
The Nursing Home Workforce
Nursing homes rely on 1.2 million health care and support workers in a wide range of occupations to help residents achieve their goals through the provision of medical, nursing, and social care to both treat illness and meet basic human needs. Nursing home workers also attend to infection prevention and control, therapeutic and recreational activities, housekeeping, and other needs of the residents. One challenge is that the heterogeneity and complexity of care needs has increased dramatically over the last 20 years, while average direct-care staffing has changed very little (MedPAC, 2016; Tyler et al., 2013). Federal guidelines dictate that facilities must “have sufficient staff to assure the safety of residents and attain or maintain the highest feasible level of physical, mental, and psychosocial well-being of each resident.”1 However, adequate staffing in nursing homes has been difficult to achieve for multiple reasons, including a negative perception of nursing homes, unsupportive working conditions, and poor pay and benefits. In his remarks to this committee, Donald Berwick, a president emeritus and senior fellow at the Institute for Healthcare Improvement, said
You can’t get patient and family experience as a central point in a demoralized workforce or undersupported workforce. And I’m thoroughly convinced that the conditions of work in the American nursing home are unsupportable if we want improvement.
This chapter provides an overview of the nursing home workforce, including their education and training, turnover rates, necessary competencies,
___________________
1 CMS Requirements for Long-Term Care Facilities—Administration, 42 CFR § 483.70(e) (2016).
challenges with recruitment and retention, and connection to quality of care. Chapter 4 discusses the range of services provided by different members of the nursing home workforce.
THE OVERALL NURSING HOME WORKFORCE
The number and types of staff members in a nursing home vary depending on the number of residents, the complexity of their needs, and the scope of services provided. While nursing homes employ many workers directly, they may also provide care through referrals to consultants or by contracting workers rather than hiring them as employees. Additionally, family members and volunteers provide various needed services for the care of nursing home residents. Given the scope of care needed, interdisciplinary teams involving multiple staff members with distinct skills and responsibilities are critical to providing high-quality care to nursing home residents. While there are specific regulations for reporting nurse staffing data and steps to ensure the accuracy of those data, much less information is available about the wide range of other providers, and the information that is provided on public sites may not be accurate (OIG, 2021).
Nursing Home Employees
People employed by nursing homes represent a wide variety of occupations from 19 different major groups of the North American Industry Classification System for business establishments in the United States (BLS, 2020a). As Figure 5-1 shows, the bulk of workers are in health care support occupations (41 percent) and health care practitioners and technical occupations (27 percent). As these data only represent individuals employed directly by nursing homes, they may not be fully reflective of the entire workforce that helps to support nursing home residents. Examples from each of the reported categories are presented in Table 5-1. While not all of these occupations will be discussed at length in this chapter, these examples show the breadth of the nursing home workforce.
Temporary Agency Staff and Consultants
Nursing homes may employ temporary staff to fill in during staff absences and shortages. These temporary staff, usually referred to as “contract” or “agency” staff (because they are typically obtained through contracts with staffing agencies), can cost the facility (because of additional agency fees) up to twice as much as a permanent employee (Hale and Hale, 2019; Seavey, 2004). Many nursing homes increased their use
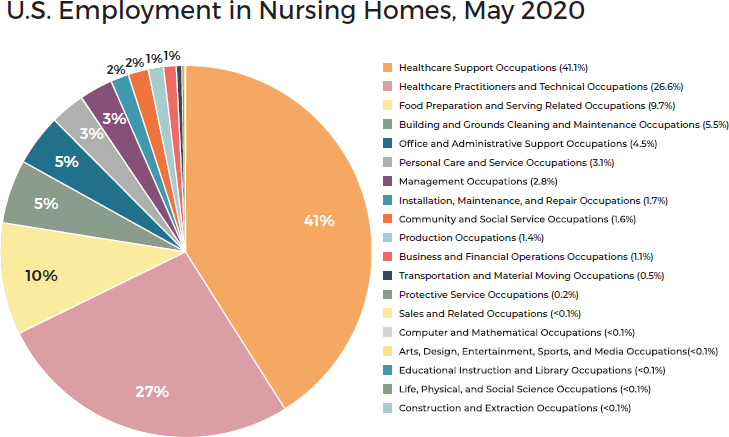
SOURCE: BLS, 2020a.
of agency staff to fill gaps during the COVID-19 pandemic (Peck, 2021; Stulick, 2021). Contract staff accounted for about 5.8 percent of all nursing staff hours in the second quarter of 2021 (LTCCC, 2022).
Nursing home residents may also receive care in the nursing home setting from consultant health care professionals who are not employed directly by nursing homes. Instead, these providers bill insurers directly for the care they provide and do not require supervision from nursing home staff. Examples include care provided by podiatrists, optometrists, and dental professionals (CMS, 2021a; Hill, 2017; Lee et al., 2001; NHLC, 2021). Consultant care may also be provided by transferring residents to health care professionals in private offices for care that cannot be provided within the nursing home setting.
Family Caregivers and Volunteers
Family caregivers (including both family and other care partners) and volunteers from the community (who are neither friends nor family members of residents) also play an important role in the care of nursing home residents. Family caregivers, described as “an invisible workforce in nursing homes,” are an essential component of the workforce, providing care even
TABLE 5-1 Occupation Classifications and Examples of Roles in U.S. Nursing Homes
| NAICS Occupations | Examples of Roles |
|---|---|
| Health Care Support (41 percent) | Nursing assistants; orderlies; occupational therapy, physical therapy, and recreational therapy assistants and aides; and medical assistants |
| Health Care Practitioners and Technical (27 percent) | Dietitians; occupational, physical, respiratory, recreational and speech-language therapists; licensed nurses (e.g., registered nurses, advanced practice registered nurses); physicians; physician assistants; pharmacists; dentists and dental hygienists; clinical laboratory and radiologic technologists and technicians; medical records specialists; and health information technologists |
| Food Preparation/Serving-related (10 percent) | Food preparation and serving workers, cooks, cafeteria attendants, and dishwashers, and supervisors |
| Building and Grounds Cleaning and Maintenance (5 percent) | Housekeeping and janitorial workers, landscaping and groundskeeper workers, and supervisors |
| Office and Administrative Support (5 percent) | Financial clerks, information and record clerks, office clerks, secretaries, and receptionists |
| Personal Care and Service (3 percent) | Entertainment workers and hairdressers |
| Management Occupations (3 percent) | Chief executives, general and operations managers, marketing and sales managers, financial managers, human resources managers, food service managers, and medical and health services managers |
| Installation, Maintenance, and Repair (2 percent) | General maintenance and repair workers and their supervisors |
| Community and Social Service (2 percent) | Social workers, social and human service assistants, substance abuse and mental health counselors, community health workers, and clergy |
| Production Occupations (1 percent) | Laundry workers |
| Business and Financial Operations (1 percent) | Human resources workers, marketing and management analysts, and financial specialists |
| Transportation and Material Moving (0.5 percent) | Drivers, parking attendants, and stockers and order fillers, and supervisors |
| Protective Services (0.2 percent) | Security guards |
| Sales and Related (<0.1 percent) | Sales and marketing representatives |
| Computer and Mathematical (<0.1 percent) | Computer network support specialists, computer user support specialists, and network and computer systems administrators |
| Arts, Design, Entertainment, Sports, and Media (<0.1 percent) | Public relations specialists and interpreters and translators |
| Educational Instruction and Library (<0.1 percent) | Special education teachers |
| Life, Physical, and Social Science (<0.1 percent) | Occupational health and safety specialists and technicians |
| Construction and Extraction (<0.1 percent) | Carpenters and painters |
SOURCE: BLS, 2020a,b.
NOTE: NAICS = North American Industry Classification System.
after their loved ones have entered the nursing home (Coe and Werner, 2021, p. 110; also see Davies and Nolan, 2006; Gaugler, 2005; Reid and Chappell, 2017). Indeed, care provided by family caregivers is even more critical today than in the past, given the nationwide shortage of direct-care workers and high turnover (Antwi and Bowblis, 2018; Gandhi et al., 2021). Furthermore, the COVID-19 pandemic revealed the impact of family caregivers in several ways. Notably, policies that prohibited family and friends from entering nursing homes may have exacerbated staffing shortages because these family members and friends were not able to contribute to the care of their loved ones (Werner and Coe, 2021). Additionally, family caregivers often provided needed social connections, and COVID-related visitation policies contributed to social isolation and loneliness for residents (Abbasi, 2020a; Bethell et al., 2021; Veiga-Seijo et al., 2021).
While volunteers from the community may also assist with the care of nursing home residents, very limited research exists on this segment of the nursing home workforce, including on their training and on its impact on the quality of care. (See later in this chapter for more on family caregivers and volunteers.)
Interdisciplinary Team Care in the Nursing Home
Meeting the physical, psychosocial, mental, emotional, and spiritual needs of persons in nursing homes requires an interdisciplinary approach. “Interdisciplinary team work is a complex process in which different types of staff work together to share expertise, knowledge, and skills to impact on patient care” (Nancarrow et al., 2013). Consistent features of successful interdisciplinary interventions include formal team-based care, communication, coordination, and leadership (Nazir et al., 2013). The 2001 Institute of Medicine (IOM) report Crossing the Quality Chasm identified interdisciplinary teams as an essential component of high-quality care delivery and improved patient safety (IOM, 2001a). In long-term care settings,
interdisciplinary teams result in improved resident outcomes for a variety of reasons. For example, interdisciplinary teams are better able to adapt to complex systems of care through improved cooperation, collaboration, and communication that ensures that care is continuous and reliable (IOM, 2003). They are also better equipped to meet residents’ needs, keep pace with the demands of new technology, respond to the demands of payers, and deliver care across settings (IOM, 2003). In addition, there is also evidence that an interdisciplinary approach for assessing and planning care is related to the psychological well-being of residents, earlier intervention of residents’ medical conditions, lower costs, reduced staff turnover, and increased staff satisfaction (IOM, 1996; Mukamel et al., 2009; Temkin-Greener et al., 2009; Zimmerman et al., 2016).
Federal nursing home regulations refer repeatedly to the interdisciplinary team in areas such as care and discharge planning, using physical and chemical restraints, preventing falls, treating incontinence and pressure injuries, managing pain, addressing behavioral health needs, accounting for significant change in health status, and preparing advance directives. Most nursing homes today have some form of an interdisciplinary team in order to comply with the Resident Assessment Instrument/Minimum Data Set process and accreditation requirements2 (Dellefield, 2006; Temkin-Greener et al., 2009). (See Box 4-3 in Chapter 4 for a description of the requirements for the interdisciplinary care team.) According to the Centers for Medicare & Medicaid Services (CMS) Resident Assessment Instrument manual, the interdisciplinary team, along with the resident and resident’s family, engages in developing a person-centered care plan that includes assessment, decision making, identification of outcomes, care planning, implementation of the care plan, and evaluation of care (CMS, 2019a). In its 2016 revised regulations for nursing homes, CMS required that certified nursing assistants (CNAs) be part of the interdisciplinary team and involved in care planning (CMS, 2016). Some have argued that to meet this requirement, nursing homes need to specifically delineate CNAs’ responsibilities on the interdisciplinary team and to provide training in order for CNAs to participate effectively in care planning (Travers et al., 2021). (See Chapter 4 for more on care planning and the role of the interdisciplinary care team.)
NURSING HOME ADMINISTRATION AND LEADERSHIP
A variety of personnel provide high-level leadership in nursing homes. The national median for turnover of “top level executives” at nursing
___________________
2 The Resident Assessment Instrument collects data to guide care planning and monitoring for long-term care residents.
homes is 20.46 percent (HHCS, 2020). In his testimony to this committee, Michael Wasserman, California Association of Long Term Care Medicine, noted:
Effectively providing care for a complex group of individuals requires competencies at every level of the organizational chart. Aside from having an appropriate level of staffing, nursing homes require properly prepared highly skilled leadership teams that can balance the financial, operational, and clinical aspects of this incredibly complex business.
Administrator
A nursing home administrator has oversight and operational responsibilities, including ensuring regulatory compliance, supporting the rights of residents, and maintaining financial accountability. The domains of practice that provide the framework for the national examination of nursing home administrators include (1) customer care, supports, and services; (2) human resources; (3) finance; (4) environment; and (5) management and leadership (NAB, 2017). In 2020, the median salary for a nursing home administrator was $113,000 (HHCS, 2020).
Education and Training
Federal regulations for nursing homes require that the administrator of a nursing home is licensed by the state. However, state requirements for the licensure of nursing home administrators vary in terms of minimum education requirements, training hours, examination requirements, and continuing education requirements (NAB, 2021). Thirty-three of the 50 states and the District of Columbia require a minimum of a bachelor’s degree to be a nursing home administrator, while eight states require only an associate’s degree, and six states require only a high school degree (NAB, 2021). Four states (i.e., Delaware, Indiana, New York, and Wisconsin) do not indicate a minimum degree requirement.
Additionally, 47 of the states and the District of Columbia specify continuing education requirements for nursing home administrators on either an annual or biennial basis (NAB, 2021). However, there is much variation among states regarding these requirements. Eleven states require an average of 24 to 30 hours annually, 26 states and the District of Columbia require an average of 20 hours annually, and 9 states require an average of 12 to 18 hours annually. Four states (i.e., Alaska, Colorado, Hawaii, and New York) do not require continuing education for nursing home administrators.
Characteristics, Tenure, and Turnover
Few studies provide insight on the characteristics of nursing home administrators, and most of the studies that are available are quite old. While these studies may not fully reflect the characteristics of nursing home administrators today, they do provide some insight.
A 2007 study conducted in just two states found the average age of nursing home administrators to be 54 years, with an average tenure of 3.5 years, and with 96 percent holding a baccalaureate or higher degree (Castle et al., 2007). This is important since higher quality of care has been associated with nursing home administrators with higher levels of education and more experience (Castle et al., 2015; Lerner et al., 2014). Older studies of nursing home administrators found annual turnover rates of over 40 percent (Castle, 2001; Castle et al., 2007) and evidence of high instability of tenure within the first 3 years (Singh and Schwab, 2000); they also found that nursing home administrators with lower job satisfaction were more likely to leave within 1 year than administrators with higher job satisfaction. Lower job satisfaction was attributed to several factors, including the administrators’ perceptions of high work demands and inadequate work skills (Castle et al., 2007). The sources of stress for nursing home administrators include challenges with regulations, difficulty with families, limited funds and resources, challenges with staffing, meeting the needs of residents, and corporate issues (Myers et al., 2018).
High turnover among the top management at nursing homes has been associated with a higher turnover of nursing assistants and licensed nursing staff (Castle, 2005), a lower quality of care (e.g., presence of pressure ulcers, use of psychoactive drugs, use of restraints) (Castle, 2001), and a number of inspection deficiencies (Geletta and Sparks, 2013). For a family member perspective on nursing home management, see Box 5-1.
Medical Director
Federal regulations mandate that all certified nursing homes have a medical director who is a physician licensed in the state where the facility is located.3 Requirements of the role include
- (1) Coordinating medical care and providing clinical guidance;
- (2) Overseeing the implementation of resident care policies;
- (3) Ensuring policies and procedures align with current standards of practice; and
- (4) Identifying and addressing issues with resident care or quality of life (CMS, 2005).
The medical director’s role has been described to include the promotion of high-quality clinical care, assistance in reviewing the quality of care, advising on infection prevention and control issues, promoting employee health and safety, and being active in facility-related education and communication (AMDA, 2005). In fact, the 2020 CMS Coronavirus Commission on Safety and Quality in Nursing Homes report reinforced “the importance of medical director engagement in nursing home emergency management planning and execution” (MITRE, 2020, p. 41). Regulations also note that the role of the medical director is separate and independent of that of the attending physician. While most medical directors are also attending physicians in the facility, they do not need to be (CMS, 2005). Regulations require nursing home surveyors to evaluate whether medical directors are licensed, serving, and collaborating with the facility to implement policies. Given the expansive role of medical directors, some facilities have identified a need for an assistant or associate medical director who can be a physician, advanced practice registered nurse (APRN), or physician assistant (Medical Direction and Medical Care Work Group, 2011).
Characteristics
Medical directors are paid for their time and expertise. Compensation arrangements generally allow payment for providing clinical care and referring patients; however, medical directors cannot receive direct payment for future referrals to the facility or other businesses of the facility (Turner, 2015). Data on the compensation, recruitment, retention, and turnover of nursing home medical directors are extremely limited. CMS does not keep any record of the characteristics of nursing home medical directors (e.g., age, medical specialty, certification status, geriatric or medical director
___________________
3 CMS Requirements for Long-Term Care Facilities—Administration, 42 CFR § 483.70 (h) (2016).
training, number of patients served, time spent in the nursing homes) in its databases, which makes research in this area challenging.
Education, Training, and Certification
To carry out their duties, medical directors need specialized knowledge, including high-level knowledge about geriatric syndromes, palliative care principles, dementia care, nursing home regulation and structure, care transitions, infection prevention and control, and quality improvement. However, except for the requirement of a license to practice medicine in the state, there are no additional specific education and training requirements for medical directors. The American Board of Post-Acute and Long-Term Care Medicine offers certification for medical directors in post-acute and long-term care medicine (ABPLM, 2022a). The board requires applicants for this training to meet specific criteria, including previous clinical and management experience in post-acute and long-term care settings (ABPLM, 2022b). Applicants must also complete the Core Curriculum on Medical Direction in Post-Acute and Long-Term Care, a course provided by the Society for Post-Acute and Long-Term Care Medicine (AMDA) (AMDA, 2022). The course focuses on the role and responsibilities of the medical director; the long-term care environment; organizational dynamics; communication skills, leadership skills, and team building skills; and resident care responsibilities (e.g., emergency care, quality management, family systems, and ethics) (AMDA, 2022). In 2021, California enacted a requirement for the certification of all medical directors in nursing homes (CALTCM, 2021).
In his testimony to this committee, Michael Wasserman, California Association of Long Term Care Medicine, noted:
There are far too many medical directors who lack even basic knowledge of geriatric medicine concepts and who have little expertise or even interest in the complex regulatory framework of nursing homes. [Additionally,] residents and their families have a right to know the identity of the medical director, who, under federal regulations, is responsible for resident care policies and coordination of care.
Relationship to Quality of Care
Limited evidence links medical director certification and activities to the quality of care in nursing homes. One 2009 study found that the 547 nursing homes with a certified medical director performed up to 15 percent better on standardized quality scores than the other 15,230 nursing homes in the CMS Online Survey Certification and Reporting database (Rowland et al., 2009).
Director of Nursing
The director of nursing is the nursing home’s chief nurse executive and is pivotal in influencing organizational and clinical outcomes (Rao and Evans, 2015; Siegel et al., 2010). A survey of directors of nursing in Florida nursing homes found that two-thirds or more held additional roles such as infection prevention and control (68 percent), quality management (79.2 percent), staff education (64 percent), and risk management (57.3 percent) (Sherman and Touhy, 2017).
Each nursing home is required to have a full-time director of nursing who is a registered nurse (RN), although there are waivers to this requirement. Directors of nursing have an average tenure of 6.8 years in their current position and 16.2 years of experience in long-term care, although 42 percent of directors of nursing have been in their current position less than 1 year (Lerner et al., 2014). A 2005 survey found a 36 percent annual turnover rate for directors of nursing (Castle, 2005). The average reported salary for directors of nursing is $92,756 with variation based on size and geographic location of the facility and the experience and education of the director of nursing (AADNS, 2019). Directors of nursing in for-profit nursing homes earn about $10,000 more annually than directors of nursing in nonprofit facilities (HHCS, 2020).
In many nursing homes, the director of nursing may be one of a few registered nurses (RNs) or even the only RN. Therefore, in addition to his or her administrative responsibilities, the director of nursing is often called upon to address the clinical needs of residents. Two-thirds of directors of nursing report they are often needed to provide direct care to residents (“pulled to the floor”), and 42 percent report this occurring daily or weekly (AADNS, 2019).
Competencies
The director of nursing needs to have knowledge and competencies in geriatric nursing as well as in administrative areas such as human resource management, staffing, budgeting and cost management, compliance and regulatory standards, and quality improvement. The director of nursing also needs effective leadership and supervision skills. Directors of nursing report spending half of their time in four areas: (1) management meetings, (2) addressing incidents and accidents, (3) staff scheduling, and (4) medication management (AADNS, 2019). Staffing and staff turnover are most consistently noted by directors of nursing as the greatest challenge and as taking most of their time (AADNS, 2019; Sherman and Touhy, 2017; Siegel et al., 2010).
The American Association of Directors of Nursing Services provides certification for directors of nursing based on seven competency domains, and the American Organization for Nursing Leadership has identified
TABLE 5-2 Director of Nursing Competencies
| AADNS Director of Nursing Competencies | AONL Director of Nursing Competencies |
|---|---|
| Leadership | Communication and relationship building |
| Management and supervision | Knowledge of the health care environment |
| Organizational oversight and management | Leadership |
| Business acumen | Professionalism |
| Quality improvement | Business skills |
| Regulatory compliance | |
| Professional development |
SOURCES: AADNS, 2021; AONE/AONL, 2015.
NOTE: AADNS = American Association of Directors of Nursing Services; AONL = American Organization for Nursing Leadership.
five competency areas for the post-acute care nurse executive (see Table 5-2). More broadly, the American Nurses Association outlines the competencies needed by nurses holding administrative positions in any health care organization (ANA, 2016).
Education and Training
The majority of directors of nursing have an associate degree or diploma in nursing (Holle et al., 2019; Olson and Zwygart-Stauffacher, 2008; Sherman and Touhy, 2017; Trinkoff et al., 2015). However, associate degree nursing programs provide no educational preparation to function in an administrative nursing role and limited training in geriatric nursing. Several reports on competencies for directors of nursing have recommended a requirement for a bachelor’s degree in nursing, with a preference for a master’s degree (ANA, 2016; Lodge, 1985). At least one analysis suggests that they should have a master’s degree in nursing administration (Siegel et al., 2010), and 22 experts in gerontological nursing joined to recommend that all directors of nursing attain certification in core geriatric nursing and leadership competencies (Kolanowski et al., 2021). Fewer than half of directors of nursing (42.5 percent) hold any national certification (Trinkoff et al., 2015).
While effective leadership from a director of nursing has been associated with high-quality care (Castle and Decker, 2011; McKinney et al., 2016), no federal or state requirements specify minimum education requirements, continuing education requirements, or additional training requirements for directors of nursing. Previous IOM reports on nursing home quality pointed to the lack of educational preparation for directors of nursing to serve as the top-level nurse leader and administrator of the organization in the context of the complexity of the environment and role (IOM, 1996, 2001b);
concern persists about the lack of administrative and leadership preparation of directors of nursing and its impact on the quality of care (Harvath et al., 2008; Olson and Zwygart-Stauffacher, 2008; Siegel et al., 2010).
Nursing home member organizations, universities, and director-of-nursing organizations have developed continuing education and certification programs to compensate for the lack of preparation that directors of nursing have for the role (LeadingAge Minnesota, 2021; Vogelsmeier et al., 2010). For example, American Association of Directors of Nursing Services and the National Association of Directors of Nursing in Long-Term Care offer the opportunity to attain national certification as a director of nursing (AAPACN, 2021).4
Director of Social Services
The director of social services oversees all social service programs and supervises social workers and social service designees within the facility. Occasionally, the director of social services assists with the implementation of some resident activities, such as the resident council, and assists in the facilitation of admissions tasks. Other leadership positions related to social care focus on activities and the spiritual health of residents, and may include a director of health and wellness, fitness coordinator, activities director/coordinator, and director of pastoral services/spiritual director.
In 2003, the National Association of Social Workers (NASW) developed a consensus statement for professional standards for social work directors in long-term care settings, stating
It is preferable that the social work director be a graduate of a master’s degree program from an accredited school of program of social work, have a minimum of 2 years postgraduate experience in long-term care or related programs, and meet equivalent state requirements for social work practice or, in jurisdictions not having such legal regulation, is a member of the Academy of Certified Social Workers (NASW, 2003, p. 8).
One recent analysis found that while most nursing homes employ social services staff, only 37 percent of nursing homes have a degreed and licensed social worker at the helm of social services, and 42 percent of social services directors do not have a degree in social work (Bern-Klug et al., 2021a). (See later in this chapter for more on the federal requirements of social workers in nursing homes.) Larger not-for-profit nursing homes and nursing homes that are not part of a chain are the most likely to hire a degreed and licensed social worker as a social services director. In 2020, the median salary for a director
___________________
4 For more information on the certification exam, see https://www.nadona.org/product/cert-director-of-nursing-cdon (accessed November 3, 2021).
of social services was $55,188 (HHCS, 2020). Evidence on the characteristics, education and training, job satisfaction, and turnover of social services directors is limited or nonexistent. The few studies that exist are dated and examine very narrow topics (Bell et al., 2010; Bern-Klug and Sabri, 2012; Liu and Bern-Klug, 2013). See the discussion of psychosocial care providers later in this chapter for more about social work staff in nursing homes.
PRIMARY CARE PROVIDERS
Primary care providers actively authorize and supervise the care of residents and review the resident’s total program of care (e.g., medications, treatments) and status (e.g., current condition; progress; and problems maintaining physical, mental, and psychosocial well-being). Regulations mandate that all nursing home residents must have 24-hour access to health care provided by a physician or other qualified practitioner such as APRNs (e.g., nurse practitioner, clinical nurse specialist) and physician assistants. State laws and regulations govern care provided by clinicians other than physicians in terms of physician supervision or collaboration.
Federal nursing home regulations require an initial visit by a physician within the first 30 days of a nursing home resident’s admission, although other required visits may alternate between a physician and other qualified practitioners.5 For initial visits at nursing homes that are not specifically designated as skilled nursing facilities, clinicians not employed by the facility may do the initial visit and documentation.6 Primary care providers are also responsible for writing and signing progress notes for each medical care visit and signing and dating all medical orders. The American Medical Directors Association outlines the comprehensive role of the attending primary care provider in the nursing home (AMDA, 2003).
Only limited and dated evidence exists regarding primary care providers for nursing home residents, particularly for physicians and physician assistants. A national survey of medical directors in nursing homes found that the majority were also the practicing physician in the nursing home and often served as medical directors in two nursing homes (Levy et al., 2007). The survey found that “nearly 80 percent of medical directors served as attending physicians and, on average, were the attending physician to 44 percent of the patients in their facilities” (p. 562). Only 12.5 percent of physicians who bill Medicare have claims for nursing home visits (Jung et al., 2021). Barriers to attracting physicians to nursing home care include the
___________________
5 CMS Requirements for Long-Term Care Facilities—Physician Services, 42 CFR § 483.30 (c)(1) (2016).
6 CMS Requirements for Long-Term Care Facilities—Physician Services, 42 CFR § 483.30 (c) (2016).
minimal geriatrics training that most physicians receive in medical school, low reimbursement, nonreimbursable activities associated with providing medical care in nursing homes, burden of regulations on the physician’s practice and time, and malpractice risk (Kane, 1993; Levy et al., 2007).
At least one recent analysis concluded that research is needed on the practice quality of medical providers and the impact of provider quality on resident outcomes as well as concluding that practice-based quality measures are needed (Katz et al., 2021). Recently, investigators identified a set of quality indicators for the practice of post-acute and long-term care by primary care providers (Mays et al., 2018).
Skilled Nursing Facility Specialists
Care models with physicians, APRNs, and physician assistants serving as skilled nursing facility specialists (SNFists) are increasing. SNFists (akin to hospitalists) are full-time providers to nursing home residents (Teno et al., 2018). For example, one study reported that between 2007 and 2014, the proportion of billing by SNFists increased from 22 to 31.5 percent (Teno et al., 2017). From 2012 to 2015, the mean number of nursing home specialists increased by nearly 34 percent, particularly for practitioners other than physicians (Ryskina et al., 2017). While the numbers of SNFists are growing, particularly among APRNs, there is extreme variation; many nursing homes have almost no full-time primary care providers while in others, almost all residents have a full-time provider (Goodwin et al., 2021). While most SNFists who are physicians have training in primary care (e.g., internal medicine, family medicine), only 6.5 percent specialized in geriatrics (Jung et al., 2021).
One study found that nursing home residents receiving care from SNFists have lower avoidable hospitalizations, are more likely to be discharged to the community, and have more provider visits (Katz et al., 2021). However, another study suggested that nursing home residents may experience a small increased benefit when they are cared for by the same physicians and advanced practice clinicians in both the hospital and nursing home (White et al., 2020a).
The nursing home specialist model often involves a collaborative practice between physicians and APRNs. An AMDA ad hoc workgroup with representation from the Gerontological Advanced Practice Nurses Association provides an in-depth description of collaborative practice between a medical doctor and an APRN and outlines the core medical competencies, roles, and responsibilities of the APRN in long-term care (AMDA, 2011). In an older national survey, 63 percent of medical directors reported APRN involvement in care of nursing home residents—with two APRNs per responding facility, on average (Rosenfeld et al., 2004). These APRNs were
most frequently part of a physician group practice (60 percent) or part of an organization practice (38 percent). Only 19 percent of APRNs were employed directly by nursing homes (Rosenfeld et al., 2004). The proportion of nursing homes employing APRN and physician assistant providers increased from 20.4 percent in 2000 to 35.0 percent in 2010 (up from less than 10 percent in the early 1990s), although there was significant variability across states (Intrator et al., 2005, 2015).
Physician Assistants
Limited and dated evidence suggests that care provided by physician assistants can improve the quality of care for nursing home residents as well as provide cost savings (Ackermann and Kemle, 1998). Many studies of the nursing home workforce consider physician assistants and APRNs together and do not distinguish the specific impact of the physician assistant (Caprio, 2006; Gupta et al., 2014). A 2017 report suggested that physician assistants may represent an underused segment of the workforce available to support nursing home residents (Himmerick et al., 2017).
Advanced Practice Registered Nurses
The APRN role in providing care in nursing homes emerged in the early 1980s and grew in popularity after the 1986 IOM report Improving the Quality of Care in Nursing Homes (IOM, 1986). A 2008 review identified the roles APRNs were playing, including as primary-care (and acute-care) providers for both long-stay and post-acute residents; educators of residents, family, and staff; and consultants on improving system-wide and facility-wide care resident care issues (Bakerjian, 2008). Medical directors have previously reported high effectiveness of and high satisfaction with nurse practitioners (Rosenfeld et al., 2004). Family and resident satisfaction has been also associated positively with APRN-provided care in nursing homes (Bakerjian, 2008; Liu et al., 2011; Mileski et al., 2020), and APRNs are effective at building relationships with families and residents for more informed care decision making (Mileski et al., 2020).
Numerous reviews have identified key outcomes resulting from APRN-provided care in nursing homes, including improved management of chronic illnesses, improved functional and health status, improved quality of life, reduced or equivalent mortality and hospital admissions, improved self-care, reduced emergency department use and transfers, lower costs, increased time spent with residents, and increased resident, family, and staff satisfaction (Bakerjian, 2008; Christian and Baker, 2009; Donald et al., 2013; Liu et al., 2011; Mileski et al., 2020; Morilla-Herrera et al., 2016; Popejoy et al., 2017; Rantz et al., 2017; Xing et al., 2013).
Strategies to decrease hospitalizations have included APRN-led advanced care planning, medication reconciliation interventions, and employing APRNs full time at nursing homes (Mileski et al., 2020; Popejoy et al., 2017). However, one literature review identified the most frequently mentioned barrier for increasing the role of APRNs in nursing homes is their restricted scope of practice due to Medicare regulations and state regulatory constraints (Mileski et al., 2020). Nursing homes are unable to employ APRNs to bill Medicare for direct-care services (Popejoy et al., 2019; Rantz et al., 2017). In 2011, the IOM report The Future of Nursing recommended that the U.S. Congress “expand the Medicare program to include coverage of [APRN] services that are within the scope of practice under applicable state law, just as physician services are now covered” (IOM, 2011, p. 9). The report further recommended that the Medicare program be amended to authorize APRNs to perform assessments for admission to nursing homes.
A core component of the Missouri Quality Initiative demonstration project to reduce avoidable hospitalizations of nursing home residents is the use of APRNs working full time in a nursing home with an interdisciplinary team (Rantz et al., 2017, 2018a). The APRNs focus primarily on the geriatric clinical management of the residents and work with the staff to embed changes in their daily care delivery in areas such as hydration, fall prevention and management, and continence management. This model successfully reduced all-cause hospitalizations, avoidable hospitalizations, all-cause emergency department visits, avoidable emergency department visits, use of antipsychotic medications, and improved composite quality measure scores (Flesner et al., 2019; Rantz et al., 2018a,b; RTI International, 2017; Vogelsmeier et al., 2018, 2020). Additionally, significant cost savings were realized, including a reduction in total Medicare expenditures (Rantz et al., 2018b). (See Chapter 3 for more on the Missouri Quality Initiative.)
LICENSED NURSES
Two types of licensed nurses work in nursing homes: licensed practical/vocational nurses (LPNs/LVNs) and RNs. An LPN/LVN has completed training through a technical education program and then taken a national licensing examination. Each respective state board of nursing determines the LPN/LVN scope of practice, and in all cases, these nurses work under the supervision of an RN. Several types of education programs prepare an individual to take the national examination for licensure as an RN, including associate degree programs, hospital-based diploma programs, baccalaureate programs (bachelor of science in nursing), or post-baccalaureate programs (master of science in nursing).
Nursing homes and extended care settings in the United States employ 4.4 percent of the country’s RNs, compared with 27.5 percent of the country’s LPN/LVNs (down from 31.7 percent in 2017) (NCSBN, 2017; Smiley et al., 2021). On average, RNs make up 12 percent of the licensed nurses in nursing homes, whereas in hospitals the majority of, if not all, licensed nurses are RNs (Denny-Brown et al., 2020; Harris-Kojetin et al., 2019). While 64 percent of RNs in the United States have a bachelor’s or master’s degree in nursing (HRSA, 2019), the percentage of nurses with a bachelor’s degree or higher working in nursing homes is unknown. In 2020, RNs at the median earned $31.00 per hour while LPNs earned $23.64 per hour (HHCS, 2020).
Roles and Responsibilities
Traditionally, nursing homes have focused on the roles of licensed nurses in general (e.g., medication administration, treatments, carrying out physician orders) and have failed to differentiate the responsibilities of RNs and LPN/LVNs. Consequently, RNs and LPN/LVNs have been used interchangeably in nursing homes at the expense of the residents’ unmet professional nursing needs (Mueller et al., 2018), and LPN/LVNs often work outside their scope of practice (Corazzini et al., 2015; Mueller et al., 2012). For example, in a survey of LPN/LVNs in two states, LPN/LVNs were actively engaged in nursing assessments and developing and evaluating care plans; the unavailability of RNs was reported as the most common reason that LPN/LVNs found themselves engaged in activities that were outside their scope of practice (Mueller et al., 2012). Corazzini and colleagues (2013) examined how RNs and LPN/LVNs in nursing homes enacted core components of their scopes of practice (i.e., assessment, care planning, delegation and supervision). Three factors influenced the effectiveness of the collaboration between RNs and LPN/LVNs and their ability to function within their scopes of practice: (1) quality of connections, (2) degree of interchangeability between RNs and LPN/LVNs, and (3) staffing ratios.
RNs also fill other roles in nursing homes aside from direct clinical care. Federal regulations require that an RN conducts or coordinates required assessments using the Resident Assessment Instrument with the appropriate participation of other health professionals.7 Additional roles that RNs may have in nursing homes include quality improvement, infection prevention and control, staff development, management, and supervision. LPN/LVNs may fulfill those roles in some nursing homes.
___________________
7 CMS Requirements for Long-Term Care Facilities—Resident Assessment, 42 CFR § 483.20 (b)(1)(xviii), (g), and (h) (2016).
Education and Training
RNs are accountable for a wide range of resident care needs, including assessment, diagnosis, outcomes identification, planning, implementation, and evaluation (ANA, 2015). Furthermore, an RN is prepared to provide ongoing assessment of the residents’ clinical condition and to use critical thinking approaches to prevent or mitigate negative outcomes such as infections, exacerbation of chronic conditions, adverse medication events, pressure injuries, falls that can lead to hospitalizations, emergency admissions, and even death (Clarke and Donaldson, 2008; Horn et al., 2005; Mileski et al., 2020).
From 2007 to 2010, the Geriatric Nursing Education Consortium carried out a national effort to provide faculty in schools of nursing with “the necessary skills, knowledge, and competency to implement sustainable curricular innovations in care of older adults” (Gray-Miceli et al., 2014, p. 447). Faculty from over 400 baccalaureate nursing programs participated in this program and subsequently incorporated geriatric content into their curricula. However, no long-term data demonstrate whether geriatric nursing content and clinical experiences have been sustained in nursing curricula. Without faculty who have expertise in geriatric nursing, the focus on the nursing care of older adults is at high risk of being minimized in nursing curricula. The 2008 IOM report Retooling for an Aging America: Building the Health Care Workforce called for requiring health care workers to demonstrate competencies in basic geriatric care in order to receive and maintain their licenses and certifications and recommended that all health professional schools and health care training programs expand coursework and training in the treatment of older adults (IOM, 2008). The CMS Coronavirus Commission on Safety and Quality in Nursing Homes also called for training of RNs, LPNs, and CNAs in long-term care settings (MITRE, 2020).
The annual mean turnover rate of RNs in nursing homes is estimated at 140.7 percent, with the median rate being 102.9 percent (Gandhi et al., 2021). Recruiting and retaining RNs in nursing homes is challenging because nursing homes generally offer nurses lower wages than they would earn in other health care settings; the annual mean wage for RNs in nursing homes ($72,090) is approximately $10,000 (roughly 12 percent) less than RNs employed in acute-care hospitals ($81,680) and approximately $17,000 (nearly 20 percent) less than RNs employed in outpatient care settings ($89,300), for example (BLS, 2020c). Furthermore, the nursing home environment is often not conducive to supporting the professional practice and development of RNs. Supportive environments include the implementation of evidence-based practices; shared decision making regarding resident care, staffing, and work environment; involvement and leadership in quality improvement initiatives; and support for professional development
(Lyons et al., 2008; Rondeau and Wagar, 2006). Supportive work environments for RNs in nursing homes lead to better resident outcomes, lower nurse burnout, and higher nurse satisfaction (White et al., 2020b).
NURSE STAFFING, REGULATION, AND QUALITY OF CARE
Increasing RN staffing and overall nurse staffing has been a consistent recommendation for improving the quality of care in nursing homes (Harrington et al., 2016, 2020). While inadequate staffing is a widespread concern, it is also cited relatively infrequently by surveyors (CMA, 2014; Harrington et al., 2008, 2020). The following sections give an overview of the evidence base for the relationship between nurse staffing and the quality of care for nursing home residents, the regulations for nurse staffing levels, the success (or failure) of meeting these standards, and other challenges.
Quality of Care
Decades of evidence support the association between inadequate nurse staffing and poor quality of care in nursing homes, particularly in the case of RNs (Aiken, 1981; Eagle, 1968; Harrington et al., 2021; IOM, 1996; Spilsbury et al., 2011; Wells, 2004). Five systematic literature reviews conducted between 2006 and 2015 examined the relationship between nurse staffing and quality of care in nursing homes (Backhaus et al., 2014; Bostick et al., 2006; Castle, 2008; Dellefield et al., 2015; Spilsbury et al., 2011). Four of the reviews concluded that there were positive and significant relationships between nurse staffing and quality, while one review found the relationship to be inconsistent. The results were mixed in regard to the relationship between quality and LPN/LVN staffing or nursing assistant staffing. (See later in this chapter for more on CNAs.) The reviews consistently noted study limitations and called for better staffing data sources, longitudinal study designs, accounting for case mix, and strengthening ways to measure quality. For example, most studies relied on self-reported staffing data collected at the time of a nursing home’s state survey (Castle, 2008; Dellefield et al., 2015; Spilsbury et al., 2011).
Studies of nurse staffing typically examine nurse staffing levels as determined by the number of nursing hours per resident; a higher staffing level indicates that there are more nursing hours per resident day (discussed in the next section on regulations). Individual studies have demonstrated associations between higher nursing assistant staffing levels and fewer numbers of deficiencies found in inspections (Harrington, 2000; Hyer et al., 2011; Lerner, 2013) and between higher RN staffing levels and the number and severity of deficiencies (Lerner, 2013). Higher RN staffing levels have also been associated with lower rates of rehospitalizations, hospitalizations,
and emergency department use (Min and Hong, 2019; Spector et al., 2013; Yang et al., 2021a).
However, fully understanding the relationship between nurse staffing and quality of care requires more than an examination of the numbers of staff or hours per resident day. Rather, the connection between staffing and quality likely also depends on the skills of the staff, the complexity of resident care needs, and the organizational context of care delivery (e.g., allocation of work assignments, supervision, teamwork, use of care-related technologies, and physical layout of the nursing home) (Arling and Mueller, 2014; Arling et al., 2007). That is to say that some well-run facilities may be able to achieve high quality with fewer staff as compared to facilities in which care delivery is poorly organized.
Regulations for Nurse Staffing
In 2001, CMS conducted a large-scale study to identify appropriate nurse staffing ratios in nursing homes (Feuerberg, 2001; Harrington et al., 2020). The resulting report concluded that a “range of serious problems including malnutrition, dehydration, pressure sores, abuse and neglect . . . have pointed to nurse staffing as a potential root cause” (Feuerberg, 2001, p. 1). In addition to the numbers of staff in nursing homes being insufficient to meet the needs of residents, the CMS report identified several other staffing-related issues that contributed to poor quality in nursing homes, including high staff turnover and low retention, inadequate expenditures on nurse staffing, needs related to staff training/competencies, and ineffective or inadequate management and supervision (Feuerberg, 2001). The report also identified staffing thresholds below which residents were at risk for serious quality-of-care issues (Table 5-3).
Since 2016, CMS has required nursing homes to electronically submit direct-care staffing data on a daily basis through their Payroll-Based Journal (CMS, 2021b). However, the 2001 proposed CMS minimum staffing standards have not been addressed in any subsequent regulatory rules, so that
TABLE 5-3 Proposed Minimum Nurse Staffing Standards for U.S. Nursing Homes in 2001
| Short-stay | Long-stay | |
|---|---|---|
| RN Hours per Resident Day | .55 | .75 |
| LPN/LVN Hours per Resident Day | 1.15 | 1.3 |
| Nursing Assistant Hours per Resident Day | 2.4 | 2.8 |
| Total Nursing Hours per Resident Day | 4.1 | 4.1 |
SOURCE: Feuerberg, 2001.
there is no minimum federal standard for RN hours per resident day and great variation in state standards (Harrington et al., 2016). Instead, current regulations include a vague nurse staffing requirement that nursing homes must provide “sufficient nursing staff to attain or maintain the highest practicable . . . well-being of each resident.”8 (See later in this chapter for more on CNA staffing levels.) In the second quarter of 2021, the average number of staff hours per resident day was 0.66 for RNs (excluding administrative RNs and directors of nursing), 0.82 for LPNs (excluding administrative LPNs), 2.04 for CNAs, and 3.75 for total nursing hours—well below the recommended thresholds for most nursing home residents (LTCCC, 2022).
The 1996 IOM report Nursing Staff in Hospitals and Nursing Homes further recommended a requirement for 24-hour RN coverage in nursing homes by the year 2000 (IOM, 1996). The recommendation was endorsed by a subsequent IOM study in 2001, and then recommended again in the 2004 IOM report Keeping Patients Safe (IOM, 2001b, 2004). Yet today the requirement is a 24-hour daily presence of licensed nurse coverage (i.e., RN or LPN/LVN) with an RN fulfilling at least 8 of those hours.9 The CMS Coronavirus Commission on Safety and Quality in Nursing Homes noted the importance of 24-hour daily presence of RNs for nursing homes with positive COVID-19 cases (MITRE, 2020). The Build Back Better Act, introduced in 2021, called for 24-hour daily presence of RNs in all nursing homes and for the U.S. Department of Health and Human Services to study what minimum nursing staff requirements would best help meet resident needs.10
An analysis of 2019 data by the U.S. Government Accountability Office (GAO) found that while virtually all nursing homes met the federal requirement of the 8-hour presence of an RN, only about one-quarter of nursing homes met the proposed staffing minimums for RN and total nurse staffing (see Table 5-3) (GAO, 2021). The GAO recommended that CMS should report on nursing homes’ minimum staffing standards below which residents are at increased risk of quality problems (such as those proposed in 2001) on Care Compare.
States may also have specific nurse staffing standards for nursing homes (Harrington, 2010). For example, in June 2021, New York State passed a law requiring minimum clinical staffing levels in nursing homes (Brown, 2021). These standards include 3.5 hours per day of clinical staffing, of which at least 2.2 hours are provided by a CNA or nurse aide and at least 1.1 hours are provided by a licensed nurse. States that regulate the level of nursing home staff have higher levels of nurse staffing (Mueller et al., 2006;
___________________
8 CMS Requirements for Long-Term Care Facilities—Nursing Services, 42 CFR § 483.35 (2016).
9 Ibid.
10 Build Back Better Act, HR 5376, 117th Cong., 1st sess., Congressional Record 167, no. 200, daily ed. (November 17, 2021).
Paek et al., 2016), with one study finding that nursing homes that meet their state’s nurse staffing standards had fewer total deficiencies and fewer quality-of-care deficiencies than nursing homes that did not meet the staffing standards (Kim et al., 2009). However, in 2021, the Consumer Voice noted that “twenty years after the CMS study found that at least 4.1 [hours per resident day] of direct care nursing staff time are needed just to prevent poor outcomes, state staffing requirements, with a few exceptions, are nowhere near that recommended level” (Consumer Voice, 2021, p. 8). For family member perspectives on staffing standards and understaffing, see Box 5-2.
Additionally, staffing level patterns show a drop in nurse staffing (i.e., RNs, LPN/LVNs, and nurse aides) during the weekends (GAO, 2021; Harrington et al., 2020). The GAO found that RN staffing hours decrease by around 40 percent on the weekends (see Figure 5-2) (GAO, 2021). GAO noted that this was an important detail for the informed decision making of consumers and recommended that CMS report weekend RN and total nursing staffing levels on Care Compare. Data collected by CMS are helpful to the state survey process. For example, CMS shares weekend staffing data with state survey agencies so that they may target weekend inspections to nursing homes that report lower weekend staffing levels (OIG, 2021). The Office of the Inspector General recommended that CMS report more types of staffing data to state survey agencies, such as nursing homes with frequent reports of lower staffing levels (including specific dates) and nursing homes at risk of having insufficient staffing (OIG, 2021).
Current staffing requirements are not adjusted by resident case mix (CMS, 2016, 2019b). A large proportion of nursing homes have staffing levels below CMS’s case-mix adjusted expected staffing levels (GAO, 2021; Geng et al., 2019). For RNs, including both the directors of nursing and RNs with administrative responsibilities, 91 percent of the facilities met the expected level less than 60 percent of the time (Geng et al., 2019). An Office of the Inspector General (OIG) report also noted that by not taking resident
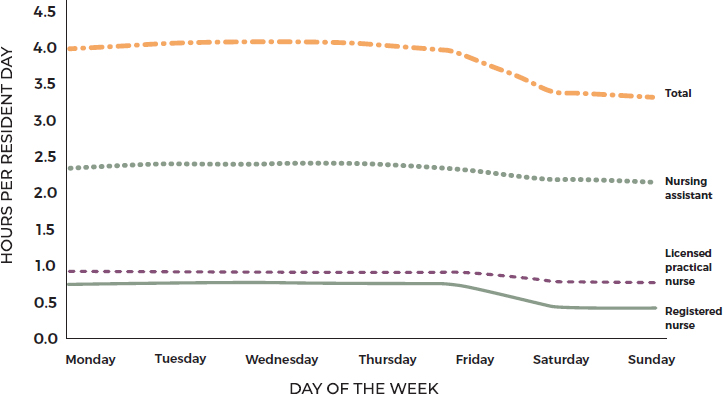
SOURCE: GAO, 2021.
acuity into account, CMS’s assessments of nursing homes with the lowest weekend staffing levels likely miss up to one-quarter of facilities that have a greater level of staffing need (OIG, 2021). For family member perspectives on staffing standards and resident acuity, see Box 5-3.
Meeting specific minimum staffing standards while also moving toward smaller, more home-like models of care may add challenges to achieving these standards. However, innovative approaches to meeting these standards will ensure that all nursing homes have the necessary expertise to achieve high-quality care.
INFECTION PREVENTION AND CONTROL LEADERSHIP
In 2016, CMS issued a final rule revising the requirements that nursing homes (and other long-term care facilities) must meet to participate in Medicare and Medicaid programs. (See Chapter 8 for more on quality assurance.) As part of the rule, nursing homes were required to designate at least one part-time or full-time staff member as the infection prevention and control specialist (also known as an infection preventionist). The role of the
infection prevention and control specialist includes assessing, implementing, and managing the facility’s infection prevention and control plan and participating in the facility’s quality assessment and assurance committees. The final rule suggested that an RN would assume the role of the infection prevention and control specialist in most facilities and that the individual would need to spend around 15 percent of his or her time on this role.11 The CMS Coronavirus Commission on Safety and Quality in Nursing Homes noted the position of infection prevention and control specialist is “traditionally assigned to a supervisor, nursing manager, or provider as an added (rather than a core) responsibility” (MITRE, 2020, p. 41). However, the commission noted that “there are no national standards for training and licensure requirements of infection preventionists that nursing homes are mandated to employ” and subsequently recommended higher qualifications and training (MITRE, 2020, p. 48).
A 2015 survey by the Association for Professionals in Infection Control and Epidemiology found that only 15 percent of infection prevention and control specialists in non–acute care settings (including nursing homes) were certified in infection control (Pogorzelska-Maziarz and Kalp, 2017). Before the 2016 rule, staffing levels for infection prevention and control specialists in nursing homes varied widely across nursing homes (Stone et al., 2020). Between 2014 and 2018, staffing levels were higher in large for-profit nursing homes than in large nonprofit nursing homes (Stone et al., 2020). Furthermore, studies have found a lack of training among the personnel responsible for infection prevention and control in nursing homes (Stone et al., 2018; Trautner et al., 2017). CDC TRAIN offers the Nursing Home Infection Preventionist Training Course; the course is free, qualifies for various continuing education credits, and covers a variety of topics such as infection surveillance, hand hygiene, injection safety, water and linen management, antibiotic stewardship, and preventing respiratory infections (CDC TRAIN, 2021).
The 2020 CMS Coronavirus Commission on Safety and Quality in Nursing Homes noted that the current regulations on infection prevention and control specialists in nursing homes yielded an “insufficient response to the demands” of the [COVID-19] pandemic (MITRE, 2020, p. 41). The commission made several recommendations related to the role of the infection preventionist, including
- Employ infection preventionists with educator capabilities and document their training of the nursing homes staff;
- Assess infection prevention and control competency among all nursing home staff;
___________________
11 CMS Requirements for Long-Term Care Facilities—Infection Control, 42 CFR § 483.80 (2016).
- Establish a full-time-equivalent-to-bed ratio for an infection preventionist educator for every nursing home (with consideration for health professional shortage areas); and
- Develop and provide a training curriculum and certification for infection preventionists in nursing homes.
See later in this chapter for more on infection prevention and control during the COVID-19 pandemic, particularly the role of strike teams.
PSYCHOSOCIAL AND SPIRITUAL CARE PROVIDERS
A variety of workers are engaged in the psychosocial care of nursing home residents. These include social workers, chaplains, and staff involved with activities, art, and wellness. (See Chapter 4 for more on psychosocial care needs.)
Social Workers
Social workers’ roles in nursing homes support person-centered care and include identifying and assessing residents’ psychosocial needs; working as part of the interdisciplinary care team; communicating and assisting residents and their families with care needs (e.g., behavioral health and psychosocial care) (see Chapter 4); eliciting and honoring resident care preferences; advocating for at-risk populations (e.g., residents belonging to racial and ethnic minorities, LGBTQ+ residents); and providing transitional care, counseling, and conflict management to residents, families, and staff (Bern-Klug and Kramer, 2013; Kusmaul et al., 2017; Miller et al., 2021; NASW, 2003, 2016). In addition, social services directors are often involved in discharge planning, transitions of care, psychosocial care planning, and interactions with family members (Bern-Klug et al., 2021a). Box 5-4 outlines the major tasks involved in providing medically related social services.
Qualifications
Professionally trained social workers with a bachelor’s degree in social work (B.S.W.) or master’s degree in social work (M.S.W.) hold a professional degree that includes training to develop clinical, organizational, and community engagement skills. Social work programs provide competency-based education to practitioners who agree to abide by a standard code of ethics and conduct, complete fieldwork, and demonstrate professional behavior and skills (CSWE, 2015). The Council on Social Work Education (CSWE)12 accredits baccalaureate-level (generalist social work practice)
___________________
12 For more information, see www.cswe.org (accessed November 3, 2021).
and master’s level (specialty practice) social work programs. CSWE defines social work competence as the ability to integrate and apply social work knowledge and values to provide professional services promoting human and community well-being (CSWE, 2015, 2021). Students who graduate from a CSWE-accredited social work program demonstrated competence, both in the classroom and through fieldwork, served under the supervision of a professional social worker (Bern-Klug et al., 2016).
Regulatory Requirements
Currently, federal regulations13 require nursing homes with 120 or more beds to hire a qualified social worker on a full-time basis, although this “qualified social worker” need not have a social work degree (Bern-Klug et al., 2021a). Specifically, the “qualified social worker” is defined as an individual with a minimum of a B.S.W. or a bachelor’s degree in a human services field including, but not limited to, sociology, gerontology, special education, rehabilitation counseling, or psychology and who has 1 year of
___________________
13 CMS Requirements for Long-Term Care Facilities—Administration, 42 CFR § 483.70 (2016).
supervised social work experience in a health care setting working directly with individuals.14 Because this requirement applies only to nursing homes with 120 or more beds, some two-thirds of nursing homes do not have to employ a social services staff member (Bern-Klug et al., 2021b). Social work is the only profession affected by the “120-bed rule” (Bern-Klug et al., 2018). However, Roberts and Bowblis (2017) concluded that the 120-bed rule “does not account for the level of psychosocial need among residents in smaller nursing homes, nor does it consider the caseload of practitioners.”
Many individual states have their own regulations regarding social work services in nursing homes, and while most do not require nursing homes with 120 or fewer beds to employ social workers, Connecticut, Maine, and Oklahoma do require that nursing home residents have access to social work services regardless of the size of the nursing home. However, 10 states do not require a “qualified social worker” to have either a social work license or a social work degree, though some require either completing a state-approved course or having some direct supervision and minimum years of experience (Bern-Klug, 2008; Bern-Klug et al., 2018).
Both state and federal guidelines provide unrealistic recommendations for social service staffing patterns. In a recent study of social service directors, 66 percent of social service directors stated that one full-time social service staff member could handle 60 residents at most, with 75 percent of social service directors recommending fewer than 30 short-term (skilled/rehab/post/sub-acute care) nursing home residents per full-time social worker (Bern-Klug et al., 2021b). One older study found that social workers serving older adults face challenges including lower pay and higher caseloads (especially in nursing facilities), which affect job satisfaction (Whitaker et al., 2006).
In 2003, the NASW developed a consensus statement for professional standards for social workers in long-term care settings. It stated:
A social worker has, at a minimum, a bachelor’s degree from an accredited school or program of social work; has 2 years of postgraduate experience in long-term care or related programs; and meets equivalent state requirements for social work practice, or, in jurisdictions not having such legal regulation, holds certification or credentialing from the National Association of Social Workers. In no instance shall a social worker have less than a baccalaureate from an accredited school or program of social work. (NASW, 2003, p. 7)
Regulatory requirements are inadequate to address the complexities of psychosocial and behavioral health care with qualified staffing, and there is a long history of advocacy for increased standards in this area
___________________
14 CMS Conditions of Participation Organization Environment—Personnel Qualifications, 42 CFR § 418.114 (2016).
(Li, 2010; Orth et al., 2019; Streim et al., 2002). Two recent developments are contributing to this push. First, CMS’s adoption of the Minimum Data Set 3.0 as the updated resident assessment instrument places more emphasis on resident-centered care, quality of life, and enhanced psychosocial and behavioral health care. In addition, in response to the industry’s move to encourage resident and family participation in care choices and the movement toward more holistic care, recommendations emerged to increase the presence of bachelor’s and master’s prepared social workers and to increase the training of all staff on behavioral health and quality-of-life issues (Simons et al., 2012).
During the required comment period prior to the updating of CMS’s 2016 rule for nursing home requirements, members of the National Nursing Home Social Work Network recommended that nursing home facilities hire graduates of accredited social work programs to fulfill the social work role in nursing homes (Bern-Klug et al., 2016). These same organizations asked that all nursing homes, regardless of size, employ a full-time social worker. In spite of these recommendations, the final rule did not require social workers as core members of the team developing a resident’s comprehensive care plan. Furthermore, the rule added an undergraduate degree in gerontology as an acceptable degree for a “qualified social worker.” The reduction in standards for qualified social workers in nursing homes occurred at the same time that these updated regulations increased requirements for psychosocial care, person-centered care, and behavioral health care (CMS, 2016).
Evidence of Social Work Contributions to Nursing Home Care
Social workers’ contributions to resident care often involve tasks that are complex and clinically challenging. The results of a national survey of social service directors indicated strong involvement in care transitions, with more than 55 percent of the respondents reporting that they spent over 50 percent of their time with short-term residents (Galambos et al., 2021). Almost 62 percent of social service directors and their staff were consistently involved in disaster planning and response activities at the nursing home facility (Kusmaul et al., 2021). Studies also point to the positive outcomes that social workers achieve in complex care situations (Sussman and Dupuis, 2014). Research has shown, for example, that social service staff with higher qualifications are integral to improving behavioral symptoms and reducing antipsychotic medications (Roberts et al., 2020), that social workers routinely intervene in resident-to-resident aggression (Bonifas, 2015), and that social workers increase advance directive completion, contributing to a reduction in potentially avoidable hospitalizations (Galambos et al., 2021).
A systematic review that examined the impact of social work interventions in aging and quality of life found that 71 percent of the studies reported significant quality-of-life outcomes, and 15 of these studies documented cost savings achieved through social work interventions, with these cost outcomes achieved through care coordination, palliative care, and end-of-life care (Rizzo and Rowe, 2016). Furthermore, a study on social integration and mental and functional health outcomes for nursing home residents found that nursing homes with degreed social workers have the capacity to provide better psychosocial care (Leedahl et al., 2015).
Given the evidence of social workers’ contributions to nursing home care, inclusion of social workers on interdisciplinary care teams can help ensure resident care preferences are met. See later in this chapter for more on the role of social workers during the COVID-19 pandemic.
Chaplains
As Chapter 4 discusses, attending to the spiritual needs of nursing home residents is a critical part of their quality of life and well-being (Gilbert et al., 2021; Koenig, 2012; Morley and Sanford, 2014). Chaplains provide residents, their families, and even staff with spiritual support. In addition, they provide human connection for residents, listening to their stories; leading prayers, religious services and rituals, and group meetings; supporting family and friends; and providing grief and bereavement support (Seidman, 2021). Their role is especially critical in the area of palliative care. Unfortunately, nursing homes employ too few chaplains to meet the needs of seriously ill patients, and those chaplains that are available have limited time to support staff (Ferrell et al., 2020). One analysis found that most post-acute and long-term care facilities do not have a budget for a chaplain or a full-time spiritual counselor and instead designate an already overworked social worker to get additional education or find a volunteer chaplain (McKnight, 2016). The COVID-19 pandemic has shed light on the urgent need to include chaplains in care teams and for chaplains to provide consistent spiritual care services (Ferrell et al., 2020).
Activities Staff
As noted in Chapter 4, wellness activities, physical activities, and art activities are vital for health, functional mobility, and the performance of everyday activities. Federal regulations require facilities to provide an ongoing activities program that is “designed to meet the interests of and support the physical, mental, and psychosocial well-being of each resident, encouraging both independence and interaction in the community.” They also require that the program be directed by a qualified professional who
is either “a qualified therapeutic recreation specialist or an activities professional,” meaning they are licensed or registered by the state, are a qualified occupational therapist or assistant, and have completed a training course by the state.15 However, data on whether nursing homes are complying with this regulation are scarce.
OTHER CLINICAL STAFF
In addition to the professionals discussed above, a variety of other health care practitioners, specialists, and staff also help support residents in nursing homes. However, evidence on these individuals specifically in nursing homes is extremely limited.
Dental Health Care Workforce
As Chapter 4 describes, “oral disease impacts physical, psychological, and social well-being through pain, diminished function, and reduced quality of life” (Dunbar, 2019; Sifuentes and Lapane, 2020). However, most nursing homes do not contract with dentists or dental hygienists, so residents tend to only receive emergency and acute care rather than routine and preventative dental care (Dunbar, 2019; Maramaldi et al., 2018). Assistance with daily oral health care for nursing home residents is typically the responsibility of the CNAs (Dunbar, 2019; Sifuentes and Lapane, 2020), who not only lack the training to provide such care, but typically face significant competing demands for their time. Other challenges include staff perceptions that oral health care is not a priority, staff hesitancy or unwillingness to perform the tasks, and residents’ resistance to staff assistance (Patterson Norrie et al., 2019; Porter et al., 2015). In addition, the dental health care workforce is often not well prepared to address the specific oral health needs of older adults. Surveys of dental students indicate that many find the geriatric dentistry training curriculum to be inadequate, and geriatric dentistry is not among the 12 specialty areas recognized by the American Dental Association (ADA, 2021).16
___________________
15 CMS Requirements for Long-Term Care Facilities—Quality of Life, 42 CFR § 483.24 (2016).
16 For a full list of the specialty areas, see https://www.ada.org/en/ncrdscb/dental-specialties/specialty-definitions (accessed November 3, 2021).
Moreover, a 2011 IOM study, Improving Access to Oral Health Care for Vulnerable and Underserved Populations, found that the American Board of General Dentistry did not explicitly require questions on geriatric dental care for board certification and that of the more than 500 residencies recognized by the American Dental Education Association, none were specifically devoted to the care of elderly patients (IOM, 2011).
Pharmacists
Nursing home residents tend to require a large number of prescriptions to help manage their health. The use of a large number of medications by a single person, including potentially inappropriate medications or duplication, is a significant concern among nursing home residents, as it can lead to adverse drug events, disability, hospitalization, and death (Hoel et al., 2021; Lee et al., 2019). Federal regulations require a nursing home contract with a consultant pharmacist to review each resident’s drug regimen monthly and to report irregularities, which the attending physician must review and respond to in the medical record.17 Problems identified by consultant pharmacists typically include missing information, an unnecessary drug, and excessive duration or dose of a drug (Lapane and Hughes, 2006). Concerns have been raised that consultant pharmacists may have conflicts of interest when their services are provided by the dispensing pharmacy of the nursing home (Barlas, 2012; Sullivan, 2018). In fact, two large nursing home pharmacies agreed to pay settlements in response to claims of kickbacks under whistleblower provisions of the False Claims Act (DOJ, 2015; McCrystal et al., 2010). These claims included that a dispensing pharmacy provided the services of consultant pharmacists at a reduced rate in order to secure pharmacy contracts, and that a dispensing pharmacy accepted incentives from a drug company in exchange for the consultant pharmacist recommending that physicians prescribe specific drugs.
Recently, the role of pharmacists has evolved from being product centered to being more person centered, with a greater emphasis on their role in ensuring quality care (Lee et al., 2019). A systematic review by Lee and colleagues (2019) found that the presence of pharmacy services in a nursing home led to an improvement in the quality of prescribing, positive trends in de-prescribing and reducing the number of medications used per resident, an improvement of nursing home staff knowledge on medication use, and a reduction in the number of resident falls. However, the study found more mixed results in terms of mortality, hospitalization, and resident admission rates. The role of consultant pharmacists in antibiotic stewardship programs has also been considered to help improve overall antibiotic use (Ashraf and Bergman, 2021).
Registered Clinical Dieticians and Feeding Assistants
Registered clinical dietitians assess, evaluate, and recommend appropriate nutrition interventions based on residents’ preferences and their health status (e.g., malnutrition, diabetes, obesity), but not all residents have access to a registered clinical dietician (Dorner and Friedrich, 2018). Federal regulation only mandates that CMS-certified facilities must have a
___________________
17 CMS Requirements for Long-Term Care Facilities—Pharmacy Services, 42 CFR § 483.45 (2022).
“qualified dietitian or other clinically qualified nutrition professional either full-time, part-time, or on a consultant basis.”18 Despite the regulations, nursing home staff may not have the resources to fully address the nutritional needs of residents (Simmons and Schnelle, 2004, 2006; Simmons et al., 2008). For example, there may be too few CNAs to assist with feeding, especially in the evenings, and too few RNs and dietitians to oversee the dining experience in nursing homes (IOM, 2000). To fill the gap in nutrition and feeding assistance, some nursing facilities employ or contract with a registered dietitian nutritionist or nutrition and dietetics technicians (Dorner and Friedrich, 2018), but it is often not enough.
In 2003, CMS allowed nursing homes to use paid feeding assistants “to provide more residents with help in eating and drinking and reduce the incidence of unplanned weight loss and dehydration” (CMS, 2007, p. 1). Paid feeding assistants are required to complete an approved state-based training program (with a minimum of 8 hours of training) and must be supervised by RNs or LPNs. Furthermore, the paid feeding assistant may only help residents who do not have complicated feeding problems (e.g., difficulty swallowing, tube feedings). Current nursing home staff may be used as paid feeding assistants as long as they have completed the required training. A small evaluation of paid feeding assistants found the quality of their care to be comparable to CNAs (Simmons et al., 2007).
The 2000 IOM report The Role of Nutrition in Maintaining Health in the Nation’s Elderly recommended that “licensing agencies need to develop more effective oversight with respect to feeding, supervision of staff, and other nutrition-related issues” (IOM, 2000, p. 235).
Therapists
A variety of types of therapists, assistants, and aides are among the extended nursing home workforce. Nursing homes are required to provide or consult for specialized rehabilitative services for a mental disorder and intellectual disability (e.g., physical therapy, speech–language pathology, occupational therapy, respiratory therapy) for nursing home residents as required by their care plans.19
Occupational Therapists and Assistants
In nursing homes, occupational therapists “address training in self-care skills; training in the use of adaptive equipment, compensatory techniques,
___________________
18 CMS Requirements for Long-Term Care Facilities—Food and Nutrition Services, 42 CFR § 483.60 (2016).
19 CMS Requirements for Long-Term Care Facilities—Specialized Rehabilitative Services, 42 CFR § 483.65 (2016).
and environmental modifications; and behavioral and mental health issues” (AOTA, 2015). Occupational therapists help residents increase physical activity, engage in self-care, reduce pain, and maintain independence (Livingstone et al., 2019, 2021). Studies have found a positive relationship between occupational therapy staffing levels and the quality of life and care for nursing home residents (Jette et al., 2005; Livingstone et al., 2019). As outlined in Chapter 4, occupational therapists can also help reduce length of stay by helping residents make the gains in function needed to be able to be discharged from the nursing home (Yurkofsky and Ouslander, 2021). However, when Medicare significantly altered the way nursing homes are paid through its patient-driven payment model (PDPM), staffing levels fell by almost 6 percent for occupational therapists and by about 10 percent for occupational therapist assistants. These cuts were also almost entirely among contracted staff (McGarry et al., 2021a).
Physical Therapists, Assistants, and Aides
Physical therapy providers in nursing homes work with residents to “reduce impairment, rehabilitate from an injury or illness, improve functioning and cognition, and prevent adverse effects or onset of disease” (Livingstone et al., 2021). This includes strength and endurance training, balance improvement exercises, and mobility training. Therapists and assistants tend to work together, rather than using assistants as an alternative to therapists. As was the case with occupational therapists, the 2019 introduction of Medicare’s PDPM resulted in a reduction of physical therapy staff. Specifically, staffing levels in nursing homes fell by about 6 percent for physical therapists and 10 percent for physical therapy assistants (McGarry et al., 2021a). Contract staffing again accounted for most of the decrease in staffing levels (McGarry et al., 2021a). One analysis suggested that some facilities may start using assistants and aides as lower-cost substitutes for therapists (Livingstone et al., 2021). A 2021 report by the OIG stated that “CMS does not audit the physical-therapist staffing information reported by nursing homes and included on Care Compare. Because CMS does not use any accuracy checks on these data, we cannot determine whether the data reported on Care Compare are accurate” (OIG, 2021, p. 15).
Respiratory Therapists
Respiratory therapists work with residents who are suffering from breathing issues resulting from illnesses such as chronic obstructive pulmonary disease, asthma, surgery, or injury or who are recovering from an illness. The full array of respiratory therapy services can include oxygen therapy, inhalation medication management, pulmonary rehabilitation, and ventilator
management (AARC, 2016). Respiratory therapists are educated and trained in all aspects of pulmonary medicine and can help residents manage all respiratory diseases and conditions. Under current regulations, respiratory therapy is considered a nontherapy ancillary service (AARC, 2017).
Speech–Language Pathologists and Speech Therapists
Speech–language pathologists help evaluate and treat a range of conditions that lead to communication, cognition, memory, problem-solving, language expression, or swallowing disorders in long-term care residents (Casper, 2013). Approximately 5 percent of all speech–language pathologists work in nursing and residential care facilities (BLS, 2021a). Among speech–language pathologists working in nursing homes, 83.4 percent are employed full time, and 82.8 percent are paid on an hourly basis; 61.7 percent work for one employer, 24.7 percent work for two employers, and 9.4 percent work for three or more employers (ASHA, 2021). More than one in five nursing homes have funded, unfilled positions (ASHA, 2021).
DIRECT-CARE WORKERS
Direct-care workers—nursing assistants (also called nurse aides), personal care aides, and home health aides—provide the majority of hands-on care to residents in nursing homes (Campbell et al., 2021). Direct-care workers provide care that includes everyday tasks such as assistance with eating, bathing, toileting, and dressing, as well as more advanced tasks such as infection control and taking care of cognitively impaired residents (BLS, 2021b; McMullen et al., 2015; PHI, 2021). Taken together, these tasks are critical to maintaining the function, well-being, and quality of life of the resident. CNAs—nursing assistants who have met specific federal and state educational and training requirements—make up the largest proportion of direct-care workers in nursing homes.
Demographics
More than 527,000 nursing assistants were employed or contracted by nursing homes across the United States in 2020 (12 percent of the total direct-care workforce) (BLS, 2021c). Among these workers, the median age was 38, and 91 percent were women; 58 percent were people of color (38 percent Black/African American, 13 percent Hispanic/Latino, 5 percent Asian or Pacific Islanders, 2 percent other), and 21 percent were born outside of the United States (PHI, 2021). More than 90 percent had completed at least high school, and 13 percent had an associate’s degree or higher (PHI, 2021).
As the demand for direct-care workers increases, nursing homes in the United States will need to fill approximately 561,800 nursing assistant jobs between 2019 and 2029 (Campbell et al., 2021; PHI, 2021). This effort will not come without challenges which have plagued the ability for nursing homes to recruit and retain an adequate supply of direct-care workers for decades, however. Many of these challenges are rooted in structural and systemic factors that play out in the form of low wages, minimal training requirements, and a lack of respect and recognition, which, to a significant degree, represent the legacy of long-standing institutional racism, sexism, and ageism (Drake, 2020; Ryosho, 2011; Sloane et al., 2021; Squillace et al., 2009; Travers et al., 2020; Truitt and Snyder, 2020). Because of the crucial role of this position in nursing homes, significantly improving the quality of care requires investment in quality jobs for direct-care workers.
Immigrant workers, both documented and undocumented, fill critical gaps in the direct-care workforce, especially in nursing homes that serve a high share of Black and Latinx residents (Lee et al., 2020; Zallman et al., 2019). As such, this group may be a primary target for recruitment efforts. However, when entering the workforce, immigrant workers face additional barriers, such as barriers in language, health literacy, and uninsured rates, compared with native-born individuals (Campbell, 2018; Lee et al., 2020). One strategy to support immigrant workers and attract them to direct-care worker positions includes a pathway to citizenship (Katz, 2019; White House, 2021).
Wages
The mean hourly wage in 2020 for nursing assistants in nursing homes was $15.41, and the mean annual wage was $32,050 (BLS, 2021c). The bottom quartile of nursing assistants earn less than $26,650 annually, and the bottom 10 percent earn less than $22,750 (BLS, 2021c). The level of pay for direct-care workers in nursing homes has drawn stark attention to comparable wages for other types of work that might be considered more desirable. For example, while nursing assistants provide increasingly complex care and face persistent challenges with inadequate training and risk of on-the-job injury, they may earn little more than cashiers ($25,020 per year), food service workers ($24,130 per year), or retail sales workers ($27,320 per year) (BLS, 2021d,e,f). A 2021 story found that many nursing home workers were leaving for jobs at Amazon:
The average starting pay for an entry-level position at Amazon warehouses and cargo hubs is more than $18 an hour, with the possibility of as much as $22.50 an hour and a $3,000 signing bonus, depending on location and shift. Full-time jobs with the company come with health benefits, 401(k)s and parental leave (Varney, 2021).
Direct-care workers often have to work multiple jobs, forgo important necessities such as health insurance and retirement benefits because of an inability to afford premiums, and live in congregate housing (Morris, 2009). Because of their low wages, 34 percent of direct-care workers require some form of public assistance, and many live in poverty; direct-care workers who are also women of color are more likely than White women and men to require public assistance, live in poverty, or live in low-income households (PHI, 2019, 2021). This could in part be a result of the fact that Black female direct-care workers make 20 cents per hour less than White female direct-care workers and 70 cents per hour less than White male direct-care workers (Scales et al., 2020). For family member perspectives on the compensation of nursing home workers, particularly CNAs, see Box 5-5.
Education and Training
CNAs are required20 to have a minimum of 75 hours of training plus at least 12 hours of continuing education annually, including 16 hours of “supervised practical training,” that covers basic nursing services, personal care services, basic restorative services, mental health and social services, care of cognitively impaired residents, residents’ rights, and other topics (Hernández-Medina et al., 2006). The minimum number of hours and topics covered by CNA trainings have been a cause for concern as these requirements have not changed since the passing of the Nursing Home Reform Act, part of the Omnibus Budget Reconciliation Act of 1987. Given the marked increase in nursing home resident acuity, complexity, and care needs, current requirements are inadequate (Hernández-Medina et al., 2006). For example, one small study found that CNAs in nursing homes had inadequate knowledge related to aging, cognition, and mental health (Kusmaul, 2016). Some states and facilities have implemented more robust training efforts, with many states requiring additional hours and topics of training beyond federal minimum requirements. CNAs themselves have expressed interest in including education on dementia and infection control (Lerner et al., 2010).
Additional training of CNAs has been associated with improved nursing home quality indicators (Hernández-Medina et al., 2006; PHI, 2011; Trinkoff et al., 2013; Zheng and Temkin-Greener, 2010). As a result, various bodies have suggested that the number of required hours for training be increased to between 100 and 120 hours, with 50 to 60 of those hours going toward clinical training (Hernández-Medina et al., 2006). Specifically, the 2008 IOM report Retooling for an Aging America recommended that “Federal requirements for the minimum training of [CNAs] and home health aides should be raised to at least 120 hours and should include demonstration of competence in the care of older adults as a criterion for certification” (IOM, 2008, p. 218). While many states have increased their requirements since 2007, only the District of Columbia and 13 states (up from 12 states in 2007) require at least 120 hours (IOM, 2008; PHI, 2020).
CNAs reporting high-quality training are more likely to work in states requiring additional initial training hours and were more satisfied with their jobs than those with low-quality training (Han et al., 2014). Training that focused specifically on work-life skills, such as problem solving, task organization, and working with others, helped to increase satisfaction (Han et al., 2014). Additionally, the implementation of orientation programs for newly hired staff in all states and facilities is needed (IOM, 2004).
___________________
20 CMS Requirements for Long-Term Care Facilities—Requirements for Approval of a Nurse Aide Training and Competency Evaluation Program, 42 CFR § 483.152 (2016).
Because the care needs of the resident are complex, dynamic, and growing, CNAs need ongoing professional development to adapt to the changing needs of the resident population. The current federal requirement for professional development is that CNAs must receive 12 hours of in-service or continuing education each year.21 The inclusion of topics such as infection control, care of the cognitively impaired, behavioral health, resident rights, skin care, communication techniques, safety and disaster training, and resident confidentiality may help ensure the competency of CNAs in carrying out their responsibilities. The National Institute of CNA Excellence, a project seeking to recruit and train CNAs, is expected to launch in 2022 (NICE, 2021). Created by the National Association of Health Care Assistants, the project provides virtual training that goes beyond traditional training in clinical skills to include topics like team building, leadership skills, conflict resolution, resident advocacy, and communication. The project further plans to support the CNA candidate through certification and job placement. For family member perspectives on the training of nursing home staff, particularly CNAs, see Box 5-6.
___________________
21 CMS Requirements for Long-Term Care Facilities—Training Requirements, 42 CFR § 483.95(g) (2016).
Job Requirements and Characteristics
Unlike licensed personnel such as RNs, direct-care workers do not have an official scope of practice. Instead, nine authorized duties are listed by the Code of Federal Regulations to be allowable by each state: (1) personal care, (2) safety/emergency procedures, (3) basic nursing, (4) infection control, (5) communication and interpersonal activities, (6) care of cognitively impaired residents, (7) basic restorative care, (8) mental health and social service activities, and (9) residents’ rights (McMullen et al., 2015). While these are duties that direct-care workers are authorized to perform, depending on the state, they may or may not be tasked to do so. Moreover, there are a number of additional duties that direct-care workers have been permitted to carry out, such as medication management, wound care, catheter care tasks, and the management of medical information, because they benefit residents and alleviate pressure from other members of the workforce (McMullen et al., 2015).
Medication aides are most often CNAs who have received training to administer medications in some capacity based on the regulations provided by the state. There are variations in the requirements of the medication aides related to supervision, hours of training, continuing education, and length of time working as a CNA and in the facility. For example, in Iowa, medication aides can only administer medications under the supervision of an RN (ANA Enterprise, 2015). As of March 2020, certified medication technicians (as defined in the 2020–2021 Nursing Home Salary and Benefits Report by the Hospital and Healthcare Compensation Service and the American Health Care Association) had a median hourly wage of $15.66 in nursing homes (HHCS, 2020).
Staffing Levels
As noted earlier in this chapter, a 2001 study by CMS proposed that minimum staffing standards for nursing assistants (thresholds below which residents were at risk for serious quality-of-care issues) should be 2.4 hours per resident day for short-stay residents and 2.8 hours per resident day for long-stay residents (Feuerberg, 2001). However, these levels are rarely achieved in all nursing homes. Furthermore, these minimum staffing standards may not reflect the acuity of the residents’ needs, and lead to excessive workloads or the inability of CNAs to provide high-quality care. For example, one simulation estimated that nurse aides needed between 2.8 and 3.6 hours per resident per day in order to meet resident needs for assistance with activities of daily living (depending on resident acuity); however, reported staffing levels averaged only between 2.3 and 2.5 hours per resident per day (Schnelle et al., 2016). On average, 1 nursing assistant
supports 12 residents per shift, and 1 in 10 nursing assistants supports 16 or more residents (PHI, 2019).
Turnover and Burnout
Adequate staffing in nursing homes has been difficult to achieve because of high turnover, stigmatized perception of the CNA role, and poor working conditions (Manchha et al., 2021). One recent analysis using data from the Payroll-Based Journal found the average turnover rate among CNAs to be 129.1 percent; in comparison, turnover rates were 140.7 percent for RNs and 114.1 percent for LPNs, with some individual facilities found to have nursing staff turnover rates over 300 percent (Gandhi et al., 2021). High turnover is expensive for nursing homes and negatively affects the quality of the services delivered and the quality of life in nursing homes (Feuerberg, 2001; IOM, 2004; Seavey, 2004). Contributors to these high turnover rates among direct-care workers in nursing homes include characteristics related to the nature of the job itself and the working environment found in nursing homes, including factors that result in injury. One analysis, for example, found that more than half of CNAs had incurred at least one work-related injury within the past year and almost one-quarter of CNAs were unable to work for at least 1 day as a result of being injured (Squillace et al., 2009).
The top reasons for direct-care workers leaving their jobs include lack of respect, low salary, staff shortages, personal health concerns, lack of appreciation by the facility, lack of teamwork among the staff, lack of trusting relationships with residents and families, lack of tools to do the job, lack of good relationships with supervisors, and not being informed of changes before they are made (Bryant, 2017; Mickus et al., 2004; U.S. Congress, 2001; Zhang et al., 2016). For example, one study of nearly 400 nursing homes in Iowa found that higher wages were associated with lower CNA turnover (Sharma and Xu, 2022). Moreover, CNAs are also often undervalued for their skills, mistreated and disrespected, and experience workplace violence in the form of physical and verbal abuse (Tak et al., 2010). While the work of the direct-care workforce has commonly been referred to as physically demanding, in 2020 during the midst of the COVID-19 pandemic, nursing home workers saw one of the highest death rates among all occupations (Lewis, 2021). The direct-care workforce is likely to experience even higher rates of burnout, though most of the literature on the topic focuses on the rate of burnout among licensed nurses and physicians (Cooper et al., 2016). For a family member perspective on staff burnout, see Box 5-7.
Greater retention of CNAs has been found to be associated with improved functional status and fewer pressure ulcers, electrolyte imbalances, and urinary tract infections among nursing home residents (Kimmey and
Stearns, 2015; Trinkoff et al., 2017). Many approaches to support the retention of this direct-care workforce have been proposed, including
- Pay a wage reflective of the risks and physical demand that direct care workers assume daily.
- Provide a separate payment that can go toward wages, benefits (e.g., sick leave, health insurance), or both, similar to New York’s Home Care Worker Parity Law.22
- Enhance work relationships by improving communication and supervision so that CNAs feel appreciated, listened to, and treated with respect.
- Improve management systems by increasing and improving staffing and scheduling along with increasing the availability of more robust training and better career ladders.
- Improve work system factors, including helping CNAs with directions, providing resources and supplies, and preventing injury and exposure to hazards or violence (Kemper et al., 2008; Morris, 2009).
- Create formal promotion programs, peer mentoring programs, and tuition reimbursement programs and proactively engage nursing assistants in efforts to enact such programs (Kemper et al., 2008; Stone and Dawson, 2008).
Tailored and ongoing training programs improve job satisfaction and reduce turnover (Ejaz and Noelker, 2006; Han et al., 2014). For example, an approach based on the occupational adaptation framework (Schkade and McClung, 2001) has been found to show greater gains in skills mastery and more cooperative approaches to solving complex problems such as dementia care needs than traditional skills training approaches (McKay et al., 2021).
___________________
22 Additional information available at https://dol.ny.gov/home-health-care-aides-and-wage-parity (accessed November 3, 2021).
There is also a need for opportunities for job advancement and upgrading the skill of CNAs (Campbell, 2021; IOM, 2004; PHI, 2016; Wiener et al., 2009). Career advancement opportunities include attaining a specialized skill or expertise area (e.g., medication aide) or advancing to a higher level of licensing (e.g., LPN/LVN, RN). One older study demonstrated that empowering CNAs led to reductions in health deficiency citations, reduced staff turnover, and a decline in urinary incontinence rates among residents (Stone et al., 2002). Strategies specific to empowerment were mostly focused on having CNAs participate in care planning and care plan implementation.
Supervision and Support
The immediate supervision of direct-care workers is carried out by both LPN/LVNs and RNs. These relationships are often challenging as a result of power dynamics arising from the hierarchical structure of most nursing homes, incivility, bullying, and undue time demands (Cooke and Baumbusch, 2021; Lundin et al., 2021). When these groups work together to communicate and support one another, it makes for a better relationship, so decentralization of hierarchical systems can promote better teamwork across disciplines and roles (Kemper et al., 2008), and encourage supervisors to demonstrate supportive behaviors (McGilton et al., 2004). Relationships among personnel can also be improved by implementing leadership training for all levels of supervisors and managers, developing self-managed work teams, improving information sharing between nurses and direct-care staff, enhancing responsibilities for direct-care workers, facilitating team building and peer mentoring, and involving direct-care workers in care management decisions (Eaton, 2000; Eaton et al., 2001; Rantz et al., 2013; Stone and Dawson, 2008). Furthermore, nursing homes need to create a culture of values that fosters respect, trust, collaboration, and interprofessional health care team building (Kemper et al., 2008). Ultimately, nursing home leadership is responsible for creating a desirable working environment in the nursing home. For nursing home workers’ perspectives on supervision, support, and the workplace environment, see Box 5-8.
Expanded Roles for CNAs
One notable example of expanding recognition of the role and importance of the CNA is the Green House model for nursing home care (see Chapter 6). Green House nursing homes employ modified staff roles to split work, empower staff, and have staff members work together. Direct-care workers in Green Houses, referred to as “shahbazim” (singular, “shahbaz”), “work in self-managed teams and are responsible for direct resident care, cleaning, laundry, meal preparation, staff scheduling, and activities, and simulating how families might organize work” (Bowers and Nolet, 2014).
The shahbaz provides general oversight, while the nurse provides more clinical direction. One study found that an integrated model (with high interaction and coordination) between shabazim and nurses resulted in the best resident outcomes (Bowers and Nolet, 2014).
FAMILY CAREGIVERS
Family caregivers provide critical supports to nursing home residents, but they do not receive sufficient support, recognition, resources, or inclusion. Family involvement in the care of a nursing home resident is a multidimensional construct that entails visiting the resident, providing hands-on care and assistance with activities of daily living, supervising and monitoring the quality of care of the resident, providing emotional support, representing the resident’s perspective and history, and advocating for the resident in terms of safety and security (Bern-Klug and Forbes-Thompson, 2008; Coe and Werner, 2021; Gaugler, 2005; Lopez et al., 2013; NASEM, 2016). Family caregivers also often play a key role as surrogate decision makers for their loved ones, which can be particularly stressful (Givens et al., 2012; NASEM, 2016). For family member perspectives on the role of family in caring for nursing home residents, see Box 5-9.
However, upon a loved one’s entrance to a nursing home, the role of the family caregiver may become indirect as the family members endeavor to ensure that high-quality care is provided by facility staff. One analysis found that family caregivers feel responsible for maintaining continuity by
- Helping the resident maintain his or her sense of identity through the continuation of loving relationships and helping staff to get to know the resident as an individual;
- Monitoring the care received, providing feedback to staff, and filling gaps; and
- Contributing to community by interacting with other residents, relatives, and staff; taking part in social events; and generally providing a link with the outside world (Davies and Nolan, 2006).
Family caregivers may be especially important for the continuity of care for nursing home residents with dementia, with responsibilities such as ensuring that the resident is being treated with respect and receiving
high-quality care (Aneshensel et al., 1995; Duncan and Morgan, 1994; Graneheim et al., 2014; Reid and Chappell, 2017; Ross et al., 2001). Recognition of family caregivers as partners in the care of the person with dementia contributes to the overall quality of care (Graneheim et al., 2014). For example, family members often can help advocate for and help provide support for nonpharmacologic alternatives to help manage residents’ behavioral and psychological symptoms of dementia (Tjia et al., 2017). Overall, family involvement is a “strong predictor of perceived resident quality of life” (Roberts and Ishler, 2018).
As such, it is important to include the family members as essential members of the resident interdisciplinary care team. Family caregivers can serve as an extension of the staff and help workers better understand the resident’s goals and preferences, so that CNAs, nurses, and other staff can deliver sensitive, nurturing, and person-centered care to the resident (Kellett, 2007). This requires the development and maintenance of effective relationships and communication between family and staff (Bauer et al., 2014; Brown Wilson et al., 2009; Cohen et al., 2014; Henkusens et al., 2014; Maas et al., 2004). Keys to such development are trust in staff (Bauer et al., 2014; Bern-Klug and Forbes-Thompson, 2008; Rosemond et al., 2017) and ongoing monitoring of staff (Bramble et al., 2009). In her presentation to this committee, Beverley Laubert, a long-term care ombudsman for the Ohio Department of Aging, said
Quality care is relationship-based. For example, a CNA is given education in the basic principles of dementia care, but to truly be equipped to support a resident with memory impairment, that CNA must know something about the resident’s family and life story. Only then can the staff know and respond to the unique needs of the resident in their care. Similarly, the housekeeper should know something about the resident to understand that moving the resident’s Bible into a drawer could be disruptive.
Among the strategies and interventions that can facilitate collaborative and partnership efforts between family and staff are support groups and family councils (Baumbusch et al., 2022; Hoek et al., 2021). (See Chapters 4 and 8 for more on resident and family councils.) The Partners in Caregiving program developed by Pillemer et al. (2003) was designed to intervene not only on the part of family members (e.g., the formation of councils or support groups), but also to engage staff and administrators to effectively change facility policies focused on integrating family caregivers (CITRA, 2021). The Families Involved in Nursing Home Decision-Making program uses video-conferencing to include family in care plan meetings (Oliver et al., 2021). Family caregivers can also experience high levels of stress and can benefit from improved education and support for themselves.
For example, family caregivers express a desire for better education about disease course, treatment options, and surrogate decision making (e.g., placement of feeding tubes, end-of-life decisions) (Givens et al., 2012).
VOLUNTEERS
Apart from the family and friends of nursing home residents, volunteers from the local community (unrelated to the nursing home resident) may contribute to the care of nursing home residents. The organizational structure of the long-term care facility influences the “amount of volunteers in a nursing home, the types of activities in which volunteers engage and [the] quality of care” (Falkowski, 2013, p. 61). For example, data from the 2004 National Nursing Home Survey show that nonprofit facilities were likely to have more volunteers, more frequent visits by volunteers, and to use volunteers to support staff (e.g., for “clerical duties, helping at mealtime, and providing personal care”), while for-profit facilities tended to use volunteers in socialization activities (e.g., “game playing, conducting religious services, and making social visits”) (Falkowski, 2013, p. 4). Both the percentage of Medicare residents and the percentage of Medicaid residents in the nursing home were associated with a lower number of volunteers that visit weekly, and the number of volunteers in a nursing home was associated with the amount of socialization activities for nursing home residents. Finally volunteers need to be properly trained for their duties to support the relationships and trust between volunteers and staff so that staff can focus on more technical work (Falkowski, 2013). However, little is known about the best practices of training for maintaining an effective volunteer workforce.
Several studies provide evidence of the impact that volunteer services can have on the quality of life for nursing home residents (Saunders et al., 2019; van der Ploeg et al., 2012; Zhao et al., 2015), including mitigating the adverse effects of social isolation (Claxton-Oldfield, 2015; Cohen-Mansfield, 2001, 2013; Damianakis et al., 2007; van der Ploeg et al., 2012, 2014). Families also appreciate and benefit from volunteer support (Candy et al., 2015). For example, during the COVID-19 pandemic, the Yale School of Medicine Geriatrics Student Interest Group initiated the Telephone Outreach in the COVID-19 Outbreak Program in which student volunteers connected with older adults in nursing homes via weekly phone calls (van Dyck et al., 2020). In the three nursing homes that implemented the program for 30 residents, initial results have been generally positive, with residents expressing appreciation for the conversations, the student volunteers perceiving personal benefits (e.g., greater sense of purpose, improved well-being), and actionable needs being identified (e.g., obtaining desired books for a resident).
Research also suggests that volunteers are successful in supporting and caring for hospice patients and residents with dementia (Candy et al., 2015; Claxton-Oldfield, 2015; Damianakis et al., 2007). They are able to support residents at the end of life by performing a variety of tasks, including emotional support (e.g., comforting the residents’ fears), social support (e.g., engaging with the resident and their family), practical support (e.g., helping the resident with personal care), informational support (e.g., providing education so families and residents know what to expect), and more. In fact, one older study found that satisfaction and emotional well-being were higher in hospice programs that involved more volunteers (Block et al., 2010). Volunteers are also beneficial in caring for residents with dementia by facilitating activities that fill unmet needs (e.g., boredom, need for relaxation, loneliness agitation, etc.) by providing or removing stimuli (Cohen-Mansfield, 2013). However, more education and research is necessary to truly understand and promote the value of volunteer support services (Claxton-Oldfield, 2015; Cohen-Mansfield, 2013). For a family member perspective on volunteers, see Box 5-10.
EQUITY AND THE WORKFORCE
Occupational segregation is defined as overrepresentation or under-representation of a particular group (e.g., defined by race, sex, or immigration status) in specific jobs or fields (Bahn and Cumming, 2020). This type of segregation is characterized as a process fueled by a desire for social distance from a marginalized group (Tomaskovic-Devey, 2018), where opportunity or positions with greater authority are reserved for the group with the most social power (i.e., White men) (Bahn and Cumming, 2020). Workplace segregation for women and racial and ethnic minorities leads to
these groups holding positions with more routinized and controlled work and less supervisory authority (Tomaskovic-Devey, 2018). The overrepresentation of historically marginalized groups in occupations reduces their wages “irrespective of other measures of productivity such as required skill level” (Bahn and Cumming, 2020).
There are substantial differences in the racial and ethnic diversity among the roles within the nursing home workforce. The percent of racial and ethnic minorities in higher-level positions in the long-term care workforce decreases as the level of educational attainment required for a given position increases (Bates et al., 2018). For example, as shown in Figure 5-3, CNAs themselves are more diverse than the nursing home workforce overall.
Specifically, a higher percentage of CNAs are either Black/African American or Hispanic/Latinx as compared with the nursing home workforce overall, suggesting that higher-level positions within nursing homes are much less diverse. When such workforce disparities exist, they affect how work is organized (e.g., the autonomy and control afforded those jobs) as well the level of compensation and benefits associated with specific job titles, with racial and ethnic minorities and women often at the bottom of the workplace hierarchy (Tomaskovic-Devey, 2018). For example, one recent analysis (Travers et al., 2020) found that racial and ethnic minorities and immigrant direct-care workers—over 90 percent of whom
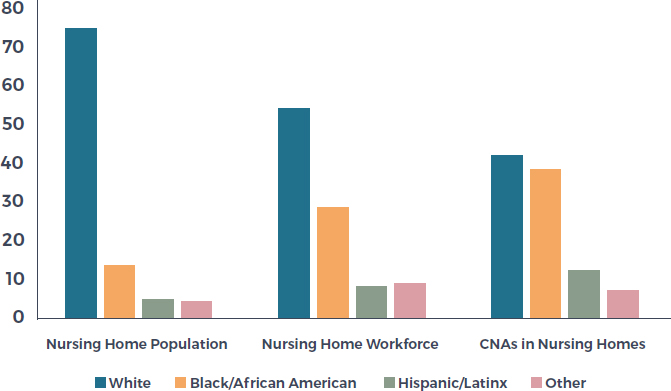
SOURCES: Bates et al., 2018; Harris-Kojetin et al., 2004; PHI, 2021.
are women—performed over 50 percent of the tasks related to helping residents with activities of daily living (Probst et al., 2010; Stacey, 2005).
A root cause for these types of disparities is systemic/structural racism, which is defined as a set of “historically and contextually specific ideological justifications for a society’s racialized social system” (Ray, 2019, p. 31). A 2021 review articulated the pathways through which systemic/structural racism has created and sustained disparities in the long-term care system in the United States (Sloane et al., 2021). Specific pathways include institutional factors such as
- Biased hiring, pay, and promotion practices that concentrate racial and ethnic minority and immigrant workers in specific low-resource nursing homes;
- Cultural factors, such as current and historic patterns of micro-aggressions, discrimination, and racial violence throughout society that influence the nursing home work environment; and
- Interpersonal factors, such as racial bias from residents and other staff members, directed at racial and ethnic minority and immigrant workers.
Therefore, all workers in nursing homes, including leadership, will likely benefit from training in principles of diversity, equity, and inclusion.
Providing Culturally Sensitive Care
In addition to concerns for the power dynamics and hierarchies of the workforce itself, the contrast between the diversity of the nursing home workforce and the residents they serve (see Figure 5-3) may create challenges in the delivery of high-quality care. For example, as noted in the 2008 IOM report Retooling for an Aging America, the diversity of the workforce is important because patients may prefer to be treated by health care professionals of the same ethnic background and a provider from a patient’s same ethnic background may have a better understanding of culturally appropriate demonstrations of respect or speak the same language (IOM, 2008). While the nursing home population is becoming more diverse, the patterns of diversity still may not match the workforce that cares for them.
FACTORS THAT INFLUENCE THE RELATIONSHIP BETWEEN STAFFING AND QUALITY
Several factors influence the relationship between staffing and quality, including the ownership status of the nursing home and employment patterns.
Ownership Status
As noted in Chapter 8, while there are important nuances related to the case mix of certain nursing homes and nursing home chains, the published literature suggests that in general, for-profit nursing homes consistently demonstrate lower levels of quality and satisfaction with care than not-for-profit nursing homes (Banaszak-Holl et al., 2002; GAO, 2011; Grabowski and Hirth, 2003; Harrington et al., 2001, 2012; Hillmer et al., 2005; Stevenson and Grabowski, 2008; You et al., 2016). In general, inadequate staffing and lower salaries have been long-standing issues in nursing homes as compared with acute-care settings. A 2012 study comparing staffing levels and deficiencies of for-profit nursing homes and five other ownership groups found that the 10 largest for-profit nursing home chains had lower RN and total nurse staffing hours than government facilities when controlling for other factors, and that they received 36 percent higher deficiencies (and 41 percent higher serious deficiencies) than government facilities (Harrington et al., 2012). (See Chapter 8 for more on transparency and ownership issues.)
Use of Temporary and Agency Staff
While many of the studies are old or not specific to nursing homes, considerable research has established that the use of high levels of temporary staff is an indicator of poor quality care and poor outcomes (Castle, 2009; Castle and Engberg, 2008; Senek et al., 2020). One study, for example, found that approximately 60 percent of nursing homes use at least some agency staff and that having agency staff account for 25 percent or more of the workforce was associated with 1 to 2 percent lower scores on quality measures (Castle, 2009). The manner in which nursing homes use agency staff may be the reason for lower quality (Castle, 2009).
Consistent Assignment
The consistent assignment of nursing staff to residents in nursing homes is a critical component of culture change and one that may help achieve quality of care and life for residents ( Advancing Excellence, 2021a; Castle, 2013; Roberts et al., 2015). Advancing Excellence in America’s Nursing Homes, a campaign to improve the quality of care and life in nursing homes, defines consistent assignment as “a resident receives care from the same nursing assistants 85 percent of the time” (Advancing Excellence, 2021b). However, studies have found that an average of only 68 percent of nursing homes use consistent assignment and only 28 percent of homes achieve the recommended level of 85 percent consistent staffing (Castle, 2011, 2013). Despite limited research on the topic, the available literature suggests that consistent staffing has been associated with lower turnover
and absenteeism among staff, fewer quality-of-care deficiency citations, and fewer quality-of-life deficiency citations (Castle, 2011, 2013). In her presentation to this committee, Beverley Laubert, a long-term care ombudsman for the Ohio Department of Aging, said
Current staff training requirements are insufficient to support residents’ quality of living. The best practice that I’ve seen for such relationship-based care is consistent assignment of staff. We know that consistent assignment matters to both the quality of work life and the residents’ living experience. Staff get to know specific residents, learn their preferences, and work proactively and efficiently. It makes the job more fulfilling. Residents and family don’t have to repeatedly train staff on their preferences then. But until consistent assignment is required and enforced, not just recommended as a best practice, that it’s the minimum practice, we won’t see sustained quality care.
For a family member perspective on consistent assignment, see Box 5-11.
COVID-19 AND NURSING HOME STAFFING
The COVID-19 pandemic resulted in disproportionate deaths of residents in nursing homes. The key predictors of nursing home COVID-19 cases and deaths—nursing home size and location—leave little room for immediate and direct intervention by the nursing homes themselves. However, staffing as a contributor to poor outcomes might be more under the control of nursing homes and more amenable to policy changes. The 2020 CMS Coronavirus Commission on Safety and Quality in Nursing Homes made many recommendations related to staff in nursing homes, including
- Mobilization of resources to support the workforce (e.g., increased breaks, identification of surges);
- Provision of safety guidance (e.g., related to testing of staff and residents, quarantine options, workers with multiple employers);
- Provision of guidance and training on the use and reuse of personal protective equipment (PPE);
- Support of 24-hour daily RN staffing in nursing homes with positive cases;
- Use of certified infection prevention and control specialists with educator capabilities; and
- Targeted recruitment of CNAs (MITRE, 2020).
Staffing Patterns and COVID-19 Impact
Multiple studies found that higher nurse staffing ratios mitigated the effect of an outbreak and resulted in fewer deaths once an outbreak occurred (Gorges and Konetzka, 2020; Konetzka et al., 2021; Li et al., 2020). At the same time, higher staffing ratios were not able to prevent the outbreak from starting, given that staff were often the source of bringing COVID-19 into facilities. One study found that while nursing homes with higher staffing ratios (just prior to the pandemic) did not have a reduced probability of an initial outbreak, higher baseline staffing ratios were helpful in stemming an outbreak once it started (Figueroa et al., 2020). Nursing homes with the highest staff hours per resident day experienced fewer cases and deaths than those at the bottom of the distribution. Several other studies demonstrated connections between staffing and impact of the COVID-19 pandemic, including
- Nursing homes with increased RN staffing had fewer confirmed COVID-19 cases and fewer deaths from COVID-19 (Li et al., 2020).
- Nursing homes in California with lower RN staffing had higher COVID-19 infections (Harrington et al., 2020).
- Staff size, including those not involved in direct resident care, was associated with more COVID-19 cases; therefore, “reducing the number of unique staff members without decreasing direct-care hours, such as by relying on full-time rather than part-time staff, could help prevent outbreaks” (McGarry et al., 2021b, p. 1261).
- Nearly half of nursing home COVID cases were attributable to cross-facility staff movement (Chen et al., 2021), contributing to the evidence of the impact of consistent staffing on quality of care.
Nurse practitioners working in nursing homes were found to be essential for containing the spread within the nursing homes and for providing much needed guidance to staff and care to residents during the pandemic (McGilton et al., 2021; Popejoy et al., 2020). Additionally, social workers (along with others) helped residents stay connected to their families (Kusmaul et al., 2020). This was particularly challenging as “access to technology was sporadic, and access to personal protective equipment, even
worse” (Kusmaul et al., 2020, p. 651). Additionally, some social workers were prevented from entering facilities or encouraged to work from home. In part, these challenges stemmed from social workers not being recognized as being “frontline workers” but rather as “non-essential.”
Staffing Shortages
Several studies and many anecdotal stories documented exacerbation of staffing shortages at various times throughout the COVID-19 pandemic (Abbasi, 2020b; Davidson and Szanton, 2020; Denny-Brown et al., 2020; Fernandez, 2021; Kirkham and Lesser, 2020; McGarry et al., 2020; Murray, 2021; Peck, 2021; Quinton, 2020; Sedensky, 2021; Weber, 2021; Xu et al., 2020). Early in the pandemic, staff shortages were found to be greater in nursing homes with lower quality scores that have a higher Medicaid population and where COVID-19 cases were more prevalent among staff or residents (McGarry et al., 2020; Xu et al., 2020). Many nursing homes increased their use of contract (agency) staff to fill these gaps (Peck, 2021; Stulick, 2021). A cross-sectional time-series study of over 15,000 nursing homes found that while urban nursing homes reported a relatively constant staffing shortage, rural nursing homes saw an increase in staffing shortages until November 2020 (Yang et al., 2021b). In December 2021, on average, 30.1 percent of nursing homes had shortages of nurses or nurse aides (AARP, 2022). However, this varied dramatically by state. For example, 73.5 percent of nursing homes in Wyoming had shortages of nurses or nurse aides, while only 3.6 percent of nursing homes in California had such shortages (AARP, 2022). Eight states had shortages in more than half of the nursing homes in the state.
Many nursing home workers, especially low-wage workers (e.g., CNAs, housekeepers) left their jobs for other positions in part due to working conditions and opportunities for higher-paying jobs (Quinton, 2020; Tan, 2022; Varney, 2021). Dr. David Gifford, chief medical officer for the American Health Care Association and the National Center for Assisted Living (AHCA/NCAL), noted
Nursing homes are in constant competition for staff. Many providers struggle to recruit and retain caregivers who can often find less demanding jobs in other settings, such as hospitals and industries that can offer better pay. (Romero, 2021)
However, Werner and Coe (2021) found a decline in the average total number of staff hours per day that was accompanied by a decline in the resident census itself, resulting in a slight increase in the number of staff hours per resident day (Werner and Coe, 2021). They suggested that this discrepancy might be explained by the increased use of contractors, the
increased intensity of the work (i.e., caring for residents during the pandemic requires more staff time), increased hours among the existing staff, or the loss of the contributions of family caregivers (Werner and Coe, 2021).
CMS Staffing Waivers and Temporary Nurse Aides
Early in the COVID-19 pandemic, CMS provided blanket waivers for a variety of regulations related to nursing home workers. For example, CMS waived certain requirements for in-person visits by physicians and others, allowed physicians to delegate certain tasks to APRNs and physician assistants, and reduced paid feeding assistant training to just one hour (CMS, 2021c). In addition, CMS waived training and certification requirements for new CNAs; these temporary nurse aides only needed to “demonstrate competency in skills and techniques necessary to care for residents’ needs” (CMA, 2021, p. 17). Serious concerns were raised about the risks that a lack of training creates for both nursing home residents and the workers themselves (Hauslohner and Sacchetti, 2020; Scales, 2020; Severens, 2020). In response, many states imposed their own training requirements for temporary nurse aides and AHCA/NCAL developed a free 8-hour online training program that many states recognized as satisfying their requirements (either alone or in conjunction with other stipulations) (AHCA/NCAL, 2022; Scales, 2021; Van Houtven et al., 2021). The Nurses Certification and Recognition of Experience (CARE) Act of 202123 proposes a pathway for temporary nurse aides to continue in their jobs after the pandemic without fulfilling the full requirements to become a CNA. However, concerns have been raised about the lack of formal training many of these workers have received (less than the current 75 hours of required training, which as discussed earlier in this chapter, has been found to be insufficient) and the provision that allows employers to attest to the competency of these workers (without testing) (CMA, 2021; Scales, 2021; Van Houtven et al., 2021). Currently, there is no systematic tracking of temporary nurse aides (Edelman, 2020; Scales, 2021).
Worker Health and Safety
Nursing home staff commonly suffered from a lack of PPE. McGarry and colleagues (2020) found that early in the pandemic, about one in five nursing homes had shortages of PPE, particularly gowns and N95 respirators. Labor unions representing health care workers advocated for improved access to personal protective equipment and infection control practices. In New York, the presence of a union for health care workers was associated with a 30 percent lower mortality rate from COVID-19 for nursing home residents. Nursing homes with unions also had lower COVID-19
___________________
23 Nurses Certification and Recognition of Experience (CARE) Act of 2021, HR 331, 117th Cong., 1st sess. (January 15, 2021).
infection rates as well as a 13.8 percent greater access to N95 respirators and 7.3 percent greater access to eye shields for staff (Dean et al., 2020)
Additionally, COVID-19 affected the health of nursing home workers themselves. Given the vulnerability of the nursing home population, nursing home workers may have increased exposure to COVID-19 as compared to workers in other settings. As of November 2021, there have been 673,591 confirmed cases of COVID-19 among nursing home staff and 2,166 deaths (CMS, 2021d). In fact, one analysis suggests that nursing home workers had one of the highest death rates among all occupations (Lewis, 2021). However, vaccination rates among nursing home workers remain relatively low (AARP, 2021; CMS, 2021d; Gharpure et al., 2021; McGarry et al., 2021c), particularly among CNAs (49.2 percent as of July 2021). Nursing home staff also experienced high rates of stress and burnout due to fears of contracting COVID-19, fear of infecting their families, and increased intensity of the work (Weber, 2021; Werner and Coe, 2021; White et al., 2021). The use of telehealth has been suggested as one modality that could lower stress among staff, enable planning and information sharing between families and staff, and provide “flexible options for staff education and training” (Edelman et al., 2020, p. 1).
Strike Teams
The COVID-19 pandemic offered unique opportunities for collaboration among public health stakeholders; health care providers; local, state, and federal governments; and other organizations. Strike teams, defined as “multidisciplinary teams deployed to support public health emergency response efforts,” supported long-term care facilities experiencing outbreaks and resource shortages by providing technical assistance and guidance to “improve infection control practices as a short-term strategy to minimize the impact of the virus” (ASTHO, 2021). Strike teams address a variety of issues, including visitor guidance, vaccine administration, infection prevention and control education, the supply of personal PPE, and more (AMDA, 2021).
Several states implemented strike teams during the COVID-19 pandemic. Massachusetts invested $130 million over 2 months to create a 28-item checklist of infection control practices which were subject to state audits and to deploy infection control teams to 123 facilities that were struggling to pass the audits (Lipsitz et al., 2020). The program also went beyond immediate technical assistance and provided weekly educational webinars, assisted with procurement of resources, and provided payment incentives to nursing homes (Lipsitz et al., 2020). Other states (e.g., Louisiana and Washington) collaborated with the CDC to support PPE distribution, arrange COVID testing and cohorting practices, and develop infection control practices and guidelines (ASTHO, 2021).
In October 2021, the CDC, in partnership with CMS, joined state efforts by allocating $500 million to allow state and other jurisdictional health departments to staff, train, and deploy strike teams to expand clinical surge capacity, address staffing shortages, and strengthen infection control policies and procedures in a variety of health care settings (including nursing homes) (CDC, 2021a,b). Awardees are required to use funds for technical assistance to prevent COVID outbreaks and may optionally use funds to supply resources and other infrastructure support (e.g., environmental assessments of ventilation) (CDC, 2021b).
KEY FINDINGS AND CONCLUSIONS
The Overall Nursing Home Workforce
- A wide variety of workers help to support nursing home residents in achieving their goals and preferences.
- Very little evidence exists about many members of the nursing home workforce, including their impact on the quality of care as well as basic demographic information.
- Family caregivers (including chosen families) provide critical supports to nursing home residents, but they do not receive sufficient support, recognition, resources, or inclusion.
- There is high turnover of many types of nursing home staff, which is associated with lower levels of quality.
- An interdisciplinary care team approach is related to reduced staff turnover and increased staff satisfaction.
- Many health care practitioners are not adequately prepared for their specific role and responsibilities in the nursing home setting.
- Many nursing home workers earn less than their counterparts in other settings of care.
- Systemic and structural racism have created and sustained racial and ethnic disparities in the long-term care system.
- Factors that can influence the relationship between staffing and quality of care include the ownership status of the nursing home, the use of temporary or agency staff, and a lack of consistent assignment.
Nursing Home Administration and Leadership
- Nursing home federal regulations require that the administrator of a nursing home is licensed by the state. However, states vary in their requirements for minimum education, training hours, examinations, and continuing education.
- Except for the requirement of a license to practice medicine in the state, there are no additional specific education and training requirements for medical directors.
- Limited data exist on the characteristics of nursing home administrators, medical directors, and directors of nursing.
- The director of nursing is often called upon to address the clinical needs of residents in addition to his or her administrative responsibilities.
- No federal or state requirements specify minimum education requirements, continuing education requirements, or additional training requirements for directors of nursing.
- Evidence on the characteristics, education and training, job satisfaction, and turnover of social services directors is limited or nonexistent.
- Forty-two percent of social services directors do not have a degree in social work.
Primary Care Providers
- Limited and dated evidence exists focusing on primary care providers for nursing home residents, particularly for physicians and physician assistants.
- APRN-provided care has been associated with improved quality of care for nursing home residents and increased resident, family, and staff satisfaction.
- The most frequently mentioned barrier for increasing the role of APRNs in nursing homes is their restricted scope of practice due to Medicare regulations and state regulatory constraints.
Nurse Staffing
- Nursing staff (including RNs, LPN/LVNs, and CNAs) are key to providing comprehensive nursing home care.
- RNs and LPN/LVNs have been used interchangeably in nursing homes, with LPN/LVNs working outside their scope of practice.
- Decades of evidence support the association between inadequate nurse staffing and poor quality of care in nursing homes, particularly for RNs.
- While several studies have called for 24-hour RN coverage in nursing homes, today the requirement is a 24-hour daily presence of a licensed nurse (i.e., RN or LPN/LVN) with an RN fulfilling at least 8 of those hours.
- The 2001 proposed CMS minimum staffing standards have not been addressed in any regulations, and current staffing requirements are not adjusted by resident case mix.
- Most nursing homes do not have sufficient nursing staff to meet the needs of residents and are not adjusting staffing to take resident acuity into account.
- Nursing levels decrease significantly over weekends; GAO recommended reporting these measures on Care Compare.
- CMS can provide staffing data to state survey agencies to help with their approach to timing of inspections.
Psychosocial and Spiritual Care Providers
- Social workers have a positive impact on quality of care.
- Two-thirds of nursing homes are not required to employ a social services staff member.
- According to federal regulations, a “qualified social worker” does not need to have a degree in social work.
- Nursing homes employ too few chaplains to meet the needs of seriously ill patients and may instead designate social workers to get additional education or find a volunteer chaplain.
Certified Nursing Assistants (CNAs)
- CNAs provide the majority of hands-on care to nursing home residents.
- In spite of decades of calls for enhancing the training of CNAs, minimum training standards for CNAs have not changed since 1987.
- The top reasons for direct-care workers leaving their jobs include a lack of respect, low salary, difficulty of the job, staff shortages, personal health concerns, a lack of appreciation by the facility, a lack of teamwork among the staff, a lack of trusting relationships with residents and families, a lack of tools to do the job, a lack of good relationships with supervisors, and not being informed of changes before they are made.
Infection Prevention and Control Leadership and the Impact of COVID-19
- There are no national standards for training and licensure of infection prevention and control specialists, and most of these specialists are not certified in infection control.
- Presence of APRNs, increased RN staffing, and consistent staffing were associated with better COVID-19 outcomes.
REFERENCES
AADNS (American Association of Directors of Nursing Services). 2019. 2019 AADNS work time study and salary report. Denver, CO: American Association Post-Acute Care Nursing, American Association of Directors of Nursing Services.
AADNS. 2021. DNS-CT candidate handbook. Denver, CO: American Association Post-Acute Care Nursing, American Association of Directors of Nursing Services.
AAPACN (American Association of Post-Acute Care Nursing). 2021. Director of nursing services–certified. https://www.aapacn.org/education/dns-ct (accessed July 7, 2021).
AARC (American Association for Respiratory Care). 2016. Position statement: Delivery of respiratory therapy services in skilled nursing facilities providing ventilator and/or high acuity respiratory care. https://www.aarc.org/wp-content/uploads/2014/10/delivery_of_services_in_snf.pdf (accessed August 18, 2021).
AARC. 2017. Skilled nursing facilities (SNF). https://www.aarc.org/advocacy/federal-policies-affecting-rts/skilled-nursing-facilities-snf (accessed August 18, 2021).
AARP. 2021. 4 in 5 U.S. nursing homes behind on staff vaccination goal, analysis finds. https://www.aarp.org/caregiving/health/info-2021/nursing-home-staff-vaccine-threshold.html (accessed November 21, 2021).
AARP. 2022. AARP nursing home COVID-19 dashboard. https://www.aarp.org/ppi/issues/caregiving/info-2020/nursing-home-covid-dashboard.html (accessed February 16, 2022).
Abbasi, J. 2020a. Social isolation—The other COVID-19 threat in nursing homes. JAMA 324(7):619–620.
Abbasi, J. 2020b. “Abandoned” nursing homes continue to face critical supply and staff shortages as COVID-19 toll has mounted. JAMA 324(2):123–125.
ABPLM (American Board of Post-Acute and Long-Term Care Medicine, Inc.) 2022a. Certified medical director (CMD). https://www.abplm.org/home (accessed February 8, 2022).
ABPLM. 2022b. Certified Medical Director (CMD) initial certification application. https://www.abplm.org/_files/ugd/c389c5_266ac9b1632c4dd992034a235b2bbbad.pdf (accessed February 8, 2022).
Ackermann, R. J., and K. A. Kemle. 1998. The effect of a physician assistant on the hospitalization of nursing home residents. Journal of the American Geriatrics Society 46(5): 610–614.
ADA (American Dental Association). 2021. Specialty definitions. https://www.ada.org/en/ncrdscb/dental-specialties/specialty-definitions (accessed September 30, 2021).
Advancing Excellence (Advancing Excellence in America’s Nursing Homes). 2021a. Implementation guide: Goal 8—Improving consistent assignment of nursing home staff. https://theconsumervoice.org/uploads/files/long-term-care-recipient/Auld,Rosenthal-3of4-Concurrent(ConsistentAssignment).pdf (accessed September 17, 2021).
Advancing Excellence. 2021b. Increasing use of consistent assignment. https://www.leadingageok.org/ConsistentAssignment.pdf (accessed September 17, 2021).
AHCA/NCAL (American Health Care Association and National Center for Assisted Living). 2022. Temporary nurse aide. https://educate.ahcancal.org/tna (accessed February 9, 2022).
Aiken, L. H. 1981. Nursing priorities for the 1980’s: Hospitals and nursing homes. American Journal of Nursing 81(2):324–330.
AMDA (Society for Post-Acute and Long-Term Care Medicine). 2003. Role of the attending physician in the nursing home. https://paltc.org/amda-white-papers-and-resolution-position-statements/role-attending-physician-nursing-home (accessed November 9, 2021).
AMDA. 2005. Roles and responsibilities of the medical director in the nursing home: Position statement A03. Journal of the American Medical Directors Association 6(6):411–412.
AMDA. 2011. Collaborative and supervisory relationships between attending physicians and advanced practice nurses in long-term care facilities. Journal of the American Medical Directors Association 12(1):12–18.
AMDA. 2021. Policy brief: Implement nursing home strike teams. https://paltc.org/sites/default/files/Policy%20Brief%20on%20NH%20Strike%20Teams%20final%20v4.pdf (accessed October 22, 2021).
AMDA. 2022. Core Curriculum: Medical direction in PALTC. https://apex.paltc.org/page/core-curriculum-on-medical-direction (accessed February 8, 2022).
ANA (American Nurses Association). 2015. Nursing: Scope and standards of practice. Silver Spring, MD: American Nurses Association.
ANA. 2016. Nursing administration: Scope and standards of practice. 2nd ed. Silver Springs, MD: American Nurses Association.
ANA Enterprise (American Nurses Association Enterprise). 2015. Medication aide/technician categories by state. https://www.nursingworld.org/~4af4e6/globalassets/docs/ana/ethics/state-chart-medication-aide-status-09-15.pdf (accessed June 23, 2021).
Aneshensel, C. S., L. I. Pearlin, J. T. Mullan, S. H. Zarit, and C. J. Whitlatch. 1995. Profiles in caregiving: The unexpected career. San Diego: Academic Press.
Antwi, Y. A., and J. R. Bowblis. 2018. The impact of nurse turnover on quality of care and mortality in nursing homes: Evidence from the great recession. American Journal of Health Economics 4(2):131–163.
AONE/AONL (American Organization of Nurse Executives, American Organization for Nursing Leadership). 2015. AONL nurse executive competencies: Post-acute care. Chicago, IL: AONE and AONL.
AOTA (American Occupational Therapy Association). 2015. Occupational therapy’s role with skilled nursing facilities. https://www.aota.org/~/media/Corporate/Files/AboutOT/Professionals/WhatIsOT/RDP/Facts/FactSheet_SkilledNursingFacilities.pdf (accessed August 18, 2021).
Arling, G., R. L. Kane, C. Mueller, J. Bershadsky, and H. B. Degenholtz. 2007. Nursing effort and quality of care for nursing home residents. The Gerontologist 47(5):672–682.
Arling, G., and C. Mueller. 2014. Nurse staffing and quality: The unanswered question. Journal of the American Medical Directors Association 15(6):376–378.
ASHA (American Speech–Language–Hearing Association). 2021. 2021 SLP health care survey: Survey summary report: Number and type of responses. https://www.asha.org/siteassets/surveys/2021-slp-health-care-survey-summary-report.pdf (accessed August 18, 2021).
Ashraf, M. S., and S. Bergman. 2021. The case for consultant pharmacists as key players in nursing home antibiotic stewardship programs. Journal of the American Medical Directors Association 22(1):6–8.
ASTHO (Association of State and Territorial Health Officials). 2021. Partner coordination efforts to strengthen infection prevention and control practices: Lessons from the COVID-19 response. https://astho.org/ASTHOReports/Partner-Coordination-Efforts-to-Strengthen-Infection-Prevention-and-Control-Practices/04-09-21 (accessed October 22, 2021).
Backhaus, R., H. Verbeek, E. van Rossum, E. Capezuti, and J. P. Hamers. 2014. Nurse staffing impact on quality of care in nursing homes: A systematic review of longitudinal studies. Journal of the American Medical Directors Association 15(6):383–393.
Bahn, K., and C. S. Cumming. 2020. Factsheet: U.S. occupational segregation by race, ethnicity, and gender. https://equitablegrowth.org/factsheet-u-s-occupational-segregation-by-race-ethnicity-and-gender (accessed July 7, 2021).
Bakerjian, D. 2008. Care of nursing home residents by advanced practice nurses. A review of the literature. Research in Gerontological Nursing 1(3):177–185.
Banaszak-Holl, J., W. B. Berta, D. M. Bowman, J. A. Baum, and W. Mitchell. 2002. The rise of human service chains: Antecedents to acquisitions and their effects on the quality of care in U.S. nursing homes. Managerial and Decision Economics 23(4–5):261–282.
Barlas, S. 2012. Medicare wants only ‘independent’ consultant pharmacists in nursing homes. Pharmacy and Therapeutics 37(1):6.
Bates, T., G. Amah, and J. Coffman. 2018. Racial/ethnic diversity in the long-term care workforce. San Francisco, CA: UCSF Health Workforce Research Center on Long-term Care.
Bauer, M., D. Fetherstonhaugh, L. Tarzia, and C. Chenco. 2014. Staff–family relationships in residential aged care facilities: The views of residents’ family members and care staff. Journal of Applied Gerontology 33(5):564–585.
Baumbusch, J., I. Sloan Yip, S. Koehn, R. C. Reid, and P. Gandhi. 2022. A survey of the characteristics and administrator perceptions of family councils in a western Canadian province. Journal of Applied Gerontology 41(2):363–370.
Bell, S. A., M. Bern-Klug, K. W. O. Kramer, and J. B. Saunders. 2010. Most nursing home social service directors lack training in working with lesbian, gay, and bisexual residents. Social Work in Health Care 49(9):814–831.
Bern-Klug, M. 2008. State variations in nursing home social worker qualifications. Journal of Gerontological Social Work 51(3–4):379–409.
Bern-Klug, M., and S. Forbes-Thompson. 2008. Family members’ responsibilities to nursing home residents: “She is the only mother I got.” Journal of Gerontological Nursing 34(2): 43–52.
Bern-Klug, M., and K. W. O. Kramer. 2013. Core functions of nursing home social services departments in the United States. Journal of the American Medical Directors Association 14(1):75.e1–75.e7.
Bern-Klug, M., and B. Sabri. 2012. Nursing home social services directors and elder abuse staff training. Journal of Gerontological Social Work 55(1):5–20.
Bern-Klug, M., R. Connolly, D. Downes, C. Galambos, N. Kusmaul, R. Kane, P. Hector, E. Beaulieu, on behalf of the National Nursing Home Social Work Network. 2016. Responding to the 2015 CMS proposed rule changes for LTC facilities: A call to redouble efforts to prepare students and practitioners for nursing homes. Journal of Gerontological Social Work 59(2):98–127.
Bern-Klug, M., E. Byram, N. Sabbagh Steinberg, H. Gamez Garcia, and K. C. Burke. 2018. Nursing home residents’ legal access to onsite professional psychosocial care: Federal and state regulations do not meet minimum professional social work standards. The Gerontologist 58(4):e260–e272.
Bern-Klug, M., K. M. Smith, A. R. Roberts, N. Kusmaul, D. Gammonley, P. Hector, K. Simons, C. Galambos, R. P. Bonifas, C. Herman, D. Downes, J. C. Munn, G. Rudderham, E. A. Cordes, and R. Connolly. 2021a. About a third of nursing home social services directors have earned a social work degree and license. Journal of Gerontological Social Work 64(7):699–720.
Bern-Klug, M., K. A. Carter, and Y. Wang. 2021b. More evidence that federal regulations perpetuate unrealistic nursing home social services staffing ratios. Journal of Gerontological Social Work 64(7):811–831.
Bethell, J., H. M. O’Rourke, H. Eagleson, D. Gaetano, W. Hykaway, and C. McAiney. 2021. Social connection is essential in long-term care homes: Considerations during COVID-19 and beyond. Canadian Geriatrics Journal 24(2):151–153.
Block, E. M., D. J. Casarett, C. Spence, P. Gozalo, S. R. Connor, and J. M. Teno. 2010. Got volunteers? Association of hospice use of volunteers with bereaved family members’ overall rating of the quality of end-of-life care. Journal of Pain and Symptom Management 39(3):502–506.
BLS (U.S. Bureau of Labor Statistics). 2020a. May 2020 national industry-specific occupational employment and wage estimates: NAICS 623100—Nursing care facilities (skilled nursing facilities). https://www.bls.gov/oes/current/naics4_623100.htm (accessed August 12, 2021).
BLS. 2020b. 2018 SOC definitions. https://www.bls.gov/soc/2018/soc_2018_definitions.pdf (accessed April 15, 2020).
BLS. 2020c. Occupational employment and wages, May 2020a, 29-1141: Registered nurses. https://www.bls.gov/oes/current/oes291141.htm#nat (accessed February 10, 2022).
BLS. 2021a. Occupational outlook handbook: Speech–language pathologists. https://www.bls.gov/ooh/Healthcare/Speech-language-pathologists.htm (accessed August 18, 2021).
BLS. 2021b. Occupational outlook handbook: Nursing assistants and orderlies. https://www.bls.gov/ooh/healthcare/nursing-assistants.htm (accessed November 21, 2021).
BLS. 2021c. Occupational employment and wages, May 2020: Nursing assistants. https://www.bls.gov/oes/current/oes311131.htm (accessed November 30, 2021).
BLS. 2021d. Occupational outlook handbook: Cashiers. https://www.bls.gov/ooh/sales/cashiers.htm (accessed February 8, 2022).
BLS. 2021e. Occupational outlook handbook: Food and beverage serving and related workers. https://www.bls.gov/ooh/food-preparation-and-serving/food-and-beverage-serving-and-related-workers.htm (accessed February 8, 2022).
BLS. 2021f. Occupational outlook handbook: Retail sales workers. https://www.bls.gov/ooh/sales/retail-sales-workers.htm (accessed February 8, 2022).
Bonifas, R. P. 2015. Resident-to-resident aggression in nursing homes: Social worker involvement and collaboration with nursing colleagues. Health & Social Work 40(3):e101–e109.
Bostick, J. E., M. J. Rantz, M. K. Flesner, and C. J. Riggs. 2006. Systematic review of studies of staffing and quality in nursing homes. Journal of the American Medical Directors Association 7(6):366–376.
Bowers, B. J., and K. Nolet. 2014. Developing the Green House nursing care team: Variations on development and implementation. The Gerontologist 54(Suppl 1):S53–S64.
Bramble, M., W. Moyle, and M. McAllister. 2009. Seeking connection: Family care experiences following long-term dementia care placement. Journal of Clinical Nursing 18(22):3118–3125.
Brown, D. 2021. New minimum staffing mandates finalized for NY providers. https://www.mcknights.com/news/new-minimum-staffing-mandates-finalized-for-ny-providers (accessed November 21, 2021).
Brown Wilson, C., S. U. E. Davies, and M. Nolan. 2009. Developing personal relationships in care homes: Realising the contributions of staff, residents and family members. Ageing and Society 29(7):1041–1063.
Bryant, O. A. 2017. Employee turnover in the long-term care industry. Walden Dissertations and Doctoral Studies 3389. https://scholarworks.waldenu.edu/dissertations/3389 (accessed May 4, 2022).
CALTCM (California Association of Long Term Care Medicine). 2021. Understanding the California requirement (AB 749) and the process to become, maintain, or reinstate the certified medical director (CMD) credential. https://www.caltcm.org/certified-medical-director-cmd-information (accessed February 8, 2022).
Campbell, S. 2018. Racial disparities in the direct care workforce: Spotlight on Black/African American workers. https://phinational.org/wp-content/uploads/2018/02/Black-DirectCare-Workers-PHI-2018.pdf (accessed August 13, 2021).
Campbell, S., A. D. R. Drake, R. Espinoza, and K. Scales. 2021. Caring for the future: The power and potential of America’s direct care workforce. New York: PHI.
Candy, B., R. France, J. Low, and L. Sampson. 2015. Does involving volunteers in the provision of palliative care make a difference to patient and family wellbeing? A systematic review of quantitative and qualitative evidence. International Journal of Nursing Studies 52(3):756–768.
Caprio, T. V. 2006. Physician practice in the nursing home: Collaboration with nurse practitioners and physician assistants. Annals of Internal Medicine 14(3):17–24.
Casper, M. L. 2013. Speech–language pathology in the long-term care setting: It isn’t your grandmother’s nursing home anymore. Seminars in Speech and Language 34(1):29–36.
Castle, N. G. 2001. Administrator turnover and quality of care in nursing homes. The Gerontologist 41(6):757–767.
Castle, N. G. 2005. Turnover begets turnover. The Gerontologist 45(2):186–195.
Castle, N. G. 2008. Nursing home caregiver staffing levels and quality of care: A literature review. Journal of Applied Gerontology 27(4):375–405.
Castle, N. G. 2009. Use of agency staff in nursing homes. Research in Gerontological Nursing 2(3):192–201.
Castle, N. G. 2011. The influence of consistent assignment on nursing home deficiency citations. The Gerontologist 51(6):750–760.
Castle, N. G. 2013. Consistent assignment of nurse aides: Association with turnover and absenteeism. Journal of Aging & Social Policy 25(1):48–64.
Castle, N. G., and F. H. Decker. 2011. Top management leadership style and quality of care in nursing homes. The Gerontologist 51(5):630–642.
Castle, N. G., and J. B. Engberg. 2008. The influence of agency staffing on quality of care in nursing homes. Journal of Aging & Social Policy 20(4):437–457.
Castle, N. G., J. Engberg, and R. A. Anderson. 2007. Job satisfaction of nursing home administrators and turnover. Medical Care Research and Review 64(2):191–211.
Castle, N. G., J. Furnier, J. C. Ferguson-Rome, D. Olson, and J. Johs-Artisensi. 2015. Quality of care and long-term care administrators’ education: Does it make a difference? Health Care Management Review 40(1):35–45.
CDC (Centers for Disease Control and Prevention). 2021a. CDC to invest $2.1 billion to protect patients and healthcare workers from COVID-19 and future infectious diseases. https://www.cdc.gov/media/releases/2021/p0917-COVID-19-funding.html (accessed October 25, 2021).
CDC. 2021b. Nursing home & long-term care facility strike team and infrastructure project guidance: Project E—Emerging issues. Washington, DC: Centers for Disease Control and Prevention.
CDC TRAIN. 2021. Nursing home infection preventionist training course. https://www.train.org/cdctrain/training_plan/3814 (accessed April 29, 2021).
Chen, M. K., J. A. Chevalier, and E. F. Long. 2021. Nursing home staff networks and COVID-19. Proceedings of the National Academy of Sciences of the United States of America 118(1):e2015455118.
Christian, R., and K. Baker. 2009. Effectiveness of nurse practitioners in nursing homes: A systematic review. JBI Library of Systematic Reviews 7(30):1333–1352.
CITRA (Cornell Institute for Translational Research on Aging). 2021. Partners in Caregiving (PIC). http://citra-pic.human.cornell.edu (accessed May 26, 2021).
Clarke, S. P., and N. E. Donaldson. 2008. Chapter 25. Nurse staffing and patient care quality and safety. In R. Hughes (ed.), Patient safety and quality: An evidence-based handbook for nurses. Rockville, MD: Agency for Healthcare Research and Quality.
Claxton-Oldfield, S. 2015. Got volunteers? The selection, training, roles, and impact of hospice palliative care volunteers in Canada’s community-based volunteer programs. Home Health Care Management & Practice 27(1):36–40.
CMA (Center for Medicare Advocacy). 2014. Staffing deficiencies in nursing facilities: Rarely cited, seldom sanctioned. https://medicareadvocacy.org/staffing-deficiencies-in-nursing-facilities-rarely-cited-seldom-sanctioned (accessed November 9, 2021).
CMA. 2021. Who provides care for nursing home residents? An update on temporary nurse aides. https://medicareadvocacy.org/wp-content/uploads/2021/09/SNF-TNAReport-09-2021.pdf (accessed January 20, 2022).
CMS (Centers for Medicare & Medicaid Services). 2005. State operations provider certification: Medical director guidance. CMS Manual System Pub. 100-07. https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R15SOMA.pdf (accessed August 20, 2021).
CMS. 2007. Nursing homes – issuance of new tag F373 (paid feeding assistants) as part of Appendix PP, State Operations Manual, including training materials. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/downloads/SCLetter07-30.pdf (accessed February 9, 2022).
CMS. 2016. Final rule: Medicare and Medicaid programs; reform of requirements for longterm care facilities. https://s3.amazonaws.com/public-inspection.federalregister.gov/2016-23503.pdf (accessed August 20, 2021).
CMS. 2019a. Long-term care facility resident assessment instrument 3.0 user’s manual. https://downloads.cms.gov/files/mds-3.0-rai-manual-v1.17.1_october_2019.pdf (accessed August 20, 2021).
CMS. 2019b. Medicare and Medicaid programs; requirements for long-term care facilities: Regulatory provisions to promote efficiency, and transparency. https://www.federalregister.gov/documents/2019/07/18/2019-14946/medicare-and-medicaid-programs-requirements-for-long-term-care-facilities-regulatory-provisions-to (accessed October 15, 2021).
CMS. 2021a. Consultation services rendered by a podiatrist in a skilled nursing facility. https://www.cms.gov/medicare-coverage-database/view/ncd.aspx?NCDId=170 (accessed November 21, 2021).
CMS. 2021b. Staffing data submission Payroll Based Journal (PBJ). https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/Staffing-Data-Submission-PBJ (accessed November 20, 2021).
CMS. 2021c. COVID-19 emergency declaration blanket waivers for health care providers. https://www.cms.gov/files/document/covid-19-emergency-declaration-waivers.pdf (accessed January 12, 2022).
CMS, 2021d. COVID-19 nursing home data. https://data.cms.gov/covid-19/covid-19-nursing-home-data (accessed November 21, 2021).
Coe, N. B., and R. M. Werner. 2021. Informal caregivers provide considerable front-line support in residential care facilities and nursing homes. Health Affairs 41(1):105–111.
Cohen, L. W., S. Zimmerman, D. Reed, P. D. Sloane, A. S. Beeber, T. Washington, J. G. Cagle, and L. P. Gwyther. 2014. Dementia in relation to family caregiver involvement and burden in long-term care. Journal of Applied Gerontology 33(5):522–540.
Cohen-Mansfield, J. 2001. Nonpharmacologic interventions for inappropriate behaviors in dementia: A review, summary, and critique. American Journal of Geriatric Psychiatry 9(4):361–381.
Cohen-Mansfield, J. 2013. Nonpharmacologic treatment of behavioral disorders in dementia. Current Treatment Options in Neurology 15(6):765–785.
Consumer Voice. 2021. State staffing nursing home standards. https://theconsumervoice.org/uploads/files/issues/CV_StaffingReport.pdf (accessed February 8, 2022).
Cooke, H. A., and J. Baumbusch. 2021. Not just how many but who is on shift: The impact of workplace incivility and bullying on care delivery in nursing homes. The Gerontologist 61(4):563–572.
Cooper, S. L., H. L. Carleton, S. A. Chamberlain, G. G. Cummings, W. Bambrick, and C. A. Estabrooks. 2016. Burnout in the nursing home health care aide: A systematic review. Burnout Research 3(3):76–87.
Corazzini, K. N., R. A. Anderson, C. Mueller, S. Hunt-McKinney, L. Day, and K. Porter. 2013. Understanding RN and LPN patterns of practice in nursing homes. Journal of Nursing Regulation 4(1):14–18.
Corazzini, K. N., E. S. McConnell, L. Day, R. A. Anderson, C. Mueller, A. Vogelsmeier, S. Kennerly, B. Walker, J. T. Flanagan, and M. Haske-Palomino. 2015. Differentiating scopes of practice in nursing homes: Collaborating for care. Journal of Nursing Regulation 6(1):43–49.
CSWE (Council on Social Work Education). 2015. Educational policy and accreditation standards https://www.cswe.org/getattachment/Accreditation/Accreditation-Process/2015-EPAS/2015EPAS_Web_FINAL.pdf.aspx (accessed November 20, 2021).
CSWE. 2021. CSWE’s Educational Policy and Accreditation Standards (EPAS) in diversity and justice. https://www.cswe.org/Centers-Initiatives/Centers/Center-for-Diversity/Curriculum-Resources/EPAS-Curricular-Guide-on-Diversity-and-Social-Ec (accessed November 20, 2021).
Damianakis, T., L. M. Wagner, S. Bernstein, and E. Marziali. 2007. Volunteers’ experiences visiting the cognitively impaired in nursing homes: A friendly visiting program. Canadian Journal on Aging 26(4):343–356.
Davidson, P. M., and S. L. Szanton. 2020. Nursing homes and COVID-19: We can and should do better. Journal of Clinical Nursing 29(15–16):2758–2759.
Davies, S., and M. Nolan. 2006. “Making it better”: Self-perceived roles of family caregivers of older people living in care homes: A qualitative study. International Journal of Nursing Studies 43(3):281–291.
Dean, A., A. Venkataramani, and S. Kimmel. 2020. Mortality rates from COVID-19 are lower in unionized nursing homes. Health Affairs 39(11):1993–2001.
Dellefield, M. E. 2006. Interdisciplinary care planning and the written care plan in nursing homes: A critical review. The Gerontologist 46(1):128–133.
Dellefield, M., N. Castle, K. McGilton, and K. Spilsbury. 2015. The relationship between registered nurses and nursing home quality: An integrative review (2008–2014). Nursing Economics 33(2):95–108.
Denny-Brown, N., D. Stone, B. Hays, and D. Gallaghe. 2020. COVID-19 intensifies nursing home workforce challenges. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services.
DOJ (U.S. Department of Justice). 2015. Nation’s second-largest nursing home pharmacy to pay $9.25 million to settle kickback allegations. https://www.justice.gov/opa/pr/nations-second-largest-nursing-home-pharmacy-pay-925-million-settle-kickback-allegations (accessed February 8, 2022).
Donald, F., R. Martin-Misener, N. Carter, E. E. Donald, S. Kaasalainen, A. Wickson-Griffiths, M. Lloyd, N. Akhtar-Danesh, and A. DiCenso. 2013. A systematic review of the effectiveness of advanced practice nurses in long-term care. Journal of Advanced Nursing 69(10):2148–2161.
Dorner, B., and E. K. Friedrich. 2018. Position of the Academy of Nutrition and Dietetics: Individualized nutrition approaches for older adults: Long-term care, post-acute care, and other settings. Journal of the Academy of Nutrition and Dietetics 118(4):724–735.
Drake, A. D. R. 2020. Direct care work is real work: Elevating the role of the direct care worker. http://phinational.org/resource/direct-care-work-is-real-work-elevating-the-role-of-the-direct-care-worker (accessed August 20, 2021).
Dunbar, S. 2019. Geriatric care: Oral hygiene challenges in care facilities. https://www.todaysrdh.com/geriatric-care-oral-hygiene-challenges-in-care-facilities (accessed August 16, 2021).
Duncan, M. T., and D. L. Morgan. 1994. Sharing the caring: Family caregivers’ views of their relationships with nursing home staff. The Gerontologist 34(2):235–244.
Eagle, E. 1968. Nursing homes and related facilities. A review of the literature. Public Health Reports 83(8):673–684.
Eaton, S. C. 2000. Beyond “unloving care”: Linking human resource management and patient care quality in nursing homes. International Journal of Human Resource Management 11(3):591–616.
Eaton, S. C., C. Green, R. Wilson, and T. Osypuk. 2001. Extended Care Career Ladder Initiative (ECCLI): Baseline evaluation report of a Massachusetts nursing home initiative. https://www.hks.harvard.edu/publications/extended-care-career-ladder-initiative-eccli-baseline-evaluation-report-massachusetts (accessed August 20, 2021).
Edelman, L. S., E. S. McConnell, S. M. Kennerly, J. Alderden, S. D. Horn, and T. L. Yap. 2020. Mitigating the effects of a pandemic: Facilitating improved nursing home care delivery through technology. JMIR Aging 3(1):e20110–e20110.
Edelman, T. 2020. CMS will not track minimally trained aides at nursing facilities. https://medicareadvocacy.org/cms-will-not-track-minimally-trained-aides-at-nursing-facilities (accessed February 9, 2022).
Ejaz, F., and L. Noelker. 2006. Tailored and ongoing training improve job retention. https://phinational.org/wp-content/uploads/legacy/clearing-house/EjazSummaryFinal.pdf (accessed April 5, 2021).
Falkowski, P. P. 2013. Volunteer programming impact on long-term care facilities. Ph.D. dissertation. The Graduate College at the University of Nebraska, Lincoln, Nebraska.
Fernandez, M. 2021. America’s nursing homes fight to find enough caregivers. https://www.axios.com/americas-nursing-homes-fight-to-find-enough-caregivers-293e5f15-3ff6-462c-b9dd-e09602fdbd94.html (accessed November 21, 2021).
Ferrell, B. R., G. Handzo, T. Picchi, C. Puchalski, and W. E. Rosa. 2020. The urgency of spiritual care: COVID-19 and the critical need for whole-person palliation. Journal of Pain and Symptom Management 60(3):e7–e11.
Feuerberg, M. 2001. Report to Congress: Appropriateness of minimum nurse staffing ratios in nursing homes: Phase II final report. Washington, DC: Centers for Medicare & Medicaid Services (CMS).
Figueroa, J. F., R. K. Wadhera, I. Papanicolas, K. Riley, J. Zheng, E. J. Orav, and A. K. Jha. 2020. Association of nursing home ratings on health inspections, quality of care, and nurse staffing with COVID-19 cases. JAMA 324(11):1103–1105.
Flesner, M., A. Lueckenotte, A. Vogelsmeier, L. Popejoy, K. Canada, D. Minner, C. Galambos, and M. J. Rantz. 2019. Advanced practice registered nurses’ quality improvement efforts to reduce antipsychotic use in nursing homes. Journal of Nursing Care Quality 34(1):4–8.
Galambos, C., L. Rollin, M. Bern-Klug, M. Oie, and E. Engelbart. 2021. Social services involvement in care transitions and admissions in nursing homes. Journal of Gerontological Social Work 64(7):740–757.
Gandhi, A., H. Yu, and D. C. Grabowski. 2021. High nursing staff turnover in nursing homes offers important quality information. Health Affairs 40(3):384–391.
GAO (U.S. Government Accountability Office). GAO. 2011. Nursing homes: Private investment homes sometimes differed from others in deficiencies, staffing, and financial performance. Washington, DC: U.S. Government Accountability Office.
GAO. 2021. Additional reporting on key staffing information and stronger payment incentives needed for skilled nursing facilities. Washington, DC: U.S. Government Accountability Office.
Gaugler, J. E. 2005. Family involvement in residential long-term care: A synthesis and critical review. Aging & Mental Health 9(2):105–118.
Geletta, S., and R. J. Sparks. 2013. Administrator turnover and quality of care in nursing homes. Annals of Long-Term Care: Clinical Care and Aging 21(4):27–30.
Geng, F., D. G. Stevenson, and D. C. Grabowski. 2019. Daily nursing home staffing levels highly variable, often below CMS expectations. Health Affairs 38(7):1095–1100.
Gharpure, R., A. Patel, and R. Link-Gelles. 2021. First-dose COVID-19 vaccination coverage among skilled nursing facility residents and staff. JAMA 325(16):1670–1671.
Gilbert, A. S., S. M. Garratt, L. Kosowicz, J. Ostaszkiewicz, and B. Dow. 2021. Aged care residents’ perspectives on quality of care in care homes: A systematic review of qualitative evidence. Research on Aging 43(7–8):294–310.
Givens, J. L., R. P. Lopez, K. M. Mazor, and S. L. Mitchell. 2012. Sources of stress for family members of nursing home residents with advanced dementia. Alzheimer Disease and Associated Disorders 26(3):254–259.
Goodwin, J. S., P. Agrawal, S. Li, M. Raji, and Y. Kuo. 2021. Growth of physicians and nurse practitioners practicing full time in nursing homes. Journal of the American Medical Directors Association 22(12):2534–2539.
Gorges, R. J., and R. T. Konetzka. 2020. Staffing levels and COVID-19 cases and outbreaks in U.S. nursing homes. Journal of the American Geriatrics Society 68(11):2462–2466.
Grabowski, D. C., and R. A. Hirth. 2003. Competitive spillovers across non-profit and for-profit nursing homes. Journal of Health Economics 22(1):1–22.
Graneheim, U. H., A. Johansson, and B. M. Lindgren. 2014. Family caregivers’ experiences of relinquishing the care of a person with dementia to a nursing home: Insights from a meta-ethnographic study. Scandinavian Journal of Caring Sciences 28(2):215–224.
Gray-Miceli, D., L. D. Wilson, J. Stanley, R. Watman, A. Shire, S. Sofaer, and M. Mezey. 2014. Improving the quality of geriatric nursing care: Enduring outcomes from the Geriatric Nursing Education Consortium. Journal of Professional Nursing 30(6):447–455.
Gupta, S., J. P. Epane, N. Patidar, and R. Weech-Maldonado. 2014. Employing nurse practitioners and physician assistants in nursing homes: Role of market factors. International Journal of Health Sciences 2(3):11–25.
Hale, J., and T. Hale. 2019. Nursing homes turn to temporary employees to fill critical vacancies. https://www.desmoinesregister.com/story/opinion/columnists/2019/10/15/nursinghomes-turn-temporary-employees-fill-critical-vacancies/3987380002 (accessed May 14, 2021).
Han, K., A. M. Trinkoff, C. L. Storr, N. Lerner, M. Johantgen, and K. Gartrell. 2014. Associations between state regulations, training length, perceived quality and job satisfaction among certified nursing assistants: Cross-sectional secondary data analysis. International Journal of Nursing Studies 51(8):1135–1141.
Harrington, C. 2000. Nursing home staffing and its relationship to deficiencies. Journals of Gerontology: Series B 55(5):S278–S287.
Harrington, C. 2010. Nursing home staffing standards in state statutes and regulations. https://theconsumervoice.org/uploads/files/issues/Harrington-state-staffing-table-2010.pdf (accessed August 20, 2021).
Harrington, C., S. Woolhandler, J. Mullan, H. Carrillo, and D. U. Himmelstein. 2001. Does investor ownership of nursing homes compromise the quality of care? American Journal of Public Health 91(9):1452–1455.
Harrington, C., T. Tsoukalas, C. Rudder, R. J. Mollot, and H. Carrillo. 2008. Variation in the use of federal and state civil money penalties for nursing homes. The Gerontologist 48(5):679–691.
Harrington, C., B. Olney, H. Carrillo, and T. Kang. 2012. Nurse staffing and deficiencies in the largest for-profit nursing home chains and chains owned by private equity companies. Health Services Research 47(1 Pt 1):106–128.
Harrington, C., J. F. Schnelle, M. McGregor, and S. F. Simmons. 2016. The need for higher minimum staffing standards in U.S. nursing homes. Health Services Insights 9:13–19.
Harrington, C., M. E. Dellefield, E. Halifax, M. L. Fleming, and D. Bakerjian. 2020. Appropriate nurse staffing levels for U.S. nursing homes. Health Services Insights 13:1178632920934785.
Harrington, C., S. Chapman, E. Halifax, M. Dellefield, and A. Montgomery. 2021. Time to ensure sufficient nursing home staffing and eliminate inequities in care. Journal of Gerontology and Geriatric Medicine 7:099.
Harris-Kojetin, L., D. Lipson, J. Fielding, K. Kiefer, and R. Stone. 2004. Recent findings on frontline long-term care workers: A research synthesis 1999–2003. Washington, DC: Institute for the Future of Aging Services.
Harris-Kojetin, L., M. Sengupta, J. P. Lendon, V. Rome, R. Valverde, and C. Caffrey. 2019. Long-term care providers and services users in the United States, 2015–2016. https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf (accessed April 2, 2021).
Harvath, T. A., K. Swafford, K. Smith, L. L. Miller, M. Volpin, K. Sexson, D. White, and H. A. Young. 2008. Enhancing nursing leadership in long-term care. A review of the literature. Research in Gerontological Nursing 1(3):187–196.
Hauslohner, A., and M. Sacchetti. 2020. Nursing homes turn to quick fix training to meet pandemic staffing needs. https://www.washingtonpost.com/national/nursing-homes-turn-to-quick-fix-training-to-meet-pandemic-staffing-needs/2020/05/28/418c3802-a020-11ea-9590-1858a893bd59_story.html (accessed January 21, 2022).
Henkusens, C., H. H. Keller, S. Dupuis, and L. Schindel Martin. 2014. Transitions to longterm care: How do families living with dementia experience mealtimes after relocating? Journal of Applied Gerontology 33(5):541–563.
Hernández-Medina, E., S. Eaton, D. Hurd, and A. White. 2006. Training programs for certified nursing assistants. https://www.aarp.org/home-garden/livable-communities/info-2006/2006_08_cna.html (accessed August 20, 2021).
HHCS (Hospital & Healthcare Compensation Service). 2020. 2020–2021 nursing home salary & benefits report. Oakland, NJ: Hospital & Healthcare Compensation Service and John R. Zabka Associates.
Hill, J. 2017. Consider nursing home optometry as practice option. https://www.optometrytimes.com/view/consider-nursing-home-optometry-practice-option (accessed November 21, 2021).
Hillmer, M. P., W. P. Wodchis, S. S. Gill, G. M. Anderson, and P. A. Rochon. 2005. Nursing home profit status and quality of care: Is there any evidence of an association? Medical Care Research and Review 62(2):139–166.
Himmerick, K. A., J. Miller, C. Toretsky, M. Jura, and J. Spetz. 2017. Employer demand for physician assistants and nurse practitioners to care for older people and people with disabilities. https://healthworkforce.ucsf.edu/sites/healthworkforce.ucsf.edu/files/REPORT_2017_PA_NP_Demand_in_LTC_Report_FINAL.pdf (accessed November 30, 2021).
Hoek, L. J., J. C. van Haastregt, E. de Vries, R. Backhaus, J. P. Hamers, and H. Verbeek. 2021. Partnerships in nursing homes: How do family caregivers of residents with dementia perceive collaboration with staff? Dementia 20(5):1631–1648.
Hoel, R. W., R. M. Giddings Connolly, and P. Y. Takahashi. 2021. Polypharmacy management in older patients. Mayo Clinic Proceedings 96(1):242–256.
Holle, C. L., L. J. Sundean, M. E. Dellefield, J. Wong, and R. P. Lopez. 2019. Examining the beliefs of skilled nursing facility directors of nursing regarding BSN completion and the impact of nurse leader education on patient outcomes. Journal of Nursing Administration 49(2):57–60.
Horn, S. D., P. Buerhaus, N. Bergstrom, and R. J. Smout. 2005. RN staffing time and outcomes of long-stay nursing home residents: Pressure ulcers and other adverse outcomes are less likely as RNs spend more time on direct patient care. American Journal of Nursing 105(11):58–70; quiz 71.
HRSA (Health Resources and Services Administration). 2019. Brief summary results from the 2018 National Sample Survey of Registered Nurses. Rockville, MD: U.S. Department of Health and Human Services Health Resources and Services Administration National Center for Health Workforce Analysis.
Hyer, K., K. S. Thomas, L. G. Branch, J. S. Harman, C. E. Johnson, and R. Weech-Maldonado. 2011. The influence of nurse staffing levels on quality of care in nursing homes. The Gerontologist 51(5):610–616.
Intrator, O., Z. Feng, V. Mor, D. Gifford, M. Bourbonniere, and J. Zinn. 2005. The employment of nurse practitioners and physician assistants in U.S. nursing homes. The Gerontologist 45(4):486–495.
Intrator, O., E. A. Miller, E. Gadbois, J. K. Acquah, R. Makineni, and D. Tyler. 2015. Trends in nurse practitioner and physician assistant practice in nursing homes, 2000–2010. Health Services Research 50(6):1772–1786.
IOM (Institute of Medicine). 1986. Improving the quality of care in nursing homes. Washington, DC: National Academy Press.
IOM. 1996. Nursing staff in hospitals and nursing homes: Is it adequate? Washington, DC: National Academy Press.
IOM. 2000. The role of nutrition in maintaining health in the nation’s elderly: Evaluating coverage of nutrition services for the Medicare population. Washington, DC: National Academy Press.
IOM. 2001a. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
IOM. 2001b. Improving the quality of long-term care. Washington, DC: National Academy Press.
IOM. 2003. Health professions education: A bridge to quality. Washington, DC: The National Academies Press.
IOM. 2004. Keeping patients safe: Transforming the work environment of nurses. Washington, DC: The National Academies Press.
IOM. 2008. Retooling for an aging America: Building the health care workforce. Washington, DC: The National Academies Press.
IOM. 2011. Improving access to oral health care for vulnerable and underserved populations. Washington, DC: The National Academies Press.
Jette, D. U., R. L. Warren, and C. Wirtalla. 2005. The relation between therapy intensity and outcomes of rehabilitation in skilled nursing facilities. Archives of Physical Medicine and Rehabilitation 86(3):373–379.
Jung, H., Y. Qian, P. R. Katz, and L. P. Casalino. 2021. The characteristics of physicians who primarily practice in nursing homes. Journal of the American Medical Directors Association 22:468–473.
Kane, R. S. 1993. Factors affecting physician participation in nursing home care. Journal of the American Geriatrics Society 41(9):1000–1003.
Katz, P. R., K. Ryskina, D. Saliba, A. Costa, H. Y. Jung, L. M. Wagner, M. A. Unruh, B. J. Smith, A. Moser, J. Spetz, S. Feldman, and J. Karuza. 2021. Medical care delivery in U.S. nursing homes: Current and future practice. The Gerontologist 61(4):595–604.
Katz, R. 2019. Workforce shortages: Bold solutions from LeadingAge. https://leadingage.org/workforce/workforce-shortaLes-bold-solutions-leadingage (accessed August 13, 2021).
Kellett, U. 2007. Seizing possibilities for positive family caregiving in nursing homes. Journal of Clinical Nursing 16(8):1479–1487.
Kemper, P., B. Heier, T. Barry, D. Brannon, J. Angelelli, J. Vasey, and M. Anderson-Knott. 2008. What do direct care workers say would improve their jobs? Differences across settings. The Gerontologist 48(Suppl 1):17–25.
Kim, H., C. Kovner, C. Harrington, W. Greene, and M. Mezey. 2009. A panel data analysis of the relationships of nursing home staffing levels and standards to regulatory deficiencies. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 64(2):269–278.
Kimmey, L. D., and S. C. Stearns. 2015. Improving nursing home resident outcomes: Time to focus on more than staffing? Journal of Nursing Home Research 1:89–95.
Kirkham, C., and B. Lesser. 2020. Special report: Pandemic exposes systemic staffing problems at U.S. nursing homes. https://www.reuters.com/article/us-health-coronavirus-nursing-homes-speci/special-report-pandemic-exposes-systemic-staffing-problems-at-u-s-nursing-homes-idUSKBN23H1L9 (accessed November 19, 2021).
Koenig, H. G. 2012. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012:278730.
Kolanowski, A., T. Coretes, C. Mueller, B. Bowers, M. Boltz, D. Bakerjian, C. Harrington, L. Popejoy, A. Vogelsmeier, M. Wallhage, D. Fick, M. Batchelor, M. Harris, R. Palan-Lopez, M. Dellefield, A. Mayo, D. Woods, A. Horgas, P. Cacchione, D. Carter, P. Tabloski, and L. Gerdner. 2021. A call to the CMS: Mandate adequate professional nurse staffing in nursing homes. American Journal of Nursing 121(3):24–27.
Konetzka, R. T., E. M. White, A. Pralea, D. C. Grabowski, and V. Mor. 2021. A systematic review of long-term care facility characteristics associated with COVID-19 outcomes. Journal of the American Geriatrics Society 69(10):2766–2777.
Kusmaul, N. 2016. The content of education for direct caregivers. Educational Gerontology 42(1):19–24.
Kusmaul, N., M. Bern-Klug, and R. Bonifas. 2017. Ethical issues in long-term care: A human rights perspective. Journal of Human Rights and Social Work 2:86–97.
Kusmaul, N., M. Bern-Klug, J. Heston-Mullins, A. R. Roberts, and C. Galambos. 2020. Nursing home social work during COVID-19. Journal of Gerontological Social Work 63(6–7):651–653.
Kusmaul, N., S. Beltran, T. Buckley, A. Gibson, and M. Bern-Klug. 2021. Structural characteristics of nursing homes and social service directors that influence their engagement in disaster preparedness processes. Journal of Gerontological Social Work 64(7):775–790.
Lapane, K. L., and C. M. Hughes. 2006. Pharmacotherapy interventions undertaken by pharmacists in the Fleetwood phase III study: The role of process control. Annals of Pharmacotherapy 40(9):1522–1526.
LeadingAge Minnesota. 2021. 2020–21 nursing leadership certificate program. https://www.leadingagemn.org/assets/docs/2020-21_NursingLeadershipCertProgram_Brochure_withLO_1.pdf (accessed January 30, 2021).
Lee, C., A. Podury, J. Kaduthodil, and L. Graham. 2020. Long-term care facilities must prioritize immigrant workers’ needs to contain COVID-19. https://www.healthaffairs.org/do/10.1377/hblog20200914.520181/full (accessed November 19, 2021).
Lee, E. E., C. A. Thomas, and T. Vu. 2001. Mobile and portable dentistry: Alternative treatment services for the elderly. Special Care in Dentistry 21(4):153–155.
Lee, S. W. H., V. S. L. Mak, and Y. W. Tang. 2019. Pharmacist services in nursing homes: A systematic review and meta-analysis. British Journal of Clinical Pharmacology 85(12):2668–2688.
Leedahl, S. N., R. K. Chapin, and T. D. Little. 2015. Multilevel examination of facility characteristics, social integration, and health for older adults living in nursing homes. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 70(1):111–122.
Lerner, N. B. 2013. The relationship between nursing staff levels, skill mix, and deficiencies in Maryland nursing homes. Health Care Manager 32(2):123–128.
Lerner, N. B., B. Resnick, E. Galik, and K. G. Russ. 2010. Advanced nursing assistant education program. Journal of Continuing Education in Nursing 41(8):356–362.
Lerner, N. B., A. Trinkoff, C. L. Storr, M. Johantgen, K. Han, and K. Gartrell. 2014. Nursing home leadership tenure and resident care outcomes. Journal of Nursing Regulation 5(3):48–52.
Levy, C., S.-I. T. Palat, and A. M. Kramer. 2007. Physician practice patterns in nursing homes. Journal of the American Medical Directors Association 8(9):558–567.
Lewis, T. 2021. Nursing home workers had one of the deadliest jobs of 2020. https://www.scientificamerican.com/article/nursing-home-workers-had-one-of-the-deadliest-jobs-of-2020 (accessed February 18, 2021).
Li, Y. 2010. Provision of mental health services in U.S. nursing homes, 1995–2004. Psychiatric Services 61(4):349–355.
Li, Y., H. Temkin-Greener, G. Shan, and X. Cai. 2020. COVID-19 infections and deaths among Connecticut nursing home residents: Facility correlates. Journal of the American Geriatrics Society 68(9):1899–1906.
Lipsitz, L. A., A. M. Lujan, A. Dufour, G. Abrahams, H. Magliozzi, L. Herndon, and M. Dar. 2020. Stemming the tide of COVID-19 infections in Massachusetts nursing homes. Journal of the American Geriatrics Society 68(11):2447–2453.
Liu, J., and M. Bern-Klug. 2013. Nursing home social services directors who report thriving at work. Journal of Gerontological Social Work 56:127–145.
Liu, L., A. Guarino, and R. Palan-Lopez. 2011. Family satisfaction with care provided by nurse practitioners to nursing home residents with dementia at the end of life. Clinical Nursing Research 21:350–367.
Livingstone, I., J. Hefele, P. Nadash, D. Barch, and N. Leland. 2019. The relationship between quality of care, physical therapy, and occupational therapy staffing levels in nursing homes in 4 years’ follow-up. Journal of the American Medical Directors Association 20(4):462–469.
Livingstone, I., J. Hefele, and N. Leland. 2021. Characteristics of nursing home providers with distinct patterns of physical and occupational therapy staffing. Journal of Applied Gerontology 40(4):443–451.
Lodge, M. P. 1985. Professional education and practice of nurse administrators/directors of nursing in long-term care: Executive summary. Kansas City, MO: American Nurses’ Foundation, Inc.
Lopez, R. P., K. M. Mazor, S. L. Mitchell, and J. L. Givens. 2013. What is family-centered care for nursing home residents with advanced dementia? American Journal of Alzheimer’s Disease & Other Dementias 28(8):763–768.
LTCCC (Long Term Care Community Coalition). 2022. Nursing home staffing Q2 2021. https://nursinghome411.org/data/staffing/staffing-q2-2021 (accessed February 16, 2022).
Lundin, A., P. H. Bülow, and J. Stier. 2021. Assistant nurses’ positioned accounts for prioritizations in residential care for older people. The Gerontologist 61(4):573–581.
Lyons, S. S., J. P. Specht, S. E. Karlman, and M. L. Maas. 2008. Everyday excellence. A framework for professional nursing practice in long-term care. Research in Gerontological Nursing 1(3):217–228.
Maas, M. L., D. Reed, M. Park, J. P. Specht, D. Schutte, L. S. Kelley, E. A. Swanson, T. TripReimer, and K. C. Buckwalte. 2004. Outcomes of family involvement in care intervention for caregivers of individuals with dementia. Nursing Research 53(2):76–86.
Manchha, A. V., N. Walker, K. A. Way, D. Dawson, K. Tann, and M. Thai. 2021. Deeply discrediting: A systematic review examining the conceptualizations and consequences of the stigma of working in aged care. The Gerontologist 61(4):e129–e146.
Maramaldi, P., T. Cadet, S. L. Burke, M. LeCloux, E. White, E. Kalenderian, and T. Kinnunen. 2018. Oral health and cancer screening in long-term care nursing facilities: Motivation and opportunity as intervention targets. Gerodontology 35(4):407–416.
Mays, A. M., D. Saliba, S. Feldman, M. Smalbrugge, C. M. P. M. Hertogh, T. L. Booker, K. A. Fulbright, S. A. Hendriks, and P. R. Katz. 2018. Quality indicators of primary care provider engagement in nursing home care. Journal of the American Medical Directors Association 19(10):824–832.
McCrystal, T., M. Burghardt, and S. Ferranti. 2010. Buyer beware: OIG shines a spotlight on provider relationships with long term care pharmacies and scrutinizes contract pricing structures. https://www.ropesgray.com/-/media/Files/in-the-news/2010/07/impact-of-omnicare-settlement-for-pharmacy-providers-and-long-term-care-facilities.pdf (accessed January 18, 2022).
McGarry, B. E., D. C. Grabowski, and M. L. Barnett. 2020. Severe staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic. Health Affairs 39(10):1812–1821.
McGarry, B. E., E. M. White, L. J. Resnik, M. Rahman, and D. C. Grabowski. 2021a. Medicare’s new patient driven payment model resulted in reductions in therapy staffing in skilled nursing facilities. Health Affairs 40(3):392–399.
McGarry, B. E., A. D. C. Grabowski, and M. L. Barnett. 2021b. Larger nursing home staff size linked to higher number of COVID-19 cases in 2020. Health Affairs 40(8):1261–1269.
McGarry, B. E., K. Shen, M. L. Barnett, D. C. Grabowski, and A. D. Gandhi. 2021c. Association of nursing home characteristics with staff and resident COVID-19 vaccination coverage. JAMA Internal Medicine 181(12):1670–1672.
McGilton, K. S., L. McGillis-Hall, D. Pringle, L. O’Brien-Pallas, and J. Krejci. 2004. Identifying and testing factors that influence supervisors’ abilities to develop supportive relationships with their staff. https://www.hhr-rhs.ca/index.php?option=com_mtree&task=viewlink&link_id=5287&Itemid=109&lang=en (accessed November 19, 2021).
McGilton, K. S., A. Krassikova, V. Boscart, S. Sidani, A. Iaboni, S. Vellani, and A. Escrig-Pinol. 2021. Nurse practitioners rising to the challenge during the coronavirus disease 2019 pandemic in long-term care homes. The Gerontologist 61(4):615–623.
McKay, M. H., N. D. Pickens, A. Medley, D. Cooper, and C. L. Evetts. 2021. Comparing occupational adaptation-based and traditional training programs for dementia care teams: An embedded mixed-methods study. The Gerontologist 61(4):582–594.
McKinney, S. H., K. Corazzini, R. A. Anderson, R. Sloane, and N. G. Castle. 2016. Nursing home director of nursing leadership style and director of nursing-sensitive survey deficiencies. Health Care Management Review 41(3):224–232.
McKnight, W. 2016. Chaplains play important part in integrated palliative care. Caring for the Ages 17(8):6.
McMullen, T. L., B. Resnick, J. Chin-Hansen, J. M. Geiger-Brown, N. Miller, and R. Rubenstein. 2015. Certified nurse aide scope of practice: State-by-state differences in allowable delegated activities. Journal of the American Medical Directors Association 16(1):20–24.
Medical Direction and Medical Care Work Group. 2011. Role of the medical director in the nursing home. https://www.health.ny.gov/professionals/nursing_home_administrator/docs/11-13_med_dir_role.pdf (accessed August 20, 2021).
MedPAC (Medicare Payment Advisory Commission). 2016. Report to the Congress: Medicare payment policy. Washington, DC: Medicare Payment Advisory Commission.
Mickus, M., C. C. Luz, and A. Hogan. 2004. Voices from the front: Recruitment and retention of direct care workers in long term care across Michigan. https://phinational.org/wp-content/uploads/legacy/clearinghouse/MI_vocices_from_the_front.pdf (accessed August 20, 2021).
Mileski, M., U. Pannu, B. Payne, E. Sterling, and R. McClay. 2020. The impact of nurse practitioners on hospitalizations and discharges from long-term nursing facilities: A systematic review. Healthcare 8(2):114.
Miller, V. J., T. Hamler, S. J. Beltran, and J. Burns. 2021. Nursing home social services: A systematic review of the literature from 2010 to 2020. Social Work in Health Care 60(4):387–409.
Min, A., and H. C. Hong. 2019. Effect of nurse staffing on rehospitalizations and emergency department visits among short-stay nursing home residents: A cross-sectional study using the U.S. Nursing Home Compare database. Geriatric Nursing 40(2):160–165.
MITRE (The MITRE Corporation). 2020. Coronavirus Commission for Safety and Quality in Nursing Homes: Commission final report. https://sites.mitre.org/nhCOVIDcomm/wp-content/uploads/sites/14/2020/09/FINAL-REPORT-of-NH-Commission-Public-Release-Case-20-2378.pdf (accessed August 20, 2021).
Morley, J. E., and A. M. Sanford. 2014. The God card: Spirituality in the nursing home. Journal of the American Medical Directors Association 15(8):533–535.
Morilla-Herrera, J. C., S. Garcia-Mayor, F. J. Martín-Santos, S. Kaknani Uttumchandani, Á. Leon Campos, J. Caro Bautista, and J. M. Morales-Asencio. 2016. A systematic review of the effectiveness and roles of advanced practice nursing in older people. International Journal of Nursing Studies 53:290–307.
Morris, L. 2009. Quits and job changes among home care workers in Maine: The role of wages, hours, and benefits. The Gerontologist 49(5):635–650.
Mukamel, D. B., S. Cai, and H. Temkin-Greener. 2009. Cost implications of organizing nursing home workforce in teams. Health Services Research 44(4):1309–1325.
Mueller, C., G. Arling, R. Kane, J. Bershadsky, D. Holland, and A. Joy. 2006. Nursing home staffing standards: Their relationship to nurse staffing levels. The Gerontologist 46(1):74–80.
Mueller, C., R. A. Anderson, E. S. McConnell, and K. Corazzini. 2012. Licensed nurse responsibilities in nursing homes: A scope-of-practice issue. Journal of Nursing Regulation 3(1):13–20.
Mueller, C., Y. Duan, A. Vogelsmeier, R. Anderson, E. McConnell, and K. Corazzini. 2018. Interchangeability of licensed nurses in nursing homes: Perspectives of directors of nursing. Nursing Outlook 66(6):560–569.
Murray, T. 2021. Nursing home safety during Covid: Staff shortages. https://uspirg.org/sites/pirg/files/reports/StaffShortages/WEB_USP_Nursing-Home-Safety-During-COVID_StaffShortages.pdf (accessed September 24, 2021).
Myers, D. R., R. Rogers, H. H. LeCrone, K. Kelley, and J. H. Scott. 2018. Work life stress and career resilience of licensed nursing facility administrators. Journal of Applied Gerontology 37(4):435–463.
NAB (National Association of Long-Term Care Administrator Boards). 2017. NHA/RCAL/HCBS domains of practice. https://www.nabweb.org/filebin/pdf/Reference_Documents/NAB_NHA_RCAL_HCBS_Domains_of_Practice_effective_07.05.2017.pdf (accessed March 31, 2021).
NAB. 2021. State licensure requirements. https://www.nabweb.org/state-licensure-requirements (accessed April 23, 2021).
Nancarrow, S. A., A. Booth, S. Ariss, T. Smith, P. Enderby, and A. Roots. 2013. Ten principles of good interdisciplinary team work. Human Resources for Health 11(1):19.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. Families caring for an aging America. Edited by R. Schulz and J. Eden. Washington, DC: The National Academies Press.
NASW (National Association of Social Workers). 2003. NASW standards for social work services in long-term care facilities. https://www.socialworkers.org/LinkClick.aspx?fileticket=cwW7lzBfYxg%3d&portalid=0 (accessed November 20, 2021).
NASW. 2016. NASW standards for social work practice in health care settings. https://www.socialworkers.org/LinkClick.aspx?fileticket=fFnsRHX-4HE%3D&portalid=0 (accessed November 20, 2021).
Nazir, A., K. Unroe, M. Tegeler, B. Khan, J. Azar, and M. Boustani. 2013. Systematic review of interdisciplinary interventions in nursing homes. Journal of the American Medical Directors Association 14(7):471–478.
NCSBN (National Council of State Boards of Nursing). 2017. National nursing workforce study. https://www.ncsbn.org/workforce.htm (accessed August 20, 2021).
NHLC (Nursing Home Law Center). 2021. Podiatry care in nursing homes? A necessity for many patients with foot injuries and complications. https://www.nursinghomelawcenter.org/news/nursing-home-abuse/podiatry-care-in-nursing-homes-a-necessity-for-many-patients-with-foot-injuries-complications (accessed November 21, 2021).
NICE (National Institute of CNA Excellence). 2021. About NICE! https://www.nicecna.org/about-nice (accessed November 20, 2021).
OIG (Office of the Inspector General). 2021. CMS use of data on nursing home staffing: Progress and opportunities to do more. Washington, DC: Department of Health and Human Services Office of the Inspector General.
Oliver, D. P., A. J. Rolbiecki, K. Washington, R. L. Kruse, L. Popejoy, J. B. Smith, and G. Demiris. 2021. A pilot study of an intervention to increase family member involvement in nursing home care plan meetings. Journal of Applied Gerontology 40(9): 1080–1086.
Olson, D., and M. Zwygart-Stauffacher. 2008. The organizational quality frontier and essential role of the director of nursing. Journal of Nursing Care Quality 23(1):11–13.
Orth, J., Y. Li, A. Simning, and H. Temkin-Greener. 2019. Providing behavioral health services in nursing homes is difficult: Findings from a national survey. Journal of the American Geriatrics Society 67(8):1713–1717.
Paek, S. C., N. J. Zhang, T. T. H. Wan, L. Y. Unruh, and N. Meemon. 2016. The impact of state nursing home staffing standards on nurse staffing levels. Medical Care Research and Review 73(1):41–61.
Patterson Norrie, T., A. R. Villarosa, A. C. Kong, S. Clark, S. Macdonald, R. Srinivas, J. Anlezark, and A. George. 2019. Oral health in residential aged care: Perceptions of nurses and management staff. Nursing Open 7(2):536–546.
Peck, L. 2021. Executive survey insights: Wave 31: July 12 to August 8, 2021. https://blog.nic.org/executive-survey-insights-wave-31 (accessed October 15, 2021).
PHI. 2011. Nurse aide training requirements by state. http://phinational.org/advocacy/nurse-aide-training-requirements-state-2016 (accessed June 23, 2021).
PHI. 2016. Raise the floor: Quality nursing home care depends on quality jobs. https://phinational.org/wp-content/uploads/legacy/research-report/phi-raisethefloor-201604012.pdf (accessed November 18, 2021).
PHI. 2019. U.S. nursing assistants employed in nursing homes. https://phinational.org/wp-content/uploads/2019/08/US-Nursing-Assistants-2019-PHI.pdf (accessed February 16, 2022).
PHI. 2020. Nursing assistant training requirements by state. http://phinational.org/advocacy/nurse-aide-training-requirements-state-2016 (accessed November 18, 2021).
PHI. 2021. Direct care workers in the United States: Key facts. https://phinational.org/resource/direct-care-workers-in-the-united-states-key-facts-2 (accessed September 10, 2021).
Pillemer, K., J. J. Suitor, C. R. Henderson, Jr., R. Meador, L. Schultz, J. Robison, and C. Hegeman. 2003. A cooperative communication intervention for nursing home staff and family members of residents. The Gerontologist 43(Spec No 2):96–106.
Pogorzelska-Maziarz, M., and E. L. Kalp. 2017. Infection prevention outside of the acute care setting: Results from the MegaSurvey of infection preventionists. American Journal of Infection Control 45(6):597–602.
Popejoy, L., A. Vogelsmeier, C. Galambos, M. Flesner, G. Alexander, A. Lueckenotte, V. Lyons, and M. Rantz. 2017. The APRN role in changing nursing home quality: The Missouri Quality improvement Initiative. Journal of Nursing Care Quality 32(3):196–201.
Popejoy, L. L., A. A. Vogelsmeier, G. L. Alexander, C. M. Galambos, C. A. Crecelius, B. Ge, M. Flesner, K. Canada, and M. Rantz. 2019. Analyzing hospital transfers using INTERACT acute care transfer tools: Lessons from MOQI. Journal of the American Geriatrics Society 67(9):1953–1959.
Popejoy, L., A. Vogelsmeier, W. Boren, N. Martin, S. Kist, K. Canada, S. J. Miller, and M. Rantz. 2020. A coordinated response to the COVID-19 pandemic in Missouri nursing homes. Journal of Nursing Care Quality 35(4):287–292.
Porter, J., A. Ntouva, A. Read, M. Murdoch, D. Ola, and G. Tsakos. 2015. The impact of oral health on the quality of life of nursing home residents. Health and Quality of Life Outcomes 13:102.
Probst, J. C., J. D. Baek, and S. B. Laditka. 2010. The relationship between workplace environment and job satisfaction among nursing assistants: Findings from a national survey. Journal of the American Medical Directors Association 11(4):246–252.
Quinton, S. 2020. Staffing nursing homes was hard before the pandemic. Now it’s even tougher. https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2020/05/18/staffing-nursing-homes-was-hard-before-the-pandemic-now-its-even-tougher (accessed May 26, 2021).
Rantz, M. J., M. Zwygart-Stauffacher, M. Flesner, L. Hicks, D. Mehr, T. Russell, and D. Minner. 2013. The influence of teams to sustain quality improvement in nursing homes that “need improvement.” Journal of the American Medical Directors Association 14(1):48–52.
Rantz, M. J., L. Popejoy, A. Vogelsmeier, C. Galambos, G. Alexander, M. Flesner, C. Crecelius, B. Ge, and G. Petroski. 2017. Successfully reducing hospitalizations of nursing home residents: Results of the Missouri Quality Initiative. Journal of the American Medical Directors Association 18(11):960–966.
Rantz, M. J., L. Popejoy, A. Vogelsmeier, C. Galambos, G. Alexander, M. Flesner, C. Murray, C. Crecelius, B. Ge, and G. Petroski. 2018a. Impact of advanced practice registered nurses on quality measures: The Missouri Quality Initiative experience. Journal of the American Medical Directors Association 19(6):541–550.
Rantz, M. J., L. Popejoy, A. Vogelsmeier, C. Galambos, G. Alexander, M. Flesner, C. Murray, and C. Crecelius. 2018b. Reducing avoidable hospitalizations and improving quality in nursing homes with APRNs and interdisciplinary support. Journal of Nursing Care Quality 33(1):5–9.
Rao, A. D., and L. K. Evans. 2015. The role of directors of nursing in cultivating nurse empowerment. Annals of Long-Term Care 23(4):27–32.
Ray, V. 2019. A theory of racialized organizations. American Sociological Review 84(1):26–53.
Reid, R. C., and N. L. Chappell. 2017. Family involvement in nursing homes: Are family caregivers getting what they want? Journal of Applied Gerontology 36(8):993–1015.
Rizzo, V. M., and J. M. Rowe. 2016. Cost-effectiveness of social work services in aging: An updated systematic review. Research on Social Work Practice 26(6):653–667.
Roberts, A. R., and J. R. Bowblis. 2017. Who hires social workers? Structural and contextual determinants of social service staffing in nursing homes. Health & Social Work 42(1):15–23.
Roberts, A. R., and K. J. Ishler. 2018. Family involvement in the nursing home and perceived resident quality of life. The Gerontologist 58(6):1033–1043.
Roberts, A. R., A. C. Smith, and J. R. Bowblis. 2020. Nursing home social services and postacute care: Does more qualified staff improve behavioral symptoms and reduce antipsychotic drug use? Journal of the American Medical Directors Association 21(3):388–394.
Roberts, T., K. Nolet, and B. Bowers. 2015. Consistent assignment of nursing staff to residents in nursing homes: A critical review of conceptual and methodological issues. The Gerontologist 55(3):434–447.
Romero, L. 2021. Pandemic, labor shortages have left long-term care facilities competing for staff. https://abcnews.go.com/US/pandemic-labor-shortages-left-long-term-care-facilities/story?id=79508224 (accessed November 21, 2021).
Rondeau, K. V., and T. H. Wagar. 2006. Nurse and resident satisfaction in magnet long-term care organizations: Do high involvement approaches matter? Journal of Nursing Management 14(3):244–250.
Rosemond, C., L. C. Hanson, and S. Zimmerman. 2017. Goals of care or goals of trust? How family members perceive goals for dying nursing home residents. Journal of Palliative Medicine 20(4):360–365.
Rosenfeld, P., M. Kobayashi, P. Barber, and M. Mezey. 2004. Utilization of nurse practitioners in long-term care: Findings and implications of a national survey. Journal of the American Medical Directors Association 5:9–15.
Ross, M. M., A. Carswell, and W. B. Dalziel. 2001. Family caregiving in long-term care facilities. Clinical Nursing Research 10(4):347–363; discussion 364–348.
Rowland, F. N., M. Cowles, C. Dickstein, and P. R. Katz. 2009. Impact of medical director certification on nursing home quality of care. Journal of the American Medical Directors Association 10(6):431–435.
RTI International. 2017. Evaluation of the initiative to reduce avoidable hospitalizations among nursing facility residents: Final report. Waltham, MA: RTI International.
Ryosho, N. 2011. Experiences of racism by female minority and immigrant nursing assistants. Affilia: Journal of Women and Social Work 26(1):59–71.
Ryskina, K. L., D. Polsky, and R. M. Werner. 2017. Physicians and advanced practitioners specializing in nursing home care, 2012–2015. JAMA 318(20):2040–2042.
Saunders, R., K. Seaman, R. Graham, and A. Christiansen. 2019. The effect of volunteers’ care and support on the health outcomes of older adults in acute care: A systematic scoping review. Journal of Clinical Nursing 28(23–24):4236–4249.
Scales, K. 2020. Nursing assistants have training standards for a reason. https://phinational.org/nursing-assistants-have-training-standards-for-a-reason (accessed November 19, 2021).
Scales, K. 2021. Temporary nurse aides need job stability and support. https://phinational.org/temporary-nurse-aides-need-job-stability-and-support (accessed May 14, 2021).
Scales, K., A. Altman, S. Campbell, A. Cook, A. Del Rio Drake, R. Espinoza, and J. M. Sturgeon. 2020. It’s time to care: A detailed profile of America’s direct care workforce. http://phinational.org/resource/its-time-to-care-a-detailed-profile-of-americas-direct-care-workforce (accessed August 20, 2021).
Schkade, J. K., and M. McClung. 2001. Occupational adaptation in practice: Concepts and cases. Thorofare, NJ: Slack.
Schnelle, J. F., L. D. Schroyer, A. A. Saraf, and S. F. Simmons. 2016. Determining nurse aide staffing requirements to provide care based on resident workload: A discrete event simulation model. Journal of the American Medical Directors Association 17(11):970–977.
Seavey, D. 2004. The cost of frontline turnover in long-term care. https://www.leadingage.org/sites/default/files/Cost_Frontline_Turnover.pdf (accessed July 7, 2021).
Sedensky, M. 2021. Ghost towns: Nursing home staffing falls amid pandemic. https://apnews.com/article/coronavirus-pandemic-nursing-homes-d1befe76a3a0680b57defb6d9f1cfb66 (accessed February 16, 2022).
Seidman, H. R. 2021. The changing role of chaplains at long-term care facilities. https://www.nextavenue.org/the-changing-role-of-chaplains-during-the-pandemic (accessed August 18, 2021).
Senek, M., S. Robertson, T. Ryan, R. King, E. Wood, and A. Tod. 2020. The association between care left undone and temporary nursing staff ratios in acute settings: A cross-sectional survey of registered nurses. BMC Health Services Research 20(1):637.
Severens, M. 2020. Trump team relaxed training rules for nursing home staff just as pandemic hit. https://www.politico.com/news/2020/07/15/coronavirus-nursing-homes-361510 (accessed January 21, 2022).
Sharma, H., and L. Xu. 2022. Association between wages and nursing staff turnover in Iowa nursing homes. Innovation in Aging. https://doi.org/10.1093/geroni/igac004 (accessed February 14, 2022).
Sherman, R. O., and T. Touhy. 2017. An exploratory descriptive study to evaluate Florida nurse leader challenges and opportunities in nursing homes settings. SAGE Open Nursing 3:1–7.
Siegel, E. O., C. Mueller, K. L. Anderson, and M. E. Dellefield. 2010. The pivotal role of the director of nursing in nursing homes. Nursing Administration Quarterly 34(2): 110–121.
Sifuentes, A. M. F., and K. L. Lapane. 2020. Oral health in nursing homes: What we know and what we need to know. Journal of Nursing Home Research 6:1–5.
Simmons, S. F., and J. F. Schnelle. 2004. Individualized feeding assistance care for nursing home residents: Staffing requirements to implement two interventions. Journals of Gerontology: Series A 59(9):M966–M973.
Simmons, S. F., and J. F. Schnelle. 2006. Feeding assistance needs of long-stay nursing home residents and staff time to provide care. Journal of the American Geriatrics Society 54(6):919–924.
Simmons, S. F., R. Bertrand, V. Shier, R. Sweetland, T. J. Moore, D. T. Hurd, and J. F. Schnelle. 2007. A preliminary evaluation of the paid feeding assistant regulation: Impact on feeding assistance care process quality in nursing homes. The Gerontologist 47(2):184–192.
Simmons, S. F., E. Keeler, X. Zhuo, K. A. Hickey, H.-W. Sato, and J. F. Schnelle. 2008. Prevention of unintentional weight loss in nursing home residents: A controlled trial of feeding assistance. Journal of the American Geriatrics Society 56(8):1466–1473.
Simons, K., M. Bern-Klug, and S. An. 2012. Envisioning quality psychosocial care in nursing homes: The role of social work. Journal of the American Medical Directors Association 13(9):800–805.
Singh, D., and R. Schwab. 2000. Predicting turnover and retention in nursing homes administrators: Management and policy implications. The Gerontologist 40(3):310–319.
Sloane, P. D., R. Yearby, R. T. Konetzka, Y. Li, R. Espinoza, and S. Zimmerman. 2021. Addressing systemic racism in nursing homes: A time for action. Journal of the American Medical Directors Association 22(4):886–892.
Smiley, R. A., C. Ruttinger, C. M. Oliveira, L. R. Hudson, R. Allgeyer, K. A. Reneau, J. H. Silvestre, and M. Alexander. 2021. The 2020 National Nursing Workforce Survey. Journal of Nursing Regulation 12(1):S1–S96.
Spilsbury, K., C. Hewitt, L. Stirk, and C. Bowman. 2011. The relationship between nurse staffing and quality of care in nursing homes: A systematic review. International Journal of Nursing Studies 48(6):732–750.
Spector, W. D., R. Limcangco, C. Williams, W. Rhodes, and D. Hurd. 2013. Potentially avoidable hospitalizations for elderly long-stay residents in nursing homes. Medical Care 51(8)673–681.
Squillace, M. R., R. E. Remsburg, L. D. Harris-Kojetin, A. Bercovitz, E. Rosenoff, and B. Han. 2009. The National Nursing Assistant Survey: Improving the evidence base for policy initiatives to strengthen the certified nursing assistant workforce. The Gerontologist 49(2):185–197.
Stacey, C. L. 2005. Finding dignity in dirty work: The constraints and rewards of low-wage home care labour. Sociology of Health and Illness 27(6):831–854.
Stevenson, D. G., and D. C. Grabowski. 2008. Private equity investment and nursing home care: Is it a big deal? Health Affairs 27(5):1399–1408.
Stone, P. W., C. T. A. Herzig, M. Agarwal, M. Pogorzelska-Maziarz, and A. W. Dick. 2018. Nursing home infection control program characteristics, CMS citations, and implementation of antibiotic stewardship policies: A national study. Inquiry 55:1–7.
Stone, P. W., M. Agarwal, and M. Pogorzelska-Maziarz. 2020. Infection preventionist staffing in nursing homes. American Journal of Infection Control 48(3):330–332.
Stone, R. I., and S. L. Dawson. 2008. The origins of Better Jobs Better Care. The Gerontologist 48(Spec No 1):5–13.
Stone, R. I., S. C. Reinhard, B. Bowers, D. Zimmerman, C. D. Phillips, C. Hawes, J. A. Fielding, and N. Jacobson. 2002. Evaluation of the Wellspring model for improving nursing home quality. New York: Commonwealth Fund.
Streim, J. E., E. W. Beckwith, D. Arapakos, P. Banta, R. Dunn, and T. Hoyer. 2002. Mental health services in nursing homes: Regulatory oversight, payment policy, and quality improvement in mental health care in nursing homes. Psychiatric Services 53(11):1414–1418.
Stulick, A. 2021. Nursing homes use of staffing agencies soars during pandemic as workforce crisis deepens. https://skillednursingnews.com/2021/06/nursing-homes-use-of-staffingagencies-soars-during-pandemic-as-workforce-crisis-deepens/?euid=1f8e8685ef&utm_source=snn-newsletter&utm_medium=email&utm_campaign=fd29b0ab54 (accessed November 21, 2021).
Sullivan, T. 2018. CMS proposed rule: Changes to the conditions of participation for long term care facilities—proposing to ban manufacturer rebates to long term care pharmacies. https://www.policymed.com/2011/10/cms-proposed-rule-changes-to-the-conditions-of-participation-for-long-term-care-facilities-proposing.html (accessed February 8, 2022).
Sussman, T., and S. Dupuis. 2014. Supporting residents moving into long-term care: Multiple layers shape residents’ experiences. Journal of Gerontological Social Work 57(5): 438–459.
Tak, S., M. H. Sweeney, T. Alterman, S. Baron, and G. M. Calvert. 2010. Workplace assaults on nursing assistants in U.S. nursing homes: A multilevel analysis. American Journal of Public Health 100(10):1938–1945.
Tan, R. 2022. Low-wage workers prop up the nursing home industry. They’re quitting in droves. https://www.washingtonpost.com/dc-md-va/2022/01/23/nursing-home-dc-staffing-omicron (accessed February 9, 2022).
Temkin-Greener, H., S. Cai, P. Katz, H. Zhao, and D. B. Mukamel. 2009. Daily practice teams in nursing homes: Evidence from New York State. The Gerontologist 49(1):68–80.
Teno, J. M., P. L. Gozalo, A. N. Trivedi, S. L. Mitchell, J. N. Bunker, and V. Mor. 2017. Temporal trends in the numbers of skilled nursing facility specialists from 2007 through 2014. JAMA Internal Medicine 177(9):1376–1378.
Teno, J. M., A. N. Trivedi, and P. Gozalo. 2018. What exactly is a “SNF-ist?”—Reply. JAMA Internal Medicine 178(1):154.
Tjia, J., C. A. Lemay, A. Bonner, C. Compher, K. Paice, T. Field, K. Mazor, J. N. Hunnicutt, K. L. Lapane, and J. Gurwitz. 2017. Informed family member involvement to improve the quality of dementia care in nursing homes. Journal of the American Geriatrics Society 65(1):59–65.
Tomaskovic-Devey, D. 2018. Labor process inequality and the sex and racial composition of jobs. In D. Tomaskovic-Devey, Gender and racial inequality at work. Ithaca, NY: Cornell University Press.
Trautner, B. W., M. T. Greene, S. L. Krein, H. L. Wald, S. Saint, A. J. Rolle, S. McNamara, B. S. Edson, and L. Mody. 2017. Infection prevention and antimicrobial stewardship knowledge for selected infections among nursing home personnel. Infection Control and Hospital Epidemiology 38(1):83–88.
Travers, J. L., A. M. Teitelman, K. A. Jenkins, and N. G. Castle. 2020. Exploring social-based discrimination among nursing home certified nursing assistants. Nursing Inquiry 27(1):e12315.
Travers, J. L., B. A. Caceres, D. Vlahov, H. Zaidi, J. S. Dill, R. I. Stone, and P. W. Stone. 2021. Federal requirements for nursing homes to include certified nursing assistants in resident care planning and interdisciplinary teams: A policy analysis. Nursing Outlook 69(4):617–625.
Trinkoff, A. M., C. L. Storr, M. Johantgen, N. Lerner, K. Han, and K. McElroy. 2013. State regulatory oversight of certified nursing assistants and resident outcomes. Journal of Nursing Regulation 3(4):53–59.
Trinkoff, A. M., N. B. Lerner, C. L. Storr, K. Han, M. E. Johantgen, and K. Gartrell. 2015. Leadership education, certification and resident outcomes in U.S. nursing homes: Cross-sectional secondary data analysis. International Journal of Nursing Studies 52(1):334–344.
Trinkoff, A. M., C. L. Storr, N. B. Lerner, B. K. Yang, and K. Han. 2017. CNA training requirements and resident care outcomes in nursing homes. The Gerontologist 57(3):501–508.
Truitt, A. R., and C. R. Snyder. 2020. Racialized experiences of Black nursing professionals and certified nursing assistants in long-term care settings. Journal of Transcultural Nursing 31(3):312–318.
Turner, S. A. 2015. Medical director and other physician compensation arrangements under scrutiny. Geriatric Nursing 36(4):314–315.
Tyler, D. A., Z. Feng, N. E. Leland, P. Gozalo, O. Intrator, and V. Mor. 2013. Trends in post-acute care and staffing in U.S. nursing homes, 2001–2010. Journal of the American Medical Directors Association 14(11):817–820.
U.S. Congress (U.S. Congress, Senate, Committee on Health, Education, Labor and Pensions). 2001. Nursing workforce: Recruitment and retention of nurses and nurse aides is a growing concern. 107th Cong., May 17 (statement of William J. Scanlon, director health care issues).
van der Ploeg, E. S., T. Mbakile, S. Genovesi, and D. W. O’Connor. 2012. The potential of volunteers to implement non-pharmacological interventions to reduce agitation associated with dementia in nursing home residents. International Psychogeriatrics 24(11):1790–1797.
van der Ploeg, E. S., H. Walker, and D. W. O’Connor. 2014. The feasibility of volunteers facilitating personalized activities for nursing home residents with dementia and agitation. Geriatric Nursing 35(2):142–146.
van Dyck, L. I., K. M. Wilkins, J. Ouellet, G. M. Ouellet, and M. L. Conroy. 2020. Combating heightened social isolation of nursing home elders: The telephone outreach in the COVID-19 outbreak program. American Journal of Geriatric Psychiatry 28(9):989–992.
Van Houtven, C., K. Miller, R. Gorges, H. Campbell, W. Dawson, J. McHugh, B. McGarry, R. Gilmartin, N. Boucher, B. Kaufman, L. Chisholm, S. Beltran, S. Fashaw, X. Wang, O. Reneau, A. Chun, J. Jacobs, K. Abrahamson, K. Unroe, C. Bishop, G. Arling, S. Kelly, R. M. Werner, R. T. Konetzka, and E. C. Norton. 2021. State policy responses to COVID-19 in nursing homes. Journal of Long-Term Care 264–282.
Varney, S. 2021. Nursing homes bleed staff as Amazon lures low-wage workers with prime packages. https://khn.org/news/article/nursing-homes-staff-shortages-amazon-lures-low-wage-workers (accessed February 8, 2022).
Veiga-Seijo, R., M. d. C. Miranda-Duro, and S. Veiga-Seijo. 2021. Strategies and actions to enable meaningful family connections in nursing homes during the COVID-19: A scoping review. Clinical Gerontologist 45(1):20–30.
Vogelsmeier, A. A., S. J. Farrah, A. Roam, and L. Ott. 2010. Evaluation of a leadership development academy for RNs in long-term care. Nursing Administration Quarterly 34(2):122–129.
Vogelsmeier, A., L. Popejoy, C. Crecelius, S. Orique, G. Alexander, and M. Rantz. 2018. APRN-conducted medication reviews for long-stay nursing home residents. Journal of the American Medical Directors Association 19(1):83–85.
Vogelsmeier, A., L. Popejoy, K. Canada, C. Galambos, G. Petroski, C. Crecelius, G. Alexander, and M. Rantz. 2020. Results of the Missouri Quality Initiative in sustaining changes in nursing home care: Six-year trends of reducing hospitalizations of nursing home residents. Journal of Nutrition, Health & Aging 25(1):5–12.
Weber, L. 2021. Nursing homes keep losing workers. https://www.wsj.com/articles/nursing-homes-keep-losing-workers-11629898200 (accessed November 21, 2021).
Wells, J. C. 2004. The case for minimum nurse staffing standards in nursing homes: A review of the literature. Alzheimer’s Care Today 5(1):39–51.
Werner, R. M., and N. B. Coe. 2021. Nursing home staffing levels did not change significantly during COVID-19. Health Affairs 40(5):795–801.
Whitaker, T., T. Weismiller, E. Clark, and M. Wilson. 2006. Assuring the sufficiency of a frontline workforce: A national study of licensed social workers. Executive summary. Washington, DC: National Association of Social Workers.
White, E. M., C. M. Kosar, M. Rahman, and V. Mor. 2020a. Trends in hospitals and skilled nursing facilities sharing medical providers, 2008–16. Health Affairs 39(8):1312–1320.
White, E. M., L. H. Aiken, D. M. Sloane, and M. D. McHugh. 2020b. Nursing home work environment, care quality, registered nurse burnout and job dissatisfaction. Geriatric Nursing 41(2):158–164.
White, E. M., T. F. Wetle, A. Reddy, and R. R. Baier. 2021. Front-line nursing home staff experiences during the COVID-19 pandemic. Journal of the American Medical Directors Association 22(1):199–203.
White House. 2021. Fact sheet: President Biden sends immigration bill to Congress as part of his commitment to modernize our immigration system. https://www.whitehouse.gov/briefing-room/statements-releases/2021/01/20/fact-sheet-president-biden-sendsimmigration-bill-to-congress-as-part-of-his-commitment-to-modernize-our-immigration-system (accessed August 13, 2021).
Wiener, J. M., M. R. Squillace, W. L. Anderson, and G. Khatutsky. 2009. Why do they stay? Job tenure among certified nursing assistants in nursing homes. The Gerontologist 49(2):198–210.
Xing, J., D. B. Mukamel, and H. Temkin-Greener. 2013. Hospitalizations of nursing home residents in the last year of life: Nursing home characteristics and variation in potentially avoidable hospitalizations. Journal of the American Geriatrics Society 61(11):1900–1908.
Xu, H., O. Intrator, and J. R. Bowblis. 2020. Shortages of staff in nursing homes during the COVID-19 pandemic: What are the driving factors? Journal of the American Medical Directors Association 21(10):1371–1377.
Yang, B. K., M. W. Carter, A. M. Trinkoff, and H. W. Nelson. 2021a. Nurse staffing and skill mix patterns in relation to resident care outcomes in U.S. nursing homes. Journal of the American Medical Directors Association 22(5):1081–1087.e1081.
Yang, B. K., M. Carter, and W. Nelson. 2021b. Trends in COVID-19 cases, related deaths, and staffing shortage in nursing homes by rural and urban status. Geriatric Nursing 42(6):1356–1361.
You, K., Y. Li, O. Intrator, D. Stevenson, R. Hirth, D. Grabowski, and J. Banaszak-Holl. 2016. Do nursing home chain size and proprietary status affect experiences with care? Medical Care 54(3):229–234.
Yurkofsky, M., and J. G. Ouslander. 2021. Medical care in skilled nursing facilities (SNFs) in the United States. https://www.uptodate.com/contents/medical-care-in-skilled-nursing-facilities-snfs-in-the-united-states (accessed July 16, 2021).
Zallman, L., K. E. Finnegan, D. U. Himmelstein, S. Touw, and S. Woolhandler. 2019. Care for America’s elderly and disabled people relies on immigrant labor. Health Affairs 38(6):919–926.
Zhang, Y., L. Punnett, B. Mawn, and R. Gore. 2016. Working conditions and mental health of nursing staff in nursing homes. Issues in Mental Health Nursing 37(7):485–492.
Zhao, L., H. Xie, and R. Dong. 2015. Volunteers as caregivers for elderly with chronic diseases: An assessment of demand and cause of demand. International Journal of Nursing Sciences 2(3):268–272.
Zheng, N. T., and H. Temkin-Greener. 2010. End-of-life care in nursing homes: The importance of CAN staff communication. Journal of the American Medical Directors Association 11(7):494–499.
Zimmerman, S., B. J. Bowers, L. W. Cohen, D. C. Grabowski, S. D. Horn, P. Kemper, and T. R. Collaborative. 2016. New evidence on the Green House model of nursing home care: Synthesis of findings and implications for policy, practice, and research. Health Services Research 51(Suppl 1):475–496.


















































































