
3
Respiratory Protection in the Workplace
Respiratory protection has long been part of a broader set of controls designed to protect the safety and health of workers, but as described in this chapter, gaps in the current system have resulted in inadequate protection against inhalation hazards for some worker populations. Such workers include those who are not covered by respiratory protection programs (RPPs) but who may face occupational exposures on a regular or intermittent/episodic basis; they also include workers who are not usually exposed to inhalation hazards in the course of their job duties but may be exposed in exceptional circumstances (e.g., epidemics, wildfires and other extreme pollution events). In approaching the goal of ensuring adequate respiratory protection for all workers, the committee reviewed the salient literature to identify lessons learned that are applicable to broadening the scope of current programs and policies to address unmet needs.
The chapter begins by providing a rationale for expanding the reach of RPPs to worker groups not currently covered, as well as for developing modified respiratory protection options when warranted. This discussion focuses on the scope of the need and contributing factors, including hazards associated with public health and environmental emergencies, as well as the changing organization of work (e.g., growth of the gig economy, rise of temporary and contract work). The chapter then examines the formal industrial hygiene approach to use and oversight of respiratory protection in the workplace, including the extensive experience with RPPs that are based on requirements of the Occupational Safety and Health Administration (OSHA), as well as voluntary initiatives and programs developed by other
agencies. The chapter concludes with in-depth analyses of the respiratory protection needs of several specific worker groups for which hazardous respiratory exposures are well documented. The committee acknowledges that this is not an exhaustive analysis of worker groups and that there are a multitude of work settings in which workers do not receive sufficient protection from inhalation hazards, both recognized and unrecognized.
UNMET RESPIRATORY PROTECTION NEEDS IN THE WORKPLACE
Unmet needs for respiratory protection result when workers are exposed to inhalation hazards but either do not have access to respiratory protection or use such devices outside of an RPP, resulting in reduced protection or even health risks from the device itself. The imperative to address these unmet needs is clear. The Occupational Safety and Health (OSH) Act of 19701 was passed with the intent to “assure so far as possible every working man and woman in the Nation safe and healthful working conditions,” in part by encouraging employers to establish and continuously refine programs for providing safe and healthful working conditions and by enabling the development of enforceable occupational safety and health standards. To this end, OSHA’s Respiratory Protection Standard2 and employer-instituted respiratory protection programs mandated by the standard, or by other regulatory agencies,3 when use of respirators is necessary to protect worker health (see Chapter 2) have been key elements of a system designed to address inhalation hazards in the workplace. In such cases, employers are required to provide all employees with respirators appropriate for the intended purpose, as well as training and medical evaluation, at no cost to the employee. OSHA-mandated RPPs are intended to provide an established administrative structure for integrating control methods into the workplace to assess and control inhalation hazard exposures effectively, and to evaluate and assure the quality of control programs. However, there have long been gaps in coverage by RPPs and exposure scenarios have changed over time. Relevant and recent examples include the rising problem of wildfire smoke exposure and the expansive scope of worker exposure to SARS-CoV-2. The sections below explore the factors contributing to current gaps in respiratory protection for workers and the challenges characterizing the scope of the need.
___________________
1 29 U.S.C. § 651.
2 2 29 C.F.R. § 1910.134.
3 The Mine Safety and Health Administration (MSHA) and the Environmental Protection Agency (EPA) have RPP requirements for exposures in mines and for pesticide handlers, respectively.
Factors Contributing to Gaps in Respiratory Protection for Workers
The constrained application of OSHA’s Respiratory Protection Standard has contributed to gaps in respiratory protection for workers. As discussed in Chapter 2, OSHA standards, including the RPP requirements and standards limiting workplace exposure to hazardous substances, are applicable only to employers covered under provisions of the OSH Act. From OSHA’s inception, its requirements have not covered all workers and workplaces, only those workplaces where OSHA is a governing authority and to which its regulations apply, which includes those workplaces in states with OSHA-approved State Plans. There are 22 State Plan states where employers are subject to state rather than federal (OSHA) regulation and enforcement. Another six states have plans that cover public-sector workers through limited OSHA-approved State Plans and other workers through federal OSHA (OSHA, 2021g). By law, OSHA-approved State Plans include coverage of public-sector workers, but the state and local government agencies in 28 states and territories, including the District of Columbia, the Northern Mariana Islands, Guam, and American Samoa, are under no legal obligation to provide RPPs or to meet other OSHA requirements. Federal OSHA’s purview does not extend to the approximately 3.1 million nonfederal,4 public-sector workers employed in states without OSHA-approved State Plans (Maciag, 2014).
Other workers not covered by OSHA include many volunteer emergency responders, including some firefighters, rescue and recovery workers, and others who provide unpaid assistance in situations in which hazardous exposures may occur. Prisoners who do paid or unpaid work in prisons operated by 28 states and territories also are not covered by OSHA (OSHA, 2011b). Furthermore, a long-standing congressional appropriations provision has prohibited OSHA from any involvement in farms with 10 or fewer workers since 1976, when the provision was first passed (OSHA, 2014b).
Additional gaps in coverage have resulted from changing work practices in the United States. The traditional employer–employee relationship that was common 50 years ago is far less frequent today, and occupational safety and health is becoming more complex with the transition away from long-term, fixed-site employment relationships. Individuals may work for many different organizations throughout their lives, with a growing number involved in a nontraditional employer–employee relationship, such as independent contracting or temporary work, as well as what is often called the sharing or gig economy (Weil, 2014). Independent contractors,
___________________
4 OSHA protections are extended to nonmilitary federal workers by Executive Order 12196 (see https://www.archives.gov/federal-register/codification/executive-order/12196.html [accessed August 17, 2021]).
self-employed workers, and gig workers5 are not currently considered employees of an employer under the OSH Act and are therefore not covered by OSHA requirements. The law has not been updated to reflect these employment relationships that have developed or become more prevalent in recent decades (Michaels and Barab, 2020). It should be noted that misclassification of workers as self-employed to avoid employer responsibilities is also common and contributes to gaps in worker protections, but is subject to existing Department of Labor regulation and enforcement (Carre, 2015).
Many workers in temporary jobs are hired either through staffing agencies or from day-labor pools. While many temporary workers are covered by OSHA, there is often confusion over whether the staffing agency or the worksite employer has responsibility for including such workers in an RPP. Per OSHA guidance on temporary workers, responsibility for the safety and health of these workers is shared between the staffing agency and the host employer. Staffing agencies are responsible for inquiring into the conditions in the workplace and verifying that the host employer has made conditions safe for the temporary worker. Host employers in turn are required to treat the temporary worker the same as any nontemporary worker in the workplace and provide the necessary training and protections (OSHA, n.d.b).
In addition to the gaps in worker protections created by the changing nature of work and employer–employee relationships in the United States, further challenges stem from workplace exposures to inhalation hazards that arise only in the context of public health and environmental emergencies, such as infectious disease epidemics and wildfires. As discussed later in this chapter, relevant examples include agricultural and other outdoor workers exposed to wildfire smoke, workers at increased risk of exposure to SARS-CoV-2 as a result of their interactions with the public and other workers, and volunteers and emergency responders involved in disaster response and recovery work. Because these hazards are not typically encountered by these workers outside of emergency situations, their employers may not have instituted an RPP. This is not to say, however, that an RPP cannot be required under OSHA for these types of nonroutine exposures. For example, OSHA has cited numerous employers for noncompliance with the Respiratory Protection Standard as a result of workplace hazards posed by both the H1N1 (Washington State Nurses Association, 2010) and COVID-19 (OSHA, 2021e) pandemics. Moreover, OSHA implemented an Emergency Temporary Standard for health care workers in June 2021 and a National Emphasis Program in March 2021 to ensure that employees in other high-hazard industries (e.g., meat processing, warehousing, grocery
___________________
5 As noted in Chapter 2, platforms through which gig workers are currently assigned and paid are not considered employers under OSHA (Conger, 2021). Federal and several state labor agencies are currently exploring whether to classify gig workers as employees (Bose, 2021).
retail, food service, corrections) would be protected from exposure to SARS-CoV-2 (OSHA, 2021c). However, OSHA’s Respiratory Protection Standard requires that employers make a judgment that an RPP is needed when no permissible exposure limit (PEL) has been established; as a result, there are workers who experience potentially dangerous exposures who are not protected by an RPP.
Even for those workplaces and workers covered by OSHA regulations, the agency has been slow to issue new standards that would result in more comprehensive respiratory protection. OSHA has standards for only a small percentage of chemicals that are encountered in commerce. The majority of current PELs date to industry consensus standards set in the 1960s or earlier, and the agency has no specific requirements for the application of the hierarchy of controls to reduce exposure levels to the PEL. OSHA itself has recognized that existing PELs are outdated and may fail to sufficiently protect workers (OSHA, n.d.a), but its attempts to address this gap have been largely unsuccessful (OSHA, 2014a). In more recent decades, OSHA’s policy has been to issue comprehensive standards limiting chemical exposures; these standards include requirements to apply the hierarchy of controls, and many include specific requirements for respiratory protection. However, OSHA’s standards-setting process is slow, and since its inception, the agency has issued comprehensive standards for only approximately 32 chemicals, only 18 of which are still present in workplaces. Moreover, there are no such federal standards for wildfire smoke (Layton, 2020) or infectious agents similar to the aerosol transmissible disease standard promulgated by the state of California (Cal/OSHA, 2020b). The regulatory processes required to issue new standards pose significant challenges to addressing emerging threats.
These gaps in respiratory protection for workers need to be addressed.
Scope of the Problem
It is difficult to estimate the number of workers who are exposed to inhalation hazards at their workplace but are not covered by an RPP. Part of the challenge stems from the fact that, with the exception of a few chemical-specific standards, OSHA does not specify industries or worker groups that are subject to its Respiratory Protection Standard. Rather, this determination must be made at the workplace level based on a hazard assessment, with consideration of whether any potential inhalation hazards can be adequately mitigated through other controls. Several data sources, including those from the Bureau of Labor Statistics (BLS) and the National Institute for Occupational Safety and Health (NIOSH), are potentially useful for indirectly identifying and estimating the size of the unprotected
worker population (see Box 3-1), but each is subject to significant data gaps and limitations.
The scope of unprotected workers could be estimated by calculating the number of workers in industries who are exposed to inhalation hazards but not covered by an RPP because of noncompliance with or exclusion from OSHA standards, as well as those working in locations that usually
require protection only in unusual circumstances. However, this approach to generating numerical estimates has a number of important limitations, which include but are not limited to the following:
- BLS data provide only a rough approximation of worker populations, as the number of workers in some industries (such as agriculture) or demographics (such as day laborers or school-aged workers) will vary depending on the season (NASEM, 2018).
- Data concerning workplace respiratory illnesses are either sparse, outdated, or lacking in sufficient detail. For example, Survey of Occupational Injuries and Illnesses (SOII) data on the workplace incidence of respiratory diseases exclude the self-employed, workers on farms with 10 or fewer employees, private household workers, volunteers, and federal government workers, as well as workers from some states based on variability in state participation each year. In addition, SOII estimates are based on only those respiratory disease cases that the reporting employer learns about, recognizes as work-related, and then decides to record on its OSHA log, so they unquestionably represent an underestimate of the actual numbers and rates of illnesses (BLS, 2020).
- Workers within the same industry may be working in very different environments with different requirements for respiratory protection (Tarlo and Malo, 2013).
- OSHA compliance/citation data are of limited value given the infrequency of OSHA workplace inspections and the fact that OSHA is most likely to cite a workplace where there is a complaint-driven inspection or workplace fatality, or if the workplace is selected for inspection as part of an “emphasis program,” where exposure to a particular hazard is expected (e.g., the Silica National Emphasis Program). Therefore, unless a formal complaint is made or the hazard is already known to OSHA, most workplaces with inhalation hazards are likely to avoid citation. Moreover, these data do not capture those workers excluded from OSHA coverage.
- The BLS/NIOSH Survey of Respirator Use and Practices provides valuable insights into inhalation hazards and use of respiratory protection in the United States but has not been updated since 2001, although plans are under way to do so (BLS, 2021a).
- Linking data from different sources (e.g., BLS, occupational illness surveillance) is complicated by the use of different industry/occupational categories and codes.
- Most of the existing data on occupational exposures and illnesses cover only workplace exposures to traditionally regulated hazards, and do not account for workers who are exposed to inhalation
- hazards in the course of their work only during exceptional circumstances (e.g., elevated ambient pollution levels, wildfires, pandemics). Data on such exposures are often not collected systematically. For example, the Centers for Disease Control and Prevention (CDC) does not require reporting of occupational, demographic, exposure, or health outcomes data for COVID-19.
Given these limitations, any estimation of the number of workers not covered by RPPs who are potentially exposed to inhalation hazards at their workplaces will necessarily be a gross undercount and incomplete. The ability to generate a reasonable estimate would require NIOSH, in conjunction with OSHA, the Mine Safety and Health Administration (MSHA), and BLS, to update previous worksite hazard surveys and conduct more widespread exposure surveillance and intervention assessment to better understand workplace exposures and which worker populations are covered by RPPs. A national occupational disease registry, similar to those used in other countries (ILO, 2013), would facilitate improved assessment of occupational respiratory illness.
Summary and Synthesis
The above discussion demonstrates that significant gaps likely exist in respiratory protection for high-risk worker populations. The growing number of employers who employ workers in settings outside of the formal employment relationship—such as temporary, gig, informal, or contingent workers—has likely increased the potential for gaps in respiratory protection for workers. Moreover, emergency situations such as wildfires and COVID-19 have highlighted occupations and settings in which known and emerging hazards occur and for which RPPs are needed to prevent acute and chronic health effects when workers are exposed incidentally. However, the full scope of the problem is unknown because of the significant gaps that exist in the data needed for both understanding compliance with and evaluating the impact of regulations in preventing inhalation exposures and adverse health effects. Existing federal and state data systems are fragmented and incomplete, precluding a clear picture of the extent to which workers continue to be exposed to inhalation hazards without needed and OSHA-mandated RPPs. For workers not covered by OSHA, the lack of information is even more problematic. Acknowledging that previous National Academies reports have identified the need for investment in improved occupational safety and health surveillance (NASEM, 2018), including surveillance of occupational exposures to inhalation hazards and associated occupational diseases (IOM and NRC, 2008), the committee further emphasizes the importance of a focus on populations not covered by OSHA
regulations (e.g., informal workers) and exposures that may be encountered by workers only in emergency settings.
SYSTEMS FOR ENSURING RESPIRATORY PROTECTION IN THE WORKPLACE
In considering approaches for addressing the above-described gaps in respiratory protection for some groups of workers, the committee sought to understand the benefits and limitations of RPPs, considering their implementation in the context of the hierarchy of controls and the factors that influence their effectiveness.
Respiratory Protection Programs and the Hierarchy of Controls in the Workplace
Chapter 1 introduces the hierarchy of controls (see Figure 1-2) as a general framework consisting of multiple layers of control methods (e.g., engineering, administrative) for reducing the exposure of workers to hazards and promoting occupational safety and health (NASEM, 2019b), ideally in the context of a comprehensive program (safety and health management system or injury and illness prevention program). Personal protective equipment (PPE), such as respiratory protective devices, is at the lowest level of the hierarchy. Unlike controls at higher levels, its effectiveness depends on having an integrated system (i.e., RPP) in place to ensure the availability of
efficacious equipment and its proper use by individual workers at all times. Consequently, individual PPE requires adequate distribution, a system of oversight, worker-level training on its use, and maintenance of the devices. Additionally, the use of respiratory protection may itself pose secondary safety hazards related to impaired visibility and communications (Hampton et al., 2020; Hignett et al., 2020) and increased stress on the wearer, associated, for example, with increased facial heat and effort to breathe (McPherson, 2008).
Compared with implementing worksite environmental engineering controls, the use of PPE generally has a lower up-front cost. The higher initial cost and other logistical challenges associated with higher-level control methods may contribute to an overreliance on PPE in some workplaces (NIOSH, 2015a), but sustaining a PPE program for workers can be costly over time. Using the World Health Organization’s (WHO’s) cost-effectiveness analysis framework, for example, Lahiri and colleagues (2005) showed that engineering controls are more cost-effective than other interventions, including respiratory protection, for prevention of occupationally acquired silicosis.
Despite the limitations of PPE as a control method, some work tasks by their very nature (e.g., firefighting, caring for infectious patients) involve potential exposures to inhalation hazards that cannot be mitigated through engineering controls or other mechanisms higher on the hierarchy of controls. In such cases, it may be necessary to use respirators in the workplace in the context of an RPP to prevent specific illnesses and exacerbation of chronic illnesses caused by breathing contaminated air.
Effectiveness of Respiratory Protection When Used in the Context of a Respiratory Protection Program
Evidence of Effectiveness
As discussed in Chapter 1 (see Box 1-2), the assigned protection factor (APF) for a respirator provides a standardized measure of the device’s workplace level effectiveness (OSHA, 2009). Yet, while protection factor studies can provide an estimate of the effectiveness of respirators at reducing exposure (when used in the context of a comprehensive RPP), understanding the effectiveness of RPPs themselves is more challenging.
Few peer-reviewed studies have evaluated the impact of OSHA-mandated RPPs on the safety and health of workers, although anecdotal reports suggest that the presence of a defined RPP provides measurable benefit in protecting employees from inhalation hazards. One example is offered by
the Texas Center for Infectious Disease (TCID), a long-term care hospital specializing in the management of difficult-to-treat tuberculosis cases. Prior to 1986, TCID had no formal infection control plan, and annual tuberculin skin tests revealed that 40–50 percent of the center’s staff had positive results, with 1–2 percent of staff developing tuberculosis (NASEM, 2019b). TCID instituted an RPP for its staff in 1995. Employees receive extensive training in how to properly use, disinfect, and store their TCID-supplied elastomeric facepiece respirators, culminating in a written test to ensure correct understanding of the elements of the RPP. Additionally, all staff who enter patient rooms are required to undergo qualitative fit testing (NASEM, 2019b). Since this RPP was implemented, no TCID employees have tested positive on a tuberculin skin test (NASEM, 2019b; The Joint Commission, 2014).
Beyond such anecdotal reports, few studies have directly measured protection against acute or chronic health effects from inhalation hazards following implementation of an RPP. Informative examples can be drawn from the literature on hazards for which biological monitoring is ongoing, such as with the OSHA lead standard. Numerous studies have demonstrated reductions in exposure biomarkers associated with use of respirators in the workplace (Burgess et al., 2001; Grauvogel, 1986; Hyatt, 1984; Liu et al., 2016). However, a notable challenge to assessing the benefits of an RPP is the difficulty of disentangling the consequences of the program from those of use of the respirator itself. An early study by Harris and colleagues (1974) on the effectiveness of respirators for protection from coal dust in underground coal mines showed that even in the absence of an RPP, use of respirators reduced exposures to the dust (Harris et al., 1974).
Further evidence for the potential benefits of RPPs is reported by Cowan and colleagues (2017), who examined fatalities associated with the use of respiratory protection in industrial settings between 1990 and 2012. The authors note a reduction in fatality rates during that time period that appears to be associated with the 1998 publication of OSHA’s revised Respiratory Protection Standard, which included new language designed to ensure that employers would have sufficient guidance to support the selection and maintenance of respiratory protective devices. The findings they report show that historical fatalities associated with respirator use appeared to be associated primarily (>90 percent) with employee error and/or lack of employer compliance with the OSHA Respiratory Protection Standard (e.g., lack of a written RPP, lack of or improper training). The authors conclude that the implementation of the revised OSHA standard, as well as enforcement, outreach, and compliance assistance, had a significantly favorable impact on fatality rates over time (Cowan et al., 2017).
Compliance as a Limiting Factor for the Effectiveness of Respiratory Protection Programs
In addition to evidence of benefit, the committee sought to understand the limitations of RPPs, finding that they relate primarily to employers’ lack of compliance with the OSHA Respiratory Protection Standard. Employers’ failure to comply with program requirements will limit the effectiveness of such systems for protecting workers from occupational respiratory illnesses, although empirical data to demonstrate such impacts are sparse. The reasons for inadequate adoption of and compliance with RPP requirements are not well understood, but research suggests that financial constraints play a major role in the failure to establish health and safety programs more broadly for small businesses (NIOSH, 2018; Vinberg, 2020). A 2007 survey of Kentucky fire departments, for example, found that funding and lack of understanding were the greatest barriers to RPP implementation (Easterling and Prince, 2007).
Several survey-based studies have demonstrated shortcomings of institutional RPPs. In 2001, NIOSH and BLS undertook a broad survey of respirator use and practices among U.S. private-sector employers (DOL and NIOSH, 2003). The survey was mailed to approximately 40,000 private-sector establishments. Based on the survey results, the authors report that respirator use was required in 4.5 percent of these establishments and for 3.1 percent of their employees. Importantly, the survey showed that among establishments requiring respirator use, 91 percent had at least one indicator of a potentially inadequate RPP, while 54 percent had at least five such indicators (Doney et al., 2005). Of the businesses surveyed in which respirators were used, 65.5 percent had no written program detailing how respirators would be used, 49.9 had no written procedure for maintaining their respirators, and 43.3 percent offered no form of fit testing (Doney et al., 2005). These findings suggest that large numbers of employers may not adhere to OSHA requirements for RPPs, putting their workers at risk. However, these data are 20 years old, and the survey was conducted shortly after the 1998 revision of the Respiratory Protection Standard, limiting the conclusions that can be drawn about RPP compliance today. NIOSH and BLS recognize the need to update this survey, and a new survey is planned (BLS, 2021a).
More recently, a study of California hospitals during the 2009–2010 H1N1 influenza pandemic showed that although health care workers reported knowing that they should wear N95 filtering facepiece respirators (FFRs) when in close contact with patients with confirmed or suspected cases of the disease, an evaluation of the hospitals’ written RPPs revealed deficiencies in the areas of recordkeeping, designation of a program administrator, program evaluation, employee training, and fit testing procedures
(Beckman et al., 2013). Other studies have found similar shortcomings in workplace RPPs for both health care and public safety workers (Sietsema, 2017; Sietsema et al., 2015).
OSHA citation data support the findings of the survey-based studies described above, further indicating that many employers are not adequately complying with the Respiratory Protection Standard. Mendeloff (2013) carried out an analysis to complement the study undertaken by BLS and NIOSH in 2001. He examined the OSHA database of all inspections in manufacturing establishments in 47 states from 1999 through 2006 (after the OSHA Respiratory Protection Standard had been revised). The study identified inspections and establishments in which respiratory protection violations had been cited, and compared the prevalence of violations by industry with the prevalence reported in the BLS survey of respirator use. The most frequent violation of the OSHA standard (representing one-third of the total) was the failure to have a written RPP. The author found that the probability of citing a respiratory protection violation was comparable across establishment sizes, except for a large decrease at establishments with more than 200 workers. For those workers covered by OSHA, increased enforcement could address RPP limitations related to compliance. However, increased enforcement will not address gaps related to those workers not covered by OSHA’s Respiratory Protection Standard, and the root factors that lead to noncompliance need to be understood.
Summary and Synthesis
How well respiratory protection works in practice depends on a sequence of steps, each representing a potential failure point (see Figure 3-1). These determinants of effectiveness include a hazard assessment that leads to the proper selection of a respirator based on its APF and use of the device in the context of a comprehensive RPP, with ongoing surveillance. Extending this framework more broadly to other groups of workers, it is important to consider the extent to which each element of this framework needs to be replicated to ensure effective programs for worker groups not currently covered by RPPs. It should be noted, however, that even for those workplaces clearly subject to the requirements of OSHA’s Respiratory Protection Standard, there is evidence of failure to implement RPPs (or to implement them adequately). The Respiratory Protection Standard is consistently among the top 10 most frequently cited OSHA standards (OSHA, 2021h). However, addressing the issue of compliance with OSHA RPP requirements will require more than increased enforcement. Efforts to better address the respiratory protection needs of workers need to include a focus on improved safety culture (IOM and NRC, 2008).
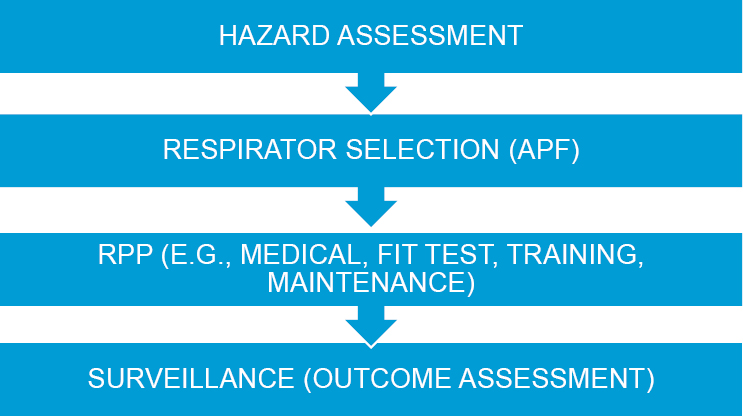
NOTE: APF = assigned protection factor; RPP = respiratory protection program.
While challenges related to latency of outcomes and confounding factors limit the availability of direct evidence on the effectiveness of RPPs, it can be inferred from indirect evidence in the form of exposure reduction studies and dose-response relationships that RPPs, when implemented appropriately and enforced, protect workers from inhalation hazards. Importantly, the committee found relatively little rigorous and systematic evidence for evaluating the best methods and strategies for implementing an RPP. More robust collection of data on the use of respiratory protection in a workplace environment is needed, applying methods recommended in the National Research Council review of the 2001 BLS/NIOSH Survey of Respirator Use and Practices, including the collection of data from employers and employees on respirator use in the workplace (NRC, 2007). Standardized measures for evaluating respirator use in the context of RPPs will also be important (Yarbrough et al., 2016). Consistent with past evaluations (IOM and NRC, 2008), the committee found that more research is needed on the facilitators of and barriers to effective use of respiratory protection in the workplace, including human factors, individual and organizational behaviors, and workplace safety culture. Such efforts will need to address previously recognized challenges to data collection and research, including lack of access to work environments and historical records, as well as lack of cooperation from employers (IOM and NRC, 2008).
BEYOND RESPIRATORY PROTECTION PROGRAM (RPP) REQUIREMENTS IN OSHA’S RESPIRATORY PROTECTION STANDARD
Although the requirements laid out in OSHA’s Respiratory Protection Standard may represent the best-known model for workplace RPPs, the committee sought to explore alternative approaches by which worker respiratory protection needs could be met. This section reviews programs regulated by other government agencies, as well as other respiratory protection models—including voluntary programs—that could be implemented when full RPPs are not required.
Other Program Types
Other Federal and Nonfederal Programs
The requirements laid out in OSHA’s Respiratory Protection Standard are widely accepted and referenced by other entities with identified inhalation hazards in their workplaces. Federal and state regulations that require respirators in the workplace generally adopt the OSHA standard by reference in whole or in part. Accreditation bodies such as The Joint Commission, a health care accreditation organization, also refer to the OSHA requirements for RPPs as the basis for their respiratory protection guidelines. The Joint Commission cites 1910.134 and the NIOSH–OSHA Hospital Respiratory Protection Program Toolkit: Resources for Respirator Program Administrators.
In some cases, regulations specific to hazards or work practices may go further, specifying the type of respirator to be used and/or specifics of how to administer the respiratory protection program. For example, the Environmental Protection Agency’s (EPA’s) worker protection standard (40 C.F.R. § 170.507) includes requirements for fit testing, medical evaluation, and training that conform to the OSHA Respiratory Protection Standard but requires pesticide handlers to be provided with respirators as specified on the product label. The U.S. Army, which requires compliance with OSHA’s Respiratory Protection Standard per Army Regulation (AR)
11-34 (Department of the Army, 1990), has established Toxic Chemical Agent Safety Standards (Department of the Army, 2018) and provides additional guidance related to respirator selection based on chemical type and concentration. Similarly, some states simply adopt the federal OSHA standard, while others have their own regulations that go beyond what OSHA requires.
Alternative Approaches in the Context of the COVID-19 Pandemic
SARS-CoV-2, which was recognized belatedly as an airborne inhalation hazard, presents extensive challenges for protecting workers and has altered the landscape for regulation of worker respiratory protection. On January 21, 2021, the Biden administration issued an executive order directing OSHA to take action to reduce the risk to workers of contracting COVID-19 at their workplaces (Executive Office of the President, 2021). OSHA issued nonmandatory guidelines for non–health care employers in late January 2021 (OSHA, 2021f) (see Box 3-2), and in June 2021, it issued an emergency temporary standard (ETS) under 29 CFR 1910 Subpart U for workers in health care settings where suspected or confirmed cases of COVID-19 are being treated. The ETS requires employers in health care settings to develop and implement effective plans for mitigating the threat of COVID-19, including developing a COVID-19 plan (in written form if they have more than 10 employees) with a designated safety coordinator, a workplace-specific hazard assessment, and policies and procedures for minimizing the risk of transmission of COVID-19 to employees (29 C.F.R. § 1910.502).
As part of the ETS for workers in health care settings, OSHA developed a “mini RPP” for use in the specific circumstances of the ETS when a respirator is not required but may provide enhanced protection for workers not exposed to confirmed or suspected cases of COVID-19. The mini RPP applies to workers not already covered by a traditional RPP and is not meant as a substitute or replacement for OSHA’s normal Respiratory Protection Standard (29 C.F.R. § 1910.134). Table 3-1 provides a comparison of requirements under OSHA’s standard RPP and the mini RPP when the respirators are employer provided.6 The mini RPP has some similarities to OSHA’s voluntary use provision (described below), but if an employer provides respirators to employees under the mini RPP (regardless of device type), that employer must provide training on the use of the device, ensure that seal checks are properly conducted, ensure that the respirators are reused properly, and ensure discontinuation of respirator use under certain conditions (OSHA, 2021d).
In the absence of a national standard to protect non–health care workers from transmission of SARS-CoV-2, states have developed their own
TABLE 3-1 Comparison of Requirements for Mini and Full Respiratory Protection Programs (RPPs)
| KEY PROGRAM ELEMENTa | MINI RPP (1910.504)b | NORMAL RPP (1910.134)c |
|---|---|---|
| Medical Evaluation | √ | |
| Fit Testing | √ | |
| Written Program | √ | |
| User Seal Checks | √ | √ |
| Training | √ | √ |
a This is not a comprehensive list of required program elements.
b These are key requirements pertaining to employer-provided respirators (as opposed to worker-provided respirators).
c For additional information about the Respiratory Protection Standard’s requirements, see NIOSH/OSHA’s “Hospital Respiratory Protection Program Toolkit Resources for Respirator Program Administrators” at www.osha.gov/sites/default/files/publications/OSHA3767.pdf (accessed September 27, 2021).
SOURCE: OSHA, 2021d.
___________________
6 If employees provide their own respirators, employers are required only to provide them with a specific notice contained in 29 C.F.R. § 1910.504(c).
regulations and protocols. Beginning in the early days of the pandemic, state governments issued public health orders covering workplaces, ranging from general guidelines to comprehensive safety and health standards. The first state to promulgate a comprehensive occupational safety and health standard was Virginia, in July 2020 (Virginia DOLI, 2020). This emergency standard required employers to conduct exposure assessments and determine whether a job task poses high, medium, or low risk. It incorporated the hierarchy of controls, and invoked OSHA PPE standards (including the respirator standard) if the assessment concludes that PPE is needed. Use of face coverings was considered to be an administrative control. Oregon and California also issued worker safety standards for COVID-19 exposure (Cal/OSHA, 2020c; Oregon OSHA, 2020).
In other states, governors issued executive orders, or regulatory agencies provided guidance, in some cases tied to general state orders for prevention of the spread of COVID-19, such as limitations on public gatherings, mandatory face coverings in public places, and social distancing, and in others tied to a state’s plans for reopening. Public health agencies issued workplace-specific guidance for occupations posing a high risk of disease transmission. Many of these measures were instituted for a limited period of time, and as the pandemic ebbed in spring 2021, were being phased out or relaxed. California, for example, initially required employers to provide face coverings and ensure that their employees used them under its ETS (Cal/OSHA, 2020a); that requirement was revised on June 17, 2021, when employers were allowed to let fully vaccinated employees forego wearing face coverings indoors (Cal/OSHA, 2021b). Other states issued guidance on which types of masks should be worn by workers based on risk level, even though the requirement for vaccinated workers to wear a mask had ended (Washington State DOLI, 2021b).
Voluntary Use of Respiratory Protection in the Workplace
This section addresses cases in which an employer chooses to provide employees with respiratory protective devices or to allow employees to bring their own devices when their use is not covered or required under federal or state regulations. Voluntary use in this context refers to the worker’s choice to use the device, not the employer’s choice to offer an RPP, which is dictated by the hazard analysis. The experience with such programs offers insights into the potential effectiveness of less formal initiatives since in such situations, a comprehensive program meeting all the requirements of OSHA’s Respiratory Protection Standard is unlikely to be followed. However, OSHA does have some mandatory requirements designed to ensure that the voluntary use of respirators does not by itself create a hazard. The discussion below reviews considerations for different types of respiratory
protective devices that may be used in the workplace when not required under federal or state regulations.
Considerations for Voluntary Use of Respirators
In some cases, workers may wear respirators to avoid exposure to a hazardous substance even if that exposure does not exceed the limits set by OSHA standards. Voluntary use of respirators is included within the OSHA Respiratory Protection Standard 1910.134, with requirements specified in Appendix D. The concept of voluntary use of respirators was introduced when OSHA first published its revised Respiratory Protection Standard in 1998; it had not been included in the previous version. According to the revised standard, if “respirator use is not required, an employer may provide respirators at the request of employees or permit employees to use their own respirators, if the employer determines that such respirator use will not in itself create a hazard” (1910.134(c)(2)). As was clarified by OSHA in a letter of interpretation issued on April 26, 2018 (OSHA, 2018), employers are not required to pay for or provide these respirators to employees, but are required to ensure that employees are familiar with the training outlined in Appendix D of the OSHA Respiratory Protection Standard.
Respirators used voluntarily include those that are not filtering facepiece devices and those that are (see Figure 3-2). Under voluntary use, filtering facepiece respirators are not specifically required to be NIOSH approved; they do not require fit testing; employees can have facial hair; and medical clearance is not required (OSHA, 2018), although employees with known respiratory limitations should be advised to consult their physician prior to wearing such a device. “Employers are not required to include in a written respiratory protection program those employees whose only use of respirators involves the voluntary use of filtering facepieces” (1910.134(c) (2)). In contrast, use of elastomeric facepiece respirators or supplied-air respirators, even voluntary use, requires that the employer include all applicable elements in a written RPP to avoid hazards associated with use. The written RPP varies by respirator type selected for use, but must encompass the medical evaluation (which the employer must pay for), cleaning, maintenance, and storage components (OSHA, 2018).
A number of problems can potentially arise when respirators are used voluntarily in the workplace outside of an OSHA-mandated RPP (Gibbs and Nonnenmann, 2020). The use of non–NIOSH-approved devices may occur if employees bring their own devices purchased from retail stores or are unable to obtain approved devices from the marketplace because of shortages. In such cases, the risk is that the protection (e.g., filter efficiency) offered by alternative devices may be untested and insufficient. These devices may have higher breathing resistances relative to approved respirators
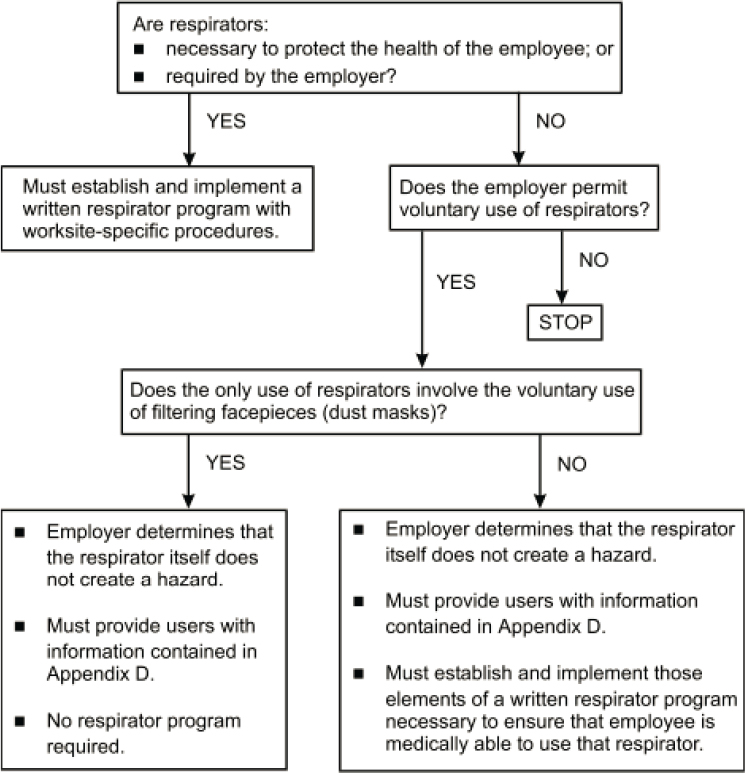
SOURCE: OSHA, 2006.
and cause unacceptable physiological stress to the user. The materials of construction that contact the face of these devices may cause irritation or rashes. Additionally, tight-fitting air-purifying respirators rely on a proper fit to ensure that the majority of air passes through the filter or cartridge and not through facepiece leaks. This assurance normally requires the combination of a fit test to select a proper respirator size and a seal check each time the device is donned. Users who wear respirators in the absence of such testing and/or checking may have a false sense of protection. Despite these concerns, employees’ use of their own personally acquired respirator (i.e., not provided by the employer) may be warranted when employers do not or
cannot provide access to protective equipment that is commensurate with the risk to which the workers are exposed (The Joint Commission, 2020).
Underlying the OSHA rules for voluntary use of respirators is the assumption that no significant inhalation hazard is present and that wearing a respirator does not by itself cause a hazard to the user. To ensure that the respirator provides adequate protection and to avoid any device-related problems for the user, the user should have some basic instruction on
- how to don the device properly, including the orientation on the face;
- any limitations of the device for the hazard at hand;
- the need to either dispose of the device after use or properly clean it;
- the need to disinfect the device when worn multiple times in the presence of an infectious agent;
- a proper method for safely storing the device if it will be reused; and
- the requirement that it not have exhalation valves when the hazard is an infectious agent.
Considerations for Voluntary Use of Medical Masks
Medical masks have historically been used to protect others from infectious diseases the wearer may have (source control), and not to provide inhalation protection against hazardous aerosols. Applicable Food and Drug Administration (FDA) regulations (discussed in Chapter 2) govern manufacturers and not employers or employees. Some employers (e.g., hospitals) may have specific rules for their employees governing the selection and use of masks in the workplace. When masks are selected, FDA-cleared devices or those tested to ASTM standards will ensure that the device has an acceptable level of performance in terms of filtration, construction (e.g., biocompatibility), and breathing resistance.
Fit testing is not a requirement for medical masks used in the workplace since the devices are not intended to provide a tight seal to the face of the wearer. However, workers using such masks voluntarily should have adequate instruction on
- how to don the device properly, including the orientation on the face;
- the need to either properly dispose of the medical mask or clean it after use;
- the need to disinfect the mask if the hazard is an infectious agent;
- a proper method for safely storing the device if it will be reused; and
- a requirement that it not have exhalation valves if the hazard is an infectious agent.
Considerations for Voluntary Use of Barrier Face Coverings
Face coverings are an unregulated product that have been widely used to limit the spread of exhaled droplets or fine-particle aerosols during the COVID-19 pandemic. There are no regulations governing the use of barrier face coverings by employers or employees. As discussed above and in Chapter 2, a recent ASTM standard has established requirements for a barrier face covering to be used as a source control product, although the standard does not include a requirement to measure the performance or effectiveness of the product for that purpose. Barrier face coverings are not a substitute for respirators, since their performance in terms of inhalation protection is unknown. However, it may be anticipated that many workers will wear barrier face coverings in the workplace voluntarily even after indoor mask mandates and individual employer policies requiring their use have been lifted, although some may prefer respirators over barrier face coverings once supply issues have been resolved.
Summary and Synthesis
Circumstances in which respiratory protection might be used by workers outside of an OSHA-mandated RPP include voluntary use of respiratory protective devices on the part of employees and an array of situations in which agencies other than OSHA may call for RPPs, although OSHA regulations remain the starting point in such situations. The review in this section affirms that the OSHA-mandated RPP is the “gold standard” for respiratory protection and makes clear that voluntary initiatives can be fraught with gaps. Consideration also needs to be given to the potential for power dynamics in the workplace to impact the ability of employees to access respiratory protection under voluntary programs.
The urgency posed by transmission of SARS-CoV-2 highlights gaps in achieving sufficient respiratory protection for the wide range of potentially exposed and at-risk workers, as discussed in further detail later in this chapter. A range of state and local public health guidance has been issued using transmission control measures with broad reach, such as social distancing, shutdowns, and increased ventilation. However, the absence of federal enforcement of an RPP recognizing airborne transmission of COVID-19 has left many workers without adequate personal protection. Medical masks and commercial face coverings have been marketed, purchased, and used, often with the user’s lack of understanding of the uncertainty of the inhalation protection provided by these devices resulting from variable fit and filtration characteristics, which are described in Appendix B. Likewise, while guidance issued by federal agencies has helped employers and employees
understand the difference between source control devices and respirators, confusing terminology and the lack of standards have hindered the implementation of adequate respiratory protection for workers, both within and outside the health care sector.
While the OSHA RPP model could be adopted for use in other situations in which workers are exposed to environmental hazards, such as wildfire smoke, or infectious agents responsible for epidemics, such as SARS-CoV-2, covering all potentially exposed workers would require a substantial expansion of effort and cost. It would be necessary to provide fit testing of respirators for each worker, or to develop a device with acceptable off-the-shelf fit characteristics such that it would not require individual fit testing, but give the wearer some indication that it had been donned properly and was providing a good seal, and therefore increased protection (e.g., through a user seal check). While some loose-fitting powered air-purifying respirators (PAPRs) have these characteristics, other innovative technologies may be on the horizon.
Overall, the committee finds that expanded initiatives to provide respiratory protection cannot be based in frameworks less structured than OSHA’s, despite the greater effort required. At the least, a structured framework will guide implementation of new programs and facilitate consideration of how rigorous each step needs to be to achieve the exposure reduction goal. The range of workers to be covered is broad, and as shown by the COVID-19 pandemic, prospective planning is needed for high-risk scenarios.
SPECIFIC WORKER GROUPS
This section examines a number of specific worker groups that face inhalation hazards but are not systematically covered by RPPs. The committee identified these groups as it considered its Statement of Task (see Box 1-1 in Chapter 1) and discussed high-priority targets for its efforts with the study sponsors (see Table 1-1 in Chapter 1). In selecting worker populations to highlight in this section, the committee aimed to include representative examples that would underscore the respiratory protection gaps for workers related to
- employment relationships (e.g., volunteers, temporary or day laborers) that exclude workers from OSHA’s Respiratory Protection Standard or obscure employer responsibility; and
- hazards not typically encountered in the normal course of duties for certain groups of workers (e.g., agricultural workers exposed to wildfire smoke and increased risks for some essential workers during infectious disease epidemics based on close and frequent contact with other workers or the public).
These are not mutually exclusive categories. For example, many agricultural workers are hired as temporary or day laborers, and such workers may on occasion be exposed to smoke if required to work in proximity to wildfires. Moreover, some worker groups discussed in this section who may remain close to a hazard even when not working, including wildland firefighters and disaster workers, are exposed to inhalation hazards on an ongoing basis in the course of their work and face unique challenges beyond these two gap areas.
Of note, this section is not intended to cover every unprotected worker group exposed to workplace inhalation hazards and should not be interpreted as a comprehensive analysis of all such populations. Instead, the selection of appropriate example worker populations is intended to highlight gaps in the existing landscape for occupational respiratory protection to inform the development of a framework for ensuring adequate respiratory protection for all workers (see Chapter 6). Here, the committee reviews what is known about exposures of these representative groups and their use of respiratory protection—drawing on the comprehensive reviews described in Chapter 1 and Appendix B—and associated gaps and needs related to guidance.
Wildland Firefighters
In 2020, a total of 10.1 million acres burned in the United States, compared to over 4.6 million acres reported in 2019 (NICC, 2020a). The increasing numbers of wildland firefighters required to combat this worsening threat bring new urgency to the need to address gaps in respiratory protection for this workforce.
Description of the Workforce, Work Environment, and Work Characteristics
Accurately estimating the number of wildland firefighters operating in U.S. states is difficult given the multiplicity of involved organizations and the seasonal variation in numbers (Butler et al., 2017). Organizations engaged in response to wildland fires span volunteer fire departments, municipalities, private contractors, and federal agencies. During extreme fire years, the National Guard or the U.S. military may be asked to respond. During the peak of the 2020 U.S. wildland fire season, 28,000 people (permanent and seasonal employees) were assigned to wildland fire management (NICC, 2020b) in the National Incident Resource Ordering Capability (IROC) system.
The work of wildland firefighters is necessarily strenuous and is carried out under harsh environmental conditions characterized by high heat. The job tasks for wildland firefighters are extremely variable and many require high levels of energy expenditure (Ruby et al., 2002). Most wildland firefighters also camp at the fire location, which can potentially lead to 24-hour smoke exposure. A study by West and colleagues (2020) followed wildland fire resources across the western United States found that 43.2 percent of the firefighters’ shifts was spent in the sedentary activity category, while 47.5 percent was in the moderate/high category (see Table 3-2). The main nonsedentary job task identified by the authors was hiking (19.2 percent). Using GPS trackers, Sol and colleagues (2018) calculated oxygen (VO2) requirements for different hikes during a shift and quantified the high level of exertion (which can be upwards of 10 metabolic equivalents [METS]) based on terrain and high load carriage (26.6±6.9 kg, 32.7±9.0 percent of body weight). As discussed below, these strenuous working conditions have implications for the kinds of respiratory protective devices that would be suitable for wildland firefighters.
Exposure and Health Impact Data
Wildfires generate a toxic mixture of particulate and chemical vapor inhalation hazards that pose significant risks to the respiratory health of
| SEDENTARY ACTIVITY | % | LIGHT PHYSICAL ACTIVITY | % | MODERATE PHYSICAL ACTIVITY | % | HIGH PHYSICAL ACTIVITY | % |
|---|---|---|---|---|---|---|---|
| ICP Stationary | 1.7 | Handline Direct Pump | 0.1 | Mop Up | 5.1 | Handline Direct Scratch | 0.7 |
| ICP Other | 0.2 | Handline Indirect Pump | 0.02 | Cold Trailing | 0.6 | Handline Direct Sawyer | 0.5 |
| Briefing | 6.7 | Handline Indirect Dozer Boss | 0.02 | Improving Direct Line | 0.2 | Handline Direct Swamper | 0.6 |
| Driving | 6.9 | Holding Direct Line | 1.3 | Improving Indirect Line | 1.1 | Handline Direct Engine | 0.1 |
| Lunch Break | 3.6 | Holding Indirect Line | 0.2 | Felling Sawyer | 0.6 | Handline Direct Squad Leader | 0.1 |
| Rest Break | 3.3 | Holding Firefighter | 0.7 | Felling Swamper | 0.6 | Handline Direct Firefighter | 0.2 |
| Operational Break | 19.5 | Holding Squad Leader | 0.2 | Working with Aviation | 0.1 | Handline Indirect Scratch | 0.4 |
| Staging | 0.9 | Holding Engine | 0.1 | Scouting Hazard Trees | 0.7 | Handline Indirect Sawyer | 0.6 |
| Other | 0.5 | Suppression Holder | 0.8 | Grid the Black | 1.5 | Handline Indirect Swamper | 1.2 |
| Total | 43.2 | Engine Pump Operator | 0.2 | Grid the Green | 0.6 | Handline Indirect Squad Leader | 0.3 |
| Holding Pump | 0.1 | Tool Up/Tool Down | 8 | Handline Indirect Firefighter | 0.2 | ||
| RX Holder | 0.2 | Total | 19 | Live Preparation | 0.5 | ||
| Refurb Tools | 3.3 | Initial Attack | 0.1 | ||||
| Structure Protection | 1.1 | RX Lighter | 0.2 | ||||
| Compound Work | 1.4 | Suppression Lighter | 0.8 | ||||
| Total | 9.4 | Physical Training | 1.3 | ||||
| Project Saw | 0.6 | ||||||
| Project Stacking | 0.7 | ||||||
| Hiking | 19.2 | ||||||
| Medical | 0.1 | ||||||
| Total | 28.4 | ||||||
SOURCE: Reproduced from Occupational and Environmental Medicine, M.R. West, S. Costello, J. A. Sol, and J. W. Domitrovich, vol. 77, 433-438, 2020 with permission from BMJ Publishing Group Ltd.
wildland firefighters. Wildland fire smoke has been a concern of the National Wildfire Coordinating Group (NWCG)7 since the 1980s (Sharkey, 1997). Studies over the past 30 years have focused on exposure quantification and potential health effects. Wildland firefighters experience other sources of health hazards, such as ground disturbance of silica, combustion engines, and site-specific hazards; in this report the committee focuses on vegetation smoke exposure.
The first study to quantify exposure to wildland fire smoke was conducted by Reinhardt and Ottmar in the early 1990s (Reinhardt and Ottmar, 2004). They found concentrations of carbon monoxide (CO), particulate matter (PM), benzene, formaldehyde, and acrolein, and their initial findings indicated that exposure to all smoke components was higher during prescribed burns compared with wildfires. They also found correlations with increased smoke exposure during higher ambient wind speeds (wind is a critical component of fire growth).
The study by Reinhardt and Ottmar (2004) was limited to a few selected locations on the West Coast. From 2008 to 2011, the United States Forest Service’s National Technology and Development Program (NTDP) conducted a larger-scale follow-up study of smoke exposure to increase the sample size and diversity of fuel models across a larger geographic region of the United States8 (Broyles, 2013; Domitrovich et al., 2017). Given the high correlations among smoke components found by Reinhart and Ottmar, this study focused on CO and PM. A novel aspect of this study was that wildland firefighters were trained as research assistants and performed direct observation on potential compounding factors in smoke exposure. The findings of this NTDP study regarding smoke exposure were similar to those of the Reinhardt and Ottmar (2004) study. More recently, Wu and colleagues (2021) studied wildland fire exposure in the Midwestern United States during prescribed burns, finding that the overall exposure levels were higher than those reported in studies of wildland firefighters in the western and southeastern areas of the United States, providing evidence for the role of fuel models and operational tasks in the smoke exposure of wildland firefighters. The authors also reported that no value was over the 8-hour OSHA PEL (Wu et al., 2021).
The NWCG created a task group, which recommended minimizing
___________________
7 The National Wildfire Coordinating Group, established in 1976, provides national leadership to enable coordination of programs and interoperable wildland fire operations across the participating federal, state, local, tribal, and territorial partners. Additional information is available at https://www.nwcg.gov (accessed September 29, 2021).
8 This study includes 7,517 hours of CO measurements on firefighters and 1,554 hours of CO measurements at Incident Command Posts (ICPs) and spike camps (satellite locations separate from the main fire camp), and a total of 179 PM4 (respirable dust) and SiO2 (crystalline silica) firefighter samples and 78 samples from ICPs and/or spike camps (Broyles, 2013).
mop up9 and rotating crews out of heavy smoke areas as mitigation measures. This task group also defined a recommended exposure level, taking into account CO, PM, and other smoke components, based on an extended work shift of 16 hours and a 24-hour period, given that a typical wildland firefighter’s shift often exceeds the 8-hour OSHA PEL. Navarro (2020) recently reviewed studies of wildland firefighter exposure to CO and PM and summarized the data in relation to the recommended exposure level and OSHA’s PEL (see Figure 3-3).
A large number of studies have examined the health effects of wood smoke, as reviewed recently (Cascio, 2018; Adetona et al., 2016), but only a limited number have focused specifically on wildland firefighters. There have been multiple short-term studies, with time scales ranging from the course of one shift to a whole season, and only one retrospective study on long-term wildland firefighter health. The latter study, conducted by Semmens and colleagues (2016) found two subclinical cardiovascular risk factors (hypertension, heart arrhythmia), as well as markers of musculoskeletal effects (knee surgery), with no other significant health effects. A major limitation of this study, however, was that the questionnaire was sent only to current wildland firefighters and not retirees. Other studies have shown both shift and seasonal changes in respiratory function (Gaughan et al., 2014; Liu et al., 1992). Navarro and colleagues (2019) extrapolated the relative risk of cancer and cardiovascular disease mortality over the course of a wildland firefighter’s career, comparing long (100 days) and short (50 days) fire seasons (see Figure 3-4). These projections suggest the need for more long-term studies to assess the health risks of smoke exposure for wildland firefighters.
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
Oversight of use of respiratory protection by wildland firefighters is complicated by the diversity of employment relationships under which wildland firefighters work. Federal wildland firefighters fall under the safety programs of their respective employing federal agencies. Five federal agencies (United States Forest Service, Bureau of Land Management, National Park Service, U.S. Fish & Wildlife Service, and Bureau of Indian Affairs) across two departments (U.S. Department of Agriculture [USDA] and Department of the Interior) have wildland fire management programs. Additionally, each state has its own department of natural resources, and local volunteer
___________________
9 Mop up is “extinguishing or removing burning material near control lines, felling snags, and trenching logs to prevent rolling after an area has burned, to make a fire safe, or to reduce residual smoke” (NWCG, 2021b).
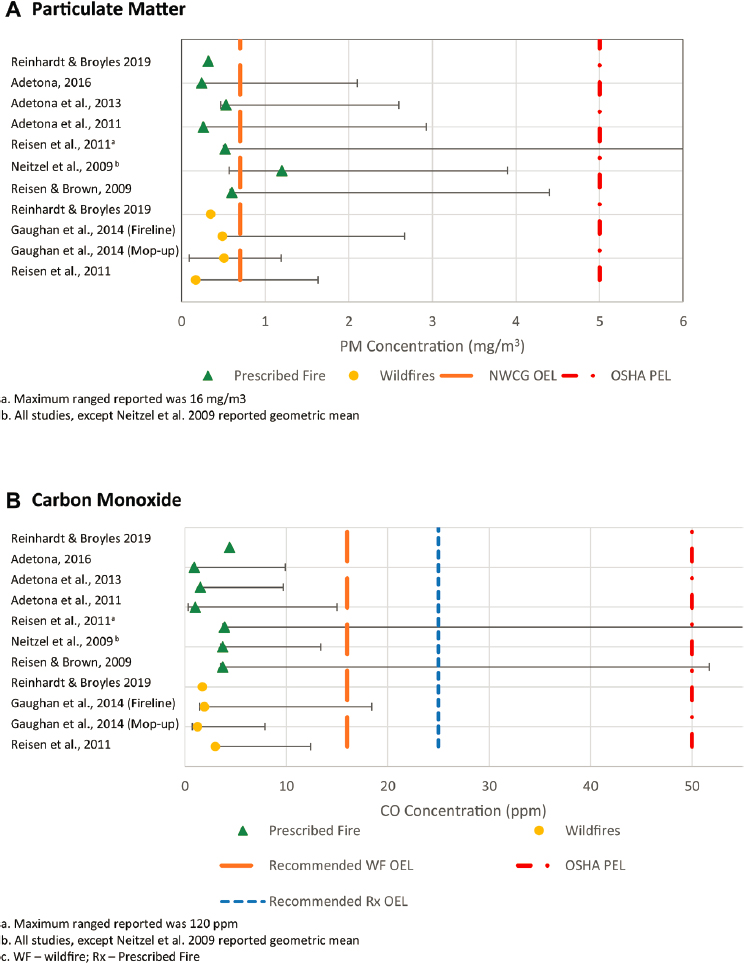
SOURCE: Reprinted from Clinics in Chest Medicine, vol. 41, ed. 4, K. Navarro, “Working in smoke: Wildfire impacts on the health of firefighters and outdoor workers and mitigation strategies,” 763-769, 2020, with permission from Elsevier.
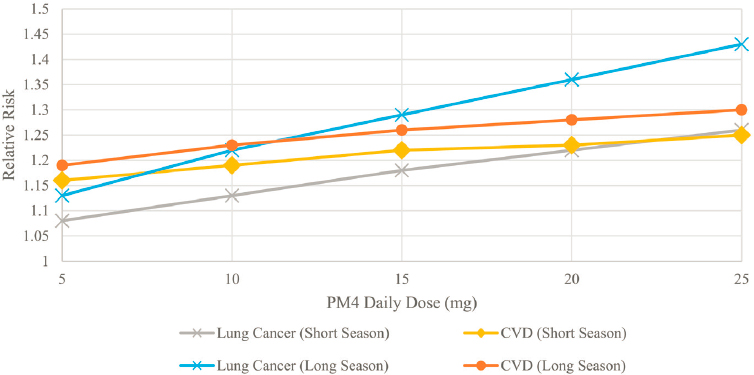
SOURCE: Reprinted from Environmental Research, vol. 173, K.M. Navarro, M.T. Kleinman, C.E. Mackay, T.E. Reinhardt, J.R. Balmes, G.A. Broyles, R.D. Ottmar, L.P. Naher, and J.W. Domitrovich, “Wildland firefighter smoke exposure and risk of lung cancer and cardiovascular disease mortality,” 462-468, Copyright 2019, with permission from Elsevier.
and municipality organizations may have responsibility for wildland fire response. The need for respiratory protection for wildland firefighters must be determined by each of these entities.
Respiratory protection has been an area of concern for federal land management fire programs since the Yellowstone fires of 1988. To date, however, no respirator has been found that meets the unique needs of wildland fire management. The strenuous activity associated with wildland firefighting and poor fit due to facial hair are examples of barriers to effective use that could result in a poor face seal and the wearer’s not receiving the intended level of protection (De Vos et al., 2006; Haston, 2007; Sharkey, 1997). Moreover, the impact of breathing resistance on work performance and interference with verbal and visual communications are a concern for firefighters wearing respirators (Beason et al., 1996; Haston, 2007; Reinhardt and Ottmar, 2000; Sharkey, 1997). Additionally, studies by the United States Forest Service’s National Technology and Development Program in the 1990s found that full-face respirators were preferred for all-day prescribed fire activity because of decreased eye irritation. However, the full-face respirators did show increased heat stress, and study participants also reported headaches. Wildland firefighters often use eye irritation
as a signal to leave a particular area—a concern also noted in the study (Sharkey, 1997).
Several types of products are marketed to wildland firefighters (e.g., shrouds with filtration devices) but are not NIOSH-approved respirators and have not been studied to validate their protection claims. The National Fire Protection Agency (NFPA) created a wildland fire respiratory performance standard (NFPA, 2022), for the first time in 2011, updated in 2016 and 2022, which outlines the minimal requirements for construction of a wildland fire respirator. NFPA’s current model for such a respirator assumes long-duration, low-concentration exposure; design criteria include being lightweight and small, with easily replaceable filtration pieces. The key air purification required in this document includes carbon monoxide, organic vapors (cyclohexane), sulfur dioxide, nitrogen dioxide, formaldehyde, acrolein, hydrogen fluoride, and hydrogen cyanide. There are three different classes of respirator protection based on the performance requirements. However, no respirators have been designed or tested to the NFPA standard (Adetona et al., 2016).
A specific section in the USDA Forest Service Manual (FSM 5130, “Self-Contained Breathing Apparatus”) allows for wildland firefighters to be trained on and carry self-contained breathing apparatus (SCBAs) that are compliant with NFPA 1981, the Standard on Open-Circuit Self-Contained Breathing Apparatus (SCBA) for Emergency Services. These devices are not to be used in a wildland fire event; SCBAs may be used only when contaminants cannot be avoided (e.g., fires involving vehicles, dumps, structures, or other nonwildland fuels).
The implementation of an RPP for wildland firefighters would be difficult given the nature of the multiagency coordination of agency-specific policy that would be required, in addition to the challenges related to equipment. Training and education on the effective use of respiratory protection would need to cover hazard assessment and the limitations of respirators for protection from wildfire smoke. For example, use of respirators designed to filter particulates without the aid of a CO dosimeter could provide a false sense of security in the field and increase immediate risk to the wearer’s health (Haston, 2007). Administrative oversight and the development of a culture of safety are important for supporting the effective use of respiratory protection for wildland firefighters in the field (Reinhardt and Ottmar, 2000), but may be challenging to achieve in a workforce characterized by a large number of seasonal and volunteer workers.
Limited authoritative guidance is available on the use of respiratory protection by wildland firefighters and their agencies/departments for such hazards as wildfire smoke and infectious respiratory diseases. Federal guidance on the prevention of exposure to wildfire smoke mentions that
wildfire-specific PPE should be used, but does not specifically recommend the use of respirators (NIOSH, 2013), and notes that if respiratory protection must be used, once administrative and engineering controls have been exhausted and as determined by the agency/department, it needs to occur within the context of an RPP (Haston, 2007; NIOSH, 2021b; NWCG, 2010). Thus, wildland firefighters face a near total absence of established federal guidance on the use of respiratory protective devices as respiratory protection from wildfire smoke.
In contrast with exposure to wildfire smoke, the emergence of COVID-19 has led to the development of more detailed guidance for this worker population with respect to the use of respiratory protective devices. Authoritative guidance on the use of respiratory protection for wildland firefighters available via the NWCG provides the most comprehensive approach to instituting respiratory protective practices specifically tailored to the needs of this worker group (NWCG, 2021a). However, federal guidance from CDC specific to wildland firefighters has now expired (CDC, 2020b, 2021d), and there has been no clear replacement to address the unique needs of deployed wildland firefighting units (e.g., communal living in bunkhouses, safety of wearing respiratory protective devices, and what devices—respirator or nonrespirator face covering—should be used).
Agricultural Workers
Description of the Workforce, Work Environment, and Work Characteristics
Agricultural workers are a diverse population. Migrant farmworkers in the United States, many of whom come from Mexico and Central America, often serve as field hands to tend to various forms of livestock or harvest a wide range of crops over the course of the growing season. These worker groups are considered vulnerable to health hazards for a number of reasons. The time-sensitive nature of much agricultural work creates pressure on agricultural businesses to maintain work activities despite such environmental risks as extreme heat and poor air quality. Worker literacy and language considerations, including limited proficiency in English and, in some cases, Spanish, can pose challenges for effective worker training and communication regarding hazard identification and controls. Precarious immigration status—whether workers are undocumented or hired through the H2-A visa program—coupled with piece-rate payment schemes common within the industry often serve as disincentives for workers to demand stronger protections from respiratory and other hazards in their work.
Exposure and Health Impact Data
Inhalation hazards for agricultural workers may include inorganic dust from the soil; organic dust containing microorganisms, mycotoxins, or allergens; decomposition gasses; and various chemical agents, including pesticides. Exposures occur when harvesting, dealing with animals, and processing or storing grains or other plant matter, as well as when the soil, plants, or stables are treated with pesticides and disinfectants (Nguyen et al., 2018; Schenker et al., 1998; Viegas et al., 2013).
The need for adequate respiratory protection for agricultural workers has garnered additional attention in recent years in the context of large-scale wildfire events in the western United States (Riden et al., 2020). A recent review of the adverse health effects of such exposures identified risks for asthma, chronic obstructive pulmonary disease (COPD), bronchitis, and pneumonia (Cascio, 2018). Accounts of farmworkers being ordered to continue harvesting crops even as smoke and ash from nearby wildland fires filled the air led worker advocates in California to demand intervention from the California Division of Occupational Safety and Health (Cal/OSHA), which took the form of a new wildfire smoke standard promulgated as an emergency measure in 2019 and subsequently made permanent in 2021 (NASEM, 2019a).
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
Overall, few agricultural workers are covered by worksite RPPs (Culp et al., 2004; Greskevitch et al., 2007). This is particularly true for the large population of migrant farmworkers. As mentioned earlier in this chapter, a long-standing congressional appropriations provision has prohibited OSHA from any involvement in farms with 10 or fewer non-family workers (OSHA, 2014b).
The respiratory protection needs of agricultural workers exposed to dusts, molds, and chemicals from farm work are likely to differ in important ways from those of workers incidentally exposed to wildfire smoke. As discussed in Chapter 2, some states in the western United States have recently passed regulations designed to protect workers, including agricultural workers, from exposure to wildfire smoke. In July 2019, Cal/OSHA promulgated a standard requiring employers to institute various control measures when the Air Quality Index (AQI) for PM2.5 reaches certain thresholds as a result of nearby wildfires (Cal/OSHA, 2021c). The standard includes requirements for respiratory protection: if the AQI for PM2.5 exceeds 151, employers must provide filtering facepiece respirators and encourage their voluntary use; if the AQI for PM2.5 exceeds 500, employers
must require respirator use, along with mandatory fit testing, if work activities are to continue. Although the Cal/OSHA standard applies to all outdoor worksites, as well as indoor sites without adequate air filtration, a major focus has been on implementation of the standard in agriculture. Similar regulations have been passed in Washington and Oregon (Oregon OSHA, 2021; Washington State DOLI, 2021a).
Few employers in the agricultural industry have had prior experience with respiratory protection as part of their safety practices, and farmworkers often have limited understanding of the functional differences between filtering facepiece respirators and cloth face coverings (Riden et al., 2020). Increased knowledge and understanding of inhalation hazards is an important factor in promoting the use of respiratory protection among agricultural workers, particularly in cases in which hazards emanate from beyond the immediate work processes and procedures (e.g., wildfire smoke, aerosol transmissible diseases). Effective training and communication strategies need to take into account the unique needs and language, literacy, and educational characteristics of this workforce, particularly in the case of migrant and seasonal workers (Basinas et al., 2016; Earle-Richardson et al., 2014; Riden et al., 2020). However, training and education are not sufficient for ensuring proper and consistent use of respiratory protection. Such factors as device discomfort, increased heat load, difficulty breathing, and lost work hours associated with fit testing and medical clearance serve as notable disincentives for individual users (Earle-Richardson et al., 2014; Kusaka et al., 1993; Mpofu et al., 2002; Riden et al., 2020). In the absence of stronger regulatory requirements, employers may be discouraged from instituting RPPs. Larger and better-resourced agricultural operations are likely in a better position to institute such programs (Cramer et al., 2017; Kearney et al., 2014; Syamlal et al., 2013; Virolainen et al., 1987), suggesting the need for both education and resources to incentivize businesses of all sizes to adopt respiratory protective measures for their workers.
In reviewing the gray literature, the committee found several examples of authoritative guidance that addresses the use of respiratory protective devices by agricultural workers for occupational hazards inherent in farm work, as well as incidental exposures such as wildfire smoke and SARS-CoV-2.
CDC guidance specifically for agricultural workers with respect to COVID-19 (CDC, 2021a) has been superseded by universal guidance on mitigation of COVID-19 in workplaces, which is designated for unvaccinated workers or workers who are “otherwise at risk.” Updated OSHA guidance indicates that workers in agricultural processing work settings are deemed to be in this “at-risk” category (OSHA, 2021f). However the general OSHA guidance does not reflect the diversity of job roles and titles captured in the original CDC guidance (e.g., workers on farms vs. ranches), and it is
unclear whether the OSHA guidance for at-risk workers is intended to cover the broader category of agricultural workers. Both the now-expired guidance from CDC and the OSHA guidance provide information about the selection, use, and cleaning of respiratory protective devices.
NIOSH has developed guidance on the potential role of respiratory protective devices in controlling exposure to wildfire smoke as part of an RPP (NIOSH, 2021b); however, this guidance does not focus specifically on agricultural workers. Indeed, it appears that no federal guidance specific to this worker group and hazard that supports correct selection and use of respiratory protective devices is available beyond the recommendation to fulfill the components of an RPP. Similarly, guidance developed by Cal/OSHA to support the translation of its wildfire smoke standard into practice is employer focused (Cal/OSHA, 2018). Beyond following the requirements of an RPP once established, workers have little in the way of protection if their employers fail to comply. This gap in user-facing materials and tools for successful integration are addressed through such materials as those produced by the University of California, Davis’s Western Center for Agricultural Health and Safety. These materials, targeted to workers and employers in the region, include training visuals, discussion guides, tools, and checklists designed to support effective implementation in the field (WCAHS, 2021). Such efforts to support the application of standards in the field are essential, but it remains unclear to what degree agricultural workers and employers in areas where wildfire smoke is of concern have access to and utilize these materials and training programs.
One notable exception within the agricultural workers category with regards to having access to respiratory protection and comprehensive guidance on its use is pesticide handlers. Under the authority of the Federal Insecticide, Fungicide, and Rodenticide Act (FIFRA), EPA regulations preempt OSHA standards for pesticide applicators. For these workers, EPA administers a worker protection program that mandates respiratory protection. Occupational safety standards implemented under FIFRA to protect agricultural workers from pesticides include the pesticide applicator certification program, as well as the Agricultural Worker Protection Standard. As part of this responsibility, EPA published a guide directed at pesticide handlers (EPA, 1993) that provides guidance for users on different types of respirators and basic information about their use. Additionally, EPA, in coordination with the Pesticide Educational Resources Collaborative (PERC), developed resources to assist employers and business owners in complying with the worker protection standard (PERC, 2017). PERC also has developed and assembled a collection of resources for pesticide handlers and medical professionals that are both specific to respirator use for pesticide exposure (Rutgers University, n.d.) and more broadly pertinent
to respirator use in general (NIOSH, 2017b; OSHA, 2011a), designed to support safe and effective use of the devices in the field. Among the guidance available to agricultural workers, that provided to support the use of respiratory protection from standard to application in the field appears to be most complete for pesticide exposures.
Construction Workers
Description of the Workforce, Work Environment, and Work Characteristics
Construction firms are overwhelmingly small employers—90 percent employ fewer than 20 people—with limited resources for proper PPE or training for their workers. Small firms represent a disproportionate percentage of construction fatalities (CPWR, 2018) and are more likely than their larger counterparts to hire workers considered at a greater risk for injury, including young workers, those who are less educated, and immigrants (Belman and Levine, 2004; NIOSH, 2015c). One study found that the communication of safety and health information to subcontractors was twice as common in larger (500+ employees) than smaller (1–9 employees) firms (Jones, 2016).
Construction is second only to agriculture in the numbers of foreign-born and temporary workers employed. Approximately 30 percent of construction workers are Hispanic (compared with 17.7 percent of workers in all industries) (Brown et al., 2020), and 15.5 percent are employed by temporary agencies, which adds complexity to determining who is responsible for worker training (CPWR, 2018).
In 2016, the construction industry had a higher rate of union representation than all other industries combined (15.5 percent versus 11.7 percent), although union participation among trades varies significantly (CPWR, 2018). Union membership is an important factor in the safety and health protection of construction workers. Building trade unions integrate safety and health training into their apprenticeship programs to ensure that a solid safety culture is part of the transition from apprentice to journeyman, irrespective of trade. The Center for Construction Research and Training (CPWR) (2018) and Dodge Data and Analytics conducted a survey in 2017 using Dodge’s member contractor panel of roughly 3,000 construction firms, 334 of which participated, and found that union firms
- reported better performance of safety management and safety culture;
- were more likely to be aware of and practice Prevention through Design (a major NIOSH initiative);
- adopted more of the organization safety practices, safety policies, and safety culture indicators considered important by the researchers; and
- were more likely to offer and require general safety and health training and OSHA 10-hour and 30-hour courses for their workers (Wang et al., 2018).
Exposure and Health Impact Data
Inhalation hazards are common in the construction sector. A longitudinal survey of U.S. adults over age 50 showed that the proportion of respiratory cancer–related deaths for workers whose longest-duration job was in construction trades was nearly double that for white-collar workers. Additionally, construction workers were approximately twice as likely to die of nonmalignant respiratory diseases compared with white-collar workers (CPWR, 2018; Wang et al., 2016). The risk of death from lung cancer associated with 5 years of work in the construction industry was comparable to the risk associated with a personal or family history of cancer or a diagnosis of COPD (Dement et al., 2020). Over a 45-year working life, 16 percent of construction workers develop COPD and the lifetime risk of an occupational disease is 2–6 times greater in the construction trades than in nonconstruction work (Ringen et al., 2014).
The onset of the COVID-19 pandemic presented new challenges for construction workers because they were deemed essential workers and could not work from home (NIOSH, 2021a). Construction worksites presented increased risks because multiple trades were forced to coordinate their efforts, often on sites with tight footprints and work practices that required person-to-person interactions, rendering social distancing difficult. Although much of this work can be done outside, projects eventually require working indoors where ventilation may be limited, particularly in cold winter months when heating is a higher priority than circulating outside air (Araya, 2021). Valuable guidance has been developed to improve ventilation on construction sites to prevent the spread of COVID-19 (CPWR, 2021b); research on the implementation of this guidance is needed prior to another pandemic.
A recent study looking specifically at COVID-19 risk factors in the construction sector found about 60 percent of the workers had at least one underlying factor—such as heart or lung disease, diabetes, or being 65 or older—that put them at elevated risk of serious health outcomes or death (Brown et al., 2020). Another study found that the observed relative risk of hospitalization from COVID-19 among construction workers compared with other occupational categories among adults aged 18–64 was 4.9 (95 percent confidence interval [CI], 3.8–6.2). The authors identify construction
as a high-contact industry and describe its association with a higher level of community transmission of the disease and larger health disparities among racial and ethnic minority groups (Pasco et al., 2020).
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
Construction workers may have access to respirators, but they tend to be filtering facepiece respirators without accompanying training. A 2003 BLS survey showed that just under 10 percent of construction workers were required by their employer to use a respirator during a 12-month period (CPWR, 2007), and only half of those employers provided them with the training mandated by OSHA. The BLS survey indicated the respirators most commonly used in construction were for protection against paint vapors (44.7 percent), solvents (27.8 percent), and silica dust (24.1 percent). Where respirators were required, N95 FFRs and other disposable dust masks, which do not provide protection for the wearer against exposure to vapors and solvents, were used most frequently (77.8 percent), and elastomeric half-mask respirators were required for fewer than half of the tasks examined (40.5 percent). In the committee’s analysis of data from federal OSHA violations related to 1910.134(c)(1) issued January 1, 2015–December 31, 2020 (see Appendix A), construction was the second most commonly cited industry.
Several federal agencies, labor unions, and professional associations provide guidance for the construction workforce on a variety of inhalation hazards, including SARS-CoV-2. CDC guidance for construction workers on COVID-19 (CDC, 2021c,j) has expired and been replaced by general OSHA guidance (2021f), which does not use the term “construction worker” and is oriented to any workers who are not vaccinated or are vaccinated but working in higher-transmission areas. OSHA also supplies a page with dedicated guidance on the use of cloth face coverings that provides information for both employers and construction workers on selection, use, and care of these devices in the context of construction work settings (OSHA, 2021a). Labor unions and nongovernmental organizations have taken an active role in calling for and providing details on COVID-19 exposure control by employers, including the use of respiratory protective devices (CPWR and NABTU, 2020; LHSF, 2021). CPWR and North America’s Building Trade Unions (NABTU) standards for construction sites, updated in April 2020 in response to the COVID-19 pandemic, recommend the use of a fit-tested respirator as part of an established RPP, but notes that some local circumstances (e.g., recommendations by local governments or supply issues) may necessitate the use of cloth face coverings (CPWR and NABTU, 2020).
The committee identified just one example of federal guidance for exposure to wildfire smoke that is inclusive of construction workers (NIOSH, 2021b). Additionally, as described earlier in the section on agricultural workers, some guidance is available for employers in California to assist in their compliance with the wildfire smoke standards (Cal/OSHA, 2018), although the committee found no supportive user-oriented guidance during a search for additional guidance materials for this worker population.
Day Laborers
Description of the Workforce, Work Environment, and Work Characteristics
The day laborer workforce in the United States is composed largely of immigrant workers hired by homeowners, business owners, and small contractors on a short-term basis to carry out any number of construction, gardening and landscaping, and property maintenance tasks. A 2006 nationwide study of day laborers estimates that on any given day, 117,600 individuals were either looking for day labor jobs at street corners, curb-sides, and hiring centers, or working as day laborers (Valenzuela et al., 2006); numbers now are surely higher.
Employment relations for this group are characterized by temporary and informal work arrangements with few written contracts, and payments often made in cash (Riley and Guzman, 2017). Limited English-language proficiency and lack of authorized or permanent immigration status further contribute to the precarious circumstances of these workers (Fussell et al., 2018).
In addition to the standing day labor workforce, researchers have recently turned their attention to the role played by day laborers as “second responders” in the context of disaster response and recovery (discussed further in the section below on disaster response and recovery workers). Communities devastated by hurricanes, floods, wildfires, and other disasters have often seen an influx of day laborers in the weeks and months following disaster events, as immigrants and other contingent workers have sought jobs on cleanup and reconstruction projects (Cordero-Guzman et al., 2013; Costirilos, 2019; Delp et al., 2009; Fletcher et al., 2006; IDEPSCA, 2020; Theodore, 2017, 2020). Property owners, developers, and contractors, in turn, have come to rely on the ready availability of low-wage workers to serve as the backbone of disaster recovery efforts (Fussell et al., 2018).
Exposure and Health Impact Data
The occupational hazards and work-related injuries faced by day laborers often mirror, in both frequency and severity, those of workers performing comparable tasks under more conventional work arrangements (Burgel et al., 2015; Riley and Majano, 2021). The tasks performed by day laborers—particularly those working in postdisaster settings—may put them at risk for exposure to any number of inhalation hazards, including vapors from paints or solvents; mold, lead, or asbestos; wildfire ash; and dust and debris.
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
RPPs for the day labor workforce are effectively nonexistent. The informal and short-term nature of most assignments, particularly when workers are hired by homeowners, means that OSHA standards and enforcement generally do not apply. Meanwhile, workers’ reluctance to turn down dangerous assignments because of economic necessity and their lack of hazard awareness have led to little pushback from workers and little incentive for employers to invest in PPE or other forms of hazard control. In this context, the onus has largely fallen on worker advocates to educate these workers and encourage employers to take appropriate protective measures. Pilot projects to train workers on inhalation hazards and to distribute PPE through local worker centers have shown positive results in terms of raising workers’ hazard awareness and encouraging more frequent use of protective equipment, such as N95 FFRs (Contreras and Buchanan, 2012). And in the absence of formal RPPs, a number of day labor hiring sites around the country have taken the lead in offering training and fit testing for these workers, and negotiating with would-be employers on working conditions and use of adequate protections.
Federal guidance on respiratory protection specifically targeting the day labor workforce are nearly nonexistent. While general federal guidance, such as that from NIOSH on exposure to wildfire smoke and outdoor workers (NIOSH, 2021b), may be applicable, these workers are unlikely to be employed in a situation in which an RPP is established. The committee identified no other guidance on other inhalation hazards addressing use of respiratory protection by day laborers or targeted employers of these workers.
Health Care and Allied Health Workers
Description of the Workforce, Work Environment, and Work Characteristics
Consistent with the scope of the committee’s charge, this section addresses only those health care and allied health workers who would not be expected to be covered by a permanent RPP.10 These include home care workers, clinicians in solo private practices, dentists, and long-term care workers. Particularly warranting attention are those workers in informal settings who have no formal employers, including those who may be funded through state or local offices on aging through dual Medicare/Medicaid programs but are considered to have been hired by the client or the client’s family.
Many of the nearly 2 million homebound adults over age 65 in the United States may rely on informal family caregivers as well as home care workers provided through state and federal support (Ornstein et al., 2015), and as of 2020, 2.5 million U.S. adults were living in nursing homes or residential care facilities (Scales, 2020). Home care workers (including home health workers and personal care attendants) are disproportionately older women of color. Half have more than two chronic illnesses, nearly half live in households with incomes below $30,000, and nearly half are Medicaid recipients themselves (Bercovitz et al., 2011; Muramatsu et al., 2017). These paid home care workers are not consistently considered to be part of a health care team (Reckrey et al., 2020). Nursing assistants working in nursing homes and long-term care facilities are predominantly (92 percent) females of color and are younger than the average home care worker, with a workforce median age of 37 and 20 percent of workers being under the age of 24. The average nursing home assistant earns $13.38 per hour and $22,200 annually, and nearly 36 percent of this workforce requires public assistance because of these low earnings (Scales, 2020). Dental hygienists provide primary oral health services in dental offices, public health clinics, schools, and nursing homes, among other locations; 226,400 dental hygienists are currently employed in the United States (ADHA, 2021) and are predominantly female (IOM, 2009). Little is known about the demographics of health care workers working in small or private practices, given the breadth of the fields of practice and the wide geographic area in which they work.
___________________
10 As a result of the OSHA emergency temporary standard related to COVID-19, employers of some health care and allied health workers who typically have not had RPPs may now be required to implement such programs. However, this requirement is temporary.
Exposure and Health Impact Data
Home care Although systematic data and studies are lacking, home care workers who are not part of a home care agency are vulnerable to inhalation hazards, in part because of limited legal protections (home care work is considered a domestic service in some states and therefore is excluded from basic health and safety protections) (Nasol and Francisco-Menchavez, 2021), and as seen during the COVID-19 pandemic, because of such factors as limited access to respirators, limited provision of training, and lack of any formal organizational preparedness and employer support (Gershon et al., 2010). In a study comparing work–life experiences of agency and nonagency home care workers, agency workers reported receiving significantly more training and supervision compared with nonagency workers (Benjamin and Matthias, 2004). A qualitative study of 33 home care workers (home health and personal care aides and home attendants) revealed that these workers received inadequate respiratory protection support during the COVID-19 pandemic, in part because of PPE shortages. Moreover, these workers did not feel that their essential front-line work during the pandemic was recognized; rather, they felt “invisible” (Allison et al., 2020; Sterling et al., 2020). In another study, 86 percent of 384 respondents had received no training specific to performing their job functions during a pandemic, and just 5 percent reported that their employer had an established pandemic plan (Gershon et al., 2010). Additionally, access to training does not translate to effective use of respiratory protective devices. In this same study, just 16 percent of home health care workers surveyed had received a respirator from their employer; of these, fewer than 72 percent had received training on how to use the device, and only 28 percent had been fit tested on the device (Gershon et al., 2010). And as discussed earlier, in addition to this lack of training and lack of access to fit-tested respiratory protective devices, use of these devices can be associated with discomfort, including difficulty breathing and feelings of overheating, as well as challenges with visual and verbal communication, issues that are perceived as a barrier to effective patient care (Gershon et al., 2010; Mojtahedzadeh et al., 2021). Furthermore, home health aides and personal care aides include a significantly higher proportion of immigrant workers compared with some other health care occupation categories; and immigrant workers are known to be disproportionally negatively affected by COVID-19 (Gelatt, 2020).
Long-term care Long-term care settings, which include nursing homes (1,300,000 residents in the United States) and assisted living facilities (800,000 residents) (Harris-Kojetin et al., 2019), have always been vulnerable to many health care safety hazards, including inhalation hazards (Nasol and Francisco-Menchavez, 2021). COVID-19 had a disproportionately
negative impact on this health care sector, with a significantly higher positivity rate for both residents and care professionals, leading to transmission between unprotected care professionals and residents and across nursing home facilities. Although representing only 1 percent of the U.S. population, long-term care facilities have been linked to 4 percent of COVID-19 cases and 31 percent of deaths nationwide (The New York Times, 2021). As of September 2021, more than 136,500 residents and more than 2,070 care professionals in nursing homes had died from COVID-19 (CMS, 2021).
Care professionals who work in assisted living facilities experience similar safety problems, including inadequate protection against inhalation hazards. Assisted living facilities have notoriously failed to comply with wage and labor standards (Shah, 2017), and concerns about their inadequate preparation for a potential pandemic were reported well in advance of COVID-19 (Lum et al., 2014).
Care professionals working in dentistry settings Dentistry entails the use of rotary dental and surgical instruments (e.g., hand pieces or ultrasonic scalers and air-water syringes), which can aerosolize saliva, blood, microorganisms, and other debris. Given the unique nature of dental practice, which requires professionals to operate very close to the patient’s mouth, the risk of aerosol transmission of infectious agents is high (Clementini et al., 2020; Gandolfi et al., 2020; Zemouri et al., 2017, 2020). A New York Times article titled “The Workers Who Face the Greatest Coronavirus Risk” identifies dentists and dental hygienists as more at risk than any other health care workers, including nurses, personal care aides, and general practitioners (Gamio, 2020).
Other care professionals in small or solo private practices Despite closures and telehealth-based alternatives, health care workers in solo practices have been disproportionately affected by COVID-19 (Rubin, 2020). An investigation of 1,004 COVID-related deaths among health care workers globally as of May 13, 2020, for example, found a significantly higher proportion of deaths from COVID-19 occurring among physicians who practice family medicine or primary care (general practitioners) (Gouda et al., 2020).
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
Inconsistent compliance with recommended guidelines for respirator use has long been a major problem in health care. NIOSH conducted a 2011 web-based survey of more than 10,000 health care workers who routinely use or are exposed to certain chemical agents (including nurses, pharmacy practitioners, technologists/technicians, anesthesia care professionals,
respiratory therapists, and dental care professionals) in the United States (Wizner et al., 2018). Only 18 percent of respondents surveyed reported using a respirator as protection against chemical agents, of which 24.9 percent reported being fit tested for the respirator they used. When respondents were asked about their respiratory protection practices when potentially exposed to 1 of the 10 specific airborne hazards on which the survey focused, their responses varied widely (see Figure 3-5). The high percentage reporting use of a surgical mask when working with these specific airborne hazards raised concerns about inappropriate use of these masks in lieu of respirators (Wizner et al., 2018).
When the survey participants who reported not using a respirator when potentially exposed to one of the 10 aerosol hazards were asked about their reason for not following the recommended respiratory protection practices, factors related to organizational characteristics were found to play a major role: respirator use not part of the local protocol (32 percent of responses), exposure perceived as minimal (21 percent), respirator not provided by employer (12 percent), respirator not readily available in work area (11 percent), no other colleague or peer in the workplace using it (10 percent), and engineering control being used (8 percent). Furthermore, job characteristics (i.e., job type, involvement with direct patient care) and worksite characteristics (number of employees) were found to be predictive of appropriate respirator use. Specifically, those employees working in large organizations (number of employees >1,000) reported significantly greater respirator use when potentially exposed to one of the 10 specific aerosol hazards compared with those working in smaller organizations (<100 employees). On the other hand, characteristics of individual health care workers (e.g., age, education level) were not a significant predictor of respirator use, a finding consistent with those of other studies (Hines et al., 2014; Nichol et al., 2013). These findings are consistent with and highlight the importance of (1) a systems approach to respiratory protection and (2) a human-centered approach to respirator design to improve and sustain appropriate use.
The Hospital Respiratory Protection Program Toolkit was developed in 2015 by NIOSH to address these challenges and the need for a coordinated systems approach to incorporate respiratory protective device use into the hospital setting (NIOSH, 2015b).
The vast majority of health care workers in the United States, including those who work in states with OSHA-approved State Plans that do not provide this protection or those in states with federal OSHA programs, are not covered by a specific, formal, permanent aerosol transmissible disease standard. Such standards are currently under development and have been adopted by a number of states. Although these standards are necessary for prevention, existing risk assessments related to the pandemic suggest that all health care workers—from clinicians performing aerosol-generating
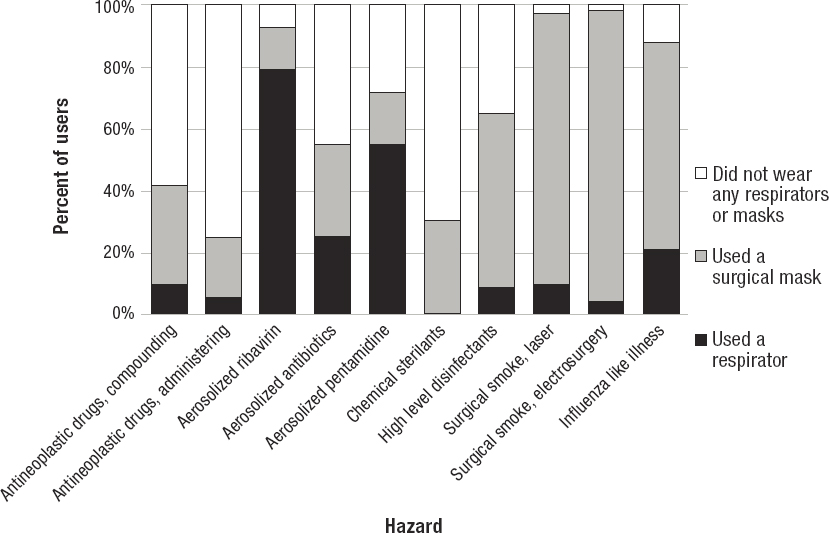
SOURCE: Wizner et al., 2018.
procedures; to clinicians in general; to clerical, environmental services, dietary, security, and other support staff in hospitals, nursing homes, and other long-term care facilities or in home care—may need to be included in full formal RPPs under OSHA’s Respiratory Protection Standard. Such programs need to extend to employees in private medical or dental offices as well, and to be strongly encouraged for self-employed practitioners. OSHA’s ETS for workers in health care settings, while temporary, represented an important step forward in addressing this need. Many of these health care and allied health worker groups are also a focus for OSHA’s National Emphasis Program, which targets inspections to high-hazard industries so as to better ensure that employees in those industries are protected from contracting COVID-19 (OSHA, 2021c).
Government underregulation of long-term care and assisted living facilities has been identified as a major factor in these facilities serving as “hot spots” for COVID-19 (Nasol and Francisco-Menchavez, 2021). As opposed to nursing homes, which are regulated at the federal level, assisted living facilities are regulated at the state level, and thus they vary greatly as to infection prevention and control requirements. Viral outbreaks are a major problem in these facilities because of gaps in infection prevention and control programs, written procedures, and training, so that staff have inadequate knowledge about appropriate respiratory protection (Bamberg et al., 2013; CDC, 2020a; Kossover et al., 2014).
Limited authoritative guidance is available that directly focuses on workers in long-term care and assisted living facilities with respect to the use of respiratory protective devices for COVID-19. However CDC definitions of health care workers are inclusive of these worker groups, so they can be encompassed by broader guidance for workers and employers in health care settings, such as CDC’s interim guidance on infection control in health care settings (CDC, 2021e). State-level guidance, such as California’s Interim Guidance for Protecting Workers at Skilled Nursing and Long-term Care Facilities, also exist, providing a structure for employers’ expansion of respiratory protection for these groups (Cal/OSHA, 2021a).
Few small or solo private health care practices (such as those in family medicine, internal medicine, and pediatrics) have adequate infrastructure or resources for providing safe care during a pandemic, such as COVID-19, or have any formal RPP. Similarly, a substantial proportion of dental care professionals in the United States work in the private sector, half in solo practice, without a formal RPP (ADA, 2021), although in the wake of the COVID-19 pandemic, one might plausibly expect a substantial increase in the establishment of RPPs that comply with OSHA regulations among dental care practices (OSHA, 2021b). Yet, while some federal guidance is available for health care practitioners in small practices, such as dentists
(OSHA, 2021b), to aid with such efforts, most of the available guidance is oriented to larger health care settings.
Workers at Increased Risk of Exposure to Infectious Diseases from Interaction with the Public or Other Workers During Epidemics and Pandemics
Description of the Workforce, Work Environment, and Work Characteristics
The COVID-19 pandemic and the 2009 H1N1 pandemic have demonstrated the importance of respiratory aerosol transmission to a wide range of public-facing workers, including teachers, wait staff, day care providers, public transportation workers, janitors, and workers in correctional facilities and homeless shelters, among many others. Those working in close proximity to others, such as in manufacturing and food processing, also have experienced high rates of worksite transmission. Ancillary personnel (e.g., Transportation Security Administration [TSA] workers in airports, USDA inspectors in meat and poultry processing plants) may be exposed as well. During the COVID-19 pandemic, many previously public-facing workers were able to work remotely, while others, chiefly in the hospitality industry, lost their jobs. However, large industry sectors, including housing construction, agriculture and food processing, energy, utilities, transportation, manufacturing, security, and others, were declared “essential,” exempted from stay-at-home orders, and continued to work with inadequate respiratory protection. Many of these workers lacked paid sick leave and faced job loss for missed work, exacerbating the risk of disease transmission.
Exposure and Health Impact Data
During the H1N1 pandemic, differential increases in absences due to illness (Tora-Rocamora et al., 2012), in hospitalizations, and in mortality were identified among different industry and occupational categories, as well as among different racial and ethnic groups, indicating occupational risk (Luckhaupt et al., 2012). Tora-Rocamora and colleagues (2012) identified the health, education, and social services sectors as seeing the earliest and sharpest rise in illness-related absences relative to other industry sectors. Comparison of the occupational categories of hospitalized adults with confirmed influenza in 10 U.S. states with the proportions employed in those sectors using the National Health Interview Survey revealed disproportionate representation among workers in transportation and warehousing, administrative support, waste management and remediation
services, health care, and accommodation and food service (Luckhaupt et al., 2012). The H1N1 pandemic also saw disparities by race, ethnicity, and socioeconomic status in self-reported influenza-like illnesses and increased household disease transmission associated with lack of available sick leave (Kumar et al., 2011).
Variation in COVID-19 impacts by industry and occupation Compared with the H1N1 pandemic, the current COVID-19 pandemic has been much more lethal for workers, although failure to capture surveillance data by industry and occupation for COVID-19 infections and deaths in the United States (with the exception of health care workers) has severely limited understanding of the pandemic’s toll. The press has consistently outpaced public health agencies in identifying important trends, ranging from health disparities to worksite outbreaks (Jordan and Dickerson, 2020).
Despite limitations of the available data, some data are available on the differential impacts of COVID-19 by industry/sector:
- Early data from six Asian countries suggested excess infections among health care workers, drivers and transport workers, services and sales workers, cleaning and domestic workers, public safety workers, and religious professionals, with increases among different groups appearing at different times (Lan et al., 2020).
- In California, workers in the health care, facilities, food and agriculture, government and community, manufacturing, retail, transportation, and logistics sectors experienced significantly increased mortality risk ratios; again, different industries peaked earlier or later in the pandemic in this regard (Chen et al., 2021).
- Washington State reported COVID-19 infection and hospitalization rates disproportionate to employment levels in the food processing, air transportation, residential services, merchants/wholesalers of nondurable goods, justice/public safety, agriculture, and health care sectors (Wuellner, 2021). In some instances, worksites concentrated exposures, contributing to community outbreaks.
- Occupational information available for 555 death certificates among those aged 16–64 dying from COVID-19 documented excess rates in the health care support; transportation and material moving; food preparation and serving; building and grounds cleaning and maintenance; production; construction and extraction; installation, maintenance, and repair; protective service; personal care and service; arts, design, entertainment, sports, and media; and community and social service sectors (Hawkins et al., 2021).
- Finally, the Council of State and Territorial Epidemiologists recently adopted exposure criteria for classifying occupational transmission
- of COVID-19 based on Department of Labor O*NET work designation for three risk factors—public-facing work, working indoors, and working in close proximity (Council of State and Territorial Epidemiologists, 2021).
Characteristics of work and the workforce that increase risk and vulnerability include exposure to infectious aerosols among those not able to work remotely; lack of appropriate occupational safety and health protections, including training; densely populated, poorly ventilated, or enclosed work spaces; prolonged face-to-face or physical contact where social distancing is not practiced; demographic characteristics; comorbidities; and coexposures (Carlsten et al., 2021). Individuals working in grocery stores and pharmacies exemplify essential workers who would be expected to experience prolonged exposures to the public, with little or no safety and health precautions in place and significant socioeconomic and demographic challenges. An investigation of COVID-19 rates in a Massachusetts grocery store in May 2020 found that 20 percent of the 104 workers screened by polymerase chain reaction (PCR) testing had positive viral assays; fewer than 50 percent of the workers who tested positive were symptomatic (Lan et al., 2021). COVID-19 infection rates among grocery workers represented by a local United Food and Commercial Workers Union (UFCW) in the mid-Atlantic region were lower than background county rates for those stores in which managers implemented a variety of safety measures, including enforced mask use by customers (Crowell et al., 2021). In one of the earliest and most devastating outbreaks of COVID-19 identified among U.S. workers, employees in meat and poultry processing plants demonstrated an extraordinarily high risk not only for infection and death but also for seeding of community outbreaks. Based on incomplete data reported by 30 states through May 31, 2020, CDC identified 8,978 infected workers across 742 agricultural and food processing worksites, with 55 deaths (Waltenburg et al., 2021).
Transportation issues arose early in the pandemic, with cruise ships and a U.S. aircraft carrier reporting explosive outbreaks (Kasper et al., 2020), and deaths among bus drivers and other transportation workers being reported through news media and transit unions. By April 9, 2020, at least 33 New York City transit workers had died from COVID-19, with bus drivers being disproportionately impacted (Martinez, 2020).
Some of the highest COVID-19 infection rates were seen among public safety and correctional workers. As of April 21, 2020, an incomplete U.S. sampling revealed COVID-19 infections among 4,893 inmates and 2,778 corrections personnel, including 88 and 15 fatalities, respectively (Wallace et al., 2020). By November 24, 2020, Colorado had reported a total of 204,000 COVID-19 cases, including 15,526 hospitalizations and 2,821 deaths, among incarcerated individuals (Quan et al., 2021). Following
compassionate early release, a project in Colorado found 4 of 165 formerly incarcerated individuals to be infected, as well as 4 of 20 staff working in community organizations assisting with community reentry (Quan et al., 2021). A seroprevalence study of SARS-CoV-2 antibodies in New York City identified the highest rate among correctional staff (39.2 percent seropositive), with traffic officers, security guards, firefighters, and others with first responder or security responsibilities having elevated rates as well (Sami et al., 2021). Furthermore, among 37,640 Federal Bureau of Prisons staff, SARS-CoV-2 infection was most prevalent among staff in institutions where social distancing by staff and inmates was limited (Toblin et al., 2021).
Workers and volunteers in homeless shelters have long been aware of respiratory transmission of tuberculosis and other infectious diseases. In March 2020, outbreak investigations at three King County, Washington, homeless shelters identified COVID-19 infections among 18 percent of residents and 21 percent of staff members (Tobolowsky et al., 2020). A subsequent cross-sectional study of 14 King County homeless shelters found a 2 percent infection rate by PCR testing; of 157 staff tested, 4 tested positive (Rogers et al., 2020).
Variation in COVID-19 impacts by race, ethnicity, and socioeconomic status Employees designated as “essential” and unable to work remotely are disproportionately low-wage racial and ethnic minorities (Hawkins, 2020). Black workers, for example, make up approximately 26 percent of public transit workers but just 11.9 percent of the total working population, while Hispanic workers constitute 40.2 percent of workers providing building cleaning services despite representing only 16.8 percent of all U.S. workers (see Table 3-3). The failure to protect large groups of these workers contributed to their widely disproportionate experience of infection and mortality from COVID-19 relative to other population groups. The demographics of the essential workforce are presented in Table 3-3, from the Center for Economic and Policy Research (Rho et al., 2020). The differential occupational exposures of these workers contributed to widespread infection among multigenerational households in populations with high rates of preexisting conditions associated with the social determinants of health, compounded by a lack of access to appropriate health care.
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
Evidence from the H1N1 pandemic and the severity of outcomes from COVID-19 point to the need for a complete safety and health program adhering to the hierarchy of controls, including a formal RPP, among large sectors of the U.S. workforce currently not likely to be covered by such a
TABLE 3-3 Characteristics of Workers in Front-Line Industries
| ALL WORKERS | ALL FRONTLINE INDUSTRIES | GROCERY, CONVENIENCE, AND DRUG STORES | PUBLIC TRANSIT | TRUCKING, WAREHOUSE, AND POSTAL SERVICE | BUILDING CLEANING SERVICES | HEALTH CARE | CHILD CARE AND SOCIAL SERVICES | |
|---|---|---|---|---|---|---|---|---|
| All Workers (16+) | 152,600,169 | 31,673,098 | 6,817,890 | 804,495 | 3,128,922 | 1,484,993 | 16,103,877 | 3,332,921 |
| Female | 47.4% | 64.4% | 50.5% | 29.1% | 22.7% | 53.2% | 76.8% | 85.2% |
| Full/Part-Time | ||||||||
| Full-Time | 78.6% | 73.3% | 63.7% | 81.0% | 90.5% | 62.6% | 79.8% | 67.4% |
| Part-Time | 21.4% | 24.7% | 36.3% | 19.0% | 9.5% | 37.4% | 20.2% | 32.6% |
| Race/Ethnicity | ||||||||
| White | 63.5% | 58.8% | 59.5% | 54.7% | 56.4% | 43.4% | 61.1% | 55.8% |
| Black | 11.9% | 17.0% | 14.2% | 26.0% | 18.2% | 12.6% | 17.5% | 19.3% |
| Hispanic | 16.8% | 16.3% | 18.5% | 14.0% | 20.0% | 40.2% | 12.1% | 18.0% |
| AAPI | 6.6% | 6.7% | 6.6% | 4.1% | 4.2% | 2.4% | 8.0% | 5.3% |
| Other | 1.2% | 1.2% | 1.3% | 1.2% | 1.1% | 1.3% | 1.2% | 1.5% |
| Foreign Born | 17.1% | 17.3% | 15.7% | 15.2% | 17.9% | 38.2% | 16.2% | 17.0% |
| Education Level |
| LTHS | 9.3% | 8.5% | 13.0% | 6.9% | 12.7% | 26.5% | 4.3% | 7.9% |
| HS | 24.5% | 25.8% | 36.0% | 38.1% | 42.6% | 38.5% | 17.2% | 21.7% |
| Some College | 32.0% | 36.3% | 35.2% | 39.4% | 34.2% | 26.0% | 38.2% | 34.7% |
| College | 21.6% | 18.1% | 11.9% | 11.4% | 8.7% | 7.4% | 22.8% | 22.9% |
| Advanced | 12.6% | 11.4% | 4.0% | 4.1% | 1.8% | 1.5% | 17.5% | 12.8% |
| Age 50+ | 33.1% | 33.9% | 27.4% | 46.7% | 40.2% | 35.6% | 34.6% | 34.4% |
| Home Ownership | 65.3% | 63.6% | 59.6% | 68.2% | 65.5% | 50.0% | 66.7% | 60.1% |
| Public Transit Commute to Work | 5.1% | 4.8% | 4.5% | 9.0% | 2.4% | 7.8% | 4.6% | 6.8% |
| Compensation and Benefits | ||||||||
| Below Poverty Line | 6.7% | 7.2% | 10.0% | 4.5% | 4.7% | 15.9% | 5.2% | 10.8% |
| <200% Poverty Line | 20.6% | 23.0% | 30.1% | 16.0% | 19.2% | 42.4% | 17.8% | 30.0% |
| No Health Insurance | 11.0% | 9.9% | 12.1% | 5.8% | 14.8% | 29.1% | 6.3% | 10.4% |
| ALL WORKERS | ALL FRONTLINE INDUSTRIES | GROCERY, CONVENIENCE, AND DRUG STORES | PUBLIC TRANSIT | TRUCKING, WAREHOUSE, AND POSTAL SERVICE | BUILDING CLEANING SERVICES | HEALTH CARE | CHILD CARE AND SOCIAL SERVICES | |
|---|---|---|---|---|---|---|---|---|
| Family Responsibilities | ||||||||
| Child in home | 35.8% | 35.9% | 33.9% | 32.6% | 33.3% | 38.8% | 36.9% | 36.0% |
| Senior (age 65+) in home | 14.8% | 16.0% | 16.8% | 18.4% | 14.9% | 15.5% | 15.3% | 18.5% |
SOURCE: CEPR’s Analysis of American Community Survey, 2014-2018 5-Year Estimates. This work is licensed under a Creative Commons Attribution 4.0 International License. It is attributed to the Center for Economic and Policy Research, and the original version can be found at https://cepr.net/a-basic-demographic-profile-of-workers-in-frontline-industries.
SOURCE: Rho et al., 2020
NOTES: “Front-line industries” refers to the cumulative industries presented in the table (e.g., grocery stores, public transit, postal service). AAPI = Asian American and Pacific Islander; HS = high school; LTHS = less than high school.
program. Employers of health care support, transportation, manufacturing, retail, service, and other workers at increased risk from infectious pandemic agents have a responsibility to provide them safe working conditions. However, this responsibility is not consistently met, impacting not only these workers’ health but also their willingness to perform their job functions during a public health emergency. Organizational preparedness that includes enforcing existing safety and health protections, as well as providing access to respirators and developing and implementing formal RPPs, among other measures, is necessary to ensure worker safety and willingness to work (Gershon et al., 2010). Misclassification of transportation, cleaning, and other workers as self-employed results in large numbers of workers for whom safety and health protections are lacking. Here again, the primary response required is adequate enforcement of existing Department of Labor protections.
Failure to protect essential workers, including health care workers, marked the first year of the pandemic. Several factors may have contributed to this inadequate protection of workers and the lack of formal RPPs:
- Both WHO and CDC were slow to recognize and acknowledge the significant role of airborne transmission of SARS-CoV-2 by aerosols (Tanne, 2020). As late as July 2020, for example, WHO posted the following statement, effectively dismissing the need for RPPs against aerosols in most settings, except certain medical situations: “Current evidence suggests that SARS-CoV-2 is primarily transmitted between people via respiratory droplets and contact routes—although aerosolization in medical settings where aerosol generating procedures are used is also another possible mode of transmission” (WHO, 2020).
- Early on, the United States experienced a widely reported and acknowledged shortage of PPE, including respirators (CRS, 2020).
- Throughout the first year of the pandemic, OSHA failed to respond adequately to worker complaints about hazardous working conditions or enforce its Respiratory Protection Standard in settings characterized by SARS-CoV-2 exposures (Whoriskey et al., 2020).
- U.S. labor laws and changing hiring practices have contributed to a workforce with large numbers of at-will workers,11 an absence of paid
___________________
11 “At-will means that an employer can terminate an employee at any time for any reason, except an illegal one, or for no reason without incurring legal liability. Likewise, an employee is free to leave a job at any time for any or no reason with no adverse legal consequences. At-will also means that an employer can change the terms of the employment relationship with no notice and no consequences” (NCSL, 2021). However, any retaliation for raising safety and health concerns with the employer or OSHA is illegal under 29 C.F.R. § 1977.3, which outlines protections for employees for certain actions related to occupational safety, although it is not an easy law to enforce (29 C.F.R. § 1977.3).
- sick leave, and workers in informal working arrangements, leaving these workers without pathways for negotiating for basic safety and health protections, such as RPPs (Kumar, 2011; Quinlan, 2021).
Thus, for the vast majority of essential workers, meaningful improvements in overall safety and health during pandemics will require enhancing existing mechanisms designed to ensure that work does not endanger the workers or their families and communities.
On the other hand, the genuinely self-employed, such as those offering home day care services or owning very small groceries or laundries, and their employees may fall outside of current regulatory requirements and would appropriately rely on the types of protections available to the public. The same is true of essential workers who are able to socially distance, such as some utility workers, as well as workers in offices where social distancing and improved ventilation are rigorously maintained. The challenge these worksites may present is one of outreach and communication, often complicated by language or other barriers. Efforts to address the needs of the self-employed and small business owners will require specific focus, for example, on the leadership role small business owners may play in the use of respiratory protection (Jones et al., 2021).
While OSHA provides extensive enforcement and outreach guidance for RPPs, CDC/NIOSH, the National Institute of Environmental Health Sciences’ (NIEHS’s) Worker Training Program, and OSHA’s Susan Harwood Training Grant program have developed or funded others to create extensive libraries supporting worker outreach and training (CDC, 2021f,h,i; NIEHS, 2021; OSHA, 2021i). A number of unions, educational institutions, nonprofit organizations, and worker centers have collaborated with end users to develop training for both workers and small businesses (CPWR, 2021a; SEIU, 2021). CDC maintains several occupation-specific guidance documents, including new or updated guidance for restaurant and bar operators, in-home social service providers, public transportation operators, and airline crews, which include links to general guidance on types of respiratory protective devices and their use (CDC, 2021b,g,k,l). OSHA guidance is available for small business owners who are required to establish an RPP to address occupational exposures that necessitate respiratory protection (OSHA, 2011a), but this guidance is not intended for use by employees and does not address the needs of all workers at increased risk of exposure to infectious agents. Future health communications about respiratory protection would benefit from clear messaging that is appropriate to workers’ literacy levels (Pan et al., 2020). Moreover, research into improved respirator design is necessary to address the needs of workers who must communicate with the public while using a respirator; to assess the potential for respirator contamination under various use scenarios; to improve comfort, ease of use,
and the ability to communicate during use; and to identify, evaluate, and determine how best to implement approaches to encouraging correct use.
Disaster Response and Recovery Workers
Description of the Workforce, Work Environment, and Work Characteristics
Various workers may be engaged in different phases of the disaster cycle (see Figure 3-6). The initial rescue phase of any disaster involves immediate action by responders to save lives. With the transition to the recovery and cleanup stage, other types of workers are brought in.
Construction workers are routinely pulled into disaster responses of all types. During the cleanup at the World Trade Center, for example, nearly all of the building trades were onsite: heavy equipment operators moved debris, ironworkers cut beams and rigged loads, electricians rerouted phone and electrical lines, laborers moved debris and sealed contaminated areas, carpenters built barriers, and teamsters hauled debris in large articulated dump trucks. Most of these workers had no training in disaster response and received no site safety and health training until 78 days after the towers had fallen (Lippy, 2002). Operators of heavy equipment are regularly pulled into much smaller disasters, such as house collapses or flooding, when the first hours are critical to saving lives.
Day laborers have also been engaged in response and recovery efforts for many disasters over the past two decades, including
- the attacks on the World Trade Center in 2001 (EHS Today, 2002);
- Hurricane Katrina in 2005 (Delp et al., 2009; Fletcher et al., 2006);
- Hurricane Sandy in 2012 (Berger, 2012; Cordero-Guzman et al., 2013);
- Hurricane Harvey in 2017 (Theodore, 2017); and
- California wildfires, including the Thomas Fire in 2017, the Woolsey Fire in 2018, and the Camp Fire in 2018 (Costirilos, 2019; IDEPSCA, 2020).
Of note, day laborers have increasingly been engaged in both wildfire first response and recovery/cleanup efforts (Costirilos, 2020).
Volunteers from the public are another important population of workers during most disaster responses. They often are the first on the scene to respond to car crashes and house fires or to save neighbors during floods or wildfires, and are the primary rescuers of fellow citizens from collapsed buildings (Macintyre et al., 2006). Even among firefighters, volunteers greatly outnumber professionals: the NFPA estimates that of the total
number of firefighters in the United States in 2018, 67 percent were volunteers (Evarts and Stein, 2020).
Volunteers often feel compelled to help during major disasters, as was the case with the many volunteers who helped serve food to responders at the World Trade Center through such organizations as the Red Cross, which also deployed an estimated 220,000 volunteers to hurricanes Katrina and Rita (American Red Cross, 2006). And many spontaneous volunteers show up at disaster sites with no affiliation, just a desire to help. Sauer and colleagues (2014) sought to understand the use of volunteers in disasters by surveying 24 of the 51 total member organizations in National Voluntary Organizations Active in Disaster (VOAD). Among those organizations, 79 percent reported regularly using spontaneous volunteers during disasters, and 68 percent found these volunteers to be useful (Sauer et al., 2014), although they were rarely credentialed, and only half (53 percent) of the organizations provided them with training.
Exposure and Health Impact Data
Workers engaged in the response to or recovery from disasters often work at uncontrolled sites where the hazards are not fully known. In the initial response phase, there is often a “risk a life to save a life” mindset. It is critical to delineate clearly when the rescue phase has concluded and the disaster has shifted to a more controlled recovery phase, during which the hazards may still be present but the pace can be slowed and the work shifts reduced, allowing responders to catch up on sleep and meals, which also reduces their risk; the key is to recognize that the longer the rescue phase continues, the greater is the risk. Yet, the shift from rescue to recovery operations is not always apparent, as was the case during the World Trade Center response, in which the rescue phase was reportedly extended through June 2002 for the entire 9 months of debris removal operations (Newman, 2013) even though the last survivor had been rescued on September 12 (Cloud, 2002). The Federal Response Plan that was in effect during the response assigned OSHA the role of making “available safety and health specialists to provide safety-specific assistance to affected disaster response agencies as required by the Federal Coordinating Officer” (FEMA, 1999, p. 260). However, enforcement was limited, and once workers were onsite, there was little leverage for ensuring compliance, and as a result, respirator use was documented as inconsistent (Lippy, 2002). Eventually, a disaster site can transition to a nearly normal construction site (see Figure 3-6), although risks to workers at the site may still be elevated. Three aspects of disaster recovery greatly increase the likelihood that construction workers will confront risks to health and safety:
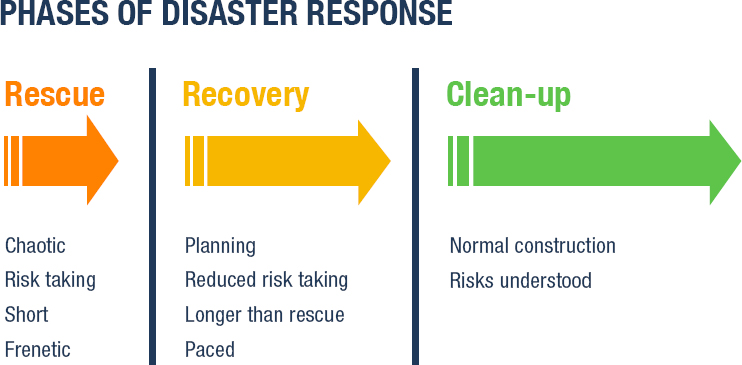
SOURCE: Courtesy of Bruce Lippy, committee member.
- “the rapid pace at which recovery operations are undertaken, including working long hours and without necessary rest breaks;
- the prevalence of multiple hazards at any given worksite; and
- the fact that hazards may be unknown to work crews that are entering a worksite.” (Theodore, 2017, p. 8)
Inhalation hazards in disaster scenarios can include ash and debris, mold, asbestos, and other airborne contaminants, depending on the nature of the disaster (Delp et al., 2009). And as discussed at length above, in the case of wildfires, exposure to wildfire smoke has been associated with respiratory symptoms, as was the case, for example, with day laborers and domestic workers who reported breathing difficulties following the Woolsey fire (IDEPSCA, 2020).
Respiratory Protection and Regulatory Frameworks (Standards, Guidance, and Oversight)
Disaster response and recovery workers are a diverse population whose respiratory protection needs may differ. Studies of past disasters have shown that different types of disaster workers may be more or less likely to use respiratory protection, highlighting the need for improved training, selection, fit testing, and consistency in use for respiratory protection among emergency responders (Antao et al., 2011).
An important factor impacting the respiratory risks to workers engaged in response and recovery efforts are the changes to regulations that may occur during disaster conditions. In some cases, OSHA standards and enforcement operations may be suspended in disaster-affected areas, removing incentives for employers to provide adequate protections (Fussell et al., 2018). The Army Corps of Engineers, often involved in disaster response and recovery, has its own regulations (EM385 manual), which are similar to OSHA’s.
Construction workers
Inadequate use of respiratory protection by construction workers at the World Trade Center is a well-documented problem. Fit testing was not widely available until more than 1 month into the disaster response. More than 100,000 elastomeric half-mask respirators were distributed but compliance with their use was routinely poor: operators of heavy equipment working in the restricted zone generally wore their elastomeric half-mask respirators less than 50 percent of the time (Lippy, 2002). In contrast, compliance with respirator use was reported to be around 90 percent at the Fresh Kills site where the debris was taken, an operation managed by the Army Corps of Engineers, which was effective at getting workers to wear respiratory protection during the World Trade Center cleanup effort (DePalma, 2006).
OSHA’s Hazardous Waste Operations and Emergency Response (HAZWOPER) standard (1910.120) clearly stipulates the training needed for each type of responder, and specifically allows construction workers to have less training relative to other responders. Under 1910.120(q)(4), the agency identifies “skilled support personnel” as
personnel, not necessarily an employer’s own employees, who are skilled in the operation of certain equipment …; and who are needed temporarily to perform immediate emergency support work that cannot reasonably be performed in a timely fashion by an employer’s own employees and who will be or may be exposed to the hazards at an emergency response scene.
These skilled support personnel are not required to meet employers’ training requirements for regular employees, merely to receive an initial briefing at the worksite before beginning response work. The briefing must include instruction in the wearing of appropriate PPE but can be of any length. The assumption is that workers deemed skilled support personnel will be onsite only briefly during the emergency phase and, if staying when the site transitions to cleanup activities, would then receive appropriate HAZWOPER training. However, this assumption proved incorrect during the World Trade Center response. To remedy this deficit, OSHA, working with safety and health representatives of the building trades unions, developed two OSHA Disaster Site Worker courses (OTI 7600 and OTI 5600)
that are now delivered across the country. Both are voluntary, however, and it has proven difficult to convince construction employers of the need to have their workers trained in anticipation of a disaster.
An overlooked and rarely cited requirement in the HAZWOPER standard is 1910.120 (o) which requires employers to “develop and implement procedures for the introduction of effective new technologies and equipment for the improved protection of employees working with hazardous waste clean-up operations, and the same shall be implemented as part of the site safety and health program to assure that employee protection is being maintained.” This requirement is essentially acknowledging the position of respiratory protection at the bottom of the hierarchy of controls and promoting more effective strategies. Limited but noteworthy efforts were made to implement control technologies at the World Trade Center cleanup (Lippy, 2003).
Day laborers
Despite the increasingly frequent role of day laborers in disaster response and recovery efforts, employers often fail to provide them with PPE or training, let alone other aspects of an effective RPP (e.g., fit testing, medical clearance), and respiratory problems may result (Delp et al., 2009). In one study day laborers reported access to key types of personal protective equipment, such as respirators, but in many cases these devices were being used long after their effective use period had ended (Delp et al., 2009). In other cases, workers reported trying to protect themselves by tying a t-shirt over their mouth and nose or otherwise trying to prevent exposure to health hazards (Theodore, 2017). For example, most of the workers involved in recovery and cleanup activities at the World Trade Center site were day laborers performing tasks such as removal of asbestos. Many of these workers describe not being given training on the hazards faced and not being provided with any type of respiratory protection or protective clothing (EHS Today, 2002). Likewise, only 18 percent of day laborers in New Orleans after Hurricane Katrina reported having access to respirators (Fletcher et al., 2006). More than 60 percent of day laborers (nearly two-thirds) surveyed during the Hurricane Harvey cleanup had no respirator; many used inadequate equipment or simply covered their noses and mouths with t-shirts. Given the unpredictability of the specific conditions that will be encountered by second responders involved in post-disaster cleanup at a worksite, it is incumbent on employers to provide appropriate PPE, including respiratory protective equipment to their crews (Theodore, 2020). Making safety and health training for day laborers in disaster areas a priority is essential, as is providing them with PPE.
Volunteer disaster response and recovery workers
Disaster volunteers routinely show up at disaster sites without PPE, such as respiratory protective
devices, or knowledge of the risks they face, which places strains on the existing response infrastructure (Van Hoving et al., 2010). Among the tens of thousands of responders at Ground Zero, for example, spontaneous volunteers carried water to the heavy equipment operators on the smoking pile of debris at the World Trade Center unaware of the hazards to which they were being exposed.
From a risk standpoint, there is a great difference between affiliated and unaffiliated volunteers. The latter population receives little or no training for the most part and does not understand critical safety issues. It is not surprising then, that 42 percent of the volunteer organizations reported injuries and two fatalities among their volunteer responders (Sauer et al., 2014). The researchers concluded that while the use of spontaneous volunteers is widespread, nongovernmental organizations are “not necessarily structured to incorporate them effectively. More structured efforts to integrate [spontaneous volunteers] are critical to safe and effective disaster response” (Sauer et al., 2014, p. 65).
NIEHS’s Worker Training Program has been a major force in protecting this vulnerable population, providing training in worker safety and health in disaster response to more than 20 grantees for more than 20 years. This adaptable training infrastructure is based on experience in training workers responding to Ground Zero, the Gulf oil spill, wildfires, and hurricanes and allows for just-in-time development of materials for future disasters (Rosen et al., 2015). In 2020, the Worker Training Program collaborated with the American Industrial Hygiene Association (AIHA) to develop user-oriented guidance for volunteers on COVID-19 prevention practices in response to growing concerns about infection-related health risks for volunteers (AIHA, 2020). Additionally, NIEHS (2013) has developed mold remediation guidance oriented toward disaster recovery volunteers and essential workers, providing them with detailed information about the selection and use of respiratory protection and other types of PPE.
Summary and Synthesis
This section has considered multiple worker groups that are potentially exposed to inhalation hazards in the workplace. The exposures discussed are diverse and may be intermittent (e.g., for those exposed to wildfire smoke and high levels of ambient air pollution) or more sustained (e.g., for construction workers). Some worker groups have situational exposures (e.g., those working in cleanup following a disaster, or those exposed to SARS-CoV-2 through contacts with people across multiple sectors beyond health care workers).
These worker groups share several characteristics: a wide range of employers, many with small numbers of employees; transient employment,
sometimes initiated on an urgent basis; a wide range of sociodemographic backgrounds and characteristics, some of which may contribute to susceptibility; and variable access to health care. Additionally, there may be no central touch point for enumerating these employees and their employers and implementing programs to protect them from exposure to inhalation hazards. Unique challenges are faced by some of these workers, such as day laborers, who represent a fluid group that may be hired because the jobs may involve hazardous exposures; such workers are unlikely to file OSHA complaints, whether because of the informal and/or temporary nature of their work assignments, fear of employer retaliation, or potential loss of employment.
Some data have been collected for some worker groups, such as wildland firefighters, a group stressed by an increasing number of larger fires. Respiratory protection for wildland firefighters has been considered, but without resolution. Further complexity stems from the multiple groups that employ these firefighters.
The COVID-19 pandemic has highlighted the enormous needs for respiratory protection for large numbers of workers across many sectors both to provide protection for the individual workers and to reduce transmission. The pandemic has surfaced problems in supply chains; in understanding of the role and effectiveness of various devices for transmission control; and in rapid implementation of a broadly reaching, multisectoral program.
The landscape of guidance available to support use of respiratory protection by the diverse worker groups discussed here is variable and has been developed by a broad range of stakeholders, including federal agencies, labor unions, professional associations, academic institutions, and nonprofit organizations (see Box 3-3 for a selection of this guidance). Much of the federal guidance reviewed for this study (outside of that focused on clinical or allied health settings) provides information about the use of face coverings and medical masks rather than respirators and as of September 2021, was labeled as temporary or expired. Additionally, much of the guidance reviewed is oriented to employers and tends to be technical in nature; in general, the committee found a paucity of user-friendly tools and resources (e.g., checklists for employers, instructive graphics, Spanish translations) targeted to specific worker groups to support the selection and use of respiratory protective devices by both employers and workers, including those workers who are self-employed or day laborers. Such materials that were identified were generally produced by trusted organizations, such as unions, associations, dedicated nonprofits, or academic centers. However, not all occupations and businesses requiring respiratory protection are represented by such organizations and have access to the supportive services these organizations can provide with regard to translating and tailoring federal standards and guidance to the needs and contexts of that worker
population. Additional research and investment may therefore be needed to tailor, translate, and disseminate technical guidance and trainings for additional worker populations and hazards of concern.
For all worker groups, there are substantial gaps in the evidence available on the hazards faced, the levels of exposure, the feasibility of an RPP, and the types of devices needed. While NIOSH approves respirators for use under an OSHA RPP, it does not have a robust and ongoing targeted research or applied intervention program to evaluate the actual implementation and use of respiratory protective devices, especially in worker populations that have not been the traditional focus of guidance and compliance efforts. Such research needs to include an emphasis on usability issues, including comfort, ease of use, and the ability to communicate while using the device, as well as to identify, evaluate, and implement approaches for encouraging correct use. Small businesses and difficult-to-reach populations need to be a particular priority for research aimed at determining how best to establish and implement an RPP, carried out with worker participation.
REFERENCES
ADA (American Dental Association). 2021. The dentist workforce—Key facts [Infographic]. Health Policy Institute. https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIgraphic_0221_1.pdf (accessed October 8, 2021).
Adetona, O., T. E. Reinhardt, J. Domitrovich, G. Broyles, A. M. Adetona, M. T. Kleinman, R. D. Ottmar, and L. P. Naeher. 2016. Review of the health effects of wildland fire smoke on wildland firefighters and the public. Inhalation Toxicology 28(3):95-139.
ADHA (American Dental Hygienists Association). 2021. Facts about the dental hygiene workforce in the United States. Chicago, IL: ADHA.
AFL-CIO. 2020. Is your face covring keeping you safe? https://aflcio.org/sites/default/files/2020-09/FaceCoveringKeepingYouSafe_ENG.pdf (accessed December 21, 2021).
AIHA (American Industrial Hygiene Association). 2020. Guidance to protect volunteers from COVID-19 during natural disaster response and recovery. In collaboration with the National Institute of Environmental Health Sciences Worker Training Program. https://aiha-assets.sfo2.digitaloceanspaces.com/AIHA/resources/Guidance-Documents/Guidance-to-Protect-Volunteers-From-COVID-19-During-Natural-Disaster-Response-and-Recovery_GuidanceDocument.pdf (accessed October 8, 2021).
Allison, T. A., A. Oh, and K. L. Harrison. 2020. Extreme vulnerability of home care-workers during the COVID-19 pandemic—A call to action. JAMA Internal Medicine 180(11):1459-1460.
American Red Cross. 2006. A year of healing: The American Red Cross response to Hurricanes Katrina, Rita and Wilma. https://reliefweb.int/sites/reliefweb.int/files/resources/7485303F8791D511492571D20010543E-arc-usa-21aug.pdf (accessed October 8, 2021).
Antao, V. C., L. L. Pallos, Y. K. Shim, J. H. Sapp Ii, R. M. Brackbill, J. E. Cone, S. D. Stellman, and M. R. Farfel. 2011. Respiratory protective equipment, mask use, and respiratory outcomes among World Trade Center rescue and recovery workers. American Journal of Industrial Medicine 54(12):897-905.
Araya, F. 2021. Modeling the spread of COVID-19 on construction workers: An agent-based approach. Safety Science 133:105022.
Bamberg, W., M. Moore, N. Stone, J. Perz, R. Dantes, and J. Wendt. 2013. Notes from the field: Outbreak of severe respiratory illness in an assisted-living facility—Colorado, 2012. Morbidity and Mortality Weekly Report 62(12):230-231.
Basinas, I., T. Sigsgaard, J. H. Bønløkke, N. T. Andersen, Ø. Omland, H. Kromhout, and V. Schlünssen. 2016. Feedback on measured dust concentrations reduces exposure levels among farmers. Annals of Occupational Hygiene 60(7):812-824.
Beason, D., J. S. Johnson, K. L. Foote, and W. A. Weaver. 1996. Summary report California Department of Forestry and Fire Protection evaluation of full-face air-purifying respirators for wildland fire fighting use. https://digital.library.unt.edu/ark:/67531/metadc666330/m2/1/high_res_d/207046.pdf (accessed October 8, 2021).
Beckman, S., B. Materna, S. Goldmacher, J. Zipprich, M. D’Alessandro, D. Novak, and R. Harrison. 2013. Evaluation of respiratory protection programs and practices in California hospitals during the 2009–2010 H1N1 influenza pandemic. American Journal of Infection Control 41(11):1024-1031.
Belman, D., and D. I. Levine. 2004. Size, skill and sorting. Labour 18(4):515-728.
Benjamin, A. E., and R. E. Matthias. 2004. Work-life differences and outcomes for agency and consumer-directed home-care workers. Gerontologist 44(4):479-488.
Bercovitz, A., A. Moss, M. Sengupta, E. Y. Park-Lee, A. Jones, L. D. Harris-Kojetin, and M. R. Squillace. 2011. An overview of home health aides: United States, 2007. National Health Statistics Reports 34:1-31.
Berger, J. 2012. For day laborers, used to scraping by, hurricane creates a wealth of work. The New York Times, December 30. https://www.nytimes.com/2012/12/31/nyregion/day-laborers-find-steady-work-after-hurricane-sandy.html (accessed October 8, 2021).
BLS (Bureau of Labor Statistics). 2020. National occupational employment and wage statistics, May 2020. https://www.bls.gov/oes/tables.htm (accessed October 8, 2021).
BLS. 2021a. Information collection activities; Comment request. Federal Register 86(46): 13914-13915. https://www.govinfo.gov/content/pkg/FR-2021-03-11/pdf/2021-05043.pdf (accessed October 8, 2021).
BLS. 2021b. Survey of occupational injuries and illnesses data. https://www.bls.gov/iif/soiidata.htm#summary (accessed October 7, 2021).
Bose, N. 2021. Labor secretary supports classifying gig workers as employees. Reuters, April 29, 2021.
Brown, S., R. Brooks, and X. S. Dong. 2020. Coronavirus and health disparities in construction. Data Bulletin. Center for Construction Research and Training. https://stacks.cdc.gov/view/cdc/107027 (accessed October 8, 2021).
Broyles, G. 2013. Wildland firefighter smoke exposure. U.S. Department of Agriculture. https://www.fs.fed.us/t-d/pubs/pdfpubs/pdf13511803/pdf13511803dpi100.pdf (accessed October 8, 2021).
Burgel, B. J., R. W. Nelson, and M. C. White. 2015. Work-related health complaints and injuries, and health and safety perceptions of Latino day laborers. Workplace Health & Safety 63(8):350-361.
Burgess, J. L., C. J. Nanson, D. M. Bolstad-Johnson, R. Gerkin, T. A. Hysong, R. C. Lantz, D. L. Sherrill, C. D. Crutchfield, S. F. Quan, A. M. Bernard, and M. L. Witten. 2001. Adverse respiratory effects following overhaul in firefighters. Journal of Occupational & Environmental Medicine 43(5):467-473.
Butler, C., S. Marsh, J. W. Domitrovich, and J. Helmkamp. 2017. Wildland fire fighter deaths in the United States: A comparison of existing surveillance systems. Journal of Occupational and Environmental Hygiene 14(4):258-270.
Cal/OSHA (California Division of Occupational Safety and Health). 2018. Respiratory protection during fire cleanup. https://www.dir.ca.gov/dosh/Fire_Resp_Protection.html (accessed September 28, 2021).
Cal/OSHA. 2020a. § 3205. COVID-19 prevention. https://www.dir.ca.gov/dosh/.archive/title8/3205-Nov.30.2020.html (accessed August 2, 2021).
Cal/OSHA. 2020b. Aerosol transmissible disease. Division of Occupational Safety and Health Publications Unit. https://www.dir.ca.gov/dosh/dosh_publications/ATD-Guide.pdf (accessed October 8, 2021).
Cal/OSHA. 2020c. General industry safety orders. https://www.dir.ca.gov/title8/sub7.html (accessed October 8, 2021).
Cal/OSHA. 2021a. Interim guidance for protecting workers at skilled nursing and long-term care facilities from exposure to coronavirus disease (COVID-19). https://www.dir.ca.gov/dosh/Coronavirus/Skilled-Nursing.html (accessed September 29, 2021).
Cal/OSHA. 2021b. Revisions to the COVID-19 prevention emergency temporary standards frequently asked questions. https://www.dir.ca.gov/dosh/coronavirus/Revisions-FAQ.html#whatchanged (accessed August 2, 2021).
Cal/OSHA. 2021c. Protection from wildfire smoke. https://www.dir.ca.gov/title8/5141_1.html (accessed October 8, 2021).
Carlsten, C., M. Gulati, S. Hines, C. Rose, K. Scott, S. M. Tarlo, K. Torén, A. Sood, and R. E. de la Hoz. 2021. COVID-19 as an occupational disease. American Journal of Industrial Medicine 64(4):227-237.
Carre, F. 2015. (In)dependent contractor misclassification. Washington, DC: Economic Policy Institute.
Cascio, W. E. 2018. Wildland fire smoke and human health. Science of the Total Environment 624:586-595.
CDC (Centers for Disease Control and Prevention). 2017. About the National Health and Nutrition Examination Survey. https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed October 8, 2021).
CDC. 2020a. Healthcare-associated hepatitis B and C outbreaks (≥ 2 cases) reported to the CDC 2008–2019. https://www.cdc.gov/hepatitis/outbreaks/healthcarehepoutbreaktable.htm (accessed October 8, 2021).
CDC. 2020b. What firefighters and EMS providers need to know about COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/firefighter-EMS.html (accessed September 28, 2021).
CDC. 2021a. Agricultural workers and employers. https://www.cdc.gov/coronavirus/2019ncov/community/guidance-agricultural-workers.html#print (accessed September 28, 2021).
CDC. 2021b. Considerations for restaurant and bar operators. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/business-employers/bars-restaurants.html (accessed September 22, 2021).
CDC. 2021c. Construction COVID-19 checklists for employers and employees. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/construction-worker-check-lists.html (accessed September 28, 2021).
CDC. 2021d. FAQS and communication resources for wildland firefighters. https://www.cdc.gov/coronavirus/2019-ncov/community/wildland-firefighters-faq.html (accessed September 28, 2021).
CDC. 2021e. Interim infection prevention and control recommendations for healthcare personnel during the coronavirus disease 2019 (COVID-19) pandemic. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (accessed September 29, 2021).
CDC. 2021f. Manufacturing workers and employers. https://www.cdc.gov/coronavirus/2019ncov/community/guidance-manufacturing-workers-employers.html (accessed September 29, 2021).
CDC. 2021g. Updated guidance for airlines and airline crew. https://www.cdc.gov/quarantine/air/managing-sick-travelers/ncov-airlines.html (accessed September 22, 2021).
CDC. 2021h. What beauty salon and barbershop employees need to know about COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/beauty-salon-barber-employees.html (accessed September 29, 2021).
CDC. 2021i. What bus transit operators need to know about COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/bus-transit-employees.html (accessed September 29, 2021).
CDC. 2021j. What construction workers need to know about COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/construction-workers.html (accessed September 28, 2021).
CDC. 2021k. What in-home social service providers and clients need to know about COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/community/in-home-social-services.html (accessed September 22, 2021).
CDC. 2021l. What transit station workers need to know about COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/transit-station-employees.html (accessed September 22, 2021).
CDC. 2021m. Meat and poultry processing workers and employers: Interim guidance from cdc and the occupational safety and health administration (OSHA). https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/meat-poultry-processing-workers-employers.html#print (accessed December 21, 2021).
Chen, Y.-H., M. Glymour, A. Riley, J. Balmes, K. Duchowny, R. Harrison, E. Matthay, and K. Bibbins-Domingo. 2021. Excess mortality associated with the COVID-19 pandemic among Californians 18–65 years of age, by occupational sector and occupation: March through November 2020. PLoS ONE 16(6):e0252454.
Cifuentes, M., J. Boyer, D. A. Lombardi, and L. Punnett. 2010. Use of O*NET as a job exposure matrix: A literature review. American Journal of Industrial Medicine 53(9):898-914.
Clementini, M., M. Raspini, L. Barbato, F. Bernardelli, G. Braga, C. Di Gioia, C. Littarru, F. Oreglia, E. Brambilla, I. Iavicoli, V. Pinchi, L. Landi, N. Marco Sforza, R. Cavalcanti, A. Crea, and F. Cairo. 2020. Aerosol transmission for SARS-CoV-2 in the dental practice. A review by SIDP COVID-19 task-force. Oral Diseases. https://pubmed.ncbi.nlm.nih.gov/33124127 (accessed October 8, 2021).
Cloud, J. 2002. The survivor: A miracle’s cost. Time, September 9.
CMS (Centers for Medicare & Medicaid Services). 2021. COVID-19 nursing home data. https://data.cms.gov/covid-19/covid-19-nursing-home-data (accessed October 5, 2021).
Conger, K. 2021. California’s gig worker law is unconstitutional, judge rules. The New York Times, August 20.
Contreras, E., and S. Buchanan. 2012. Piloting a personal protection equipment distribution program among Chicago day laborers. American Journal of Industrial Medicine 55(2):159-166.
Cordero-Guzman, H., E. Pantaleon, and M. Chavez. 2013. Day labor, worker centers & disaster relief work in the aftermath of Hurricane Sandy. https://www.gc.cuny.edu/CUNY_GC/media/365-Images/Aftermath-of-Hurricane-Sandy-Report-FINAL-11-4-13.pdf (accessed October 26, 2021).
Costirilos, T. 2019. Immigrant workers endure brutal labor conditions as California burns. Center for Health Journalism, University of Southern California, Annenberg. https://centerforhealthjournalism.org/2019/07/27/immigrant-workers-endure-brutal-labor-conditions-california-burns (accessed October 26, 2021).
Costirilos, T. 2020. When fires burn through neighborhoods, some immigrant workers become first responders. Crosscurrents. KALW Public Media. https://www.kalw.org/show/cross-currents/2020-02-27/when-fires-burn-though-neighborhoods-some-immigrants-workers-become-first-responders#stream/0 (accessed October 26, 2021).
Council of State and Territorial Epidemiologists. 2021. Occupational health publications. https://www.cste.org/page/OHPublications (accessed October 4, 2021).
Cowan, D. M., S. M. Benson, T. J. Cheng, S. Hecht, N. M. Boulos, and J. Henshaw. 2017. Evaluation of reported fatality data associated with workers using respiratory protection in the United States (1990–2012). Archives of Environmental & Occupational Health 72(4):235-246.
CPWR (The Center for Construction Research and Training). 2007. The construction chart book: The U.S. construction industry and its workers. https://www.cpwr.com/wp-content/uploads/publications/CB4_Final-for-web.pdf (accessed October 8, 2021).
CPWR. 2018. The construction chart book. https://www.cpwr.com/wp-content/uploads/publications/The_6th_Edition_Construction_eChart_Book.pdf (accessed October 8, 2021).
CPWR. 2021a. COVID-19 resources. https://www.cpwr.com/covid-19-resources (accessed October 7, 2021).
CPWR. 2021b. Quick tips to increase ventilation at indoor construction sites without operating HVAC systems. https://www.cpwr.com/wp-content/uploads/CPWR-COVID-19-ventilation-guidance-1-14-21.pdf (accessed September 28, 2021).
CPWR and NABTU (North America’s Building Trades Unions). 2020. NABTU and CPWR COVID-19 standards for U.S. construction sites. https://www.cpwr.com/wp-content/uploads/publications/NABTU_CPWR_Standards_COVID-19.pdf (accessed October 8, 2021).
Cramer, M. E., M. J. Wendl, H. Sayles, E. Duysen, and C. Achutan. 2017. Knowledge, attitudes, and practices for respiratory and hearing health among Midwestern farmers. Public Health Nursing 34(4):348-358.
Crowell, N. A., A. Hanson, L. Boudreau, R. Robbins, and R. K. Sokas. 2021. Union efforts to reduce COVID-19 infections among grocery store workers. New Solutions 31(2):170-177.
CRS (Congressional Research Service). 2020. COVID-19 and Domestic PPE Production and Distribution: Issues and Policy Options. https://crsreports.congress.gov/product/pdf/R/R46628 (accessed October 8, 2021).
Culp, K., and M. Umbarger. 2004. Seasonal and migrant agricultural workers: a neglected workforce. AAOHN Journal 52(9):203-209.
De Vos, A. J. B. M., A. Cook, B. Devine, P. J. Thompson, and P. Weinstein. 2006. Effect of protective filters on fire fighter respiratory health during simulated bushfire smoke exposure. American Journal of Industrial Medicine 49(9):740-750.
Delp, L., L. Podolsky, and T. Aguilar. 2009. Risk amid recovery: Occupational health and safety of Latino day laborers in the aftermath of the Gulf Coast hurricanes. Organization & Environment 22(4):479-490.
Dement, J. M., K. Ringen, S. Hines, K. Cranford, and P. Quinn. 2020. Lung cancer mortality among construction workers: Implications for early detection. Occupational and Environmental Medicine 77(4):207-213.
DePalma, A. 2006. Air masks at issue in claims of 9/11 illnesses. The New York Times, June 5. https://www.nytimes.com/2006/06/05/nyregion/05masks.html (accessed October 8, 2021).
Department of the Army. 1990. Army programs: The army respiratory protection program. https://armypubs.army.mil/epubs/DR_pubs/DR_a/pdf/web/r11_34.pdf (accessed October 8, 2021).
Department of the Army. 2018. Toxic chemical agent safety standards. https://armypubs.army.mil/epubs/DR_pubs/DR_a/pdf/web/ARN12692_PAM385-61_WEB_FINALL.pdf (accessed October 8, 2021).
DOL and NIOSH (Department of Labor and National Institute for Occupational Safety and Health). 2003. Respirator usage in private sector firms, 2001. https://www.cdc.gov/niosh/docs/respsurv/default.html (accessed October 8, 2021).
Domitrovich, J. W., G. A. Broyles, R. D. Ottmar, T. E. Reinhardt, L. P. Naeher, M. T. Kleinman, K. M. Navarro, C. E. Mackay, and O. Adetona. 2017. Wildland fire smoke health effects on wildland firefighters and the public. Final report to the Joint Fire Science Program. Missoula, MT: U.S. Forest Service. https://www.frames.gov/catalog/24570 (accessed October 8, 2021).
Doney, B. C., D. W. Groce, D. L. Campbell, M. F. Greskevitch, W. A. Hoffman, P. J. Middendorf, G. Syamlal, and K. M. Bang. 2005. A survey of private sector respirator use in the United States: An overview of findings. Journal of Occupational and Environmental Hygiene 2(5):267-276.
Earle-Richardson, G., T. Fiske, S. Wyckoff, J. Shuford, and J. May. 2014. Respiratory fit testing for farmworkers in the Black Dirt region of Hudson Valley, New York. Journal of Agromedicine 19(4):346-353.
Easterling, G. H., and S. Prince. 2007. Respiratory protection programs for firefighters: A survey of practices for the state of Kentucky. Public Health Reports 122(6):725-732. https://doi.org/10.1177/003335490712200604.
EHS Today. 2002. Mobile health clinic tests cleanup workers at WTC. https://www.ehstoday.com/archive/article/21905530/mobile-health-clinic-tests-cleanup-workers-at-wtc (accessed October 8, 2021).
EPA (Environmental Protection Agency). 1993. Protect yourself from pesticides—Guide for pesticide handlers. https://www.epa.gov/sites/default/files/2015-06/documents/wps_handler_training_english_735_b_06_003_dec_1993.pdf (accessed October 8, 2021).
Evarts, B., and G. P. Stein. 2020. US fire department profile 2018. https://www.nfpa.org/-/media/Files/News-and-Research/Fire-statistics-and-reports/Emergency-responders/osfdprofile.pdf (accessed October 8, 2021).
Executive Office of the President. 2021. Protecting worker health and safety. Federal Register 86(15):7211-7213.
FEMA (Federal Emergency Management Agency). 1999. Federal response plan. https://biotech.law.lsu.edu/blaw/FEMA/frpfull.pdf (accessed December 15, 2021).
Fletcher, L. W., P. Pham, E. Stover, and P. Vinck. 2006. Rebuilding after Katrina: A population-based study of labor and human rights in New Orleans. https://escholarship.org/uc/item/5jc0909m (accessed October 8, 2021).
Fussell, E., L. Delp, K. Riley, S. Chavez, and A. Valenzuela, Jr. 2018. Implications of social and legal status on immigrants’ health in disaster zones. American Journal of Public Health 108(12):1617-1620.
Gamio, L. 2020. The workers who face the greatest coronavirus risk. The New York Times, March 15. https://www.nytimes.com/interactive/2020/03/15/business/economy/coronavirus-worker-risk.html (accessed October 8, 2021).
Gandolfi, M. G., F. Zamparini, A. Spinelli, V. Sambri, and C. Prati. 2020. Risks of aerosol contamination in dental procedures during the second wave of COVID-19—Experience and proposals of innovative IPC in dental practice. International Journal of Environmental Research and Public Health 17(23).
Gaughan, D. M., C. A. Piacitelli, B. T. Chen, B. F. Law, M. A. Virji, N. T. Edwards, P. L. Enright, D. E. Schwegler-Berry, S. S. Leonard, G. R. Wagner, L. Kobzik, S. N. Kales, M. D. Hughes, D. C. Christiani, P. D. Siegel, J. M. Cox-Ganser, and M. D. Hoover. 2014. Exposures and cross-shift lung function declines in wildland firefighters. Journal of Occupational and Environmental Hygiene 11(9):591-603.
Gelatt, J. 2020. Immigrant workers—Vital to the U.S. COVID-19 response, disproportionately vulnerable. Migration Policy Institute. https://www.migrationpolicy.org/research/immigrant-workers-us-covid-19-response (accessed October 8, 2021).
Gershon, R. R., L. A. Magda, A. N. Canton, H. E. Riley, F. Wiggins, W. Young, and M. F. Sherman. 2010. Pandemic-related ability and willingness in home healthcare workers. American Journal of Disaster Medicine 5(1):15-26.
Gibbs, J. L., and M. W. Nonnenmann. 2020. OSHA voluntary respirator use: Challenges incurred with use of N95 filtering facepiece respirators during the COVID-19 pandemic. Toxicology and Industrial Health 36(9):681-688.
Gouda, D., P. Singh, P. Gouda, and B. Goudra. 2020. The demography of deaths in healthcare workers—An overview of 1004 reported COVID-19 deaths. American Board of Family Medicine. https://www.jabfm.org/sites/default/files/COVID_20-0248.pdf (accessed October 8, 2021).
Grauvogel, L. W. 1986. Effectiveness of a positive pressure respirator for controlling lead exposure in acid storage battery manufacturing. American Industrial Hygiene Association Journal 47(2):144-146.
Greskevitch, M., B. Doney, D. Groce, G. Syamlal, and K. M. Bang. 2008. Respirator use and practices in agricultural crop production establishments. Journal of Agromedicine 12(3):25-31.
Hampton, T., R. Crunkhorn, N. Lowe, J. Bhat, E. Hogg, W. Afifi, S. De, I. Street, R. Sharma, M. Krishnan, R. Clarke, S. Dasgupta, S. Ratnayake, and S. Sharma. 2020. The negative impact of wearing personal protective equipment on communication during coronavirus disease 2019. Journal of Laryngology & Otology 134(7):577-581.
Harris, H. E., W. C. DeSieghardt, W. A. Burgess, and P. C. Reist. 1974. Respirator usage and effectiveness in bituminous coal mining operations. American Industrial Hygiene Association Journal 35(3):159-164.
Harris-Kojetin, L., M. Sengupta, J. Lendon, V. Rome, R. Valverde, and C. Caffrey. 2019. Long-term care providers and services users in the United States, 2015–2016. Vital Health Statistics 3(43).
Haston, D. 2007. Respirator usage by wildland firefighters. Fire management tech tips. U.S. Department of Agriculture Fire Service. https://www.fs.fed.us/t-d/pubs/pdf/hi_res/07511301hi.pdf (accessed October 26, 2021).
Hawkins, D. 2020. Differential occupational risk for COVID-19 and other infection exposure according to race and ethnicity. American Journal of Industrial Medicine 63(9):817-820.
Hawkins, D., L. Davis, and D. Kriebel. 2021. COVID-19 deaths by occupation, Massachusetts, March 1–July 31, 2020. American Journal of Industrial Medicine 64(4):238-244.
Hignett, S., R. Welsh, and J. Banerjee. 2020. Human factors issues of working in personal protective equipment during the COVID-19 pandemic. Anaesthesia 76.
Hines, L., E. Rees, and N. Pavelchak. 2014. Respiratory protection policies and practices among the health care workforce exposed to influenza in New York State: Evaluating emergency preparedness for the next pandemic. American Journal of Infection Control 42(3):240-245.
Hyatt, E. C. 1984. Respirators: How well do they really protect? International Society of Respiratory Protection 2(1).
IDEPSCA (Instituto de Educación Popular del Sur de California). 2020. On the frontlines: The role of domestic workers and day laborers in confronting recent wildfires in southern california. California Domestic Workers Coalition. https://www.cadomesticworkers.org/news/on-the-frontlines-the-role-of-domestic-workers-and-day-laborers-in-confronting-recent-wildfires-in-california (accessed October 8, 2021).
ILO (International Labour Office). 2013. National system for recording and notification of occupational diseases: Practical guide. https://www.ilo.org/wcmsp5/groups/public/--ed_protect/---protrav/---safework/documents/publication/wcms_210950.pdf (accessed October 8, 2021).
International Brotherhood of Teamsters. 2020. Facemask and respirator use: Coronavirus. https://teamster.org/wp-content/uploads/2020/05/4620ibtsafetyandhealthcovid19facemaskandrespiratoruse.pdf (accessed December 21, 2021).
IOM (Institute of Medicine). 2009. The U.S. oral health workforce in the coming decade: Workshop summary. Washington, DC: The National Academies Press.
IOM and NRC (National Research Council). 2008. The personal protective technology program at NIOSH: Reviews of research programs of the National Institute for Occupational Safety and Health. Washington, DC: The National Academies Press.
Jones, H. J., R. Hutchins, P. Brown, S. Crute, L. Ntumba, and C. Ward. 2021. Barriers related to mask wearing in African American neighborhood businesses. Journal of Community Health 46(5):1008-1012.
Jones, S. A. 2016. Building a safety culture: Improving safety and health management in the construction industry. Smart Market Report. https://www.cpwr.com/wp-content/uploads/publications/Building-a-Safety-Culture-SmartMarket-Report-2016-ff.pdf (accessed October 25, 2021).
Jordan, M., and C. Dickerson. 2020. Poultry worker’s death highlights spread of coronavirus in meat plants. The New York Times, April 9. https://www.nytimes.com/2020/04/09/us/coronavirus-chicken-meat-processing-plants-immigrants.html (accessed October 8, 2021).
Kasper, M. R., J. R. Geibe, C. L. Sears, A. J. Riegodedios, T. Luse, A. M. Von Thun, M. B. McGinnis, N. Olson, D. Houskamp, R. Fenequito, T. H. Burgess, A. W. Armstrong, G. DeLong, R. J. Hawkins, and B. L. Gillingham. 2020. An outbreak of COVID-19 on an aircraft carrier. New England Journal of Medicine 383(25):2417-2426.
Kearney, G. D., R. Shaw, M. Prentice, and R. Tutor-Marcom. 2014. Evaluation of respiratory symptoms and respiratory protection behavior among poultry workers in small farming operations. Journal of Agromedicine 19(2):162-170.
Kossover, R. A., C. J. Chi, M. E. Wise, A. H. Tran, N. D. Chande, and J. F. Perz. 2014. Infection prevention and control standards in assisted living facilities: Are residents’ needs being met? Journal of the American Medical Directors Association 15(1):47-53.
Kumar, S., S. C. Quinn, K. H. Kim, L. H. Daniel, and V. S. Freimuth. 2011. The impact of workplace policies and other social factors on self-reported influenza-like illness incidence during the 2009 H1N1 pandemic. American Journal of Public Health 102(1):134-140.
Kusaka, H., M. Munakata, K. Tanimura, H. Ukita, N. Denzumi, Y. Kawakami, H. Ogasawara, and Y. Homma. 1993. Two-year follow up on the protective value of dust masks against farmer’s lung disease. Internal Medicine 32(2):106-111.
Lahiri, S., C. Levenstein, D. I. Nelson, and B. J. Rosenberg. 2005. The cost effectiveness of occupational health interventions: Prevention of silicosis. American Journal of Industrial Medicine 48(6):503-514.
Lan, F.-Y., C.-F. Wei, Y.-T. Hsu, D. C. Christiani, and S. N. Kales. 2020. Work-related COVID-19 transmission in six Asian countries/areas: A follow-up study. PLoS One 15(5):e0233588.
Lan, F. Y., C. Suharlim, S. N. Kales, and J. Yang. 2021. Association between SARS-CoV-2 infection, exposure risk and mental health among a cohort of essential retail workers in the USA. Occupational and Environmental Medicine 78(4):237-243.
Layton, K. 2020. Proposed federal OSHA standards for wildfire smoke. Seattle Journal of Technology, Environmental & Innovation Law 10(1):5. https://digitalcommons.law.seattleu.edu/sjteil/vol10/iss1/5 (accessed October 8, 2021).
LHSF (Laborers’ Health and Safety Fund of North America). 2021. Responding to COVID-19 in construction. https://www.lhsfna.org/LHSFNA/assets/File/Responding%20to%20COVID-19%20in%20Construction%207_26_20%20Final.pdf (accessed September 28, 2021).
Lippy, B. E. 2002. Safety and health of heavy equipment operators at Ground Zero. American Journal of Industrial Medicine 42(6):539-542.
Lippy, B. E. 2003. Protecting the health and safety of rescue and recovery workers. In Terrorism and public health, edited by B. L. a. V. Sidel. New York: Oxford University Press. P. 98.
Liu, D., I. B. Tager, J. R. Balmes, and R. J. Harrison. 1992. The effect of smoke inhalation on lung function and airway responsiveness in wildland fire fighters. American Review of Respiratory Diseases 146(6):1469-1473.
Liu, H. H., C. Y. Chen, C. H. Lan, C. P. Chang, and C. Y. Peng. 2016. Effects of a powered air-purifying respirator intervention on indium exposure reduction and indium related biomarkers among ITO sputter target manufacturing workers. Journal of Occupational and Environmental Hygiene 13(5):346-355.
Luckhaupt, S. E., M. H. Sweeney, R. Funk, G. M. Calvert, M. Nowell, T. D’Mello, A. Reingold, J. Meek, K. Yousey-Hindes, K. E. Arnold, P. Ryan, R. Lynfield, C. Morin, J. Baumbach, S. Zansky, N. M. Bennett, A. Thomas, W. Schaffner, and T. Jones. 2012. Influenza-associated hospitalizations by industry, 2009-10 influenza season, United States. Emerging Infectious Diseases Journal 18(4):556-562.
Lum, H. D., L. Mody, C. R. Levy, and A. A. Ginde. 2014. Pandemic influenza plans in residential care facilities. Journal of the American Geriatrics Society 62(7):1310-1316.
Maciag, M. 2014. States with most government employees: Totals and per capita rates. https://www.governing.com/archive/states-most-government-workers-public-employees-by-job-type.html (accessed September 1, 2021).
Macintyre, A. G., J. A. Barbera, and E. R. Smith. 2006. Surviving collapsed structure entrapment after earthquakes: A “time-to-rescue” analysis. Prehospital and Disaster Medicine 21(1):4-17; discussion 18-19.
Martinez, J. 2020. New York City bus drivers are being hit the hardest by deaths as COVID-19 devastates the MTA. The City, April 7. https://www.thecity.nyc/health/2020/4/7/21216831/bus-drivers-hardest-hit-by-deaths-as-covid-19-devastates-mta (accessed October 8, 2021).
McPherson, D. 2008. Balancing PPE protection with comfort, fit & style. Professional Safety 53(3):50-52.
Mendeloff, J. 2013. Using OSHA inspection data to analyze respirator protection program compliance. Monthly Labor Review. https://www.bls.gov/opub/mlr/2013/article/using-osha-inspection (accessed October 8, 2021).
Michaels, D., and J. Barab. 2020. The occupational safety and health administration at 50: Protecting workers in a changing economy. American Journal of Public Health 110(5):631-635.
Mojtahedzadeh, N., T. Wirth, A. Nienhaus, V. Harth, and S. Mache. 2021. Job demands, resources and strains of outpatient caregivers during the COVID-19 pandemic in Germany: A qualitative study. International Journal of Environmental Research & Public Health 18(7):3684. https://doi.org/10.3390/ijerph18073684.
Mpofu, D., L. Lockinger, J. Bidwell, and H. H. McDuffie. 2002. Evaluation of a respiratory health program for farmers and their families. Journal of Occupational and Environmental Medicine 44(11):1064-1074.
Muramatsu, N., L. Yin, and T. T. Lin. 2017. Building health promotion into the job of home care aides: Transformation of the workplace health environment. International Journal of Environmental Research & Public Health 14(4).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2018. A smarter national surveillance system for occupational safety and health in the 21st century. Washington, DC: The National Academies Press.
NASEM. 2019a. Implications of the California wildfires for health, communities, and preparedness: Proceedings of a workshop. Washington, DC: The National Academies Press.
NASEM. 2019b. Reusable elastomeric respirators in health care: Considerations for routine and surge use. Washington, DC: The National Academies Press.
Nasol, K., and V. Francisco-Menchavez. 2021. Filipino home care workers: Invisible frontline workers in the COVID-19 crisis in the United States. American Behavioral Scientist 65(10):1365-1383.
Navarro, K. 2020. Working in smoke: Wildfire impacts on the health of firefighters and outdoor workers and mitigation strategies. Clinics in Chest Medicine 41(4):763-769.
Navarro, K. M., M. T. Kleinman, C. E. Mackay, T. E. Reinhardt, J. R. Balmes, G. A. Broyles, R. D. Ottmar, L. P. Naher, and J. W. Domitrovich. 2019. Wildland firefighter smoke exposure and risk of lung cancer and cardiovascular disease mortality. Environmental Research 173:462-468.
NCSL (National Conference of State Legislatures). 2021. At-will employment—Overview. https://www.ncsl.org/research/labor-and-employment/at-will-employment-overview.aspx (accessed October 7, 2021).
NDWA (National Domestic Workers Alliance). 2020. Safety tips for domestic workers: Using face masks and other PPE. https://membership-dev.ndwa.io/wp-content/uploads/2020/05/Masks_COVID_5_12.pdf (accessed December 21, 2021).
Newman, D. M. 2013. Protecting worker and community health: Are we prepared for the next 9/11? New York Committee for Occupational Safety and Health. http://nycosh.org/wp-content/uploads/2014/09/NYCOSH-Protecting-Worker-1-17-14-FINAL.pdf (accessed December 15, 2021).
NFPA (National Fire Protection Association). 2022. NFPA 1984—Standard on respirators for wildland fire-fighting operations and wildland urban interface operations. https://www.nfpa.org/codes-and-standards/all-codes-and-standards/list-of-codes-and-standards/detail?code=1984 (acessed January 9, 2022).
Nguyen, T.-H.-Y., M. Bertin, J. Bodin, N. Fouquet, N. Bonvallot, and Y. Roquelaure. 2018. Multiple exposures and coexposures to occupational hazards among agricultural workers: A systematic review of observational studies. Safety and Health at Work 9(3):239-248.
NICC (National Interagency Coordination Center). 2020a. 2020 statistics and summary. https://www.predictiveservices.nifc.gov/intelligence/2020_statssumm/annual_report_2020.pdf (accessed November 8, 2021).
NICC. 2020b. Incident management situation report. https://www.predictiveservices.nifc.gov/IMSR/2020/20200827IMSR.pdf (accessed November 8, 2021).
Nichol, K., A. McGeer, P. Bigelow, L. O’Brien-Pallas, J. Scott, and D. L. Holness. 2013. Behind the mask: Determinants of nurse’s adherence to facial protective equipment. American Journal of Infection Control 41(1):8-13.
NIEHS (National Institute of Environmental Health Sciences). 2013. NIEHS disaster recovery—Mold remediation guidance. https://tools.niehs.nih.gov/wetp/public/hasl_get_blob.cfm?ID=9795 (accessed October 8, 2021).
NIEHS. 2021. COVID-19. https://tools.niehs.nih.gov/wetp/covid19worker/index.cfm (accessed October 7, 2021).
NIOSH (National Institute for Occupational Safety and Health). 2013. Wildland fire fighting—Hot tips to stay safe and healthy. https://www.cdc.gov/niosh/docs/2013-158/pdfs/2013-158v2.pdf?id=10.26616/NIOSHPUB2013158 (accessed October 8, 2021).
NIOSH. 2015a. Hierarchy of controls. https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed October 8, 2021).
NIOSH. 2015b. Hospital respiratory protection toolkit. https://www.cdc.gov/niosh/docs/2015117/default.html (accessed October 8, 2021).
NIOSH. 2015c. Overlapping vulnerabilities: The occupational health and safety of young immigrant workers in small construction firms. https://www.cdc.gov/niosh/docs/2015-178/default.html (accessed October 8, 2021).
NIOSH. 2017a. Health and safety practices survey of healthcare workers. https://www.cdc.gov/niosh/topics/healthcarehsps/aboutstudy.html (accessed October 7, 2021).
NIOSH. 2017b. To beard or not to beard? That’s a good question! https://blogs.cdc.gov/nioshscience-blog/2017/11/02/noshave (accessed September 28, 2021).
NIOSH. 2018. Small business—Understanding small business challenges. https://www.cdc.gov/niosh/topics/smbus/challenges.html (accessed September 16, 2021).
NIOSH. 2021a. COVID-19 poses big challenges for small construction firms. https://blogs.cdc.gov/niosh-science-blog/2021/03/09/construction_covid (accessed September 28, 2021).
NIOSH. 2021b. Outdoor workers exposed to wildfire smoke. https://www.cdc.gov/niosh/topics/firefighting/wffsmoke.html#anchor_1604590670073 (accessed October 4, 2021).
NIOSH. 2021c. Welcome to eworld. https://wwwn.cdc.gov/eworld (accessed October 4, 2021).
NRC (National Research Council). 2007. Measuring respirator use in the workplace. Washington, DC: The National Academies Press.
NSC (National Safety Council). 2020. Helpful facts on respirators and face coverings. https://nsckenticotest.blob.core.windows.net/cms/nsc.org/media/site-media/docs/workplace/facecoverings.pdf (accessed December 21, 2021).
NWCG (National Wildfire Coordinating Group). 2010. Safety advisory: Wildland fire smoke—Employee exposure and health. https://www.nwcg.gov/sites/default/files/committee/docs/rmc-sa-07042010-wildland-fire-smoke-employee-exposure-and-health.pdf (accessed October 8, 2021).
NWCG. 2021a. Guidance for prevention and management of COVID-19 during wildland fire operations. https://www.nwcg.gov/partners/fmb/guidance-prevention-management (accessed September 29, 2021).
NWCG. 2021b. NWCG glossary of wildland fire, PMS 205. https://www.nwcg.gov/glossary/az (accessed October 1, 2021).
Oregon OSHA (Occupational Safety and Health). 2020. Temporary rule addressing COVID-19 workplace risks. https://osha.oregon.gov/OSHARules/div1/437-001-0744.pdf (accessed October 6, 2021).
Oregon OSHA. 2021. Temporary rule on protection from wildfire smoke. https://osha.oregon.gov/OSHARules/adopted/2021/temp-rule-protection-from-wildfire-smoke.pdf (accessed October 6, 2021).
Ornstein, K. A., B. Leff, K. E. Covinsky, C. S. Ritchie, A. D. Federman, L. Roberts, A. S. Kelley, A. L. Siu, and S. L. Szanton. 2015. Epidemiology of the homebound population in the United States. JAMA Internal Medicine 175(7):1180-1186.
OSHA (Occupational Safety and Health Administration). 2006. Major requirements of OSHA’s respiratory protection standard 29 CFR 1910.134. https://www.osha.gov/sites/default/files/training-library_major_requirements.pdf (accessed October 8, 2021).
OSHA. 2009. Assigned protection factors for the revised respiratory protection standard. https://www.osha.gov/sites/default/files/publications/3352-APF-respirators.pdf (accessed October 1, 2021).
OSHA. 2011a. Small entity compliance guide for the respiratory protection standard. https://www.osha.gov/sites/default/files/publications/3384small-entity-for-respiratory-protection-standard-rev.pdf (accessed October 8, 2021).
OSHA. 2011b. Standard interpretations. https://www.osha.gov/laws-regs/standardinterpretations/2011-12-13 (accessed November 5, 2021).
OSHA. 2014a. Chemical management and permissible exposure limits (PELs). https://www.osha.gov/laws-regs/federalregister/2014-10-10 (accessed October 8, 2021).
OSHA. 2014b. Policy clarification on OSHA’s enforcement authority at small farms. https://www.osha.gov/memos/2014-07-29/policy-clarification-oshas-enforcement-authority-small-farms (accessed October 4, 2021).
OSHA. 2018. OSHA letter of interpretation for voluntary use of respirators. https://www.osha.gov/laws-regs/standardinterpretations/2018-04-26 (accessed October 8, 2021).
OSHA. 2021a. Construction work. https://www.osha.gov/coronavirus/control-prevention/construction (accessed September 28, 2021).
OSHA. 2021b. Dentistry workers and employers. https://www.osha.gov/coronavirus/controlprevention/dentistry (accessed September 29, 2021).
OSHA. 2021c. DIR 2021–03 (CPL 03)—Revised national emphasis program—coronavirus disease 2019 (COVID-19). https://www.osha.gov/sites/default/files/enforcement/directives/DIR_2021-03_CPL_03.pdf (accessed October 8, 2021).
OSHA. 2021d. Fact sheet—Mini respiratory protection program. https://www.osha.gov/sites/default/files/publications/OSHA4121.pdf (accessed October 8, 2021).
OSHA. 2021e. Inspections with COVID-19 related violations. https://www.osha.gov/enforcement/covid-19-data/inspections-covid-related-citations (accessed September 16, 2021).
OSHA. 2021f. Protecting workers: Guidance on mitigating and preventing the spread of COVID-19 in the workplace. https://www.osha.gov/coronavirus/safework (accessed September 29, 2021).
OSHA. 2021g. State plans. https://www.osha.gov/stateplans (accessed October 8, 2021).
OSHA. 2021h. Top 10 most frequently cited standards for fiscal year 2020 (Oct. 1, 2019, to Sept. 30, 2020). https://www.osha.gov/top10citedstandards (accessed September 21, 2021).
OSHA. 2021i. Susan Harwood training grant program. https://www.osha.gov/harwoodgrants (accessed October 7, 2021).
OSHA. n.d.a. Permissible exposure limits—Annotated tables. https://www.osha.gov/annotated-pels (accessed December 8, 2021).
OSHA. n.d.b. Protecting temporary workers. https://www.osha.gov/temporaryworkers (accessed September 21, 2021).
Pan, Y., Y. Fang, M. Xin, W. Dong, L. Zhou, Q. Hou, F. Li, G. Sun, Z. Zheng, J. Yuan, Z. Wang, and Y. He. 2020. Self-reported compliance with personal preventive measures among Chinese factory workers at the beginning of work resumption following the COVID-19 outbreak: Cross-sectional survey study. Journal of Medical Internet Research 22(9):e22457.
Pasco, R. F., S. J. Fox, S. C. Johnston, M. Pignone, and L. A. Meyers. 2020. Estimated association of construction work with risks of COVID-19 infection and hospitalization in Texas. JAMA Network Open 3(10):e2026373.
PERC (Pesticide Educational Resources Collaborative). 2017. How to comply with the 2015 revised Worker Protection Standard for agricultural pesticides—What owners and employers need to know. http://www.pesticideresources.org/wps/htc/htcmanual.pdf (accessed October 8, 2021).
Quan, N. G., H. Latif, M. Krsak, M. F. Corbisiero, J. Solis, T. Wand, P. Mortaji, M. A. Vrolijk, S. Kon, N. Ghandnoosh, and C. Franco-Paredes. 2021. Benefits of COVID-19 viral screening of formerly incarcerated individuals during community reentry. Therapeutic Advances in Infectious Disease 8.
Quinlan, M. 2021. COVID-19, health and vulnerable societies. Annals of Work Exposures and Health 65(3):239-243.
Reckrey, J. M., A. D. Federman, E. Bollens-Lund, R. S. Morrison, and K. A. Ornstein. 2020. Homebound status and the critical role of caregiving support. Journal of Aging & Social Policy 32(6):590-603.
Reinhardt, T. E., and R. D. Ottmar. 2000. Smoke exposure at western wildfires. USDA Forest Service—Research Papers (PNW RP 525). https://www.fs.fed.us/pnw/pubs/pnw_rp525.pdf (accessed October 8, 2021).
Reinhardt, T. E., and R. D. Ottmar. 2004. Baseline measurements of smoke exposure among wildland firefighters. Journal of Occupational and Environmental Hygiene 1(9):593-606.
Rho, H., H. Brown, and S. Fremstad. 2020. A basic demographic profile of workers in frontline industries. Center for Economic and Policy Research. https://cepr.net/a-basic-demographic-profile-of-workers-in-frontline-industries (accessed October 8, 2021).
Riden, H. E., R. Giacinto, G. Wadsworth, J. Rainwater, T. Andrews, and K. E. Pinkerton. 2020. Wildfire smoke exposure: Awareness and safety responses in the agricultural workplace. Journal of Agromedicine 25(3):330-338.
Riley, K., and J. Guzman. 2017. On-the-job injuries and workers’ compensation eligibility among day laborers in residential worksites in California. Research Brief. Labor Occupational Safety and Health Program and National Day Laborer Organizing Network.
Riley, K., and R. Majano. 2021. Using workers’ compensation claims to investigate occupational injuries among residential day laborers and domestic workers. American Journal of Industrial Medicine 64(5):358-368.
Ringen, K., J. Dement, L. Welch, X. S. Dong, E. Bingham, and P. S. Quinn. 2014. Risks of a lifetime in construction. Part II: Chronic occupational diseases. American Journal of Industrial Medicine 57(11):1235-1245.
Rogers, J. H., A. C. Link, D. McCulloch, E. Brandstetter, K. L. Newman, M. L. Jackson, J. P. Hughes, J. A. Englund, M. Boeckh, N. Sugg, M. Ilcisin, T. R. Sibley, K. Fay, J. Lee, P. Han, M. Truong, M. Richardson, D. A. Nickerson, L. M. Starita, T. Bedford, and H. Y. Chu. 2020. Characteristics of COVID-19 in homeless shelters. Annals of Internal Medicine 174(1):42-49.
Rosen, J., A. Miller, J. Hughes, and J. Remington. 2015. National Institute of Environmental Health Sciences worker training program: Perspectives on the health and safety of workers, volunteers, and residents involved in the cleanup and rebuilding of New York City housing damaged by Hurricane Sandy. Environmental Justice 8(3):105-109.
Rubin, R. 2020. COVID-19’s crushing effects on medical practices, some of which might not survive. Journal of the American Medical Association 324(4):321-323.
Ruby, B. C., T. C. Shriver, T. W. Zderic, B. J. Sharkey, C. Burks, and S. Tysk. 2002. Total energy expenditure during arduous wildfire suppression. Medicine & Science in Sports & Exercise 34(6):1048-1054.
Rutgers University. n.d. Respirators. https://pesticidestewardship.org/respirators (accessed September 28, 2021).
Sami, S., L. Akinbami, L. Petersen, A. Crawley, S. Lukacs, D. Weiss, R. Henseler, N. Vuong, L. Mackey, A. Patel, L. Grohskopf, B. M. Morgenthau, D. Daskalakis, and P. Pathela. 2021. Prevalence of SARS-CoV-2 antibodies in first responders and public safety personnel, New York City, New York, USA, May–July 2020. Emerging Infectious Disease Journal 27(3):796.
Sauer, L. M., C. Catlett, R. Tosatto, and T. D. Kirsch. 2014. The utility of and risks associated with the use of spontaneous volunteers in disaster response: A survey. Disaster Medicine and Public Health Preparedness 8(1):65-69.
Scales, K. 2020. It’s time to care: A detailed profile of America’s direct care workforce. Bronx, NY: Paraprofessional Healthcare Institute.
Schenker, M. B., D. Christiani, Y. Cormier, H. Dimich-Ward, G. Doekes, Dosman, J., J. Douwes, K. Dowling, D. Enarson, F. Green, and D. Heederik. 1998. Respiratory health hazards in agriculture. American Journal of Respiratory and Critical Care Medicine 158(5 Pt 2):S1-S76.
SEIU (Service Employees International Union). 2021. COVID-19 (coronavirus) caregiver training. https://www.myseiubenefits.org/covid-19-bg (accessed October 7, 2021).
Semmens, E. O., J. Domitrovich, K. Conway, and C. W. Noonan. 2016. A cross-sectional survey of occupational history as a wildland firefighter and health. American Journal of Industrial Medicine 59(4):330-335.
Shah, H. B. 2017. Understaffed and overworked: Poor working conditions and quality of care in residential care facilities for the elderly. Golden Gate University School of Law Digital Commons. https://digitalcommons.law.ggu.edu/cgi/viewcontent.cgi?article=1789&context=pubs (accessed October 8, 2021).
Sharkey, B. 1997. Health hazards of smoke: Recommendations of the consensus conference April 1997. Washington, DC: U.S. Department of Agriculture.
Sietsema, M. 2017. Analysis of respiratory program practices and simulated workplace protection factor studies. University of Illinois at Chicago [master’s thesis]. https://hdl.handle.net/10027/19570 (accessed February 28, 2022).
Sietsema, M., L. M. Conroy, and L. M. Brosseau. 2015. Comparing written programs and self-reported respiratory protection practices in acute care hospitals. Journal of Occupational & Environmental Hygiene 12(3):189-198.
Sol, J. A., B. C. Ruby, S. E. Gaskill, C. L. Dumke, and J. W. Domitrovich. 2018. Metabolic demand of hiking in wildland firefighting. Wilderness & Environmental Medicine 29(3):304-314.
Sterling, M. R., N. Dell, E. Tseng, F. Okeke, J. Cho, B. Piantella, and J. N. Tobin. 2020. Home care workers caring for adults with heart failure need better access to training and technology: A role for implementation science. Journal of Clinical and Translational Science 4(3):224-228.
Syamlal, G., P. L. Schleiff, J. M. Mazurek, B. Doney, and M. Greskevitch. 2013. Respirator use among US farm operators: Evidence from the 2006 farm and ranch safety survey. Journal of Agromedicine 18(1):27-38.
Tanne, J. H. 2020. COVID-19: CDC publishes then withdraws information on aerosol transmission. British Medical Journal 370:m3739.
Tarlo, Susan M., and Malo, Jean-Luc. 2013. An official American Thoracic Society Proceedings: Work-related asthma and airway diseases: Presentations and discussion from the fourth Jack Pepys workshop on asthma in the workplace. Annals of the American Thoracic Society 10(4):S17-S24.
The Joint Commission. 2014. Implementing hospital respiratory protection programs: Strategies from the field. https://www.jointcommission.org/-/media/tjc/documents/resources/health-services-research/implementing_hospital_rpp_2-19-15pdf.pdf (accessed October 8, 2021).
The Joint Commission. 2020. Announcement: Joint Commission statement on use of face masks brought from home. https://www.jointcommission.org/-/media/tjc/documents/covid19/public-statement-on-masks-from-home-w-faqs.pdf (accessed October 8, 2021).
The New York Times. 2021. Nearly one-third of U.S. coronavirus deaths are linked to nursing homes. https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html (accessed October 8, 2021).
Theodore, N. 2017. After the storm: Houston’s day labor markets in the aftermath of Hurricane Harvey. University of Illinois at Chicago. https://www.researchgate.net/publication/321371398_After_the_Storm_Houston’s_Day_Labor_Markets_in_the_Aftermath_of_Hurricane_Harvey (accessed October 8, 2021).
Theodore, N. 2020. Day laborers in the eye of the storm. North American Congress on Latin America: Report on the Americas 52(2):192-198.
Toblin, R., S. I. Cohen, and L. M. Hagan. 2021. SARS-CoV-2 infection among correctional staff in the Federal Bureau of Prisons. American Journal of Public Health 111(6):1164-1167.
Tobolowsky, F., E. Gonzales, J. Self, C. Rao, R. Keating, G. Marx, T. McMichael, M. Lukoff, J. Duchin, K. Huster, J. Rauch, H. McLendon, M. Hanson, D. Nichols, S. Pogosjans, M. Fagalde, J. Lenahan, E. Maier, H. Whitney, and M. Kay. 2020. COVID-19 outbreak among three affiliated homeless service sites—King County, Washington, 2020. Morbidity and Mortality Weekly Report 69(17):523-526.
Tora-Rocamora, I., G. L. Delclos, J. M. Martinez, J. Jardi, C. Alberti, R. Manzanera, Y. Yasui, R. Cleries, A. Tobias, and F. G. Benavides. 2012. Occupational health impact of the 2009 H1N1 flu pandemic: Surveillance of sickness absence. Occupational and Environmental Medicine 69(3):205-210.
University of Michigan. 2020. The health and retirement study. https://hrs.isr.umich.edu/about (accessed August 2, 2021).
Valenzuela, A., Jr., N. Theodore, E. Melendez, and A. Gonzalez. 2006. On the corner: Day labor in the United States. Los Angeles, CA: Center for the Study of Urban Poverty.
Van Hoving, D. J., L. A. Wallis, F. Docrat, and S. De Vries. 2010. Haiti disaster tourism—A medical shame. Prehospital and Disaster Medicine 25(3):201-202.
Viegas, S., V. M. Faisca, H. Dias, A. Clerigo, E. Carolino, and C. Viegas. 2013. Occupational exposure to poultry dust and effects on the respiratory system in workers. Journal of Toxicology and Environmental Health, Part A 76(4-5):230-239.
Vinberg, S. 2020. Occupational safety and health challenges in small-scale enterprises. Industrial Health 58(4):303-305.
Virginia DOLI (Department of Labor and Industry). 2020. Emergency temporary standard infectious disease prevention: SARS-CoV-2 virus that causes COVID-19. https://www.doli.virginia.gov/wp-content/uploads/2020/07/RIS-filed-RTD-Final-ETS-7.24.2020.pdf (accessed October 8, 2021).
Virolainen, R., K. Tupi, E. O. Terho, K. Husman, V. Notkola, and I. Vohlonen. 1987. Characteristics of farmers who have obtained personal dust respirators. European Journal of Respiratory Diseases 152:199-205.
Wallace, M., L. Hagan, and K. G. e. a. Curran. 2020. COVID-19 in correctional and detention facilities—United States, February–April 2020. Morbidity and Mortality Weekly Report 69(19):587-590.
Waltenburg, M., C. Rose, T. Victoroff, M. Butterfield, J. Dillaha, A. Heinzerling, M. Chuey, M. Fierro, R. Jervis, K. Fedak, A. Leapley, J. Gabel, A. Feldpausch, E. Dunne, C. Austin, C. Pedati, F. Ahmed, S. Tubach, C. Rhea, J. Tonzel, A. Krueger, D. Crum, J. Vostok, M. Moore, H. Kempher, J. Scheftel, G. Turabelidze, D. Stover, M. Donahue, D. Thomas, K. Edge, B. Gutierrez, E. Berl, M. McLafferty, K. Kline, N. Martz, J. Rajotte, E. Julian, A. Diedhiou, R. Radcliffe, J. Clayton, D. Ortbahn, J. Cummins, B. Barbeau, S. Carpenter, J. Pringle, J. Murphy, B. Darby, N. Graff, T. K. H. Dostal, I. Pray, C. Tillman, D. Rose, and M. Honein. 2021. Coronavirus disease among workers in food processing, food manufacturing, and agriculture workplaces. Emerging Infectious Disease Journal 27(1):243.
Wang, X., X. S. Dong, L. Welch., and J. Largay. 2016. Respiratory cancer and non-malignant respiratory disease-related mortality among older construction workers-findings from the health and retirement study. Occupational Medicine & Health Affairs 4(235).
Wang, X., R. Katz, and X. Sue Dong. 2018. Union effect on safety management and safety culture in the construction industry.CPWR Quarterly Data Report. https://www.researchgate.net/publication/325019667_Union_Effect_on_Safety_Management_and_Safety_Culture_in_the_Construction_Industry (accessed October 8, 2021).
Washington State DOLI (Department of Labor and Industries). 2021a. Washington administrative code 296-62-085 wildfire smoke. https://lni.wa.gov/safety-health/safety-rules/chapter-pdfs/WAC296-62.pdf#WAC_296_62_085 (accessed October 8, 2021).
Washington State DOLI. 2021b. Which mask for which task? https://www.lni.wa.gov/forms-publications/F414-168-000.pdf (accessed October 8, 2021).
Washington State Nurses Association. 2010. Sacred Heart Medical Center cited for violation of safety standards in H1N1 prevention. https://www.prnewswire.com/news-releases/sacred-heart-medical-center-cited-for-violation-of-safety-standards-in-h1n1-prevention-84740292.html (accessed September 21, 2021).
WCAHS (Western Center for Agricultural Health and Safety). 2021. Wildfire resources. https://aghealth.ucdavis.edu/wildfires (accessed September 28, 2021).
Weil, D. 2014. The fissured workplace: Why work became so bad for so many and what can be done to improve it. Cambridge, MA: Harvard University Press.
West, M. R., S. Costello, J. A. Sol, and J. W. Domitrovich. 2020. Risk for heat-related illness among wildland firefighters: Job tasks and core body temperature change. Occupational & Environmental Medicine 77(7):433-438.
WHO (World Health Organization). 2020. Transmission of SARS-CoV-2: Implications for infection prevention precautions. https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions (accessed October 7, 2021).
Whoriskey, P., J. Stein, and N. Jones. 2020. Thousands of OSHA complaints filed against companies for virus workplace safety concerns, records show. The Washington Post, April 16.
Wizner, K., M. Nasarwanji, E. Fisher, A. L. Steege, and J. M. Boiano. 2018. Exploring respiratory protection practices for prominent hazards in healthcare settings. Journal of Occupational and Environmental Hygiene 15(8):588-597.
Wu, C. M., C. C. Song, R. Chartier, J. Kremer, L. Naeher, and O. Adetona. 2021. Characterization of occupational smoke exposure among wildland firefighters in the midwestern United States. Environmental Research 193:110541.
Wuellner, S. 2021. Washington COVID-19 cases by industry, January 2020–June 2020. Washington State Department of Labor and Industries. https://lni.wa.gov/safety-health/safety-research/files/2021/103_06_2021_COVID_Industry_Report.pdf (accessed October 8, 2021).
Yarbrough, M. I., M. E. Ficken, C. U. Lehmann, T. R. Talbot, M. D. Swift, P. W. McGown, R. F. Wheaton, M. Bruer, S. W. Little, and C. A. Oke. 2016. Respirator use in a hospital setting: Establishing surveillance metrics. Journal of the International Society for Respiratory Protection 33(1):1-11.
Zemouri, C., H. de Soet, W. Crielaard, and A. Laheij. 2017. A scoping review on bio-aerosols in healthcare and the dental environment. PLoS ONE 12(5):e0178007.
Zemouri, C., S. F. Awad, C. M. C. Volgenant, W. Crielaard, A. Laheij, and J. J. de Soet. 2020. Modeling of the transmission of coronaviruses, measles virus, influenza virus, mycobacterium tuberculosis, and legionella pneumophila in dental clinics. Journal of Dental Research 99(10):1192-1198.
















































































