
2
The Regulatory Landscape for Respiratory Protection
This chapter describes the regulatory landscape for respiratory protection in the United States, which involves multiple agencies at the federal and subfederal levels with varying responsibilities and authority regarding different inhalation hazards. The chapter examines separately the authorities related to use and approval of respiratory protection, as well as supply issues. The evaluation of gaps and overlaps in authority highlighted in this analysis is intended to inform the need for a framework to ensure access to and effective use of respiratory protection by the public and all workers (see Chapter 5). The chapter also describes conformity assessment processes for respiratory protection and the challenges and limitations of current approaches.
USE OF RESPIRATORY PROTECTION IN THE WORKPLACE1
This section summarizes the federal and state authorities relevant to protection of workers from inhalation hazards, including approval of devices and requirements for use of respiratory protection in the workplace.
___________________
1 This section draws on a paper commissioned by the committee on “The Regulatory Landscape Regarding Respiratory Protection,” by Arden Rowell, J. D. (see Appendix C).
Federal Oversight of Use of Respiratory Protection in the Workplace
The Occupational Safety and Health (OSH) Act of 19702 gave the Occupational Safety and Health Administration (OSHA) and the National Institute for Occupational Safety and Health (NIOSH) substantial authority over regulation of the health and safety of many workplaces and over respiratory protection of workers in those workplaces. Other federal agencies, including the Environmental Protection Agency (EPA), have authority over specific inhalation hazards and in specific workplaces. The authority of different federal agencies for use of respiratory protection in the workplace are described in the sections below.
OSHA’s Oversight Authorities Regarding Use of Respiratory Protection in the Workplace
OSHA is empowered to issue and enforce safety standards to ensure that workers are protected from safety and health threats in the workplace.3 OSHA’s Respiratory Protection Standard4 requires employers to establish and implement a respiratory protection program (RPP) for workplaces where respirators are necessary to protect the health of employees from known inhalation hazards when higher forms of protection are insufficient (see Box 2-1 for the components of an OSHA-compliant RPP). At workplaces where respirators are not found to be “necessary to protect the health of the employee,” no RPP is required.5 As discussed further in Chapter 3, the Respiratory Protection Standard does allow for voluntary provision and use of respiratory protection in these workplaces, though it imposes limitations on that voluntary use. The employer is required to provide the employee with guidance developed by OSHA, “Information for Employees Using Respirators When Not Required Under the Standard.”6 In addition to regulation, such guidance provides another mechanism for OSHA to address the respiratory protection needs of workers. Guidance such as that available through OSHA’s respiratory protection website7 may be general or hazard-specific, and may function as the primary vehicle for providing government direction on respiratory protection for workers not covered by current regulations.
___________________
2 29 U.S.C. § 651.
3 29 U.S.C. § 655.
4 C.F.R. § 1910.134(c)(1).
5 29 C.F.R. § 1910.134(c)(2).
6 29 C.F.R. § 1910.134, Appendix D.
OSHA has also issued comprehensive exposure standards for a few agents that pose inhalation hazards, including asbestos and silica. These standards require employers to follow the hierarchy of controls, first attempting to remove the hazard from the workplace or use engineering controls to reduce or eliminate exposure. Depending on the circumstances, however, employers may provide their employees with respirators to ensure that exposure levels are below the permissible exposure limits (PELs). In these cases, the employer must establish and implement an RPP.8
Most workers are not covered by an RPP or by mandatory workplace safety standards addressing the use of respiratory protection. Consequently, in the face of novel or unanticipated threats, such as wildfire smoke or SARS-CoV-2, there is for most workers no preexisting foundation on which employers can build to ensure adequate respiratory protection. OSHA has the statutory authority to implement new or expanded requirements for RPPs for workers who are not part of a statutorily excepted group (e.g., state and local government workers in federal OSHA states or the self-employed) if it finds that the inhalation hazards faced by those workers pose a “significant risk.” OSHA also has the authority to issue emergency temporary standards requiring respiratory protection against such threats if it determines “that employees are exposed to grave danger from exposure,” and that the emergency temporary standard is “necessary” to reduce the danger.9 In June 2021, OSHA implemented an emergency temporary standard for health care workers to address COVID-19 risk. It has also issued multiple enforcement response plans during the pandemic10 and directed implementation of a National Emphasis Program (NEP) in an effort to ensure that employees in high-hazard industries (e.g., meat processing, warehousing, retail grocery, food service, corrections) would be protected from exposure to SARS-CoV-2 (OSHA, 2021). OSHA’s oversight authorities are described more fully in Appendix C.
Other Federal Agency Oversight Authorities Regarding Use of Respiratory Protection in the Workplace
Although OSHA has the primary authority for regulating workplace safety, the OSH Act prohibits OSHA from issuing workplace safety standards in any workplace where another federal agency creates or enforces workplace safety and health standards.11 This provision contributes to the complexity of the regulatory landscape and limits OSHA’s authority.
___________________
8 29 C.F.R. § 1910(Z).
9 29 U.S.C. § 655(c).
10 29 C.F.R. §§ 1910.132, 1910.134, 1910.141, 1910.145, 1910.1020.
11 29 U.S.C. § 653(b)(1).
EPA has authority for regulating a number of environmental inhalation hazards, some of which arise in workplaces. When it issues occupational safety and health standards under its statutory authority, these standards displace OSHA protections that would otherwise apply. There are areas of overlap between the authorities of EPA and OSHA, and the agencies generally coordinate their efforts. Examples include worker protection against pesticides and asbestos (Aagaard, 2011). Under the Federal Insecticide, Fungicide, and Rodenticide Act,12 EPA has issued the Agricultural Worker Protection Standard (WPS) to protect agricultural workers from pesticide exposures. It has used its authority under the Toxic Substances Control Act13 to protect state and local government workers engaged in asbestos abatement activities by implementing a requirement for an RPP that mandates use of NIOSH-approved respirators (Aagaard, 2011). This is of particular note since state and local government workers constitute an excepted group under OSHA. To eliminate possible duplication, EPA has harmonized its regulations with OSHA’s by cross-referencing them, thereby requiring state and local government employers to comply with OSHA’s asbestos regulations (and with any changes to those regulations that OSHA subsequently promulgates) (Aagaard, 2011).
Other agencies have statutory authority that displaces OSHA’s with regard to particular workplaces and the inhalation hazards those workplaces present. The chief example of this is the Mine Safety and Health Administration (MSHA), the successor to the Bureau of Mines. The primary statute empowering MSHA is the Federal Mine Safety and Health Act of 1977, which requires MSHA to establish mandatory health and safety standards for “coal and other mines.”14 MSHA thus has broad authority to regulate both use and oversight of respiratory protection, though this authority applies to the relatively limited set of workplaces that is made up of mines. The Nuclear Regulatory Commission (NRC) is the coordinating agency for incidents at or caused by nuclear facilities. In the event of a radiological release, the NRC is specifically responsible for providing recommendations for protective actions at the nuclear facility and for performing postincident surveillance and monitoring (DHS, 2016).
Gaps in Federal Oversight of Use of Respiratory Protection in the Workplace
Some workers appear to fall into gaps such that for them, no clear authority is responsible for regulating occupational respiratory protection.
___________________
12 7 U.S.C. §§ 136 et seq.
13 15 U.S.C. §§ 2601 et seq.
14 30 U.S.C. § 3; Federal Mine Safety and Health Act of 1977, 30 U.S.C. §§ 801.
These include self-employed persons, gig workers,15 unpaid volunteers, sole proprietors, partners, family members of farm employees, domestic workers in a residential setting, and independent subcontractors. These workers are exempted under OSHA’s interpretation of the OSH Act, and do not appear to be protected by occupational safety and health standards issued by any other federal authority.
The definitions of “employer” and “employee” in the OSH Act are vague and circular: “‘Employer’ means a person engaged in a business affecting commerce who has employees”; “‘Employee’ means an employee of an employer who is employed in a business of his employer which affects commerce.” OSHA has chosen to interpret these definitions narrowly, and reinterpretation of the definitions could result in coverage of additional workers not currently under OSHA’s jurisdiction. Other gaps in OSHA oversight are created by statutory language, such as that included in the general duty clause,16 which limits OSHA’s authority to conditions faced by an employer’s employees, thereby excluding workers not considered to be employees (e.g., gig workers). OSHA’s interpretation of the definitions of employer and employee in the OSH Act and its regulatory language focused on employer–employee relationships reflects the occupational landscape when the act was enacted, but it does not provide adequate protection for workers given the contemporary range of employment models (Michaels and Barab, 2020).
___________________
15 Gig workers represent a subset of contingent workers for whom “gigs,” generally short-term jobs, are mediated through a digital online platform. Contingent workers are those whose work arrangement does not include an explicit or implicit contract for long-term employment (Tran and Sokas, 2017). Currently, platforms through which gig workers are assigned and paid are not considered employers under OSHA (Bloom, 2019).
16 The General Duty Clause of the OSH Act stipulates that employers have a general duty to furnish to their employees “employment and a place of employment which are free from recognized hazards that are causing or are likely to cause death or serious physical harm to [their] employees” (Occupational Safety and Health Act of 1970, 29 U.S.C. §§ 654).
State and Local Authorities Regarding Use of Respiratory Protection in the Workplace
State and local authorities retain substantial authority over the regulation of several types of workplaces, most notably state and local government workplaces. Many states also administer their own occupational safety and health programs via OSHA-approved State Plans. There are currently 22 State Plans covering private and public state and local government workers and six State Plans covering only state and local workers (DOL, 2021). Analysis of census data suggests that 3.1 million state and local government workers in states without State Plans are not covered either by OSHA standards or by OSHA-approved State Plans (Maciag, 2014).
State Plan states must meet federal OSHA requirements but also may implement additional regulations to address specific hazards that pose threats to the health and safety of workers in their states. For example, California has promulgated two regulations that specifically address inhalation hazards and controls, including respirators for wildland fire smoke and for aerosol transmissible diseases (see Boxes 2-2 and 2-3, respectively). These standards set requirements for evaluating the risk of these hazards and specific respiratory protection requirements when they are needed. Washington (WAC 296-62-085 Wildfire Smoke) and Oregon (Oregon OSHA, 2021a) have issued temporary standards similarly intended to protect workers from exposure to unhealthy levels of wildfire smoke. All three states use EPA’s Air Quality Index for PM2.5 to trigger mitigation measures, including respirator use.
Authorities Regarding Development, Approval, and Marketing of Respiratory Protection for Use in the Workplace
NIOSH, with its division the National Personal Protective Technology Laboratory (NPPTL), is the primary federal authority for researching and approving respirators for the workplace. (See Box 2-4 for an explanation of certification versus approval.) While other federal and state organizations are involved in oversight for some workers in some industries or some hazards, these recommendations tend to be coordinated with NIOSH/NPPTL, which plays a critical role in centralizing evaluation of occupational respiratory protection. NIOSH also provides guidance for workers outside its programs, and in some cases has acted historically as a consultant on matters of respiratory oversight that touch on its expertise. However, NIOSH’s mandate, authority, and consequent testing protocols are directed toward workplace respiratory protection rather than public protection.
A variety of other federal agencies have authority over some aspects of oversight of the development, approval, marketing, or postmarket surveillance of devices used for the purpose of occupational respiratory protection. For example, some masks and respirators are intended for occupational use in a health care setting, and thus subject to Food and Drug Administration (FDA) regulation.17 Several years ago, concerns arose that some medical workers were using NIOSH-approved respirators that were not FDA
___________________
17 21 C.F.R. § 878.4040 (2020).
cleared18 (NASEM, 2017). FDA and NIOSH have since coordinated their overlapping authority for respirators used in medical care workplaces via a memorandum of understanding (FDA, 2017b).
During a public health emergency (as declared by the Secretary of Health and Human Services), FDA has the authority to issue an emergency use authorization (EUA) to allow the use of devices that are not approved (or are approved for a different use) if certain conditions are met (FDA,
___________________
18 Respiratory Protective Devices Used in Healthcare, 79 Fed. Reg. 14,515 (March 14, 2014).
2021b). EUAs issued during the COVID-19 pandemic (and later revoked) allowed respirators that had not been NIOSH approved but had been tested and approved under international standards (e.g., KN95s, FFPs) to be used in health care settings in the United States for a limited period of time (FDA, 2020, 2021c).
MSHA has substantial authority over a wide range of standards-setting and oversight functions within U.S. mines. It manages this authority via collaboration with OSHA and NIOSH for both functions. This coordination is robust with regard to respirator oversight, an area in which MSHA has established a memorandum of understanding with NIOSH whereby NIOSH has the lead role in respirator approval, while MSHA and NIOSH
jointly review and approve the respirators used for mine emergencies and rescues.19 MSHA also retains primary responsibility for several testing and oversight requirements specific to the use of respirators in mines, including investigation of complaints and potential deficiency of approved respirators that are used in mines, and for testing and approval of electrical and electronic components of respirators for use in potentially explosive atmospheres (an unusual feature of some mining contexts that poses additional hazards beyond those presented in many other workplaces).20
___________________
19 42 C.F.R. § 84.3 (2020). See also Respirator Protective Devices, 60 Fed. Reg. 30,336; 30,339 (June 8, 1995).
20 Respirator Protective Devices, 60 Fed. Reg. 30,338-39; 30,343; 30,349–30,351.
RESPIRATORY PROTECTION FOR THE PUBLIC21
While OSHA and NIOSH have primary oversight roles in respiratory protection in the United States, their authorities are limited to occupational settings. No central federal authority is responsible for respiratory protection for the public, nor is there even any centralized repository of information on which authorities are responsible for which hazards. This section summarizes the federal and state authorities relevant to protection of the public from inhalation hazards, including authorities to mandate or provide guidance on use of respiratory protection and authorities related to approval or clearance of devices that may be used by the public for that purpose.
___________________
21 This section draws on a paper commissioned by the committee on “The Regulatory Landscape Regarding Respiratory Protection,” by Arden Rowell, J. D. (see Appendix C).
Federal Oversight of Use of Respiratory Protection by the Public
EPA and the Centers for Disease Control and Prevention (CDC) have the broadest mandates regarding use of respiratory protection by the public, as described below, but no federal agency is currently tasked with addressing respiratory protection for the public from all hazards. In the absence of comprehensive federal regulation in this area, significant authority is left to the states. States may receive guidance from federal agencies; however, there is no formal system for coordinating the development and distribution of such guidance to state and local health agencies or the public.
EPA
EPA has authority to regulate some inhalation hazards faced by the public, although that authority is limited to environmental hazards, such as those resulting from exposure to toxic chemicals or air pollution, and it is not always clear how much authority the agency has to manage those hazards via respiratory protection. The Clean Air Act and the Toxic Substances Control Act, both administered by EPA, give the agency most of its authority in this realm.
EPA maintains substantial public resources regarding wildfires, including guidance for the public on how to address high levels of wildfire-related air pollution with respiratory protection (EPA, 2021f). It has developed information on reducing exposure to wildfire-related air pollution, highlighting that “the right respirator and proper fit can reduce your exposure to wildfire smoke” (EPA, 2021b), that respirators are not designed to fit children, and that facial hair prevents a proper fit (EPA, 2021b). EPA also maintains a downloadable app, SmokeSense, to help the public learn about health risks from wildfire smoke in their area and advise them on taking actions to reduce their exposure, such as wearing a well-fitting N95 filtering facepiece respirator (FFR) (EPA, 2021e).
EPA has adopted a number of voluntary programs addressing indoor air quality (EPA, 2021d). It has provided consumer information on best practices for remodeling and reducing radon, as well as advice on adequate and proper ventilation, much of which encompasses use of respiratory protection (EPA, 2021d).
As an example of how EPA has expanded its activities beyond the environmental hazards that have in the past been its primary focus, during the COVID-19 pandemic it issued guidance and conducted research related to SARS-CoV-2. For example, it issued information to the public regarding the coronavirus and indoor air (EPA, 2021c) and investigated the filtration performance of face coverings (Sickbert-Bennett et al., 2021).
CDC
Various centers within CDC have oversight responsibilities related to exposure of the public to inhaled agents, including, most notably, infectious diseases. Such oversight includes issuing guidance and, in limited cases, requirements related to respiratory protection. For example, CDC issued an emergency action requiring the use of face coverings on public transportation conveyances and at transportation hubs during the pandemic for purposes of source control (CDC, 2021c). It also has issued information for members of the public entering homes that have been flooded (CDC, 2019), including recommendations regarding the use of respirators (CDC, 2021b). CDC’s National Center for Environmental Health (NCEH) performs and coordinates applied research on a number of environmental hazards, including inhalation hazards; engages in public communication and education; and takes part in public health emergency training (CDC, 2021a). The Agency for Toxic Substances & Disease Registry (ATSDR) was created to protect the public from hazardous wastes and environmental substances (ATSDR, 2018).22 NCEH and ATSDR have established significant expertise regarding the health impacts of respiratory and other environmental hazards within CDC. Notably, these agencies, unlike NIOSH—an agency within CDC with a distinct occupational safety and health mission—are focused on health hazards faced by the public. Currently, there appears to be no division within NCEH/ATSDR working as a counterpart to NPPTL in NIOSH.
State and Local Authorities Regarding Use of Respiratory Protection by the Public
In the absence of a coherent federal system for addressing public use of respiratory protection, authority is left to state and local governments for creating and administering schemes for ensuring adequate public protection. States may choose to address respiratory protection for the public via proactive regulatory regimes, such as mask mandates, when those regimes have not been preempted by comprehensive federal action. Variation in state laws addressing public respiratory protection have been particularly salient during the COVID-19 pandemic. While no state has issued public mandates for respirators, many states have issued “mask mandates” requiring face coverings, the specific requirements, duration, and enforcement of which have varied by state (Chiwaya, 2021). The management of source control through mask mandates is legally justified by states’ “police power,”
___________________
22 See Comprehensive Environmental Response, Compensation, and Liability Act of 1980, 42 U.S.C. §§ 9601–9675; Resource Conservation and Recovery Act of 1976, 42 U.S.C. §§ 6901–6992 (as amended).
which gives them authority over matters of public safety23 (Berman, 2020; Blum, 2020; Gostin, 2003; Richards, 2020), as well as by states’ authority to declare and enforce quarantine within their borders (Thaler, 2021). Such power is particularly broad where, as is the case with the COVID-19 pandemic, no federal action preempts state authority on communicable diseases (Blum, 2020).
Authorities Regarding Development, Approval, and Marketing of Respiratory Protective Devices for Use by the Public
In the absence of an equivalent to NPPTL for nonoccupational settings, no single federal entity is responsible for overseeing the development, approval, marketing, or postmarketing surveillance of respiratory protective devices for the public, or for generating or overseeing a conformity assessment program for managing these processes.
FDA is responsible for regulating foods, drug products, and medical devices.24 When respiratory protection is provided by a medical device intended for a medical purpose, such as preventing disease, it is subject to regulation by FDA, through both potential premarket approval processes and control over device adulteration and misbranding. Respiratory protection not intended for medical purposes is not subject to FDA oversight or control. Yet, given that many inhalation hazards—including environmental hazards—can produce such diseases as cancer, it can be difficult to determine how far FDA’s authority reaches. Thus far, the agency does not appear to have claimed authority for regulating all respiratory protective devices for use in all circumstances to protect against any inhalation hazard that can cause any disease, and it has specifically disclaimed authority, for instance, over N95 FFRs used in “construction” (FDA, 2021a). The question of just how far FDA’s authority over respirators as devices reaches and how it interacts with the authorities of EPA, OSHA, and other entities, remains ambiguous.
During the COVID-19 pandemic, FDA claimed authority under the Federal Food, Drug and Cosmetic Act for regulating all face masks, shields, and respirators used by the public for a medical purpose (FDA, 2021a), including FFRs,25 which are classified as Class II devices. FDA had established this latter classification in 2007 (FDA, 2007) (see Box 2-5), and it was applied in 2009 during the H1N1 influenza pandemic, when two manufacturers received regulatory approval for four respirator models for
___________________
23 Gibbons v. Ogden, 22 U.S. 1, 203 (1824).
24 Federal Food, Drug, and Cosmetic Act of 1938, 21 U.S.C. §§ 301–392.
25 21 C.F.R. § 880.6260 Filtering facepiece respirator for use by the general public in public health medical emergencies.
use by the public (FDA, 2009). Two of these devices were discontinued in 2013 because of the lack of a market for them (McCullough, 2021), and it is unclear whether the other two models are currently available. Under current FDA classifications, face masks that are not surgical masks are regulated as Class I devices, and thus are not subject to performance standards or postmarket surveillance.26 In response to product shortages during the pandemic, FDA issued guidance indicating that for the duration of the pandemic, it would not object to the distribution and use for source control of face masks, barrier face coverings, and non-NIOSH-approved respirators that do not comply with its regulations as long as their use does not create an undue risk (FDA, 2021a).
The Consumer Product Safety Commission (CPSC) has some authority regarding face masks and respirators when they qualify as “products” for
___________________
26 21 C.F.R. § 878.4040 (2021) and § 880.6260.
regulation under the Federal Hazardous Substances Act (FHSA). It applies labeling, testing, and certification requirements, as well as flammability testing requirements, to consumer face masks (CPSC, 2021). It has disclaimed authority for regulating either face masks that qualify as “medical devices” or respirators (CPSC, 2021). CPSC does, however, consider consumer and children’s face masks to be apparel that is subject to the flammability testing requirements of the Flammable Fabrics Act.27
In the void left by the lack of a centralized federal authority, multiple agencies have issued nonbinding guidance to advise the public on use of respiratory protection in particular situations, such as when they are remediating mold in flooded homes (CDC, 2019; EPA, 2021a). This guidance often relies on oversight and approval provided by NIOSH for occupational contexts. However, neither NIOSH nor NPPTL appears to have any current guidance to provide to other agencies or authorities seeking to transfer NIOSH’s approval standards for public use. As a result, there appears to be no centralized authority identifying the ways in which approval of occupational respirators may be a misfit for or address needs other than respiratory protection for the public.
An additional legal factor that may affect the development and approval of respirators for the public is judicial liability regimes, such as retroactive liability in tort, that affect the liability of manufacturers and sellers of respiratory protection. Torts are civil wrongs that can arise when a wrong by one person or company causes harm to another (Garner, 2009). They generally arise out of state law and are often adjudicated in state courts (see, e.g., Dobbs, 2000; Kritchevsky, 2010). In environmental and public health contexts, tort law can provide additional incentives for manufacturers and sellers of respirators and other protective gear, thus forming part of the regulatory landscape that can affect the actions taken by firms and individuals with regard to manufacturing, selling, and marketing of respiratory protective devices for the public28 (Schwartz et al., 2009). In many cases, designers, manufacturers, and sellers of protective gear, including respirators, can be liable under products liability law29 if their products cause harm to others—even if their products were designed and manufactured according to regulatory standards such as those set by NIOSH for N95 FFRs (Schwartz et al., 2009). Additionally, potential liability for fraud may incentivize honest marketing of products, including respiratory protective devices available to the public. In Colorado, for example, the state attorney general secured a settlement with a company that had made misleading
___________________
27 Flammable Fabrics Act, 15 U.S.C. §§ 1191–1204. CPSC has indicated that consumer face masks must be tested to either 16 C.F.R. § 1610 or 1611.
28 30 U.S.C. § 811(a)(6)(A).
29 Products liability is an area of law that seeks to ensure that products are reasonably safe.
claims about the masks and respirators it sold during the COVID-19 pandemic (State of Colorado Office of the Attorney General, 2021).
CONFORMITY ASSESSMENT OF RESPIRATORY PROTECTION
Overview of Conformity Assessment
Conformity assessment is at the core of the ability to regulate products; it demonstrates that the “specified requirements relating to a product, process, system, person, or body are fulfilled” (ISO/IEC 17000), and verifies that a “particular product meets a given level of quality or safety” (ANSI, 2014, p. 3). The process of conformity assessment can provide information about a product and its characteristics, describe the product’s performance and consistency, increase a buyer’s confidence in the product, and help substantiate advertising and labeling claims (ANSI, 2014), as well as help regulators and buyers make decisions about safety and suitability by assessing whether a product conforms to a particular standard (ANSI, 2014).
The specific process of conformity assessment varies depending on the product in question, the organization conducting the assessment, and the governing standards and policies. Conformity assessment programs exist for a wide variety of products, including medical devices; aircraft; nuclear reactors; and personal protective equipment (PPE), such as helmets and respirators. Oversight of these programs is performed by various organizations, both federal and nonfederal (RTI, 2014). Such organizations are referred to as the “scheme owners”30 for those products.
___________________
30 A scheme owner is the person or organization responsible for the development and maintenance of a conformity assessment system (ISO/IEC 17000:2020).
In 2017, NIOSH published a National Framework for Personal Protective Equipment Conformity Assessment (NIOSH, 2017) to help the PPE industry meet the need for a consistent risk-based approach to PPE conformity assessment (see Figure 2-1).
Within this framework, the steps shown as “direct activities” are the primary activities of conformity assessment:
- determining the level of conformity assessment appropriate to the PPE type, intended use, and risk of failure;
- identifying the product requirements and standards against which conformity is to be assessed;
- collecting examples of the products to be assessed;
- gathering evidence of conformity through testing, inspection, examination of technical documentation, and/or auditing of the supplier’s quality system, as appropriate;
- reviewing the evidence and making a determination about conformity;
- attesting to conformity, through a supplier’s declaration, third-party certificate, and conformity marks as applicable;
- conducting market surveillance to determine ongoing conformity;
- taking enforcement or corrective action where necessary; and
- ensuring that all service providers in the process are competent through accreditation, auditing, and peer evaluation (NIOSH, 2017).
Organizations with roles in the conformity assessment process include
- manufacturers and suppliers whose products are assessed;
- standards-development organizations, governmental or private-sector, that provide product performance requirements and test procedures;
- testing organizations that evaluate products and provide test reports;
- certification organizations that manage the process of third-party certification;
- accreditation organizations that audit and determine the competence of testing and certification bodies; and
- government agencies that oversee conformity assessment processes and mandate the use of standards and conformity assessment in regulation.
Not all of these entities may be involved in every conformity assessment program. For example, a manufacturer may conduct testing of its products in its own laboratory or have a third-party laboratory do that testing. These labs may be third-party accredited. A certification body may have its own laboratory or contract with another organization to conduct the testing.
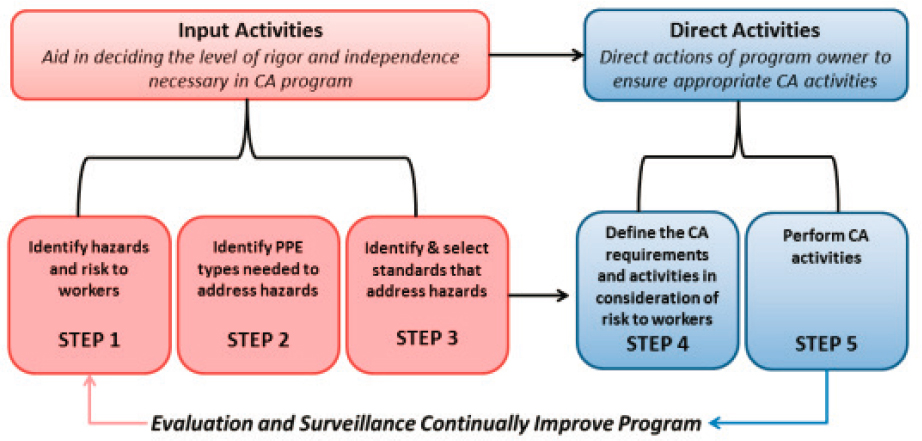
SOURCE: NIOSH, 2017.
Product standards used for conformity assessment may be developed by government agencies or voluntary consensus standards bodies. These standards may include product physical and performance requirements, test procedures for measuring or determining conformity with these requirements, and requirements for conformity assessment (NIOSH, 2017).
Conformity assessment has benefits for manufacturers, regulators, consumers, and the public (IOM, 2011). Manufacturers can gain valuable quality control feedback from the process, which can enable consistency in manufacturing and help avoid the costs of product failure. The process may also help differentiate a product from a competitor’s and validate marketing claims. Regulators benefit from conformity assessment by having a designated pathway to follow for determining that product claims are valid and verifying the consistency of the manufacturing process, which provides a platform for enforcing health, safety, and environmental regulations. The conformity assessment process gives consumers valuable information about a product, its intended use, and its limitations, all of which may assist them in evaluating label claims and making purchasing decisions. Finally, the public benefits from conformity assessment because it provides a common language with which to discuss a product (e.g., “NIOSH approved”) and because it ensures that products conform to standards designed to protect workers and the public from illness, injury, or death. Workers and the public may be more likely to use a product appropriately if they are confident that it will provide the intended protection (NIOSH, 2017).
Conformity Assessment Process for Respiratory Protective Devices
In the United States, the conformity assessment process for PPE entails a patchwork of different standards, policies, and organizations. Multiple public and private organizations conduct conformity assessment for PPE, and these conformity assessment programs “vary along a continuum of rigor in requirements and testing as well as independence from the PPE supplier” (NIOSH, 2017). Each approach to conformity assessment results in a different dynamic and culture among certifiers, users, and manufacturers (NASEM, 2021). In contrast with other PPE types, the conformity assessment processes for respiratory protective devices is comparatively regimented. The processes for different types of devices are described in the sections below.
Conformity Assessment for Respirators
NIOSH is the principal governmental agency with responsibility for testing and approving respirators. NIOSH’s NPPTL carries out all conformity assessment activities, including defining conformity assessment
requirements, conducting site qualifications for first-time applicants, performing testing and inspection, carrying out all preapproval activities (e.g., engineering and quality assurance review), and conducting postmarket surveillance (both approved product and approval holder site audits). NPPTL also conducts research, develops guidance and recommendations, develops and conducts intervention studies, and disseminates information as part of its mission to “to prevent disease, injury and death for millions of workers by advancing the state of knowledge and application of personal protective technologies (PPT).” (NIOSH, 2018b). The standards used by NIOSH include mandatory government standards outlined in 42 C.F.R. § 84 and those required by FDA as outlined in 21 C.F.R. § 878.4040, as well as voluntary consensus standards. The NIOSH Respirator Approval Program approves all classes of respirators used in workplaces across the United States; OSHA and MSHA require the use of NIOSH-approved respirators in certain occupational settings (NASEM, 2021). Importantly, NIOSH approval of respirators is premised on their use in the context of a workplace RPP.
To begin the NIOSH approval process, a manufacturer completes and submits a Manufacturer’s Questionnaire (NIOSH, 2021c). NIOSH reviews the completed questionnaire and assigns a manufacturer code if the information is satisfactory. Next, the manufacturer submits a Standard Application Form with all required documentation, including a written description of the product, drawings and specifications, and sample hardware for evaluation (IOM, 2011; RTI, 2014). The approval process is depicted in Figure 2-2. Specific tests required vary, depending on the type of respirator, hazard, and intended use, but may include such tests as
- airflow resistance test,
- exhalation valve leakage test,
- filter efficiency test,
- fit test,
- noise level test,
- particulate loading test,
- silica dust test, and
- communication performance test.
Of note, a fit test is not required as part of the approval process for FFRs—for such products, fit, which varies across devices and is critically important to achieving the intended level of protection, is ensured solely through the workplace RPP-based user fit testing (Coffey and Miller, 2019). As there is no equivalent user fit testing program for the public, the lack of a fit test during the conformity assessment process contributes to problems with public use of FFRs approved by NIOSH for workers. No single agency is charged with setting requirements for or conducting testing on all
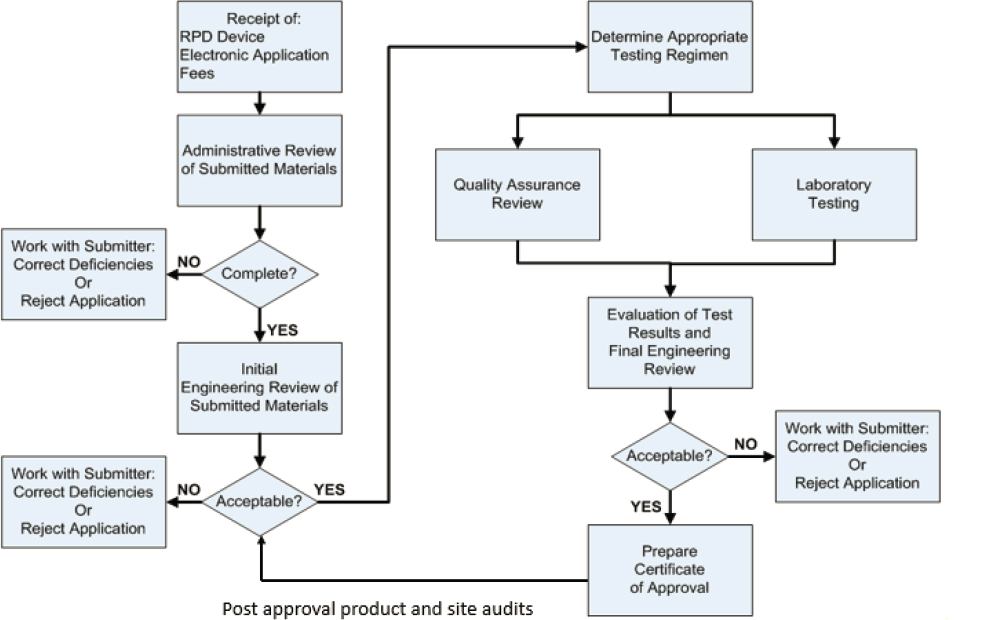
SOURCES: D’Alessandro and Peterson, 2020; NASEM, 2021.
products intended for public use. While some respirators have been found to have good fitting characteristics, others have been found to perform poorly in comparison (ASTM, 2021b). Fit capability testing (see Box 2-6) could provide users—both the public and workers—with some assurance that a respirator is capable of fitting a wide variety of faces, but it is not a substitute for user fit testing (Coffey et al., 2021). Users who are unable to perform respirator fit testing should expect lower respirator performance relative to the devices’ use in an RPP that includes fit testing.
In addition to conducting testing on a product, NPPTL evaluates the manufacturer’s quality assurance program and quality control plan (RTI, 2014). If the product is approved, NIOSH grants the manufacturer authorization to market the respirator as “NIOSH certified,” and adds the product to the Certified Equipment List on the NIOSH website (RTI, 2014). If the product is found not to be in compliance with the necessary standards, NIOSH issues a letter to the manufacturer explaining the problem and the corrective action that can be taken (RTI, 2014). Once products enter the market, NIOSH audits them by testing samples obtained through normal sales channels, and also investigates user complaints and products involved in serious illnesses, injuries, or fatalities (RTI, 2014). Every other year, NIOSH also conducts an inspection of a product’s manufacturing facility and its quality assurance program. These postmarket investigations can
result in voluntary product recalls, product retrofits, sales stops, or revocation of approval (RTI, 2014).
FDA is generally responsible for oversight of respiratory protective devices used in medical settings, which are classified as medical devices. In 2018, FDA and NIOSH entered into a memorandum of understanding aimed at streamlining the regulatory oversight for surgical respirators between the two agencies and allowing certain manufacturers to submit a single application to NIOSH instead of having to obtain approval from both agencies (NIOSH, 2018c). Since 2018, NIOSH has had the authority to approve surgical N95 FFRs without the need for FDA 510(k) clearance, except when applications submitted to NIOSH are determined to exceed CDC’s and FDA’s mutually agreed-upon threshold evaluation criteria. Applicants must supply NIOSH with documentation of testing for fluid resistance, flammability, and biocompatibility performed by a laboratory meeting FDA good laboratory practices (NIOSH and FDA, 2017).
Conformity Assessment for Nonrespirator Masks and Face Coverings
FDA 510K requirements for surgical masks
Surgical masks—also called dental or medical masks—are cleared for marketing through FDA’s 510(k) process (FDA, 2004). This process requires a manufacturer to submit information to FDA demonstrating that its product is as safe and effective as—that is, substantially equivalent to—a product that is legally marketed (the “predicate”) in the United States. Section 510(k) of the Federal Food, Drug, and Cosmetic Act (Public Law 75-717) describes this process and the requirements for demonstrating substantial equivalence. For a 510(k) submission for a surgical mask, FDA recommends that manufacturers include information including any identified risks from using the product, as well as measures for mitigating these risks (FDA, 2004). FDA also recommends that manufacturers test their products for
- fluid resistance,
- filtration efficiency,
- differential pressure,
- flammability, and
- biocompatibility.
For each of these characteristics, FDA provides recommended test methods or standards (FDA, 2004). For example, FDA recognizes the ASTM F2100-21 Standard Specification for Performance of Materials Used in Medical Face Masks, among others (FDA, 2021d). Once FDA has
determined that a product is substantially equivalent to the predicate, the manufacturer may market it.
Conformity assessment for barrier face coverings
In the context of the COVID-19 pandemic, ASTM developed a voluntary consensus standard (ASTM F3502-21) for barrier face coverings. ASTM defines barrier face coverings as devices that are “worn on the face, specifically covering at least the wearer’s nose and mouth, with the primary purpose of providing source control and to provide a degree of particulate filtration to reduce the amount of inhaled particulate matter” (ASTM, 2021c). Barrier face coverings are neither medical masks nor respirators. The standard notes that barrier face coverings can vary significantly, and that a wide range of factors (e.g., perspiration, length of time worn) could affect their performance. The conformity assessment process for barrier face coverings follows ASTM Guide F3050, Annex A3, Model A, which outlines requirements for design, performance, labeling, and user information. The standard also requires barrier face coverings to be tested by an accredited laboratory for
- submicron particle filtration efficiency, and
- airflow resistance.
Two levels of filtration efficiency (20 percent or higher and 50 percent or higher) and breathing resistance (15 mm H2O or below and 5 mm H20 or below) are established by the standard and require the use of testing methods similar to those used by NIOSH (Szalajda et al., 2021). While manufacturers are required to perform a design analysis to assess leakage of exhaled air from a barrier face covering, the ASTM standard does not require testing to demonstrate the effectiveness of the device for source control. Quantitative testing of leakage is optional, as is bacterial filtration efficiency testing. User instructions for barrier face coverings must include information about sizing, proper use and care, and product limitations.
Conformance with the standard is not predicated on third-party certification; instead, the manufacturer provides a declaration of conformity. It is also important to note that this is a voluntary standard, and as of this writing, there is no regulatory requirement for manufacturers to demonstrate that their products conform to the standard prior to sale.
Following the release of the ASTM standard for barrier face coverings, NIOSH issued interim guidance with criteria for workplace performance masks that build on the standard. The specifications are intended for masks that will be worn in the workplace to prevent the spread of SARS-CoV-2, but masks meeting the NIOSH criteria are not meant to serve as a substitute for respirators. In addition to the ASTM criteria for filtration and breathability, NIOSH has set criteria for leakage and requires quantitative
leakage testing, which is optional under the ASTM standard. Based on performance related to filtration, breathability, and leakage, masks can be labeled as Meets Workplace Performance or Meets Workplace Performance Plus (NIOSH, 2021a).
Standards Development for Respiratory Protective Devices
Before a product can be tested to ensure that it conforms to standards, those standards must be in place. The standards for respirator testing and approval are by statute issued by NIOSH and codified in 42 C.F.R. § 84. As a result, any new standards development process undertaken by NIOSH necessitates a change in regulations, which can be a lengthy process.
There are also voluntary consensus standards developed by nongovernmental organizations, which are often incorporated into government standards by reference31 (RTI, 2014). Use of voluntary standards helps harmonize standards, eliminates the cost to the government of developing its own standards, and provides incentives to establish standards that serve national needs (OMB, 1998). The National Technology Transfer and Advancement Act (NTTAA),32 signed into law in 1996, required government agencies to use voluntary consensus standards to the extent possible, and directed the National Institute of Standards and Technology (NIST) to eliminate unnecessary duplication by coordinating the conformity assessment activities of federal, state, and local entities with private-sector activities on technical standards and conformity assessment. Circular A-119, which is published and periodically revised by the Office of Management and Budget, establishes the policies on federal development and use of voluntary consensus standards and conformity assessment activities (OMB, 2016). Government agency staff often participate in the development of voluntary consensus standards, and in some cases take leadership roles in moving these standards through the consensus process. For example, NIOSH, which has extensive involvement and leadership in consensus standards for PPE (e.g., gloves, protective clothing, eye protection, hearing protection),33 helped initiate and participated in the development process for the above-described ASTM barrier face covering standard. In addition to the operational benefits of developing a new consensus standard, the process allows
___________________
31 “Incorporation by reference (IBR) allows Federal agencies to comply with the requirement to publish rules in the Federal Register and the Code of Federal Regulations (CFR) by referring to materials already published elsewhere” (NIST, 2020).
32 Public Law 104-113.
33 NPPTL staff members have served on standards committees at ASTM, the American National Standards Institute (ANSI), the International Organization for Standardization (ISO), and the National Fire Protection Association (NFPA).
for a more collaborative and responsive relationship between NIOSH and stakeholders who are critical for adoption. Despite these benefits, however, the incorporation of a consensus standard by reference can be a lengthy process (Smith, J., 2021).
Voluntary consensus standards are developed or approved by a number of national and international organizations. ANSI is the national standards body of the United States; it does not develop standards itself, but coordinates, facilitates, and promotes the development of voluntary standards (ANSI, 2021). ANSI accredits the procedures of organizations that develop standards and approves standards as American National Standards (ANS). ANSI-accredited organizations that develop standards for PPE, including respiratory protective devices include NFPA, the American Society of Safety Professionals (ASSP), ASTM International, and the International Safety Equipment Association (ISEA). Some of these organizations develop test specifications, while others develop standards that include requirements for conformity assessment. These voluntary consensus standards are used by a number of government agencies in their oversight of products. For example, FDA uses ASTM F2100, Standard Specification for Performance of Materials Used in Medical Face Masks (ASTM, 2021a).
International Organization for Standardization (ISO) brings together experts to develop voluntary international standards, and establishes standards and principles used for conformity assessment worldwide. Members of ISO include 165 national standards bodies; ANSI serves as the U.S. member body. ISO partners with the International Electrotechnical Commission (IEC) to form the system of worldwide standardization. Numerous ISO/IEC standards cover elements of conformity assessment systems, including standards for conformity assessment principles, guidelines for drafting standards suitable for conformity assessment, requirements for conformity assessment bodies, requirements for accreditation of those bodies, requirements for test laboratory competence, and requirements for certification bodies (ISO/IEC, 2020). In addition, a number of ISO product standards are related specifically to respiratory protection, including standards for testing leakage, particle filter penetration, resistance to flame, and fit testing (ISO, 2021).
Across the globe, there have been recent trends toward harmonizing standards, with a focus on such human factors as fit and comfort and on defining how different respirators can be selected and used for a variety of populations and purposes (Miller, 2020).
Conformity Assessment Approaches Outside the United States
The regulatory schemes for and approaches to conformity assessment vary from country to country. The Technical Barriers to Trade agreement
within the World Trade Organization prohibits the signatories (including the United States) from having conformity assessment procedures that are more trade-restrictive than necessary to meet their legitimate regulatory objectives. The United States employs a “license to use” model for respirators, whereby a respirator must meet set requirements for use in an RPP, and OSHA requires employers to select these respirators from the NIOSH Certified Equipment List. Thus, responsibility for ensuring that NIOSH-approved respirators are used falls on the employer. The public and workers without RPPs in their workplaces may have access to nonapproved devices on the market that do not meet a set standard. Other countries, including those in the European Union (EU), use a “license to sell” model whereby a product must have the certification mark in order to be sold, imported, or distributed, thereby putting responsibility on the manufacturer (European Commission, 2020). Unlike the United States, which has no path for approval of respirators intended for use outside of the workplace, some countries and regions, including China and the European Union, do not have separate respirator performance standards for occupational and public use (McCullough, 2021).
European requirements for PPE are established by regulation applicable to all member countries of the European Union. The PPE Regulation, which was approved in 2016 and became effective in 2018, superseded a PPE Directive that had been in place since 1989.34 Under the regulation, respirators are classed as Type III PPE, designed to protect against life-threatening hazards. They must be tested and certified by a Notified Body, a certification organization approved by a member state, and bear the “CE” mark, which ensures that the PPE will be acceptable for use anywhere in the EU. To qualify for the CE mark, respirators are tested to standards developed by the European Committee for Standardization (CEN) or ISO standards that are recognized by CEN.
Finally, there is a difference between “system approval” and “component approval.” System approval—which is used by NIOSH and countries including Brazil, Japan, and China—requires that respirators be tested and approved in every unique configuration possible. Component approval, on the other hand, requires that each individual component be held to a particular standard. CEN uses a component approval system, but also requires manufacturers to detail all combinations and issue recommendations for use, and it uses postmarket surveillance to monitor for compliance (Miller, 2020).
___________________
34 Regulation (EU) 2016/425.
Challenges and Limitations of the Current Conformity Assessment Approach in the United States
The current approach to conformity assessment for respiratory protection involves a number of challenges and limitations. While a certification or approval demonstrates conformance to a certain set of standards, it does not necessarily ensure that the standards themselves are sufficient and appropriate for the intended use and specific hazard (NASEM, 2021). Standards for respiratory protective devices have traditionally focused on device performance and less on such human factors as comfort and usability. Moreover, 42 C.F.R. § 84 does not specify standards for evaluating the fit of FFRs. The lack of a standard has resulted in issues that include approval of devices that do not fit the intended population and higher costs for the fit test required by OSHA (Coffey and Miller, 2019). The potential mismatch between standards and use may be particularly relevant when respiratory protective devices are used by the public for protection from a variety of hazards (e.g., wildfire smoke and SARS-CoV-2). Such devices were designed for use by healthy workers in occupational settings and for defined hazards, but as respiratory protection is increasingly used by the public and workers not subject to RPP requirements, challenges may arise with respect to defining the hazards and developing standards that are sufficient and appropriate for the intended use (NASEM, 2021).
The rigidity of the conformity assessment process—specifically, requirements for NIOSH testing of respirators—makes it difficult to respond to emergency situations. For example, during the COVID-19 pandemic, the demand for NIOSH-approved respirators skyrocketed, making it difficult for health care personnel and other workers to obtain the PPE they needed (Andrews et al., 2021; Friese et al., 2020). In response, NIOSH, FDA, and OSHA implemented a crisis strategy designed to improve the availability of respirators (de Perio et al., 2020); for example, NIOSH assessed international respirators against standards to which the international devices claimed conformance, rather than the U.S. standards (Andrews et al., 2021). However, these efforts were insufficient to meet the demand, and several other laboratories throughout the United States adopted NIOSH testing methods to evaluate the effectiveness of uncertified products (Irby and Nelsen, 2020; Manning, 2020). Existing laboratories that meet ISO quality standards and can conduct respirator testing in accordance with NIOSH requirements could be beneficial in responding to circumstances (e.g., pandemics) in which demands on NIOSH testing personnel result in delays in approvals and in enabling NIOSH to focus its unique expertise and resources on higher-level activities, such as research (Smith, A., 2021).
OVERSIGHT OF THE SUPPLY CHAIN FOR RESPIRATORY PROTECTIVE DEVICES
The supply chain for respiratory protective devices in the United States is part of a global marketplace, driven by supply and demand. Most respirators are sold through distributors—safety specialist and industrial distributors for industrial users and medical distributors for respirators used in health care. Manufacturers source raw materials, and in many cases finished products, from around the world. Customers order respirators through distributors with which they have ongoing business relationships, maintaining only enough inventory to supply immediate needs. Distributors respond by ordering respirators from manufacturers, who schedule their production and procurement of imports accordingly. This system is efficient and cost-effective, but it is subject to disruption when there is a sudden surge in demand due to a pandemic or other public health emergency (Patel et al., 2017).
With minimal inventories, customer demand can quickly outstrip product availability. Many manufacturers lack the excess capacity to increase production quickly; distributors are swamped with demands from existing customers and others seeking supplies; and customers seek sources of respirators outside their normal channels, placing orders from multiple vendors (Patel et al., 2017). Opportunistic brokers enter the market, often overcharging or providing questionable products.
Against this background, the sections below describe the nation’s existing systems for ensuring consistent supplies in emergency situations.
Federal Authorities35
The federal government has two primary mechanisms for stockpiling respirators and/or amplifying respirator availability during pandemics and other large-scale incidents: the Strategic National Stockpile (SNS) and the Defense Production Act (DPA). Federal authorities related to these two mechanisms are discussed below.
Authorities Related to Manufacturing of Respiratory Protection in Emergency Scenarios
The SNS, described below, can be only a short-term stopgap; the federal government’s more robust solution in the face of a pandemic and spiking demand is the DPA. Under the DPA, the president can address matters of critical infrastructure, technology, national economic security, and national public health and safety, from human-made and natural disasters as well as wartime concerns, through a series of mechanisms that mobilize national industrial capacity. The DPA allows the government to jump to the front of the line in purchasing goods and empowers the President to allocate resources as “necessary or appropriate”; it authorizes the government to assist private manufacturers, either by supporting existing supply chains or stimulating new technologies or modes of production; it authorizes the President to assess the industrial base, with power to obtain information by subpoena if necessary; and it facilitates partnerships with the private sector, including in the form of voluntary agreements, to build capacity (Anderson and Burris, 2021). The Federal Emergency Management Agency (FEMA) Administrator chairs the Defense Production Act Committee, which advises on effective use of the DPA and also reports to Congress.
Authorities Related to Stockpiling of Respiratory Protection
The SNS is the nation’s repository of medical countermeasures (e.g., antibiotics, antiviral drugs, vaccines) and other medical materiel, including respiratory protective devices (NASEM, 2016). The SNS is currently run by the Office of the Assistant Secretary for Preparedness and Response (ASPR) within the Department of Health and Human Services (HHS). The stockpile’s origins lie in a charge from Congress in 1999 to HHS and CDC to acquire a pharmaceutical and vaccine stockpile that could counter potential biological and chemical threats (HHS, 2021c). The program has expanded over the years to include additional supplies and has undergone name and
___________________
35 This section draws on the commissioned paper “The Regulatory Landscape Regarding Respiratory Protection,” by Arden Rowell, J. D. (see Appendix C).
oversight changes. Federal stockpiling authority is governed largely by the Public Health Services Act of 1944,36 amended by the Pandemic and All-Hazards Preparedness Act (PAHPA) of 2006.37
The SNS was designed to supplement the supplies of and resupply state and local public health agencies in the event of a national emergency. It consists of a series of large, strategically placed warehouses ready to distribute necessary materials across the country in the event of a health crisis, when states can request supplies from the SNS.
The Public Health Emergency Medical Countermeasures Enterprise (PHEMCE), led by ASPR, is a federal interagency group established by HHS that is charged with determining which items make up the SNS formulary38 based on a review of material threat determinations (CDC, 2014; Gerstein, 2020; NASEM, 2016). The PHEMCE works to define requirements for every medical countermeasure (MCM) to be included in the stockpile, leads research and procurement efforts based on these requirements, and also considers the most effective deployment strategies for these supplies (NASEM, 2016). The selection of every item to be included in the formulary is based on specific criteria, including a product’s ability to be rotated back into the commercial market, its demonstrated effectiveness against specific agents or threats, “its supply availability in the commercial market,” and considerations relating to its storage and cost (CDC, 2014). SNS products are organized in accordance with their effectiveness against specific threats, including those posed by biological, chemical, and radiological agents, as well as natural disasters and pandemic influenza. To determine the selection of PPE, subject matter experts are tasked with reviewing products against federal guidelines and creating performance standards designed to ensure that each item can meet the needs of affected communities during a public health crisis (NASEM, 2016). Moreover, ASPR can utilize its rapid purchasing power to buy medical supplies not included in its inventory by utilizing preestablished contracts with vendors (CDC, 2014).
The inclusion of PPE as a critical component of the SNS was expanded in 2006, when HHS purchased 104 million N95 FFRs for the SNS as preparation against a possible influenza pandemic (HHS, 2006). The decision making behind this purchase was based on “the need for protection, funding, and availability of products on the market that could immediately increase US readiness” (Patel et al., 2017). In 2009, this supply was largely depleted when the H1N1 pandemic caused demand for N95 FFRs to
___________________
36 Public Health Service Act, Public Law 104-321; Codified at 42 U.S.C. § 247d.
37 Public Law 109-417.
38 The wide variety of medical supplies and medical countermeasures (MCMs) included in the SNS are known as its formulary.
spike, and the federal government dispersed approximately 85 million of the N95 FFRs in the stockpile to state health departments to reduce shortages in health care settings. At the time, the supply was not replenished. A 2015 study estimated that the United States would need 3.5 billion N95 FFRs in a scenario in which 30 percent of the U.S. population became ill from pandemic influenza (Carias et al., 2015). The SNS currently holds multiple models of surgical and standard N95 FFRs, in addition to face shields, surgical gowns and coveralls, goggles, and gloves; the amount of stockpiled PPE has also increased in response to the COVID-19 pandemic (HHS, 2021b).
As with other materials included in the SNS that expire, the shelf life of stockpiled respirators and masks and the need for disposal and replacement present a challenge to ensuring that effective products are available for distribution when needed during emergencies. For this reason, ASPR is charged with routinely evaluating medical supplies on a quarterly or annual basis to ensure quality maintenance, monitor storage and environmental conditions, and oversee the proper rotation of products that have exceeded their shelf life (ASTHO, 2021).
Of note, NIOSH does not designate specific requirements related to the shelf life or ideal storage conditions of particulate-only air-purifying respirators as part of its respirator approval program, having left this responsibility to the approval holder of each product (NIOSH, 2021b). To examine the performance and quality of stockpiled respirators, NIOSH conducted a series of evaluations across federal, state, regional, and county facilities (NIOSH, 2021b). The results from one of the studies conducted at a federal facility showed that all 430 of the N95 FFRs that were tested “maintained their inhalation and exhalation resistance and filtration performance in accordance with NIOSH performance standards” after being stored for 12–13 years (NIOSH, 2020b, p. 1). Given that these respirators were not designed for long-term use, however, continual quality assurance is still necessary for all PPE included in the SNS.
Authorities Related to Distribution of Respiratory Protection
FEMA, the federal agency responsible for managing critical response to national emergencies, has an expanded role in respiratory protection during emergencies and natural disasters. When emergencies present inhalation hazards, as with COVID-19, wildfires, and radiological disasters, FEMA has a coordinating role that can affect the oversight of respiratory protection in both occupational and nonoccupational settings. For example, the agency issued a series of temporary final rules aimed at managing the distribution and availability of PPE during the COVID-19 pandemic (FEMA, 2020). While these responsibilities do not conflict with NIOSH’s
authority for oversight of respiratory protection, they may affect the availability and provision of PPE, including respiratory protection, in emergency circumstances.
Respiratory Protection Supply Chain During the COVID-19 Pandemic: Experiences and Lessons Learned
In the face of the sudden surge in demand resulting from the COVID-19 pandemic, shortcomings in the supply chain for PPE were not a surprise. Demand-based N95 FFR production, overreliance on imports, and insufficient government coordination of PPE supply and distribution were all recognized issues during the 2009 H1N1 influenza pandemic and the 2014 Ebola virus epidemic (Patel et al., 2017). In 2017, CDC staff outlined strategies for improving the acquisition and use of PPE during a public health emergency. Their recommendations included the creation of additional stockpiles at the federal, state, and local levels; improved domestic manufacturing surge capacity at the time of an event; and improved sharing of situational and supply information between the federal government and the private sector (Patel et al., 2017). These strategies, however, were not implemented in the 3 years prior to the COVID-19 pandemic’s arrival in the United States. As evidenced by the scarcity of N95 FFRs throughout most of 2020 and as seen in previous pandemics and epidemics, global supply chains and just-in-time manufacturing undermine the nation’s ability to respond to sudden surges in demand.
N95 FFRs are currently manufactured in multiple countries worldwide. In the years leading up to the COVID-19 pandemic, U.S. companies transferred the vast majority (~90 percent) of N95 FFR production overseas (Dai et al., 2020). This global supply chain keeps costs down for manufacturers and consumers, but exposes respirator supply to external pressures. At the start of the COVID-19 outbreak, global shortages of respirators and other PPE products emerged as many affected countries imposed export controls and sought ways to boost domestic output (Cohen and Rodgers, 2020; Gruley and Clough, 2020).
In addition to global export fluctuations, respirator availability is limited by the industry’s embrace of just-in-time manufacturing and purchasing. Under that framework, goods are manufactured and purchased in limited quantities—enough to meet current demand without creating excess inventory. This approach helps suppliers control costs, but leaves them unable to respond to sudden spikes in demand (Gereffi, 2020; Kim, 2020; Whalen et al., 2020). In addition, the current just-in-time business model prioritizes products made in low-cost foreign locations, such as China (Gereffi, 2020), which adds export vulnerabilities to the limited supplies. For instance, the grounding of the container ship Evergreen in the Suez Canal
in March 2021 led to significant disruptions in the supply chain, since nearly 12 percent of the annual volume of world trade passes through the canal (Kumon, 2021). Moreover, manufacturers are not alone in reducing inventory; hospitals have adopted just-in-time purchasing of such items as N95 FFRs as a cost-saving measure (Gereffi, 2020; Whalen et al., 2020).
Surge manufacturing can help meet a sudden large and unpredictable demand, but it is relatively uncommon because of the costs of maintaining unused assembly lines. Following the epidemic of severe acute respiratory syndrome (SARS) of 2002–2003, 3M acknowledged that it was not equipped to handle spikes in demand and developed surge capacity in its respirator factories around the world (Gruley and Clough, 2020). However, the need generated by the COVID-19 pandemic outstripped 3M’s production surge for most of 2020.
Furthermore, even if manufacturers have surge capability to meet potential demands, production bottlenecks can slow output. Early in the COVID-19 pandemic, for example, the supply of meltblown nonwoven polypropylene, which serves as the primary filter material in N95 FFRs, quickly became a bottleneck (Gereffi, 2020; Handfield, 2020; Mendoza et al., 2020). Polypropylene is a commonly produced material, but creating meltblown nonwoven polypropylene fiber requires specialty machinery with a high capital investment (OECD, 2020), which limits the number of companies producing the fabric. The shortage of raw materials made it difficult for respirator manufacturers to quickly increase their N95 FFR supplies or switch to producing N95 FFRs to meet surging demand during the pandemic (Gereffi, 2020). To address this material shortage, new manufacturers entered the scene and developed partnerships to increase output. For example, a collaboration between Cummins Inc. and the Carbon Fiber Technology Facility at the Department of Energy’s Oak Ridge National Laboratory resulted in the capacity to manufacture enough filter media to produce more than 1 million face masks and respirators per day for use in health care facilities (ORNL, 2020). Additionally, the inherent challenges involved in producing certain respiratory protective devices, such as FFRs, that require molding during the manufacturing process can cause bottlenecks due to the expense and time demands of the molding process. Alternative designs using flat filters that do not require the use of molding equipment represent a design modification that could allow for improved surge capacity (Couch, 2021).
As the country headed into the COVID-19 pandemic in 2020, the SNS housed only 12 million N95 FFRs and 30 million surgical masks (Sun and Goldstein, 2020). To complicate matters, the PPE in the SNS had not been rotated out in a timely manner, resulting in respirators that were past their shelf life. Given the nationwide N95 FFR shortage, NIOSH examined the stockpile and recommended use of the expired N95 FFRs during the
pandemic (CDC, 2020). Also during the pandemic, NPPTL focused significant efforts on increasing the supply of respirators available to workers, conducting a series of limited assessments for respirators in the following categories: (1) respirators that are stockpiled beyond their shelf life, (2) respirators that purport to meet an international certification standard but are not NIOSH approved, (3) respirators that have been decontaminated, and (4) non-NIOSH-approved respirators produced by novel commercial equipment (NIOSH, 2021d).
Should the stockpile be replenished, product shelf life will continue to be an issue. Patel and colleagues (2017) recommend a strategic approach to stockpiling with expiration dates in mind: For products, such as respirators, with a 5-year shelf life, 20 percent of the required target number of products could be purchased annually over 5 years to achieve 100 percent of the target; in year 6, product would begin to be replenished (Patel et al., 2017). Improvements in respirator design (e.g., exchangeable elastics) could also potentially extend shelf life.
As supplies in the SNS dwindled during the COVID-19 pandemic, the SNS mission diminished in scope. In April 2020, the language on its website text changed. Until then, the website stated:
The Strategic National Stockpile is the nation’s largest supply of life-saving pharmaceuticals and medical supplies for use in a public health emergency severe enough to cause local supplies to run out…. When state, local, tribal, and territorial responders request federal assistance to support their response efforts, the stockpile ensures that the right medicines and supplies get to those who need them most during an emergency.
According to the revised language,
The Strategic National Stockpile’s role is to supplement state and local supplies during public health emergencies…. Many states have products stockpiled, as well. The supplies, medicines, and devices for life-saving care contained in the stockpile can be used as a short-term stopgap buffer when the immediate supply of adequate amounts of these materials may not be immediately available. (Blake, 2020)
This new emphasis on the SNS as a stopgap measure reflects the government’s inability to keep pace with the demand for PPE.
From the onset of the COVID-19 pandemic, the federal government has failed to coordinate PPE production and distribution. Early on, the SNS had inadequate supplies to meet the immediate need, and the Trump Administration did not use the DPA to increase supply. Thus instead of using the DPA to require U.S. manufacturers to share information and work together to ramp up N95 FFR production, the government allowed them to
continue to protect their manufacturing processes as intellectual property, making it difficult for new manufacturers to rapidly design and produce respirators that would meet NIOSH specifications (Contrera, 2020). In addition, the Trump Administration initially opted into private contracts for N95 FFR procurement, a strategy that led to unfulfilled obligations, fraud, and other criminal activity (Sinha, 2020). When the administration finally implemented the DPA for N95 FFRs, it was to require that manufacturers sell their products to the federal government. However, the federal government did not disperse an adequate supply of respirators to the states, which led to competition for the still-scarce respirators between states and the federal government (Anderson and Burris, 2021).
In March 2020, the federal government committed to spurring respirator production by purchasing 500 million N95 FFRs for the SNS. In its news release announcing the purchase, HHS acknowledged manufacturers’ hesitancy to produce respirators without a guaranteed market, stating, “These guaranteed orders offer reassurance to manufacturers that they will not be left with excess supplies if private sector orders are cancelled once the COVID-19 response subsides” (HHS, 2020, para. 2). The government also used the DPA to order 3M to import more than 166 million respirators. By May 2020, FEMA had issued more than $600 million in new contracts for N95 FFRs to both large U.S. suppliers (3M and Honeywell) and smaller entrants to the market (Gereffi, 2020).
Throughout 2020, U.S. respirator production and imports grew significantly. 3M quadrupled its monthly domestic manufacturing output from 22 million to 95 million respirators/month and doubled its worldwide annual output. The manufacturer also provided a total of 228.4 million N95 FFRs, KN95, and KN90 respirators from 3M plants in the Asia-Pacific (APAC) region for FEMA to import to the United States (3M, 2020). By 2021, 3M and Honeywell were producing a combined 120 million masks/month. Meanwhile, new manufacturers entered the respirator market, churning out millions of N95 FFRs, but not always finding customers (Jacobs, 2021). Major online retailers, trying to follow CDC’s request that N95 FFRs be reserved for health care workers, did not allow manufacturers to advertise N95 FFRs to the public. Meanwhile, major health care buyers preferred to work with well-known companies such as 3M and Honeywell, leaving new N95 FFR manufacturers with excess inventory and few customers (Jacobs, 2021). This disconnect led to continued scarcity for both the public and health care workers.
Despite increased production and imports, 12 months following the first recorded COVID-19 case in the United States, N95 FFRs were still difficult to come by for both health care workers and the public. Medical
professionals continued to ration their respirators, and N95 FFRs were sparsely available to the public (Noguchi, 2021).
In early 2021, the incoming Biden administration announced it would use the DPA to ramp up PPE manufacturing. In an executive order (“A Sustainable Public Health Supply Chain”), the administration directed agency heads to review the availability of critical supplies, such as N95 FFRs, and “take appropriate action using all available legal authorities, including the Defense Production Act, to fill those shortfalls as soon as practicable by acquiring additional stockpiles, improving distribution systems, building market capacity, or expanding the industrial base” (Executive Office of the President, 2021, sec. 2[B][ii]). The same executive order also directed the development of a new Pandemic Supply Chain Resilience Strategy, which was released in July 2021 (HHS, 2021a).
This massive push to acquire and stockpile PPE during the height of the COVID-19 pandemic later resulted in an excess of supplies as the number of cases began to drop, with hospitals and manufacturers sitting on inventory that exceeded the demand for respiratory protection. This glut in supplies was due in part to the nature of the contracts signed during the worst part of the pandemic. Since manufacturers had to rapidly ramp up the production of PPE in a short timeframe, hospitals had to sign “very large, multiyear contracts” to enable this level of production (West, 2021). As a result, manufacturers were left with large stockpiles of masks and other PPE that have become a major strain on their finances; in August 2021, Cardinal Health Inc. reported that this stockpile was one of the main contributors to a 40 percent drop in earnings in the most recent quarter (Smith, J., 2021).
OVERARCHING CONCLUSION
The gaps and overlaps in authority highlighted in this chapter point to the need for a framework for ensuring access to and effective use of respiratory protection by the public and all workers. The specific needs and challenges for workers and the public, respectively, are examined in the two chapters that follow.
REFERENCES
3M. 2020. 3M is dedicated to increasing supply to help protect citizens. https://www.3m.com/3M/en_US/company-us/coronavirus/us-policy-creation-supply-chain (accessed October 7, 2021).
Aagaard, T. S. 2011. Regulatory overlap, overlapping legal fields, and statutory discontinuities. Virginia Environmental Law Journal 29(3):237-303.
Anderson, E. D., and S. C. Burris. 2021. Assuring essential medical supplies during a pandemic: Using federal law to measure need, stimulate production, and coordinate distribution. In COVID-19 policy playbooks: Legal recommendations for a safer, more equitable future, edited by S. Burris, S. de Guia, L. Gable, D. E. Levin, W. E. Parmet, and N. P. Terry. Boston, MA: Public Health Law Watch.
Andrews, A. S., J. R. Powers, Jr., J. K. Cichowicz, C. C. Coffey, M. L. Fries, P. L. Yorio, and M. M. D’Alessandro. 2021. Respiratory protection in a time of crisis: NIOSH testing of international respiratory protective devices for emergency use. Health Security 19(4):379-385.
ANSI (American National Standards Institute). 2011. United States conformity assessment principles. https://ansi.org/uscap (accessed October 7, 2021).
ANSI. 2014. National conformity assessment principles for the U.S. https://www.standardsportal.org/usa_en/conformity_assessment/conformity_assessment.aspx (accessed October 7, 2021).
ANSI. 2021. About ANSI. https://www.ansi.org/about/introduction (accessed October 7, 2021).
ANSI. n.d. American National Standards: Value of the ANS designation. https://www.ansi.org/ansvalue (accessed December 29, 2021).
ASTHO (Association of State and Territorial Health Officials). 2021. Strategic National Stockpile. https://www.astho.org/Programs/Preparedness/Public-Health-Emergency-Law/Emergency-Use-Authorization-Toolkit/Strategic-National-Stockpile-Fact-Sheet (accessed September 2, 2021).
ASTM (ASTM International). 2021a. ASTM F2100-21, Standard specification for performance of materials used in medical face masks. West Conshohocken, PA: ASTM International. https://www.astm.org/f2100-21.html (accessed December 21, 2021).
ASTM. 2021b. ASTM F3407-21, standard test method for respirator fit capability for negative-pressure half-facepiece particulate respirators. West Conshohocken, PA: ASTM International. https://www.astm.org/f3407-21.html (accessed December 29, 2021).
ASTM. 2021c. ASTM F3502-21, standard specification for barrier face coverings. West Conshohocken, PA: ASTM International. http://www.astm.org/cgi-bin/resolver.cgi?F3502-21 (accessed December 29, 2021).
ATSDR (Agency for Toxic Substances and Disease Registry). 2018. ATSDR background and congressional mandates. https://www.atsdr.cdc.gov/about/congress.html (accessed October 1, 2021).
Berman, E. 2020. The roles of the state and federal governments in a pandemic. Journal of National Security Law & Policy 11:61-81.
Blake, A. 2020. The Trump administration just changed its description of the national stockpile to jibe with Jared Kushner’s controversial claim. The Washington Post, April 3. https://www.washingtonpost.com/politics/2020/04/03/jared-kushner-stands-trump-proceeds-offer-very-trumpian-claim-about-stockpiles (accessed October 7, 2021).
Bloom, A. S. 2019. DOL validates independent contractor relationships in the on-demand marketplace. Proskauer: Law and the Workplace, April 20. https://www.lawandtheworkplace.com/2019/04/dol-validates-independent-contractor-relationships-in-the-on-demand-marketplace (accessed October 7, 2021).
Blum, S. C. 2020. Federalism: Fault or feature—An analysis of whether the United States should implement a federal pandemic statute. Washburn Law Journal 60(1).
Carias, C., G. Rainisch, M. Shankar, B. B. Adhikari, D. L. Swerdlow, W. A. Bower, S. K. Pillai, M. I. Meltzer, and L. M. Koonin. 2015. Potential demand for respirators and surgical masks during a hypothetical influenza pandemic in the United States. Clinical Infectious Diseases 60:S42-S51.
CDC (Centers for Disease Control and Prevention). 2014. Receiving, distributing, and dispensing strategic national stockpile assets: Guide to preparedness, version 11. https://stacks.cdc.gov/view/cdc/77036 (accessed October 7, 2021).
CDC. 2019. Respiratory protection for residents reentering and/or cleaning homes that were flooded. https://www.cdc.gov/disasters/disease/respiratory.html (accessed September 1, 2021).
CDC. 2020. Release of stockpiled N95 filtering facepiece respirators beyond the manufacturer-designated shelf life: Considerations for the COVID-19 response. https://stacks.cdc.gov/view/cdc/86280 (accessed October 7, 2021).
CDC. 2021a. About NCEH. https://www.cdc.gov/nceh/information/about.htm (accessed September 1, 2021).
CDC. 2021b. What to wear before entering a home or building with mold damage. https://www.cdc.gov/mold/pdfs/What_to_Wear_Mold_Damage_Oct5_508c.pdf (accessed October 7, 2021).
CDC. 2021c. Order under section 361 of the Public Health Service Act (42 U.S.C. 264) and 42 code of federal regulations 70.2, 71.31(b), 71.32(b): Requirement for persons to wear masks while on conveyances and at transportation hubs. https://www.cdc.gov/quarantine/pdf/Mask-Order-CDC_GMTF_01-29-21-p.pdf (accessed October 7, 2021).
Chiwaya, N. 2021. Mask tracker: Does your state still require face masks? https://www.nbcnews.com/news/us-news/map-mask-mandate-tracker-2021-n1269023 (accessed September 1, 2021).
Coffey, C., and C. Miller. 2019. The respirator fit capability test: Enhancing the efficacy of filtering facepiece respirators. Synergist 9.
Coffey, C., L. Brosseau, M. E. B. Rogers, and J. Szalajda. 2021. Overview of the ASTM F3407 standard test method for respirator fit capability. NIOSH Science Blog. https://blogs.cdc.gov/niosh-science-blog/2021/01/26/astm-rfc-standard (accessed October 4, 2021).
Cohen, J., and Y. v. d. M. Rodgers. 2020. Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Preventive Medicine 141:106263.
Contrera, J. 2020. The N95 shortage America can’t seem to fix. The Washington Post, September 21. https://www.washingtonpost.com/graphics/2020/local/news/n-95-shortage-covid (accessed October 7, 2020).
Couch, E. 2021. Achieving high quality barrier face covering protection for lower-risk worker categories and public. Document provided to the Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces, Washington, DC, February 22, 2021. Available by request through the National Academies’ Public Access Records Office.
CPSC (Consumer Product Safety Commission). 2021. Coronavirus disease- (COVID-19) related products business guidance. https://www.cpsc.gov/COVID-19 (accessed September 2, 2021).
Dai, T., G. Bai, and G. F. Anderson. 2020. PPE supply chain needs data transparency and stress testing. Journal of General Internal Medicine 35(9):2748-2749.
D’Alessandro, M., and J. Peterson. 2020. Current issues in the assessment of respiratory protective devices: Nontraditional workers and public use. Presentation at workshop on Current Issues in the Assessment of Respiratory Protective Devices, Washington, DC, August 5.
de Perio, M. A., C. H. Dowell, L. J. Delaney, L. J. Radonovich, D. T. Kuhar, N. Gupta, A. Patel, S. K. Pillai, and M. D’Alessandro. 2020. Strategies for optimizing the supply of N95 filtering facepiece respirators during the coronavirus disease 2019 (COVID-19) pandemic. Disaster Medicine and Public Health Preparedness 14(5):658-669.
DHS (Department of Homeland Security). 2016. Nuclear/radiological incident annex to the response and recovery federal interagency operational plans, October 2016—Final. https://www.fema.gov/sites/default/files/2020-07/fema_incident-annex_nuclear-radiological.pdf (accessed October 7, 2021).
Dobbs, D. 2008. Law of torts. Eagan, MN: West Academic.
DOL (Department of Labor). 2021. OSHA offices by state. https://www.osha.gov/contactus/bystate (accessed September 1, 2021).
EPA (Environmental Protection Agency). 2021a. A brief guide to mold, moisture and your home. https://www.epa.gov/mold/brief-guide-mold-moisture-and-your-home (accessed October 1, 2021).
EPA. 2021b. How to order the infographic card on “reduce health risks in areas with wildfire smoke.” https://www.epa.gov/air-research/how-order-infographic-card-reduce-health-risks-areas-wildfire-smoke (accessed September 1, 2021).
EPA. 2021c. Indoor air and coronavirus (COVID-19). https://www.epa.gov/coronavirus/indoor-air-and-coronavirus-covid-19 (accessed September 1, 2021).
EPA. 2021d. Indoor air quality (IAQ). https://www.epa.gov/indoor-air-quality-iaq (accessed September 1, 2021).
EPA. 2021e. Smoke sense study: A citizen science project using a mobile app. https://www.epa.gov/air-research/smoke-sense-study-citizen-science-project-using-mobile-app (accessed September 1, 2021).
EPA. 2021f. Wildfires. https://www.epa.gov/natural-disasters/wildfires (accessed September 1, 2021).
European Commission. 2020. Conformity assessment procedures for protective equipment. https://ec.europa.eu/docsroom/documents/42311 (accessed October 7, 2021).
Executive Office of the President. 2021. A sustainable public health supply chain. https://www.whitehouse.gov/briefing-room/presidential-actions/2021/01/21/executive-order-a-sustainable-public-health-supply-chain (accessed October 7, 2021).
FDA (Food and Drug Administration). 2004. Surgicalmasks—Premarketnotification [510(k)]sub-missions. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/surgical-masks-premarket-notification-510k-submissions (accessed September 2, 2021).
FDA. 2007. Filtering facepiece respirator for use by the general public in public health medical emergencies—Class II special controls guidance for industry and FDA staff. https://www.fda.gov/medical-devices/guidance-documents-medical-devices-and-radiation-emitting-products/filtering-facepiece-respirator-use-general-public-public-health-medical-emergencies-class-ii-special#6 (accessed December 21, 2021).
FDA. 2009. Summary fact sheet for disposable respirators for use during the swine flu emergency. https://www.fda.gov/media/76708/download (accessed December 11, 2021).
FDA. 2017a. Is it really “FDA approved”? https://www.fda.gov/consumers/consumer-updates/it-really-fda-approved (accessed October 1, 2021).
FDA. 2017b. Memorandum of understanding between the Food and Drug Administration/Center for Devices & Radiological Health and the Centers for Disease Control & Prevention/National Institute for Occupational Safety & Health/National Personal Protective Technology Laboratory, MOU 225-18-006. https://www.fda.gov/about-fda/domestic-mous/mou-225-18-006 (accessed September 1, 2021).
FDA. 2020. Manufacturers of imported, non-NIOSH-approved disposable filtering facepiece respirators manufactured in China, health care personnel, hospital purchasing departments and distributors, importers and commercial wholesalers, and any other applicable stakeholders. https://www.fda.gov/media/136664/download (accessed December 13, 2021).
FDA. 2021a. Enforcement policy for face masks, barrier face coverings, face sheilds, surgical masks, and respirators during the coronavirus disease (COVID-19) public health emergency (revised). https://www.fda.gov/media/136449/download (accessed October 7, 2021).
FDA. 2021b. FAQs on Emergency Use Authorizations (EUAs) for medical devices during the COVID-19 pandemic. https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/faqs-emergency-use-authorizations-euas-medical-devices-during-covid-19-pandemic (accessed December 18, 2021).
FDA. 2021c. Manufacturers of imported, non-NIOSH-approved disposable filtering facepiece respirators, health care personnel, hospital purchasing departments and distributors, importers and commercial wholesalers; and any other applicable stakeholders. https://www.fda.gov/media/136403/download (accessed December 13, 2021).
FDA. 2021d. Recognized consensus standards. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfStandards/results.cfm (accessed November 7, 2021).
FEMA (Federal Emergency Management Agency). 2020. Prioritization and allocation of certain scarce and critical health and medical resources for domestic use. Federal Register Notice 85(215):86835-86843.
Friese, C. R., T. G. Veenema, J. S. Johnson, S. Jayaraman, J. C. Chang, and L. H. Clever. 2020. Respiratory protection considerations for healthcare workers during the COVID-19 pandemic. Health Security 18(3):237-240.
GAO (Government Accountability Office). 2011. Influenza pandemic: Lessons from the H1N1 pandemic should be incorporated into future planning. https://www.gao.gov/products/gao-11-632 (accessed September 2, 2021).
Garner, B. (Ed.). 2009. Black’s Law Dictionary, 9th ed. Eagan, MN: West Academic.
Gereffi, G. 2020. What does the COVID-19 pandemic teach us about global value chains? The case of medical supplies. Journal of International Business Policy 3:287-301.
Gerstein, D. M. 2020. The strategic national stockpile and COVID-19: Rethinking the stockpile. Testimony presented before the Senate Committee on Homeland Security and Governmental Affairs on June 24, 2020. RAND Corporation. https://www.rand.org/pubs/testimonies/CTA530-1.html (accessed October 7, 2021).
Gostin, L. O. 2003. The Model State Emergency Health Powers Act: Public health and civil liberties in a time of terrorism. Health Matrix 13(1).
Gruley, B., and R. Clough. 2020. How 3M plans to make more than a billion masks by end of the year. Bloomberg Businessweek, March 25. https://www.bloomberg.com/news/features/2020-03-25/3m-doubled-production-of-n95-face-masks-to-fight-coronavirus (accessed October 7, 2021).
Handfield, R. 2020. Where are all the N95 masks? A supply chain dilemma. https://scm.ncsu.edu/scm-articles/article/where-are-all-the-n95-masks-a-supply-chain-dilemma (accessed October 7, 2021).
HHS (Department of Health and Human Services). 2006. Report to Congress: Pandemic influenza preparedness spending. Conference Report 109-359. https://www.medicalcountermeasures.gov/BARDA/documents/hhspanfluspending-0606.pdf (accessed October 7, 2021).
HHS. 2020. HHS to procure N95 respirators to support healthcare workers in COVID-19 outbreaks. https://www.hhs.gov/about/news/2020/03/04/hhs-to-procure-n95-respirators-to-support-healthcare-workers-in-covid-19-outbreaks.html (accessed October 7, 2021).
HHS. 2021a. National strategy for a resilient public health supply chain. https://www.phe.gov/Preparedness/legal/Documents/National-Strategy-for-Resilient-Public-Health-Supply-Chain.pdf (accessed October 7, 2021).
HHS. 2021b. Personal protective equipment. https://www.phe.gov/about/sns/COVID/Pages/personal-protective-equipment.aspx (accessed September 2, 2021).
HHS. 2021c. Stockpile responses (SNS). https://www.phe.gov/about/sns/Pages/responses.aspx (accessed October 7, 2021).
IOM (Institute of Medicine). 2011. Certifying personal protective technologies: Improving worker safety. Washington, DC: The National Academies Press.
Irby, S., and E. Nelsen. 2020. Spurred by COVID-19, researcher Linsey Marrlinsey Marr evaluates efficacy of sterilized N95 respirators, alternative mask materials. https://eng.vt.edu/media-center/articles/2020/spurred-by-covid-19-researcher-linsey-marr-evaluates-efficacy-of-sterilized-n95-respirators-alternative-mask-materials.html (accessed October 4, 2021). ISO (International Organization for Standardization). 2021. Standards by ISO/TC 94/SC 15 respiratory protective devices. https://www.iso.org/committee/291088/x/catalogue (accessed October 7, 2021).
ISO/IEC (International Electrotechnical Commission). 2020. ISO/IEC 17000:2020 conformity assessment—Vocabulary and general principles. https://webstore.ansi.org/Standards/ISO/ISOIEC170002020?gclid=Cj0KCQjwl7qSBhD-ARIsACvV1X2CCyBgCV1V3Kml22msVh1FgLG9yIGCmS9zDPgqv9McdtkcQmsfJcEaAqTDEALw_wcB (accessed April 7, 2022).
Jacobs, A. 2021. Can’t find an N95 mask? This company has 30 million that it can’t sell. The New York Times, February 10. Updated May 29. https://www.nytimes.com/2021/02/10/health/covid-masks-china-united-states.html (accessed October 7, 2021).
Kim, A. 2020. Contributor: Made in NC—Reimagining the PPE supply chain and saving each other just in time. American Journal of Managed Care, November 5. https://www.ajmc.com/view/dr-peter-dicpinigaitis-discusses-the-state-of-chronic-cough-treatment (accessed October 7, 2021).
Kritchevsky, B. 2010. Tort law is state law: Why courts should distinguish state and federal law in negligence-per-se litigation. American University Law Review 60(1).
Kumon, T. 2021. Blocked Suez Canal raises new threat to global supply chains. Nikkei Asia, March 25. https://asia.nikkei.com/Business/Transportation/Blocked-Suez-Canal-raises-new-threat-to-global-supply-chains (accessed October 7, 2021).
Maciag, M. 2014. States with most government employees: Totals and per capita rates. https://www.governing.com/archive/states-most-government-workers-public-employees-by-job-type.html (accessed September 1, 2021).
Manning, A. 2020. Engineering lab at CSU transformed into testing site for COVID-19 medical protective gear. https://engr.source.colostate.edu/engineering-lab-at-csu-transformed-into-testing-site-for-covid-19-medical-protective-gear (accessed October 4, 2021).
McCullough, N. V. 2021. Presentation at the January 26, 2021, meeting of the National Academies of Sciences, Engineering, and Medicine Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces, virtual. https://www.nationalacademies.org/event/01-25-2021/respiratory-protection-for-the-public-and-workers-without-respiratory-protection-programs-at-their-workplaces-committee-meeting-3 (accessed September 28, 2021).
Mendoza, M., J. Linderman, T. Peipert, and I. Hwang. 2020. Scarcity of raw material still squeezes N95 mask makers. AP News, September 10. https://apnews.com/article/automated-insights-earnings-virus-outbreak-pandemics-1295eae6f73d1870a23cb8e2cb66ad05 (accessed October 7, 2021).
Michaels, D., and J. Barab. 2020. The Occupational Safety and Health Administration at 50: Protecting workers in a changing economy. American Journal of Public Health 110(5):631-635.
Miller, C. 2020. Presentation at the November 5, 2020, meeting of the National Academies of Sciences, Engineering, and Medicine Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. The nation’s medical countermeasure stockpile: Opportunities to improve the efficiency, effectiveness, and sustainability of the CDC strategic national stockpile: Workshop summary. Washington, DC: The National Academies Press.
NASEM. 2017. Integration of FDA and NIOSH processes used to evaluate respiratory protective devices for health care workers: Proceedings of a workshop. Washington, DC: The National Academies Press.
NASEM. 2021. Current issues in the assessment of respiratory protective devices for occupational and non-occupational uses: Proceedings of a workshop. Washington, DC: The National Academies Press.
NIOSH (National Institute for Occupational Safety and Health). 2017. National framework for personal protective equipment conformity assessment—Infrastructure. DHHS (NIOSH) Publication Number 2018-102. https://www.cdc.gov/niosh/docs/2018-102/default.html (accessed October 7, 2021).
NIOSH. 2018a. A guide to air-purifying respirators. https://www.cdc.gov/niosh/docs/2018-176 (accessed December 7, 2021).
NIOSH. 2018b. National Personal Protective Technology Laboratory factsheet. https://www.cdc.gov/niosh/docs/2018-141/pdfs/2018-141.pdf?id=10.26616/NIOSHPUB2018141 (accessed December 19, 2021).
NIOSH. 2018c. Section 1: NIOSH-approved respirators. https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/respsource1.html (accessed December 22, 2021).
NIOSH. 2020a. NIOSH conformity assessment letter to manufacturers. NIOSH CA 2020-1031. https://www.cdc.gov/niosh/npptl/resources/pressrel/letters/conformitymanuf/CA-2018-1010-R1.html (accessed October 4, 2021).
NIOSH. 2020b. Performance of stockpiled air-purifying respirators, facility two of ten: Inhalation and exhalation resistance and filtration efficiency performance. https://www.cdc.gov/niosh/npptl/ppecase/pdfs/PPE-CASE-Stockpile-2-v2-03012020-508.pdf (accessed October 7, 2021).
NIOSH. 2021a. Making masks for the workplace. https://www.cdc.gov/niosh/topics/emres/pandemic/default.html (accessed September 2, 2021).
NIOSH. 2021b. NPPTL respirator assessments to support the COVID-19 response. https://www.cdc.gov/niosh/npptl/respirators/testing/ExpiredN95results.html (accessed September 9, 2021).
NIOSH. 2021c. Respirator approval information. https://www.cdc.gov/niosh/npptl/RespApprovalInfo.html (accessed October 7, 2021).
NIOSH. 2021d. NPPTL respirator assessments to support the COVID-19 response. https://www.cdc.gov/niosh/npptl/respirators/testing/default.html (accessed November 5, 2021).
NIOSH and FDA (Food and Drug Administration). 2017. MOU 225-18-006. https://www.fda.gov/about-fda/domestic-mous/mou-225-18-006 (accessed December 17, 2021).
NIST (National Institute of Standards and Technology). 2020. Standards incorporated by reference. https://www.nist.gov/standardsgov/what-we-do/federal-policy-standards/sibr-database (accessed September 28, 2021).
Noguchi, Y. 2021. Why N95 masks are still in short supply in the U.S. Shots: Health News from NPR, January 27. https://www.npr.org/sections/health-shots/2021/01/27/960336778/why-n95-masks-are-still-in-short-supply-in-the-u-s (accessed October 7, 2021).
OECD (Organisation for Economic Co-operation and Development). 2020. The face mask global value chain in the COVID-19 outbreak: Evidence and policy lessons. https://www.oecd.org/coronavirus/policy-responses/the-face-mask-global-value-chain-in-the-covid-19-outbreak-evidence-and-policy-lessons-a4df866d (accessed October 7, 2020).
OMB (Office of Management and Budget). 1998. Circular No. A-119 revised: Memorandum for heads of executive departments and agencies. https://www.whitehouse.gov/wp-content/uploads/2017/11/Circular-119-1.pdf (accessed October 7, 2021).
OMB. 2016. Revision of OMB Circular No. A-119, federal participation in the development and use of voluntary consensus standards and in conformity assessment activities. Federal Register 81(17):4673-4674.
Oregon OSHA (Occupational Safety and Health). 2021a. Temporary rule on protection from wildfire smoke. https://osha.oregon.gov/OSHARules/adopted/2021/temp-rule-protection-from-wildfire-smoke.pdf (accessed October 7, 2021).
Oregon OSHA. 2021b. Oregon OSHA coordinating distribution of particulate respirators in light of wildfire smoke and emergency requirements. https://osha.oregon.gov/news/2021/Pages/nr2021-39.aspx (accessed October 7, 2021).
ORNL (Oak Ridge National Laboratory). 2020. Cummins Inc. and Oak Ridge National Laboratory collaboration enables capability to produce millions of face masks. https://www.ornl.gov/blog/cummins-inc-and-oak-ridge-national-laboratory-collaboration-enables-capability-produce (accessed October 7, 2021).
OSHA (Occupational Safety and Health Administration). 2021. Dir 2021–03 (CPL 03)—Revised national emphasis program—Coronavirus disease 2019 (COVID-19). https://www.osha.gov/sites/default/files/enforcement/directives/DIR_2021-03_CPL_03.pdf (accessed October 8, 2021).
Patel, A., M. M. D’Alessandro, K. J. Ireland, W. G. Burel, E. B. Wencil, and S. A. Rasmussen. 2017. Personal protective equipment supply chain: Lessons learned from recent public health emergency responses. Health Security 15(3):244-252.
Richards, E. P. 2020. A historical review of the state police powers and their relevance to the COVID-19 pandemic of 2020. Journal of National Security Law & Policy 11:83-105.
Rowell, A. 2021. The regulatory landscape regarding respiratory protection. Paper commissioned by the Committee on the Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces (see Appendix C).
RTI (RTI International). 2014. Third-party conformity assessment in the United States: Profiles of 14 public and private sector schemes. Document provided to the Committee on Respiratory Protection for the Public and Workers without Respiratory Protection Programs at their Workplaces on September 29, 2021. Available by request through the National Academies’ Public Access Records Office.
Schwartz, V. E., C. Silverman, and C. Appel. 2009. Respirators to the rescue: Why tort law should encourage, not deter, the manufacture of products that make us safer. American Journal of Trial Advocacy 33:13-69.
Sickbert-Bennett, E. E., J. M. Samet, S. E. Prince, H. Chen, K. L. Zeman, H. Tong, and W. D. Bennett. 2021. Fitted filtration efficiency of double masking during the COVID-19 pandemic. JAMA Internal Medicine 181(8):1126-1128.
Sinha, M. S. 2020. Strategies to address the chronic shortage of N95 masks and other filtering facepiece respirators during the COVID-19 pandemic. In COVID-19 policy playbook: Legal recommendations for a safer, more equitable future. Public Health Law Watch. Pp. 132-136. https://static1.squarespace.com/static/5956e16e6b8f5b8c45f1c216/t/6058f2719044b35649c1af67/1616441969874/Chp21-Sinha_COVIDPolicyPlaybook-March2021.pdf (accessed October 7, 2021).
Smith, A. 2021. Information request for NPPTL on respirator conformity assessment. Document provided to the Committee on Respiratory Protection for the Public and Workers Without Respiratory Protection Programs at Their Workplaces on September 29, 2021. Available by request through the National Academies’ Public Access Records Office.
Smith, J. 2021. COVID-19 medical stockpiles weigh on Cardinal Health results. The Wall Street Journal, August 6. https://www.wsj.com/articles/covid-19-medical-stockpiles-weigh-on-cardinal-health-results-11628282384 (accessed October 7, 2021).
State of Colorado Office of the Attorney General. 2021. Colorado business agrees to pay $70,000 to the state after misleading buyers about masks and respirators, price gouging during COVID-19 crisis. https://coag.gov/press-releases/1-25-21 (accessed September 2, 2021).
Sun, L. H. and A. Goldstein. 2020. Washington State asked the U.S. stockpile for coronavirus masks. The response raises concerns. The Washington Post, March 5. https://www.washingtonpost.com/health/2020/03/05/washington-state-asked-us-stockpile-coronavirus-masks-response-raises-concerns (accessed November 5, 2021).
Szalajda, J., J. O. Stull, and L. M. Brosseau. 2021. Overview of the ASTM F3502-21 barrier face covering standard. NIOSH Science Blog. https://blogs.cdc.gov/niosh-science-blog/2021/04/23/bfc-standard (accessed December 6, 2021).
Thaler, J. 2021. The next surges are here: What can American governments lawfully do in response to the ongoing COVID-19 pandemic? Mitchell Hamline Law Journal of Public Policy and Practice 42(1).
Tran, M., and R. K. Sokas. 2017. The gig economy and contingent work: An occupational health assessment. Journal of Occupational and Environmental Medicine 59(4):e63-e66.
UCI (University of California, Irvine). 2020. Aerosol Transmissible Disease (ATD) Program. https://ehs.uci.edu/programs/_pdf/biosafety/atd-program.pdf (accessed December 29, 2021).
Washington State Department of Labor and Industries. 2021. Washington administrative code 296-62-085 wildfire smoke. https://lni.wa.gov/safety-health/safety-rules/chapter-pdfs/WAC296-62.pdf#WAC_296_62_085 (accessed October 7, 2021).
West, M. G. 2021. New York hospitals now have stockpiles of personal protective equipment. The Wall Street Journal, July 1. https://www.wsj.com/articles/new-york-hospitals-now-have-stockpiles-of-personal-protective-equipment-11625159140 (accessed October 7, 2021).
Whalen, J., R. S. Helderman, and T. Hamburger. 2020. Inside America’s mask crunch: A slow government reaction and an industry wary of liability. The Washington Post, April 2. https://www.washingtonpost.com/politics/inside-americas-mask-crunch-a-slow-government-reaction-and-an-industry-wary-of-liability/2020/04/02/b3155e2a-6f85-11ea-aa80-c2470c6b2034_story.html (accessed October 7, 2021).
This page intentionally left blank.
















































