
Quality Assurance: Oversight and Regulation
Regulation is common to a wide range of products and services, such as food, construction, pharmaceuticals, transportation, and electronics. The purpose of regulation is to assure that products and services are safe and meet certain standards for minimum acceptable quality. A standard economic justification for why nursing home care needs regulation is that regulations can help address market failures, such as consumers’ difficulty in accessing, monitoring, and responding to information about the quality of care (GAO, 1997; Grabowski and Stevenson, 2006; IOM, 2001; Shugarman and Brown, 2006). The typically frail health of the nursing home resident population, combined with the relatively high level of government financing for nursing home care in the United States, further bolsters the political and policy justifications for governmental oversight of the sector. In that respect, government regulations are intended to protect consumers and ensure accountability in the use of public funds by developing quality standards, evaluating whether nursing homes meet those standards, and enforcing sanctions when necessary (IOM, 2001). This chapter reviews the history and current state of quality assurance, accomplished largely through oversight and regulation, of the nursing home sector.
HISTORY OF QUALITY ASSURANCE IN NURSING HOMES
The federal government’s formal involvement with the oversight of nursing homes started with the enactment of Medicare and Medicaid in 1965. Over the decades, various laws and federal regulations sought to improve the quality of care in nursing homes and also improve the oversight and regulation of nursing homes’ performance (see Box 8-1).
OMNIBUS BUDGET RECONCILIATION ACT OF 1987
The 1986 Institute of Medicine (IOM) report Improving the Quality of Care in Nursing Homes cited widespread quality-of-care problems and substantial concerns about the ineffectiveness—and unevenness—of oversight at that point in time (IOM, 1986). Specifically, the report stated
The implicit goal of the regulatory system is to ensure that any person requiring nursing home care be able to enter any certified nursing home and receive appropriate care, be treated with courtesy, and enjoy continued civil and legal rights. This happens in many nursing homes in all parts of this country. But in many other government-certified nursing homes, individuals who are admitted receive very inadequate—sometimes shockingly deficient—care that is likely to hasten the deterioration of their physical, mental, and emotional health. (p. 2)
Soon after the release of the 1986 IOM report, Congress enacted the Nursing Home Reform Act as part of the Omnibus Budget Reconciliation Act of 1987 (OBRA 87).1 OBRA 87 regulations raised the expectations for nursing homes considerably by establishing uniform and tougher nationwide standards. The regulations strengthened and consolidated quality standards (including standards related to quality of life and residents’ rights), expanded the types of sanctions that could be imposed, and required data collection using the Minimum Data Set. Overall, the regulations in OBRA 87 established the modern survey and enforcement system, detailing the expectation that facilities be surveyed once every 9 to 15 months at times that were unannounced to the facilities and adding several intermediate sanctions that would be available to aid in enforcement. For family member perspectives on the importance of regulations to the quality of care in nursing homes, see Box 8-2.
Quality Assurance and Nursing Homes in the 21st Century
For more than 30 years, the statutory requirements of OBRA 87 and associated regulations promulgated by the Centers for Medicare & Medicaid Services (CMS) have largely defined nursing home quality assurance activities. To remain eligible for Medicare and Medicaid payments, nursing homes must meet requirements of participation2 covering a range of dimensions such as residents’ rights, quality of care, and the physical environment
___________________
1 Omnibus Budget Reconciliation Act of 1987, Public Law 100-203; 100th Cong., 1st sess. (December 22, 1987).
2 CMS Requirements for Long Term Care Facilities—Quality of Life, 42 CFR Part §483, Subpart B (2016).
(CMS, 2021a; Kapp, 2000). However, while substantial changes have occurred in nursing home care since the implementation of the OBRA 87 regulations, the general structure of the oversight and regulation of nursing homes has, for the most part, remained the same. A notable exception is the incorporation of new regulations as part of the Patient Protection and Affordable Care Act (ACA)3 (see Box 8-1) (Wells and Harrington, 2013). The ACA includes provisions such as requiring facilities to disclose information concerning ownership and governance, directing CMS to collect payroll data on direct care staffing, and establishing the Civil Monetary Penalty Reinvestment Program (KFF, 2013). In 2016, CMS released a final rule updating its requirements of participation.4 The full rule, the first significant revision of federal regulations of nursing homes in over 25 years, was designed to streamline existing nursing home regulations, remove duplication, and align with current legislation. The 2016 rule expanded regulations to facilitate person-centered care, infection control, and quality improvement activities. The 2016 rule also restricted the ability of nursing homes to require that residents enter into pre-dispute arbitration agreements, a
___________________
3 Patient Protection and Affordable Care Act of 2010, Public Law 111-148; 111th Cong., 2nd sess. (March 23, 2010).
4 CMS Requirements for Long Term Care Facilities, 42 CFR § 483 (2016).
provision the nursing home industry challenged almost immediately. As a result, the July 2019 final rule allowed nursing homes to offer residents pre-dispute binding arbitration but not require it.
In accordance with the January 2017 executive order “Reducing Regulation and Controlling Regulatory Costs,” the oversight and enforcement of the requirements of participation were scaled back as part of a broader movement to reduce bureaucracy and government intervention, including the encouragement of regulators to not impose fines for “one-time” events (Musumeci and Chidambaram, 2020; Rau, 2017). The executive order proposed relaxing regulations in other areas, such as emergency preparedness, as well (CMS, 2018a).
Today, challenges are evident in the current quality assurance framework. While great progress has been made since the passage of OBRA 87, substantial quality problems have persisted. With its emphasis on minimum standards for operation, the main purpose of regulation is to identify and deter poor-quality care practices. In 1998, a report to Congress by the Health Care Financing Administration (HCFA) noted that “ongoing press reports of questionable practice reinforce a widespread negative perception of the quality of nursing home care and underscore the importance of the Federal government’s responsibilities” (HCFA, 1998, p. i). However, recent investigative and government reports have documented substantial lapses in nursing home oversight processes across multiple states (see later in this chapter for more on oversight of the state survey process). The following sections will provide an overview of quality assurance roles and responsibilities today.
FEDERAL AND STATE REGULATION
The 1986 IOM report noted three components of government regulation of nursing homes that are important to quality assurance:
- Criteria to determine quality;
- Determining compliance with these criteria; and
- Enforcing compliance with the criteria (IOM, 1986).
Chapter 3 of this report examines quality measurement in nursing homes as a means of determining the quality of care. This section gives a high-level overview of the role that the federal government, state governments, and the private sector play in the oversight of nursing homes by determining their compliance with regulations.
States have the primary responsibility for licensing providers, giving each state some control over nursing home market entry and retention. State licensure imposes minimum standard requirements that a home must meet in order to continue operating. Historically, however, state licensing
decisions have excluded few facilities, as regulators consider the loss or denial of a license to operate to be a drastic remedy that should be reserved for only serious breaches of resident safety and quality-of-care standards (Li et al., 2010). States could potentially take a more active role in screening applications to assess the quality of performance at facilities owned by applicants for the license to operate.
Consequently, the primary locus of regulatory stringency lies in the federal requirements of participation as a Medicare- or Medicaid-certified nursing home provider (Furrow et al., 2008; IOM, 2001, p. 21; Walshe, 2001). The requirements of participation include requirements that likely parallel most states’ licensure standards but that also specify the minimum quality of care that a nursing home must provide. For example, the requirements of participation state that nursing homes must provide services and activities to “attain or maintain the highest practicable physical, mental, and psychosocial well-being of each resident” according to a written plan of care.5
Even though requirements of participation go beyond what might be considered the absolute minimum standards of quality, the increased requirements are rather modest. On the other hand, some have argued that the sheer number of requirements of participation creates long checklists that encourage technical compliance but do not adequately allow providers to focus on their residents’ quality of life (Harrar et al., 2021; Jaffe, 2020; Walshe, 2001). This tension emerged prominently between the 2016 revision of nursing home standards and the subsequent repeated efforts to scale these standards back (Justice in Aging, 2020; Musumeci and Chidambaram, 2020; National Consumer Voice, 2019). Despite the ideological nature of this particular dispute, there is still potential merit to the exercise of ensuring that the requirements of participation are both thorough in ensuring quality and maintain a focus on what matters to nursing home residents.
Medicare and Medicaid are the predominant purchasers of nursing home care, and the need to maintain beneficiary access limits the ability of Medicare and Medicaid to demand quality that exceeds the requirements of participation. More demanding requirements of participation also need to be balanced with potential increases in program payments that ensure sufficient numbers of nursing homes will continue to serve beneficiaries.
Certificate of Need and Construction Moratoria
As part of the licensing process, some states maintain certificate-of-need requirements to regulate expansions in the health care market as a strategy to constrain health care spending. Certificate-of-need policies
___________________
5 CMS Requirements for Long Term Care Facilities—Administration, 42 CFR § 483.70 (2016).
employ a need-based evaluation of all applications for new construction or additions to existing facilities that would increase the number of beds. Additionally, some states have implemented construction moratoria that prohibit the building of new health care facilities. By 1979, almost all states had certificate-of-need regulations, and these policies typically included nursing homes (Feder and Scanlon, 1980). As of December 2021, 35 states and Washington, DC, have certificate-of-need policies in place, with wide variability among the states in how these policies are structured, including how “need” is defined (Cavanaugh et al., 2020; NCSL, 2021; Wiener et al., 1998).
Impact of Certificate-of-Need Policies in Health Care
The general rationale for certificate-of-need and construction moratorium regulations rests on Roemer’s law, which states “a built bed is a filled bed is a billed bed” (Shain and Roemer, 1959). That is, these policies seek to compensate for a concern that the principles of supply and demand in a third-party payment system may result in overinvestment in health care facilities, misdistribution of health care resources, and delivery of more services than actually needed, given that consumers are not impacted by the cost of services (Bruneau, 2014; Feder and Scanlon, 1980; Havighurst, 2005). For health care in general, certificate-of-need regulations have been found to be largely ineffective, and “in fact, by limiting supply and monopolizing local health care, [they] seem to raise costs and undermine quality care. More than anything, though, they limit access to health care services” (Mitchell, 2021). In 2004, the Department of Justice (DOJ) and the Federal Trade Commission recommended reconsidering these regulations, stating that they believed that “on balance, [they] are not successful in containing health care costs, and that they pose serious anticompetitive risks that usually outweigh their purported economic benefits. Market incumbents can too easily use [certificate-of-need] procedures to forestall competitors from entering an incumbent’s market” (DOJ and FTC, 2004, p. 22). In 2016, Mitchell and Koopman noted that “forty years of peer-reviewed academic research suggests that [certificate-of-need] laws have not only failed to achieve their goals but have in many cases led to the opposite of what those who enacted the laws intended” (Mitchell and Koopman, 2016).
Impact of Certificate-of-Need and Construction Moratoria on Nursing Homes
The general principles behind certificate-of-need regulations may not apply to the nursing home setting, in that residents and their families often do have out-of-pocket expenditures for care (see Chapter 7) (Feder and
Scanlon, 1980). The logic behind these regulations for nursing homes specifically is that limiting the number of beds will, in turn, limit the number of Medicaid beneficiaries in nursing home settings, thus keeping state Medicaid spending low. However, the evidence does not suggest that the regulations have much effect (Grabowski et al., 2003; Rahman et al., 2016). As noted by Wiener and colleagues, “most states feel that supply controls have contributed to cost containment, although none could quantify the effect” (Wiener et al., 1998, p. 10). In fact, Medicare and Medicaid spending on nursing home care has been shown to grow faster in states with certificate-of-need laws (as compared to states without those laws) (Rahman et al., 2016). Moreover, when states repeal certificate-of-need laws, they do not experience increases in nursing home spending, with the likely reason being that most families will exhaust every community option before seeking nursing home care (Grabowski and Gruber, 2007; Grabowski et al., 2003; Konetzka et al., 2019; Mattimore et al., 1997). The cost of compliance with certificate-of-need regulations may also exceed their benefits and decrease social welfare (Conover and Bailey, 2020).
While certificate-of-need regulations do not appear to have their intended effect of holding down Medicaid nursing home spending, they can have the unintended effect of harming consumers. Studies have found that these regulations limit choice and lower access to medical services and health care resources, especially for those in rural areas (Feder and Scanlon, 1980; Mitchell, 2017; Wiener et al., 1998); decrease the quality of care for some measures of quality (Fayissa et al., 2020; Grabowski et al., 2008; Stratmann and Wille, 2016; Zinn, 1994); and increase private-pay prices (Nyman, 1994). For example, Fayissa and colleagues (2020) found that nursing homes in states with such regulations (as compared to nursing homes in states without these regulations) had lower health survey scores (by 18 to 24 percent) and lower levels of employment for registered nurses and licensed practical nurses (along with increased employment of certified nurse aides) (Fayissa et al., 2020). Additionally, the presence of these policies did not result in fewer complaints.
Certificate-of-need regulations and construction moratoria can also discourage innovation by preventing the entry of more modern and desirable nursing home options and restricting facility renovation and remodeling (Grabowski, 2017; Mitchell, 2021; Reinhard and Hado, 2021; Wiener et al., 1998). As Chapter 6 notes, many of today’s nursing homes were built using design features adapted from hospitals constructed in the 1960s and 1970s and therefore have an institutional environment (Eijkelenboom et al., 2017; Schwarz, 1997). Furthermore, certificate-of-need regulations may contribute to the perpetuation of larger nursing homes, rather than the smaller, more home-like settings that are more desirable. These regulations have been associated with a higher average nursing home size (Ferdows
and Rahman, 2020; Kosar and Rahman, 2021; Nastasi, 2020; Rahman, 2016); the average number of beds is roughly 110 in states without such a regulation and 131 in states with one (Rahman et al., 2016). The experience of small-home models such as the Green House (see Chapter 6) have highlighted the importance of capital investments for developing higher-quality models of nursing home care.
Some have argued that certificate-of-need policies and construction moratoria are needed because of the decreasing occupancy rates in nursing homes. However, one examination of nursing home moratoria in Indiana noted that “focusing solely on occupancy rates ignores the underlying reasons why the beds are unoccupied” (Glans, 2015). The author suggests that lower occupancy rates may reflect that “they are older and are not offering the services consumers want or need” and that new facilities will naturally replace older, less desirable nursing homes (rather than “forcing” residents into older facilities) (Glans, 2015). Others have raised concerns that lifting certificate-of-need regulations will increase Medicaid spending on institutional care and so reduce investment in home- and community-based settings of long-term care (Kitchener et al., 2005; Miller et al., 2002; Williams, 2019). However, no evidence suggests that this has occurred. In fact, limited evidence demonstrates that between 1992 and 2009, “spending on home health care by both Medicare and Medicaid increased at a much faster rate in states without [certificate of need]” (Rahman et al., 2016).
At the height of the COVID-19 pandemic in spring of 2020, 24 states eased, suspended, or temporarily lifted certificate-of-need regulations to increase flexibility (Erickson, 2021). Several other states introduced legislation to repeal or reform such restrictions (Mitchell, 2021).
State Surveys
States assist with the assessment of facilities’ compliance with requirements of participation and, as necessary, with the investigation of complaints and adverse incidents. States have some discretion in how they administer these responsibilities, but all states are expected to adhere to the detailed protocols outlined in the State Operations Manual (CMS, 2017a). Using the federal survey protocol and other federal guidance, states report state survey findings about the scope and severity of deficiencies as well as their recommendations for enforcement actions to CMS. However, CMS has the ultimate authority to sanction facilities and to audit all state inspection activities (CMS, 2018b; IOM, 1986). Accordingly, the federal government has the statutory power to review state decisions and overrule them, known as the “look behind” provision (Walshe and Harrington, 2002).
The overall survey process (Figure 8-1) is uniform across states. In 2017, the process was updated to use “as much structure as possible to
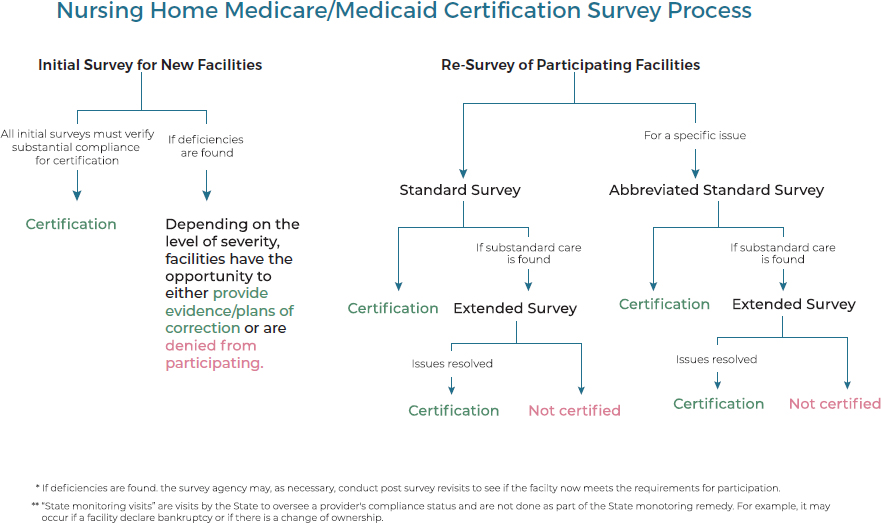
SOURCE: Adapted from CMS, 2018b.
ensure consistency while allowing surveyors the autonomy to make decisions based on their expertise and judgment” (CMS, 2017b). The process is also completely automated (instead of using paper as was previously done in some surveys). Most commonly, facilities receive a standard survey. However, if a surveyor finds evidence of substandard care, the choice can be made to then conduct an extended survey, which evaluates additional participation requirements. The survey agency then compiles its findings of deficiencies and recommends action to CMS and the state. It is up to CMS and the state to determine whether they give a facility the opportunity to correct its deficiencies before CMS imposes penalties. If CMS and the state give a facility the opportunity to correct deficiencies, it must submit an acceptable plan of correction or proof of correction for past noncompliance (CMS, 2018b).
Upon completing the entire survey process, facilities have the opportunity to dispute cited deficiencies through an informal dispute resolution process beyond the plans of correction. However, if there is evidence of “immediate jeopardy—a situation in which the facility’s noncompliance with one or more requirements of participation has caused, or is likely to cause, serious injury, harm, impairment, or death to a resident”—the regional office or state Medicaid agency will immediately terminate the facility’s Medicare/Medicaid participation, mandate installing temporary management, or impose other penalties (CMS, 2018b).
State Surveyors for Long-Term Care
Minimum standards to be a federal surveyor in long-term care facilities for the determination of Medicare/Medicaid compliance include
- Appropriate background in the health professions or health administration;
- Completion of an orientation program and basic surveyor training course;
- Passing the Surveyor Minimum Qualifications Test;
- Annual job-related training courses;
- Lack of conflict of interest; and
- Dedication of at least 50 percent of one’s working time to survey activities or to meeting the professional qualifications for the surveyor’s health profession (CMS, 2019a).
The survey team’s composition and size varies, depending primarily on the following factors: the number of beds in the facility, whether the facility has a history of deficiencies, if a facility has a special care unit,
and whether the team includes surveyors-in-training. CMS guidance calls for states to staff the survey teams with multidisciplinary individuals who have expertise and knowledge of best practices in working with the care population. Ultimately, “the state (or, for federal teams, the regional office) decides what the composition of the survey team will be,” as long as it meets statutory and regulatory requirements (CMS, 2016). In addition, a multidisciplinary team of professionals, at least one of whom is a registered nurse, must conduct nursing home standard surveys.
The 1986 IOM report Improving the Quality of Long-Term Care included several recommendations regarding the training of nursing home surveyors, including
- Implementation of programs for effective training and monitoring of surveyor performance to reduce inconsistency;
- A revision of guidelines to be more specific about the qualifications of surveyors and the composition and numbers of survey team staff; and
- Increased federal training efforts and support of state-level training programs.
A 1999 report from the Office of the Inspector General (OIG) also called for evaluating surveyor staff to ensure that there is adequate staffing, additional training for state surveyors with a forum to meet and discuss common issues to ensure consistency, and standardized ongoing training requirements across states (OIG, 1999). Several reports note the challenges in hiring qualified surveyor staff. For example, a 2005 report from the Government Accountability Office (GAO) highlighted “continuing problems in hiring and retaining qualified surveyors, a factor that states indicated can contribute to variability in the citation of serious deficiencies” (GAO, 2005, p. 37). In 2008, the GAO noted two factors that contributed to significant understatement of serious care problems by surveyors: weaknesses in surveyors’ investigative skills and weaknesses in surveyors’ ability to properly analyze the information they had collected (GAO, 2008). A follow-up study in 2009 concluded that “workforce shortages and training inadequacies affected states’ ability to complete thorough surveys, contributing to the understatement of nursing home deficiencies” (GAO, 2009a, p. 22). States often identify staffing as a key factor in their inability to meet the standard for survey timeliness, noting “the most common staffing-related description centered on the inability to attract and retain surveyors, often due to not being able to offer high enough salaries to compete in local markets” (OIG, 2022a, p. 11).
Similar to recruiting care providers to the nursing home setting, recruiting qualified surveyors can also be a challenge. In her testimony to this committee, Alice Bonner, a senior advisor with the Institute for Healthcare Improvement (IHI), noted
How are we training surveyors? [. . . .] How [can] we get really good, dedicated people to want to become surveyors? This is one of the most important jobs in health care. And it’s critical to people who live in nursing homes and who work in nursing homes. And to the care partners in the community. So how can we recruit really good people who are registered nurses and social workers, who can make a lot more money doing something else in a lot of states?
Overall, state survey agencies need more surveyors (in sheer numbers), competitive compensation, and enhanced training to ensure that surveyors have the qualifications and supports needed to effectively carry out their responsibilities.
Funding of the Survey Process
The survey process is funded by a combination of Medicare, Medicaid, and non-Medicaid state funds (GAO, 2009b). Medicare surveys are funded by a discretionary appropriation from Congress based on budget requests submitted by CMS while states receive 75 percent federal matching funds for Medicaid surveys (GAO, 2009b; OIG, 2022a). CMS’ budget for these activities remained flat since fiscal year (FY) 2014, at about $397 million annually (OIG, 2022a). However, during that time period, CMS increased the allotment to states by about 4 percent. In 2020, CMS received additional funding through the Coronavirus Aid, Relief, and Economic Security Act6 for survey and certification expenses during the COVID-19 pandemic. In addition to paying the 25 percent of Medicare-covered expenditures for surveys, states are also expected to contribute additional funds for other reasons, including the costs associated with state licensure (GAO, 2009b). In 2009, the GAO noted that “CMS oversight of states’ use of survey funds is limited because it relies on state-reported data, has inadequate information about non-Medicaid state funding, and does not require states to justify supplemental funding” (GAO, 2009b, p. 15). See later in this chapter for more on CMS oversight of the state survey process.
___________________
6 Coronavirus Aid, Relief, and Economic Security Act, Public Law 116-136; 116th Cong., 2nd sess. (March 27, 2020).
Complaints
In addition to standard survey inspections that nursing homes undergo, residents and other parties may file complaints with the state or federal regulatory agency related to adverse events or general dissatisfaction with the quality of care. Medicare- and Medicaid-certified nursing homes are required to have established procedures for complaints by residents and people acting on the resident’s behalf. Specifically, nursing homes must
- Make survey, certification, and complaint investigation reports available;
- Investigate complaints and monitor compliance; and
- Make information about what complaint forms are, how they are used, and how to file a complaint with the state survey and certification program and the state long-term care ombudsman program available.7,8
States are responsible for receiving, prioritizing, and investigating complaints. The most serious complaints are categorized as either “immediate jeopardy” or “high priority” (also known as non-immediate jeopardy–high) and require immediate attention (see Box 8-3). Less serious complaints may require onsite investigation by the state, desk review, or referral, but do not have a specific timeframe for action.
While there are many ways to file a complaint at a nursing home, states must have standard complaint forms for residents to file with the state survey agency and a state long-term care ombudsman program (depending on the facility). They also must have a formal complaint resolution process. The ACA sought to make filing such complaints easier by providing standardized complaint forms and streamlining the complaint resolution process (KFF, 2013). However, substantial barriers still exist—including barriers related to the process itself as well as those related to fear of reprisal (Carlson, 2015; Lee et al., 2021). For example, according to reports by ombudsmen, racial and ethnic minority residents may avoid filing complaints out of fear of retaliation (Lee et al., 2021).
Data on consumer complaints have improved in recent years with Care Compare’s addition of information on complaints and deficiencies. As shown in Table 8-1, the number of overall complaints per 1,000 nursing homes increased steadily between 2011 and 2018 (OIG, 2020a). The percentage of complaints prioritized as either immediate jeopardy or high priority remained relatively consistent. As shown in Table 8-2, between
___________________
7 Social Security Act, Title XVIII §1819 (d)(1)(C), 42 U.S. Code 1395i–3, 89th Cong., 1st sess. (July 30, 1965).
8 Social Security Act, Title XI §1128I (f), 42 U.S. Code § 1320a-7j, 89th Cong., 1st sess. (July 30, 1965).
TABLE 8-1 Numbers and Prioritization of Complaints, 2011–2018
| 2011 | 2015 | 2016 | 2018 | |
|---|---|---|---|---|
| Total number of complaints | 47,279 | 62,790 | 66,077 | 71,602 |
| Number of complaints per 1,000 nursing home residents | 32.7 | 44.9 | 47.3 | 52.3 |
| Percentage of complaints prioritized as immediate jeopardy | 6% | 8.5% | 9% | 7% |
| Percentage of complaints prioritized as high priority | 49.1% | 50.6% | 50% | 47% |
SOURCE: OIG, 2020a.
TABLE 8-2 Numbers and Investigations of Immediate Jeopardy and High Priority Complaints, 2016–2018
| 2016 | 2017 | 2018 | |
|---|---|---|---|
| Immediate Jeopardy Complaints | |||
| Number of immediate jeopardy complaints | 6,039 | 5,451 | 5,245 |
| Percentage of immediate jeopardy complaints not investigated within 2 days | 24.0% | 17.7% | 12.8% |
| High Priority Complaints | |||
| Number of high priority complaints | 32,774 | 32,722 | 33,974 |
| Percentage of high priority complaints not investigated within 10 days | 15.4% | 16.2% | 19.3% |
SOURCE: OIG, 2019a.
2016 and 2018, the percentage of immediate jeopardy complaints that were not investigated within the required timeline decreased, but the percentage of high-priority complaints that were not investigated within the required timeline increased. Moreover, from 2016 through 2018, “twenty-one states failed to meet CMS’ timeliness threshold for high priority complaints in all three years” (OIG, 2020a, p. 6); among these states, 10 did not meet performance thresholds for timeliness for 8 consecutive years (2011–2018). (See more on timeliness of survey activities later in this chapter.)
In one example, as of April 2014, long-term care facilities in California had more than 10,000 open complaints and facility-reported incidents (California State Auditor, 2014). A 2014 report from the California State Auditor recommended establishing specific timelines for the investigation of these complaints, ensuring adequate staff, and following specific procedures for review and approval; as of November 2019, these recommendations had not been implemented (California State Auditor, 2014, 2020).
For a nursing home staff perspective on the complaints process, see Box 8-4.
For more on states’ performance in addressing complaints, see later in this chapter for a discussion of CMS oversight and performance of the state survey process.
Additional State-Based Roles
Although the most important role of states in nursing home oversight is assessing compliance with federal requirements, states that wish to increase the stringency of nursing home quality control have additional mechanisms available. For instance, states might impose more stringent
staffing standards than those in federal guidelines (Harrington et al., 2020). States also have primary oversight responsibility for the very small portion of nursing homes that do not participate in the Medicare or Medicaid programs and therefore are not subject to the detailed requirements of participation.
PRIVATE ACCREDITATION
Beyond the required government oversight, nursing homes can elect to undergo additional voluntary scrutiny through private accrediting entities such as The Joint Commission. Typically funded by fees from participating facilities, private accrediting agencies generally set detailed accreditation standards, assess facilities’ compliance with those standards, and subsequently work with providers to address identified shortcomings and improve operations (Castle et al., 2011). Relative to government oversight, the approach of private accrediting agencies is oriented more to quality improvement, something that is outside the standard purview of regulatory agencies. There is very little evidence, however, suggesting that nursing home providers who choose to engage in voluntary accreditation efforts have subsequently improved care practices (Wagner et al., 2012).
CMS allows certain health care organizations to receive a “deemed status”—that is, the organization can participate in Medicare and Medicaid but be exempt from the Medicare survey and certification process if a qualifying private accrediting entity determines that the organization meets or exceeds federal requirements of participation (ASHE, 2021; CMS, 2008). However, a 1998 report to Congress from HCFA found that private accreditation (as compared to the traditional survey process) emphasized process and structure measures over resident-centeredness, were less transparent than the traditional nursing home survey process, and tended to miss serious deficiencies; the authors concluded that “the potential cost savings to deeming would not appear to justify the risk to the health and safety of the vulnerable nursing home population” (HCFA, 1998, p. iv). Determinations by private accrediting bodies are not sufficient for nursing homes’ participation in Medicare and Medicaid, and are strictly voluntary.
ENFORCEMENT AND PENALTIES
After the determination of compliance with quality criteria through requirements of participation, the third component of regulation for nursing homes is the enforcement of compliance with these criteria, largely through various sanctions.
Sanctions by CMS and State Survey Agencies
To enforce compliance and penalize poor performers, CMS and state survey agencies can levy a range of sanctions against nursing homes. Depending on the seriousness of the deficiency, penalties can range from directed plans of correction and in-service trainings to the imposition of civil monetary (or money) penalties (CMPs), the appointment of temporary management, denial of payment, and termination from participation in the Medicare and Medicaid programs.
Prior to OBRA 87, termination from participating in Medicare and Medicaid programs was the only available sanction for noncompliant facilities, but today there are a wider variety of intermediate options for penalizing noncompliant nursing homes. As noted earlier, states report survey findings about the scope and severity of deficiencies as well as their recommendations for enforcement actions to CMS. Despite the range of enforcement options available, CMPs have by far been the most common remedy used in recent years to sanction nursing homes. Specifically, as Table 8-3 shows, CMPs accounted for nearly 72 percent of the 28,077 enforcement actions taken from FY 2016 through FY 2020. (See below for more on CMPs.)
More stringent sanctions, such as temporary management and termination from participation in Medicare and Medicaid, are rarely used (CMS, 2021b; GAO, 2009c; Li et al., 2010; OIG, 2006a). For example, in 2006, OIG found that CMS terminated the participation of only 45 percent of the facilities that warranted that sanction (OIG, 2006a).
Civil Monetary Penalties
CMPs are fines imposed by CMS for noncompliance with requirements of participation—either a total fine based on the number of days out of compliance for a single infraction (per day) or for each instance of noncompliance (CMS, 2021c). In 2019, almost $120 million was collected in CMPs (about $100 million from per day penalties and nearly $20 million from per instance penalties); the average total dollar amount was $68,126 for per day penalties and $9,950 for per instance penalties (CMS, 2022). The average days in effect for per day penalties was 57 days (CMS, 2022). In 2005, the OIG found that CMS tended to impose penalties at the lower end of the range (OIG, 2005). Additionally, some studies have found interstate variability in how CMP is enforced and how the funds are used (Harrington et al., 2008; Wang et al., 2019).
Through the CMP Reinvestment Program, a portion of these funds are returned to states to be used for activities to improve the quality of care for nursing home residents. Examples of permissible use of the funds include assistance for residents of facilities that are closed or decertified,
TABLE 8-3 Enforcement Actions Report, FY 2016–2019
| Enforcement Action | 2016 | 2017 | 2018 | 2019 | TOTAL |
|---|---|---|---|---|---|
| State Monitoring | 67 | 100 | 95 | 38 | 300 |
| Directed Plan of Correction | 37 | 46 | 63 | 75 | 221 |
| Temporary Management | 3 | 5 | 1 | 7 | 16 |
| Discretionary Denial of Payment for New Admits | 445 | 551 | 453 | 577 | 2,026 |
| Mandatory Denial of Payment for New Admits—3 Months | 221 | 161 | 191 | 162 | 735 |
| Denial of Payment for All Residents | 5 | 5 | 7 | 3 | 20 |
| Directed In-Service Training | 337 | 278 | 275 | 292 | 1,182 |
| Civil Monetary Penalty | 2,726 | 4,206 | 3,399 | 3,421 | 13,752 |
| CMS-Approved Alternative or Additional | 5 | 11 | 8 | 8 | 32 |
| Transfer of Residents/Closure of Facility | 0 | 1 | 1 | 0 | 2 |
| Transfer of Residents | 2 | 0 | 0 | 0 | 2 |
| Discretionary Termination | 8 | 7 | 3 | 2 | 20 |
| Mandatory Termination | 15 | 12 | 7 | 12 | 46 |
| Total Number of Enforcement Actions | 3,871 | 5,383 | 4,503 | 4,597 | 18,354 |
| Total Number of Nursing Homes with Enforcement Actions* | 2,537 | 3,474 | 2,944 | 2,991 | 11,946 |
SOURCE: CMS, 2021b.
NOTE: While more recent data are available, the impact of the COVID-19 pandemic on enforcement actions may skew data trends, and require separate analysis.
*These data come from the Certification and Survey Provider Enhanced Reporting (CASPER) system. CASPER notes that the provider (i.e., nursing home) count is “valid for the subset of providers or suppliers for which there are survey records in CASPER.” For more information, see https://qcor.cms.gov (accessed November 10, 2021).
relocation of residents, support for resident and family councils, training of nursing home staff and surveyors, and technical assistance for quality improvement in nursing homes (CMS, 2021c). CMP funds cannot be used for expenses such as research, capital improvements, nursing home employee salaries, and expenses associated with requirements of participation (CMS, 2019c).
Civil and Criminal Action
Distinct from the mechanisms described above, the government can hold nursing homes liable for damages under fraud and abuse laws, such as under the federal False Claims Act (Landsberg and Keville, 2001). This law provides sanctions against any health care provider that defrauds the government, either by billing CMS for services it did not actually render or, in some cases, for delivering services that do not meet baseline standards. Although
regulators use the False Claims Act relatively infrequently to police nursing home quality, it can be an option for extreme cases of noncompliance with requirements of participation.
Additionally, government agencies are not the only entities that can impose penalties; the courts can hold nursing homes liable for certain violations (Stevenson and Studdert, 2003). As with traditional medical malpractice claims, nursing home residents and their families have a private right of action against facilities for damages and potentially even for breach of contract. While some argue that liability for harm increases the incentives for delivering high-quality care, evidence shows little difference in the susceptibility to claims of harm among lower-quality and higher-quality homes (Studdert and Stevenson, 2004; Studdert et al., 2011). Furthermore, liability claims have little impact on the subsequent care that facilities provide (Konetzka et al., 2013; Stevenson et al., 2013a).
Many states have passed tort reform legislation, most notably caps on non-economic damages, which can have a particularly negative impact on nursing home cases (Studdert and Stevenson, 2004). Furthermore, during the COVID-19 pandemic, several states passed liability protections for nursing homes against pandemic-related claims or enhanced existing laws (Associated Press, 2021; Brown, 2021; Critchfield, 2021). In July 2020, the American Bar Association noted that more than half of all states “have granted some sort of immunity from civil liability to long-term care facilities and health care providers. Three states have granted facilities and providers immunity from criminal and civil liability” (Brooks et al., 2021). Most of the states provide protections from accusations of negligence, requiring proof of willful or gross negligence.
In 1998, President Clinton announced a large initiative to improve the quality of care in nursing homes (White House, 1998). Part of this initiative directed HCFA (in conjunction with the Office of the Inspector General and DOJ) to “refer egregious violations of quality of care standards for criminal or civil investigation and prosecution when appropriate.” In March 2020, the DOJ announced the National Nursing Home Initiative (NNHI), a program coordinated by the Elder Justice Initiative in collaboration with the U.S. Attorneys’ Offices. NNHI aims to pursue civil and criminal actions against nursing homes that provide substandard care and “owners and operators who have profited at the expense of their residents” (DOJ, 2020). NNHI looks for facilities that lack proper hygiene and infection control protocols, fail to provide proper food to residents, withhold pain medication from residents, fail to provide adequate staffing, or use chemical and physical restraints. DOJ plans to scrutinize data from whistleblowers, wrongful death lawsuits, federal and state inspections and audits, and COVID-19 reporting data from federal agencies (e.g., CMS) (Hall et al.,
2020). NNHI will also work to ensure compliance with the False Claims Act (Yoder, 2020). DOJ has not released more information about NNHI since it launched the program.
Corporate Integrity Agreements
Beyond the traditional survey process, a corporate integrity agreement allows nursing homes with identified quality-of-care problems to remain in the Medicare and Medicaid programs if they contract with an independent quality monitor that has been authorized by OIG to oversee clinical improvement and compliance. Corporate integrity agreements generally last for 5 years (OIG, 2022b). The OIG sometimes negotiates a corporate integrity agreement as part of a settlement for investigations of fraud arising under the False Claims Act (DOJ, 2014, 2016; OIG, 2022b).
In 2009, the OIG studied 15 nursing home corporations that had entered into corporate integrity agreements (OIG, 2009). While all 15 corporations ultimately instituted structures and processes related to quality, the OIG was unable to determine the actual impact on the quality of care because of the “lack of agreed-upon benchmarks for quality of care outcome measures throughout the nursing home industry” (OIG, 2009, p. 17). In 2018, in response to media coverage of the use of corporate integrity agreements in the settlements of False Claims Act cases, the Center for Medicare Advocacy called for more transparency of corporate integrity agreements (Edelman, 2018). It noted
Transparency would both enable the monitor to receive comprehensive, timely information that is relevant to determining the company’s compliance with the [corporate integrity agreement] (or whether there has been a material breach) and inform the public about the ongoing status of the company’s compliance. (Edelman, 2018)
The Special Focus Facility Program
The Special Focus Facility (SFF) program, created in 1998, is a program in which CMS and states identify the lowest-performing facilities as determined by numbers of deficiencies found during survey, the severity of those citations, and patterns of serious problems over time and then subject those facilities to more frequent inspections and quality improvement activities (CMS, 2021d). States use a points-based system to create a list of candidates for the program. The states then select a subset of the candidate list to participate in the SFF program. CMS regulations state,
“Once a state selects a facility as an SFF, the state survey agency, on CMS’s behalf, conducts a full, onsite inspection of all Medicare health and safety requirements every six months and recommends progressive enforcement (e.g., fines, denial of Medicare payment) until the nursing home either (1) graduates from the SFF program; or (2) is terminated from the Medicare and/or Medicaid program(s)” (CMS, 2021d). According to CMS, most SFF nursing homes improve significantly within 18 to 24 months, with CMS terminating about 10 percent from participating in Medicare and Medicaid (CMS, 2021d). Improving this small program has been a recent focus of federal policy makers and is a central component of the proposed Nursing Home Reform Modernization Act. However, many graduates fail to sustain improvement (or may even regress) and the budget for the SFF program only allows for oversight of a small fraction of the nursing homes deemed to be among the most poorly performing (CMA, 2019; GAO, 2010a; Rau, 2017).
CMS OVERSIGHT AND PERFORMANCE OF THE STATE SURVEY AND CERTIFICATION PROCESSES
As noted earlier, CMS holds responsibility for overseeing the state survey process. Several reports from GAO and OIG over the past two decades have found failures in the survey process to properly identify serious care problems, fully correct and prevent recurrence of identified problems, and investigate complaints in a timely manner, as well as failures in CMS’s oversight of these surveys (GAO, 1999, 2003, 2007, 2008, 2009a, 2010b, 2018, 2019; OIG, 2006b, 2019b,c, 2020a, 2022a). For example, a 2008 GAO study found that surveyors “sometimes understate the extent of serious care problems in homes because they miss deficiencies” (GAO, 2008, p. 2). In January 2022, OIG reported that “just over half of states repeatedly failed to meet requirements for conducting nursing home surveys, most commonly for failures of survey timeliness” (OIG, 2022a, p. 8); 23 percent of failures for timeliness were for failure to conduct high-priority complaints within 10 days of the allegation. In 2020, OIG raised questions about “some states’ ability to address serious nursing home complaints and also about the effectiveness of CMS’ oversight of states” (OIG, 2020a, p. 14). Furthermore, investigative reports have also highlighted stories of failures in the regulatory process to detect or report serious issues (e.g., abuse, neglect) (Gebeloff et al., 2021; Levinson, 2017; Rau, 2018a; Silver-Greenberg and Gebeloff, 2021).
Improving the survey and certification process requires consideration of several overarching issues, including CMS’s oversight of state performance, variability in survey performance, and the limited ability of surveyors to tailor the process based on a facility’s previous performance.
Evaluating State Performance of Surveys
A major part of CMS’s oversight responsibility includes evaluating state performance in survey and certification activities. The State Performance Standards System allows CMS regional offices to monitor state performance and identify areas for improvement through the use of performance metrics across three domains:
- Frequency (number and time frame of surveys),
- Quality (surveys conducted in accordance with federal guidelines and accurately identify deficiencies), and
- Enforcement and remedy (effectiveness of enforcement) (OIG, 2022a).
If a state is found to have performed inadequately, CMS can impose remedies (e.g., training, technical assistance, and corrective action plans) or sanctions (e.g., meeting with governor and other state officials, reducing federal financial participation, and terminating the state’s agreement) (OIG, 2022a). Financial penalties can be imposed in addition to such remedies and sanctions. A 2008 GAO report found that CMS was “not using the database to oversee consistent implementation of the program by the regional offices—for example, the agency is not using the database to identify inconsistencies between comparative and observational survey results” (GAO, 2008, p. 2). In January 2022, OIG reported that many corrective action plans were missing or lacked detail, CMS often did not track training and technical assistance efforts, and CMS rarely imposed formal sanctions (OIG, 2022a). OIG’s recommendations included better tracking of the outcomes of remedies, establishing guidelines for progressive enforcement actions on the state, and actively disseminating state performance metrics with other stakeholders.
Variability in Survey Performance
Whether in the implementation of routine inspection responsibilities, imposition of sanctions, or in the investigation of complaints, considerable variation in processes and outcomes exists across states (Castle et al., 2007; CMS, 2021e; GAO, 2005, 2011a; Hansen et al., 2017; Harrington et al., 2008; OIG, 2003, 2019a, 2020a, 2022a; Stevenson, 2006). For example, a 2003 OIG report found that states use different deficiency tags to cite the same problem (OIG, 2003). A 2005 GAO report identified inconsistency in how states conduct surveys (as demonstrated by “wide interstate variability in the proportion of homes found to have serious deficiencies”) as a challenge to ensuring high-quality care (GAO, 2005). As mentioned earlier, the responsibility for surveying and enforcing compliance with nursing home standards falls largely to individual states. This approach may increase
bureaucracy and inevitably introduces state-level variation in the regulatory process (OIG, 2003). Such variation in implementing federal oversight standards and processes may occur both within and across states. However, it can be difficult to determine what portion of this variation reflects true quality-of-care differences and what portion reflects different state approaches to regulation. For example, states may interpret regulations differently (GAO, 2011a). States can also have limited capacity to faithfully execute oversight responsibilities, and these constraints are especially acute in some states.
Responsiveness to Previous Performance
Nursing home oversight in the United States is largely a standardized enterprise, with almost all facilities inspected for compliance with the same standards on a roughly annual basis. In contrast, a more targeted approach to regulation would scrutinize low- and high-quality performers with differing intensity. The idea of targeted or responsive regulation has a broad theoretical foundation aimed at making oversight more effective. Regulatory theorists have outlined the potential strengths and limitations of the approach (Braithwaite et al., 2007; Walshe, 2001), and both the 1986 and 2001 IOM reports on long-term care quality raised the notion of targeting inspection efforts more efficiently (IOM, 1986, 2001). In 1986, the IOM noted
the introduction into the survey cycle of flexibility that is tied to performance and key events should enable survey resources to be targeted to those facilities most in need of attention: problem or marginal facilities and facilities where new circumstances could adversely affect residents. Facilities that are performing well would be rewarded for their good behavior by less-intense monitoring. That will allow survey agency staff to be used for more urgent tasks. (IOM, 1986, p. 112)
In fact, the current approach to nursing home oversight already incorporates elements of responsive regulation, albeit primarily at the lower end of the quality spectrum, such as through the SFF program. CMS’s Quality Improvement Organization program (see Chapter 3) has also targeted relatively poor performers (Stevenson and Mor, 2009). Federal regulations also allow states to vary inspection frequencies between 9 and 15 months and to tailor the inspections themselves based on the anticipated quality of care in the facility. One analysis of the most recent Community Assessment for Public Health Emergency Response survey found that this happens only to a small extent. In 2018, for example, one- and five-star nursing homes differed in survey frequency by only 11 days on average, with an average of 399 days between surveys for all facilities (Stevenson, 2019).
Still, many advocates oppose targeted survey efforts and argue that “the approach fails to recognize our current ability to identify high-performing facilities and how quickly quality of care can decline at even the best nursing homes” (Stevenson, 2019; see also Edelman, 2019). In particular, it has been challenging to conceptualize and implement a revised or scaled-back survey approach for better-performing nursing homes. Such an approach would depend on two key elements: regulators being able to reliably identify better facilities deserving of less scrutiny, and the oversight system being sufficiently responsive to detect and respond if care faltered. At a recent Senate Finance Committee hearing on nursing homes, Senator Ron Wyden (D-OR) characterized the five-star quality rating system as a “mess,” in part because of the fact that four- and five-star facilities were among those that had cases of reported abuse and neglect (Wyden, 2019). In addition, a March 2021 New York Times article raised additional concerns about the veracity of the data underlying the five-star system, some of which are self-reported (Silver-Greenberg and Gebeloff, 2021). (See Chapter 3 for more on the five-star quality reporting system.)
Collaboration for Quality Improvement
Federal statutes currently preclude survey agencies from consulting with or guiding the nursing homes they oversee, based on the assumption that if surveyors are too collegial with nursing homes, they may be less likely to cite deficiencies or impose sanctions (Li et al., 2012; Stevenson, 2018). Examples of possible collaborations include that state survey agencies could require nursing homes to develop and implement plans of correction for areas where they are falling short, or in advance of imposing fines, survey agencies could encourage nursing homes to work with quality improvement technical-assistance programs to help them identify and address the root causes of their problems (Stevenson and Mor, 2009). In its 1998 report to Congress, HCFA found little evidence that quality improvement initiatives could supplant the normal survey process (HCFA, 1998).
LONG-TERM CARE OMBUDSMAN PROGRAMS
Long-term care ombudsman programs, administered by the Administration for Community Living, represent the only type of entity within the nursing home system whose sole mission is to be an advocate for the residents to ensure that they receive the care to which they are entitled (NORC, 2019). State ombudsmen work to (1) monitor, protect, and promote resident rights by investigating and resolving complaints from nursing home residents; (2) advocate for systems-level change; and (3) perform outreach activities and educate residents, their loved ones, staff, and collaborating
agencies on the rights of residents (NORC, 2019). The program plays an important extra-regulatory role in nursing home quality assurance in that these complaints and investigations are distinct from the legally required complaint mechanisms that state regulatory agencies direct (Berish et al., 2019; Hunt, 2008). Ombudsmen can serve as liaisons between the government and facilities by communicating information about best practices to nursing homes, responding to concerns about oversight and quality of care, and alerting government agencies to problems that require their attention (Berish et al., 2019). One study noted, “Though ombudsmen have limited power in their oversight and have no binding regulatory authority, they play three major roles in the long-term care environment: mediator, informal therapist, and resident advocate” (Berish et al., 2019, p. 1326).
The Long-Term Care Ombudsman Program began as a demonstration program in 1972 and was elevated to a statutory level in 1978 through an amendment to the Older Americans Act which required each state to establish an ombudsman program (ACL, 2021b; Hunt, 2008; NASUAD, 2019). Over time, additional amendments expanded the program to other long-term care settings, provided various legal protections for the ombudsmen themselves, established the National Long-Term Care Ombudsman Resource Center,9 and required all ombudsmen to participate in training provided by that center. In 2016, the State Long-Term Care Ombudsman Programs Final Rule provided guidance for operating state-based programs, including defining the responsibilities of key figures and entities, criteria and roles for approaches to resolving complaints, and conflicts of interest (ACL, 2021b; NASUAD, 2019). Today, the Long-Term Care Ombudsman Program has an official Office of the State Long-Term Care Ombudsman in all U.S. states, the District of Columbia, Puerto Rico, and Guam (ACL, 2021b). By statute, ombudsmen are required to
- Identify, investigate, and resolve complaints made by or on behalf of residents;
- Provide information to residents about long-term services and supports;
- Ensure that residents have regular and timely access to ombudsman services;
- Represent the interests of residents before governmental agencies and seek administrative, legal, and other remedies to protect residents; and
- Analyze, comment on, and recommend changes in laws and regulations pertaining to the health, safety, welfare, and rights of residents (ACL, 2021b).
___________________
9 For more information, see https://ltcombudsman.org (accessed August 16, 2021).
Structure and Funding of Long-Term Care Ombudsman Programs
The Administration for Community Living provides grants to each State Unit on Aging to develop an annual state plan for its long-term care ombudsman program and establish an Office of the State Long-Term Care Ombudsman. The state ombudsman administers the state program and oversees designated representatives of the state office who serve as local staff as well as volunteers (NORC, 2019); long-term care ombudsman programs often have few paid staff at the state and local level, with volunteers conducting most of their activities (Berish et al., 2019). In FY 2017, the program overall had 1,319 full-time paid staff and 8,810 total volunteers (NORC, 2019). Having a lower full-time staff to facility ratio correlates with a higher percentage of facilities being visited at least quarterly. Expenditures on these programs totaled $106.7 million across all funding sources in FY 2017; the federal government provided 50 percent, states provided 43 percent, and local governments 7 percent of this funding (NORC, 2019).
While regulations require state units on aging to ensure that the ombudsman programs have sufficient resources and protections to conduct their legislatively mandated functions, there is considerable variation in the amount of resources, funding, and staffing among all programs, with limited funding affecting many programs’ abilities to meet federal mandates. For example,
- Only 23 percent of state ombudsmen report having sufficient financial resources,
- Only 27 percent of state ombudsmen report having sufficient staff,
- Only 15 percent of state ombudsmen report having enough volunteers, and
- Only 56 percent of state ombudsmen report having adequate legal counsel (NORC, 2019).
At least half of state ombudsmen report that a lack of resources hinders their ability to fully conduct the following activities: recruitment and retention of volunteers, development and support of resident and family council development and support, community education, legal assistance for residents, and regular nursing home visits (NORC, 2019).
Extent of Services
In FY 2017, ombudsmen visited 68 percent of all nursing homes on at least a quarterly basis for routine visits and, when also including complaint investigations, 79 percent of nursing homes (NORC, 2019). While state ombudsmen do some onsite visits, they are primarily responsible for overseeing the program, and local and volunteer ombudsmen
TABLE 8-4 Services Provided by Long-Term Care Ombudsmen and Level of Activity, FY 2017
| Services Provided by Long-Term Care Ombudsmen | Level of Activity in FY 2017 |
|---|---|
| Complaints | 201,460* |
| Provision of information to individuals and staff | 529,098 |
| Attendance at resident and family council meetings | 22,999 |
| Community education sessions | 10,170 |
SOURCE: NORC, 2019.
NOTES: *The top three categories for complaints are discharge/eviction, failure to respond to requests for assistance, and issues related to dignity and respect. Complaints were most often received from residents (40 percent), nursing home staff (19 percent), and relatives and friends (18 percent).
typically perform the in-person visits (NORC, 2019). Among the paid state ombudsmen who reported visiting nursing homes, 45 percent did so on a routine basis, compared with 81 percent of local ombudsmen and 95 percent of volunteer ombudsmen (NORC, 2019). Table 8-4 above provides an overview of the extent of services provided by ombudsmen to nursing home residents in 2017.
Evidence of Impact
Although few rigorous studies have quantified the program’s impact, researchers have noted that the “existence of a local [long-term care ombudsman program] is a significant predictor of quality of care, suggesting a positive preventative presence,” (Estes et al., 2010, p. 775) especially given the modest investment of governmental resources (Hollister and Estes, 2013). The presence of an ombudsman has been associated with increased levels of complaints and deficiency citations, which suggests that ombudsmen are able to bring more issues to the attention of surveyors; additionally, ombudsman are more likely to be present at surveys of nursing homes with persistently poorer quality (Berish et al., 2019). Studies have found that the effectiveness of ombudsmen increases significantly with more autonomy and investment of resources, including funding; a larger number of paid staff; and minimum staffing requirements, smaller case-loads, and higher percentages of nursing facilities visited (Estes et al., 2004).
Seventy-eight percent of volunteer ombudsmen, but only 51 percent of state ombudsmen and 66 percent of local ombudsmen, report that the majority of their relationships in nursing homes are effective (NORC, 2019). The volunteers attributed this effectiveness to “the ongoing presence they maintain in facilities and the positive working relationships they develop with facility staff who come to view them as a resource” (NORC, 2019).
Local ombudsman also reported that “their knowledge, confidence and experience level are crucial factors in determining the effectiveness of their relationships with facility staff” (NORC, 2019).
RESIDENT AND FAMILY COUNCILS
As described in Chapter 4, resident and family councils are independent groups for residents and families to discuss and address any issues or concerns within a facility. The primary goal of such councils is to improve the quality of care and life within nursing homes (Grant, 2021). Additionally, councils meet to discuss issues and policies that affect resident care, plan activities, provide education, and serve as a bridge between residents and the facility, among other activities (Grant, 2021; LTCCC, 2017).
OBRA 87 first included regulatory requirements for family and resident councils. The act requires facilities to10
- Provide existing councils with private meeting spaces,
- Designate a staff person to assist with council requests, and
- Respond to concerns and recommendations of the council regarding resident care and quality of life (Legal Aid Justice Center, 2013).
The 2016 federal regulations updated and strengthened the requirements for these councils. Specifically, the new 2016 regulations updated the requirements concerning resident and family councils with the following:11
- Residents must invite their families/individuals to participate in the councils;
- Councils must include people beyond family members, called resident representatives, if a resident chooses;
- Residents themselves can participate in the councils;
- The facility and council must both approve the designated staff person;
- The facility must make residents, family members, and resident representatives aware of upcoming council meetings in a way that the council approves;
- The facility must act promptly upon grievances and recommendations from the council and provide a rationale for their response (Justice in Aging, National Consumer Voice, and CMA, 2021; National Consumer Voice, 2017).
For more on resident and family councils, see Box 4-7 in Chapter 4.
___________________
10 Omnibus Budget Reconciliation Act of 1987, Public Law 100-203; 42 USC §1396r(c).
11 CMS Requirements for Long Term Care Facilities—Resident Rights, 42 CFR § 483.10 (2016).
EFFECTIVENESS OF QUALITY ASSURANCE FOR IMPROVING THE QUALITY OF CARE
Despite the prominent role of nursing home oversight and regulation, there is relatively modest evidence concerning its effectiveness in ensuring a minimum standard of quality. Much of the evidence is observational and follows the national implementation of OBRA 87. Measuring how well nursing home oversight activities minimize poor-quality care is challenging, not only because all U.S. nursing homes are subject to the same minimum federal standards, but also because of the many other changes that have occurred in the nursing home sector over the decades since OBRA 87 was passed. With this caveat, many studies have documented improvements in resident outcomes and care practices in the years following the implementation of OBRA 87. Nursing home regulations seem particularly effective at improving quality in certain easily measured and discrete categories. For example, in the years following OBRA 87, there was a substantial decrease in the use of restraints and catheters; reductions in dehydration rates and pressure ulcers; more discussions between residents and care providers about care plans, end-of-life plans, and other issues; and increased overall staffing levels (Fashaw et al., 2020; Hawes, 1996; Hawes et al., 1997; HCFA, 1998; IOM, 1996; Wiener et al., 2007; Zhang and Grabowski, 2004). Although notable improvements in care practices and selected quality measures followed the implementation of OBRA 87, nursing home care still demonstrates persistent quality challenges, at least among a subset of facilities. It is unclear whether these recurring challenges reflect inadequate implementation and enforcement of existing standards (as described earlier in this chapter) or deeper limitations in what quality-directed regulation can achieve.
Regulation specifies that the role of the federal government is to ensure the requirements of participation are enforced and “are adequate to protect the health, safety, welfare, and rights of residents and to promote the effective and efficient use of public moneys.”12 (See later in this chapter for more on transparency related to the financing of nursing home care.) It is difficult to calculate the total costs to federal and state governments of regulating nursing homes, and few studies have done so. A 2001 study estimated the annual costs of the nursing home survey and certification process at $382 million, or $22,000 per home (Walshe, 2001). After accounting for inflation and other changes in the nursing home sector over the past two decades, the direct costs to the government today are likely to be considerably higher. Moreover, in addition to the costs of regulation for government,
___________________
12 Nursing Home Reform Law of 1987, Public Law 100-203, 42 USC 1395i-3(f)(1), 100th Cong., 1st sess. (December 22, 1987).
the direct and indirect costs of regulatory oversight to nursing homes are important to consider against the benefits to residents’ quality of care and quality of life (Mor, 2011; Mukamel et al., 2011, 2012, 2014; Stevenson, 2019). Some of the only research in this area found that greater regulatory stringency was significantly associated with better quality for four of seven quality measures studied and that the cost-effectiveness for the activities of daily living measure in particular was estimated to be around $72,000 per quality-adjusted life year in 2011 (Mukamel et al., 2012).
Most resident advocates and nursing home providers are dissatisfied with the effectiveness of the current nursing home regulatory model, yet little consensus exists on how to improve the system (Stevenson, 2018). Nursing home advocates highlight the fact that, as noted earlier, existing regulations are often not being completely and consistently enforced and suggest that additional regulations need to be put in place to fully protect residents. Alternatively, many providers believe that the existing regulations are excessive and impede innovation and good-quality care. Unlike other areas of nursing home care, little common ground exists between the two groups. The lack of empirical evidence to guide policy makers is a further barrier to progress.
TRANSPARENCY AND ACCOUNTABILITY
A key aim of nursing home oversight over the past decade has been to ensure greater transparency in ownership and financing. Most nursing homes have been for-profit entities for decades. In the early 2000s, increased private equity investment and ownership complexity spurred a renewed focus on this topic (Duhigg, 2007; Stevenson and Grabowski, 2008), culminating with the ACA including provisions to encourage the disclosure of ownership and financial relationships (KFF, 2013). Still, it is clear that such transparency has not occurred. The committee recognizes that these issues are prevalent across the entire health care system, and not limited to nursing homes. However, the following sections highlight the implications of this lack of transparency on improving the quality of nursing home care.
Nursing Home Ownership
Nursing homes can be classified as either for-profit, nonprofit, or government-owned nursing homes. As Chapter 2 notes, 69.3 percent of nursing homes are for-profit entities, and nearly 60 percent are affiliated with companies that own or operate more than one nursing home (chain ownership) (Harris-Kojetin et al., 2019).
Despite important nuances related to the case mix of certain nursing homes and nursing home chains, the literature suggests that, in general,
for-profit nursing homes consistently demonstrate lower levels of quality, including satisfaction with care, than not-for-profit nursing homes (Banaszak-Holl et al., 2002; Comondore et al., 2009; GAO, 2011b; Grabowski and Hirth, 2003; Grabowski et al., 2013; Harrington et al., 2001; Hillmer et al., 2005; Stevenson and Grabowski, 2008; You et al., 2016). For example, for-profit nursing homes, compared with nonprofit or government-owned nursing homes, have been associated with fewer registered nurse and total nurse staffing hours, fewer nurses per resident, and more deficiencies (Harrington et al., 2012; O’Neill et al., 2003; Rau and Lucas, 2018). In addition, nursing homes designated as SFFs are more likely to be for-profit facilities or part of a chain (GAO, 2009d). Studies suggest a possible association between for-profit ownership and higher rates of COVID-19 cases and deaths (as compared to nonprofit or government-owned nursing homes) (Bach-Mortensen et al., 2021; Ochieng et al., 2021).The relationship between quality of care and ownership status has also been observed when for-profit nursing homes convert to not-for-profit ownership and subsequently demonstrate improvements in quality, nonprofit nursing homes convert to for-profit and show a decline in performance (Grabowski and Stevenson, 2008), or chains are purchased by private equity companies (Harrington et al., 2012).
Data from the first 5 years (2009–2013) of the five-star rating system reveal that for-profit nursing homes had lower ratings than the nonprofit and government-owned nursing homes (Abt Associates Inc., 2014). “Indeed nearly twice as many non-profit as for-profit nursing homes a five-star overall quality rating (35.6 percent vs. 19.7 percent)” (Abt Associates Inc., 2014, p. 8). Furthermore, only 5.7 percent of for-profit nursing homes received five stars in the staffing domain, compared to 21 percent of nonprofit nursing homes and 26 percent of government-owned nursing homes. (See Chapter 3 for more on the five-star quality rating.) Nursing home chains are more likely to acquire nursing homes of lower quality, and these quality problems persist after the acquisition (Grabowski et al., 2016).
One challenge associated with chain ownership is that chain owners may have pressures to prioritize corporate interests over the residents’ needs (Banaszak-Holl et al., 2002; Harrington et al., 2001; You et al., 2016). Beyond chain ownership, nursing home ownership has become more complex over the past few decades. For example, private equity ownership and real estate investment trusts (REITs) have been expanding in health care, including among nursing homes (Cockburn, 2020; Finn, 2020; GAO, 2010c; Harrington et al., 2017, 2021; Stevenson and Grabowski, 2008). Private equity ownership of nursing homes has been associated with higher short-term mortality; lower measures of well-being, such as mobility; higher numbers of total deficiencies; lower total nurse staffing ratios (i.e., fewer hours per resident day); and increased costs (Braun et al., 2021; GAO, 2011b; Gupta et al., 2021). Private equity ownership of nursing homes has
also been associated with a lower likelihood of having adequate supply of personal protective equipment (PPE) (Braun et al., 2020). Private equity and REIT engagement helped fuel a restructuring in how nursing home companies are organized. Harrington and colleagues (2021) found that
Many nursing homes separated their operating companies from their asset and property companies in an effort to shield parent companies from liability and reduce regulatory oversight. Real estate investment companies (REITs) have dramatically expanded their ownership since the Housing and Economic Recovery Act of 2008 allowed REITs to buy health care facilities. These companies lease their facilities and property to nursing home operating companies at sometimes exorbitant rents.
Given the influence of ownership status on the quality of care in nursing homes, enhanced transparency regarding the details of ownership, including corporate structure and spending priorities, would provide important insights. Nursing homes are required to report certain details about their ownership structures, which is captured in CMS’s Provider Enrollment Chain and Ownership System (PECOS). However, PECOS data are incomplete and somewhat difficult for consumers, payers, regulators, and others to use (GAO, 2010c). Furthermore, CMS does not audit the data for accuracy and has not enforced reporting requirements related to the nursing home’s organization (e.g., parent companies, related-party entities) (Harrington et al., 2021).
As discussed earlier in this chapter, the assurance of nursing home quality centers largely on public-sector oversight through licensure and certification. The focus of these efforts is on whether an individual nursing home is performing acceptably. When problems are present, the nursing home must make corrections or, in cases of extremely deficient care, a nursing home may face a range of sanctions (or, rarely, lose its certification to serve Medicare or Medicaid residents). However, with some exceptions (e.g., fraud and abuse), regulatory policy focuses on and sanctions the facility-level provider rather than looking at performance across nursing homes with a common owner or management company. Similarly, information available on Care Compare, including the five-star rating system, is all at the level of the individual facility (see Chapter 3). Consumers, payers, regulators, and others could benefit from a readily available capacity to examine facilities and other related entities in which owners have a stake. Publicly available ownership information needs to reflect and capture the complexity of today’s nursing home sector (e.g., operations, ownership structures) to enable tracking quality across nursing homes with a common owner, understand which entities are responsible for care, and determine which entities are benefiting from Medicare and Medicaid payments or favorable tax policies that might further entice them into the sector (e.g., REIT investors).
Financing
Quality assurance efforts have not focused extensively on the potential labyrinth of financial ties that shape what facilities are able to do, including how they are able to respond during a crisis. For example, while many for-profit nursing homes receive funds from the federal government (i.e., CMS), there are no specific requirements for how these funds are spent (in spite of the federal government’s responsibility, noted earlier, in overseeing how public funds are spent). Improving the ability to understand where nursing homes spend their resources and gaining a more accurate sense of their overall financial well-being are essential elements of transparency. Progress has been made in simplifying nursing home cost reporting, yet substantial questions remain regarding the accuracy and completeness of these data (GAO, 2016). In fact, a significant lack of transparency characterizes the overall state of nursing home financing.
While nursing homes report low operating margins, with potential negative impacts on patient care and quality, some are using third-party transactions or unrelated business entities to hide profits (Cenziper et al., 2020; Harrington et al., 2015, 2021; Rau, 2017, 2018b). For example, a case study of a for-profit nursing home chain in California found that “the chain’s complex, interlocking individual and corporate owners and property companies obscured its ownership structure and financial arrangements” (Harrington et al., 2015, p. 779). In addition, it has become more apparent over the last few decades that nursing homes’ real estate assets are central to the entities that choose to invest in this sector. Furthermore, the engagement of private equity and REITs is fueled by the tax advantages of these arrangements, including their potential role in operating facilities.
Moreover, Rau (2017) reported that owners of nursing homes “outsource a wide variety of goods and services to companies in which they have a financial interest or that they control” through related-party transactions, sometimes at prices that are well over the market rates in order to accrue higher profits that nursing homes do not record in their financial accounts. In 2018, Rau reported that related party transactions accounted for $11 billion in nursing home expenditures in 2015 (one-tenth of their costs) and that “homes with related companies were fined 22 percent more often for serious health violations than independent homes” (Rau, 2018b); nursing homes that outsource to related organizations tend to have lower staffing levels, higher rates of patient injuries and unsafe practices, and almost twice as many complaints as independent homes (Rau, 2017).
Evidence suggests that this outsourcing practice may be widespread. A 2009 study from the Office of the Assistant Secretary for Planning and Evaluation, for example, found that an increasing number of nursing homes were changing hands to regionally focused private-investment-owned facilities that increasingly used limited liability corporation structures and
partnership structures, such as general partnerships and limited partnerships (ASPE, 2009). Owners had also arranged for additional corporations to create layers in between themselves and their nursing homes, an arrangement that replaced previous basic for-profit and not-for-profit owner-operator structures (ASPE, 2009; Stevenson et al., 2013b). For a family member perspective on nursing home ownership and financing, see Box 8-5.
The lack of transparency or accountability in payment, funds flow, and nursing home finances makes it extremely difficult to assess the adequacy of current Medicaid payments. (See Chapter 7 for more on financing of nursing homes.) Though it is not an illegal practice, advocates have raised concerns that nursing home operators may use public Medicare and Medicaid funds to cover non-direct-care services (e.g., administrative costs) and earn significant profit while reporting low margins (LTCCC, 2021). For example, in the aforementioned case study of a California for-profit nursing home chain, the authors found that “profits were hidden in the chain’s management fees, lease agreements, interest payments to owners, and purchases from related-party companies” (Harrington et al., 2015, p. 779). Furthermore, despite claims of financial challenges during the COVID-19 pandemic, one analysis of 11 publicly traded nursing home companies found that they had suffered relatively little financial impact (Kingsley and Harrington, 2021).
Consolidated annual reports that include data from operators and entities related by common ownership or management could help provide greater transparency and financial accountability needed to improve regulatory oversight (Harrington et al., 2021). For example, in 2021, California passed legislation requiring such a report, including information about the owner/operator and all related parties that have an ownership or control
interest of 5 percent or more and provide any service, facility, or supply to the nursing home (Grajeda and Yood, 2021). Sponsors of the legislation argued that large, for-profit nursing homes were “using complex ownership structures to increase profitability by shielding funds behind the corporate family so that these funds cannot be fully considered by the state when it sets rates and reimbursements for care” and that the reports would allow the state to evaluate if nursing homes were diverting revenues into related entities rather than directing the funds toward resident care (Grajeda and Yood, 2021).
NURSING HOME OVERSIGHT DURING COVID-19
The threat posed by COVID-19 resulted in a different approach to oversight. More immediate and effective regulation could have helped guide facilities to better protect nursing home residents, staff, and families. For example, CMS did not require routine COVID-19 testing until 6 months after the pandemic started, facilities did not have access to a reliable supply of PPE, and no state imposed limitations on part-time or agency staff who visited multiple facilities (Kohn, 2021). Chronic underenforcement (i.e., lack of proper identification of deficiencies and imposition of penalties) exacerbated these problems. In fact, at the start of the pandemic, per-day fines for noncompliance were replaced with per-instance fines, key requirements were waived, and nursing homes restricted access to surveyors and ombudsmen (Kohn, 2021).
To limit the spread of COVID-19 in nursing homes, outside visitation by anyone other than essential health care personnel (including family, surveyors, and ombudsmen) was restricted (except in some very limited circumstances), and group activities and communal dining were eliminated. The initial CMS regulatory guidance emphasized flexibility and prioritized protecting residents over compliance with certain regulations. For example, CMS temporarily suspended specific reporting requirements such as resident assessment and staffing data, and it also waived some requirements related to residents’ rights in the name of physical safety (Stevenson and Bonner, 2020; Stevenson and Cheng, 2021). CMS also directed state survey agencies to stop regular inspection efforts and instead focus inspection efforts on infection control and investigating allegations of immediate jeopardy to residents (CMS, 2020a,b; 2021f). See Figure 8-2 for CMS guidance changes early in the pandemic.
Regulators had a difficult balance to strike during the public health emergency—“maintaining general protections and accountability while ensuring that nursing homes had sufficient flexibility and resources to meet residents’ needs” (Stevenson and Bonner, 2020). Early in the pandemic, these steps were seen as essential for resident safety, but the repercussions
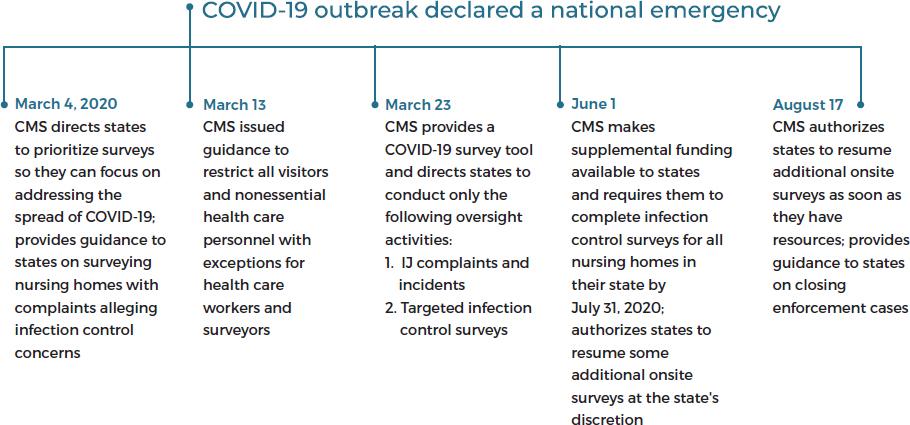
SOURCE: OIG, 2020b.
of these actions were substantial and carried separate harms of their own (Dolan and Mejia, 2020a; Mo and Shi, 2020; Montgomery et al., 2020; Rodney et al., 2021). Disaster planning focused on the physical safety of residents and overlooked other aspects of psychosocial well-being. The sudden loss of connections to family, friends, and volunteers and the new barriers to health and social services staff undercut modern expectations for high-quality nursing home care. For example, findings from a national survey revealed that 76 percent of nursing home residents felt lonelier than usual and 64 percent did not even leave their rooms to socialize (Montgomery et al., 2020). Families expressed concern that their loved ones in nursing homes seemed more lethargic, had worse physical health, and stopped smiling and laughing amidst the visitation restrictions and reduced oversight (HRW, 2021; Nash et al., 2021). For family member perspectives on the impact of visitation policies during the COVID-19 pandemic, see Box 8-6. (See Chapters 2 and 4 for more on social isolation and loneliness during the pandemic.)
As a result of this guidance, surveys were less thorough, and there were fewer documented complaints from ombudsman, families, and residents (OIG, 2020b; Stevenson and Cheng, 2021). In fact, “Deficiency citations generally decreased to near zero by April 2020 with the exception of infection prevention and control deficiencies and citations for failure to report COVID-19 data to the national health safety network” (Stevenson and Cheng, 2021). Consequently, nursing homes were not being held liable or accountable for deficiencies, such as understaffing (Kohn, 2021). Backlogs for standard surveys grew exponentially during the pandemic,
ranging from 22 to 96 percent of nursing homes by state (with a national average of 71 percent) going without a standard survey for at least 16 months from February 1, 2020, through May 31, 2021 (OIG, 2021). Furthermore, investigative reports drew attention to cases of inappropriate evictions and unsafe transfers of older adults and people with disabilities from nursing homes, many to homeless shelters, ostensibly as a way to make room for more lucrative short-stay residents with COVID-19 coming from hospitals (Dolan and Mejia, 2020b; Silver-Greenberg and Harris, 2020).
With facilities in lockdown, oversight was needed to ensure not only the adequacy of infection controls but the quality of resident care more generally. Quality assurance was challenging before the pandemic, and the “significantly scaled back oversight and data reporting was concerning, even if temporary” (Stevenson and Bonner, 2020). For example, problem facilities such as SFFs still needed to be monitored for general quality, but guidance did not prioritize or distinguish the continued need for enhanced oversight of these facilities during the pandemic.
Careful emergency planning and regulatory changes can help facilities better respond to emergencies—both event-specific emergencies such as hurricanes, but also broader and longer-lasting public health emergencies, such as COVID-19—and prevent such disproportionate devastation on nursing home communities in the future. (See Chapter 6 for more on emergency planning.) Contingency plans to address the lack of PPE and
in-person visitation “should be viewed as essential for bolstering care oversight, residents’ mental and physical health, and delivering high quality care” (Stevenson and Cheng, 2021). This may include options such as virtual monitoring activities, equipping facilities with PPE resources and technology for safe in-person or virtual visitation, and improving data collection and communication between facilities and regulatory bodies (Stevenson and Bonner, 2020; Stevenson and Cheng, 2021). Maintaining regulatory activities, transparency, and oversight will be a critical part of protecting residents’ health, well-being, and quality of life during future emergencies.
KEY FINDINGS AND CONCLUSIONS
General Oversight and Regulation
- While substantial changes have occurred in nursing home care since the implementation of OBRA 87 regulations, the general structure of the oversight and regulation of nursing homes has largely remained the same.
- The oversight and enforcement of nursing home rules were scaled back in 2017 as part of a broader movement to reduce bureaucracy and government intervention.
- Requirements of participation provide the primary focus for regulation and cover a range of dimensions, such as residents’ rights, quality of care, quality of life, and the physical environment.
- States have the primary responsibility for licensure of nursing home providers as a way to control the market, but few facilities have been denied licensure.
- Certificate-of-need regulations and construction moratoria do not appear to have had their intended effect of holding down Medicaid nursing home spending; rather, these laws can discourage innovation and decrease access.
- Certificate-of-need regulations may contribute to the perpetuation of larger nursing homes.
- Despite the prominent role of nursing home oversight and regulation, the evidence base for its effectiveness in ensuring a minimum standard of quality is relatively modest.
- Many resident advocates and nursing home providers are dissatisfied with the effectiveness of the current nursing home regulatory model. Yet, little consensus exists on how to improve the system.
State Surveys and Sanctions
- States assist with the assessment of facilities’ compliance with requirements of participation and, as necessary, with the investigation of complaints and adverse incidents. States have some discretion in how they administer these responsibilities, but all states are expected to adhere to the detailed protocols outlined in the State Operations Manual.
- Nursing home oversight in the United States is largely a standardized process, with almost all facilities inspected for compliance with the same standards on a roughly annual basis. However, there is considerable variation in processes and outcomes in the implementation of routine inspection responsibilities, in the imposition of sanctions, and in the investigation of complaints.
- There is some evidence that states have difficulty finding qualified surveyors, and limited evidence on the quality of training and effectiveness of state surveyors.
- CMS and state survey agencies can levy a range of sanctions against out-of-compliance nursing homes, but the imposition of CMPs is most common.
- State survey agencies may not have adequate capacity or resources to fulfill all their responsibilities.
- Decades of evidence document failures in the survey process to properly identify serious care problems, to fully correct and prevent recurrence of identified problems, to investigate complaints in a timely manner, and in CMS’s oversight of these surveys.
- CMS is able to impose remedies or sanctions if a state is found to have performed inadequately, but CMS does not fully track performance and rarely imposes formal sanctions.
- While the current regulatory process needs significant improvement, particularly in relation to the uneven enforcement of regulations, there is a dearth of evidence to suggest which approaches would ultimately lead to improvement in the quality of care.
- Real-time metrics need to be used in the testing of new approaches to surveys (e.g., changed frequency) in order to monitor for signals of decreasing quality.
- The budget of the SFF program allows for oversight of only a very small fraction of low-performing nursing homes, and many facilities that graduate from the program fail to sustain improvement.
Long-Term Care Ombudsman Program
- There is considerable variation in the resources, funding, and staffing among ombudsman programs, and limited funding affects programs’ abilities to meet federal and state requirements and to fully
- provide nursing home residents and their families with the best support possible.
- The impact of the Long-Term Care Ombudsman Program has been largely positive, especially given the modest investment of governmental resources.
Transparency and Accountability
- Current data sources provide little insight into the corporate structure, finances, and operations of individual nursing homes.
- In general, for-profit nursing homes consistently demonstrate lower levels of quality, including satisfaction with care, than not-for-profit nursing homes.
- Current data sources do not allow for an examination of performance across nursing homes by a common owner.
- Nursing homes may use related-party transactions or unrelated business entities to hide profits. There is a lack of transparency regarding these transactions.
- Progress has been made in simplifying nursing home cost reporting, yet there are still substantial questions about the accuracy and completeness of these data.
- Increased transparency and accountability of the finances, operations, and ownership of nursing homes is important for improving the financial investment in nursing home care as well as to improve quality assurance, all toward the common goal of improving the quality of care in nursing homes.
COVID-19
- During the pandemic, regulators had a difficult balance to strike—maintaining general protections and accountability while ensuring that nursing homes had sufficient flexibility and resources to meet residents’ needs.
- Early responses to the pandemic prioritized resident safety over other aspects of psychosocial well-being.
- Limiting visitation by family, surveyors, and ombudsmen affected the quality of care.
- CMS directed state survey agencies to scale back regular inspection efforts in order to focus on infection control and investigations of immediate jeopardy.
- Surveys were less thorough, and there were fewer documented complaints from ombudsman, families, and residents.
- During the COVID-19 pandemic, many states sought liability protections for nursing homes against pandemic-related claims of negligence.
- Maintaining regulatory activities, transparency, and oversight will be a critical part of protecting residents’ health, well-being, and quality of life during future emergencies.
REFERENCES
Abt Associates. 2014. Nursing home compare five-star quality rating system: Year five report [public version]. Baltimore, MD: Abt Associates Inc.
ACL (Administration for Community Living). 2021a. Older Americans Act. https://acl.gov/about-acl/authorizing-statutes/older-americans-act (accessed December 2, 2021).
ACL. 2021b. Long-Term Care Ombudsman Program. https://acl.gov/programs/Protecting-Rights-and-Preventing-Abuse/Long-term-Care-Ombudsman-Program (accessed August 19, 2021).
ASHE (American Society for Health Care Engineering). 2021. Deemed status. https://www.ashe.org/advocacy/orgs/deemedstatus (accessed September 2, 2021).
ASPE (Assistant Secretary for Planning and Evaluation). 2009. Nursing home ownership trends and their impact on quality of care. Washington, DC: HHS Office of the Assistant Secretary for Planning and Evaluation.
Associated Press. 2021. Critics say Indiana COVID-19 law allows nursing home neglect. NPR, May 8. https://www.wfyi.org/news/articles/critics-say-indiana-COVID-19-law-allows-nursing-home-neglect (accessed November 17, 2021).
Bach-Mortensen, A. M., B. Verboom, A. Movsisyan, and M. D. Esposti. 2021. A systematic review of the associations between care home ownership and COVID-19 outbreaks, infections and mortality. Nature Aging 1:948–961.
Banaszak-Holl, J., W. B. Berta, D. M. Bowman, J. A. Baum, and W. Mitchell. 2002. The rise of human service chains: Antecedents to acquisitions and their effects on the quality of care in U.S. nursing homes. Managerial and Decision Economics 23(4–5):261–282.
Berish, D. E., J. Bornstein, and J. R. Bowblis. 2019. The impact of long-term care ombudsman presence on nursing home survey deficiencies. Journal of the American Medical Directors Association 20(10):1325–1330.
Braithwaite, J., T. Makkai, and V. A. Braithwaite. 2007. Regulating aged care: Ritualism and the new pyramid. Cheltenham, UK: Edward Elgar Publishing.
Braun, R. T., H. Yun, L. P. Casalino, Z. Myslinski, F. M. Kuwonza, H. Jung, and M. A. Unruh. 2020. Comparative performance of private equity-owned U.S. nursing homes during the COVID-19 pandemic. JAMA Network Open 3(10). https://doi.org/10.1001/jamanetworkopen.2020.26702.
Braun, R. T., H. Jung, L. P. Casalino, Z. Myslinski, and M. A. Unruh. 2021. Association of private equity investments in U.S. nursing homes with the quality and cost of care for long-stay residents. JAMA Health Forum 2(11). https://doi.org/10.1001/jamahealthforum.2021.3817.
Brinker, P. A., and B. Walker. 1962. The Hill-Burton Act: 1948–1954. Review of Economics and Statistics 44(2):208–212.
Brooks, S., R. Grant, and M. F. Bonamarte. 2020. States move to shield LTC facilities from civil liability. Bifocal 41(6): July 6. https://www.americanbar.org/groups/law_aging/publications/bifocal/vol-41/vol-41--issue-no-6--july-august-2020-/states-move-to-shield-ltc-facilities-from-liability/ (accessed January 25, 2022).
Brown, D. 2021. Providers rejoice after receiving liability protections for nursing homes. McKnights Long-Term Care News, April 7. https://www.mcknights.com/news/providers-rejoice-after-receiving-liability-protections-for-nursing-homes (accessed November 17, 2021).
Bruneau, J. 2014. The great healthcare CON. https://fee.org/articles/the-great-healthcare-con (accessed February 4, 2022).
California State Auditor. 2014. California Department of Public Health: It has not effectively managed investigations of complaints related to long-term health care facilities: Report 2014-111. https://www.auditor.ca.gov/pdfs/reports/2014-111.pdf (accessed February 5, 2022).
California State Auditor. 2020. State high risk: The California State Auditor’s updated assessment of high-risk issues faced by the state and select state agencies. https://www.bsa.ca.gov/pdfs/reports/2019-601.pdf (accessed February 5, 2022).
Carlson, E. 2015. 20 common nursing home problems—and how to resolve them. https://www.waombudsman.org/files/2015/10/20CommonNurseHomeProblems.pdf (accessed November 16, 2021).
Castle, N. G., J. Engberg, and A. Men. 2007. Variation in the use of nursing home deficiency citations. Journal of Healthcare Quality 29(6):12–23.
Castle, N. G., L. M. Wagner, J. C. Ferguson, and S. M. Handler. 2011. Safety culture of nursing homes: Opinions of top managers. Health Care Management Review 36(2):175–187.
Cavanaugh, J., C. G. Brothers, A. Griffin, R. Hoover, M. LoPresti, and J. Wrench. 2020. Conning the competition: A nationwide survey of certificate of need laws. Arlington, VA: Institute for Justice.
Cenziper, D., J. Jacobs, A. Crites, and W. Englund. 2020. Profit and pain: How California’s largest nursing home chain amassed millions as scrutiny mounted. The Washington Post, December 31. https://www.washingtonpost.com/business/2020/12/31/brius-nursing-home (accessed November 8, 2021).
CMA (Center for Medicare Advocacy). 2019. Special report: “Graduates” from the Special Focus Facility Program provide poor care. https://medicareadvocacy.org/graduates-from-the-special-focus-facility-program-provided-poor-care (accessed February 5, 2022).
CMS (Centers for Medicare & Medicaid Services). 2008. Center for Medicaid and State Operations/Survey and Certification Group: Accreditation and its impact on various survey and certification scenarios. https://www.cms.gov/Medicare/Provider-Enrollmentand-Certification/SurveyCertificationGenInfo/downloads/SCLetter09-08.pdf (accessed September 2, 2021).
CMS. 2016. Chapter 7 state operations manual—Survey and enforcement process for skilled nursing facilities and nursing facilities. Washington, DC: Centers for Medicare & Medicaid Services.
CMS. 2017a. State operations manual: Appendix PP—Guidance to surveyors for long term care facilities. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/GuidanceforLawsAndRegulations/Downloads/Appendix-PP-State-Operations-Manual.pdf (accessed July 8, 2021).
CMS. 2017b. New long-term care survey process. https://www.cms.gov/Medicare/ProviderEnrollment-andCertification/GuidanceforLawsAndRegulations/Downloads/New-Long-term-Care-Survey-Process%E2%80%93Slide-Deck-andSpeaker-Notes.pptx (accessed February 1, 2022).
CMS. 2018a. Medicare and Medicaid programs; proposed regulatory provisions to promote program efficiency, transparency, and burden reduction. https://www.cms.gov/newsroom/fact-sheets/Medicare-and-Medicaid-programs-proposed-regulatory-provisions-promote-program-efficiency-0 (accessed March 4, 2019).
CMS. 2018b. State operations manual: Chapter 7—Survey and enforcement process for skilled nursing facilities and nursing facilities. https://www.cms.gov/regulations-and-guidance/guidance/manuals/downloads/som107c07pdf.pdf (accessed August 10, 2021).
CMS. 2019a. State operations manual: Chapter 4—Program administration and fiscal management. https://www.cms.gov/regulations-and-guidance/guidance/manuals/downloads/som107c04pdf.pdf (accessed November 9, 2021).
CMS. 2019b. State operations manual: Chapter 5—complaint procedures. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/som107c05pdf.pdf (accessed February 2, 2022).
CMS. 2019c. Examples of non-allowable uses of CMP reinvestment funds. Washington, DC: Centers for Medicare & Medicaid Services.
CMS. 2020a. Prioritization of survey activities. https://www.cms.gov/files/document/qso-2020-all.pdf (accessed January 12, 2022).
CMS. 2020b. Guidance for infection control and prevention of coronavirus disease 2019 (COVID-19) in nursing homes (revised). https://www.cms.gov/files/document/qso-2014-nh-revised.pdf (accessed November 15, 2021).
CMS. 2021a. Nursing homes. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/GuidanceforLawsAndRegulations/Nursing-Homes (accessed February 7, 2021).
CMS. 2021b. S&C’s Quality, Certification and Oversight Reports (QCOR). https://qcor.cms.gov/report_select.jsp?which=0 (accessed October 25, 2021).
CMS. 2021c. Civil Money Penalty Reinvestment Program. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/LTC-CMP-Reinvestment (accessed February 5, 2022).
CMS. 2021d. Special Focus Facility (“SFF”) program. https://www.cms.gov/Medicare/Provider-Enrollment-and-certification/CertificationandComplianc/downloads/sfflist.pdf (accessed April 29, 2021).
CMS, 2021e. Fiscal year (FY) 2020 state performance standards system (SPSS) findings, FY 2021 SPSS guidance, and FY 2019 results. https://www.cms.gov/files/document/admininfo-letter-21-08-all.pdf (accessed February 1, 2022).
CMS. 2021f. Prioritization of survey activities. https://www.cms.gov/files/document/qso-2020-allpdf.pdf-0 (accessed April 6, 2021).
CMS. 2022. Civil money penalty (CMP) report. https://qcor.cms.gov/nh_wizard.jsp?which=0&report=enf_cmp.jsp (accessed February 5, 2022).
Cockburn, A. 2020. Elder abuse: Nursing homes, the coronavirus, and the bottom line. https://harpers.org/archive/2020/09/elder-abuse-nursing-homes-covid-19 (accessed February 6, 2022).
Comondore, V. R., P. J. Devereaux, Q. Zhou, S. B. Stone, J. W. Busse, N. C. Ravindran, K. E. Burns, T. Haines, B. Stringer, D. J. Cook, S. D. Walter, T. Sullivan, O. Berwanger, M. Bhandari, S. Banglawala, J. N. Lavis, B. Patrisor, H. Schunemann, K. Walsh, N. Bhatnager, and G. H. Guyatt. 2009. Quality of care in for-profit and not-for-profit nursing homes: Systematic review and meta-analysis. BMJ 339:b2732.
Conover, C. J., and J. Bailey. 2020. Certificate of need laws: A systematic review and cost-effectiveness analysis. BMC Health Services Research 20:748.
Critchfield, H. 2021. Florida protected nursing homes from COVID lawsuits. Then cases began to spike. Tampa Bay Times, September 28. https://www.tampabay.com/news/health/2021/09/28/florida-protected-nursing-homes-from-COVID-lawsuits-then-cases-began-to-spike (accessed November 17, 2021).
DOJ (U.S. Department of Justice). 2014. Extendicare Health Services Inc. agrees to pay $38 million to settle False Claims Act allegations relating to the provision of substandard nursing care and medically unnecessary rehabilitation therapy. https://www.justice.gov/opa/pr/extendicare-health-services-inc-agrees-pay-38-million-settle-false-claims-act-allegations (accessed February 6, 2022).
DOJ. 2016. Nursing home chain to pay $5.3 million to resolve False Claims Act allegations. https://www.justice.gov/usao-ndtx/pr/nursing-home-chain-pay-53-million-resolve-false-claims-act-allegations (accessed February 6, 2022).
DOJ. 2020. Department of Justice launches a national nursing home initiative. https://www.justice.gov/opa/pr/department-justice-launches-national-nursing-home-initiative (accessed March 30, 2021).
DOJ and FTC (Federal Trade Commission). 2004. Improving health care: A dose of competition. https://www.ftc.gov/sites/default/files/documents/reports/improving-health-care-dose-competition-report-federal-trade-commission-and-department-justice/040723healthcarerpt.pdf (accessed February 4, 2022).
Dolan, J., and B. Mejia. 2020a. As coronavirus raged through nursing homes, inspectors found nothing wrong. https://www.latimes.com/california/story/2020-06-28/coronavirus-nursing-homes-state-inspector-covid-19 (accessed February 5, 2022).
Dolan, J., and B. Mejia. 2020b. Coronavirus patients could be cash cows for nursing homes. https://canhrnews.com/coronavirus-patients-could-be-cash-cows-for-nursing-homes (accessed February 5, 2022).
Duhigg, C. 2007. Nursing homes owned by private equity face U.S. inquiries. The New York Times, October 24. https://www.nytimes.com/2007/10/24/business/worldbusiness/24ihtnursing.4.8037461.html (accessed April 29, 2021).
Edelman, T. 2018. Corporate integrity agreements and nursing homes. https://medicareadvocacy.org/corporate-integrity-agreements-and-nursing-homes (accessed April 29, 2021).
Edelman, T. 2019. Annual surveys at nursing facilities are essential to protect residents. https://medicareadvocacy.org/annual-surveys-at-nursing-facilities-are-essential-to-protect-residents (accessed November 16, 2021).
Eijkelenboom, A., H. Verbeek, E. Felix, and J. van Hoof. 2017. Architectural factors influencing the sense of home in nursing homes: An operationalization for practice. Frontiers of Architectural Research 6(2):111–122.
Erickson, A. C. 2021. States are suspending certificate-of-need laws in the wake of COVID-19 but the damage might already be done. https://pacificlegal.org/certificate-of-need-laws-COVID-19 (accessed November 9, 2021).
Estes, C. L., D. M. Zulman, S. C. Goldberg, and D. D. Ogawa. 2004. State long term care ombudsman programs: Factors associated with perceived effectiveness. The Gerontologist 44(1):104–115.
Estes, C. L., S. P. Lohrer, S. Goldberg, B. R. Grossman, M. Nelson, M. J. Koren, and B. Hollister. 2010. Factors associated with perceived effectiveness of local long-term care ombudsman programs in New York and California. Journal of Aging and Health 22(6):772–803.
Fashaw, S. A., K. S. Thomas, E. McCreedy, and V. Mor. 2020. Thirty-year trends in nursing home composition and quality since the passage of the Omnibus Reconciliation Act. Journal of the American Medical Directors Association 21(2):233–239.
Fayissa, B., S. Alsaif, F. Mansour, T. E. Leonce, and F. G. Mixon, Jr. 2020. Certificate-of-need regulation and healthcare service quality: Evidence from the nursing home industry. Healthcare 8(4):423.
Feder, J., and W. Scanlon. 1980. Regulating the bed supply in nursing homes. Milbank Memorial Fund Quarterly: Health and Society 58(1):54–88.
Ferdows, N. B., and M. Rahman. 2020. Evolution of the nursing home industry in states with different certificate of need policies. Journal of the American Medical Directors Association 21(4):559–561.
Finn, I. 2020. U.S. nursing homes: A goldmine for real estate and private equity firms. https://www.wsws.org/en/articles/2020/04/27/nur2-a27.html (accessed February 6, 2022).
Furrow, B. R., T. L. Greaney, S. H. Johnson, T. S. Jost, and R. L. Schwartz. 2008. Health law: Cases, materials and problems. St. Paul, MN: West Publishing.
GAO (U.S. Government Accountability Office). 1997. Long-term care: Consumer protection and quality-of-care issues in assisted living. Washington, DC: U.S. Government Accountability Office.
GAO. 1999. Nursing home care: Enhanced HCFA oversight of state programs would better ensure quality. Washington, DC: U.S. Government Accountability Office.
GAO. 2003. Nursing home quality: Prevalence of serious problems, while declining, reinforces importance of enhanced oversight. Washington, DC: U.S. Government Accountability Office.
GAO. 2005. Nursing homes: Despite increased oversight, challenges remain in ensuring high-quality care and resident safety. Washington, DC: U.S. Government Accountability Office.
GAO. 2007. Nursing homes: Efforts to strengthen federal enforcement have not deterred some homes from repeatedly harming residents. Washington, DC: U.S. Government Accountability Office.
GAO. 2008. Federal monitoring surveys demonstrate continued understatement of serious care problems and CMS oversight weakness. Washington, DC: U.S. Government Accountability Office.
GAO. 2009a. Nursing homes: Addressing the factors underlying understatement of serious care problems requires sustained CMS and state commitment. Washington, DC: U.S. Government Accountability Office.
GAO. 2009b. Medicare and Medicaid participating facilities: CMS needs to reexamine its approach for funding state oversight of health care facilities. Washington, DC: U.S. Government Accountability Office.
GAO. 2009c. Nursing homes: Opportunities exist to facilitate the use of the temporary management sanction. Washington, DC: U.S. Government Accountability Office.
GAO. 2009d. Nursing homes: CMS’s special focus facility methodology should better target the most poorly performing homes, which tended to be chain affiliated and for-profit. Washington, DC: U.S. Government Accountability Office.
GAO, 2010a. Poorly performing nursing homes: Special focus facilities are often improving, but CMS’s program could be strengthened. Washington, DC: U.S. Government Accountability Office.
GAO, 2010b. Nursing homes: Some improvement seen in understatement of serious deficiencies, but implications for the longer-term trend are unclear. Washington, DC: U.S. Government Accountability Office.
GAO, 2010c. Nursing homes: Complexity of private investment purchases demonstrates need for CMS to improve the usability and completeness of ownership data. Washington, DC: U.S. Government Accountability Office.
GAO. 2011a. Nursing homes: More reliable data and consistent guidance would improve CMS oversight of state complaint investigations. Washington, DC: U.S. Government Accountability Office.
GAO. 2011b. Nursing homes: Private investment homes sometimes differed from others in deficiencies, staffing, and financial performance. Washington, DC: U.S. Government Accountability Office.
GAO. 2016. Skilled nursing facilities: CMS should improve accessibility and reliability of expenditure data. Washington, DC: U.S. Government Accountability Office.
GAO. 2018. Nursing home quality: Continued improvements needed in CMS’s data and oversight. (GAO-18-694T):1-17. https://www.gao.gov/products/GAO-18-694T (accessed August 27, 2020).
GAO. 2019. Nursing homes: Improved oversight needed to better protect residents from abuse. Washington, DC: U.S. Government Accountability Office.
Gebeloff, R., K. Thomas, and J. Silver-Greenberg. 2021. How nursing homes’ worst offenses are hidden from the public. https://www.nytimes.com/2021/12/09/business/nursing-home-abuse-inspection.html?smid=em-share (accessed February 2, 2022).
Glans, M. 2015. Indiana nursing home moratorium. https://www.jamesmadison.org/the-heartland-institute-research-commentary-indiana-nursing-home-moratorium (accessed February 4, 2022).
Grabowski, D. C. 2007. Medicare and Medicaid: Conflicting incentives for long-term care. The Milbank Quarterly 85(4):579–610.
Grabowski, D. C., and D. G. Stevenson. 2008. Ownership conversions and nursing home performance. Health Services Research 43(4):1184–1203.
Grabowski, D. C. 2017. Nursing home certificate-of-need laws should be repealed. Health Affairs Forefront, June 9. https://www.healthaffairs.org/do/10.1377/hblog20170609.060529/full (accessed February 10, 2021).
Grabowski, D. C., and J. Gruber. 2007. Moral hazard in nursing home use. Journal of Health Economics 26(3):560–577.
Grabowski, D. C., and R. A. Hirth. 2003. Competitive spillovers across non-profit and for-profit nursing homes. Journal of Health Economics 22(1):1–22.
Grabowski, D. C., and D. G. Stevenson. 2006. Long-term care regulation. In R. Schulz (ed.), The encyclopedia of aging, 4th ed. New York: Springer Publishing. Pp. 701–704.
Grabowski, D. C., R. L. Ohsfeldt, and M. A. Morrisey. 2003. The effects of CON repeal on Medicaid nursing home and long-term care expenditures. Inquiry 40(2):146–157.
Grabowski, D. C., J. Gruber, and J. J. Angelelli. 2008. Nursing home quality as a common good. Review of Economics and Statistics 90(4):754–764.
Grabowski, D. C., Z. Feng, R. Hirth, M. Rahman, and V. Mor. 2013. Effect of nursing home ownership on the quality of post-acute care: An instrumental variables approach. Journal of Health Economics 32(1):12–21.
Grabowski, D. C., R. A. Hirth, O. Intrator, Y. Li, J. Richardson, D. G. Stevenson, Q. Zheng, and J. Banaszak-Holl. 2016. Low-quality nursing homes were more likely than other nursing homes to be bought or sold by chains in 1993–2010. Health Affairs 35(5):907–914.
Grajeda, H., and K. Yood. 2021. What price transparency? California SB 650 shines light on skilled nursing facility ownership while creating new reporting burdens for California skilled nursing facilities. https://www.jdsupra.com/legalnews/what-price-transparency-california-sb-3985939/ (accessed February 2, 2022).
Grant, R. 2021. Family guide to effective family councils. National Long-Term Care Ombudsman Resource Center and National Citizens’ Coalition for Nursing Home Reform. https://theconsumervoice.org/uploads/files/family-member/Guide-toEffective-FamilyCouncils.pdf (accessed August 5, 2021).
Gupta, A., S. T. Howell, C. Yannelis, and A. Gupta. 2021. Does private equity investment in healthcare benefit patients? Evidence from nursing homes. National Bureau of Economic Research working paper no. 28474. https://www.nber.org/papers/w28474 (accessed February 25, 2021).
Hall, S. M., C. R. Haper, and B. K. Steinwascher. 2020. Insight: Nursing homes face heightened criminal enforcement during COVID-19. Bloomberg Law, June 15. https://news.bloomberglaw.com/us-law-week/insight-nursing-homes-face-heightened-criminal-enforcement-during-COVID-19 (accessed March 30, 2021).
Hansen, K. E., K. Hyer, A. A. Holup, K. M. Smith, and B. J. Small. 2017. Analyses of complaints, investigations of allegations, and deficiency citations in United States nursing homes. Medical Care Research and Review 76(6): 736–757.
Harrar, S., J. Eaton, and H. Meyer. 2021. 10 steps to reform and improve nursing homes. https://www.aarp.org/caregiving/health/info-2021/steps-to-improve-nursing-homes (accessed January 13, 2021).
Harrington, C., S. Woolhandler, J. Mullan, H. Carrillo, and D. U. Himmelstein. 2001. Does investor ownership of nursing homes compromise the quality of care? American Journal of Public Health 91(9):1452–1455.
Harrington, C., T. Tsoukalas, C. Rudder, R. J. Mollot, and H. Carrillo. 2008. Variation in the use of federal and state civil money penalties for nursing homes. The Gerontologist 48(5):679–691.
Harrington, C., B. Olney, H. Carrillo, and T. Kang. 2012. Nurse staffing and deficiencies in the largest for-profit nursing home chains and chains owned by private equity companies. Health Services Research 47(1 Pt 1):106–128.
Harrington, C., L. Ross, and T. Kang. 2015. Hidden owners, hidden profits, and poor nursing home care: A case study. International Journal of Health Services 45(4):779–800.
Harrington, C., F. F. Jacobsen, J. Panos, A. Pollock, S. Sutaria, and M. Szebehely. 2017. Marketization in long-term care: A cross-country comparison of large for-profit nursing home chains. Health Services Insights 10:1–23.
Harrington, C., M. E. Dellefield, E. Halifax, M. L. Fleming, and D. Bakerjian. 2020. Appropriate nurse staffing levels for U.S. nursing homes. Health Services Insights 13:1–14.
Harrington, C., A. Montgomery, T. King, D. C. Grabowski, and M. Wasserman. 2021. These administrative actions would improve nursing home ownership and financial transparency in the post COVID-19 period. Health Affairs Forefront, February 11. https://www.healthaffairs.org/do/10.1377/hblog20210208.597573/full (accessed February 25, 2021).
Harris-Kojetin, L., M. Sengupta, J. P. Lendon, V. Rome, R. Valverde, and C. Caffrey. 2019. Long-term care providers and services users in the United States, 2015–2016. DHHS publication no. 2019-1427. https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf (accessed November 19, 2021).
Havighurst, C. C. 2005. Monopoly is not the answer. Health Affairs 24(Suppl1):W5-373–W5-375.
Hawes, C. 1996. Assuring nursing home quality: The history and impact of federal standards in OBRA-87. https://www.commonwealthfund.org/publications/fund-reports/1996/dec/assuring-nursing-home-quality-history-and-impact-federal (accessed February 10, 2021).
Hawes, C., V. Mor, C. D. Phillips, B. E. Fries, J. N. Morris, E. Steele-Friedlob, A. M. Greene, and M. Nennstiel. 1997. The OBRA-87 nursing home regulations and implementation of the resident assessment instrument: Effects on process quality. Journal of the American Geriatrics Society 45(8):977–985.
HCFA (Health Care Financing Administration). 1998. Report to Congress: Study of private accreditation (deeming) of nursing homes, regulatory incentives and non-regulatory initiatives, and effectiveness of the survey and certification system. https://ia801605.us.archive.org/3/items/reporttocongress00unit_11/reporttocongress00unit_11.pdf (accessed February 23, 2022).
Hillmer, M. P., W. P. Wodchis, S. S. Gill, G. M. Anderson, and P. A. Rochon. 2005. Nursing home profit status and quality of care: Is there any evidence of an association? Medical Care Research and Review 62(2):139–166.
Hollister, B. A., and C. L. Estes. 2013. Local long-term care ombudsman program effectiveness and the measurement of program resources. Journal of Applied Gerontology 32(6):708–728.
HRW (Human Rights Watch). 2021. U.S.: Concerns of neglect in nursing homes—Pandemic exposes need for improvements in staffing, oversight, accountability. https://www.hrw.org/news/2021/03/25/us-concerns-neglect-nursing-homes# (accessed September 8, 2021).
Hunt, S. S. 2008. History and role of the Long-Term Care Ombudsman Program. https://ltcombudsman.org/uploads/files/support/history-and-role.pdf (accessed May 7, 2021).
IOM (Institute of Medicine). 1986. Improving the quality of care in nursing homes. Washington, DC: National Academy Press.
IOM. 1996. Nursing staff in hospitals and nursing homes: Is it adequate? Washington, DC: National Academy Press.
IOM. 2001. Improving the quality of long-term care. Washington, DC: National Academy Press.
Jaffe, I. 2020. Ideal nursing homes: Individual rooms, better staffing, more accountability. NPR, May 21. https://www.npr.org/2020/05/21/855821083/ideal-nursing-homes-individual-rooms-better-staffing-more-accountability (accessed September 2, 2021).
Justice in Aging. 2020. Fighting the rollback of nursing home protections. https://justiceinaging.org/fighting-rollback-nursing-home-protections (accessed April 16, 2021).
Justice in Aging, National Consumer Voice, and CMA (Justice in Aging, the National Consumer Voice for Quality Long-Term Care, and the Center for Medicare Advocacy). 2021. A closer look at the revised nursing facility regulations: Grievances and resident/family councils. https://www.justiceinaging.org/wp-content/uploads/2017/05/Revised-Nursing-Facility-Regulations_Grievances-and-Resident-or-Family-Councils.pdf (accessed August 5, 2021).
Kapp, M. 2000. Quality of care and quality of life in nursing facilities: What’s regulation got to do with it? McGeorge Law Review 31:707–731.
KFF (Kaiser Family Foundation). 2013. Implementation of Affordable Care Act provisions to improve nursing home transparency, care quality, and abuse prevention. https://www.kff.org/medicaid/report/implementation-of-affordable-care-act-provisions-to-improve-nursing-home-transparency-care-quality-and-abuse-prevention (accessed February 10, 2021).
KFF. 2015. Long-term care in the United States: A timeline. https://www.kff.org/medicaid/timeline/long-term-care-in-the-united-states-a-timeline/#1978 (accessed October 23, 2020).
Kingsley, D. E., and C. Harrington. 2021. COVID-19 had little financial impact on publicly traded nursing home companies. American Geriatrics Society 69:2099–2102.
Kitchener, M., T. Ng, N. Miller, and C. Harrington. 2005. Medicaid and home and community-based services: National program trends. Health Affairs 24(1):206–212.
Klauber, M., and B. Wright. 2001. The 1987 Nursing Home Reform Act. https://www.aarp.org/home-garden/livable-communities/info-2001/the_1987_nursing_home_reform_act.html (accessed October 20, 2020).
Kohn, N. A. 2021. Nursing homes, COVID-19, and the consequences of regulatory failure. Georgetown Law Journal Online 110. https://www.law.georgetown.edu/georgetown-lawjournal/wp-content/uploads/sites/26/2021/04/Kohn_Nursing-Homes-COVID-19-and-the-Consequences-of-Regulatory-Failure.pdf (accessed January 25, 2022).
Konetzka, R. T., J. Park, R. Ellis, and E. Abbo. 2013. Malpractice litigation and nursing home quality of care. Health Services Research 48(6 Pt 1):1920–1938.
Konetzka, R. T., H. Daifeng, J. Dong, and J. A. Nyman. 2019. Moral hazard and long-term care insurance. The Geneva Papers on Risk and Insurance—Issues and Practice 44:231–251.
Kosar, C. M., and M. Rahman. 2021. Early acceleration of COVID-19 in areas with larger nursing homes and certificate of need laws. Journal of General Internal Medicine 36(4):990–997.
Landsberg, B. S., and T. D. Keville. 2001. Nursing homes face quality-of-care scrutiny under the False Claims Act. Healthcare Financial Management 55(1):54–58.
Lee, K., R. L. Mauldin, W. Tang, J. Connolly, J. Harwerth, and K. Magruder. 2021. Examining racial and ethnic disparities among older adults in long-term care facilities. The Gerontologist 61(6):858–869.
Legal Aid Justice Center. 2013. The rights of family councils in nursing homes. https://www.justice4all.org/wp-content/uploads/2013/05/Rights-of-Family-Councils.pdf (accessed August 10, 2021).
Levinson, D. R. 2017. Early alert: The Centers for Medicare & Medicaid Services has inadequate procedures to ensure that incidents of potential abuse or neglect at skilled nursing facilities are identified and reported in accordance with applicable requirements (A-01-17-00504). https://oig.hhs.gov/oas/reports/region1/11700504.pdf (accessed November 1, 2021).
Li, Y., C. Harrington, W. D. Spector, and D. B. Mukamel. 2010. State regulatory enforcement and nursing home termination from the Medicare and Medicaid programs. Health Services Research 45(6 Pt 1):1796–1814.
Li, Y., W. D. Spector, L. G. Glance, and D. B. Mukamel. 2012. State “technical assistance programs” for nursing home quality improvement: Variations and potential implications. Journal of Aging & Social Policy 24(4):349–367.
LTCCC (Long Term Care Community Coalition). 2017. Consumer factsheet: Resident & family councils. https://nursinghome411.org/wp-content/uploads/2017/05/LTCCC-Factsheet-Resident-Family-Councils.pdf (accessed August 5, 1997).
LTCCC. 2021. Nursing home Medicaid funding: Separating fact from fiction. https://nursinghome411.org/wp-content/uploads/2021/01/LTCCC-Policy-Brief-Medicaid-Funding-Facts-vs-Fiction.pdf (accessed November 17, 2021).
Mattimore, T. J., N. S. Wenger, N. A. Desbiens, J. M. Teno, M. B. Hamel, H. Liu, R. Califf, A. F. Connors, Jr., J. Lynn, and R. K. Oye. 1997. Surrogate and physician understanding of patients’ preferences for living permanently in a nursing home. Journal of the American Geriatrics Society 45(7):818–824.
Miller, N. A., C. Harrington, and E. Goldstein. 2002. Access to community-based long-term care: Medicaid’s role. Journal of Aging and Health 14(1):138–159.
Mitchell, M. D. 2017. Certificate-of-need laws: Are they achieving their goals? https://www.mercatus.org/system/files/mitchell-con-qa-mop-mercatus-v2.pdf (accessed November 9, 2021).
Mitchell, M. 2021. It’s time for states to ditch certificate-of-need laws. U.S. News and World Report, July 9. https://www.usnews.com/news/best-states/articles/2021-07-09/on-the-heels-of-the-pandemic-states-should-get-rid-of-certificate-of-need-laws (accessed November 9, 2021).
Mitchell, M. D., and C. Koopman. 2016. 40 years of certificate-of-need laws across America. https://www.mercatus.org/publications/corporate-welfare/40-years-certificate-need-laws-across-america (accessed February 4, 2022).
Mo, S., and J. Shi. 2020. The psychological consequences of the COVID-19 on residents and staff in nursing homes. Work, Aging and Retirement 6(4):254–259.
Montgomery, A., S. Slocum, and C. Stanik. 2020. Experiences of nursing home residents during the pandemic. https://altarum.org/sites/default/files/uploaded-publication-files/Nursing-Home-Resident-Survey_Altarum-Special-Report_FINAL.pdf (accessed October 22, 2020).
Mor, V. 2011. Cost of nursing home regulation: Building a research agenda. Medical Care 49(6):535–537.
Mukamel, D. B., Y. Li, C. Harrington, W. D. Spector, D. L. Weimer, and L. Bailey. 2011. Does state regulation of quality impose costs on nursing homes? Medical Care 49(6):529–534.
Mukamel, D. B., D. L. Weimer, C. Harrington, W. D. Spector, H. Ladd, and Y. Li. 2012. The effect of state regulatory stringency on nursing home quality. Health Services Research 47(5):1791–1813.
Mukamel, D. B., S. F. Haeder, and D. L. Weimer. 2014. Top-down and bottom-up approaches to health care quality: The impacts of regulation and report cards. Annual Review of Public Health 35(1):477–497.
Musumeci, M., and P. Chidambaram. 2020. Key questions about nursing home regulation and oversight in the wake of COVID-19. https://www.kff.org/coronavirus-COVID-19/issue-brief/key-questions-about-nursing-home-regulation-and-oversight-in-the-wake-of-COVID-19 (accessed December 7, 2020).
Nash, W. A., L. M. Harris, K. E. Heller, and B. D. Mitchell. 2021. “We are saving their bodies and destroying their souls”: Family caregivers’ experiences of formal care setting visitation restrictions during the COVID-19 pandemic. Journal of Aging & Social Policy 33(4–5):398–413.
Nastasi, V. 2020. Protecting Florida’s most vulnerable: Market-based reform to improve nursing home care. https://www.jamesmadison.org/wp-content/uploads/2021/01/Policy-Brief_Nursing_Homes_Dec2020_v02.pdf (accessed February 4, 2022).
NASUAD (National Association of States United for Aging and Disabilities, National Long-Term Care Ombudsman Resource Center, and National Consumer Voice for Quality Long-Term Care). 2019. State Long-Term Care Ombudsman Program: 2019 revised primer for state agencies. Washington, DC: National Association of States United for Aging and Disabilities, National Long-Term Care Ombudsman Resource Center, and National Consumer Voice for Quality Long-Term Care.
National Consumer Voice (The National Consumer Voice for Quality Long-Term Care). 2017. Factsheet: Resident council rights in nursing homes. https://theconsumervoice.org/uploads/files/long-term-care-recipient/Resident_Council_Rights_Fact_Sheet.pdf (accessed August 10, 2021).
National Consumer Voice. 2019. Side-by-side comparison of current & proposed federal nursing home regulations (including arbitration agreements). https://theconsumervoice.org/uploads/files/general/Side-by-Side_Comparison_of_Proposed_and_Current_ROP_8-2-2019.pdf (accessed August 10, 2021).
NCSL (National Conference of State Legislatures). 2021. Certificate of need (CON) state laws. https://www.ncsl.org/research/health/con-certificate-of-need-state-laws.aspx (accessed February 4, 2022).
NORC (NORC at the University of Chicago). 2019. Final report: Process evaluation of the Long-Term Care Ombudsman Program (LTCOP). https://acl.gov/sites/default/files/programs/2020-10/LTCOPProcessEvaluationFinalReport_2.pdf (accessed August 19, 2021).
Nyman, J. A. 1994. The effects of market concentration and excess demand on the price of nursing home care. Journal of Industrial Economics 42:193–204.
Ochieng, N., P. Chidambaram, R. Garfield, and T. Neuman. 2021. Factors associated with COVID-19 cases and deaths in long-term care facilities: Findings from a literature review. https://www.kff.org/coronavirus-covid-19/issue-brief/factors-associated-with-covid-19-cases-and-deaths-in-long-term-care-facilities-findings-from-a-literature-review (accessed February 1, 2022).
OIG (Office of the Inspector General). 1999. Nursing home survey and certification overall capacity. Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2003. Nursing home deficiency trends and survey and certification process consistency. Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2005. Nursing home enforcement: The use of civil money penalties. Washington, DC: HHS Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2006a. Nursing home enforcement: Application of mandatory remedies. Washington, DC: HHS Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2006b. Nursing home complaint investigations. Washington, DC: HHS Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2009. Nursing home corporations under quality of care corporate integrity agreements. Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2019a. Trends in nursing home complaints: Text-based data. https://oig.hhs.gov/oei/maps/2019-nursing-home/text-map.asp (accessed February 1, 2022).
OIG. 2019b. CMS guidance to state survey agencies on verifying correction of deficiencies needs to be improved to help ensure the health and safety of nursing home residents. Washington, DC: HHS Office of the Inspector General.
OIG. 2019c. Incidents of potential abuse and neglect at skilled nursing facilities were not always reported and investigated. Washington, DC: HHS Office of the Inspector General.
OIG. 2020a. States continued to fall short in meeting required timeframes for investigating nursing home complaints: 2016–2018. Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2020b. Onsite surveys of nursing homes during the COVID-19 pandemic: March 23–May 30, 2020 Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2021. States’ backlogs of standard surveys of nursing homes grew substantially during the COVID-19 pandemic: Addendum to oei-01-20-00430. Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2022a. CMS should take further action to address states with poor performance in conducting nursing home surveys. Washington, DC: Office of the Inspector General, U.S. Department of Health and Human Services.
OIG. 2022b. Corporate integrity agreements. https://oig.hhs.gov/compliance/corporate-integrity-agreements (accessed February 6, 2022).
O’Neill, C., C. Harrington, M. Kitchener, and D. Saliba. 2003. Quality of care in nursing homes: An analysis of relationships among profit, quality, and ownership. Medical Care 41(12):1318–1330.
Rahman, M., O. Galarraga, J. S. Zinn, D. C. Grabowski, and V. Mor. 2016. The impact of certificate-of-need laws on nursing home and home health care expenditures. Medical Care Research and Review 73(1):85–105.
Rau, J. 2017. Trump administration eases nursing home fines in victory for industry. The New York Times, December 24. https://www.nytimes.com/2017/12/24/business/trumpadministration-nursing-home-penalties.html (accessed April 29, 2021).
Rau, J. 2018a. “It’s almost like a ghost town.” Most nursing homes overstated staffing for years. The New York Times, August 7. https://www.nytimes.com/2018/07/07/health/nursing-homes-staffing-medicare.html (accessed April 29, 2021).
Rau, J. 2018b. Care suffers as more nursing homes feed money into corporate webs. The New York Times, January 2. https://www.nytimes.com/2018/01/02/business/nursing-homescare-corporate.html (accessed February 2, 2021).
Rau, J., and E. Lucas. 2018. 1,400 nursing homes get lower Medicare ratings because of staffing concerns. https://khn.org/news/1400-nursing-homes-get-lower-medicare-ratings-because-of-staffing-concerns (accessed February 6, 2022).
Reinhard, S. C., and E. Hado. 2021. LTSS choices: Small-house nursing homes. https://www.aarp.org/ppi/info-2021/ltss-choices-small-house-nursing-homes (accessed February 25, 2021).
Rodney, T., N. Josiah, and D.-L. Baptiste. 2021. Loneliness in the time of COVID-19: Impact on older adults. Journal of Advanced Nursing 77(9):e24–e26.
Schwarz, B. 1997. Nursing home design: A misguided architectural model. Journal of Architectural and Planning Research 14(4):343–359.
Shain, M., and M. I. Roemer. 1959. Hospital costs relate to the supply of beds. Modern Hospital 92(4):71–73.
Shugarman, L. R., and J. A. Brown. 2006. Nursing home selection: How do consumers choose? Volume I: Findings from Focus Groups of Consumers and Information Intermediaries. https://aspe.hhs.gov/basic-report/nursing-home-selection-how-do-consumers-choose-volume-i-findings-focus-groups-consumers-and-information-intermediaries (accessed February 25, 2021).
Silver-Greenberg, J., and R. Gebeloff. 2021. Maggots, rape and yet five stars: How U.S. ratings of nursing homes mislead the public. The New York Times, March 13. https://www.nytimes.com/2021/03/13/business/nursing-homes-ratings-Medicare-COVID.html?campaign_id=9&emc=edit_nn_20210313&instance_id=28051&nl=themorning®i_id=98348276&segment_id=53394&te=1&user_id=d3b6076e56d56335bd158430d6fd0d63 (accessed March 15, 2021).
Silver-Greenberg, J., and A. J. Harris. 2020. ‘They just dumped him like trash’: Nursing homes evict vulnerable residents. https://www.nytimes.com/2020/06/21/business/nursing-homes-evictions-discharges-coronavirus.html?action=click&module=Top%20Stories&pgtype=Homepage (accessed February 5, 2022).
Stevenson, D. G. 2006. Nursing home consumer complaints and quality of care: A national view. Medical Care Research and Review 63(3):347–368.
Stevenson, D. G. 2018. The future of nursing home regulation: Time for a conversation? https://www.healthaffairs.org/do/10.1377/hblog20180820.660365/full (accessed September 3, 2020).
Stevenson, D. G. 2019. Pushing past the status quo to protect nursing home residents. https://www.healthaffairs.org/do/10.1377/hblog20190926.292183/full (accessed November 9, 2021).
Stevenson, D. G., and A. Bonner. 2020. The importance of nursing home transparency and oversight, even in the midst of a pandemic. Health Affairs Forefront, May 12. https://www.healthaffairs.org/do/10.1377/hblog20200511.431267/full (accessed November 15, 2021).
Stevenson, D. G., and A. K. Cheng. 2021. Nursing home oversight during the COVID-19 pandemic. Journal of the American Geriatrics Society 69(4):850–860.
Stevenson, D. G., and D. C. Grabowski. 2008. Private equity investment and nursing home care: Is it a big deal? Health Affairs 27(5):1399–1408.
Stevenson, D. G., and V. Mor. 2009. Targeting nursing homes under the Quality Improvement Organization program’s 9th statement of work. Journal of the American Geriatrics Society 57(9):1678–1684.
Stevenson, D. G., and D. M. Studdert. 2003. The rise of nursing home litigation: Findings from a national survey of attorneys. Health Affairs (Millwood) 22(2):219–229.
Stevenson, D. G., M. J. Spittal, and D. M. Studdert. 2013a. Does litigation increase or decrease health care quality? A national study of negligence claims against nursing homes. Medical Care 51(5):430–436.
Stevenson, D. G., J. S. Bramson, and D. C. Grabowski. 2013b. Nursing home ownership trends and their impacts on quality of care: A study using detailed ownership data from Texas. Journal of Aging & Social Policy 25(1):30–47.
Stratmann, T., and D. Wille. 2016. Certificate-of-need laws and hospital quality. https://www.mercatus.org/system/files/mercatus-stratmann-wille-con-hospital-quality-v1.pdf (accessed November 9, 2021).
Studdert, D. M., and D. G. Stevenson. 2004. Nursing home litigation and tort reform: A case for exceptionalism. The Gerontologist 44(5):588–595.
Studdert, D. M., M. J. Spittal, M. M. Mello, A. J. O’Malley, and D. G. Stevenson. 2011. Relationship between quality of care and negligence litigation in nursing homes. New England Journal of Medicine 364(13):1243–1250.
Wagner, L. M., S. M. McDonald, and N. G. Castle. 2012. Impact of voluntary accreditation on deficiency citations in U.S. nursing homes. The Gerontologist 52(4):561–570.
Walshe, K. 2001. Regulating U.S. nursing homes: Are we learning from experience? Health Affairs 20(6):128–144.
Walshe, K., and C. Harrington. 2002. Regulation of nursing facilities in the United States: An analysis of resources and performance of state survey agencies. The Gerontologist 42(4):475–487.
Wang, X., D. Gammonley, and F. Bender. 2019. Civil money penalty enforcement actions for quality deficiencies in nursing homes. The Gerontologist 60(5):868–877.
Watson, S. D. 2012. From almshouses to nursing homes and community care: Lessons from Medicaid’s history. Georgia State University Law Review 26(3):937–969.
Wells, J., and C. Harrington. 2013. Implementation of Affordable Care Act provisions to improve nursing home transparency, care quality, and abuse prevention. https://www.kff.org/medicaid/report/implementation-of-affordable-care-act-provisions-to-improve-nursinghome-transparency-care-quality-and-abuse-prevention (accessed February 25, 2021).
White House. 1998. President Clinton announces initiative to improve the quality of nursing homes. https://clintonwhitehouse6.archives.gov/1998/07/1998-07-21-presidentannounces-initiative-to-improve-nursing-homes.html (accessed January 24, 2022).
Wiener, J. M., D. G. Stevenson, and S. M. Goldenson. 1998. Controlling the supply of longterm care providers at the state level. Washington, DC: The Urban Institute.
Wiener, J. M., M. P. Freiman, D. Brown, and RTI International. 2007. Nursing home care quality: Twenty years after the Omnibus Budget Reconciliation Act of 1987. https://www.kff.org/wp-content/uploads/2013/01/7717.pdf (accessed January 29, 2021).
Williams, B. 2019. Opening the floodgates: Repealing certificate of needs laws could drown nursing home care. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3447410 (accessed February 4, 2022).
Wyden, R. 2019. Wyden statement at Finance Committee hearing on nursing homes and elder abuse. https://www.finance.senate.gov/wyden-statement-at-finance-committee-hearing-on-nursing-homes-and-elder-abuse (accessed April 29, 2021).
Yoder, T. 2020. DOJ announces initiative to combat substandard care in nursing homes; emphasizes importance of whistleblowers. National Law Review 10(70), March 10. https://www.natlawreview.com/article/doj-announces-initiative-to-combat-substandard-care-nursing-homes-emphasizes (accessed January 25, 2022).
You, K., Y. Li, O. Intrator, D. Stevenson, R. Hirth, D. Grabowski, and J. Banaszak-Holl. 2016. Do nursing home chain size and proprietary status affect experiences with care? Medical Care 54(3):229–234.
Zhang, X., and D. C. Grabowski. 2004. Nursing home staffing and quality under the Nursing Home Reform Act. The Gerontologist 44(1):13–23.
Zinn, J. S. 1994. Market competition and the quality of nursing home care. Journal of Health Politics, Policy and Law 19(3):555–582.






















































