid transplant programs - outcome thresholds - revised guidelines. https://www.cms.gov/medicare/provider-enrollment-and-certification/surveycertificationgeninfo/downloads/survey-and-cert-letter-16-24.pdf (accessed November 4, 2021).
CMS. 2020a. Organ procurement organization (OPO) conditions for coverage final rule: Revisions to outcome measures for OPOs cms-3380-f. https://www.cms.gov/newsroom/fact-sheets/organ-procurement-organization-opo-conditions-coverage-final-rule-revisions-outcome-measures-opos (accessed November 4, 2021).
CMS. 2020b. Medicare and Medicaid programs; organ procurment organizations conditions for coverage; revisions to the outcome measure requirements for organ procurement organizations. A rule by the Centers for Medicare & Medicaid Services. https://www.federalregister.gov/d/2020-26329/p-195 (accessed February 2, 2022).
CMS. 2020c. Transplant. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/Transplant (accessed November 4, 2021).
CMS. 2021. HHS seeks public comments to advance equity and reduce disparities in organ transplantation, improve life-saving donations, and dialysis facility quality of care. https://www.cms.gov/newsroom/press-releases/hhs-seeks-public-comments-advance-equity-and-reduce-disparities-organ-transplantation-improve-life (accessed January 26, 2022).
The Commonwealth Fund. 2020. New international report on health care: U.S. suicide rate highest among wealthy nations. https://www.commonwealthfund.org/press-release/2020/new-international-report-health-care-us-suicide-rate-highest-among-wealthy (accessed February 2, 2022).
Dayoub, J. C., F. Cortese, A. Anžič, T. Grum, and J. P. de Magalhães. 2018. The effects of donor age on organ transplants: A review and implications for aging research. Experimental Gerontology 110:230-240.
Dolgin, N. H., B. Movahedi, P. N. Martins, R. Goldberg, K. L. Lapane, F. A. Anderson, and A. Bozorgzadeh. 2016. Decade-long trends in liver transplant waitlist removal due to illness severity: The impact of Centers for Medicare and Medicaid Services policy. Journal of the American College of Surgeons 222(6):1054-1065.
Doyle, M. B. M., N. Vachharajani, J. R. Wellen, J. A. Lowell, S. Shenoy, G. Ridolfi, M. D. Jendrisak, J. Coleman, M. Maher, D. Brockmeier, D. Kappel, and W. C. Chapman. 2014. A novel organ donor facility: A decade of experience with liver donors. American Journal of Transplantation 14(3):615-620.
Doyle, M., V. Subramanian, N. Vachharajani, K. Collins, J. R. Wellen, E. Stahlschmidt, D. Brockmeier, J. Coleman, D. Kappel, and W. C. Chapman. 2016. Organ donor recovery performed at an organ procurement organization-based facility is an effective way to minimize organ recovery costs and increase organ yield. Journal of the American College of Surgeons 222(4):591-600.
Englesbe, M. J., and R. M. Merion. 2009. The riskiest job in medicine: Transplant surgeons and organ procurement travel. American Journal of Transplantation 9(10):2406-2415.
Gill, J. R., and M. E. DeJoseph. 2020. The importance of proper death certification during the COVID-19 pandemic. JAMA 324(1):27-28.
Giorgakis, E., and A. K. Mathur. 2020. Expedited placement to maximize utilization of marginal organs. Current Opinion in Organ Transplantation 25(6):640-646.
Goldberg, D. S., B. French, J. D. Lewis, F. I. Scott, R. Mamtani, R. Gilroy, S. D. Halpern, and P. L. Abt. 2016. Liver transplant center variability in accepting organ offers and its impact on patient survival. Journal of Hepatology 64(4):843-851.
Goldberg, D. S., P. L. Abt, E. A. Blumberg, V. M. Van Deerlin, M. Levine, K. R. Reddy, R. D. Bloom, S. M. Nazarian, D. Sawinski, and P. Porrett. 2017. Trial of transplantation of HCV-infected kidneys into uninfected recipients. New England Journal of Medicine 376(24):2394-2395.
Gordon, E. J., Z. Butt, S. E. Jensen, A. Lok-Ming Lehr, J. Franklin, Y. Becker, L. Sherman, W. J. Chon, N. Beauvais, J. Hanneman, D. Penrod, M. G. Ison, and M. M. Abecassis. 2013. Opportunities for shared decision making in kidney transplantation. American Journal of Transplantation 13(5):1149-1158.
Greer, D. M. 2021. Determination of brain death. New England Journal of Medicine 385(27):2554-2561.
Grinshteyn, E., and D. Hemenway. 2019. Violent death rates in the US compared to those of other high-income countries, 2015. Preventive Medicine 123:20-26.
Ho, J. Y. 2019. The contemporary American drug overdose epidemic in international perspective. Population and Development Review 45(1):7-40.
Husain, S. A., F. S. Winterhalter, and S. Mohan. 2018. Kidney transplant offers to deceased candidates. American Journal of Transplantation 18(11):2836-2837.
Husain, S. A., K. L. King, S. Pastan, R. E. Patzer, D. J. Cohen, J. Radhakrishnan, and S. Mohan. 2019. Association between declined offers of deceased donor kidney allograft and outcomes in kidney transplant candidates. JAMA Network Open 2(8):e1910312.
Ibrahim, M., G. Vece, J. Mehew, R. Johnson, J. Forsythe, D. Klassen, C. Callaghan, and D. Stewart. 2020. An international comparison of deceased donor kidney utilization: What can the United States and the United Kingdom learn from each other? American Journal of Transplantation 20(5):1309-1322.
IOM (Institute of Medicine). 1997. Non-heart-beating organ transplantation: Medical and ethical issues in procurement. Edited by J. T. Potts and R. Herdman. Washington, DC: National Academy Press.
IOM. 2000. To err is human: Building a safer health system. Edited by L. T. Kohn, J. M. Corrigan, and M. S. Donaldson. Washington, DC: National Academy Press.
IOM. 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
IOM. 2006. Organ donation: Opportunities for action. Edited by J. F. Childress and C. T. Liverman. Washington, DC: The National Academies Press.
IRODaT (International Registry in Organ Donation and Transplantation. 2021. International registry in organ donation and transplantation. https://www.irodat.org/?p=database (accessed January 7, 2022).
Israni, A. K., D. Zaun, J. D. Rosendale, C. Schaffhausen, W. McKinney, and J. J. Snyder. 2021. OPTN/SRTR 2019 annual data report: Deceased organ donors. American Journal of Transplantation 21(S2):567-604.
Kalisvaart, M., K. P. Croome, R. Hernandez-Alejandro, J. Pirenne, M. Cortés-Cerisuelo, E. Miñambres, and P. L. Abt. 2021. Donor warm ischemia time in DCD liver transplantation-working group report from the ILTS DCD, liver preservation, and machine perfusion consensus conference. Transplantation 105(6):1156-1164.
Karp, S., and G. Segal. 2021. New regulation for organ procurement will improve equity and save lives. https://www.thehastingscenter.org/new-regulation-for-organ-procurement-will-improve-equity-and-save-lives (accessed February 2, 2022).
Karp, S., G. Segal, and D. J. Patil. 2020. Fixing organ donation—what gets measured, gets fixed. JAMA Surgery 155(8):687-688.
Kasiske, B. L., N. Salkowski, A. Wey, A. K. Israni, and J. J. Snyder. 2016. Potential implications of recent and proposed changes in the regulatory oversight of solid organ transplantation in the United States. American Journal of Transplantation 16(12):3371-3377.
Kelen, G. D., R. Wolfe, G. D’Onofrio, A. M. Mills, D. Diercks, S. A. Stern, M. Wadman, and P. E. Sokolove. 2021. Emergency department crowding: The canary in the health care system. NEJM Catalyst. https://doi.org/10.1056/CAT.21.0217.
Khush, K. K., J. G. Zaroff, J. Nguyen, R. Menza, and B. A. Goldstein. 2015. National decline in donor heart utilization with regional variability: 1995-2010. American Journal of Transplantation 15(3):642-649.
Kim, D. W., D. Tsapepas, K. L. King, S. A. Husain, F. A. Corvino, A. Dillon, W. Wang, T. J. Mayne, and S. Mohan. 2020. Financial impact of delayed graft function in kidney transplantation. Clinical Transplantation 34(10):e14022.
King, K. L., S. A. Husain, D. J. Cohen, and S. Mohan. 2019. Deceased donor kidneys are harder to place on the weekend. Clinical Journal of the American Society of Nephrology 14(6):904-906.
King, K. L., S. A. Husain, J. D. Schold, R. E. Patzer, P. P. Reese, Z. Jin, L. E. Ratner, D. J. Cohen, S. O. Pastan, and S. Mohan. 2020. Major variation across local transplant centers in probability of kidney transplant for wait-listed patients. Journal of the American Society of Nephrology 31(12):2900-2911.
King, K. L., S. G. Chaudhry, L. E. Ratner, D. J. Cohen, S. A. Husain, and S. Mohan. 2021. Declined offers for deceased donor kidneys are not an independent reflection of organ quality. Kidney360. https://doi.org/10.34067/KID.0004052021.
King, K. L., S. A. Husain, A. Perotte, J. T. Adler, J. D. Schold, and S. Mohan. 2022. Deceased donor kidneys allocated out of sequence by organ procurement organizations. American Journal of Transplantation. https://doi.org/10.1111/ajt.16951.
Kinkhabwala, M., J. Lindower, J. F. Reinus, A. L. Principe, and P. J. Gaglio. 2013. Expedited liver allocation in the United States: A critical analysis. Liver Transplantation 19(10):1159-1165.
Kotloff, R. M., S. Blosser, G. J. Fulda, D. Malinoski, V. N. Ahya, L. Angel, M. C. Byrnes, M. A. DeVita, T. E. Grissom, S. D. Halpern, T. A. Nakagawa, P. G. Stock, D. L. Sudan, K. E. Wood, S. J. Anillo, T. P. Bleck, E. E. Eidbo, R. A. Fowler, A. K. Glazier, C. Gries, R. Hasz, D. Herr, A. Khan, D. Landsberg, D. J. Lebovitz, D. J. Levine, M. Mathur, P. Naik, C. U. Niemann, D. R. Nunley, K. J. O’Connor, S. J. Pelletier, O. Rahman, D. Ranjan, A. Salim, R. G. Sawyer, T. Shafer, D. Sonneti, P. Spiro, M. Valapour, D. Vikraman-Sushama, and T. P. Whelan. 2015. Management of the potential organ donor in the ICU: Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations consensus statement. Critical Care Medicine 43(6):1291-1325.
Koval, C. E., E. D. Poggio, Y.-C. Lin, H. Kerr, M. Eltemamy, and A. Wee. 2021. Early success transplanting kidneys from donors with new SARS-CoV-2 RNA positivity: A report of 10 cases. American Journal of Transplantation 21(11):3743-3749.
Kress, J., D. L. Smith, P. C. Fehling, and E. J. Gordon. 2009. Improving the recruitment and retention of organ procurement coordinators: A survey study. American Journal of Transplantation 9(6):1451-1459.
Kwong, A. J., W. R. Kim, J. R. Lake, J. M. Smith, D. P. Schladt, M. A. Skeans, S. M. Noreen, J. Foutz, S. E. Booker, M. Cafarella, J. J. Snyder, A. K. Israni, and B. L. Kasiske. 2021. OPTN/SRTR 2019 annual data report: Liver. American Journal of Transplantation 21(S2):208-315.
Lentine, K. L., B. Kasiske, and D. A. Axelrod. 2021. Procurement biopsies in kidney transplantation: More information may not lead to better decisions. Journal of the American Society of Nephrology 32(8):1835-1837.
Li, M. T., K. L. King, S. A. Husain, J. D. Schold, and S. Mohan. 2021. Deceased donor kidneys utilization and discard rates during COVID-19 pandemic in the United States. Kidney International Reports 6(9):2463-2467.
Lia, D., P. Singer, V. Nair, J. Yang, L. Teperman, and E. Grodstein. 2021. DCD renal transplantation from donors with acute kidney injury. Transplantation 105(4):886-890.
Lindemann, J., L. A. Dageforde, N. Vachharajani, E. Stahlschmidt, D. Brockmeier, J. R. Wellen, A. Khan, W. C. Chapman, and M. M. Doyle. 2018. Cost evaluation of a donation after cardiac death program: How cost per organ compares to other donor types. Journal of the American College of Surgeons 226(5):909-916.
Lindemann, J., L. A. Dageforde, D. Brockmeier, N. Vachharajani, M. Scherer, W. Chapman, and M. B. M. Doyle. 2019. Organ procurement center allows for daytime liver transplantation with less resource utilization: May address burnout, pipeline, and safety for field of transplantation. American Journal of Transplantation 19(5):1296-1304.
Litvak, E., and H. V. Fineberg. 2013. Smoothing the way to high quality, safety, and economy. New England Journal of Medicine 369(17):1581-1583.
Litvak, E., S. Keshavjee, B. L. Gewertz, and H. V. Fineberg. 2021. How hospitals can save lives and themselves: Lessons on patient flow from the COVID-19 pandemic. Annals of Surgery 274(1):37-39.
Lynch, R. J., B. L. Doby, D. S. Goldberg, K. J. Lee, A. Cimeno, and S. J. Karp. 2021. Procurement characteristics of high- and low-performing OPOs as seen in OPTN/SRTR data. American Journal of Transplantation. https://doi.org/10.1111/ajt.16832.
Madan, S., O. Saeed, S. J. Forest, D. J. Goldstein, U. P. Jorde, and S. R. Patel. 2022. Feasibility and potential impact of heart transplantation from adult donors after circulatory death. JACC 79(2):148-162.
Madhusoodanan, J. 2021. Inner workings: Advances in infectious disease treatment promise to expand the pool of donor organs. Proceedings of the National Academy of Sciences of the United States of America 118(8):e2100577118.
Marsolais, P., P. Durand, E. Charbonney, K. Serri, A.-M. Lagacé, F. Bernard, and M. Albert. 2017. The first 2 years of activity of a specialized organ procurement center: Report of an innovative approach to improve organ donation. American Journal of Transplantation 17(6):1613-1619.
Matesanz, R., B. Domínguez-Gil, E. Coll, G. de la Rosa, and R. Marazuela. 2011. Spanish experience as a leading country: What kind of measures were taken? Transplant International 24(4):333-343.
McGivern, L., L. Shulman, J. K. Carney, S. Shapiro, and E. Bundock. 2017. Death certification errors and the effect on mortality statistics. Public Health Reports 132(6):669-675.
Moazami, N., O. H. Javadi, D. F. Kappel, J. Wagner, and M. D. Jendrisak. 2007. The feasibility of organ procurement at a hospital-independent facility: A working model of efficiency. Journal of Thoracic and Cardiovascular Surgery 133(5):1389-1390.
Mohan, S., and J. D. Schold. 2021. Accelerating deceased donor kidney utilization requires more than accelerating placement. American Journal of Transplantation. https://doi.org/10.1111/ajt.16866.
Mohan, S., K. Foley, M. C. Chiles, G. K. Dube, R. E. Patzer, S. O. Pastan, R. J. Crew, D. J. Cohen, and L. E. Ratner. 2016. The weekend effect alters the procurement and discard rates of deceased donor kidneys in the United States. Kidney International 90(1):157-163.
Mohan, S., M. C. Chiles, R. E. Patzer, S. O. Pastan, S. A. Husain, D. J. Carpenter, G. K. Dube, R. J. Crew, L. E. Ratner, and D. J. Cohen. 2018. Factors leading to the discard of deceased donor kidneys in the United States. Kidney International 94(1):187-198.
Mohan, S., S. L. Tummalapalli, and J. Schold. 2021 (unpublished). Identifying innovative solutions to financial and policy barriers to increase deceased donor transplantation in the United States. Paper commissioned by the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine, Washington, DC.
Mulvihill, M. S., H. J. Lee, J. Weber, A. Y. Choi, M. L. Cox, B. A. Yerokun, M. A. Bishawi, J. Klapper, M. Kuchibhatla, and M. G. Hartwig. 2020. Variability in donor organ offer acceptance and lung transplantation survival. Journal of Heart and Lung Transplantation 39(4):353-362.
Noreen, S. M., D. Klassen, R. Brown, Y. Becker, K. O’Connor, J. Prinz, and M. Cooper. 2022. Kidney accelerated placement project: Outcomes and lessons learned. American Journal of Transplantation 22(1):210-221.
NQF (National Quality Forum). 2021. How measures will serve our future. https://www.qualityforum.org/Measuring_Performance/ABCs/How_Measures_Will_Serve_Our_Future.aspx (accessed November 3, 2021).
OPTN (Organ Procurement and Transplantation Network). 2021a. National data. https://optn.transplant.hrsa.gov/data/view-data-reports/national-data (accessed November 4, 2021).
OPTN. 2021b. OPTN Kidney Transplantation Committee Meeting Summary: November 15, 2021. https://optn.transplant.hrsa.gov/media/5lkpjmp2/20211115_kidney-committee_-meeting-summary.pdf (accessed January 27, 2022).
Padilla, M., E. Coll, C. Fernández-Pérez, T. Pont, Á. Ruiz, M. Pérez-Redondo, E. Oliver, L. Atutxa, J. M. Manciño, D. Daga, E. Miñambres, J. Moya, B. Vidal, J. M. Dueñas-Jurado, F. Mosteiro, A. Rodríguez-Salgado, E. FernándezGarcía, R. Lara, D. Hernández-Marrero, B. Estébanez, M. L. Rodríguez-Ferrero, M. Barber, F. García-López, A. Andrés, C. Santiago, A. Zapatero, R. Badenes, F. Carrizosa, J. J. Blanco, J. L. Bernal, F. J. Elola, C. Vidal, C. Terrón, P. Castro, J. Comas, and B. Domínguez-Gil. 2021. Improved short-term outcomes of kidney transplants in controlled donation after the circulatory determination of death with the use of normothermic regional perfusion. American Journal of Transplantation 21(11):3618-3628.
Pagani, F. D. 2022. Heart transplantation using organs from donors following circulatory death: The journey continues. JACC 79(2):163-165.
Parker, W. F., Y. Becker, and R. Gibbons. 2021 (unpublished). Calculating the lives saved with deceased donor kidney transplantation. Paper commissioned by the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine, Washington, DC.
Pearson, R., C. Geddes, P. Mark, M. Clancy, and J. Asher. 2021. Transplantation of kidneys after normothermic perfusion: A single center experience. Clinical Transplantation 35(10):e14431.
POGO (Project on Government Oversight). 2021. Re: First response to December 23, 2020 letter to AOPO. https://www.documentcloud.org/documents/20529235-aopo-first-response-to-house-oversight-committee-final (accessed February 2, 2022).
Pritt, B. S., N. J. Hardin, J. A. Richmond, and S. L. Shapiro. 2005. Death certification errors at an academic institution. Archives of Pathology and Laboratory Medicine 129(11):1476-1479.
Reese, P. P., O. Aubert, M. Naesens, E. Huang, V. Potluri, D. Kuypers, A. Bouquegneau, G. Divard, M. Raynaud, Y. Bouatou, A. Vo, D. Glotz, C. Legendre, C. Lefaucheur, S. Jordan, J. P. Empana, X. Jouven, and A. Loupy. 2021. Assessment of the utility of kidney histology as a basis for discarding organs in the United States: A comparison of international transplant practices and outcomes. Journal of the American Society of Nephrology 32(2):397-409.
Ryckman, F. C., P. A. Yelton, A. M. Anneken, P. E. Kiessling, P. J. Schoettker, and U. R. Kotagal. 2009. Redesigning intensive care unit flow using variability management to improve access and safety. Joint Commission Journal on Quality and Patient Safety 35(11):535-543.
Saade, M., J. Davies, E. Torres, L. Morales-Otero, Z. Gonzalez-Caraballo, and E. A. Santiago-Delpin. 2005. A marked increase in organ donation in Puerto Rico. Transplantation Proceedings 37(9):3618-3620.
Segev, D. L., C. E. Simpkins, R. E. Thompson, J. E. Locke, D. S. Warren, and R. A. Montgomery. 2008. Obesity impacts access to kidney transplantation. Journal of the American Society of Nephrology 19(2):349-355.
Shafer, T. J., D. Wagner, J. Chessare, M. W. Schall, V. McBride, F. A. Zampiello, J. Perdue, K. O’Connor, M. J. Lin, and J. Burdick. 2008. U.S. organ donation breakthrough collaborative increases organ donation. Critical Care Nursing Quarterly 31(3):190-210.
Shah, A. S. 2021. Normothermic regional perfusion in donor heart recovery: Establishing a new normal. Journal of Thoracic and Cardiovascular Surgery. https://doi.org/10.1016/j.jtcvs.2021.11.084.
Sise, M. E., D. S. Goldberg, J. J. Kort, D. E. Schaubel, R. R. Alloway, C. M. Durand, R. J. Fontana, R. S. Brown, J. J. Friedewald, S. Prenner, J. R. Landis, M. Fernando, C. C. Phillips, E. S. Woodle, A. Rike-Shields, K. E. Sherman, N. Elias, W. W. Williams, J. L. Gustafson, N. M. Desai, B. Barnaba, S. P. Norman, M. Doshi, S. T. Sultan, M. J. Aull, J. Levitsky, D. S. Belshe, R. T. Chung, and P. P. Reese. 2020. Multicenter study to transplant hepatitis C–infected kidneys (MYTHIC): An open-label study of combined glecaprevir and pibrentasvir to treat recipients of transplanted kidneys from deceased donors with hepatitis C virus infection. Journal of the American Society of Nephrology 31(11):2678-2687.
Smith, C. D., T. Spackman, K. Brommer, M. W. Stewart, M. Vizzini, J. Frye, and W. C. Rupp. 2013. Re-engineering the operating room using variability methodology to improve health care value. Journal of the American College of Surgeons 216(4):559-568.
SRTR (Scientific Registry of Transplant Recipients). 2019. 2019 annual data report. http://srtr.transplant.hrsa.gov/annual_reports/Default.aspx (accessed November 4, 2021).
SRTR. 2021. OPTN/SRTR 2019 annual data report: Preface. American Journal of Transplantation 21(S2):1-10.
SRTR. 2022a. Guide to Key OPO Metrics. https://www.srtr.org/about-the-data/guide-to-key-opo-metrics (accessed January 27, 2022).
SRTR. 2022b. Calculating the 5-tier assesments: A guide for pre- and posttransplant metrics. https://www.srtr.org/about-the-data/guide-to-using-the-srtr-website/txguidearticles/5-tier-outcome-assessment (accessed January 27, 2022).
Steggerda, J. A., M. B. Bloom, M. Noureddin, T. V. Brennan, T. Todo, N. N. Nissen, A. S. Klein, and I. K. Kim. 2020. Higher thresholds for the utilization of steatotic allografts in liver transplantation: Analysis from a U.S. national database. PLoS ONE 15(4):e0230995.
Stewart, D. E., V. C. Garcia, J. D. Rosendale, D. K. Klassen, and B. J. Carrico. 2017. Diagnosing the decades-long rise in the deceased donor kidney discard rate in the United States. Transplantation 101(3):575-587.
Thornton, J. 2021. Expanding HIV-positive organ donation. Lancet 397(10270):184-185.
Traino, H. M., A. J. Molisani, and L. A. Siminoff. 2017. Regional differences in communication process and outcomes of requests for solid organ donation. American Journal of Transplantation 17(6):1620-1627.
UNOS (United Network of Organ Sharing). 2020. Establish better metrics for OPOs and transplant hospitals. https://unos.org/news/media-resources/5-ways/establish-better-metrics-for-opos-and-transplant-hospitals (accessed November 4, 2021).
UNOS. 2021a. How we match organs. https://unos.org/TRANSPLANT/HOW-WE-MATCH-ORGANS/ (accessed November 17, 2021).
UNOS. 2021b. Updated list of organ refusal reasons will go into effect on Dec. 2. https://unos.org/news/updated-list-of-organ-refusal-reasons-will-go-into-effect-on-dec-2 (accessed February 4, 2022).
van der Windt, D. J., R. Mehta, D. R. Jorgensen, S. Hariharan, P. S. Randhawa, P. Sood, M. Molinari, M. Wijkstrom, A. Ganoza, and A. D. Tevar. 2021. Donation after circulatory death is associated with increased fibrosis on 1-year post-transplant kidney allograft surveillance biopsy. Clinical Transplantation 35(9):e14399.
Veatch, R. M. 2008. Donating hearts after cardiac death—reversing the irreversible. New England Journal of Medicine 359:672-673.
Verzelloni Sef, A., D. Sef, V. Trkulja, B. Raj, N. J. Lees, C. Walker, I. McGovern, J. Mitchell, F. De Robertis, and U. Stock. 2021. Postoperative acute kidney injury and renal replacement therapy after DCD lung transplantation. Clinical Transplantation 36(2):e14468.
Volk, M. L., H. A. Reichert, A. S. F. Lok, and R. A. Hayward. 2011. Variation in organ quality between liver transplant centers. American Journal of Transplantation 11(5):958-964.
Washburn, K., and K. Olthoff. 2012. Truth and consequences: The challenge of greater transparency in liver distribution and utilization. American Journal of Transplantation 12(4):808-809.
Wexelman, B. A., E. Eden, and K. M. Rose. 2013. Survey of New York City resident physicians on cause-of-death reporting, 2010. Preventing Chronic Disease 10:120288.
WHO (World Health Organization). 2018. Global status report on road safety 2018: Summary. Geneva: World Health Organization. https://www.who.int/publications/i/item/9789241565684 (accessed February 2, 2022).
WHO. 2021. Global patient safety action plan 2021-2030. https://www.who.int/publications/i/item/9789240032705 (accessed November 11, 2021).
Wolfe, R. A., F. B. LaPorte, A. M. Rodgers, E. C. Roys, G. Fant, and A. B. Leichtman. 2007. Developing organ offer and acceptance measures: When ‘good’ organs are turned down. American Journal of Transplantation 7(5 Pt 2):1404-1411.
Woolley, A. E., S. K. Singh, H. J. Goldberg, H. R. Mallidi, M. M. Givertz, M. R. Mehra, A. Coppolino, A. E. Kusztos, M. E. Johnson, K. Chen, E. A. Haddad, J. Fanikos, D. P. Harrington, P. C. Camp, and L. R. Baden. 2019. Heart and lung transplants from HCV-infected donors to uninfected recipients. New England Journal of Medicine 380(17):1606-1617.
Yasinski, E. 2016. When donated organs go to waste. https://www.theatlantic.com/health/archive/2016/02/when-donated-organs-go-to-waste/470838 (accessed November 17, 2021).
Yu, K., K. King, S. A. Husain, G. K. Dube, J. S. Stevens, L. E. Ratner, M. Cooper, C. R. Parikh, and S. Mohan. 2020. Kidney nonprocurement in solid organ donors in the United States. American Journal of Transplantation 20(12):3413-3425.
This page intentionally left blank.














































