
1
Introduction
Almost 2 years into the COVID-19 pandemic and with wildfire smoke visibly and frequently permeating the air in much of the western United States, the American public and many workers still have questions: Why do I need to wear a mask? Is it safe? What product is best to protect myself, my family, and my community? How do I obtain the right device for my situation? Having the right answers to these questions and having the right devices available for use can prevent illness and save lives. However, substantial gaps in existing approaches for making devices for respiratory protection and getting them into people’s hands impair timely access to appropriate devices and guidance on their effective use. As the nation reflects on this time and looks to the future, its leadership has a fundamental responsibility to address these gaps and establish a system that is better prepared and resourced to react swiftly and effectively to the next threat. As this report goes to press, more than 800,000 lives have been lost to COVID-19 in the United States (CDC, 2021a), with millions more affected. The burden has not been borne equitably, with low-income groups and communities of color experiencing excess morbidity and mortality due to COVID-19 compared with other groups (Moore et al., 2020). Clearly, then, the time to take action to ensure that respiratory protection can be provided for all when needed is now.
Individuals in the United States and Americans abroad are exposed to inhalation hazards from a variety of sources—some in workplaces, some indoors, and some outdoors—and these hazards can have short- and long-term adverse effects on health. For example, exposure to wildfire smoke,
which contains particulate matter (PM) and toxic chemicals, can lead to respiratory problems (e.g., worsening of asthma symptoms), increased risk for heart attacks, and other adverse health outcomes (Chen et al., 2021; Holm et al., 2021). Individuals also may be exposed to airborne infectious agents through aerosol or droplet transmission, and as demonstrated by the COVID-19 pandemic, the individual and public health consequences of these exposures can be severe. Storms, floods, and hurricanes can increase exposure to moisture-driven hazards, such as mold, and to accidental releases from production facilities or transport vehicles that may result in chemical exposures (NIOSH, 2019b).
These and other inhalation hazards can adversely impact the public generally, as well as workers whose jobs typically do not require respiratory protection, such as teachers, grocery store workers, and federal civilian workers (e.g., Foreign Service officers) and their families stationed in locations where ambient air pollution levels are routinely or periodically elevated to unsafe levels (e.g., from agricultural burning, dust storms, and industrial emissions). As with COVID-19, the burden of these hazards is not shared equally across the population: poorer communities and some racial and ethnic groups experience greater exposure to certain inhalation hazards and may be less able than other population groups to avoid or mitigate those hazards (American Lung Association, 2020a). Furthermore, some individuals, including children, the elderly, and people with underlying health conditions, are at heightened risk of adverse health outcomes associated with inhalation hazards (American Lung Association, 2020b; CDC and HUD, 2006).
While more permanent solutions are required and are preferable to relying on individual action to reduce these exposures, the use of individual respiratory protection nevertheless remains an important protective measure of last resort. Currently, however, the United States has no coordinated system to support the development of standards and guidance1 for respiratory protection for the public and those workers whose employers are not required to have a respiratory protection program (RPP) by the Occupational Safety and Health Administration (OSHA) or other entities. The current regulatory system is focused primarily on ensuring access to respiratory protection in occupational settings characterized by well-defined hazards and clearly defined employer–employee relationships. With this narrow regulatory focus on selected worker groups, the respiratory protection needs of the public and many workers are not being met.
___________________
1 Agency actions that are not legally enforceable are generally characterized as “guidance.” Guidance includes interpretive rules, general statements of policy, memoranda, manuals, bulletins, and advisories. It also often includes some forms of interagency cooperation, such as those imbedded in interagency memoranda of cooperation (Rowell, 2021).
As climate change increases the incidence and severity of wildfires, hurricanes, floods, infectious disease outbreaks, and other phenomena that impact air quality and human health, it is imperative that the United States close the gap and ensure that the respiratory protection needs of the public and all workers are met. Recognizing the urgent need to address the gaps in the nation’s ability to meet the respiratory protection needs of the public and workers without workplace RPPs, three federal sponsors (the National Institute for Occupational Safety and Health [NIOSH], the Environmental Protection Agency [EPA], and the Department of State) and the CDC Foundation asked the National Academies of Sciences, Engineering, and Medicine to convene an ad hoc committee charged with formulating recommendations for a framework of responsibilities and authorities that would provide a unified and authoritative source of information and effective oversight for the development, approval, and use of respiratory protection. The committee’s full Statement of Task is presented in Box 1-1. This report presents the committee’s findings, conclusions, and recommendations.
STUDY SCOPE AND KEY TERMINOLOGY
The types of inhalation hazards and circumstances of exposure that may require respiratory protection are wide-ranging. During its first meeting on November 5, 2020, the committee had an opportunity to clarify the scope of the study with representatives of the sponsoring organizations. In the course of that discussion, the study sponsors helped the committee focus the scope of this report by presenting a matrix laying out the priority hazards and populations to be addressed (see Table 1-1, provided by the study sponsors). The highest-priority hazards reflect the current context: air pollution (including wildfire smoke) and infectious biological agents (including respiratory viruses). Target populations are the public and groups of workers not covered by an RPP; these groups include some worker populations that face occupational exposures to inhalation hazards and arguably should be covered by an RPP (e.g., some wildland firefighters, home care workers). While worker populations covered by RPPs were not a priority focus for this report, the committee acknowledges that an RPP may not by itself ensure adequate protection from inhalation hazards, as may be the case, for example, when OSHA RPP requirements are not adequately implemented or enforced within workplaces.
The committee uses the term respiratory protection to broadly describe any approach designed to reduce exposure to hazards that can be inhaled (i.e., inhalation hazards), which may be in the form of gases, vapors, or particles, including airborne transmissible microorganisms (bacteria, viruses, molds). Inhalation hazards relevant to this report are described later in this chapter. As clarified by the sponsors, the scope of this study is limited to
| Air pollution (including wildfire smoke) |
Biological agents (respiratory viruses, molds) |
Chemicals from disasters/public health emergencies (accidental spills/environmental release following a disaster, chemical weapons) |
Chemicals from regular occupational use (e.g., pesticides, cleaning solvents) |
Inhaled radionuclides (accidental or intentional release) |
|
|---|---|---|---|---|---|
| Wildland firefighters | |||||
| Other trained emergency responders (paid and volunteer) | |||||
| Outdoor workers, including day laborers and other workers with temporary/informal occupational arrangements (e.g., agricultural workers) | |||||
| Indoor workers, including those with formal or temporary/informal occupational arrangements (e.g., grocery store workers, domestic day laborers, and home health workers) | (wildfire smoke) | ||||
| U.S. government workers overseas |
|||||
| The public (adults and children, including those overseas, with nonoccupational exposures) |
NOTE: Colors indicate the priority of focus areas for the study: green indicates the highest-priority areas, yellow lower-priority areas, and orange the lowest-priority areas (which should be acknowledged but not be a major focus).
SOURCE: Adapted from D’Alessandro, 2020.
personal devices that are worn to provide respiratory protection. In using this definition of respiratory protection, the committee recognizes that such devices can protect the wearers or, for some hazards (e.g., airborne microorganisms), protect others because infected people are the source, and the device reduces the amount of the agent they release into the air. Some devices may provide some level of protection to both the wearer and to others. While acknowledging that other forms of control (e.g., ventilation systems or vaccination) may be more protective when feasible to implement, the committee notes that such controls are not within the scope of this study.
A number of terms are used by federal agencies and others to describe the various personal devices designed and worn to reduce adverse health effects from inhalation hazards (see Annex 1-1 at the end of this chapter); however, no consistent descriptions of these devices—respirators, masks, face coverings, and barrier face coverings—exist. Below, the committee provides its descriptions of these devices for the purposes of this report, using terminology intended to be generally understood. Examples of these devices are depicted in Figure 1-1. In meetings with the committee, the study sponsors clarified that the focus of the study was not limited to respirators, but also included masks and face coverings.
Respirator is the term used in this report to describe personal devices designed to protect the user from the adverse effects of inhalation hazards. In the United States, respirators are designed, manufactured, tested, and approved for use in the workplace, and performance standards for respirators are embodied in federal regulation at 42 C.F.R. § 84. This regulation also assigns responsibility for testing and approving respirators to NIOSH—a research agency within the Centers for Disease Control and Prevention (CDC) focused on occupational safety and health.2 NIOSH’s rigorous conformity assessment program for respirators includes premarket evaluations, laboratory testing, examination of the manufacturers’ quality control programs, and postmarket surveillance. NIOSH maintains a publicly available list of those respirators that have been approved and are authorized to use the NIOSH certification mark. The use of respiratory protection in the workplace is regulated by OSHA and other regulatory agencies at the federal and state levels. OSHA-mandated respiratory protection programs provide an established administrative structure for integrating control methods into
___________________
2 Manufacturers in other countries produce respirators, and there are a number of different national and international respirator standards. These manufacturers can submit their respirators to NIOSH for testing and certification. NIOSH-approved respirators are the only respirators accepted for use in U.S. workplaces by OSHA and other regulatory agencies. Respirators that are tested and approved only to other international standards (for example, KN95s, FFP2s) are not acceptable for use in workplaces except under an emergency use authorization by the Food and Drug Administration.

SOURCES: Photo of powered air-purifying respirator provided courtesy of 3M. Photo of barrier face covering provided courtesy of Puraka Masks, www.purakamasks.com.
the workplace so as to effectively assess, control, and evaluate inhalation hazard exposures for workers. The regulatory landscape for respiratory protection is described in detail in Chapter 2. In an OSHA-mandated RPP, selection of a respirator must be based on an assessment of the hazard. Proper training of wearers on its use and fit testing are also required since many respirator types must be fitted to the individual user to ensure proper performance. (See Box 1-2 for further description of respirator types and factors influencing their selection.)
For the purposes of this report, with the notable exception of dust masks3 (or nuisance masks), masks are personal devices designed and intended to reduce the spread of infectious agents found in large droplets, such as those from saliva, sneezes, and coughs. They also may provide a barrier to infection by preventing users from touching their mouth or nose with contaminated fingers, although concerns have been raised that use of masks may increase face-touching behaviors, and thereby the risk of infection (Chen et al., 2020; Lucas et al., 2020). While they may be similar in construction and appearance, masks are not respirators. Medical or surgical masks (also commonly referred to as medical procedure, dental, or isolation
___________________
3 Dust masks or nuisance masks are nonapproved devices that are worn to reduce exposure to airborne contaminants when working in dusty environments. They do not protect against toxic dusts and are not approved as respirators. In contrast with medical or surgical masks, no standards govern their construction or the quality of their filtration.
masks) are unfitted devices that may provide some protection against contamination of the surrounding environment by their wearers by reducing the amount of infectious agents released during exhalation, coughing, or sneezing. Surgical/medical masks may also provide some protection to the user against liquid splash and droplets, but they are not tested or intended as protection from inhalation hazards as they are not designed to fit tightly to the face. As discussed further in Chapter 2, medical or surgical masks sold as medical devices are required to be cleared by the Food and Drug Administration (FDA).
Face coverings are devices that cover the mouth and nose, but, absent testing at present, do not provide a known degree of protection. Face coverings may be mask-style devices (i.e., products that look like surgical/medical masks but are not FDA cleared and do not conform to any specific standard), bandanas, gaiters, or other configurations. They may be constructed
of cloth in a single layer or multiple layers, filtering material, or a combination of base material and filter elements. Barrier face coverings are designed and manufactured to comply with the ASTM F3502-21 standard, which was released in February 2021 in response to the COVID-19 pandemic. These devices cover at least the wearer’s nose and mouth, provide a measured degree of particulate filtration, and are intended to provide a better fit than masks and other face coverings, but there is no requirement for fit testing of the wearer.4 They do not meet OSHA requirements for use in the context of an OSHA-mandated RPP, including training and fitting. The ASTM F3502-21 standard and the required testing are described further in Chapter 2. Barrier face coverings are not respirators and are not intended for medical use. In Europe, similar devices are known as community masks.
As described above, personal devices designed to reduce exposure to inhalation hazards may be used for personal protection and/or to protect others (i.e., source control). Source control, in the context of this report,5 denotes reduction of the release of infectious agents from the wearer, which decreases the potential danger to others in the immediate environment. While respirators are designed specifically to protect the individual wearing the device from the risks of inhalation hazards, these devices also will function as a form of source control in the context of airborne infections when people become the source of the inhalation hazard, thus additionally serving to benefit public health. Masks and face coverings (including barrier face coverings) are intended primarily to reduce emissions of infectious agents by the wearer, and may also provide more limited protection against inhaling airborne infectious agents (and various forms of air pollution), depending on the device’s fit and filtration characteristics. However, there are no standards for evaluating these devices for source control. FDA relies on ASTM tests for filter efficiency to determine that cleared devices are suitable to protect others. A similar approach applies to barrier face coverings, with the additional requirement that the manufacturer make some statement regarding the fit capability of the device. NIOSH-approved respirators will likely provide greater source control relative to masks or barrier face coverings because of their superior filter performance and because they are tight
___________________
4 The purpose of fit testing is to determine that a respirator model and size adequately fit the individual user’s face (NPPTL, 2021), which is important to minimize leakage around the sealing surfaces.
5 Source control, in other contexts outside of this report, may refer more broadly to an approach designed to eliminate or reduce the introduction of harmful substances into the environment (e.g., curbing emissions into the air).
fitting6 (the filtration and fit of different devices are discussed in Appendix B). Many respirators, especially elastomeric facepiece respirators, have exhalation valves to improve comfort by reducing the resistance to exhaled air from the respirator. There has been debate and speculation regarding the significance of exhalation valves as a source of viral contamination from the wearer, leading some respirator manufacturers to redesign their elastomeric facepiece respirators so that they no longer have exhalation valves or have covers for these valves. The lack of a specific standard(s) for source control limits the proper selection of respirators, masks, face coverings, and barrier face coverings based on the hazard because the hazard arises from being in proximity to an infected individual or in an airspace containing infectious aerosol.
The ongoing COVID-19 pandemic and widely visible wildfire smoke, often present at unsafe levels, have heightened the public’s awareness of various personal devices used to reduce exposure to these inhalation hazards, although likely not the distinctions among the devices that are often based on technical specifications and standards as described above. Much of the technical terminology used in this area is unfamiliar to the public, and the nuanced details that are appreciated by the technical community are hindrances to effective communication of key messages to workers and the public generally. For example, the public may not appreciate the differences among the various types of devices used to reduce the spread of airborne infection and the fact that some devices can function both as a form of source control to protect others and as a means of individual protection to reduce the inhalation of transmissible agents. Consequently, the committee views effective communication as a critical element of any framework for providing respiratory protection for the public.
In this report, the committee refers to the various types of devices now in use with the specific terms reflecting their characteristics and the processes under which they are manufactured: respirators, masks (e.g., surgical/medial masks), face coverings, and barrier face coverings. However, the absence of a field-accepted term encompassing all personal devices that provide protection against inhalation hazards when used effectively presented challenges during the course of this study, and if not addressed, the lack of an umbrella term will continue to pose impediments to effective communication regarding respiratory protection, particularly as device technology continues to evolve. To fill this need and for the purposes of this report and the framework described herein, the committee uses the term
___________________
6 PAPRs, which are not tight fitting but are designed to keep contaminants from entering the hood by creating a positive pressure with a blower, dilute but do not filter exhaled air that is released into the environment.
respiratory protective device.7 This function-based definition acknowledges that each device may offer either personal protection or source control or both at varying levels. The blend of personal protection and source control is context specific (i.e., depends on both the device and the hazard in question). At present, this function-based definition is qualitative until data quantifying the efficacy of devices when used for personal protection and/or source control in different use scenarios, particularly for the public, are available. This function-based definition also should prove useful in the future as additional devices that may not fit into existing device categories are developed. However, the committee anticipates that terminology and definitions will be refined as its recommendations are pursued and it may be that a different umbrella term will be implemented.
STUDY CONTEXT
Inhalation Hazards and Their Contribution to the Burden of Disease
An understanding of how exposures to inhalation hazards occur in occupational or general environmental settings is critical for the design of respiratory protection strategies. Consistent with its charge, while acknowledging the important contribution of regulated workplace exposures to the burden of disease in the United States, the committee did not conduct a review of common and well-characterized occupational inhalation hazards (e.g., silica, coal dust), but instead focused on ambient air pollution and wildfire smoke, along with various forms of biological, chemical, and radioactive agents that may be encountered during public health emergencies or other incidents.
Harmful inhaled agents may present as PM of varying sizes and composition, as gases, as vapors, or as a combination thereof. The form and composition of an inhaled agent dictate the type of respiratory protection needed to prevent or limit exposure.
Exposure occurs when people come into contact with air that has been contaminated by inhalation hazards. Exposure is calculated for air pollutants as the product of the pollutant concentration in the place(s) where time is spent and the amount of time spent in that place. Intake refers to the amount of material entering the respiratory tract over the exposure period. Following intake, hazards must deposit in various regions of the respiratory tract in order to deliver a dose to the target site. For example,
___________________
7 The committee recognizes that this usage constitutes an expansion of a term defined in existing international standards to refer to devices designed to protect the wearer against inhalation hazards.
larger particles tend to deposit in the upper airways; smaller particles are generally of greater concern as they are more likely to penetrate to and deposit in the deepest portions of the respiratory tract, including the narrow, distal airways and the alveolar spaces where gas exchange takes place (Hinds, 1999); and some particle sizes deport with minimal efficiency and tend to get exhaled back into the environment (Hinds, 1999). Thus, dose refers to the amount of material that ultimately reaches a target organ or tissue. Exposure to inhalation hazards can lead to an array of adverse health outcomes, contributing to, causing, and exacerbating respiratory illnesses and increasing risk for such conditions as cardiovascular disease and cancer, among others (Bowe et al., 2019; EPA, 2019). The influence of the exposure time profile on the risk of adverse health outcomes resulting from an exposure depends on the dynamics of the underlying processes of injury. For exacerbation of asthma, for example, relatively brief periods of exposure may be relevant, even minutes at sufficiently high concentrations; such brief time periods are also relevant for airborne infections. For carcinogens, far longer timeframes are relevant.
The upstream drivers of exposure—the determinants of the potential for exposures—encompass the social determinants of health. For example, industrial sources of exposure are often located more densely in poorer neighborhoods in urban areas, as are busy roadways, increasing exposures to air pollution and the potential for unintentional spills or releases that create higher concentrations of airborne pollutants. To protect against the adverse effects of exposure, people may choose to leave a location where airborne contamination (e.g., wildfire smoke) poses a threat, or to modify the environment to be more protective (e.g., by reducing air exchange or adding air-cleaning devices). However, the ability to leave or modify one’s environment to reduce exposure to a hazard will be limited for some groups (e.g., the elderly or infirm, workers housed by their employers and required to continue outdoor work), and the ability to do so will be influenced by the social determinants of health. During the COVID-19 pandemic, for example, workers in the service, food processing, and transportation sectors, typically in lower-wage jobs, were at elevated risk for infection because their jobs demanded contact with others and could not be carried out from remote locations.
Ambient Air Pollution and the Contribution of Wildfire Smoke
Ambient air pollution is a mixture of toxic substances that can arise from natural sources, such as wildfires, dust storms, and volcanoes, or from sources both stationary (e.g., manufacturing plants) and mobile (e.g.,
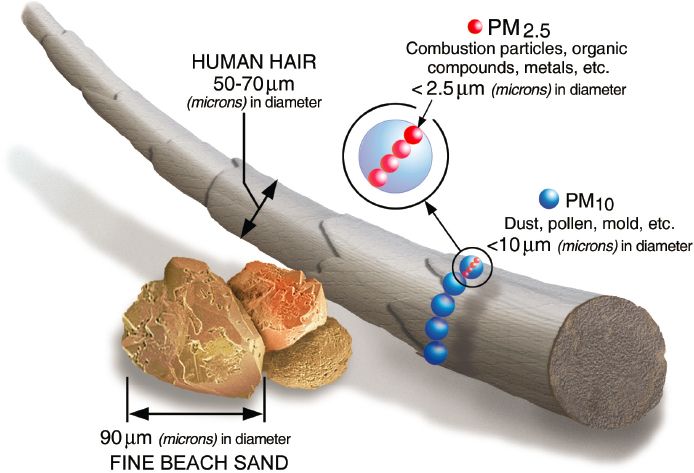
combustion engines in motor vehicles, airplanes) associated with human activity. PM in ambient air pollution includes particles of varying sizes that are defined by cut-points in sampling (see Figure 1-2): PM10 refers to particles with aerodynamic diameters of 10 micrometers or less, while PM2.5 denotes fine particles with aerodynamic diameters of 2.5 micrometers or less (EPA, 2021a). Both particle size and composition have implications for risk of adverse health outcomes.
Ambient air pollution contributes substantially to death and disability worldwide. In 2019, ambient PM pollution was one of three risk factors responsible for more than 1 percent of total disability-adjusted life years (DALYs) globally, with exposure levels increasing at a rate greater than 1 percent annually (Murray et al., 2020). In the United States, 100,000–200,000 excess deaths every year are attributable to air pollution, a figure that does not include the burden caused by wildfire smoke (Thakrar et al., 2020). PM2.5 exposure in particular has well-established associations with
SOURCE: EPA, 2021a.
cardiovascular disease, type 2 diabetes, pneumonia, lung cancer, chronic obstructive pulmonary disease (COPD), and other adverse outcomes (Bowe et al., 2019; EPA, 2019), and this burden of disease is borne disproportionately by communities of color and those with lower incomes (Bowe et al., 2019). Climate-exacerbated air pollution is anticipated to increase the burden of related adverse health effects among disproportionately exposed populations, further contributing to the health disparities seen throughout the nation (Rudolph et al., 2018).
Wildfire smoke is an increasingly important source of high-level exposure to hazardous air pollution. PM2.5 levels attributable to wildfire smoke have increased in recent years, particularly in the western United States but also in locations many hundreds of miles to the east (Burke et al., 2021). Beyond PM2.5, wildfires generate other air pollutants, including ozone precursors (Xu et al., 2020), carbon monoxide, oxides of nitrogen, methane, and volatile organic compounds (Cascio, 2018; Flannigan et al., 2009; Urbanski et al., 2008).
Globally, approximately 339,000 deaths annually are attributable to exposure to smoke from wildland fires (Cascio, 2018; Johnston et al., 2012), as are various forms of respiratory morbidity, including exacerbation of symptoms of COPD, asthma, bronchitis, and pneumonia (Cascio, 2018; Doubleday et al., 2020; Liu et al., 2015; Reid et al., 2016; Stowell et al., 2019; Youssouf et al., 2014). Some populations may be especially susceptible to the adverse health effects of wildfire smoke, including older individuals and people with preexisting respiratory illness and chronic disease (Liu et al., 2015; Reid et al., 2016), as well as pregnant women (CDC, 2021e). There is also some evidence suggesting that exposure to wildfire smoke during gestation can be associated with preterm birth and birthweight reduction (Amjad et al., 2021; Heft-Neal, 2021). Children are susceptible because, compared with adults, they breathe more air relative to their body mass (i.e., they receive a higher dose), their lungs are still developing, and they are more likely to be exposed to smoke since they spend more time outdoors (EPA, 2018; Holm et al., 2021).
Biological, Chemical, and Radiological Inhalation Agents
Biological, chemical, and radiological agents are significant inhalation hazards faced by the public and workers not covered by RPPs. Whether these hazards are naturally occurring, originate from accidental releases, or are the result of acts of terrorism, the associated adverse health effects necessitate a wide range of respiratory protection methods.
Biological agents of concern include bacteria, fungi, and viruses that can produce adverse health effects through infection and, for some agents, associated toxins (OSHA, 2021a). Communicable biological agents, such as respiratory viruses (e.g., influenza, measles, and chicken pox viruses), can be transmitted from person to person, while other biological agents may be infectious but not generally communicable. Molds, for example, which can pose risks to homeowners and recovery workers in the aftermath of a flood or hurricane (HUD, 2015), are not communicable from person to person, but inhaled spores can cause allergic reactions and hay fever symptoms, and potentially trigger asthma attacks (AAFA, 2015). Likewise, legionella bacterium, which causes severe respiratory disease in 10,000 to 28,000 individuals per year in the United States, is infectious via aerosol transmission but not communicable from person to person (Legionella.org, 2021).
Droplet transmission of communicable infectious agents occurs when particles greater than 100 micrometers in aerodynamic diameter (Samet et al., 2021) are propelled a short distance from an infectious source onto the mouth, nose, or eyes of a susceptible person (Jones and Brosseau, 2015; WHO, 2020). Airborne transmission, a term sometimes used interchangeably with aerosol transmission, involves the inhalation of aerosols or droplet nuclei—solid or liquid particles smaller than 100 micrometers in aerodynamic diameter—that are present in the air (Samet et al., 2021) and can remain infectious over a period of time and over longer distances (Jones and Brosseau, 2015; WHO, 2020). Additionally, compared with exposure to ambient air pollution, exposure to these agents tends to be spatially nonuniform and highly temporal.
Whether an infectious agent is communicable via the inhalational route and the mode of its transmission have implications for the selection of respiratory protection and where and when it is used. For example, surgical masks can be effective against larger-sized droplets by acting as a physical barrier and preventing these particles from reaching the respiratory tract (Tellier et al., 2019). By contrast, smaller-sized aerosols have a greater propensity to follow air flows, thus requiring a respiratory protective device with a tighter seal to protect the airways and a better filtering capacity than what a surgical mask can provide to ensure proper protection (Tellier et al., 2019).
Table 1-2 shows the enormous scale of the burden of disease associated with Mycobacterium tuberculosis (the cause of tuberculosis), influenza viruses, and coronaviruses, all of which are airborne transmissible biological agents.
| PREVALENCE | MORTALITY | |||
|---|---|---|---|---|
| TYPE OF AGENT | Global | U.S. | Global | U.S. |
| Mycobacterium tuberculosis | 1.7 billion infecteda 10 million ill | 7,174 casesb (2020) | 1.5 milliona | 526b (2019) |
| Influenza viruses | 1 billion total casesc 3–5 million severe cases | 35 million influenza-related casesd (2019–2020) | 290,000–650,000c | 20,000d (2019–2020) |
| Novel coronaviruses: | ||||
| a. SARS | 8,098 casese (2003) | 8 casese (2003) | 774e | — |
| b. SARS-CoV-2 | 249,743,428 casesf | 46,405,254 casesg | 5,047,652f | 752,196g |
| c. MERS-CoV | 2578 casesh | 2 casesi | 888h | — |
a CDC, 2020b.
b CDC, 2020a.
c WHO, 2019.
d CDC, 2021c.
e CDC, 2017.
f As of November 2021 (WHO, 2021b).
g As of November 2021 (CDC, 2021b).
h As of October 2021 (WHO, 2021a).
i CDC, 2019.
Chemical and radiological inhalation hazards are less frequent causes of public health disasters compared with biological hazards but can be extremely harmful to human health and the environment. Acute chemical incidents may result from leakages, explosions, and fires from, for example, damage to chemical plants and releases from railroad transport of chemicals (Bongers et al., 2008), such as chlorine gas. There have been several dozen public health disasters since 1940 during which large populations of people were exposed to chlorine gas (Culley and Svendsen, 2014).
Only specific types of respiratory protection are effective against a chemical inhalation hazard. Therefore, it is important to give careful consideration to proper respiratory protection in preparation for such an event, including the challenges of meeting surges in demand following large-scale incidents. Preparedness activities also need to take into account the
respiratory protection and guidance needs associated with the potential for inhalation of radioactive dust during radiation emergencies. Preparedness needs to focus not just on those “responders operating within Radiation Control (Fallout) Areas” (DHS, 2016, p. 31), but also on a larger group of emergency responders and public health workers working outside of these “hot zones” who may not be covered by an RPP but may be exposed while attending to contaminated people being evacuated from the area (Ansari, 2021).
Current Approach for Providing Respiratory Protection in the United States
As discussed previously, the use of respiratory protection in the United States has historically been associated with occupational settings in which workers are exposed to defined inhalation hazards—for example, health care workers exposed to tuberculosis, firefighters exposed to smoke, and miners exposed to coal dust and silica (NIOSH, 2019). The United States has an employer-based approach to occupational respiratory protection whereby employers are required to ensure that their workplaces are safe and their employees are protected from hazards, including inhalation hazards; compliance with this requirement is overseen primarily by OSHA. Other federal agencies oversee safety and health for specific types of workplaces (e.g., the Mine Safety and Health Administration [MSHA] for mining-related inhalation hazards) or exposures (e.g., pesticide exposure for pesticide handlers, regulated by EPA).
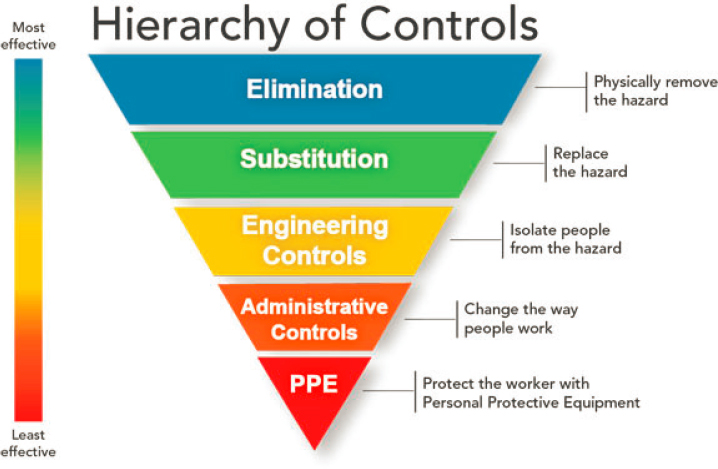
Respiratory protection is best realized when considered in the context of a larger system for injury and illness prevention that allows for the identification of hazards, the development of prevention and control measures to address these hazards, and evaluation of the efficacy of this system as part of an ongoing feedback loop. The hierarchy of controls (see Figure 1-3) is a framework initially developed for occupational settings8 as a component of such systems to limit the number of workers exposed to hazardous materials, reduce the intensity of exposures, and provide the most effective protection available (NASEM, 2019). Control methods at the top of the
___________________
8 Although the hierarchy of controls has traditionally been used as a means of determining how to implement control measures to protect workers, it can also be applied to protecting the health and safety of the public from such inhalation hazards as smoke and infectious agents. Management of COVID-19, for example, has required the concurrent implementation of administrative and engineering controls, such as mandated social distancing protocols (CDC, 2021d) and improved ventilation within schools, as means of protecting public health (NASEM, 2020).
NOTE: PPE = personal protective equipment.
SOURCE: NIOSH, 2015b.
hierarchy, such as elimination, substitution, or engineering controls, are typically more effective and reach more broadly than those at the bottom, such as personal protective equipment (PPE), use of which often occurs concurrently with other control methods. However, those higher-level controls may be more difficult to implement (NIOSH, 2015b) and, particularly in the case of engineering controls, can require higher initial capital costs, even though they may be more financially sustainable in the long term (NIOSH, 2015a). Compared with engineering controls, the use of PPE incurs a lower initial capital expense but is costly to maintain over time and requires adequate distribution, a system of oversight, and individual-level training on the devices’ use and maintenance. The conduct of hazard and exposure assessments to determine which hazards are present and the potential for exposure forms the basis for understanding the effectiveness of different control strategies and is the first step in ensuring people’s protection.
In workplaces where measures higher in the hierarchy of controls are insufficient to reduce hazardous exposures to known inhalation hazards and PPE in the form of respirators becomes necessary to protect the health
of employees, employers may be required by OSHA (or by other federal agencies with oversight authorities for specific populations or hazards) to establish an RPP to guide the selection and the safe and effective use of respirators that have been approved by NIOSH. Thus, while OSHA sets and enforces standards for use of respirators in workplaces to ensure safe and healthful working conditions, NIOSH—a research agency within CDC focused on occupational safety and health—establishes and enforces performance standards for respirators for workers. While some inhalation hazards are limited primarily to specific occupational settings, others, such as wildfire smoke, ambient air pollution, and respiratory viruses, may be ubiquitous, with exposures not limited to the workplace. Yet for members of the public and workers not covered by an RPP, no clear authorities are tasked with ensuring that respiratory protection meets user requirements or with providing information and guidance on the selection and use of these devices.
Origin of the Study
While the recommendations of this report will necessarily be viewed through the current lens of the global experience with the COVID-19 pandemic, recognition of critical gaps in the nation’s system for meeting respiratory protection needs preceded the emergence of SARS-CoV-2. Prior to the pandemic, NIOSH and its National Personal Protective Technology Laboratory (NPPTL) initiated efforts to address these gaps through discussions with the Department of State, EPA, the United States Forest Service, and other federal public health stakeholders regarding respiratory protection needs associated with exposure to wildfire smoke for the public and workers not covered by RPPs. As a result of increasing concerns among the public about wildfire smoke and associated poor air quality, NIOSH/NPPTL, along with EPA, had to field questions about the use of respiratory protection to mitigate this hazard (D’Alessandro, 2020). EPA also was asked for guidance on mitigating the harmful effects of mold exposure following flooding, which has become a frequent phenomenon in certain parts of the country. In parallel, Americans working overseas in locations with high levels of air pollution—such as China, India, and Indonesia—have sought guidance from the Department of State on safe and effective respiratory protection for themselves and their families (Huson et al., 2020). As noted, however, there are no clear authorities for providing such guidance.
A New Sense of Urgency
When the COVID-19 pandemic hit the United States in early 2020, it underscored the need to address gaps in oversight and messaging around respiratory protection for the public and for workers not previously considered at risk from inhalation hazards. An initial ad hoc approach to respiratory protection for the public and unclear messaging created significant confusion as to the purpose of respiratory protection and when to use it. Even after the use of respiratory protective devices had become common practice amongst the public, confusion persisted as to their purpose (protecting the wearer versus protecting others), the type of products that should be used (e.g., cloth face covering versus surgical mask versus respirator), who should wear them, and when and where they should be worn. Inconsistent public health messaging and widespread misinformation worsened the confusion (Schwellenback and Zagorin, 2020; Shelus et al., 2020; Stoller, 2021). Moving forward, the nation cannot afford to repeat the ad hoc and inconsistent measures taken during the pandemic to address safety and respiratory protection; the same holds for wildfires. The public and all workers need to be able to turn to a clear and authoritative source of information, and a system for providing accurate guidance and effective messaging needs to be in place.
STUDY APPROACH
Given the complexities of the systems for respiratory protection described throughout this report, the committee undertook its charge by taking a systems approach. As discussed below, this approach had to build on a foundation of concepts of risk and how it can be reduced. Illustrative examples of inhalation hazards, most notably related to wildfire smoke and COVID-19, are woven throughout the report to ground the discussion in real-world scenarios requiring the use of respiratory protection.
Guiding Principles
The committee’s approach to its charge was grounded in guiding principles that emerged from discussions among its members. These principles reflect issues that will underlie the development and functioning of all components of a future system for respiratory protection, and accordingly guided the development of the committee’s framework and its recommendations:
- No person should be subject to adverse health effects from inhalation of respiratory hazards. All possible measures should be taken to control the risk of exposure to such hazards at their source. When elimination, engineering, administrative, and other controls are not feasible or available, effective respiratory protective devices should be available for the public as well as all workers.
- A framework for respiratory protection should incorporate a systems approach, given the diverse processes (e.g., hazard identification and assessment, product design and manufacturing, device selection and use) and the many and diverse stakeholders involved. Feedback loops are critical components supporting refinement and improved effectiveness of the system over time.
- Respiratory protection does not confer absolute protection. Although a level of risk remains with available devices, respiratory protection decreases the risk for harms to health. When details of a hazard are known, appropriate respiratory protection should decrease risk to a level considered acceptable based on a structured risk assessment.
- Recommendations on respiratory protection for the public, especially during public health emergencies, will be based on evolving and incomplete information, which will necessitate decision making under uncertainty. Therefore, the actions taken and recommendations made in response to such emerging evidence must be guided by the ultimate aim of optimizing benefits to public health. Decisions should be justified and explained in a transparent fashion, and should take into account the context, cultural characteristics, socioeconomic conditions, and linguistic needs of those who are most vulnerable.
- The framework for a respiratory protection system needs to incorporate preparedness into every process, or failures may occur during times of acute need or stress (i.e., during disasters or public health emergencies). Efforts to enhance preparedness need to have a broad reach, from individuals and systems to private- and public-sector entities. Preparedness must also include robust mechanisms for surveillance and scientific research (to address the aforementioned uncertainties).
- The population requiring access to functional, acceptable, and accessible respiratory protection is highly heterogeneous across multiple dimensions: age, racial and ethnic background, variation in facial profiles, underlying health and disease status, level of education, income, language, geographic location, and others. Ensuring equitable access to effective respiratory protection for all people in
- all subgroups of the population, as defined by these and other factors, represents a challenge that must be met by all aspects of the framework.
A Risk-Based, Systems Approach to the Development of a Framework for Ensuring Access to and Effective Use of Appropriate Respiratory Protection
Framing Risks
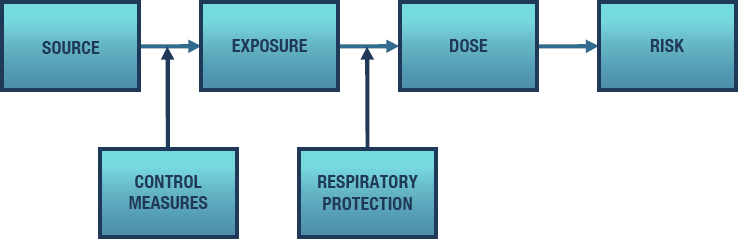
In the context of this report, the term “risk” refers to the likelihood that a hazardous exposure will result in an adverse outcome. A further imperative for respiratory protection comes from the severity of the potential adverse outcomes. The goal of respiratory protection, regardless of who is using it, is to reduce the risk of adverse responses to inhaled agents. Figure 1-4 provides a simplified version of a toxicological paradigm that extends from the sources of hazardous agents to the consequences of exposures—an increase in risk for one or more adverse health outcomes. Control measures within the hierarchy of controls (described earlier in this chapter) are directed at the connection between the source and exposure. Examples include engineering controls to reduce emissions or to increase ventilation of indoor spaces so as to reduce the concentration at which exposure occurs, and administrative controls, such as social distancing. When such higher-level forms of protection in the hierarchy are unavailable, insufficient, or inapplicable, respiratory protection reduces the amount of hazardous agent inhaled (and, by extension, the dose received). This paradigm applies to both target populations for this report: workers not covered by RPPs and the general population.
The NIOSH conformity assessment framework for PPE, which provides a structure for ensuring that a product will perform as intended (see Chapter 2), has “hazard & risk assessment” as a primary driver. For those workers covered by an RPP mandated by OSHA or MSHA, the goal is to prevent the consequences of known exposures to hazardous substances with identified adverse outcomes. For those specific agents and environments targeted by RPPs, the hazards are well established, and dose-response relationships are generally characterized. The circumstances of workplace exposures are also generally known with regard to concentrations typically encountered, the temporal profile of exposure, and the duration of exposure. The risks of these exposures can reasonably be predicted without great uncertainty. In contrast, the evidence is far more limited for many agents that pose risks to workers not covered by RPPs and to the public.
The model for workplace RPPs offers a useful benchmark for considering the hazards faced by the general population and by those workers not covered by an RPP. However, for the populations—workers not covered by an RPP and the public—that are the targets of this study, the specificity that characterizes the OSHA and MSHA programs is lacking; the agents of concern and the circumstances of exposure are broad and not readily specifiable; the populations affected are diverse and varying in demographic characteristics, vulnerability,9 and susceptibility;10 and exposures and risks may not be readily quantified.
With regard to the committee’s charge, an overall goal of any new respiratory protection system is to reduce risk from inhalation hazards to an acceptable level. In his 1976 book Of Acceptable Risk: Science and the Determination of Safety, William Lowrance writes: “A thing is safe if its risks are judged to be acceptable” (Lowrance, 1976). As the committee proposes a new framework for respiratory protection, that framework should have the goal of ensuring that risk remains within acceptable levels. To that end, first, risks need to be quantified so they can be judged, and, second, the acceptability of those risks needs to be determined. The challenges inherent in addressing these two tasks to achieve acceptable risk are evident.
The acceptability of risk is determined on a national level through legislation, executive branch regulations and enforcement, court decisions, and
___________________
9 The committee defines vulnerability as the likelihood of an individual being exposed to a hazard because of who they are or where they work, study, play, or live. Interindividual variability across these factors and others is associated with differences in exposure. For example, living closer to the source of an inhalation hazard may increase exposure and thus vulnerability.
10 Susceptibility can be defined as an individual’s risk for harm when exposed to a particular hazard. Susceptibility may be influenced by such factors as genetics, health status, and age, depending on the particular hazard.
public engagement through a variety of channels (e.g., nongovernmental organizations). Risk assessment is a central feature in some of these contexts, providing a mechanism for evaluating public health issues, developing policy, prioritizing research, and directing funding (NRC, 2009). EPA has formal procedures for risk assessment that include identifying the hazardous exposure and characterizing its health effects, measuring the level of exposure in environmental media, and estimating the dose received by individuals through various known routes of exposure. Risk communication and risk management follow.
U.S. regulatory efforts for environmental and occupational exposures assume that society will tolerate some risk to obtain the potential benefits of use of the hazardous substance. Societal acceptance has changed dramatically over time, but in general is lower for hazards that affect children or those for which exposure is perceived to be involuntary. EPA regulations typically are aimed at reducing the risk of lifetime adverse health effects, such as cancer, to between 1 in 10,000 and 1 in 1,000,000 excess deaths (EPA, 2021b). By contrast, the Occupational Safety and Health Act’s economic and technological feasibility requirements, as well a Supreme Court decision,11 have limited OSHA’s ability to set risk levels as low as those of EPA, allowing it to identify an acceptable exposure level above which it can issue fines or take other enforcement actions. In contrast, regulatory agencies in the European Union, upon determining that a hazard exists, require that it be reduced to levels that are as low as is reasonably achievable.
These regulatory and judicial precedents, however, have limited applicability to the target populations for this report. The methods for determining whether a hazard exists and quantifying risk are applicable, but the risk thresholds described above have uncertain relevance to establishing a framework for respiratory protection.
For workers not currently covered by an RPP, there are many gaseous and particulate workplace contaminants that might contribute to risk. The list is similarly expansive for the public. Some of these hazards (e.g., dust storms and accidental releases at chemical plants) have been long-standing, while others, such as airborne infectious agents and wildfire smoke, are emerging with greater intensity and are likely to become more frequent and severe. Moreover, exposure profiles are likely to vary in time, place, and intensity. In the case of wildfires, for example, persons adjacent to a fire or directly impacted by smoke plumes may be exposed to high levels of smoke with PM2.5 concentrations exceeding health-based National Ambient Air Quality Standards by a factor of 10 or more. Typically, people would tolerate such conditions only briefly and take steps to distance themselves
___________________
11 Industrial Union Department v. American Petroleum Institute, 448 U.S. 607 (1980) (generally referred to as the “Benzene decision”).
if possible. Yet, some exposures, albeit at lower levels, may last for weeks and even months, as occurred with recent fires in California, Colorado, and Canada.
For both workers not covered by an RPP and the public, judgments about the acceptability of the risks posed by inhalation hazards cannot readily and immediately be made, given the wide range of exposures and broad spectrum of susceptibility, as well as the present lack of a path for achieving consensus on what constitutes an acceptable level of risk. There are also two broad perspectives to be taken: reduction of individual risk and of population risk. Finally, the potential for limiting exposure varies across subgroups of the population. In its general framework for respiratory protection and its frameworks for the two populations targeted by this study—workers not covered by an RPP and the public—the committee addresses the need to incorporate estimates of risk and consideration of its magnitude, but does not provide guidance on specific methods for doing so, an issue beyond the scope of the committee’s charge.
Adopting a Systems Approach to Respiratory Protection
In early discussions with the study sponsors regarding the study scope, the committee was encouraged to adopt a systems view of respiratory protection in addressing its task.
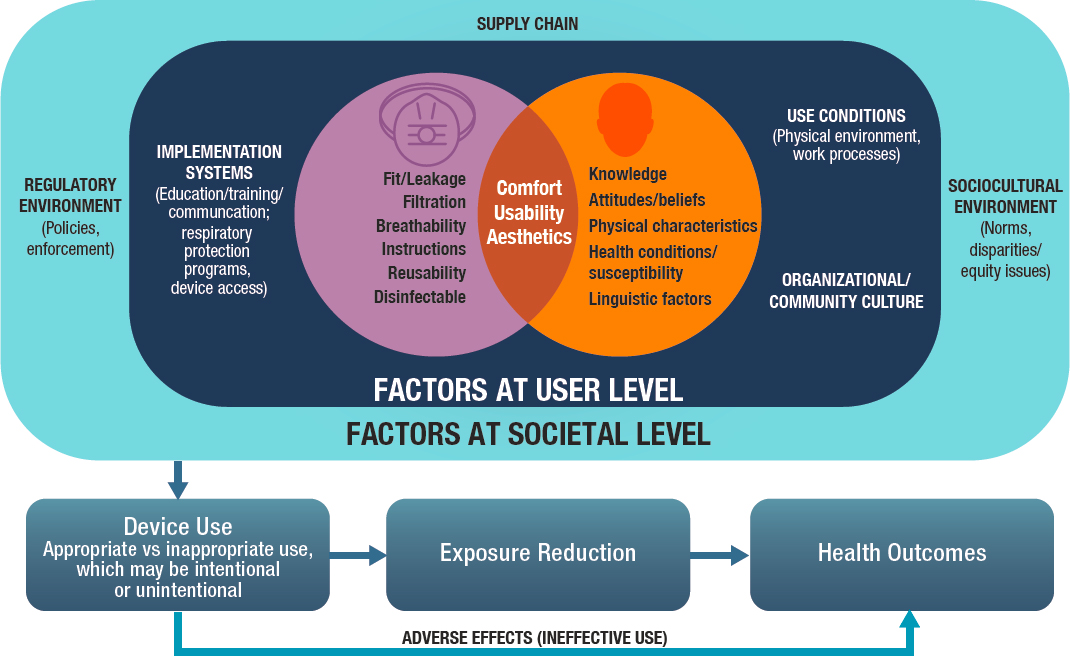
A systems approach, as conceptualized by the committee, seeks to understand the system elements that influence the desired outcome (in this case, access to and effective use of respiratory protection), as well as the relationships among those elements. Based on this understanding, approaches (e.g., designs, constructs, processes, policies) to achieving the desired outcome can be identified. In the context of this report, the systems approach has two distinct applications. The first is the committee’s development of a framework of authorities and responsibilities, central to its charge, which required consideration of complex and interdependent roles, processes, and resources of stakeholder organizations. The second application relates to the committee’s review of the evidence on factors that influence the effectiveness of respiratory protective devices, as measured by reduced exposures and risk of adverse health outcomes from inhalation hazards, along with associated gaps. In this application, the committee adopted an ecological model (see Figure 1-5) as a foundation for exploring the varied system components (e.g., devices, users, societal factors) involved and their interrelationships. Thus, the committee’s information-gathering approach included not only the specific characteristics of different devices (e.g., fit, filtration), but also a range of factors within a broader system related to how, whether, and when respiratory protection is used (e.g., sociobehavioral,
environmental, and regulatory factors). This approach is particularly crucial for understanding use of respiratory protection by the public and by workers not covered by an RPP because for these populations, no structure currently exists for selecting and providing an appropriate device and then, importantly, ensuring its effective use.
Approach to the Development of the Committee’s Frameworks
In developing and defining its frameworks, the committee
- evaluated other frameworks and systems in place (e.g., National Planning Frameworks for National Preparedness, Public Health Emergency Medical Countermeasures Enterprise) to ensure the health and safety of the nation during unforeseen events, such as terrorist incidents and natural disasters;
- applying the set of guiding principles presented above, identified the key characteristics or capabilities required to ensure access to and effective use of respiratory protective devices while overcoming the shortcomings of the current system, as enumerated in the conclusions presented in Chapters 2 through 4;
- identified the current stakeholders, if any, engaged in carrying out activities to evaluate inhalation hazards and ensure the availability and effective use of respiratory protective devices;
- explored the potential to expand the existing responsibilities and authorities of these current stakeholders to carry out the necessary activities in the committee’s proposed frameworks and associated challenges, if any; and
- identified a set of key strategic, organizational, regulatory, and operational factors important to ensuring successful implementation of the proposed frameworks.
The committee was charged with recommending a framework of responsibilities and authorities related to oversight and guidance for respiratory protection; the implementation of this framework is beyond the study scope. Moreover, given the diversity of inhalation hazards and scenarios for use of respiratory protection, the framework’s implementation will necessarily be complex and iterative. Accordingly, the committee does not explore implementation approaches in depth in this report, but provides illustrative examples of approaches that might be considered when such examples are helpful in describing the framework.
Comprehensive Literature Reviews
The committee was charged with determining current gaps in and the need for guidance for the public and workers not covered by an RPP across a range of inhalation hazards (see Table 1-1). In the language of the charge and during the first committee meeting, one of the sponsors emphasized that this evaluation of gaps in guidance should be based on an assessment of existing knowledge about the spectrum of factors that influence the effectiveness of respiratory protection used by specific user populations for specific inhalation hazards. The committee approached this aspect of its charge by carrying out comprehensive reviews of the literature to capture what is currently known about these factors across a set of prioritized use scenarios (see the section “Prioritizing Comprehensive Review Topics” below). Using this approach, the committee sought to capture literature on the breadth of interrelated factors within the system model depicted in Figure 1-5 above and to assess where research may be needed to understand the nuances of effective use of respiratory protection across different use scenarios. For example, the committee reviewed literature on traditional measures of performance, such as fit and filtration efficiency, but also on user-oriented considerations—such as comfort, usability, and attitudes and perceptions—as well as broader factors within the user’s environment and society, such as the regulatory environment, access to and availability of products, and education and training, among others.
The committee uses the term “comprehensive reviews” to denote the deep dives requested by the sponsors, and notes that these were not systematic reviews using, for example, Cochrane or other methods. Given the constraints of time and available resources, such formal systematic reviews were not feasible. The findings from its reviews informed the committee’s understanding of user needs across the prioritized use scenarios (see Appendix B). The committee notes that the paucity of literature on respiratory protection in the context of some of those scenarios limited the conclusions that could be drawn and instead indicated where research is needed to inform future guidance. Gaps and needs related to guidance are discussed in Chapters 3 and 4 for workers not covered by RPPs and the public, respectively, and draw on the findings from the literature reviews and an assessment of existing guidance related to inhalation hazards faced by these populations, including SARS-CoV-2 and wildfire smoke. However, the development of guidance for specific inhalation hazards was beyond the scope of the committee’s charge.
Prioritizing Comprehensive Review Topics
In approaching its comprehensive reviews, the committee needed to establish priorities in addressing an expandable matrix of agents, exposure scenarios, and populations (see Table 1-1). An initial matrix, which was provided by the sponsors, included six different populations of interest and five different sets of agents, some comprising complex mixtures (e.g., ambient air pollution and wildfire smoke). The agents identified as potential foci for the committee’s reviews are all known to pose health risks, but through quite diverse mechanisms: inflammation (e.g., wildfire smoke), infection (e.g., respiratory viruses), and radiation (e.g., internal emitters). Exposure scenarios are also quite diverse, extending from acute to chronic (e.g., brief exposures to high levels of particles during a dust storm versus sustained exposures of wildland firefighters across repeated fire seasons). The scope of populations involved is also wide-ranging, from the entire U.S. population to particular worker groups.
From this matrix, cells defined by population and agent were selected based on the potential size of the exposed population, the likelihood of different exposure scenarios, and the risk posed by the agent. Together, these parameters define the potential burden of risk that could occur and provide insights as to the potential benefits of respiratory protection measures. The nature of the health outcome consequent to exposure was also considered.
For example, as of this writing, the COVID-19 pandemic is ongoing. The entire global population is at risk, with a range determined by the likelihood of exposure. For the public, the spectrum of risk reflects characteristics determining the likelihood of a more serious outcome (e.g., hospitalization or death). For workers, risk depends on the likelihood of face-to-face contact with infected individuals, also covering a range that is defined at its high end by front-line health care workers.
The committee used its judgment around these determinants of individual- and population-level risk, specifically
- the likelihood of exposure to the agent,
- the profile of exposures in time and place,
- the size of the population(s) potentially exposed,
- the distribution of susceptibility within the exposed population(s),
- the nature of the adverse health effects caused by the agent, and
- the burden of ill health and disease caused by the agent and the potential for a respiratory protection program to reduce that burden.
Based on these considerations, the committee prioritized its work to focus on specific exposure scenarios (defined by agent and population) in the matrix (see Table 1-1).
Methods for the Reviews
Appendix A describes the detailed methodology and supporting materials for the committee’s comprehensive reviews; a brief overview of the methodology is included here. To reiterate, the committee did not conduct systematic reviews; consequently, PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagrams are not provided, and a formal system for study evaluation was not implemented.
Literature searches for each of the ten comprehensive reviews were carried out in PubMed, Scopus, and EMBASE using lists of search terms developed through review of relevant articles and committee discussion. In some cases, additional articles were identified for inclusion in a review through reference mining, targeted searches, and committee input. Article titles and abstracts were screened for further full-text assessment for inclusion in the review based on the committee-approved criteria of interest described above (population, exposures, and outcome of interest). Articles that failed to meet these screening criteria were excluded. Full article texts were assessed using the criteria described in Appendix A. Committee members applied judgment in selecting articles for ultimate inclusion in the synthesis and excluded those that had limited relevance or applicability to the U.S. context, as well as those for which there were concerns regarding major methodological limitations (e.g., failure to use reproducible test methods and controls). A table summarizing the number of articles retrieved through the searches and remaining after screening can be found in Appendix A. A narrative synthesis of the evidence from the included articles was generated, and the committee identified key findings for each summarizing the salient points regarding what is known about factors that influence the effectiveness of respiratory protection within these use scenarios (see Appendix B).
The findings from the comprehensive reviews identify factors that influence the effective use of respiratory protection within the contexts of specific use scenarios, as well as many gaps where further research is needed. Findings from the reviews were integrated into Chapters 3 and 4 as part of the evidence base for descriptions of the current state of and critical needs for use of respiratory protection by workers not covered by an RPP and the public, respectively.
To address the aspect of its charge related to determining the need for guidance, the committee supplemented its reviews of the peer-reviewed literature with a separate assessment of the landscape of standards and guidance on respiratory protection for selected use scenarios in Table 1-1. For the purposes of this assessment, guidance included written, visual, or auditory information on webpages provided directly to users or to other stakeholders with roles in guidance dissemination (e.g., employers, public
health professionals, clinicians) for the purpose of supporting the selection, proper use, care, and disposal of respiratory protection for the hazards of interest. Information on standards and guidance was collected through a search of the gray literature, from sources that included PPE-Info;12 consensus standards organizations; and reports and webpages of federal agencies, state and local public health and air quality agencies, labor unions, professional associations, and academic and nonprofit institutions.
Other Information-Gathering Approaches
To supplement the evidence captured from its comprehensive literature reviews, the committee employed a multipronged approach to addressing knowledge gaps. Committee meetings held in November 2020, January 2021, July 2021, and October 2021 included public information-gathering sessions that provided an opportunity to hear from various stakeholders, including worker populations; representatives of national, state, local, and tribal public health agencies; manufacturers of respiratory protective devices; and federal agencies with oversight responsibilities and authorities related to respiratory protection and/or inhalation hazards (see Appendix A for all public meeting agendas and description of the committee’s deliberative process). Additionally, a request for clarifying information was made to NIOSH/NPPTL in September 2021 as follow-up to information shared at the July 2021 public meeting.
Finally, recognizing that the development of a framework of authorities and responsibilities would need to be grounded in a clear understanding of the existing statutes and regulations that address inhalation hazards and respiratory protection, the committee commissioned a paper on the regulatory landscape for respiratory protection (see Appendix C).
ORGANIZATION OF THE REPORT
This report is organized into seven chapters. Following this introductory chapter, Chapter 2 provides an overview of the regulatory landscape for respiratory protection, including critical gaps in current systems for ensuring access to and effective use of respiratory protective devices. Chapters 3 and 4 examine the needs, experiences, and challenges related to use of respiratory protection by workers and the public, respectively. Chapter 5 presents the committee’s general framework for respiratory protection,
___________________
12 NIOSH’s PPE-Info database serves as a compendium of federal regulations and consensus standards relevant to PPE and can be accessed at https://wwwn.cdc.gov/PPEInfo (accessed September 24, 2021).
including core functions, stakeholder responsibilities, and the authorities necessary to address current gaps in the nation’s system for oversight of respiratory protection. In Chapters 6 and 7, the committee explores the application of this general framework in frameworks specifically targeting workers and the public, respectively, and presents recommendations designed to ensure access to and effective use of respiratory protective devices by these two populations.
ANNEX 1-1 RESPIRATORY PROTECTIVE DEVICE TERMINOLOGY
| DEVICE | AGENCY | DEFINITION |
|---|---|---|
| Respirator | Food and Drug Administration (FDA)a | An N95 respirator is a respiratory protective device designed to achieve a very close facial fit and very efficient filtration of airborne particles. Note that the edges of the respirator are designed to form a seal around the nose and mouth. |
| 42 C.F.R. 84b | Respirator means any device designed to provide the wearer with respiratory protection against inhalation of a hazardous atmosphere. | |
| Occupational Safety and Health Administration (OSHA) Emergency Temporary Standard (ETS)c | Respirator means a type of personal protective equipment (PPE) that is certified by the National Institute for Occupational Safety and Health (NIOSH) under 42 C.F.R. § 84 or is authorized under an emergency use authorization (EUA) by FDA. Respirators protect against airborne hazards by removing specific air contaminants from the ambient (surrounding) air or by supplying breathable air from a safe source. Common types of respirators include filtering facepiece respirators, elastomeric respirators, and powered air-purifying respirators (PAPRs). Face coverings, facemasks, and face shields are not respirators. |
| Face mask | FDAa | A face mask is a product that covers the wearer’s nose and mouth. Face masks are for use as source control by the general public and health care personnel (HCP) in accordance with CDC recommendations, and are not personal protective equipment. Face masks may or may not meet any fluid barrier or filtration efficiency levels; therefore, they are not a substitute for N95 respirators or other filtering facepiece respirators. |
| OSHA ETSc | Face mask means a surgical, medical procedure, dental, or isolation mask that is FDA-cleared, authorized by an FDA EUA, or offered or distributed as described in an FDA enforcement policy. Facemasks may also be referred to as “medical procedure masks.” | |
| Surgical mask | FDAa | A surgical mask is a loose-fitting, disposable device that creates a physical barrier between the mouth and nose of the wearer and potential contaminants in the immediate environment. Surgical masks are regulated under 21 C.F.R. § 878.4040. |
| OSHA ETSc | Surgical mask means a mask that covers the user’s nose and mouth and provides a physical barrier to fluids and particulate materials. The mask meets certain fluid barrier protection standards and Class I or Class II flammability tests. Surgical masks are generally regulated by FDA as Class II devices under 21 C.F.R. § 878.4040—Surgical apparel. |
| DEVICE | AGENCY | DEFINITION |
|---|---|---|
| Barrier face covering | FDAa | A barrier face covering, as described in ASTM F3502-21, is a product worn on the face specifically covering at least the wearer’s nose and mouth, with the primary purpose of providing source control and a degree of particulate filtration to reduce the amount of inhaled particulate material. Barrier face coverings are not a substitute for N95 respirators and other filtering facepiece respirators. |
| ASTMd | A barrier face covering is a product worn on the face, specifically covering at least the wearer’s nose and mouth, with the primary purpose of providing source control and a degree of particulate filtration to reduce the amount of inhaled particulate matter. |
b 42 C.F.R. § 84.174.
REFERENCES
AAFA (Asthma and Allergy Foundation of America). 2015. Mold allergy. https://www.aafa.org/mold-allergy (accessed October 1, 2021).
American Lung Association. 2020a. Disparities in the impact of air pollution. https://www.lung.org/clean-air/outdoors/who-is-at-risk/disparities (accessed September 27, 2021).
American Lung Association. 2020b. Who is at risk? https://www.lung.org/clean-air/outdoors/who-is-at-risk (accessed July 20, 2021).
Amjad, S., D. Chojecki, A. Osornio-Vargas, and M. B. Ospina. 2021. Wildfire exposure during pregnancy and the risk of adverse birth outcomes: A systematic review. Environment International 156:106644.
Ansari, A. 2020. Respiratory protection needs during a nuclear/radiological emergency. Presentation at the January 25, 2020, public meeting of the National Academies of Sciences, Engineering, and Medicine Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces, virtual. https://www.nationalacademies.org/event/01-25-2021/respiratory-protection-for-the-public-and-workers-without-respiratory-protection-programs-at-their-workplaces-committee-meeting-3 (accessed September 27, 2021).
ASTM. 2021. Standard specification for barrier face coverings. ASTM F3502-21. https://www.astm.org/Standards/F3502.htm (accessed September 24, 2021).
Bongers, S., N. A. H. Janssen, B. Reiss, L. Grievink, E. Lebret, and H. Kromhout. 2008. Challenges of exposure assessment for health studies in the aftermath of chemical incidents and disasters. Journal of Exposure Science & Environmental Epidemiology 18(4):341-359.
Bowe, B., Y. Xie, Y. Yan, and Z. Al-Aly. 2019. Burden of cause-specific mortality associated with PM2.5 air pollution in the United States. JAMA Network Open 2(11):e1915834.
Burke, M., A. Driscoll, S. Heft-Neal, J. Xue, J. Burney, and M. Wara. 2021. The changing risk and burden of wildfire in the United States. Proceedings of the National Academy of Sciences 118(2):e2011048118.
Cascio, W. E. 2018. Wildland fire smoke and human health. Science of the Total Environment 624:586-595.
CDC (Centers for Disease Control and Prevention). 2017. SARS basics fact sheet. https://www.cdc.gov/sars/about/fs-sars.html (accessed October 1, 2021).
CDC. 2019. MERS in the U.S. https://www.cdc.gov/coronavirus/mers/us.html (accessed March 8, 2022).
CDC. 2020a. Trends in tuberculosis, 2020. https://www.cdc.gov/tb/publications/factsheets/statistics/tbtrends.htm (accessed March 8, 2022).
CDC. 2020b. Tuberculosis. https://www.cdc.gov/globalhealth/newsroom/topics/tb/index.html (accessed October 1, 2021).
CDC. 2021a. COVID data tracker. https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed September 28, 2021).
CDC. 2021b. COVID data tracker weekly review: Interpretive summary for July 9, 2021. https://covid.cdc.gov/covid-data-tracker/#trends_dailycases (accessed November 8, 2021).
CDC. 2021c. Estimated influenza illnesses, medical visits, hospitalizations, and deaths in the United States—2019–2020 influenza season. https://www.cdc.gov/flu/about/burden/2019-2020.html (accessed October 1, 2021).
CDC. 2021d. Participate in outdoor and indoor activities: Activities, gatherings, and holidays. https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/outdoor-activities.html (accessed October 1, 2021).
CDC. 2021e. Wildfire smoke and pregnancy. https://www.cdc.gov/air/wildfire-smoke/pregnancy.htm (accessed September 30, 2021).
CDC and HUD (Department of Housing and Urban Development). 2006. Indoor air pollutants and toxic materials. In Healthy housing reference manual. Atlanta, GA: Department of Health and Human Services. https://www.cdc.gov/nceh/publications/books/housing/cha05.htm (accessed July 20, 2021).
Chen, Y.-J., G. Qin, J. Chen, J.-L. Xu, D.-Y. Feng, X.-Y. Wu, and X. Li. 2020. Comparison of face-touching behaviors before and during the coronavirus disease 2019 pandemic. JAMA Network Open 3(7):e2016924.
Chen, H., J. M. Samet, P. A. Bromberg, and H. Tong. 2021. Cardiovascular health impacts of wildfire smoke exposure. Particle and Fibre Toxicology 18(1):2.
Coffey, C. C., R. B. Lawrence, D. L. Campbell, Z. Zhuang, C. A. Calvert, and P. A. Jensen. 2004. Fitting characteristics of eighteen N95 filtering-facepiece respirators. Journal of Occupational and Environmental Hygiene 1(4):262-271.
Culley, J. M., and E. Svendsen. 2014. A review of the literature on the validity of mass casualty triage systems with a focus on chemical exposures. American Journal of Disaster Medicine 9(2):137-150.
D’Alessandro, M. 2020. Presentation at the November 5, 2020, public meeting of the National Academies of Sciences, Engineering, and Medicine Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces, virtual. https://www.nationalacademies.org/event/11-05-2020/meeting-1-committee-on-respiratory-protection-for-the-public-and-workers-without-respiratory-protection-programs-at-their-workplaces (accessed September 27, 2021).
DHS (Department of Homeland Security). 2016. Health and safety planning guide: For planners, safety officers, and supervisors for protecting responders following a nuclear detonation. https://www.dhs.gov/publication/ind-health-and-safety-planning-guide (accessed October 1, 2021).
Doubleday, A., J. Schulte, L. Sheppard, M. Kadlec, R. Dhammapala, J. Fox, and T. Busch Isaksen. 2020. Mortality associated with wildfire smoke exposure in Washington State, 2006–2017: A case-crossover study. Environmental Health 19(1):4.
EPA (Environmental Protection Agency). 2018. Wildfire smoke factsheet: Protecting children from wildfire smoke and ash. https://www.epa.gov/sites/default/files/2018-11/documents/protecting-children-from-wildfire-smoke-and-ash.pdf (accessed October 1, 2021).
EPA. 2019. Integrated science assessment (ISA) for particulate matter (final report, Dec 2019). https://cfpub.epa.gov/ncea/isa/recordisplay.cfm?deid=347534 (accessed October 1, 2021).
EPA. 2021a. NATA Frequently Asked Questions. https://www.epa.gov/national-air-toxics-assessment/nata-frequent-questions (accessed October 22, 2021).
EPA. 2021b. Particulate matter (PM) basics. https://www.epa.gov/pm-pollution/particulate-matter-pm-basics (accessed October 1, 2021).
FDA (Food and Drug Administration). 2021. N95 respirators, surgical masks, face masks, and barrier face coverings. https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-surgical-masks-face-masks-and-barrier-face-coverings#s3 (accessed December 6, 2021).
Flannigan, M. D., M. A. Krawchuk, W. J. de Groot, B. M. Wotton, and L. M. Gowman. 2009. Implications of changing climate for global wildland fire. International Journal of Wildland Fire 18(5):483-507.
Heft-Neal, S., A. Driscoll, W. Yang, G. Shaw, and M. Burke. 2021. Associations between wildfire smoke exposure during pregnancy and risk of preterm birth in California. Environmental Research 203:111872.
Hinds, W. C. 1999. Aerosol technology: Properties, behavior, and measurement of airborne particles. New York: Wiley.
Holm, S. M., M. D. Miller, and J. R. Balmes. 2021. Health effects of wildfire smoke in children and public health tools: A narrative review. Journal of Exposure Science & Environmental Epidemiology 31(1):1-20.
HUD (Department of Housing and Urban Development). 2015. Mold: Worker and employer guide to hazards and recommended controls. https://www.hud.gov/sites/documents/IEPWG_MOLD_WORKER.PDF (accessed October 1, 2021).
Huson, C., S. Surendra, and M. Patel. 2020. Presentation on November 5, 2021, at the public meeting of the National Academies of Sciences, Engineering, and Medicine Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces, virtual. https://www.nationalacademies.org/event/11-05-2020/meeting-1-committee-on-respiratory-protection-for-the-public-and-workers-without-respiratory-protection-programs-at-their-workplaces (accessed September 27, 2021).
Johnston, F. H., S. B. Henderson, Y. Chen, J. T. Randerson, M. Marlier, R. S. Defries, P. Kinney, D. M. Bowman, and M. Brauer. 2012. Estimated global mortality attributable to smoke from landscape fires. Environmental Health Perspectives 120(5):695-701.
Jones, R. M., and L. M. Brosseau. 2015. Aerosol transmission of infectious disease. Journal of Occupational and Environmental Medicine 57(5).
Legionella.org. 2021. What is Legionnaires’ disease. https://legionella.org/about-the-disease/what-is-legionnaires-disease (accessed December 6, 2021).
Liu, J. C., G. Pereira, S. A. Uhl, M. A. Bravo, and M. L. Bell. 2015. A systematic review of the physical health impacts from non-occupational exposure to wildfire smoke. Environmental Research 136:120-132.
Lowrance, W. W. 1976. Of acceptable risk: Science and the determination of safety. Los Altos, CA: Kaufmann.
Lucas, T. L., R. Mustain, and R. E. Goldsby. 2020. Frequency of face touching with and without a mask in pediatric hematology/oncology health care professionals. Pediatric Blood & Cancer 67(9):e28593.
Moore, J. T., J. N. Ricaldi, C. E. Rose, et al. 2020. Disparities in incidence of COVID-19 among underrepresented racial/ethnic groups in counties identified as hotspots during June 5–18, 2020—22 states, February–June 2020. Morbidity Mortality Weekly Report 69:1122-1126.
Murray, C. J. L., A. Y. Aravkin, P. Zheng, C. Abbafati, K. M. Abbas, M. Abbasi-Kangevari, F. Abd-Allah, et al. 2020. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet 396(10258):1223-1249.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. Reusable elastomeric respirators in health care: Considerations for routine and surge use. Washington, DC: The National Academies Press.
NASEM. 2020. Reopening K–12 schools during the COVID-19 pandemic: Prioritizing health, equity, and communities. Washington, DC: The National Academies Press.
NIOSH (National Institute for Occupational Safety and Health). 2015a. Engineering controls. https://www.cdc.gov/niosh/engcontrols (accessed June 12, 2021).
NIOSH. 2015b. Hierarchy of controls. https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed October 1, 2021).
NIOSH. 2019a. 100 years of respiratory protection history. https://www.cdc.gov/niosh/npptl/Respiratory-Protection-history.html (accessed July 7, 2021).
NIOSH. 2019b. Emergency response resources. Page last reviewed February 15, 2019. https://www.cdc.gov/niosh/topics/emres/flood.html (accessed September 27, 2021).
NPPTL (National Personal Protective Technology Laboratory). 2021. The respiratory protection information trusted source. https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/respsource3fittest.html (accessed November 9, 2021).
NRC (National Research Council). 2009. Science and decisions: Advancing risk assessment. Washington, DC: The National Academies Press.
OSHA (Occupational Safety and Health Administration). 2021a. Biological agents. https://www.osha.gov/biological-agents (accessed October 1, 2021).
OSHA. 2021b. Subpart U—COVID-19 emergency temporary standard. https://www.osha.gov/sites/default/files/covid-19-healthcare-ets-reg-text.pdf (accessed December 6, 2021).
Reid, C. E., M. Brauer, H. Johnston Fay, M. Jerrett, R. Balmes John, and T. Elliott Catherine. 2016. Critical review of health impacts of wildfire smoke exposure. Environmental Health Perspectives 124(9):1334-1343.
Rowell, A. 2021. The regulatory landscape regarding respiratory protection. Paper commissioned by the Committee on the Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces.
Rudolph, L., C. Harrison, L. Buckley, and S. North. 2018. Climate change, health, and equity: A guide for local health departments. Oakland, CA: Public Health Institute; and Washington, DC: American Public Health Association
Samet, J. M., K. Prather, G. Benjamin, S. Lakdawala, J.-M. Lowe, A. Reingold, J. Volckens, and L. C. Marr. 2021. Airborne transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): What we know. Clinical Infectious Diseases 73(10):1924-1926.
Schwellenback, N., and A. Zagorin. 2020. Mask confusion. Washington, DC: Project on Government Oversight. https://www.pogo.org/investigation/2020/03/mask-confusion-looming-shortages-n95-masks (accessed July 20, 2021).
Shelus, V. S., S. C. Frank, A. J. Lazard, I. C. A. Higgins, M. Pulido, A. P. C. Richter, S. M. Vandegrift, R. N. Vereen, K. M. Ribisl, and M. G. Hall. 2020. Motivations and barriers for the use of face coverings during the COVID-19 pandemic: Messaging insights from focus groups. International Journal of Environmental Research and Public Health 17(24):9298.
Stoller, G. 2021. Expert advice about which mask to wear when traveling. Forbes, January 27. https://www.forbes.com/sites/garystoller/2021/01/27/expert-advice-about-which-mask-to-wear-when-traveling/?sh=3ad0c62e5b9c (accessed July 20, 2021).
Stowell, J. D., G. Geng, E. Saikawa, H. H. Chang, J. Fu, C.-E. Yang, Q. Zhu, Y. Liu, and M. J. Strickland. 2019. Associations of wildfire smoke PM2.5 exposure with cardiorespiratory events in Colorado 2011–2014. Environment International 133:105151.
Tellier, R., Y. Li, B. J. Cowling, and J. W. Tang. 2019. Recognition of aerosol transmission of infectious agents: A commentary. BMC Infectious Diseases 19(1):101.
Thakrar, S. K., S. Balasubramanian, P. J. Adams, I. M. L. Azevedo, N. Z. Muller, S. N. Pandis, S. Polasky, C. A. Pope, A. L. Robinson, J. S. Apte, C. W. Tessum, J. D. Marshall, and J. D. Hill. 2020. Reducing mortality from air pollution in the United States by targeting specific emission sources. Environmental Science & Technology Letters 7(9):639-645.
Urbanski, S., W. Hao, and S. Baker. 2008. Chemical composition of wildland fire emissions. In Developments in environmental science, Vol. 8. Netherlands: Elsevier. 79-107.
WHO (World Health Organization). 2019. WHO launches new global influenza strategy. https://www.who.int/news/item/11-03-2019-who-launches-new-global-influenza-strategy (accessed November 8, 2021).
WHO. 2020. Transmission of SARS-Cov-2: Implications for infection prevention precautions. https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions (accessed September 29, 2021).
WHO. 2021a. Middle East respiratory syndrome. http://www.emro.who.int/health-topics/mers-cov/mers-outbreaks.html (accessed December 16, 2021).
WHO. 2021b. WHO coronavirus (COVID-19) dashboard. https://covid19.who.int (accessed May 2020).
Xu, R., P. Yu, M. J. Abramson, F. H. Johnston, J. M. Samet, M. L. Bell, A. Haines, K. L. Ebi, S. Li, and Y. Guo. 2020. Wildfires, global climate change, and human health. New England Journal of Medicine 383(22):2173-2181.
Youssouf, H., C. Liousse, L. Roblou, E.-M. Assamoi, R. O. Salonen, C. Maesano, S. Banerjee, and I. Annesi-Maesano. 2014. Non-accidental health impacts of wildfire smoke. International Journal of Environmental Research and Public Health 11(11):11772-11804.










































