
8
Establishing a Culture of Continual Learning
Throughout this report, the committee has called for leaders to rely on systems thinking approaches to guide their efforts to restructure health care to improve quality and put patients at the center of care. But what does “systems thinking” really mean? And what beliefs, behaviors, and investments does it call upon? This chapter elucidates the concept and offers suggestions for putting it into practice, using the lens of a “learning health care system” (LHCS), a concept established in the National Academy of Medicine’s Learning Health System Series (NAM, 2018). In effect, an LHCS is an organization that uses continuous cycles of learning and reflection to inspire growth and development, involving all stakeholders—staff, managers, executives, clinicians, patients, communities, and others—in that enterprise. While the label and terminology of an LHCS are used most commonly in the United States and, more recently, in Europe, the fundamental components of such an organization are global, and examples exist in many countries.
Technologies and proper financing can be key technical tools to support an LHCS. The advances in digital technology in health care explored in Chapter 3 will be invaluable—indeed essential—in the health care systems of the future. So, too, can smart payer and government financing strategies that incentivize high-quality care, especially using universal health coverage (UHC) as a lever, as explored in Chapter 7. However, an LHCS’s most significant, core characteristics are not technical but cultural. The essence of an LHCS is an organizational ecosystem that enables and encourages continual learning, information exchange, and improvement, illustrated in the third level of the committee’s framework in Figure 2-2. The committee
believes an LHCS may be the best possible vehicle for health care leaders who choose to act on the recommendations offered in this report.
The first section of this chapter describes an LHCS, its underlying philosophy of continual improvement, how it is supported by sociotechnical systems theory and principles of human factors, and its benefits. The chapter then describes the essential components of an LHCS and suggests how these components shape the work of organizational leaders, using examples from around the world. Finally, the committee has highlighted areas throughout the report in which information and research are lacking. The third section of the chapter outlines a research and development agenda to provide the information needed to improve the picture of health care quality around the world. The chapter closes with a summary and recommendations.
WHAT IS A LEARNING HEALTH CARE SYSTEM?
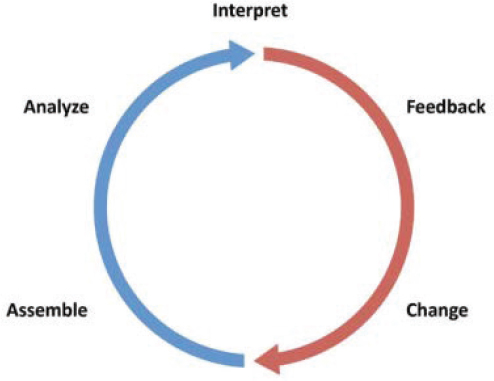
According to the Institute of Medicine, an LHCS is a system in which “science, informatics, and care culture align to generate new knowledge as an ongoing, natural by-product of the care experience, and seamlessly refine and deliver best practice for continuous improvement in health and health care” (IOM, 2011a, p. 1). An LHCS seeks to transform clinical care and better align people, processes, and technology by weaving continuous, rapid, and systematic evidence generation into routine medical practice (Smoyer et al., 2016). Although LHCSs have been implemented in various forms and at various scales, they all follow a cycle of “assembling, analyzing, and interpreting data, followed by feeding it back into practice” (Foley and Fairmichael, 2015, p. 4) to support productive change. Figure 8-1 depicts the learning cycle that characterizes an LHCS. Collecting data from routine patient care and using proper analytic techniques, learning organizations can feed back valuable and timely information to clinicians, public health officials, health care managers, and patients to help them continually improve the quality of health care (Foley and Fairmichael, 2015).
Although the LHCS label is relatively new, the concepts underlying an LHCS have a long history in the enterprise of health care quality improvement. In fact, the cycle depicted in Figure 8-1 is nearly identical to the “Plan, Do, Study, Act” cycle (AHRQ, 2015) that is familiar to many quality improvement experts and used worldwide in many industries. A “decision to study” lies at the base of the LHCS cycle, after which an LHCS will support the assembly and analysis of relevant data, ideally coming directly from routine work processes, patients, and health care workers. Interpretation of the data can provide lessons based on experience, which are immediately available for clinical decision support (Friedman and Macy, 2014).
SOURCE: Foley and Fairmichael, 2015.
This cycle of continual learning and action is rare today in health care systems around the world, despite the level of resources available. In some cases, resource-constrained environments are poised to become learning systems and generators of frugal innovations because they have no other choice. However, their growth will require time and investment, especially in the face of approaches that treat health system solutions as “magic bullets” instead of recognizing the need for long-term institutional and behavioral change (Morain et al., 2016). Conventionally, health care organizations rely on clinical research or health systems and services research to determine how to change care practices. However, this process of evidence generation and passive uptake can take years to develop and make its way into clinical practice. Conversely, an LHCS is a “change machine,” seeking to close the gap between knowledge and action and quicken the pace of change, supporting the rapid testing of best practices and lessons and their incorporation into routine clinical practice (IOM, 2011b). However, even these lessons will not happen overnight. In a Harvard Business Review article, the authors examine three innovation models at top health care institutions, finding that all of them report a challenge of navigating pressures to show immediate value (Bhatti et al., 2018). The committee recognizes that these organizational changes are not a quick fix and may take time to show return on investment. However, that does not mean they are not worth pursuing, as several health systems are already doing (see Box 8-1).
The Application of Principles of Sociotechnical Systems and Human Factors
Given the complex interplay among technologies, patients, health care workers, behavior, and organizational decision making (Friedman et al., 2015), an LHCS can best be achieved when fully informed by sociotechnical systems and human factors theories. In fact, an LHCS is a sociotechnical system (Foley and Fairmichael, 2015). Mastering and implementing the sociotechnical frameworks presented in Chapter 2, such as the Systems Engineering Initiative for Patient Safety (SEIPS) model,1 will help
___________________
1 The SEIPS model is a sociotechnical systems model that builds on the traditional Donabedian model of health care (Structure + Processes = Outcomes). By introducing sociotechnical systems theory, it expands on each component of the Donabedian model. The first, redubbed the “Work System,” is composed of technology, the organization, the environment, tasks, and the person. The second, still called “Processes,” takes into account care and other processes, such as administrative rules. The third, still termed “Outcomes,” takes into account patient and organizational outcomes (Carayon et al., 2006).
hospitals and health care facilities become LHCSs. The goal of an LHCS is to improve the work system and processes so as to improve outcomes by transforming clinical care. In addition to identifying failures and striving to reduce their occurrence, LHCSs can employ the elements of the “Safety II”2 approach toward resilient health care and work to understand what makes things go right in a complex, nonlinear health care system, leading to successful outcomes. An LHCS can engage with clinicians and all providers to identify and promote the characteristics and circumstances that lead to good care, and then make that information available to others to extend the network of learning. As argued in Chapter 2, an ideal health care system will strive for joint optimization, to the extent possible, for patients, health care workers, and the health care organization, rather than optimizing one at the expense of the others. Thus, an LHCS focuses its goals on the inner
___________________
2 Safety II is a new approach to understanding safety that acknowledges a provider’s “ability to succeed under varying conditions, so that the number of intended and acceptable outcomes is as high as possible” (Hollnagel et al., 2015).
two circles of the committee’s framework in Chapter 2 to optimize health care quality, often driven by circumstances in the outer circle.
As discussed in Chapters 2 and 3, a systems thinking approach to designing a health care system requires acknowledging human factors, which involve constant interactions among information, technology, and people (Roth et al., 2016). Human factors science can help everyone in an organization understand the strengths and vulnerabilities of human performance, help shape work processes to better support the people involved, and help present information in ways that make its interpretation and use easier and more reliable (Roth et al., 2016). Mastery of human factors science can result in far better designs that are much more capable of assuring quality.
Experience suggests that establishing LHCSs in low-resource settings is feasible. It may become even more feasible in the near future as digital health technologies burgeon, bringing technical expertise more quickly and at lower cost to places that formerly lacked such access.
Benefits of a Learning Health Care System
Although traditional approaches to improving health care quality, such as auditing, accreditation, inspections, and public reporting (when used in conjunction) are essential and have important and generally favorable effects on basic quality assurance (that is, reducing egregiously bad care), they are double-edged. When too heavily relied upon, surveillance, reward, and punishment can sometimes negatively reinforce quality improvement, and they can breed unwanted behaviors, such as misreporting of outcomes and bias in case selection. Moreover, if not used appropriately, they can create a culture of fear and blame, leading to health care that is compliant with minimal standards and reactive to adverse events. Furthermore, if such tools are not paired with feedback and guidelines for improvement, they can seem unnecessary and burdensome for health care workers, leading to disengagement with quality improvement efforts.
An LHCS is different, using positive reinforcement, long-term investment, and the celebration of teamwork to breed a culture of learning, not fear. An LHCS confers benefits to both providers and patients by emphasizing feedback and learning rather than mere surveillance (Wollaston, 2013). In addition, because LHCSs acknowledge that people are fallible and prone to making mistakes, they create a culture in which people freely report hazards, errors, and defects in care, opening the door to improvement and giving life to the Japanese phrase “every defect is a treasure” (IHI, 2018). Thus, with learning as a foundation, an LHCS will strive not just to meet quality benchmarks but to achieve improvements beyond them. It will measure not just static achievements but also rates of improvement over time.
THE COMPONENTS OF A LEARNING HEALTH CARE SYSTEM
Figure 8-1 depicts an LHCS as having five main components: (1) assembly of data, (2) analysis, (3) interpretation, (4) feedback, and (5) change. To support these components, an LHCS should be comprise various technical and system-level characteristics. These foundational elements of an LHCS are described in Table 8-1.
These LHCS components align well with and reinforce the committee’s design principles articulated in Chapter 2. Each has strong implications for the activities and investments by leaders in both wealthy and resource-limited settings. The committee’s remarks below elucidate which design principles these components particularly support and how they can function when resources are low.
Real-Time Access to Knowledge and Digital Capture of the Care Experience
The new digital era, as explored in Chapter 3, holds enormous promise for extending subject-matter expertise, such as specialty medical consultation, into low-income and austere environments far faster and at far lower cost relative to conventional care. The LHCS components of real-time access to knowledge and digital capture of the care experience embody an essential feature of the future of health care envisioned by the committee: Continuous feedback and learning generates knowledge to make decision making evidence-based and locally relevant, anticipatory, and cognizant of true sources of adverse events. This vision requires knowledge that is gathered rapidly and implemented quickly. Access to near-real-time knowledge (not just raw data) will bridge the “know-do” gap and act as the engine for the learning cycle. An LHCS attempting to offer real-time information collects information steadily from its own care processes. Information management is integrated into the workflow, rather than being layered on top of it. The result is that information is fresher, cleaner, and easier to interpret, and collecting it is far less burdensome.
However, paper-based records and reporting are still all too common in low- and middle-income countries (LMICs), impeding rapid reflection, adjustments, and growth. Digitizing the data and knowledge now commonly contained in paper-based records can make decision making and care delivery adjustments quicker and safer. For example, the Mobile Triage app developed by The Open Medicine Project in South Africa uses patient information to help nurses triage patients in emergency rooms. Typically, nurses use paper charts and calculate triage scores from memory, but as many as one in four patients in some settings may be incorrectly triaged
TABLE 8-1 Components of a Learning Health Care System
| Science and Informatics | |
| Real-time access to knowledge | A learning health system continuously and reliably captures, curates, and delivers the best available evidence to guide, support, tailor, and improve clinical decision making and care safety and quality. |
| Digital capture of the care experience | A learning health system captures the care experience on digital platforms for real-time generation and application of knowledge for care improvement. |
| Patient–Clinician Partnership | |
| Engaged, empowered patients | A learning health system is anchored on patient needs and perspectives and promotes the inclusion of patients, families, and other caregivers as vital members of the continuously learning care team. |
| Incentives | |
| Incentives aligned for value | A learning health system has incentives actively aligned to encourage continuous improvement, identify and reduce waste, and reward high-value care. |
| Full transparency | A learning health system systematically monitors the safety, quality, processes, prices, costs, and outcomes of care, and makes information available for care improvement and informed choices and decision making by clinicians, patients, and their families. |
| Continual Learning Culture | |
| Leadership-instilled culture of learning | A learning health system is stewarded by leadership committed to a culture of teamwork, collaboration, and adaptability in support of continuous learning as a core aim. |
| Supportive systems competencies | A learning health system constantly refines complex care operations and processes through ongoing team training and skill building, systems analysis and information development, and creation of the feedback loops for continuous learning and system improvement. |
SOURCE: Excerpted from NASEM, 2016, p. 121.
(The Open Medicine Project, 2014). The app can assist otherwise underresourced emergency centers in accurately screening and prioritizing patients, and it is already being used in 63 countries worldwide.
Related design principles:
- Decision making is evidence based and context specific.
- Care makes optimal use of technologies to be anticipatory and predictive at all system levels.
- Problems are addressed at the source, and patients and health care staff are empowered to solve them.
- The transformation of care delivery is driven by continuous feedback, learning, and improvement.
Engaged, Empowered Patients
The committee has spoken repeatedly about the centrality of the patient experience, the importance of streamlining the entire patient journey, and the value of co-design and co-production of health care systems with patients and communities. A commitment to these precepts requires both culture change, to shift the balance of power between those who give and those who receive care, and practice change, to support ongoing, authentic conversations among patients, caregivers, and the organizations that serve them. Empowerment, at the end of the day, comes from refocusing health care from the conventional question of “What is the matter with you?” to the modern question of “What matters to you?” (DiGloia et al., 2016).
Thus, the information needed by LHCSs includes not only clinical data but also information on the needs and perspectives of patients, families, and communities. This could include, for example, information on patients’ ability or inability to receive maternal and neonatal care at the same facility. Taking into account people’s perspectives, however, requires that the health care organization have the ability to inquire about what matters to them, and to incorporate their perspectives and those of their communities into the operations of the health care system at all levels, from clinical encounters, to improvement projects, to governance. This approach can lead to the development of a network of integrated health centers, such as was accomplished by Aprofe, a not-for-profit provider in Ecuador. Originally a provider of sexual and reproductive health care, Aprofe now provides surgical, maternal, and rural health care. This diversification of services occurred in part in response to demand from patients. The quality of services and patient-centered care provided at Aprofe clinics benefit the organization, as its customer base expands predominantly through patient referrals. In fact, Aprofe regularly implements improvements to person-centered care, such
as by conducting patient flow analysis to reduce wait times (Innovations in Healthcare, 2012).
Engaging and empowering patients, especially by leveraging digital tools they are already using, can also create opportunities to collect data, helping an LHCS better prioritize patients’ needs on their journey, determine how to structure care such that it is integrated and coordinated, and create a space for patients and health care workers to co-design care transformation. As a result, the purposeful act of empowering and engaging patients will help create a system that is easy and transparent to navigate.
Related design principles:
- Care delivery prioritizes the needs of patients, health care staff, and the larger community.
- Care is integrated and coordinated across the patient journey.
- Navigating the care delivery system is transparent and easy.
- Patients and health care staff co-design the transformation of care delivery and engage together in continual improvement.
Incentives Aligned for Value
The committee has emphasized the importance of systems thinking in redesigning care and the need for alignment of leadership, policy, culture, and incentives to deliver value. However, value can take on many meanings. In traditional quality discussions, value has the meaning of “value for money,” a catchphrase that has driven financing and payment away from volume and toward outcomes, as evidenced by the numerous pay-for-performance schemes now emerging globally. However, “value” can vary depending on the local context, necessitating contextually appropriate trade-offs.
To be able to deliver value, an LHCS will embrace and encourage new system designs that align the incentives of all parties. All too often, different parties (patients, health workers, administrators, and leaders) have competing priorities, which can foster fragmentation and myopia and inhibit learning. By striving for the joint optimization of outcomes among patients, health care workers, and the health care organization, an LHCS can improve value. For example, consider PurpleSource Healthcare in Lagos, Nigeria, described in Chapter 7. In Lagos, private health care is highly fragmented, with 90 percent of facilities being sole proprietorships. Poor management capacity, lack of quality assurance, and lack of access to finance lead to unsustainable business performance and poor patient outcomes. PurpleSource aggregates such facilities and deploys financial management, SafeCare quality certification, and technology solutions to integrate care across facilities. It also works with its patients to understand
what matters to them, and builds its services around those priorities. This alignment of patient and organizational needs places PurpleSource on the path to becoming one of the largest networks of health care providers in Nigeria (Center for Health Market Innovations, 2018b; Innovations in Healthcare, 2018; PharmAccess Foundation, 2016).
The value created can be further improved by capturing the care experience; providing real-time knowledge; and giving voice to patients, their families, and their communities. An LHCS will best thrive when payment methods support and reward alignment, teamwork across boundaries, and truly person-centered care. Thus, an LHCS should also embrace forms of financing that reward such activities and cooperation among caregivers. The era of UHC bodes well for smarter payment if nations leverage the potential of UHC policy and financial mechanisms, as discussed in Chapter 7.
Related design principles:
- Systems thinking drives the transformation and continual improvement of care delivery.
- Care delivery prioritizes the needs of patients, health care staff, and the larger community.
- Trade-offs in health care reflect societal values and priorities.
- Leadership, policy, culture, and incentives are aligned at all system levels to achieve quality aims, and to promote integrity, stewardship, and accountability.
Full Transparency
An LHCS should align and make transparent incentives to create value. Monitoring of information on quality, prices, and outcomes needs to be complemented by an effort to share the information. Without that dual effort, continuous feedback and learning cannot be achieved. Furthermore, without full transparency, investigation of adverse events will likely revert to outmoded root-cause point analysis instead of tracing the problem to longitudinal system sources.
Thus, transparency for an LHCS is a prerequisite for improvement. It can not only identify priority areas for focused improvement by highlighting problems, but also support identification of so-called “positive deviants,”3 organizations and systems that significantly outperform expectations. These
___________________
3 Positive deviancy denotes a behavioral and social change approach based on the observation that in a group or organization, individuals may use uncommon but successful strategies to deliver better solutions than their colleagues despite facing similar challenges and having no extra knowledge resources (Sternin and Coo, 2000). Positive deviancy thus serves as an asset-based approach (Baxter et al., 2015), and lessons developed from so-called “positive deviants” can be particularly valuable (Lawton et al., 2014).
organizations merit special study since they may offer breakthrough models and lessons on which others can build. For example, the positive deviance approach was used to identify and disseminate information that improved compliance with hand hygiene in Brazil (Marra et al., 2010), nurse–patient communication in Indonesia (Kim et al., 2008), and newborn care practices in Pakistan (Marsh et al., 2002). Sharing this information freely can facilitate broad uptake of the lessons as providers attempt to better themselves and patients self-select higher-performing providers. Similarly, transparency in an LHCS can serve as a foundation for productive exchange between providers and patients. In essence, it illuminates what matters in the patient journey and can direct where to strengthen efforts to simplify navigating the care process.
Transparency in an LHCS can produce positive externalities. For example, those who believe in the power of market forces to energize improvement will want patients, families, and health insurers (public or private) to see the relative performance of the providers from whom they can choose. Regulators will want to know which providers to inspect more thoroughly or with whom to intervene. And transparency can shine a light on corruption, which is a toxic impediment to the accountability, trust, and integrity of a system on which learning depends.
Related design principles:
- Navigating the care delivery system is transparent and easy.
- The transformation of care delivery is driven by continuous feedback, learning, and improvement.
Leadership-Instilled Culture of Learning
Developing an LHCS is a structural commitment to a culture of continual learning and improvement that has implications for all parties interacting with the health care system. In fact, many of the components of an LHCS can feel threatening and unwelcome. Empowered patients bring new demands and expectations. Measurement and transparency can be perceived as threats of blame and punishment. Incentives can seem like unjust sources of pressure. Improvement requires change, which a workforce can oppose if it seems infeasible or is not implemented strategically—or, most important, if it is not supported by an invested leadership. If an LHCS is to strive for continual learning and improvement, empowerment of patients, and transparency, a shift in organizational culture is needed. A key component of culture change for an LHCS is building a supportive and motivating culture, which takes time to accomplish. Without such a culture, obtaining buy-in from staff will be arduous, and changes made will not be sustainable. If done well, however, the building of such a culture can have posi-
tive and encouraging results. Project Fives Alive! in Ghana, for example, focused on harnessing the creativity of front-line workers and managers and having them solve problems at their level (Twum-Danso et al., 2012). It also used local data to identify problems and adapt the design of the system to improve, seeing mortality among children under 5 and infant mortality decline by one-third (Sodzi-Tettey et al., 2015).
The potential of this culture change has been demonstrated in a systematic review analyzing 62 studies (Braithwaite et al., 2017a). In more than 90 percent of the studies, the authors found organizational and workplace culture to be correlated with a range of patient health outcomes across multiple settings, nearly three-quarters of which were positive. For example, patient mortality rates were nearly 48 percent lower in hospitals with better nurse work environments in South Korea (Cho et al., 2015). These changes in culture offer tremendous opportunity for improvement. Finally, culture change must be led by motivated and dedicated leaders prepared to invest the appropriate resources (Morain et al., 2016). Health care leaders who want to cross the quality chasm documented in this report will consciously nurture the beliefs and behaviors essential for learning, such as curiosity, mutual trust, a willingness to try, systems knowledge, and transparency. They will do so by modeling such norms in their own daily behaviors and by coaching those who work for them to do the same. The committee sees no reason why these basic characteristics are any less applicable to leaders in resource-constrained settings than to those in wealthy ones. Indeed, one can find a growing number of examples in low-income settings of organizations that have begun to practice continual improvement and have reaped the benefits, as described previously in Box 8-1.
Related design principles:
- Leadership, policy, culture, and incentives are aligned at all system levels to achieve quality aims, and to promote integrity, stewardship, and accountability.
- Problems are addressed at the source, and patients and health care staff are empowered to solve them.
- The transformation of care delivery is supported by invested leaders.
Supportive System Competencies
Culture may be the “soft side” of transformation to an LHCS. Its partner is the “harder” side of supportive systems, both human and technological. To participate actively in continual improvement, the entire workforce can benefit from skills in understanding systems and processes; statistical thinking and data interpretation; teamwork; approaches to testing changes
on a small scale (e.g., “Plan-Do-Study-Act” cycles locally); and the establishment of new, more balanced relationships with patients and families. To streamline and improve processes, for example, Senegal recently tested the well-known 5S management method for improving the quality of health care services, and included it in its national strategy following a successful pilot project (Kanamori et al., 2015). Leaders can learn to study and assess their own work locally—right at the “sharp end” of care—and to embrace measurement as a friendly tool, not an outside threat. Modernized data systems, including new digital applications and telemedicine, can be invaluable, but they must be implemented with a systems approach in mind. Piecemeal pilots and ad hoc digital interventions over the past 15 years have proven that potential can be wasted if implementation, evaluation, and sustainability are not well designed at the outset. Methods for better analyzing and displaying data can help, as can collaborative structures within and among organizations in which people grappling with similar problems can exchange lessons, discovering that they know more together than they do separately. For example, the newly established program on Developing Excellence in Leadership, Training and Science Africa is aiming to shape and drive a locally relevant research agenda among 21 countries across the continent, creating a network of researchers poised for collaboration and information sharing (AESA, 2017). Such learning collaboratives have thrived in many low-resource settings, and have very likely accelerated improvement among their members.
Related design principles:
- Systems thinking drives the transformation and continual improvement of care delivery.
- Decision making is evidence based and context specific.
- Care is integrated and coordinated across the patient journey.
- The transformation of care delivery is driven by continuous feedback, learning, and improvement.
- The transformation of care delivery is a multidisciplinary process with adequate resources and support.
A RESEARCH AND DEVELOPMENT AGENDA
Throughout this report, the committee has identified gaps in knowledge about the prevalence, patterns, costs, and causes of and remedies for quality defects in global health care. Closing those gaps through research would help better inform policy, management, and practice, all of which should ideally be based on sound evidence. LHCSs generate and use evidence mainly in cycles of pragmatic, local action and reflection in real-world settings, rather than deriving evidence from formal experimental trials (English
et al., 2016). The distinction between the former evidence and that obtained through traditional randomized controlled trials and other formal designs is important, and sometimes controversial. The committee recognizes that both forms of evidence are valuable in pursuit of better care (Massoud et al., 2016). Additionally, given the massive increase in connectivity and the globalized nature of the world today, the research and development agenda outlined here need not be applied in silos across the world. Instead, to support the existing and emerging learning networks and collaboratives aiming to improve health care quality, there is also great potential for bidirectional information sharing, as discussed in Chapter 1. It is increasingly recognized that while countries may be different, health challenges and populations across borders can be quite similar. Researchers at the University of California, for example, are testing models for improving birth outcomes and have created sister programs in Fresno County, California, and five districts in Rwanda, partnering with the country’s Ministry of Health and universities (Evangelista, 2018). Together, they can compare models with similar populations and share lessons that emerge during the study. The Fresno program learned from Rwanda the importance of stakeholder engagement, for example, and the Rwandan team is interested in Fresno’s lessons on mental health, reduction of stress, and provision of psychosocial care. In this pursuit for better quality of care and better health outcomes globally, borderless research provides great opportunity (Evangelista, 2018).
Applying the findings from the research and development agenda outlined below will be another important step. The aims of an LHCS have much in common with the arena of study that has recently become known as “implementation science,” defined as
the use of strategies to adopt and integrate evidence-based health interventions and change practice patterns within certain settings (NIH, n.d.);
and
the study of methods to promote the integration of research findings and evidence into healthcare policy and practice (NICHSR, 2018).
Implementation science is thus about how to move good models into widespread use. And this is what an LHCS is about: generating practice-based evidence (from its own studies and those of others) and translating that knowledge into evidence-based practice that applies to the local contexts of the system. This relatively new discipline has the potential to develop and identify effective, evidence-based strategies and speed the translation of knowledge into practice. Examples of its application and utility in low-resource settings are already emerging, such as the integration
of implementation research into Population Health Implementation and Training partnership projects in five African countries. Ghana’s experience resulted in successful scale-up of effective practices, including reduction of neonatal mortality and improved data utilization, and added to understanding of the role of mentoring and coaching in improving the quality of care (Awoonor-Williams and Appiah-Denkyira, 2017). The committee supports the further development of and investments in implementation science.
Reflecting on findings in prior chapters, the committee proposes the following set of important research topics for the next decade to support the acceleration of care improvement globally. These topics fall into four general categories: (1) digital health care and measurement of quality, (2) applications and adaptations in LMICs, (3) payment and policy strategies to motivate and support improvement, and (4) organizational and clinical interventions to accelerate improvement.
Research on Digital Health Care and Measurement of Quality
Chapter 4 summarizes much of what is known about the prevalence and patterns of high and low quality globally. However, the endeavor to gather that information repeatedly encounters a dramatic deficit in reliable, high-quality data. Without such data, it will be difficult to target resources and interventions effectively. Along with that need is the complementary challenge of creating and adopting helpful metrics, especially in the coming age of digital health, as highlighted in Chapter 3. In the future the committee envisions, in which digital health care and traditional health care as a whole increasingly overlap, measuring the impact of digital health care on health outcomes will become vital. The committee highlights the following two questions in these arenas:
- What is the impact of the digitization of health care on population health outcomes?
- What innovative or proven models exist for local use of measurement for improvement?
Research on Applications and Adaptations in Low- and Middle-Income Countries
Questions about the quality of global care assume special forms in the context of LMICs. Effective forms of quality management and improvement in those settings need to be better understood. One particularly important related topic is corruption and its impact on health care quality, as emphasized in Chapter 6. Unfortunately, corruption, by its nature hidden and opaque, does not lend itself to easy measurement or research, and
thus its impact on care is not well understood. The committee is interested in the following four questions, the answers to which would yield a better understanding of the determinants of and some remedies for poor quality:
- What is the role of various actors in quality management across LMICs?
- Which digital health technologies can best contribute to better quality of care in resource-constrained settings?
- Do private markets reward higher quality?
- To what degree does corruption have effects on the quality of health care delivered in various settings? How can these effects best be mitigated?
Research on Payment and Policy Strategies to Motivate and Support Improvement
Chapters 5 and 7 identify several areas of major deficits in knowledge about strategies for improving the quality of care in specific settings and using specific levers. Chapter 5 identifies these deficits for settings of extreme adversity and for the informal sector, while Chapter 7 highlights uncertainties about the effects of policy and payment tools and raises questions about the roles that patients could play in demanding improvements in health care quality. The recent 2018 joint report of the World Health Organization (WHO), the World Bank, and the Organisation for Economic Co-operation and Development (OECD) (WHO et al., 2018) highlights seven categories of interventions employing policy, clinical, and cultural levers and represents a major step forward, but many questions continue to loom large. Six related questions emerged as of special interest to the committee:
- What 10 interventions are most likely to improve health care quality in settings of extreme adversity?
- What 10 interventions are most likely to improve the quality of care in the informal sector?
- What are the best strategies for addressing quality in fragmented settings, where most patients pay out of pocket?
- What strategies can reduce overuse of health care delivery services in low-resource settings, especially when regulatory capacity is limited or absent?
- How can strategic purchasing best help improve the quality of care delivery?
- What strategies are most effective in engaging patients and people in general to demand high-quality (and, especially, safe) care for themselves and their families?
Research on Organizational and Clinical Interventions to Accelerate Improvement
Much more needs to be known about optimizing strategies in local contexts and organizations. This is an area in which the LHCS and implementation science can become especially useful. Chapter 2 emphasizes the importance of using a systems approach to designing health care. But what, more precisely, does that mean for the daily work of health care leaders? Chapter 3 calls for a workforce with a vastly different skill set to meet the needs of the digital age in health care. But what skills are most valuable? Key questions for optimizing organizational strategies for quality improvement include the following:
- How can leaders implement a systems approach for improving the quality of health care in LMICs effectively and efficiently?
- What skill sets for the workforce are linked to better health outcomes for patients, especially in the coming digital age of health care?
SUMMARY AND RECOMMENDATIONS
The basic technical principles of systems thinking, quality improvement, and a learning organization are generic in that they apply to improvement at all levels and in all sizes of systems, from very local enterprises, such as one’s chess game or weaving, to very large-scale enterprises, such as national policy frameworks or the strategy of corporations. In the case of health care quality, this means the same approaches that can help improve antibiotic use in a clinic or pain control in surgery can also be used at the level of health care policy and finance. While this chapter on creating a learning culture focuses mainly on the clinical level—or the inner circles of the committee’s framework in Chapter 2—great opportunity lies in doing the same in the outer circle, with a focus on the environment affecting care. Clearly, conducting learning cycles at such a large scale can be daunting, but it is not out of reach for leaders who want to ensure that policy, like practice, is based to the extent possible on evidence and the continual growth of knowledge. Indeed, a nation that fails to learn from its trials of new policies and tactics is thereby at a disadvantage compared with nations that learn. For a health system, this cycle of learning will require a skilled clinical and nonclinical workforce able to actively co-design and co-produce care with patients and communities. In most nations and most organizations, the development of such a workforce will in turn require a profound cultural shift from reliance on inspection and punishment of “bad actors” and failures to
investments in transparency, openness, learning, and improvement. Examples of this potential already exist, as mentioned throughout this chapter:
- The positive deviance approach was used to identify and disseminate information that improved hand hygiene compliance in Brazil, nurse–patient communication in Indonesia, and newborn care practices in Pakistan.
- A project in Ghana focused on harnessing the creativity of frontline workers and managers, having them solve problems at their level, and used local data to identify problems and adapt the design of the system to improve. As a result, infant and child mortality declined by one-third.
- In South Korean hospitals where nurses experienced better work environments, patient mortality rates were nearly 48 percent lower.
At the same time, however, as with the many other topics across quality health care discussed in this report, context is important. The existing evidence and examples offer ideas and inspiration for other similar countries, but each learning health care system must take the elements outlined here and adapt them to its own local needs and priorities to see success.
Additionally, an enormous number of questions related to quality and the strength of the evidence supporting interventions remain unanswered. Given these gaps in knowledge and the importance of people’s health, the amount of funding directed toward quality control and quality improvement in health care, compared with that in other industries, is too low, and multifaceted and interdisciplinary investments are needed.
Conclusion: Realizing the benefits of a learning health care system will require a culture change in which learning is institutionalized and systemically rewarded. There are no “magic bullet” solutions. Instead, long-term investment and behavior change will be needed, adapted to the local context. All of those who work in a learning system help drive improvement of the system as a whole on behalf of the people and communities the system serves. And all understand what the desired outcomes are; how they contribute to these outcomes; and how and why to avoid suboptimizing their own department, specialty, or local organization at the expense of the whole.
Recommendation 8-1: Encourage a Culture of Learning to Fundamentally Redesign Health Care
Health care leaders in all settings should master and adopt the vision and culture of a learning health care system, striving for continual learning and avoiding an approach that relies primarily on blame and
shame. This learning system should extend beyond hospitals and providers to include patients, payers, administrators, community health workers, and others involved in health.
- Country governments should implement policies designed to effectively educate and supply health care professionals who are trained to provide high-quality care. These professionals should include a cadre of clinical and nonclinical leaders that are versed in creating a culture that rewards openness, transparency, and a commitment to improvement.
- Governmental and organizational leaders should ensure that efforts to create accountability in the health care system, though fundamental, do not create a culture of fear and reaction, which is inimical to system improvement and change. Performance in all domains of quality should be measured and reported transparently, and the results should be widely available to patients to encourage feedback and improvement over time.
- Governmental and organizational leaders should learn and use modern approaches to improving science, practice, and organizational culture.
- Nations, regions, and health systems should establish and maintain programs to facilitate shared, collaborative learning about improvements and innovations in health care.
- Leaders should ensure that health care systems harness new digital health technology to help reduce costs and improve care through real-time use of data.
Conclusion: There is a clear need for a much more locally relevant, robust research agenda related to quality of care. Investments are required to fund this agenda, which could have exponentially positive effects. A parallel investment to create a global learning community surrounding quality that can mobilize to share lessons and to understand what strategies and interventions to employ would multiply the benefits of that research.
Recommendation 8-2: Define and Mobilize a Research and Development Agenda
The U.S. National Institutes of Health, philanthropic organizations, and other bilateral donors, as well as low- and middle-income country (LMIC) governments and other stakeholders, should increase investments in research and development on interventions that would improve the quality of care at the system level, encompassing both primary and implementation research. The following questions should be priorities:
- What is the impact on population health outcomes of the digitization of health care?
- What innovative or proven models exist for local use of measurement for improvement?
- What are the roles of various actors in quality management across LMICs?
- Which digital health technologies can best contribute to better quality of care in resource-constrained settings?
- Do private markets reward higher quality?
- To what degree does corruption have effects on the quality of health care delivered in various settings? How can these effects best be mitigated?
- What 10 interventions are most likely to improve health care quality in settings of extreme adversity?
- What 10 interventions are most likely to improve the quality of care in the informal sector?
- What are the best strategies for addressing quality in fragmented settings where most patients pay out of pocket?
- What strategies can reduce overuse of health care services in low-resource settings, especially when regulatory capacity is limited or absent?
- How can strategic purchasing best help improve the quality of care delivery?
- What strategies are effective in engaging patients and people in general to demand high-quality (and, especially, safe) care for themselves and their families?
- How can leaders effectively and efficiently implement a systems approach for strengthening the quality of health care in LMICs?
- What skill sets for the workforce are linked to better health outcomes for patients, especially in the emerging digital age of health care?
REFERENCES
AESA (Alliance for Accelerating Excellence in Science in Africa). 2017. DELTAS Africa. https://aesa.ac.ke/programmes/deltas (accessed May 29, 2018).
AHRQ (Agency for Healthcare Research and Quality). 2015. Health literacy universal precautions toolkit, 2nd ed. https://www.ahrq.gov/professionals/quality-patient-safety/qualityresources/tools/literacy-toolkit/healthlittoolkit2-tool2b.html (accessed July 10, 2018).
Awoonor-Williams, J. K., and E. Appiah-Denkyira. 2017. Bridging the intervention-implementation gap in primary health care delivery: The critical role of integrated implementation research. BMC Health Services Research 17(Suppl. 3):772. doi:10.1186/s12913-017-2663-8.
Baobab Health. n.d. Software innovations. http://baobabhealth.org/?page_id=23 (accessed April 25, 2018).
Baxter, R., N. Taylor, I. Kellar, and R. Lawton. 2015. What methods are used to apply positive deviance within healthcare organisations? A systematic review. BMJ Quality & Safety 25(3):190–201. doi:10.1136/bmjqs-2015-004386.
Bhatti, Y., J. D. Castillo, K. Olson, and A. Darzi. 2018. Putting humans at the center of health care innovation. Harvard Business Review, March 2. https://hbr.org/2018/03/putting-humans-at-the-center-of-health-care-innovation (accessed July 10, 2018).
Braithwaite, J., J. Herkes, K. Ludlow, L. Testa, and G. Lamprell. 2017a. Association between organisational and workplace cultures, and patient outcomes: Systematic review. BMJ Open 7(11).
Braithwaite, J., R. Mannion, Y. Matsuyama, P. Shekelle, S. Whittaker, and S. Al-Adawi. 2017b. Health systems improvement across the globe: Success stories from 60 countries. Boca Raton, FL: CRC Press.
Braithwaite, J., E. Hollnagel, and R. L. Wears. 2018. Resilient health care. Boca Raton, FL: CRC Press.
Carayon, P., A. S. Hundt, B. T. Karsh, A. P. Gurses, C. J. Alvarado, M. Smith, and P. F. Brennan. 2006. Work system design for patient safety: The SEIPS model. Quality & Safety in Health Care 15(Suppl. 1):i50–i58.
Center for Health Market Innovations. 2018a. Boabab health trust. https://healthmarketinnovations.org/program/baobab-health-trust (accessed May 15, 2018).
Center for Health Market Innovations. 2018b. PurpleSource healthcare. https://healthmarketinnovations.org/program/purplesource-healthcare (accessed May 20, 2018).
Cho, E., D. M. Sloane, E.-Y. Kim, S. Kim, M. Choi, I. Y. Yoo, H. S. Lee, and L. H. Aiken. 2015. Effects of nurse staffing, work environments, and education on patient mortality: An observational study. International Journal of Nursing Studies 52(2):535–542.
DiGloia, A. M., S. B. Clayton, and M. B. Giarrusso. 2016. “What matters to you?”: A pilot project for implementing patient-centered care. Patient Experience Journal 3(2):7. http://pxjournal.org/journal/vol3/iss2/17 (accessed June 4, 2018).
English, M., G. Irimu, A. Agweyu, D. Gathara, J. Oliwa, P. Ayieko, F. Were, C. Paton, S. Tunis, and C. B. Forrest. 2016. Building learning health systems to accelerate research and improve outcomes of clinical care in low- and middle-income countries. PLoS Medicine 13(4):e1001991.
Evangelista, A. 2018. In health research, local efforts have global benefit. http://ucghi.universityofcalifornia.edu/news/health-research-local-efforts-have-global-benefit (accessed June 20, 2018).
Foley, T., and F. Fairmichael. 2015. The potential of learning healthcare systems. http://www.learninghealthcareproject.org/LHS_Report_2015.pdf (accessed June 4, 2018).
Friedman, C. P., and J. J. Macy. 2014. Toward complete & sustainable learning systems. Paper presented at University of Michigan. https://medicine.umich.edu/sites/default/files/2014_12_08-Friedman-IOM%20LHS.pdf (accessed June 4, 2018).
Friedman, C., J. Rubin, J. Brown, M. Buntin, M. Corn, L. Etheredge, C. Gunter, M. Musen, R. Platt, W. Stead. 2015. Toward a science of learning systems: A research agenda for the high-functioning learning health system. Journal of the American Medical Informatics Association 22(1):43–50.
Hollnagel, E., R. L. Wears, and J. Braithwaite. 2015. From Safety-I to Safety-II: A white paper. Denmark, UK: University of Southern Denmark; Gainesville: University of Florida; and Sydney, Australia: Macquarie University. https://www.england.nhs.uk/signuptosafety/wp-content/uploads/sites/16/2015/10/safety-1-safety-2-whte-papr.pdf (accessed August 10, 2018).
IHI (Institute for Healthcare Improvement). 2018. Treat every defect as a treasure. http://www.ihi.org/resources/Pages/ImprovementStories/TreatEveryDefectasaTreasure.aspx (accessed May 20, 2018).
Innovations in Healthcare. 2012. Aprofe. Durham, NC: Innovations in Healthcare.
Innovations in Healthcare. 2018. PurpleSource. https://www.innovationsinhealthcare.org/profile/purplesource (accessed May 20, 2018).
IOM (Instute of Medicine). 2011a. Digital infrastructure for the learning health system: The foundation for continuous improvement in health and health care—workshop highlights. http://www.nationalacademies.org/hmd/~/media/Files/Report%20Files/2010/Digital-Infrastructure-for-the-Learning-Health-System/Digital%20Infrastructure%20Workshop%20Highlights.pdf (accessed April 10, 2018).
IOM. 2011b. The learning health system and its innovation collaboratives: Update report. Washington, DC: The National Academies Press.
Irimu, G., M. Ogero, G. Mbevi, A. Agweyu, S. Akech, T. Julius, R. Nyamai, D. Githang’a, P. Ayieko, and M. English. 2018. Approaching quality improvement at scale: A learning health system approach in Kenya. Archives of Disease in Childhood. doi:10.1136/archdischild-2017-314348.
Kanamori, S., S. Sow, M. C. Castro, R. Matsuno, A. Tsuru, and M. Jimba. 2015. Implementation of 5S management method for lean healthcare at a health center in Senegal: A qualitative study of staff perception. Global Health Action 8:27256.
Kim, Y. M., M. Heerey, and A. Kols. 2008. Factors that enable nurse–patient communication in a family planning context: A positive deviance study. International Journal of Nursing Studies 45(10):1411–1421.
Lawton, R., N. Taylor, R. Clay-Williams, and J. Braithwaite. 2014. Positive deviance: A different approach to achieving patient safety. BMJ Quality & Safety 23(11):880.
Marra, A. R., L. R. Guastelli, C. M. de Araujo, J. L. dos Santos, L. C. Lamblet, M. Silva, Jr., G. de Lima, R. G. Cal, A. T. Paes, M. Cendoroglo Neto. 2010. Positive deviance: A new strategy for improving hand hygiene compliance. Infection Control & Hospital Epidemiology 31(1):12–20.
Marsh, D. R., M. Sternin, R. Khadduri, T. Ihsan, R. Nazir, A. Bari, and K. Lapping. 2002. Identification of model newborn care practices through a positive deviance inquiry to guide behavior-change interventions in Haripur, Pakistan. Food and Nutrition Bulletin 23(4 Suppl.):109–118.
Massoud, M. R., D. Barry, A. Murphy, Y. Albrecht, S. Sax, and M. Parchman. 2016. How do we learn about improving health care: A call for a new epistemological paradigm. International Journal for Quality in Health Care 28(3):420–424.
Morain, S. R., N. E. Kass, and C. Grossmann. 2016. What allows a health care system to become a learning health care system: Results from interviews with health system leaders. Learning Health Systems 1(1):e10015.
NAM (National Academy of Medicine). 2018. The learning health system series: Continuous improvement and innovation in health and health care. https://nam.edu/programs/value-science-driven-health-care/learning-health-system-series (accessed April 20, 2018).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. A national trauma care system: Integrating military and civilian trauma systems to achieve zero preventable deaths after injury. Washington, DC: The National Academies Press.
NICHSR (National Information Center on Health Services Research and Health Care Technology). 2018. Dissemination and implementation science. https://www.nlm.nih.gov/hsrinfo/implementation_science.html (accessed June 20, 2018).
NIH (National Institutes of Health). n.d. NIH PAR 07-086: Dissemination and implementation research in health (R01). https://grants.nih.gov/grants/guide/pa-files/PAR-07-086.html (accessed July 10, 2018).
PharmAccess Foundation. 2016. PharmAccess partners with PurpleSource healthcare in Nigeria. https://www.pharmaccess.org/update/pharmaccess-partners-with-purplesource-healthcare-in-nigeria (accessed June 4, 2018).
Roth, M. G., J. C. Rubin, K. Omollo, C. P. Friedman, and F. J. Seagull. 2016. The learning health-system: A new frontier for human factors. Proceedings of the International Symposium on Human Factors and Ergonomics in Health Care 5(1):141–144.
Smoyer, W. E., P. J. Embi, and S. Moffatt-Bruce. 2016. Creating local learning health systems: Think globally, act locally. Journal of the American Medical Association 316(23):2481–2482.
Sodzi-Tettey, S., N. A. Y. Twum-Danso, L. N. Mobisson-Etuk, L. H. Macy, J. Roessner, and P. M. Barker. 2015. Lessons learned from Ghana’s Project Fives Alive!: A practical guide for designing and executing large-scale improvement initiatives. Cambridge, MA: Institute for Healthcare Improvement.
Sternin, J., and R. Coo. 2000. The power of positive deviancy. https://hbr.org/2000/01/the-power-of-positive-deviancy (accessed May 15, 2018).
The Open Medicine Project. 2014. Mobile triage app. http://openmedicineproject.org/photogallery/mobile-triage-app (accessed May 24, 2018).
Twum-Danso, N. A. Y., G. B. Akanlu, E. Osafo, S. Sodzi-Tettey, R. O. Boadu, S. Atinbire, A. Adondiwo, I. Amenga-Etego, F. Ashagbley, and E. A. Boadu. 2012. A nationwide quality improvement project to accelerate Ghana’s progress toward Millennium Development Goal four: Design and implementation progress. International Journal for Quality in Health Care 24(6):601–611.
WHO (World Health Organization), OECD (Organisation for Economic Co-operation and Development), and World Bank. 2018. Delivering quality health services: A global imperative for universal health coverage. Geneva, Switzerland: WHO, OECD, and World Bank.
Wollaston, S. 2013. Why a culture of fear and blame won’t fix the NHS. The Telegraph, August 7. https://www.telegraph.co.uk/news/politics/10228052/Why-a-culture-of-fearand-blame-wont-fix-the-NHS.html (accessed June 4, 2018).
























