3
Scientific Basis for Radiation Protection
This chapter provides background information on the radiation protection framework in the United States (Section 3.1) and the agencies with radiation protection responsibilities (Section 3.2), and it discusses how new science is incorporated in the radiation protection framework (Section 3.3). This chapter also attempts to address the seventh charge of the Statement of Task, which asks the committee to identify and, to the extent possible, quantify potential monetary and health-related impacts to federal agencies, the general public, industry, research communities, and other users of information produced by such a research program. The committee explains why it cannot provide a quantitative assessment of the economic impacts. Instead, the committee offers its assessment of whether knowledge from low-dose radiation research can affect the decision-making frameworks in the federal regulatory system and how (Section 3.4).
3.1 THE RADIATION PROTECTION FRAMEWORK
Governments around the world manage health, safety, and environmental risks from radiation through regulations and guidance that shape radiation protection systems. In the case of human health, these systems aim to avoid tissue reactions and keep stochastic effects (cancer and hereditary effects) to a level as low as reasonably achievable (ALARA)1 by considering the estimated risks and the benefit to the individual or society derived from the use of the
___________________
1 Based on the ALARA principle, even a low-dose exposure below the regulatory limit or proposed guideline needs to be avoided. See https://www.nrc.gov/reading-rm/basic-ref/glossary/alara.html.
particular application (ICRP, 2007). The basic approaches to radiation protection are consistent globally. Low-dose radiation protection standards have been developed to be applied for prospective planning purposes, and the associated regulation and guidance and, more specifically, dose limits are derived on the basis of a notional sex- and age-averaged person and are therefore not indicative of the outcome to any one individual. Radiation protection systems have evolved and will continue to evolve as scientific knowledge increases and the applications of radiation change in nature and scope (Clement et al., 2021).
Exposures to low levels of radiation may carry low levels of risk to an exposed individual; nonetheless they are a high priority for the radiation protection system, and the vast majority of regulations and guidance in the radiation protection system tend to address low-dose radiation exposures. In the absence of clear evidence of risks at low doses of radiation, radiation
protection systems are based on certain assumptions about the possible risks (see Box 3.1).
The standard model used by regulatory agencies to describe the relationship between radiation dose and cancer risk is the linear no-threshold (LNT) model. This relatively simple model assumes that the excess risk of cancer from exposure to low doses of radiation is not zero regardless of how small the dose is (i.e., there is no threshold below which there is no effect) and that the excess risk is proportional to the dose of radiation (i.e., the risk increases as the dose increases). While a linear association between radiation dose and cancer risk has been established at moderate to high doses, linearity at low doses is typically assumed based on models that fit over the full dose range.
The LNT model has provided an adequate fit to the data from several major epidemiological studies of cancer risk following radiation exposures, including the Life Span Study of the Japanese atomic bomb survivors. Although no alternative model has convincingly been shown to provide a better fit to these data (Hauptmann et al., 2020; NCRP, 2018a; UNSCEAR, 2020a), recent analyses of the Life Span Study data have suggested a linear-quadratic association2 of radiation dose with cancer risk when considering all solid cancers together, although such a nonlinear association could arise due to different associations of radiation dose with risk for different types of cancer (Brenner et al., 2022).
The use of the LNT model to describe risks in the low-dose range is also supported by biophysical arguments regarding the stochastic nature of ionizing radiation energy deposition. At least two biological processes have been identified in vitro which suggest a nonlinear induction of radiation effects at low doses. These are bystander effects observed in the vicinity of cells irradiated with alpha particles and adaptive response of cells exposed to low doses of ionizing radiation (Hamada et al., 2011; Morgan, 2003a,b; Rühm et al., 2017). Still, the use of the LNT model for radiation protection purposes is often justified as being “conservative” (Puskin, 2009).
LNT has been used in radiation protection as a regulatory model for more than 40 years and is also used in regulating chemical carcinogens (see Clewell et al., 2019, for review). For regulatory purposes it is assumed that the burden of proof for a model other than LNT is on those who suggest a different model. In addition to the LNT model (curve “a” in Figure 3.1), four other basic model options might be considered to describe risks following low doses of radiation (but not equally plausible, based on current knowledge): downward curving (decreasing slope, curve “b”), upward
___________________
2 That means that at higher doses and dose rates, risk increases more sharply than at lower doses and dose rates, such that risks due to low-dose exposure are considered to be lower than estimated based on a simple linear dose-response model.
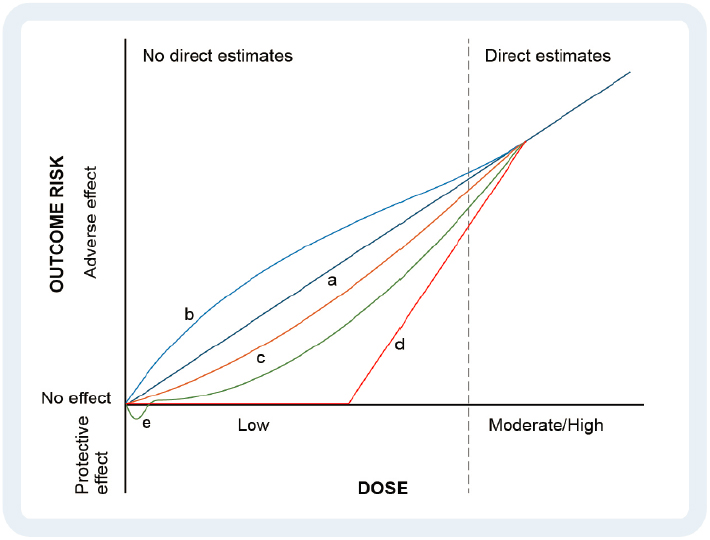
curving (increasing slope, curve “c”), threshold (curve “d”), and adaptive response (curve “e”; see Figure 3.1). The only dose-response curve that predicts more risk at low doses than the linear model is curve “b.” Any divergences from the LNT model imply that the current radiation protection system either overestimates or underestimates risks at low doses.
A broadly accepted illustration (see Figure 3.2) of the approximate magnitude of the risk from low-dose radiation based on the LNT model is that if 100 individuals (all circles in Figure 3.2) were each exposed to 100 millisieverts (mSv) in their lifetime, then approximately 1 of them (red circle) would develop a radiation-induced cancer over their lifetime, whereas around 42 (blue circles) would develop cancer from other causes (NRC, 2006a). Although the magnitude of risk from low doses of radiation can be considered to be small compared to the risk from all other causes
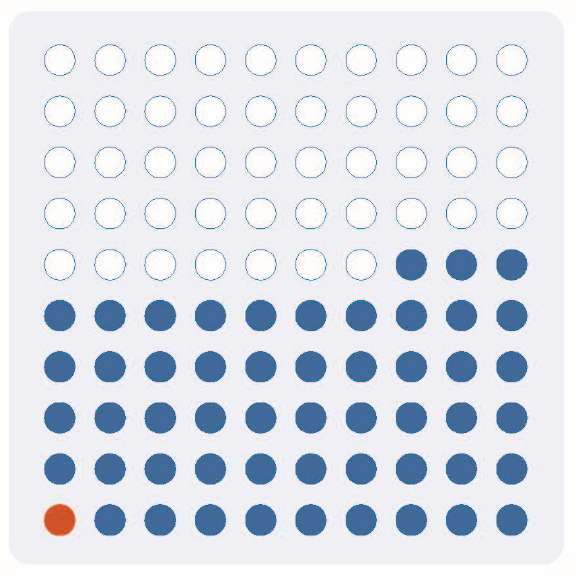
combined, if large numbers of individuals are exposed to even small doses, then the magnitude of the radiation-induced health effects can become important at the population level and in terms of burdens on health care systems (Brenner, 2014). Notably, radiation-induced cancers cannot currently be distinguished from cancers of the same type initiated by other causes because no unique signature of radiation-induced damage in tumors has been identified to date (Behjati et al., 2016; Kocakavuk et al., 2021; Morton et al., 2021). One study found an excess of small deletions and balanced inversions (Behjati et al., 2016), but radiation dose estimates were not available in that study.3
___________________
3 As discussed in Chapter 5, genome sequencing studies have identified genomic signatures in cancers that suggest specific, non-radiation causative agents for individual tumors (Alexandrov et al., 2020). These genomic signatures can be excluded from consideration in an assessment of radiation-induced carcinogenesis.
3.2 AGENCIES WITH RADIATION PROTECTION RESPONSIBILITIES IN THE UNITED STATES
In the United States, several federal agencies, and in some instances states, administer radiation protection standards. The Environmental Protection Agency (EPA) is the lead federal agency responsible for establishing human health and environmental radiation standards for air, surface water, drinking water, uranium mill tailings sites, and deep geologic repositories.4 Various laws authorize other federal agencies to set regulatory limits and issue guidelines to protect the public and workers from exposure to ionizing radiation. The authority of a federal agency to administer those limits and guidance is rooted in statute and tends to vary depending on the setting in which radiation exposure occurs.
EPA issues Protective Action Guides (PAGs; EPA, 2017)5 for use during a nuclear or a radiological emergency and suggests that public safety measures such as evacuation to minimize or prevent radiation exposure during an emergency be triggered when the projected dose to an individual is 10 to 50 mSv over 4 days. EPA also provides guidelines for drinking water interdiction. EPA has also developed guidance on establishing protective cleanup levels for radioactive contamination at sites managed under the Comprehensive Environmental Response, Compensation, and Liability Act (CERCLA or “Superfund”). When not based on other environmental standards that are Applicable or Relevant and Appropriate Requirements (ARARs), these cleanup levels correspond to acceptable lifetime excess cancer risk levels of 1 in 10,000 to 1 in 1,000,000 due to exposure to a site-related carcinogen but can vary across sites because of land use, exposure scenarios, and the statutory requirement for cost-effectiveness. EPA discourages decision-makers from using dose-based guidance6 when developing cleanup levels and encourages using the CERCLA risk range instead for consistency with guidance for chemical carcinogens. According to EPA, dose assessments should only be conducted under CERCLA where necessary to demonstrate compliance with ARARs. For this purpose, EPA has defined protective dose-based standards as 0.12 mSv per year or below (EPA, 2014). This cleanup level is considerably lower than that recommended by the U.S. Nuclear Regulatory Commission (U.S. NRC) and the Department of Energy (DOE), as discussed below.
The U.S. NRC regulates worker exposure to radiation for specific radioactive materials for which it issues licenses. The U.S. NRC limits occupational doses to 50 mSv per year for workers in commercial nuclear facilities
___________________
4 See https://www.epa.gov/radiation/radiation-regulations-and-laws.
5 PAGs consider the risks to individuals from exposure to radiation and the risks and costs associated with a specific protective action such as evacuation or sheltering in place.
6 Guidance that estimates risk from a given dose.
such as nuclear power plants, industrial radiography, and nuclear medicine7 and the annual dose to the lens of the eye at 150 mSv (equivalent dose).8
DOE sets occupational dose limits for workers at DOE facilities. Similar to the U.S. NRC, it limits occupational doses to 50 mSv per year and public dose limits, including from cleanup of radioactive waste at DOE sites, to 1 mSv. Many contaminated DOE sites are being regulated by CERCLA authority (DOE and EPA, 1995), which requires the sites to clean up on the basis of acceptable risk ranges calculated by methods defined by EPA and state laws.
The Occupational Safety and Health Administration (OSHA) sets radiation limits for workers from exposure to radiation sources that are not regulated by the U.S. NRC or other federal agencies, such as X-ray equipment, some accelerators, and some naturally occurring radioactive material. OSHA’s limits for workers vary by industry.9
The Department of Defense is responsible for military exposure and remediation as well as for setting requirements to operate in environments that could expose personnel to low doses of ionizing radiation.
The National Aeronautics and Space Administration (NASA) sets radiation limits for career exposure to astronauts but these limits are above the doses of interest for this report. The career limit was set at 3 percent risk of exposure-induced cancer death at 95 percent confidence level from fatal cancers, which corresponds to approximately 180 mSv for a 30-year-old female and approximately 700 mSv for a 60-year-old male astronaut. Following a recommendation by the National Academies (NASEM, 2021c), NASA revised the limit to 600 mSv career exposure for astronauts of all ages and sexes (NASA, 2022).
Other federal agencies apply radiation protection guidance and requirements (see Figure 1.4). These include the Federal Aviation Administration, which recommends limits to aircrews (a 5-year average effective dose of 20 mSv per year with no more than 50 mSv in a single year; FAA, 2003) and provides computer software for estimating the amount of galactic cosmic radiation received on a flight; the Food and Drug Administration, which issues radiation safety regulations for medical equipment (e.g., for mammography, these are based on the Mammography Quality Standards Act; FDA, 1998); the National Institute of Standards and Technology within the Department of Commerce, which maintains and disseminates the national
___________________
7 The International Commission on Radiological Protection (ICRP) recommends limiting the annual exposure to radiation workers to 20 mSv (ICRP, 2007).
8 ICRP recommends limiting exposure to the lens of the eye to 20 mSv averaged over 5 years, not to exceed 50 mSv in one year (ICRP, 2012) and the National Council on Radiation Protection and Measurements (NCRP) recommends a limit of 50 mSv in 1 year (Dauer et al., 2017; NCRP, 2016).
measurement standards for ionizing radiation, carries out research in dosimetry, disseminates air kerma and absorbed dose standard data, and provides calibration services; the Department of Homeland Security, which is responsible for coordinating the federal response to a nuclear or radiological incident; the Department of Veteran Affairs and the Department of Justice, which manage radiation compensation programs; the Customs and Border Protection, which responds to incidents involving inadvertently imported radioactive materials; the Department of State, which coordinates the response to foreign incidents involving radioactive materials, if assistance from the United States is requested; and the United States Coast Guard, which responds to incidents not managed by other agencies that impact the coastal zone.
Representatives of agencies with radiation protection responsibilities are members of the Interagency Steering Committee on Radiation Standards (ISCORS). The goal of ISCORS is to improve consistency in federal radiation protection programs. Specific objectives relevant to this report include facilitating consensus on acceptable levels of radiation risk and promoting consistent risk-assessment and risk-management approaches in setting and implementing standards for radiation protection.10 However, experts who briefed the committee noted that ISCORS does not provide a centralized radiation science and policy leadership within the U.S. government.11 Individual agencies set the regulatory frameworks that are appropriate for their jurisdictions.
3.3 SCIENCE BEHIND RADIATION PROTECTION
Most U.S. radiation protection regulations and guidelines are informed by and are broadly consistent with the recommendations of ICRP; NCRP; and the International Atomic Energy Agency’s Basic Safety Standards for Radiation Protection that are published jointly with the World Health Organization, the International Labour Organization, and the Organisation for Economic Co-operation and Development’s Nuclear Energy Agency. ICRP and NCRP recommendations are based on scientific consensus publications such as the National Academies’ Biological Effects of Ionizing Radiation (BEIR) committee reports and reports issued by the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Both the National Academies and UNSCEAR periodically review the available scientific literature of epidemiological and mechanistic studies of radiation exposure and develop models for calculating
___________________
10 See http://www.iscors.org.
11 Vincent Holahan, U.S. NRC, and Mike Boyd, EPA, presentation to the committee on August 26, 2021.
risks of radiogenic cancers following low doses of radiation. Models and approaches recommended by the National Academies and UNSCEAR and extensions and modifications to them have been foundational in the radiation protection systems worldwide.12 Both the National Research Council’s BEIR reports (NRC, 2006a) and the UNSCEAR reports (UNSCEAR, 2006a) have supported the use of LNT and application of a dose and dose-rate effectiveness factor for solid cancers but have used a linear-quadratic model for leukemia. The BEIR VII committee notes that the difference between the linear and linear-quadratic models in the low-dose ranges is small relative to the uncertainty in the risk estimates (NRC, 2006a). A pooled analysis of leukemia risk following low-dose exposures in childhood, published over a decade after the BEIR VII and UNSCEAR reports, did not find strong evidence for departure from a linear model (Little et al., 2018).
A strong scientific underpinning for radiation protection is critical to adequately and appropriately protect people from exposure to radiation while making the most effective use of resources. Uncertainties in low-dose radiation risks raise questions about whether dose limits and guidance levels are set appropriately or whether they are set too high and therefore do not sufficiently protect workers and members of the public or too low and therefore result in unnecessary costs to reduce radiation exposure. Federal agencies have been formally challenged by members of the public about the use of LNT to set radiation protection standards at least twice in the recent past.
In 2015, the U.S. NRC received three petitions proposing that the agency raise its occupational and public dose limits so that higher exposures become permissible compared to those allowed today (U.S. NRC, 2015a). The U.S. NRC denied these petitions for rulemaking in 2021 and stated that “the LNT model continues to provide a sound regulatory basis for minimizing the risk of unnecessary radiation exposure” to both members of the public and radiation workers (U.S. NRC, 2021). Also in 2021, following a complaint that alleged that EPA is not following the best-available science regarding low-dose radiation because of its reliance on the LNT model, EPA’s Office of Inspector General began an evaluation to examine EPA’s process for updating federal radiation policies and guidance, specifically those that rely on the LNT model (EPA, 2021). The investigation found that although EPA does not have a formal process for updating its federal radiation guidance, the agency has taken steps to ensure that its radiation guidance, including that regarding low-dose
___________________
12 For example, in 2011, EPA updated its estimates of cancer incidence and mortality risks due to low doses of ionizing radiation based on the 2006 BEIR VII recommendations.
radiation exposure, is updated and informed by the best-available and peer-reviewed science (EPA, 2022).
EPA states that “new science on radiation health effects” would affect its approach to protecting the public from radiation exposure (EPA, 2018b). Although state-of-the-art science is the essential ingredient in improving radiation regulations and guidance, regulations and guidance are not automatically updated when new scientific recommendations occur. For example, the U.S. NRC’s regulations for protection against radiation (known as 10 CFR Part 20) are still based primarily on scientific publications issued in the 1970s (ICRP, 1977, 1979) despite these publications being superseded by newer ones (ICRP, 1991, 1994, 1995, 2007). An example of differences between scientific consensus and U.S. radiation protection regulations relates to the allowable exposure to radiation workers and to the lens of the eye. ICRP recommends limiting the annual exposure to radiation workers to 20 mSv (ICRP, 2007) and made a substantial revision to the equivalent dose limit to the lens of the eye for radiation workers and reduced it from 150 mSv per year to 20 mSv per year (ICRP, 2012). The U.S. NRC regulatory limit for the annual exposure to radiation workers is 50 mSv total effective dose equivalent, with an additional limit for the lens of the eye at 150 mSv per year. According to the U.S. NRC, these requirements and adherence to the principle of ALARA result in occupational exposures that are generally below these newer ICRP recommendations.
3.3.1 The Regulatory Development Process
When a change in standards requires a new regulation or a change in an existing regulation, the process typically involves the following steps:13
- Agency develops proposed regulation and supporting analysis.
- Office of Management and Budget (OMB) reviews the proposed regulation and supporting analysis, if applicable.14
- Agency publishes preamble and proposed rule in the Federal Register, placing supporting technical documents in the regulatory docket, and requests public comments.
- Agency develops, OMB reviews (if applicable), and agency publishes final rule and supporting documents.
___________________
13 Lisa Robinson, Harvard T.H. Chan School of Public Health, presentation to the committee on October 27, 2021.
14 The U.S. NRC is excluded from OMB review because it operates independently of the White House, like the Federal Reserve Board or the Consumer Product Safety Commission.
- Congress reviews rule under the Congressional Review Act, if applicable.
- Federal courts review the rule, if applicable, for example, when an agency is sued by one or more stakeholders.
3.3.2 Decision-Making Frameworks for Radiation Protection
Risk-based regulation is a particular strategy or set of strategies that regulators use to target their resources at those sites and activities that present threats to their ability to achieve their objectives.
Economic analysis of the impacts of the proposed change (Step 1 in the regulatory development process described in the previous section) is required if the regulation is economically significant or the regulation is issued by an executive branch agency, such as EPA, and cabinet agencies that report to the President. Agencies may also choose to assess the impacts of less significant regulations, and independent agencies such as the U.S. NRC typically follow the analytical requirements voluntarily. Central to the analysis of proposed changes to regulations is an understanding of the risks with and without regulation. The expert who briefed the committee15 noted that such risk assessments, and the benefit-cost analyses they support, motivate detailed examination of impacts, and important discoveries are typically made during the process. These discoveries may include a better understanding of the preferences of those affected by the regulation; the key sources of uncertainty; the magnitudes of the costs and benefits; the effectiveness of alternative policies; the distribution of the impacts across types of organizations and advantaged and disadvantaged individuals and groups; sources of support and opposition; and otherwise unanticipated consequences. Comparison of alternative regulatory and nonregulatory alternatives is desirable to identify the most appropriate use of resources.
Typically these regulatory benefit-cost analyses inform rather than determine a decision. Decision-makers also consider legal and political issues, budgetary constraints, and ethical ramifications and community sentiments. Independent of the outcome, this type of analysis can assemble and integrate relevant evidence to support complex decision-making in transparent ways.
Several federal agencies have published extensive guidance on regulatory analysis (see, e.g., DOT, 2021; EPA, 2010 [with updates; undergoing revision]; HHS, 2016; U.S. NRC, 2017 [draft update]). In radiation protection regulations, the usefulness and acceptability of an analysis depends
___________________
15 Lisa Robinson, Harvard T.H. Chan School of Public Health, presentation to the committee on October 27, 2021.
on how well its scientific evidence and underlying assumptions and their implications are understood by those planning to use its results. A crucial element of regulatory analysis is a characterization of the risk of the disease caused by the level of radiation the regulation aims to limit. This is often called the baseline risk; the residual risk is the amount of risk expected to remain after the regulatory limit is implemented.
3.3.3 Characterization of Risk in the Regulatory Development Process
Lave (1981) identified the different frameworks used by regulatory federal agencies, arranged them in a typology, and described the informational requirements that each framework places on those responsible for managing risk. Each framework seeks to answer the same question: How safe is safe enough? The committee simplified Lave’s typology into four basic frameworks—negligible risk, lowest feasible risk, net risk, and cost-benefit balancing—and discusses each framework briefly below. Although these frameworks are only part of the radiation protection risk governance, this discussion illustrates the importance of low-dose radiation knowledge and therefore research in low-dose radiation health effects to inform radiation protection regulation and guidance. Each aspect of a risk-based framework involves a complex set of decisions that regulators need to take including selecting the methods they will use to assess those risks; managing the implementation of the risk-based framework; justifying and communicating about it; responding to changes; and, ultimately, setting the level of acceptable risk.
Negligible Risk
When protecting the public from exposure to ionizing radiation, the most ambitious goal might be to eliminate exposure in its entirety and thereby accomplish zero risk. However, accomplishing zero risk from radiation is impractical and in fact impossible due to background radiation that constitutes about half of the annual exposure to the U.S. population today. As a step toward practicality, regulators developed the concept of negligible risk, also called “de minimis risk.”16 Whether a risk is negligible depends on multiple factors such as the incremental probability of harm, the severity of the harm, whether the risk of harm is assumed voluntarily or involuntarily by those exposed, and the number of people exposed to the potential harm. Regulators could either consider that no safety measures need to be taken to address a negligible risk or regulate it in a more permissive way than a non-negligible risk.
___________________
16 Monsanto Co. v. Kennedy, 613 F.2d 947 (DC Cir. 1979); see, generally, Whipple (1987).
There is no general agreement on how small a risk must be for it to be considered negligible; the most common approach in cancer risk management, where exposures are often involuntary and the harm can be premature death, is to define a threshold probability that is sufficiently small above which risks are addressed and below which risks may be accepted. The number of people exposed may also be considered.
The concept of negligible risk originated in food law where exceptions were needed to allow minute concentrations of chemical additives or contaminants in food or animal feed that pose at most a negligible risk of cancer to the public. In food law the threshold for fatal cancer was defined as a 1 in 1,000,000 chance on a lifetime basis when an LNT model is used to compute risk (FDA, 1977). For comparison, the risk of dying from cancer is 1 in 5 (ACS, 2020). An incremental risk might be considered negligible if it increased that background risk of cancer death to no more than 1.00001 in 5.
Another way to comprehend such a small risk of death is to compare it to another involuntary risk of death that people experience routinely. Commercial aviation poses an involuntary risk of fatality to people on the ground as well as a voluntary risk to passengers and crew. According to one rough calculation, the lifetime probability that a person on the ground in the United States will be killed by a crashing airplane is about 4 in 1,000,000. The risk to groundlings is larger for people living near airport runways, and some measures are taken to protect those groundlings. This comparison has for decades been used in risk communication (Goldstein et al., 1992).
Negligible-risk concepts also have a place in the history of federal radiation protection policies, especially at the U.S. NRC and EPA. In 1986, the U.S. NRC adopted a variety of qualitative and quantitative safety goals for the operation of nuclear power plants. For example, the risk of latent cancer fatalities from living within 10 miles of such plants should not exceed “one tenth of one percent” or 0.001 of the sum of cancer fatality risks resulting from all causes (U.S. NRC, 1986). Assuming a baseline fatal cancer risk of 1 in 5 (ACS, 2020), this translates into a safety goal for cancer death risk of 2 in 10,000 per year, or 140 in 10,000 per lifetime, assuming the standard lifetime assumption at the time, which was 70 years.
Under both the Clean Air Act and the Superfund program for cleanup of hazardous wastes, EPA uses a negligible-risk range for fatal cancer of 1 in 10,000 to 1 in 1,000,000 per lifetime. The most exposed individual must be protected against risks at the higher end of the range, and as many exposed people as possible must be protected against the smaller risk level of 1 in 1,000,000.17 Inherent in EPA’s risk formulation is that at any such
___________________
17 Natural Resources Defense Council v. EPA, 838 F.2d 1224 (D.C. Cir. 1987).
risk level, the size of the exposed population will determine the number of cases that will occur during any given time period. For example, consider the risk of cancer due to long-lived radionuclides in nuclear waste near a community with a population of 10,000. Assuming a stable population and an average 85-year life span, a lifetime risk of 1 in 100,000 would result in one additional cancer every 850 years. Weinstein et al. (1996) reported that such formulations for lower-level risks are of less concern to the public.
In the early 1990s, the U.S. NRC and EPA engaged in a harmonization effort on radiation risk management because EPA’s negligible-risk range under the Clean Air Act appears more protective than the U.S. NRC’s negligible-risk level for community exposure (GAO, 1994, 2000). These discrepancies in the standards arise because of their different regulatory applications and different technical methodologies to derive them. The agencies acknowledged that EPA tends to set stringent risk limits but then permits variances or exemptions for facilities on a case-by-case basis where compliance is not practical. The U.S. NRC’s risk-based limits on radiation doses appear less stringent, but the U.S. NRC requires licensees to consider additional measures (“reasonably demonstrated technology”) to drive exposures as far below the risk limits as reasonably achievable. Thus, the net impact of the two agencies’ regulatory practices is more alike than one would assume by simply comparing the numerical risk levels of negligible risk (Sadowitz and Graham, 1995). Despite decades of dialogue, the two agencies have not accomplished complete harmonization of radiation risk management methodologies.
The level of negligible risk for a worker is typically different—and larger—than for a community resident, presumably because risk to the worker arises from a contractual relationship (and therefore financial benefit) and the size of the exposed worker population may be smaller than the size of the exposed community population. Concerning fatal cancer risk, OSHA has not precisely defined a level of negligible risk but has indicated that cancer death risk levels above 1 in 1,000 for a career are “significant” enough to justify rulemaking, and risks below 1 in 100,000 might be considered safe (Sunstein, 2002). This “significant” risk threshold emerged from litigation (discussed below) surrounding OSHA’s 1980 benzene standard (Graham et al., 1988).
Decision theorists have raised some thorny normative problems with the concept of negligible risk (Lundgren and Stefánsson, 2020). For example, if it is inexpensive to eliminate negligible risks, why not eliminate them? If a person is exposed to 100 negligible risks from different sources, is the cumulative overall risk still negligible? The concept of negligible risk survives, however, due to tradition and practicality considerations.
Net Risk
In a setting where a regulation would reduce some risks but increase other risks, the regulator could compare the risks and ensure that the regulation is designed to reduce net risk (Graham et al., 1995). The risk-tradeoff concern emerged at EPA under the Safe Drinking Water Act where the chlorination—and alternative processes (e.g., ozonation)—of drinking water is associated with both health benefits and health risks. In the Safe Drinking Water Act amendments of 1996, Congress required EPA to weigh such “health-health tradeoffs” when setting maximum contaminant levels (Sunstein, 2002). The tradeoff analysis ensures that reducing exposure to one contaminant to benefit health does not cause unacceptably large increases in risk from exposure to a different contaminant.
The net-risk framework may be applicable to decisions about whether to evacuate or relocate communities following a nuclear or radiological incident. As discussed earlier in this report (see Section 2.1.5), recent research following the 2011 Fukushima nuclear power plant accident suggests that evacuations intended to avoid radiation exposure may trigger both immediate and longer-term risks in the impacted communities. At the same time, the risks of staying in the contaminated area due to damaged infrastructure, interruptions in food and medical supplies, human assistance, and other factors have not been sufficiently quantified. A net-risk decision framework would require the risk manager to analyze and weigh these risk tradeoffs.
Lowest Feasible Risk
The feasibility standard in risk management has roots in the Occupational Safety and Health Act of 1970. Congress stipulated that OSHA, when setting health standards, “shall set the standard which most adequately assures, to the extent feasible, on the basis of the best available evidence that no employee will suffer material impairment of health or functional capacity even if such employee has regular exposure to the hazard dealt with by such standard for the period of his working lifetime” (Occupational Safety and Health Act § 6(b)(5)). What did Congress mean by the word “feasible”?
Based on a series of rulemakings and judicial decisions from 1970 to 1979, OSHA defined two dimensions of feasibility: technological capability to reduce worker exposures and financial capability of the industry to reduce worker exposures. OSHA argued that the health standard should be as health protective as possible for workers unless no technology is available to meet the standard or the standard would be so costly that it would bankrupt a substantial segment of the affected industry (OSHA, 1977). According to this definition of feasibility, OSHA did not need to conduct a
quantitative risk assessment or perform a cost-benefit analysis to support a new health standard. Instead, a qualitative determination of hazard is sufficient to support rulemaking, and the stringency of rule is based on the industry’s financial capability to reduce worker exposures.
Industry challenged OSHA’s definition of feasibility in litigation about new standards to limit worker exposure to benzene and cotton dust. Industry argued that OSHA should be required to support a new health standard with a quantitative risk assessment of worker exposures and with a cost-benefit analysis of alternative standards.
The U.S. Supreme Court rejected OSHA’s complete reliance on the affordability test and in the benzene case (1980), vacated OSHA’s new benzene standard. In a plurality opinion, Justice John Paul Stevens explained, based on “reasonably necessary” language in the preface of the Act, that OSHA had not demonstrated that benzene exposure at the prevailing standard was a “significant risk” and that the lower standard would “significantly reduce that risk.”18 In response to this decision, OSHA now supports new health standards with quantitative risk assessments.
In the cotton dust case (1981), the court affirmed OSHA’s new cotton dust standard. Writing for a court majority, Justice William Brennan reasoned that “feasible” means “capable of being done,” which does not entail a cost-benefit analysis. Brennan reaffirmed the court’s previous reasoning concerning significant risk.19
In the 40 years since the court’s cotton dust decision, two developments have limited the Brennan reasoning to the OSHA context (Masur and Posner, 2018). First, feasibility-like concepts also appear in environmental laws such as the Clean Air Act and the Clean Water Act. Recent judicial interpretations of those concepts (e.g., “best available technology”), where the policy objective is protection of the public, have tended to permit cost-benefit considerations (Noe and Graham, 2020; Sunstein, 2017). Second, presidential executive orders since 1981 have required agencies to prepare cost-benefit analyses of economically significant rulemakings. The findings from such analyses may not be used to override statutory requirements (Carey, 2014). This “cost-benefit balancing” is discussed in the next section.
Feasibility-like concepts influence radiation protection at the U.S. NRC, but they have evolved differently from those at OSHA and EPA. The U.S. NRC’s safety goals for the design of nuclear power plants call for a first level of risk-based protection (regardless of costs) plus additional protection based on “reasonably demonstrated technology” to protect the residents living within 50 miles of the plant. Technically, this approach has been
___________________
18 Industrial Union Department, AFL-CIO v. American Petroleum Institute, 448 U.S. 607 (1980).
19 American Textile Manufacturers Institute v. Donovan, 452 U.S. 490 (1981).
defined to reduce radiation exposures to ALARA, subject to a favorable ratio of benefits to costs. The U.S. NRC’s approach, including use of cost-benefit analysis, is also discussed in the next section.
Cost-Benefit Balancing
In the laws governing consumer product safety, toxic substances, and pesticides, Congress has called for prevention of “unreasonable” risks, which means weighing the costs and benefits of regulatory alternatives and choosing the alternative with the most favorable balance of benefit to cost. Where Congress is silent or ambiguous about the applicable decision-making framework, presidential executive orders require agencies to support new regulations with an analysis of benefits and costs.
In some laws, Congress expressly uses cost-benefit language. In the Safe Drinking Water Act Amendments of 1996, Congress directed EPA to establish a drinking water standard for radon based on a novel cost-benefit approach. Since control of radon in drinking water can be costly, Congress authorized EPA to allow states and water systems to offset high levels of radon in drinking water with programs to reduce indoor air radon levels. Based on a National Academies report on radon (NRC, 1999a), EPA estimated that radon is responsible for about 21,000 lung cancer deaths every year (EPA, 2003), only 160 of them due to inhalation of radon that evaporated from drinking water. In its 1999 proposed rule, which allowed states to focus on indoor air radon levels instead of waterborne radon, EPA estimated $362 million in benefits due to reductions in the number of cancers compared to a best estimate of $121 million in costs related to engineering costs of treatment systems, with a range of cost estimates from $60 million per year to $408 million per year (EPA, 1999). The EPA rulemaking is still pending.
The U.S. NRC staff conduct a regulatory analysis, including cost-benefit analysis, of any changes to the agency’s radiation protection guidance. To compare the monetary costs of radiation protection measures to health benefits, the U.S. NRC uses a “dollar per person-rem”20 conversion factor of $5,200 in 2014 dollars (U.S. NRC, 2022).21 The number results from the multiplication of the U.S. NRC’s $9 million value of a statistical life (VSL) by a mortality risk coefficient of 5.8 × 10−4 per person-rem.22,23
___________________
20 The U.S. NRC continues to use the conventional unit “rem.”
21 The U.S. NRC recently reassessed its dollar per person-rem conversion factor policy (U.S. NRC, 2022). The dollar per person-rem conversion factor used by the U.S. NRC until recently was $2,000 (U.S. NRC, 1995).
22 Letter from John Tappert, U.S. NRC, to Ourania Kosti, National Academies, on October 8, 2021.
23 The U.S. NRC adopted the EPA cancer mortality risk coefficient that is based on the 2006 BEIR VII committee report (NRC, 2006a) and is specific to the U.S. population.
VSL is an economic value used to approximate society’s willingness to pay for reductions in mortality risks. Because mortality risk reduction is most often the basis for the justification for government policies, VSL is an important component of the benefit-cost analyses that are part of the regulatory process in the United States. The U.S. NRC’s VSL value of $9 million is consistent with the values used at other federal agencies. For example, EPA and the Department of Transportation use VSL values around $9–$10 million (Viscusi, 2018).
A literature review discussed in the U.S. NRC’s recent white paper (U.S. NRC, 2020b) indicated that federal agencies vary considerably in how they monetize nonfatal health effects. Moreover, since the U.S. NRC’s VSL measure is based primarily on studies of fatal injury in the workplace, the U.S. NRC may consider a cancer premium on the basis that public willingness to pay to prevent a cancer death could be larger than a death from occupational injury. As knowledge of low-dose radiation health effects advances to quantify non-cancer health effects (e.g., cardiovascular effects, neurological disorders, and other effects), monetization techniques will also be necessary for those health effects.
When radiation protection measures are analyzed in medicine, the VSL approach to monetization is rarely used (IOM, 2006). Instead, clinical strategies are compared with cost-effectiveness ratios, where the numerator of the ratio is the net cost of the clinical strategy (gross costs of technology and labor minus any savings in health care costs from less disease) and the denominator is the number of life years saved or the number of quality-adjusted life years (QALYs) saved, which accounts for morbidity and other quality-of-life factors. Decision-makers then use a critical threshold for the ratio to help determine whether the clinical strategy is worthwhile. There is no consensus among experts as to what the critical threshold needs to be (Menzel, 2021).
One of the advantages of using the QALY approach is that health-utility tools have already been developed to estimate the quality-of-life decrements attributable to contracting cancer and other chronic diseases. Thus, if radiation science quantifies cardiovascular as well as carcinogenic effects, the two health outcomes can be combined with the QALY metric. A disadvantage of the QALY method is that it is not grounded rigorously in welfare-economic theory, which is the intellectual foundation for cost-benefit analysis (IOM, 2006).
One of the limitations of cost-benefit balancing is that it can be seen as disrespectful of fundamental human rights as defined by the United Nations (UN, 2021). Some commentators argue that there is tragedy when premature deaths are not prevented due to cost-benefit considerations (Tallarita, 2020). Others argue that cost-benefit analysis can strengthen the case for protection of human rights (Aceves, 2018).
3.4 POTENTIAL ECONOMIC IMPACTS OF THE LOW-DOSE RADIATION RESEARCH PROGRAM
Costs for complying with radiation protection standards and guidelines, administering radiation compensation programs, or for using technologies that utilize radiation in medical and other applications are balanced with the health, societal, and other benefits based on current scientific understanding of low-dose radiation exposures. These costs are substantial. For example,
- Costs for mitigating the 5 million houses in the United States that have high indoor radon levels exceed $5 billion (see Section 2.1.1).
- Medical costs for radiology services for computed tomography scans alone (see Section 2.1.2) exceed $74 billion assuming cost per scan of $1,000 (Jiang et al., 2022).
- Annual costs to the nuclear industry to comply with regulatory standards (see Section 2.1.4) are about $16 billion (Batkins, 2016; Batkins et al., 2017).
- Costs to respond to nuclear or radiological incidents (see Section 2.1.5) vary significantly depending on the incident. The costs for cleanup of the Fukushima nuclear site, for example, are estimated to reach 35 trillion to 80 trillion yen (approximately $290 billion to $670 billion) over 40 years (JCER, 2019).
- Future liability for compensation program payments will cost billions of dollars. For example, Energy Employees Occupational Illness Compensation Act payments (see Section 2.1.6) alone have been estimated to be about $43 billion (Gross, 2021).
- Cleanup of nuclear waste sites will cost hundreds of billions of dollars over several decades (see Section 2.1.7) and the costs per site accelerate the more restrictive the protection levels (GAO, 2000). For example, although decades old, past analysis of cleanup options for plutonium contamination at the Nevada Test Site estimated $35 million in costs to achieve a 1-mSv/year level. The costs were three times higher to achieve a 0.25-mSv/year level, six times higher to achieve a 0.15-mSv/year level, and 28 times higher to achieve a 0.5-mSv/year level (GAO, 2000).
To the committee’s knowledge, comprehensive estimates of overall costs to federal agencies and society to comply with current radiation protection standards and guidelines are unavailable. Similarly, comprehensive estimates for the overall cost savings for protecting the U.S. population’s health by implementing these standards and guidelines are also unavailable. Without these current estimates as a starting point, preparing comprehensive
estimates of overall costs to comply with prospective radiation protection standards or guidelines is not possible. In addition, the committee judges that it would be inappropriate to speculate what the new scientific information might be or how it may be used by radiation protection agencies; therefore, it cannot quantitatively estimate the potential economic impacts of the low-dose radiation research program. When adjustments in radiation protection standards and guidance are proposed based on new information, agencies can estimate the economic impacts of the changes and perform benefit-cost and cost-effectiveness analyses of alternative measures. These analyses can also be informed by econometric studies of the social impacts of low-dose radiation exposures on health or other endpoints (e.g., education) which have provided plausibly causal economic loss estimates associated with these exposures (Almond et al., 2009; Black et al., 2019; Danzer and Danzer, 2016). Although the committee does not provide a quantitative estimate of the potential economic impacts of the low-dose radiation program, it assesses whether knowledge from low-dose radiation research can affect the decision-making frameworks in the federal regulatory system and how.
The committee’s review of decision-making frameworks in the federal regulatory system reveals that knowledge from low-dose radiation research plays a central role in three of the four frameworks. The negligible-risk, net-risk, and cost-benefit frameworks require estimates of low-dose radiation risks to be implemented. Only the lowest-feasible-risk framework, as implemented by OSHA in the 1970s, did not require knowledge of low-dose health effects, since standard setting could proceed based on a qualitative determination of possible hazard and the stringency of standards was determined entirely by engineering and industrial-affordability considerations. However, the Supreme Court’s decision in the 1980 benzene case required OSHA to perform quantitative risk assessment in the standard-setting process, which in turn required OSHA to estimate benzene-related low-dose health effects. OSHA then justified a new benzene standard as necessary to protect against leukemia and quantified the risk of leukemia to workers on the basis of the LNT model.
Feasibility-like concepts are also employed by EPA and the U.S. NRC, but those concepts typically permit or require cost-benefit analysis as part of the feasibility determination. Thus, the committee concludes that advances in knowledge of low-dose radiation effects will be inherently useful for federal agencies in radiation protection decisions and likely by some agencies charged with compensating impacted communities for damage suffered due to radiation exposures (see Box 2.1).
New knowledge that emerges from the low-dose program can inform the radiation protection regulations and guidance in several ways: by improving understanding of adverse human health effects from exposures at doses and dose rates experienced by the U.S. population, identifying
mechanisms for induction of these health effects, developing improved risk models for doses and dose rates at which direct measurement of risks is not possible, and ultimately developing more individualized risk estimates.
This new information can help address specific concerns raised by patients, workers, members of the public, and communities because of their medical, occupational, and environmental low-dose and low-dose-rate radiation exposures. This new information can also inform national policies such as the future of nuclear power, response to nuclear or radiological incidents, nuclear waste management, and radiation compensation programs.
New findings on health effects emerging from the low-dose radiation program will provide evidence on whether current (primarily cancer) risk estimates at low doses are accurate, underestimated, or overestimated. This evidence may impact radiation protection by confirming that current regulations and guidance sufficiently protect human health or by supporting either more restrictive or less restrictive regulations and guidance. Importantly, new findings will inform radiation protection for health outcomes currently not considered in radiation protection systems or radiation compensation programs.
In some setting(s), anti-backsliding provisions in agency statutes preclude changes to current regulations unless changes provide for greater protection of the health of persons. In any case, a challenge for the federal government agencies with radiation protection responsibilities will be reaching consensus on how new findings on health effects emerging from the low-dose radiation program need to inform or alter radiation protection regulation and guidance and achieve harmonization of risk goals.
3.5 CHAPTER SUMMARY AND FINDINGS
Exposures to low levels of radiation may carry low levels of risk to an exposed individual; nonetheless, they are a high priority for the radiation protection system. The vast majority of regulations and guidance in the radiation protection system tend to address low-dose exposures. In the United States, several federal agencies, and in some instances states, administer radiation protection standards and guidelines.
A strong scientific basis for radiation protection is critical to ensuring adequate and appropriate protection of the U.S. population from the use of radiation while making the most effective use of resources. Uncertainties in low-dose radiation risks raise questions about whether dose limits and guidance levels are set appropriately or whether they are set too high and therefore do not sufficiently protect workers and members of the public or too low and therefore result in unnecessary costs to reduce radiation exposure. The regulatory development process to update standards is a multistep process that requires a supporting analysis that involves an
understanding of the risks without the proposed regulation and risk-reduction improvements of the proposed regulation. Advances in knowledge of low-dose radiation effects will be inherently useful for federal agencies in radiation protection decisions and in decisions in support of radiation compensation programs.
Costs for complying with radiation protection standards and guidelines, administering radiation compensation programs, or for using technologies that utilize radiation in medical and other applications are balanced with the health, societal, and other benefits based on current scientific understanding of low-dose radiation exposures. These costs are substantial but to the committee’s knowledge, comprehensive estimates of overall costs to federal agencies and society to comply with current radiation protection standards and guidelines are unavailable. Similarly, comprehensive estimates for the overall cost savings for protecting the U.S. population’s health by implementing these standards and guidelines are also unavailable. Without these current estimates as a starting point, preparing comprehensive estimates of overall costs to comply with prospective radiation protection standards or guidelines is not possible.
Finding 2: Comprehensive understanding of adverse human health effects emerging from the multidisciplinary low-dose radiation program will enable better assessment of whether current risk estimates (primarily for cancer) at low doses and low dose rates are accurate, underestimated, or overestimated and provide improved risk estimates for other adverse health outcomes. This assessment may impact radiation protection by confirming that current regulations and guidance sufficiently protect human health or by supporting either more restrictive or less restrictive regulations and guidance.
Finding 3: The committee is unable to quantify the low-dose radiation program’s economic impacts because comprehensive estimates of overall costs to comply with current radiation standards are unavailable. Additionally, any changes to the current estimates will depend on new information on adverse health effects that will be generated by the low-dose radiation research program. When adjustments in radiation protection standards and guidance are proposed based on new information, agencies can estimate the economic impacts of the changes and perform benefit-cost and cost-effectiveness analyses of alternative measures.